Acute Low Back Pain Workshop
|
|
|
- Charity Hodges
- 8 years ago
- Views:
Transcription
1 Acute Low Back Pain Workshop Charlie Ng MBChB FAFMM Musculoskeletal Physician GPCME 20 June 2013

2 Key points Acute LBP is common; most patients recover fully in 3 months Serious causes are rare and can be excluded with careful history & examination Imaging is not required in absence of red flags An exact diagnosis is often not possible, nor needed for management Beliefs, attitudes and fear about pain contribute to chronicity & should be addressed Management includes reassurance, education & staying active Adequate analgesia

3 An algorithm for acute LBP

4 Is it truly low back pain? Using a pain map

5 Low back pain terminology Lumbar spinal pain T12 spinous process Lumbar erector spinae muscles. S1 spinous process

6 L4
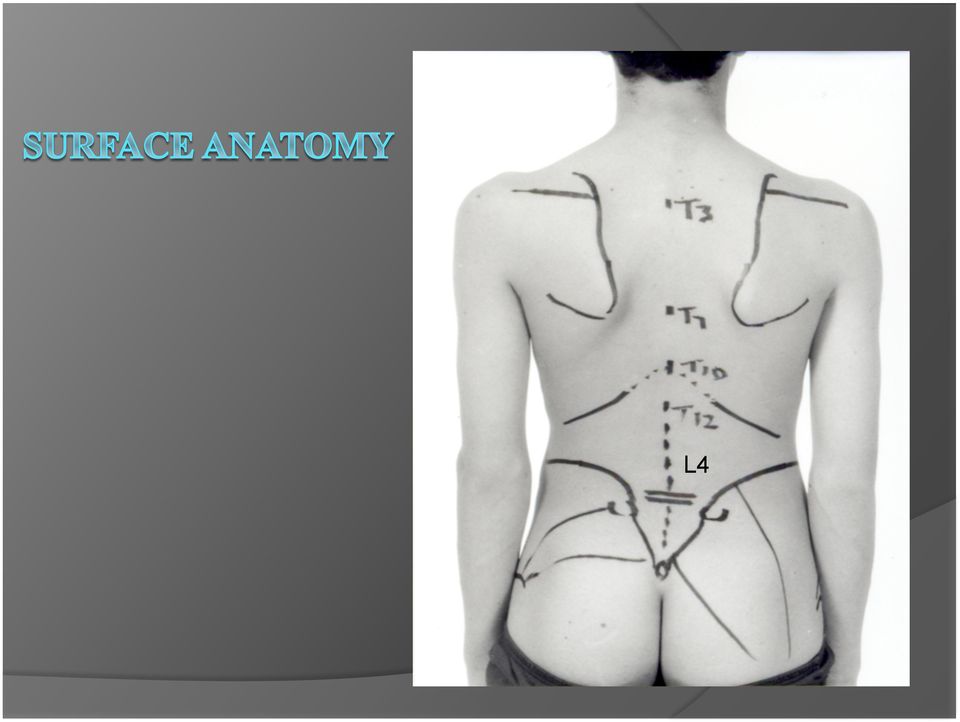
7 Low back pain terminology Sacral spinal pain S1 spinous process PSIS and PSIS Sacrococcygeal joint

8 What is not low back pain? Flank / loin pain Visceral Gluteal pain Local causes Sciatica (radicular pain) Not LBP Lower limb pain Causes are different Mechanisms of pain are different

9 Acute LBP Acute 0 to 6 weeks Subacute 6 to 12 weeks Chronic > 12 weeks

10 Prevalence, natural history Acute LBP (ALBP) is common In any given year, 1/3 of adults affected 1/3 of these seek treatment Most acute LBP resolves within 2 weeks 70-90% recover fully <3 months Relapse is common Up to 10% develop chronic pain & disability

11 Assessment Differentiate: 1. Serious pathology (red flag conditions) 2. Radicular nerve involvement 3. Non-specific back pain

12 Red flag conditions Fracture Major trauma Minor trauma associated with osteoporosis age >50 corticosteroid use

13 Red flag conditions Cancer Weight loss LR 2.5 Age > 50yo 2.7 PAST HISTORY 15.5 Failure to improve 3.1 Prolonged pain 2.6 ESR > Haematocrit <30% 15 Nocturnal pain

14 Red flag conditions Infection Fever LR History of: skin infection iv catheters UTI

15 Red flag conditions Ankylosing spondylitis Chest expansion <2.5cm LR out of 5 of: morning stiffness LR 6.3 improved with exercise onset <40 yo slow onset duration >3 months

16 History Onset and duration of pain Site and radiation Precipitating and relieving factors Severity and disability Neurological deficit Symptoms of systemic illness

17 Onset and duration Pain triggered by specific event Spontaneous onset Onset during normal activity Significant trauma?fracture

18 Site of pain and radiation Back pain only With leg pain somatic referred pain radicular pain determine dominant pain, LBP or leg pain Leg pain dominant Probably radicular

19 (somatic) referred or radicular pain? A B

20 Somatic pain Pain evoked by noxious stimulation of nerve endings innervating spinal structures: discs zygapophysial/facet joints sacroiliac joints dura ligaments muscles Pain can be felt locally and/or referred

