NERVE CONDUCTION MANUAL
|
|
|
- Darrell Carr
- 10 years ago
- Views:
Transcription
1 NERVE CONDUCTION MANUAL James W. Albers, M.D., Ph.D Emeritus Professor of Neurology Electroneuromyography Laboratory Department of Physical Medicine and Rehabilitation University of Michigan Hospital Ann Arbor, Michigan Page 1 of 30

2 The normal values contained in the chart at the end of this manual (Table 1) for the various nerves have been determined for use in this laboratory and may vary from one laboratory to another. There are three parameters used in determining whether a conduction study is normal or abnormal. These parameters are amplitude of the MUAP, latency of the response, and conduction velocity. The motor amplitude represents the summation of the individual muscle fiber action potentials within that muscle and correlates highly with the number of viable axons. The amplitude is measured in millivolts from the baseline to the negative peak of the response obtained from supramaximal nerve stimulation (Figure 1). Sensory amplitude (peak-to-peak) is measured in microvolts and also correlates with the number of viable axons (Figure 2). The latency refers to the elapsed time between the start of the stimulus and the onset of the response. It represents the propagation of the impulse along the nerve, the transmission across the end-plate, and the depolarization of the muscle fibers. The latency is measured in milliseconds from the onset of the stimulus to the first negative deflection from the baseline in motor conduction (Figure 1) and to the peak of the response in sensory conduction (Figure 2). The conduction velocity is obtained by stimulating the nerve at two different points along the nerve at least 10 cm apart. To calculate the conduction velocity, the difference between the latencies onset obtained at the two points is divided by the distance between the two points. It is calculated in meters per second. Conduction velocity = Distance (cm) X 10 Latency 2 Latency 1 (msec) There are a number of problems and pitfalls encountered in performing nerve conduction studies. The most common pitfall occurs from incorrect measurement of nerve length caused by one of the following: 1. Stretching the skin while measuring 2. Not following the course of the nerve 3. Using a non-standard limb position Other common errors include the following: 1. Reversed polarity of the stimulating or recording electrodes 2. Active recording electrode not over the motor point of the muscle 3. Submaximal stimulation 4. Skin temperature below 32 C 5. Stimulus spread Page 2 of 30
.")
3 Another problem encountered in performing nerve conduction studies is artifact. The most common types are: 1. Stimulus artifact commonly caused by one of the following: a. Inadequate grounding b. High impedance of recording electrode contact with skin c. Inadvertent electrical connection between stimulating electrodes and ground or recording electrodes Hz interference commonly caused by one of the following: a. Fluorescent light b. IVAC or other electrical equipment in contact with the patient c. Ungrounded wall outlet 3. Movement artifact caused by poor patient relaxation When any of these problems are encountered the cause should be found and eliminated before proceeding with the nerve conduction study. Figure 1. Motor responses recorded distally (top) and proximally (bottom). S represents the stimulus, L1 (distal) and L2 (proximal) represent the latencies of the responses, and A represents the amplitude. Figure 2. Sensory response recorded distally. S represents the stimulus, L represents the latency of the response, and A represents the amplitude. Page 3 of 30

4 Median Nerve Course and Distribution Diagram of the Course and Distribution of the Median Nerve. The muscles supplied are indicated in italics. In the hand the cutaneous branches are marked by stipple, as is also the field of cutaneous innervation (see inset). The nerve indicated by 1 is the palmar cutaneous of the median nerve; and those by 2, the palmar digital nerves. The corresponding areas of cutaneous innervations are indicated in the inset. In some individuals the region of innervations of the dorsal aspect of the fingers in somewhat more proximal than indicated in this drawing. Page 4 of 30

5 Median Motor Conduction The active recording electrode is placed over the abductor pollicis brevis muscle as described below. A line is drawn across the palmar aspect of the wrist crease (1). A second line is drawn across the palmar surface of the first MCP joint at right angles to the axis of the first metacarpal (2). A third line connects the midpoint of the first two lines (3). It runs along the middle of the long axis of the thenar muscles. The midpoint of the third line is considered to be the center of the median innervated thenar muscles. The inactive electrode is placed over the thenar tendons on the lateral surface of the thumb. The ground is located over the dorsum of the wrist. The median nerve is stimulated approximately 2 cm proximal to the wrist crease between the flexor carpi radialis and palmaris longus tendons. The average distance is 7 cm from the cathodal stimulation site to the active recording electrode. The median nerve is stimulated proximally at the elbow between the biceps tendon and the medial epicondyle over the brachial pulse. Page 5 of 30

6 Median Sensory Conduction (Antidromic) Antidromic conduction. The recording electrodes are placed 3-4 centimeters apart on the index figure on the proximal and distal phalanxes. A ground is placed over the palm of the hand and the distal stimulation site is over the median nerve at the wrist between the flexor carpi radialis and palmaris longus tendons 14 cm from the active recording electrode. Median sensory nerve conduction velocity can be determined by stimulating proximally at the elbow as with the median motor nerve conduction velocity. Orthodromic conduction. The recording electrodes are placed 3-4 cm apart between the FCR and PL tendons, 14 cm away from the stimulating electrode. The stimulating electrodes are placed over the index finger or occasionally over the first or third digits, as described above. The ground is again placed on the palm. Page 6 of 30

7 Median Mid-palmar Sensory Conduction The recording electrodes are placed on the volar surface of the wrist between the flexor carpi radialis and palmaris longus tendons, with the active electrode located 8 cm proximal to the cathode of the stimulator and the inactive electrode placed 3-4 cm proximal to the active electrode. The ground is placed across the palm between the stimulator and recording electrodes. The stimulator is placed so that the cathode is in the center of the palm over the crease formed by palmar abduction of the thumb, and the anode is distal to the cathode. Page 7 of 30

8 Ulnar Nerve Course and Distribution The Origin and Distribution of the Ulnar Nerve, the Medial Cutaneous Nerve of the Forearm and the Medial Cutaneous Nerve of the Arm. The muscles supplied are indicated in italics. The patterns of the different nerves are duplicated in the inset. The numbered nerves are the following: 1, palmar branch; 2, dorsal branch; 3, superficial terminal branch; 4, deep terminal branch. The fields of innervation of cutaneous branches 1, 2, and 3 are illustrated in the inset. Page 8 of 30

9 Ulnar Motor Conduction The active recording electrode is placed over the hyprothenar muscles one-half way between the distal wrist crease across the ulnar border of the wrist and the distal traverse palmar crease across the ulnar border of the hand. The electrode is placed along this line over the highest prominence of the hypothenar muscle when viewed along its long axis. The inactive electrode is placed over the hypothenar tendon at the level of the M-P joint on the fifth digit. The ground strap is placed around the dorsum of the wrist. The ulnar nerve is stimulated distally 2 cm proximal to the wrist crease over the flexor carpi ulnaris tendon. The standard distance between the distal stimulation site and the recording electrode is 7 cm. The proximal stimulation site is over the ulnar nerve just proximal to the medial epicondyle at the elbow. Conduction velocition can also be determined by stimulating the ulnar nerve below the elbow and in the supraclavicular area (Erb s point). Page 9 of 30

10 Ulnar Sensory Conduction (Antidromic) Antidromic conduction. Sensory recording electrodes are placed on the proximal and distal phalanxes of the fifth digit 3-4 cm apart, the proximal electrode being the active recording electrode. The ulnar nerve is stimulated at the wrist 14 cm from the active recording electrode. Conduction velocities can be determined by stimulating the ulnar nerve at any proximal location such as the elbow, upper arm, or supraclavicular area (Erb s point). The ground strap is located on the palm. Orthodromic conduction. Stimulation is applied to the fifth digit using the recording electrode positions described above, the proximal electrode being the cathode. The ground is located on the palm and active recording electrode is located 14 cm from the cathode over the volar aspect of the wrist toward the flexor carpi ulnaris tendon. The inactive recording electrode is located 3-4 cm proximally. Page 10 of 30
.")
11 Radial Nerve Course and Distribution The Course and Distribution of the Radial Nerve. The patterns of the cutaneous nerves are duplicated in the inset. The names of the various muscles supplied by the radial are in italics. Page 11 of 30

12 Radial Motor Conduction The recording electrodes are placed over the extensor digitorum communis or the extensor indicis muscle with the active electrode over the belly of the muscle and the reference electrode at least 3 cm distal to the active electrode over the distal muscle tendon. A ground is placed over the dorsum of the wrist. The nerve can be stimulated distally at the elbow, lateral to the biceps tendon beneath the brachial radialis muscle and proximally on the lateral aspect of the arm at the spiral groove. Nerve conduction velocity can also be determined by stimulation of the radial nerve in the supraclavicular area (Erb s point). Proximal stimulation may be associated with an initial positive deflection of the CMAP because of activation of other muscles innervated by the radial nerve. Page 12 of 30
.")
13 Radial Sensory Conduction The active recording electrode is placed over the palpable portion of the superficial radial nerve. The nerve can be palpated over the extensor pollicis longus tendon. The inactive or reference electrode is placed 4 cm distally on the index finger. The ground is placed over the dorsum of the wrist. The nerve can be stimulated distally, two-thirds the distance down the forearm, over the dorsal edge of the radius. The stimulation site is approximately 10 cm from the active recording electrode. The nerve can be stimulated proximally at the elbow, lateral to the biceps tendon beneath the brachial radialis muscle. Page 13 of 30

14 Musculocutaneous Nerve Course and Distribution The Course and Distribution of the Musculocutaneous Nerve. The names of the muscles supplied by this nerve are in italics. The cutaneous distribution is indicated in the inset. Page 14 of 30

15 Musculocutaneous Motor Conduction The active recording electrode is placed over the mid-portion of the biceps brachii muscle. The inactive electrode is placed just proximal to the antecubital fossa over the biceps tendon. The ground is placed on the upper arm between the recording electrodes and the stimulator. The musculocutaneous nerve is stimulated at the axilla 13 cm proximal to the active recording electrode, and in the supraclavicular area (Erb s point). Page 15 of 30

16 Superficial Peroneal Nerve- Course and Distribution The Course and Distribution of the Superficial Peroneal Nerve. The names of the muscles innervated are in italics. The dotted pattern in the inset indicates the cutaneous field of the superficial peroneal nerve; the lined pattern that of a branch of the common peroneal nerve, the lateral cutaneous nerve of the calf. Page 16 of 30

17 Peroneal, Superficial (sensory-antidromic) / dorsum of foot Page 17 of 30
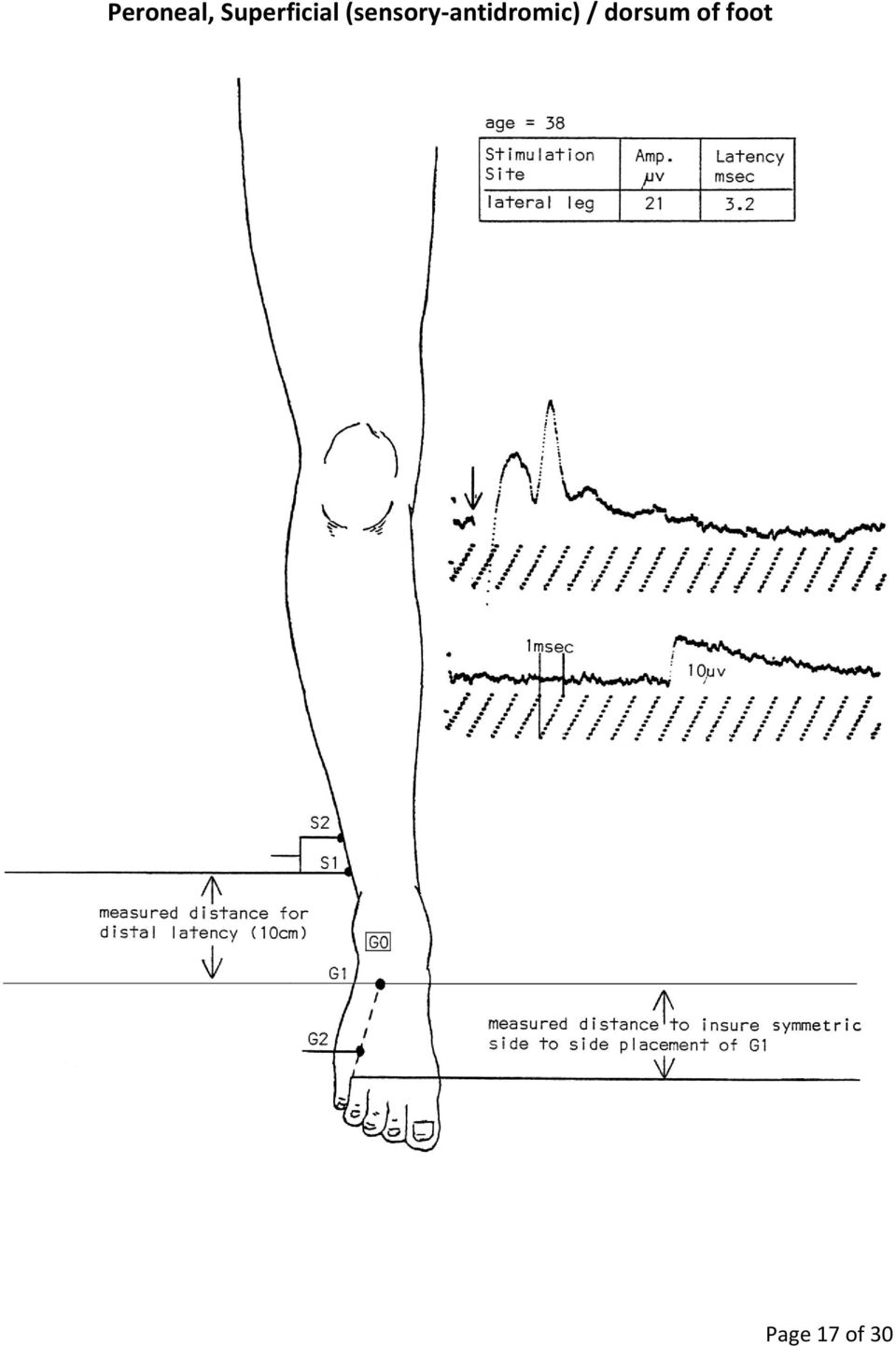
18 Peroneal Motor Conduction The active recording electrode is placed over the extensor digitorum brevis muscle approximately 1 cm distal to the bony prominence of the talus over the metatarsophalangeal joint. The reference electrode is placed over the lateral surface of the fifth digit. The ground electrode is placed over the dorsum of the ankle. The peroneal nerve can be stimulated distally over the anterior ankle, 2-5 cm lateral to the anterior tibial muscle, 5 cm proximal to the lateral malleolus. The distance between the distal stimulation site and the recording electrode is 9 cm. Occasionally, it will be necessary to stimulate the peroneal nerve posterior to the lateral malleolus near the sural nerve when there is an accessory deep peroneal nerve branch innervating the EDB muscle. The peroneal nerve is stimulated proximally at the knee over the palpable portion of the peroneal nerve in the lateral popliteal fossa 5 cm above the fibula head. Peroneal nerve conduction velocity can also be determined by stimulation 5 cm distal to the head of the fibula. Page 18 of 30

