Outpatient Management of COPD. Alan DeAngelo, MD, FACP, FCCP LTC, MC Eisenhower Army Medical Center 25 October 2014
|
|
|
- Emily Lynch
- 7 years ago
- Views:
Transcription


1 Outpatient Management of COPD Alan DeAngelo, MD, FACP, FCCP LTC, MC Eisenhower Army Medical Center 25 October 2014
2 Disclosure No financial relationships. The following presentation does not reflect the views or opinions of EAMC, the Army Medical Corps or the Department of Defense.
3 Learning Objectives Review the classification schemes for COPD Enhance knowledge of non-pharmacologic and pharmacologic treatments for COPD Utilize disease severity to determine the optimal treatment regimen
4 WHO defines COPD Chronic obstructive pulmonary disease (COPD), a common preventable and treatable disease, is characterized by airflow limitation that is usually progressive and associated with an enhanced chronic inflammatory response in the airways and the lung to noxious particles or gases. Exacerbations and comorbidities contribute to the overall severity in individual patients."
5 Outline Introduction Classification and Prognostic determination Therapy and Management Non-pharmacologic Pharmacologic Surgical Acute exacerbation Questions
6 Which is true regarding mortality of COPD? A. 4 th leading cause of death in US and affects more women then men. B. #1 cause of death and affects sexes equally C. 4 th leading cause of death in US and affects more men than women D. 8 th leading cause of death The correct answer is A.
7 Overview Growing global health problem 5% of population affected Chronicity resulting in rising health care costs Mortality rate: 4 th leading cause of death according WHO statistics 3 rd in US; 120k per year (Natl Vital Stat Rep Dec;59(10):1-126). Women account for rise in death rate over past 30 years (Mannino DM. Resp Care 2002;47: ).
8 Symptoms Dyspnea Cough Sputum production Exposure risk Tobacco (80%) Occupational and Environmental exposure Biomass fuels, dust, particulate matter Airflow obstruction, persistent FEV1/FVC < 0.7 Definition
9 Pathophysiological Features of Airflow ObstrucPation in Chronic Obstructive Pulmonary Disease (PhPathoCOPD). Niewoehner DE. N Engl J Med 2010;362:
10
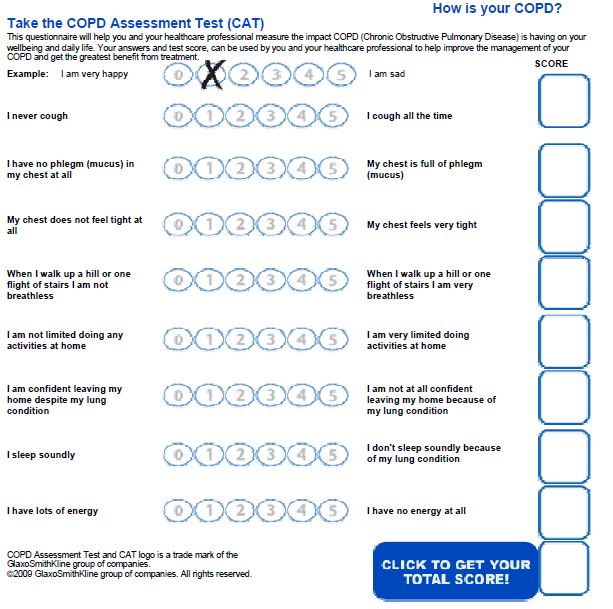
11 Classification Symptom scales Modified Medical Research Council (MMRC) COPD assessment test (CAT) St George s Respiratory Questionnaire (SGRQ) Prognostic indicator BODE=Body mass index, obstruction, dyspnea, exercise capacity GOLD 2011 vs 2007 Symptoms, exacerbation history & FEV1 to guide therapy
12 MMRC Grade: Description 0 = I only get breathless with strenuous exercise 1 = I get short of breath when hurrying on level ground or walking up a slight hill 2 = On level ground, I walk slower than people of the same age because of breathlessness, or have to stop for breath when walking at my own pace 3 = I stop for breath after walking about 100 yards or after a few minutes on level ground 4 = I am too breathless to leave the house or I am breathless when dressing. Fletcher CM, et al. BMJ 1959;2:257
13 COPD Assessment Test Designed as a quality of life measure 8 questions, each rated 0-5 Low impact 0-10 Medium impact High impact Very high impact Developed by industry and can be accessed at Integrated by GOLD 2011 initiative
14
15 SGRQ Widely used in research protocols 76 item questionnaire 3 component scores Symptoms Activity Impact on daily life Total score Not used in routine clinical practice
16 Prognostic Tool Body Mass Index Less than 21 Obstruction Severity of FEV1 post bronchodilator Dyspnea MMRC rating Exercise Capacity 6minute walk distance Estimates 4 year survival Points Survival (%) CElli BR. N Engl J Med 2004 ;350:
17 GOLD Classification Global Initiative for chronic obstructive lung disease NHLBI and WHO collaboration 2007 Classification based on FEV modifies classification Deemphasize FEV1 alone Adds symptom control and risk assessment Annual updates
18 GOLD 2007 Stage Severity Post BD FEV1 (%predicted) 1 Mild >80 2 Moderate Severe Very severe <30, or <50 + CRF
19 GOLD 2011
20
21 Which of the following management strategies provides a mortality benefit in COPD? A. Optimal medical therapy B. Pulmonary rehabilitation program C. Smoking cessation D. Insuring appropriate vaccination status The answer is C. smoking cessation
22 Management Goals Combine Non-pharmacologic and pharmacologic treatments Disease severity guides therapy Reduce symptom impact Relieve acute and mitigate chronic symptoms Improve exercise tolerance Reduce risk of long term complications Prevent disease progression Prevent and treat acute exacerbations Reduce mortality GOLD 2011 (updated Jan 2014).
