How To Achieve a Patient Centered Medical Home (PCMH) Using
|
|
|
- Penelope Blake
- 7 years ago
- Views:
Transcription

1 How To Achieve a Patient Centered Medical Home (PCMH) Using Nusrat Khan M.D. MBA FAAP Medical Director, MedPeds Medical Clinic, PA Robbye Penrod CPC RMC RMA Office Manager, MedPeds Medical Clinic, PA
2 MedPeds Medical Clinic, PA Internal Medicine and Pediatrics NCQA PCMH Level III Certified Facility (by 2011 Standards ) 1 st Clinic in Texas to Achieve this Status under NCQA 2011 credentialing guidelines NCQA Recognition in Diabetes Care Management (DRP) NCQA Recognition in Heart/Stroke Care Management (HSRP) Bridges to Excellence Recognition in Medical Home Clinic Bridges to Excellence Recognition in Diabetes Care Bridges to Excellence Recognition in Preventative Cardiac Care Bridges to Excellence Recognition in Coronary Artery Disease Bridges to Excellence Recognition in Office Systems Management
3 PCMH and Primary Care Concept supported by the: American Academy of Family Physicians American College of Physicians American Academy of Pediatrics American Osteopathic Association American Association of Nurse Practitioners American Association of Physician Assistants -Principles for the Patient Centered Medical Home; this defines critical principles within the PCMH model.

4 What is PCMH?
5 PCMH-The Concept Enhanced Patient Access - during and after office hours Team-Based Care approach from the clinic team Improved delivery & tracking of preventive services Clinical excellence in chronic disease management Improved care at Transition of Care points: Reduced utilization of ER and hospitals Shared Decision Making: better quality and experience of care Long-term Patient & Provider Relationships High performing, cost effective, integrated care delivery system
6 Why bother with PCMH? POINT Primary care reimbursement has not kept pace with the care burden For now there is no incentive payments for PCMH COUNTER POINT Market forces & regulations within the system are forcing changes in healthcare: the practice of medicine is transforming Consumers of healthcare are demanding better access to care, and third party payers are transitioning to pay for performance There is a tsunami of change that is going to move us away from a fee for service industry PCMH concepts are born out a need for such health care reform
7 Standard 1 Enhance Access and Continuity Access during office hours Access after hours Electronic access Continuity Medical Home responsibilities Culturally and linguistically appropriate Practice Team Approach
8 Access During Office Hours Provide Same-day appointments Provide timely clinical advice by telephone during office hours Provide clinical advice by secure electronic messages during office hours Documenting clinical advice in medical record
9 What We did Improved Access to Care Offered timely care during & after hours --innovative scheduling Adopted patient portals (Updox and A Charts) Electronic messaging Educated our patients to Call Us First --so that we could direct their care

10 Electronic Access Through
11 Standard 2 Identify and Manage Patient Populations Patient Information- demographics Clinical Data- problem list, allergies, vital signs Comprehensive Health Assessment -PMHx, SocHx, Advance Care Planning, Developmental screenings, Depression screening
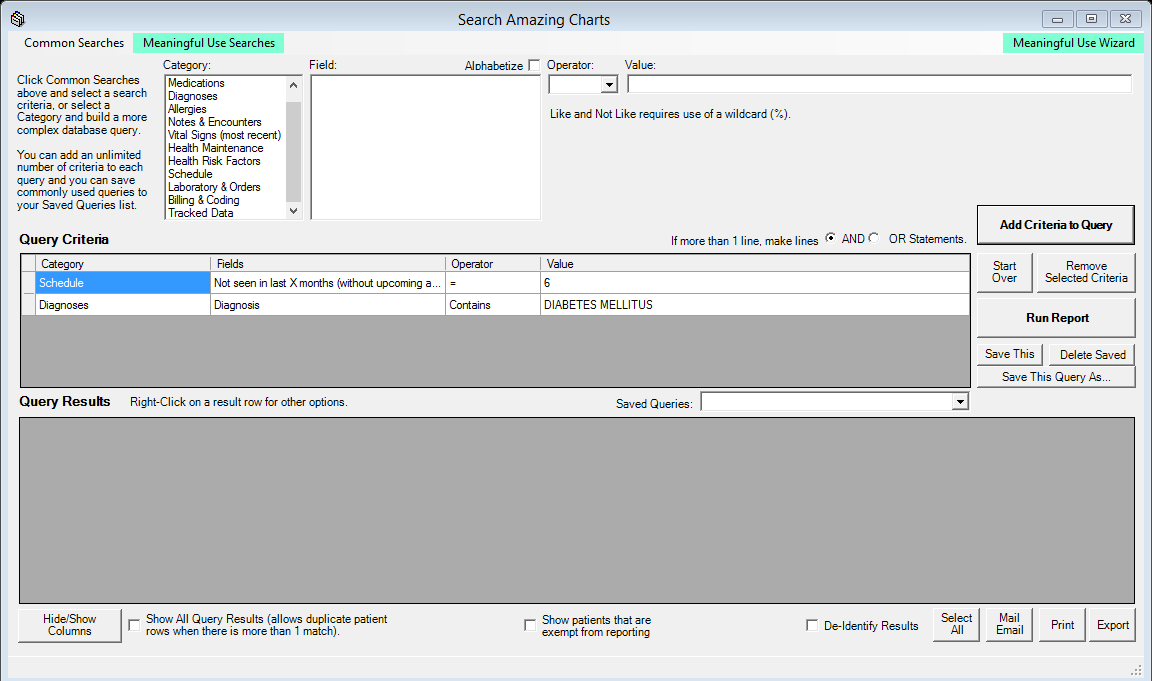
12 What We did Use Amazing Charts to create reminders in the system for age appropriate screenings Chronic Disease specific services:- example in DM, CKD Use Amazing Charts to identify chronic disease patients = high utilizers of care Use Amazing Charts to identify noncompliance with follow-up
13
14 Standard 3 Plan and Manage Care Implement Evidence Based guidelines Identify High Risk Patients Care Management Medication Management Use Electronic Prescribing
15 Care Management Conducts pre-visit preparations Collaborates with patient to develop individual care plan and gives patient written plan of care Assesses barriers when the patient has not met treatment goals Identifies patients who might benefit from additional care/management support
16 What We Did Creating a healthcare delivery team in the office Diabetes Team Leader Preventative Care Team Leader Patient Care Coordinator Individual Care Plan
17 Standard 4 Provide Self-Care Support and Community Resources Support Self-Care Process Provide Referrals to Community Resources
18 Provide Self-Care Support Use EHR to identify patient-specific education resources and provide them to more than 10% of patients
19 What We did Enhanced our website to include patient education accessible 24/7 Began a monthly newsletter to inform patients about current healthcare issues and ongoing series such as Diabetes Today Began in-house Diabetes Education Classes Made a registry of community based resources
