Health Care Coverage, Access, and Cost: Wisconsin s Medicaid and BadgerCare Programs
|
|
|
- Angelica Douglas
- 8 years ago
- Views:
Transcription
1 Health Care Coverage, Access, and Cost: Wisconsin s Medicaid and BadgerCare Programs A Tour of Research Underway at the UW Population Health Institute Donna Friedsam, MPH Researcher & Health Policy Programs Director 1
2 Project Team Thomas DeLeire, PhD, Principal Investigator Laura Dague, PhD Donna Friedsam, MPH Daphne Kuo, PhD Lindsey Leininger, PhD Sarah Meier, MSc Kristen Voskuil, MA Joining our team: Marguerite Burns, PhD, PHS Assistant Professor Kara Mandell, PHS doctoral student Gaston Palmucci, economics doctoral student 2
3 Medicaid / BadgerCare Projects Enrollment, Take-up and Churning (HSR, 2011) Auto-enrollment (MMRR, June 2012) Crowd-out (NBER WP # 17009) Effect of Childless Adult Coverage on the Use of Health Care Innovative use of Health Needs Assessment in Medicaid Managed Care Effect of Public Insurance for Childless Adults on Labor Supply Medicaid Medical Homes for High Risk Pregnant Women 3
4 Funders Completed: RWJF, DHS New funding: RWJF SHARE: Adult Coverage Affects on Utilization, Cost HNA Predictive Value ICTR-CAP Marshfield Medicaid Utilization W.E. Upjohn Institute for Employment Research UC-Davis Center for Poverty Research Labor Market Impact Study UW Partnership Fund Medicaid Medical Homes for High Risk Pregnant Women
5

6
7 Presentations Academy Health Annual Research Meeting Association of Public Policy and Management (APPAM) American Society of Health Economics (ASHE) Population Association of America (PAA) National Bureau of Economic Research (NBER) Briefings: DHS Secretary, Medicaid Director, staff Pop Health Sciences Poster Sessions La Follette School of Public Affairs Seminar

8
9 Data Sets Medicaid CARES Eligibility and Enrollment Medicaid/BadgerCare Claims TPL Third Party Liability (DHS) EVHI Employer Verification of Health Insurance (DHS) Unemployment Insurance (DWD) ERISA self-insured employers (U.S. DOL) HNA - Health Needs Assessment (DHS) Wisconsin Health Information Exchange (WHIE) ACS and CPS (U.S. Census) Milwaukee County GAMP Claims Marshfield Clinic Claims Family Health Survey Vital Statistics Birth and Death records HMO High Risk Pregnancy Registry
10 Medicaid / BadgerCare Projects Enrollment, Take-up and Churning (HSR, 2011) Auto-enrollment (MMRR, June 2012) Crowd-out (NBER WP # 17009) Effect of Childless Adult Coverage on the Use of Health Care Innovative use of Health Needs Assessment in Medicaid Managed Care Effect of Public Insurance for Childless Adults on Labor Supply Medicaid Medical Homes for High Risk Pregnant Women 10
11 Medicaid / BadgerCare Projects Enrollment, Take-up and Churning (HSR, 2011) Auto-enrollment (MMRR, in press) Crowd-out (NBER WP # 17009) Effect of Childless Adult Coverage on the Use of Health Care Innovative use of Health Needs Assessment in Medicaid Managed Care Effect of Public Insurance for Childless Adults on Labor Supply Medicaid Medical Homes for High Risk Pregnant Women 11
12 Medicaid / BadgerCare Projects Enrollment, Take-up and Churning (HSR, 2011) Auto-enrollment (MMRR, June 2012) Crowd-out (NBER WP # 17009) Effect of Childless Adult Coverage on the Use of Health Care Innovative use of Health Needs Assessment in Medicaid Managed Care Effect of Public Insurance for Childless Adults on Labor Supply Medicaid Medical Homes for High Risk Pregnant Women 12
13 Medicaid / BadgerCare Projects Enrollment, Take-up and Churning (HSR, 2011) Auto-enrollment (MMRR, June 2012) Crowd-out (NBER WP # 17009) Effect of Childless Adult Coverage on the Use of Health Care Innovative use of Health Needs Assessment in Medicaid Managed Care Effect of Public Insurance for Childless Adults on Labor Supply Medicaid Medical Homes for High Risk Pregnant Women 13
14 Example of Completed Research Estimates of Crowd-Out from a Public Health Insurance Expansion Using Administrative Data Research Question: To what degree do new enrollees in public health insurance come from private sector coverage?
15 Policy Treatment Wisconsin expanded Medicaid in February 2008 to two populations: All children without access to insurance (no income limits) Parents and caretaker relatives with family incomes below 200% of the Federal Poverty Level
16 Approach Use set of linked administrative databases from Wisconsin to estimate: % of new public enrollees with access to private health insurance at the time of their enrollment % of new public enrollees uninsured at time of enrollment % of new public enrollees that dropped private coverage in the six months prior to or following enrollment
17 Matched Administrative Data Combine four administrative datasets using SSNs and FEINs: CARES: Wisconsin's program eligibility database; TPL: Wisconsin's Third Party Liability database; UI: Unemployment Insurance and quarterly wage records; and DOL: a U.S. Department of Labor database of all self-insured firms. Monthly enrollment data for a total of 1,392,185 new enrollees in 433,525 unique households.
18 Implementation
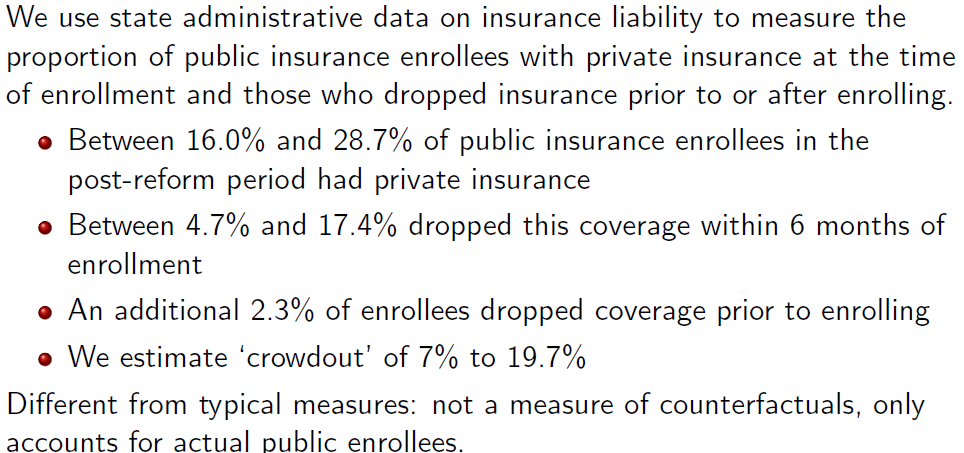
19 Conclusion
20 Expanding Coverage to Uninsured Childless Adults: Effect on the Use of Health Care Research Question: Does covering the uninsured with public insurance reduce the ineffective and inappropriate use of medical care, increase the use of primary and preventive care, and improve health? 20
21 Why is this question relevant for policymakers? The Affordable Care Act will expand Medicaid coverage to 138% FPL for all individuals, including childless adults The 25.2 million uninsured childless adults in the U.S. account for 57.2% of all uninsured non-elderly in the U.S. Of all childless uninsured childless adults, 9.6 million (38.4%) will be eligible for the coverage under the Medicaid expansion to those with incomes less than 138% FPL (Dubay et al., 2009) 21

22 Core Plan: Expansion of Coverage to Childless Adults In January 2009 Wisconsin began a new public program for uninsured childless adults <200% FPL Coverage of services is similar to, but more limited than, Medicaid Included the automatic enrollment of roughly 12,000 very low-income uninsured in Milwaukee Co. who were part of the Milwaukee County General Assistance Medical Program (GAMP) 22
23 Quasi-Experimental Study Design Take advantage of the individuals in GAMP system being automatically enrolled into BC+ Core An exogenous change from uninsured to publicly insured Move occurred because of a policy change and roll-out of a new program, not because of a choice to enroll We have both pre- and post-enrollment medical claims for this population Comparison group Low income BC+ adult enrollees from Milwaukee County 23
24 External Validity: How Representative is the GAMP Population? Low-income population in Milwaukee County Chronically Ill Covered by a decent health safety net Perhaps had better access to care than a `typical uninsured person? FQHCs are widespread nationally, but are not everywhere DSH payments to hospitals to care for indigent populations 24
25 Research Question Does enrollment into Medicaid (from Uninsured / GAMP) lead to changes in the use of: Inefficient care Total Emergency Department (ED) visits Avoidable or unnecessary ED visits Hospitalizations Avoidable hospitalizations Outpatient care Primary / Preventive Care Specialty Care 25
26 How Do Public Insurance Expansions Affect Utilization 1. Access Effect: insurance should increase utilization 2. Efficiency Effect: access to primary and specialty care should reduce inefficient use of care (e.g. ED) 3. Health Effect: both 1 and 2 should improve health and reduce hospitalizations Previous studies tend to find that insurance coverage increases utilization, including both ED use and hospitalizations Andersen et al., 2011; Finkelstein et al., 2011; Card et al., 2009; Dafney and Gruber,
27 Data Medicaid claims from the Wisconsin administrative claims database (interchange) system All claims for BC+ CORE enrollees for 2009 All claims for GAMP enrollees from 2008 Match GAMP claims to BC+ CORE claims at the individual level (using SSN) 9,619 successful matches 27
28 Methods 2 approaches: Pre-post 9,619 GAMP population enrolled into CORE Compare outcomes in 2008 (under GAMP) with outcomes in 2009 (under CORE) Individual fixed effects model, with month dummies and controls for exposure Difference-in-Differences Same, but also use a sample of BC+ adults as controls Milwaukee County, income < 150% FPL 28
29 Outcomes Emergency Department (ED) visits Ambulatory Care Sensitive (ACS) ED visits (Billings et al., 2009) Hospitalizations ACS Hospitalizations: AHRQ (2010) Prevention Quality Indicators (PQIs) Conditions for which good outpatient care can potentially prevent the need for hospitalization, or for which early intervention can prevent complications or more severe disease Outpatient visits Primary, Preventive, Episodic, Therapeutic, and Specialist, Care: total, by provider type 29
