Alternatives to Surgical Resection for Early Stage Lung Cancer
|
|
|
- Blaise Blankenship
- 8 years ago
- Views:
Transcription
1 Alternatives to Surgical Resection for Early Stage Lung Cancer Neil A. Christie MD University of Pittsburgh Medical Center Department of Thoracic Surgery Allied Health Personnel Symposium AATS 2014

2 Conflicts Educational speaker for Varian

3 Lung Cancer: Scope of the Problem 170,000 plus cases in US each year Leading cause of cancer death with 15% 5 year survival

4 Limited Stage Lung Cancer 16% of new cases stage IA or IB with tumor confined to the lung Surgical cure rates for early stage lung cancer 75% for pathologic stage IA 60% for pathologic stage IB

5
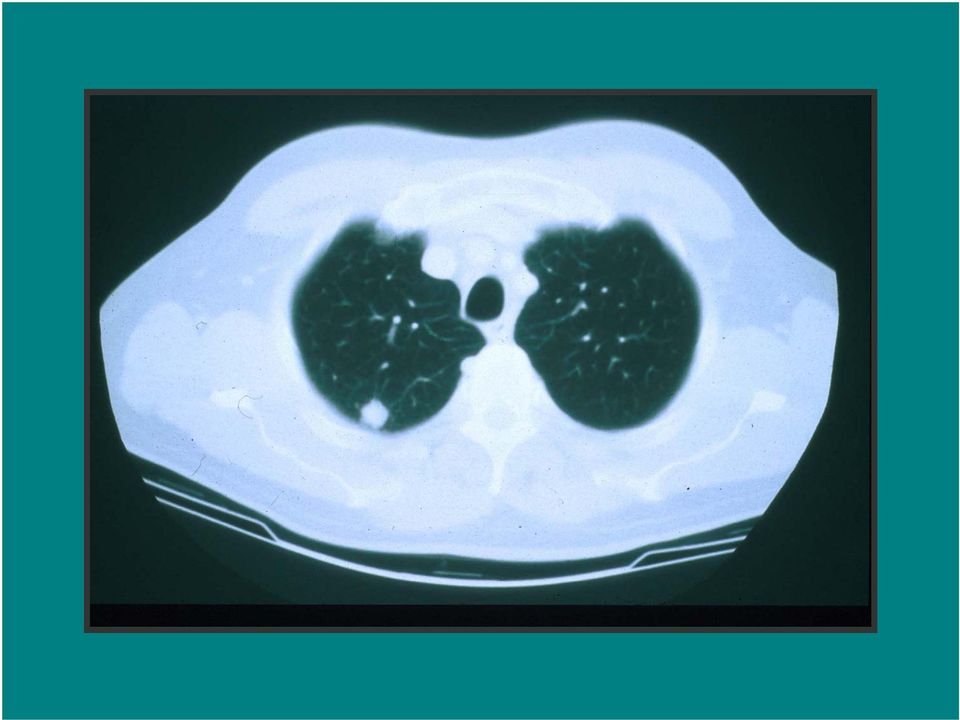
6 Surgery for Lung Cancer anatomic lobectomy along with the N1 lymph nodes that are within the visceral pleural envelope Sampling or formal lymphadenectomy of the central mediastinal N2 lymph nodes

7 Medical Comorbidities and Early Stage Lung Cancer Coexisting medical conditions can preclude surgery in some patients COPD Cardiac disease Other medical comorbidities Poor functional status

8 Conventional XRT for Stage I Lung Cancer Poor long term survival and poor local control

9 Newer Ablative Therapies for Localized Lung Cancer Radiofrequency Ablation (RFA) Stereotactic Radiotherapy (SRT) Potentially less morbid procedures which also allow preservation of lung function

10 Talk Overview Radiofrequency Ablation therapy results Stereotactic Radiotherapy results Rationale for patient selection for therapy in marginal patients with early stage lung cancer Conclusions

11 Radiofrequency Ablation (RFA) Alternating current that moves from an active electrode (within a tumor) to dispersive electrodes (electrosurgical return pads)

12 RFA System Generator Active electrode Dispersive electrodes (return pads)

13 RF generator Needle electrode Patient return pads (4 total; 2 on each thigh)

14 Typical Thermal Lesions Produced in Liver 1.0 cm 3.5 cm

15 Goal of RFA Therapy Homogeneous necrosis of the entire tumor as well as a surrounding 1 cm margin of normal lung

16 Upper limits of RF Ablation Upper limit of homogenous tissue ablation for most RF ablation systems is between 4 or 5 cm For ablation of tumors larger than 3 cm multiple overlapping spheres or cylinders of ablation are required with active electrode probe repositioning

17 Published Results of RFA Therapy 22 peer reviewed manuscripts reporting an experience in over 900 patients since 1 st report in year 2000

18 RFA Procedure Anesthetic 50% done with conscious sedation 40% done with general anesthesia 10% done with epidural or local anesthesia only Mean hospital stay 1.3 to 6 days with range from same day discharge to 35 days

19 Results- Tumor Response After RFA Pre-RFA 1 month post-rfa 3 months post-rfa

20 Tumor Ablation Rates Tumor diameter is an important prognostic variable Complete necrosis much more likely in tumors < 3 cm