20 Standard 5 Track and Coordinate Care Test Tracking and Follow-up Referral Tracking and Follow-up Coordinate with Facilities/Care Transitions
21 What We Did Care co-ordination with specialists Continuity of care at Transition of Care points:-hospital d/c, rehab d/c, etc. Clinical Care Coordinator continues to play a role
22 Referral Tracking and Follow-up Demonstrate electronic exchange of key clinical information between clinicians
23 Standard 6 Measure and Improve Performance Measure Performance Measure Patient Experience Implement Continuous Quality Improvements Demonstrate Continuous Quality Improvements Report Performance Report Data Externally Use of Certified EHR Technology
24 Demonstrate Continuous Improvement Track Results Over Time Assessing the effect of its action Achieving improved performance on one measure Achieving improved performance on a second measure
25 What We did Surveyed our patients to obtain their perceptions of care and customer service Assessed and addressed areas for improvement Re-Surveyed our patients The Importance of Surveys Meaningful Use-2 CG-CAHPS MOC
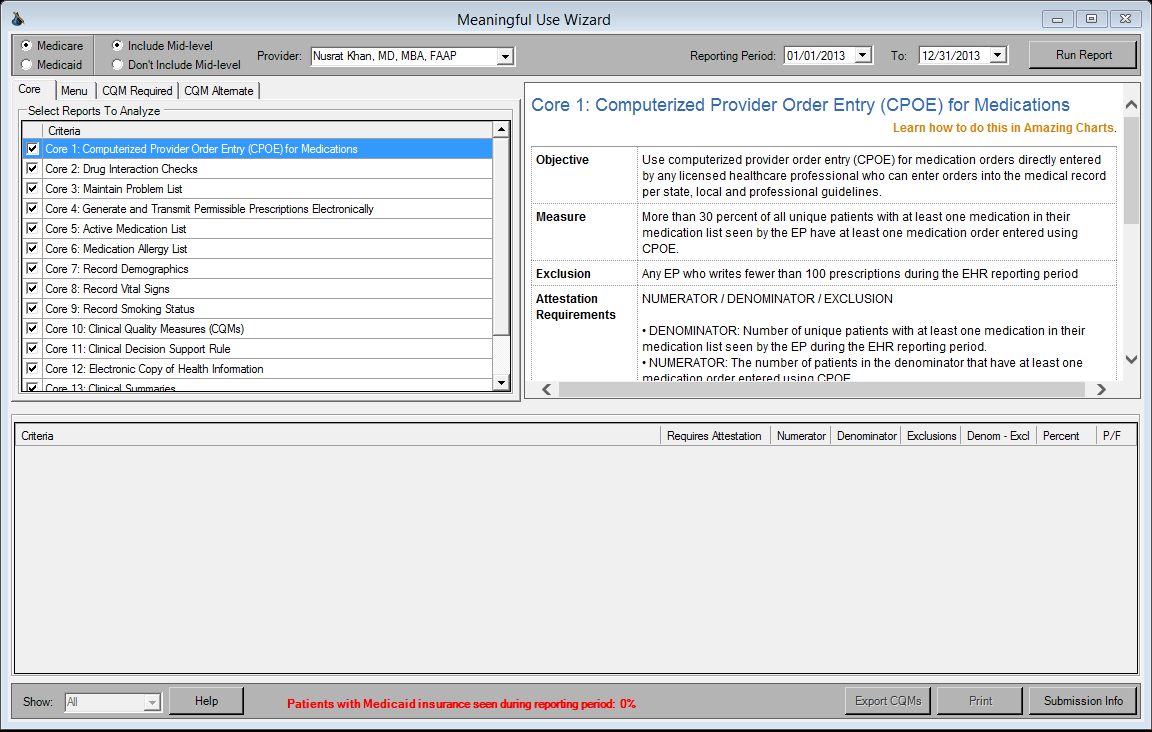
26 Meaningful Use Data
27 PCMH: one size does not fit all Its not for every practice. and may not be needed for every patient in the practice Large healthcare delivery systems seem to be adopting it first. Smaller practices may have challenges in such transformation. Strategy:- Chronic disease = high risk patients = >High utilizers of care. Particular focus on the complex patients Pay 4 Performance Friedberg M. et al. Association Between Participation in a Multipayer Medical Home Intervention and Changes in Quality, Utilization, and Costs of Care.JAMA.2014;311(8) Schwenk,T. The Patient Centered Medical Home. One size Does Not Fit All. JAMA.Feb
28 Consider PCMH Concepts use on High Utilizers of Care Use Amazing Charts Queries to: cull data on subset populations identify high risk groups Identify patients that need further intervention in care Identify lack of follow-up Resolve poly-pharmacy and medication interaction issues at point of care
29 Proposal for Your Practice Establish a Clinical Care Coordinator in office Intervene at Transition of Care points Enhance communication with your specialists Survey your patient perceptions of care
30 Creating a Healthcare Delivery Team in Your Office Keep employees who share in the vision and mission of the organization Evolve away from top-down leadership trends into a shared leadership philosophy Assign specific task oriented roles to specific team members.. identify the strength of each employee and utilize it but cross train all employees shared decision making ---listen to patients and employees regularly. Regular team meetings.
31 Questions & Discussion.
32 Care Management Codes Transitional Care Management Services with the following required elements: Communication (direct contact, telephone, electronic) with the patient and/or caregiver within 2 business days of discharge Medical decision making of at least moderate complexity during the service period Face-to-face visit, within 14 calendar days of discharge Transitional Care Management Services with the following required elements: Communication (direct contact, telephone, electronic) with the patient and/or caregiver within 2 business days of discharge Medical decision making of high complexity during the service period Face-to-face visit, within 7 calendar days of discharge
Physician Practice Connections Patient Centered Medical Home
 Physician Practice Connections Patient Centered Medical Home Getting Started Any practice assessing its ability to achieve NCQA Physician Recognition in PPC- PCMH is taking a bold step toward aligning
Physician Practice Connections Patient Centered Medical Home Getting Started Any practice assessing its ability to achieve NCQA Physician Recognition in PPC- PCMH is taking a bold step toward aligning
NCQA PCMH 2011 Standards, Elements and Factors Documentation Guideline/Data Sources
 NCQA PCMH 2011 Standards, Elements and Factors Documentation Guideline/Data Sources Key: DP = Documented Process N/D = Report numerator and denominator creating percent of use RPT = Report of data or information
NCQA PCMH 2011 Standards, Elements and Factors Documentation Guideline/Data Sources Key: DP = Documented Process N/D = Report numerator and denominator creating percent of use RPT = Report of data or information
NCQA Standards Workshop Patient-Centered Medical Home PCMH 2011. Part 1: Standards 1-3
 NCQA Standards Workshop PCMH 2011 Part 1: Standards 1-3 Agenda: Part 1 Overview Content of PCMH 2011 Standards 1 3 Documentation examples* * Examples in the presentation only illustrate the element intent.
NCQA Standards Workshop PCMH 2011 Part 1: Standards 1-3 Agenda: Part 1 Overview Content of PCMH 2011 Standards 1 3 Documentation examples* * Examples in the presentation only illustrate the element intent.
PCMH and Care Management: Where do we start?