30 ACS ED Visits Non-emergent - immediate medical care was not required Emergent/Primary Care Treatable - care could have been provided in a primary care setting Emergent - ED Care Needed - Preventable/Avoidable - the emergent nature of the condition was potentially preventable/avoidable Emergent - ED Care Needed - Not Preventable/Avoidable Injuries, mental health, alcohol, drug 30
31 Classification of ED Visits NYU EMERGENCY DEPARTMENT NYU EMERGENCY DEPARTMENT CLASSIFICATION ALGORITHM [V2.0] CLASSIFICATION ALGORITHM [V2.0] Emergent Emergent ED care needed ED care needed Not preventable/avoidable Not preventable/avoidable Preventable/avoidable Preventable/avoidable Primary care treatable Primary care treatable Non-Emergent Non-Emergent Mental health related Mental health related Alcohol related Alcohol related Substance abuse related Substance abuse related Injury Injury Unclassified Unclassified 31
32 Results 32
33 ED Visits per Month Increase 26%

34 0.200 Increase Driven by ACS and Behavioral Health Visits ACS Emergent, Not PC Treatable, Not Avoidable or Injury % % Mental Health / Drug / Alcohol / Other -0.72% 34

35 Monthly Hospitalization Rate Declines 40%
36 Declines in ACS Hospitalization Rates
37 Total Outpatient Visits per Month Increase 32%

38 Increase Driven by Specialty Care 23% 16% Primary Care Provider Specialist 61% Unknown / Missing Increase Driven by Episodic / Therapeutic Care 2% 52% 46% Preventive Episodic Therapeutic 38
39 Summary Increase in ED visits Driven by increase in ACS visits Decline in hospitalizations Corresponding decline in PQIs Increase in outpatient visits Driven by increases in the use of specialty care, behavioral health services, and PT/OT not by increased use of preventive or primary care Strong research design; non-representative (but still relevant) population 39
40 Policy Implications: Access and Quality Good news: declines in total hospitalizations and in hospitalizations related to preventable disease Almost certainly indicates an improvement in the health in this poor and previously uninsured population Bad news: ambulatory care is increasingly happening in the ED, rather than in a primary care/community setting Despite expanding public insurance, we still need to resolve the problem of lack of access to and/or use of primary care 40
41 Policy Implications: Cost In progress: we are creating a Laspeyres cost index using Medicaid FFS fees as weights Will allow us to assess whether this policy, on net, reduced costs Today: back of the envelope Assume each type of service (ED, hospitalization, outpatient) has the average cost for that type Costs would have been 3.3% higher in 2009 than in 2008 Reductions in hospitalizations partially offset increases in ED visits and outpatient visits Completing analysis of pent-up demand response 41
42 Informing Medicaid Program Design: The Promise of Self-Reported Health Measures Research Questions: How useful are self-reported health measures in informing benefit design for Medicaid? How well does the model prospectively classifies at risk individuals and support risk adjustment and case management? What is the HNA utility for predictive modeling of future health care costs and utilization?

43
44
45 Hypotheses H 1 : The use of self-reported health measures at the time of Medicaid application appreciably increases predictive ability over the use of sociodemographic measures alone H 2 : In using a combination of self-reported health and sociodemographic measures collected at application, Medicaid programs could build their own models that perform at the level of accepted quality thresholds
46 Data Merged records from CARES and InterChange Study sample 35,910 Core Plan members who entered coverage between July October % of all Core Plan members (excluding former general assistance members) Not complete coverage, but better than most comparable pilot study in the literature Working with agency officials to understand who lacks HNA; have a few answers, we are seeking more
47 Measures Key predictors of interest = HNA measures Categorical variable of # of conditions (0, 1, 2, 3+) Any ER or hospitalization due to condition in past twelve months Tobacco use Alcohol/other drug problem Outcomes = membership in top utilization deciles during the first year in Core Plan ER utilization Hospitalization Sociodemographic predictors from CARES Base specification: age, age ^ 2, sex Additional variables: race, income, Hispanic ethnicity
48 Methodology Multivariate logistic regression Split-sample approach Test of discriminative ability: c statistic MODELS: 1. Age, age^2, male 2. Model 1 + race + Hispanic ethnicity + income 3. Model 2 + HNA conditions 4. Model 3 + HNA utilization 5. Model 4 + tobacco + alcohol/drug
49 Crosstabs High ER High inpatient No conditions One condition Two conditions Three + conditions
50 Discriminative Ability High hosp. High ER Model Number Specification c c (1) Age + Sex (2) (1) + Race + Hispanic Eth. + Income (3) (2) + Conditions (4) (3) + Previous Year's Utilization (5) (4) + Smoking + Alcohol/Drug Abuse
51 Future Directions Additional HNA predictors Usual source of care 5+ scrips at application Additional outcomes Expenditures PQI hospitalizations Condition-specific hospitalizations (esp. psychiatric) Test different treatments of HNA conditions (simple sum, Charlson-like index) More thorough Goodness-of-Fit testing
52 Conclusion Preliminary results suggestive of predictive ability on par with the literature Richest model predicting high ER utilization meets H-L criterion Ultimately usefulness will depend upon likely cost-effectiveness of application
53 Medical Homes for High-Risk Pregnant Women in SE Wisconsin: Do They Improve Birth Outcomes? Goal: To determine the effectiveness of the medical home model in improving birth outcomes among publicly insured, high-risk pregnant women in SE Wisconsin.
54 Intervention: The Basics DHS contract for health services in SE WI Kenosha, Milwaukee, Racine, Ozaukee, Washington and Waukesha. Contracted HMOs (4) required to implement a medical home pilot for high-risk pregnant women. High-risk Definition: living in a targeted zip code; having a chronic condition; being under 18 years of age; and/or being on or eligible to be on the DHS HMO High-Risk Registry. 54
55 Provider Incentive Payments BadgerCare Plus will pay participating providers: an additional $1,000 for each birth to a woman enrolled in a medical home pilot. bonus amount of an additional $1,000 for a positive birth outcome. This is a substantial increase over the current global payment for pregnancy and delivery of approximately $3,
56 Timelines and Enrollment Pilots began on January 1, Operational through December As of April 30, the HMOs have contracted with more than a dozen clinics. Sites will collectively enroll a minimum of 400 high-risk BadgerCare Plus (Medicaid) members in year one, 800 in year two and 1,200 in year three. 56
57 Outcome Measures Primary outcomes: birth weight and gestational age. Potential mediator: adequacy of pre-natal care receipt. Other outcome: inpatient stay associated with the birth. Power analysis (conducted for primary outcomes): Lower bound of 665 women will have been enrolled in the pilot and have had a birth by February 15, 2013, allowing for a six month delay in administrative data availability between the birth and the final proposed data pull, on August 15, The study is sufficiently powered to detect small changes in continuous measures of the primary outcomes of interest Likely detectable effect size of ~3% in both mean birth weight and mean gestational age. 57
58 Evaluation Methodology: Within-Group, Pre-Post Design Treatment group: Patients receiving care in the medical home pilot clinics. Comparison group: Similar patients receiving care in the pilot clinics in the two years (2009 & 2010) prior to the intervention s launch. Strengths of design: no unobserved confounding resulting from clinic-level heterogeneity or within-clinic treatment spillover effects. Major threats to validity: unobserved confounding resulting from patient-level heterogeneity; secular trends. 58
59 Implementation Study Assess fidelity of implementation (a process measure). Using a survey instrument adapted from the Commonwealth Fund s Safety Net Medical Home Initiative. Assess pre-program clinic care features and then compare them to post-implementation care features. Assess the degree to which providers meet the medical home parameters as specified in their contracts with DHS and in their response to the SE WI HMO RFP. 59