23 Non-pharmacologic Therapy Smoking cessation Vaccines Pulmonary rehabilitation Oxygen therapy
24 Smoking Cessation Lung Health Study findings Cessation resulted in: Reduction in FEV1 decline Reduced long term, all cause mortality Mild to moderate COPD subjects Extrapolated to severe patients JAMA 1994: 272; Ann Intern Med 2005:142;233-39
25 Smoking Cessation Approaches Physician role Counselling/group program Nicotine replacement Oral agents ecigarettes Best results with combination therapy Effect of lung age on cessation Ask Advise Assess Assist Arrange 35% at 1 year 22% sustained at 5 years Lung Health Study BMJ 2008;336: JAMA 1994;272:
26 Tobacco Use #1 risk factor 80% of COPD patients in US Environmental exposure Dose response relationship Genetic predisposition for susceptibility <15pk years unlikely to result in obstruction 40pk years predicts obstruction
27 Fletcher-Peto Curve Natural history of chronic airflow obstruction and smoking status Fletcher and Peto. Br Med J 1977;1:1645-8
28 Disease Specific Vaccines Increased morbidity in COPD Influenza Pneumonia ACIP/ACP recommendations Influenza for all patients > 6 months; annual PPV 23 all adults with COPD; re-vaccinate in 5 yrs Any adult >65 PCV 13 all adults > 65 (1 time dose)
29 Targets of Exercise Training as Part of a Pulmonary Rehabilitation Program for Patients with COPD. Casaburi R, ZuWallack R. N Engl J Med 2009;360:
30 Pulmonary Rehabilitation Disease progression and functional status Muscle and CV deconditioning Goal: improve functional status Structured and individualized Exercise and education Multiple sessions over 6-12 weeks
31 Pulmonary Rehabilitation Studies in severe disease (FEV1 < 50%) Improvement in: Dyspnea scores 6 minute walk distance Quality of life, depression, sense of breathlessness Waning effect in 1 year Conflicting results in setting of AECOPD BMJ 2004;329: BMJ 2014;349:4315
32 Pulmonary Rehabilitation Who should be referred Moderate to Severe disease Reduced functional capacity Cardiovascular disease excluded Combine with smoking cessation
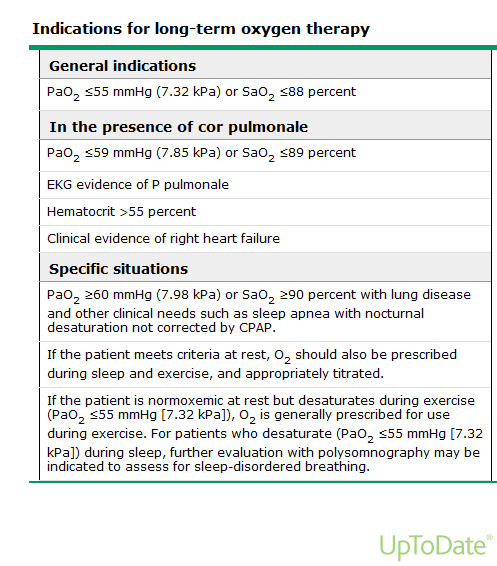
33 Which of the following patient s will derive a mortality benefit from long term oxygen therapy? A. 65 year old male with SaO2 86% during 6 minute walk test. B. 64 year old female with SaO2 nadir 84% during overnight oximetry testing C. 66 year old male with resting SaO2 86% D. 59 year old female with resting SaO2 89% without signs of cor pulmonale The answer is C.
34 Long Term Oxygen Therapy Mortality benefit in severe hypoxemia (PaO2 <55, SaO2 < 88% at rest) NOTT (Ann Intern Med 1980;93:391-8) MMRC (Lancet 1981:1:681-6) Established use of continuous O2 18 hours/day including sleep Target SaO2 >92%
35 Long Term Oxygen Therapy Mortality Benefit not proven Moderate hypoxemia (PaO ) Thorax 1997;52:674-9 Isolated nocturnal desaturation Eur Respir J 1999;14: Isolated exertional desaturation Am J Respir Crit Care Med 2007;176:343-9 Quality of life improvement? In laboratory setting Self reported metrics
36
37 Long Term Oxygen Therapy Testing completed in stable, outpatient setting Target flow rate to SaO2 >92% 18 hours per day including sleep For rest hypoxemia Exertional plus nocturnal use For ambulatory only desaturation Nocturnal only Isolated nocturnal hypoxemia in COPD Consider PSG
38
39 All of the following are true statements except: A. Long acting bronchodilators are favored over short acting agents for disease control B. Inhaled corticosteroid monotherapy is recommended for symptomatic COPD C. Oral glucocorticoids are not recommended for maintenance therapy D. Novel agents may reduce risk of exacerbations (roflumilast, azithromycin) The answer is B.