21 Z joint SI joint Referred pain Stimulation of peripheral endings of nociceptive afferent fibers Pain perceived in a region innervated by nerves other than the ones that innervate the actual source of pain
22 Radicular pain Neurogenic pain Stimulation or irritation of the nerve roots or dorsal root ganglion of a spinal nerve
23 Radicular pain Vs Referred pain
24 Sacroiliac joint pain Consider if: pain entirely caudal to L5 normal neurology sacroiliac provocation tests FABER test (Flexion ABduction External Rotation) POSH test (POsterior SHeer) = thigh thrust test Laslett et al (Australian J of Physiotherapy 2003 Vol 49) Distraction test Thigh thrust test Gaenslen s test Compression test Sacral thrust test ( 3 or more positive: kappa ; LR 4-6) (chronic cases: consider if XR normal & MRI normal discs)
25 Precipitating & relieving factors Mechanical LBP better at rest worse with activity Inflammatory spondyloarthropathy pain at rest better with activity Disc disorders worse with flexion e.g. prolonged sitting Spinal stenosis & facet joint disorders worse with extension
26 Severity & disability VAS (Visual Analogue Scale) NRS (Numerical Rating Scale) Effect on ADLs e.g. sleeping, sitting, standing, walking, driving, work, sports Sleep nocturnal pain?red flag Functional/disability scale short OMPSQ (short Orebro Musculoskeletal Pain Screening Questionnaire)
27 Neurological deficit Radiculopathy refers to neurological deficit with nerve root lesions (is not synonymous with radicular pain) i.e. leg numbness weakness impaired reflexes tends to be associated with radicular pain
28 Neurological deficit Cauda equina syndrome result of compression of the neural elements below the end of the spinal cord (L1-2 level) causing: severe LBP bilateral leg symptoms: pain, weakness impairing gait paralysis, sensory changes Saddle anaesthesia, perineal numbness Urinary dysfunction: retention, difficulty starting/ stopping stream, overflow incontinence Reduced bladder and urethral sensation Bowel disturbance: incontinence, constipation, reduced anal tone on PR Sexual dysfunction Refer urgently to hospital for assessment, MRI, surgical spinal decompression, to prevent permanent neurological damage
29 Symptoms of systemic illness Loss of appetite Weight loss Fever, night sweats Fatigue
30 Examination 1. To identify serious pathology 2. Radicular features 3. Non-specific LBP Pain behaviour, posture, gait ROM lumbar, SLR, femoral nerve stretch, hips Neurological Tenderness
31 Sacroiliac joint pain Pain with normal pelvic alignment due to: sprain sacroiliitis fracture, tumour Pain with pelvic malalignment/sij dysfunction due to: sprain
32 Pelvic malalignment/sij dysfunction height of iliac crests, PSIS, ASIS leg length difference (LLD) (apparent LLD vs true LLD) supine long-sitting position asymmetry pelvic landmarks: PSIS, ASIS ischial tuberosities symphysis pubis provocation tests treatment SIJ mobilisation ( for anterior innominate )
33 Examination Standing observation: pain behaviour, posture, gait, spinal curvature, symmetry, iliac crests, skin folds, pelvic shift, wasting movement: lumbar ROM Supine LLD, SLR, hips, SIJ stress tests Neurological: reflexes, power, sensation Prone femoral nerve stretch, tenderness, gluteal muscles Sidelying gluteal muscles, perineal sensation, anal sphincter tone
34 Features of radicular irritation Leg pain > back pain Narrow band of pain in lower leg or foot (in segmental NOT dermatomal distribution) Numbness and paraesthesia in dermatomal distribution Reduced leg reflexes Positive SLR (L4-S1 roots) Positive FNS (L2-L4 roots) Segmental weakness Impulse pain coughing, sneezing
35 Investigations Red flags major trauma or minor trauma with osteoporosis -> x-ray Unrelenting pain, worse at night Age <20 years, or new back pain age >50 years History of cancer Systemic symptoms eg fever, weight loss IV drug use Immunosuppression or steroids x-ray, FBC, CRP, alk phos, Calcium, PSA, referral Sphincter disturbance Gait disturbance, progressive neurological deficit Saddle anaesthesia?cauda equina refer hospital for emergency assessment
36 Investigations Non-serious conditions = 95% of of LBP non-specific LBP X-ray most non-specific LBP does not require x-ray false positive findings consider radiation exposure if no improvement after 4 weeks
37 Investigations MRI non-specific LBP does not require MRI for: unresolving radicular pain chronic LBP
38 Overall the recommendations in the current guidelines regarding diagnosis and treatment of low back pain did not change substantially compared to the guidelines issued about a decade ago. May illustrate the lack of new evidence showing better results with new diagnostic and therapeutic approaches and/or new evidence showing the inefficacy of existing interventions. A less nihilistic view could be that already a decade ago the most valid recommendations for the management of low back pain were identified. much more effort should now be given to implementation of guidelines. In the past decade many countries have issued (updated) clinical guidelines for the management of low back pain. In general these guidelines provide similar advice on the management of low back pain.
39 Management Address fears fear about pain can be disabling contributes to disability and chronicity Determine beliefs and attitudes regarding condition and pain Feelings: what are your concerns? Ideas: what do you understand is the cause of your back pain? Function: how is it affecting you? Expectations: what do you think is needed to help?
40 Yellow flags Factors associated with poorer prognosis Belief that back pain is harmful and potentially severely disabling I hurt, I can t move, I can t work and I m scared Avoiding behaviours for fear of damaging back PH chronic pain, somatisation, preoccupation with health Negative attitudes and outlook; tendency towards lowered mood and social withdrawal Expectation that passive treatments will help more than active participation
41 Management Provide reassurance offer biological model of the pain e.g. sprained ligaments, muscles, disc; takes days to weeks to heal; gradual return to activity no sign of serious disease most acute LBP gets better most resolves < 2weeks 70-90% < 3 months relapses possible; overall recovery
42 Management pain occurring with movement does not indicate ongoing damage; therefore light activity not harmful muscle tension and spasm can be relieved with stretching and light activity
43 Management Encourage activity stay active despite pain rather than waiting for pain to settle completely continue normal activities if possible continue work: speeds recovery, reduces recurrences selected duties rather than off work if unfit for work, RTW ASAP; do not wait until pain-free teach simple stretches or refer physiotherapy for exercises walking, swimming/aquajogging bedrest is harmful; delays recovery
44 Management Analgesia (lacks evidence;mainly empirical) provide adequate analgesia to assist mobilisation paracetamol, 1g four times daily Add: Add: NSAID eg ibuprofen 400mg qid codeine 30-60mg 4 hourly, or tramadol 50mg 6 hourly laxatives?muscle relaxants tricyclics not indicated Heat (some evidence for heatwraps) Manual therapy to encourage activity
45 Management Review regularly (few days to weekly) to: develop relationship with patient monitor progress reinforce active participation reassure assess for red/yellow flags After 4 to 6 weeks: if not resolving x-ray, bloods refer for specialist assessment
46 Radicular pain 50% resolve < 4weeks 90% start to improve < 6weeks, resolve <12 weeks no need for x-rays adequate analgesia if no improvement over 4-6 weeks x-ray refer specialist assessment MRI TFI (TransForaminal Injection of steroid)
47 Chronic Low back pain Validated sources of CLBP: lumbar intervertebral discs - prevalence 40% zygapophysial joints ( Z joints ) = facet joints 10-15% younger injured workers; 40% older noninjured population Sacroiliac joints %
