Depressive Symptoms Quality Measures Skilled Nursing Facility Setting
|
|
|
- Kelley Moody
- 10 years ago
- Views:
Transcription
1 Depressive Symptoms Quality Measures Skilled Nursing Facility Setting Prepared for: CMS Quality Measures Work Group Forum 21 June 2012

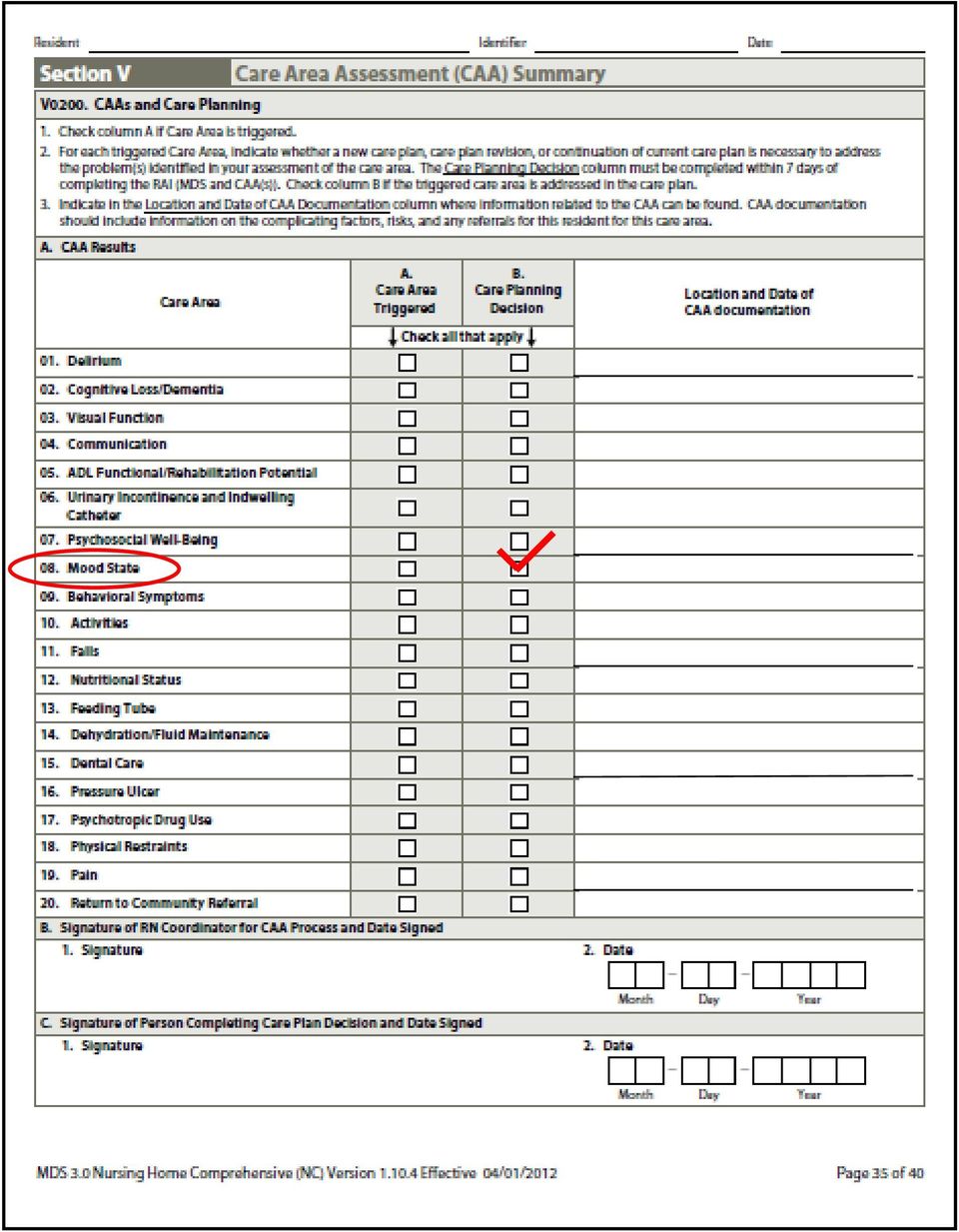
2 Moderate/Severe Depressive Symptoms Care Plan Measure (long-stay; #0690a) I. Measure Title: Percentage of residents with moderate to severe depressive symptoms who received a care plan (long-stay) II. Description: This measure is based on data from MDS 3.0 assessments of nursing home residents and indicates the percentage of residents who had the Mood State Care Plan addressed (score=01; i.e., in Section V0200 CAAs and Care Planning; subsection A. CAA Results) for those residents who received a score of 10-27/30 moderate to severe depressive symptoms on the PHQ-9. III. Numerator Statement: The numerator is the total number of long-stay residents who had Care Area 08. Mood State Care Planned Addressed (score =1; see image on next page) in the Care Area Assessment (CAA) Summary Section V, V0200, CAAs and Care Planning; A. CAA Result. IV. Denominator Statement: The denominator is the total number of all long-stay residents in the nursing facility who have received an annual MDS assessment during the selected quarter (3- month period). Using the PHQ-9 items in the MDS 3.0, the total sum severity score of 10-27/30 (D0300, D0500) on the most recent annual MDS assessment in the selected quarter. VII. Information on the Impact: Depression is a very expensive, complicating, and treatable factor for nursing facility residents. The total economic cost of depression in the U.S. in CY 2000 was $83.1 billion, including $26.1 billion in direct medical costs (#0690). The prevalence of moderate to severe depressive symptoms among nursing facility residents as of the most recent MDS 3.0 quality indicator was 7%. Therefore, depression among the nursing home residents is a significant clinical issue. VIII. Guidelines which Support Measure: Described elsewhere (#0690) are guidelines for screening, evaluation (including: changes in social or family situation, new stressors or situational factors such as changes in staff, availability of social and meaningful activities, availability of positive [reinforcing] experiences and unmet needs), and treatment (including non-pharmacological and pharmacological interventions effectiveness).

3
4 Mild Depressive Symptoms Measure (long-stay; #0690b) I. Measure Title: Percentage of residents who have mild depressive symptoms (long-stay) II. Description: This measure is based on data from MDS 3.0 assessments of nursing home residents and indicates the percentage of resident by resident interview or staff assessment that Patient Health Questionnaire (PHQ-9) depression instrument score in the mild range (5-9). III. Numerator Statement: Using the PHQ-9 items in the MDS 3.0, the total sum severity score of 5-9 (D0300, D0500) on the most recent MDS assessment in the selected quarter. The total severity score reflects long-stay resident responses to question asking about the frequency of nine symptoms over the last 2 weeks, including interest, mood, energy, appetite, self-value, ability to concentrate, change in responsiveness, or patience. IV. Denominator Statement: The denominator is the total number of all long-stay residents in the nursing facility who have received an MDS assessment (which may be an annual, quarterly, significant change or significant correction assessment) during the selected quarter (3-month period). VII. Information on the Impact: Depression is a very expensive, complicating, and treatable factor for nursing facility residents. The total economic cost of depression in the U.S. in CY 2000 was $83.1 billion, including $26.1 billion in direct medical costs (#0690). The prevalence of moderate to severe depressive symptoms among nursing facility residents as of the most recent MDS 3.0 quality indicator was 7%. In addition, according the PA Sample, another 16% of residents have less severe, but nevertheless clinically significant depression. Therefore, depression among the nursing home residents is a significant clinical issue. VIII. Guidelines which Support Measure: Described elsewhere (#0690) are guidelines for screening, evaluation (including: changes in social or family situation, new stressors or situational factors such as changes in staff, availability of social and meaningful activities, availability of positive [reinforcing] experiences and unmet needs), and treatment (including non-pharmacological and pharmacological interventions effectiveness). IX. Supporting Evidence: An estimated 5 million have subsyndromal depression, symptoms that fall short of meeting the full diagnostic criteria for a disorder (Horwath et al. [1992]). Horwath and colleagues (1992), in an analysis of data from a one-year re-interview-based longitudinal study with focus on DSM-III mental disorders, found that subsyndromal depression is especially common among older persons and is associated with a greater than 4 time risk of developing major depression. In addition, the authors found that approximately 50% of those with new-onset Major Depressive Disorder have subsyndromal depression in the prior year; they recommended behaviorally based programs for depression prevention. In a recent Institute of Medicine report (2009) on the prevention of mental health disorders the authors concluded that the evidence indicates that major depression can be prevented this is a turn-around from as recent as 25 years earlier (1984, NIMH depression pamphlet). In a recent review of the literature, Munoz et al. (2012) conclude from the results of a meta-analysis that 22 38% of major depressive episodes can be prevented.