60 Stay Tuned!
Will Expanding Medicaid Coverage to Low-Income Uninsured Childless Adults under the Affordable Care Act Improve Health? Evidence from Wisconsin
 Will Expanding Medicaid Coverage to Low-Income Uninsured Childless Adults under the Affordable Care Act Improve Health? Evidence from Wisconsin Thomas DeLeire, Ph.D., Laura Dague, M.A., Lindsey Leininger,
Will Expanding Medicaid Coverage to Low-Income Uninsured Childless Adults under the Affordable Care Act Improve Health? Evidence from Wisconsin Thomas DeLeire, Ph.D., Laura Dague, M.A., Lindsey Leininger,
Evaluation of Wisconsin s BadgerCare Plus Health Care Coverage Program
 Evaluation of Wisconsin s BadgerCare Plus Health Care Coverage Program Report #1: Executive Summary Findings on Enrollment, Take-Up, Continuity, Target Efficiency, and Participation in Employer-Sponsored
Evaluation of Wisconsin s BadgerCare Plus Health Care Coverage Program Report #1: Executive Summary Findings on Enrollment, Take-Up, Continuity, Target Efficiency, and Participation in Employer-Sponsored
Evaluation of Wisconsin s BadgerCare Plus Health Care Coverage Program
 Evaluation of Wisconsin s BadgerCare Plus Health Care Coverage Program Report #4 Wisconsin's Lessons about the Potential of Medicaid Auto-Enrollment Submitted to the Wisconsin Department of Health Services
Evaluation of Wisconsin s BadgerCare Plus Health Care Coverage Program Report #4 Wisconsin's Lessons about the Potential of Medicaid Auto-Enrollment Submitted to the Wisconsin Department of Health Services
NBER WORKING PAPER SERIES ESTIMATES OF CROWD-OUT FROM A PUBLIC HEALTH INSURANCE EXPANSION USING ADMINISTRATIVE DATA
 NBER WORKING PAPER SERIES ESTIMATES OF CROWD-OUT FROM A PUBLIC HEALTH INSURANCE EXPANSION USING ADMINISTRATIVE DATA Laura Dague Thomas DeLeire Donna Friedsam Daphne Kuo Lindsey Leininger Sarah Meier Kristen
NBER WORKING PAPER SERIES ESTIMATES OF CROWD-OUT FROM A PUBLIC HEALTH INSURANCE EXPANSION USING ADMINISTRATIVE DATA Laura Dague Thomas DeLeire Donna Friedsam Daphne Kuo Lindsey Leininger Sarah Meier Kristen
NBER WORKING PAPER SERIES ESTIMATES OF CROWD-OUT FROM A PUBLIC HEALTH INSURANCE EXPANSION USING ADMINISTRATIVE DATA
 NBER WORKING PAPER SERIES ESTIMATES OF CROWD-OUT FROM A PUBLIC HEALTH INSURANCE EXPANSION USING ADMINISTRATIVE DATA Laura Dague Thomas DeLeire Donna Friedsam Daphne Kuo Lindsey Leininger Sarah Meier Kristen
NBER WORKING PAPER SERIES ESTIMATES OF CROWD-OUT FROM A PUBLIC HEALTH INSURANCE EXPANSION USING ADMINISTRATIVE DATA Laura Dague Thomas DeLeire Donna Friedsam Daphne Kuo Lindsey Leininger Sarah Meier Kristen
OM 10-55 Page 2 of 5. All four HMOs will provide medical and dental services to BadgerCare Plus for Families members in all six counties.
 DEPARTMENT OF CHILDREN AND FAMILIES Secretary Reggie Bicha 201 East Washington Avenue, Room G200 P.O. Box 8916 Madison, WI 53708-8916 Telephone: 608-266-8684 Fax: 608-261-6972 www.dcf.wisconsin.gov State
DEPARTMENT OF CHILDREN AND FAMILIES Secretary Reggie Bicha 201 East Washington Avenue, Room G200 P.O. Box 8916 Madison, WI 53708-8916 Telephone: 608-266-8684 Fax: 608-261-6972 www.dcf.wisconsin.gov State
Managed Care in Wisconsin
 in Wisconsin This profile reflects state managed care program information as of August 2014, and only includes information on active federal operating authorities, and as such, the program start date may
in Wisconsin This profile reflects state managed care program information as of August 2014, and only includes information on active federal operating authorities, and as such, the program start date may
The Target Efficiency of Online Medicaid/CHIP Enrollment: An Evaluation of Wisconsin s ACCESS Internet Portal
 February 2011 The Target Efficiency of Online Medicaid/CHIP Enrollment: An Evaluation of Wisconsin s ACCESS Internet Portal Lindsey J. Leininger, Donna Friedsam, Kristen Voskuil, Thomas DeLeire University
February 2011 The Target Efficiency of Online Medicaid/CHIP Enrollment: An Evaluation of Wisconsin s ACCESS Internet Portal Lindsey J. Leininger, Donna Friedsam, Kristen Voskuil, Thomas DeLeire University
LINDSEY JEANNE LEININGER December 2013
 LINDSEY JEANNE LEININGER December 2013 CONTACT INFORMATION University of Illinois-Chicago School of Public Health Department of Health Policy and Administration 1603 W. Taylor Street Chicago, IL 60612
LINDSEY JEANNE LEININGER December 2013 CONTACT INFORMATION University of Illinois-Chicago School of Public Health Department of Health Policy and Administration 1603 W. Taylor Street Chicago, IL 60612
Mental Health and Substance Abuse Services in Medicaid and SCHIP in Colorado
 Mental Health and Substance Abuse Services in Medicaid and SCHIP in Colorado As of July 2003, 377,123 people were covered under Colorado s Medicaid and SCHIP programs. There were 330,499 enrolled in the
Mental Health and Substance Abuse Services in Medicaid and SCHIP in Colorado As of July 2003, 377,123 people were covered under Colorado s Medicaid and SCHIP programs. There were 330,499 enrolled in the
Update January 2008. BadgerCare Plus Information for Providers. BadgerCare Plus Overview. Definition of the New Benefit. No.
 Update January 2008 No. 2008-04 BadgerCare Plus Information for Providers To: All Providers, HMOs and Other Managed Care Programs Mental Health and Substance Abuse Screening, Preventive Mental Health Counseling,
Update January 2008 No. 2008-04 BadgerCare Plus Information for Providers To: All Providers, HMOs and Other Managed Care Programs Mental Health and Substance Abuse Screening, Preventive Mental Health Counseling,
New Substance Abuse Screening and Intervention Benefit Covered by BadgerCare Plus and Medicaid
 Update December 2009 No. 2009-96 Affected Programs: BadgerCare Plus, Medicaid To: All Providers, HMOs and Other Managed Care Programs New Substance Abuse Screening and Intervention Benefit Covered by BadgerCare
Update December 2009 No. 2009-96 Affected Programs: BadgerCare Plus, Medicaid To: All Providers, HMOs and Other Managed Care Programs New Substance Abuse Screening and Intervention Benefit Covered by BadgerCare
Overview of the Maryland Primary Adult Care (PAC) Program. Rhode Island Policy Makers Breakfast November 17, 2010
 Program. Rhode Island Policy Makers Breakfast November 17, 2010") Overview of the Maryland Primary Adult Care (PAC) Program Rhode Island Policy Makers Breakfast November 17, 2010 Stacey Davis Deputy Director of Planning Maryland Medicaid Program Maryland Medicaid Provides
Overview of the Maryland Primary Adult Care (PAC) Program Rhode Island Policy Makers Breakfast November 17, 2010 Stacey Davis Deputy Director of Planning Maryland Medicaid Program Maryland Medicaid Provides
Non-Emergent Emergency Department Use among Adults with Disabilities
 Non-Emergent Emergency Department Use among Adults with Disabilities June 8, 2014 David Idala, Nancy Miller, Adele Kirk, Charles Betley, Seung Kim, Yi-An Chen, Ming Liang Dai Introduction Disparities in
Non-Emergent Emergency Department Use among Adults with Disabilities June 8, 2014 David Idala, Nancy Miller, Adele Kirk, Charles Betley, Seung Kim, Yi-An Chen, Ming Liang Dai Introduction Disparities in
The Impact of Health Care Reform. Evidence from Massachusetts
 The Impact of Health Care Reform on Hospital Careandand Preventive Care: Evidence from Massachusetts Jonathan T. Kolstad, Wharton School, University of Pennsylvania Amanda E. Kowalski, Department of Economics,
The Impact of Health Care Reform on Hospital Careandand Preventive Care: Evidence from Massachusetts Jonathan T. Kolstad, Wharton School, University of Pennsylvania Amanda E. Kowalski, Department of Economics,
I. INFORMATION ABOUT THE DEMONSTRATION
 EVALUATION DESIGN FOR THE WISCONSIN SENIORCARE SECTION 1115 PHARMACEUTICAL BENEFIT DEMONSTRATION I. INFORMATION ABOUT THE DEMONSTRATION This Evaluation Design is for project number 11-W-00149/5, the Wisconsin
EVALUATION DESIGN FOR THE WISCONSIN SENIORCARE SECTION 1115 PHARMACEUTICAL BENEFIT DEMONSTRATION I. INFORMATION ABOUT THE DEMONSTRATION This Evaluation Design is for project number 11-W-00149/5, the Wisconsin
Utah Data as of July 2003. Mental Health and Substance Abuse Services in Medicaid and SCHIP in Utah
 Mental Health and Substance Abuse Services in Medicaid and SCHIP in Utah As of July 2003, 196,600 people were covered under Utah s Medicaid/SCHIP programs. There were 157,322 enrolled in the Medicaid program,
Mental Health and Substance Abuse Services in Medicaid and SCHIP in Utah As of July 2003, 196,600 people were covered under Utah s Medicaid/SCHIP programs. There were 157,322 enrolled in the Medicaid program,
Universal Health Insurance And Mortality: Evidence From Massachusetts
 Universal Health Insurance And Mortality: Evidence From Massachusetts Charles Courtemanche Georgia State University and NBER Daniela Zapata IMPAQ International Chapter 58 and the ACA follow the same Three-legged
Universal Health Insurance And Mortality: Evidence From Massachusetts Charles Courtemanche Georgia State University and NBER Daniela Zapata IMPAQ International Chapter 58 and the ACA follow the same Three-legged
Mental Health and Substance Abuse Services Under BadgerCare Plus
 Update January 2008 No. 2008-05 BadgerCare Plus Information for Providers To: Advanced Practice Nurse Prescribers with Psychiatric Specialty, AODA Counselors, Community Support Programs, Comprehensive
Update January 2008 No. 2008-05 BadgerCare Plus Information for Providers To: Advanced Practice Nurse Prescribers with Psychiatric Specialty, AODA Counselors, Community Support Programs, Comprehensive
How do Medicaid, Medicare, and Commercial Insurance Vary in. Community-Level Performance?