48 Procedures for investigation of chronic LBP ( ISIS protocol) provocation discography zygapophysial (facet) joint blocks sacroiliac joint blocks
49 Chronic Low back pain Intervertebral disc diagnosis rehabilitation exercises activity modification surgery Facet joint intra-articular injections medial branch nerve blocks ->radiofrequency neurotomy Sacroiliac joint pelvic mobilisation intra-articular injections Chronic Pain Syndrome/centrally mediated pain/central sensitisation explanation medication exercise psychological management
50 Key points Acute LBP is common; most patients recover in 3 months Serious causes are rare; excluded with careful history & examination No imaging if no red flags Exact diagnosis often not possible, nor needed Beliefs, attitudes and fear about pain contribute to chronicity & should be addressed Management includes reassurance, education & staying active Adequate analgesia
51 Dr Charles Ng NZ Association Musculoskeletal Medicine
6/3/2011. High Prevalence and Incidence. Low back pain is 5 th most common reason for all physician office visits in the U.S.
 High Prevalence and Incidence Prevalence 85% of Americans will experience low back pain at some time in their life. Incidence 5% annual Timothy C. Shen, M.D. Physical Medicine and Rehabilitation Sub-specialty
High Prevalence and Incidence Prevalence 85% of Americans will experience low back pain at some time in their life. Incidence 5% annual Timothy C. Shen, M.D. Physical Medicine and Rehabilitation Sub-specialty
Low Back Pain Protocols
 Low Back Pain Protocols Introduction: Diagnostic Triage And 1. Patient Group Adults aged 18 years and over with routine low back problems. Patients who have had recent surgery should be referred directly
Low Back Pain Protocols Introduction: Diagnostic Triage And 1. Patient Group Adults aged 18 years and over with routine low back problems. Patients who have had recent surgery should be referred directly
BACK PAIN PATHWAY DEFINTIONS
 BACK PAIN PATHWAY DEFINTIONS Cauda Equina Syndrome (CES) Current or imminent compression of the sacral nerve roots resulting in neurogenic bladder and bowel dysfunction. Symptoms typically include: severe
BACK PAIN PATHWAY DEFINTIONS Cauda Equina Syndrome (CES) Current or imminent compression of the sacral nerve roots resulting in neurogenic bladder and bowel dysfunction. Symptoms typically include: severe
Sample Treatment Protocol
 Sample Treatment Protocol 1 Adults with acute episode of LBP Definition: Acute episode Back pain lasting
Sample Treatment Protocol 1 Adults with acute episode of LBP Definition: Acute episode Back pain lasting
Pathophysiology of Acute and Chronic Low Back Pain
 Pathophysiology of Acute and Chronic Low Back Pain Mary Beth Partyka MSN APN Adult Nurse Practitioner Adult Pain Service Advocate Christ Medical Center Presentation Objectives Review the incidence of acute
Pathophysiology of Acute and Chronic Low Back Pain Mary Beth Partyka MSN APN Adult Nurse Practitioner Adult Pain Service Advocate Christ Medical Center Presentation Objectives Review the incidence of acute
Acute low back pain. Key reviewers: Mr Chris Hoffman, Orthopaedic Surgeon, Mana Orthopaedics, Wellington
 Acute low back pain Key reviewers: Mr Chris Hoffman, Orthopaedic Surgeon, Mana Orthopaedics, Wellington Dr John MacVicar, Medical Director, Southern Rehab, Christchurch Key concepts: Acute low back pain
Acute low back pain Key reviewers: Mr Chris Hoffman, Orthopaedic Surgeon, Mana Orthopaedics, Wellington Dr John MacVicar, Medical Director, Southern Rehab, Christchurch Key concepts: Acute low back pain
Clinical Guideline. Low Back Pain Orthopaedics. Princess Alexandra Hospital Emergency Department. 1 Purpose. 2 Background
 Princess Alexandra Hospital Emergency Department Clinical Guideline Orthopaedics Review Officer: Katherine Isoardi Version no: 1 Approval date: 18/03/2015 Review date: 18/03/2017 Approving Officer Dr James
Princess Alexandra Hospital Emergency Department Clinical Guideline Orthopaedics Review Officer: Katherine Isoardi Version no: 1 Approval date: 18/03/2015 Review date: 18/03/2017 Approving Officer Dr James
CLINICAL PRACTICE GUIDELINES FOR MANAGEMENT OF LOW BACK PAIN
 CLINICAL PRACTICE GUIDELINES FOR MANAGEMENT OF LOW BACK PAIN Low back pain is very common, up to 90+% of people are affected by back pain at some time in their lives. Most often back pain is benign and
CLINICAL PRACTICE GUIDELINES FOR MANAGEMENT OF LOW BACK PAIN Low back pain is very common, up to 90+% of people are affected by back pain at some time in their lives. Most often back pain is benign and
Spinal Surgery 2. Teaching Aims. Common Spinal Pathologies. Disc Degeneration. Disc Degeneration. Causes of LBP 8/2/13. Common Spinal Conditions
 Teaching Aims Spinal Surgery 2 Mr Mushtaque A. Ishaque BSc(Hons) BChir(Cantab) DM FRCS FRCS(Ed) FRCS(Orth) Hunterian Professor at The Royal College of Surgeons of England Consultant Orthopaedic Spinal
Teaching Aims Spinal Surgery 2 Mr Mushtaque A. Ishaque BSc(Hons) BChir(Cantab) DM FRCS FRCS(Ed) FRCS(Orth) Hunterian Professor at The Royal College of Surgeons of England Consultant Orthopaedic Spinal
Advanced Practice Provider Academy
 (+)Dean T. Harrison, MPAS,PA C,DFAAPA Director of Mid Level Practitioners; Assistant Medical Director Clinical Evaluation Unit, Division of Emergency Medicine, Department of Surgery, Duke University Medical
(+)Dean T. Harrison, MPAS,PA C,DFAAPA Director of Mid Level Practitioners; Assistant Medical Director Clinical Evaluation Unit, Division of Emergency Medicine, Department of Surgery, Duke University Medical
Spine Trauma: When to Transfer. Alexander Ching, MD Director, Orthopaedic Spine Trauma OHSU
 Spine Trauma: When to Transfer Alexander Ching, MD Director, Orthopaedic Spine Trauma OHSU Disclosures Depuy Spine Consultant (teaching and courses) Department education and research funds Atlas Spine
Spine Trauma: When to Transfer Alexander Ching, MD Director, Orthopaedic Spine Trauma OHSU Disclosures Depuy Spine Consultant (teaching and courses) Department education and research funds Atlas Spine
Sciatica Yuliya Mutsa PTA 236
 Sciatica Yuliya Mutsa PTA 236 Sciatica is a common type of pain affecting the sciatic nerve, which extends from the lower back all the way through the back of the thigh and down through the leg. Depending
Sciatica Yuliya Mutsa PTA 236 Sciatica is a common type of pain affecting the sciatic nerve, which extends from the lower back all the way through the back of the thigh and down through the leg. Depending
DIFFERENTIAL DIAGNOSIS OF LOW BACK PAIN. Arnold J. Weil, M.D., M.B.A. Non-Surgical Orthopaedics, P.C. Atlanta, GA
 DIFFERENTIAL DIAGNOSIS OF LOW BACK PAIN Arnold J. Weil, M.D., M.B.A. Non-Surgical Orthopaedics, P.C. Atlanta, GA MEDICAL ALGORITHM OF REALITY LOWER BACK PAIN Yes Patient will never get better until case
DIFFERENTIAL DIAGNOSIS OF LOW BACK PAIN Arnold J. Weil, M.D., M.B.A. Non-Surgical Orthopaedics, P.C. Atlanta, GA MEDICAL ALGORITHM OF REALITY LOWER BACK PAIN Yes Patient will never get better until case
Low Back Injury in the Industrial Athlete: An Anatomic Approach
 Low Back Injury in the Industrial Athlete: An Anatomic Approach Earl J. Craig, M.D. Assistant Professor Indiana University School of Medicine Department of Physical Medicine and Rehabilitation Epidemiology
Low Back Injury in the Industrial Athlete: An Anatomic Approach Earl J. Craig, M.D. Assistant Professor Indiana University School of Medicine Department of Physical Medicine and Rehabilitation Epidemiology
Spine University s Guide to Cauda Equina Syndrome
 Spine University s Guide to Cauda Equina Syndrome 2 Introduction Your spine is a very complicated part of your body. It s made up of the bones (vertebrae) that keep it aligned, nerves that channel down
Spine University s Guide to Cauda Equina Syndrome 2 Introduction Your spine is a very complicated part of your body. It s made up of the bones (vertebrae) that keep it aligned, nerves that channel down