19 Peroneal (motor) / tibialis anterior Page 19 of 30

20 Posterior Tibial Nerve Course and Distribution The Course and Distribution of the Sciatic, Tibial, Posterior Tibial and Plantar Nerves. A dotted line marks the transition between tibial and posterior tibial nerves. The cutaneous fields of the medial calcanean and medial plantar nerves are indicated in the inset by lines; the field of the sural nerve and its lateral calcanean branch by dots; and that of the lateral plantar nerve, by crosshatch. The names of the muscles supplied are italicized. The numbered branches of the plantar nerves are as follows: 1, flexor digitorum brevis; 2, abductor hallucis; 3, flexor hallucis brevis; 4, 1 st lumbrical; 5, abductor digiti quinti; 6, flexor digitorum accessorius; 7, flexor digiti quinti brevis; 8, adductor hallucis; 9, interossei; 10, 2 nd 3 rd and 4 th lumbricals. In order to simplify, the sural nerve is indicated as arising solely from the tibial nerve; actually it usually receives an anastomotic branch from the common peroneal nerve. Page 20 of 30

21 Posterior Tibial Motor Conduction The active recording electrode is placed over the abductor hallucis muscle, 1 cm below and behind the navicular tubercle, 8 cm from the stimulating electrodes. The inactive electrode is placed on the muscle tendon at the level of the first digit. The ground is placed over the dorsum of the ankle. The nerve is stimulated distally behind and above the medial malleolus and proximally at the level of the knee in the lower border of the popliteal space near the popliteal artery. Page 21 of 30
22 H-reflex With the patient in a prone position, a horizontal line is drawn along the crease behind the knee. The active recording electrode is placed over the posterior aspect of the lower leg, onehalf the distance between the medial malleolus and the midpoint of the horizontal line. The inactive recording electrode is placed over the Achilles tendon. The posterior tibial nerve is stimulated orthodromically at the level of the knee in the lower border of the popliteal space. The ground is placed on the leg approximately half-way between the stimulator and the active recording electrode. The contralateral leg should be tested in the same manner as described above, taking care that the distance between the stimulating and recording electrodes is the same for the two legs. Page 22 of 30
23 Femoral Nerve Course and Distribution The Course and Distribution of the Femoral Nerve. The names of the muscles supplied by this nerve are in italics. The patterns of the cutaneous nerves are duplicated in the insets. In the field of the saphenous nerve the broken line represents the boundary between the fields of the infrapatellar and terminal branches. Page 23 of 30
24 Femoral Motor Conduction The active recording electrode is placed over the center of the vastus medialis muscle. The inactive electrode is placed at least 3-4 cm distal to the active electrode over the quadriceps tendon just proximal to the patella. The ground is placed on the leg half-way between the recording and stimulating electrodes. The site of stimulation is a point below the inguinal ligament and lateral to the femoral artery. Page 24 of 30
25 Sural Sensory Conduction The active recording electrode is placed immediately behind the lateral malleolus with the inactive electrode 3-4 cm away on the lateral surface of the foot. The ground is placed on the posterior lateral surface of the ankle. The nerve is stimulated on the posterior surface of the lower leg 1-3 cm lateral to the mid-line at 7, 14, and 21 cm from the recording electrodes. Page 25 of 30
26 Facial Motor Conduction The active recording electrode is placed on the orbicularis oculi muscle directly below the pupil with the patient looking straight ahead. The inactive recording electrode is placed on the bridge of the nose. The ground is placed on the forehead. The facial nerve is stimulated below the ear anterior to the mastoid process. Page 26 of 30
27 Phrenic Nerve Conduction The active recording electrode is placed over the eighth intercostal space. The inactive recording electrode is placed 3-5 cm distally. The ground is placed approximately 3 cm above the nipple. The phrenic nerve is stimulated at the posterior border of the sternomastoid muscles at the level of the upper edge of the thyroid cartilage. Page 27 of 30
28 Autonomic Nerve Response Two pairs of recording electrodes (infant ECG electrodes) are used. One pair is placed on the hand with the active electrode placed on the palm and the inactive electrode placed on the dorsum. The second pair is placed on the ipsilateral foot with the active electrode placed on the sole and the inactive electrode placed on the dorsum. The median nerve is stimulated orthodromically at the wrist on the contralateral side. The ground is placed on the forearm proximal to the stimulating electrode. The autonomic response is recorded from the hand and foot simultaneously. Page 28 of 30
29 Blink Reflex Two pairs of recording electrodes are used. The active recording electrodes are placed on the orbicularis oculi muscle bilaterally. The inactive recording electrodes are placed on the lateral surfaces of the nose. The ground is placed on the chin. The supraorbital nerve is stimulated with the cathode placed over the respective foramen on one side. The reflex responses are recorded from the orbicularis muscle on both sides simultaneously. Page 29 of 30
30 Spinal Accessory Nerve Page 30 of 30
31 months months (variable distance) Table 1 Normal Values UMMC 1-3 years years years (standard distance) Motor Conduction Neonate Median Amplitude Conduction Velocity Distal Latency Distance Ulnar Amplitude Conduction Velocity Distal Latency Distance Peroneal Amplitude Conduction Velocity Distal Latency Distance Tibial Amplitude Conduction Velocity Distal Latency Distance Sensory Conduction Median Amplitude >20 Conduction Velocity Distal Latency Distance Ulnar Amplitude >10 Conduction Velocity Distal Latency Distance Sural Amplitude Conduction Velocity >40 Distal Latency Distance years >60 years Standard Adult Normal Range
32 Table 2 Electrodes 1. Stimulating Electrodes a. DISA Bipolar surface electrode consisting of two felt tips in a plastic coated stainless steel holder with attached cable. b. TECA Bipolar surface electrode consisting of two metal rods mounted in an insulated plastic holder with potentiometer intensity control and attached cable. 2. Recording Electrodes a. TECA Two 10 mm stainless steel discs with connecting wires and phone tip plugs Two stainless steel digital rings with connecting wires and phone tip plugs Two 10 mm stainless steel discs in rigid plastic mount with connecting wires and phone tip plugs b. NDM Infant ECG electrode with snap-on cable (used for autonomic nerve response) 3. Grounds a. DISA Large surface electrode encased in felt with a Velcro strap and attached cable b. TECA Thirty millimeter stainless steel disc with attached cable
33 Updated K.A. Stolp-Smith, M.D. EMG Conference NERVE CONDUCTION STUDIES: PRINCIPLES, PROBLEMS, AND SOURCES OF ERROR I. PRINCIPLES OF NERVE CONDUCTION STUDIES A. STIMULATION 1. Electrodes a) Surface - silver plate, 0.5 to 0.1 cm in diameter b) Needle (EEG or monopolar) 2. Bipolar stimulation - both electrodes over nerve a) Cathode - negative pole (1) Attracts cations (2) Closest to recording site (3) Nerve depolarized b) Anode positive pole (1) Attracts anions (2) Furthest from recording site (3) Nerve hyperpolarized c) Current (1) Flows from anode to cathode (2) Negative charges accumulate under cathode and depolarize nerve d) Stimulator (1) Cathode and anode usually 2 to 3 cm apart Page 1 of 10
34 (2) Types: (a) (b) Constant voltage - current varies with skin, electrode impedance Constant current - current adjusts to impedance; better for serial assessment of level of shock intensity as a measure of nerve excitability. e) Stimulus (1) Intensity to 300 V (20 to 40 m A) for healthy nerve (2) Duration 0.05 to 1.0 msec (0.1 msec) for healthy nerve (3) Threshold - level required to achieve response, but not all axons activated (a) (b) Maximal - all axons activated Supramaximal - greater than maximal 3. Problems Encountered with Stimulation a) Cathode/Anode (1) Anodal block (a) (b) Clearly label anode and cathode Rotate anode off nerve (2) Avoid measurement from anode rather than cathode b) Stimulator (1) High skin impedance - grease, callous, edema (a) (b) (c) (d) Clean, dry skin Trim callous Rub skin with high conductance cream Use needle electrodes c) Stimulus (1) Submaximal stimulation - always use supramaximal Page 2 of 10
35 B. RECORDING (2) Submaximal stimulation - if large fibers are always activated initially, can measure latency of fastest fibers, however, relationship of stimulator to these fibers and length of the axonal terminals may alter this measurement; may achieve better stimulus placement with needles and can use less stimulus intensity (3) Avoid NCS in patients with CVP or Swan Ganz lines inserted directly in heart (4) Cardiac pacemakers - only consideration if using a large stimulus near the implantation site d) Stimulator Artifact 1. Electrodes a) Type (1) If stimulator and recording electrode too close together and recording electrodes too far apart (2) Overloading input (3) Can reduce surface spread of stimulation (4) Always place ground between stimulating and recording electrodes (1) Sensory nerves (a) (b) Surface Needle - increases amplitude, decreases noise (2) Motor nerves (a) Surface - advantage - records compound muscle action potential (CMAP) from all fibers innervated by nerve; onset = fastest fibers; amplitude = # of muscle fibers activated and the timing of their activation Page 3 of 10
36 (b) Needle - advantage - less interference from other muscles, so better CMAP take-off; good for proximal muscle that is difficult to isolate; disadvantage - only records small portion of CMAP b) Placement (1) Should remain constant (2) Motor nerve - over endplate 2. Instrument settings a) Sensory (1) Filters: 20 Hz-2 khz (2) Gain: uv b) Motor (1) Filters: 2 Hz-10 khz (2) Gain: 1-2 mv 3. Problems and Sources of Error a) Sensory recording (1) Signal within expected noise level (a) Averaging removes noise - degree of enhancement proportional to the square root of the # of trials, i.e. 4 trials gives double the response (2) Requires 100,000 x amplification which also amplified noise b) Motor recording (1) Moving fingers/contracting muscle - changes position of electrode over muscle belly - relaxation important (2) Initial positive deflection - electrode not over endplate (3) Avoid stretching skin Page 4 of 10
37 c) Sensory and motor recording (1) High skin impedance - clean off oils, trim callous, no smeared electrode paste; if edema - use needles (2) Excessive noise - poor ground, moisten ground; check for crossed wires, check gain and filter settings (3) Measurement errors (4) Temperature errors II. MOTOR NERVE CONDUCTION A. STIMULATION AND RECORDING 1. Electrodes a) Cathode closest to active (recording) electrode, G1 b) G1 over endplate c) G2 on tendon or bone d) Use supramaximal stimulation = 20-30% > maximal stimulation threshold B. CONDUCTION VELOCITY 1. Terminal/Distal Latency - Depends on: a) Integrity of nerve from point of stimulation to axon terminals b) Length of axon terminals c) Neuromuscular junction transmission d) Time for generation of muscle action potential 2. Calculation a) Measure distance between cathodes b) CV = Distance (mm) Latency (prox) Latency (dist) c) Conduction velocity is measured over main nerve trunk Page 5 of 10
38 3. CMAP C. SOURCES OF ERROR a) Latency - measured at take-off; corresponds to fastest nerve fibers b) Amplitude - baseline to negative peak; corresponds to number of muscle fibers activated 1. Proximal and distal waveforms differ a) Temporal dispersion - conduction block b) Submaximal stimulus or variable stimulus point-to-point c) Anomalous innervation 2. Small initial negative peak if high gain used - may arise from nerve; can ignore 3. Small positive dip a) G1 not over endplate b) Volume conduction from other muscles (1) Avoid stimulating more than one nerve (2) Consider anomalous innervation D. TYPES OF ABNORMALITIES - STIMULATING PROXIMAL TO LESION 1. Decreased amplitude, normal or slightly increased latency a) Neurapraxia or axonal loss - before onset of distal degeneration (3-4 days) 2. Amplitude normal, slow conduction velocity a) Segmental demyelination b) Temporal dispersion - will see decreased amplitude Page 6 of 10
39 3. Absent response a) Neurotmesis b) At 4-7 days - cannot tell if lesion neurapraxic or complete transection III. SENSORY NERVE CONDUCTION A. STIMULATION AND RECORDING 1. Orthodromic - more difficult to differentiate motor and sensory response especially if diseased nerve 2. Antidromic - larger response; easier to see B. AMPLITUDE, DURATION 1. Measure baseline to negative peak 2. Latency to peak 3. Amplitude a measure of the density of innervation C. CONDUCTION VELOCITY 1. Can calculate based on distal latency alone since NMJ time not a consideration 2. Amplitude drop of as much as 50% can occur with proximal stimulation - dispersion; both fast and slow fibers; SCV not necessarily a measure of fastest fibers 3. Use take-offs for CV calculation D. SOURCES OF ERROR 1. Improper stimulation or recording sites 2. Stimulus too high IV. VARIABILITY IN MEASUREMENT A. TEMPERATURE 1. CV increases m/s or 5% per degree between C sensory and motor nerves Page 7 of 10
40 B. AGE 2. Latency from the wrist to muscle increases 0.3 ms per degree for median and ulnar nerves 3. Amplitude increases if cool - temperature slows recovery period; preferential slowing of fast fibers 4. Duration increases 5. If skin is 34 C, muscle is approximately 37 C 6. The technician is not a thermometer 1. CV in full term infants is 50% than in adults; normal by age 3-5 years 2. Age 70-88: motor CV 15% slower than (Buchthal) 3. Age > 60: motor CV 10% slower than < age 60 (Wagman) 4. Median sensory amplitude age = 1/3 the sensory amplitude of age (Buchthal) C. VARIATION IN NERVES AND SEGMENTS 1. Both proximal and distal conduction velocities are slower in the lower extremities than upper extremities 2. Inverse relationship between height and CV 3. Median CV = ulnar CV; tibial CV < peroneal CV 4. CV > proximally than distally a) Decreasing axon diameter distally b) Colder distally c) Shorter internodal distance 5. F-wave stimulation - latency, cord-to-elbow = latency, elbow-to-hand 6. Other a) Few studies suggest differences due to gender? b) Hand dominance correlates with faster CV? c) Circadian rhythm? Page 8 of 10