 How do Medicaid, Medicare, and Commercial Insurance Vary in Community-Level Performance? Using Claims Data from the Wisconsin Health Information Organization (WHIO) to Assess Variation in Population Health
How do Medicaid, Medicare, and Commercial Insurance Vary in Community-Level Performance? Using Claims Data from the Wisconsin Health Information Organization (WHIO) to Assess Variation in Population Health
THE MEDICAID PROGRAM AT A GLANCE. Health Insurance Coverage
 on on medicaid and and the the uninsured March 2013 THE MEDICAID PROGRAM AT A GLANCE Medicaid, the nation s main public health insurance program for low-income people, covers over 62 million Americans,
on on medicaid and and the the uninsured March 2013 THE MEDICAID PROGRAM AT A GLANCE Medicaid, the nation s main public health insurance program for low-income people, covers over 62 million Americans,
PUBLIC HEALTH INSURANCE EXPANSIONS FOR PARENTS: EVIDENCE FROM WISCONSIN
 PUBLIC HEALTH INSURANCE EXPANSIONS FOR PARENTS: EVIDENCE FROM WISCONSIN Jason R. Davis, University of Wisconsin Stevens Point ABSTRACT The State Children s Health Insurance Program federal legislation
PUBLIC HEALTH INSURANCE EXPANSIONS FOR PARENTS: EVIDENCE FROM WISCONSIN Jason R. Davis, University of Wisconsin Stevens Point ABSTRACT The State Children s Health Insurance Program federal legislation
Health Care Utilization and Costs of Full-Pay and Subsidized Enrollees in the Florida KidCare Program: MediKids
 Health Care Utilization and Costs of Full-Pay and Subsidized Enrollees in the Florida KidCare Program: MediKids Prepared for the Florida Healthy Kids Corporation Prepared by Jill Boylston Herndon, Ph.D.
Health Care Utilization and Costs of Full-Pay and Subsidized Enrollees in the Florida KidCare Program: MediKids Prepared for the Florida Healthy Kids Corporation Prepared by Jill Boylston Herndon, Ph.D.
Enrollment under the Medicaid Expansion and Health Insurance Exchanges. A Focus on Those with Behavioral Health Conditions in Washington
 Enrollment under the Medicaid Expansion and Health Insurance Exchanges A Focus on Those with Behavioral Health Conditions in Washington Data Sources National Survey on Drug Use and Health Sponsored by
Enrollment under the Medicaid Expansion and Health Insurance Exchanges A Focus on Those with Behavioral Health Conditions in Washington Data Sources National Survey on Drug Use and Health Sponsored by
THE EFFECT OF INSURANCE ON INFANT HEALTH: A CASE STUDY OF LOW-INCOME WOMEN IN NEW JERSEY. Center for Research on Child Wellbeing Working Paper #98-30
 THE EFFECT OF INSURANCE ON INFANT HEALTH: A CASE STUDY OF LOW-INCOME WOMEN IN NEW JERSEY Center for Research on Child Wellbeing Working Paper #98-30 Robert Kaestner Nancy Reichman Theodore Joyce Effect
THE EFFECT OF INSURANCE ON INFANT HEALTH: A CASE STUDY OF LOW-INCOME WOMEN IN NEW JERSEY Center for Research on Child Wellbeing Working Paper #98-30 Robert Kaestner Nancy Reichman Theodore Joyce Effect
Division of Medical Assistance Programs
 January 23-24, 2007 CLIENTS WE SERVE Medicaid eligibility is limited to individuals who fall into specified categories and who are in financial need. The federal Medicaid statute identifies over 25 different
January 23-24, 2007 CLIENTS WE SERVE Medicaid eligibility is limited to individuals who fall into specified categories and who are in financial need. The federal Medicaid statute identifies over 25 different
Florida Data as of July 2003. Mental Health and Substance Abuse Services in Medicaid and SCHIP in Florida
 Mental Health and Substance Abuse Services in Medicaid and SCHIP in Florida As of July 2003 2,441,266 people were covered under Florida's Medicaid and SCHIP programs. There were 2,113,820 enrolled in the
Mental Health and Substance Abuse Services in Medicaid and SCHIP in Florida As of July 2003 2,441,266 people were covered under Florida's Medicaid and SCHIP programs. There were 2,113,820 enrolled in the
Enrollment under the Medicaid Expansion and Health Insurance Exchanges. A Focus on Those with Behavioral Health Conditions in Maine
 Enrollment under the Medicaid Expansion and Health Insurance Exchanges A Focus on Those with Behavioral Health Conditions in Maine Data Sources National Survey on Drug Use and Health Sponsored by SAMHSA
Enrollment under the Medicaid Expansion and Health Insurance Exchanges A Focus on Those with Behavioral Health Conditions in Maine Data Sources National Survey on Drug Use and Health Sponsored by SAMHSA
Home Care Association of Washington Conference. MaryAnne Lindeblad, State Medicaid Director Washington Health Care Authority
 Home Care Association of Washington Conference MaryAnne Lindeblad, State Medicaid Director Washington Health Care Authority April 25, 2013 Overview Overview of Health Care Authority Public Employees Benefits
Home Care Association of Washington Conference MaryAnne Lindeblad, State Medicaid Director Washington Health Care Authority April 25, 2013 Overview Overview of Health Care Authority Public Employees Benefits
IMPLICATIONS OF IMPLEMENTATION THE AFFORDABLE CARE ACT AND CRIMINAL JUSTICE
 THE AFFORDABLE CARE ACT AND CRIMINAL JUSTICE A FORUM PRESENTED BY CJCC S SATMHSIT IN PARTNERSHIP WITH THE PUBLIC WELFARE FOUNDATION AND THE LEGAL ACTION CENTER In July 2013, the Criminal Justice Coordinating
THE AFFORDABLE CARE ACT AND CRIMINAL JUSTICE A FORUM PRESENTED BY CJCC S SATMHSIT IN PARTNERSHIP WITH THE PUBLIC WELFARE FOUNDATION AND THE LEGAL ACTION CENTER In July 2013, the Criminal Justice Coordinating
How do Medicaid, Medicare, and Commercial Insurance Vary in Community-Level Performance?
 How do Medicaid, Medicare, and Commercial Insurance Vary in Community-Level Performance? Using Claims Data from the Wisconsin Health Information Organization (WHIO) to Assess Variation in Population Health
How do Medicaid, Medicare, and Commercial Insurance Vary in Community-Level Performance? Using Claims Data from the Wisconsin Health Information Organization (WHIO) to Assess Variation in Population Health
PHYSICIANS. 202.420.7896 888 16 th St. NW, Suite 800, Washington DC 20006 www.npalliance.org
 N A T I O N A L PHYSICIANS A L L I A N C E My name is Dr. Valerie Arkoosh. I am an Anesthesiologist at the University of Pennsylvania School of Medicine and the President of the National Physicians Alliance.
N A T I O N A L PHYSICIANS A L L I A N C E My name is Dr. Valerie Arkoosh. I am an Anesthesiologist at the University of Pennsylvania School of Medicine and the President of the National Physicians Alliance.