5 Mild Depressive Symptoms Care Plan Measure (long-stay; #0690c) I. Measure Title: Percentage of residents with mild depressive symptoms who received a care plan (long-stay) II. Description: This measure is based on data from MDS 3.0 assessments of nursing home residents and indicates the percentage of residents who had the Mood State Care Plan addressed (score=01; i.e., in Section V0200 CAAs and Care Planning; subsection A. CAA Results) for those residents who received a score of 5-9 mild depression on the PHQ-9. III. Numerator Statement: The numerator is the total number of long-stay residents who had Care Area 08. Mood State Care Planned Addressed (score =1; see image on next page) in the Care Area Assessment (CAA) Summary Section V, V0200, CAAs and Care Planning; A. CAA Result. Currently the Mood State Care Area Assessment triggers for those residents who score 10-27/30; it would need to be changed to 5-27/30 in order to allow for a response to be indicated in the Addressed in Care Plan section. IV. Denominator Statement: The denominator is the total number of all long-stay residents in the nursing facility who have received an annual MDS assessment during the selected quarter (3- month period). Using the PHQ-9 items in the MDS 3.0, the total sum severity score of 5-9 (D0300, D0500) on the most recent annual MDS assessment in the selected quarter. VII. Information on the Impact: Depression is a very expensive, complicating, and treatable factor for nursing facility residents. The total economic cost of depression in the U.S. in CY 2000 was $83.1 billion, including $26.1 billion in direct medical costs (#0690). The prevalence of moderate to severe depressive symptoms among nursing facility residents as of the most recent MDS 3.0 quality indicator was 7%. In addition, according the PA Sample, another 16% of residents have less severe, but nevertheless clinically significant depression. Therefore, depression among the nursing home residents is a significant clinical issue. VIII. Guidelines which Support Measure: Described elsewhere (#0690) are guidelines for screening, evaluation (including: changes in social or family situation, new stressors or situational factors such as changes in staff, availability of social and meaningful activities, availability of positive [reinforcing] experiences and unmet needs), and treatment (including non-pharmacological and pharmacological interventions effectiveness). IX. Supporting Evidence: An estimated 5 million have subsyndromal depression, symptoms that fall short of meeting the full diagnostic criteria for a disorder (Horwath et al. [1992]). Horwath and colleagues (1992), in an analysis of data from a one-year re-interview-based longitudinal study with focus on DSM-III mental disorders, found that subsyndromal depression is especially common among older persons and is associated with a greater than 4 time risk of developing major depression. In addition, the authors found that approximately 50% of those with new-onset Major Depressive Disorder have subsyndromal depression in the prior year; they recommended behaviorally based programs for depression prevention. In a recent Institute of Medicine report (2009) on the prevention of mental health disorders the authors concluded that the evidence indicates that major depression can be prevented this is a turn-around from as recent as 25 years earlier (1984, NIMH depression pamphlet). In a recent review of the literature, Munoz et al. (2012) conclude from the results of a meta-analysis that 22 38% of major depressive episodes can be prevented with currently available interventions.
 in the Care Area Assessment (CAA) Summary Section V, V0200, CAAs and Care Planning; A. CAA Result.")
6

7 Mild Depressive Symptoms Measure (short-stay; #0690d) I. Measure Title: Percentage of residents who have mild depressive symptoms (short-stay) II. Description: This measure is based on data from MDS 3.0 assessments of nursing home residents and indicates the percentage of resident by resident interview or staff assessment that Patient Health Questionnaire (PHQ-9) depression instrument score in the mild range (5-9). III. Numerator Statement: Using the PHQ-9 items in the MDS 3.0, the total sum severity score of 5-9 (D0300, D0500) on the most recent MDS assessment in the selected quarter. The total severity score reflects long-stay resident responses to question asking about the frequency of nine symptoms over the last 2 weeks, including interest, mood, energy, appetite, self-value, ability to concentrate, change in responsiveness, or patience. IV. Denominator Statement: The denominator is the total number of all short-stay residents in the nursing facility who have received an MDS assessment (which may be a 5-day, 14-day, 30-day, 60-day, annual, quarterly, change of therapy, significant change or significant correction assessment, discharge assessment) during the selected quarter (3-month period). VII. Information on the Impact: Depression is a very expensive, complicating, and treatable factor for nursing facility residents. The total economic cost of depression in the U.S. in CY 2000 was $83.1 billion, including $26.1 billion in direct medical costs (#0690). The prevalence of moderate to severe depressive symptoms among nursing facility residents as of the most recent MDS 3.0 quality indicator was 7%. In addition, according the PA Sample, another 16% of residents have less severe, but nevertheless clinically significant depression. Therefore, depression among the nursing home residents is a significant clinical issue. In a recent secondary analysis of the Project Red, randomized controlled trial in the acute setting, Mitchell et al. (2010) found a 73% higher incidence rate for hospital utilization within 30 days of discharge for those with symptoms of depression. This places symptoms of depression on par with frequent prior rehospitalization, advanced age and low social support, as known risk factors for rehospitalization. As short-stay post-acute SNF patients are likely a more clinically compromised sub-population of acute patients, depression is apt to be at least as much of a risk factor if not more than those discharged to home from the hospital. VIII. Guidelines which Support Measure: Described elsewhere (#0690) are guidelines for screening, evaluation (including: changes in social or family situation, new stressors or situational factors such as changes in staff, availability of social and meaningful activities, availability of positive [reinforcing] experiences and unmet needs), and treatment (including non-pharmacological and pharmacological interventions effectiveness). IX. Supporting Evidence: An estimated 5 million have subsyndromal depression, symptoms that fall short of meeting the full diagnostic criteria for a disorder (Horwath et al. [1992]). Horwath and colleagues (1992), in an analysis of data from a one-year re-interview-based longitudinal study with focus on DSM-III mental disorders, found that subsyndromal depression is especially common among older persons and is associated with a greater than 4 time risk of developing major depression. In addition, the authors found that approximately 50% of those with new-onset Major Depressive Disorder have subsyndromal depression in the prior year; they recommended behaviorally based programs for depression prevention. In a recent Institute of Medicine report (2009) on the prevention of mental health disorders the authors concluded that the evidence indicates that major depression can be prevented this is a turn-around from as recent as 25 years earlier (1984, NIMH depression pamphlet). In a recent review of the literature, Munoz et al. (2012) conclude from the results of a meta-analysis that 22 38% of major depressive episodes can be prevented.
. III. Numerator Statement: Using the PHQ-9 items in the MDS 3.0, the total sum severity score of 5-9 (D0300, D0500) on the most recent MDS assessment in the selected quarter.")