The Spine Center at Beth Israel Deaconess
 Spinal Pain The Spine Center at Beth Israel Deaconess Medical Center developed the following detailed eplanation of our care pathways for primary care providers to help support your interactions with patients
Spinal Pain The Spine Center at Beth Israel Deaconess Medical Center developed the following detailed eplanation of our care pathways for primary care providers to help support your interactions with patients
Acute Low Back Pain. North American Spine Society Public Education Series
 Acute Low Back Pain North American Spine Society Public Education Series What Is Acute Low Back Pain? Acute low back pain (LBP) is defined as low back pain present for up to six weeks. It may be experienced
Acute Low Back Pain North American Spine Society Public Education Series What Is Acute Low Back Pain? Acute low back pain (LBP) is defined as low back pain present for up to six weeks. It may be experienced
Practice Guidelines For Low Back Pain
 Consumers Guide Practice Guidelines For Low Back Pain Copyright 2008 American Chronic Pain Association Page 1 Written by: Penney Cowan Founder Executive Director American Chronic Pain Association Editors:
Consumers Guide Practice Guidelines For Low Back Pain Copyright 2008 American Chronic Pain Association Page 1 Written by: Penney Cowan Founder Executive Director American Chronic Pain Association Editors:
Fact Sheet. Queensland Spinal Cord Injuries Service. Pain Management Following Spinal Cord Injury for Health Professionals
 Pain Management Following Injury for Health Professionals and Introduction Pain is a common problem following SCI. In the case where a person with SCI does have pain, there are treatments available that
Pain Management Following Injury for Health Professionals and Introduction Pain is a common problem following SCI. In the case where a person with SCI does have pain, there are treatments available that
There are four main regions of the back; the cervical (C), thoracic (T), lumbar (L), and sacral (S) regions
, thoracic (T), lumbar (L), and sacral (S) regions") Low Back Pain Overview Low back pain is one of the most common disorders in the United States. About 80 percent of people have at least one episode of low back pain during their lifetime. Factors that
Low Back Pain Overview Low back pain is one of the most common disorders in the United States. About 80 percent of people have at least one episode of low back pain during their lifetime. Factors that
A Syndrome (Pattern) Approach to Low Back Pain. History
 Approach to Low Back Pain. History") A Syndrome (Pattern) Approach to Low Back Pain Hamilton Hall MD FRCSC Professor, Department of Surgery, University of Toronto Medical Director, CBI Health Group Executive Director, Canadian Spine Society
A Syndrome (Pattern) Approach to Low Back Pain Hamilton Hall MD FRCSC Professor, Department of Surgery, University of Toronto Medical Director, CBI Health Group Executive Director, Canadian Spine Society
Hitting a Nerve: The Triggers of Sciatica. Bruce Tranmer MD FRCS FACS
 Hitting a Nerve: The Triggers of Sciatica Bruce Tranmer MD FRCS FACS Disclosures I have no financial disclosures Objectives - Sciatica Historical Perspective What is Sciatica What can cause Sciatica Clinical
Hitting a Nerve: The Triggers of Sciatica Bruce Tranmer MD FRCS FACS Disclosures I have no financial disclosures Objectives - Sciatica Historical Perspective What is Sciatica What can cause Sciatica Clinical
The Essential Lower Back Exam
 STFM National Convention 2011 New Orleans The Essential Lower Back Exam Judith A. Furlong, M.D., Cathee McGonigle, D.O. & Rob Rutherford, MD Objectives Brief review of the anatomy of the back, (hip and
STFM National Convention 2011 New Orleans The Essential Lower Back Exam Judith A. Furlong, M.D., Cathee McGonigle, D.O. & Rob Rutherford, MD Objectives Brief review of the anatomy of the back, (hip and
.org. Herniated Disk in the Lower Back. Anatomy. Description
 Herniated Disk in the Lower Back Page ( 1 ) Sometimes called a slipped or ruptured disk, a herniated disk most often occurs in your lower back. It is one of the most common causes of low back pain, as
Herniated Disk in the Lower Back Page ( 1 ) Sometimes called a slipped or ruptured disk, a herniated disk most often occurs in your lower back. It is one of the most common causes of low back pain, as
INFORMATION FOR YOU. Lower Back Pain
 INFORMATION FOR YOU Lower Back Pain WHAT IS ACUTE LOWER BACK PAIN? Acute lower back pain is defined as low back pain present for up to six weeks. It may be experienced as aching, burning, stabbing, sharp
INFORMATION FOR YOU Lower Back Pain WHAT IS ACUTE LOWER BACK PAIN? Acute lower back pain is defined as low back pain present for up to six weeks. It may be experienced as aching, burning, stabbing, sharp
Herniated Lumbar Disc
 Herniated Lumbar Disc North American Spine Society Public Education Series What Is a Herniated Disc? The spine is made up of a series of connected bones called vertebrae. The disc is a combination of strong
Herniated Lumbar Disc North American Spine Society Public Education Series What Is a Herniated Disc? The spine is made up of a series of connected bones called vertebrae. The disc is a combination of strong
L5 S1 Extruded Disc Relieved with Cox Technic Decompression Spinal Adjusting
 1 L5 S1 Extruded Disc Relieved with Cox Technic Decompression Spinal Adjusting submitted by Joseph d'angiolillo DC 11 Clyde Road, Suite 103 Somerset, NJ 08873 (732) 873 2222 This is a case study of a patient
1 L5 S1 Extruded Disc Relieved with Cox Technic Decompression Spinal Adjusting submitted by Joseph d'angiolillo DC 11 Clyde Road, Suite 103 Somerset, NJ 08873 (732) 873 2222 This is a case study of a patient
BACK PAIN MEASURES GROUP OVERVIEW
 2014 PQRS OPTIONS F MEASURES GROUPS: BACK PAIN MEASURES GROUP OVERVIEW 2014 PQRS MEASURES IN BACK PAIN MEASURES GROUP: #148. Back Pain: Initial Visit #149. Back Pain: Physical Exam #150. Back Pain: Advice
2014 PQRS OPTIONS F MEASURES GROUPS: BACK PAIN MEASURES GROUP OVERVIEW 2014 PQRS MEASURES IN BACK PAIN MEASURES GROUP: #148. Back Pain: Initial Visit #149. Back Pain: Physical Exam #150. Back Pain: Advice
Temple Physical Therapy
 Temple Physical Therapy A General Overview of Common Neck Injuries For current information on Temple Physical Therapy related news and for a healthy and safe return to work, sport and recreation Like Us
Temple Physical Therapy A General Overview of Common Neck Injuries For current information on Temple Physical Therapy related news and for a healthy and safe return to work, sport and recreation Like Us
Treating Bulging Discs & Sciatica. Alexander Ching, MD
 Treating Bulging Discs & Sciatica Alexander Ching, MD Disclosures Depuy Spine Teaching and courses K2 Spine Complex Spine Study Group Disclosures Take 2 I am a spine surgeon I like spine surgery I believe
Treating Bulging Discs & Sciatica Alexander Ching, MD Disclosures Depuy Spine Teaching and courses K2 Spine Complex Spine Study Group Disclosures Take 2 I am a spine surgeon I like spine surgery I believe
Herniated Disk. This reference summary explains herniated disks. It discusses symptoms and causes of the condition, as well as treatment options.
 Herniated Disk Introduction Your backbone, or spine, has 24 moveable vertebrae made of bone. Between the bones are soft disks filled with a jelly-like substance. These disks cushion the vertebrae and keep
Herniated Disk Introduction Your backbone, or spine, has 24 moveable vertebrae made of bone. Between the bones are soft disks filled with a jelly-like substance. These disks cushion the vertebrae and keep
SPINE. Postural Malalignments 4/9/2015. Cervical Spine Evaluation. Thoracic Spine Evaluation. Observations. Assess position of head and neck
 SPINE Observations Body type Postural alignments and asymmetries should be observed from all views Assess height differences between anatomical landmarks Figure 25-9 Figure 25-10 Figure 25-11 & 12 Postural
