The Key Elements of Stroke Rehabilitation: Mark Bayley MD FRCPC
|
|
|
- Leonard Simmons
- 10 years ago
- Views:
Transcription


1 The Key Elements of Stroke Rehabilitation: Mark Bayley MD FRCPC 1

2 Presenter Disclosure Information Presenter: Mark Bayley Associate Professor, University of Toronto and Medical Director, Neuro Rehabilitation, Toronto Rehabilitation Institute FINANCIAL DISCLOSURE: I have no conflicts of interest to declare with this material UNLABELED/UNAPPROVED USES DISCLOSURE: None 2

3 Some Miracle Happens Understanding the Black Box of Stroke Rehabilitation 3

4 Objectives for Presentation By the end of this presentation participants will be able to 1. Name main mechanisms of recovery after stroke 2. Identify important elements of Continuum of Stroke Care 3. To identify some important gaps in care particularly for those with severe stroke and for community based survivors 4

5 Objective 1 Mechanisms for Recovery after stroke 5

6 Mechanisms of Recovery Resolution of Temporary Factors Central Nervous System Reorganization 6

7 Resolution of Temporary Phenomena Resolution of edema Resolution of ischemic penumbra A focal ischemic injury consists of a core of low blood flow which eventually infarcts (Astrup et al 1981, Lyden and Zivin 2000), surrounded by a region of moderate blood flow, known as the ischemic penumbra (Astrup et al 1981, Lyden and Zivin 2000), which is at risk of infarction but is still salvageable 7
, which is at risk of infarction but is still")
8 Resolution of Diaschisis 8

9 Crossed Cerebellar Diaschisis 9

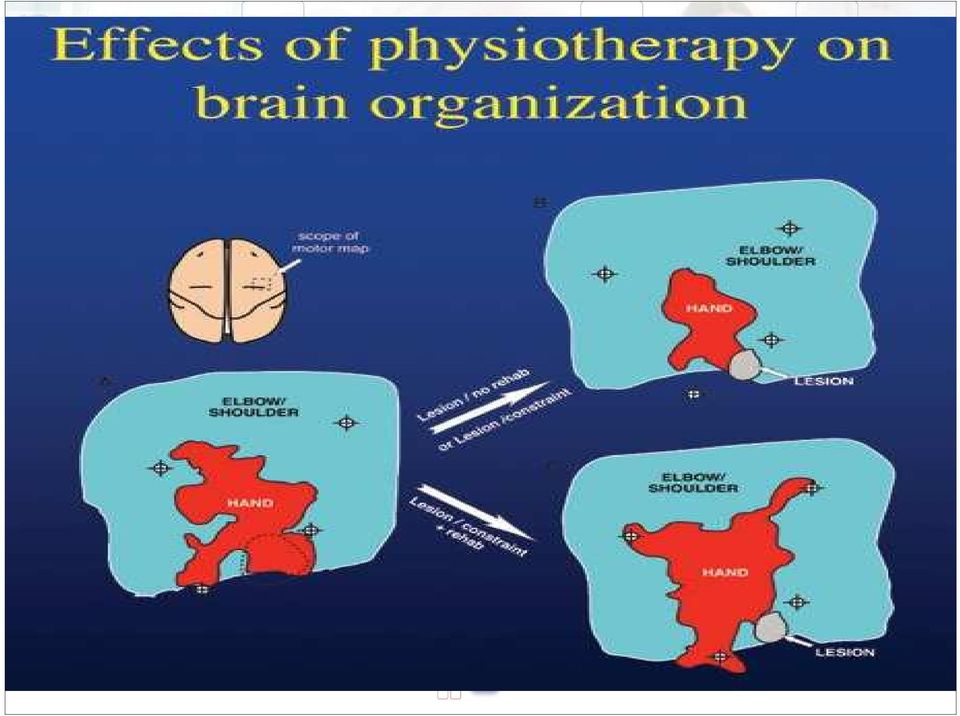
10 Mechanism 2-2 Brain Reorganization Nudo (2003), based on animal research, suggested that changes occurring during motor learning, are likely the same type of changes that occur during this part of recovery from stroke 10

11 CNS Reorganization and Plasticity Axonal Sprouting 11

12 Plasticity Concepts 12
13 Activation of the Other Hemisphere of Brain on FMRI 13

14 Local Processes Resolution of edema Resolution of ischemic penumbra Resolution of remote functional depression (diaschisis) Time course of Recovery Weeks to 2 months Hours to weeks Days to months CNS Reorganization Weeks to months 14

15 Objective 2 Identify key elements of stroke rehabilitation system 15

16 16

17 Best practice recommendation 5.2: Provision of Inpatient stroke rehabilitation All patients with stroke who are admitted to hospital and who require rehabilitation should be treated in a comprehensive or rehabilitation stroke unit by an interdisciplinary team [Evidence Level A] 17

18 Models of Stroke Care that have Been Studied General Medical Ward Acute Stroke Units Combined acute and subacute stroke units ( also known as Integrated Stroke Units) Subacute Stroke Rehab units Roving/Mobile Stroke Teams 18
 Subacute Stroke Rehab units Roving/Mobile Stroke")
19 Acute Stroke Units Geographic Unit with specialized teams. Patients on the stroke unit were treated medically more aggressively including increased use of parenteral fluids and antibiotics (Ronning) Combined Acute/Subacute Units Integrated specialized interdisciplinary combined acute and rehabilitation stroke units Heterogeneous definitions of SU Variations in timing of onset and patients admitted 19

20 Subacute Stroke Rehabilitation Units Geographically distinct units with focus on rehabilitation sometimes in freestanding hospitals Most studies involve moderate or severe stroke patients 20