 PCMH and Care Management: Where do we start? Patricia Bohs, RN, BSN Quality Assurance Manager Kelly McCloughan QA Data Manager Wayne Memorial Community Health Centers Honesdale, PA Wayne Memorial Community
PCMH and Care Management: Where do we start? Patricia Bohs, RN, BSN Quality Assurance Manager Kelly McCloughan QA Data Manager Wayne Memorial Community Health Centers Honesdale, PA Wayne Memorial Community
Turning on the Care Coordination Switch in Rural Primary Care Practices
 Turning on the Care Coordination Switch in Rural Primary Care Practices AHRQ Master Contract Task Order #5 HHSA2902007100016I (9/07-11/09) Care Management Plus research at OHSU is supported by funding
Turning on the Care Coordination Switch in Rural Primary Care Practices AHRQ Master Contract Task Order #5 HHSA2902007100016I (9/07-11/09) Care Management Plus research at OHSU is supported by funding
Continuity of Care Guide for Ambulatory Medical Practices
 Continuity of Care Guide for Ambulatory Medical Practices www.himss.org t ra n sf o r m i ng he a lth c a re th rou g h IT TM Table of Contents Introduction 3 Roles and Responsibilities 4 List of work/responsibilities
Continuity of Care Guide for Ambulatory Medical Practices www.himss.org t ra n sf o r m i ng he a lth c a re th rou g h IT TM Table of Contents Introduction 3 Roles and Responsibilities 4 List of work/responsibilities
Patient Centered Medical Homes
 Patient Centered Medical Homes Paul Kleeberg, MD, FAAFP, FHIMSS CMIO Stratis Health North Dakota e-health Summit November 20, 2013 REACH - Achieving - Achieving meaningful meaningful use of your use EHR
Patient Centered Medical Homes Paul Kleeberg, MD, FAAFP, FHIMSS CMIO Stratis Health North Dakota e-health Summit November 20, 2013 REACH - Achieving - Achieving meaningful meaningful use of your use EHR
Patient-Centered Medical Home (PCMH) 2014
 2014") Patient-Centered Medical Home (PCMH) 2014 Part 1: Standards 1-3 All materials 2014, National Committee for Quality Assurance Agenda Part 1 Content t of PCMH 2014 Standards d and Guidelines Standards 1
Patient-Centered Medical Home (PCMH) 2014 Part 1: Standards 1-3 All materials 2014, National Committee for Quality Assurance Agenda Part 1 Content t of PCMH 2014 Standards d and Guidelines Standards 1
Patient Centered Medical Home: An Approach for the Health Plan
 : An Approach for the Health Plan By Marissa A. Harper and JoAnn E. Balara Excellence in healthcare consulting The Medical Home Concept Works Recent Medicare demonstration projects on Patient Centered
: An Approach for the Health Plan By Marissa A. Harper and JoAnn E. Balara Excellence in healthcare consulting The Medical Home Concept Works Recent Medicare demonstration projects on Patient Centered
Chronic Care Management (CCM) from a Physician Practice Administrator s Perspective
 from a Physician Practice Administrator s Perspective") Chronic Care Management (CCM) from a Physician Practice Administrator s Perspective Chronic Care Management (CCM) from a Physician Practice Administrator s Perspective 1 ABOUT THE AUTHOR Dennis Breslin
Chronic Care Management (CCM) from a Physician Practice Administrator s Perspective Chronic Care Management (CCM) from a Physician Practice Administrator s Perspective 1 ABOUT THE AUTHOR Dennis Breslin
GUIDELINES FOR ADVERTISING AND MARKETING RECOGNITION PROGRAMS. Table of Contents
 GUIDELINES FOR ADVERTISING AND MARKETING RECOGNITION PROGRAMS Table of Contents INTRODUCTION 2 USE OF RECOGNITION SEALS 2 GUIDELINES FOR MARKETING AND ADVERTISING RECOGNITION 4 APPROVED QUOTE 6 RECOMMENDED
GUIDELINES FOR ADVERTISING AND MARKETING RECOGNITION PROGRAMS Table of Contents INTRODUCTION 2 USE OF RECOGNITION SEALS 2 GUIDELINES FOR MARKETING AND ADVERTISING RECOGNITION 4 APPROVED QUOTE 6 RECOMMENDED
Advancing Health Equity. Through national health care quality standards
 Advancing Health Equity Through national health care quality standards TABLE OF CONTENTS Stage 1 Requirements for Certified Electronic Health Records... 3 Proposed Stage 2 Requirements for Certified Electronic
Advancing Health Equity Through national health care quality standards TABLE OF CONTENTS Stage 1 Requirements for Certified Electronic Health Records... 3 Proposed Stage 2 Requirements for Certified Electronic
Care Navigation Council. Nenick Vu Care Navigation Council Director
 Care Navigation Council Nenick Vu Care Navigation Council Director Care Navigation Council The Challenge With the passage of the Affordable Care Act, Medi-Cal coverage for all legally present low income
Care Navigation Council Nenick Vu Care Navigation Council Director Care Navigation Council The Challenge With the passage of the Affordable Care Act, Medi-Cal coverage for all legally present low income
Kaiser Permanente of Ohio
 Kaiser Permanente of Ohio Chronic Disease Management Program March 11, 2011 Presenters: Amy Kramer and Audrey L. Callahan 1 Objectives 1. Define the roles and responsibilities of the Care Managers in the
Kaiser Permanente of Ohio Chronic Disease Management Program March 11, 2011 Presenters: Amy Kramer and Audrey L. Callahan 1 Objectives 1. Define the roles and responsibilities of the Care Managers in the
Meaningful Use. Goals and Principles
 Meaningful Use Goals and Principles 1 HISTORY OF MEANINGFUL USE American Recovery and Reinvestment Act, 2009 Two Programs Medicare Medicaid 3 Stages 2 ULTIMATE GOAL Enhance the quality of patient care
Meaningful Use Goals and Principles 1 HISTORY OF MEANINGFUL USE American Recovery and Reinvestment Act, 2009 Two Programs Medicare Medicaid 3 Stages 2 ULTIMATE GOAL Enhance the quality of patient care
Appendix 2. PCMH 2014 and CMS Stage 2 Meaningful Use Requirements
 Appendix 2 PCMH 2014 and CMS Stage 2 Meaningful Use Requirements Appendix 2 PCMH 2014 and CMS Stage 2 Meaningful Use Requirements 2-1 APPENDIX 2 PCMH 2014 AND CMS STAGE 2 MEANINGFUL USE REQUIREMENTS Medicare
Appendix 2 PCMH 2014 and CMS Stage 2 Meaningful Use Requirements Appendix 2 PCMH 2014 and CMS Stage 2 Meaningful Use Requirements 2-1 APPENDIX 2 PCMH 2014 AND CMS STAGE 2 MEANINGFUL USE REQUIREMENTS Medicare
The Health Care Incentives Improvement Institute 13 Sugar Street Newtown, CT 06470
 Clinician Guide: Bridges to Excellence Congestive Heart Failure Care Recognition Program The Health Care Incentives Improvement Institute 13 Sugar Street Newtown, CT 06470 bteinformation@bridgestoexcellence.org
Clinician Guide: Bridges to Excellence Congestive Heart Failure Care Recognition Program The Health Care Incentives Improvement Institute 13 Sugar Street Newtown, CT 06470 bteinformation@bridgestoexcellence.org
ESSENTIA HEALTH AS AN ACO (ACCOUNTABLE CARE ORGANIZATION)
") ESSENTIA HEALTH AS AN ACO (ACCOUNTABLE CARE ORGANIZATION) Hello and welcome. Thank you for taking part in this presentation entitled "Essentia Health as an ACO or Accountable Care Organization -- What
ESSENTIA HEALTH AS AN ACO (ACCOUNTABLE CARE ORGANIZATION) Hello and welcome. Thank you for taking part in this presentation entitled "Essentia Health as an ACO or Accountable Care Organization -- What
Our Patient-Centered Medical Home a Process, not a Click
 Our Patient-Centered Medical Home a Process, not a Click Richard Johnston, M.D. President, Medical Clinic of North Texas, P.A. Medical Clinic of North Texas, P.A. MCNT Physician Owned Primary Care Medical
Our Patient-Centered Medical Home a Process, not a Click Richard Johnston, M.D. President, Medical Clinic of North Texas, P.A. Medical Clinic of North Texas, P.A. MCNT Physician Owned Primary Care Medical
CROSSWALK NCQA 2014 PCMH HRSA 19 Requirements Meaningful Use
 P a g e 1 CROSSWALK NCQA 2014 PCMH HRSA 19 Requirements Meaningful Use PCMH 1 PATIENT-CENTERED ACCESS 1A Patient-Centered Appointment Access (Must Pass) No.4 Accessible Hours of Operation / Locations 1B
P a g e 1 CROSSWALK NCQA 2014 PCMH HRSA 19 Requirements Meaningful Use PCMH 1 PATIENT-CENTERED ACCESS 1A Patient-Centered Appointment Access (Must Pass) No.4 Accessible Hours of Operation / Locations 1B
Welcome to Crozer-Keystone Health Network Primary Care
 Welcome to Crozer-Keystone Health Network Primary Care A Guide to Your CKHN Patient-Centered Medical Home: What you can expect from us... What we will need from you......so you can gain the full benefits
Welcome to Crozer-Keystone Health Network Primary Care A Guide to Your CKHN Patient-Centered Medical Home: What you can expect from us... What we will need from you......so you can gain the full benefits
MaineCare Value Based Purchasing Initiative
 MaineCare Value Based Purchasing Initiative The Accountable Communities Strategy Jim Leonard, Deputy Director, MaineCare Peter Kraut, Acting Accountable Communities Program Manager Why Value-Based Purchasing
MaineCare Value Based Purchasing Initiative The Accountable Communities Strategy Jim Leonard, Deputy Director, MaineCare Peter Kraut, Acting Accountable Communities Program Manager Why Value-Based Purchasing
Adirondack Region Medical Home Pilot
 Adirondack Region Medical Home Pilot John Rugge, M.D Adirondack Health Institute Patient-Centered Primary Care Collaborative February 10, 2011 Demographics Population ~ 200,000 Micropolitan (2)/Rural/Frontier
Adirondack Region Medical Home Pilot John Rugge, M.D Adirondack Health Institute Patient-Centered Primary Care Collaborative February 10, 2011 Demographics Population ~ 200,000 Micropolitan (2)/Rural/Frontier
Community Health Centers and Health Reform: Issues and Ideas for States
 Community Health Centers and Health Reform: Issues and Ideas for States Ann S. Torregrossa, Esq. Deputy Director & Director of Policy Governor s Office of Health Care Reform Commonwealth of Pennsylvania
Community Health Centers and Health Reform: Issues and Ideas for States Ann S. Torregrossa, Esq. Deputy Director & Director of Policy Governor s Office of Health Care Reform Commonwealth of Pennsylvania
Patient Centered Medical Home
 Patient Centered Medical Home 2013 2014 Program Overview Florida Blue is a trade name of Blue Cross and Blue Shield of Florida Inc., an Independent Licensee of the Blue Cross and Blue Shield Association.