8 Moderate-Severe Depressive Symptoms Measure (short-stay; #0690e) I. Measure Title: Percentage of residents who have depressive symptoms (short-stay) II. Description: This measure is based on data from MDS 3.0 assessments of nursing home residents and indicates the percentage of resident by resident interview or staff assessment that Patient Health Questionnaire (PHQ-9) depression instrument score in the moderate-severe range (10-27/30). III. Numerator Statement: Using the PHQ-9 items in the MDS 3.0, the total sum severity score of 10-27/30 (D0300, D0500) on the most recent MDS assessment in the selected quarter. The total severity score reflects long-stay resident responses to question asking about the frequency of nine symptoms over the last 2 weeks, including interest, mood, energy, appetite, self-value, ability to concentrate, change in responsiveness, or patience. IV. Denominator Statement: The denominator is the total number of all short-stay residents in the nursing facility who have received an MDS assessment (which may be a 5-day, 14-day, 30-day, 60-day, annual, quarterly, change of therapy, significant change or significant correction assessment, discharge assessment) during the selected quarter (3-month period). VII. Information on the Impact: Depression is a very expensive, complicating, and treatable factor for nursing facility residents. The total economic cost of depression in the U.S. in CY 2000 was $83.1 billion, including $26.1 billion in direct medical costs (#0690). The prevalence of moderate to severe depressive symptoms among nursing facility residents as of the most recent MDS 3.0 quality indicator was 7%. Therefore, depression among the nursing home residents is a significant clinical issue. In a recent secondary analysis of the Project Red, randomized controlled trial in the acute setting, Mitchell et al. (2010) found a 73% higher incidence rate for hospital utilization within 30 days of discharge for those with symptoms of depression. This places symptoms of depression on par with frequent prior rehospitalization, advanced age and low social support, as known risk factors for rehospitalization. As short-stay post-acute SNF patients are likely a more clinically compromised sub-population of acute patients, depression is apt to be at least as much of a risk factor if not more than those discharged to home from the hospital. VIII. Guidelines which Support Measure: Described elsewhere (#0690) are guidelines for screening, evaluation (including: changes in social or family situation, new stressors or situational factors such as changes in staff, availability of social and meaningful activities, availability of positive [reinforcing] experiences and unmet needs), and treatment (including non-pharmacological and pharmacological interventions effectiveness).
. III. Numerator Statement: Using the PHQ-9 items in the MDS 3.")
Dr. Anna M. Acee, EdD, ANP-BC, PMHNP-BC Long Island University, Heilbrunn School of Nursing
 Dr. Anna M. Acee, EdD, ANP-BC, PMHNP-BC Long Island University, Heilbrunn School of Nursing Overview Depression is significantly higher among elderly adults receiving home healthcare, particularly among
Dr. Anna M. Acee, EdD, ANP-BC, PMHNP-BC Long Island University, Heilbrunn School of Nursing Overview Depression is significantly higher among elderly adults receiving home healthcare, particularly among
Depression Remission at Six Months Specifications 2014 (Follow-up Visits for 07/01/2012 to 06/30/2013 Index Contact Dates)
") Description Methodology Rationale Measurement Period A measure of the percentage of adults patients who have reached remission at six months (+/- 30 days) after being identified as having an initial PHQ-9
Description Methodology Rationale Measurement Period A measure of the percentage of adults patients who have reached remission at six months (+/- 30 days) after being identified as having an initial PHQ-9
DEPRESSION Depression Assessment PHQ-9 Screening tool Depression treatment Treatment flow chart Medications Patient Resource
 E-Resource March, 2015 DEPRESSION Depression Assessment PHQ-9 Screening tool Depression treatment Treatment flow chart Medications Patient Resource Depression affects approximately 20% of the general population
E-Resource March, 2015 DEPRESSION Depression Assessment PHQ-9 Screening tool Depression treatment Treatment flow chart Medications Patient Resource Depression affects approximately 20% of the general population
MOLINA HEALTHCARE OF CALIFORNIA
 MOLINA HEALTHCARE OF CALIFORNIA MAJOR DEPRESSION IN ADULTS IN PRIMARY CARE HEALTH CARE GUIDELINE (ICSI) Health Care Guideline Twelfth Edition May 2009. The guideline was reviewed and adopted by the Molina
MOLINA HEALTHCARE OF CALIFORNIA MAJOR DEPRESSION IN ADULTS IN PRIMARY CARE HEALTH CARE GUIDELINE (ICSI) Health Care Guideline Twelfth Edition May 2009. The guideline was reviewed and adopted by the Molina
Assessment of depression in adults in primary care
 Assessment of depression in adults in primary care Adapted from: Identification of Common Mental Disorders and Management of Depression in Primary care. New Zealand Guidelines Group 1 The questions and
Assessment of depression in adults in primary care Adapted from: Identification of Common Mental Disorders and Management of Depression in Primary care. New Zealand Guidelines Group 1 The questions and
DEPRESSION CARE PROCESS STEP EXPECTATIONS RATIONALE
 1 DEPRESSION CARE PROCESS STEP EXPECTATIONS RATIONALE ASSESSMENT/PROBLEM RECOGNITION 1. Did the staff and physician seek and document risk factors for depression and any history of depression? 2. Did staff
1 DEPRESSION CARE PROCESS STEP EXPECTATIONS RATIONALE ASSESSMENT/PROBLEM RECOGNITION 1. Did the staff and physician seek and document risk factors for depression and any history of depression? 2. Did staff
Pennsylvania Depression Quality Improvement Collaborative
 Pennsylvania Depression Quality Improvement Collaborative Carol Hann, RN, MSN, CPHQ, Collaborative Manager Southeastern Pennsylvania Association for Healthcare Quality (SPAHQ) David Payne, Psy.D., Senior
Pennsylvania Depression Quality Improvement Collaborative Carol Hann, RN, MSN, CPHQ, Collaborative Manager Southeastern Pennsylvania Association for Healthcare Quality (SPAHQ) David Payne, Psy.D., Senior
Measurement Tool for Clinical Practice Guideline Implementation: Measures for Depression
 ment Tool for Clinical Practice Guideline : Establish process and clinical outcomes measures before implementing the Depression in the Long Term Care Setting Clinical Practice Guideline (CPG). As much
ment Tool for Clinical Practice Guideline : Establish process and clinical outcomes measures before implementing the Depression in the Long Term Care Setting Clinical Practice Guideline (CPG). As much
Running Head: INTERNET USE IN A COLLEGE SAMPLE. TITLE: Internet Use and Associated Risks in a College Sample
 Running Head: INTERNET USE IN A COLLEGE SAMPLE TITLE: Internet Use and Associated Risks in a College Sample AUTHORS: Katherine Derbyshire, B.S. Jon Grant, J.D., M.D., M.P.H. Katherine Lust, Ph.D., M.P.H.
Running Head: INTERNET USE IN A COLLEGE SAMPLE TITLE: Internet Use and Associated Risks in a College Sample AUTHORS: Katherine Derbyshire, B.S. Jon Grant, J.D., M.D., M.P.H. Katherine Lust, Ph.D., M.P.H.