21 Roving or Mobile Stroke Teams Langhorne et al. (2005) conducted a systematic review of mobile stroke teams evaluating studies which compared care provided by a mobile team of specialized stroke professionals on various wards versus alternative forms of stroke rehabilitation, 21
22 Pooled Analysis for Death and Dependency Model of Care OR (95% CI) Acute stroke care 0.70 (0.56, 0.86) Combined acute 0.56(0.44, 0.7 and subacute Subacute Rehab 0.63 (0.48,0.83) Mobile stroke team 1.00 (0.73, 1.38) Overall 0.68 ( ) 22
23 Stroke Rehab Units Stroke rehab units discharge stroke patients with fewer neurological deficits, improved ADL, reduced mortality and greater chance of being at home NB: For Every 13 patients treated in a stroke rehab unit, 1 patient is saved from death or dependence 23
24 Best practice recommendation 5.2 ( Cont d): Provision of Inpatient stroke rehabilitation i. Post acute stroke care should be delivered in a setting in which rehabilitation care is formally coordinated and organized [Evidence Level A] ii. All patients should be referred to a specialist rehabilitation team on a geographically defined unit as soon as possible after admission [Evidence Level A] (RCP). 24
25 PSROP (Post-Stroke Rehabilitation Outcomes Project) Study of 7 stroke rehab centers (6 in United States, n=1161; 1 in New Zealand, n=130) Comprehensive study of stroke rehabilitation examining the black box PSROP study, Archives of PM&R Dec 2005 suppl 25
26 What did the more efficient Stroke centers do? Admitted to specialized inter-disciplinary stroke rehab units Admitted earlier and more disabled More intensive therapy (incl. W/E) Less time in assessments Move to high level tasks early Well developed outpatient services 26
27 The Earlier the Better 27
28 The Earlier the Better Brain is primed to recover early in poststroke period Animal studies suggest there is a time window when brain is primed for maximal response to rehab therapies Delays are detrimental to recovery Clinical association between early admission to rehab and better outcomes 28
29 Benefit of Early Therapy in Animals Methods: Biernaskie et al. (2004) subjected rats to rehab x 5 weeks beginning at 5, 14 and 30 days post small strokes Control animals social housing 29
30 Benefit of Early Therapy in Animals- Results: All received 5 weeks of enriched environment Day 5 admission marked improvement Day 14 moderate improvement Day 30 no improvement vs. controls Corresponding cortical reorganization in brain around stroke 30
31 Therapy Intensity 31
32 % D/C SRU GMU Weeks 32
33 * OT PT SRU GMW 33 Mean hrs/pt
34 In German and Swiss centers, the rehabilitation programs were strictly timed (therapists had less freedom), while in UK and Belgian centers they were organized on an ad hoc basis (therapists had more freedom to decide)! No differences were found in the content of physiotherapy and occupational therapy More formal management in the German center may have resulted in the most efficient use of human resources, which may have resulted in more therapy time for the patients De Wit et al. Stroke 2007:38:
35 In a therapeutic day >50% time in bed 28% sitting out of bed 13% in therapeutic activities Alone for 60% of the time (Inactive and alone, Bernhardt et al, Stroke 2004) Contrary to the evidence that increased activity and environmental stimulation is 35 important to neurological recovery
36 Reality Check: Therapy is Cheap; LOS is Not Therapists are not replaced when sick or absent Laissez-faire attitude towards rehab therapies even though it is what we are supposed to be doing At least 60% of stroke rehab budget costs are nursing (versus <20% of core therapies) which have better developed accountabilities Stroke rehab patient gets an average of a little over one hour of therapy per day 36
37 Task-Specific Directed Stimulation 37
38 Stroke Rehab Must Be Task-Specific To be most effective rehab needs to be task-specific, focusing on tasks important and meaningful to the patient e.g. Obstacle Courses Sit-to Stand Training Aerobic Training 38
39 Best practice recommendation 5.3: Components of inpatient stroke rehabilitation All patients with stroke should begin rehabilitation therapy as early as possible once medical stability is reached [Evidence Level A] (ASA). i. Patients should receive the intensity and duration of clinically relevant therapy defined in their individualized rehabilitation plan and appropriate to their needs [Evidence Level A]. ii. Stroke patients should receive, through an individualized treatment plan, a minimum of 1 hour of direct therapy by the interprofessional stroke team for each relevant core therapy, for a minimum of 5 days per week based on individual need and tolerance [Evidence Level A] with duration of therapy being dependent on stroke severity [Evidence Level C]. iii. The team should promote the practice of skills gained in therapy into the patient s daily routine in a consistent manner [Evidence Level A]. iv. Therapy should include repetitive and intense use of novel tasks that challenge the patient to acquire necessary motor skills to use the involved limb during functional tasks and activities [Evidence Level A] 39
40 Best practice recommendation 5.3: Components of inpatient stroke rehabilitation v. Stroke unit teams should conduct at least one formal interdisciplinary meeting per week at which patient problems are identified, rehabilitation goals set, progress monitored and support after discharge planned [Evidence Level B] vi. The care management plan should include a predischarge needs assessment to ensure a smooth transition from rehabilitation back to the community. Elements of discharge planning should include home visit by a health care professional, Determine equipment needs and home modifications, begin caregiver training NB Care Pathways do not seem to improve outcomes 40
41 First Story 41
42 Objective 3 To identify some important gaps in care particularly for those with severe stroke and for community based survivors 42
43 Should More Severe Strokes be Rehabilitated? 43
44 Rehab of Severe Strokes Patients with severe strokes improve to a lesser degree and at slower rate Multiple trials demonstrated severe strokes receiving rehab are more likely to be discharged home, have shorter LOS and reduced mortality rates Benefit of rehab more prevention of complications and improved discharge planning 44
45 Jorgensen et al. (2000) Comparative trial N = 1241 consecutive stroke patients Group 1 (n = 305) - general and neurological wards Group 2 (n = 936) - single stroke unit Patients similar in two groups 88% of all strokes admitted to hospital 45
46 Jorgensen et al. (2000) Relative risks of poor outcome (mortality or nursing home discharge) reduced by 47% on stroke unit For severe strokes poor outcome reduced by 86%; relative risk of 1 and 5 year mortality reduced by 40% and 70% Authors attributed it to an interdisciplinary rehab approach 46
47 Rehab of Severe Strokes 196 nonambulatory stroke patients with mean FIM 46 at day 56, avg age 72 admitted to a special stroke rehab unit Received daily therapy all disciplines in an interdisciplinary setting FIM increased from 46 to 70 in mean rehab stay of 88 days (FIM efficiency =.27) 43% were discharged home; savings were $4 for every $1 spent on rehab and home care Teasell et al
48 Should there be Slow Stream? Also Known in Toronto as Low Tolerance Long Duration Typically occurring in Complex Continuing Care Typical Maximum amount of therapy is 150 minutes per week 48
49 Severe Strokes Admission Motor FIM (RPG 1100, 1110) Fiscal 09/ Mean Acute LOS Mean Rehab LOS Mean FIM change E-Stroke Data HTSD 49 LTLD
50 Story 2-2 Milder Stroke 50
