Suffolk County Community College School of Nursing NUR 133 ADULT NURSING I
|
|
|
- Randall Franklin
- 8 years ago
- Views:
Transcription
1 Suffolk County Community College School of Nursing NUR 133 ADULT NURSING I Page # 1 Instructions for students: Case study # 1 For this lab, you are planning to provide care to the following client: CB is a 75 year old married female experiencing pneumonia is suspected of developing sepsis and has inadequate renal perfusion and is prescribed Dopamine (Intropin). 1. Refer to your Iggy text page 664. What indicators support the likelihood that your client may be experiencing sepsis? 2. Refer to Iggy page 839. The complication of sepsis can lead systemic inflammation response syndrome (SIRS) resulting in decreased tissue perfusion. What assessment data would the nurse collect that indicates that a client has inadequate renal tissue perfusion as a result of SIRS? 3. Early detection of sepsis is an important nursing responsibility. Page 842. What might you notice if sepsis is impending? Iggy page What assessments should you be prepared to perform? Iggy page What lab/diagnostics would you evaluate? 1
 resulting in decreased tissue perfusion.")
2 Review the lab reports: Name Gender Barker, Cathy F DOB 1/1/1935 MR # Physician Dr Thomas Admitting date 1/9/2010 DATE: 1/9/2010 1/10/2010 1/11/2010 LABORATORY REPORT TIME: Lab Test Reference Range Complete Blood Count HCT MALE 40-52% HCT FEM 37-46% HGB MALE gm/dl HGB FEM gm/dl RBC MALE x10 6 /µl RBC FEMALE x10 6 /µl WBC x10 3 /µl WBC Differential PMN 35-80% BANDS 0-10% LYMPH 20-50% MONO 2-12% EOS 0-7% BAS 0-2% PLT x10 3 /µl BLEEDING TIMES PT seconds PTT seconds METABOLIC PANEL Sodium meq/l Potassium meq/l Chloride mmol/l Glucose mg/dl CO mmol/l BUN 7-21 mg/dl Creatinine mg/dl Interpretation CBC and bleeding times BMP Page # 2 ARTERIAL BLOOD GAS RA 2lpm 35% VM ph pco mmhg po mmhg HCO meq/l O2 SAT % ABG How do you interpret these labs? 2

3 Page # 3 6. What should you be prepared to do? Page How do you expect the client to respond to your interventions? The client has not had any urine output for 2 hours. The systolic blood pressure is 100 mm Hg and the heart rate is 126. The hospitalist prescribes an IV normal saline bolus, but the client remain anuric and hypotensive. The hospitalist suggests a Dopamine infusion. 8. Review the policy on Dopamine administration in your lab reading list. What is Dopamine (Intropin) and what dose is used for renal perfusion? 9. What assessment data is necessary before initiating Dopamine infusions? 10.What continued monitoring is required? 11.For which complications should the nurse plan care? 12.Why is an electronic pump necessary when administering this medication? 13.What is the policy for local infiltration of Dopamine? 3

4 Page # 4 14.Review the advanced IV calculation tips in your lab reading. You are instructed to start a second IV for a dopamine infusion. If you are ordered to administer Dopamine 1 mcg/kg/minute, your client weighs 70 kgs and you have a dopamine infusion of 400 mgs in 500 ml of D5W, at what rate would you program the infusion pump? Enter the value on the flowsheet below: NS bolus Dopamine 400 mg/500 ml 0.9 % NaCl 125 ml/hr BP HR RR Pulse ox T Urine output ml / / The client s urine output has not increased. What is the maximum infusion rate for renal dose dopamine? The rapid response team continues to work on the client and stabilizes her. She is then prepared for transfer to the ICU. A transfer summary is completed and handoff communication is performed with the ICU receiving nurse. What should be included in the handoff communication? 4

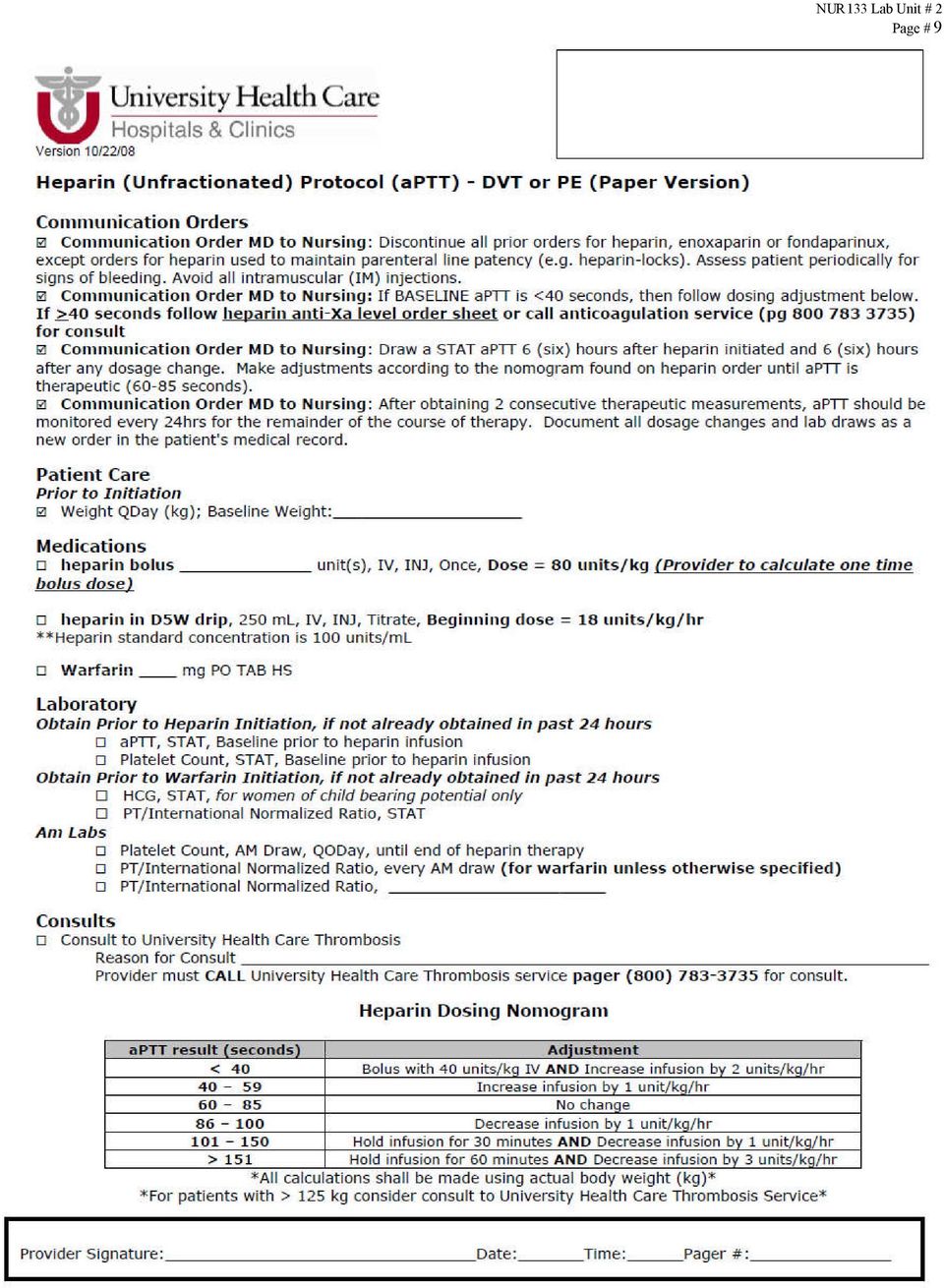
5 Case study # 2 See Iggy page 818 Page # 5 PB is a 71 year old male s/p right total hip arthroplasty who has developed unilateral edema of his left extremity associated with pain down the length of his leg. He had sequential teds in use and was started on Lovenox injections for which he is due to receive at 10 am. His health history is complicated by 100 pack years of cigarette smoking. Daily Peripheral Neurovascular Check Flowsheet Date: 1/10/ L R L R L R L R L R L R Color: normal X X X X pale X X mottled cyanotic Temp: warm X X X X X cool X Pulses 0/4 1/4 2/4 X 3/4 X X X X X 4/4 Edema 0 1+ X X X X 2+ X X Mobility intact X X X X X decreased X absent 16.How would you interpret the data from the peripheral NV flowsheet above? The client is evaluated by the surgeon and the heparin protocol is ordered. 17.Review the Heparin protocol. Your client is prescribed the heparin protocol for suspected DVT. What is heparin and its therapeutic action? 5

6 Page # 6 18.Your client is on Lovenox (Enoxaparin). What concerns arise when considering Heparin therapy initiation? 19.What lab/diagnostics should be performed? 20.For what potential complications should the nurse plan care? 21.What lab/diagnostics should be performed prior to initiation of heparin? 22.What equipment would the nurse gather prior to initiating a heparin infusion? 23.Prior to initiation of a heparin infusion, an IV loading bolus dose is administered at What are the procedural steps in performing an IV bolus? 24.If your client weighs 90 kgs and you are ordered to administer Heparin 80 units/kg IV, how much heparin would you administer? 25.If you have Heparin unit/1 ml, how many ml would you draw up in your syringe? 26.Review the advanced IV calculation tips in your lab reading. If you are ordered to administer Heparin 18 units/kg/hour, your client weighs 90 kgs and you have a Heparin infusion of units in 250 ml D5W. At what rate would you program the infusion pump? 27.When should you redraw your PTT? 6

7 Page # 7 28.What assessment data indicating a potential complication would the nurse remain alert for during this therapy? Name Gender Bulmer, Peter M DOB 12/17/1938 MR # Physician Dr June Admitting date 1/9/2010 DATE: 1/6/2010 1/9/2010 1/10/2010 1/10/2010 LABORATORY REPORT TIME: Lab Test Reference Range Complete Blood Count HCT MALE 40-52% HCT FEM 37-46% HGB MALE gm/dl HGB FEM gm/dl RBC MALE x10 6 /µl RBC FEMALE x10 6 /µl WBC x10 3 /µl WBC Differential PMN 35-80% BANDS 0-10% LYMPH 20-50% MONO 2-12% EOS 0-7% BAS 0-2% PLT x10 3 /µl BLEEDING TIMES PT seconds PTT seconds METABOLIC PANEL Sodium meq/l Potassium meq/l Chloride mmol/l Glucose mg/dl CO mmol/l BUN 7-21 mg/dl Creatinine mg/dl

