ND Health Enterprise MMIS ADA-Dental Claim Form Instructions
|
|
|
- Bennett Briggs
- 8 years ago
- Views:
Transcription
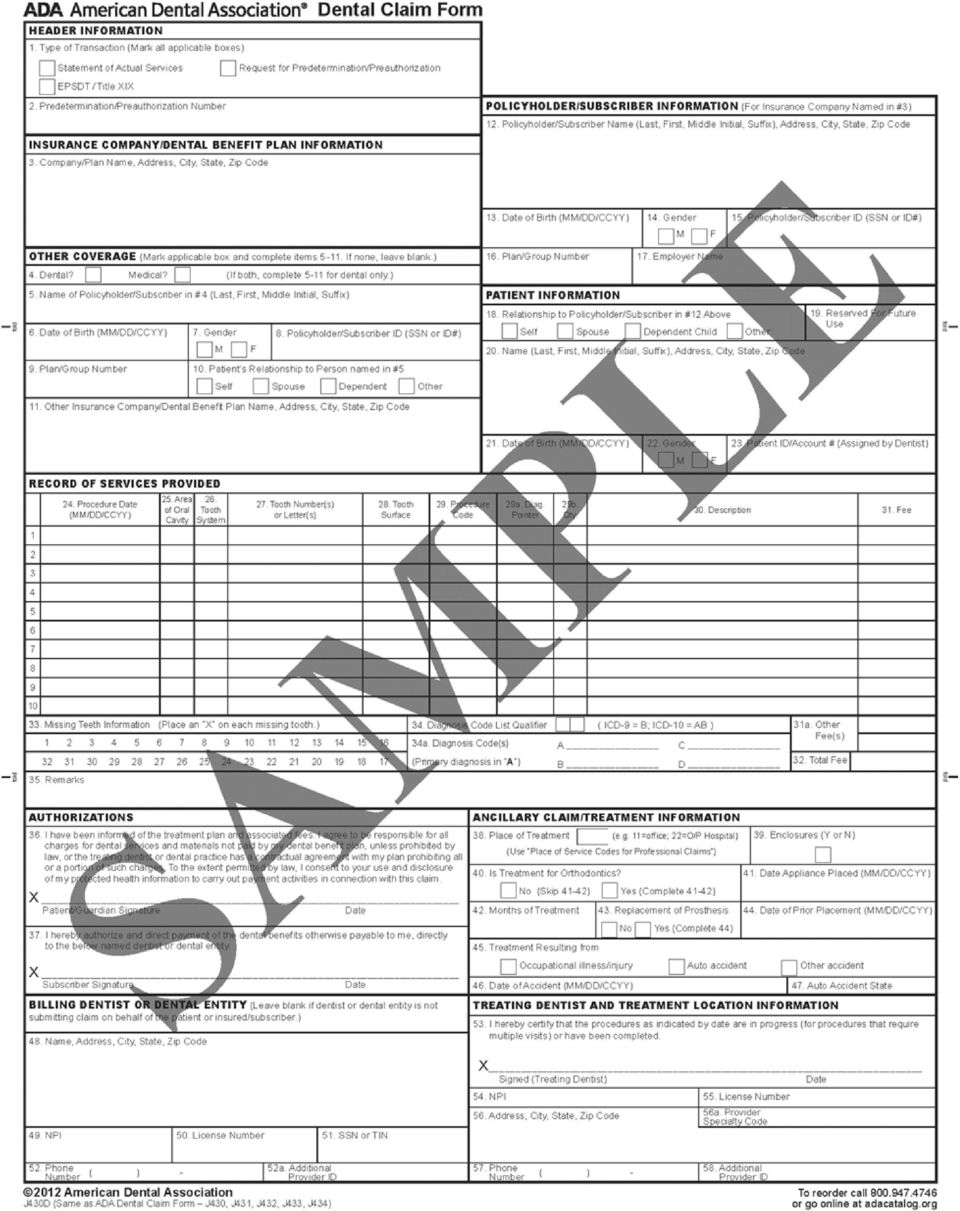
1 October 2015 ND Health Enterprise MMIS ADA-Dental Claim Form Instructions These instructions address the North Dakota Health Enterprise MMIS paper claim requirements. You must be an enrolled ND Medicaid provider to submit a claim. If you are not an enrolled provider, you can apply at: Enrollment instructions, updates, billing manuals, and companion guides are available online at Questions If you have any questions, please call the ND Health Enterprise MMIS Call Center at Claims Mailing Address ND Department of Human Services Medical Services Division Department East Boulevard Ave Bismarck, ND

2 Field Requirement Definitions Required Fields marked Required in the claim form instructions are required on all paper claim submissions. The claim will be denied if a Required field is incomplete. Not Required Fields marked Not Required are not used in processing the claim. Providers are free to populate the field if desired. Recommended Fields marked Recommended are not required, but will be returned with the provider s remittance advice if supplied on the claim. For example, if the provider's in-house patient account number is provided, it will be returned on the remittance advice, thereby allowing billing staff to cross reference the claim with the provider s records. Situational Fields marked Situational are required when they apply to the claim 2

3 Field Requirement Field Name and Description 1 Required Type of Transaction: Check statement of actual services. Also check EPSDT/Title XIX box if this claim is for a member under age Situational Predetermination/Preauthorization Number: Enter the 12-digit authorization number if you are submitting a claim for a service that was prior authorized. Only enter one authorization number per claim form. 3 Not Required Company/Plan Name, Address, City, State, ZIP Code 4 Situational Other Coverage: Mark the box after Dental if a member has coverage under any other dental plan. When the dental box is marked, complete Fields 5 through Situational Name of Policyholder/Subscriber with other Coverage Indicated in #4 (Last, First, Middle Initial): If the member has other coverage through a spouse, or if a child through both parents, enter the name of the policyholder of the other coverage. 6 Situational Date of Birth (MM/DD/YYYY): If there is TPL, enter the birth date of the policyholder. 7 Situational Gender: If there is TPL, mark the appropriate box to specify the policyholder s gender. 8 Situational Policyholder/Subscriber Identifier (SSN or ID#): If there is TPL, enter the policyholder s unique identifier for that policy. 9 Situational Plan/Group Number: Enter the group plan/policy number of the person named in Field Situational Patient s Relationship to Person Named in Field 5: Mark the relationship of the member to the policyholder identified in Field Situational Other Insurance Company/Dental Benefit Plan Name, Address, City, State, and ZIP Code: If the member has dental insurance, enter the name and address of the other carrier. 12 Required Subscriber/Policyholder name (Last, First, Middle Initial), Address, City, State, and ZIP Code: Enter the member s full name and complete address. 13 Required Date of Birth (MM/DD/YYYY): Enter the member s birth date. 14 Required Gender: Mark the appropriate box to specify the member s gender. 15 Required Policyholder/Subscriber Identifier (SSN or ID#): Enter the member s 9-digit member ID. 16 Not Required Plan/Group number 17 Not Required Employer Name 18 Not Required Relationship to policyholder/subscriber in Field 12 above 19 Not Required Reserved for future use 3

4 20 Not Required Name (Last, First, Middle Initial), Address, City, State, ZIP Code 21 Not Required Date of Birth (MM/DD/YYYY) 22 Not Required Gender 23 Recommended Patient ID/Account #: Enter the member s unique control number assigned by the provider (internal patient account number). 24 Required Procedure Date (MM/DD/YYYY): Enter the date the service was provided. 25 Situational Are of Oral Cavity: Enter the quadrant when applicable. Ex: 10, 20, 30, Not Required Tooth System 27 Situational Tooth Number(s) or Letter(s): When the procedure directly involves a tooth or range of teeth, enter tooth number(s) 1-32 for permanent dentition, for supernumerary teeth, A-T for primary dentition or AS-TS for primary supernumerary teeth. If the same procedure is performed on more than a single tooth on the same date of service, report each procedure and tooth involved on separate lines on the claim form. When reporting a range of teeth, use a hyphen - to separate the first and last tooth in the range (e.g., 1-4, 7-10, 22-27), or use commas to separate individual tooth numbers or ranges (e.g., 1, 2, 4, 7-10, 3-5, 22-27). 28 Situational Tooth Surface: Enter a tooth surface code. The following single letter codes are used to identify surfaces: B for Buccal, D for Distal, F for Facial, I for Incisal, L for Lingual, M for Mesial and O for Occlusal. 29 Required Procedure Code: Enter the appropriate procedure code for the service provided. 29a Not Required Diagnosis Pointer: Enter the diagnosis pointer (A-D) on this claim line for diagnosis codes entered in Field 34a. 29b Not Required Quantity 30 Required Description of Service 31 Required Fee: Enter your usual and customary charge for the procedure on each claim line. 31a Situational Other Fee(s): Enter the exact TPL payment (do not include contractual write-offs). 4
 or Letter(s): When the procedure directly involves a tooth or range of teeth, enter tooth number(s) 1-32 for permanent dentition, 51-82 for")
5 32 Required Total Fee: Single page claim or last page of a multi-page claim. If Medicaid is primary; enter the amount of total covered charges for all pages on Line A. If there is TPL, enter the total charges less prior payment. Do not include write-off or contractual adjustment amounts. 33 Not Required Missing Teeth Information 34 Not Required Diagnosis Code List Qualifier 34a Not Required Diagnosis Code(s): Enter up to 4 applicable diagnosis codes after each letter (A-D). The primary diagnosis code is entered adjacent to the letter A. 35 Situational Remarks: Field is used to submit a Void or Replacement claim. Complete this Field to replace or void a previously paid claim. Otherwise, leave this Field blank. See Void and Replace information on page Not Required Patient/Guardian Signature, Date 37 Not Required Subscriber Signature, Date 38 Required Place of Treatment: Enter the 2-digit Place of Service Code for Professional Claims. Frequently used codes are 11 = office; 12 = home; 21 = inpatient hospital; 22 = outpatient hospital; 31 = skilled nursing facility; 32 = nursing facility. 39 Not Required Number of enclosures 40 Not Required Is Treatment for Orthodontics? 41 Not Required Date Appliance Placed (MM/DD/YYYY) 42 Not Required Months of Treatment Remaining 43 Not Required Replacement of Prosthesis 44 Not Required Date Prior Placement (MM/DD/YYYY) 45 Situational Treatment Resulting From: If treatment/services were provided as a result of an occupational illness/injury, auto accident, or other accident, check the appropriate box and complete Field 46. If treatment is a result of an auto accident, also complete Field Situational Date of Accident (MM/DD/YYYY): Enter the date on which the accident noted in Field 45 occurred. 47 Situational Auto Accident State: Enter the state in which the auto accident noted in Field 45 occurred. 48 Required Billing Dentist or Dental Entity: Enter the name and address of the billing provider. 49 Required NPI (National Provider Identifier): Enter the 10-digit NPI of the billing provider or group. 50 Not Required License Number 5