51 Outpatient Therapy Outpatient therapy improves short-term functional outcomes Hospital same as home-based Outpatient therapy is relatively inexpensive (1 PT/1 OT/0.5 SLP/0.5 SW = cost of 1 rehab inpt bed) Reduces rehospitalization and allows earlier discharge home Estimated savings is $2 for every $1 spent on outpatient therapies 51
52 Cochrane Review of Outpatient Rehab 14 RCTs of 1,617 patients (Outpatient Trialists 2003) involved in home based, day hospital and outpatient clinic Therapy reduced the odds of a poor outcome (death, deterioration or dependency) (OR 0.72; 95% CI ; p=0.009) Number needed to treat in order to spare one person from experiencing a poor outcome was 14 52
53 Best practice recommendation 5.4: Outpatient and community-based rehabilitation After leaving hospital, stroke survivors must have access to specialized stroke care and rehabilitation services appropriate to their needs (acute and/or inpatient rehabilitation) [Evidence Level A] 53
54 Best practice recommendation 5.4: Outpatient and community-based rehabilitation iii. Multifactorial interventions provided in the community including an individually prescribed exercise program, may be provided for people who are at risk of falling, in order to prevent or reduce the number and severity of falls [Evidence Level A]. iv. People with difficulties in mobility should be offered an exercise program and monitored throughout the program [Level B] v. Patients with aphasia should be taught supportive conversation techniques [Evidence Level A] vi. Patients with dysphagia should be offered swallowing therapy and opportunity for reassessment as required [Level A] 54
55 Best practice recommendation 5.5: Follow-up and community reintegration People with stroke living in the community should have regular and ongoing followup assessment to assess recovery, prevent deterioration and maximize functional outcome. 55
56 Summary Stroke Rehabilitation improves outcomes Key elements- Geographically distinct specialized unit Early onset Intensity of therapy Task Specific Therapy Outpatient Therapy 56
57 57
58 Acknowledgements Robert Teasell MD FRCP University of Western Ontario Canadian Stroke Network Heart and Stroke Foundation of Canada 58
59 References Look for tools menu for SCORE guidelines and Canadian stroke Strategy Guidelines 59
60 Thanks for Listening! Questions? 60
How many RCTs in Stroke Rehab?
 Evidence Based Stroke Rehabilitation: Maximizing Recovery and Improving Outcomes Robert Teasell MD FRCPC Professor and Chair Chief Physical Medicine & Rehabilitation St. Joseph s Health Care London University
Evidence Based Stroke Rehabilitation: Maximizing Recovery and Improving Outcomes Robert Teasell MD FRCPC Professor and Chair Chief Physical Medicine & Rehabilitation St. Joseph s Health Care London University
Best Practice Recommendations for Inpatient Stroke Care: Rationale and Evidence for Integrated Stroke Units in North Simcoe Muskoka LHIN
 Best Practice Recommendations for Inpatient Stroke Care: Rationale and Evidence for Integrated Stroke Units in North Simcoe Muskoka LHIN Physician Education Session May 24, 2013 Dr. Mark Bayley,, Cheryl
Best Practice Recommendations for Inpatient Stroke Care: Rationale and Evidence for Integrated Stroke Units in North Simcoe Muskoka LHIN Physician Education Session May 24, 2013 Dr. Mark Bayley,, Cheryl
TORONTO STROKE FLOW INITIATIVE - Inpatient Rehabilitation Best Practice Recommendations Guide (updated January 23, 2014)
") TORONTO STROKE FLOW INITIATIVE - Inpatient Rehabilitation Best Practice Guide (updated January 23, 2014) Objective: To enhance system-wide performance and outcomes for persons with stroke in Toronto. Goals:
TORONTO STROKE FLOW INITIATIVE - Inpatient Rehabilitation Best Practice Guide (updated January 23, 2014) Objective: To enhance system-wide performance and outcomes for persons with stroke in Toronto. Goals:
Stroke Rehabilitation Triage Severe Strokes
 The London Stroke Rehab Data Base Project Robert Teasell MD FRCPC Professor and Chair-Chief Department of Phys Med Rehab London Ontario Retrospective Data Bases In stroke rehab limited funding for clinical
The London Stroke Rehab Data Base Project Robert Teasell MD FRCPC Professor and Chair-Chief Department of Phys Med Rehab London Ontario Retrospective Data Bases In stroke rehab limited funding for clinical
TORONTO STROKE FLOW INITIATIVE - Outpatient Rehabilitation Best Practice Recommendations Guide (updated July 26, 2013)
") Objective: To enhance system-wide performance and outcomes for persons with stroke in Toronto. Goals: Timely access to geographically located acute stroke unit care with a dedicated interprofessional team
Objective: To enhance system-wide performance and outcomes for persons with stroke in Toronto. Goals: Timely access to geographically located acute stroke unit care with a dedicated interprofessional team
Stroke Rehab Across the Continuum of Care in Quinte Region
 Stroke Rehab Across the Continuum of Care in Quinte Region Adrienne Bell Smith Manager of Rehab Therapies QHC Karen Brown Manger Client Services, Hospital Access South East CCAC Disclosure of Potential
Stroke Rehab Across the Continuum of Care in Quinte Region Adrienne Bell Smith Manager of Rehab Therapies QHC Karen Brown Manger Client Services, Hospital Access South East CCAC Disclosure of Potential
Stroke Rehabilitation
 Stroke Rehabilitation Robert Teasell MD FRCPC Professor and Chair-Chief Dept Physical Medicine and Rehabilitation Schulich School of Medicine University of Western Ontario Lawson Health Research Institute
Stroke Rehabilitation Robert Teasell MD FRCPC Professor and Chair-Chief Dept Physical Medicine and Rehabilitation Schulich School of Medicine University of Western Ontario Lawson Health Research Institute
Waterloo Wellington CCAC Community Stroke Program
 Waterloo Wellington CCAC Community Stroke Program Stroke Collaborative 2014 October 27, 2014 Maria Fage, OT Reg. (Ont.) Manager, Client Services Map of Waterloo Wellington LHIN 2 Background Integration
Waterloo Wellington CCAC Community Stroke Program Stroke Collaborative 2014 October 27, 2014 Maria Fage, OT Reg. (Ont.) Manager, Client Services Map of Waterloo Wellington LHIN 2 Background Integration
Hamilton Health Sciences Integrated Stroke Model of Care. Rhonda Whiteman, Stroke Best Practices Coordinator, Hamilton Health Sciences
 Hamilton Health Sciences Integrated Stroke Model of Care Rhonda Whiteman, Stroke Best Practices Coordinator, Hamilton Health Sciences Integrated Stroke Model of Care Goals To provide a more comprehensive
Hamilton Health Sciences Integrated Stroke Model of Care Rhonda Whiteman, Stroke Best Practices Coordinator, Hamilton Health Sciences Integrated Stroke Model of Care Goals To provide a more comprehensive
Ontario Stroke System. Prepared by: Stroke Rehabilitation Evaluation Working Group Stroke Evaluation Advisory Committee May, 2007
 Ontario Stroke System Stroke Rehabilitation Performance Measurement Manual Prepared by: Stroke Rehabilitation Evaluation Working Group Stroke Evaluation Advisory Committee May, 2007 Stroke Rehabilitation
Ontario Stroke System Stroke Rehabilitation Performance Measurement Manual Prepared by: Stroke Rehabilitation Evaluation Working Group Stroke Evaluation Advisory Committee May, 2007 Stroke Rehabilitation
What do these stories illustrate about ER/ALC issue?
 What do these stories illustrate about ER/ALC issue? Maximizing the Impact of Rehab on Provincial Priority Issues Mark Bayley, MD, FRCPC Medical Director, Neuro Rehabilitation Program, Toronto Rehab and