41 D. GENERAL TROUBLESHOOTING QUESTIONS 1. No response a) Is stimulator delivering a stimulus? Check on technician. b) Check anatomical electrode placement c) Check skin and electrodes - lotion, saline, electrode paste - too much, too little d) Make sure you are using a supramaximal stimulus e) Check gain and filters 2. Muscle contraction but no response a) Is pre-amplifier on? b) Are electrodes plugged into pre-amplifier? Into correct preamplifier? c) Are connections between patient and EMG machine connected? d) Clean skin e) Increase sweep speed 3. Stimulus artifact a) Ground not functioning b) Ground near recording electrodes c) Clean skin REFERENCES 1. Albers JW, Donofrio PD, McGonagle TK: Sequential electrodiagnostic abnormalities in acute inflammatory demyelinating polyradiculoneuropathy. Muscle & Nerve 8: , Aminoff MJ: Electrodiagnosis in Clinical Neurology. Churchill Livingstone, New York, 1986, pp Jabre JF, Hackett ER: EMG Manual. Charles C. Thomas, Springfield, IL, pp Kimura J: Principles of Nerve Conduction Studies in Electrodiagnosis in Diseases of Nerve and Muscle: Principles and Practice. Philadelphia, F.A. Davis,1983, pp Page 9 of 10
42 5. Lambert EH: Measurement of Sensory and Motor Nerve Conduction Velocity in Man. From Notes for Neuromuscular Conference, October 29, Ma. DM: Nerve Conduction Handbook. FA Davis, Philadelphia, 1983, pp Miller RG, Kuntz, NL: Nerve conduction studies in infants and children. J Child Neurol 1:19-26, Oh SJ: Clinical Electromyography: Nerve Conduction Studies. University Park Press, Baltimore, 1984, pp Page 10 of 10
43
44
45 To determine which sensory nerve conduction studies (S-NCS) are helpful in detecting supraclavicular axon loss brachial plexopathies, we selected 53 cases (of 417 reviewed) in whom complicating factors were absent and which, by needle electrode examination findings, involved only a single truncal element (upper, middle, or lower) of the brachial plexus. Extensive S-NCS included: median, recording thumb (Med-Dl), index (Med-D2), and middle fingers (Med-D3); ulnar, recording fifth finger (Uln-D5); dorsal ulnar cutaneous, recording dorsum of the hand (DUC); radial, recording base of thumb; and both medial and lateral antebrachial cutaneous (MABC, LABC), recording forearm. Except for the median sensory fibers, the cord elements traversed by the sensory fibers assessed during the S-NCS listed above are anatomically defined (i.e., the sensory fibers enter the brachial plexus at only one cord). In regard to the median sensory fibers, however, there are two possible pathways through the infraclavicular plexus: (1) the lateral cord and/or (2) the medial cord. Because the lower trunk is only accessible via the medial cord, any sensory fibers found to be traversing the lower trunk had to first traverse the medial cord. Similarly, those traversing the upper and middle trunks must first be a component of the lateral cord. The frequency that the various S-NCS responses were abnormal (unelicitable, below laboratory normal value, or 60% of the contralateral response) for a given brachial plexus element lesion was as follows: (1) upper trunk (UT): 25 of 26 Med-D1, 25 of 26 LABC, 15 of 26 radial, 5 of 26 Med-D2, 2 of 26 Med-D3; (2) middle trunk (MT): 1 of 1 Med-D3; (3) lower trunk (LT): 25 of 26 Uln-D5, 22 of 23 DUC, 11 of 17 MABC, 3 of 23 Med-D3. With lower trunk brachial plexopathies, both routine (Uln-D5) and uncommon (DUC; MABC) S-NCS are abnormal. With upper trunk brachial plexopathies, in contrast, only the uncommon S-NCS (Med-D1 ; LABC) are consistently affected. The routine median S-NCS recording digit 2 (Med-D2) is far less reliable than the median S-NCS recording digit 1 (Med-D1) in detecting upper trunk axon loss brachial plexopathies. Additionally, the various pathways traversed by the fibers contributing to the individual S-NCS responses can be predicted, an important point when the full extent of a brachial plexus lesion is sought John Wiley & Sons, Inc. Key words: brachial plexus sensory nerve conduction MUSCLE 81 NERVE 18: THE UTILITY OF VARIOUS SENSORY NERVE CONDUCTION RESPONSES IN ASSESSING BRACHIAL PLEXOPATHIES MARK A. FERRANTE, MD, and ASA J. WILBOURN, MD INTRODUCTION From the EMG Laboratory. Neurology Department, Cleveland Clinic Foundation, Cleveland, Ohio This material was presented in part at the San Francisco AAEM meeting on 1 October Acknowledgment: We would like to thank Robert W. Shields, Jr., MD, and Erik P.J. Pioro, MD, PhD, for their helpful criticisms and suggestions. Address reprint requests to Asa J. Wilbourn, MD, Cleveland Clinic Foundation, EMG Department, Desk S-90,9500 Euclid Avenue, Cleveland, OH Accepted for publication March 15, Dawson4 introduced sensory nerve conduction studies (S-NCS) in He stimulated the digital nerves of the second and fifth fingers, while recording over the median and ulnar nerves at the wrist. In 1958, using these same orthodromic techniques, Gilliatt and Searsg showed that both the median and the ulnar sensory nerve action potentials (SNAPS) were unelicitable in the presence of diffuse axon loss brachial plexus (BP) lesions, while only the ulnar SNAP was affected by lower trunk CCC W95/ John Wiley & Sons, Inc. Utility of Sensory Responses MUSCLE & NERVE August
46 (LT) brachial plexopathies. Thus, they demonstrated that upper extremity S-NCS can be independently affected by focal brachial plexopathies. Nonetheless, most current textbooks and journal artic.es2. 13,17,21,22,27,30 concerned with the electrodiagnostic evaluation of the BP discuss upper extremity S-NCS primarily in regard to differentiating preganglionic (usually avulsion injuries) from postganglionic lesions, noting that the SNAP amplitudes are affected only by postganglionic axon loss. They also address electrodiagnostic evaluation of the terminal branch elements of the BP. Few sources, however, describe an approach for evaluating the various internal BP elements (i.e., trunks and cords), nor do they discuss the internal elements traversed by the sensory fibers studied during the various routine and uncommon S-NCS. Because none of the sensory fibers studied distally traverses all elements of the BP, it is not possible for a single S-NCS to assess the entire BP. Consequently, the individual S-NCS have the potential for providing localizing information with focal brachial plexopathies. While some authors have mentioned only the routine S-NCS (i.e., median, stimulatinghecording the index finger; ulnar, stimulatinglrecording the fifth finger) in regard to BP asse~sment,~ ~ others have discussed the importance of performing uncommon S-NCS for optimal assessment. ~6. s~24,25~31~32 Still, there have been no series published to validate these claims, nor any attempt to identify the trunk elements evaluated by the routine and uncommon S-NCS. For this reason, we designed this study to determine the BP trunk element traversed by the sensory fibers studied during the various S-NCS, so that the latter can be logically utilized in the assessment of focal axon loss brachial plexopathies. Because lesions involving the terminal elements (i.e., branches) and preganglionic elements (i.e., roots) are well discussed in other sources, we did not seek to identify them. Moreover, the cord elements traversed by the sensory fibers of the S-NCS assessed distally are anatomically defined (e.g., the LABC nerve derives from the lateral cord, the radial nerve from the posterior cord, and the ulnar and MABC nerves from the medial cord). The exception to this is the median nerve, which is composed of fibers from both the lateral and medial cords. Still, because the upper and middle trunks can contain median sensory fibers derived only from the lateral cord, and similarly the lower trunk can receive sensory fibers solely from the medial cord, whenever sensory fibers are shown to traverse a particular trunk element, the cord element they traverse is also defined. METHODS We retrospectively evaluated all electrodiagnostic studies performed at the Cleveland Clinic Foundation over the past 11 years that had been coded as a brachial plexopathy (n = 417). Our inclusion criterion was that each BP lesion be confined to a single trunk element (upper, middle, or lower), based on needle electrode examination (NEE), using established muscle domains (Table 1).12,15,16,23,26,330 ur exclusion criteria were: (1) evidence of any BP abnormalities not confined to a single trunk element (as noted); (2) any other neuromuscular lesion(s) (eg., coexisting carpal tunnel syndrome) in the affected limb; (3) plexopathies studied less than 2 1 days from weakness onset; and (4) any S-NCS abnormalities involving the contralateral limb; this latter exclusion criterion was applied because the SNAP responses were judged abnormal not only by their absolute values, but also by comparison to the SNAPS of the contralateral unaffected limb. Thus, changes in the contralateral S-NCS could obscure a S-NCS abnormality of the studied limb. In our study, NEE of a muscle was considered abnormal if it showed evidence of acute and/or chronic motor axon loss (MAL). Acute MAL is reflected by the presence of fibrillation potentials and a decreased recruitment pattern, whereas chronic MAL is reflected by changes in the external configuration (e.g., increased duration and sometimes amplitude) and a decreased recruitment pattern. Generally, the average duration for a given muscle must be increased by at least 50% before we consider it to be abnormal. Utilizing the NEE of these 417 brachial plexopathies, we were able to identify 53 lesions confined to a single Table 1. The muscle domains of the trunk elements Upper trunk Middle trunk Lower trunk ~ Supraspinatus lnfraspinatus Biceps Deltoid Teres minor Triceps Pronator teres Flex carpi radialis Brachioradialis Ext carpi radialis Gnator teres Flex carpi radialis Triceps Anconeus Ext carpi radialis Ext carpi ulnaris Ext digit communis Ext indicis proprius ~ ~~ Flex pollicis brevis Abd pollicis brevis Ext carpi ulnaris Ext digit cornmunis Ext pollicis brevis Ext indicis proprius Flex carpi ulnaris Flex digit prof45 Abd digiti rninirni First dorsal inteross This fabie is rnoditied from several published rnyotorne charts (Refs , 76, 23, 26, 33) 880 Utility of Sensory Responses MUSCLE & NERVE August 1995
47 trunk element of the BP: 26 upper trunk (UT); 1 middle trunk (MT); and 26 lower trunk (LT). The majority of BP lesions involving trunk elements were rejected from this study because more than a single trunk element was affected: combined UT and MT lesions, for example, were far more common than UT lesions alone, as were combined MT and LT lesions compared to LT lesions in isolation. Also, it is well known that MT lesions rarely occur in isolation, a point again confirmed by our study (discussed later). Thus, our rigid exclusion criteria necessitated rejection of approximately 87% of the brachial plexopathies reviewed. Of the 53 EMG examinations accepted into this study, all had had the following routine S-NCS performed: median sensory response, recording digit 2 (Med-D2); ulnar sensory response, recording digit 5 (Uln-D5); and radial sensory response, recording dorsum of the hand (radial). Where applicable, additional uncommon S-NCS were performed (all antidromically), using published techniques. These included median sensory responses, recording digit 1 (Med-D1) and digit 3 (Med-D3); dorsal ulnar cutaneous sensory response, recording dorsum of the hand (DUC); and medial and lateral antebrachial cutaneous sensory responses (MABC, LABC), recording forearm. All the S-NCS responses performed in these 53 patients with unilateral BP lesions were evaluated. Peak-to-peak amplitudes were measured from the trough of the first positive component to the peak of the aftercoming negative component. In the event that an initial positivity was not apparent, then the response amplitude was measured from the baseline to the peak of the initial negative component. In our EMG laboratory we utilize malleable lead grounds (approximately 20 X 2.5 cm) to help reduce shock artifact. In the event that shock artifact is noted, we utilize standard approaches to eliminate it. In all of our 53 cases, shock artifact was not a significant problem. We never found it necessary to resort to such techniques as electronic averaging. Abnormalities were identified when the SNAPS were: (1) unelicitable; (2) lower in amplitude than the previously established age-related normal laboratory control values; or (3) c50% lower in amplitude than that obtained from the corresponding study on the contralateral limb. It was then determined what effect each BP lesion had on the various S-NCS performed. The borderline amplitude decrements (>40%, but <50%) identified in Table 2 were considered as normals for all calculations. RESULTS Twenty-six UT lesions were identified using the NEE criteria outlined above. Both the LABC response and the Med-D1 responses were abnormal in 25 of 26 (96%) of these. The single normal Med-D 1 response was borderline low in amplitude, when compared with the contralateral limb study. The radial response was abnormal in 15 of 26 (58%). The Med-D2 response was abnormal in only 5 of 26 (19%), and was of borderline low amplitude in an additional 3 instances. The Med-D3 response was abnormal in 2 of 26 (8%). The Uln- D5 response was normal in all. These results are listed in Table 2. Only one MT lesion met the study criteria. The Med-D3 response was abnormal with it. The LABC, Med-D 1, Med-D2, radial, and Uln-D5 responses were normal (in this single study), although the Med-2 response was borderline low (47% amplitude decrement when compared to the contralatera1 side). These results are also listed in Table 2. Twenty-six LT lesions were identified. The Med-D3 response was abnormal in 3 of 23 (13%); of the 20 normal responses, 2 had borderline amplitude decrements (44%; 47%). Both the Uln- D5 and the DUC responses were abnormal in 96% (Uln-D5: 25 of 26; DUC: 22 of 23); the remaining Uln-D5 response showed a decrement of 43% when compared to the contralateral side, and was thus borderline low in amplitude. The MABC response was abnormal in 11 of 17 (65%) (see Discussion below). The following responses were within normal limits: LABC (n = 14), Med-D1 (n = 20), Med-D2 (n = 26), and radial (n = 26). These results are also listed in Table 2. DISCUSSION As pointed out by Stewart,25 knowing the origins of branches arising from the BP, and the muscles Table 2. The incidence of abnormal S-NCS responses with various BP element lesions. Abnormal response UT MT LABC Med-D1 25/ Med-D2 5/ * Med-D3 2/ Radial 15/ Uln-D DUC MABC *The normal response revealed a 46% amplitude decrement in comparison to the other side. jtwo of the normal responses revealed borderline amplitude decrements (44%, 47%). LT /23? /26 22/23 11/17 Utility of Sensory Responses MUSCLE & NERVE August
