Ambulatory Surgery Center (ASC) Billing Instructions
|
|
|
- Tyler Price
- 9 years ago
- Views:
Transcription
1 All related services performed by an ambulatory surgery center must be billed on the UB04 claim form following the instructions listed below. Tips Claim Form Completion Claims for ASC covered services must use type of bill (TOB) Must have the same from and through dates indicated in form locator (FL) 6 Revenue codes 0490 or 0360 should be used for procedures that have been assigned to ASC payment groups. The CPT 4 code that best describes the procedure is required and must be entered in FL 44. When billing for chemotherapy related services, must include the national drug code (NDC) Reimbursement A maximum of five (5) surgeries may be performed per day per claim The reimbursement for multiple surgeries performed is as follows: o First surgery performed will be reimbursed at 100% of the allowed amount o Second surgery performed will be reimbursed at 50% of the allowed amount o Three to five surgeries performed per day will be reimbursed at 25% of the allowed amount Page 1 of 8

2 Claim Form Instructions Page 2 of 8
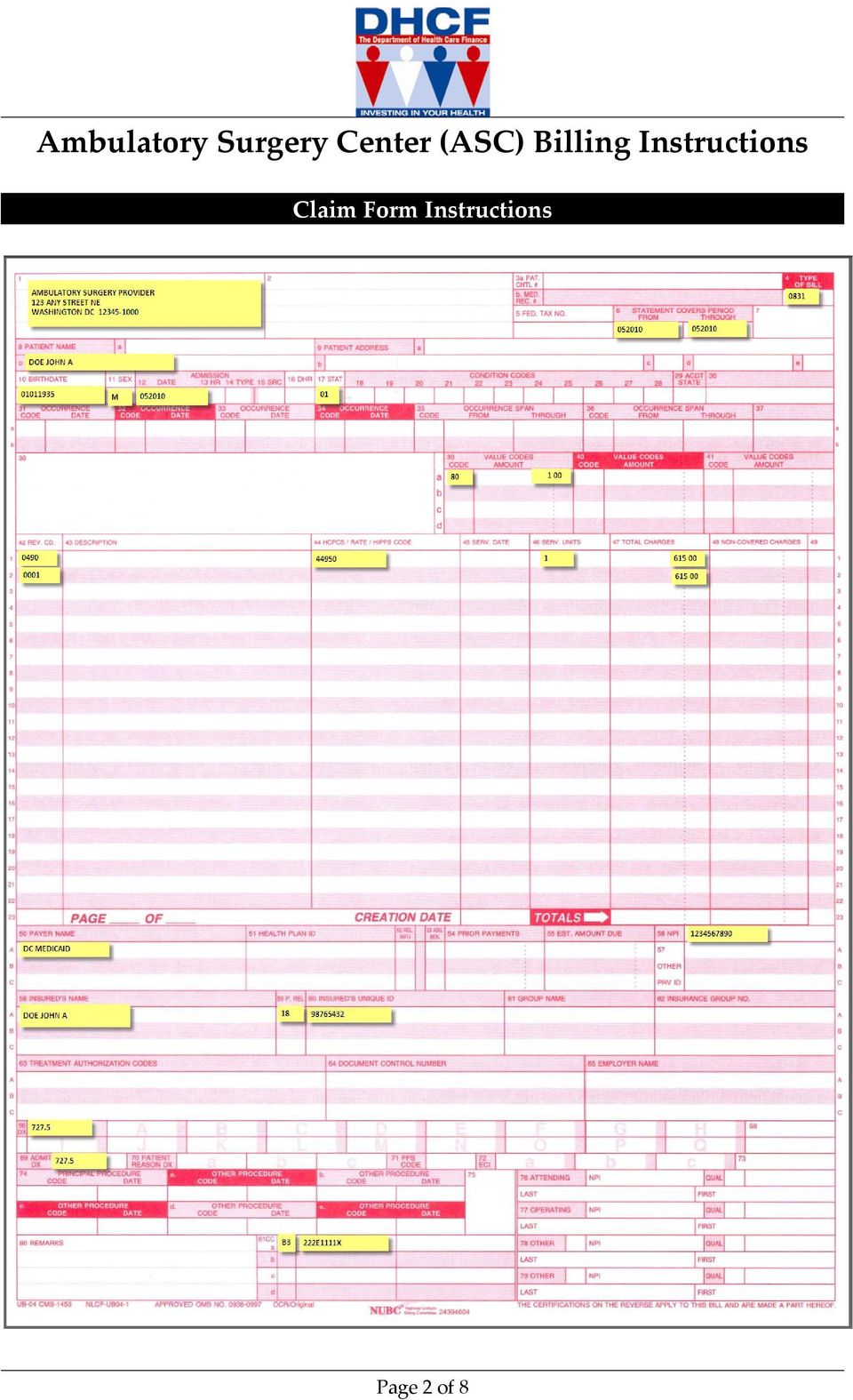
3 1 Required 4 Required Type of Bill Provider Name, Address, and Telephone Number 6 Required Statement Covers Period 8b Required Patient Name/Identifier Billing Provider Name, Address and Telephone Number: Enter the agency name, street, city, state, zip code, and telephone number. Line 1 Provider Name Line 2 Provider Street Address Line 3 Provider City, State, Zip +4 Line 4 Provider Telephone Enter the three digit type of bill code. This field has been expanded from three to four characters with zero being the first digit. Claims will be processed based on the last three digits (Special Facility Ambulatory Surgery Center) Enter the beginning and ending dates of service billed in MMDDYY format. Enter the patient s name as it appears on the Medical Assistance Card in last name, first name, middle initial format. 10 Required Patient Birth date Enter patient s date of birth in MMDDYYYY format 11 Required Patient Sex Indicate the patient s gender M: Male F: Female U: Unknown 12 Required Admission Date Enter the date the patient was admitted for care in MMDDYY format. 17 Required Patient Status Enter the code that identifies the patient s status as of the statement covers through date. 01: Discharge to home or self care (routine discharge) 02: Discharged/transferred to another short term general hospital for inpatient care 03: Discharged/transferred to skilled nursing facility 04: Discharged/transferred to an intermediate care facility 05: Discharged/transferred to another type of institution for inpatient care or referred for outpatient services to another institution 06: Discharged/transferred to home under care of organized home health service organization 07: Left against medical advice or discontinued care 08: Discharged/transferred to home under care of a Home IV provider 09: Admitted as an inpatient to this hospital Page 3 of 8

4 39 41 Required Value Codes 20: Expired 30: Still a patient 40: Expired at home (Medicare hospice claim only) 41: Expired in a medical facility (e.g., hospital, SNF, ICF, or freestanding hospice)(medicare hospice claims only) 43: Discharged/transferred to federal healthcare facility 50: Discharged to Hospice Home 51: Discharged to Hospice Medical Facility (certified) providing hospice level of care 61: Discharged/transferred within the institution to a hospital based, Medicare approved swing bed 62: Discharged/transferred to inpatient rehabilitation facility, including rehabilitation distinct part units of a hospital 63: Discharged/transferred to a Medicare certified longterm care hospital 64: Discharged/transferred to a nursing facility certified under Medicaid, but not under Medicare 65: Discharged/transferred to a psychiatric hospital or psychiatric distinct part unit of a hospital 66: Discharged/transferred to a critical access hospital 70: Discharged/transferred to another type of health care institution not defined in code list Enter the appropriate value code and amount. 80: Covered days 81: Non covered days 82: Co insurance days (required only for Medicare crossover claims) 83: Lifetime reserve days (required only for Medicare crossover claims) 42 Required Rev. Code Enter the appropriate Value Code in the code portion of the field and the Number of Days in the Dollar portion of the Amount section of the field. Enter 00 in the Cents portion of the Amount section of the field Enter the revenue code that identifies the specific accommodation, ancillary service or billing calculation Operating Room Services General Classification 0490 Ambulatory Surgical Care General Classification On the last line, enter 0001 for the total. Page 4 of 8

5 43 Required if applicable 44 Required Description HCPCS/Rates/HIPPS Code 46 Required Serv. Units 47 Required Total Charges 50 Required Payer Name 56 Required Billing Provider NPI 58A C Required Insured s Name 59A C Required P. Rel 60A C Required Insured s Unique ID Enter the 11 digit National Drug Code (NDC) if billing for chemotherapy drugs Enter the appropriate CPT or HCPCS code relevant to the accommodation revenue code entered for the services being billed (see field 42 for more info). Enter the total number of covered accommodation days or ancillary units of service for each revenue code billed as appropriate Enter the total charges for each related revenue/procedure code. Enter the grand total charges at the bottom of this field to be associated with revenue code As applicable, enter the name of the beneficiary s primary, secondary, and tertiary insurance on lines A, B, and C. For claims with no TPL, DC Medicaid is entered on line A. Enter the National Provider Identifier for the billing provider As applicable, enter the insured s name for the primary, secondary and tertiary insurance on lines A, B, and C according to proper billing order. On the line that shows payer, Medicaid, enter the beneficiary s name exactly as it appears on the Medical Assistance card. Enter the appropriate code indicating the relationship of the patient to the identified insured. 01: Spouse 18: Self 19: Child 20: Employee 21: Unknown 39: Organ Donor 40: Cadaver Donor 53: Life Partner G8: Other Relative Enter the insured s ID for the plans listed in 50 A, B, and C that relates to the insured s name in 58 A, B, and C. Enter the patient s Medicaid ID as it appears on their Medical Assistance Card omitting the leading zeroes in Page 5 of 8
.")