SPINE Observations Body type Postural alignments and asymmetries should be observed from all views Assess height differences between anatomical landmarks Figure 25-9 Figure 25-10 Figure 25-11 & 12 Postural
Musculoskeletal: Acute Lower Back Pain
 Musculoskeletal: Acute Lower Back Pain Acute Lower Back Pain Back Pain only Sciatica / Radiculopathy Possible Cord or Cauda Equina Compression Possible Spinal Canal Stenosis Red Flags Initial conservative
Musculoskeletal: Acute Lower Back Pain Acute Lower Back Pain Back Pain only Sciatica / Radiculopathy Possible Cord or Cauda Equina Compression Possible Spinal Canal Stenosis Red Flags Initial conservative
Clinical guidance for MRI referral
 MRI for cervical radiculopathy Referral by a medical practitioner (excluding a specialist or consultant physician) for a scan of spine for a patient 16 years or older for suspected: cervical radiculopathy
MRI for cervical radiculopathy Referral by a medical practitioner (excluding a specialist or consultant physician) for a scan of spine for a patient 16 years or older for suspected: cervical radiculopathy
Cervical Spondylosis (Arthritis of the Neck)
") Copyright 2009 American Academy of Orthopaedic Surgeons Cervical Spondylosis (Arthritis of the Neck) Neck pain is extremely common. It can be caused by many things, and is most often related to getting
Copyright 2009 American Academy of Orthopaedic Surgeons Cervical Spondylosis (Arthritis of the Neck) Neck pain is extremely common. It can be caused by many things, and is most often related to getting
Clinical Signs of Low Back Pain
 Review of Clinical Signs Series Editor: Bernard Karnath, MD Clinical Signs of Low Back Pain Bernard Karnath, MD Back pain has been cited as the fifth most common reason that patients visit a physician.
Review of Clinical Signs Series Editor: Bernard Karnath, MD Clinical Signs of Low Back Pain Bernard Karnath, MD Back pain has been cited as the fifth most common reason that patients visit a physician.
Efficacy of Epidural Steroid Injections for Lumbar Radiculopathy. Dr Chris Milne Sports Physician Hamilton
 Efficacy of Epidural Steroid Injections for Lumbar Radiculopathy Dr Chris Milne Sports Physician Hamilton Clinical Background 1-Low back pain is common 2-Early resolution is the usual outcome 3-A small
Efficacy of Epidural Steroid Injections for Lumbar Radiculopathy Dr Chris Milne Sports Physician Hamilton Clinical Background 1-Low back pain is common 2-Early resolution is the usual outcome 3-A small
About your presenter LOW BACK PAIN. Epidemiology. Outline. Outline. Anatomy: Superficial Muscles 12/10/2012
 About your presenter LOW BACK PAIN Chronic Care Lecture Series Brian Liem, MD Sports Medicine Fellow University of Washington Department of Rehabilitation Medicine Hometown: Seattle, WA College: University
About your presenter LOW BACK PAIN Chronic Care Lecture Series Brian Liem, MD Sports Medicine Fellow University of Washington Department of Rehabilitation Medicine Hometown: Seattle, WA College: University
Information on the Chiropractic Care of Lower Back Pain
 Chiropractic Care of Lower Back Pain Lower back pain is probably the most common condition seen the the Chiropractic office. Each month it is estimated that up to one third of persons experience some type
Chiropractic Care of Lower Back Pain Lower back pain is probably the most common condition seen the the Chiropractic office. Each month it is estimated that up to one third of persons experience some type
Clinical Reasoning The patient presents with no red flags and no indications of maladaptive behaviour in regard to fear avoidance.
 The McKenzie Institute International 2014 Vol. 3, No. 3 CASE REVIEW: A CLINICIAN S PERSPECTIVE Case Review: 35-Year-Old Male with History of Low Back Pain Brian Østergaard Sørensen, PT, Dip.MDT Introduction
The McKenzie Institute International 2014 Vol. 3, No. 3 CASE REVIEW: A CLINICIAN S PERSPECTIVE Case Review: 35-Year-Old Male with History of Low Back Pain Brian Østergaard Sørensen, PT, Dip.MDT Introduction
Spine conditionsnew treatments. Ben Okafor FRCS FRCS.orth Consultant Orthopaedic Surgeon
 Spine conditionsnew treatments Ben Okafor FRCS FRCS.orth Consultant Orthopaedic Surgeon Certainties of life Death Taxes Back pain New Advances Minimal access surgery Indirect Lumbar decompression Dynamic
Spine conditionsnew treatments Ben Okafor FRCS FRCS.orth Consultant Orthopaedic Surgeon Certainties of life Death Taxes Back pain New Advances Minimal access surgery Indirect Lumbar decompression Dynamic
III./8.4.2: Spinal trauma. III./8.4.2.1 Injury of the spinal cord
 III./8.4.2: Spinal trauma Introduction Causes: motor vehicle accidents, falls, sport injuries, industrial accidents The prevalence of spinal column trauma is 64/100,000, associated with neurological dysfunction
III./8.4.2: Spinal trauma Introduction Causes: motor vehicle accidents, falls, sport injuries, industrial accidents The prevalence of spinal column trauma is 64/100,000, associated with neurological dysfunction
1 REVISOR 5223.0070. (4) Pain associated with rigidity (loss of motion or postural abnormality) or
 Pain associated with rigidity (loss of motion or postural abnormality) or") 1 REVISOR 5223.0070 5223.0070 MUSCULOSKELETAL SCHEDULE; BACK. Subpart 1. Lumbar spine. The spine rating is inclusive of leg symptoms except for gross motor weakness, bladder or bowel dysfunction, or sexual
1 REVISOR 5223.0070 5223.0070 MUSCULOSKELETAL SCHEDULE; BACK. Subpart 1. Lumbar spine. The spine rating is inclusive of leg symptoms except for gross motor weakness, bladder or bowel dysfunction, or sexual
Musculoskeletal System
 CHAPTER 3 Impact of SCI on the Musculoskeletal System Voluntary movement of the body is dependent on a number of systems. These include: The brain initiates the movement and receives feedback to assess
CHAPTER 3 Impact of SCI on the Musculoskeletal System Voluntary movement of the body is dependent on a number of systems. These include: The brain initiates the movement and receives feedback to assess
LOW BACK PAIN EXAMINATION
 LOW BACK PAIN EXAMINATION John Petty, M.D. Medical Director Department of Physical Medicine & Rehabilitation Kettering Medical Center February 8, 2014 PRE-TEST QUESTION What part of the low back physical
LOW BACK PAIN EXAMINATION John Petty, M.D. Medical Director Department of Physical Medicine & Rehabilitation Kettering Medical Center February 8, 2014 PRE-TEST QUESTION What part of the low back physical
Approach to Back Pain
 Approach to Back Pain Year 3 Clerkship Guide, Family Medicine Department Schulich School of Medicine and Dentistry Objectives 1. Define acute low back pain. 2. Define chronic back pain. 3. What is the
Approach to Back Pain Year 3 Clerkship Guide, Family Medicine Department Schulich School of Medicine and Dentistry Objectives 1. Define acute low back pain. 2. Define chronic back pain. 3. What is the
How To Treat Pain With Pain Management
 SUTTER PHYSICIANS ALLIANCE (SPA) 2800 L Street, 7 th Floor Sacramento, CA 95816 SPA PCP Treatment & Referral Guidelines Pain Management Developed June 1, 2003 Revised - (Format Revisions) November 13,
SUTTER PHYSICIANS ALLIANCE (SPA) 2800 L Street, 7 th Floor Sacramento, CA 95816 SPA PCP Treatment & Referral Guidelines Pain Management Developed June 1, 2003 Revised - (Format Revisions) November 13,
LUMBAR. Hips R L B R L B LUMBAR. Hips R L B R L B LUMBAR. Hips R L B R L B
 1 Patient Name In order to properly assess your condition, we must understand how much your BACK/LEG (SCIATIC) PAIN has affected your ability to manage everyday activities. For each item below, please
1 Patient Name In order to properly assess your condition, we must understand how much your BACK/LEG (SCIATIC) PAIN has affected your ability to manage everyday activities. For each item below, please
A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH)
") A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH) Introduction Diffuse Idiopathic Skeletal Hyperostosis (DISH) is a phenomenon that more commonly affects older males. It is associated