Patient Centered Medical Home 2013 2014 Program Overview Florida Blue is a trade name of Blue Cross and Blue Shield of Florida Inc., an Independent Licensee of the Blue Cross and Blue Shield Association.
Announcing New York Medicaid s Statewide Patient-Centered Medical Home Incentive Program
 DECEMBER 2009 SPECIAL EDITION Volume 25, Number 16, DAVID A. PATERSON GOVERNOR State of New York RICHARD F. DAINES, M.D. COMMISSIONER New York State DOH New York State DECEMBER 2009 SPECIAL EDITION NEW
DECEMBER 2009 SPECIAL EDITION Volume 25, Number 16, DAVID A. PATERSON GOVERNOR State of New York RICHARD F. DAINES, M.D. COMMISSIONER New York State DOH New York State DECEMBER 2009 SPECIAL EDITION NEW
Medical Homes- Understanding the Model Bob Perna, MBA, FACMPE WSMA Practice Resource Center
 Bob Perna, MBA, FACMPE WSMA Practice Resource Center Bob Perna, MBA, FACMPE Senior Director, WSMA Practice Resource Center E-mail: rjp@wsma.org Phone: 206.441.9762 1.800.552.0612 2 Program Objectives:
Bob Perna, MBA, FACMPE WSMA Practice Resource Center Bob Perna, MBA, FACMPE Senior Director, WSMA Practice Resource Center E-mail: rjp@wsma.org Phone: 206.441.9762 1.800.552.0612 2 Program Objectives:
Patient-Centered Medical Home. Transform Your Practice
 Patient-Centered Medical Home Transform Your Practice 1 The New York ehealth Collaborative (NYeC) Regional Extension Center (REC) The NYeC Regional Extension Center is the physician s trusted advisor in
Patient-Centered Medical Home Transform Your Practice 1 The New York ehealth Collaborative (NYeC) Regional Extension Center (REC) The NYeC Regional Extension Center is the physician s trusted advisor in
NCQA Standards Workshop Patient-Centered Medical Home PCMH 2011. Part 2: Standards 4-6
 NCQA Standards Workshop PCMH 2011 Part 2: Standards 4-6 Agenda: Part 2 Content of PCMH 2011 Standards 4 6 Documentation examples* * Examples in the presentation only illustrate the element intent. They
NCQA Standards Workshop PCMH 2011 Part 2: Standards 4-6 Agenda: Part 2 Content of PCMH 2011 Standards 4 6 Documentation examples* * Examples in the presentation only illustrate the element intent. They
Quality Improvement Case Study: Improving Blood Pressure Control in a 3- Provider Primary Care Practice
 Quality Improvement Case Study: Improving Blood Pressure Control in a 3- Provider Primary Care Practice EXECUTIVE SUMMARY Organization Ellsworth Medical Clinic 1 is a family medicine practice in Wisconsin
Quality Improvement Case Study: Improving Blood Pressure Control in a 3- Provider Primary Care Practice EXECUTIVE SUMMARY Organization Ellsworth Medical Clinic 1 is a family medicine practice in Wisconsin
Andrew C. Bledsoe, MBA, CHPA, PCMH CCE Executive Director. Northeast KY Regional Health Information Organization. www.nekyrhio.org
 Andrew C. Bledsoe, MBA, CHPA, PCMH CCE Executive Director Northeast KY Regional Health Information Organization www.nekyrhio.org NCQA Program Setup Standards Six Standards Outline Program Elements Six
Andrew C. Bledsoe, MBA, CHPA, PCMH CCE Executive Director Northeast KY Regional Health Information Organization www.nekyrhio.org NCQA Program Setup Standards Six Standards Outline Program Elements Six
Stuart Levine MD MHA Corporate Medical Director, HealthCare Partners Assistant Clinical Professor, Internal Medicine and Psychiatry, UCLA David
 Stuart Levine MD MHA Corporate Medical Director, HealthCare Partners Assistant Clinical Professor, Internal Medicine and Psychiatry, UCLA David Geffen School of Medicine 1 HealthCare Partners Delivery
Stuart Levine MD MHA Corporate Medical Director, HealthCare Partners Assistant Clinical Professor, Internal Medicine and Psychiatry, UCLA David Geffen School of Medicine 1 HealthCare Partners Delivery
Key Strategic and Tactical Steps to Excel as Community Hospital May 2011
 Key Strategic and Tactical Steps to Excel as Community Hospital May 2011 1 2 3 Pillars of Excellence 4 Transformation from Hospital-Centric to Community-Centric with Triple Aim as Framework 5 Objectives
Key Strategic and Tactical Steps to Excel as Community Hospital May 2011 1 2 3 Pillars of Excellence 4 Transformation from Hospital-Centric to Community-Centric with Triple Aim as Framework 5 Objectives
Patient-Centered Medical Home and Meaningful Use
 Health Home Series: Patient-Centered Medical Home and Meaningful Use Presenters: Christine Stroebel, MPH, PCIP/NYC REACH Natalie Fuentes, MPH, PCIP/NYC REACH Alan Silver, MD, MPH/IPRO March 27, 2012, 2:00
Health Home Series: Patient-Centered Medical Home and Meaningful Use Presenters: Christine Stroebel, MPH, PCIP/NYC REACH Natalie Fuentes, MPH, PCIP/NYC REACH Alan Silver, MD, MPH/IPRO March 27, 2012, 2:00
Why Electronic Health Records are Ill-Suited for Population Health Management An InfoMC White Paper January 2016
 Why Electronic Health Records are Ill-Suited for Population Health Management An InfoMC White Paper January 2016 Many studies have demonstrated that cost of care for patients with chronic illnesses is
Why Electronic Health Records are Ill-Suited for Population Health Management An InfoMC White Paper January 2016 Many studies have demonstrated that cost of care for patients with chronic illnesses is
Massachusetts Medicaid EHR Incentive Payment Program
 Massachusetts Medicaid EHR Incentive Payment Program Agenda Vision & Goals High-level overview where we are going Medicare vs. Medicaid EHR Incentive Programs Performance and Progress Eligibility Overview
Massachusetts Medicaid EHR Incentive Payment Program Agenda Vision & Goals High-level overview where we are going Medicare vs. Medicaid EHR Incentive Programs Performance and Progress Eligibility Overview
Oregon Standards for Certified Community Behavioral Health Clinics (CCBHCs)
") Oregon Standards for Certified Community Behavioral Health Clinics (CCBHCs) Senate Bill 832 directed the Oregon Health Authority (OHA) to develop standards for achieving integration of behavioral health
Oregon Standards for Certified Community Behavioral Health Clinics (CCBHCs) Senate Bill 832 directed the Oregon Health Authority (OHA) to develop standards for achieving integration of behavioral health
February 29, 2016. Andy Slavitt, Acting Administrator Centers for Medicare & Medicaid Services 200 Independence Ave., SW Washington, DC 20201
 Andy Slavitt, Acting Administrator Centers for Medicare & Medicaid Services 200 Independence Ave., SW Washington, DC 20201 Dear Acting Administrator Slavitt: On behalf of the American Academy of Family
Andy Slavitt, Acting Administrator Centers for Medicare & Medicaid Services 200 Independence Ave., SW Washington, DC 20201 Dear Acting Administrator Slavitt: On behalf of the American Academy of Family
Meaningful Use as the Foundation of the Medical Home
 Meaningful Use as the Foundation of the Medical Home Thomas Novak Director of Delivery System Reform Health IT Use computerized provider order entry (CPOE) for medication, laboratory and radiology orders
Meaningful Use as the Foundation of the Medical Home Thomas Novak Director of Delivery System Reform Health IT Use computerized provider order entry (CPOE) for medication, laboratory and radiology orders
Guidelines for Patient-Centered Medical Home (PCMH) Recognition and Accreditation Programs. February 2011
 Recognition and Accreditation Programs. February 2011") American Academy of Family Physicians (AAFP) American Academy of Pediatrics (AAP) American College of Physicians (ACP) American Osteopathic Association (AOA) Guidelines for Patient-Centered Medical Home