Self-management strategies for mild to moderate depression
 Department of Epidemiology & Public Health Lunchtime seminar, 18 th Feb 2014 Self-management strategies for mild to moderate depression The internet-based ifightdepression tool Dr Celine Larkin National
Department of Epidemiology & Public Health Lunchtime seminar, 18 th Feb 2014 Self-management strategies for mild to moderate depression The internet-based ifightdepression tool Dr Celine Larkin National
How To Be A Nurse Practitioner
 NURSE PRACTITIONER PROGRAM THE PENNSYLVANIA STATE UNIVERSITY College of Nursing Preceptor Evaluation of Student Clinical Performance: Adult Gerontology Acute Care Nurse Practitioner Option Nursing 863
NURSE PRACTITIONER PROGRAM THE PENNSYLVANIA STATE UNIVERSITY College of Nursing Preceptor Evaluation of Student Clinical Performance: Adult Gerontology Acute Care Nurse Practitioner Option Nursing 863
Measure #370 (NQF 0710): Depression Remission at Twelve Months National Quality Strategy Domain: Effective Clinical Care
: Depression Remission at Twelve Months National Quality Strategy Domain: Effective Clinical Care") Measure #370 (NQF 0710): Depression Remission at Twelve Months National Quality Strategy Domain: Effective Clinical Care 2016 PQRS OPTIONS F INDIVIDUAL MEASURES: REGISTRY ONLY DESCRIPTION: Adult patients
Measure #370 (NQF 0710): Depression Remission at Twelve Months National Quality Strategy Domain: Effective Clinical Care 2016 PQRS OPTIONS F INDIVIDUAL MEASURES: REGISTRY ONLY DESCRIPTION: Adult patients
Depression: Facility Assessment Checklists
 Depression: Facility Assessment Checklists A facility system assessment is a starting point for a quality improvement project. The checklists included in this booklet will be most useful if you take a
Depression: Facility Assessment Checklists A facility system assessment is a starting point for a quality improvement project. The checklists included in this booklet will be most useful if you take a
Postpartum Depression (PPD) Beth Buxton, LCSW Massachusetts Department of Public Health [email protected]
 Beth Buxton, LCSW Massachusetts Department of Public Health beth.buxton@state.ma.us") Postpartum Depression (PPD) Beth Buxton, LCSW Massachusetts Department of Public Health [email protected] Mental Health Disorders An estimated 57.7 million adults (26.2% of adult population) suffer
Postpartum Depression (PPD) Beth Buxton, LCSW Massachusetts Department of Public Health [email protected] Mental Health Disorders An estimated 57.7 million adults (26.2% of adult population) suffer
Depression and its Treatment in Older Adults. Gregory A. Hinrichsen, Ph.D. Geropsychologist New York City
 Depression and its Treatment in Older Adults Gregory A. Hinrichsen, Ph.D. Geropsychologist New York City What is Depression? Everyday use of the word Clinically significant depressive symptoms : more severe,
Depression and its Treatment in Older Adults Gregory A. Hinrichsen, Ph.D. Geropsychologist New York City What is Depression? Everyday use of the word Clinically significant depressive symptoms : more severe,
Mental Health Needs Assessment Personality Disorder Prevalence and models of care
 Mental Health Needs Assessment Personality Disorder Prevalence and models of care Introduction and definitions Personality disorders are a complex group of conditions identified through how an individual
Mental Health Needs Assessment Personality Disorder Prevalence and models of care Introduction and definitions Personality disorders are a complex group of conditions identified through how an individual
Algorithm for Initiating Antidepressant Therapy in Depression
 Algorithm for Initiating Antidepressant Therapy in Depression Refer for psychotherapy if patient preference or add cognitive behavioural office skills to antidepressant medication Moderate to Severe depression
Algorithm for Initiating Antidepressant Therapy in Depression Refer for psychotherapy if patient preference or add cognitive behavioural office skills to antidepressant medication Moderate to Severe depression
Mellen Center for Multiple Sclerosis
 Mellen Center Cleveland Clinic Marie Namey, RN, MSN, MSCN Mellen Center Cleveland Clinic Cleveland, OH Home of. Mellen Center for Multiple Sclerosis Mellen Center Mission The Mellen Center remains committed
Mellen Center Cleveland Clinic Marie Namey, RN, MSN, MSCN Mellen Center Cleveland Clinic Cleveland, OH Home of. Mellen Center for Multiple Sclerosis Mellen Center Mission The Mellen Center remains committed
The diagnosis of dementia for people living in care homes. Frequently Asked Questions by GPs
 The diagnosis of dementia for people living in care homes Frequently Asked Questions by GPs A discussion document jointly prepared by Maggie Keeble, GP with special interest in palliative care and older
The diagnosis of dementia for people living in care homes Frequently Asked Questions by GPs A discussion document jointly prepared by Maggie Keeble, GP with special interest in palliative care and older
Managing depression after stroke. Presented by Maree Hackett
 Managing depression after stroke Presented by Maree Hackett After stroke Physical changes We can see these Depression Emotionalism Anxiety Confusion Communication problems What is depression? Category
Managing depression after stroke Presented by Maree Hackett After stroke Physical changes We can see these Depression Emotionalism Anxiety Confusion Communication problems What is depression? Category
Worksite Depression Screening and Treatment: An Innovative, Integrated Program
 Photos placed in horizontal position with even amount of white space between photos and header Photos placed in horizontal position with even amount of white space between photos and header Worksite Depression
Photos placed in horizontal position with even amount of white space between photos and header Photos placed in horizontal position with even amount of white space between photos and header Worksite Depression
Step 4: Complex and severe depression in adults
 Step 4: Complex and severe depression in adults A NICE pathway brings together all NICE guidance, quality standards and materials to support implementation on a specific topic area. The pathways are interactive
Step 4: Complex and severe depression in adults A NICE pathway brings together all NICE guidance, quality standards and materials to support implementation on a specific topic area. The pathways are interactive
Trends in Publicly Reported Nursing Facility Quality Measures
 Trends in Publicly Reported Nursing Facility Quality Measures American Health Care Association Reimbursement and Research Department January 2011 Trends in Publicly Reported Nursing Facility Quality Measures
Trends in Publicly Reported Nursing Facility Quality Measures American Health Care Association Reimbursement and Research Department January 2011 Trends in Publicly Reported Nursing Facility Quality Measures
Major Depressive Disorders Questions submitted for consideration by workshop participants
 Major Depressive Disorders Questions submitted for consideration by workshop participants Prioritizing Comparative Effectiveness Research Questions: PCORI Stakeholder Workshops June 9, 2015 Patient-Centered
Major Depressive Disorders Questions submitted for consideration by workshop participants Prioritizing Comparative Effectiveness Research Questions: PCORI Stakeholder Workshops June 9, 2015 Patient-Centered
Population Health Management For Behavioral Health. MHA s 2015 Annual Conference June 3, 2015
 Population Health Management For Behavioral Health MHA s 2015 Annual Conference June 3, 2015 Goals of the Affordable Care Act Improve the health of populations Lower per capita costs Improve the patient