6 the filed that corresponds with DC Medicaid 67 Required Principal Diagnosis Code 69 Required Admit DX code 77 Required if applicable Operating provider Enter the principal diagnosis code(s) provided at the time of admission as stated by the physician Enter the diagnosis code provided at the time of admission as stated by the physician Enter the NPI of the provider performing surgery, as well as the last name/first name. If the operating provider is atypical, leave this field blank. Instead enter the Medicaid provider number to the right hand side of the qualifier box. Enter G2 in the qualifier box. Enter the NPI of the other provider (e.g., referring, ordering, assisting provider, etc.), as well as the last name/first name Required if applicable Required if applicable Other (A or B) provider Remarks If Referring enter DN as qualifier code for Other in field 79, then the Referring Providerʹs NPI and Last, First name If the other provider (e.g., referring, ordering, assisting provider, etc.) is atypical, leave this field blank. Instead enter the Medicaid provider number to the right hand side of the qualifier box. Enter G2 in the qualifier box. If submitting an adjustment or void of a previously paid claim, enter the 17 digit transaction control number of the paid claim to be adjusted or voided along with the appropriate adjustment/void reason code in this field. 101: Void Payment To PIP Hospital 102: Accommodation Charge Correct 103: Patient Payment Amt Changed 104: Procedure Service Dates Fix 105: Correcting Diagnosis Code 106: Correcting Charges 107: Unit Visit Studies Prcd Fix 108: Reconsideration Of Allowance 109: Fix Admit Refer Presc Provider 110: Correcting Tooth Code 111: Correcting Site Code 112: Correct Transportation Data 113: Inpatient Drg 114: Adjusting Patient Level Care 115: Recovery Based On Pro Review Page 6 of 8
, as well as the last name/first name.")
7 116: Adjusted For Recp Bedhold Days 117: Manual Capitation Void Claims 118: Reprocessed Claims 119: Auto Recoupment System Error 120: Auto Recoupment System Chang 121: PCG Services 300: Recipient Deceased New 086: Claim Void Medicare Recovery 089: Refund Fiscal Agent Error 090: Prov Rtrn Chk/Pd For Inc Bene 011: Retro Rate Chg / No Cutback 099: Prov Return Chk/ Incorr Prov 099: Prov Return Chk/ Incorr Prov 011: Retro Rate Chg / No Cutback 086: Claim Void Medicare Recovery 019: POS Prov File Corr/Legal Sett 082: Clm Void/Fisc Agent Proc Error 083: Clm Vd/Pd In Error/Rcp Incorre 084: Clm Vd/Pd Error/Prov Fil Incor 085: Clm Vd/Pd Error/Incorrect Prov 068: Provider Refund/Clm Overpaymnt 069: Prov Rfnd/Overpay Fisc Error 070: Prov Refund For Health Insur 071: Prov Refund For Casualty Ins Page 7 of 8

8 81A D Required CC 088: Refund Provider Error 089: Refund Fiscal Agent Error 088: Refund Provider Error 089: Refund Fiscal Agent Error 088: Refund Provider Error 089: Refund Fiscal Agent Error Enter the taxonomy code of the billing/pay to provider preceded by the B3 qualifier. Page 8 of 8

UB-04 Claim Form Instructions
 UB-04 Claim Form Instructions FORM LOCATOR NAME 1. Billing Provider Name & Address INSTRUCTIONS Enter the name and address of the hospital/facility submitting the claim. 2. Pay to Address Pay to address
UB-04 Claim Form Instructions FORM LOCATOR NAME 1. Billing Provider Name & Address INSTRUCTIONS Enter the name and address of the hospital/facility submitting the claim. 2. Pay to Address Pay to address
Billing Manual for In-State Long Term Care Nursing Facilities
 Billing Manual for In-State Long Term Care Nursing Facilities Medical Services North Dakota Department of Human Services 600 E Boulevard Ave, Dept 325 Bismarck, ND 58505 September 2003 INTRODUCTION The
Billing Manual for In-State Long Term Care Nursing Facilities Medical Services North Dakota Department of Human Services 600 E Boulevard Ave, Dept 325 Bismarck, ND 58505 September 2003 INTRODUCTION The
Chapter 6. Billing on the UB-04 Claim Form
 Chapter 6 This Page Intentionally Left Blank Chapter: 6 Page: 6-3 INTRODUCTION The UB-04 claim form is used to bill for all hospital inpatient, outpatient, and emergency room services. Dialysis clinic,
Chapter 6 This Page Intentionally Left Blank Chapter: 6 Page: 6-3 INTRODUCTION The UB-04 claim form is used to bill for all hospital inpatient, outpatient, and emergency room services. Dialysis clinic,
UB04 INSTRUCTIONS Home Health
 UB04 INSTRUCTIONS Home Health 1 Provider Name, Address, Telephone 2 Pay to Name/Address/ID Required. Enter the name and address of the facility Situational. Enter the name, address, and Louisiana Medicaid
UB04 INSTRUCTIONS Home Health 1 Provider Name, Address, Telephone 2 Pay to Name/Address/ID Required. Enter the name and address of the facility Situational. Enter the name, address, and Louisiana Medicaid
UB-04 Billing Instructions
 UB-04 Billing Instructions 11/1/2012 The UB-04 is a claim form that is utilized for Hospital Services and select residential services. Please note that these instructions are specifically written to correlate
UB-04 Billing Instructions 11/1/2012 The UB-04 is a claim form that is utilized for Hospital Services and select residential services. Please note that these instructions are specifically written to correlate
UB-04, Inpatient / Outpatient
 UB-04, Inpatient / Outpatient Hospital (Inpatient and Outpatient), Hospice (Nursing Home and Home Services), Home Health, Rural Health linic, Federally Qualified Health enter, IF/MR, Birthing enter, and
UB-04, Inpatient / Outpatient Hospital (Inpatient and Outpatient), Hospice (Nursing Home and Home Services), Home Health, Rural Health linic, Federally Qualified Health enter, IF/MR, Birthing enter, and
Instructions for Completing the UB-04 Claim Form
 Instructions for Completing the UB-04 Claim Form The UB04 claim form is used to submit claims for inpatient and outpatient services by institutional facilities (for example, outpatient departments, Rural
Instructions for Completing the UB-04 Claim Form The UB04 claim form is used to submit claims for inpatient and outpatient services by institutional facilities (for example, outpatient departments, Rural
ebilling Support ebilling Support webinar: ebilling terms Lifecycle of a claim
 ebilling Support ebilling Support webinar: ebilling terms ebilling enrollment Lifecycle of a claim 2 Terms EDI Electronic Data Interchange Flow of electronic information, specifically claims information
ebilling Support ebilling Support webinar: ebilling terms ebilling enrollment Lifecycle of a claim 2 Terms EDI Electronic Data Interchange Flow of electronic information, specifically claims information
Provider Billing Manual. Description
 UB-92 Billing Instructions Revision Table Revision Date Sections Revised 7/1/02 Section 2.3 Form Locator 42 and 46 Description Language is being added to clarify UB-92 billing instructions for form locator
UB-92 Billing Instructions Revision Table Revision Date Sections Revised 7/1/02 Section 2.3 Form Locator 42 and 46 Description Language is being added to clarify UB-92 billing instructions for form locator
How To Bill For A Medicaid Claim
 UB-04 CLAIM FORM INSTRUCTIONS FIELD NUMBER FIELD NAME 1 Billing Provider Name & Address INSTRUCTIONS Enter the name and address of the hospital/facility submitting the claim. 2 Pay to Address Pay to address
UB-04 CLAIM FORM INSTRUCTIONS FIELD NUMBER FIELD NAME 1 Billing Provider Name & Address INSTRUCTIONS Enter the name and address of the hospital/facility submitting the claim. 2 Pay to Address Pay to address
STATE OF MARYLAND KIDNEY DISEASE PROGRAM UB-04. Billing Instructions. for. Freestanding Dialysis Facility Services. Revised 9/1/08.