6 51 Required SSN or TIN: Enter the federal tax ID number of the billing provider or entity. If a billing provider does not have a federal tax ID number, a Social Security Number may be used. 52 Not Required Phone Number 52a Required Additional Provider ID. Enter the Taxonomy for the billing provider. Example: 1223G0001X 53 Required Treating Dentist and Treatment Location Information. Certification: The provider who rendered the service(s) must sign and date this Field. Original, rubber-stamped and electronic signatures are acceptable. 54 Required NPI (National Provider Identifier): Enter the NPI of treating provider. 55 Not Required License Number 56 Required Address, City, State, ZIP Code: Enter the address where the services were rendered. 56a Required Provider Specialty Code: Enter the servicing provider s Taxonomy code. Example: 1223G0001X 57 Not Required Phone Number: Enter the servicing provider s phone number. 58 Not Required Additional Provider ID 6
: Enter the NPI of treating provider.")
7 Replacing a Claim A claim replacement may be submitted to modify a previously paid claim. Timely filing limits apply. To submit a claim replacement, complete the claim form fields below: Field 35: Enter the Resubmission Code of 7 and then enter the claim's Transaction Control Number (TCN) or Internal Control Number (ICN). If replacing a claim processed in the ND Health Enterprise MMIS, enter the 17-digit TCN for the previously processed claim. If replacing a claim processed in the ND Legacy MMIS insert the century code in the 3rd and 4th positions of the ICN. Enter the 15- digit ICN for the previously processed claim. Example: Legacy ICN: Replaced Legacy ICN: Voiding a Claim Voiding a claim reverses a previously processed Medicaid claim. Timely filing limits apply. To submit a claim void, complete the claim form fields below: Field 35: Enter the Resubmission Code of 8 and then enter the claim's Transaction Control Number (TCN) or Internal Control Number (ICN). If voiding a claim processed in the ND Health Enterprise MMIS, enter the 17-digit TCN for the previously processed claim. If voiding a claim processed in the ND Legacy MMIS insert the century code in the 3rd and 4th positions of the ICN. Enter the 15-digit ICN for the previously processed claim. Example: Legacy ICN: Replaced Legacy ICN:


8 8
9 Revision History Section Topic Location Revision Date All Change header revision date from June 2015 to All pages 10/26/15 Oct 2015 Intro Updated contact history. Page 1 10/26/15 52a Remove reference to qualifier code of ZZ and Page 6 10/26/15 remove reference to ZZ on example 54 Remove reference to qualifier code of XX Page 6 10/26/15 56a Remove reference to qualifier code of ZZ and remove reference to ZZ qualifier on example Page 6 10/26/15 9

2012 ADA Dental Claim Form Instructions
 2012 ADA Dental Claim Form Instructions June 9, 2015 Date (mm/dd/yyyy) Description of Changes Impact 02/11/2014 Initial version 07/16/2014 Updated instructions for fields 29a and 32 06/09/2015 Clarified
2012 ADA Dental Claim Form Instructions June 9, 2015 Date (mm/dd/yyyy) Description of Changes Impact 02/11/2014 Initial version 07/16/2014 Updated instructions for fields 29a and 32 06/09/2015 Clarified
2012 American Dental Association Claim Form Completion Instructions
 01 American Dental Association Claim Form Completion Instructions COMPLETING THE ADA CLAIM FORM The following instructions explain how to complete the ADA Claim Form and whether a field is Required, Required
01 American Dental Association Claim Form Completion Instructions COMPLETING THE ADA CLAIM FORM The following instructions explain how to complete the ADA Claim Form and whether a field is Required, Required
ADA Dental Claim Form (2012 American Dental Association) Completion Instructions Page 1 of 17
 Completion Instructions Page 1 of 17") Page 1 of 17 Introduction The ADA Dental Claim Form has been revised to incorporate key changes to the HIPAA standard electronic dental claim transaction. This version of the form, front and reverse sides,
Page 1 of 17 Introduction The ADA Dental Claim Form has been revised to incorporate key changes to the HIPAA standard electronic dental claim transaction. This version of the form, front and reverse sides,
POLICY HOLDER/SUBSCRIBER INFORMATION
 Dental Claim Form Instructions Claim Field Identification 1. Type of Transaction Statement of Actual Services EPSDT/Title XIX Request for Predetermination 2. Predetermination/ Prior Authorization Code
Dental Claim Form Instructions Claim Field Identification 1. Type of Transaction Statement of Actual Services EPSDT/Title XIX Request for Predetermination 2. Predetermination/ Prior Authorization Code
UHIN STANDARDS COMMITTEE Version 3.2 5010 Dental Claim Billing Standard J430
 UHIN STANDARDS COMMITTEE Version 3.2 5010 Dental Claim Billing Standard J430 Purpose: The purpose of the Dental Billing Standard, is to clearly describe the standard use of each Item Number (for print
UHIN STANDARDS COMMITTEE Version 3.2 5010 Dental Claim Billing Standard J430 Purpose: The purpose of the Dental Billing Standard, is to clearly describe the standard use of each Item Number (for print
The following provider types should bill using the Dental claim form:
 Section: 4.0 Dental Claim Form This section explains the procedures for obtaining reimbursement for dental services submitted to Medicaid. Mississippi Medicaid accepts both electronic and paper dental
Section: 4.0 Dental Claim Form This section explains the procedures for obtaining reimbursement for dental services submitted to Medicaid. Mississippi Medicaid accepts both electronic and paper dental
ADA 2006 Paper Claim Form Changes and Requirements
 INDIANA HEALTH COVERAGE PROGRAMS P R O V I D E R B U L L E T I N B T 2 0 0 7 0 5 F E B R U A R Y 1 3, 2 0 0 7 To: All Dental Providers Subject: Overview The Indiana Health Coverage Program (IHCP) will
INDIANA HEALTH COVERAGE PROGRAMS P R O V I D E R B U L L E T I N B T 2 0 0 7 0 5 F E B R U A R Y 1 3, 2 0 0 7 To: All Dental Providers Subject: Overview The Indiana Health Coverage Program (IHCP) will
Providers must attach a copy of the payer s EOB with the UnitedHealthcare Community Plan dental claim (2012 ADA form).