40 Pharmacologic Management Determine symptoms Classify risk = stage Initiate therapy Step up therapy based on risk stratification and clinical course
41 Pharmacologic Therapy Bronchodilators Short acting Long acting Inhaled corticosteroid + Bronchodilator PDE-4 inhibitor Macrolide Oral corticosteroids Theophylline
42 Pharmacologic Therapy Short acting bronchodilators Beta agonist Anticholinergic Provide immediate symptom relief Improve FEV1 and symptoms Intermittent vs scheduled Alone or in combination Bronchodilator effect additive No clear impact on frequency of exacerbations
43 Pharmacologic Therapy Long acting bronchodilators Beta agonist Anticholinergic (LAMA) Sustained symptom control First line monotherapy Improve lung function, dyspnea Reduce exacerbations Additive effect of combination therapy CV risk not clear
44 Pharmacologic Therapy Inhaled corticosteroids Not for monotherapy Indicated in more severe disease In combination with LABA Reduce frequency of exacerbations Improve lung function Risk of Pneumonia ICS/LABA vs LABA or LAMA monotherapy
45 Pharmacologic Therapy Methylxanthine Theophylline Bronchodilator effect Benefit vs Placebo in lung function, dyspnea scores Toxicity limits utility Phosphodiesterase 4 inhibitor Roflumilast Decrease inflammation, bronchodilator Reduce frequency of exacerbations in severe disease
46 Pharmacologic Therapy Macrolide antibiotics Erythromycin and Azithromycin Anti-inflammatory properties Reduce exacerbations? N Engl J Med 2011;365: Oral corticosteroids Not recommended for maintenance therapy Treat acute exacerbations
47 Pharmacologic Therapy by GOLD Stage A SABA or SA AC prn SABA + SA AC B LABA or LAMA LABA + LAMA SABA prn C ICS + LABA or LAMA ICS+LABA & LAMA Add PDE 4 inhibitor SABA prn D ICS+LABA & LAMA Add PDE 4 inhibitor Add macrolide SABA prn
48 Inhaled Medications by Class SABA Albuterol Levalbuterol SA AC Ipratropium Ipratropium/albuterol LABA Salmeterol Formoterol Indacaterol Arformoterol LAMA Tiotropium Aclidinium Umeclidium ICS + LABA Fluticasone/salmeterol Mometasone/formoterol Budesonide/formoterol LABA + LAMA Vilanterol/umeclidium
49 All the following statements regarding surgical management of COPD are true except? A. Lung volume reduction surgery (LVRS) improves lung function and quality of life B. LVRS improves survival in all COPD patients C. Lung transplantation (LT) has no mortality benefit compared to medical therapy in COPD D. LT improves quality of life and exercise capacity in COPD patients. The answer is B.
50 Surgical management LVRS Resect emphysematous segments Reduce hyperinflation Improve physiologic function Who benefits (NETT 2001,2003) No mortality benefit vs optimal medical therapy Improved FEV1, exercise capacity, quality of life Sub group analysis Increased mortality : homogeneous disease by CT (FEV1 < 20%, DLCO < 20%) Improved survival: Upper lobe predominant and low exercise capacity at baseline NETT Research Group. N Engl J Med 2001;345: & N Engl J Med 2003;348:
51 Surgical management Transplant No clear mortality benefit vs medical therapy Median survival =5 years Lower than most other solid organ transplant Improves QOL and functional capacity Criteria for referral BODE Index > 5 PH, Cor Pulmonale despite O2 therapy Progressive decline despite optimal therapy Acute hypercapnea (PaCO2 > 50) J Heart Lung Transpl 2010;29:
52 Follow up visits Smoking cessation Oxygen therapy Symptom control (MMRC, CAT) Exacerbation history Functional status (6min walk) PFT Annual (GOLD 2014) Radiograph Lung Cancer Screening Medication reconciliation Vaccination status Pulmonary rehabilitation
53 Acute Exacerbation: Change in respiratory symptoms beyond baseline leading to change in medications Defined by change in: Cough Dyspnea Sputum production Precipitants/Risk Viral or bacterial URI Smoke/pollutant exposure Comorbid disease exacerbation Medication noncompliance Prior exacerbation Impact Quality of life Physiologic decline Morbidity Mortality
54 Outpatient Management of Acute Exacerbation Goals of therapy Reduce symptoms/minimize impact Prevent future exacerbations Components of therapy Bronchodilators Short acting provide symptom relief Corticosteroids Recovery time, lung function, relapse rate, LOS Short vs long course 40mg prednisone x 5 days (GOLD 2014) Antibiotics Moderate to Severe Sputum purulence as marker of bacterial infection? H influenza, M catarrhalis, S pneumonia
55 Questions?
Prevention of Acute COPD exacerbations
 December 3, 2015 Prevention of Acute COPD exacerbations George Pyrgos MD 1 Disclosures No funding received for this presentation I have previously conducted clinical trials with Boehringer Ingelheim. Principal
December 3, 2015 Prevention of Acute COPD exacerbations George Pyrgos MD 1 Disclosures No funding received for this presentation I have previously conducted clinical trials with Boehringer Ingelheim. Principal
COPD and Asthma Differential Diagnosis
 COPD and Asthma Differential Diagnosis Chronic Obstructive Pulmonary Disease (COPD) is the third leading cause of death in America. Learning Objectives Use tools to effectively diagnose chronic obstructive
COPD and Asthma Differential Diagnosis Chronic Obstructive Pulmonary Disease (COPD) is the third leading cause of death in America. Learning Objectives Use tools to effectively diagnose chronic obstructive
Pathway for Diagnosing COPD
 Pathway for Diagnosing Visit 1 Registry Clients at Risk Patient presents with symptoms suggestive of Exertional breathlessness Chronic cough Regular sputum production Frequent bronchitis ; wheeze Occupational
Pathway for Diagnosing Visit 1 Registry Clients at Risk Patient presents with symptoms suggestive of Exertional breathlessness Chronic cough Regular sputum production Frequent bronchitis ; wheeze Occupational
RES/006/APR16/AR. Speaker : Dr. Pither Sandy Tulak SpP
 RES/006/APR16/AR Speaker : Dr. Pither Sandy Tulak SpP Definition of Asthma (GINA 2015) Asthma is a common and potentially serious chronic disease that imposes a substantial burden on patients, their families
RES/006/APR16/AR Speaker : Dr. Pither Sandy Tulak SpP Definition of Asthma (GINA 2015) Asthma is a common and potentially serious chronic disease that imposes a substantial burden on patients, their families
Bronchodilators in COPD