Maryland Data as of July 2003. Mental Health and Substance Abuse Services in Medicaid and SCHIP in Maryland
 Mental Health and Substance Abuse Services in Medicaid and SCHIP in Maryland As of July 2003, 638,662 people were covered under Maryland's Medicaid/SCHIP programs. There were 525,080 enrolled in the Medicaid
Mental Health and Substance Abuse Services in Medicaid and SCHIP in Maryland As of July 2003, 638,662 people were covered under Maryland's Medicaid/SCHIP programs. There were 525,080 enrolled in the Medicaid
Medicaid. (Title XIX and Title XXI) STATE REPORTS FY 2001. Division of Health Services Research INDIANA. SUK-FONG S TANG, PhD.
 STATE REPORTS FY 2001. Division of Health Services Research INDIANA. SUK-FONG S TANG, PhD.") Medicaid STATE REPORTS FY 2001 (Title XIX and Title XXI) Text7: Division of Health Services Research SUK-FONG S TANG, PhD General Information about CMS/MSIS2082, data source of this report: (Based on CMS
Medicaid STATE REPORTS FY 2001 (Title XIX and Title XXI) Text7: Division of Health Services Research SUK-FONG S TANG, PhD General Information about CMS/MSIS2082, data source of this report: (Based on CMS
Health Policy Brief. Nigel Lo, Dylan H. Roby, Jessica Padilla, Xiao Chen, Erin N. Salce, Nadereh Pourat, Gerald F. Kominski
 Health Policy Brief October 2014 Increased Service Use Following Medicaid Expansion Is Mostly Temporary: Evidence from California s Low Income Health Program Nigel Lo, Dylan H. Roby, Jessica Padilla, Xiao
Health Policy Brief October 2014 Increased Service Use Following Medicaid Expansion Is Mostly Temporary: Evidence from California s Low Income Health Program Nigel Lo, Dylan H. Roby, Jessica Padilla, Xiao
Enrollment under the Medicaid Expansion and Health Insurance Exchanges. A Focus on Those with Behavioral Health Conditions in Indiana
 Enrollment under the Medicaid Expansion and Health Insurance Exchanges A Focus on Those with Behavioral Health Conditions in Indiana Data Sources National Survey on Drug Use and Health Sponsored by SAMHSA
Enrollment under the Medicaid Expansion and Health Insurance Exchanges A Focus on Those with Behavioral Health Conditions in Indiana Data Sources National Survey on Drug Use and Health Sponsored by SAMHSA
A Healthy Florida Works Program. Policy Proposal. The smart choice for individuals and businesses in Florida
 A Healthy Florida Works Program Policy Proposal The smart choice for individuals and businesses in Florida TABLE OF CONTENTS Introduction Executive Summary Program Description 3 5 6 Coverage Population
A Healthy Florida Works Program Policy Proposal The smart choice for individuals and businesses in Florida TABLE OF CONTENTS Introduction Executive Summary Program Description 3 5 6 Coverage Population
Los Angeles County Counties, Clinics, Hospitals, Managed Care and the Uninsured: Ten-Year Trend Report (1996-2006)
") Insure the Uninsured Project Los Angeles County Counties, Clinics, Hospitals, Managed Care and the Uninsured: Ten-Year Trend Report (1996-2006) Prepared By: Erica Crall & Lucien Wulsin, Jr. COUNTY ECONOMY
Insure the Uninsured Project Los Angeles County Counties, Clinics, Hospitals, Managed Care and the Uninsured: Ten-Year Trend Report (1996-2006) Prepared By: Erica Crall & Lucien Wulsin, Jr. COUNTY ECONOMY
Enrollment under the Medicaid Expansion and Health Insurance Exchanges. A Focus on Those with Behavioral Health Conditions in Florida
 Enrollment under the Medicaid Expansion and Health Insurance Exchanges A Focus on Those with Behavioral Health Conditions in Florida Data Sources National Survey on Drug Use and Health Sponsored by SAMHSA
Enrollment under the Medicaid Expansion and Health Insurance Exchanges A Focus on Those with Behavioral Health Conditions in Florida Data Sources National Survey on Drug Use and Health Sponsored by SAMHSA
Massachusetts Evidence-Based Home Visiting Program: Needs Assessment Narrative
 Narrative Appendix C: Data Indicator Definitions and Sources Used in Community Risk Ranking Outcome #1 Maternal & Infant Health 1 Premature births -Percent: # live births before 37 weeks/total # live births
Narrative Appendix C: Data Indicator Definitions and Sources Used in Community Risk Ranking Outcome #1 Maternal & Infant Health 1 Premature births -Percent: # live births before 37 weeks/total # live births
Evaluating Medicaid s Options & Obligations After the Supreme Court s ACA Decision. Washington Health Care Authority August 8, 2012
 Evaluating Medicaid s Options & Obligations After the Supreme Court s ACA Decision Washington Health Care Authority August 8, 2012 Overview of the Supreme Court Decision Overview of the Decision A divided
Evaluating Medicaid s Options & Obligations After the Supreme Court s ACA Decision Washington Health Care Authority August 8, 2012 Overview of the Supreme Court Decision Overview of the Decision A divided
Enrollment under the Medicaid Expansion and Health Insurance Exchanges. A Focus on Those with Behavioral Health Conditions in Georgia
 Enrollment under the Medicaid Expansion and Health Insurance Exchanges A Focus on Those with Behavioral Health Conditions in Georgia Data Sources National Survey on Drug Use and Health Sponsored by SAMHSA
Enrollment under the Medicaid Expansion and Health Insurance Exchanges A Focus on Those with Behavioral Health Conditions in Georgia Data Sources National Survey on Drug Use and Health Sponsored by SAMHSA
Enrollment under the Medicaid Expansion and Health Insurance Exchanges. A Focus on Those with Behavioral Health Conditions in Idaho
 Enrollment under the Medicaid Expansion and Health Insurance Exchanges A Focus on Those with Behavioral Health Conditions in Idaho Data Sources National Survey on Drug Use and Health Sponsored by SAMHSA
Enrollment under the Medicaid Expansion and Health Insurance Exchanges A Focus on Those with Behavioral Health Conditions in Idaho Data Sources National Survey on Drug Use and Health Sponsored by SAMHSA
Strengthening Community Health Centers. Provides funds to build new and expand existing community health centers. Effective Fiscal Year 2011.
 Implementation Timeline Reflecting the Affordable Care Act 2010 Access to Insurance for Uninsured Americans with a Pre-Existing Condition. Provides uninsured Americans with pre-existing conditions access
Implementation Timeline Reflecting the Affordable Care Act 2010 Access to Insurance for Uninsured Americans with a Pre-Existing Condition. Provides uninsured Americans with pre-existing conditions access
Analysis of the Costs and Impact of Universal Health Care Coverage Under a Single Payer Model for the State of Vermont
 Analysis of the Costs and Impact of Universal Health Care Coverage Under a Single Payer Model for the State of Vermont Prepared for: The Vermont HRSA State Planning Grant, Office of Vermont Health Access
Analysis of the Costs and Impact of Universal Health Care Coverage Under a Single Payer Model for the State of Vermont Prepared for: The Vermont HRSA State Planning Grant, Office of Vermont Health Access
Health Insurance Exchange & Network Management Solutions
 Health Insurance Exchange & Network Management Solutions Mike Flanagan AVP, Product Management June 19, 2013 Today s Presenter Mike Flanagan Associate Vice President of Product Management McKesson Health
Health Insurance Exchange & Network Management Solutions Mike Flanagan AVP, Product Management June 19, 2013 Today s Presenter Mike Flanagan Associate Vice President of Product Management McKesson Health
Enrollment under the Medicaid Expansion and Health Insurance Exchanges. A Focus on Those with Behavioral Health Conditions in New Hampshire
 Enrollment under the Medicaid Expansion and Health Insurance Exchanges A Focus on Those with Behavioral Health Conditions in New Hampshire Data Sources National Survey on Drug Use and Health Sponsored
Enrollment under the Medicaid Expansion and Health Insurance Exchanges A Focus on Those with Behavioral Health Conditions in New Hampshire Data Sources National Survey on Drug Use and Health Sponsored
BadgerCare Plus: Medicaid and Subsidies Under One Umbrella
 BadgerCare Plus: Medicaid and Subsidies Under One Umbrella by K atharine E. Witg e rt I S S U E B R I E F Introduction Many proposals for federal health reform include two key elements: a Medicaid expansion
BadgerCare Plus: Medicaid and Subsidies Under One Umbrella by K atharine E. Witg e rt I S S U E B R I E F Introduction Many proposals for federal health reform include two key elements: a Medicaid expansion