 STATE OF MARYLAND KIDNEY DISEASE PROGRAM UB-04 Billing Instructions for Freestanding Dialysis Facility Services Revised 9/1/08 Page 1 of 13 UB04 Instructions TABLE of CONTENTS Introduction 4 Sample UB04
STATE OF MARYLAND KIDNEY DISEASE PROGRAM UB-04 Billing Instructions for Freestanding Dialysis Facility Services Revised 9/1/08 Page 1 of 13 UB04 Instructions TABLE of CONTENTS Introduction 4 Sample UB04
CLAIMS AND BILLING INSTRUCTIONAL MANUAL
 CLAIMS AND BILLING INSTRUCTIONAL MANUAL 2007 TABLE OF ONTENTS Paper Claims and Block Grant Submission Requirements... 3 State Requirements for Claims Turnaround Time... 12 Claims Appeal Process... 13 Third
CLAIMS AND BILLING INSTRUCTIONAL MANUAL 2007 TABLE OF ONTENTS Paper Claims and Block Grant Submission Requirements... 3 State Requirements for Claims Turnaround Time... 12 Claims Appeal Process... 13 Third
1. Coverage Indicator Enter an "X" in the appropriate box.
 CMS 1500 Claim Form FIELD NAME INSTRUCTIONS 1. Coverage Indicator Enter an "X" in the appropriate box. 1a. Insured's ID Number Enter the patient's nine-digit Medical Assistance identification number (SSN).
CMS 1500 Claim Form FIELD NAME INSTRUCTIONS 1. Coverage Indicator Enter an "X" in the appropriate box. 1a. Insured's ID Number Enter the patient's nine-digit Medical Assistance identification number (SSN).
SOUTH CAROLINA MEDICAID WEB-BASED CLAIMS SUBMISSION TOOL
 SOUTH CAROLINA MEDICAID WEB-BASED CLAIMS SUBMISSION TOOL User Guide Addendum CMS-500 October 28, 2003 Updated June 03, 203 CMS-500 CLAIMS ENTRY This document describes the correspondence between the South
SOUTH CAROLINA MEDICAID WEB-BASED CLAIMS SUBMISSION TOOL User Guide Addendum CMS-500 October 28, 2003 Updated June 03, 203 CMS-500 CLAIMS ENTRY This document describes the correspondence between the South
Completing a Paper UB-04 Form
 Completing a Paper UB-04 Information in this policy does not apply to members with the Choice or Choice Plus products offered through Passport Connect S. For UnitedHealthcare s related policies/procedures,
Completing a Paper UB-04 Information in this policy does not apply to members with the Choice or Choice Plus products offered through Passport Connect S. For UnitedHealthcare s related policies/procedures,
CMS 1500 (02/12) CLAIM FORM INSTRUCTIONS
 CLAIM FORM INSTRUCTIONS") CMS 1500 (02/12) CLAIM FORM INSTRUCTIONS FIELD NUMBER FIELD NAME 1 a INSURED S ID NUMBER INSTRUCTIONS Enter the patient s nine digit Medicaid identification number (SSN) 2 PATIENT S NAME Enter the recipient
CMS 1500 (02/12) CLAIM FORM INSTRUCTIONS FIELD NUMBER FIELD NAME 1 a INSURED S ID NUMBER INSTRUCTIONS Enter the patient s nine digit Medicaid identification number (SSN) 2 PATIENT S NAME Enter the recipient
To submit electronic claims, use the HIPAA 837 Institutional transaction
 3.1 Claim Billing 3.1.1 Which Claim Form to Use Claims that do not require attachments may be billed electronically using Provider Electronic Solutions (PES) software (provided by Electronic Data Systems
3.1 Claim Billing 3.1.1 Which Claim Form to Use Claims that do not require attachments may be billed electronically using Provider Electronic Solutions (PES) software (provided by Electronic Data Systems
Chapter 8 Billing on the CMS 1500 Claim Form
 8 Billing on the CMS 1500 Claim form INTRODUCTION The CMS 1500 claim form is used to bill for non-facility services, including professional services, freestanding surgery centers, transportation, durable
8 Billing on the CMS 1500 Claim form INTRODUCTION The CMS 1500 claim form is used to bill for non-facility services, including professional services, freestanding surgery centers, transportation, durable
Chapter 5. Billing on the CMS 1500 Claim Form
 Chapter 5 Billing on the CMS 1500 Claim Form This Page Intentionally Left Blank Fee-For-Service Provider Manual April 2012 Billing on the UB-04 Claim Form Chapter: 5 Page: 5-2 INTRODUCTION The CMS 1500
Chapter 5 Billing on the CMS 1500 Claim Form This Page Intentionally Left Blank Fee-For-Service Provider Manual April 2012 Billing on the UB-04 Claim Form Chapter: 5 Page: 5-2 INTRODUCTION The CMS 1500
PENNSYLVANIA UNIFORM CLAIMS AND BILLING FORM REPORTING MANUAL
 PENNSYLVANIA UNIFORM CLAIMS AND BILLING FORM REPORTING MANUAL Inpatient UB-04 Data Reporting April 2007 Revised: August 2015 ay Status Report for Table of Contents Overview... 1 Detail Record Quick Reference
PENNSYLVANIA UNIFORM CLAIMS AND BILLING FORM REPORTING MANUAL Inpatient UB-04 Data Reporting April 2007 Revised: August 2015 ay Status Report for Table of Contents Overview... 1 Detail Record Quick Reference
Illustration 1-1. Revised CMS-1500 Claim Form (front)
") Florida Medicaid Provider Reimbursement Handbook, CMS-1500 Illustration 1-1. Revised CMS-1500 Claim Form (front) Incorporated by reference in 59G-4.001, F.A.C. July 2008 1-11 Florida Medicaid Provider
Florida Medicaid Provider Reimbursement Handbook, CMS-1500 Illustration 1-1. Revised CMS-1500 Claim Form (front) Incorporated by reference in 59G-4.001, F.A.C. July 2008 1-11 Florida Medicaid Provider
Kentucky Inpatient and Outpatient Data Coordinator s Manual For Hospitals
 Kentucky Inpatient and Outpatient Coordinator s Manual For Hospitals Revised December 1, 2014 Collection Help Desk 1-888-992-4320 www.kyipop.org Contents KY IPOP Coordinator s Manual for Hospitals Highlight
Kentucky Inpatient and Outpatient Coordinator s Manual For Hospitals Revised December 1, 2014 Collection Help Desk 1-888-992-4320 www.kyipop.org Contents KY IPOP Coordinator s Manual for Hospitals Highlight
Instructions for Completing the CMS 1500 Claim Form
 Instructions for Completing the CMS 1500 Claim Form The Center of Medicaid and Medicare Services (CMS) form 1500 must be used to bill SFHP for medical services. The form is used by Physicians and Allied
Instructions for Completing the CMS 1500 Claim Form The Center of Medicaid and Medicare Services (CMS) form 1500 must be used to bill SFHP for medical services. The form is used by Physicians and Allied
Inpatient and Outpatient Services Billing. Presented by EDS Provider Field Consultants