 TSANZSRS Gold Coast 2015 Can average outcomes in COPD clinical trials guide treatment strategies? Long live the FEV1? Christine McDonald Dept of Respiratory and Sleep Medicine Austin Health Institute for
TSANZSRS Gold Coast 2015 Can average outcomes in COPD clinical trials guide treatment strategies? Long live the FEV1? Christine McDonald Dept of Respiratory and Sleep Medicine Austin Health Institute for
PLAN OF ACTION FOR. Physician Name Signature License Date
 PLAN OF ACTION FOR Patient s copy (patient s name) I Feel Well Lignes I feel short directrices of breath: I cough up sputum daily. No Yes, colour: I cough regularly. No Yes I Feel Worse I have changes
PLAN OF ACTION FOR Patient s copy (patient s name) I Feel Well Lignes I feel short directrices of breath: I cough up sputum daily. No Yes, colour: I cough regularly. No Yes I Feel Worse I have changes
CLINICAL PATHWAY. Acute Medicine. Chronic Obstructive Pulmonary Disease
 CLINICAL PATHWAY Acute Medicine Chronic Obstructive Pulmonary Disease Chronic Obstructive Pulmonary Disease Table of Contents (tap to jump to page) INTRODUCTION 1 Scope of this Pathway 1 Pathway Contacts
CLINICAL PATHWAY Acute Medicine Chronic Obstructive Pulmonary Disease Chronic Obstructive Pulmonary Disease Table of Contents (tap to jump to page) INTRODUCTION 1 Scope of this Pathway 1 Pathway Contacts
Pulmonary Rehabilitation in Newark and Sherwood
 Pulmonary Rehabilitation in Newark and Sherwood With exception of smoking cessation pulmonary rehabilitation is the single most effective intervention for any patient with COPD. A Cochrane review published
Pulmonary Rehabilitation in Newark and Sherwood With exception of smoking cessation pulmonary rehabilitation is the single most effective intervention for any patient with COPD. A Cochrane review published
James F. Kravec, M.D., F.A.C.P
 James F. Kravec, M.D., F.A.C.P Chairman, Department of Internal Medicine, St. Elizabeth Health Center Chair, General Internal Medicine, Northeast Ohio Medical University Associate Medical Director, Hospice
James F. Kravec, M.D., F.A.C.P Chairman, Department of Internal Medicine, St. Elizabeth Health Center Chair, General Internal Medicine, Northeast Ohio Medical University Associate Medical Director, Hospice
COPD MANAGEMENT PROTOCOL STANFORD COORDINATED CARE
 I. PURPOSE To establish guidelines f the collabative management of patients with a diagnosis of chronic obstructive pulmonary disease (COPD) who are not adequately controlled and to define the roles and
I. PURPOSE To establish guidelines f the collabative management of patients with a diagnosis of chronic obstructive pulmonary disease (COPD) who are not adequately controlled and to define the roles and
Topic: New Treatment = Better Outcome?
 Session on COPD: Novel Concepts and Promising New Drugs Topic: New Treatment = Better Outcome? Through a CME Grant sponsored by New Treatment = Better Outcome? Tim S. Trinidad, MD Disclosure Present: COPD
Session on COPD: Novel Concepts and Promising New Drugs Topic: New Treatment = Better Outcome? Through a CME Grant sponsored by New Treatment = Better Outcome? Tim S. Trinidad, MD Disclosure Present: COPD
Understanding COPD. Carolinas Healthcare System
 Understanding COPD Carolinas Healthcare System 2013 This self-directed learning module contains information about the pathophysiology, diagnosis, and treatment of COPD. Target Audience: All RNs and LPNs
Understanding COPD Carolinas Healthcare System 2013 This self-directed learning module contains information about the pathophysiology, diagnosis, and treatment of COPD. Target Audience: All RNs and LPNs
Pulmonary Rehabilitation in Chronic Obstructive Pulmonary Disease (COPD)
") Pulmonary Rehabilitation in Chronic Obstructive Pulmonary Disease (COPD) Development of disability in COPD The decline in airway function may initially go unnoticed as people adapt their lives to avoid
Pulmonary Rehabilitation in Chronic Obstructive Pulmonary Disease (COPD) Development of disability in COPD The decline in airway function may initially go unnoticed as people adapt their lives to avoid
COPD Prescribing Guidelines
 South Staffordshire Area Prescribing Group COPD Prescribing Guidelines Inhaler choices in this guideline are different from previous versions produced by the APG. It is not expected patients controlled
South Staffordshire Area Prescribing Group COPD Prescribing Guidelines Inhaler choices in this guideline are different from previous versions produced by the APG. It is not expected patients controlled
Pulmonary Diseases. Lung Disease: Pathophysiology, Medical and Exercise Programming. Overview of Pathophysiology
 Lung Disease: Pathophysiology, Medical and Exercise Programming Overview of Pathophysiology Ventilatory Impairments Increased airway resistance Reduced compliance Increased work of breathing Ventilatory
Lung Disease: Pathophysiology, Medical and Exercise Programming Overview of Pathophysiology Ventilatory Impairments Increased airway resistance Reduced compliance Increased work of breathing Ventilatory
Marilyn Borkgren-Okonek, APN, CCNS, RN, MS Suburban Lung Associates, S.C. Elk Grove Village, IL
 Marilyn Borkgren-Okonek, APN, CCNS, RN, MS Suburban Lung Associates, S.C. Elk Grove Village, IL www.goldcopd.com GLOBAL INITIATIVE FOR CHRONIC OBSTRUCTIVE LUNG DISEASE GLOBAL STRATEGY FOR DIAGNOSIS, MANAGEMENT
Marilyn Borkgren-Okonek, APN, CCNS, RN, MS Suburban Lung Associates, S.C. Elk Grove Village, IL www.goldcopd.com GLOBAL INITIATIVE FOR CHRONIC OBSTRUCTIVE LUNG DISEASE GLOBAL STRATEGY FOR DIAGNOSIS, MANAGEMENT
Management of exacerbations in chronic obstructive pulmonary disease in Primary Care
 Management of exacerbations in chronic obstructive pulmonary disease in Primary Care Acute exacerbations of chronic obstructive pulmonary disease (COPD) are associated with significant morbidity and mortality.
Management of exacerbations in chronic obstructive pulmonary disease in Primary Care Acute exacerbations of chronic obstructive pulmonary disease (COPD) are associated with significant morbidity and mortality.
AECOPD: Management and Prevention
 AECOPD: Management and Prevention Neil MacIntyre MD Duke University Medical Center Durham NC AECOPD: Management and Prevention AECOPD: Definitions and impact Acute management of AECOPD Preventing AECOPD.