What do these stories illustrate about ER/ALC issue? Maximizing the Impact of Rehab on Provincial Priority Issues Mark Bayley, MD, FRCPC Medical Director, Neuro Rehabilitation Program, Toronto Rehab and
Dedicated Stroke Interprofessional Rehab Team. Mixed Rehab Unit. Dedicated Rehab Unit
 Outpatient & Community I n p a t I e n t Stroke Rehab Definition Framework Institutional Setting Inpatient Rehab in Acute Care or Rehab Hospitals* Acute Care Integrated Specialized Units Transitional Care
Outpatient & Community I n p a t I e n t Stroke Rehab Definition Framework Institutional Setting Inpatient Rehab in Acute Care or Rehab Hospitals* Acute Care Integrated Specialized Units Transitional Care
ISSUED BY: TITLE: ISSUED BY: TITLE: President
 CLINICAL PRACTICE GUIDELINE PROFESSIONAL PRACTICE TITLE: Stroke Care Rehabilitation Unit DATE OF ISSUE: 2005, 05 PAGE 1 OF 7 NUMBER: CPG 20-3 SUPERCEDES: New ISSUED BY: TITLE: Chief of Medical Staff ISSUED
CLINICAL PRACTICE GUIDELINE PROFESSIONAL PRACTICE TITLE: Stroke Care Rehabilitation Unit DATE OF ISSUE: 2005, 05 PAGE 1 OF 7 NUMBER: CPG 20-3 SUPERCEDES: New ISSUED BY: TITLE: Chief of Medical Staff ISSUED
Rehabilitation Nurses: Champions for Optimizing Stroke Rehabilitation Across the Continuum of Care
 Rehabilitation Nurses: Champions for Optimizing Stroke Rehabilitation Across the Continuum of Care Presenters Sandra Melchiorre RN, MN, ACNP, CNN (c) Regional Stroke Acute Care Advanced Practice Nurse,
Rehabilitation Nurses: Champions for Optimizing Stroke Rehabilitation Across the Continuum of Care Presenters Sandra Melchiorre RN, MN, ACNP, CNN (c) Regional Stroke Acute Care Advanced Practice Nurse,
Stroke Rehabilitation Intensity Frequently Asked Questions
 Stroke Rehabilitation Intensity Frequently Asked Questions 1) What is the provincial definition of Rehabilitation Intensity? Rehabilitation Intensity 1 is: The amount of time the patient spends in individual,
Stroke Rehabilitation Intensity Frequently Asked Questions 1) What is the provincial definition of Rehabilitation Intensity? Rehabilitation Intensity 1 is: The amount of time the patient spends in individual,
Summary Report. Moving to Best Practice. Southwestern Ontario Stroke Rehabilitation Action Planning Day November 28, 2006
 Southwestern Ontario Stroke Rehabilitation Action Planning Day November 28, 2006 Summary Report Moving to Best Practice Prepared by: Deborah Willems Southwestern Ontario Stroke Strategy January 29, 2007
Southwestern Ontario Stroke Rehabilitation Action Planning Day November 28, 2006 Summary Report Moving to Best Practice Prepared by: Deborah Willems Southwestern Ontario Stroke Strategy January 29, 2007
Importance of Integrating Stroke Rehabilitation Across the Continuum of Care
 Importance of Integrating Stroke Rehabilitation Across the Continuum of Care Dori Tooke, MHA, PT, CSCS Manager-Inpatient Rehab Program St. Luke s Medical Center Milwaukee, WI Disclosure Nothing to disclose
Importance of Integrating Stroke Rehabilitation Across the Continuum of Care Dori Tooke, MHA, PT, CSCS Manager-Inpatient Rehab Program St. Luke s Medical Center Milwaukee, WI Disclosure Nothing to disclose
Marina Richardson, M.Sc. Deb Willems, BSc.PT David Ure, OT Robert Teasell, MD FRCPC
 Assessing the Impact of Southwestern Ontario s Community Stroke Rehabilitation Teams: An Economic Analysis Presenters: Laura Allen, M.Sc. (cand.) Matthew Meyer, Ph.D (cand.) Marina Richardson, M.Sc. Deb
Assessing the Impact of Southwestern Ontario s Community Stroke Rehabilitation Teams: An Economic Analysis Presenters: Laura Allen, M.Sc. (cand.) Matthew Meyer, Ph.D (cand.) Marina Richardson, M.Sc. Deb
ALBERTA PROVINCIAL STROKE STRATEGY (APSS)
") ALBERTA PROVINCIAL STROKE STRATEGY (APSS) Stroke Systems of Care Key Components APSS Pillar Recommendations March 28, 2007 1 The following is a summary of the key components and APSS Pillar recommendations
ALBERTA PROVINCIAL STROKE STRATEGY (APSS) Stroke Systems of Care Key Components APSS Pillar Recommendations March 28, 2007 1 The following is a summary of the key components and APSS Pillar recommendations
The following document was directed to the North East LHIN.
 The following document was directed to the North East LHIN. If you require any further details into the information presented here please feel free to contact Jenn Fearn, Regional Rehabilitation Coordinator,
The following document was directed to the North East LHIN. If you require any further details into the information presented here please feel free to contact Jenn Fearn, Regional Rehabilitation Coordinator,
Complex Outpatient. Injury. Rehab. Integrated, evidence-based rehab that supports a timely return to home, life, work or school
 Complex Outpatient Injury Rehab Integrated, evidence-based rehab that supports a timely return to home, life, work or school Toronto Rehabilitation Institute At Toronto Rehab, our goal is to advance rehabilitation
Complex Outpatient Injury Rehab Integrated, evidence-based rehab that supports a timely return to home, life, work or school Toronto Rehabilitation Institute At Toronto Rehab, our goal is to advance rehabilitation
THE FUTURE OF STROKE REHABILITATION
 Disclosure of Financial Relationships Gary M. Abrams M.D. THE FUTURE OF STROKE REHABILITATION Gary M. Abrams M.D. Professor of Clinical Neurology Director of Neurorehabilitation UCSF Has disclosed the
Disclosure of Financial Relationships Gary M. Abrams M.D. THE FUTURE OF STROKE REHABILITATION Gary M. Abrams M.D. Professor of Clinical Neurology Director of Neurorehabilitation UCSF Has disclosed the
STROKE REHABILITATION RESOURCE GUIDE
 STROKE REHABILITATION RESOURCE GUIDE INTRODUCTION The intent of the Stroke Rehabilitation Resource Guide is to enable stroke care providers seeking information related to the rehabilitation of the stroke
STROKE REHABILITATION RESOURCE GUIDE INTRODUCTION The intent of the Stroke Rehabilitation Resource Guide is to enable stroke care providers seeking information related to the rehabilitation of the stroke
Virtual Reality Technology in Stroke Rehabilitation: Ready for Prime Time
 Virtual Reality Technology in Stroke Rehabilitation: Ready for Prime Time Hillel Finestone, MD CM, FRCPC (Physiatrist/PM&R) Ontario Hospital Association Third Annual Senior Friendly Hospital Care Conference
Virtual Reality Technology in Stroke Rehabilitation: Ready for Prime Time Hillel Finestone, MD CM, FRCPC (Physiatrist/PM&R) Ontario Hospital Association Third Annual Senior Friendly Hospital Care Conference
Brief, Evidence Based Review of Inpatient/Residential rehabilitation for adults with moderate to severe TBI
 Brief, Evidence Based Review of Inpatient/Residential rehabilitation for adults with moderate to severe TBI Reviewer Peter Larking Date Report Completed 7 October 2011 Important Note: This brief report
Brief, Evidence Based Review of Inpatient/Residential rehabilitation for adults with moderate to severe TBI Reviewer Peter Larking Date Report Completed 7 October 2011 Important Note: This brief report
STROKE REHABILITATION SURVEY
 STROKE REHABILITATION SURVEY INDIANA STROKE PREVENTION TASK FORCE PRESENTED BY VICKI SCOTT, MS, CTRS RECREATIONAL THERAPIST TASK FORCE MEMBER BACKGROUND Stroke is the third leading cause of death in all
STROKE REHABILITATION SURVEY INDIANA STROKE PREVENTION TASK FORCE PRESENTED BY VICKI SCOTT, MS, CTRS RECREATIONAL THERAPIST TASK FORCE MEMBER BACKGROUND Stroke is the third leading cause of death in all
Communiqué 2: STROKE GUIDELINE IMPLEMENTATION. Toronto Central LHIN MSK/Stroke Implementation Group COMMUNIQUÉ 2: STROKE GUIDELINE IMPLEMENTATION 1
 2 Communiqué 2: STROKE GUIDELINE IMPLEMENTATION Toronto Central LHIN MSK/Stroke Implementation Group COMMUNIQUÉ 2: STROKE GUIDELINE IMPLEMENTATION 1 IN DECEMBER 2012, THE TORONTO CENTRAL LHIN (TCLHIN)