8 Based on the nomogram below, how do you interpret these labs? Heparin Dosing Nomogram aptt Adjustment < 40 seconds Bolus 40 units/kg IV and increase infusion by 2 units/kg/hr seconds Increase infusion by 1 unit/kg/hr seconds No change seconds Decrease infusion by 1 unit/kg/hr seconds Hold infusion for 30 minutes and Decrease infusion by 1 unit/kg/hr > 150 seconds Hold infusion for 60 minutes and Decrease infusion by 3 unit/kg/hr Page # 8 29.What action would you take? 30.How would you calculate the change in rate? 31.How would you adjust the infusion pump? 32.According to the orders, when can you stop checking PTT levels every 6 hours? 33.What action should you take if excessive bruising or bleeding is noted? 34.What bleeding precautions should you employ? Iggy Chart 38-6 page See Warfarin (Coumadin) therapy page 819. What levels are monitored if Warfarin is added to the regimen? 36.What is the antidote for Warfarin? 37.What is the antidote for Heparin? 8

9 9 Page # 9
Georgia Northwestern Technical College Practical Nursing Program CLINICAL DAILY ASSESSMENT WORKSHEET FOR MODULES I-IV STUDENT: CLINICAL INSTRUCTOR:
 Georgia Northwestern Technical College Practical Nursing Program CLINICAL DAILY ASSESSMENT WORKSHEET FOR MODULES I-IV STUDENT: CLINICAL INSTRUCTOR: CLINICAL UNIT: ASSIGNMENT DATES: PATIENT (last initial):
Georgia Northwestern Technical College Practical Nursing Program CLINICAL DAILY ASSESSMENT WORKSHEET FOR MODULES I-IV STUDENT: CLINICAL INSTRUCTOR: CLINICAL UNIT: ASSIGNMENT DATES: PATIENT (last initial):
Inpatient Anticoagulation Safety. To provide safe and effective anticoagulation therapy through a collaborative approach.
 Inpatient Anticoagulation Safety Purpose: Policy: To provide safe and effective anticoagulation therapy through a collaborative approach. Upon the written order of a physician, Heparin, Low Molecular Weight
Inpatient Anticoagulation Safety Purpose: Policy: To provide safe and effective anticoagulation therapy through a collaborative approach. Upon the written order of a physician, Heparin, Low Molecular Weight
SUFFOLK COUNTY COMMUNITY COLLEGE NURSING DEPARTMENT MEDICATION ADMINISTRATION TEST NR 40 Practice test questions READ INSTRUCTIONS CAREFULLY
 NR40 MEDICATION MATH TEST Practice questions page 1 SUFFOLK COUNTY COMMUNITY COLLEGE NURSING DEPARTMENT MEDICATION ADMINISTRATION TEST NR 40 Practice test questions READ INSTRUCTIONS CAREFULLY Students
NR40 MEDICATION MATH TEST Practice questions page 1 SUFFOLK COUNTY COMMUNITY COLLEGE NURSING DEPARTMENT MEDICATION ADMINISTRATION TEST NR 40 Practice test questions READ INSTRUCTIONS CAREFULLY Students
Clinical Reasoning Case Study: I. Data Collection Chief complaint/history of Present Illness:
 Clinical Reasoning Case Study: I. Data Collection Chief complaint/history of Present Illness: What data is relevant that must be recognized as clinically significant to the nurse? Rationale: Personal/Social
Clinical Reasoning Case Study: I. Data Collection Chief complaint/history of Present Illness: What data is relevant that must be recognized as clinically significant to the nurse? Rationale: Personal/Social
Planning: Patient Goals and Expected Outcomes The patient will: Remain free of unusual bleeding Maintain effective tissue perfusion Implementation
 Obtain complete heath history including allergies, drug history and possible drug Assess baseline coagulation studies and CBC Assess for history of bleeding disorders, GI bleeding, cerebral bleed, recent
Obtain complete heath history including allergies, drug history and possible drug Assess baseline coagulation studies and CBC Assess for history of bleeding disorders, GI bleeding, cerebral bleed, recent
Core Measures SEPSIS UPDATES
 Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Sepsis Core Measures Bundle Requirements
Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Sepsis Core Measures Bundle Requirements
Jeopardy Topics: THE CLOT STOPS HERE (anticoagulants) SUGAR, SUGAR, HOW D YOU GET SO HIGH (insulins)
 SUGAR, SUGAR, HOW D YOU GET SO HIGH (insulins)") Jeopardy Topics: THE CLOT STOPS HERE (anticoagulants) SUGAR, SUGAR, HOW D YOU GET SO HIGH (insulins) I HEAR YA KNOCKING BUT YOU CAN T COME IN (electrolytes) TAKE MY BREATH AWAY (Opiates-morphine) OUT WITH
Jeopardy Topics: THE CLOT STOPS HERE (anticoagulants) SUGAR, SUGAR, HOW D YOU GET SO HIGH (insulins) I HEAR YA KNOCKING BUT YOU CAN T COME IN (electrolytes) TAKE MY BREATH AWAY (Opiates-morphine) OUT WITH
Procedure for Inotrope Administration in the home
 Procedure for Inotrope Administration in the home Purpose This purpose of this procedure is to define the care used when administering inotropic agents intravenously in the home This includes: A. Practice
Procedure for Inotrope Administration in the home Purpose This purpose of this procedure is to define the care used when administering inotropic agents intravenously in the home This includes: A. Practice
Mind the Gap: Navigating the Underground World of DKA. Objectives. Back That Train Up! 9/26/2014
 Mind the Gap: Navigating the Underground World of DKA Christina Canfield, MSN, RN, ACNS-BC, CCRN Clinical Nurse Specialist Cleveland Clinic Respiratory Institute Objectives Upon completion of this activity
Mind the Gap: Navigating the Underground World of DKA Christina Canfield, MSN, RN, ACNS-BC, CCRN Clinical Nurse Specialist Cleveland Clinic Respiratory Institute Objectives Upon completion of this activity
Quiz 5 Heart Failure scores (n=163)
") Quiz 5 Heart Failure summary statistics The correct answers to questions are indicated by *. Students were awarded 2 points for question #3 for either selecting spironolactone or eplerenone. However, the
Quiz 5 Heart Failure summary statistics The correct answers to questions are indicated by *. Students were awarded 2 points for question #3 for either selecting spironolactone or eplerenone. However, the
Sepsis Reassess patient Monitor and maintain respiratory/ hemodynamic status
 Patient exhibits two or more of the following SIRS criteria: Temperature greater than 38 o C (100.4 o F) or less SIRS than criteria 36 o C (96.8 o F) Heart Rate greater than 90 beats/minute Respiratory
Patient exhibits two or more of the following SIRS criteria: Temperature greater than 38 o C (100.4 o F) or less SIRS than criteria 36 o C (96.8 o F) Heart Rate greater than 90 beats/minute Respiratory
Interpretation of Laboratory Values
 Interpretation of Laboratory Values Konrad J. Dias PT, DPT, CCS Overview Electrolyte imbalances Renal Function Tests Complete Blood Count Coagulation Profile Fluid imbalance Sodium Electrolyte Imbalances