21 Tumor Ablation Rates Herrera University of Pittsburgh with modified RECIST criteria Complete or partial response 67% of tumors < 5cm 33% of tumors > 5 cm Akebashi with contrast enhanced CT and PET Complete ablation 69% of tumors < 3 cm 39% of tumors >3 cm
22 Ablate and Resect Studies Nguyen and Ambrogi Complete necrosis in 38% and 67% respectively Complete ablation more probable in tumors < 2 cm
23 Survival following RFA Ambrogi Median survival for stage I lung cancer 18.9 months Tumor < 3 cm median survival 30.5 mo Tumor > 3 cm median survival 14.9 mo
24 Survival following RFA Simon with 75 stage I lung cancer patients median survival 29 months 1 year 78% 2 year 57% 3 year 36% 4 year 27% 5 year 27%
25 Complications of RFA Mortality One large study of 153 patients had a 2.6% mortality rate
26 Complications of RFA Pneumothorax: 0 54% (usually 20%) Pneumonia: 0 22% (1 fatal) COPD Exacerbation: 0 6% ARDS: 0 3% (3 fatal) Pulmonary abscess: 0 6% Hemoptysis: 0 12% (1 fatal) Hemothorax: 0 4% Pleural effusion: 0 4% Empyema: 1% BP fistula: 1% Pulmonary Contusion: 0 1%
27 Stereotactic Radiotherapy (SRT)
28 Conventional Radiotherapy Standard approach Gy total dose in 1.8 to 2 Gy fractions 5 year survival rates 10 30%
29 Dose Escalation Benefit to dose escalation with dose response relationship with local control and survival Dose escalation limited by toxicity to lung with radiation pneumonitis
30 3-D Conformal RT More sophisticated planning techniques that limit treatment volumes and radiation to normal lung tissue to allow safer dose escalation Still have significant local failure
31 Stereotactic Radiotherapy (SRT) Three dimensional conformal planning techniques Stereotactic targeting with image guidance Systems to decrease the effect of lung motion
32 Tumor targeting Ablative doses to the tumor Limit radiation to normal tissue to prevent toxicity
33 Compensating for Respiratory Motion Tumor tracking Gating Respiratory inhibition
34 Diagnostic X-Ray Source Linear Accelerator Robotic Arm Image Detectors Treatment Couch
35 Dosimetry Potent dose which confidently hits the target while having a very sharp fall off dose gradient outside the region of the tumor Multiple bream paths from multiple directions
36 Pre Rx
37 xxxxxxxxxxxx
38 Radiosurgery Results Onishi 2007 Hypofractionated stereotactic radiotherapy for stage I lung cancer in 257 patients in a Japanese multi-institutional study Gray in 1 22 fractions Median F/U 38 months 5.4% incidence of symptomatic radiation pneumonitis
39 Radiosurgery Results Local recurrence in 36 patients (14%) BED> 100 Gray 8.4% BED< 100 Gray42.9% 5 year survival 71% for those with BED> 100 vs 30% for BED< 100 Nodal recurrences in 11% 5.1% isolated to LN 3.1% LN and local 2.8% LN and distal
40 Radiosurgery Results Timmerman 2003 Dose escalation study in 37 patients with medically inoperable stage I lung cancer 3 fractions starting at 8 Gray and escalated to 20 Gray No change in pulmonary function 2 patients with grade three pneumonitis 87% tumor response rate 6 patients experienced relapse by 15 months
41 Radiosurgery results Timmerman patients witht1 or T2 lung cancer 60 to 66 Gray in three fractions over 1 2 weeks Local control at 2 years was 95% Median overall survival 32 months Grade 3 5 severe toxicity or death in 14 patients Median time to toxicity was 10.5 months
42 Radiosurgery Results Central tumor predictor of toxicity Large tumor predictor of toxicity
43 Outcomes with current Regimen 20 Gy X 3 peripheral tumors 12 Gy X 4 central tumors Minimal toxicity / no change in PFTs Local control rates 85 to 90 %
44 Phase II Trial SBRT peripheral tumors Timmerman et al. JAMA 2010 Phase II North American Multicenter trial SBRT for T1T2N0 NSCLC (<5cm) peripheral medically inoperable 18 Gy x 3, 3 year F/U 55 patients (44T1, 11T2)
45 Timmerman et al. 51% complete response rate at 6.5 months post Rx Complete or partial response in 89% patients
46 Timmerman et al 1/55 patients had recurrence at treated site 3 year primary control rate 98% 3/55 patients had recurrence within the involved lobe 3 year primary tumor and involved lobe control rate 91%
47 Timmerman et al. 2/55 regional nodal failures (33 and 36 months) 3 year local/regional control rate 87% 11/55 metastatic disease
48 Timmerman et al. 26 patients died in F/U (10 of cancer) 3 year disease free survival 48% 3 year overall survival 56% No treatment related deaths 2 patients with grade III or IV adverse events
49 SBRT vs Wedge Resection Grills et al. Journal of Clinical Oncology, T1-T2NO NSCLC (< 5 cm) Wedge resection 69 patients SBRT 58 patients (medically inoperable) 12 Gy x 4 or 12 Gy x 5 Staged PET/CT +/- mediastinoscopy (30% wedge patients and 20% SBRT patients)
50 Grills et al. Mean FEV both groups SBRT patients older and higher comorbidity index Median F/U 2.5 years
51 Grills et al. Loc Rec Reg Rec Loc Reg Dist Mets Over Surv Can Surv Rec SBRT n=55 4% 4% 9% 19% 72% 93% Wedg n=69 20% 18% 27% 21% 87% 94%
52 SBRT vs Surgery Crabtree et al. JTCVS surgical patients F/U 31 months 49 wedge, 16 seg, 375 lobe, 22 pneum 76 SBRT patients F/U 19 months Staged with CT and PET/CT Surgical patients younger, lower comorbidity scores, better pulmonary function
53 Crabtree et al. Overall Survival Cancer Specific Local Control Survival surgery 68% 82% 96% SBRT 32% 82% 89% 3 year follow-up
54 Crabtree et al. Propensity matching to find 2 similar groups wrt age, clinical stage and comorbidity No difference in overall survival, cancer specific survival, or local control In high risk group operative mortality 7% with 44% complication rate (27% pneumonia or resp failure)
55 Conclusions RFA results comparable to conventional XRT, inferior to surgery and SBRT Await results of ACOSOG phase II trial with standardized technique
56 Conclusions SBRT has excellent local control and better than expected regional control Long term recurrences may be underestimated due to high non-cancer deaths in patient population studied Results of SBRT in operative candidates now showing 80% T1N0 and 70% T2N0
57 Selection of Therapy in Patients with Pulmonary Compromise
58 Treatment Options for Stage I NSCLC (T1/T2 N0 M0) Surgical Resection Lobectomy Sublobar Resection Segmentectomy Wedge Resection Nonsurgical Therapy Ablative techniques Stereotactic Radiosurgery Radiofrequency Ablation Radiation Therapy No Treatment
59 Lobectomy versus Sublobar Resection Type of Resection: / Ablation Lobectomy Local Control + - Sublobar Resection/ Ablation Survival + - Lung Function - +
60 Local Control: Lobectomy vs Sublobar Resection Ginsberg RJ, Rubinstein LV. Randomized Trial of Lobectomy versus limited Resection for T1N0 NSCLC. Annals of Thoracic Surgery (3):615. Local recurrence 21/122 (17%) sublobar resection 8/125 (6%) lobectomy
61 Survival: Lobectomy vs sublobar resection LCSG Limited resection associated with 30% increase in overall death rate and 50% increase in death with cancer
62 5 year survival after resection Okada et al Tumor size lobectomy Segmental resection Wedge resection 20 mm or less 21 to 30 mm Greater than 30 mm 96.7% 92.4% 85.7% 87.4% 84.6% 39.4% 81.3% 62.9% 0%
63 Lung Fuction: Lobectomy vs sublobar resection LCSG FEV1 at 6 and 12 months F/U was preserved in the sublobar resection group versus the lobectomy group
64 Periop mortality in patients with very poor lung Function (NETT) 140 patients FEV1 < 20% DLCO < 20% Perioperative mortality 28.6%
65 Comorbidity, Functional Status and Survival in Stage I NSCLC All were independent predictors of survival for lung cancer; independent of age and treatment modality Age was not a predictor of poor outcome When KPS < 70 and CIRS-G4 no benefit to Surgery Surgical survival 11% XRT survival 6%
66 Lung Resection in the elderly Port et al. Surgical resection for lung cancer in the octogenarian. Chest : patients mean age 82 (range 80 87) 4 pneumonectomies 46 lobectomies 6 segmentectomies 5 wedge resections Death 1/61 (1.6%) Major complications 13% Length of stay 7 days 82% 5 year survival for Stage IA NSCLC