 Inpatient and Outpatient Services Billing Presented by EDS Provider Field Consultants October 2007 Agenda Objectives NPI New Paper Claim Form Who bills on a UB-04 Claim Form? Inpatient Claims Reimbursement
Inpatient and Outpatient Services Billing Presented by EDS Provider Field Consultants October 2007 Agenda Objectives NPI New Paper Claim Form Who bills on a UB-04 Claim Form? Inpatient Claims Reimbursement
Kentucky Inpatient and Outpatient Data Coordinator s Manual For Hospitals
 Kentucky Inpatient and Outpatient Coordinator s Manual For Hospitals Revised January 1, 2014 Collection Help Desk 1 888 992 4320 www.kyipop.org Contents KY IPOP Coordinator s Manual for Hospitals Highlight
Kentucky Inpatient and Outpatient Coordinator s Manual For Hospitals Revised January 1, 2014 Collection Help Desk 1 888 992 4320 www.kyipop.org Contents KY IPOP Coordinator s Manual for Hospitals Highlight
Claim Form Billing Instructions CMS 1500 Claim Form
 Claim Form Billing Instructions CMS 1500 Claim Form Item Required Field? Description and Instructions. number 1 Optional Indicate the type of health insurance for which the claim is being submitted. 1a
Claim Form Billing Instructions CMS 1500 Claim Form Item Required Field? Description and Instructions. number 1 Optional Indicate the type of health insurance for which the claim is being submitted. 1a
NURSING FACILITY SERVICES
 MARYLAND MEDICAID NURSING FACILITY SERVICES UB-04 BILLING INSTRUCTIONS Issued: February 5, 2013 Applicable for Dates of Service beginning July 1, 2012 UB-04 BILLING INSTRUCTIONS FOR NURSING FACILITY SERVICES
MARYLAND MEDICAID NURSING FACILITY SERVICES UB-04 BILLING INSTRUCTIONS Issued: February 5, 2013 Applicable for Dates of Service beginning July 1, 2012 UB-04 BILLING INSTRUCTIONS FOR NURSING FACILITY SERVICES
Medicare Intermediary Manual Part 3 - Claims Process
 Medicare Intermediary Manual Part 3 - Claims Process Department of Health and Human Services (DHHS) HEALTH CARE FINANCING ADMINISTRATION (HCFA) Transmittal 1795 Date: APRIL 2000 CHANGE REQUEST 1111 HEADER
Medicare Intermediary Manual Part 3 - Claims Process Department of Health and Human Services (DHHS) HEALTH CARE FINANCING ADMINISTRATION (HCFA) Transmittal 1795 Date: APRIL 2000 CHANGE REQUEST 1111 HEADER
Clarification of Patient Discharge Status Codes and Hospital Transfer Policies
 The Acute Inpatient Prospective Payment System Fact Sheet (revised November 2007), which provides general information about the Acute Inpatient Prospective Payment System (IPPS) and how IPPS rates are
The Acute Inpatient Prospective Payment System Fact Sheet (revised November 2007), which provides general information about the Acute Inpatient Prospective Payment System (IPPS) and how IPPS rates are
Tips for Completing the CMS-1500 Claim Form
 Tips for Completing the CMS-1500 Claim Form Member Information (s 1-13) 1 Coverage Optional Show the type of health insurance coverage applicable to this claim by checking the appropriate box (e.g., if
Tips for Completing the CMS-1500 Claim Form Member Information (s 1-13) 1 Coverage Optional Show the type of health insurance coverage applicable to this claim by checking the appropriate box (e.g., if
The following is a description of the fields that appear on the results page for the Procedure Code Search.
 Fee Schedule Legend Updated: 9/21/2015 The following is a description of the fields that appear on the results page for the Procedure Code Search. Procedure Code the five-character procedure code as listed
Fee Schedule Legend Updated: 9/21/2015 The following is a description of the fields that appear on the results page for the Procedure Code Search. Procedure Code the five-character procedure code as listed
UHIN STANDARDS COMMITTEE Version 3.2 5010 Dental Claim Billing Standard J430
 UHIN STANDARDS COMMITTEE Version 3.2 5010 Dental Claim Billing Standard J430 Purpose: The purpose of the Dental Billing Standard, is to clearly describe the standard use of each Item Number (for print
UHIN STANDARDS COMMITTEE Version 3.2 5010 Dental Claim Billing Standard J430 Purpose: The purpose of the Dental Billing Standard, is to clearly describe the standard use of each Item Number (for print
You must write REHAB at the top center of the claim form!
 CMS 1500 (02/12 INSTRUCTIONS FOR REHABILITATION CENTER SERVICES You must write REHAB at the top center of the claim form! Locator # Description Instructions Alerts 1 Medicare / Medicaid / Tricare Champus
CMS 1500 (02/12 INSTRUCTIONS FOR REHABILITATION CENTER SERVICES You must write REHAB at the top center of the claim form! Locator # Description Instructions Alerts 1 Medicare / Medicaid / Tricare Champus
Transactions Module. 70 Royal Little Drive. Providence, RI 02904. Copyright 2002-2014 Optum. All rights reserved. Updated: 3/1/14
 70 Royal Little Drive Providence, RI 02904 Copyright 2002-2014 Optum. All rights reserved. Updated: 3/1/14 Table of Contents 1 Transactions Module...1 2 Charge Overview...3 2.1.1 Explosion Codes...3 2.1.2
70 Royal Little Drive Providence, RI 02904 Copyright 2002-2014 Optum. All rights reserved. Updated: 3/1/14 Table of Contents 1 Transactions Module...1 2 Charge Overview...3 2.1.1 Explosion Codes...3 2.1.2
Inpatient Transfers, Discharges and Readmissions July 19, 2012
 Inpatient Transfers, Discharges and Readmissions July 19, 2012 Discharge Status Codes Two-digit code Identifies where the patient is at conclusion of encounter Visit Inpatient stay End of billing cycle
Inpatient Transfers, Discharges and Readmissions July 19, 2012 Discharge Status Codes Two-digit code Identifies where the patient is at conclusion of encounter Visit Inpatient stay End of billing cycle
UB-04 Billing Guide for PROMISe ICF/MR, ICF/ORCs and State MR Centers
 October 2008 UB-04 Billing Guide for PROISe ICF/R, ICF/ORCs and State R Centers Purpose of the Document Document at Font Sizes The purpose of this document is to provide a block-by-block reference guide
October 2008 UB-04 Billing Guide for PROISe ICF/R, ICF/ORCs and State R Centers Purpose of the Document Document at Font Sizes The purpose of this document is to provide a block-by-block reference guide
HCPCS codes should be used to describe outpatient diagnostic laboratory procedures (revenue codes 300 to 319).