.") UnitedHealthcare Community Plan (formerly APIPA) Medicaid Dental Claims and Billing Process Effective Dates of Service October 01, 2015 or after AHCCCS Provider Identification Number and NPI Number All
UnitedHealthcare Community Plan (formerly APIPA) Medicaid Dental Claims and Billing Process Effective Dates of Service October 01, 2015 or after AHCCCS Provider Identification Number and NPI Number All
ADA Claim Form Version 2012 Completion Aid for Dentists
 Prior Authorization/Benefit Limit Exception Request Purpose of the document Document format The purpose of this document is to provide a block-by-block reference guide to assist the following provider
Prior Authorization/Benefit Limit Exception Request Purpose of the document Document format The purpose of this document is to provide a block-by-block reference guide to assist the following provider
Dental Billing Instructions
 Dental Billing Instructions DIVISION OF MEDICAL ASSISTANCE PROGRAMS Billing instructions for Provider Web Portal and ADA 2012 dental claim formats for Oregon Medicaid providers April 2014 Contents Introduction...
Dental Billing Instructions DIVISION OF MEDICAL ASSISTANCE PROGRAMS Billing instructions for Provider Web Portal and ADA 2012 dental claim formats for Oregon Medicaid providers April 2014 Contents Introduction...
CHAPTER 7 (E) DENTAL PROGRAM CLAIMS FILING CHAPTER CONTENTS
 DENTAL PROGRAM CLAIMS FILING CHAPTER CONTENTS") CHAPTER 7 (E) DENTAL PROGRAM CHAPTER CONTENTS 7.0 CLAIMS SUBMISSION AND PROCESSING...1 7.1 ELECTRONIC MEDIA CLAIMS (EMC) FILING...1 7.2 CLAIMS DOCUMENTATION...2 7.3 THIRD PARTY LIABILITY (TPL)...2 7.4
CHAPTER 7 (E) DENTAL PROGRAM CHAPTER CONTENTS 7.0 CLAIMS SUBMISSION AND PROCESSING...1 7.1 ELECTRONIC MEDIA CLAIMS (EMC) FILING...1 7.2 CLAIMS DOCUMENTATION...2 7.3 THIRD PARTY LIABILITY (TPL)...2 7.4
Examples of a Suffix are: Jr. or Sr. 5. Optionally, enter the Beneficiary s Suffix. Beneficiary Information. 6. Enter the Beneficiary s Date of Birth
 Submit Dental Claims Online (Direct Data Entry) Quick Reference Business Rules o Fields marked with an asterisk (*) are required and must be completed for the Claim to be submitted successfully. o DDE
Submit Dental Claims Online (Direct Data Entry) Quick Reference Business Rules o Fields marked with an asterisk (*) are required and must be completed for the Claim to be submitted successfully. o DDE
MITS WEB PORTAL BILLING GUIDE FOR DENTAL CLAIMS
 MITS WEB PORTAL BILLING GUIDE FOR DENTAL CLAIMS Revised 2011.12.21 Fields marked with an asterisk (*) require an entry. Information entered into a field must be "recorded" before the system can use it.
MITS WEB PORTAL BILLING GUIDE FOR DENTAL CLAIMS Revised 2011.12.21 Fields marked with an asterisk (*) require an entry. Information entered into a field must be "recorded" before the system can use it.
Dental Benefits Summary Delta Dental PPO plus Premier WESLEYAN UNIVERSITY. Group # 6507
 Dental Benefits Summary Delta Dental PPO plus Premier WESLEYAN UNIVERSITY Group # 6507 January 1, 2011 Topics Covered in This Booklet Page 1 About This Brochure 1 About Delta Dental 1 How to Use Your Program
Dental Benefits Summary Delta Dental PPO plus Premier WESLEYAN UNIVERSITY Group # 6507 January 1, 2011 Topics Covered in This Booklet Page 1 About This Brochure 1 About Delta Dental 1 How to Use Your Program
Dental Benefits Summary Delta Dental PPO plus Premier INTERNATIONAL UNION OF OPERATING ENGINEERS LOCAL NO. 478. Group # 4634
 Dental Benefits Summary Delta Dental PPO plus Premier INTERNATIONAL UNION OF OPERATING ENGINEERS LOCAL NO. 478 Group # 4634 Topics Covered in This Booklet Page 1 About This Brochure 1 About Delta Dental
Dental Benefits Summary Delta Dental PPO plus Premier INTERNATIONAL UNION OF OPERATING ENGINEERS LOCAL NO. 478 Group # 4634 Topics Covered in This Booklet Page 1 About This Brochure 1 About Delta Dental
Dental Benefits Summary Delta Dental PPO plus Premier CENTENARY COLLEGE. Group # 7656
 Dental Benefits Summary Delta Dental PPO plus Premier CENTENARY COLLEGE Group # 7656 Topics Covered in This Booklet Page 1 About This Brochure 1 About Delta Dental 1 How to Use Your Program 2 Locating
Dental Benefits Summary Delta Dental PPO plus Premier CENTENARY COLLEGE Group # 7656 Topics Covered in This Booklet Page 1 About This Brochure 1 About Delta Dental 1 How to Use Your Program 2 Locating
Medicaid Management Information Systems
 Medicaid Management Information Systems Maine Integrated Health Management Solution Health PAS Online: Dental Claim Submission and Claim Status User Guide Date of Publication: 09/02/2015 Document Number:
Medicaid Management Information Systems Maine Integrated Health Management Solution Health PAS Online: Dental Claim Submission and Claim Status User Guide Date of Publication: 09/02/2015 Document Number:
You must write REHAB at the top center of the claim form!