A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH) Introduction Diffuse Idiopathic Skeletal Hyperostosis (DISH) is a phenomenon that more commonly affects older males. It is associated
LOW BACK INJURIES PROGRAM OF CARE PROGRAM OF CARE 4TH EDITION 2014
 LOW BACK INJURIES PROGRAM OF CARE PROGRAM OF CARE 4TH EDITION 2014 GUIDE Acknowledgements Acknowledgements The WSIB would like to acknowledge the significant contributions of the following regulated Health
LOW BACK INJURIES PROGRAM OF CARE PROGRAM OF CARE 4TH EDITION 2014 GUIDE Acknowledgements Acknowledgements The WSIB would like to acknowledge the significant contributions of the following regulated Health
Lumbar Disc Herniation/Bulge Protocol
 Lumbar Disc Herniation/Bulge Protocol Anatomy and Biomechanics The lumbar spine is made up of 5 load transferring bones called vertebrae. They are stacked in a column with an intervertebral disc sandwiched
Lumbar Disc Herniation/Bulge Protocol Anatomy and Biomechanics The lumbar spine is made up of 5 load transferring bones called vertebrae. They are stacked in a column with an intervertebral disc sandwiched
MALIGNANT SPINAL CORD COMPRESSION. Kate Hamilton Head of Medical Oncology Ballarat Health Services
 MALIGNANT SPINAL CORD COMPRESSION Kate Hamilton Head of Medical Oncology Ballarat Health Services OVERVIEW Background Epidemiology Pathophysiology Diagnosis Investigation Differential Diagnosis Management
MALIGNANT SPINAL CORD COMPRESSION Kate Hamilton Head of Medical Oncology Ballarat Health Services OVERVIEW Background Epidemiology Pathophysiology Diagnosis Investigation Differential Diagnosis Management
Physiotherapy fees and utilization guidelines for auto insurance accident claimants
 No. A-12/97 Property & Casualty ) Auto Physiotherapy fees and utilization guidelines for auto insurance accident claimants To the attention of all insurance companies licensed to transact automobile insurance
No. A-12/97 Property & Casualty ) Auto Physiotherapy fees and utilization guidelines for auto insurance accident claimants To the attention of all insurance companies licensed to transact automobile insurance
Do you have Back Pain? Associated with:
 Do you have Back Pain? Associated with: Herniated Discs? Protruding Discs? Degenerative Disk Disease? Posterior Facet Syndrome? Sciatica? You may be a candidate for Decompression Therapy The Dynatronics
Do you have Back Pain? Associated with: Herniated Discs? Protruding Discs? Degenerative Disk Disease? Posterior Facet Syndrome? Sciatica? You may be a candidate for Decompression Therapy The Dynatronics
Cervical Spondylosis. Understanding the neck
 Page 1 of 5 Cervical Spondylosis This leaflet is aimed at people who have been told they have cervical spondylosis as a cause of their neck symptoms. Cervical spondylosis is a 'wear and tear' of the vertebrae
Page 1 of 5 Cervical Spondylosis This leaflet is aimed at people who have been told they have cervical spondylosis as a cause of their neck symptoms. Cervical spondylosis is a 'wear and tear' of the vertebrae
LOW BACK PAIN; MECHANICAL
 1 ORTHO 16 LOW BACK PAIN; MECHANICAL Background This case definition was developed by the Armed Forces Health Surveillance Center (AFHSC) for the purpose of epidemiological surveillance of a condition
1 ORTHO 16 LOW BACK PAIN; MECHANICAL Background This case definition was developed by the Armed Forces Health Surveillance Center (AFHSC) for the purpose of epidemiological surveillance of a condition
Management of Low back pain
 Management of Low back pain Dr Prabhu Gandhimani MD;FRCA;FIPP;FFPMRCA Kingston Hospital Queen Mary s Hospital, Roehampton New Victoria,Parkside Hospital and Putney ( NHS Choose and Book) Incidence About
Management of Low back pain Dr Prabhu Gandhimani MD;FRCA;FIPP;FFPMRCA Kingston Hospital Queen Mary s Hospital, Roehampton New Victoria,Parkside Hospital and Putney ( NHS Choose and Book) Incidence About
 Low Back Pain Mansour Dib MD Physical Medicine and Rehabilitation Pain generators Disc Posterior elements Sacro-iliac joint Education - Spine Positioning Neutral Extension Flexion Disc disease Discogenic
Low Back Pain Mansour Dib MD Physical Medicine and Rehabilitation Pain generators Disc Posterior elements Sacro-iliac joint Education - Spine Positioning Neutral Extension Flexion Disc disease Discogenic
IMPAIRMENT RATING 5 TH EDITION MODULE II
 IMPAIRMENT RATING 5 TH EDITION MODULE II THE SPINE AND ALTERATION OF MOTION SEGMENT INTEGRITY (AOMSI) PRESENTED BY: RONALD J. WELLIKOFF, D.C., FACC, FICC In conjuction with: The chapter on the spine includes
IMPAIRMENT RATING 5 TH EDITION MODULE II THE SPINE AND ALTERATION OF MOTION SEGMENT INTEGRITY (AOMSI) PRESENTED BY: RONALD J. WELLIKOFF, D.C., FACC, FICC In conjuction with: The chapter on the spine includes
The Newest Breakthrough In Non- Surgical Treatment of Herniated or Degenerative Discs
 The Newest Breakthrough In Non- Surgical Treatment of Herniated or Degenerative Discs The DRX 9000 is Your Answer To Persistent Back Pain To People Who Want To Be Rid Of Lower Back Pain But Think They
The Newest Breakthrough In Non- Surgical Treatment of Herniated or Degenerative Discs The DRX 9000 is Your Answer To Persistent Back Pain To People Who Want To Be Rid Of Lower Back Pain But Think They
Herniated Cervical Disc
 Herniated Cervical Disc North American Spine Society Public Education Series What Is a Herniated Disc? The backbone, or spine, is composed of a series of connected bones called vertebrae. The vertebrae
Herniated Cervical Disc North American Spine Society Public Education Series What Is a Herniated Disc? The backbone, or spine, is composed of a series of connected bones called vertebrae. The vertebrae
Whiplash and Whiplash- Associated Disorders
 Whiplash and Whiplash- Associated Disorders North American Spine Society Public Education Series What Is Whiplash? The term whiplash might be confusing because it describes both a mechanism of injury and
Whiplash and Whiplash- Associated Disorders North American Spine Society Public Education Series What Is Whiplash? The term whiplash might be confusing because it describes both a mechanism of injury and
What is a Sports Physician?
 What is a Sports Physician? Dr Mike Bundy MBBS MRCGP Dip Sports Med FFSEM Consultant in Sport and Exercise Medicine Medical Director at Pure Sports Medicine Ex-England Rugby senior team Doctor www.puresportsmed.com
What is a Sports Physician? Dr Mike Bundy MBBS MRCGP Dip Sports Med FFSEM Consultant in Sport and Exercise Medicine Medical Director at Pure Sports Medicine Ex-England Rugby senior team Doctor www.puresportsmed.com
Low back pain. Quick reference guide. Issue date: May 2009. Early management of persistent non-specific low back pain
 Issue date: May 2009 Low back pain Early management of persistent non-specific low back pain Developed by the National Collaborating Centre for Primary Care About this booklet This is a quick reference
Issue date: May 2009 Low back pain Early management of persistent non-specific low back pain Developed by the National Collaborating Centre for Primary Care About this booklet This is a quick reference
OVERVIEW. NEUROSURGICAL ASSESSMENT CERVICAL PROBLEMS Dirk G. Franzen, M.D. WHAT IS THE MOST IMPORTANT PART OF THE PHYSICAL EXAM?
 NEUROSURGICAL ASSESSMENT CERVICAL PROBLEMS Dirk G. Franzen, M.D. Neurological Surgery Bluegrass Orthopaedics and Hand Care OVERVIEW SCOPE OF THE PROBLEM PREVALENCE PATHOLOGY ANATOMIC CONSIDERATIONS ASSESSMENT
NEUROSURGICAL ASSESSMENT CERVICAL PROBLEMS Dirk G. Franzen, M.D. Neurological Surgery Bluegrass Orthopaedics and Hand Care OVERVIEW SCOPE OF THE PROBLEM PREVALENCE PATHOLOGY ANATOMIC CONSIDERATIONS ASSESSMENT
High Impact Rheumatology
 High Impact Rheumatology Evaluation and Management of Low Back Pain Back Pain in the Primary Care Clinic 90% of low back pain is mechanical Injury to muscles, ligaments, bones, disks Spontaneous resolution