.") 6How Do I Bill Tribal Outpatient Hospital Services? Complete the UB-04 form for outpatient hospital services. Refer to How do I complete the UB-04? in the Billing Guidelines section for specific information
6How Do I Bill Tribal Outpatient Hospital Services? Complete the UB-04 form for outpatient hospital services. Refer to How do I complete the UB-04? in the Billing Guidelines section for specific information
Item Seq # Data Element Format Position Position. Locator
 1 Provider Number (Medicare/VHI) PIC X(6) 1 6 Medicare Provider Number or number assigned by VHI. 2 Provider NPI PIC X(10) 7 16 Provider's NPI 56 3 Patient Control Number PIC X(20) 17 36 Patient Control
1 Provider Number (Medicare/VHI) PIC X(6) 1 6 Medicare Provider Number or number assigned by VHI. 2 Provider NPI PIC X(10) 7 16 Provider's NPI 56 3 Patient Control Number PIC X(20) 17 36 Patient Control
Inpatient/Outpatient Hospital
 Inpatient/Outpatient Hospital Inpatient/Outpatient Hospital... i Inpatient/Outpatient Hospital...3 Billing Information...3 National Provider Identifier (NPI)... 3 Paper Claims... 3 Electronic Claims...
Inpatient/Outpatient Hospital Inpatient/Outpatient Hospital... i Inpatient/Outpatient Hospital...3 Billing Information...3 National Provider Identifier (NPI)... 3 Paper Claims... 3 Electronic Claims...
INSTITUTIONAL. billing module
 INSTITUTIONAL billing module UB-92 Billing Module Basic Rules... 2 Before You Begin... 2 Reimbursement and Co-payment... 2 How to Complete the UB-92... 5 1 Basic Rules Instructions for completing the UB-92
INSTITUTIONAL billing module UB-92 Billing Module Basic Rules... 2 Before You Begin... 2 Reimbursement and Co-payment... 2 How to Complete the UB-92... 5 1 Basic Rules Instructions for completing the UB-92
Postacute Care Transfer Rule Review. HFMA Northern California COMPLIANCE WEBINAR SERIES California Statewide Webinar February 2012.
 Postacute Care Transfer Rule Review HFMA Northern California COMPLIANCE WEBINAR SERIES California Statewide Webinar February 2012 Speaker Gloryanne Bryant, RHIA, RHIT, CCS, CCDS Regional Managing Director
Postacute Care Transfer Rule Review HFMA Northern California COMPLIANCE WEBINAR SERIES California Statewide Webinar February 2012 Speaker Gloryanne Bryant, RHIA, RHIT, CCS, CCDS Regional Managing Director
Please follow these suggestions in order to facilitate timely reimbursement of claims and to avoid timely filing issues:
 Claims/Payment Section K-1 New Claims Submissions All claims must be submitted and received by Molina Healthcare of New Mexico, Inc. (Molina Healthcare) within ninety (90) days from the date of service
Claims/Payment Section K-1 New Claims Submissions All claims must be submitted and received by Molina Healthcare of New Mexico, Inc. (Molina Healthcare) within ninety (90) days from the date of service
INSTITUTIONAL. [Type text] [Type text] [Type text] Version 2015-01
![INSTITUTIONAL. [Type text] [Type text] [Type text] Version 2015-01](/thumbs/40/21640943.jpg "INSTITUTIONAL. [Type text] [Type text] [Type text] Version 2015-01") New York State Medicaid General Billing Guidelines [Type text] [Type text] [Type text] Version 2015-01 10/1/2015 EMEDNY INFORMATION emedny is the name of the electronic New York State Medicaid system.
New York State Medicaid General Billing Guidelines [Type text] [Type text] [Type text] Version 2015-01 10/1/2015 EMEDNY INFORMATION emedny is the name of the electronic New York State Medicaid system.
Institutional Claim Billing Reimbursement. HP Provider Relations/October 2013
 Institutional Claim Billing Reimbursement HP Provider Relations/October 2013 Agenda Objectives Institutional Claim Basics Inpatient Claim Payment Outpatient Claim Payment Enhanced Code Auditing Billing
Institutional Claim Billing Reimbursement HP Provider Relations/October 2013 Agenda Objectives Institutional Claim Basics Inpatient Claim Payment Outpatient Claim Payment Enhanced Code Auditing Billing
FAILURE TO PROVIDE VALID INFORMATION MATCHING THE INSURED S ID CARD COULD RESULT IN A REJECTION OF YOUR CLAIM.
 FAILURE TO PROVIDE VALID INFORMATION MATCHING THE INSURED S ID CARD COULD RESULT IN A REJECTION OF YOUR CLAIM. Enter in the white, open carrier area the name and address of the payer to whom this claim
FAILURE TO PROVIDE VALID INFORMATION MATCHING THE INSURED S ID CARD COULD RESULT IN A REJECTION OF YOUR CLAIM. Enter in the white, open carrier area the name and address of the payer to whom this claim
professional billing module
 professional billing module Professional CMS-1500 Billing Module Coding Requirements...2 Evaluation and Management Services...2 Diagnosis...2 Procedures...2 Basic Rules...3 Before You Begin...3 Modifiers...3
professional billing module Professional CMS-1500 Billing Module Coding Requirements...2 Evaluation and Management Services...2 Diagnosis...2 Procedures...2 Basic Rules...3 Before You Begin...3 Modifiers...3
Home Health Services Billing Manual
 Home Health Services Billing Manual F245-424-000 (07-2015) Home Health Services Billing Instructions About Billing Instructions... 1 Where can you find help with L&I billing procedures?... 1 About Labor
Home Health Services Billing Manual F245-424-000 (07-2015) Home Health Services Billing Instructions About Billing Instructions... 1 Where can you find help with L&I billing procedures?... 1 About Labor
How To Discharge From A Hospital
 Principal Source of Payment Principal Source of Payment Length: 2 Expected principal source of payment for this hospital admission. 01 = Medicare (Fee For Service Plans Only) 02 = Medicaid/QUEST Expanded
Principal Source of Payment Principal Source of Payment Length: 2 Expected principal source of payment for this hospital admission. 01 = Medicare (Fee For Service Plans Only) 02 = Medicaid/QUEST Expanded
HOW TO SUBMIT OWCP - 1500 BILLS TO ACS
 HOW TO SUBMIT OWCP - 1500 BILLS TO ACS The services performed by the following providers should be billed on the OWCP-1500 Form: Physicians (MD, DO) Radiologists Independent Laboratories Audiologists/Speech
HOW TO SUBMIT OWCP - 1500 BILLS TO ACS The services performed by the following providers should be billed on the OWCP-1500 Form: Physicians (MD, DO) Radiologists Independent Laboratories Audiologists/Speech
Provider Adjustment, Time limit & Medicare Override Job Aid
 Provider Adjustment, Time limit & Medicare Override Job Aid Contents Overview... 1 Medicaid Resolution Inquiry Form... 1 Medicare Overrides... 3 Time Limit Overrides... 3 Adjusting a Claim through the
Provider Adjustment, Time limit & Medicare Override Job Aid Contents Overview... 1 Medicaid Resolution Inquiry Form... 1 Medicare Overrides... 3 Time Limit Overrides... 3 Adjusting a Claim through the
CMS 1500 Training 101
 CMS 1500 Training 101 HP Enterprise Services Learning Objective Welcome, this training presentation will educate you on how to complete a CMS 1500 claim form; this includes a detailed explanation of all
CMS 1500 Training 101 HP Enterprise Services Learning Objective Welcome, this training presentation will educate you on how to complete a CMS 1500 claim form; this includes a detailed explanation of all
1500 Claims Processing Manual DHMP Health Insurance Claim Form CMS-1500
 DENVER HEALTH MEDICAL PLAN, INC. 1500 Claims Processing Manual DHMP Health Insurance Claim Form CMS-1500 Box 1 Medicare, Medicaid, Group Health Plan or other insurance Information Show the type of health
DENVER HEALTH MEDICAL PLAN, INC. 1500 Claims Processing Manual DHMP Health Insurance Claim Form CMS-1500 Box 1 Medicare, Medicaid, Group Health Plan or other insurance Information Show the type of health
Glossary. Adults: Individuals ages 19 through 64. Allowed amounts: See prices paid. Allowed costs: See prices paid.