67 Minimally Invasive Lung resection (Thoracoscopic Lobectomy) Onaitis et al. Thoracoscopic lobectomy is a safe and versatile procedure. Experience with 500 consecutive patients. Annals of Surgery 2006; 24(3): % conversion rate Periop mortality 1% Periop morbidity A fib 10% Resp failure 1.2 % MI 0.4% Median length of hospitalization 3 days NSCLC Stage IA 2 year survival 85%
68 Sx vs SBRT Surgery Pros Definitive pathologic diagnosis Enables invasive nodal staging Adjuvant therapy in node pos patients Cons Morbidity and mortality Possible benign disease
69 Sx vs SBRT SBRT Pros 5 year local control rates better than 90% Outpatient and mild toxicity Prservation of lung function and quality of life Cons Treatment without pathologic verification Post treatment fibrosis masking local disease recurrence
70 Clinical staging underestimates regional nodal involvement in up to 25% of cases and would not be addressed by SRT Cure rate for stage II lung cancer with surgery alone is 40% and would expected to be 0% with SRT Determination of residual disease by imaging is not reliable so salvage surgery could be delayed allowing progression of cancer to an advanced (incurable) stage
71 Thank You Lung Ablation Techniques, University of Pittsburgh
A Practical Guide to Advances in Staging and Treatment of NSCLC
 A Practical Guide to Advances in Staging and Treatment of NSCLC Robert J. Korst, M.D. Director, Thoracic Surgery Medical Director, The Blumenthal Cancer Center The Valley Hospital Objectives Revised staging
A Practical Guide to Advances in Staging and Treatment of NSCLC Robert J. Korst, M.D. Director, Thoracic Surgery Medical Director, The Blumenthal Cancer Center The Valley Hospital Objectives Revised staging
Lung Cancer Treatment Guidelines
 Updated June 2014 Derived and updated by consensus of members of the Providence Thoracic Oncology Program with the aid of evidence-based National Comprehensive Cancer Network (NCCN) national guidelines,
Updated June 2014 Derived and updated by consensus of members of the Providence Thoracic Oncology Program with the aid of evidence-based National Comprehensive Cancer Network (NCCN) national guidelines,
Definitive Treatment of Poor-Risk Patients with Stage I Lung Cancer. A Single Institution Experience
 ORIGINAL ARTICLE Definitive Treatment of Poor-Risk Patients with Stage I Lung Cancer A Single Institution Experience Michael Hsie, MD,* Stefania Morbidini-Gaffney, MD,* Leslie J. Kohman, MD, Elisabeth
ORIGINAL ARTICLE Definitive Treatment of Poor-Risk Patients with Stage I Lung Cancer A Single Institution Experience Michael Hsie, MD,* Stefania Morbidini-Gaffney, MD,* Leslie J. Kohman, MD, Elisabeth
Lung cancer forms in tissues of the lung, usually in the cells lining air passages.
 Scan for mobile link. Lung Cancer Lung cancer usually forms in the tissue cells lining the air passages within the lungs. The two main types are small-cell lung cancer (usually found in cigarette smokers)
Scan for mobile link. Lung Cancer Lung cancer usually forms in the tissue cells lining the air passages within the lungs. The two main types are small-cell lung cancer (usually found in cigarette smokers)
Accelerated hemithoracic radiation followed by extrapleural pneumonectomy for malignant pleural mesothelioma
 Accelerated hemithoracic radiation followed by extrapleural pneumonectomy for malignant pleural mesothelioma Marc de Perrot, Ronald Feld, Natasha B Leighl, Andrew Hope, Thomas K Waddell, Shaf Keshavjee,
Accelerated hemithoracic radiation followed by extrapleural pneumonectomy for malignant pleural mesothelioma Marc de Perrot, Ronald Feld, Natasha B Leighl, Andrew Hope, Thomas K Waddell, Shaf Keshavjee,
GUIDELINES FOR THE MANAGEMENT OF LUNG CANCER
 GUIDELINES FOR THE MANAGEMENT OF LUNG CANCER BY Ali Shamseddine, MD (Coordinator); as04@aub.edu.lb Fady Geara, MD Bassem Shabb, MD Ghassan Jamaleddine, MD CLINICAL PRACTICE GUIDELINES FOR THE TREATMENT
GUIDELINES FOR THE MANAGEMENT OF LUNG CANCER BY Ali Shamseddine, MD (Coordinator); as04@aub.edu.lb Fady Geara, MD Bassem Shabb, MD Ghassan Jamaleddine, MD CLINICAL PRACTICE GUIDELINES FOR THE TREATMENT
Table of Contents. Data Supplement 1: Summary of ASTRO Guideline Statements. Data Supplement 2: Definition of Terms
 Definitive and Adjuvant Radiotherapy in Locally Advanced Non-Small-Cell Lung Cancer: American Society of Clinical Oncology Clinical Practice Guideline Endorsement of the American Society for Radiation
Definitive and Adjuvant Radiotherapy in Locally Advanced Non-Small-Cell Lung Cancer: American Society of Clinical Oncology Clinical Practice Guideline Endorsement of the American Society for Radiation
Management of Postmenopausal Women with T1 ER+ Tumors: Options and Tradeoffs. Case Study. Surgery. Lumpectomy and Radiation
 Management of Postmenopausal Women with T1 ER+ Tumors: Options and Tradeoffs Michael Alvarado, MD Associate Professor of Surgery University of California San Francisco Case Study 59 yo woman with new palpable
Management of Postmenopausal Women with T1 ER+ Tumors: Options and Tradeoffs Michael Alvarado, MD Associate Professor of Surgery University of California San Francisco Case Study 59 yo woman with new palpable
Adjuvant Therapy Non Small Cell Lung Cancer. Sunil Nagpal MD Director, Thoracic Oncology Jan 30, 2015
 Adjuvant Therapy Non Small Cell Lung Cancer Sunil Nagpal MD Director, Thoracic Oncology Jan 30, 2015 No Disclosures Number of studies Studies Per Month 12 10 8 6 4 2 0 1 2 3 4 5 6 7 8 9 10 11 12 1 2 3
Adjuvant Therapy Non Small Cell Lung Cancer Sunil Nagpal MD Director, Thoracic Oncology Jan 30, 2015 No Disclosures Number of studies Studies Per Month 12 10 8 6 4 2 0 1 2 3 4 5 6 7 8 9 10 11 12 1 2 3
Radiation Therapy in the Treatment of
 Lung Cancer Radiation Therapy in the Treatment of Lung Cancer JMAJ 46(12): 537 541, 2003 Kazushige HAYAKAWA Professor and Chairman, Department of Radiology, Kitasato University School of Medicine Abstract:
Lung Cancer Radiation Therapy in the Treatment of Lung Cancer JMAJ 46(12): 537 541, 2003 Kazushige HAYAKAWA Professor and Chairman, Department of Radiology, Kitasato University School of Medicine Abstract:
L Lang-Lazdunski, A Bille, S Marshall, R Lal, D Landau, J Spicer
 Pleurectomy/decortication, hyperthermic pleural lavage with povidone-iodine and systemic chemotherapy in malignant pleural mesothelioma. A 10-year experience. L Lang-Lazdunski, A Bille, S Marshall, R Lal,
Pleurectomy/decortication, hyperthermic pleural lavage with povidone-iodine and systemic chemotherapy in malignant pleural mesothelioma. A 10-year experience. L Lang-Lazdunski, A Bille, S Marshall, R Lal,
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: microwave_tumor_ablation 12/2011 11/2015 11/2016 11/2015 Description of Procedure or Service Microwave ablation
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: microwave_tumor_ablation 12/2011 11/2015 11/2016 11/2015 Description of Procedure or Service Microwave ablation
Mesothelioma. Malignant Pleural Mesothelioma
 Mesothelioma William G. Richards, PhD Brigham and Women s Hospital Malignant Pleural Mesothelioma 2,000-3,000 cases per year (USA) Increasing incidence Asbestos (50-80%, decreasing) 30-40 year latency
Mesothelioma William G. Richards, PhD Brigham and Women s Hospital Malignant Pleural Mesothelioma 2,000-3,000 cases per year (USA) Increasing incidence Asbestos (50-80%, decreasing) 30-40 year latency
Radiotherapy in locally advanced & metastatic NSC lung cancer
 Radiotherapy in locally advanced & metastatic NSC lung cancer Dr Raj Hegde. MD. FRANZCR Consultant Radiation Oncologist. William Buckland Radiotherapy Centre. Latrobe Regional Hospital. Locally advanced
Radiotherapy in locally advanced & metastatic NSC lung cancer Dr Raj Hegde. MD. FRANZCR Consultant Radiation Oncologist. William Buckland Radiotherapy Centre. Latrobe Regional Hospital. Locally advanced
The Need for Accurate Lung Cancer Staging
 The Need for Accurate Lung Cancer Staging Peter Baik, DO Thoracic Surgery Cancer Treatment Centers of America Oklahoma Osteopathic Association 115th Annual Convention Financial Disclosures: None 2 Objectives
The Need for Accurate Lung Cancer Staging Peter Baik, DO Thoracic Surgery Cancer Treatment Centers of America Oklahoma Osteopathic Association 115th Annual Convention Financial Disclosures: None 2 Objectives