48 and cutaneous areas they supply, is important in the accurate localization of brachial plexopathies. Although S-NCS have been known to be useful in the electrodiagnostic evaluation of brachial plexopathies for over 35 years,g the potential for their anatomy to be applied electrodiagnostically has been underutilized. Axon loss lesions at the plexus level separate the sensory cell bodies in the dorsal root ganglia (DRG) from their peripheral projections (axons), causing the latter to undergo Wallerian degeneration. When these degenerated nerve fibers are a component of a sensory nerve assessed during S-NCS, they do not contribute to the SNAP and, consequently, its amplitude is decreased. With rather severe lesions the S-NCS responses become unelicitable. Because the sensory fibers assessed by a single S-NCS do not traverse all the BP elements, there is no single S-NCS capable of assessing all the BP elements simultaneously. Consequently, knowing the pathway through the plexus traversed by the sensory fibers assessed during S-NCS can he very helpful in BP evaluation. Each of the 53 cases included in this study was selected because it had NEE abnormalities restricted to muscles within the domain of just a single trunk element, as determined by various standard myotome charts. 12,15,16.23,26,33 The NEE abnormalities included fibrillation potentials, frequently accompanied by a neurogenic motor unit potential (MUP) firing pattern (decreased recruitment), and sometimes by chronic neurogenic MUP changes. The degree of acute versus chronic MAL is a reflection of the temporal relationship between the onset of symptoms and the time the NEE was performed. As stated previously, all studies were performed at least 3 weeks after the onset of weakness. Given that the S-NCS responses are much more susceptible to pathologic insult than are the M-NCS responses, the acuteness or chronicity of the NEE findings does not adversely influence our interpretation. Table 1 shows the muscle domains for the 3 trunk elements of the BP. It was derived from previously published studies ,23,26,33 dealing with the muscle domains of various root (i.e., anterior primary rami, APR) elements. Except for the relatively few peripheral nerves arising from the APR level of the BP (e.g., dorsal scapular nerve, long thoracic nerve), the trunk elements of the BP are direct continuations of the APR (i.e., the UT is formed by the fusion of the C5 and C6 APR, the MT is a direct continuation of the C7 APR, and the LT is formed by the fusion of the C8 and T1 APR).I4 Thus, the muscle domain of a given trunk element is equal to the muscle domain(s) of its contributing APR, minus the muscle domain(s) of the peripheral nerves (if any) given off at the APR level of the BP. The overlap in our table, like the overlap in the studies from which it was derived, reflects the fact that essentially all of the muscles sampled on NEE receive multisegmental innervation. Thus, in order to accurately localize axon loss BP lesions, one must be familiar with the muscle domains of all the BP elements. For example, if we noted NEE abnormalities in the supraspinatus, infraspinatus, deltoid, biceps, brachioradialis, and pronator teres muscles, the lesion was considered an UT brachial plexopathy. All of the above muscles receive motor axons from the C5 and C6 segments of the spinal cord, except for the pronator teres, which receives motor axons from the C6 and C7 segments. Thus, motor axons innervating the pronator teres traverse both the UT and the MT. Given that no abnormalities were noted in any other muscles of the MT muscle domain, we considered it unlikely that the lesion was affecting both the UT and the MT; rather, we assumed it involved the UT in isolation and the pronator teres contained fibrillation potentials because of its C6/UT innervation. A second, more complex example of this reasoning process, is that of the single MT lesion identified in this study. Note in Table 1 that 4 of the muscles listed in the MT muscle domain are also listed in the UT muscle domain, and that 3 of them also appear in the LT muscle domain. Because it lies between 2 other trunk elements, its muscles are for the most part shared. It becomes important, therefore, to sample the unshared muscles of both the upper and lower trunks. If they are all spared, and only if they are all spared, then the possibility that the lesion is a mixed trunk element lesion is quite remote, since it is very unlikely that involvement of a second trunk element would affect only those motor nerve fascicles innervating muscles found in both domains, while sparing the unshared muscles. Our MT case went to surgery, based in part on our electrodiagnostic examination, and was found to have a fibrotic process of unknown etiology involving solely the MT. The overlap seen in the MT muscle domain is analogous to that seen in the C7 APR muscle domain (as expected given that it is a direct continuation of that root), and we are unaware of any electromyographers who consider it impossible to make a diagnosis of a C7 radiculopathy. Thus, the rarity of an isolated MT lesion is not due to the complexity involved in making the electrodiagnosis. Although the muscle domains of 882 Utility of Sensory Responses MUSCLE & NERVE August 1995
49 the BP elements overlap, the shared muscles are important in evaluating the full extent of a brachial plexopathy, so we elected to utilize them in our search for focal lesions. Moreover, we were concerned that excluding such lesions would result in a selection bias toward more partial (i.e., less severe) BP element lesions. Less severe lesions would be more likely to spare the sensory fibers studied by the various S-NCS and could adversely affect our results. We are well aware of the limitations of this approach. First, variations in BP anatomy (both vertical and horizontal variations) could conceivably have an affect on both the NEE and the NCS findings.5,1o,28,34.35 p erhaps the most discussed BP anomaly is that of pre- and post-fixation.29 It is interesting to note, however, that with these vertical anomalies, while the root contribution of the trunk elements changes, the plexus arrangement itself remains the same. Thus, although the sensory fibers derive from an adjacent DRG (either the one above or the one below the typical DRG), the pattern of NCS and NEE abnormalities would localize to the same BP element. Regarding horizontal variations, Leffert14 has reported that the trunk elements are seldom anomalous, the M T being a direct extension of the C7 APR in 10096, and the UT and LT being of classical formation in >90% and >95%, respectively. A second limitation of this study is that we often were unable to verify that the BP trunk element identified electrodiagnostically was truly the pathological site of involvement. Neuroimaging studies (which were not performed on all patients) usually were not helpful because they are not sensitive enough to permit lesion identification confined to a single trunk element. Similarly, operative verification that only one BP element was involved was not possible because only a minority of our patients underwent surgical exploration (e.g., the MT case). Yet electromyographers are called upon to assess all BP lesions, regardless of whether or not they are surgically explored. Moreover, even if all patients underwent surgical confirmation, electrodiagnostic evaluation would still be required preoperatively, and thus the dilemma would remain. We, like other authors before us, did the next best thing. We correlated all of our electrodiagnostic impressions with the clinical examinations. In addition to credible histories of a focal BP lesion, all 53 cases had clinical examination features consistent with involvement of the BP element ultimately diagnosed by NEE. The NEE either confirmed the clinical impression or further refined it. While our brachial plexopathy series represents a biased population (i.e., focal brachial plexopathies), their etiologies were varied: trauma (18), true neurogenic thoracic outlet syndrome (lo), post median sternotomy (open heart surgery) (7), neoplastic (4), neuralgic amyotrophy (3), post irradiation treatment (l), iatrogenic (l), neurofibromatosis type I (l), and unknown (8). Of note is that in the 3 patients with neuralgic amyotrophy, both the clinical and NEE features were suggestive of an UT BP lesion and not, as is more often the case, one or more proximal monone~ropathies.~ The individual S-NCS and the likely course of their sensory fibers through the BP will next be discussed. The LABC Response. The lateral antebrachial cutaneous nerve is the terminal portion of the musculocutaneous nerve, derived from the LC of the BP. Consequently, by anatomical definition, the cord element traversed by the sensory fibers assessed by the LABC S-NCS is the lateral cord. Thus only LC lesions, but not PC or MC lesions, have the potential to affect the LABC S-NCS at the cord level of the BP. With regard to the trunk elements that the LABC fibers traverse, they could traverse the upper trunk, the middle trunk, or both. Since the LABC response was abnormal in 25 of 26 UT lesions, our results suggest that they traverse predominantly the UT. Our study did not adequately assess the MT, since only one MT lesion was identified. However, Inouye and Buchthal recorded spinal nerve potentials evoked by stimulation of the sensory fibers of the musculocutaneous nerve and showed that the maximum amplitude occurred at the C6 root, while Yoss and coworkers35 have shown that C6, but not C5, radiculopathies cause sensory symptoms in the lateral forearm (i.e., in the sensory distribution of the LABC nerve). These studies support our finding that the predominant course taken through the BP for those sensory fibers assessed by the LABC S-NCS is the LC and the UT. They also suggest that the sensory axons assessed by the LABC SNAP have their cell bodies of origin in the C6 DRG cells. Importantly, the LT element of the BP is not assessed by the LABC sensory response (nor are the MC or PC). Figure 1 illustrates the suggested pathway. The Med-Dl Response. The median nerve is composed of fibers derived from both the LC and the MC. Because the Med-D1 response was abnormal in 25 of 26 UT lesions, 0 of 1 MT lesion, and 0 of Utility of Sensory Responses MUSCLE & NERVE August
50 I, c5 ROOTS p p ~ dorsal scapular n. TERMINAL NERVES med. antebrach. cutaneous n. radial n. FIGURE 1. Proposed brachial plexus pathway for the sensory fibers assessed by the LABC SNAP. 20 LT lesions, our study suggests that the Med-D1 SNAP is elicited from fibers that traverse the UT (and LC). Whether or not some of the fibers it assesses sometimes traverse the MT could not be determined by this study because only a single MT lesion was identified. Of importance is that the LT, MC, and PC elements of the BP are not assessed by the Med-D1 sensory response. Figure 2 illustrates the suggested pathway. The Med-D2 Response. The Med-D2 SNAP was abnormal in 5 of 26 UT lesions, although 3 of 21 normal responses were borderline low in amplitude when compared to the contralateral side (see Table 2). The Med-D2 SNAP was abnormal with 0 of 1 MT lesion, but this response was borderline low in amplitude (47%) compared to that found in the contralateral limb (see Table 2). The Med-D2 SNAP was abnormal with 0 of 26 LT lesions. Even though only one MT lesion was available for evaluation (borderline low in amplitude), the absolute lack of involvement of the Med-D2 SNAP with LT lesions coupled with the rather minimal involvement (32% at most, if borderline low amplitudes are included as abnormal) with UT lesions suggests, by default, that the MT is the trunk element most often traversed by the sensory fibers supplying the index finger. However, due to the limited number of MT lesions in our study, no definite conclusions can be drawn. Nonetheless, it is pertinent to note that while we were collecting the 53 isolated trunk element lesions included in this study, we rejected dozens of plexopathies in which the Med-D2 response was abnormal because, on NEE, abnormalities were present outside of the predefined MT muscle domain (i.e., they were UTiMT or MTiLT lesions). Thus, the Med-D2 response assesses the UT in a minority of patients, _ ROOTS, p p ~ dorsal scapular n. k,? ERG., suprascapular n. /,... I2.-- I /- TERMINAL >.. 1 L meo. anreoracn. cutaneous 0. radial n. Ulnarn. median n. FIGURE 2. Proposed brachial plexus pathway for the sensory fibers assessed by the Med-D1 SNAP. 884 Utility of Sensory Responses MUSCLE i3 NERVE August 1995
51 presumably the MT in most patients, and the LC in all patients. Importantly, the LT (along with the MC and the PC) element is not assessed by the Med-D2 response. Figure 3 illustrates the suggested pathway. The Med-DB Response. The Med-D3 SNAP was abnormal in 2 of 26 UT lesions, 1 of 1 MT lesion, and 3 of 23 LT lesions (2 of the 20 normal with LT lesions were borderline low in amplitude, 44% and 47%, compared to the other side) (see Table 2). These findings suggest that the sensory fibers supplying the middle finger can traverse the UT, MT, and/or LT elements. Because our study showed that the Med-D3 response was seldom affected with isolated UT lesions, it is probable that the sensory axons subserving this response derive primarily from the C7 DRG and therefore traverse the MT. However, because only one isolated MT lesion was included in this study, no definite conclusions are possible. Nonetheless, analogous to the circumstances surrounding the Med-D2 response, we found that the Med-D3 response was typically abnormal with combined UT and MT brachial plexopathies, as well as with combined MT and LT lesions. This again suggested that the MT is the predominant trunk element traversed by the sensory fibers contributing to the Med-D3 SNAP. The major difference between the Med-D2 and the Med-D3 responses was that the latter was abnormal with 13% of the LT lesions, revealing, contrary to past beliefs, that the median sensory axons contributing to the Med-D3 SNAP sometimes pass through the MC and the LT elements of the BP on their way to their DRG cell bodies of origin. The suggested pathways are shown in Figure 4. The Radial Responses. The radial sensory response was abnormal with 15 of 26 (58%) lesions involving the UT, 0 of 1 affecting the MT, and 0 of 26 involving the LT. As with the Med-D2 and Med-D3 responses, accurately determining the MT contribution was not possible, because only 1 MT lesion was identified. However, the fact that the radial SNAP was abnormal in only 58% of UT lesions suggests that this is not the only trunk element these fibers traverse. Moreover, the fact that the radial SNAP was normal in all 26 LT lesions indicates that the LT is not the additional trunk element traversed. By default, these results suggest that the MT serves as an important conduit for radial sensory fibers approximately 42% of the time. Supporting this concept is that the radial SNAP frequently was abnormal both with combined UT/MT lesions and with combined MT/LT lesions, two categories of BP lesions not included in this study. This concept is also supported by the work of Inouye and Buchthal, who showed that the maximum amplitude response with radial nerve stimulation occurred at the C6 and C7 roots, suggesting that the UT and MT function as pathways for these fibers. Thus, the radial sensory fibers appear to traverse both the UT and the MT (the particular pathway varying from patient to patient) as well as the PC. Importantly, the radial sensory fibers do not traverse the LT, MC, or LC. Figure 5 depicts the suggested pathways. By anatomic def- The Uln-DS and DUC Responses. inition, the sensory fibers contributing to the Uln- D5 and the DUC SNAPS must traverse the MC and the LT BP elements. Thus, it is not surprising that the Uln-D5 SNAP was abnormal in 25 of 26 LT /-- -^.I ROOTS TERMINAL med. antebrach. cutaneous n. radial n. FIGURE 3. Proposed brachial plexus pathway for the sensory fibers assessed by the Med-DP SNAP. Utility of Sensory Responses MUSCLE & NERVE August