 Glossary Acute inpatient: A subservice category of the inpatient facility clams that have excluded skilled nursing facilities (SNF), hospice, and ungroupable claims. This subcategory was previously known
Glossary Acute inpatient: A subservice category of the inpatient facility clams that have excluded skilled nursing facilities (SNF), hospice, and ungroupable claims. This subcategory was previously known
Institutional Billing Guide
 Program KANSAS MEDICAL ASSISTANCE PROGRAM Institutional Billing Guide Updated 10.2013 Institutional Billing The Kansas Medical Assistance Program (KMAP) offers different billing options to all providers.
Program KANSAS MEDICAL ASSISTANCE PROGRAM Institutional Billing Guide Updated 10.2013 Institutional Billing The Kansas Medical Assistance Program (KMAP) offers different billing options to all providers.
Psychiatric Residential Treatment Facilities (PRTFs)
") Psychiatric Residential Treatment Facilities (PRTFs) Providers must be enrolled as a Colorado Medical Assistance Program provider in order to: Treat a Colorado Medical Assistance Program client Submit
Psychiatric Residential Treatment Facilities (PRTFs) Providers must be enrolled as a Colorado Medical Assistance Program provider in order to: Treat a Colorado Medical Assistance Program client Submit
Professional Claim (CMS-1500) Field Descriptions
 Field Descriptions") Professional Claim (CMS-1500) Field s Following are Group Health s clean claim requirements for the professional claims form. The electronic descriptions provided here are intended only as a guide for
Professional Claim (CMS-1500) Field s Following are Group Health s clean claim requirements for the professional claims form. The electronic descriptions provided here are intended only as a guide for
UB-04 Billing Guide for PROMISe Ambulatory Surgical Centers
 February 6, 2014 UB-04 Billing Guide for PROISe mbulatory Surgical Purpose of the Document Document at Font Sizes The purpose of this document is to provide a block-by-block reference guide to assist the
February 6, 2014 UB-04 Billing Guide for PROISe mbulatory Surgical Purpose of the Document Document at Font Sizes The purpose of this document is to provide a block-by-block reference guide to assist the
Get With The Guidelines - Stroke PMT Special Initiatives Tab for Ohio Coverdell Stroke Program CODING INSTRUCTIONS Effective 10-24-15
 Get With The Guidelines - Stroke PMT Special Initiatives Tab for Ohio Coverdell Stroke Program CODING INSTRUCTIONS Effective 10-24-15 Date and time first seen by ED MD: The time entered should be the earliest
Get With The Guidelines - Stroke PMT Special Initiatives Tab for Ohio Coverdell Stroke Program CODING INSTRUCTIONS Effective 10-24-15 Date and time first seen by ED MD: The time entered should be the earliest
Place of Service Codes for Professional Claims Database (updated November 1, 2012)
") Place of Codes for Professional Claims Database (updated November 1, 2012) Listed below are place of service codes and descriptions. These codes should be used on professional claims to specify the entity
Place of Codes for Professional Claims Database (updated November 1, 2012) Listed below are place of service codes and descriptions. These codes should be used on professional claims to specify the entity
The New Hampshire Comprehensive Health Care Information System (NH CHIS) Public Use Data Dictionary Version 1
 Public Use Data Dictionary Version 1") The New Hampshire Comprehensive Health Care Information System (NH CHIS) Public Use Data Dictionary Version 1 February 2015 Prepared for the New Hampshire Department of Health and Human Services Maintained
The New Hampshire Comprehensive Health Care Information System (NH CHIS) Public Use Data Dictionary Version 1 February 2015 Prepared for the New Hampshire Department of Health and Human Services Maintained
UB04 Hospital Billing Instructions
 Department of Health & Mental Hygiene Medical Assistance UB04 Hospital Billing Instructions Revised 2/12 Medical Assistance Problem Resolution Institutional Hotline: 410-767-5457 Stacy A. Hromanik, Division
Department of Health & Mental Hygiene Medical Assistance UB04 Hospital Billing Instructions Revised 2/12 Medical Assistance Problem Resolution Institutional Hotline: 410-767-5457 Stacy A. Hromanik, Division
Place of Service Codes for Professional Claims Database (updated August 6, 2015)
") Place of Codes for Professional Claims Database (updated August 6, 2015) Listed below are place of service codes and descriptions. These codes should be used on professional claims to specify the entity
Place of Codes for Professional Claims Database (updated August 6, 2015) Listed below are place of service codes and descriptions. These codes should be used on professional claims to specify the entity
Medicare Claims Processing Manual
 Medicare Claims Processing Manual Chapter 11 - Processing Hospice Claims Transmittals for Chapter 11 Crosswalk to Source Material 10 - Overview Table of Contents (Rev. 1673, 01-30-09) (Rev. 1708, 04-03-09)
Medicare Claims Processing Manual Chapter 11 - Processing Hospice Claims Transmittals for Chapter 11 Crosswalk to Source Material 10 - Overview Table of Contents (Rev. 1673, 01-30-09) (Rev. 1708, 04-03-09)
CHAPTER 7 (E) DENTAL PROGRAM CLAIMS FILING CHAPTER CONTENTS
 DENTAL PROGRAM CLAIMS FILING CHAPTER CONTENTS") CHAPTER 7 (E) DENTAL PROGRAM CHAPTER CONTENTS 7.0 CLAIMS SUBMISSION AND PROCESSING...1 7.1 ELECTRONIC MEDIA CLAIMS (EMC) FILING...1 7.2 CLAIMS DOCUMENTATION...2 7.3 THIRD PARTY LIABILITY (TPL)...2 7.4
CHAPTER 7 (E) DENTAL PROGRAM CHAPTER CONTENTS 7.0 CLAIMS SUBMISSION AND PROCESSING...1 7.1 ELECTRONIC MEDIA CLAIMS (EMC) FILING...1 7.2 CLAIMS DOCUMENTATION...2 7.3 THIRD PARTY LIABILITY (TPL)...2 7.4
IWCC 50 ILLINOIS ADMINISTRATIVE CODE 7110 7110.90. Section 7110.90 Illinois Workers' Compensation Commission Medical Fee Schedule
 Section 7110.90 Illinois Workers' Compensation Commission Medical Fee Schedule a) In accordance with Sections 8(a), 8.2 and 16 of the Workers' Compensation Act [820 ILCS 305/8(a), 8.2 and 16] (the Act),
Section 7110.90 Illinois Workers' Compensation Commission Medical Fee Schedule a) In accordance with Sections 8(a), 8.2 and 16 of the Workers' Compensation Act [820 ILCS 305/8(a), 8.2 and 16] (the Act),
Top 50 Billing Error Reason Codes With Common Resolutions (09-12)
") Top 50 Billing Error Reason Codes With Common Resolutions (09-12) On the following table you will find the top 50 Error Reason Codes with Common Resolutions for denied claims at Virginia Medicaid. This
Top 50 Billing Error Reason Codes With Common Resolutions (09-12) On the following table you will find the top 50 Error Reason Codes with Common Resolutions for denied claims at Virginia Medicaid. This
Minnesota Health Care Programs (MHCP) MN ITS Interactive User Guide http://mn-its.dhs.state.mn.us. Using MN ITS Interactive. Entering an Online Claim
 MN ITS Interactive User Guide http://mn-its.dhs.state.mn.us. Using MN ITS Interactive. Entering an Online Claim") Minnesota Health Care Programs (MHCP) MN ITS Interactive User Guide http://mn-its.dhs.state.mn.us Objective Performed by Background Claim Form Completing a MN ITS Interactive Professional (837P) claim
Minnesota Health Care Programs (MHCP) MN ITS Interactive User Guide http://mn-its.dhs.state.mn.us Objective Performed by Background Claim Form Completing a MN ITS Interactive Professional (837P) claim
BILL TYPES PAGE 1 OF 8 UPDATED: 9/13
 INPATIENT HOSPITAL 111 REGULAR INPATIENT 112 FIRST PORTION: CONTINUOUS STAY INPATIENT 113 SUBSEQUENT PORTION: CONTINUOUS STAY INPATIENT 114 FINAL PORTION: CONTINUOUS STAY INPATIENT 115 INPATIENT: LATE
INPATIENT HOSPITAL 111 REGULAR INPATIENT 112 FIRST PORTION: CONTINUOUS STAY INPATIENT 113 SUBSEQUENT PORTION: CONTINUOUS STAY INPATIENT 114 FINAL PORTION: CONTINUOUS STAY INPATIENT 115 INPATIENT: LATE
UB-92 Billing Instructions for Inpatient Chemical Dependency Services
 UB-92 Billing Instructions for Inpatient Chemical Dependency Services General Instructions The placing authority (county or tribe) authorizes Chemical Dependency services for eligible recipients. Bill
UB-92 Billing Instructions for Inpatient Chemical Dependency Services General Instructions The placing authority (county or tribe) authorizes Chemical Dependency services for eligible recipients. Bill
Critical Access Hospital (CAH) and CAH Swingbed Questions and Answers
 and CAH Swingbed Questions and Answers") Critical Access Hospital (CAH) and CAH Swingbed Questions and Answers The following questions and answers are from the April 2012 CAH and CAH Swingbed web-based trainings: Q1. Is a non-covered/no pay bill
Critical Access Hospital (CAH) and CAH Swingbed Questions and Answers The following questions and answers are from the April 2012 CAH and CAH Swingbed web-based trainings: Q1. Is a non-covered/no pay bill
Remittance and Status (R&S) Reports
 Reports") Remittance and Status (R&S) Reports Chapter.1 R&S Report Information........................................................... -2.1.1 Electronic Remittance and Status (ER&S) Reports.............................