Epidemiology, Staging and Treatment of Lung Cancer. Mark A. Socinski, MD
 Epidemiology, Staging and Treatment of Lung Cancer Mark A. Socinski, MD Associate Professor of Medicine Multidisciplinary Thoracic Oncology Program Lineberger Comprehensive Cancer Center University of
Epidemiology, Staging and Treatment of Lung Cancer Mark A. Socinski, MD Associate Professor of Medicine Multidisciplinary Thoracic Oncology Program Lineberger Comprehensive Cancer Center University of
Protons vs. CyberKnife. Protons vs. CyberKnife. Page 1 UC SF. What are. Alexander R. Gottschalk, M.D., Ph.D.
 Protons vs. CyberKnife UC SF Protons vs. CyberKnife UC SF Alexander R. Gottschalk, M.D., Ph.D. Associate Professor and Director of the CyberKnife Radiosurgery Program Department of Radiation Oncology University
Protons vs. CyberKnife UC SF Protons vs. CyberKnife UC SF Alexander R. Gottschalk, M.D., Ph.D. Associate Professor and Director of the CyberKnife Radiosurgery Program Department of Radiation Oncology University
Moving forward, where are we with Clinical Trials?
 Moving forward, where are we with Clinical Trials? Dennis A. Wigle Division of Thoracic Surgery Mayo Clinic AATS/STS General Thoracic Surgery Symposium Sunday, April 27 th 2014 2012 MFMER slide-1 Where
Moving forward, where are we with Clinical Trials? Dennis A. Wigle Division of Thoracic Surgery Mayo Clinic AATS/STS General Thoracic Surgery Symposium Sunday, April 27 th 2014 2012 MFMER slide-1 Where
Radiocirugía y radioterapia estereotáxica corporal
 Radiocirugía y radioterapia estereotáxica corporal Eficacia, seguridad y eficiencia en cáncer de pulmón primario y oligometastásis pulmonares Radiosurgery and stereotactic body radiation therapy. Efficacy,
Radiocirugía y radioterapia estereotáxica corporal Eficacia, seguridad y eficiencia en cáncer de pulmón primario y oligometastásis pulmonares Radiosurgery and stereotactic body radiation therapy. Efficacy,
Objectives. Mylene T. Truong, MD. Malignant Pleural Mesothelioma Background
 Imaging of Pleural Tumors Mylene T. Truong, MD Imaging of Pleural Tumours Mylene T. Truong, M. D. University of Texas M.D. Anderson Cancer Center, Houston, TX Objectives To review tumors involving the
Imaging of Pleural Tumors Mylene T. Truong, MD Imaging of Pleural Tumours Mylene T. Truong, M. D. University of Texas M.D. Anderson Cancer Center, Houston, TX Objectives To review tumors involving the
How TARGIT Intra-operative Radiotherapy can help Older Patients with Breast cancer
 How TARGIT Intra-operative Radiotherapy can help Older Patients with Breast cancer Jeffrey S Tobias, Jayant S Vaidya, Frederik Wenz and Michael Baum, University College Hospital, London, UK - on behalf
How TARGIT Intra-operative Radiotherapy can help Older Patients with Breast cancer Jeffrey S Tobias, Jayant S Vaidya, Frederik Wenz and Michael Baum, University College Hospital, London, UK - on behalf
SMALL CELL LUNG CANCER
 Protocol for Planning and Treatment The process to be followed in the management of: SMALL CELL LUNG CANCER Patient information given at each stage following agreed information pathway 1. DIAGNOSIS New
Protocol for Planning and Treatment The process to be followed in the management of: SMALL CELL LUNG CANCER Patient information given at each stage following agreed information pathway 1. DIAGNOSIS New
Radiotherapy in Plasmacytoma and Myeloma. David Cutter Multiple Myeloma NSSG Annual Meeting 14 th September 2015
 Radiotherapy in Plasmacytoma and Myeloma David Cutter Multiple Myeloma NSSG Annual Meeting 14 th September 2015 Contents Indications for radiotherapy: Palliation in Multiple Myeloma Solitary Bone Plasmacytoma
Radiotherapy in Plasmacytoma and Myeloma David Cutter Multiple Myeloma NSSG Annual Meeting 14 th September 2015 Contents Indications for radiotherapy: Palliation in Multiple Myeloma Solitary Bone Plasmacytoma
Diagnóstico y Terapias Locales
 Diagnóstico y Terapias Locales Dra Marga Majem Hospital de la Santa Creu i Sant Pau AGENDA Revised (8th) Edition of TNM Staging System for Lung Cancer Surgical Approaches in Localized Lung Cancer Radiation
Diagnóstico y Terapias Locales Dra Marga Majem Hospital de la Santa Creu i Sant Pau AGENDA Revised (8th) Edition of TNM Staging System for Lung Cancer Surgical Approaches in Localized Lung Cancer Radiation
Treatment Algorithms for the Management of Lung Cancer in NSW Guide for Clinicians
 Treatment Algorithms for the Management of Lung Cancer in NSW Guide for Clinicians Background The Cancer Institute New South Wales Oncology Group Lung (NSWOG Lung) identified the need for the development
Treatment Algorithms for the Management of Lung Cancer in NSW Guide for Clinicians Background The Cancer Institute New South Wales Oncology Group Lung (NSWOG Lung) identified the need for the development
Lung Cancer Treatment
 Scan for mobile link. Lung Cancer Treatment Lung cancer overview More than one in four of all diagnosed cancers involve the lung, and lung cancer remains the most common cancer-related cause of death among
Scan for mobile link. Lung Cancer Treatment Lung cancer overview More than one in four of all diagnosed cancers involve the lung, and lung cancer remains the most common cancer-related cause of death among
Results of Surgery in a New Lung Institute in South Texas Focused on the Treatment of Lung Cancer
 Results of Surgery in a New Lung Institute in South Texas Focused on the Treatment of Lung Cancer Lung cancer accounts for 13% of all cancer diagnoses and is the leading cause of cancer death in both males
Results of Surgery in a New Lung Institute in South Texas Focused on the Treatment of Lung Cancer Lung cancer accounts for 13% of all cancer diagnoses and is the leading cause of cancer death in both males
Extrapleural Pneumonectomy for Malignant Mesothelioma: Pro. Joon H. Lee 9/17/2012
 Extrapleural Pneumonectomy for Malignant Mesothelioma: Pro Joon H. Lee 9/17/2012 Malignant Pleural Mesothelioma (Epidemiology) Incidence: 7/mil (Japan) to 40/mil (Australia) Attributed secondary to asbestos
Extrapleural Pneumonectomy for Malignant Mesothelioma: Pro Joon H. Lee 9/17/2012 Malignant Pleural Mesothelioma (Epidemiology) Incidence: 7/mil (Japan) to 40/mil (Australia) Attributed secondary to asbestos
FOLLOW UP OF TREATED NON-SMALL CELL LUNG CANCER PATIENTS
 FOLLOW UP OF TREATED NON-SMALL CELL LUNG CANCER PATIENTS THE ART AND THE SCIENCE GIOVANNI BATTISTA MORGAGNI 1682-1771 ITALIAN ANATOMIST FATHER OF PATHOLOGIC ANATOMY 1 ST DESCRIPTION OF LUNG CANCER IN 1761
FOLLOW UP OF TREATED NON-SMALL CELL LUNG CANCER PATIENTS THE ART AND THE SCIENCE GIOVANNI BATTISTA MORGAGNI 1682-1771 ITALIAN ANATOMIST FATHER OF PATHOLOGIC ANATOMY 1 ST DESCRIPTION OF LUNG CANCER IN 1761
Komorbide brystkræftpatienter kan de tåle behandling? Et registerstudie baseret på Danish Breast Cancer Cooperative Group
 Komorbide brystkræftpatienter kan de tåle behandling? Et registerstudie baseret på Danish Breast Cancer Cooperative Group Lotte Holm Land MD, ph.d. Onkologisk Afd. R. OUH Kræft og komorbiditet - alle skal
Komorbide brystkræftpatienter kan de tåle behandling? Et registerstudie baseret på Danish Breast Cancer Cooperative Group Lotte Holm Land MD, ph.d. Onkologisk Afd. R. OUH Kræft og komorbiditet - alle skal
Radioterapia panencefalica. Umberto Ricardi
 Radioterapia panencefalica Umberto Ricardi Background Systemic disease to the brain is unfortunately a quite common event Radiotherapy, especially with the great technical development during the past decades,
Radioterapia panencefalica Umberto Ricardi Background Systemic disease to the brain is unfortunately a quite common event Radiotherapy, especially with the great technical development during the past decades,
Probe: Could you tell me about when?
 PERIODIC ASSESSMENT OF TREATMENT AND VITAL/DISEASE STATUS Periodic Assessment of Cancer Treatment and Disease Status (To be administered to patient at 3 months and reviewed at 6, 9 and 12 months) Instructions:
PERIODIC ASSESSMENT OF TREATMENT AND VITAL/DISEASE STATUS Periodic Assessment of Cancer Treatment and Disease Status (To be administered to patient at 3 months and reviewed at 6, 9 and 12 months) Instructions:
Protein kinase C alpha expression and resistance to neo-adjuvant gemcitabine-containing chemotherapy in non-small cell lung cancer
 Protein kinase C alpha expression and resistance to neo-adjuvant gemcitabine-containing chemotherapy in non-small cell lung cancer Dan Vogl Lay Abstract Early stage non-small cell lung cancer can be cured
Protein kinase C alpha expression and resistance to neo-adjuvant gemcitabine-containing chemotherapy in non-small cell lung cancer Dan Vogl Lay Abstract Early stage non-small cell lung cancer can be cured
Management of Non-Small Cell Lung Cancer Guide for General Practitioners
 Management of n-small Cell Lung Cancer Guide for General Practitioners Clinical Stage I Cancer only in one lobe of lung and
Management of n-small Cell Lung Cancer Guide for General Practitioners Clinical Stage I Cancer only in one lobe of lung and
Particle Therapy for Lung Cancer. Bradford Hoppe MD, MPH Assistant Professor University of Florida bhoppe@floridaproton.org
 Particle Therapy for Lung Cancer Bradford Hoppe MD, MPH Assistant Professor University of Florida bhoppe@floridaproton.org Content Rationale for Particle Therapy in Lung Cancer Proof of Principle Treatment
Particle Therapy for Lung Cancer Bradford Hoppe MD, MPH Assistant Professor University of Florida bhoppe@floridaproton.org Content Rationale for Particle Therapy in Lung Cancer Proof of Principle Treatment
Clinical Trials and Radiation Treatment. Gerard Morton Odette Cancer Centre Sunnybrook Research Institute University of Toronto
 Clinical Trials and Radiation Treatment Gerard Morton Odette Cancer Centre Sunnybrook Research Institute University of Toronto What I will cover.. A little about radiation treatment The clinical trials
Clinical Trials and Radiation Treatment Gerard Morton Odette Cancer Centre Sunnybrook Research Institute University of Toronto What I will cover.. A little about radiation treatment The clinical trials
Principles of Radiation Therapy A Bapsi Chakravarthy, MD Associate e P rofessor Professor Radiation Oncology
 Principles of Radiation Therapy A Bapsi Chakravarthy, MD Associate Professor Radiation Oncology Disclosure Information I have no financial relationships to disclose relevant to the conten of this presentation.
Principles of Radiation Therapy A Bapsi Chakravarthy, MD Associate Professor Radiation Oncology Disclosure Information I have no financial relationships to disclose relevant to the conten of this presentation.
Prostate Cancer Treatment: What s Best for You?
 Prostate Cancer Treatment: What s Best for You? Prostate Cancer: Radiation Therapy Approaches I. Choices There is really a variety of options in prostate cancer management overall and in radiation therapy.
Prostate Cancer Treatment: What s Best for You? Prostate Cancer: Radiation Therapy Approaches I. Choices There is really a variety of options in prostate cancer management overall and in radiation therapy.
The lungs What is lung cancer? How common is it? Risks & symptoms Diagnosis & treatment options
 Why We re Here The lungs What is lung cancer? How common is it? Risks & symptoms Diagnosis & treatment options What Are Lungs? What Do They Do? 1 Located in the chest Allow you to breathe Provide oxygen
Why We re Here The lungs What is lung cancer? How common is it? Risks & symptoms Diagnosis & treatment options What Are Lungs? What Do They Do? 1 Located in the chest Allow you to breathe Provide oxygen
Targeted Therapy What the Surgeon Needs to Know
 Targeted Therapy What the Surgeon Needs to Know AATS Focus in Thoracic Surgery 2014 David R. Jones, M.D. Professor & Chief, Thoracic Surgery Memorial Sloan Kettering Cancer Center I have no disclosures
Targeted Therapy What the Surgeon Needs to Know AATS Focus in Thoracic Surgery 2014 David R. Jones, M.D. Professor & Chief, Thoracic Surgery Memorial Sloan Kettering Cancer Center I have no disclosures
Carcinoma of the Cervix. Kathleen M. Schmeler, MD Associate Professor Department of Gynecologic Oncology
 Carcinoma of the Cervix Kathleen M. Schmeler, MD Associate Professor Department of Gynecologic Oncology Cervical Cancer Treatment Treatment Microinvasive (Stage IA1): Simple (extrafascial) hysterectomy/cone
Carcinoma of the Cervix Kathleen M. Schmeler, MD Associate Professor Department of Gynecologic Oncology Cervical Cancer Treatment Treatment Microinvasive (Stage IA1): Simple (extrafascial) hysterectomy/cone
CANCER PULMON: ESTADIOS INICIALES POSTMUNDIAL PULMON DENVER 2015. 8-10-2015.Manuel Cobo Dols S. Oncología Médica HU Málaga Regional y VV
 CANCER PULMON: ESTADIOS INICIALES POSTMUNDIAL PULMON DENVER 2015 8-10-2015.Manuel Cobo Dols S. Oncología Médica HU Málaga Regional y VV Meta-analisis LACE: adyuvancia vs no adyuvancia Pignon JP, et al.
CANCER PULMON: ESTADIOS INICIALES POSTMUNDIAL PULMON DENVER 2015 8-10-2015.Manuel Cobo Dols S. Oncología Médica HU Málaga Regional y VV Meta-analisis LACE: adyuvancia vs no adyuvancia Pignon JP, et al.
A Decade of Advances in Treatment of Early- Stage Lung Cancer
 A Decade of Advances in Treatment of Early- Stage Lung Cancer Luca Paoletti, MD a, Nicholas J. Pastis, MD a, Chadrick E. Denlinger, MD b, Gerard A. Silvestri, MD, MS a, * KEYWORDS Lung cancer Treatment
A Decade of Advances in Treatment of Early- Stage Lung Cancer Luca Paoletti, MD a, Nicholas J. Pastis, MD a, Chadrick E. Denlinger, MD b, Gerard A. Silvestri, MD, MS a, * KEYWORDS Lung cancer Treatment
Prostatectomy, pelvic lymphadenect. Med age 63 years Mean followup 53 months No other cancer related therapy before recurrence. Negative.
 Adjuvante und Salvage Radiotherapie Ludwig Plasswilm Klinik für Radio-Onkologie, KSSG CANCER CONTROL WITH RADICAL PROSTATECTOMY ALONE IN 1,000 CONSECUTIVE PATIENTS 1983 1998 Clinical stage T1 and T2 Mean
Adjuvante und Salvage Radiotherapie Ludwig Plasswilm Klinik für Radio-Onkologie, KSSG CANCER CONTROL WITH RADICAL PROSTATECTOMY ALONE IN 1,000 CONSECUTIVE PATIENTS 1983 1998 Clinical stage T1 and T2 Mean
Current Status and Perspectives of Radiation Therapy for Breast Cancer
 Breast Cancer Current Status and Perspectives of Radiation Therapy for Breast Cancer JMAJ 45(10): 434 439, 2002 Masahiro HIRAOKA, Masaki KOKUBO, Chikako YAMAMOTO and Michihide MITSUMORI Department of Therapeutic
Breast Cancer Current Status and Perspectives of Radiation Therapy for Breast Cancer JMAJ 45(10): 434 439, 2002 Masahiro HIRAOKA, Masaki KOKUBO, Chikako YAMAMOTO and Michihide MITSUMORI Department of Therapeutic
Radiotherapy for Non-Small Cell Lung Cancer. Standard Treatment Options Radiotherapy Planning
 Radiotherapy for Non-Small Cell Lung Cancer I II Standard Treatment Options Radiotherapy Planning TNM Staging System Disease Staging - Management is based on disease stage - Stage I-II: early stage - Stage
Radiotherapy for Non-Small Cell Lung Cancer I II Standard Treatment Options Radiotherapy Planning TNM Staging System Disease Staging - Management is based on disease stage - Stage I-II: early stage - Stage
Innovative RT SBRT. The variables with REQ in superscript are required.
 The variables with REQ in superscript are required. The variables with a are single-select variables; only one answer can be selected. The variables with a are multi-select variables; multiple answers
The variables with REQ in superscript are required. The variables with a are single-select variables; only one answer can be selected. The variables with a are multi-select variables; multiple answers
ROLE OF RADIATION THERAPY FOR RESECTABLE LUNG CANCER
 AFA 08958 From Bench to Bedside From KK DT1 10/27/2015 12:04 PM 01 ROLE OF RADIATION THERAPY FOR RESECTABLE LUNG CANCER Hak Choy, MD University of Texas Southwestern Medical Center Dallas, Texas, USA Orchestrating
AFA 08958 From Bench to Bedside From KK DT1 10/27/2015 12:04 PM 01 ROLE OF RADIATION THERAPY FOR RESECTABLE LUNG CANCER Hak Choy, MD University of Texas Southwestern Medical Center Dallas, Texas, USA Orchestrating
Breast Cancer Accelerated Partial Breast Irradiation Bruce G. Haffty, MD Professor and Chairman Dept Radiation Oncology UMDNJ-RWJMS Cancer Institute