High Impact Rheumatology Evaluation and Management of Low Back Pain Back Pain in the Primary Care Clinic 90% of low back pain is mechanical Injury to muscles, ligaments, bones, disks Spontaneous resolution
TWO CONTRASTING CASES OF SCIATIC RADICULOPATHY: ONE WITH NORMAL MRI AND ONE WITH A FREE FRAGMENT. WHAT S A CHIROPRACTOR TO DO?
 Cox Case Report #59 by Dr. James Cox published 4/08 1 TWO CONTRASTING CASES OF SCIATIC RADICULOPATHY: ONE WITH NORMAL MRI AND ONE WITH A FREE FRAGMENT. WHAT S A CHIROPRACTOR TO DO? A 26-year-old, white,
Cox Case Report #59 by Dr. James Cox published 4/08 1 TWO CONTRASTING CASES OF SCIATIC RADICULOPATHY: ONE WITH NORMAL MRI AND ONE WITH A FREE FRAGMENT. WHAT S A CHIROPRACTOR TO DO? A 26-year-old, white,
.org. Cervical Spondylosis (Arthritis of the Neck) Anatomy. Cause
 Anatomy. Cause") Cervical Spondylosis (Arthritis of the Neck) Page ( 1 ) Neck pain can be caused by many things but is most often related to getting older. Like the rest of the body, the disks and joints in the neck (cervical
Cervical Spondylosis (Arthritis of the Neck) Page ( 1 ) Neck pain can be caused by many things but is most often related to getting older. Like the rest of the body, the disks and joints in the neck (cervical
REFERRAL GUIDELINES: NEUROSURGERY
 Outpatient Referral Guidelines Page 1 1 REFERRAL GUIDELINES: NEUROSURGERY Essential Referral Content Date of birth Demographic Contact details (including mobile phone) Referring GP details Interpreter
Outpatient Referral Guidelines Page 1 1 REFERRAL GUIDELINES: NEUROSURGERY Essential Referral Content Date of birth Demographic Contact details (including mobile phone) Referring GP details Interpreter
BACK PAIN: WHAT YOU SHOULD KNOW
 BACK PAIN: WHAT YOU SHOULD KNOW Diane Metzer LOWER BACK PAIN Nearly everyone at some point has back pain that interferes with work, recreation and routine daily activities. Four out of five adults experience
BACK PAIN: WHAT YOU SHOULD KNOW Diane Metzer LOWER BACK PAIN Nearly everyone at some point has back pain that interferes with work, recreation and routine daily activities. Four out of five adults experience
Primary and revision lumbar discectomy. (nerve root decompression)
") Primary and revision lumbar discectomy (nerve root decompression) The aim of this leaflet is to help answer some of the questions you may have about having a lumbar discectomy. It explains the benefits,
Primary and revision lumbar discectomy (nerve root decompression) The aim of this leaflet is to help answer some of the questions you may have about having a lumbar discectomy. It explains the benefits,
Urinary Incontinence FAQ Sheet
 Urinary Incontinence FAQ Sheet Are you reluctant to talk to your doctor about your bladder control problem? Don t be. There is help. Loss of bladder control is called urinary incontinence. It can happen
Urinary Incontinence FAQ Sheet Are you reluctant to talk to your doctor about your bladder control problem? Don t be. There is help. Loss of bladder control is called urinary incontinence. It can happen
X Stop Spinal Stenosis Decompression
 X Stop Spinal Stenosis Decompression Am I a candidate for X Stop spinal surgery? You may be a candidate for the X Stop spinal surgery if you have primarily leg pain rather than mostly back pain and your
X Stop Spinal Stenosis Decompression Am I a candidate for X Stop spinal surgery? You may be a candidate for the X Stop spinal surgery if you have primarily leg pain rather than mostly back pain and your
Spine Injury and Back Pain in Sports
 Spine Injury and Back Pain in Sports DAVID W. GRAY, MD 1 Back Pain Increases with Age Girls>Boys in Teenage years Anywhere from 15 to 80% of children and adolescents have back pain depending on the studies
Spine Injury and Back Pain in Sports DAVID W. GRAY, MD 1 Back Pain Increases with Age Girls>Boys in Teenage years Anywhere from 15 to 80% of children and adolescents have back pain depending on the studies
Introduction: Anatomy of the spine and lower back:
 Castleknock GAA club member and Chartered Physiotherapist, James Sherry MISCP, has prepared an informative article on the common causes of back pain and how best it can be treated. To book a physiotherapy
Castleknock GAA club member and Chartered Physiotherapist, James Sherry MISCP, has prepared an informative article on the common causes of back pain and how best it can be treated. To book a physiotherapy
Whiplash Associated Disorder
 Whiplash Associated Disorder The pathology Whiplash is a mechanism of injury, consisting of acceleration-deceleration forces to the neck. Mechanism: Hyperflexion/extension injury Stationary vehicle hit
Whiplash Associated Disorder The pathology Whiplash is a mechanism of injury, consisting of acceleration-deceleration forces to the neck. Mechanism: Hyperflexion/extension injury Stationary vehicle hit
Lumbar Laminectomy and Interspinous Process Fusion
 Lumbar Laminectomy and Interspinous Process Fusion Introduction Low back and leg pain caused by pinched nerves in the back is a common condition that limits your ability to move, walk, and work. This condition
Lumbar Laminectomy and Interspinous Process Fusion Introduction Low back and leg pain caused by pinched nerves in the back is a common condition that limits your ability to move, walk, and work. This condition
Urinary Incontinence in Women. Susan Hingle, M.D. Department of Medicine
 Urinary Incontinence in Women Susan Hingle, M.D. Department of Medicine Background Estimated 13 million Americans with urinary incontinence Women are affected twice as frequently as men Only 25% will seek
Urinary Incontinence in Women Susan Hingle, M.D. Department of Medicine Background Estimated 13 million Americans with urinary incontinence Women are affected twice as frequently as men Only 25% will seek
The Effects of Cox Decompression Technic in the Treatment of Low Back Pain and Sciatica in a Golf Professional
 Cox Technic Email Case Report 72, June 2009, James Schantz DC 1 The Effects of Cox Decompression Technic in the Treatment of Low Back Pain and Sciatica in a Golf Professional James E. Schantz, D.C. Leading
Cox Technic Email Case Report 72, June 2009, James Schantz DC 1 The Effects of Cox Decompression Technic in the Treatment of Low Back Pain and Sciatica in a Golf Professional James E. Schantz, D.C. Leading
Low Back Pain. What is the deal? What We Will Talk About. Fact or Fiction? Fact or Fiction? Fact or Fiction? 2/19/2010
 What is the deal? Low Back Pain What You Need to Know Jonathan Clapp, MD, MS Colorado Comprehensive Spine Institute 3277 S. Lincoln St. Englewood, CO 80113 What We Will Talk About Facts and Fiction /Kinetic
What is the deal? Low Back Pain What You Need to Know Jonathan Clapp, MD, MS Colorado Comprehensive Spine Institute 3277 S. Lincoln St. Englewood, CO 80113 What We Will Talk About Facts and Fiction /Kinetic
Closed Automobile Insurance Third Party Liability Bodily Injury Claim Study in Ontario
 Page 1 Closed Automobile Insurance Third Party Liability Bodily Injury Claim Study in Ontario Injury Descriptions Developed from Newfoundland claim study injury definitions No injury Death Psychological
Page 1 Closed Automobile Insurance Third Party Liability Bodily Injury Claim Study in Ontario Injury Descriptions Developed from Newfoundland claim study injury definitions No injury Death Psychological
Herniated Disk in the Lower Back
 Nader M. Hebela, MD Fellow of the American Academy of Orthopaedic Surgeons http://orthodoc.aaos.org/hebela Cleveland Clinic Abu Dhabi Cleveland Clinic Abu Dhabi Neurological Institute Al Maryah Island
Nader M. Hebela, MD Fellow of the American Academy of Orthopaedic Surgeons http://orthodoc.aaos.org/hebela Cleveland Clinic Abu Dhabi Cleveland Clinic Abu Dhabi Neurological Institute Al Maryah Island
A review of spinal problems
 Dr Ulrich R Hähnle MD, FCS Orthopaedic Surgeon, Wits Facharzt für Orthopädie, Berlin Phone: +27 11 485 3236 Fax: +27 11 485 2446 Suite 102, Medical Centre, Linksfield Park Clinic P.O. Box 949, Johannesburg