American Academy of Family Physicians (AAFP) American Academy of Pediatrics (AAP) American College of Physicians (ACP) American Osteopathic Association (AOA) Guidelines for Patient-Centered Medical Home
Overview. Consider the materials presented in this webinar during your initial PCMH planning sessions
 p. 1 Overview NCQA PCMH 2014 Standards Strategy to create a PCMH work plan Quality improvement planning A word about renewals Summary Consider the materials presented in this webinar during your initial
p. 1 Overview NCQA PCMH 2014 Standards Strategy to create a PCMH work plan Quality improvement planning A word about renewals Summary Consider the materials presented in this webinar during your initial
State Innovation Model
 State Innovation Model P a t i e n t C e n t e r e d M e d i c a l H o m e W e b i n a r M a y 1 1, 2 0 1 6 1 Agenda SIM Overview & Updates Patient Centered Medical Home Overview Questions 2 1 SIM Overview
State Innovation Model P a t i e n t C e n t e r e d M e d i c a l H o m e W e b i n a r M a y 1 1, 2 0 1 6 1 Agenda SIM Overview & Updates Patient Centered Medical Home Overview Questions 2 1 SIM Overview
Question & Answer Guide
 Joint Commission Primary Care Medical Home (PCMH) Certification for Accredited Ambulatory Health Care Organizations Question & Answer Guide A. SCORING/DECISION-RELATED Question: We are already Joint Commission
Joint Commission Primary Care Medical Home (PCMH) Certification for Accredited Ambulatory Health Care Organizations Question & Answer Guide A. SCORING/DECISION-RELATED Question: We are already Joint Commission
Who are Parent Navigators?
 Parent Navigators: A New Care Team Member in Your Medical Home or Specialty Practice Faculty Disclosure: We have no financial relationships to disclose relating to the subject matter of this presentation.
Parent Navigators: A New Care Team Member in Your Medical Home or Specialty Practice Faculty Disclosure: We have no financial relationships to disclose relating to the subject matter of this presentation.
THE ROLE OF HEALTH INFORMATION TECHNOLOGY IN PATIENT-CENTERED CARE COLLABORATION. 2012 Louisiana HIPAA & EHR Conference Presenter: Chris Williams
 THE ROLE OF HEALTH INFORMATION TECHNOLOGY IN PATIENT-CENTERED CARE COLLABORATION 2012 Louisiana HIPAA & EHR Conference Presenter: Chris Williams Agenda Overview Impact of HIT on Patient-Centered Care (PCC)
THE ROLE OF HEALTH INFORMATION TECHNOLOGY IN PATIENT-CENTERED CARE COLLABORATION 2012 Louisiana HIPAA & EHR Conference Presenter: Chris Williams Agenda Overview Impact of HIT on Patient-Centered Care (PCC)
Blueprint Integrated Pilot Programs Evaluation & Financial Impact
 Blueprint Integrated Pilot s Academy and CommonWealth Fund State Institute May 27 28, 2009 Craig Jones MD Director, Vermont Blueprint for craig.jones@vdh.state.vt.us 1 Coordinated System Hospitals Mental
Blueprint Integrated Pilot s Academy and CommonWealth Fund State Institute May 27 28, 2009 Craig Jones MD Director, Vermont Blueprint for craig.jones@vdh.state.vt.us 1 Coordinated System Hospitals Mental
Medical Management. G.2 At a Glance. G.3 Procedures Requiring Prior Authorization. G.5 How to Contact or Notify Medical Management
 G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.9 Case Management Services G.12 Special Needs Services
G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.9 Case Management Services G.12 Special Needs Services
Patient Centered Medical Home (PCMH): Communication and Care Coordination
: Communication and Care Coordination") Patient Centered Medical Home (PCMH): Communication and Care Coordination Phillip Roemer, MD Assistant Professor of Medicine General Internal Medicine Feinberg School of Medicine Northwestern University
Patient Centered Medical Home (PCMH): Communication and Care Coordination Phillip Roemer, MD Assistant Professor of Medicine General Internal Medicine Feinberg School of Medicine Northwestern University
Practice Readiness Assessment
 Practice Demographics Practice Name: Tax ID Number: Practice Address: REC Implementation Agent: Practice Telephone Number: Practice Fax Number: Lead Physician: Project Primary Contact: Lead Physician Email
Practice Demographics Practice Name: Tax ID Number: Practice Address: REC Implementation Agent: Practice Telephone Number: Practice Fax Number: Lead Physician: Project Primary Contact: Lead Physician Email
Idaho Health Home State Plan Amendment Matrix: Summary Overview. Overview of Approved Health Home SPAs
 Idaho Health Home State Plan Amendment Matrix: Summary Overview This matrix outlines key program design features from health home State Plan Amendments (SPAs) approved by the Centers for Medicare & Medicaid
Idaho Health Home State Plan Amendment Matrix: Summary Overview This matrix outlines key program design features from health home State Plan Amendments (SPAs) approved by the Centers for Medicare & Medicaid
Going beyond Meaningful Use with EMR solutions from the Centricity portfolio
 Going beyond Meaningful Use with EMR solutions from the Centricity portfolio The IT tools and services you need now. The support you need for the future. GE Healthcare is focused on providing customers
Going beyond Meaningful Use with EMR solutions from the Centricity portfolio The IT tools and services you need now. The support you need for the future. GE Healthcare is focused on providing customers
Terry McGeeney, MD MBA, President, CEO of TransforMED
 Terry McGeeney, MD MBA, President, CEO of TransforMED Terry McGeeney, MD MBA, President, CEO of TransforMED According to the Future of Family Medicine Report: unless there are changes in the broader healthcare
Terry McGeeney, MD MBA, President, CEO of TransforMED Terry McGeeney, MD MBA, President, CEO of TransforMED According to the Future of Family Medicine Report: unless there are changes in the broader healthcare
Question & Answer Guide. (Effective July 1, 2014)
") Joint Commission Primary Care Medical Home (PCMH) Certification for Accredited Ambulatory Health Care Organizations Question & Answer Guide (Effective July 1, 2014) A. ELIGIBILITY/DECISION-RELATED Question:
Joint Commission Primary Care Medical Home (PCMH) Certification for Accredited Ambulatory Health Care Organizations Question & Answer Guide (Effective July 1, 2014) A. ELIGIBILITY/DECISION-RELATED Question:
Pennsylvania s Chronic Care/ Medical Home Initiative: Transforming Primary Care
 Pennsylvania s Chronic Care/ Medical Home Initiative: Transforming Primary Care Ann S. Torregrossa, Esq. Director Governor s Office of Health Care Reform Commonwealth of Pennsylvania WORKING TO ACHIEVE
Pennsylvania s Chronic Care/ Medical Home Initiative: Transforming Primary Care Ann S. Torregrossa, Esq. Director Governor s Office of Health Care Reform Commonwealth of Pennsylvania WORKING TO ACHIEVE
Beyond Meaningful Use -- Multi- disciplinary Team Integration of Customized Smoking Cessation Patient Education Into EMR Clinical Decision Support
 Beyond Meaningful Use -- Multi- disciplinary Team Integration of Customized Smoking Cessation Patient Education Into EMR Clinical Decision Support Wendy Angelo, MD Capital Region Healthcare Learning Objectives
Beyond Meaningful Use -- Multi- disciplinary Team Integration of Customized Smoking Cessation Patient Education Into EMR Clinical Decision Support Wendy Angelo, MD Capital Region Healthcare Learning Objectives
The Patient-Centered Medical Home How Does Managed Care Pharmacy Add Value?