AECOPD: Management and Prevention Neil MacIntyre MD Duke University Medical Center Durham NC AECOPD: Management and Prevention AECOPD: Definitions and impact Acute management of AECOPD Preventing AECOPD.
Department of Surgery
 What is emphysema? 2004 Regents of the University of Michigan Emphysema is a chronic disease of the lungs characterized by thinning and overexpansion of the lung-like blisters (bullae) in the lung tissue.
What is emphysema? 2004 Regents of the University of Michigan Emphysema is a chronic disease of the lungs characterized by thinning and overexpansion of the lung-like blisters (bullae) in the lung tissue.
Acute Care of COPD: Gaps in our knowledge. Robert A. Wise, M.D. May 20, 2010
 Acute Care of COPD: Gaps in our knowledge Robert A. Wise, M.D. May 20, 2010 Outline of talk Importance of COPD exacerbations Current treatments Areas for improvement Significant knowledge gaps Strategies
Acute Care of COPD: Gaps in our knowledge Robert A. Wise, M.D. May 20, 2010 Outline of talk Importance of COPD exacerbations Current treatments Areas for improvement Significant knowledge gaps Strategies
COPD PROTOCOL CELLO. Leiden
 COPD PROTOCOL CELLO Leiden May 2011 1 Introduction This protocol includes an explanation of the clinical picture, diagnosis, objectives and medication of COPD. The Cello way of working can be viewed on
COPD PROTOCOL CELLO Leiden May 2011 1 Introduction This protocol includes an explanation of the clinical picture, diagnosis, objectives and medication of COPD. The Cello way of working can be viewed on
Rehabilitation and Lung Cancer Resection. Roberto Benzo MD MS Mindful Breathing Laboratory Division of Pulmonary & CCM Mayo Clinic
 Rehabilitation and Lung Cancer Resection Roberto Benzo MD MS Mindful Breathing Laboratory Division of Pulmonary & CCM Mayo Clinic Disclosure Funded by the National Cancer Institute NIH for Preoperative
Rehabilitation and Lung Cancer Resection Roberto Benzo MD MS Mindful Breathing Laboratory Division of Pulmonary & CCM Mayo Clinic Disclosure Funded by the National Cancer Institute NIH for Preoperative
NICE Pathways bring together all NICE guidance, quality standards and other NICE information on a specific topic.
 bring together all NICE guidance, quality standards and other NICE information on a specific topic. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published.
bring together all NICE guidance, quality standards and other NICE information on a specific topic. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published.
Global Initiative for Chronic Obstructive Lung Disease
 Global Initiative for Chronic Obstructive Lung Disease POCKET GUIDE TO COPD DIAGNOSIS, MANAGEMENT, AND PREVENTION A Guide for Health Care Professionals REVISED 2011 Global Initiative for Chronic Obstructive
Global Initiative for Chronic Obstructive Lung Disease POCKET GUIDE TO COPD DIAGNOSIS, MANAGEMENT, AND PREVENTION A Guide for Health Care Professionals REVISED 2011 Global Initiative for Chronic Obstructive
Chronic obstructive pulmonary disease (COPD)
") Chronic obstructive pulmonary disease (COPD) Chronic obstructive pulmonary disease (COPD) is the name for a group of lung diseases including chronic bronchitis, emphysema and chronic obstructive airways
Chronic obstructive pulmonary disease (COPD) Chronic obstructive pulmonary disease (COPD) is the name for a group of lung diseases including chronic bronchitis, emphysema and chronic obstructive airways
Sponsor Novartis Pharmaceuticals
 Clinical Trial Results Database Page 1 Sponsor Novartis Pharmaceuticals Generic Drug Name Indacaterol Therapeutic Area of Trial Chronic Obstructive Pulmonary Disease (COPD) Indication studied: COPD Study
Clinical Trial Results Database Page 1 Sponsor Novartis Pharmaceuticals Generic Drug Name Indacaterol Therapeutic Area of Trial Chronic Obstructive Pulmonary Disease (COPD) Indication studied: COPD Study
30 DAY COPD READMISSIONS AND PULMONARY REHAB
 30 DAY COPD READMISSIONS AND PULMONARY REHAB Trina M. Limberg, Bs, RRT, FAARC, MAACVPR Director, Preventative Pulmonary and Rehabilitation Services UC San Diego Health System OVERVIEW The Impact of COPD
30 DAY COPD READMISSIONS AND PULMONARY REHAB Trina M. Limberg, Bs, RRT, FAARC, MAACVPR Director, Preventative Pulmonary and Rehabilitation Services UC San Diego Health System OVERVIEW The Impact of COPD
National Learning Objectives for COPD Educators
 National Learning Objectives for COPD Educators National Learning Objectives for COPD Educators The COPD Educator will be able to achieve the following objectives. Performance objectives, denoted by the
National Learning Objectives for COPD Educators National Learning Objectives for COPD Educators The COPD Educator will be able to achieve the following objectives. Performance objectives, denoted by the
Classifying Asthma Severity and Initiating Treatment in Children 0 4 Years of Age
 Classifying Asthma Severity and Initiating Treatment in Children 0 4 Years of Age Components of Severity Symptoms Intermittent 2 days/week Classification of Asthma Severity (0 4 years of age) Persistent
Classifying Asthma Severity and Initiating Treatment in Children 0 4 Years of Age Components of Severity Symptoms Intermittent 2 days/week Classification of Asthma Severity (0 4 years of age) Persistent
IN-HOME QUALITY IMPROVEMENT. BEST PRACTICE: DISEASE MANAGEMENT Chronic Obstructive Pulmonary Disease NURSE TRACK
 IN-HOME QUALITY IMPROVEMENT BEST PRACTICE: DISEASE MANAGEMENT Chronic Obstructive Pulmonary Disease NURSE TRACK Best Practice Intervention Packages were designed for use by any In-Home Provider Agency
IN-HOME QUALITY IMPROVEMENT BEST PRACTICE: DISEASE MANAGEMENT Chronic Obstructive Pulmonary Disease NURSE TRACK Best Practice Intervention Packages were designed for use by any In-Home Provider Agency
Drug therapy SHORT-ACTING BETA AGONISTS SHORT-ACTING ANTICHOLINERGICS LONG-ACTING BETA AGONISTS LONG-ACTING ANTICHOLINERGICS