 CMS 1500 (02/12 INSTRUCTIONS FOR REHABILITATION CENTER SERVICES You must write REHAB at the top center of the claim form! Locator # Description Instructions Alerts 1 Medicare / Medicaid / Tricare Champus
CMS 1500 (02/12 INSTRUCTIONS FOR REHABILITATION CENTER SERVICES You must write REHAB at the top center of the claim form! Locator # Description Instructions Alerts 1 Medicare / Medicaid / Tricare Champus
DDE for Dental Claims Submission
 DDE for Dental Claims Submission Purpose: The Health PAS-Online application will enable Dental Providers to bill and adjust claims electronically. To access Health PAS- Online, logon to http://provider.kymmis.com
DDE for Dental Claims Submission Purpose: The Health PAS-Online application will enable Dental Providers to bill and adjust claims electronically. To access Health PAS- Online, logon to http://provider.kymmis.com
Minnesota Health Care Programs (MHCP) MN ITS Interactive User Guide http://mn-its.dhs.state.mn.us. Using MN ITS Interactive. Entering an Online Claim
 MN ITS Interactive User Guide http://mn-its.dhs.state.mn.us. Using MN ITS Interactive. Entering an Online Claim") Minnesota Health Care Programs (MHCP) MN ITS Interactive User Guide http://mn-its.dhs.state.mn.us Objective Performed by Background Claim Form Completing a MN ITS Interactive Professional (837P) claim
Minnesota Health Care Programs (MHCP) MN ITS Interactive User Guide http://mn-its.dhs.state.mn.us Objective Performed by Background Claim Form Completing a MN ITS Interactive Professional (837P) claim
International Emergency and Expatriate Dental Program Instructions for Dentists
 International Emergency and Expatriate Dental Program Instructions for Dentists PROGRAM OUTLINE We want to ensure you have the information you need to assist our members. Members of Delta Dental of Minnesota,
International Emergency and Expatriate Dental Program Instructions for Dentists PROGRAM OUTLINE We want to ensure you have the information you need to assist our members. Members of Delta Dental of Minnesota,
CMS 1500 (02/12) CLAIM FORM INSTRUCTIONS
 CLAIM FORM INSTRUCTIONS") CMS 1500 (02/12) CLAIM FORM INSTRUCTIONS FIELD NUMBER FIELD NAME 1 a INSURED S ID NUMBER INSTRUCTIONS Enter the patient s nine digit Medicaid identification number (SSN) 2 PATIENT S NAME Enter the recipient
CMS 1500 (02/12) CLAIM FORM INSTRUCTIONS FIELD NUMBER FIELD NAME 1 a INSURED S ID NUMBER INSTRUCTIONS Enter the patient s nine digit Medicaid identification number (SSN) 2 PATIENT S NAME Enter the recipient
CMS 1500 Training 101
 CMS 1500 Training 101 HP Enterprise Services Learning Objective Welcome, this training presentation will educate you on how to complete a CMS 1500 claim form; this includes a detailed explanation of all
CMS 1500 Training 101 HP Enterprise Services Learning Objective Welcome, this training presentation will educate you on how to complete a CMS 1500 claim form; this includes a detailed explanation of all
Dental Benefits Summary Delta Dental PPO plus Premier
 Dental Benefits Summary Delta Dental PPO plus Premier Yale Graduate & Professional Student Dental Plan Group # 4255 October 1, 2013 Topics Covered in This Booklet Page 1 About This Brochure 1 About Delta
Dental Benefits Summary Delta Dental PPO plus Premier Yale Graduate & Professional Student Dental Plan Group # 4255 October 1, 2013 Topics Covered in This Booklet Page 1 About This Brochure 1 About Delta
CLAIMS AND BILLING INSTRUCTIONAL MANUAL
 CLAIMS AND BILLING INSTRUCTIONAL MANUAL 2007 TABLE OF ONTENTS Paper Claims and Block Grant Submission Requirements... 3 State Requirements for Claims Turnaround Time... 12 Claims Appeal Process... 13 Third
CLAIMS AND BILLING INSTRUCTIONAL MANUAL 2007 TABLE OF ONTENTS Paper Claims and Block Grant Submission Requirements... 3 State Requirements for Claims Turnaround Time... 12 Claims Appeal Process... 13 Third
UB04 INSTRUCTIONS Home Health
 UB04 INSTRUCTIONS Home Health 1 Provider Name, Address, Telephone 2 Pay to Name/Address/ID Required. Enter the name and address of the facility Situational. Enter the name, address, and Louisiana Medicaid
UB04 INSTRUCTIONS Home Health 1 Provider Name, Address, Telephone 2 Pay to Name/Address/ID Required. Enter the name and address of the facility Situational. Enter the name, address, and Louisiana Medicaid
Chapter 5. Billing on the CMS 1500 Claim Form
 Chapter 5 Billing on the CMS 1500 Claim Form This Page Intentionally Left Blank Fee-For-Service Provider Manual April 2012 Billing on the UB-04 Claim Form Chapter: 5 Page: 5-2 INTRODUCTION The CMS 1500
Chapter 5 Billing on the CMS 1500 Claim Form This Page Intentionally Left Blank Fee-For-Service Provider Manual April 2012 Billing on the UB-04 Claim Form Chapter: 5 Page: 5-2 INTRODUCTION The CMS 1500
1. Coverage Indicator Enter an "X" in the appropriate box.
 CMS 1500 Claim Form FIELD NAME INSTRUCTIONS 1. Coverage Indicator Enter an "X" in the appropriate box. 1a. Insured's ID Number Enter the patient's nine-digit Medical Assistance identification number (SSN).
CMS 1500 Claim Form FIELD NAME INSTRUCTIONS 1. Coverage Indicator Enter an "X" in the appropriate box. 1a. Insured's ID Number Enter the patient's nine-digit Medical Assistance identification number (SSN).
ND HEALTH ENTERPRISE MMIS PHASE III TRAINING SUBMITTING DENTAL CLAIMS ONLINE JANUARY 2016
 ND HEALTH ENTERPRISE MMIS PHASE III TRAINING SUBMITTING DENTAL CLAIMS ONLINE JANUARY 2016 1 Today we will learn how to create, save and submit Dental claims using ND Health Enterprise MMIS. Learning Objectives:
ND HEALTH ENTERPRISE MMIS PHASE III TRAINING SUBMITTING DENTAL CLAIMS ONLINE JANUARY 2016 1 Today we will learn how to create, save and submit Dental claims using ND Health Enterprise MMIS. Learning Objectives:
Dental Benefits Summary Delta Dental PPO plus Premier Delta Dental PPO SM PPI/COMCO. Group # 3449
 Dental Benefits Summary Delta Dental PPO plus Premier Delta Dental PPO SM PPI/COMCO Group # 3449 Topics Covered in This Booklet About This Brochure About Delta Dental How to Use Your Program Locating a
Dental Benefits Summary Delta Dental PPO plus Premier Delta Dental PPO SM PPI/COMCO Group # 3449 Topics Covered in This Booklet About This Brochure About Delta Dental How to Use Your Program Locating a
SOUTH CAROLINA MEDICAID WEB-BASED CLAIMS SUBMISSION TOOL
 SOUTH CAROLINA MEDICAID WEB-BASED CLAIMS SUBMISSION TOOL User Guide Addendum CMS-500 October 28, 2003 Updated June 03, 203 CMS-500 CLAIMS ENTRY This document describes the correspondence between the South
SOUTH CAROLINA MEDICAID WEB-BASED CLAIMS SUBMISSION TOOL User Guide Addendum CMS-500 October 28, 2003 Updated June 03, 203 CMS-500 CLAIMS ENTRY This document describes the correspondence between the South
Electronic Transaction Manual for Arkansas Blue Cross and Blue Shield FEDERAL EMPLOYEE PROGRAM (FEP) Dental Claims
 Dental Claims") Electronic Transaction Manual for Arkansas Blue Cross and Blue Shield FEDERAL EMPLOYEE PROGRAM (FEP) Dental Claims HIPAA Transaction Companion Document Guide Refers to the X12N Implementation Guide: 005010X224A2:
Electronic Transaction Manual for Arkansas Blue Cross and Blue Shield FEDERAL EMPLOYEE PROGRAM (FEP) Dental Claims HIPAA Transaction Companion Document Guide Refers to the X12N Implementation Guide: 005010X224A2:
Data Layouts and Formats
 Data Layouts and Formats Pharmacy, Dental, and Provider Files March 13, 2008 INSTITUTE FOR CHILD HEALTH POLICY 1 ENCOUNTERS SUBMISSION GUIDELINES 03/13//2008 Table of Contents 1. INTRODUCTION 3 2. GENERAL
Data Layouts and Formats Pharmacy, Dental, and Provider Files March 13, 2008 INSTITUTE FOR CHILD HEALTH POLICY 1 ENCOUNTERS SUBMISSION GUIDELINES 03/13//2008 Table of Contents 1. INTRODUCTION 3 2. GENERAL
Chapter 4 - Billing Instructions Table of Contents
 Chapter 4 - Billing Instructions Table of Contents A. General Information 4-1 B. Provider Bill Type Form Requirements 4-2 C. General Form Instructions 4-2 D. CMS-1500 Form 4-3 E. UB-04 Form 4-8 F. Service
Chapter 4 - Billing Instructions Table of Contents A. General Information 4-1 B. Provider Bill Type Form Requirements 4-2 C. General Form Instructions 4-2 D. CMS-1500 Form 4-3 E. UB-04 Form 4-8 F. Service
CMS-1500 Billing Guide for PROMISe Audiologists
 CMS-1500 Billing Guide for PROMISe udiologists Purpose of the document Document format The purpose of this document is to provide a block-by-block reference guide to assist the following provider types
CMS-1500 Billing Guide for PROMISe udiologists Purpose of the document Document format The purpose of this document is to provide a block-by-block reference guide to assist the following provider types
Chapter 8 Billing on the CMS 1500 Claim Form
 8 Billing on the CMS 1500 Claim form INTRODUCTION The CMS 1500 claim form is used to bill for non-facility services, including professional services, freestanding surgery centers, transportation, durable
8 Billing on the CMS 1500 Claim form INTRODUCTION The CMS 1500 claim form is used to bill for non-facility services, including professional services, freestanding surgery centers, transportation, durable
Direct Data Entry of a Dental Claim
 Operational instructional series: Direct Data Entry of a Dental Claim Presented by the Provider Relations Team Office of the Chief Medical Officer Washington Medicaid 10-14-2011 1 How to submit a Direct
Operational instructional series: Direct Data Entry of a Dental Claim Presented by the Provider Relations Team Office of the Chief Medical Officer Washington Medicaid 10-14-2011 1 How to submit a Direct
Therapies Physical, Occupational, Speech
 Therapies Physical, Occupational, Speech Provider Manual Volume II April 1, 2013 New Hampshire Medicaid Table of Contents 1. NH MEDICAID PROVIDER BILLING MANUALS OVERVIEW... 1 Intended Audience... 1 Provider
Therapies Physical, Occupational, Speech Provider Manual Volume II April 1, 2013 New Hampshire Medicaid Table of Contents 1. NH MEDICAID PROVIDER BILLING MANUALS OVERVIEW... 1 Intended Audience... 1 Provider
NEW YORK STATE MEDICAID PROGRAM DENTAL BILLING GUIDELINES
 NEW YORK STATE MEDICAID PROGRAM DENTAL BILLING GUIDELINES TABLE OF CONTENTS Section I Purpose Statement...3 Section II Claims Submission... 4 Electronic Claims... 5 Paper Claims... 9 Claim Form A-eMedNY-000201...