Interpretation of Laboratory Values Konrad J. Dias PT, DPT, CCS Overview Electrolyte imbalances Renal Function Tests Complete Blood Count Coagulation Profile Fluid imbalance Sodium Electrolyte Imbalances
SE5h, Sepsis Education.pdf. Surviving Sepsis
 Surviving Sepsis 1 Scope and Impact of the Problem: Severe sepsis is a major healthcare problem that affects millions of people around the world each year with an extremely high mortality rate of 30 to
Surviving Sepsis 1 Scope and Impact of the Problem: Severe sepsis is a major healthcare problem that affects millions of people around the world each year with an extremely high mortality rate of 30 to
Lynda Richardson, RN, BSN Sepsis/Septic Shock Abstractor. No disclosures
 Lynda Richardson, RN, BSN Sepsis/Septic Shock Abstractor No disclosures 1 2 3 Discuss data requirements -3 hour bundle -6 hour bundle Challenges and compliance issues Success 4 Based on the Surviving Sepsis
Lynda Richardson, RN, BSN Sepsis/Septic Shock Abstractor No disclosures 1 2 3 Discuss data requirements -3 hour bundle -6 hour bundle Challenges and compliance issues Success 4 Based on the Surviving Sepsis
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 One Children s Plaza Dayton, OH 45404-1815 www.childrensdayton.org DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended
One Children s Plaza Dayton, OH 45404-1815 www.childrensdayton.org DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended
Subject: Severe Sepsis/Septic Shock Published Date: August 9, 2013 Scope: Hospital Wide Original Creation Date: August 9, 2013
 Stony Brook Medicine Severe Sepsis/Septic Shock Recognition and Treatment Protocols Subject: Severe Sepsis/Septic Shock Published Date: August 9, 2013 Scope: Hospital Wide Original Creation Date: August
Stony Brook Medicine Severe Sepsis/Septic Shock Recognition and Treatment Protocols Subject: Severe Sepsis/Septic Shock Published Date: August 9, 2013 Scope: Hospital Wide Original Creation Date: August
Medications or therapeutic solutions may be injected directly into the bloodstream
 Intravenous Therapy Medications or therapeutic solutions may be injected directly into the bloodstream for immediate circulation and use by the body. State practice acts designate which health care professionals
Intravenous Therapy Medications or therapeutic solutions may be injected directly into the bloodstream for immediate circulation and use by the body. State practice acts designate which health care professionals
Medical Direction and Practices Board WHITE PAPER
 Medical Direction and Practices Board WHITE PAPER Use of Pressors in Pre-Hospital Medicine: Proper Indication and State of the Science Regarding Proper Choice of Pressor BACKGROUND Shock is caused by a
Medical Direction and Practices Board WHITE PAPER Use of Pressors in Pre-Hospital Medicine: Proper Indication and State of the Science Regarding Proper Choice of Pressor BACKGROUND Shock is caused by a
Acute Myocardial Infarction (the formulary thrombolytic for AMI at AAMC is TNK, please see the TNK monograph in this manual for information)
") ANNE ARUNDEL MEDICAL CENTER CRITICAL CARE MEDICATION MANUAL DEPARTMENT OF NURSING AND PHARMACY Guidelines for Use of Intravenous Alteplase (Tissue Plasminogen Activator (t-pa)), Activase in the Treatment
ANNE ARUNDEL MEDICAL CENTER CRITICAL CARE MEDICATION MANUAL DEPARTMENT OF NURSING AND PHARMACY Guidelines for Use of Intravenous Alteplase (Tissue Plasminogen Activator (t-pa)), Activase in the Treatment
[ ] POCT glucose Routine, As needed, If long acting insulin is given and patient NPO, do POCT glucose every 2 hours until patient eats.
![[ ] POCT glucose Routine, As needed, If long acting insulin is given and patient NPO, do POCT glucose every 2 hours until patient eats.](/thumbs/35/17205932.jpg "[ ] POCT glucose Routine, As needed, If long acting insulin is given and patient NPO, do POCT glucose every 2 hours until patient eats.") Glycemic Control - Insulin Infusion NOTE: For treatment of Diabetic Ketoacidosis or Hyperglycemic Hyperosmolar Syndrome please go to order set named Diabetic Ketoacidosis (DKA) and Hyperglycemic Hyperosmolar
Glycemic Control - Insulin Infusion NOTE: For treatment of Diabetic Ketoacidosis or Hyperglycemic Hyperosmolar Syndrome please go to order set named Diabetic Ketoacidosis (DKA) and Hyperglycemic Hyperosmolar
PHYSICIAN ORDERS TRANSIENT ISCHEMIC ATTACK (TIA) OBSERVATION
 OBSERVATION") SCREENING- ABCD-2 Score The ABCD2 score is a risk assessment tool designed to improve the prediction of short-term stroke risk after a transient ischemic attack (TIA). Higher ABCD2 scores are associated
SCREENING- ABCD-2 Score The ABCD2 score is a risk assessment tool designed to improve the prediction of short-term stroke risk after a transient ischemic attack (TIA). Higher ABCD2 scores are associated
Inotropes/Vasoactive Agents Hina N. Patel, Pharm.D., BCPS Cathy Lawson, Pharm.D., BCPS
 Inotropes/Vasoactive Agents Hina N. Patel, Pharm.D., BCPS Cathy Lawson, Pharm.D., BCPS 1. Definition -an agent that affects the contractility of the heart -may be positive (increases contractility) or
Inotropes/Vasoactive Agents Hina N. Patel, Pharm.D., BCPS Cathy Lawson, Pharm.D., BCPS 1. Definition -an agent that affects the contractility of the heart -may be positive (increases contractility) or
Acid-Base Disorders. Jai Radhakrishnan, MD, MS. Objectives. Diagnostic Considerations. Step 1: Primary Disorder. Formulae. Step 2: Compensation
 Objectives Diagnostic approach to acid base disorders Common clinical examples of acidoses and alkaloses Acid-Base Disorders Jai Radhakrishnan 1 2 Diagnostic Considerations Data points required: ABG: ph,
Objectives Diagnostic approach to acid base disorders Common clinical examples of acidoses and alkaloses Acid-Base Disorders Jai Radhakrishnan 1 2 Diagnostic Considerations Data points required: ABG: ph,
The Sepsis Puzzle: Identification, Monitoring and Early Goal Directed Therapy
 The Sepsis Puzzle: Identification, Monitoring and Early Goal Directed Therapy Cindy Goodrich RN, MS, CCRN Content Description Sepsis is caused by widespread tissue injury and systemic inflammation resulting
The Sepsis Puzzle: Identification, Monitoring and Early Goal Directed Therapy Cindy Goodrich RN, MS, CCRN Content Description Sepsis is caused by widespread tissue injury and systemic inflammation resulting