Connecticut Data as of July 2003
 Mental Health and Substance Abuse Services in Medicaid and SCHIP in Connecticut As of July 2003, 378,961 people were covered under Connecticut Medicaid/SCHIP programs. There were 364,692 enrolled in the
Mental Health and Substance Abuse Services in Medicaid and SCHIP in Connecticut As of July 2003, 378,961 people were covered under Connecticut Medicaid/SCHIP programs. There were 364,692 enrolled in the
National Findings on Access to Health Care and Service Use for Non-elderly Adults Enrolled in Medicaid
 National Findings on Access to Health Care and Service Use for Non-elderly Adults Enrolled in Medicaid By Sharon K. Long Karen Stockley Elaine Grimm Christine Coyer Urban Institute MACPAC Contractor Report
National Findings on Access to Health Care and Service Use for Non-elderly Adults Enrolled in Medicaid By Sharon K. Long Karen Stockley Elaine Grimm Christine Coyer Urban Institute MACPAC Contractor Report
Basic Health Plan Offers a Chance to Provide Comprehensive Health Care Coverage for Low-Income Minnesotans
 Basic Health Plan Offers a Chance to Provide Comprehensive Health Care Coverage for Low-Income Minnesotans The number of uninsured in Minnesota has been on the rise over the last decade, with one out of
Basic Health Plan Offers a Chance to Provide Comprehensive Health Care Coverage for Low-Income Minnesotans The number of uninsured in Minnesota has been on the rise over the last decade, with one out of
Racial and Ethnic Disparities in Women s Health Coverage and Access To Care Findings from the 2001 Kaiser Women s Health Survey
 March 2004 Racial and Ethnic Disparities in Women s Health Coverage and Access To Care Findings from the 2001 Kaiser Women s Health Survey Attention to racial and ethnic differences in health status and
March 2004 Racial and Ethnic Disparities in Women s Health Coverage and Access To Care Findings from the 2001 Kaiser Women s Health Survey Attention to racial and ethnic differences in health status and
SENATE BUDGET AND APPROPRIATIONS COMMITTEE STATEMENT TO SENATE COMMITTEE SUBSTITUTE FOR. SENATE, No. 2236 STATE OF NEW JERSEY DATED: JUNE 23, 2005
 SENATE BUDGET AND APPROPRIATIONS COMMITTEE STATEMENT TO SENATE COMMITTEE SUBSTITUTE FOR SENATE, No. 2236 STATE OF NEW JERSEY DATED: JUNE 23, 2005 The Senate Budget and Appropriations Committee reports
SENATE BUDGET AND APPROPRIATIONS COMMITTEE STATEMENT TO SENATE COMMITTEE SUBSTITUTE FOR SENATE, No. 2236 STATE OF NEW JERSEY DATED: JUNE 23, 2005 The Senate Budget and Appropriations Committee reports
Preliminary Health Insurance Landscape Analysis
 Preliminary Health Insurance Landscape Analysis Prior to addressing some of the issues listed under Section 3.1 3.5 of the HRSA State Planning Grant report template, here is some of the information available
Preliminary Health Insurance Landscape Analysis Prior to addressing some of the issues listed under Section 3.1 3.5 of the HRSA State Planning Grant report template, here is some of the information available
(,, x. rh>l. Children s Health Insurance Program Reauthorization Act
 TO: Executive Office of Health and Human Services Office of Medicaid 600 Washington Street Boston, MA 021 11 www.mass.gov/masshealth MassHealth Eligibility Operations Staff rh>l FROM: Russ Kulp, Director,
TO: Executive Office of Health and Human Services Office of Medicaid 600 Washington Street Boston, MA 021 11 www.mass.gov/masshealth MassHealth Eligibility Operations Staff rh>l FROM: Russ Kulp, Director,
Pennsylvania s Medicaid program (Medical Assistance) has dozens of eligibility groups and programs, each with its own qualifying criteria.
 has dozens of eligibility groups and programs, each with its own qualifying criteria.") 1 Pennsylvania s Medicaid program (Medical Assistance) has dozens of eligibility groups and programs, each with its own qualifying criteria. Non Financial Factors include: Age; Disability (temporary, permanent
1 Pennsylvania s Medicaid program (Medical Assistance) has dozens of eligibility groups and programs, each with its own qualifying criteria. Non Financial Factors include: Age; Disability (temporary, permanent
Examples of Consumer Incentives and Personal Responsibility Requirements in Medicaid
 TECHNICAL ASSISTANCE TOOL Examples of Consumer Incentives and Personal Responsibility Requirements in Medicaid Many states are incorporating policies into their Medicaid programs that seek to enhance beneficiaries
TECHNICAL ASSISTANCE TOOL Examples of Consumer Incentives and Personal Responsibility Requirements in Medicaid Many states are incorporating policies into their Medicaid programs that seek to enhance beneficiaries
Medicare Beneficiaries Out-of-Pocket Spending for Health Care
 Insight on the Issues OCTOBER 2015 Beneficiaries Out-of-Pocket Spending for Health Care Claire Noel-Miller, MPA, PhD AARP Public Policy Institute Half of all beneficiaries in the fee-for-service program
Insight on the Issues OCTOBER 2015 Beneficiaries Out-of-Pocket Spending for Health Care Claire Noel-Miller, MPA, PhD AARP Public Policy Institute Half of all beneficiaries in the fee-for-service program
Welcome to the LogistiCare seminar on arranging non-emergency medical transportation (NEMT) services for Medicaid and BadgerCare Plus members, except
 services for Medicaid and BadgerCare Plus members, except") Welcome to the LogistiCare seminar on arranging non-emergency medical transportation (NEMT) services for Medicaid and BadgerCare Plus members, except those residing in a nursing home, or enrolled in the
Welcome to the LogistiCare seminar on arranging non-emergency medical transportation (NEMT) services for Medicaid and BadgerCare Plus members, except those residing in a nursing home, or enrolled in the
United 2020: Measuring Impact
 United 2020: Measuring Impact Health The Institute for Urban Policy Research At The University of Texas at Dallas Kristine Lykens, PhD United 2020: Measuring Impact Health Overview In the Dallas area,
United 2020: Measuring Impact Health The Institute for Urban Policy Research At The University of Texas at Dallas Kristine Lykens, PhD United 2020: Measuring Impact Health Overview In the Dallas area,
Assessing State Administrative Data to Monitor Health Care Reform
 Assessing State Administrative Data to Monitor Health Care Reform U.S. Department of Health and Human Services Data Council - September 9, 2012 Funded by the Assistant Secretary for Planning and Evaluation
Assessing State Administrative Data to Monitor Health Care Reform U.S. Department of Health and Human Services Data Council - September 9, 2012 Funded by the Assistant Secretary for Planning and Evaluation
DRAFT. The Effect of Public Insurance Coverage for Childless Adults on Labor Supply * Laura Dague, Texas A&M University
 DRAFT The Effect of Public Insurance Coverage for Childless Adults on Labor Supply * Laura Dague, Texas A&M University Thomas DeLeire, University of Wisconsin-Madison, NBER, and IZA Lindsey Leininger,
DRAFT The Effect of Public Insurance Coverage for Childless Adults on Labor Supply * Laura Dague, Texas A&M University Thomas DeLeire, University of Wisconsin-Madison, NBER, and IZA Lindsey Leininger,
Tax Credits + Medicaid. An Integrated Approach to Health Insurance Coverage. Lynn Etheredge
 4/8/05 Tax Credits + Medicaid An Integrated Approach to Health Insurance Coverage by Lynn Etheredge President Bush has recently proposed a major initiative for expanding health insurance coverage. It would
4/8/05 Tax Credits + Medicaid An Integrated Approach to Health Insurance Coverage by Lynn Etheredge President Bush has recently proposed a major initiative for expanding health insurance coverage. It would
Evaluation of Florida's Family Planning Waiver Program: Report on Cost Effectiveness. During Demonstration Year 9, 2006-07,
 Evaluation of Florida's Family Planning Waiver Program: Report on Cost Effectiveness During Demonstration Year 9, 2006-07, Using Required CMS Methodology Prepared for the Office of Medicaid Research and
Evaluation of Florida's Family Planning Waiver Program: Report on Cost Effectiveness During Demonstration Year 9, 2006-07, Using Required CMS Methodology Prepared for the Office of Medicaid Research and
PUBLIC BENEFITS. What are disability benefits? How is disability determined for SSDI and SSI?