52 med. antebrach. \.. -\ I cutaneous n. I Ulnal n. median n. radial n. FIGURE 4. Proposed brachial plexus pathway for the sensory fibers assessed by the Med-D3 SNAP. lesions, with the only normal response showing a borderline amplitude decrement compared to the other side. The DUC SNAP was abnormal in 22 of 23 LT lesions. Thus, our results confirm the undisputed fact that the Uln-D5 and DUC SNAPs evaluate the MC and LT elements of the BP; they do not assess the UT, MT, LC, or PC. We did not perform a DUC S-NCS on any of our UT patients, because the sensory fibers subserving this response are known not to traverse the UT, and the studies, as is, were already quite timeconsuming. Moreover, as these data show, the DUC S-NCS response was always abnormal whenever the Uln-D5 S-NCS response was abnormal; and we did perform an Uln-D5 S-NCS in all 53 of these patients (and thus in all 26 of the UT lesions). As suspected, it was never involved. The MABC Response. The medial antebrachial cutaneous nerve originates from the MC, which is continuous with the LT. By anatomical definition, the MABC SNAP should assess fibers that traverse the LT element of the BP. Our study confirmed this, showing abnormal MABC SNAPs in 11 of 17 LT lesions. However, a pertinent question arises: Why were only two thirds of the MABC sensory responses affected by the LT lesions if this is the only trunk element traversed by these sensory fibers? First, it is important to note that all the LT plexopathies in which the normal MABC response occurred had the same etiology: postmedian sternotomy. These particular LT plexopathies (i.e., those associated with median sternotomy) differ from most other LT lesions in that they consistently affect the ulnar motor and sensory fibers disproportionately more than they affect the C8/ T1 median motor fibers and the MABC fibers. We believe this occurs because these lesions actually involve primarily the C8 APR rather than the LT itself. Conversely, we believe that the lesion char- ROOTS TERMINAL ulnar n. median n. radial n. FIGURE 5. Proposed brachial plexus pathway for the sensory fibers assessed by the radial SNAP. 886 Utility of Sensory Responses MUSCLE & NERVE August 1995
53 20% acteristic of true neurogenic thoracic outlet syndrome (TN-TOS) actually involves primarily the T1 APR rather than the LT. Both Maggiano et al. and Nishida et a1.,20 in separate reports dealing almost exclusively with TN-TOS, have reported consistently finding MABC response abnormalities with these lesions. The operative results Gilliatt reported (34 patients) are also consistent with this conclusion ; he noted that usually the C8 and T1 APR crossed the congenital taut band (extending from the tip of the rudimentary cervical rib to the first thoracic rib) and that the T 1 APR appeared to be more affected. With TN-TOS the electrodiagnostic findings are typically the obverse of those found with postmedian sternotomy: the median motor NCS and the MABC NCS are severely involved, while the ulnar sensory NCS, and particularly the ulnar motor NCS, are less affected. Thus in TN-TOS, the ulnar sensory NCS response, while absolutely or relatively low in amplitude, is rarely unelicitable, whereas the MABC response is typically unelicitable. We did not perform a MABC S-NCS in any of the UT cases because it would be anatomically impossible for these fibers to traverse that element of the BP. CONCLUSIONS A number of conclusions regarding both the anatomy of the BP and the optimal method for assessing it with S-NCS can be derived from this study. Regarding anatomy, some previously held concepts apparently are incorrect regarding the various BP elements traversed by the median sensory fibers supplying the digits. First, the index finger digital nerves seldom derive from the UT. By default, it appears that they usually originate from the C7 DRG cells, and pass through the M T to the LC, rather than arising from the C6 DRG cells and traversing the UT to the LC. Second, probably not all the median digital nerve fibers traverse the lateral cord. The fact that the Med-D3 SNAP occasionally (1 3%) was abnormal with LT lesions, suggests that the middle finger is sometimes supplied by median sensory fibers derived from the C8 DRG, via the LT and MC elements of the BP. Regarding the optimal use of the S-NCS for assessing brachial plexopathies, we conclude the following: --:* LABC RADIAL UT - 96%\ MT - 0% UT MT (?42%) 5:\ LT 0% LT -,-,, Med - D1 UT - 96% MT- 0% LT - 0% c5& L 7 49 \/ With possible UT lesions, the routine Med- D2 study is inadequate. Either the LABC SNAP, the Med-D1 SNAP, or both, should be performed. In our EMG laboratory, we usually perform a combination of motor and sensory NCS (our UT package ) consisting of the LABC sensory, the Med-D1 sensory, the musculocutaneous motor (recording biceps), and the axillary motor (recording deltoid) studies. Our routine assessment also includes the radial SNAP, which may also be helpful in approximately 58% of UT lesions. With possible MT lesions, the Med-D2 and the Med-D3 S-NCS appear to be optimal; although the radial S-NCS may also be abnormal (42%). With possible LT or MC lesions only one ulnar S-NCS, Uln-D5 or DUC, needs to be UT ~ Med - D2 MT - (780%) LT - 0% Med - D3 - UT - 0% MABC DUC LT - 65% LT - 96% UT- 0% MT - 0% LT - 96% FIGURE 6. Illustration of the incidence of S-NCS involvement for the supraclavicular brachial plexus elements. Utility of Sensory Responses MUSCLE & NERVE August
54 performed since the axons assessed by both traverse identical BP elements and therefore yield identical results. Except for lesions resulting from median sternotomy, the MABC S-NCS is also an excellent S-NCS for assessing these BP elements. In our EMG laboratory, we usually perform a combination of S-NCS and M-NCS when assessing patients with possible LTiMC lesions (our LT package ) consisting of the following: Uln-D5, MABC, median motor (recording APB), and ulnar motor (recording ADM and frequently FDI as well). We have recently omitted the DUC response because, in this study, its results so closely paralleled the results of the Uln-D5 response. 4. Although the Med-D4 sensory response was not utilized in this study, it may be useful for demonstrating LT brachial plexopathies. Conceivably, it could be very helpful in differentiating LT lesions from ulnar nerve lesions in the postmedian sternotomy patients with LT plexopathies predominantly affecting ulnar nerve fibers. This is the population of LT lesions in which the MABC response is notoriously spared, probably because the lesion actually involves the C8 APR. 5. With possible LC lesions, the LABC, Med- D1, Med-D2, and usually the Med-D3 responses should be affected while the radial response should always be unaffected. Thus, like the muscle domains of the individual BP elements, there exist S-NCS domains for each of the BP elements (see Fig. 6). Although there also exist M-NCS domains for each of the BP elements, they are not as helpful for localization due to the limited number of M-NCS available and to their considerable overlap. We find M-NCS to be more useful in assessing the severity of the lesion (a direct reflection of their amplitude decrements). REFERENCES 1. Aminoff MJ, Olney RK, Parry GJ, Raskin NH: Relative utility of different electrophysiologic techniques in the evaluation of brachial plexopathies. Neurology 1988;38: Benecke R, Conrad B: The distal sensory nerve action potential as a diagnostic tool for the differentiation of lesions in dorsal roots and peripheral nerves. J Neurol 1980;223: Daube JR: Nerve conduction studies, in Aminoff MJ (ed): Electrodiagnosis in Clinical Neurology, 2nd ed. New York, Churchill Livingstone, 1986, pp Dawson GD: The relative excitability and conduction velocity of sensory and motor nerve fibers in man.j Physioll956; 131:43& DeJong RN: The Neurologzcal Examination, 2nd ed. New York, Hoeber and Harper, 1958, p Eisen AA: The electrodiagnosis of plexopathies, in Brown WF, Bolton CF (eds): Clinical Electromyography, 2nd ed. Boston, Butterworth-Heinemann, 1993, pp England JD, Sumner AJ: Neuralgic amyotrophy: an increasingly diverse entity. Muscle Nerve 1987;10: Gilliatt RW: Thoracic Outlet Syndromes, in Dyck PJ, Thomas PK (eds): Peripheral Neuropathy, 2nd ed. Philadelphia, Saunders, 1984, pp Gilliatt RW, Sears TA: Sensory nerve action potentials in patients with peripheral nerve lesions. J Neural Neurosurg Psychiatry 1958;21: Goss CM: Gray s Anatomy, 29th American edition. Philadelphia, Lea and Febiger, 1973, p 962. Inouye Y, Buchthal F: Segmental sensory innervation determined by potentials recorded from cervical spinal nerves. Brain 1977;100: Kendall FP, McCreary EK, Provance PG: Muscles: Testing and Function, 4th ed. Baltimore, Williams and Wilkins, 1993, pp Kimura J: Assessment of individual nerves, in Electrodiagnosis in Diseases of Nerve and Muscle: Principles and Practice, 2nd ed. Philadelphia, Davis, 1989, pp Leffert RD: Brachial Plexus Injuries. New York, Churchill Livingstone, 1985, pp Liveson JA: Peripheral Neurology: Case Studies in Electrodiagnosis. 2nd ed. Philadelphia, Davis, 1992, pp 3W2. Liveson JA, Ma DM: Laboratory Reference for Clinical Neurophysiology. Philadelphia, Davis, 1991, pp Liveson JA, Ma DM: Laboratory Reference for Clinical Neuro- physiology. Philadelphia, Davis, 1992, pp Ma DM, Wilbourn AJ, Kraft GH: Unusual sensory conduction studies (2nd ed), an American Association of Electrodiagnostic Medicine Workshop; Rochester, MN, AAEM, 1992, pp Maggiano H, Levin KH, Wilbourn AJ: Relationship between the medial antebrachial cutaneous sensory and median motor responses in brachial plexopathies [abstract]. MuscleNerue 1993;16: Nishida T, Price SJ, Minieka MM: Medial antebrachial cutaneous nerve conduction in true neurogenic thoracic outlet syndrome. Electromyogr Clin Neurophysiol 1993;33: Oh SJ: Anatomical guide for common nerve conduction studies, in Clinical Electromyography Nerve Conduction Studies, 2nd ed. Baltimore, Williams and Wilkins, 1993, pp Olney RK, Wilbourn AJ: Sensory nerve conduction study workshop, in Course 150, American Academy of Neurology Annual Meeting, Perotto AO: Anatomical Guide for the Electromyographer: The Limbs and Trunk, 3rd ed. Springfield, Charles Thomas, DD I I I 24. Rubin M, Lange DJ: Sensory nerve abnormalities in bra- chial plexopathy. Eur Neurol 1992;32: Stewart JD: Focal Perapheral Neuropathies. New York, Elsevier, 1987, p Stewart JD: Focal Peripheral Neuropathies, 2nd ed. New York, Raven Press, 1993, p Sunderland S: Nerves and Nerve Injuraes. New York, Churchill Livingstone, 1978, pp Sunderland S: Nerves and Nerve Injuries. New York, Churchill Livingstone, 1978, p Swash M: Diagnosis of brachial root and plexus lesions. J Neurol 1986;233: Wilbourn AJ: Electrodiagnosis of plexopathies. Neurologzc Clinics 1985;233: Wilbourn AJ: Iatrogenic brachial plexopathies: Clinical 888 Utility of Sensory Responses MUSCLE & NERVE August 1995
55 and EMG features. In 1990 American Association of Electrodiagnostic Medicine Course D: Electrodiagnosis vf Iatrogenic Neurvpathies. Rochester, MN, AAEM, 1990, pp Wilbourn AJ: Brachial Plexus Disorders, in Dyck PJ, Thomas PK (eds): Peripheral Neuropathy, 3rd ed. Philadelphia, Saunders, 1993, pp Wilbourn AJ, Aminoff AJ: Radiculopathies, in Brown WF, Bolton CF (eds): Clinical Electrvmyvgraphy, 2nd ed. Boston, Butterworth-Heinemann, 1993, pp Williams PL, Warwick R (eds): Gray s Anatomy, 36th British edition. New York, Churchill Livingstone, 1980, pp Yoss RE, Kendall BC, MacCarty CS, Love JC: Significance of symptoms and signs in localization of involved root in cervical disk protrusion. Neurology 1957;7: Utility of Sensory Responses MUSCLE & NERVE August
56 Machine settings Sensory Sensitivity 20 uv Time base 2 ms per division Filters 20 Hz/2kHz or 3kHz Motors Sensitivity 5 mv Time base 2 ms per division Filters 2 Hz/10kHz F-waves UE 500 uv sensitivity 5ms time base LE 500 uv sensitivity 10ms time base Needle Filters 20 Hz/10 khz Begin at 50 uv to look at insert ional activity
Carpal Tunnel Syndrome, an overview
 Carpal Tunnel Syndrome, an overview Jim Lewis, R.NCS.T. Learning Objectives: Median nerve compression at the wrist is the most common entrapment seen in the electrodiagnostic laboratory. Although it is
Carpal Tunnel Syndrome, an overview Jim Lewis, R.NCS.T. Learning Objectives: Median nerve compression at the wrist is the most common entrapment seen in the electrodiagnostic laboratory. Although it is
3nd Biennial Contemporary Clinical Neurophysiological Symposium October 12, 2013 Fundamentals of NCS and NMJ Testing
 3nd Biennial Contemporary Clinical Neurophysiological Symposium October 12, 2013 Fundamentals of NCS and NMJ Testing Peter D. Donofrio, M.D. Professor of Neurology Vanderbilt University Medical Center
3nd Biennial Contemporary Clinical Neurophysiological Symposium October 12, 2013 Fundamentals of NCS and NMJ Testing Peter D. Donofrio, M.D. Professor of Neurology Vanderbilt University Medical Center
Ulnar Neuropathy Differential Diagnosis and Prognosis. Disclosures: None
 Ulnar Neuropathy Differential Diagnosis and Prognosis Disclosures: None Goals of Lecture Describe anatomy: sites of entrapment Ulnar nerve Discuss differential diagnosis of ulnar nerve pathology Identify
Ulnar Neuropathy Differential Diagnosis and Prognosis Disclosures: None Goals of Lecture Describe anatomy: sites of entrapment Ulnar nerve Discuss differential diagnosis of ulnar nerve pathology Identify
Differentiating Cervical Radiculopathy and Peripheral Neuropathy. Adam P. Smith, MD
 Differentiating Cervical Radiculopathy and Peripheral Neuropathy Adam P. Smith, MD I have no financial, personal, or professional conflicts of interest to report Radiculopathy versus Neuropathy Radiculopathy