Remittance and Status (R&S) Reports Chapter.1 R&S Report Information........................................................... -2.1.1 Electronic Remittance and Status (ER&S) Reports.............................
CODE DESCRIPTION 011 Claim denial (claim level) due to SF message 012 Line denial (line level) due to SF message 017 Incorrect Alpha Prefix 030
 due to SF message 012 Line denial (line level) due to SF message 017 Incorrect Alpha Prefix 030") CODE DESCRIPTION 011 Claim denial (claim level) due to SF message 012 Line denial (line level) due to SF message 017 Incorrect Alpha Prefix 030 Missing service provider zip code (box 32) 031 Missing pickup
CODE DESCRIPTION 011 Claim denial (claim level) due to SF message 012 Line denial (line level) due to SF message 017 Incorrect Alpha Prefix 030 Missing service provider zip code (box 32) 031 Missing pickup
Completing a CMS 1500 Form
 Completing a CMS 1500 Form 1 So you want to submit clean paper claims! Most offices submit electronic claims, but there are still small offices that submit paper claims and other times when a paper claim
Completing a CMS 1500 Form 1 So you want to submit clean paper claims! Most offices submit electronic claims, but there are still small offices that submit paper claims and other times when a paper claim
Glossary of Terms. Account Number/Client Code. Adjudication ANSI. Assignment of Benefits
 Account Number/Client Code Adjudication ANSI Assignment of Benefits Billing Provider/Pay-to-Provider Billing Service Business Associate Agreement Clean Claim Clearinghouse CLIA Number (Clinical Laboratory
Account Number/Client Code Adjudication ANSI Assignment of Benefits Billing Provider/Pay-to-Provider Billing Service Business Associate Agreement Clean Claim Clearinghouse CLIA Number (Clinical Laboratory
MEDICARE CREDIT BALANCE REPORT CERTIFICATION PAGE
 DEPAR ARTMENT OF HEALTH AND HUMAN SERVICES Form Approved OMB No. 0938-0600 MEDICARE CREDIT BALANCE REPORT CERTIFICATION PAGE The Credit Balance Report is required under the authority of sections 1815(a),
DEPAR ARTMENT OF HEALTH AND HUMAN SERVICES Form Approved OMB No. 0938-0600 MEDICARE CREDIT BALANCE REPORT CERTIFICATION PAGE The Credit Balance Report is required under the authority of sections 1815(a),
The following provider types should bill using the Dental claim form:
 Section: 4.0 Dental Claim Form This section explains the procedures for obtaining reimbursement for dental services submitted to Medicaid. Mississippi Medicaid accepts both electronic and paper dental
Section: 4.0 Dental Claim Form This section explains the procedures for obtaining reimbursement for dental services submitted to Medicaid. Mississippi Medicaid accepts both electronic and paper dental
Inpatient Services. Guide to Billing Facility Services. November 2013. Preface. Summary of Changes. Table of Contents.
 Inpatient Services Preface Summary of Changes Table of Contents Service Contacts November 2013 Replaces: December 2012 S-5781 11/13 Preface The Wellmark Provider Guide and specialty guides are billing
Inpatient Services Preface Summary of Changes Table of Contents Service Contacts November 2013 Replaces: December 2012 S-5781 11/13 Preface The Wellmark Provider Guide and specialty guides are billing
2012 ADA Dental Claim Form Instructions
 2012 ADA Dental Claim Form Instructions June 9, 2015 Date (mm/dd/yyyy) Description of Changes Impact 02/11/2014 Initial version 07/16/2014 Updated instructions for fields 29a and 32 06/09/2015 Clarified
2012 ADA Dental Claim Form Instructions June 9, 2015 Date (mm/dd/yyyy) Description of Changes Impact 02/11/2014 Initial version 07/16/2014 Updated instructions for fields 29a and 32 06/09/2015 Clarified
CLAIM FORM REQUIREMENTS
 CLAIM FORM REQUIREMENTS When billing for services, please pay attention to the following points: Submit claims on a current CMS 1500 or UB04 form. Please include the following information: 1. Patient s
CLAIM FORM REQUIREMENTS When billing for services, please pay attention to the following points: Submit claims on a current CMS 1500 or UB04 form. Please include the following information: 1. Patient s
Chapter 7: Inpatient & Outpatient Hospital Care
 7 Inpatient & Outpatient Hospital Care ACUTE INPATIENT ADMISSIONS All elective and emergent admissions require prior authorization and/or notification for all Health Choice Generations Members admissions.
7 Inpatient & Outpatient Hospital Care ACUTE INPATIENT ADMISSIONS All elective and emergent admissions require prior authorization and/or notification for all Health Choice Generations Members admissions.
Physician, Health Care Professional, Facility and Ancillary Provider Administrative Guide for American Medical Security Life Insurance Company
 Physician, Health Care Professional, Facility and Ancillary Provider Administrative Guide for American Medical Security Life Insurance Company Insureds 2009 Contents How to contact us... 2 Our claims process...
Physician, Health Care Professional, Facility and Ancillary Provider Administrative Guide for American Medical Security Life Insurance Company Insureds 2009 Contents How to contact us... 2 Our claims process...