 Breast Cancer Accelerated Partial Breast Irradiation Bruce G. Haffty, MD Professor and Chairman Dept Radiation Oncology UMDNJ-RWJMS Cancer Institute of New Jersey Rationale for Partial Breast Radiation
Breast Cancer Accelerated Partial Breast Irradiation Bruce G. Haffty, MD Professor and Chairman Dept Radiation Oncology UMDNJ-RWJMS Cancer Institute of New Jersey Rationale for Partial Breast Radiation
SBRT (Elekta), 45 Gy in fractions of 3 Gy 3x/week for 5 weeks (N=22) vs.
, 45 Gy in fractions of 3 Gy 3x/week for 5 weeks (N=22) vs.") Uitgangsvraag 6: Wat is de plaats van stereotactische radiotherapiebehandeling (SBRT) bij HCC patiënten? Primaire studies I Study ID II Method III Patient characteristics IV Intervention(s) V Results primary
Uitgangsvraag 6: Wat is de plaats van stereotactische radiotherapiebehandeling (SBRT) bij HCC patiënten? Primaire studies I Study ID II Method III Patient characteristics IV Intervention(s) V Results primary
Post-recurrence survival in completely resected stage I non-small cell lung cancer with local recurrence
 Post- survival in completely resected stage I non-small cell lung cancer with local J-J Hung, 1,2,3 W-H Hsu, 3 C-C Hsieh, 3 B-S Huang, 3 M-H Huang, 3 J-S Liu, 2 Y-C Wu 3 See Editorial, p 185 c A supplementary
Post- survival in completely resected stage I non-small cell lung cancer with local J-J Hung, 1,2,3 W-H Hsu, 3 C-C Hsieh, 3 B-S Huang, 3 M-H Huang, 3 J-S Liu, 2 Y-C Wu 3 See Editorial, p 185 c A supplementary
B. Dingle MD, FRCPC, Brian Yaremko MD,FRCPC, R. Ash, MD, FRCPC, P. Truong, MD, FRCPC
 Lung Cancer B. Dingle MD, FRCPC, Brian Yaremko MD,FRCPC, R. Ash, MD, FRCPC, P. Truong, MD, FRCPC EPIDEMIOLOGY The estimated incidence of lung cancer in Canada for 2007 is 23,300 with 12,400 occurring in
Lung Cancer B. Dingle MD, FRCPC, Brian Yaremko MD,FRCPC, R. Ash, MD, FRCPC, P. Truong, MD, FRCPC EPIDEMIOLOGY The estimated incidence of lung cancer in Canada for 2007 is 23,300 with 12,400 occurring in
Goals and Objectives: Breast Cancer Service Department of Radiation Oncology
 Goals and Objectives: Breast Cancer Service Department of Radiation Oncology The breast cancer service provides training in the diagnosis, management, treatment, and follow-up of breast malignancies, including
Goals and Objectives: Breast Cancer Service Department of Radiation Oncology The breast cancer service provides training in the diagnosis, management, treatment, and follow-up of breast malignancies, including
بسم هللا الرحمن الرحيم
 بسم هللا الرحمن الرحيم Updates in Mesothelioma By Samieh Amer, MD Professor of Cardiothoracic Surgery Faculty of Medicine, Cairo University History Wagner and his colleagues (1960) 33 cases of mesothelioma
بسم هللا الرحمن الرحيم Updates in Mesothelioma By Samieh Amer, MD Professor of Cardiothoracic Surgery Faculty of Medicine, Cairo University History Wagner and his colleagues (1960) 33 cases of mesothelioma
Outcomes of Stereotactic Ablative Radiotherapy in Patients With Potentially Operable Stage I Non-Small Cell Lung Cancer
 CME International Journal of Radiation Oncology biology physics www.redjournal.org Clinical Investigation: Thoracic Cancer Outcomes of Stereotactic Ablative Radiotherapy in Patients With Potentially Operable
CME International Journal of Radiation Oncology biology physics www.redjournal.org Clinical Investigation: Thoracic Cancer Outcomes of Stereotactic Ablative Radiotherapy in Patients With Potentially Operable
Small Cell Lung Cancer
 Small Cell Lung Cancer Types of Lung Cancer Non-small cell carcinoma (NSCC) (87%) Adenocarcinoma (38%) Squamous cell (20%) Large cell (5%) Small cell carcinoma (13%) Small cell lung cancer is virtually
Small Cell Lung Cancer Types of Lung Cancer Non-small cell carcinoma (NSCC) (87%) Adenocarcinoma (38%) Squamous cell (20%) Large cell (5%) Small cell carcinoma (13%) Small cell lung cancer is virtually
Thomas A. Kollmorgen, M.D. Oregon Urology Institute
 Thomas A. Kollmorgen, M.D. Oregon Urology Institute None 240,000 new diagnosis per year, and an estimated 28,100 deaths (2012) 2 nd leading cause of death from cancer in U.S.A. Approximately 1 in 6 men
Thomas A. Kollmorgen, M.D. Oregon Urology Institute None 240,000 new diagnosis per year, and an estimated 28,100 deaths (2012) 2 nd leading cause of death from cancer in U.S.A. Approximately 1 in 6 men
Finding an Appropriate Treatment
 Focus on CME at the University of Toronto Early Detected Lung Cancer: Finding an Appropriate Treatment Thanks to modern technology, subcentimeter tumors are now being identified. As with other malignant
Focus on CME at the University of Toronto Early Detected Lung Cancer: Finding an Appropriate Treatment Thanks to modern technology, subcentimeter tumors are now being identified. As with other malignant
Current Status and Future Direction of Proton Beam Therapy
 Current Status and Future Direction of Proton Beam Therapy National Cancer Center Hospital East Division of Radiation Oncology and Particle Therapy Tetsuo Akimoto Comparison of status of particle therapy
Current Status and Future Direction of Proton Beam Therapy National Cancer Center Hospital East Division of Radiation Oncology and Particle Therapy Tetsuo Akimoto Comparison of status of particle therapy
How To Compare The Effects Of A Hysterectomy And A Hysterectomy
 A RANDOMIZED TRIAL COMPARING RADICAL HYSTERECTOMY AND PELVIC NODE DISSECTION VS SIMPLE HYSTERECTOMY AND PELVIC NODE DISSECTION IN PATIENTS WITH LOW RISK EARLY STAGE CERVICAL CANCER A Gynecologic Cancer
A RANDOMIZED TRIAL COMPARING RADICAL HYSTERECTOMY AND PELVIC NODE DISSECTION VS SIMPLE HYSTERECTOMY AND PELVIC NODE DISSECTION IN PATIENTS WITH LOW RISK EARLY STAGE CERVICAL CANCER A Gynecologic Cancer
The National Clinical Lung Cancer Audit (LUCADA)
") The National Clinical Lung Cancer Audit (LUCADA) DATA MANUAL Title: Version: 3.1.5 Date: September 2013 LUCADA Lung Cancer Audit VERSION HISTORY Version Date Issued Brief Summary of Change Owner s Name
The National Clinical Lung Cancer Audit (LUCADA) DATA MANUAL Title: Version: 3.1.5 Date: September 2013 LUCADA Lung Cancer Audit VERSION HISTORY Version Date Issued Brief Summary of Change Owner s Name
Non-Small Cell Lung Cancer Treatment Comparison to NCCN Guidelines
 Non-Small Cell Lung Cancer Treatment Comparison to NCCN Guidelines April 2008 (presented at 6/12/08 cancer committee meeting) By Shelly Smits, RHIT, CCS, CTR Conclusions by Dr. Ian Thompson, MD Dr. James
Non-Small Cell Lung Cancer Treatment Comparison to NCCN Guidelines April 2008 (presented at 6/12/08 cancer committee meeting) By Shelly Smits, RHIT, CCS, CTR Conclusions by Dr. Ian Thompson, MD Dr. James
SUNY DOWNSTATE MEDICAL CENTER SURGERY GRAND ROUNDS February 28, 2013 VERENA LIU, MD ROSEANNA LEE, MD
 SUNY DOWNSTATE MEDICAL CENTER SURGERY GRAND ROUNDS February 28, 2013 VERENA LIU, MD ROSEANNA LEE, MD Case Presentation 35 year old male referred from PMD with an asymptomatic palpable right neck mass PMH/PSH:
SUNY DOWNSTATE MEDICAL CENTER SURGERY GRAND ROUNDS February 28, 2013 VERENA LIU, MD ROSEANNA LEE, MD Case Presentation 35 year old male referred from PMD with an asymptomatic palpable right neck mass PMH/PSH:
PET/CT in Lung Cancer
 PET/CT in Lung Cancer Rodolfo Núñez Miller, M.D. Nuclear Medicine and Diagnostic Imaging Section Division of Human Health International Atomic Energy Agency Vienna, Austria GLOBOCAN 2012 #1 #3 FDG-PET/CT
PET/CT in Lung Cancer Rodolfo Núñez Miller, M.D. Nuclear Medicine and Diagnostic Imaging Section Division of Human Health International Atomic Energy Agency Vienna, Austria GLOBOCAN 2012 #1 #3 FDG-PET/CT
Radiation therapy involves using many terms you may have never heard before. Below is a list of words you could hear during your treatment.
 Dictionary Radiation therapy involves using many terms you may have never heard before. Below is a list of words you could hear during your treatment. Applicator A device used to hold a radioactive source
Dictionary Radiation therapy involves using many terms you may have never heard before. Below is a list of words you could hear during your treatment. Applicator A device used to hold a radioactive source
Jedi Wisdom for Lung Cancer Radiotherapy: May the Force Be With You