2 Communiqué 2: STROKE GUIDELINE IMPLEMENTATION Toronto Central LHIN MSK/Stroke Implementation Group COMMUNIQUÉ 2: STROKE GUIDELINE IMPLEMENTATION 1 IN DECEMBER 2012, THE TORONTO CENTRAL LHIN (TCLHIN)
Behaviour Management: Partnering To Bridge The Continuum. Presented by: Nancy Boaro, MN, CNN(C), CRN(C) Karey-Anne Fannon, BA, BST, RRP.
, CRN(C) Karey-Anne Fannon, BA, BST, RRP.") Behaviour Management: Partnering To Bridge The Continuum Presented by: Nancy Boaro, MN, CNN(C), CRN(C) Karey-Anne Fannon, BA, BST, RRP Objectives Review some of the behaviours exhibited by patients with
Behaviour Management: Partnering To Bridge The Continuum Presented by: Nancy Boaro, MN, CNN(C), CRN(C) Karey-Anne Fannon, BA, BST, RRP Objectives Review some of the behaviours exhibited by patients with
Good Samaritan Inpatient Rehabilitation Program
 Good Samaritan Inpatient Rehabilitation Program Living at your full potential. Welcome When people are sick or injured, our goal is their maximum recovery. We help people live to their full potential.
Good Samaritan Inpatient Rehabilitation Program Living at your full potential. Welcome When people are sick or injured, our goal is their maximum recovery. We help people live to their full potential.
SAM KARAS ACUTE REHABILITATION CENTER
 SAM KARAS ACUTE REHABILITATION CENTER 1 MEDICAL CARE Sam Karas Acute Rehabilitation The Sam Karas Acute Rehabilitation Center is a comprehensive and interdisciplinary inpatient unit. Medical care is directed
SAM KARAS ACUTE REHABILITATION CENTER 1 MEDICAL CARE Sam Karas Acute Rehabilitation The Sam Karas Acute Rehabilitation Center is a comprehensive and interdisciplinary inpatient unit. Medical care is directed
National Stroke Association s Guide to Choosing Stroke Rehabilitation Services
 National Stroke Association s Guide to Choosing Stroke Rehabilitation Services Rehabilitation, often referred to as rehab, is an important part of stroke recovery. Through rehab, you: Re-learn basic skills
National Stroke Association s Guide to Choosing Stroke Rehabilitation Services Rehabilitation, often referred to as rehab, is an important part of stroke recovery. Through rehab, you: Re-learn basic skills
Post-Acute Rehab: Community Re-Entry After Stroke? Sheldon Herring, Ph.D. Roger C. Peace Rehab Hospital Greenville Hospital System
 Post-Acute Rehab: Community Re-Entry After Stroke? Sheldon Herring, Ph.D. Roger C. Peace Rehab Hospital Greenville Hospital System 2014 Neurocognitive Deficits After Stroke: The Hidden Disability Sheldon
Post-Acute Rehab: Community Re-Entry After Stroke? Sheldon Herring, Ph.D. Roger C. Peace Rehab Hospital Greenville Hospital System 2014 Neurocognitive Deficits After Stroke: The Hidden Disability Sheldon
Rehabilitation. Care
 Rehabilitation Care Bruyère Continuing Care is the champion of well-being for aging Canadians and those requiring Continuing Care, helping them to become and remain as healthy and independent as possible
Rehabilitation Care Bruyère Continuing Care is the champion of well-being for aging Canadians and those requiring Continuing Care, helping them to become and remain as healthy and independent as possible
Stakeholder s Report. 2525 SW 75 th Ave Miami, Florida 33155 305.262.6800 www.westgablesrehabhospital.com
 212 Stakeholder s Report 2525 SW 75 th Ave Miami, Florida 33155 35.262.68 www.westgablesrehabhospital.com PROFILE REPORT For more than 25 years, West Gables Rehabilitation Hospital has made a mission of
212 Stakeholder s Report 2525 SW 75 th Ave Miami, Florida 33155 35.262.68 www.westgablesrehabhospital.com PROFILE REPORT For more than 25 years, West Gables Rehabilitation Hospital has made a mission of
ACUTE CARE TO REHABILITATION
 ACUTE CARE TO REHABILITATION JONATHAN P. QUEVEDO, M.D. JFK-JOHNSON REHABILITATION HOSPITAL PRESENTER DISCLOSURE INFORMATION JONATHAN P. QUEVEDO M.D. ACUTE CARE TO REHABILITATION FINANCIAL DISCLOSURE EMPLOYED
ACUTE CARE TO REHABILITATION JONATHAN P. QUEVEDO, M.D. JFK-JOHNSON REHABILITATION HOSPITAL PRESENTER DISCLOSURE INFORMATION JONATHAN P. QUEVEDO M.D. ACUTE CARE TO REHABILITATION FINANCIAL DISCLOSURE EMPLOYED
Sex Differences in Profiles & Outcomes of Patients with Traumatic Brain Injury in an Inpatient Rehabilitation Sample
 Sex Differences in Profiles & Outcomes of Patients with Traumatic Brain Injury in an Inpatient Rehabilitation Sample Dr. Angela Colantonio Vincy Chan Tatyana Mollayeva Background & Significance Traumatic
Sex Differences in Profiles & Outcomes of Patients with Traumatic Brain Injury in an Inpatient Rehabilitation Sample Dr. Angela Colantonio Vincy Chan Tatyana Mollayeva Background & Significance Traumatic
Complex Continuing Care Restorative Care (Combined Functional Enhancement and Restorative Care Programs)
") Complex Continuing Care Restorative Care (Combined Functional Enhancement and Restorative Care Programs) Description: The Restorative Care program provides a moderate to low intensity goal-oriented rehabilitation
Complex Continuing Care Restorative Care (Combined Functional Enhancement and Restorative Care Programs) Description: The Restorative Care program provides a moderate to low intensity goal-oriented rehabilitation
Discharge Planning. Home Assess / Treat. inpatient CCC (active/ltld) rehab = ALC Designation LTC. Admit
 rehab = ALC Designation LTC. Admit") DISCHARGE PLANNING GUIDELINES FOR INPATIENT REHABILITATION The Discharge Planning Guidelines for Inpatient Rehabilitation have been developed by the GTA Rehab Network s Patient Access and Flow Committee
DISCHARGE PLANNING GUIDELINES FOR INPATIENT REHABILITATION The Discharge Planning Guidelines for Inpatient Rehabilitation have been developed by the GTA Rehab Network s Patient Access and Flow Committee
Implementing Evidence Based Community Stroke Services
 Implementing Evidence Based Community Stroke Services Dr Rebecca Fisher & Professor Marion Walker University of Nottingham () Damian Jenkinson & Ian Golton (NHS Stroke Improvement Programme) A partnership
Implementing Evidence Based Community Stroke Services Dr Rebecca Fisher & Professor Marion Walker University of Nottingham () Damian Jenkinson & Ian Golton (NHS Stroke Improvement Programme) A partnership
Canadian Stroke Guidelines for Rehabilitation
 Canadian Stroke Guidelines for Rehabilitation Robert Teasell MD FRCPC Professor Physical Medicine and Rehabilitation Schulich School of Medicine Western University London, Ontario, Canada In theory there
Canadian Stroke Guidelines for Rehabilitation Robert Teasell MD FRCPC Professor Physical Medicine and Rehabilitation Schulich School of Medicine Western University London, Ontario, Canada In theory there
Outpatient Neurological Rehabilitation Victoria General Hospital. Pam Loadman BSC.P.T., MSc. Physiotherapist
 Outpatient Neurological Rehabilitation Victoria General Hospital Pam Loadman BSC.P.T., MSc. Physiotherapist OPN - overview Who we see: Inclusion criteria Diagnoses Who we are: Clinicians involved What
Outpatient Neurological Rehabilitation Victoria General Hospital Pam Loadman BSC.P.T., MSc. Physiotherapist OPN - overview Who we see: Inclusion criteria Diagnoses Who we are: Clinicians involved What
New Technologies and Their Role in Enhancing Neurological Recovery
 REHABILITATION CARE 2014: under the ACA Patient Centered Medical Home for Persons with Disability: Acute Neurology, Medicine, Surgery services seamlessly blending into Acute inpatient Rehabilitation Ambulatory
REHABILITATION CARE 2014: under the ACA Patient Centered Medical Home for Persons with Disability: Acute Neurology, Medicine, Surgery services seamlessly blending into Acute inpatient Rehabilitation Ambulatory