Differentiating Cervical Radiculopathy and Peripheral Neuropathy Adam P. Smith, MD I have no financial, personal, or professional conflicts of interest to report Radiculopathy versus Neuropathy Radiculopathy
ELECTRODIAGNOSTIC MEDICINE
 ELECTRODIAGNOSTIC MEDICINE OBJECTIVES BEGINNER Patient Care Perform a comprehensive electrodiagnostic evaluation of each patient and to provide a concise diagnosis and plan for further treatment Describe
ELECTRODIAGNOSTIC MEDICINE OBJECTIVES BEGINNER Patient Care Perform a comprehensive electrodiagnostic evaluation of each patient and to provide a concise diagnosis and plan for further treatment Describe
Aetna Nerve Conduction Study Policy
 Aetna Nerve Conduction Study Policy Policy Aetna considers nerve conduction velocity (NCV) studies medically necessary when both of the following criteria are met: 1. Member has any of the following indications:
Aetna Nerve Conduction Study Policy Policy Aetna considers nerve conduction velocity (NCV) studies medically necessary when both of the following criteria are met: 1. Member has any of the following indications:
International Standards for the Classification of Spinal Cord Injury Motor Exam Guide
 C5 Elbow Flexors Biceps Brachii, Brachialis Patient Position: The shoulder is in neutral rotation, neutral flexion/extension, and adducted. The elbow is fully extended, with the forearm in full supination.
C5 Elbow Flexors Biceps Brachii, Brachialis Patient Position: The shoulder is in neutral rotation, neutral flexion/extension, and adducted. The elbow is fully extended, with the forearm in full supination.
The Carpal Tunnel CTS. Stålberg 1. Dysfunction of median nerve in the carpal tunnel resulting in
 The Carpal Tunnel CTS Dysfunction of median nerve in the carpal tunnel resulting in 1 Symptoms in CTS pain and numbness in the abd worse on finger activity aggravated by forceful gripping g symptoms more
The Carpal Tunnel CTS Dysfunction of median nerve in the carpal tunnel resulting in 1 Symptoms in CTS pain and numbness in the abd worse on finger activity aggravated by forceful gripping g symptoms more
EMG and the Electrodiagnostic Consultation for the Family Physician
 EMG and the Electrodiagnostic Consultation for the Family Physician Stephanie Kopey, D.O., P.T. 9/27/15 The American Association of Neuromuscular & Electrodiagnostic Medicine (AANEM) Marketing Committee
EMG and the Electrodiagnostic Consultation for the Family Physician Stephanie Kopey, D.O., P.T. 9/27/15 The American Association of Neuromuscular & Electrodiagnostic Medicine (AANEM) Marketing Committee
Medical Report Checklist: Upper Extremities Peripheral Nerve Disorders Impairments (PND)
") http://www.pdratings.com/ Craig Andrew Lange [email protected] California Workers Compensation Certified AMA Guides Impairment & Disability Rating Specialists Voice: (415) 861-4040 / Fax: (415) 276-3741
http://www.pdratings.com/ Craig Andrew Lange [email protected] California Workers Compensation Certified AMA Guides Impairment & Disability Rating Specialists Voice: (415) 861-4040 / Fax: (415) 276-3741
CTS the Best EDX. Ernest W Johnson MD Emeritus Professor Physical Medicine & Rehabilitation The Ohio State University
 CTS the Best EDX Ernest W Johnson MD Emeritus Professor Physical Medicine & Rehabilitation The Ohio State University 1 Definition of CTS A syndrome 2d to dysfunction of median nerve in carpal tunnel resulting
CTS the Best EDX Ernest W Johnson MD Emeritus Professor Physical Medicine & Rehabilitation The Ohio State University 1 Definition of CTS A syndrome 2d to dysfunction of median nerve in carpal tunnel resulting
LATE RESPONSES IN MEDIAN NERVE ENTRAPMENT NEUROPATHY IN THE CARPAL TUNNEL
 Bulletin of the Transilvania University of Braşov Series VI: Medical Sciences Vol. 7 (56) No.2-2014 LATE RESPONSES IN MEDIAN NERVE ENTRAPMENT NEUROPATHY IN THE CARPAL TUNNEL A. M. GALAMB 1 I. D. MINEA
Bulletin of the Transilvania University of Braşov Series VI: Medical Sciences Vol. 7 (56) No.2-2014 LATE RESPONSES IN MEDIAN NERVE ENTRAPMENT NEUROPATHY IN THE CARPAL TUNNEL A. M. GALAMB 1 I. D. MINEA
Brachial Plexopathy, an overview
 Brachial Plexopathy, an overview Learning Objectives: The brachial plexus is the network of nerves that originate from cervical and upper thoracic nerve roots and eventually terminate as the named nerves
Brachial Plexopathy, an overview Learning Objectives: The brachial plexus is the network of nerves that originate from cervical and upper thoracic nerve roots and eventually terminate as the named nerves
Chapter 7 The Wrist and Hand Joints
 Chapter 7 The Wrist and Hand Manual of Structural Kinesiology R.T. Floyd, EdD, ATC, CSCS Many Archery, Relate wrist require sports require precise functioning of flexion, & hand & hand functional combined
Chapter 7 The Wrist and Hand Manual of Structural Kinesiology R.T. Floyd, EdD, ATC, CSCS Many Archery, Relate wrist require sports require precise functioning of flexion, & hand & hand functional combined
Manual of Nerve Conduction Studies. Second Edition
 Manual of Nerve Conduction Studies Second Edition This page intentionally left blank Manual of Nerve Conduction Studies Second Edition Ralph M. Buschbacher, MD Nathan D. Prahlow, MD Indiana University
Manual of Nerve Conduction Studies Second Edition This page intentionally left blank Manual of Nerve Conduction Studies Second Edition Ralph M. Buschbacher, MD Nathan D. Prahlow, MD Indiana University
Hemiplegic shoulder pain/shoulder subluxation
 UPPER LIMB NEUROMUSCULAR ELECTRICAL STIMULATION: Electrode positions Please note that the polarity (red and black leads) can be altered according to your clinical reasoning. The area in which you want
UPPER LIMB NEUROMUSCULAR ELECTRICAL STIMULATION: Electrode positions Please note that the polarity (red and black leads) can be altered according to your clinical reasoning. The area in which you want
Automated Analysis of Electromyography Data
 Automated Analysis of Electromyography Data Jeffrey L. Sponsler, MD, MS Alaska Brain Center, LLC 4551 E Bogard Rd Wasilla, AK 99654 ABSTRACT Background: Interpretation of nerve conduction studies (NCS)
Automated Analysis of Electromyography Data Jeffrey L. Sponsler, MD, MS Alaska Brain Center, LLC 4551 E Bogard Rd Wasilla, AK 99654 ABSTRACT Background: Interpretation of nerve conduction studies (NCS)
AMA Guides & California Code of Regulations P&S Report Checklist
 http://www.pdratings.com/ AMA Guides & California Code of Regulations P&S Report Checklist [L.C. 139.2 (J)-(2)&(3), (k)-(5), 4060(b)(1), 4062 (d)(2), 4068, 4620, 8 CCR WCAB 10606 & 8 CCR 9785] AMA Brachial
http://www.pdratings.com/ AMA Guides & California Code of Regulations P&S Report Checklist [L.C. 139.2 (J)-(2)&(3), (k)-(5), 4060(b)(1), 4062 (d)(2), 4068, 4620, 8 CCR WCAB 10606 & 8 CCR 9785] AMA Brachial
Basic Concepts. Focal and Entrapment Neuropathies and EMG. Pathophysiology. Median Nerve. A Clinical Approach
 Basic Concepts Focal and Entrapment Neuropathies and EMG A Clinical Approach Nerves predisposed by a narrow anatomic pathway or superficial course are most susceptible May occur acutely, intermittantly,
Basic Concepts Focal and Entrapment Neuropathies and EMG A Clinical Approach Nerves predisposed by a narrow anatomic pathway or superficial course are most susceptible May occur acutely, intermittantly,
Nerve conduction studies
 clinical William Huynh Matthew C Kiernan Nerve conduction studies This article forms part of our Tests and results series for 2011 which aims to provide information about common tests that general practitioners
clinical William Huynh Matthew C Kiernan Nerve conduction studies This article forms part of our Tests and results series for 2011 which aims to provide information about common tests that general practitioners
Chapter 2 Carpal Tunnel Syndrome, Electroneurography, Electromyography, and Statistics
 Chapter 2 Carpal Tunnel Syndrome, Electroneurography, Electromyography, and Statistics After reading this chapter you should: Know what basic techniques are employed in electroneurography Know what basic
Chapter 2 Carpal Tunnel Syndrome, Electroneurography, Electromyography, and Statistics After reading this chapter you should: Know what basic techniques are employed in electroneurography Know what basic
EXTENSOR POLLICIS TENDONITIS SYNDROME
 EXTENSOR POLLICIS TENDONITIS SYNDROME The extensor pollicis longus muscle has its origin on the lateral part of the middle third of the ulnar shaft on the dorsal border below the abductor pollicis longus
EXTENSOR POLLICIS TENDONITIS SYNDROME The extensor pollicis longus muscle has its origin on the lateral part of the middle third of the ulnar shaft on the dorsal border below the abductor pollicis longus
Muscles of the Forearm and Hand
 8 Muscles of the Forearm and Hand 132 PRONATOR TERES Strengthening exercises Pronation with strength bar Self stretches Weight of stick increases supination via gravity PRONATOR TERES 133 Latin, pronate,
8 Muscles of the Forearm and Hand 132 PRONATOR TERES Strengthening exercises Pronation with strength bar Self stretches Weight of stick increases supination via gravity PRONATOR TERES 133 Latin, pronate,
Entrapment and Compressive Neuropathies
 Entrapment and Compressive Neuropathies Barbara E. Shapiro, MD, PhD*, David C. Preston, MD KEYWORDS Entrapment neuropathy Compressive neuropathy Entrapment and compressive neuropathies of the upper and
Entrapment and Compressive Neuropathies Barbara E. Shapiro, MD, PhD*, David C. Preston, MD KEYWORDS Entrapment neuropathy Compressive neuropathy Entrapment and compressive neuropathies of the upper and
Billing and Coding Guidelines: NEURO-005 Nerve Conduction Studies and Electromyography. Contractor Name Wisconsin Physicians Service (WPS)
") Billing and Coding Guidelines: NEURO-005 Nerve Conduction Studies and Electromyography Contractor Name Wisconsin Physicians Service (WPS) Contractor Number 00951, 00952, 00953, 00954 05101, 05201, 05301,
Billing and Coding Guidelines: NEURO-005 Nerve Conduction Studies and Electromyography Contractor Name Wisconsin Physicians Service (WPS) Contractor Number 00951, 00952, 00953, 00954 05101, 05201, 05301,
Name of Policy: Neuromuscular and Electrodiagnostic Testing (EDX): Nerve Conduction Studies (NCS) and Electromyography (EMG) Studies
: Nerve Conduction Studies (NCS) and Electromyography (EMG) Studies") Name of Policy: Neuromuscular and Electrodiagnostic Testing (EDX): Nerve Conduction Studies (NCS) and Electromyography (EMG) Studies Policy #: 228 Latest Review Date: August 2015 Category: Medicine Policy
Name of Policy: Neuromuscular and Electrodiagnostic Testing (EDX): Nerve Conduction Studies (NCS) and Electromyography (EMG) Studies Policy #: 228 Latest Review Date: August 2015 Category: Medicine Policy
EMG AND NCS: A PRACTICAL APPROACH TO ELECTRODIAGNOSTICS
 EMG AND NCS: A PRACTICAL APPROACH TO ELECTRODIAGNOSTICS Dr. Harp Sangha, Dr. Tania R. Bruno Staff Physiatrists Toronto Rehab UHN Lecturers, Department of Medicine University of Toronto February 1, 2013
EMG AND NCS: A PRACTICAL APPROACH TO ELECTRODIAGNOSTICS Dr. Harp Sangha, Dr. Tania R. Bruno Staff Physiatrists Toronto Rehab UHN Lecturers, Department of Medicine University of Toronto February 1, 2013
Diagnostic MSK Case Submission Requirements
 Diagnostic MSK Case Submission Requirements Note: MSK Ultrasound-Guided Interventional Procedures (USGIP) is considered a separate specialty. Corresponds with 4/21/16 Accred Newsletter* From the main site:
Diagnostic MSK Case Submission Requirements Note: MSK Ultrasound-Guided Interventional Procedures (USGIP) is considered a separate specialty. Corresponds with 4/21/16 Accred Newsletter* From the main site:
Electrodiagnostic Assessment: An Introduction to NCS and EMG
 Electrodiagnostic Assessment: An Introduction to NCS and EMG Barry Bernacki BSc MD FRCPC CSCN (EMG) Clinical Asst. Professor EMG Lab Director Saskatoon City Hospital Objectives Understand technique and
Electrodiagnostic Assessment: An Introduction to NCS and EMG Barry Bernacki BSc MD FRCPC CSCN (EMG) Clinical Asst. Professor EMG Lab Director Saskatoon City Hospital Objectives Understand technique and
The wrist and hand are constructed of a series of complex, delicately balanced joints whose function is essential to almost every act of daily living.
 TOPIC OUTLINE 9- THE WRIST AND HAND. Introduction. The wrist and hand are constructed of a series of complex, delicately balanced joints whose function is essential to almost every act of daily living.
TOPIC OUTLINE 9- THE WRIST AND HAND. Introduction. The wrist and hand are constructed of a series of complex, delicately balanced joints whose function is essential to almost every act of daily living.
Structure & Function of the Ankle and Foot. A complicated model of simplicity that you really think little about until you have a problem with one.
 Structure & Function of the Ankle and Foot A complicated model of simplicity that you really think little about until you have a problem with one. The Foot and Ankle Terminology Plantar flexion Dorsi flexion
Structure & Function of the Ankle and Foot A complicated model of simplicity that you really think little about until you have a problem with one. The Foot and Ankle Terminology Plantar flexion Dorsi flexion
Anatomical Consideration and Brachial Plexus Anesthesia. Anatomy
 Brachial Plexus Anesthesia There are four approaches to the brachial plexus. These include the interscalene, supraclavicular, infraclavicular, and axillary approach. For the purposes of this lecture we
Brachial Plexus Anesthesia There are four approaches to the brachial plexus. These include the interscalene, supraclavicular, infraclavicular, and axillary approach. For the purposes of this lecture we
Elbow, Forearm, Wrist, & Hand. Bony Anatomy. Objectives. Bones. Bones. Bones
 Objectives Elbow, Forearm, Wrist, & Hand Chapter 19 Identify and discuss the functional anatomy of the elbow and forearm Discuss the common injuries associated with these anatomical structures Bones Humerus
Objectives Elbow, Forearm, Wrist, & Hand Chapter 19 Identify and discuss the functional anatomy of the elbow and forearm Discuss the common injuries associated with these anatomical structures Bones Humerus
a) Nerve conduction studies (NCS) test the peripheral nervous system for:
 Nerve conduction studies (NCS) test the peripheral nervous system for:") Health Plan Coverage Policy ARBenefits Approval: 11/02/2011 Effective Date: 01/01/2012 Revision Date: 09/18/2013 Comments: Code additions only. Title: Electrodiagnostic Testing Document: ARB0256 Public
Health Plan Coverage Policy ARBenefits Approval: 11/02/2011 Effective Date: 01/01/2012 Revision Date: 09/18/2013 Comments: Code additions only. Title: Electrodiagnostic Testing Document: ARB0256 Public
The Electrodiagnosis of Cervical and Lumbosacral Radiculopathy
 Neurol Clin 25 (2007) 473 494 The Electrodiagnosis of Cervical and Lumbosacral Radiculopathy Bryan Tsao, MD* Department of Neurology, Loma Linda University, 11175 Campus Street, Loma Linda, CA 92354, USA