 Jedi Wisdom for Lung Cancer Radiotherapy: May the Force Be With You SHAUN LOEWEN MD PhD FRCPC Assistant Professor, University of Manitoba Radiation Oncologist, CancerCare Manitoba Disclosure Relationship
Jedi Wisdom for Lung Cancer Radiotherapy: May the Force Be With You SHAUN LOEWEN MD PhD FRCPC Assistant Professor, University of Manitoba Radiation Oncologist, CancerCare Manitoba Disclosure Relationship
Lung cancer case study
 Change Presentation title and date in Footer dd.mm.yyyy Lung cancer case study Dr Jaishree Bhosle Consultant Medical Oncologist Change Presentation title and date in Footer dd.mm.yyyy 1 2 Part One Initial
Change Presentation title and date in Footer dd.mm.yyyy Lung cancer case study Dr Jaishree Bhosle Consultant Medical Oncologist Change Presentation title and date in Footer dd.mm.yyyy 1 2 Part One Initial
Overview of Gynaecologic Cancer
 Overview of Gynaecologic Cancer Stuart Salfinger Gynaecologic Oncologist St John of God Hospital King Edward Memorial Hospital Cervical Cancer Cervical Cancer Risk HPV Smoking?OCP Cervical Cancer Symptoms
Overview of Gynaecologic Cancer Stuart Salfinger Gynaecologic Oncologist St John of God Hospital King Edward Memorial Hospital Cervical Cancer Cervical Cancer Risk HPV Smoking?OCP Cervical Cancer Symptoms
Malignant Mesothelioma State of the Art
 Malignant Mesothelioma State of the Art Paul Baas The Netherlands Cancer Institute August 12, 2011, Carlsbad, CA Summary Diagnosis; epithelial type subdivided Pleiomorphic vs other Staging: IASLC-IMIG
Malignant Mesothelioma State of the Art Paul Baas The Netherlands Cancer Institute August 12, 2011, Carlsbad, CA Summary Diagnosis; epithelial type subdivided Pleiomorphic vs other Staging: IASLC-IMIG
The evolution of rectal cancer therapy. Objectives
 The evolution of rectal cancer therapy Hagen Kennecke MD MHA FRCPC Western Canada Consensus Conference September 5, 2014 Objectives Identify standard therapy: stage II/III rectal cancer Update recent adjuvant
The evolution of rectal cancer therapy Hagen Kennecke MD MHA FRCPC Western Canada Consensus Conference September 5, 2014 Objectives Identify standard therapy: stage II/III rectal cancer Update recent adjuvant
Resection of Lung Cancer Invading the Mediastinum
 Resection of Lung Cancer Invading the Mediastinum Philippe G. Dartevelle MARIE-LANNELONGUE HOSPITAL GUSTAVE ROUSSY INSTITUTE INSTITUTE OF THORACIC ONCOLOGY PARIS SUD UNIVERSITY Mediastinal Invasion Superior
Resection of Lung Cancer Invading the Mediastinum Philippe G. Dartevelle MARIE-LANNELONGUE HOSPITAL GUSTAVE ROUSSY INSTITUTE INSTITUTE OF THORACIC ONCOLOGY PARIS SUD UNIVERSITY Mediastinal Invasion Superior
Implementation Date: April 2015 Clinical Operations
 National Imaging Associates, Inc. Clinical guideline PROSTATE CANCER Original Date: March 2011 Page 1 of 5 Radiation Oncology Last Review Date: March 2015 Guideline Number: NIA_CG_124 Last Revised Date:
National Imaging Associates, Inc. Clinical guideline PROSTATE CANCER Original Date: March 2011 Page 1 of 5 Radiation Oncology Last Review Date: March 2015 Guideline Number: NIA_CG_124 Last Revised Date:
Corporate Medical Policy Brachytherapy Treatment of Breast Cancer
 Corporate Medical Policy Brachytherapy Treatment of Breast Cancer File Name: Origination: Last CAP Review: Next CAP Review: Last Review: brachytherapy_treatment_of_breast_cancer 7/1996 5/2015 5/2016 5/2015
Corporate Medical Policy Brachytherapy Treatment of Breast Cancer File Name: Origination: Last CAP Review: Next CAP Review: Last Review: brachytherapy_treatment_of_breast_cancer 7/1996 5/2015 5/2016 5/2015
7. Prostate cancer in PSA relapse
 7. Prostate cancer in PSA relapse A patient with prostate cancer in PSA relapse is one who, having received a primary treatment with intent to cure, has a raised PSA (prostate-specific antigen) level defined
7. Prostate cancer in PSA relapse A patient with prostate cancer in PSA relapse is one who, having received a primary treatment with intent to cure, has a raised PSA (prostate-specific antigen) level defined
Corso Integrato di Clinica Medica ONCOLOGIA MEDICA AA 2010-2011 LUNG CANCER. VIII. THERAPY. V. SMALL CELL LUNG CANCER Prof.
 Corso Integrato di Clinica Medica ONCOLOGIA MEDICA AA 2010-2011 LUNG CANCER. VIII. THERAPY. V. SMALL CELL LUNG CANCER Prof. Alberto Riccardi SMALL CELL LUNG CARCINOMA Summary of treatment approach * limited
Corso Integrato di Clinica Medica ONCOLOGIA MEDICA AA 2010-2011 LUNG CANCER. VIII. THERAPY. V. SMALL CELL LUNG CANCER Prof. Alberto Riccardi SMALL CELL LUNG CARCINOMA Summary of treatment approach * limited
Esperienza di stereotassia polmonare al Campus Bio-Medico: tecnica e risultati Rolando M. D Angelillo
 Esperienza di stereotassia polmonare al Campus Bio-Medico: tecnica e risultati Rolando M. D Angelillo Università Campus Bio-Medico di Roma - Via Álvaro del Portillo, 21-00128 Roma Italia BED 10 > 100 Gy
Esperienza di stereotassia polmonare al Campus Bio-Medico: tecnica e risultati Rolando M. D Angelillo Università Campus Bio-Medico di Roma - Via Álvaro del Portillo, 21-00128 Roma Italia BED 10 > 100 Gy
Stomach (Gastric) Cancer. Prof. M K Mahajan ACDT & RC Bathinda
 Cancer. Prof. M K Mahajan ACDT & RC Bathinda") Stomach (Gastric) Cancer Prof. M K Mahajan ACDT & RC Bathinda Gastric Cancer Role of Radiation Layers of the Stomach Mucosa Submucosa Muscularis Serosa Stomach and Regional Lymph Nodes Stomach and Regional
Stomach (Gastric) Cancer Prof. M K Mahajan ACDT & RC Bathinda Gastric Cancer Role of Radiation Layers of the Stomach Mucosa Submucosa Muscularis Serosa Stomach and Regional Lymph Nodes Stomach and Regional
A new score predicting the survival of patients with spinal cord compression from myeloma
 A new score predicting the survival of patients with spinal cord compression from myeloma (1) Sarah Douglas, Department of Radiation Oncology, University of Lubeck, Germany; sarah_douglas@gmx.de (2) Steven
A new score predicting the survival of patients with spinal cord compression from myeloma (1) Sarah Douglas, Department of Radiation Oncology, University of Lubeck, Germany; sarah_douglas@gmx.de (2) Steven
TITLE: Comparison of the dosimetric planning of partial breast irradiation with and without the aid of 3D virtual reality simulation (VRS) software.
 software.") SAMPLE CLINICAL RESEARCH APPLICATION ABSTRACT: TITLE: Comparison of the dosimetric planning of partial breast irradiation with and without the aid of 3D virtual reality simulation (VRS) software. Hypothesis:
SAMPLE CLINICAL RESEARCH APPLICATION ABSTRACT: TITLE: Comparison of the dosimetric planning of partial breast irradiation with and without the aid of 3D virtual reality simulation (VRS) software. Hypothesis:
Brigham and Women s Hospital, Boston, MA, USA; 2 Verastem, Inc., Boston, MA, USA
 Determination of Biomarker Response in a Phase II Window of Opportunity Study of Defactinib (VS 6063), a Focal Adhesion Kinase (FAK) Inhibitor, in Patients with Resectable Malignant Pleural Mesothelioma
Determination of Biomarker Response in a Phase II Window of Opportunity Study of Defactinib (VS 6063), a Focal Adhesion Kinase (FAK) Inhibitor, in Patients with Resectable Malignant Pleural Mesothelioma
Veterinary Oncology: The Lumps We Hate To Treat
 Veterinary Oncology: The Lumps We Hate To Treat Michelle Turek, DVM, DACVIM (Oncology), DACVR (Radiation Oncology) College of Veterinary Medicine University of Georgia Athens, GA Veterinary Oncology Veterinary
Veterinary Oncology: The Lumps We Hate To Treat Michelle Turek, DVM, DACVIM (Oncology), DACVR (Radiation Oncology) College of Veterinary Medicine University of Georgia Athens, GA Veterinary Oncology Veterinary
Kidney Cancer OVERVIEW
 Kidney Cancer OVERVIEW Kidney cancer is the third most common genitourinary cancer in adults. There are approximately 54,000 new cancer cases each year in the United States, and the incidence of kidney
Kidney Cancer OVERVIEW Kidney cancer is the third most common genitourinary cancer in adults. There are approximately 54,000 new cancer cases each year in the United States, and the incidence of kidney