By way of introduction. Inpatient Medical Rehabilitation
 Inpatient Medical Rehabilitation The Brookdale Center is part of a continuum of care at the NCH Healthcare System Strategic Focus Cascaded to Department & Individual Workgroup Levels Focus & Accountability
Inpatient Medical Rehabilitation The Brookdale Center is part of a continuum of care at the NCH Healthcare System Strategic Focus Cascaded to Department & Individual Workgroup Levels Focus & Accountability
How To Plan A Rehabilitation Program
 Project Plan to Rehabilitation Service Connecting and Collaborating in the Continuity of Care in Rehabilitation Presented By: Arlene Whitehead, May 31, 2011 Rehabilitation Collaborative Overview OUTLINE
Project Plan to Rehabilitation Service Connecting and Collaborating in the Continuity of Care in Rehabilitation Presented By: Arlene Whitehead, May 31, 2011 Rehabilitation Collaborative Overview OUTLINE
REHABILITATION SERVICES
 REHABILITATION SERVICES Table of Contents GENERAL... 2 TERMS AND ABBREVIATIONS... 2 PRIOR AUTHORIZATION REQUIREMENTS FOR MEDICAID REIMBURSEMENT OF INPATIENT REHABILITATION SERVICES (Updated 4/1/11)...
REHABILITATION SERVICES Table of Contents GENERAL... 2 TERMS AND ABBREVIATIONS... 2 PRIOR AUTHORIZATION REQUIREMENTS FOR MEDICAID REIMBURSEMENT OF INPATIENT REHABILITATION SERVICES (Updated 4/1/11)...
STROKE CARE NOW NETWORK CONFERENCE MAY 22, 2014
 STROKE CARE NOW NETWORK CONFERENCE MAY 22, 2014 Rehabilitation Innovations in Post- Stroke Recovery Madhav Bhat, MD Fort Wayne Neurological Center DISCLOSURE Paid speaker for TEVA Neuroscience Program.
STROKE CARE NOW NETWORK CONFERENCE MAY 22, 2014 Rehabilitation Innovations in Post- Stroke Recovery Madhav Bhat, MD Fort Wayne Neurological Center DISCLOSURE Paid speaker for TEVA Neuroscience Program.
PREPARING THE PATIENT FOR TRANSFER TO AN INPATIENT REHABILITATON FACILITY (IRF) University Hospitals 8th Annual Neuroscience Nursing Symposium
 University Hospitals 8th Annual Neuroscience Nursing Symposium") PREPARING THE PATIENT FOR TRANSFER TO AN INPATIENT REHABILITATON FACILITY (IRF) University Hospitals 8th Annual Neuroscience Nursing Symposium May 31, 2013 2 DEFINITION: INPATIENT REHABILITATION FACILITY
PREPARING THE PATIENT FOR TRANSFER TO AN INPATIENT REHABILITATON FACILITY (IRF) University Hospitals 8th Annual Neuroscience Nursing Symposium May 31, 2013 2 DEFINITION: INPATIENT REHABILITATION FACILITY
CURRENT AND FUTURE TRENDS IN POST ACUTE CARE The Value and Role of Acute Inpatient Rehab
 CURRENT AND FUTURE TRENDS IN POST ACUTE CARE The Value and Role of Acute Inpatient Rehab Robert S. Djergaian, M.D. Medical Director Banner Good Samaritan Rehabilitation Institute Stewardship Profitability
CURRENT AND FUTURE TRENDS IN POST ACUTE CARE The Value and Role of Acute Inpatient Rehab Robert S. Djergaian, M.D. Medical Director Banner Good Samaritan Rehabilitation Institute Stewardship Profitability
Implementation of an Interprofessional Team Approach to Stroke Rehabilitation Among Stroke Survivors Using Home Care: Evaluation and Lessons Learned
 Implementation of an Interprofessional Team Approach to Stroke Rehabilitation Among Stroke Survivors Using Home Care: Evaluation and Lessons Learned Maureen Markle-Reid, RN, MScN, PhD Associate Professor
Implementation of an Interprofessional Team Approach to Stroke Rehabilitation Among Stroke Survivors Using Home Care: Evaluation and Lessons Learned Maureen Markle-Reid, RN, MScN, PhD Associate Professor
Rehabilitation After Debilitation. James Inzerillo MD Physiatrist
 Rehabilitation After Debilitation James Inzerillo MD Physiatrist What Happens to Me If I m I m Not Able to Take Care of Myself? Rehabilitation Options Self-Rehabilitation Outpatient Rehab At Home Rehab
Rehabilitation After Debilitation James Inzerillo MD Physiatrist What Happens to Me If I m I m Not Able to Take Care of Myself? Rehabilitation Options Self-Rehabilitation Outpatient Rehab At Home Rehab
Using Objective Measures to Facilitate Rehabilitation Referral
 Using Objective Measures to Facilitate Rehabilitation Referral Mark Bayley MD, FRCPC Medical Director, Neuro Rehabilitation Program, Toronto Rehabilitation Institute Associate Professor, Division of Physiatry,
Using Objective Measures to Facilitate Rehabilitation Referral Mark Bayley MD, FRCPC Medical Director, Neuro Rehabilitation Program, Toronto Rehabilitation Institute Associate Professor, Division of Physiatry,
Mount Sinai Rehabilitation Center. 2014 Outcomes. Mount Sinai Rehabilitation Center 2014 Outcomes
 Mount Sinai Rehabilitation Center 2014 Outcomes Mount Sinai Rehabilitation Center 2014 Outcomes TABLE OF CONTENTS A Message from the Chair... 3 About Our Programs. 4-5 Inpatient Rehabilitation. 6-12 Outpatient
Mount Sinai Rehabilitation Center 2014 Outcomes Mount Sinai Rehabilitation Center 2014 Outcomes TABLE OF CONTENTS A Message from the Chair... 3 About Our Programs. 4-5 Inpatient Rehabilitation. 6-12 Outpatient
REHABILITATION. begins right here
 REHABILITATION begins right here Select Rehabilitation Hospital of Denton offers you a new direction in medical rehabilitation. Our 44-bed, state-of-the-science hospital offers unparalleled treatment to
REHABILITATION begins right here Select Rehabilitation Hospital of Denton offers you a new direction in medical rehabilitation. Our 44-bed, state-of-the-science hospital offers unparalleled treatment to
Neuro-rehabilitation in Stroke. Amit Kumar Neuro-Occupational Therapist
 Neuro-rehabilitation in Stroke Amit Kumar Neuro-Occupational Therapist Neuro-rehabilitation A process whereby patients who suffer from impairment following neurologic diseases regain their former abilities
Neuro-rehabilitation in Stroke Amit Kumar Neuro-Occupational Therapist Neuro-rehabilitation A process whereby patients who suffer from impairment following neurologic diseases regain their former abilities
Exploring inpatient rehabilitation data and information with CIHI s National Rehabilitation Reporting System
 Exploring inpatient rehabilitation data and information with CIHI s National Rehabilitation Reporting System Ian Joiner Manager, Rehabilitation and Mental Health 1 Key points for this presentation > Not-for-profit
Exploring inpatient rehabilitation data and information with CIHI s National Rehabilitation Reporting System Ian Joiner Manager, Rehabilitation and Mental Health 1 Key points for this presentation > Not-for-profit
Outpatient/Ambulatory Rehab. Dedicated Trans-disciplinary Team (defined within Annotated References)
") CARDIAC The delivery of Cardiac Rehab is unlike most other rehab populations. The vast majority of patients receive their rehab in outpatient or community settings and only a small subset requires an inpatient
CARDIAC The delivery of Cardiac Rehab is unlike most other rehab populations. The vast majority of patients receive their rehab in outpatient or community settings and only a small subset requires an inpatient
Where Should Rehabilitation Take Place?!
 Where Should Rehabilitation Take Place?! Three Basic Questions! 1. Is rehabilitation effective in improving a patient s functional abilities?!yes" yes" 2. Is rehabilitation cost effective?!yes" where"
Where Should Rehabilitation Take Place?! Three Basic Questions! 1. Is rehabilitation effective in improving a patient s functional abilities?!yes" yes" 2. Is rehabilitation cost effective?!yes" where"
Admission to Inpatient Rehabilitation (Rehab) Services
 Services") Family Caregiver Guide Admission to Inpatient Rehabilitation (Rehab) Services What Is Rehab? Your family member may have been referred to rehab after being in a hospital due to acute (current) illness,