Nursing Care and Considerations for Patients with Atrial Fibrillation. Kris Kinghorn RN, MSN, ANP-BC
 Nursing Care and Considerations for Patients with Atrial Fibrillation Kris Kinghorn RN, MSN, ANP-BC Case Study 66 y/o female (Mrs. Olus A. Blader) Admitted with c/o palpitations and lightheadedness PMH:
Nursing Care and Considerations for Patients with Atrial Fibrillation Kris Kinghorn RN, MSN, ANP-BC Case Study 66 y/o female (Mrs. Olus A. Blader) Admitted with c/o palpitations and lightheadedness PMH:
DVT/PE Management with Rivaroxaban (Xarelto)
") DVT/PE Management with Rivaroxaban (Xarelto) Rivaroxaban is FDA approved for the acute treatment of DVT and PE and reduction in risk of recurrence of DVT and PE. FDA approved indications: Non valvular
DVT/PE Management with Rivaroxaban (Xarelto) Rivaroxaban is FDA approved for the acute treatment of DVT and PE and reduction in risk of recurrence of DVT and PE. FDA approved indications: Non valvular
Basic Medication Administration Exam RN (BMAE-RN) Study Guide
 Study Guide") Basic Medication Administration Exam RN (BMAE-RN) Study Guide Review correct procedure and precautions for the following routes of administration: Ear drops Enteral feeding tube Eye drops IM, subcut injections
Basic Medication Administration Exam RN (BMAE-RN) Study Guide Review correct procedure and precautions for the following routes of administration: Ear drops Enteral feeding tube Eye drops IM, subcut injections
Inpatient Code Sepsis March Update. Sarah Prebil
 Inpatient Code Sepsis March Update Sarah Prebil 3 hour bundle Time is life Kumar et al. Crit Care Med 2006; 34:1589-1596 But Sarah, why are you harassing us about sepsis? Pilot Results 10 Code Sepsis pabents
Inpatient Code Sepsis March Update Sarah Prebil 3 hour bundle Time is life Kumar et al. Crit Care Med 2006; 34:1589-1596 But Sarah, why are you harassing us about sepsis? Pilot Results 10 Code Sepsis pabents
Reference Range: 0.5-1.6 mmol/l (arterial) 0.7-2.1 mmol/l (venous) CPT Code: 83605
 0.7-2.1 mmol/l (venous) CPT Code: 83605") LACTIC ACID Fasting, arterial specimen preferred. Please note whether arterial or venous. 0.5 ml heparinized plasma. Green top or PST must be drawn, placed on ice, and spun within 15 minutes. Immediately
LACTIC ACID Fasting, arterial specimen preferred. Please note whether arterial or venous. 0.5 ml heparinized plasma. Green top or PST must be drawn, placed on ice, and spun within 15 minutes. Immediately
For Examiner Only Case Minor complaint with substance abuse issues Author; John Rose, MD Reviewer; Douglas Char, MD Approved; 10/26/05
 For Examiner Only Case Minor complaint with substance abuse issues Author; John Rose, MD Reviewer; Douglas Char, MD Approved; 10/26/05 CONTENT AREA Psychiatric/ Behavioral/Substance abuse ORAL CASE SUMMARY
For Examiner Only Case Minor complaint with substance abuse issues Author; John Rose, MD Reviewer; Douglas Char, MD Approved; 10/26/05 CONTENT AREA Psychiatric/ Behavioral/Substance abuse ORAL CASE SUMMARY
[ ] Cardiac monitoring Routine, Until discontinued, Starting today, PACU (only)
![[ ] Cardiac monitoring Routine, Until discontinued, Starting today, PACU (only)](/thumbs/26/8687689.jpg "[ ] Cardiac monitoring Routine, Until discontinued, Starting today, PACU (only)") If appropriate for patient condition, please consider the following order sets: Hydration Order for Reducing Risk of Radiocontrast Induced Nephrotoxicity #683 Over the Counter Patient Care Products #767
If appropriate for patient condition, please consider the following order sets: Hydration Order for Reducing Risk of Radiocontrast Induced Nephrotoxicity #683 Over the Counter Patient Care Products #767
PEDIATRIC DIABETIC KETOACIDOSIS
 PEDIATRIC DIABETIC KETOACIDOSIS October 2011 Quality Improvement Resources Illinois Emergency Medical Services for Children is a collaborative program between the Illinois Department of Public Health and
PEDIATRIC DIABETIC KETOACIDOSIS October 2011 Quality Improvement Resources Illinois Emergency Medical Services for Children is a collaborative program between the Illinois Department of Public Health and
Outpatient Treatment of Deep Vein Thrombosis with Low Molecular Weight Heparin (LMWH) Clinical Practice Guideline August 2013
 Clinical Practice Guideline August 2013") Outpatient Treatment of Deep Vein Thrombosis with Low Molecular Weight Heparin (LMWH) Clinical Practice Guideline August 2013 General Principles: There is compelling data in the medical literature to support
Outpatient Treatment of Deep Vein Thrombosis with Low Molecular Weight Heparin (LMWH) Clinical Practice Guideline August 2013 General Principles: There is compelling data in the medical literature to support
LAMC Reversal Agent Guideline for Anticoagulants 2013. Time to resolution of hemostasis (hrs) Therapeutic Options
 Therapeutic Options") LAMC Reversal Agent Guideline for Anticoagulants 2013 Medication resolution of hemostasis (hrs) Intervention Administration Instructions Heparin 3-4 Protamine 1mg IV for every 100 units of heparin Slow
LAMC Reversal Agent Guideline for Anticoagulants 2013 Medication resolution of hemostasis (hrs) Intervention Administration Instructions Heparin 3-4 Protamine 1mg IV for every 100 units of heparin Slow
Anticoagulant Reversal
 No Conflicts of Interest to Report Anticoagulant Reversal Matthew Bondi Pharm.D., BCPS March 14, 2015 Matthew Bondi Pharm.D., BCPS. Clinical Pharmacist Sparrow Hospital Matthew.bondi@sparrow.org Ph. 517.364.2031
No Conflicts of Interest to Report Anticoagulant Reversal Matthew Bondi Pharm.D., BCPS March 14, 2015 Matthew Bondi Pharm.D., BCPS. Clinical Pharmacist Sparrow Hospital Matthew.bondi@sparrow.org Ph. 517.364.2031
INR: RUPTURED ANEURYSM: POST EMBOLIZATION Patient Identification Page 1 of 5. Allergies: Weight: kg Diagnosis:
 Page 1 of 5 Allergies: Weight: kg Diagnosis: Service: Admission Admit to Inpatient Admit to Daypatient Place on Outpatient Observation Status Hospital Attending: Attending Physician Attending Provider:
Page 1 of 5 Allergies: Weight: kg Diagnosis: Service: Admission Admit to Inpatient Admit to Daypatient Place on Outpatient Observation Status Hospital Attending: Attending Physician Attending Provider:
Neonatal Reference Guide
 Operated by REACH Air Medical Services Assessment Heart Rate (beats/min.) Rate
Operated by REACH Air Medical Services Assessment Heart Rate (beats/min.) Rate