Image. 3.11.3 SW Review the anatomy of the EAC and how this plays a role in the spread of tumors.
 Neoplasms of the Ear and Lateral Skull Base Image 3.11.1 SW What are the three most common neoplasms of the auricle? 3.11.2 SW What are the four most common neoplasms of the external auditory canal (EAC)
Neoplasms of the Ear and Lateral Skull Base Image 3.11.1 SW What are the three most common neoplasms of the auricle? 3.11.2 SW What are the four most common neoplasms of the external auditory canal (EAC)
FAQ About Prostate Cancer Treatment and SpaceOAR System
 FAQ About Prostate Cancer Treatment and SpaceOAR System P. 4 Prostate Cancer Background SpaceOAR Frequently Asked Questions (FAQ) 1. What is prostate cancer? The vast majority of prostate cancers develop
FAQ About Prostate Cancer Treatment and SpaceOAR System P. 4 Prostate Cancer Background SpaceOAR Frequently Asked Questions (FAQ) 1. What is prostate cancer? The vast majority of prostate cancers develop
Mesothelioma. 1. Introduction. 1.1 General Information and Aetiology
 Mesothelioma 1. Introduction 1.1 General Information and Aetiology Mesotheliomas are tumours that arise from the mesothelial cells of the pleura, peritoneum, pericardium or tunica vaginalis [1]. Most are
Mesothelioma 1. Introduction 1.1 General Information and Aetiology Mesotheliomas are tumours that arise from the mesothelial cells of the pleura, peritoneum, pericardium or tunica vaginalis [1]. Most are
Robert Bristow MD PhD FRCPC
 Robert Bristow MD PhD FRCPC Clinician-Scientist and Professor, Radiation Oncology and Medical Biophysics, University of Toronto and Ontario Cancer Institute/ (UHN) Head, PMH-CFCRI Prostate Cancer Research
Robert Bristow MD PhD FRCPC Clinician-Scientist and Professor, Radiation Oncology and Medical Biophysics, University of Toronto and Ontario Cancer Institute/ (UHN) Head, PMH-CFCRI Prostate Cancer Research
Tricia Cox on 7/18/2012 at Oncology Center. Sarah Randolf. Female
 SAMPLE This Survivorship Care Plan will facilitate cancer care following active treatment. It may include important contact information, a treatment summary, recommendations for follow-up care testing,
SAMPLE This Survivorship Care Plan will facilitate cancer care following active treatment. It may include important contact information, a treatment summary, recommendations for follow-up care testing,
Lung Cancer: An Overview
 VOL. I Issue 2 2010 Lung Cancer: An Overview By Matthew F. Koscielski, M.D. Lung cancer is the most common cause of cancer mortality worldwide. In the United States there are about 220,000 new cases of
VOL. I Issue 2 2010 Lung Cancer: An Overview By Matthew F. Koscielski, M.D. Lung cancer is the most common cause of cancer mortality worldwide. In the United States there are about 220,000 new cases of
Columbia University Mesothelioma Applied Research Foundation - 2009 - www.curemeso.org. Mesothelioma Center www.mesocenter.org
 Columbia University Mesothelioma Center www.mesocenter.org Multimodal clinical trials, treatment (surgery, radiation, chemotherapy) Peritoneal mesothelioma program Immunotherapy translational, experimental
Columbia University Mesothelioma Center www.mesocenter.org Multimodal clinical trials, treatment (surgery, radiation, chemotherapy) Peritoneal mesothelioma program Immunotherapy translational, experimental
INTERNATIONAL ASSOCIATION FOR THE STUDY OF LUNG CANCER Prospective Mesothelioma Staging Project
 INTERNATIONAL ASSOCIATION FOR THE STUDY OF LUNG CANCER Prospective Mesothelioma Staging Project Data Forms and Fields in CRAB Electronic Data Capture System - Reduced Set - Pivotal data elements for developing
INTERNATIONAL ASSOCIATION FOR THE STUDY OF LUNG CANCER Prospective Mesothelioma Staging Project Data Forms and Fields in CRAB Electronic Data Capture System - Reduced Set - Pivotal data elements for developing
Management of stage III A-B of NSCLC. Hamed ALHusaini Medical Oncologist
 Management of stage III A-B of NSCLC Hamed ALHusaini Medical Oncologist Global incidence, CA cancer J Clin 2011;61:69-90 Stage III NSCLC Includes heterogeneous group of patients with differences in the
Management of stage III A-B of NSCLC Hamed ALHusaini Medical Oncologist Global incidence, CA cancer J Clin 2011;61:69-90 Stage III NSCLC Includes heterogeneous group of patients with differences in the
Guidelines for the treatment of breast cancer with radiotherapy
 London Cancer Guidelines for the treatment of breast cancer with radiotherapy March 2013 Review March 2014 Version 1.0 Contents 1. Introduction... 3 2. Indications and dosing schedules... 3 2.1. Ductal
London Cancer Guidelines for the treatment of breast cancer with radiotherapy March 2013 Review March 2014 Version 1.0 Contents 1. Introduction... 3 2. Indications and dosing schedules... 3 2.1. Ductal
PATIENT INFORMATION ABOUT ADJUVANT THERAPY AFTER THE WHIPPLE OPERATION FOR ADENOCARCINOMA ( CANCER ) OF THE PANCREAS AND RELATED SITES.
 OF THE PANCREAS AND RELATED SITES.") PATIENT INFORMATION ABOUT ADJUVANT THERAPY AFTER THE WHIPPLE OPERATION FOR ADENOCARCINOMA ( CANCER ) OF THE PANCREAS AND RELATED SITES. Radiation Oncology Sidney Kimmel Cancer Center at Johns Hopkins Last
PATIENT INFORMATION ABOUT ADJUVANT THERAPY AFTER THE WHIPPLE OPERATION FOR ADENOCARCINOMA ( CANCER ) OF THE PANCREAS AND RELATED SITES. Radiation Oncology Sidney Kimmel Cancer Center at Johns Hopkins Last
Re irradiation Using HDR Interstitial Brachytherapy for Locally Recurrent. Disclosure
 Re irradiation Using HDR Interstitial Brachytherapy for Locally Recurrent Cervical lcancer Yasuo Yoshioka, MD Department of Radiation Oncology Osaka University Graduate School of Medicine Osaka, Japan
Re irradiation Using HDR Interstitial Brachytherapy for Locally Recurrent Cervical lcancer Yasuo Yoshioka, MD Department of Radiation Oncology Osaka University Graduate School of Medicine Osaka, Japan
Non-Small Cell Lung Cancer Therapies
 Non-Small Cell Lung Cancer Therapies Guest Expert: Roy, MD, PhD Assistant Professor of Therapeutic Radiology Scott, MD Assistant Professor of Medical Oncology www.wnpr.org www.yalecancercenter.org Welcome
Non-Small Cell Lung Cancer Therapies Guest Expert: Roy, MD, PhD Assistant Professor of Therapeutic Radiology Scott, MD Assistant Professor of Medical Oncology www.wnpr.org www.yalecancercenter.org Welcome
Gamma Knife and Axesse Radiosurgery
 Gamma Knife and Axesse Radiosurgery John C Flickinger MD Departments of Radiation Oncology & Neurological Surgery University of Pittsburgh School of Medicine Pittsburgh, Pennsylvania Origin of Radiosurgery
Gamma Knife and Axesse Radiosurgery John C Flickinger MD Departments of Radiation Oncology & Neurological Surgery University of Pittsburgh School of Medicine Pittsburgh, Pennsylvania Origin of Radiosurgery
Principal Investigator: Valerie W. Rusch, MD, FACS, Chief, Thoracic Surgery Memorial Sloan-Kettering Cancer Center
 Protocol 1101-1088 Phase I study of intra-pleural administration of GL-ONC1 in patients with malignant pleural effusion: primary, metastases and mesothelioma Principal Investigator: Valerie W. Rusch, MD,
Protocol 1101-1088 Phase I study of intra-pleural administration of GL-ONC1 in patients with malignant pleural effusion: primary, metastases and mesothelioma Principal Investigator: Valerie W. Rusch, MD,
Stage IIIB disease includes patients with T4 tumors,
 Guidelines on Treatment of Stage IIIB Non-small Cell Lung Cancer* James R. Jett, MD, FCCP; Walter J. Scott, MD, FCCP; M. Patricia Rivera MD, FCCP; and William T. Sause, MD, FACR Stage IIIB includes patients
Guidelines on Treatment of Stage IIIB Non-small Cell Lung Cancer* James R. Jett, MD, FCCP; Walter J. Scott, MD, FCCP; M. Patricia Rivera MD, FCCP; and William T. Sause, MD, FACR Stage IIIB includes patients
WA Asbestos Review Program
 WA Asbestos Review Program Dr Fraser Brims Consultant Respiratory Physician, SCGH, Head of Occupational and Respiratory Health Unit, LIWA Asbestos awareness week seminar, 2014 Introduction Asbestos and
WA Asbestos Review Program Dr Fraser Brims Consultant Respiratory Physician, SCGH, Head of Occupational and Respiratory Health Unit, LIWA Asbestos awareness week seminar, 2014 Introduction Asbestos and