 PUBLIC BENEFITS Public benefits are government programs that are set up to help people who need health care, cash assistance, food stamps, housing assistance, and other programs. Determining which programs
PUBLIC BENEFITS Public benefits are government programs that are set up to help people who need health care, cash assistance, food stamps, housing assistance, and other programs. Determining which programs
Oregon Data as of July 2003. Mental Health and Substance Abuse Services in Medicaid and SCHIP in Oregon
 Mental Health and Substance Abuse Services in Medicaid and SCHIP in Oregon As of July 2003, 398,874 people were covered under Oregon s Medicaid/SCHIP programs. There were 380,546 enrolled in the Medicaid
Mental Health and Substance Abuse Services in Medicaid and SCHIP in Oregon As of July 2003, 398,874 people were covered under Oregon s Medicaid/SCHIP programs. There were 380,546 enrolled in the Medicaid
Kansas Data as of July 2003. Mental Health and Substance Abuse Services in Medicaid and SCHIP in Kansas
 Mental Health and Substance Abuse Services in Medicaid and SCHIP in Kansas As of July 2003, 262,791 people were covered under Kansas's Medicaid and SCHIP programs. There were 233,481 enrolled in the Medicaid
Mental Health and Substance Abuse Services in Medicaid and SCHIP in Kansas As of July 2003, 262,791 people were covered under Kansas's Medicaid and SCHIP programs. There were 233,481 enrolled in the Medicaid
Research & Hennepin Health
 Research & Hennepin Health 1 Research & Publication Team Committee within the ACO Goal: To coordinate and prioritize research and publication about Hennepin Health by internal and external partners; to
Research & Hennepin Health 1 Research & Publication Team Committee within the ACO Goal: To coordinate and prioritize research and publication about Hennepin Health by internal and external partners; to
INSIGHT on the Issues
 INSIGHT on the Issues AARP Public Policy Institute Medicare Beneficiaries Out-of-Pocket for Health Care Claire Noel-Miller, PhD AARP Public Policy Institute Medicare beneficiaries spent a median of $3,138
INSIGHT on the Issues AARP Public Policy Institute Medicare Beneficiaries Out-of-Pocket for Health Care Claire Noel-Miller, PhD AARP Public Policy Institute Medicare beneficiaries spent a median of $3,138
How To Calculate The Cost Of A Health Insurance Tax Credit In Oregona
 Oregon Health Fund Board INITIAL ECONOMETRIC MODELING FOR THE OREGON HEALTH FUND BOARD Final Report February 2009 SUMMARY The Oregon Health Fund Board worked with consultants from the Massachusetts Institute
Oregon Health Fund Board INITIAL ECONOMETRIC MODELING FOR THE OREGON HEALTH FUND BOARD Final Report February 2009 SUMMARY The Oregon Health Fund Board worked with consultants from the Massachusetts Institute
Medicaid. (Title XIX and Title XXI) STATE REPORTS FY 2001. Division of Health Services Research VIRGINIA. SUK-FONG S TANG, PhD.
 STATE REPORTS FY 2001. Division of Health Services Research VIRGINIA. SUK-FONG S TANG, PhD.") Medicaid STATE REPORTS FY 2001 (Title XIX and Title XXI) Text7: Division of Health Services Research SUK-FONG S TANG, PhD General Information about CMS/MSIS2082, data source of this report: (Based on CMS
Medicaid STATE REPORTS FY 2001 (Title XIX and Title XXI) Text7: Division of Health Services Research SUK-FONG S TANG, PhD General Information about CMS/MSIS2082, data source of this report: (Based on CMS
Medical Assistance Program Importance and Alternatives
 Report 11-15 December 2011 An Evaluation Medical Assistance Program Department of Health Services 2011-2012 Joint Legislative Audit Committee Members Senate Members: Robert Cowles, Co-chairperson Mary
Report 11-15 December 2011 An Evaluation Medical Assistance Program Department of Health Services 2011-2012 Joint Legislative Audit Committee Members Senate Members: Robert Cowles, Co-chairperson Mary
Bending the Health Care Cost Curve by Expanding Alcohol/Drug Treatment
 September 2010 RDA Report 4.81 Olympia, Washington Bending the Health Care Cost Curve by Expanding Alcohol/Drug Treatment David Mancuso, PhD and Barbara E.M. Felver, MES, MPA In collaboration with the
September 2010 RDA Report 4.81 Olympia, Washington Bending the Health Care Cost Curve by Expanding Alcohol/Drug Treatment David Mancuso, PhD and Barbara E.M. Felver, MES, MPA In collaboration with the
MONROE COUNTY OFFICE OF MENTAL HEALTH, DEPARTMENT OF HUMAN SERVICES RECOVERY CONNECTION PROJECT PROGRAM EVALUATION DECEMBER 2010
 MONROE COUNTY OFFICE OF MENTAL HEALTH, DEPARTMENT OF HUMAN SERVICES RECOVERY CONNECTION PROJECT PROGRAM EVALUATION DECEMBER 2010 Prepared For: Kathleen Plum, RN, PhD Director, Monroe County Office of Mental
MONROE COUNTY OFFICE OF MENTAL HEALTH, DEPARTMENT OF HUMAN SERVICES RECOVERY CONNECTION PROJECT PROGRAM EVALUATION DECEMBER 2010 Prepared For: Kathleen Plum, RN, PhD Director, Monroe County Office of Mental
Expanding Medicaid in Ohio
 Expanding Medicaid in Ohio Analysis of likely effects February 2013 Introduction The Ohio Medicaid Expansion Study ( study ) was conducted to inform Ohio s leaders who must decide whether to expand Medicaid
Expanding Medicaid in Ohio Analysis of likely effects February 2013 Introduction The Ohio Medicaid Expansion Study ( study ) was conducted to inform Ohio s leaders who must decide whether to expand Medicaid
WHAT S IN THE PROPOSED FY 2016 BUDGET FOR HEALTH CARE?
 An Affiliate of the Center on Budget and Policy Priorities 820 First Street NE, Suite 460 Washington, DC 20002 (202) 408-1080 Fax (202) 408-1073 www.dcfpi.org April 16, 2015 WHAT S IN THE PROPOSED FY 2016
An Affiliate of the Center on Budget and Policy Priorities 820 First Street NE, Suite 460 Washington, DC 20002 (202) 408-1080 Fax (202) 408-1073 www.dcfpi.org April 16, 2015 WHAT S IN THE PROPOSED FY 2016
TOBACCO CESSATION PILOT PROGRAM. Report to the Texas Legislature
 TOBACCO CESSATION PILOT PROGRAM Report to the Texas Legislature As Required by S.B. 10, 80 th Legislature, Regular Session, 2007 Texas Health and Human Services Commission September 2010 Table of Contents
TOBACCO CESSATION PILOT PROGRAM Report to the Texas Legislature As Required by S.B. 10, 80 th Legislature, Regular Session, 2007 Texas Health and Human Services Commission September 2010 Table of Contents
Health Insurance Coverage: Early Release of Estimates From the National Health Interview Survey, January March 2013
 Health Insurance Coverage: Early Release of Estimates From the National Health Interview Survey, January March 2013 by Robin A. Cohen, Ph.D., and Michael E. Martinez, M.P.H., M.H.S.A. Division of Health
Health Insurance Coverage: Early Release of Estimates From the National Health Interview Survey, January March 2013 by Robin A. Cohen, Ph.D., and Michael E. Martinez, M.P.H., M.H.S.A. Division of Health
Care needs for dual-eligible beneficiaries
 C h a p t e r6 Care needs for dual-eligible beneficiaries C H A P T E R 6 Care needs for dual-eligible beneficiaries Chapter summary In this chapter Dual-eligible beneficiaries are eligible for both Medicare
C h a p t e r6 Care needs for dual-eligible beneficiaries C H A P T E R 6 Care needs for dual-eligible beneficiaries Chapter summary In this chapter Dual-eligible beneficiaries are eligible for both Medicare
Chapter 3: Healthy Start Risk Screening
 Introduction Healthy Start legislation requires that all pregnant women and infants be offered screening for risk factors that may affect their pregnancy, health, or development. The prenatal and infant
Introduction Healthy Start legislation requires that all pregnant women and infants be offered screening for risk factors that may affect their pregnancy, health, or development. The prenatal and infant
Office of Health Transformation Extend Medicaid Coverage and Automate Enrollment
 Office of Health Transformation Extend Medicaid Coverage and Automate Enrollment Background: Eligibility determination for health and human services programs in Ohio are fragmented, overly complex, and
Office of Health Transformation Extend Medicaid Coverage and Automate Enrollment Background: Eligibility determination for health and human services programs in Ohio are fragmented, overly complex, and
Analysis of the Costs and Impact of Universal Health Care Models for the State of Maryland: The Single-Payer and Multi-Payer Models
 Analysis of the Costs and Impact of Universal Health Care Models for the State of Maryland: The Single-Payer and Multi-Payer Models Final Report Presented to: The Maryland Citizens Health Initiative Education
Analysis of the Costs and Impact of Universal Health Care Models for the State of Maryland: The Single-Payer and Multi-Payer Models Final Report Presented to: The Maryland Citizens Health Initiative Education
FINDINGS FROM THE 2014 MASSACHUSETTS HEALTH INSURANCE SURVEY
 CENTER FOR HEALTH INFORMATION AND ANALYSIS FINDINGS FROM THE MASSACHUSETTS HEALTH INSURANCE SURVEY MAY 2015 Prepared by: Laura Skopec and Sharon K. Long, Urban Institute Susan Sherr, David Dutwin, and
CENTER FOR HEALTH INFORMATION AND ANALYSIS FINDINGS FROM THE MASSACHUSETTS HEALTH INSURANCE SURVEY MAY 2015 Prepared by: Laura Skopec and Sharon K. Long, Urban Institute Susan Sherr, David Dutwin, and
State of Alaska Health and Social Services Medicaid Study
 State of Alaska Health and Social Services Medicaid Study Prepared by Mike Humphrey Gregg Davis, PhD Bernard Khomenko The Wilson Agency, LLC 3000 A Street, Suite 400 Anchorage, AK 99503 Phone: (907) 277-1616
State of Alaska Health and Social Services Medicaid Study Prepared by Mike Humphrey Gregg Davis, PhD Bernard Khomenko The Wilson Agency, LLC 3000 A Street, Suite 400 Anchorage, AK 99503 Phone: (907) 277-1616
Evaluations. Nursing Contact Hours, CME and CHES credits are available.