NEW YORK STATE MEDICAID PROGRAM DENTAL BILLING GUIDELINES TABLE OF CONTENTS Section I Purpose Statement...3 Section II Claims Submission... 4 Electronic Claims... 5 Paper Claims... 9 Claim Form A-eMedNY-000201...
5010 Gap Analysis for Dental Claims. Based on ASC X12 837 v5010 TR3 X224A2 Version 2.0 August 2010
 5010 Gap Analysis for Dental Claims Based on ASC X12 837 v5010 TR3 X224A2 Version 2.0 August 2010 This information is provided by Emdeon for education and awareness use only. Even though Emdeon believes
5010 Gap Analysis for Dental Claims Based on ASC X12 837 v5010 TR3 X224A2 Version 2.0 August 2010 This information is provided by Emdeon for education and awareness use only. Even though Emdeon believes
You must write AMB at the top center of the claim form!
 CMS 1500 (08/05) INSTRUCTIONS FOR AMBULANCE AND AIR AMBULANCE SERVICES You must write AMB at the top center of the claim form! Locator # Description Instructions Alerts 1 Medicare / Medicaid / Tricare
CMS 1500 (08/05) INSTRUCTIONS FOR AMBULANCE AND AIR AMBULANCE SERVICES You must write AMB at the top center of the claim form! Locator # Description Instructions Alerts 1 Medicare / Medicaid / Tricare
STATE OF MARYLAND KIDNEY DISEASE PROGRAM UB-04. Billing Instructions. for. Freestanding Dialysis Facility Services. Revised 9/1/08.
 STATE OF MARYLAND KIDNEY DISEASE PROGRAM UB-04 Billing Instructions for Freestanding Dialysis Facility Services Revised 9/1/08 Page 1 of 13 UB04 Instructions TABLE of CONTENTS Introduction 4 Sample UB04
STATE OF MARYLAND KIDNEY DISEASE PROGRAM UB-04 Billing Instructions for Freestanding Dialysis Facility Services Revised 9/1/08 Page 1 of 13 UB04 Instructions TABLE of CONTENTS Introduction 4 Sample UB04
Professional Billing Instructions
 Professional Billing Instructions DIVISION OF MEDICAL ASSISTANCE PROGRAMS Billing instructions for CMS- 1500, DMAP 505 and Provider Web Portal professional claim formats for Oregon Medicaid providers August
Professional Billing Instructions DIVISION OF MEDICAL ASSISTANCE PROGRAMS Billing instructions for CMS- 1500, DMAP 505 and Provider Web Portal professional claim formats for Oregon Medicaid providers August
CMS-1500 Billing Guide for PROMISe Certified Registered Nurse Anesthetists (CRNAs)
") CMS-1500 Billing Guide for PRMISe Certified Registered Nurse nesthetists (CRNs) Purpose of the document Document format The purpose of this document is to provide a block-by-block reference guide to assist
CMS-1500 Billing Guide for PRMISe Certified Registered Nurse nesthetists (CRNs) Purpose of the document Document format The purpose of this document is to provide a block-by-block reference guide to assist
NEW YORK STATE MEDICAID PROGRAM CLINICAL SOCIAL WORKER BILLING GUIDELINES
 NEW YORK STATE MEDICAID PROGRAM CLINICAL SOCIAL WORKER BILLING GUIDELINES TABLE OF CONTENTS Section I - Purpose Statement... 2 Section II Claims Submission... 3 Electronic Claims... 3 Paper Claims... 7
NEW YORK STATE MEDICAID PROGRAM CLINICAL SOCIAL WORKER BILLING GUIDELINES TABLE OF CONTENTS Section I - Purpose Statement... 2 Section II Claims Submission... 3 Electronic Claims... 3 Paper Claims... 7
 epaces Help Table Of Contents What is epaces?...1 System Requirements...1 Key Features...2 What's New in epaces...3 Logging Into epaces...4 Navigational Tips...5 Change Provider...8 Enter New Claims...9
epaces Help Table Of Contents What is epaces?...1 System Requirements...1 Key Features...2 What's New in epaces...3 Logging Into epaces...4 Navigational Tips...5 Change Provider...8 Enter New Claims...9
Illustration 1-1. Revised CMS-1500 Claim Form (front)
") Florida Medicaid Provider Reimbursement Handbook, CMS-1500 Illustration 1-1. Revised CMS-1500 Claim Form (front) Incorporated by reference in 59G-4.001, F.A.C. July 2008 1-11 Florida Medicaid Provider
Florida Medicaid Provider Reimbursement Handbook, CMS-1500 Illustration 1-1. Revised CMS-1500 Claim Form (front) Incorporated by reference in 59G-4.001, F.A.C. July 2008 1-11 Florida Medicaid Provider
CMS-1500 Billing Guide for PROMISe Renal Dialysis Centers
 CMS-1500 Billing Guide for PROMISe Renal Purpose of the document Document format The purpose of this document is to provide a block-by-block reference guide to assist the following provider types in successfully
CMS-1500 Billing Guide for PROMISe Renal Purpose of the document Document format The purpose of this document is to provide a block-by-block reference guide to assist the following provider types in successfully
Real Time Responses... 153 Real Time Claim Status Response Details... 154 Claim Level Information... 154 Service Line Information...
 epaces Help Table Of Contents What is epaces?... 1 System Requirements... 2 Key Features... 2 What's New in epaces... 3 June 2014... 3 ICD-10... 3 June 2013... 3 Eligibility Requests... 3 Eligibility
epaces Help Table Of Contents What is epaces?... 1 System Requirements... 2 Key Features... 2 What's New in epaces... 3 June 2014... 3 ICD-10... 3 June 2013... 3 Eligibility Requests... 3 Eligibility
Top 50 Billing Error Reason Codes With Common Resolutions (09-12)
") Top 50 Billing Error Reason Codes With Common Resolutions (09-12) On the following table you will find the top 50 Error Reason Codes with Common Resolutions for denied claims at Virginia Medicaid. This
Top 50 Billing Error Reason Codes With Common Resolutions (09-12) On the following table you will find the top 50 Error Reason Codes with Common Resolutions for denied claims at Virginia Medicaid. This
Billing Manual for In-State Long Term Care Nursing Facilities
 Billing Manual for In-State Long Term Care Nursing Facilities Medical Services North Dakota Department of Human Services 600 E Boulevard Ave, Dept 325 Bismarck, ND 58505 September 2003 INTRODUCTION The
Billing Manual for In-State Long Term Care Nursing Facilities Medical Services North Dakota Department of Human Services 600 E Boulevard Ave, Dept 325 Bismarck, ND 58505 September 2003 INTRODUCTION The
National Uniform Claim Committee. 1500 Health Insurance Claim Form Reference Instruction Manual for Form Version 02/12. June 2013. Version 1.