Population Health Management For Behavioral Health MHA s 2015 Annual Conference June 3, 2015 Goals of the Affordable Care Act Improve the health of populations Lower per capita costs Improve the patient
MS an Mental Health. Alison Carolan MS Mental Health Nurse Kings College Hospital. IMPARTS December 2013
 MS an Mental Health Alison Carolan MS Mental Health Nurse Kings College Hospital IMPARTS December 2013 MS and Mental Health MS is an autoimmune disease MS carries high risk of common mental disorders and
MS an Mental Health Alison Carolan MS Mental Health Nurse Kings College Hospital IMPARTS December 2013 MS and Mental Health MS is an autoimmune disease MS carries high risk of common mental disorders and
DATE DUE: RESIDENT NAME: DATE(S) OF COMPLETION: STAFF COMPLETING RESIDENT REVIEW:
 OF COMPLETION: STAFF COMPLETING RESIDENT REVIEW:") 483.25 QUALITY OF CARE F309 CARE AND SERVICES FOR RESIDENT WITH PAIN Based on QIS CE Pathway CMS-20076 - Pain Recognition and Management http://www.aging.ks.gov/manuals/qismanual.htm Use of this tool is
483.25 QUALITY OF CARE F309 CARE AND SERVICES FOR RESIDENT WITH PAIN Based on QIS CE Pathway CMS-20076 - Pain Recognition and Management http://www.aging.ks.gov/manuals/qismanual.htm Use of this tool is
Depre r s e sio i n o i n i a dults Yousuf Al Farsi
 Depression in adults Yousuf Al Farsi Objectives 1. Aetiology 2. Classification 3. Major depression 4. Screening 5. Differential diagnosis 6. Treatment approach 7. When to refer 8. Complication 9. Prognosis
Depression in adults Yousuf Al Farsi Objectives 1. Aetiology 2. Classification 3. Major depression 4. Screening 5. Differential diagnosis 6. Treatment approach 7. When to refer 8. Complication 9. Prognosis
Co-Occurring Disorder-Related Quick Facts: ELDERLY
 Co-Occurring Disorder-Related Quick Facts: ELDERLY Elderly: In 2004, persons over the age of 65 reached a total of 36.3 million in the United States, an increase of approximately nine percent over the
Co-Occurring Disorder-Related Quick Facts: ELDERLY Elderly: In 2004, persons over the age of 65 reached a total of 36.3 million in the United States, an increase of approximately nine percent over the
How To Treat A Mental Illness At Riveredge Hospital
 ABOUT US n Riveredge Hospital maintains the treatment philosophy of Trauma Informed Care. n Our commitment to providing the highest quality of care includes offering Animal Assisted Therapy, and Expressive
ABOUT US n Riveredge Hospital maintains the treatment philosophy of Trauma Informed Care. n Our commitment to providing the highest quality of care includes offering Animal Assisted Therapy, and Expressive
MDS 3.0 QUALITY MEASURE (QM) REPORTS
 REPORTS") 11 MDS 3.0 QUALITY MEASURE (QM) REPORTS GENERAL INFORMATION...2 INTRODUCTION...2 SUPPORTING QM CONCEPTS...2 ACCESSING THE MDS 3.0 QM REPORTS...4 MDS 3.0 FACILITY CHARACTERISTICS REPORT...5 MDS 3.0 FACILITY
11 MDS 3.0 QUALITY MEASURE (QM) REPORTS GENERAL INFORMATION...2 INTRODUCTION...2 SUPPORTING QM CONCEPTS...2 ACCESSING THE MDS 3.0 QM REPORTS...4 MDS 3.0 FACILITY CHARACTERISTICS REPORT...5 MDS 3.0 FACILITY
TECHNICAL/CLINICAL TOOLS BEST PRACTICE 7: Depression Screening and Management
 TECHNICAL/CLINICAL TOOLS BEST PRACTICE 7: Depression Screening and Management WHY IS THIS IMPORTANT? Depression causes fluctuations in mood, low self esteem and loss of interest or pleasure in normally
TECHNICAL/CLINICAL TOOLS BEST PRACTICE 7: Depression Screening and Management WHY IS THIS IMPORTANT? Depression causes fluctuations in mood, low self esteem and loss of interest or pleasure in normally
Major Depressive Disorder (MDD) Guideline Diagnostic Nomenclature for Clinical Depressive Conditions
 Guideline Diagnostic Nomenclature for Clinical Depressive Conditions") Major Depressive Disorder Major Depressive Disorder (MDD) Guideline Diagnostic omenclature for Clinical Depressive Conditions Conditions Diagnostic Criteria Duration Major Depression 5 of the following
Major Depressive Disorder Major Depressive Disorder (MDD) Guideline Diagnostic omenclature for Clinical Depressive Conditions Conditions Diagnostic Criteria Duration Major Depression 5 of the following
Depression Screening in Primary Care
 Depression Screening in Primary Care Toni Johnson, MD Kristen Palcisco, BA, MSN, APRN MetroHealth System Our Vision Make Greater Cleveland a healthier place to live and a better place to do business. 2
Depression Screening in Primary Care Toni Johnson, MD Kristen Palcisco, BA, MSN, APRN MetroHealth System Our Vision Make Greater Cleveland a healthier place to live and a better place to do business. 2
Treating Depression to Remission in the Primary Care Setting. James M. Slayton, M.D., M.B.A. Medical Director United Behavioral Health
 Treating Depression to Remission in the Primary Care Setting James M. Slayton, M.D., M.B.A. Medical Director United Behavioral Health 2007 United Behavioral Health 1 2007 United Behavioral Health Goals
Treating Depression to Remission in the Primary Care Setting James M. Slayton, M.D., M.B.A. Medical Director United Behavioral Health 2007 United Behavioral Health 1 2007 United Behavioral Health Goals
Using Epic to Improve Care of Older Patients. Elizabeth Eckstrom,M.D. Michael L. Malone,M.D. January 19,2013
 Using Epic to Improve Care of Older Patients Elizabeth Eckstrom,M.D. Michael L. Malone,M.D. January 19,2013 Learning Objectives: Discuss the successes and challenges of using the EMR to document care.
Using Epic to Improve Care of Older Patients Elizabeth Eckstrom,M.D. Michael L. Malone,M.D. January 19,2013 Learning Objectives: Discuss the successes and challenges of using the EMR to document care.
Optum s Role in Mycare Ohio
 Optum s Role in Mycare Ohio What is MyCare Ohio? New opportunities generated by the Affordable Care Act have allowed Ohio to implement the MyCare Ohio program. MyCare Ohio is a demonstration project that
Optum s Role in Mycare Ohio What is MyCare Ohio? New opportunities generated by the Affordable Care Act have allowed Ohio to implement the MyCare Ohio program. MyCare Ohio is a demonstration project that
GUIDELINES FOR USE OF PSYCHOTHERAPEUTIC MEDICATIONS IN OLDER ADULTS
 GUIDELINES GUIDELINES FOR USE OF PSYCHOTHERAPEUTIC MEDICATIONS IN OLDER ADULTS Preamble The American Society of Consultant Pharmacists has developed these guidelines for use of psychotherapeutic medications
GUIDELINES GUIDELINES FOR USE OF PSYCHOTHERAPEUTIC MEDICATIONS IN OLDER ADULTS Preamble The American Society of Consultant Pharmacists has developed these guidelines for use of psychotherapeutic medications
Treatment Interventions for Suicide Prevention. Kate Comtois, PhD, MPH University of Washington
 Treatment Interventions for Suicide Prevention Kate Comtois, PhD, MPH University of Washington Suicide prevention has many forms Treating Depression Gatekeeper Training Public health or injury prevention
Treatment Interventions for Suicide Prevention Kate Comtois, PhD, MPH University of Washington Suicide prevention has many forms Treating Depression Gatekeeper Training Public health or injury prevention
3/11/15. COPD Disease Management Tackling the Transition. Objectives. Describe the multidisciplinary approach to inpatient care for COPD patients
 Faculty Disclosures COPD Disease Management Tackling the Transition Dr. Cappelluti has no actual or potential conflicts of interest associated with this presentation. Jane Reardon has no actual or potential
Faculty Disclosures COPD Disease Management Tackling the Transition Dr. Cappelluti has no actual or potential conflicts of interest associated with this presentation. Jane Reardon has no actual or potential