Neurol Clin 25 (2007) 473 494 The Electrodiagnosis of Cervical and Lumbosacral Radiculopathy Bryan Tsao, MD* Department of Neurology, Loma Linda University, 11175 Campus Street, Loma Linda, CA 92354, USA
Neuromuscular Medicine Fellowship Curriculum
 Neuromuscular Medicine Fellowship Curriculum General Review Goals and Objectives Attend weekly EMG sessions as assigned Take a Directed History and Exam of each EMG patient Attend every other week Muscle
Neuromuscular Medicine Fellowship Curriculum General Review Goals and Objectives Attend weekly EMG sessions as assigned Take a Directed History and Exam of each EMG patient Attend every other week Muscle
Muscles of Mastication
 Muscles of Mastication Masseter Zygomatic Arch Mandibular angle Elevates mandible Mandibular ramus Temporalis Temporal fossa of the temporal bone Coronoid process of the mandible Elevates mandible Retracts
Muscles of Mastication Masseter Zygomatic Arch Mandibular angle Elevates mandible Mandibular ramus Temporalis Temporal fossa of the temporal bone Coronoid process of the mandible Elevates mandible Retracts
Most active and intricate part of the upper extremity Especially vulnerable to injury Do not respond well to serious trauma. Magee, 2008. pg.
 PTA 216 Most active and intricate part of the upper extremity Especially vulnerable to injury Do not respond well to serious trauma Magee, 2008. pg. 396 28 bones Numerous articulations 19 intrinsic muscles
PTA 216 Most active and intricate part of the upper extremity Especially vulnerable to injury Do not respond well to serious trauma Magee, 2008. pg. 396 28 bones Numerous articulations 19 intrinsic muscles
Reflex Physiology. Dr. Ali Ebneshahidi. 2009 Ebneshahidi
 Reflex Physiology Dr. Ali Ebneshahidi Reflex Physiology Reflexes are automatic, subconscious response to changes within or outside the body. a. Reflexes maintain homeostasis (autonomic reflexes) heart
Reflex Physiology Dr. Ali Ebneshahidi Reflex Physiology Reflexes are automatic, subconscious response to changes within or outside the body. a. Reflexes maintain homeostasis (autonomic reflexes) heart
Electroneuromyographic studies
 Electroneuromyographic studies in the diagnosis of Pudendal Entrapment Syndrome BY NAGLAA ALI GADALLAH PROFESSOR OF PHYSICAL MEDICINE, RHEUMATOLOGY& REHABILITATION AIN SHAMS UNIVERSITY Pudendal neuralgia
Electroneuromyographic studies in the diagnosis of Pudendal Entrapment Syndrome BY NAGLAA ALI GADALLAH PROFESSOR OF PHYSICAL MEDICINE, RHEUMATOLOGY& REHABILITATION AIN SHAMS UNIVERSITY Pudendal neuralgia
LOW BACK PAIN EXAMINATION
 LOW BACK PAIN EXAMINATION John Petty, M.D. Medical Director Department of Physical Medicine & Rehabilitation Kettering Medical Center February 8, 2014 PRE-TEST QUESTION What part of the low back physical
LOW BACK PAIN EXAMINATION John Petty, M.D. Medical Director Department of Physical Medicine & Rehabilitation Kettering Medical Center February 8, 2014 PRE-TEST QUESTION What part of the low back physical
9/11/12. EMG for OPAs. Amy Eswein, MSPT. Evaluation of Peripheral Nerve Injuries. Exam has two parts:! Nerve Conduction Study! Needle EMG!
 EMG for OPAs Amy Eswein, MSPT Evaluation of Peripheral Nerve Injuries Exam has two parts:! Nerve Conduction Study! Needle EMG! 1 Nerve Conduction Study Latency/NCV! State of the MYELIN Amplitude! State
EMG for OPAs Amy Eswein, MSPT Evaluation of Peripheral Nerve Injuries Exam has two parts:! Nerve Conduction Study! Needle EMG! 1 Nerve Conduction Study Latency/NCV! State of the MYELIN Amplitude! State
Ankle Block. Indications The ankle block is suitable for the following: Orthopedic and podiatry surgical procedures of the distal foot.
 Ankle Block The ankle block is a common peripheral nerve block. It is useful for procedures of the foot and toes, as long as a tourniquet is not required above the ankle. It is a safe and effective technique.
Ankle Block The ankle block is a common peripheral nerve block. It is useful for procedures of the foot and toes, as long as a tourniquet is not required above the ankle. It is a safe and effective technique.
Muscle Movements, Types, and Names
 Muscle Movements, Types, and Names A. Gross Skeletal Muscle Activity 1. With a few exceptions, all muscles cross at least one joint 2. Typically, the bulk of the muscle lies proximal to the joint it crossed
Muscle Movements, Types, and Names A. Gross Skeletal Muscle Activity 1. With a few exceptions, all muscles cross at least one joint 2. Typically, the bulk of the muscle lies proximal to the joint it crossed
5/13/2013. Evaluation of Peripheral Nervous System Dysfunction. Disclosures. Peripheral Nervous System
 Evaluation of Peripheral Nervous System Dysfunction Christian M. Custodio, M.D. Cancer Rehabilitation Fellowship Director Memorial Sloan-Kettering Cancer Center Assistant Professor Weill Cornell Medical
Evaluation of Peripheral Nervous System Dysfunction Christian M. Custodio, M.D. Cancer Rehabilitation Fellowship Director Memorial Sloan-Kettering Cancer Center Assistant Professor Weill Cornell Medical
CERVICAL DISC HERNIATION
 CERVICAL DISC HERNIATION Most frequent at C 5/6 level but also occur at C 6 7 & to a lesser extent at C4 5 & other levels In relatively younger persons soft disk protrusion is more common than hard disk
CERVICAL DISC HERNIATION Most frequent at C 5/6 level but also occur at C 6 7 & to a lesser extent at C4 5 & other levels In relatively younger persons soft disk protrusion is more common than hard disk
WHEN TO ORDER; HOW TO INTERPRET
 ELECTROMYOGRAPHY AND 1 NERVE CONDUCTION TESTING: WHEN TO ORDER; HOW TO INTERPRET Ronald N. Kent, M.D., Ph.D. 2 ELECTROMYOGRAPHY AND NERVE CONDUCTION TESTING EMG/NCS Testing is a component of a complete
ELECTROMYOGRAPHY AND 1 NERVE CONDUCTION TESTING: WHEN TO ORDER; HOW TO INTERPRET Ronald N. Kent, M.D., Ph.D. 2 ELECTROMYOGRAPHY AND NERVE CONDUCTION TESTING EMG/NCS Testing is a component of a complete
Coding for Difficult Tendon Repairs and Transfers. Current Procedural Terminology 2013 American Medical Association. All Rights Reserved.
 Coding for Difficult Tendon Repairs and Transfers Rotator Cuff Repair 23420 February 2002 page 11 Code 23420 describes a repair of a complete shoulder (rotator) cuff avulsion, referring to the repair of
Coding for Difficult Tendon Repairs and Transfers Rotator Cuff Repair 23420 February 2002 page 11 Code 23420 describes a repair of a complete shoulder (rotator) cuff avulsion, referring to the repair of
Multifocal Motor Neuropathy. Jonathan Katz, MD Richard Lewis, MD
 Multifocal Motor Neuropathy Jonathan Katz, MD Richard Lewis, MD What is Multifocal Motor Neuropathy? Multifocal Motor Neuropathy (MMN) is a rare condition in which multiple motor nerves are attacked by
Multifocal Motor Neuropathy Jonathan Katz, MD Richard Lewis, MD What is Multifocal Motor Neuropathy? Multifocal Motor Neuropathy (MMN) is a rare condition in which multiple motor nerves are attacked by
The Reflex Arc and Reflexes Laboratory Exercise 28
 The Reflex Arc and Reflexes Laboratory Exercise 28 Background A reflex arc represents the simplest type of nerve pathway found in the nervous system. This pathway begins with a receptor at the dendrite
The Reflex Arc and Reflexes Laboratory Exercise 28 Background A reflex arc represents the simplest type of nerve pathway found in the nervous system. This pathway begins with a receptor at the dendrite
How To Know If You Can Get A Carpal Tunnel Injury Compensation
 U. S. DEPARTMENT OF LABOR Employees Compensation Appeals Board In the Matter of BARBARA SNYDER and DEPARTMENT OF THE TREASURY, INTERNAL REVENUE SERVICE, Germansville, PA Docket No. 03-1467; Submitted on
U. S. DEPARTMENT OF LABOR Employees Compensation Appeals Board In the Matter of BARBARA SNYDER and DEPARTMENT OF THE TREASURY, INTERNAL REVENUE SERVICE, Germansville, PA Docket No. 03-1467; Submitted on
Compression Neuropathies. Andrew Martin DO, MBA, CAQSM OMED 2013
 Compression Neuropathies Andrew Martin DO, MBA, CAQSM OMED 2013 Compression Neuropathies Carpal Tunnel Syndrome Cubital Tunnel Syndrome Spinal Accessory Nerve Upper/Lower Trunk Plexopathy Long Thoracic
Compression Neuropathies Andrew Martin DO, MBA, CAQSM OMED 2013 Compression Neuropathies Carpal Tunnel Syndrome Cubital Tunnel Syndrome Spinal Accessory Nerve Upper/Lower Trunk Plexopathy Long Thoracic
Internet Journal of Medical Update
 Internet Journal of Medical Update 2010 July;5(2):15-20 Internet Journal of Medical Update Journal home page: http://www.akspublication.com/ijmu Original Work Early diagnosis of Carpal Tunnel Syndrome
Internet Journal of Medical Update 2010 July;5(2):15-20 Internet Journal of Medical Update Journal home page: http://www.akspublication.com/ijmu Original Work Early diagnosis of Carpal Tunnel Syndrome
The Symptomatic Upper Extremity: An Algorithmic Approach to Diagnosis, Part 2
 Journal of the American Chiropractic Association May 1999 The Symptomatic Upper Extremity: An Algorithmic Approach to Diagnosis, Part 2 By David J. Schimp, DC, DACNB, DAAPM Dorsal scapular nerve entrapment:
Journal of the American Chiropractic Association May 1999 The Symptomatic Upper Extremity: An Algorithmic Approach to Diagnosis, Part 2 By David J. Schimp, DC, DACNB, DAAPM Dorsal scapular nerve entrapment:
Radiculopathy vs. Peripheral Neuropathy. What to do with arm pain? Defining Arm Pain. Arm Pain
 Radiculopathy vs. Peripheral Neuropathy What to do with arm pain? Miriana G. Popadich RN, MSN Clinical Care Coordinator Brachial Plexus Program Department of Neurosurgery University of Michigan Timing
Radiculopathy vs. Peripheral Neuropathy What to do with arm pain? Miriana G. Popadich RN, MSN Clinical Care Coordinator Brachial Plexus Program Department of Neurosurgery University of Michigan Timing
REVIEW OF RADICULOPATHY
 REVIEW OF RADICULOPATHY Ileana Howard, MD Clinical Assistant Professor of Rehabilitation Medicine, University of Washington VA Puget Sound Health Care System March 17, 2015 Overview Introduction Pathophysiology
REVIEW OF RADICULOPATHY Ileana Howard, MD Clinical Assistant Professor of Rehabilitation Medicine, University of Washington VA Puget Sound Health Care System March 17, 2015 Overview Introduction Pathophysiology
The Hand Exam: Tips and Tricks
 The Hand Exam: Tips and Tricks Nikki Strauss Schroeder, MD Assistant Clinical Professor, UCSF Department of Orthopaedic Surgery November 4, 2013 Outline Surface Anatomy Hand Anatomy Exam Management of
The Hand Exam: Tips and Tricks Nikki Strauss Schroeder, MD Assistant Clinical Professor, UCSF Department of Orthopaedic Surgery November 4, 2013 Outline Surface Anatomy Hand Anatomy Exam Management of
Fundamentals of Electromyography. Amanda Peltier, MD MS Department of Neurology
 Fundamentals of Electromyography Amanda Peltier, MD MS Department of Neurology Importance of EMG Studies Diagnosis Localization Assist in further testing (i.e. identify potential biopsy sites) Prognosis
Fundamentals of Electromyography Amanda Peltier, MD MS Department of Neurology Importance of EMG Studies Diagnosis Localization Assist in further testing (i.e. identify potential biopsy sites) Prognosis
Syndesmosis Injuries
 Syndesmosis Injuries Dr. Alex Rabinovich Outline Anatomy Injury types and classification Treatment options Nonoperative vs. Operative Indications for operative Operative technique Postoperative management
Syndesmosis Injuries Dr. Alex Rabinovich Outline Anatomy Injury types and classification Treatment options Nonoperative vs. Operative Indications for operative Operative technique Postoperative management
The cervical spine has three functions: supporting the head, allowing for the head s ROM and housing the spinal cord (Fig. 2.1).
.") F10001-Ch02.qxd 4/7/06 9:04 AM Page 11 Spine 2 THE CERVICAL SPINE AND NECK The cervical spine has three functions: supporting the head, allowing for the head s ROM and housing the spinal cord (Fig. 2.1).
F10001-Ch02.qxd 4/7/06 9:04 AM Page 11 Spine 2 THE CERVICAL SPINE AND NECK The cervical spine has three functions: supporting the head, allowing for the head s ROM and housing the spinal cord (Fig. 2.1).
by joe muscolino body mechanics
 by joe muscolino body mechanics carpal tunnel syndrome The word carpal means wrist. Therefore, the carpal tunnel is a tunnel that is formed by the structural configuration of the wrist (carpal) bones.
by joe muscolino body mechanics carpal tunnel syndrome The word carpal means wrist. Therefore, the carpal tunnel is a tunnel that is formed by the structural configuration of the wrist (carpal) bones.
Common Regional Nerve Blocks Quick Guide developed by UWHC Acute Pain Service Jan 2011
 Common Regional Nerve Blocks Quick Guide developed by UWHC Acute Pain Service Jan 2011 A single shot nerve block is the injection of local anesthetic to block a specific nerve distribution. It can be placed
Common Regional Nerve Blocks Quick Guide developed by UWHC Acute Pain Service Jan 2011 A single shot nerve block is the injection of local anesthetic to block a specific nerve distribution. It can be placed
10/15/2012. The Hand. Clarification of Terms. Osteology of the Hand (Bones) http://www.youtube.com/watch?v=idxuwerttj A&feature=related
 http://www.youtube.com/watch?v=idxuwerttj A&feature=related") The Hand http://www.youtube.com/watch?v=idxuwerttj A&feature=related Clarification of Terms The hand is made up of the thumb, metacarpals, and phalanges The digits are numbered (with the thumb being #1
The Hand http://www.youtube.com/watch?v=idxuwerttj A&feature=related Clarification of Terms The hand is made up of the thumb, metacarpals, and phalanges The digits are numbered (with the thumb being #1
www.ghadialisurgery.com
 P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
Nerve Conduction Velocity (NCV) & Electromyography (EMG) Studies
 & Electromyography (EMG) Studies") Nerve Conduction Velocity (NCV) & Electromyography (EMG) Studies [Preauthorization Required] Medical Policy: MP-ME-09-09 Original Effective Date: November 5, 2010 Reviewed: November 5, 2010 Reviewed: November
Nerve Conduction Velocity (NCV) & Electromyography (EMG) Studies [Preauthorization Required] Medical Policy: MP-ME-09-09 Original Effective Date: November 5, 2010 Reviewed: November 5, 2010 Reviewed: November
Anatomy and Physiology 121: Muscles of the Human Body
 Epicranius Anatomy and Physiology 121: Muscles of the Human Body Covers upper cranium Raises eyebrows, surprise, headaches Parts Frontalis Occipitalis Epicranial aponeurosis Orbicularis oculi Ring (sphincter)
Epicranius Anatomy and Physiology 121: Muscles of the Human Body Covers upper cranium Raises eyebrows, surprise, headaches Parts Frontalis Occipitalis Epicranial aponeurosis Orbicularis oculi Ring (sphincter)
Upper Limb QUESTIONS UPPER LIMB: QUESTIONS
 1 Upper Limb QUESTIONS 1.1 Which of the following statements best describes the scapula? a. It usually overlies the 2nd to 9th ribs. b. The spine continues laterally as the coracoid process. c. The suprascapular