 The Patient-Centered Medical Home How Does Managed Care Pharmacy Add Value? With heath care reform now being implemented, it is important that managed care pharmacy understand how to provide value for
The Patient-Centered Medical Home How Does Managed Care Pharmacy Add Value? With heath care reform now being implemented, it is important that managed care pharmacy understand how to provide value for
Disease Management Identifications and Stratification Health Risk Assessment Level 1: Level 2: Level 3: Stratification
 Disease Management UnitedHealthcare Disease Management (DM) programs are part of our innovative Care Management Program. Our Disease Management (DM) program is guided by the principles of the UnitedHealthcare
Disease Management UnitedHealthcare Disease Management (DM) programs are part of our innovative Care Management Program. Our Disease Management (DM) program is guided by the principles of the UnitedHealthcare
What is an Accountable Care Organization & Why is it Important to Your Home Infusion Company?
 What is an Accountable Care Organization & Why is it Important to Your Home Infusion Company? Lisa Harvey McPherson RN, MBA, MPPM EMHS Vice President Continuum of Care & Chief Advocacy Officer Disclosures
What is an Accountable Care Organization & Why is it Important to Your Home Infusion Company? Lisa Harvey McPherson RN, MBA, MPPM EMHS Vice President Continuum of Care & Chief Advocacy Officer Disclosures
CentraCare Health System Creates New Tools to Treat Tobacco Dependence
 CentraCare Health System Creates New Tools to Treat Tobacco Dependence Between October 2010 and June 2012, ClearWay Minnesota SM provided the CentraCare Health Foundation with funding and technical assistance
CentraCare Health System Creates New Tools to Treat Tobacco Dependence Between October 2010 and June 2012, ClearWay Minnesota SM provided the CentraCare Health Foundation with funding and technical assistance
NCQA Patient-Centered Medical Home. Improving experiences for patients, providers and practice staff
 NCQA Patient-Centered Medical Home Improving experiences for patients, providers and practice staff PCMH Recognition The patient-centered medical home is a model of care that emphasizes care coordination
NCQA Patient-Centered Medical Home Improving experiences for patients, providers and practice staff PCMH Recognition The patient-centered medical home is a model of care that emphasizes care coordination
Quality and Performance Improvement Program Description 2016
 Quality and Performance Improvement Program Description 2016 Introduction and Purpose Contra Costa Health Plan (CCHP) is a federally qualified, state licensed, county sponsored Health Maintenance Organization
Quality and Performance Improvement Program Description 2016 Introduction and Purpose Contra Costa Health Plan (CCHP) is a federally qualified, state licensed, county sponsored Health Maintenance Organization
What is an Accountable Care Organization & Why is it Important to Your Home Infusion Company? Disclosures. Overview 3/10/2015
 What is an Accountable Care Organization & Why is it Important to Your Home Infusion Company? Lisa Harvey McPherson RN, MBA, MPPM EMHS Vice President Continuum of Care & Chief Advocacy Officer Disclosures
What is an Accountable Care Organization & Why is it Important to Your Home Infusion Company? Lisa Harvey McPherson RN, MBA, MPPM EMHS Vice President Continuum of Care & Chief Advocacy Officer Disclosures
Achieving Quality and Value in Chronic Care Management
 The Burden of Chronic Disease One of the greatest burdens on the US healthcare system is the rapidly growing rate of chronic disease. These statistics illustrate the scope of the problem: Nearly half of
The Burden of Chronic Disease One of the greatest burdens on the US healthcare system is the rapidly growing rate of chronic disease. These statistics illustrate the scope of the problem: Nearly half of
Incentives to Accelerate EHR Adoption
 Incentives to Accelerate EHR Adoption The passage of the American Recovery and Reinvestment Act (ARRA) of 2009 provides incentives for eligible professionals (EPs) to adopt and use electronic health records
Incentives to Accelerate EHR Adoption The passage of the American Recovery and Reinvestment Act (ARRA) of 2009 provides incentives for eligible professionals (EPs) to adopt and use electronic health records
MedStar Family Choice (MFC) Case Management Program. Cyd Campbell, MD, FAAP Medical Director, MFC MCAC June 24, 2015
 Case Management Program. Cyd Campbell, MD, FAAP Medical Director, MFC MCAC June 24, 2015") MedStar Family Choice (MFC) Case Management Program Cyd Campbell, MD, FAAP Medical Director, MFC MCAC June 24, 2015 Case Management Program Presentation Overview CM Programs Disease Management Complex
MedStar Family Choice (MFC) Case Management Program Cyd Campbell, MD, FAAP Medical Director, MFC MCAC June 24, 2015 Case Management Program Presentation Overview CM Programs Disease Management Complex
Presbyterian Health Plan State of NM Group Benefits Plan Plan Year January-December 2014
 Presbyterian Health Plan State of NM Group Benefits Plan Plan Year January-December 2014 Our Purpose Presbyterian serves to improve the health of the patients, members, and communities we serve. 2 Who
Presbyterian Health Plan State of NM Group Benefits Plan Plan Year January-December 2014 Our Purpose Presbyterian serves to improve the health of the patients, members, and communities we serve. 2 Who
CHRONIC CARE MANAGEMENT TOOL KIT What Practices Need to Do to Implement and Bill CCM Codes
 CHRONIC CARE MANAGEMENT TOOL KIT What Practices Need to Do to Implement and Bill CCM Codes Understanding CCM Chronic Care Management (CCM) is defined as the non-face-to-face services provided to Medicare
CHRONIC CARE MANAGEMENT TOOL KIT What Practices Need to Do to Implement and Bill CCM Codes Understanding CCM Chronic Care Management (CCM) is defined as the non-face-to-face services provided to Medicare
ESCO- Information Technology Requirements With An Example of Solutions
 ESCO- Information Technology Requirements With An Example of Solutions Pramen Applasamy DCI Application Manager Doug Johnson, MD DCI Vice Chairman of the Board July 15, 2014 15-WEEK WEBINAR SERIES EVERY
ESCO- Information Technology Requirements With An Example of Solutions Pramen Applasamy DCI Application Manager Doug Johnson, MD DCI Vice Chairman of the Board July 15, 2014 15-WEEK WEBINAR SERIES EVERY
Cornerstone Health Care s ACO Playbook. Grace E. Terrell, MD January 17, 2012
 Cornerstone Health Care s ACO Playbook Grace E. Terrell, MD January 17, 2012 Mission: To be your medical home Vision: To be the model for physician-led health care in America Values: As a physician owned
Cornerstone Health Care s ACO Playbook Grace E. Terrell, MD January 17, 2012 Mission: To be your medical home Vision: To be the model for physician-led health care in America Values: As a physician owned
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual
 Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2015 This document is a guide to the 2015 Arkansas Blue Cross and Blue Shield Patient- Centered Medical Home program (Arkansas
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2015 This document is a guide to the 2015 Arkansas Blue Cross and Blue Shield Patient- Centered Medical Home program (Arkansas
Pennsylvania s Efforts to Transform Primary Care
 Pennsylvania s Efforts to Transform Primary Care Ann S. Torregrossa, Esq. Director Governor s Office of Health Care Reform Commonwealth of Pennsylvania Prescription for Pennsylvania Prescription for Pennsylvania
Pennsylvania s Efforts to Transform Primary Care Ann S. Torregrossa, Esq. Director Governor s Office of Health Care Reform Commonwealth of Pennsylvania Prescription for Pennsylvania Prescription for Pennsylvania
Diabetes Care 2011-2012
 Clinical Innovations in the Patient Centered Medical Home to Improve Diabetes Care Robert A. Gabbay, MD, PhD, FACP Chief Medical Officer & Senior Vice President Joslin Diabetes Center Harvard Medical School
Clinical Innovations in the Patient Centered Medical Home to Improve Diabetes Care Robert A. Gabbay, MD, PhD, FACP Chief Medical Officer & Senior Vice President Joslin Diabetes Center Harvard Medical School
2015 HEDIS/CAHPS Effectiveness of Care Report for 2014 Service Measures Oregon, Idaho and Montana Commercial Business
 2015 HEDIS/CAHPS Effectiveness of Care Report for 2014 Service Measures Oregon, Idaho and Montana Commercial Business About HEDIS The Healthcare Effectiveness Data and Information Set (HEDIS 1 ) is a widely
2015 HEDIS/CAHPS Effectiveness of Care Report for 2014 Service Measures Oregon, Idaho and Montana Commercial Business About HEDIS The Healthcare Effectiveness Data and Information Set (HEDIS 1 ) is a widely
Health Care Homes Certification Assessment Tool- With Examples
 Guidelines: Health Care Homes Certification Assessment Form Structure: This is the self-assessment form that HCH applicants should use to determine if they meet the requirements for HCH certification.