Preferred Practice Guidelines Bipolar Disorder in Children and Adolescents
 These Guidelines are based in part on the following: American Academy of Child and Adolescent Psychiatry s Practice Parameter for the Assessment and Treatment of Children and Adolescents With Bipolar Disorder,
These Guidelines are based in part on the following: American Academy of Child and Adolescent Psychiatry s Practice Parameter for the Assessment and Treatment of Children and Adolescents With Bipolar Disorder,
Part 1: Depression Screening in Primary Care
 Part 1: Depression Screening in Primary Care Toni Johnson, MD Kristen Palcisco, BA, MSN, APRN MetroHealth System Objectives Part 1: Improve ability to screen and diagnose Depression in Primary Care Increase
Part 1: Depression Screening in Primary Care Toni Johnson, MD Kristen Palcisco, BA, MSN, APRN MetroHealth System Objectives Part 1: Improve ability to screen and diagnose Depression in Primary Care Increase
Profile: Incorporating Routine Behavioral Health Screenings Into the Patient-Centered Medical Home
 104 A LOOK TO THE FUTURE Profile: Incorporating Routine Behavioral Health Screenings Into the Patient-Centered Medical Home Background Management of chronic diseases can be challenging in primary care,
104 A LOOK TO THE FUTURE Profile: Incorporating Routine Behavioral Health Screenings Into the Patient-Centered Medical Home Background Management of chronic diseases can be challenging in primary care,
MEDICAL POLICY: Telehealth Services
 POLICY........ PG-0142 EFFECTIVE......01/01/08 LAST REVIEW... 01/12/16 MEDICAL POLICY: Telehealth Services GUIDELINES This policy does not certify benefits or authorization of benefits, which is designated
POLICY........ PG-0142 EFFECTIVE......01/01/08 LAST REVIEW... 01/12/16 MEDICAL POLICY: Telehealth Services GUIDELINES This policy does not certify benefits or authorization of benefits, which is designated
Clinical Criteria 4.201 Inpatient Medical Withdrawal Management 4.201 Substance Use Inpatient Withdrawal Management (Adults and Adolescents)
") 4.201 Inpatient Medical Withdrawal Management 4.201 Substance Use Inpatient Withdrawal Management (Adults and Adolescents) Description of Services: Inpatient withdrawal management is comprised of services
4.201 Inpatient Medical Withdrawal Management 4.201 Substance Use Inpatient Withdrawal Management (Adults and Adolescents) Description of Services: Inpatient withdrawal management is comprised of services
LEVEL I SA: OUTPATIENT INDIVIDUAL THERAPY - Adult
 LEVEL I SA: OUTPATIENT INDIVIDUAL THERAPY - Adult Definition The following is based on the Adult Criteria of the Patient Placement Criteria for the Treatment of Substance-Related Disorders of the American
LEVEL I SA: OUTPATIENT INDIVIDUAL THERAPY - Adult Definition The following is based on the Adult Criteria of the Patient Placement Criteria for the Treatment of Substance-Related Disorders of the American
Psychosocial treatment of late-life depression with comorbid anxiety
 Psychosocial treatment of late-life depression with comorbid anxiety Viviana Wuthrich Centre for Emotional Health Macquarie University, Sydney, Australia Why Comorbidity? Comorbidity is Common Common disorders,
Psychosocial treatment of late-life depression with comorbid anxiety Viviana Wuthrich Centre for Emotional Health Macquarie University, Sydney, Australia Why Comorbidity? Comorbidity is Common Common disorders,
See page 16. Billing compliance for non-physician providers: Understanding the CMS billing regulations. Debbie Bohr
 Compliance TODAY March 2014 a publication of the health care compliance association www.hcca-info.org How do you know if your compliance program is working? an interview with Kim Otte Chief Compliance
Compliance TODAY March 2014 a publication of the health care compliance association www.hcca-info.org How do you know if your compliance program is working? an interview with Kim Otte Chief Compliance
Depressive Disorders Inpatient Management v.1.1
 Depressive Disorders Inpatient Management v.1.1 Executive Summary Citation Information Explanation of Evidence Ratings Summary of Version Changes Intake Admission interview, physical exam, and review of
Depressive Disorders Inpatient Management v.1.1 Executive Summary Citation Information Explanation of Evidence Ratings Summary of Version Changes Intake Admission interview, physical exam, and review of
`çããçå=jéåí~ä= aáëçêçéêëw=^åñáéíó=~åç= aééêéëëáçå. aêk=`=f=lâçåü~ jéçáå~ä=aáêéåíçê lñäé~ë=kep=cçìåç~íáçå=qêìëí=
 `çããçå=jéåí~ä= aáëçêçéêëw=^åñáéíó=~åç= aééêéëëáçå aêk=`=f=lâçåü~ jéçáå~ä=aáêéåíçê lñäé~ë=kep=cçìåç~íáçå=qêìëí= Overview: Common Mental What are they? Disorders Why are they important? How do they affect
`çããçå=jéåí~ä= aáëçêçéêëw=^åñáéíó=~åç= aééêéëëáçå aêk=`=f=lâçåü~ jéçáå~ä=aáêéåíçê lñäé~ë=kep=cçìåç~íáçå=qêìëí= Overview: Common Mental What are they? Disorders Why are they important? How do they affect
A Survey of Registered Nurses Knowledge and Attitudes Regarding Paediatric Pain Assessment and Management: An Irish Perspective
 A Survey of Registered Nurses Knowledge and Attitudes Regarding Paediatric Pain Assessment and Management: An Irish Perspective Thursday 26th March 2009 RCN International Research Conference Cardiff, Wales.
A Survey of Registered Nurses Knowledge and Attitudes Regarding Paediatric Pain Assessment and Management: An Irish Perspective Thursday 26th March 2009 RCN International Research Conference Cardiff, Wales.
Kaiser Permanente Southern California Depression Care Program
 Kaiser Permanente Southern California Depression Care Program Abstract In 2001, Kaiser Permanente of Southern California (KPSC) adopted the IMPACT model of collaborative care for depression, developed
Kaiser Permanente Southern California Depression Care Program Abstract In 2001, Kaiser Permanente of Southern California (KPSC) adopted the IMPACT model of collaborative care for depression, developed
Rehab and Restorative Critical Element Pathway
 Use this pathway for a sampled resident who has had a lack of improvement in any areas of functional ability to determine if the resident received necessary rehabilitative services. Review the following
Use this pathway for a sampled resident who has had a lack of improvement in any areas of functional ability to determine if the resident received necessary rehabilitative services. Review the following
D0100: Should Resident Mood Interview Be Conducted?
 SECTION D: MOOD Intent: The items in this section address mood distress, a serious condition that is underdiagnosed and undertreated in the nursing home and is associated with significant morbidity. It
SECTION D: MOOD Intent: The items in this section address mood distress, a serious condition that is underdiagnosed and undertreated in the nursing home and is associated with significant morbidity. It
Bipolar Disorder and Substance Abuse Joseph Goldberg, MD
 Diabetes and Depression in Older Adults: A Telehealth Intervention Julie E. Malphurs, PhD Asst. Professor of Psychiatry and Behavioral Science Miller School of Medicine, University of Miami Research Coordinator,
Diabetes and Depression in Older Adults: A Telehealth Intervention Julie E. Malphurs, PhD Asst. Professor of Psychiatry and Behavioral Science Miller School of Medicine, University of Miami Research Coordinator,
Rosalie LO, PsyD Senior Clinical Psychologist Certified Traumatologist. Corporate Clinical Psychology Services Hospital Authority Hong Kong
 1 Rosalie LO, PsyD Senior Clinical Psychologist Certified Traumatologist Corporate Clinical Psychology Services Hospital Authority Hong Kong 1 2 Introduction Service Needs Service Planning Service Delivery