 Drug therapy 6 6.1 What is the role of bronchodilators in COPD? 52 SHORT-ACTING BETA AGONISTS 6.2 How do short-acting beta agonists work? 52 6.3 What are the indications for their use? 52 6.4 What is the
Drug therapy 6 6.1 What is the role of bronchodilators in COPD? 52 SHORT-ACTING BETA AGONISTS 6.2 How do short-acting beta agonists work? 52 6.3 What are the indications for their use? 52 6.4 What is the
Irish Association for Emergency Medicine (IAEM) submission to the National COPD Strategy
 submission to the National COPD Strategy") 31 st Irish Association for Emergency Medicine (IAEM) submission to the National COPD Strategy 1 Introduction Chronic obstructive pulmonary disease (COPD) is an important disease for patients, the health
31 st Irish Association for Emergency Medicine (IAEM) submission to the National COPD Strategy 1 Introduction Chronic obstructive pulmonary disease (COPD) is an important disease for patients, the health
Tests. Pulmonary Functions
 Pulmonary Functions Tests Static lung functions volumes Dynamic lung functions volume and velocity Dynamic Tests Velocity dependent on Airway resistance Resistance of lung tissue to change in shape Dynamic
Pulmonary Functions Tests Static lung functions volumes Dynamic lung functions volume and velocity Dynamic Tests Velocity dependent on Airway resistance Resistance of lung tissue to change in shape Dynamic
Before prescribing for COPD management, the patient should have had appropriate assessment, including spirometry, as per NICE guidelines.
 Formulary Guidance for Management of COPD patients Before prescribing for COPD management, the patient should have had appropriate assessment, including spirometry, as per NICE guidelines. For inhaler
Formulary Guidance for Management of COPD patients Before prescribing for COPD management, the patient should have had appropriate assessment, including spirometry, as per NICE guidelines. For inhaler
Pre-Operative Services Teaching Rounds 2 Jan 2011
 Pre-Operative Services Teaching Rounds 2 Jan 2011 Deborah Richman MBChB FFA(SA) Director Pre-Operative Services Department of Anesthesia Stony Brook University Medical Center, NY drichman@notes.cc.sunysb.edu
Pre-Operative Services Teaching Rounds 2 Jan 2011 Deborah Richman MBChB FFA(SA) Director Pre-Operative Services Department of Anesthesia Stony Brook University Medical Center, NY drichman@notes.cc.sunysb.edu
Chronic Obstructive Pulmonary Disease
 COPD Guideline Team Team Leader Davoren A Chick, MD General Medicine Team Members Paul J Grant, MD General Medicine Meilan K Han, MD, MS Pulmonary Medicine R Van Harrison, PhD Medical Education Elisa B
COPD Guideline Team Team Leader Davoren A Chick, MD General Medicine Team Members Paul J Grant, MD General Medicine Meilan K Han, MD, MS Pulmonary Medicine R Van Harrison, PhD Medical Education Elisa B
An Overview of Asthma - Diagnosis and Treatment
 An Overview of Asthma - Diagnosis and Treatment Asthma is a common chronic disorder of the airways that is complex and characterized by variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness,
An Overview of Asthma - Diagnosis and Treatment Asthma is a common chronic disorder of the airways that is complex and characterized by variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness,
Clinical Guideline. Recommendation 3: For stable COPD patients with respiratory symptoms
 Clinical Guideline Diagnosis and Management of Stable Chronic Obstructive Pulmonary Disease: A Clinical Practice Guideline Update from the American College of Physicians, American College of Chest Physicians,
Clinical Guideline Diagnosis and Management of Stable Chronic Obstructive Pulmonary Disease: A Clinical Practice Guideline Update from the American College of Physicians, American College of Chest Physicians,
Outcome of Drug Counseling of Outpatients in Chronic Obstructive Pulmonary Disease Clinic at Thawangpha Hospital
 Mahidol University Journal of Pharmaceutical Sciences 008; 35(14): 81. Original Article Outcome of Drug Counseling of Outpatients in Chronic Obstructive Pulmonary Disease Clinic at Thawangpha Hospital
Mahidol University Journal of Pharmaceutical Sciences 008; 35(14): 81. Original Article Outcome of Drug Counseling of Outpatients in Chronic Obstructive Pulmonary Disease Clinic at Thawangpha Hospital
Clinical Guideline. Recommendation 3: For stable COPD patients with respiratory symptoms
 Clinical Guideline Diagnosis and Management of Stable Chronic Obstructive Pulmonary Disease: A Clinical Practice Guideline Update from the American College of Physicians, American College of Chest Physicians,
Clinical Guideline Diagnosis and Management of Stable Chronic Obstructive Pulmonary Disease: A Clinical Practice Guideline Update from the American College of Physicians, American College of Chest Physicians,
Global Strategy for the Diagnosis, Management and Prevention of Chronic Obstructive Pulmonary Disease
 Page 1 of 67 AJRCCM Articles in Press. Published on August 9, 2012 as doi:10.1164/rccm.201204-0596pp GOLD Executive Summary Global Strategy for the Diagnosis, Management and Prevention of Chronic Obstructive
Page 1 of 67 AJRCCM Articles in Press. Published on August 9, 2012 as doi:10.1164/rccm.201204-0596pp GOLD Executive Summary Global Strategy for the Diagnosis, Management and Prevention of Chronic Obstructive
Pharmacology of the Respiratory Tract: COPD and Steroids
 Pharmacology of the Respiratory Tract: COPD and Steroids Dr. Tillie-Louise Hackett Department of Anesthesiology, Pharmacology and Therapeutics University of British Columbia Associate Head, Centre of Heart
Pharmacology of the Respiratory Tract: COPD and Steroids Dr. Tillie-Louise Hackett Department of Anesthesiology, Pharmacology and Therapeutics University of British Columbia Associate Head, Centre of Heart
GEORGIA MEDICAID FEE-FOR-SERVICE ASTHMA and COPD AGENTS PA SUMMARY