Note: The number in parenthesis corresponds to the number of the variable on the CMS Version K file documentation. 1
 1 Patient ID (patient_id) SEER Cases (Patient ID) 11 Use First 10 Characters only for SEER cases. 1 Registry 2 02 = Connecticut 20 = Detroit 21 = Hawaii 22 = Iowa 23 = New Mexico 25 = Seattle 26 = Utah
1 Patient ID (patient_id) SEER Cases (Patient ID) 11 Use First 10 Characters only for SEER cases. 1 Registry 2 02 = Connecticut 20 = Detroit 21 = Hawaii 22 = Iowa 23 = New Mexico 25 = Seattle 26 = Utah
Medicare Claims Processing Manual Chapter 11 - Processing Hospice Claims
 Medicare Claims Processing Manual Chapter 11 - Processing Hospice Claims Transmittals for Chapter 11 Table of Contents (Rev. 3118, 11-06-14) 10 - Overview 10.1 - Hospice Pre-Election Evaluation and Counseling
Medicare Claims Processing Manual Chapter 11 - Processing Hospice Claims Transmittals for Chapter 11 Table of Contents (Rev. 3118, 11-06-14) 10 - Overview 10.1 - Hospice Pre-Election Evaluation and Counseling
Claim Status Response Explanation of Benefits List
 20 Accepted for processing 066 CLAIM CURRENTLY IN PROCESS. DO NOT RESUBMIT 21 Missing or invalid information 018 REFERRING PHYSICIAN INFORMATION REQUIRED AND NOT PRESENT Referring 21 Missing or invalid
20 Accepted for processing 066 CLAIM CURRENTLY IN PROCESS. DO NOT RESUBMIT 21 Missing or invalid information 018 REFERRING PHYSICIAN INFORMATION REQUIRED AND NOT PRESENT Referring 21 Missing or invalid
Institutional Claim (UB-04) Field Descriptions
 Field Descriptions") Institutional Claim (UB-04) Field s Following are Group Health s clean claim requirements for the institutional claims form. The electronic descriptions provided here are intended only as a guide for discussions
Institutional Claim (UB-04) Field s Following are Group Health s clean claim requirements for the institutional claims form. The electronic descriptions provided here are intended only as a guide for discussions
Preface. Summary of Changes. Table of Contents. Service Contacts. October 2014 Replaces: May 2014 S-5781 10/14
 Preface Summary of Changes Table of Contents Service Contacts October 2014 Replaces: May 2014 S-5781 10/14 Preface The Wellmark Provider Guide and specialty guides are billing resources for providers doing
Preface Summary of Changes Table of Contents Service Contacts October 2014 Replaces: May 2014 S-5781 10/14 Preface The Wellmark Provider Guide and specialty guides are billing resources for providers doing
This guide was designed for employees in the University System of Georgia Indemnity HealthCare plan who reside abroad
 University System of Georgia Guide for GA TECH Employees Residing Abroad This guide was designed for employees in the University System of Georgia Indemnity HealthCare plan who reside abroad. Frequently
University System of Georgia Guide for GA TECH Employees Residing Abroad This guide was designed for employees in the University System of Georgia Indemnity HealthCare plan who reside abroad. Frequently
Medicare-Medicaid Crossover Claims FAQ
 Medicare-Medicaid Crossover Claims FAQ Table of Contents 1. Benefits of Crossover Claims... 1 2. General Information... 1 3. Medicare Part B Professional Claims and DMERC Claims... 2 4. Professional Miscellaneous...
Medicare-Medicaid Crossover Claims FAQ Table of Contents 1. Benefits of Crossover Claims... 1 2. General Information... 1 3. Medicare Part B Professional Claims and DMERC Claims... 2 4. Professional Miscellaneous...
Claims Procedures. H.2 At a Glance. H.4 Submission Guidelines. H.9 Claims Documentation. H.17 Codes and Modifiers. H.
 H.2 At a Glance H.4 Submission Guidelines H.9 Claims Documentation H.17 Codes and Modifiers H.22 Reimbursement H.25 Denials and Appeals At a Glance pledges to provide accurate and efficient claims processing.
H.2 At a Glance H.4 Submission Guidelines H.9 Claims Documentation H.17 Codes and Modifiers H.22 Reimbursement H.25 Denials and Appeals At a Glance pledges to provide accurate and efficient claims processing.
ForwardHealth Provider Portal Professional Claims
 P- ForwardHealth Provider Portal Professional Claims User Guide i Table of Contents 1 Introduction... 1 2 Access the Claims Page... 2 3 Submit a Professional Claim... 5 3.1 Professional Claim Panel...
P- ForwardHealth Provider Portal Professional Claims User Guide i Table of Contents 1 Introduction... 1 2 Access the Claims Page... 2 3 Submit a Professional Claim... 5 3.1 Professional Claim Panel...
COM Compliance Policy No. 3
 COM Compliance Policy No. 3 THE UNIVERSITY OF ILLINOIS AT CHICAGO NO.: 3 UIC College of Medicine DATE: 8/5/10 Chicago, Illinois PAGE: 1of 7 UNIVERSITY OF ILLINOIS COLLEGE OF MEDICINE CODING AND DOCUMENTATION
COM Compliance Policy No. 3 THE UNIVERSITY OF ILLINOIS AT CHICAGO NO.: 3 UIC College of Medicine DATE: 8/5/10 Chicago, Illinois PAGE: 1of 7 UNIVERSITY OF ILLINOIS COLLEGE OF MEDICINE CODING AND DOCUMENTATION
HIPAA 5010 Issues & Challenges: 837 Claims
 HIPAA 5010 Issues & Challenges: 837 Claims Physicians Hospitals Dentists Payers Last update: March 22, 2012 Table of Contents Physicians... 4 Billing Provider Address... 4 Pay-to Provider Name Information...
HIPAA 5010 Issues & Challenges: 837 Claims Physicians Hospitals Dentists Payers Last update: March 22, 2012 Table of Contents Physicians... 4 Billing Provider Address... 4 Pay-to Provider Name Information...
CMS-1500 Claim Form/American National Standards Institute (ANSI) Crosswalk for Paper/Electronic Claims
 Crosswalk for Paper/Electronic Claims") There are two ways to file Medicare claims to CGS - electronically or through a paper form created by the Centers for Medicare & Medicaid Services (CMS-1500). The required information is the same regardless
There are two ways to file Medicare claims to CGS - electronically or through a paper form created by the Centers for Medicare & Medicaid Services (CMS-1500). The required information is the same regardless
Medi-Cal Retroactive Claim Submissions
 Medi-Cal Retroactive Claim Submissions This training made possible by funding from the CMSP Governing Board Presented by Penni Wright, EDS/Medi-Cal, Provider Training Introduction Some CMSP members may
Medi-Cal Retroactive Claim Submissions This training made possible by funding from the CMSP Governing Board Presented by Penni Wright, EDS/Medi-Cal, Provider Training Introduction Some CMSP members may
Claim Filing Instructions. For AmeriHealth Caritas Louisiana Providers
 Claim Filing Instructions For AmeriHealth Caritas Louisiana Providers September 2015 AmeriHealth Caritas Louisiana Claim Filing Instructions Table of Contents Claim Filing... 1 Procedures for Claim Submission...
Claim Filing Instructions For AmeriHealth Caritas Louisiana Providers September 2015 AmeriHealth Caritas Louisiana Claim Filing Instructions Table of Contents Claim Filing... 1 Procedures for Claim Submission...
University of Mississippi Medical Center. Access Management. Patient Access Specialists II
 Financial Terminology in Access Management University of Mississippi Medical Center Access Management Patient Access Specialists II As a Patient Access Specialist You are the FIRST STAGE in the Revenue
Financial Terminology in Access Management University of Mississippi Medical Center Access Management Patient Access Specialists II As a Patient Access Specialist You are the FIRST STAGE in the Revenue
UB-04 Billing Guide for PROMISe Inpatient Rehabilitation Hospitals & Facilities
 February 6, 2014 Hospitals & Facilities Purpose of the Document Document at Font Sizes Signature pproval The purpose of this document is to provide a block-by-block reference guide to assist the following
February 6, 2014 Hospitals & Facilities Purpose of the Document Document at Font Sizes Signature pproval The purpose of this document is to provide a block-by-block reference guide to assist the following