PHYSICIAN SIGNATURE DATE TIME DRUG ALLERGIES WT: KG
 DRUG AND TREATMENT Condition/Status This powerplan is only intended for use in those patients having symptoms related to alcohol withdrawal. See DSM-IV-TR criteria listed in the Alcohol Withdrawal ICU
DRUG AND TREATMENT Condition/Status This powerplan is only intended for use in those patients having symptoms related to alcohol withdrawal. See DSM-IV-TR criteria listed in the Alcohol Withdrawal ICU
ACID-BASE DISORDER. Presenter: NURUL ATIQAH AWANG LAH Preceptor: PN. KHAIRUL BARIAH JOHAN
 ACID-BASE DISORDER Presenter: NURUL ATIQAH AWANG LAH Preceptor: PN. KHAIRUL BARIAH JOHAN OBJECTIVES OF PRESENTATION 1. To refresh knowledge of acid-base disorders 2. To evaluate acid-base disorders using
ACID-BASE DISORDER Presenter: NURUL ATIQAH AWANG LAH Preceptor: PN. KHAIRUL BARIAH JOHAN OBJECTIVES OF PRESENTATION 1. To refresh knowledge of acid-base disorders 2. To evaluate acid-base disorders using
Chronic Thromboembolic Disease. Chronic Thromboembolic Disease Definition. Diagnosis Prevention Treatment Surgical Nonsurgical
 Chronic Thromboembolic Disease Diagnosis Prevention Treatment Surgical Nonsurgical Chronic Thromboembolic Disease Definition Pulmonary Hypertension due to chronic thromboembolism 6 months post acute PE:
Chronic Thromboembolic Disease Diagnosis Prevention Treatment Surgical Nonsurgical Chronic Thromboembolic Disease Definition Pulmonary Hypertension due to chronic thromboembolism 6 months post acute PE:
PROTOCOL TITLE: Ambulatory Initiation and Management of Warfarin for Adults
 PROTOCOL NUMBER: 7 PROTOCOL TITLE: Ambulatory Initiation and Management of Warfarin for Adults THIS PROTOCOL APPLIES TO: UW Health Clinics: all adult outpatients with an active order for warfarin TARGET
PROTOCOL NUMBER: 7 PROTOCOL TITLE: Ambulatory Initiation and Management of Warfarin for Adults THIS PROTOCOL APPLIES TO: UW Health Clinics: all adult outpatients with an active order for warfarin TARGET
Lothian Diabetes Handbook MANAGEMENT OF DIABETIC KETOACIDOSIS
 MANAGEMENT OF DIABETIC KETOACIDOSIS 90 MANAGEMENT OF DIABETIC KETOACIDOSIS Diagnosis elevated plasma and/or urinary ketones metabolic acidosis (raised H + /low serum bicarbonate) Remember that hyperglycaemia,
MANAGEMENT OF DIABETIC KETOACIDOSIS 90 MANAGEMENT OF DIABETIC KETOACIDOSIS Diagnosis elevated plasma and/or urinary ketones metabolic acidosis (raised H + /low serum bicarbonate) Remember that hyperglycaemia,
General PROVIDER INITIALS: PHYSICIAN ORDERS
 Height Weight Allergies If appropriate for patient condition, please consider the following order sets: Initiate Electrolyte Replcement: Med/Surg, Med/Surg Tele Physician Order #842 General Vital Signs
Height Weight Allergies If appropriate for patient condition, please consider the following order sets: Initiate Electrolyte Replcement: Med/Surg, Med/Surg Tele Physician Order #842 General Vital Signs
REFERENCE. Admit to: Program/Service: Diagnosis: Droplet/ Contact Airborne/ Contact
 Weight (kg) REFER TO THE ALLERGY SCREEN IN MEDITECH FOR ALLERGY INFORMATION To complete the order form, fill in the required blanks and/or check the appropriate boxes. To delete orders, draw one line through
Weight (kg) REFER TO THE ALLERGY SCREEN IN MEDITECH FOR ALLERGY INFORMATION To complete the order form, fill in the required blanks and/or check the appropriate boxes. To delete orders, draw one line through
CRRT: I and O. I and O Sheet
 CRRT: I and O I and O Sheet The following slide outlines a 12 hour CRRT I and O record. The individual lines of the I and O portion of the record will be reviewed. At the end of each hour, the ICU nurse
CRRT: I and O I and O Sheet The following slide outlines a 12 hour CRRT I and O record. The individual lines of the I and O portion of the record will be reviewed. At the end of each hour, the ICU nurse
Neonatal Reference Guide
 Operated by REACH Air Medical Services Assessment Heart Rate (beats/min.) Age Rate
Operated by REACH Air Medical Services Assessment Heart Rate (beats/min.) Age Rate
9/22/2015. About the Exam Itself. Test Taking Skills for Nursing Board Certification Exams. Day of the Exam MOMENT OF TRUTH RIGHT BEFORE THE EXAM
 Test Taking Skills for Nursing Board Certification Exams About the Exam Itself Test questions or items are written by certified nurses in the specialty of medical-surgical nursing Successful or unsuccessful
Test Taking Skills for Nursing Board Certification Exams About the Exam Itself Test questions or items are written by certified nurses in the specialty of medical-surgical nursing Successful or unsuccessful
PHYSICIAN ORDERS / PROGRESS NOTES
 PHYSICIAN / PROGRESS NOTES Drs Joseph Thibodeau and Louis Violi Created: 4/10 - Next Review: 4/10 Page 1 of 5 Initiation Phase: Emergency Department Notify Interventional Cardiology and Cath Lab immediately
PHYSICIAN / PROGRESS NOTES Drs Joseph Thibodeau and Louis Violi Created: 4/10 - Next Review: 4/10 Page 1 of 5 Initiation Phase: Emergency Department Notify Interventional Cardiology and Cath Lab immediately
Quiz 4 Arrhythmias summary statistics and question answers
 1 Quiz 4 Arrhythmias summary statistics and question answers The correct answers to questions are indicated by *. All students were awarded 2 points for question #2 due to no appropriate responses for
1 Quiz 4 Arrhythmias summary statistics and question answers The correct answers to questions are indicated by *. All students were awarded 2 points for question #2 due to no appropriate responses for
Section Two: Arterial Pressure Monitoring
 Section Two: Arterial Pressure Monitoring Indications An arterial line is indicated for blood pressure monitoring for the patient with any medical or surgical condition that compromises cardiac output,
Section Two: Arterial Pressure Monitoring Indications An arterial line is indicated for blood pressure monitoring for the patient with any medical or surgical condition that compromises cardiac output,
2. Order: Nipride 500 mg IV in 250 ml D5w at 2 mcg/kg/min for a patient weighing 125 lb. Administer at ml/hr
 1 Pharmacology Review Quiz: 1. Order: Xylocaine 1 g IV in 500 ml D5W at 3 mg/min. Set the infusion pump at ml/hr 2. Order: Nipride 500 mg IV in 250 ml D5w at 2 mcg/kg/min for a patient weighing 125 lb.
1 Pharmacology Review Quiz: 1. Order: Xylocaine 1 g IV in 500 ml D5W at 3 mg/min. Set the infusion pump at ml/hr 2. Order: Nipride 500 mg IV in 250 ml D5w at 2 mcg/kg/min for a patient weighing 125 lb.