Family Caregiver Guide Admission to Inpatient Rehabilitation (Rehab) Services What Is Rehab? Your family member may have been referred to rehab after being in a hospital due to acute (current) illness,
Homeward Bound. Amanda Melvin, MSW Emily Hartman, BSN, RN Tiffany Curtis, BSN, RN, CRRN Cindy Regan, MSN, RN - BC
 Homeward Bound Amanda Melvin, MSW Emily Hartman, BSN, RN Tiffany Curtis, BSN, RN, CRRN Cindy Regan, MSN, RN - BC Objectives Identify and differentiate the levels of stroke rehabilitation care. Identify
Homeward Bound Amanda Melvin, MSW Emily Hartman, BSN, RN Tiffany Curtis, BSN, RN, CRRN Cindy Regan, MSN, RN - BC Objectives Identify and differentiate the levels of stroke rehabilitation care. Identify
Complex Care Planning in the Emergency Department: Demonstrating Rehabilitation Contributions
 Complex Care Planning in the Emergency Department: Demonstrating Rehabilitation Contributions CAOT Conference 2016 Inspired for Higher Summits Banff, AB No conflict of interest Project Team all from Sunnybrook
Complex Care Planning in the Emergency Department: Demonstrating Rehabilitation Contributions CAOT Conference 2016 Inspired for Higher Summits Banff, AB No conflict of interest Project Team all from Sunnybrook
PARTNERSHIP HEALTHPLAN OF CALIFORNIA POLICY / PROCEDURE:
 PARTNERSHIP HEALTHPLAN OF CALIFORNIA POLICY/PROCEDURE Policy Number: MCUP3003 (previously UP100303) Reviewing Entities: Credentialing IQI P & T QUAC Approving Entities: BOARD CEO COMPLIANCE FINANCE PAC
PARTNERSHIP HEALTHPLAN OF CALIFORNIA POLICY/PROCEDURE Policy Number: MCUP3003 (previously UP100303) Reviewing Entities: Credentialing IQI P & T QUAC Approving Entities: BOARD CEO COMPLIANCE FINANCE PAC
CLINICAL PRACTICE GUIDELINES Treatment of Schizophrenia
 CLINICAL PRACTICE GUIDELINES Treatment of Schizophrenia V. Service Delivery Service Delivery and the Treatment System General Principles 1. All patients should have access to a comprehensive continuum
CLINICAL PRACTICE GUIDELINES Treatment of Schizophrenia V. Service Delivery Service Delivery and the Treatment System General Principles 1. All patients should have access to a comprehensive continuum
2016 International Stroke Conference Hot Topics Lori M. Massaro, MSN, CRNP Kari Moore, MSN, AGACNP-BC
 2016 International Stroke Conference Hot Topics Lori M. Massaro, MSN, CRNP Kari Moore, MSN, AGACNP-BC Disclosures Lori M. Massaro, MSN,CRNP speakers bureau Genentech Kari Moore, MSN, AGACNP-BC -none 1
2016 International Stroke Conference Hot Topics Lori M. Massaro, MSN, CRNP Kari Moore, MSN, AGACNP-BC Disclosures Lori M. Massaro, MSN,CRNP speakers bureau Genentech Kari Moore, MSN, AGACNP-BC -none 1
GP workshop. Maria Fitzpatrick Nurse Consultant Kings College Stroke Centre
 GP workshop Maria Fitzpatrick Nurse Consultant Kings College Stroke Centre Stroke: the Facts Stroke: the Facts Every 5 minutes someone in the UK has a stroke 1 in 4 men and 1 in 5 women will have a stroke
GP workshop Maria Fitzpatrick Nurse Consultant Kings College Stroke Centre Stroke: the Facts Stroke: the Facts Every 5 minutes someone in the UK has a stroke 1 in 4 men and 1 in 5 women will have a stroke
Hamilton Health Sciences Acquired Brain Injury Program
 Overview of Program The Acquired Brain Injury (ABI) Program at the Regional Rehabilitation Centre, Hamilton General Hospital serve the rehabilitation needs of adults with acquired brain injuries and their
Overview of Program The Acquired Brain Injury (ABI) Program at the Regional Rehabilitation Centre, Hamilton General Hospital serve the rehabilitation needs of adults with acquired brain injuries and their
Organization of Rehabilitation and Post-Acute Care
 Organization of Rehabilitation and Post-Acute Care Inaugural Meeting of NECC Boston, MA - September 13, 2006 Janet Prvu Bettger, ScD University of Pennsylvania Department of Physical Medicine and Rehabilitation
Organization of Rehabilitation and Post-Acute Care Inaugural Meeting of NECC Boston, MA - September 13, 2006 Janet Prvu Bettger, ScD University of Pennsylvania Department of Physical Medicine and Rehabilitation
Research Summary. Towards Earlier Discharge, Better Outcomes, Lower Cost: Stroke Rehabilitation in Ireland. September 2014
 Towards Earlier Discharge, Better Outcomes, Lower Cost: Stroke Rehabilitation in Ireland September 2014 Research Summary Report prepared for the Irish Heart Foundation by the Economic and Social Research
Towards Earlier Discharge, Better Outcomes, Lower Cost: Stroke Rehabilitation in Ireland September 2014 Research Summary Report prepared for the Irish Heart Foundation by the Economic and Social Research
REMINDER: Please ensure all stroke and TIA patients admitted to hospital are designated as "Stroke Service" in Cerner.
 ACUTE STROKE CLINICAL PATHWAY QEH/HH PCH KCMH Souris Western Stewart Memorial O'Leary PATIENT ID INCLUSION CRITERIA* All patients admitted to hosptial with a suspected diagnosis of acute ischemic stroke
ACUTE STROKE CLINICAL PATHWAY QEH/HH PCH KCMH Souris Western Stewart Memorial O'Leary PATIENT ID INCLUSION CRITERIA* All patients admitted to hosptial with a suspected diagnosis of acute ischemic stroke
A STAR is born. Collaborative Strategy that works!
 A STAR is born Collaborative Strategy that works! Objective Demonstrate the importance of developing and nurturing partnerships in achieving quality outcomes, providing the right care at the right place
A STAR is born Collaborative Strategy that works! Objective Demonstrate the importance of developing and nurturing partnerships in achieving quality outcomes, providing the right care at the right place
STROKE REHABILITATION RESOURCE GUIDE
 STROKE REHABILITATION RESOURCE GUIDE INTRODUCTION The intent of the Stroke Rehabilitation Guide is to enable stroke care providers seeking information related to the rehabilitation of the stroke survivor
STROKE REHABILITATION RESOURCE GUIDE INTRODUCTION The intent of the Stroke Rehabilitation Guide is to enable stroke care providers seeking information related to the rehabilitation of the stroke survivor
Mobile Rehabilitation Team St Vincent s Style. Dr Shari Parker Rehabilitation Physician
 Mobile Rehabilitation Team St Vincent s Style Dr Shari Parker Rehabilitation Physician Drivers for Change 1. Pressure on beds, bed blocks 2. Evidence for Early Rehabilitation 3. The problem of Deconditioning
Mobile Rehabilitation Team St Vincent s Style Dr Shari Parker Rehabilitation Physician Drivers for Change 1. Pressure on beds, bed blocks 2. Evidence for Early Rehabilitation 3. The problem of Deconditioning
Managing the Stroke Rehabilitation Triage Process
 EBRSR [Evidence-Based Review of Stroke Rehabilitation] 4 Managing the Stroke Rehabilitation Triage Process Robert Teasell MD, Norhayati Hussein MBBS, Norine Foley MSc Last updated November 2013 Abstract
EBRSR [Evidence-Based Review of Stroke Rehabilitation] 4 Managing the Stroke Rehabilitation Triage Process Robert Teasell MD, Norhayati Hussein MBBS, Norine Foley MSc Last updated November 2013 Abstract
Rehabilitation Therapies
 Bluebonnet Medical Rehabilitation Hospital Rehabilitation Therapies 512-444-4835 or 800-252-5151 www.texasneurorehab.com Austin, Texas What Sets Us Apart Rehabilitation Therapies Physical Therapy - Neuromuscular
Bluebonnet Medical Rehabilitation Hospital Rehabilitation Therapies 512-444-4835 or 800-252-5151 www.texasneurorehab.com Austin, Texas What Sets Us Apart Rehabilitation Therapies Physical Therapy - Neuromuscular
How To Run An Acquired Brain Injury Program
 ` Acquired Brain Injury Program Regional Rehabilitation Centre at the Hamilton General Hospital Table of Contents Page Introduction... 3-4 Acquired Brain Injury Program Philosophy... 3 Vision... 3 Service