1 Rosalie LO, PsyD Senior Clinical Psychologist Certified Traumatologist Corporate Clinical Psychology Services Hospital Authority Hong Kong 1 2 Introduction Service Needs Service Planning Service Delivery
CPT Coding Update And Other Issues
 CPT Coding Update And Other Issues Robert E. Smith, M.D. Alison Lynch, M.D. November 13, 2013 1 Disclaimer This information is for educational and informational purposes only, and represents the understanding
CPT Coding Update And Other Issues Robert E. Smith, M.D. Alison Lynch, M.D. November 13, 2013 1 Disclaimer This information is for educational and informational purposes only, and represents the understanding
ADVANCED BEHAVIORAL HEALTH, INC. Clinical Level of Care Guidelines - 2015
 The Clinical Level of Care Guidelines contained on the following pages have been developed as a guide to assist care managers, physicians and providers in making medical necessity decisions about the least
The Clinical Level of Care Guidelines contained on the following pages have been developed as a guide to assist care managers, physicians and providers in making medical necessity decisions about the least
Addiction Billing. Kimber Debelak, CMC, CMOM, CMIS Director, Recovery Pathways
 Addiction Billing Kimber Debelak, CMC, CMOM, CMIS Director, Recovery Pathways Objectives Provide overview of addiction billing contrasting E&M vs. behavioral health codes Present system changes in ICD-9
Addiction Billing Kimber Debelak, CMC, CMOM, CMIS Director, Recovery Pathways Objectives Provide overview of addiction billing contrasting E&M vs. behavioral health codes Present system changes in ICD-9
THE OFFICE OF SUBSTANCE ABUSE SERVICES REQUIREMENTS FOR THE PROVISION OF RESIDENTIAL DETOXIFICATION SERVICES BY PROVIDERS FUNDED WITH DBHDS RESOURCES
 THE OFFICE OF SUBSTANCE ABUSE SERVICES REQUIREMENTS FOR THE PROVISION OF RESIDENTIAL DETOXIFICATION SERVICES BY PROVIDERS FUNDED WITH DBHDS RESOURCES PURPOSE: The goal of this document is to describe the
THE OFFICE OF SUBSTANCE ABUSE SERVICES REQUIREMENTS FOR THE PROVISION OF RESIDENTIAL DETOXIFICATION SERVICES BY PROVIDERS FUNDED WITH DBHDS RESOURCES PURPOSE: The goal of this document is to describe the
CARE MANAGEMENT FOR LATE LIFE DEPRESSION IN URBAN CHINESE PRIMARY CARE CLINICS
 CARE MANAGEMENT FOR LATE LIFE DEPRESSION IN URBAN CHINESE PRIMARY CARE CLINICS Dept of Public Health Sciences February 6, 2015 Yeates Conwell, MD Dept of Psychiatry, University of Rochester Shulin Chen,
CARE MANAGEMENT FOR LATE LIFE DEPRESSION IN URBAN CHINESE PRIMARY CARE CLINICS Dept of Public Health Sciences February 6, 2015 Yeates Conwell, MD Dept of Psychiatry, University of Rochester Shulin Chen,
Geriatric Psychiatrists
 Mentoring the Next Generation of Geriatric Psychiatrists Tips for Inspiring, Encouraging, and Guiding Medical Students 7910 Woodmont Avenue Suite 1050 Bethesda, MD 20814 phone: 3016547850 [email protected]
Mentoring the Next Generation of Geriatric Psychiatrists Tips for Inspiring, Encouraging, and Guiding Medical Students 7910 Woodmont Avenue Suite 1050 Bethesda, MD 20814 phone: 3016547850 [email protected]
Database of randomized trials of psychotherapy for adult depression
 Database of randomized trials of psychotherapy for adult depression In this document you find information about the database of 352 randomized controlled trials on psychotherapy for adult depression. This
Database of randomized trials of psychotherapy for adult depression In this document you find information about the database of 352 randomized controlled trials on psychotherapy for adult depression. This
ANTIPSYCHOTIC DRUG USE. HHS Has Initiatives to Reduce Use among Older Adults in Nursing Homes, but Should Expand Efforts to Other Settings
 United States Government Accountability Office Report to Congressional Requesters January 2015 ANTIPSYCHOTIC DRUG USE HHS Has Initiatives to Reduce Use among Older Adults in Nursing Homes, but Should Expand
United States Government Accountability Office Report to Congressional Requesters January 2015 ANTIPSYCHOTIC DRUG USE HHS Has Initiatives to Reduce Use among Older Adults in Nursing Homes, but Should Expand
An Integrated Substance Abuse Treatment Needs Assessment for Alaska EXECUTIVE SUMMARY FROM FINAL REPORT. Prepared by
 An Integrated Substance Abuse Treatment Needs Assessment for Alaska EXECUTIVE SUMMARY FROM FINAL REPORT Prepared by William McAuliffe, Ph.D. Ryan P. Dunn, B. A. Caroline Zhang, M.A. North Charles Research
An Integrated Substance Abuse Treatment Needs Assessment for Alaska EXECUTIVE SUMMARY FROM FINAL REPORT Prepared by William McAuliffe, Ph.D. Ryan P. Dunn, B. A. Caroline Zhang, M.A. North Charles Research
Antidepressant Skills @ Work Dealing with Mood Problems in the Workplace
 Antidepressant Skills @ Work Dealing with Mood Problems in the Workplace Dr. Joti Samra PhD, R.Psych. Adjunct Professor & Research Scientist CARMHA www.carmha.ca Dr. Merv Gilbert PhD, R.Psych. Principal
Antidepressant Skills @ Work Dealing with Mood Problems in the Workplace Dr. Joti Samra PhD, R.Psych. Adjunct Professor & Research Scientist CARMHA www.carmha.ca Dr. Merv Gilbert PhD, R.Psych. Principal
Mild depression: Few, if any, symptoms in excess of the 5 required to make the diagnosis, and symptoms result in only minor functional impairment.
 6.1 Anxiety Depression - Adults Anxiety is a condition characterized by persistent worry or unease and is usually accompanied by fear, panic, irritability, poor sleep, poor concentration and avoidance,
6.1 Anxiety Depression - Adults Anxiety is a condition characterized by persistent worry or unease and is usually accompanied by fear, panic, irritability, poor sleep, poor concentration and avoidance,
CRITICALLY APPRAISED PAPER (CAP)
") CRITICALLY APPRAISED PAPER (CAP) FOCUSED QUESTION What is the effect of life review through writing on depressive symptoms in older adults residing in senior residences? Chippendale, T., & Bear-Lehman,
CRITICALLY APPRAISED PAPER (CAP) FOCUSED QUESTION What is the effect of life review through writing on depressive symptoms in older adults residing in senior residences? Chippendale, T., & Bear-Lehman,
H.R 2646 Summary and S. 1945 Comparison
 H.R 2646 Summary and S. 1945 Comparison TITLE I ASSISTANT SECRETARY FOR MENTAL HEALTH AND SUBSTANCE USE DISORDERS It establishes an Office of the Assistant Secretary for Mental Health and Substance Use
H.R 2646 Summary and S. 1945 Comparison TITLE I ASSISTANT SECRETARY FOR MENTAL HEALTH AND SUBSTANCE USE DISORDERS It establishes an Office of the Assistant Secretary for Mental Health and Substance Use
The Collaborative Models of Mental Health Care for Older Iowans. Model Administration. Collaborative Models of Mental Health Care for Older Iowans 97
 6 The Collaborative Models of Mental Health Care for Older Iowans Model Administration Collaborative Models of Mental Health Care for Older Iowans 97 Collaborative Models of Mental Health Care for Older
6 The Collaborative Models of Mental Health Care for Older Iowans Model Administration Collaborative Models of Mental Health Care for Older Iowans 97 Collaborative Models of Mental Health Care for Older
See page 331 of HEDIS 2013 Tech Specs Vol 2. HEDIS specs apply to plans. RARE applies to hospitals. Plan All-Cause Readmissions (PCR) *++
 *++") Hospitalizations Inpatient Utilization General Hospital/Acute Care (IPU) * This measure summarizes utilization of acute inpatient care and services in the following categories: Total inpatient. Medicine.
Hospitalizations Inpatient Utilization General Hospital/Acute Care (IPU) * This measure summarizes utilization of acute inpatient care and services in the following categories: Total inpatient. Medicine.