 GEORGIA MEDICAID FEE-FOR-SERVICE ASTHMA and COPD AGENTS PA SUMMARY Preferred Anticholinergics and Combinations Atrovent HFA (ipratropium) Combivent Respimat (ipratropium/albuterol) Ipratropium neb inhalation
GEORGIA MEDICAID FEE-FOR-SERVICE ASTHMA and COPD AGENTS PA SUMMARY Preferred Anticholinergics and Combinations Atrovent HFA (ipratropium) Combivent Respimat (ipratropium/albuterol) Ipratropium neb inhalation
Managing dyspnea in patients with advanced chronic obstructive pulmonary disease. A Canadian Thoracic Society clinical practice guideline (2011)
") Managing dyspnea in patients with advanced chronic obstructive pulmonary disease A Canadian Thoracic Society clinical practice guideline (2011) 2011 Canadian Thoracic Society and its licensors All rights
Managing dyspnea in patients with advanced chronic obstructive pulmonary disease A Canadian Thoracic Society clinical practice guideline (2011) 2011 Canadian Thoracic Society and its licensors All rights
Documenting & Coding. Chronic Obstructive Pulmonary Disease (COPD) Presented by: David S. Brigner, MLA, CPC
 Presented by: David S. Brigner, MLA, CPC") Documenting & Coding Chronic Obstructive Pulmonary Disease (COPD) Presented by: David S. Brigner, MLA, CPC Sr. Provider Training & Development Consultant Professional Profile David Brigner currently performs
Documenting & Coding Chronic Obstructive Pulmonary Disease (COPD) Presented by: David S. Brigner, MLA, CPC Sr. Provider Training & Development Consultant Professional Profile David Brigner currently performs
David J. Lederer, MD, MS
 COPD: Definition Chronic Obstructive Pulmonary Disease Chronic airflow obstruction due to chronic bronchitis and/or pulmonary emphysema David J. Lederer, MD, MS Associate Medical Director, Lung Transplant
COPD: Definition Chronic Obstructive Pulmonary Disease Chronic airflow obstruction due to chronic bronchitis and/or pulmonary emphysema David J. Lederer, MD, MS Associate Medical Director, Lung Transplant
Breathing Easier In Tennessee: Employers Mitigate Health and Economic Costs of Chronic Obstructive Pulmonary Disease
 Breathing Easier In Tennessee: Employers Mitigate Health and Economic Costs of Chronic Obstructive Pulmonary Disease By John W. Walsh, Co-Founder and President of the COPD Foundation Breathing Easier In
Breathing Easier In Tennessee: Employers Mitigate Health and Economic Costs of Chronic Obstructive Pulmonary Disease By John W. Walsh, Co-Founder and President of the COPD Foundation Breathing Easier In
Pulmonary Rehabilitation: more than just an exercise prescription
 Pulmonary Rehabilitation: more than just an exercise prescription Robert Stalbow, RRT, RCP Pulmonary Rehabilitation Therapist Oregon Heart & Vascular Institute Objectives To describe the role of pulmonary
Pulmonary Rehabilitation: more than just an exercise prescription Robert Stalbow, RRT, RCP Pulmonary Rehabilitation Therapist Oregon Heart & Vascular Institute Objectives To describe the role of pulmonary
Clinical guideline Published: 23 June 2010 nice.org.uk/guidance/cg101
 Chronic obstructive pulmonary disease in over 16s: diagnosis and management Clinical guideline Published: 23 June 2010 nice.org.uk/guidance/cg101 NICE 2010. All rights reserved. Your responsibility The
Chronic obstructive pulmonary disease in over 16s: diagnosis and management Clinical guideline Published: 23 June 2010 nice.org.uk/guidance/cg101 NICE 2010. All rights reserved. Your responsibility The
This clinical study synopsis is provided in line with Boehringer Ingelheim s Policy on Transparency and Publication of Clinical Study Data.
 abcd Clinical Study for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the clinical
abcd Clinical Study for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the clinical
J of Evolution of Med and Dent Sci/ eissn- 2278-4802, pissn- 2278-4748/ Vol. 3/ Issue 65/Nov 27, 2014 Page 13575
 EFFECT OF BREATHING EXERCISES ON BIOPHYSIOLOGICAL PARAMETERS AND QUALITY OF LIFE OF PATIENTS WITH COPD AT A TERTIARY CARE CENTRE Sudin Koshy 1, Rugma Pillai S 2 HOW TO CITE THIS ARTICLE: Sudin Koshy, Rugma
EFFECT OF BREATHING EXERCISES ON BIOPHYSIOLOGICAL PARAMETERS AND QUALITY OF LIFE OF PATIENTS WITH COPD AT A TERTIARY CARE CENTRE Sudin Koshy 1, Rugma Pillai S 2 HOW TO CITE THIS ARTICLE: Sudin Koshy, Rugma
Medications for Managing COPD in Hospice Patients. Jim Joyner, PharmD, CGP Director of Clinical Operations Outcome Resources
 Medications for Managing COPD in Hospice Patients Jim Joyner, PharmD, CGP Director of Clinical Operations Outcome Resources Goal of medications in COPD Decrease symptoms and/or complications Reduce frequency
Medications for Managing COPD in Hospice Patients Jim Joyner, PharmD, CGP Director of Clinical Operations Outcome Resources Goal of medications in COPD Decrease symptoms and/or complications Reduce frequency
Lothian Guideline for Domiciliary Oxygen Therapy Service for COPD
 Lothian Guideline for Domiciliary Oxygen Therapy Service for COPD This document describes the standard for clinical assessment, prescription, optimal management and follow-up of patients receiving domiciliary
Lothian Guideline for Domiciliary Oxygen Therapy Service for COPD This document describes the standard for clinical assessment, prescription, optimal management and follow-up of patients receiving domiciliary
Waterloo Wellington Rehabilitative Care System Integrated Care Pathway for COPD Stream of Care (short version)
") Waterloo Wellington Rehabilitative Care System Integrated Care Pathway for COPD Stream of Care (short version) Care Setting ACUTE Activity Confirmation of COPD diagnoses: If time and the patient s condition
Waterloo Wellington Rehabilitative Care System Integrated Care Pathway for COPD Stream of Care (short version) Care Setting ACUTE Activity Confirmation of COPD diagnoses: If time and the patient s condition
The patient s response to therapy within the first hour in the Emergency Room is one of the most reliable ways to predict need for hospitalization.