 National Uniform Claim Committee 1500 Health Insurance Claim Form Reference Instruction Manual for Form Version 02/12 June 2013 06/13 06/13 Disclaimer and Notices 2013 American Medical Association This
National Uniform Claim Committee 1500 Health Insurance Claim Form Reference Instruction Manual for Form Version 02/12 June 2013 06/13 06/13 Disclaimer and Notices 2013 American Medical Association This
Dental Dispatch. Dental Provider Resources Available on our Website
 Dental Dispatch FALL 2014 I Vol.3 Dental Provider Resources Available on our Website Empire has important information available online that assists our providers in obtaining information regarding contract
Dental Dispatch FALL 2014 I Vol.3 Dental Provider Resources Available on our Website Empire has important information available online that assists our providers in obtaining information regarding contract
CMS-1500 Billing Guide for PROMISe Non-JCAHO Residential Treatment Facilities (RTFs)
") CS-1500 Billing Guide for PROISe Non-JCHO Residential Treatment Facilities () Purpose of the document Document format The purpose of this document is to provide a block-by-block reference guide to assist
CS-1500 Billing Guide for PROISe Non-JCHO Residential Treatment Facilities () Purpose of the document Document format The purpose of this document is to provide a block-by-block reference guide to assist
Chapter 6. Billing on the UB-04 Claim Form
 Chapter 6 This Page Intentionally Left Blank Chapter: 6 Page: 6-3 INTRODUCTION The UB-04 claim form is used to bill for all hospital inpatient, outpatient, and emergency room services. Dialysis clinic,
Chapter 6 This Page Intentionally Left Blank Chapter: 6 Page: 6-3 INTRODUCTION The UB-04 claim form is used to bill for all hospital inpatient, outpatient, and emergency room services. Dialysis clinic,
NEW YORK STATE MEDICAID PROGRAM DURABLE MEDICAL EQUIPMENT MEDICAL/SURGICAL SUPPLIES ORTHOPEDIC FOOTWEAR ORTHOTIC AND PROSTHETIC APPLIANCES
 NEW YORK STATE MEDICAID PROGRAM DURABLE MEDICAL EQUIPMENT MEDICAL/SURGICAL SUPPLIES ORTHOPEDIC FOOTWEAR ORTHOTIC AND PROSTHETIC APPLIANCES 150002 BILLING GUIDELINES TABLE OF CONTENTS Section I Purpose
NEW YORK STATE MEDICAID PROGRAM DURABLE MEDICAL EQUIPMENT MEDICAL/SURGICAL SUPPLIES ORTHOPEDIC FOOTWEAR ORTHOTIC AND PROSTHETIC APPLIANCES 150002 BILLING GUIDELINES TABLE OF CONTENTS Section I Purpose
1500 Claims Processing Manual DHMP Health Insurance Claim Form CMS-1500
 DENVER HEALTH MEDICAL PLAN, INC. 1500 Claims Processing Manual DHMP Health Insurance Claim Form CMS-1500 Box 1 Medicare, Medicaid, Group Health Plan or other insurance Information Show the type of health
DENVER HEALTH MEDICAL PLAN, INC. 1500 Claims Processing Manual DHMP Health Insurance Claim Form CMS-1500 Box 1 Medicare, Medicaid, Group Health Plan or other insurance Information Show the type of health
UB-04 Claim Form Instructions
 UB-04 Claim Form Instructions FORM LOCATOR NAME 1. Billing Provider Name & Address INSTRUCTIONS Enter the name and address of the hospital/facility submitting the claim. 2. Pay to Address Pay to address
UB-04 Claim Form Instructions FORM LOCATOR NAME 1. Billing Provider Name & Address INSTRUCTIONS Enter the name and address of the hospital/facility submitting the claim. 2. Pay to Address Pay to address
HCFA-1500 Form Completion. For the RLISYS NSF Electronic Claims Software. 2 Patient Name Patient s name as Last Name, First Name (Example: Doe, John)
") 1 HCFA-1500 Form Completion For the RLISYS NSF Electronic Claims Software 2 Patient Name Patient s name as Last Name, First Name (Example: Doe, John) Do not include a prefix, suffix, or middle initial
1 HCFA-1500 Form Completion For the RLISYS NSF Electronic Claims Software 2 Patient Name Patient s name as Last Name, First Name (Example: Doe, John) Do not include a prefix, suffix, or middle initial
Medical Claim Submissions
 Medical Claim Submissions New CMS 1500 Claim Form Requirements 10/28/2015 Hewlett Packard Enterprise 1 Learning objectives Understand the new requirements and deadlines Understand how to complete the new
Medical Claim Submissions New CMS 1500 Claim Form Requirements 10/28/2015 Hewlett Packard Enterprise 1 Learning objectives Understand the new requirements and deadlines Understand how to complete the new
Quick Reference for Denti-Cal Providers
 Quick Reference for Denti-Cal Providers (This is a summary of key information and requirements of the Denti-Cal program. It is not meant to replace the detailed information in the Denti-Cal Provider Handbook.)
Quick Reference for Denti-Cal Providers (This is a summary of key information and requirements of the Denti-Cal program. It is not meant to replace the detailed information in the Denti-Cal Provider Handbook.)
CMS-1500 Billing Guide for PROMISe Home Residential Rehabilitation Providers
 CMS-1500 Billing Guide for PRMISe Home Residential Rehabilitation Providers Purpose of the document Document format The purpose of this document is to provide a block-by-block reference guide to assist
CMS-1500 Billing Guide for PRMISe Home Residential Rehabilitation Providers Purpose of the document Document format The purpose of this document is to provide a block-by-block reference guide to assist
HEALTH INSURANCE CLAIM FORM APPROVED BY THE BERMUDA HEALTH COUNCIL 10/09
 HEALTH INSURANCE CLAIM FORM APPROVED BY THE BERMUDA HEALTH COUNCIL 10/09 1. NAME OF INSURANCE COMPANY PLEASE PRINT OR TYPE IN UPPERCASE LETTERS 1a. INSURED S CERTIFICATE NUMBER ARGUS BF&M COLONIAL FM GEHI
HEALTH INSURANCE CLAIM FORM APPROVED BY THE BERMUDA HEALTH COUNCIL 10/09 1. NAME OF INSURANCE COMPANY PLEASE PRINT OR TYPE IN UPPERCASE LETTERS 1a. INSURED S CERTIFICATE NUMBER ARGUS BF&M COLONIAL FM GEHI
MEDICAID DENTAL PROGRAMS CODING, POLICY AND RELATED FEE REVISION INFORMATION
 MEDICAID DENTAL PROGRAMS CODING, POLICY AND RELATED FEE REVISION INFORMATION Effective for dates of service on and after November 1, 2005, the following dental coding, policy and related fee revisions
MEDICAID DENTAL PROGRAMS CODING, POLICY AND RELATED FEE REVISION INFORMATION Effective for dates of service on and after November 1, 2005, the following dental coding, policy and related fee revisions
Molina Healthcare of Ohio, Inc. PO Box 22712 Long Beach, CA 90801
 Section 9. Claims As a contracted provider, it is important to understand how the claims process works to avoid delays in processing your claims. The following items are covered in this section for your
Section 9. Claims As a contracted provider, it is important to understand how the claims process works to avoid delays in processing your claims. The following items are covered in this section for your
Claim Form Billing Instructions CMS 1500 Claim Form
 Claim Form Billing Instructions CMS 1500 Claim Form Item Required Field? Description and Instructions. number 1 Optional Indicate the type of health insurance for which the claim is being submitted. 1a
Claim Form Billing Instructions CMS 1500 Claim Form Item Required Field? Description and Instructions. number 1 Optional Indicate the type of health insurance for which the claim is being submitted. 1a
UB-04, Inpatient / Outpatient
 UB-04, Inpatient / Outpatient Hospital (Inpatient and Outpatient), Hospice (Nursing Home and Home Services), Home Health, Rural Health linic, Federally Qualified Health enter, IF/MR, Birthing enter, and
UB-04, Inpatient / Outpatient Hospital (Inpatient and Outpatient), Hospice (Nursing Home and Home Services), Home Health, Rural Health linic, Federally Qualified Health enter, IF/MR, Birthing enter, and