 Evaluations Nursing Contact Hours, CME and CHES credits are available. Please visit www.phlive.org to fill out your evaluation and complete the post-test. 1 Conflict of Interest & Disclosure Statements
Evaluations Nursing Contact Hours, CME and CHES credits are available. Please visit www.phlive.org to fill out your evaluation and complete the post-test. 1 Conflict of Interest & Disclosure Statements
BadgerCare Plus Standard Plan
 BadgerCare Plus Standard Plan Part 6 BadgerCare Plus BadgerCare Plus (BC+) is a state/federal program that provides health coverage for Wisconsin families. 1 BadgerCare Plus Potential BC+ members include:
BadgerCare Plus Standard Plan Part 6 BadgerCare Plus BadgerCare Plus (BC+) is a state/federal program that provides health coverage for Wisconsin families. 1 BadgerCare Plus Potential BC+ members include:
uninsured RESEARCH BRIEF: INSURANCE COVERAGE AND ACCESS TO CARE IN PRIMARY CARE SHORTAGE AREAS
 kaiser commission on medicaid and the uninsured RESEARCH BRIEF: INSURANCE COVERAGE AND ACCESS TO CARE IN PRIMARY CARE SHORTAGE AREAS Prepared by Catherine Hoffman, Anthony Damico, and Rachel Garfield The
kaiser commission on medicaid and the uninsured RESEARCH BRIEF: INSURANCE COVERAGE AND ACCESS TO CARE IN PRIMARY CARE SHORTAGE AREAS Prepared by Catherine Hoffman, Anthony Damico, and Rachel Garfield The
Improving Service Delivery Through Administrative Data Integration and Analytics
 Improving Service Delivery Through Administrative Data Integration and Analytics Getty Images David Mancuso, PhD October 2, 2015 1 Analytics in the Social and Health Service Environment Program costs are
Improving Service Delivery Through Administrative Data Integration and Analytics Getty Images David Mancuso, PhD October 2, 2015 1 Analytics in the Social and Health Service Environment Program costs are
REACHING THE REMAINING UNINSURED IN MASSACHUSETTS: CHALLENGES AND OPPORTUNITIES
 REACHING THE REMAINING IN MASSACHUSETTS: CHALLENGES AND OPPORTUNITIES MARCH 2013 Sharon K. Long Dana Goin Victoria Lynch Urban Institute EXECUTIVE SUMMARY While Massachusetts has the lowest uninsurance
REACHING THE REMAINING IN MASSACHUSETTS: CHALLENGES AND OPPORTUNITIES MARCH 2013 Sharon K. Long Dana Goin Victoria Lynch Urban Institute EXECUTIVE SUMMARY While Massachusetts has the lowest uninsurance
How Health Reform Will Help Children with Mental Health Needs
 How Health Reform Will Help Children with Mental Health Needs The new health care reform law, called the Affordable Care Act (or ACA), will give children who have mental health needs better access to the
How Health Reform Will Help Children with Mental Health Needs The new health care reform law, called the Affordable Care Act (or ACA), will give children who have mental health needs better access to the
Health Insurance Coverage: Early Release of Estimates From the National Health Interview Survey, January June 2013
 Health Insurance Coverage: Early Release of Estimates From the National Health Interview Survey, January June 2013 by Michael E. Martinez, M.P.H., M.H.S.A., and Robin A. Cohen, Ph.D. Division of Health
Health Insurance Coverage: Early Release of Estimates From the National Health Interview Survey, January June 2013 by Michael E. Martinez, M.P.H., M.H.S.A., and Robin A. Cohen, Ph.D. Division of Health
issue brief Medicaid: A Key Source of Insurance in New Hampshire
 issue brief April 20, 2011 Medicaid: A Key Source of Insurance in New Hampshire As state and federal policymakers come to grips with substantial budget shortfalls both now and into the future one public
issue brief April 20, 2011 Medicaid: A Key Source of Insurance in New Hampshire As state and federal policymakers come to grips with substantial budget shortfalls both now and into the future one public
Family Income and the Impact of a Children s Health Insurance Program on Reported Need for Health Services and Unmet Health Need
 Family Income and the Impact of a Children s Health Insurance Program on Reported Need for Health Services and Unmet Health Need Emily Feinberg, ScD* ; Kathy Swartz, PhD ; Alan Zaslavsky, PhD ; Jane Gardner,
Family Income and the Impact of a Children s Health Insurance Program on Reported Need for Health Services and Unmet Health Need Emily Feinberg, ScD* ; Kathy Swartz, PhD ; Alan Zaslavsky, PhD ; Jane Gardner,
The Patient Protection and Affordable Care Act. Implementation Timeline
 The Patient Protection and Affordable Care Act Implementation Timeline 2009 Credit to Encourage Investment in New Therapies: A two year temporary credit subject to an overall cap of $1 billion to encourage
The Patient Protection and Affordable Care Act Implementation Timeline 2009 Credit to Encourage Investment in New Therapies: A two year temporary credit subject to an overall cap of $1 billion to encourage
Chapter 7 Acute Care Inpatient/Outpatient Hospital Services
 Chapter 7: Acute Care Inpatient/ Outpatient Hospital Services Executive Summary Description Acute care hospitals are the largest group of enrolled hospital providers. Kansas Medicaid has 144 acute care
Chapter 7: Acute Care Inpatient/ Outpatient Hospital Services Executive Summary Description Acute care hospitals are the largest group of enrolled hospital providers. Kansas Medicaid has 144 acute care
The Effect of Public Insurance Coverage for Childless Adults on Labor Supply
 DISCUSSION PAPER SERIES IZA DP No. 8187 The Effect of Public Insurance Coverage for Childless Adults on Labor Supply Laura Dague Thomas DeLeire Lindsey Leininger May 2014 Forschungsinstitut zur Zukunft
DISCUSSION PAPER SERIES IZA DP No. 8187 The Effect of Public Insurance Coverage for Childless Adults on Labor Supply Laura Dague Thomas DeLeire Lindsey Leininger May 2014 Forschungsinstitut zur Zukunft
Report to Congress. Improving the Identification of Health Care Disparities in. Medicaid and CHIP
 Report to Congress Improving the Identification of Health Care Disparities in Medicaid and CHIP Sylvia Mathews Burwell Secretary of the Department of Health and Human Services November 2014 TABLE OF CONTENTS
Report to Congress Improving the Identification of Health Care Disparities in Medicaid and CHIP Sylvia Mathews Burwell Secretary of the Department of Health and Human Services November 2014 TABLE OF CONTENTS
IowaCare. Purpose. Who Is Helped. IowaCare Enrollment. Member Percent of Poverty (July 2012) 201+ opregnant Women 0.8%
 201+ opregnant Women 0.8%") IowaCare Purpose Who Is Helped IowaCare is an expansion of Medicaid authorized through an 1115 demonstration waiver. It provides limited health benefits to low income adults who do not otherwise qualify
IowaCare Purpose Who Is Helped IowaCare is an expansion of Medicaid authorized through an 1115 demonstration waiver. It provides limited health benefits to low income adults who do not otherwise qualify
Health, Private and Public Insurance, G 15, 16. U.S. Health care > 16% of GDP (7% in 1970), 8% in U.K. and Sweden, 11% in Switzerland.
, 8% in U.K. and Sweden, 11% in Switzerland.") Health, Private and Public Insurance, G 15, 16 U.S. Health care > 16% of GDP (7% in 1970), 8% in U.K. and Sweden, 11% in Switzerland. 60% have private ins. as primary ins. Insured pay about 20% out of
Health, Private and Public Insurance, G 15, 16 U.S. Health care > 16% of GDP (7% in 1970), 8% in U.K. and Sweden, 11% in Switzerland. 60% have private ins. as primary ins. Insured pay about 20% out of
TABLE OF CONTENTS INTRODUCTION CONSUMER RIGHTS. All Health Plans. Page. olorado law provides you certain protections regarding health insurance.
 TABLE OF ONTENTS INTRODUTION ONSUMER RIGHTS WHAT RIGHTS DO I HAVE REGARDING HEALTH INSURANE? A BROHURE EXPLAINING HOW YOU ARE PROTETED BY STATE LAW A publication of the Department of Regulatory Agencies
TABLE OF ONTENTS INTRODUTION ONSUMER RIGHTS WHAT RIGHTS DO I HAVE REGARDING HEALTH INSURANE? A BROHURE EXPLAINING HOW YOU ARE PROTETED BY STATE LAW A publication of the Department of Regulatory Agencies