` Acquired Brain Injury Program Regional Rehabilitation Centre at the Hamilton General Hospital Table of Contents Page Introduction... 3-4 Acquired Brain Injury Program Philosophy... 3 Vision... 3 Service
Community Stroke Rehabilitation Model May, 2013
 Community Stroke Rehabilitation Model May, 2013 Community Stroke Rehabilitation Model May 2013 i Table of Contents EXECUTIVE SUMMARY... ii BACKGROUND...1 HNHB LHIN GEOGRAPHY AND POPULATION...1 STROKE AND
Community Stroke Rehabilitation Model May, 2013 Community Stroke Rehabilitation Model May 2013 i Table of Contents EXECUTIVE SUMMARY... ii BACKGROUND...1 HNHB LHIN GEOGRAPHY AND POPULATION...1 STROKE AND
Discharge Information Information for patients This leaflet is intended to help you, your carer, relatives and friends understand and prepare for
 Discharge Information Information for patients This leaflet is intended to help you, your carer, relatives and friends understand and prepare for your discharge or transfer from hospital. Healthcare professionals
Discharge Information Information for patients This leaflet is intended to help you, your carer, relatives and friends understand and prepare for your discharge or transfer from hospital. Healthcare professionals
GENERAL ADMISSION CRITERIA INPATIENT REHABILITATION PROGRAMS
 Originator: Case Management Original Date: 9/94 Review/Revision: 6/96, 2/98, 1/01, 4/02, 8/04, 3/06, 03/10, 3/11, 3/13 Stakeholders: Case Management, Medical Staff, Nursing, Inpatient Therapy GENERAL ADMISSION
Originator: Case Management Original Date: 9/94 Review/Revision: 6/96, 2/98, 1/01, 4/02, 8/04, 3/06, 03/10, 3/11, 3/13 Stakeholders: Case Management, Medical Staff, Nursing, Inpatient Therapy GENERAL ADMISSION
Stroke Rehabilitation - Evidence Based Practice
 Stroke Rehabilitation - Evidence Based Practice Section 1 1) What percent of stroke patients are left with moderate functional impairment? a) 25% b) 40% c) 55% d) 70% 2) Which is not a component of the
Stroke Rehabilitation - Evidence Based Practice Section 1 1) What percent of stroke patients are left with moderate functional impairment? a) 25% b) 40% c) 55% d) 70% 2) Which is not a component of the
Pathways of Care for People With Stroke in Ontario
 July 2012 Pathways of Care for People With Stroke in Ontario Health System Performance Overview Stroke represents a significant burden for patients, their families and the health care system. It is a leading
July 2012 Pathways of Care for People With Stroke in Ontario Health System Performance Overview Stroke represents a significant burden for patients, their families and the health care system. It is a leading
Current State Review of Outpatient Rehabilitation Services in Ontario 2
 Current State Review of Outpatient Rehabilitation Services Available at Ontario Acute and Rehabilitation Hospitals and Recommendations to Optimize the System October 2011 Contents Executive Summary...
Current State Review of Outpatient Rehabilitation Services Available at Ontario Acute and Rehabilitation Hospitals and Recommendations to Optimize the System October 2011 Contents Executive Summary...
fact sheet Acquired Brain Injury Questions to Consider When Selecting a Rehabilitation Treatment Program
 fact sheet 2020 Peachtree Rd. N.W. Atlanta, GA 30309 404-352-2020 shepherd.org Acquired Brain Injury Questions to Consider When Selecting a Rehabilitation Treatment Program Choosing a rehabilitation facility
fact sheet 2020 Peachtree Rd. N.W. Atlanta, GA 30309 404-352-2020 shepherd.org Acquired Brain Injury Questions to Consider When Selecting a Rehabilitation Treatment Program Choosing a rehabilitation facility
Background. Does the Organization of Post- Acute Stroke Care Really Matter? Changes in Provider Supply. Sites for Post-Acute Care.
 Does the Organization of Post- Acute Stroke Care Really Matter? Pamela W. Duncan, PhD, FAPTA University of Florida Brooks Center for Rehabilitation Studies Department of Veteran Affairs Rehabilitation
Does the Organization of Post- Acute Stroke Care Really Matter? Pamela W. Duncan, PhD, FAPTA University of Florida Brooks Center for Rehabilitation Studies Department of Veteran Affairs Rehabilitation
BEYOND ACUTE CARE: NEXT STEPS IN UNDERSTANDING ALC DAYS
 BEYOND ACUTE CARE: NEXT STEPS IN UNDERSTANDING ALC DAYS MARCH 19, 2008 1.0 EXECUTIVE SUMMARY In its continued efforts to improve the delivery of and access to rehabilitation services, the GTA Rehab Network
BEYOND ACUTE CARE: NEXT STEPS IN UNDERSTANDING ALC DAYS MARCH 19, 2008 1.0 EXECUTIVE SUMMARY In its continued efforts to improve the delivery of and access to rehabilitation services, the GTA Rehab Network
The Sector Linkage Model for Improved Patient Flow. Dr. Peter Nord
 The Sector Linkage Model for Improved Patient Flow Dr. Peter Nord Based on Premise that Better Quality Outcomes Result from Better Flow Healing Trajectories Current & Future Health Status Measures (FIM)
The Sector Linkage Model for Improved Patient Flow Dr. Peter Nord Based on Premise that Better Quality Outcomes Result from Better Flow Healing Trajectories Current & Future Health Status Measures (FIM)
INTERPROFESSIONAL LEARNING OBJECTIVES FOR STROKE CARE INTRODUCTION
 INTERPROFESSIONAL LEARNING OBJECTIVES FOR STROKE CARE INTRODUCTION Supporting Interprofessional Education through Shared Learning Opportunities APRIL 2007 Interprofessional Learning Objectives for Stroke
INTERPROFESSIONAL LEARNING OBJECTIVES FOR STROKE CARE INTRODUCTION Supporting Interprofessional Education through Shared Learning Opportunities APRIL 2007 Interprofessional Learning Objectives for Stroke
Pediatric and Adolescent Brain Injury Rehabilitation Program
 Pediatric and Adolescent Brain Injury Rehabilitation Program Services Provided Physical Therapy Vision Therapy Educational Therapy Behavioral Intervention Speech-Language Pathology Secondary Education
Pediatric and Adolescent Brain Injury Rehabilitation Program Services Provided Physical Therapy Vision Therapy Educational Therapy Behavioral Intervention Speech-Language Pathology Secondary Education
AlphaFIM Instrument Too ol1 Mild Stroke Project (Part II) Report
 Report") 1 AlphaFIM Instrument Tool 1 Mild Stroke Project (Part II) Report Prepared by: Carmel Forrestal Regional Stroke Rehab Coordinator 1 The FIM instrument and AlphaFIM instrument referenced herein are the
1 AlphaFIM Instrument Tool 1 Mild Stroke Project (Part II) Report Prepared by: Carmel Forrestal Regional Stroke Rehab Coordinator 1 The FIM instrument and AlphaFIM instrument referenced herein are the
Key Terms. Chapter 38. Disability, p. 640. Rehabilitation, p. 640. Rehab (cont) p. 640. Rehab. (cont), p. 640
 p. 640. Rehab. (cont), p. 640") Key Terms Chapter 38 Rehabilitation & Restorative Care Activities of daily living (ADL s) Disability Rehabilitation Restorative aide Restorative nursing care Disability, p. 640 Is any loss, absent, or
Key Terms Chapter 38 Rehabilitation & Restorative Care Activities of daily living (ADL s) Disability Rehabilitation Restorative aide Restorative nursing care Disability, p. 640 Is any loss, absent, or
Inpatient Rehabilitation Facilities (IRFs) [Preauthorization Required]
![Inpatient Rehabilitation Facilities (IRFs) [Preauthorization Required]](/thumbs/25/4903617.jpg "Inpatient Rehabilitation Facilities (IRFs) [Preauthorization Required]") Inpatient Rehabilitation Facilities (IRFs) [Preauthorization Required] Medical Policy: MP-ME-05-09 Original Effective Date: February 18, 2009 Reviewed: April 22, 2011 Revised: This policy applies to products
Inpatient Rehabilitation Facilities (IRFs) [Preauthorization Required] Medical Policy: MP-ME-05-09 Original Effective Date: February 18, 2009 Reviewed: April 22, 2011 Revised: This policy applies to products