Pennsylvania Department Of Human Services ESC Error Status Code Descriptions 201 BILLING PROVIDER IDENTIFICATION NUMBER IS MISSING FROM CLAIM 202
 Pennsylvania Department Of Human Services ESC Error Status Code Descriptions 201 BILLING PROVIDER IDENTIFICATION NUMBER IS MISSING FROM CLAIM 202 BILLING PROVIDER IDENTIFICATION NUMBER IS IN INVALID FORMAT
Pennsylvania Department Of Human Services ESC Error Status Code Descriptions 201 BILLING PROVIDER IDENTIFICATION NUMBER IS MISSING FROM CLAIM 202 BILLING PROVIDER IDENTIFICATION NUMBER IS IN INVALID FORMAT
CODE DESCRIPTION 011 Claim denial (claim level) due to SF message 012 Line denial (line level) due to SF message 017 Incorrect Alpha Prefix 030
 due to SF message 012 Line denial (line level) due to SF message 017 Incorrect Alpha Prefix 030") CODE DESCRIPTION 011 Claim denial (claim level) due to SF message 012 Line denial (line level) due to SF message 017 Incorrect Alpha Prefix 030 Missing service provider zip code (box 32) 031 Missing pickup
CODE DESCRIPTION 011 Claim denial (claim level) due to SF message 012 Line denial (line level) due to SF message 017 Incorrect Alpha Prefix 030 Missing service provider zip code (box 32) 031 Missing pickup
Kansas Medical Assistance Program
 Kansas Medical Assistance Program Vertical Perspective Kansas Medical Assistance Program 2009 Spring Supplemental Billing Packet: Local Education Agency Professional Claims Introduction The Kansas Medical
Kansas Medical Assistance Program Vertical Perspective Kansas Medical Assistance Program 2009 Spring Supplemental Billing Packet: Local Education Agency Professional Claims Introduction The Kansas Medical
DENTAL PROVIDER MANUAL
 DENTAL PROVIDER MANUAL Connecticut Dental Health Partnership (The dental plan for Husky Health) The Connecticut Department of Social Services BeneCare Dental Plans ii Welcome to the Connecticut Dental
DENTAL PROVIDER MANUAL Connecticut Dental Health Partnership (The dental plan for Husky Health) The Connecticut Department of Social Services BeneCare Dental Plans ii Welcome to the Connecticut Dental
National Uniform Claim Committee
 National Uniform Claim Committee 1500 Health Insurance Claim Form Reference Instruction Manual for 08/05 Version Disclaimer and Notices 2005 American Medical Association This document is published in cooperation
National Uniform Claim Committee 1500 Health Insurance Claim Form Reference Instruction Manual for 08/05 Version Disclaimer and Notices 2005 American Medical Association This document is published in cooperation
Domestic Accident & Health Division 80 Pine Street, 13 th Floor New York, NY 10005
 Domestic Accident & Health Division 80 Pine Street, 13 th Floor New York, NY 10005 Welcome to the AIG Companies family of customers. We appreciate that you had a choice when placing your insurance and
Domestic Accident & Health Division 80 Pine Street, 13 th Floor New York, NY 10005 Welcome to the AIG Companies family of customers. We appreciate that you had a choice when placing your insurance and
CMS1500 Billing Tips
 CMS1500 Billing Tips INSTRUCTION ADVICE FOR COMPLETING THE CMS1500 FORM FOR OREGON WORKERS COMPENSATION CLAIMS Page 1 of 30 Field 1: Page 2 of 30 Field 1: 1: Always mark the OTHER box. This informs the
CMS1500 Billing Tips INSTRUCTION ADVICE FOR COMPLETING THE CMS1500 FORM FOR OREGON WORKERS COMPENSATION CLAIMS Page 1 of 30 Field 1: Page 2 of 30 Field 1: 1: Always mark the OTHER box. This informs the
Reimbursement and Claims Submission Changes for Nursing Home Provided Non-emergency Transportation for Nursing Home Residents
 Update February 2010 No. 2010-05 Affected Programs: BadgerCare Plus Standard Plan, BadgerCare Plus Benchmark Plan, Medicaid To: Nursing Homes, HMOs and Other Managed Care Programs Reimbursement and Claims
Update February 2010 No. 2010-05 Affected Programs: BadgerCare Plus Standard Plan, BadgerCare Plus Benchmark Plan, Medicaid To: Nursing Homes, HMOs and Other Managed Care Programs Reimbursement and Claims
NEW YORK STATE MEDICAID PROGRAM CLINICAL SOCIAL WORKER 150002 BILLING GUIDELINES
 NEW YORK STATE MEDICAID PROGRAM CLINICAL SOCIAL WORKER 150002 BILLING GUIDELINES TABLE OF CONTENTS Section I Purpose Statement... 3 Section II Claims Submission... 4 Electronic Claims... 5 Paper Claims...
NEW YORK STATE MEDICAID PROGRAM CLINICAL SOCIAL WORKER 150002 BILLING GUIDELINES TABLE OF CONTENTS Section I Purpose Statement... 3 Section II Claims Submission... 4 Electronic Claims... 5 Paper Claims...
Generali Worldwide Health Insurance Dental Claim Form
 Generali Worldwide Health Insurance Dental Claim Form Please complete all sections in BLOCK CAPITALS or tick the boxes, where appropriate. INSTRUCTIONS FOR FILING A DENTAL CLAIM 1. Please type or print
Generali Worldwide Health Insurance Dental Claim Form Please complete all sections in BLOCK CAPITALS or tick the boxes, where appropriate. INSTRUCTIONS FOR FILING A DENTAL CLAIM 1. Please type or print
Instructions for Completing the CMS 1500 Claim Form
 Instructions for Completing the CMS 1500 Claim Form The Center of Medicaid and Medicare Services (CMS) form 1500 must be used to bill SFHP for medical services. The form is used by Physicians and Allied
Instructions for Completing the CMS 1500 Claim Form The Center of Medicaid and Medicare Services (CMS) form 1500 must be used to bill SFHP for medical services. The form is used by Physicians and Allied
Dental Claim Form HEALTH INSURANCE. 1 of 5 PLEASE COMPLETE THIS FORM USING BLOCK CAPITALS
 Dental Claim Form HEALTH INSURANCE PLEASE COMPLETE THIS FORM USING BLOCK CAPITALS INSTRUCTIONS FOR FILING A DENTAL CLAIM 1. Please type or print and include all requested information 2. A separate claim
Dental Claim Form HEALTH INSURANCE PLEASE COMPLETE THIS FORM USING BLOCK CAPITALS INSTRUCTIONS FOR FILING A DENTAL CLAIM 1. Please type or print and include all requested information 2. A separate claim
DENTAL SERVICES PROVIDER MANUAL Chapter Sixteen of the Medicaid Services Manual
 DENTAL SERVICES PROVIDER MANUAL Chapter Sixteen of the Medicaid Services Manual Issued March 15, 2012 State of Louisiana Bureau of Health Services Financing SECTION: TABLE OF CONTENTS PAGE(S) 4 CHAPTER
DENTAL SERVICES PROVIDER MANUAL Chapter Sixteen of the Medicaid Services Manual Issued March 15, 2012 State of Louisiana Bureau of Health Services Financing SECTION: TABLE OF CONTENTS PAGE(S) 4 CHAPTER
Completing a CMS 1500 Form
 Completing a CMS 1500 Form 1 So you want to submit clean paper claims! Most offices submit electronic claims, but there are still small offices that submit paper claims and other times when a paper claim
Completing a CMS 1500 Form 1 So you want to submit clean paper claims! Most offices submit electronic claims, but there are still small offices that submit paper claims and other times when a paper claim
CLAIMS Section 5. Overview. Clean Claim. Prompt Payment. Timely Claims Submission. Claim Submission Format
 Overview The Claims department partners with the Provider Relations, Health Services and Customer Service departments to assist providers with any claims-related questions. The focus of the Claims department
Overview The Claims department partners with the Provider Relations, Health Services and Customer Service departments to assist providers with any claims-related questions. The focus of the Claims department
TexMedConnect Acute Care Manual
 TexMedConnect Acute Care Manual v2015_0811 Contents 1.0 Overview.......................................... 1 2.0 TexMedConnect Internet Requirements.......................... 2 3.0 Getting Support......................................