Guidelines: Health Care Homes Certification Assessment Form Structure: This is the self-assessment form that HCH applicants should use to determine if they meet the requirements for HCH certification.
3/9/2011 ELECTRONIC HEALTH RECORDS: A NATIONAL PRIORITY. Mandate for electronic health records is tied to:
 To lower health care cost, cut medical errors, And improve care, we ll computerize the nation s health records in five years, saving billions of dollars in health care costs and countless lives. ELECTRONIC
To lower health care cost, cut medical errors, And improve care, we ll computerize the nation s health records in five years, saving billions of dollars in health care costs and countless lives. ELECTRONIC
NCQA Standards Workshop Physician Practice Connections - Patient-Centered Medical Home (PPC -PCMH )
") NCQA Physician Practice Connections - Patient-Centered Medical Home (PPC -PCMH ) Agenda Patient-Centered Medical Home Overview Content of PPC-PCMH Standards Documentation examples* Recognition Process
NCQA Physician Practice Connections - Patient-Centered Medical Home (PPC -PCMH ) Agenda Patient-Centered Medical Home Overview Content of PPC-PCMH Standards Documentation examples* Recognition Process
Texas Medicaid EHR Incentive Program
 Texas Medicaid EHR Incentive Program Medicaid HIT Team July 23, 2012 Why Health IT? Benefits of Health IT A 2011 study* found that 92% of articles published from July 2007 to February 2010 reached conclusions
Texas Medicaid EHR Incentive Program Medicaid HIT Team July 23, 2012 Why Health IT? Benefits of Health IT A 2011 study* found that 92% of articles published from July 2007 to February 2010 reached conclusions
The Power of PopIQ and Big Data. i2i Systems West Coast Regional User Conference September 5, 2014
 The Power of PopIQ and Big Data i2i Systems West Coast Regional User Conference September 5, 2014 Statewide Collaboration & Data Analytics Community Clinics Health Network Founded in 1993 Current Initiatives/Areas
The Power of PopIQ and Big Data i2i Systems West Coast Regional User Conference September 5, 2014 Statewide Collaboration & Data Analytics Community Clinics Health Network Founded in 1993 Current Initiatives/Areas
Department of Human Services Health Care Reform Review Committee Representative George Keiser, Chairman March 19, 2014
 Department of Human Services Health Care Reform Review Committee Representative George Keiser, Chairman March 19, 2014 Chairman Keiser, members of the Health Care Reform Review Committee, I am Julie Schwab,
Department of Human Services Health Care Reform Review Committee Representative George Keiser, Chairman March 19, 2014 Chairman Keiser, members of the Health Care Reform Review Committee, I am Julie Schwab,
Beacon User Stories Version 1.0
 Table of Contents 1. Introduction... 2 2. User Stories... 2 2.1 Update Clinical Data Repository and Disease Registry... 2 2.1.1 Beacon Context... 2 2.1.2 Actors... 2 2.1.3 Preconditions... 3 2.1.4 Story
Table of Contents 1. Introduction... 2 2. User Stories... 2 2.1 Update Clinical Data Repository and Disease Registry... 2 2.1.1 Beacon Context... 2 2.1.2 Actors... 2 2.1.3 Preconditions... 3 2.1.4 Story
AHA/ASA Support Network. Anne Vigil, MSN, RN SLUCare Cardiac Rehabilitation American Heart Association Volunteer
 AHA/ASA Support Network Anne Vigil, MSN, RN SLUCare Cardiac Rehabilitation American Heart Association Volunteer Overview The Support Network establishes AHA/ASA as a trusted source for patients, families
AHA/ASA Support Network Anne Vigil, MSN, RN SLUCare Cardiac Rehabilitation American Heart Association Volunteer Overview The Support Network establishes AHA/ASA as a trusted source for patients, families
Physicians, EHR Stimulus and Healthcare Reform
 Physicians, EHR Stimulus and Healthcare Reform The Physicians Foundation is proud to present this webinar on the evolving world of EHRs and office practice as part of its mission to improve the care, quality
Physicians, EHR Stimulus and Healthcare Reform The Physicians Foundation is proud to present this webinar on the evolving world of EHRs and office practice as part of its mission to improve the care, quality
Patient Centered Health Home and Data Analytics. Amanda Stangis, Director of Programs, CPCA Andrew Principe, VP Strategy, Arcadia Solutions
 Patient Centered Health Home and Data Analytics Amanda Stangis, Director of Programs, CPCA Andrew Principe, VP Strategy, Arcadia Solutions Agenda What is a Health Home? What is the connection between Health
Patient Centered Health Home and Data Analytics Amanda Stangis, Director of Programs, CPCA Andrew Principe, VP Strategy, Arcadia Solutions Agenda What is a Health Home? What is the connection between Health
How To Get A Pcmh
 A Comparison of the National Patient-Centered Medical Home Accreditation and Recognition Programs David N. Gans, MSHA, FACMPE, Senior Fellow Industry Affairs, Medical Group Management Association Englewood,
A Comparison of the National Patient-Centered Medical Home Accreditation and Recognition Programs David N. Gans, MSHA, FACMPE, Senior Fellow Industry Affairs, Medical Group Management Association Englewood,
Meaningful Use - The Basics
 Meaningful Use - The Basics Presented by PaperFree Florida 1 Topics Meaningful Use Stage 1 Meaningful Use Barriers: Observations from the field Help and Questions 2 What is Meaningful Use Meaningful Use
Meaningful Use - The Basics Presented by PaperFree Florida 1 Topics Meaningful Use Stage 1 Meaningful Use Barriers: Observations from the field Help and Questions 2 What is Meaningful Use Meaningful Use
Connec&ng(the(Dots(in(Pediatric(Care(Across(Ohio:( (((((((((The(CliniSync(Health(Informa&on(Exchange(((((((((((((((
 Connec&ng(the(Dots(in(Pediatric(Care(Across(Ohio:( (((((((((The(CliniSync(Health(Informa&on(Exchange((((((((((((((( Ohio(Chapter,(American(Academy(of(Pediatrics( Fred(Richards,(CIO,(COO( Ohio(Health(Informa&on(Partnership/CliniSync(
Connec&ng(the(Dots(in(Pediatric(Care(Across(Ohio:( (((((((((The(CliniSync(Health(Informa&on(Exchange((((((((((((((( Ohio(Chapter,(American(Academy(of(Pediatrics( Fred(Richards,(CIO,(COO( Ohio(Health(Informa&on(Partnership/CliniSync(
THE MYERS GROUP MEDICARE CAHPS RESEARCH SERIES
 THE MYERS GROUP MEDICARE CAHPS RESEARCH SERIES Background Each year, CMS rates each Medicare Advantage plan using a five star rating system. While originally developed to provide members with the ability
THE MYERS GROUP MEDICARE CAHPS RESEARCH SERIES Background Each year, CMS rates each Medicare Advantage plan using a five star rating system. While originally developed to provide members with the ability