1 Upper Limb QUESTIONS 1.1 Which of the following statements best describes the scapula? a. It usually overlies the 2nd to 9th ribs. b. The spine continues laterally as the coracoid process. c. The suprascapular
Role of Electrodiagnostic Tests in Neuromuscular Disease
 Role of Electrodiagnostic Tests in Neuromuscular Disease Electrodiagnostic tests Electroencephalogram (EEG) Electromyography (NCV, EMG) Cerebral evoked potentials (CEP) Motor evoked potentials (MEP) Electronystagmogram
Role of Electrodiagnostic Tests in Neuromuscular Disease Electrodiagnostic tests Electroencephalogram (EEG) Electromyography (NCV, EMG) Cerebral evoked potentials (CEP) Motor evoked potentials (MEP) Electronystagmogram
Muscle Name Origin Insertion Action Innervation Muscles of Upper Extremity Pectoralis Major Medial half of clavicle, front of sternum, costal
 Muscle Name Origin Insertion Action Innervation Muscles of Upper Extremity Pectoralis Major Medial half of clavicle, front of sternum, costal Crest of greater tubercle (Lateral lip of bicipital groove)
Muscle Name Origin Insertion Action Innervation Muscles of Upper Extremity Pectoralis Major Medial half of clavicle, front of sternum, costal Crest of greater tubercle (Lateral lip of bicipital groove)
Median Nerve Injuries in, Fractures in the Region of the Wrist
 252 Median Nerve Injuries in, Fractures in the Region of the Wrist N. MEADOFF, M.D., Bakersfield SUMMARY Injuries of the median nerve in fractures in the region of the wrist are not uncommon. Median nerve
252 Median Nerve Injuries in, Fractures in the Region of the Wrist N. MEADOFF, M.D., Bakersfield SUMMARY Injuries of the median nerve in fractures in the region of the wrist are not uncommon. Median nerve
EFFECT OF BODY MASS INDEX ON PARAMETERS OF NERVE CONDUCTION STUDY IN INDIAN POPULATION
 Indian 88 Pawar J Physiol et al Pharmacol 2012; 56(1) : 88 93 Indian J Physiol Pharmacol 2012; 56(1) EFFECT OF BODY MASS INDEX ON PARAMETERS OF NERVE CONDUCTION STUDY IN INDIAN POPULATION SACHIN M. PAWAR,
Indian 88 Pawar J Physiol et al Pharmacol 2012; 56(1) : 88 93 Indian J Physiol Pharmacol 2012; 56(1) EFFECT OF BODY MASS INDEX ON PARAMETERS OF NERVE CONDUCTION STUDY IN INDIAN POPULATION SACHIN M. PAWAR,
Elbow & Forearm H O W V I T A L I S T H E E L B O W T O O U R D A I L Y L I V E S?
 Elbow & Forearm H O W V I T A L I S T H E E L B O W T O O U R D A I L Y L I V E S? Clarification of Terms The elbow includes: 3 bones (humerus, radius, and ulna) 2 joints (humeroulnar and humeroradial)
Elbow & Forearm H O W V I T A L I S T H E E L B O W T O O U R D A I L Y L I V E S? Clarification of Terms The elbow includes: 3 bones (humerus, radius, and ulna) 2 joints (humeroulnar and humeroradial)
of Nerve Conduction Studies
 ~ ~ ~ NEUROLOGICAL PROGRESS Principles and Pitfalls of Nerve Conduction Studies Jun IGmura, MD This report reviews the fundamental principles and the changing concepts of nerve stimulation techniques,
~ ~ ~ NEUROLOGICAL PROGRESS Principles and Pitfalls of Nerve Conduction Studies Jun IGmura, MD This report reviews the fundamental principles and the changing concepts of nerve stimulation techniques,
Abdominal Pedicle Flaps To The Hand And Forearm John C. Kelleher M.D., F.A.C.S.
 Abdominal Pedicle Flaps To The Hand And Forearm John C. Kelleher M.D., F.A.C.S. Global-HELP Publications Chapter Eight: TECHNICAL REQUIREMENTS FOR FORMATION OF A TUBED PEDICLE FLAP Creating a tube pedicle
Abdominal Pedicle Flaps To The Hand And Forearm John C. Kelleher M.D., F.A.C.S. Global-HELP Publications Chapter Eight: TECHNICAL REQUIREMENTS FOR FORMATION OF A TUBED PEDICLE FLAP Creating a tube pedicle
The Nervous System: The Spinal Cord and Spinal Nerves
 14 The Nervous System: The Spinal Cord and Spinal Nerves PowerPoint Lecture Presentations prepared by Steven Bassett Southeast Community College Lincoln, Nebraska Introduction The Central Nervous System
14 The Nervous System: The Spinal Cord and Spinal Nerves PowerPoint Lecture Presentations prepared by Steven Bassett Southeast Community College Lincoln, Nebraska Introduction The Central Nervous System
Buccinator Presses cheek against molar teeth Facial (CNVII) wrinkles forehead
 wrinkles forehead") Muscles to Identify on the Cadaver and/or Models You are required to identify each of the following muscles or associated structures on the cadavers and/or models in lab. If the box is shaded in a particular
Muscles to Identify on the Cadaver and/or Models You are required to identify each of the following muscles or associated structures on the cadavers and/or models in lab. If the box is shaded in a particular
TransFx External Fixation System Large and Intermediate Surgical Technique
 TransFx External Fixation System Large and Intermediate Surgical Technique TransFx External Fixation System Large and Intermediate Surgical Technique 1 Surgical Technique For TransFx External Fixation
TransFx External Fixation System Large and Intermediate Surgical Technique TransFx External Fixation System Large and Intermediate Surgical Technique 1 Surgical Technique For TransFx External Fixation
INJURIES OF THE HAND AND WRIST By Derya Dincer, M.D.
 05/05/2007 INJURIES OF THE HAND AND WRIST By Derya Dincer, M.D. Hand injuries, especially the fractures of metacarpals and phalanges, are the most common fractures in the skeletal system. Hand injuries
05/05/2007 INJURIES OF THE HAND AND WRIST By Derya Dincer, M.D. Hand injuries, especially the fractures of metacarpals and phalanges, are the most common fractures in the skeletal system. Hand injuries
Electrodiagnostic Testing
 Electrodiagnostic Testing Electromyogram and Nerve Conduction Study North American Spine Society Public Education Series What Is Electrodiagnostic Testing? The term electrodiagnostic testing covers a
Electrodiagnostic Testing Electromyogram and Nerve Conduction Study North American Spine Society Public Education Series What Is Electrodiagnostic Testing? The term electrodiagnostic testing covers a
Proximal border = palmar wrist crease Distal border = Kaplan + ring finger axis
 FPL FCR Proximal border = palmar wrist crease Distal border = Kaplan + ring finger axis Thenar motor branch Kaplan s cardinal line: distal TCL thenar branch Superficial palmar arch superficial arch Originates
FPL FCR Proximal border = palmar wrist crease Distal border = Kaplan + ring finger axis Thenar motor branch Kaplan s cardinal line: distal TCL thenar branch Superficial palmar arch superficial arch Originates
CLINICAL NEUROPHYSIOLOGY
 CLINICAL NEUROPHYSIOLOGY Barry S. Oken, MD, Carter D. Wray MD Objectives: 1. Know the role of EMG/NCS in evaluating nerve and muscle function 2. Recognize common EEG findings and their significance 3.
CLINICAL NEUROPHYSIOLOGY Barry S. Oken, MD, Carter D. Wray MD Objectives: 1. Know the role of EMG/NCS in evaluating nerve and muscle function 2. Recognize common EEG findings and their significance 3.
Laboratory Guide. Anatomy and Physiology
 Laboratory Guide Anatomy and Physiology TBME04, Fall 2010 Name: Passed: Last updated 2010-08-13 Department of Biomedical Engineering Linköpings Universitet Introduction This laboratory session is intended
Laboratory Guide Anatomy and Physiology TBME04, Fall 2010 Name: Passed: Last updated 2010-08-13 Department of Biomedical Engineering Linköpings Universitet Introduction This laboratory session is intended
Chapter 3. Ulnar nerve infiltration
 Chapter 3 LOCAL ANESTHESIA KEY FIGURES: Digital block/anatomy Sensation to hand Median nerve infiltration Ulnar nerve infiltration Facial block: skeleton Full surgical evaluation of a wound and suture
Chapter 3 LOCAL ANESTHESIA KEY FIGURES: Digital block/anatomy Sensation to hand Median nerve infiltration Ulnar nerve infiltration Facial block: skeleton Full surgical evaluation of a wound and suture
Whether a physician is
 ILLUSTRATIONS BY SCOT BODELL Hand and Wrist Injuries: Part I. Nonemergent Evaluation JAMES M. DANIELS II, M.D., M.P.H., Southern Illinois University School of Medicine, Quincy, Illinois ELVIN G. ZOOK,
ILLUSTRATIONS BY SCOT BODELL Hand and Wrist Injuries: Part I. Nonemergent Evaluation JAMES M. DANIELS II, M.D., M.P.H., Southern Illinois University School of Medicine, Quincy, Illinois ELVIN G. ZOOK,
The Muscular System. Appendicular Musculature
 11 The Muscular System Appendicular Musculature CHAPTER OBJECTIVES 1. Describe the functions of the appendicular musculature. 2. Identify and locate the principal appendicular muscles of the body, together
11 The Muscular System Appendicular Musculature CHAPTER OBJECTIVES 1. Describe the functions of the appendicular musculature. 2. Identify and locate the principal appendicular muscles of the body, together
Electrodiagnostic Testing
 Electrodiagnostic Testing Table of Contents Related Policies Policy Number 359 Policy Statement Purpose.. 1 2 Competency in Electrophysiologic Testing Original Effective Date: Current Approval Date: 1/1997
Electrodiagnostic Testing Table of Contents Related Policies Policy Number 359 Policy Statement Purpose.. 1 2 Competency in Electrophysiologic Testing Original Effective Date: Current Approval Date: 1/1997
Laser Treatment Policy
 Laser Treatment Policy Pursuant to federal law 21 CFR 812.2(c)7 and 812.3(b), physician(s) at this pain center may advise and use unapproved laser s on patients under one or more of the following conditions:
Laser Treatment Policy Pursuant to federal law 21 CFR 812.2(c)7 and 812.3(b), physician(s) at this pain center may advise and use unapproved laser s on patients under one or more of the following conditions:
ELECTROMYOGRAPHY (EMG), NEEDLE, NERVE CONDUCTION STUDIES (NCS) AND QUANTITATIVE SENSORY TESTING (QST)
, NEEDLE, NERVE CONDUCTION STUDIES (NCS) AND QUANTITATIVE SENSORY TESTING (QST)") AND QUANTITATIVE SENSORY TESTING (QST) Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Medical
AND QUANTITATIVE SENSORY TESTING (QST) Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Medical
Guideline 11B: RECOMMENDED STANDARDS FOR INTRAOPERATIVE MONITORING OF SOMATOSENSORY EVOKED POTENTIALS
 Guideline 11B: RECOMMENDED STANDARDS FOR INTRAOPERATIVE MONITORING OF SOMATOSENSORY EVOKED POTENTIALS Somatosensory evoked potentials (SSEPs) can be used intraoperatively to assess the function of the
Guideline 11B: RECOMMENDED STANDARDS FOR INTRAOPERATIVE MONITORING OF SOMATOSENSORY EVOKED POTENTIALS Somatosensory evoked potentials (SSEPs) can be used intraoperatively to assess the function of the
Electrocardiography I Laboratory
 Introduction The body relies on the heart to circulate blood throughout the body. The heart is responsible for pumping oxygenated blood from the lungs out to the body through the arteries and also circulating
Introduction The body relies on the heart to circulate blood throughout the body. The heart is responsible for pumping oxygenated blood from the lungs out to the body through the arteries and also circulating
Anatomic Percutaneous Ankle Reconstruction of Lateral Ligaments (A Percutaneous Anti ROLL)
") Anatomic Percutaneous Ankle Reconstruction of Lateral Ligaments (A Percutaneous Anti ROLL) Mark Glazebrook James Stone Masato Takao Stephane Guillo Introduction Ankle stabilization is required when a patient
Anatomic Percutaneous Ankle Reconstruction of Lateral Ligaments (A Percutaneous Anti ROLL) Mark Glazebrook James Stone Masato Takao Stephane Guillo Introduction Ankle stabilization is required when a patient
Elbow Examination. Haroon Majeed
 Elbow Examination Haroon Majeed Key Points Inspection Palpation Movements Neurological Examination Special tests Joints above and below Before Starting Introduce yourself Explain to the patient what the
Elbow Examination Haroon Majeed Key Points Inspection Palpation Movements Neurological Examination Special tests Joints above and below Before Starting Introduce yourself Explain to the patient what the
Anatomy for Workers Compensation Attorneys
 Anatomy for Workers Compensation Attorneys Donato J. Borrillo MD JD Plant Medical Advisor Chrysler/Jeep Assembly Toledo Zoll, Kranz, and Borgess May 16, 2015 Imaging studies neck 1 Bulge and herniation
Anatomy for Workers Compensation Attorneys Donato J. Borrillo MD JD Plant Medical Advisor Chrysler/Jeep Assembly Toledo Zoll, Kranz, and Borgess May 16, 2015 Imaging studies neck 1 Bulge and herniation
Background Š Compression neuropathy: Nerve compression resulting in nerve dysfunction. Upper Extremity Nerve Entrapments
 Upper Extremity Nerve Entrapments Compression Neuropathies: Pathophysiology Scott P. Olvey, MD 1 2 Goals Understand peripheral nerve histology Understand the pathophysiology of peripheral nerve compression
Upper Extremity Nerve Entrapments Compression Neuropathies: Pathophysiology Scott P. Olvey, MD 1 2 Goals Understand peripheral nerve histology Understand the pathophysiology of peripheral nerve compression
Ergonomics Monitor Training Manual
 Table of contents I. Introduction Ergonomics Monitor Training Manual II. Definition of Common Injuries Common Hand & Wrist Injuries Common Neck & Back Injuries Common Shoulder & Elbow Injuries III. Ergonomics
Table of contents I. Introduction Ergonomics Monitor Training Manual II. Definition of Common Injuries Common Hand & Wrist Injuries Common Neck & Back Injuries Common Shoulder & Elbow Injuries III. Ergonomics
Nervous System: Spinal Cord and Spinal Nerves (Chapter 13) Lecture Materials for Amy Warenda Czura, Ph.D. Suffolk County Community College
 Lecture Materials for Amy Warenda Czura, Ph.D. Suffolk County Community College") Nervous System: Spinal Cord and Spinal Nerves (Chapter 13) Lecture Materials for Amy Warenda Czura, Ph.D. Suffolk County Community College Primary Sources for figures and content: Eastern Campus Marieb,
Nervous System: Spinal Cord and Spinal Nerves (Chapter 13) Lecture Materials for Amy Warenda Czura, Ph.D. Suffolk County Community College Primary Sources for figures and content: Eastern Campus Marieb,
Recommended Policy for Electrodiagnostic Medicine American Association of Neuromuscular & Electrodiagnostic Medicine
 Recommended Policy for Electrodiagnostic Medicine American Association of Neuromuscular & Electrodiagnostic Medicine Executive Summary The electrodiagnostic medicine (EDX) evaluation is an important and
Recommended Policy for Electrodiagnostic Medicine American Association of Neuromuscular & Electrodiagnostic Medicine Executive Summary The electrodiagnostic medicine (EDX) evaluation is an important and
PHYSICAL EXAMINATION OF THE FOOT AND ANKLE
 PHYSICAL EXAMINATION OF THE FOOT AND ANKLE Presenter Dr. Richard Coughlin AOFAS Lecture Series OBJECTIVES 1. ASSESS 2. DIAGNOSE 3. TREAT HISTORY TAKING Take a HISTORY What is the patient s chief complaint?
PHYSICAL EXAMINATION OF THE FOOT AND ANKLE Presenter Dr. Richard Coughlin AOFAS Lecture Series OBJECTIVES 1. ASSESS 2. DIAGNOSE 3. TREAT HISTORY TAKING Take a HISTORY What is the patient s chief complaint?