Dr Ulrich R Hähnle MD, FCS Orthopaedic Surgeon, Wits Facharzt für Orthopädie, Berlin Phone: +27 11 485 3236 Fax: +27 11 485 2446 Suite 102, Medical Centre, Linksfield Park Clinic P.O. Box 949, Johannesburg
Return to same game if sx s resolve within 15 minutes. Return to next game if sx s resolve within one week Return to Competition
 Assessment Skills of the Spine on the Field and in the Clinic Ron Burke, MD Cervical Spine Injuries Sprains and strains Stingers Transient quadriparesis Cervical Spine Injuries Result in critical loss
Assessment Skills of the Spine on the Field and in the Clinic Ron Burke, MD Cervical Spine Injuries Sprains and strains Stingers Transient quadriparesis Cervical Spine Injuries Result in critical loss
SPINE AND NECK SURGERY: MAKING A DECISION THAT S RIGHT FOR YOU
 1. GET THE FACTS: Back and neck pain affects 8 out of 10 people at some point in their life. Acute back and neck pain comes on suddenly and usually lasts from a few days to a few weeks. Chronic back and
1. GET THE FACTS: Back and neck pain affects 8 out of 10 people at some point in their life. Acute back and neck pain comes on suddenly and usually lasts from a few days to a few weeks. Chronic back and
Standard of Care: Cervical Radiculopathy
 Department of Rehabilitation Services Physical Therapy Diagnosis: Cervical radiculopathy, injury to one or more nerve roots, has multiple presentations. Symptoms may include pain in the cervical spine
Department of Rehabilitation Services Physical Therapy Diagnosis: Cervical radiculopathy, injury to one or more nerve roots, has multiple presentations. Symptoms may include pain in the cervical spine
If you or a loved one have suffered because of a negligent error during spinal surgery, you will be going through a difficult time.
 If you or a loved one have suffered because of a negligent error during spinal surgery, you will be going through a difficult time. You may be worried about your future, both in respect of finances and
If you or a loved one have suffered because of a negligent error during spinal surgery, you will be going through a difficult time. You may be worried about your future, both in respect of finances and
THE LUMBAR SPINE (BACK)
") THE LUMBAR SPINE (BACK) At a glance Chronic back pain, especially in the area of the lumbar spine (lower back), is a widespread condition. It can be assumed that 75 % of all people have it sometimes or
THE LUMBAR SPINE (BACK) At a glance Chronic back pain, especially in the area of the lumbar spine (lower back), is a widespread condition. It can be assumed that 75 % of all people have it sometimes or
Back Pain Measure Group Patient Visit Form
 Please complete the form below for 20 unique patients meeting the patient sample criteria for the measure group. For the Back Pain Measure Group, patients you enter that have a diagnosis of back pain,
Please complete the form below for 20 unique patients meeting the patient sample criteria for the measure group. For the Back Pain Measure Group, patients you enter that have a diagnosis of back pain,
Biomechanical Basis of Lumbar Pain. Prepared by S. Pollak. Introduction:
 Biomechanical Basis of Lumbar Pain Prepared by S. Pollak Introduction: The lumbar area of the back is made up of five movable L1-L5 vertebrae which have intervertebral discs in between them 1. The intervertebral
Biomechanical Basis of Lumbar Pain Prepared by S. Pollak Introduction: The lumbar area of the back is made up of five movable L1-L5 vertebrae which have intervertebral discs in between them 1. The intervertebral
New York State Workers' Comp Board. Mid and Lower Back Treatment Guidelines. Summary From 1st Edition, June 30, 2010. Effective December 1, 2010
 New York State Workers' Comp Board Mid and Lower Back Treatment Guidelines Summary From 1st Edition, June 30, 2010 Effective December 1, 2010 General Principles Treatment should be focused on restoring
New York State Workers' Comp Board Mid and Lower Back Treatment Guidelines Summary From 1st Edition, June 30, 2010 Effective December 1, 2010 General Principles Treatment should be focused on restoring
Neck Pain Overview Causes, Diagnosis and Treatment Options
 Neck Pain Overview Causes, Diagnosis and Treatment Options Neck pain is one of the most common forms of pain for which people seek treatment. Most individuals experience neck pain at some point during
Neck Pain Overview Causes, Diagnosis and Treatment Options Neck pain is one of the most common forms of pain for which people seek treatment. Most individuals experience neck pain at some point during
Management of spinal cord compression
 Management of spinal cord compression (SUMMARY) Main points a) On diagnosis, all patients should receive dexamethasone 10mg IV one dose, then 4mg every 6h. then switched to oral dose and tapered as tolerated
Management of spinal cord compression (SUMMARY) Main points a) On diagnosis, all patients should receive dexamethasone 10mg IV one dose, then 4mg every 6h. then switched to oral dose and tapered as tolerated
Preventing & Treating Low Back Pain
 Preventing & Treating Low Back Pain An Introduction to Low Back Pain Low back pain is the number two reason that Americans see a health care practitioner second only to colds and flu. While most people
Preventing & Treating Low Back Pain An Introduction to Low Back Pain Low back pain is the number two reason that Americans see a health care practitioner second only to colds and flu. While most people
UPPER LUMBAR DISC HERNIATION WITH CENTRAL AND FAR LATERAL STENOTIC CHANGES RESULTING IN ANTERIOR THIGH PAIN
 Cox Technic Case Report #60 sent 5/13/08 1 UPPER LUMBAR DISC HERNIATION WITH CENTRAL AND FAR LATERAL STENOTIC CHANGES RESULTING IN ANTERIOR THIGH PAIN History, Examination & Imaging Review: A 53-year-old
Cox Technic Case Report #60 sent 5/13/08 1 UPPER LUMBAR DISC HERNIATION WITH CENTRAL AND FAR LATERAL STENOTIC CHANGES RESULTING IN ANTERIOR THIGH PAIN History, Examination & Imaging Review: A 53-year-old
 More information >>> HERE
More information >>> HERE MEDICAL PROTOCOLS: INTRODUCTION
 MEDICAL PROTOCOLS: INTRODUCTION JANUARY 1, 1996 REVISIONS & UPDATES: JULY 1, 2012; JULY 1, 2013; APRIL 1, 2014; APRIL 1, 2015; AUGUST 15, 2015 CONTENTS BACKGROUND NEW EFFECTIVE DATES FUTURE UPDATES ACKNOWLEDGMENTS
MEDICAL PROTOCOLS: INTRODUCTION JANUARY 1, 1996 REVISIONS & UPDATES: JULY 1, 2012; JULY 1, 2013; APRIL 1, 2014; APRIL 1, 2015; AUGUST 15, 2015 CONTENTS BACKGROUND NEW EFFECTIVE DATES FUTURE UPDATES ACKNOWLEDGMENTS
Lumbar Spinal Stenosis
 Lumbar Spinal Stenosis North American Spine Society Public Education Series What Is Lumbar Spinal Stenosis? The vertebrae are the bones that make up the lumbar spine (low back). The spinal canal runs through
Lumbar Spinal Stenosis North American Spine Society Public Education Series What Is Lumbar Spinal Stenosis? The vertebrae are the bones that make up the lumbar spine (low back). The spinal canal runs through
OUTLINE. Anatomy Approach to LBP Discogenic LBP. Treatment. Herniated Nucleus Pulposus Annular Tear. Non-Surgical Surgical
 DISCOGENIC PAIN OUTLINE Anatomy Approach to LBP Discogenic LBP Herniated Nucleus Pulposus Annular Tear Treatment Non-Surgical Surgical Facet Joints: bear 20% of weight Discs bear 80% of weight Neural Foramen
DISCOGENIC PAIN OUTLINE Anatomy Approach to LBP Discogenic LBP Herniated Nucleus Pulposus Annular Tear Treatment Non-Surgical Surgical Facet Joints: bear 20% of weight Discs bear 80% of weight Neural Foramen
1st Edition 2015. Quick reference guide for the management of acute whiplash. associated disorders
 1 1st Edition 2015 Quick reference guide for the management of acute whiplash associated disorders 2 Quick reference guide for the management of acute whiplash associated disorders, 2015. This quick reference
1 1st Edition 2015 Quick reference guide for the management of acute whiplash associated disorders 2 Quick reference guide for the management of acute whiplash associated disorders, 2015. This quick reference