Vendor Evaluation Matrix Tool Presented By: Developed By: Version: Date: Description: Table of Contents:
 Vendor Evaluation Matrix Tool Presented By: The National Learning Consortium (NLC) Developed By: Health Information Technology Research Center (HITRC) Vendor Selection and Management Community of Practice
Vendor Evaluation Matrix Tool Presented By: The National Learning Consortium (NLC) Developed By: Health Information Technology Research Center (HITRC) Vendor Selection and Management Community of Practice
UPDATED NOVEMBER 2015. Providing and Billing Medicare for Chronic Care Management
 UPDATED NOVEMBER 2015 Providing and Billing Medicare for Chronic Care Management Research studies have demonstrated time and again that care management reduces total costs of care for chronic disease patients
UPDATED NOVEMBER 2015 Providing and Billing Medicare for Chronic Care Management Research studies have demonstrated time and again that care management reduces total costs of care for chronic disease patients
POPULATION HEALTH. Annual Wellness Visit (AWV) Matthew Brown, MD Chief Medical Officer Presence Health Partners
 Matthew Brown, MD Chief Medical Officer Presence Health Partners") POPULATION HEALTH Annual Wellness Visit (AWV) Chief Medical Officer Presence Health Partners November 10, 2015 Purpose Presence Health partnered with physicians to form as a means of helping providers
POPULATION HEALTH Annual Wellness Visit (AWV) Chief Medical Officer Presence Health Partners November 10, 2015 Purpose Presence Health partnered with physicians to form as a means of helping providers
COMPARISON: PPC-PCMH 2008 With PCMH 2011
 COMPARISON: PPC-PCMH 008 With PCMH 011 About This Crosswalk The following crosswalk compares Physician Practice Connections Patient-Centered Medical Home (PPC -PCMH ) 008 with NCQA s Patient-Centered Medical
COMPARISON: PPC-PCMH 008 With PCMH 011 About This Crosswalk The following crosswalk compares Physician Practice Connections Patient-Centered Medical Home (PPC -PCMH ) 008 with NCQA s Patient-Centered Medical
PCMH 2011 FAQs. PCMH Element/Factors Question Answer
 IMPORTANT GENERAL RECOMMENDATIONS: Refer to the following documents in addition to reviewing the questions and answers below related to specific standards, elements and factors: 1. PCMH 2011 Standards
IMPORTANT GENERAL RECOMMENDATIONS: Refer to the following documents in addition to reviewing the questions and answers below related to specific standards, elements and factors: 1. PCMH 2011 Standards
How To Integrate Diabetes Manager With Allscripts Ehr
 Intégration de la Télémédecine dans le Dossier Médical Hospitalier Joshua L. Cohen, M.D. Professor of Medicine Division of Endocrinology & Metabolism Director, Medical Faculty Associates Diabetes Center
Intégration de la Télémédecine dans le Dossier Médical Hospitalier Joshua L. Cohen, M.D. Professor of Medicine Division of Endocrinology & Metabolism Director, Medical Faculty Associates Diabetes Center
Patient-Centered Medical Home (PCMH) 2014
 2014") Patient-Centered Medical Home (PCMH) 2014 Part 1: Standards 1-3 All materials 2015, National Committee for Quality Assurance Agenda Part 1 Content of PCMH 2014 Standards and Guidelines Standards 1 3 Documentation
Patient-Centered Medical Home (PCMH) 2014 Part 1: Standards 1-3 All materials 2015, National Committee for Quality Assurance Agenda Part 1 Content of PCMH 2014 Standards and Guidelines Standards 1 3 Documentation
Profile: Incorporating Routine Behavioral Health Screenings Into the Patient-Centered Medical Home
 104 A LOOK TO THE FUTURE Profile: Incorporating Routine Behavioral Health Screenings Into the Patient-Centered Medical Home Background Management of chronic diseases can be challenging in primary care,
104 A LOOK TO THE FUTURE Profile: Incorporating Routine Behavioral Health Screenings Into the Patient-Centered Medical Home Background Management of chronic diseases can be challenging in primary care,
Oregon Health Authority Patient-Centered Primary Care Home Program 2014 Recognition Criteria
 Oregon Health Authority Patient-Centered Primary Care Home Program 2014 Recognition Criteria www.primarycarehome.oregon.gov Email: PCPCH@state.or.us Technical Specifications and Reporting Guide (TA Guide)
Oregon Health Authority Patient-Centered Primary Care Home Program 2014 Recognition Criteria www.primarycarehome.oregon.gov Email: PCPCH@state.or.us Technical Specifications and Reporting Guide (TA Guide)
Statement for the Record. Bernadette Loftus, MD. Executive-in-Charge, Mid-Atlantic Permanente Medical Group. Kaiser Permanente
 Statement for the Record Bernadette Loftus, MD Executive-in-Charge, Mid-Atlantic Permanente Medical Group Kaiser Permanente Defense Health Care Reform Subcommittee on Personnel of the Committee on Armed
Statement for the Record Bernadette Loftus, MD Executive-in-Charge, Mid-Atlantic Permanente Medical Group Kaiser Permanente Defense Health Care Reform Subcommittee on Personnel of the Committee on Armed
Johns Hopkins HealthCare LLC: Care Management and Care Coordination for Chronic Diseases
 Johns Hopkins HealthCare LLC: Care Management and Care Coordination for Chronic Diseases Epidemiology Over 145 million people ( nearly half the population) - suffer from asthma, depression and other chronic
Johns Hopkins HealthCare LLC: Care Management and Care Coordination for Chronic Diseases Epidemiology Over 145 million people ( nearly half the population) - suffer from asthma, depression and other chronic
Provider Delivered Care Management Payment Policy and Billing Guidelines for Medicare Advantage
 Provider Delivered Care Management Payment Policy and Billing Guidelines for Medicare Advantage Purpose Beginning April 1, 2012, BCBSM began accepting and paying claims for Provider Delivered Care Management
Provider Delivered Care Management Payment Policy and Billing Guidelines for Medicare Advantage Purpose Beginning April 1, 2012, BCBSM began accepting and paying claims for Provider Delivered Care Management
2015 Year Over Year HEALTHCARE JOBS SNAPSHOT. A quarterly report produced by Health ecareers
 2015 Year Over Year HEALTHCARE JOBS SNAPSHOT A quarterly report produced by Health ecareers TABLE of CONTENTS Executive Summary 3 Key Findings General Findings 4 Physicians/Surgeons 5 Nurses, Nurse Practitioners
2015 Year Over Year HEALTHCARE JOBS SNAPSHOT A quarterly report produced by Health ecareers TABLE of CONTENTS Executive Summary 3 Key Findings General Findings 4 Physicians/Surgeons 5 Nurses, Nurse Practitioners