Behavioral Health Policy Phototherapy Light for the Treatment of Seasonal Affective (SAD) and Other Depressive Disorders
 and Other Depressive Disorders") Behavioral Health Policy Phototherapy Light for the Treatment of Seasonal Affective (SAD) and Other Depressive Disorders Table of Contents Policy: Commercial Coding Information Information Pertaining to
Behavioral Health Policy Phototherapy Light for the Treatment of Seasonal Affective (SAD) and Other Depressive Disorders Table of Contents Policy: Commercial Coding Information Information Pertaining to
The Quality Concern: Behavioral Health Inpatient Readmissions
 The Readmissions Quality Collaborative Kick-Off Conference June 21, 2012 The Quality Concern: Behavioral Health Inpatient Readmissions Molly Finnerty, MD Director, Bureau of Evidence Based Services and
The Readmissions Quality Collaborative Kick-Off Conference June 21, 2012 The Quality Concern: Behavioral Health Inpatient Readmissions Molly Finnerty, MD Director, Bureau of Evidence Based Services and
Stage A & C Sample Data Collection Form
 Stage A & C Sample Data Collection Form Instructions: Review a minimum of 20 patient charts (or another number determined to be appropriate) from patients most recently admitted, and complete this Data
Stage A & C Sample Data Collection Form Instructions: Review a minimum of 20 patient charts (or another number determined to be appropriate) from patients most recently admitted, and complete this Data
Providing and Billing Medicare for Transitional Care Management
 PYALeadership Briefing Providing and Billing Medicare for Transitional Care Management Updated November 2014 2014 Pershing Yoakley & Associates, PC (PYA). No portion of this white paper may be used or
PYALeadership Briefing Providing and Billing Medicare for Transitional Care Management Updated November 2014 2014 Pershing Yoakley & Associates, PC (PYA). No portion of this white paper may be used or
Geriatric Mood and Anxiety Disorders: 5 Things you need to know about Treating Depression in the Elderly
 Geriatric Mood and Anxiety Disorders: 5 Things you need to know about Treating Depression in the Elderly Kiran Rabheru MD, CCFP, FRCP Geriatric Psychiatrist, The Ottawa Hospital Professor, University of
Geriatric Mood and Anxiety Disorders: 5 Things you need to know about Treating Depression in the Elderly Kiran Rabheru MD, CCFP, FRCP Geriatric Psychiatrist, The Ottawa Hospital Professor, University of
Athlete Mental Health Policy
 Athlete Mental Health Policy Owner: Chief Medical Officer Version: 2.1 Approved by: Executive Director Effective from: August 2013 Next review date: August 2015 Last Date of Edit: 13 May 2014 CONTENTS
Athlete Mental Health Policy Owner: Chief Medical Officer Version: 2.1 Approved by: Executive Director Effective from: August 2013 Next review date: August 2015 Last Date of Edit: 13 May 2014 CONTENTS
Depression Flow Chart
 Depression Flow Chart SCREEN FOR DEPRESSION ANNUALLY Assess for depression annually with the PHQ-9. Maintain a high index of suspicion in high risk older adults. Consider suicide risk and contributing
Depression Flow Chart SCREEN FOR DEPRESSION ANNUALLY Assess for depression annually with the PHQ-9. Maintain a high index of suspicion in high risk older adults. Consider suicide risk and contributing
NURSING FACILITY ASSESSMENTS
 Department of Health and Human Services OFFICE OF INSPECTOR GENERAL NURSING FACILITY ASSESSMENTS AND CARE PLANS FOR RESIDENTS RECEIVING ATYPICAL ANTIPSYCHOTIC DRUGS Daniel R. Levinson Inspector General
Department of Health and Human Services OFFICE OF INSPECTOR GENERAL NURSING FACILITY ASSESSMENTS AND CARE PLANS FOR RESIDENTS RECEIVING ATYPICAL ANTIPSYCHOTIC DRUGS Daniel R. Levinson Inspector General
CLINICAL PRACTICE GUIDELINES Treatment of Schizophrenia
 CLINICAL PRACTICE GUIDELINES Treatment of Schizophrenia V. Service Delivery Service Delivery and the Treatment System General Principles 1. All patients should have access to a comprehensive continuum
CLINICAL PRACTICE GUIDELINES Treatment of Schizophrenia V. Service Delivery Service Delivery and the Treatment System General Principles 1. All patients should have access to a comprehensive continuum
Improving Transitions & Reducing Readmissions from Skilled Nursing Facilities. Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies
 Improving Transitions & Reducing Readmissions from Skilled Nursing Facilities Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies Agenda Why this is so important What we know: a review of the
Improving Transitions & Reducing Readmissions from Skilled Nursing Facilities Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies Agenda Why this is so important What we know: a review of the
Q: Rehabilitation Nursing
 Q: Rehabilitation Nursing Alberta Licensed Practical Nurses Competency Profile 163 Priority: One Competency: Q-1 Apply the Rehabilitation Process Q-1-1 Q-1-2 Q-1-3 Q-1-4 Q-1-5 Q-1-6 Demonstrate knowledge
Q: Rehabilitation Nursing Alberta Licensed Practical Nurses Competency Profile 163 Priority: One Competency: Q-1 Apply the Rehabilitation Process Q-1-1 Q-1-2 Q-1-3 Q-1-4 Q-1-5 Q-1-6 Demonstrate knowledge
Schneps, Leila; Colmez, Coralie. Math on Trial : How Numbers Get Used and Abused in the Courtroom. New York, NY, USA: Basic Books, 2013. p i.
 New York, NY, USA: Basic Books, 2013. p i. http://site.ebrary.com/lib/mcgill/doc?id=10665296&ppg=2 New York, NY, USA: Basic Books, 2013. p ii. http://site.ebrary.com/lib/mcgill/doc?id=10665296&ppg=3 New
New York, NY, USA: Basic Books, 2013. p i. http://site.ebrary.com/lib/mcgill/doc?id=10665296&ppg=2 New York, NY, USA: Basic Books, 2013. p ii. http://site.ebrary.com/lib/mcgill/doc?id=10665296&ppg=3 New
Suicide Assessment in the Elderly Geriatric Psychiatric for the Primary Care Provider 2008
 Suicide Assessment in the Elderly Geriatric Psychiatric for the Primary Care Provider 2008 Lisa M. Brown, Ph.D. Aging and Mental Health Louis de la Parte Florida Mental Health Institute University of South
Suicide Assessment in the Elderly Geriatric Psychiatric for the Primary Care Provider 2008 Lisa M. Brown, Ph.D. Aging and Mental Health Louis de la Parte Florida Mental Health Institute University of South
Behavioral and Physical Treatments for Tension-type and Cervicogenic Headache
 Evidence Report: Behavioral and Physical Treatments for Tension-type and Cervicogenic Headache Douglas C. McCrory, MD, MHSc Donald B. Penzien, PhD Vic Hasselblad, PhD Rebecca N. Gray, DPhil Duke University
Evidence Report: Behavioral and Physical Treatments for Tension-type and Cervicogenic Headache Douglas C. McCrory, MD, MHSc Donald B. Penzien, PhD Vic Hasselblad, PhD Rebecca N. Gray, DPhil Duke University
NORTH COUNTRY COMMUNITY MENTAL HEALTH NORTHERN AFFILIATION UTILIZATION MANAGEMENT PLAN November 1, 2001. Revised January 2013
 NORTH COUNTRY COMMUNITY MENTAL HEALTH NORTHERN AFFILIATION UTILIZATION MANAGEMENT PLAN November 1, 2001 Revised January 2013 I. Mission II. III. IV. Scope Philosophy Authority V. Utilization Management
NORTH COUNTRY COMMUNITY MENTAL HEALTH NORTHERN AFFILIATION UTILIZATION MANAGEMENT PLAN November 1, 2001 Revised January 2013 I. Mission II. III. IV. Scope Philosophy Authority V. Utilization Management
Question ID: 6 Question type: Intervention Question: Does treatment of overactive bladder symptoms prevent falls in the elderly?
 PRIORITY BRIEFING The purpose of this briefing paper is to aid Stakeholders in prioritising topics to be taken further by PenCLAHRC as the basis for a specific evaluation or implementation projects. QUESTION
PRIORITY BRIEFING The purpose of this briefing paper is to aid Stakeholders in prioritising topics to be taken further by PenCLAHRC as the basis for a specific evaluation or implementation projects. QUESTION
Interviewable: Yes No Resident Room: Initial Admission Date: Care Area(s): Use
: Use") Facility Name: Facility ID: Date: Surveyor Name: Resident Name: Resident ID: Initial Admission Date: Care Area(s): Interviewable: Yes No Resident Room: Use Use this protocol to determine whether the facility
Facility Name: Facility ID: Date: Surveyor Name: Resident Name: Resident ID: Initial Admission Date: Care Area(s): Interviewable: Yes No Resident Room: Use Use this protocol to determine whether the facility
Revenue Cycle in Post- Acute Care Deloitte & Touche LLP Victor Shutack, Senior Manager June 2015
 6/9/2015 Revenue Cycle in Post- Acute Care Deloitte & Touche LLP Victor Shutack, Senior Manager June 2015 Discussion topics Changing healthcare environment Understanding the home health care environment
6/9/2015 Revenue Cycle in Post- Acute Care Deloitte & Touche LLP Victor Shutack, Senior Manager June 2015 Discussion topics Changing healthcare environment Understanding the home health care environment