PREPARATIONS: Adrenaline 1mg in 1ml (1:1000) Adrenaline 100micrograms in 1ml (1:10,000)
 Adrenaline 100micrograms in 1ml (1:10,000)") ADRENALINE Acute hypotension Via a CENTRAL venous line Initially 100-300 nanograms/kg/minute 0.1-0.3 microgram/kg/minute adjusted according to response up to a maximum of 1.5 micrograms/kg/minute. Increase
ADRENALINE Acute hypotension Via a CENTRAL venous line Initially 100-300 nanograms/kg/minute 0.1-0.3 microgram/kg/minute adjusted according to response up to a maximum of 1.5 micrograms/kg/minute. Increase
TOTAL PARENTERAL NUTRITION (TPN) Revised January 2013
 Revised January 2013") TOTAL PARENTERAL NUTRITION (TPN) Revised January 2013 OBJECTIVES Definition Indications for TPN administration Composition of TPN solutions Access routes for TPN administration Monitoring TPN administration
TOTAL PARENTERAL NUTRITION (TPN) Revised January 2013 OBJECTIVES Definition Indications for TPN administration Composition of TPN solutions Access routes for TPN administration Monitoring TPN administration
Acute Ischemic Stroke with tpa
 Admission/Condition/Diagnosis Admission: Admitting Physician Attending Physician Assign to Inpatient Status Transfer to Level of Care: Physician MUST document in notes the risk, severity, and skilled nursing
Admission/Condition/Diagnosis Admission: Admitting Physician Attending Physician Assign to Inpatient Status Transfer to Level of Care: Physician MUST document in notes the risk, severity, and skilled nursing
ROYAL HOSPITAL FOR WOMEN
 ROYAL HOSPITAL FOR WOMEN LOCAL OPERATING PROCEDURE CLINICAL POLICIES, PROCEDURES & GUIDELINES Approved by Quality & Patient Safety Committee 17 April 2014 INSULIN INFUSION PROTOCOL INSULIN DEXTROSE INFUSION
ROYAL HOSPITAL FOR WOMEN LOCAL OPERATING PROCEDURE CLINICAL POLICIES, PROCEDURES & GUIDELINES Approved by Quality & Patient Safety Committee 17 April 2014 INSULIN INFUSION PROTOCOL INSULIN DEXTROSE INFUSION
Replacement post-filter (ml/hr) Blood flow (ml/min) Dialysate (ml/hr) Weight (kg)
 Blood flow (ml/min) Dialysate (ml/hr) Weight (kg)") 404FM.1 CONTINUOUS RENAL REPLACEMENT THERAPY (CRRT) USING CITRATE Target Audience: Hospital only ICU (Based on Gambro and Kalmar Hospital protocols) CRRT using regional citrate anticoagulation This is
404FM.1 CONTINUOUS RENAL REPLACEMENT THERAPY (CRRT) USING CITRATE Target Audience: Hospital only ICU (Based on Gambro and Kalmar Hospital protocols) CRRT using regional citrate anticoagulation This is
RGN JOY LAUDE WATFORD GENERAL HOSPITAL, ENGLAND
 RGN JOY LAUDE WATFORD GENERAL HOSPITAL, ENGLAND Monitor patient on the ward to detect trends in vital signs and to manage accordingly To recognise deteriorating trends and request relevant medical/out
RGN JOY LAUDE WATFORD GENERAL HOSPITAL, ENGLAND Monitor patient on the ward to detect trends in vital signs and to manage accordingly To recognise deteriorating trends and request relevant medical/out
Early Warning Scores (EWS) Clinical Sessions 2011 By Bhavin Doshi
 Clinical Sessions 2011 By Bhavin Doshi") Early Warning Scores (EWS) Clinical Sessions 2011 By Bhavin Doshi What is EWS? After qualifying, junior doctors are expected to distinguish between the moderately sick patients who can be managed in the
Early Warning Scores (EWS) Clinical Sessions 2011 By Bhavin Doshi What is EWS? After qualifying, junior doctors are expected to distinguish between the moderately sick patients who can be managed in the
Case 2:10-md-02179-CJB-SS Document 6427-14 Filed 05/03/12 Page 1 of 5 EXHIBIT 12
 Case 2:10-md-02179-CJB-SS Document 6427-14 Filed 05/03/12 Page 1 of 5 EXHIBIT 12 Case 2:10-md-02179-CJB-SS Document 6427-14 Filed 05/03/12 Page 2 of 5 Components of the PERIODIC MEDICAL CONSULTATION PROGRAM
Case 2:10-md-02179-CJB-SS Document 6427-14 Filed 05/03/12 Page 1 of 5 EXHIBIT 12 Case 2:10-md-02179-CJB-SS Document 6427-14 Filed 05/03/12 Page 2 of 5 Components of the PERIODIC MEDICAL CONSULTATION PROGRAM
ESIM 2014 WHEN CHRONIC BECOMES ACUTE
 ESIM 2014 WHEN CHRONIC BECOMES ACUTE Anna Salina, MD Pauls Stradins Clinical University Hospital Riga, Latvia 37 years old female, 50 kg, 150 cm Complaints Severe edema +8 kg Tiredness, dry cough Chills
ESIM 2014 WHEN CHRONIC BECOMES ACUTE Anna Salina, MD Pauls Stradins Clinical University Hospital Riga, Latvia 37 years old female, 50 kg, 150 cm Complaints Severe edema +8 kg Tiredness, dry cough Chills
How To Treat An Alcoholic Patient
 Height Weight Allergies If appropriate for patient condition, please consider the following order sets: Initiate Electrolyte Replcement: Med/Surg, Med/Surg Tele Physician Order #842 Discontinue all lorazepam
Height Weight Allergies If appropriate for patient condition, please consider the following order sets: Initiate Electrolyte Replcement: Med/Surg, Med/Surg Tele Physician Order #842 Discontinue all lorazepam
NICE Pathways bring together all NICE guidance, quality standards and other NICE information on a specific topic.
 Diabetic ketoacidosis in children and young people bring together all NICE guidance, quality standards and other NICE information on a specific topic. are interactive and designed to be used online. They
Diabetic ketoacidosis in children and young people bring together all NICE guidance, quality standards and other NICE information on a specific topic. are interactive and designed to be used online. They
Continuous Renal Replacement Therapy. Jai Radhakrishnan, MD, MS
 Continuous Renal Replacement Therapy Jai Radhakrishnan, MD, MS History of the CRRT program 1988 Open heart program Active transplant program Deep dissatisfaction with peritoneal dialysis in hemodynamically
Continuous Renal Replacement Therapy Jai Radhakrishnan, MD, MS History of the CRRT program 1988 Open heart program Active transplant program Deep dissatisfaction with peritoneal dialysis in hemodynamically
2011 EBM-hyperglycemia
 嗎 2011 EBM-hyperglycemia 陳 莉 瑋 醫 師 一 定 要 打 打 bolus insulin? 用 FinePrint 列 印 - 可 在 www.ahasoft.com.tw/fineprint 訂 購 Question 1 Is bolus insulin necessary in DKA? P:DKA adult patient I:initial bolus insulin+insulin
嗎 2011 EBM-hyperglycemia 陳 莉 瑋 醫 師 一 定 要 打 打 bolus insulin? 用 FinePrint 列 印 - 可 在 www.ahasoft.com.tw/fineprint 訂 購 Question 1 Is bolus insulin necessary in DKA? P:DKA adult patient I:initial bolus insulin+insulin
ACID- BASE and ELECTROLYTE BALANCE. MGHS School of EMT-Paramedic Program 2011
 ACID- BASE and ELECTROLYTE BALANCE MGHS School of EMT-Paramedic Program 2011 ACID- BASE BALANCE Ions balance themselves like a see-saw. Solutions turn into acids when concentration of hydrogen ions rises
ACID- BASE and ELECTROLYTE BALANCE MGHS School of EMT-Paramedic Program 2011 ACID- BASE BALANCE Ions balance themselves like a see-saw. Solutions turn into acids when concentration of hydrogen ions rises
DRUG CALCULATIONS FOR REGISTERED NURSES ADULT SERVICES
 Serving the people of north east Essex DRUG CALCULATIONS FOR REGISTERED NURSES ADULT SERVICES A Programmed Approach - It is essential you read this pack & practice the questions prior to your drug calculation
Serving the people of north east Essex DRUG CALCULATIONS FOR REGISTERED NURSES ADULT SERVICES A Programmed Approach - It is essential you read this pack & practice the questions prior to your drug calculation
PHYSICIAN SIGNATURE DATE TIME DRUG ALLERGIES WT: KG
 MED Hospitalist Stroke-TIA Vital Signs Vital Signs Q4H (DEF)* Q2H Q1H Vital Signs Orthostatic Activity Activity Bedrest, for 12 hours then Up ad lib (DEF)* Bedrest, for 24 hours then Up ad lib Up Ad Lib
MED Hospitalist Stroke-TIA Vital Signs Vital Signs Q4H (DEF)* Q2H Q1H Vital Signs Orthostatic Activity Activity Bedrest, for 12 hours then Up ad lib (DEF)* Bedrest, for 24 hours then Up ad lib Up Ad Lib
Dabigatran (Pradaxa) Guidelines
 Guidelines") Dabigatran (Pradaxa) Guidelines Dabigatran is a new anticoagulant for reducing the risk of stroke in patients with atrial fibrillation. Dabigatran is a direct thrombin inhibitor, similar to warfarin, without
Dabigatran (Pradaxa) Guidelines Dabigatran is a new anticoagulant for reducing the risk of stroke in patients with atrial fibrillation. Dabigatran is a direct thrombin inhibitor, similar to warfarin, without
USC Pediatric Residency Program Quality Improvement Pre-Program Self Assessment
 USC Pediatric Residency Program Quality Improvement Pre-Program Self Assessment 1. Have you had previous experience in quality improvement (QI)? Yes No 2. How many formal quality improvement projects have
USC Pediatric Residency Program Quality Improvement Pre-Program Self Assessment 1. Have you had previous experience in quality improvement (QI)? Yes No 2. How many formal quality improvement projects have
Sepsis: Identification and Treatment
 Sepsis: Identification and Treatment Daniel Z. Uslan, MD Associate Clinical Professor Division of Infectious Diseases Medical Director, UCLA Sepsis Task Force Severe Sepsis: A Significant Healthcare Challenge
Sepsis: Identification and Treatment Daniel Z. Uslan, MD Associate Clinical Professor Division of Infectious Diseases Medical Director, UCLA Sepsis Task Force Severe Sepsis: A Significant Healthcare Challenge
Chronic Obstructive Pulmonary Disease (COPD) Admission Order Set
 Admission Order Set") Patient Name: PHN: Page 1/1 Admit to Dr: Notified Consult: Dr: Family Dr: Precautions: Contact Droplet Enhanced Droplet Airborne - Reason: _ Code Status: Full Resuscitation or Consults: Reason: Dietician
Patient Name: PHN: Page 1/1 Admit to Dr: Notified Consult: Dr: Family Dr: Precautions: Contact Droplet Enhanced Droplet Airborne - Reason: _ Code Status: Full Resuscitation or Consults: Reason: Dietician
Chapter 16. Learning Objectives. Learning Objectives 9/11/2012. Shock. Explain difference between compensated and uncompensated shock
 Chapter 16 Shock Learning Objectives Explain difference between compensated and uncompensated shock Differentiate among 5 causes and types of shock: Hypovolemic Cardiogenic Neurogenic Septic Anaphylactic
Chapter 16 Shock Learning Objectives Explain difference between compensated and uncompensated shock Differentiate among 5 causes and types of shock: Hypovolemic Cardiogenic Neurogenic Septic Anaphylactic
What You Need to KnowWhen Taking Anticoagulation Medicine
 What You Need to KnowWhen Taking Anticoagulation Medicine What are anticoagulant medicines? Anticoagulant medicines are a group of medicines that inhibit blood clotting, helping to prevent blood clots.