TexMedConnect Acute Care Manual v2015_0811 Contents 1.0 Overview.......................................... 1 2.0 TexMedConnect Internet Requirements.......................... 2 3.0 Getting Support......................................
Ambulatory Surgery Center (ASC) Billing Instructions
 Billing Instructions") All related services performed by an ambulatory surgery center must be billed on the UB04 claim form following the instructions listed below. Tips Claim Form Completion Claims for ASC covered services
All related services performed by an ambulatory surgery center must be billed on the UB04 claim form following the instructions listed below. Tips Claim Form Completion Claims for ASC covered services
DENTAL SERVICES PROVIDER MANUAL Chapter Sixteen of the Medicaid Services Manual
 DENTAL SERVICES PROVIDER MANUAL Chapter Sixteen of the Medicaid Services Manual Issued March 15, 2012 Claims/authorizations for dates of service on or after October 1, 2015 must use the applicable ICD-10
DENTAL SERVICES PROVIDER MANUAL Chapter Sixteen of the Medicaid Services Manual Issued March 15, 2012 Claims/authorizations for dates of service on or after October 1, 2015 must use the applicable ICD-10
The Utilization Threshold Program
 The Utilization Threshold Program In order to contain costs while continuing to provide medically necessary care and services, the Utilization Threshold (UT) program places limits on the number of services
The Utilization Threshold Program In order to contain costs while continuing to provide medically necessary care and services, the Utilization Threshold (UT) program places limits on the number of services
Institutional Billing Guide
 Program KANSAS MEDICAL ASSISTANCE PROGRAM Institutional Billing Guide Updated 10.2013 Institutional Billing The Kansas Medical Assistance Program (KMAP) offers different billing options to all providers.
Program KANSAS MEDICAL ASSISTANCE PROGRAM Institutional Billing Guide Updated 10.2013 Institutional Billing The Kansas Medical Assistance Program (KMAP) offers different billing options to all providers.
Colorado Medical Assistance Program Web Portal Dental Claims User Guide
 Colorado Medical Assistance Program Web Portal Dental Claims User Guide The Dental Claim Lookup screen (Figure 1) is the main screen from which to manage Dental claims. It consists of different sections
Colorado Medical Assistance Program Web Portal Dental Claims User Guide The Dental Claim Lookup screen (Figure 1) is the main screen from which to manage Dental claims. It consists of different sections
UB-04 Billing Instructions
 UB-04 Billing Instructions 11/1/2012 The UB-04 is a claim form that is utilized for Hospital Services and select residential services. Please note that these instructions are specifically written to correlate
UB-04 Billing Instructions 11/1/2012 The UB-04 is a claim form that is utilized for Hospital Services and select residential services. Please note that these instructions are specifically written to correlate
CSHCN Services Program Prior Authorization Request for Inpatient Rehabilitation Admission Form and Instructions
 CSHCN Services Program Prior Authorization Request for Inpatient Rehabilitation Admission Form and Instructions General Information Ensure the most recent version of the Prior Authorization Request for
CSHCN Services Program Prior Authorization Request for Inpatient Rehabilitation Admission Form and Instructions General Information Ensure the most recent version of the Prior Authorization Request for
Dental Outline of Coverage
 Dental Outline of Coverage Blue Cross and Blue Shield of Texas (herein called (BCBSTX, We, Us, Our) Dental Indemnity Insurance Contract REQUIRED OUTLINE OF COVERAGE A. Read Your Contract Carefully. This
Dental Outline of Coverage Blue Cross and Blue Shield of Texas (herein called (BCBSTX, We, Us, Our) Dental Indemnity Insurance Contract REQUIRED OUTLINE OF COVERAGE A. Read Your Contract Carefully. This
OSCAR Health Insurance Frequently Asked Questions/General Information
 Q: What is the relationship between Oscar and ValueOptions? A. ValueOptions administers the mental health and substance abuse benefits for Oscar Health Insurance. They have contracted with ValueOptions,
Q: What is the relationship between Oscar and ValueOptions? A. ValueOptions administers the mental health and substance abuse benefits for Oscar Health Insurance. They have contracted with ValueOptions,
CMS 1500 (08/05) Claim Filing Instructions
 Claim Filing Instructions") CMS 1500 (08/05) Claim Filing Instructions Field 1. Leave blank 1a. Insured s ID - Enter the Member identification number exactly as it appears on the patient s ID card. The member s ID number is the subscriber
CMS 1500 (08/05) Claim Filing Instructions Field 1. Leave blank 1a. Insured s ID - Enter the Member identification number exactly as it appears on the patient s ID card. The member s ID number is the subscriber
Medical and Dental Plan Application for Individuals and Families
 Medical and Dental Plan Application for Individuals and Families Please be sure to complete ALL information below to avoid delays in processing. Please print clearly using blue or black ink. Section 1
Medical and Dental Plan Application for Individuals and Families Please be sure to complete ALL information below to avoid delays in processing. Please print clearly using blue or black ink. Section 1
Claim Status Response Explanation of Benefits List
 20 Accepted for processing 066 CLAIM CURRENTLY IN PROCESS. DO NOT RESUBMIT 21 Missing or invalid information 018 REFERRING PHYSICIAN INFORMATION REQUIRED AND NOT PRESENT Referring 21 Missing or invalid
20 Accepted for processing 066 CLAIM CURRENTLY IN PROCESS. DO NOT RESUBMIT 21 Missing or invalid information 018 REFERRING PHYSICIAN INFORMATION REQUIRED AND NOT PRESENT Referring 21 Missing or invalid
Completing a Paper UB-04 Form
 Completing a Paper UB-04 Information in this policy does not apply to members with the Choice or Choice Plus products offered through Passport Connect S. For UnitedHealthcare s related policies/procedures,
Completing a Paper UB-04 Information in this policy does not apply to members with the Choice or Choice Plus products offered through Passport Connect S. For UnitedHealthcare s related policies/procedures,
How To Bill For A Medicaid Claim
 UB-04 CLAIM FORM INSTRUCTIONS FIELD NUMBER FIELD NAME 1 Billing Provider Name & Address INSTRUCTIONS Enter the name and address of the hospital/facility submitting the claim. 2 Pay to Address Pay to address
UB-04 CLAIM FORM INSTRUCTIONS FIELD NUMBER FIELD NAME 1 Billing Provider Name & Address INSTRUCTIONS Enter the name and address of the hospital/facility submitting the claim. 2 Pay to Address Pay to address
ebilling Support ebilling Support webinar: ebilling terms Lifecycle of a claim
 ebilling Support ebilling Support webinar: ebilling terms ebilling enrollment Lifecycle of a claim 2 Terms EDI Electronic Data Interchange Flow of electronic information, specifically claims information
ebilling Support ebilling Support webinar: ebilling terms ebilling enrollment Lifecycle of a claim 2 Terms EDI Electronic Data Interchange Flow of electronic information, specifically claims information
Presented by January 6, 2006. The National Provider Identifier (NPI): What Dentists Need to Know
: What Dentists Need to Know") Presented by January 6, 2006 The National Provider Identifier (NPI): What Dentists Need to Know The National Provider Identifier (NPI): What Dentists Need to Know The information provided in this presentation
Presented by January 6, 2006 The National Provider Identifier (NPI): What Dentists Need to Know The National Provider Identifier (NPI): What Dentists Need to Know The information provided in this presentation