What You Need to KnowWhen Taking Anticoagulation Medicine What are anticoagulant medicines? Anticoagulant medicines are a group of medicines that inhibit blood clotting, helping to prevent blood clots.
PAH. Salman Bin AbdulAziz University College Of Pharmacy 22/01/35
 Salman Bin AbdulAziz University College Of Pharmacy PAH Therapeutics II PHCL 430 Ahmed A AlAmer PharmD R.W. is a 38-year-old obese woman who presents with increasing symptoms of fatigue and shortness of
Salman Bin AbdulAziz University College Of Pharmacy PAH Therapeutics II PHCL 430 Ahmed A AlAmer PharmD R.W. is a 38-year-old obese woman who presents with increasing symptoms of fatigue and shortness of
Implementation Guide
 HAWAII HEALTH INFORMATION CORPORATION HAWAII S SOURCE FOR HEALTHCARE Implementation Guide ASCII HL7 Specifications for Laboratory Observation Reporting Technical Specifications and Transmittal Instructions
HAWAII HEALTH INFORMATION CORPORATION HAWAII S SOURCE FOR HEALTHCARE Implementation Guide ASCII HL7 Specifications for Laboratory Observation Reporting Technical Specifications and Transmittal Instructions
Session 3 Topics. Argatroban. Argatroban. Drug Use and Adverse Effects. Laboratory Monitoring of Anticoagulant Therapy
 ~~Marshfield Labs Presents~~ Laboratory Monitoring of Anticoagulant Therapy Session 3 of 4 Michael J. Sanfelippo, M.S. Technical Director, Coagulation Services Session 3 Topics Direct Thrombin Inhibitors:
~~Marshfield Labs Presents~~ Laboratory Monitoring of Anticoagulant Therapy Session 3 of 4 Michael J. Sanfelippo, M.S. Technical Director, Coagulation Services Session 3 Topics Direct Thrombin Inhibitors:
National Patient Safety Goals Effective January 1, 2015
 National Patient Safety Goals Goal 1 Nursing are enter ccreditation Program Improve the accuracy of patient and resident identification. NPSG.01.01.01 Use at least two patient or resident identifiers when
National Patient Safety Goals Goal 1 Nursing are enter ccreditation Program Improve the accuracy of patient and resident identification. NPSG.01.01.01 Use at least two patient or resident identifiers when
Acid-Base Disorders. Jai Radhakrishnan, MD, MS
 Acid-Base Disorders Jai Radhakrishnan, MD, MS 1 Diagnostic Considerations Data points required: ABG: ph, pco 2, HCO 3 Chem-7 panel: anion gap Step 1: Acidemia/alkalemia (Primary disorder) Step 2: Compensation
Acid-Base Disorders Jai Radhakrishnan, MD, MS 1 Diagnostic Considerations Data points required: ABG: ph, pco 2, HCO 3 Chem-7 panel: anion gap Step 1: Acidemia/alkalemia (Primary disorder) Step 2: Compensation
Anticoagulation Dosing at UCDMC Indication Agent Standard Dose Comments and Dose Adjustments VTE Prophylaxis All Services UFH 5,000 units SC q 8 h
 Indication Agent Standard Dose Comments and Dose Adjustments VTE Prophylaxis All Services UFH 5,000 units SC q 8 h See EMR adult VTE prophylaxis CI order set Enoxaparin See service specific dosing Assess
Indication Agent Standard Dose Comments and Dose Adjustments VTE Prophylaxis All Services UFH 5,000 units SC q 8 h See EMR adult VTE prophylaxis CI order set Enoxaparin See service specific dosing Assess
V: Infusion Therapy. Alberta Licensed Practical Nurses Competency Profile 217
 V: Infusion Therapy Alberta Licensed Practical Nurses Competency Profile 217 Competency: V-1 Knowledge of Intravenous Therapy V-1-1 V-1-2 V-1-3 V-1-4 V-1-5 Demonstrate knowledge and ability to apply critical
V: Infusion Therapy Alberta Licensed Practical Nurses Competency Profile 217 Competency: V-1 Knowledge of Intravenous Therapy V-1-1 V-1-2 V-1-3 V-1-4 V-1-5 Demonstrate knowledge and ability to apply critical
Anticoagulant therapy
 Anticoagulation: The risks Anticoagulant therapy 1990 2002: 600 incidents reported 120 resulted in death of patient 92 deaths related to warfarin usage 28 reports related to heparin usage Incidents in
Anticoagulation: The risks Anticoagulant therapy 1990 2002: 600 incidents reported 120 resulted in death of patient 92 deaths related to warfarin usage 28 reports related to heparin usage Incidents in
Advanced Issues in Peri-Operative VTE Prevention
 Advanced Issues in Peri-Operative VTE Prevention Michael-Anthony (M-A) Williams, M.D. Consultant Physician Centura Medical Consultants September 27th, 2012 Main Topics 1. The perils of the early mover-
Advanced Issues in Peri-Operative VTE Prevention Michael-Anthony (M-A) Williams, M.D. Consultant Physician Centura Medical Consultants September 27th, 2012 Main Topics 1. The perils of the early mover-
ACLS Cardiac Arrest Algorithm Neumar, R. W. et al. Circulation 2010;122:S729-S767
 ACLS Cardiac Arrest Algorithm Neumar, R. W. et al. Circulation 2010;122:S729-S767 Copyright 2010 American Heart Association ACLS Cardiac Arrest Circular Algorithm Neumar, R. W. et al. Circulation 2010;122:S729-S767
ACLS Cardiac Arrest Algorithm Neumar, R. W. et al. Circulation 2010;122:S729-S767 Copyright 2010 American Heart Association ACLS Cardiac Arrest Circular Algorithm Neumar, R. W. et al. Circulation 2010;122:S729-S767
Upstate University Health System Medication Exam - Version A
 Upstate University Health System Medication Exam - Version A Name: ID Number: Date: Unit: Directions: Please read each question below. Choose the best response for each of the Multiple Choice and Medication
Upstate University Health System Medication Exam - Version A Name: ID Number: Date: Unit: Directions: Please read each question below. Choose the best response for each of the Multiple Choice and Medication
User guide Basal-bolus Insulin Dosing Chart: Adult
 Contacts and further information Local contact Clinical pharmacy or visiting pharmacy Diabetes education service Director of Medical Services Visiting or local endocrinologist or diabetes physician For
Contacts and further information Local contact Clinical pharmacy or visiting pharmacy Diabetes education service Director of Medical Services Visiting or local endocrinologist or diabetes physician For
3% Sodium Chloride Injection, USP 5% Sodium Chloride Injection, USP
 PRESCRIBING INFORMATION 3% Sodium Chloride Injection, USP 5% Sodium Chloride Injection, USP IV Fluid and Electrolyte Replenisher Baxter Corporation Mississauga, Ontario L5N 0C2 Canada Date of Revision:
PRESCRIBING INFORMATION 3% Sodium Chloride Injection, USP 5% Sodium Chloride Injection, USP IV Fluid and Electrolyte Replenisher Baxter Corporation Mississauga, Ontario L5N 0C2 Canada Date of Revision:
Policies & Procedures. ID Number: 1118
 Policies & Procedures Title: INTRAVENOUS AND/OR PERIPHERAL SALINE LOCK INSERTION AND MAINTENANCE ID Number: 1118 Authorization [X] SHR Nursing Practice Committee Source: Nursing Date Revised: September
Policies & Procedures Title: INTRAVENOUS AND/OR PERIPHERAL SALINE LOCK INSERTION AND MAINTENANCE ID Number: 1118 Authorization [X] SHR Nursing Practice Committee Source: Nursing Date Revised: September
0.9% Sodium Chloride injection may be used in most cases.
 Table 2. Alternatives to Heparin Sodium in Selected Situations 12-14 Situation Alternative Dose Maintain patency of peripheral venous catheters* 21-26 0.9% Sodium Chloride injection may be used in most
Table 2. Alternatives to Heparin Sodium in Selected Situations 12-14 Situation Alternative Dose Maintain patency of peripheral venous catheters* 21-26 0.9% Sodium Chloride injection may be used in most
Allergy Emergency Treatment Protocol
 Allergy Emergency Treatment Protocol I. Initial evaluation of possible allergic reaction a. Cease administration of allergenic extracts b. Notify physician c. Record vital signs: blood pressure, pulse,
Allergy Emergency Treatment Protocol I. Initial evaluation of possible allergic reaction a. Cease administration of allergenic extracts b. Notify physician c. Record vital signs: blood pressure, pulse,
SECTION: NM NUMBER: 20. HENRY FORD HOSPITAL DETROIT, MICHIGAN TITLE: GLYCEMIC CONTROL INTENSIVE CARE PROTOCOL UNIT: All ICUs
 CLINICALPROTOCOL MULTIDISCIPLINARY SECTION: NM NUMBER: 2 HENRY FORD HOSPITAL DETROIT, MICHIGAN TITLE: GLYCEMIC CONTROL INTENSIVE CARE PROTOCOL UNIT: All ICUs APPROVED: 3/3 REVIEWED: REVISED: 12/3, 5/,
CLINICALPROTOCOL MULTIDISCIPLINARY SECTION: NM NUMBER: 2 HENRY FORD HOSPITAL DETROIT, MICHIGAN TITLE: GLYCEMIC CONTROL INTENSIVE CARE PROTOCOL UNIT: All ICUs APPROVED: 3/3 REVIEWED: REVISED: 12/3, 5/,
University of Gezira. Faculty of Medicine. Department of Paediatrics and Child Health. Integrated Management of Diabetes in Children (IMDC) Project
 Project") University of Gezira Faculty of Medicine Department of Paediatrics and Child Health Integrated Management of Diabetes in Children (IMDC) Project Guidelines for Diabetes Management in Children 2007 1 These
University of Gezira Faculty of Medicine Department of Paediatrics and Child Health Integrated Management of Diabetes in Children (IMDC) Project Guidelines for Diabetes Management in Children 2007 1 These
5/21/2012. Perioperative Use Issues. On admission: During hospitalization:
 Dabigatran and Rivaroxaban: Challenges in the Perioperative Setting Claudia Swenson, Pharm.D., CDE, BC-ADM, FASHP Central Washington Hospital Wenatchee, WA claudia.swenson@cwhs.com Dabigatran and Rivaroxaban:
Dabigatran and Rivaroxaban: Challenges in the Perioperative Setting Claudia Swenson, Pharm.D., CDE, BC-ADM, FASHP Central Washington Hospital Wenatchee, WA claudia.swenson@cwhs.com Dabigatran and Rivaroxaban:
Cardiac Arrest. Perioperative. Summary of case. Length 15-20 minutes
 scenario overview Summary of case This 45-year-old obese patient is positioned on the OR table for left inguinal hernia repair. New Anesthesia Provider comes to the ED to relieve the current Anesthesia
scenario overview Summary of case This 45-year-old obese patient is positioned on the OR table for left inguinal hernia repair. New Anesthesia Provider comes to the ED to relieve the current Anesthesia
Basic Medication Administration Exam LPN/LVN (BMAE-LPN/LVN) Study Guide
 Study Guide") Basic Medication Administration Exam LPN/LVN (BMAE-LPN/LVN) Study Guide Review correct procedure and precautions for the following routes of administration: Ear drops Enteral feeding tube Eye drops IM,
Basic Medication Administration Exam LPN/LVN (BMAE-LPN/LVN) Study Guide Review correct procedure and precautions for the following routes of administration: Ear drops Enteral feeding tube Eye drops IM,
Level III Stroke Center Data Collection Requirements
 Who? Level III Stroke Center Data Collection Requirements All LERN Level III Stroke Centers. LERN Level I and II Stroke Centers have reporting requirements to The Joint Commission or other Board approved
Who? Level III Stroke Center Data Collection Requirements All LERN Level III Stroke Centers. LERN Level I and II Stroke Centers have reporting requirements to The Joint Commission or other Board approved
2.5mg SC daily. INR target 2-3 30 mg SC q 12 hr or 40mg daily. 10 mg PO q day (CrCl 30 ml/min). Avoid if < 30 ml/min. 2.
. Avoid if < 30 ml/min. 2.") Anticoagulation dosing at UCDMC (SC=subcutaneously; CI=continuous infusion) Indication Agent Dose Comments Prophylaxis Any or No bleeding risk factors see adult heparin (VTE prophylaxis) IV infusion order
Anticoagulation dosing at UCDMC (SC=subcutaneously; CI=continuous infusion) Indication Agent Dose Comments Prophylaxis Any or No bleeding risk factors see adult heparin (VTE prophylaxis) IV infusion order
Intravenous Therapy. Marjorie Wiltshire, RN
 Intravenous Therapy Marjorie Wiltshire, RN :OBJECTIVES Define key terms related to intravenous therapy. Demonstrate the procedure for IV insertion, conversion to a saline lock, administration of IV fluids,
Intravenous Therapy Marjorie Wiltshire, RN :OBJECTIVES Define key terms related to intravenous therapy. Demonstrate the procedure for IV insertion, conversion to a saline lock, administration of IV fluids,
Medication Calculation Practice Problems
 1 Medication Calculation Practice Problems Dosage Calculation 1. The order is for 60 mg of furosemide (Lasix) po daily. Available to the nurse is Lasix 40 mg/tablet. The nurse would administer how many
1 Medication Calculation Practice Problems Dosage Calculation 1. The order is for 60 mg of furosemide (Lasix) po daily. Available to the nurse is Lasix 40 mg/tablet. The nurse would administer how many
Diabetic Ketoacidosis: When Sugar Isn t Sweet!!!
 Diabetic Ketoacidosis: When Sugar Isn t Sweet!!! W Ricks Hanna Jr MD Assistant Professor of Pediatrics University of Tennessee Health Science Center LeBonheur Children s Hospital Introduction Diabetes
Diabetic Ketoacidosis: When Sugar Isn t Sweet!!! W Ricks Hanna Jr MD Assistant Professor of Pediatrics University of Tennessee Health Science Center LeBonheur Children s Hospital Introduction Diabetes
DATE / TIME PROVIDER INITIALS PHYSICIAN ORDERS
 If appropriate for this patient, please consider the following order sets: Heart Failure Addendum #609; Acute COPD #789, Glycemic Control - Insulin Infusion #824, Glycemic Control - Subcutaneous Addendum
If appropriate for this patient, please consider the following order sets: Heart Failure Addendum #609; Acute COPD #789, Glycemic Control - Insulin Infusion #824, Glycemic Control - Subcutaneous Addendum