 Emergency Room Asthma Management Algorithm The Emergency Room Asthma Management Algorithm is to be used for any patient seen in the Emergency Room with the diagnosis of asthma. (The initial history should
Emergency Room Asthma Management Algorithm The Emergency Room Asthma Management Algorithm is to be used for any patient seen in the Emergency Room with the diagnosis of asthma. (The initial history should
Asthma. Micah Long, MD
 Asthma Micah Long, MD Goals Define the two components of asthma. Describe the method of action and uses for: Steroids (inhaled and IV) Quick Beta Agonists (Nebs and MDIs) The "Others" Magnesium, Epi IM,
Asthma Micah Long, MD Goals Define the two components of asthma. Describe the method of action and uses for: Steroids (inhaled and IV) Quick Beta Agonists (Nebs and MDIs) The "Others" Magnesium, Epi IM,
Reducing COPD Readmissions and Implications for Pulmonary Rehab. Janie Knipper, APN, MA, AE-C, FAACVPR jane-knipper@uiowa.edu
 Reducing COPD Readmissions and Implications for Pulmonary Rehab Janie Knipper, APN, MA, AE-C, FAACVPR jane-knipper@uiowa.edu Statement of Disclosure I have no disclosures. The opinions expressed are my
Reducing COPD Readmissions and Implications for Pulmonary Rehab Janie Knipper, APN, MA, AE-C, FAACVPR jane-knipper@uiowa.edu Statement of Disclosure I have no disclosures. The opinions expressed are my
Pulmonary Disorders. Chronic Obstructive Pulmonary Disease (COPD) Chronic Obstructive Pulmonary Disease (COPD)
 Chronic Obstructive Pulmonary Disease (COPD)") RCS 6080 Medical and Psychosocial Aspects of Rehabilitation Counseling Pulmonary Disorders Chronic Obstructive Pulmonary Disease (COPD) Characterized by decreased expiratory airflow Reduction in expiratory
RCS 6080 Medical and Psychosocial Aspects of Rehabilitation Counseling Pulmonary Disorders Chronic Obstructive Pulmonary Disease (COPD) Characterized by decreased expiratory airflow Reduction in expiratory
Exploring the Chronic Obstructive Pulmonary Disease (COPD) Clinical Pathway. Health Quality Ontario s integrated episode of care for COPD
 Clinical Pathway. Health Quality Ontario s integrated episode of care for COPD") Exploring the Chronic Obstructive Pulmonary Disease (COPD) Clinical Pathway Health Quality Ontario s integrated episode of care for COPD Dr. Charlie Chan Health Quality Ontario Expert Panel Co-Chair May/June
Exploring the Chronic Obstructive Pulmonary Disease (COPD) Clinical Pathway Health Quality Ontario s integrated episode of care for COPD Dr. Charlie Chan Health Quality Ontario Expert Panel Co-Chair May/June
Interpretation of Pulmonary Function Tests
 Interpretation of Pulmonary Function Tests Dr. Sally Osborne Cellular & Physiological Sciences University of British Columbia Room 3602, D.H Copp building 604 822-3421 sally.osborne@ubc.ca www.sallyosborne.com
Interpretation of Pulmonary Function Tests Dr. Sally Osborne Cellular & Physiological Sciences University of British Columbia Room 3602, D.H Copp building 604 822-3421 sally.osborne@ubc.ca www.sallyosborne.com
DRUG UTILISATION STUDY IN BRONCHIAL ASTHMA IN A TERTIARY CARE HOSPITAL
 International Journal of Pharmaceutical Applications ISSN 0976-2639, Online ISSN 2278 6023 Vol 3, Issue 2, 2012, pp 297-305 http://www.bipublication.com DRUG UTILISATION STUDY IN BRONCHIAL ASTHMA IN A
International Journal of Pharmaceutical Applications ISSN 0976-2639, Online ISSN 2278 6023 Vol 3, Issue 2, 2012, pp 297-305 http://www.bipublication.com DRUG UTILISATION STUDY IN BRONCHIAL ASTHMA IN A
3/11/15. COPD Disease Management Tackling the Transition. Objectives. Describe the multidisciplinary approach to inpatient care for COPD patients
 Faculty Disclosures COPD Disease Management Tackling the Transition Dr. Cappelluti has no actual or potential conflicts of interest associated with this presentation. Jane Reardon has no actual or potential
Faculty Disclosures COPD Disease Management Tackling the Transition Dr. Cappelluti has no actual or potential conflicts of interest associated with this presentation. Jane Reardon has no actual or potential
COPD - Education for Patients and Carers Integrated Care Pathway
 Patient NHS COPD - Education for Patients and Carers Integrated Care Pathway Date ICP completed:. Is the patient following another Integrated Care Pathway[s].. / If yes, record which other Integrated Care
Patient NHS COPD - Education for Patients and Carers Integrated Care Pathway Date ICP completed:. Is the patient following another Integrated Care Pathway[s].. / If yes, record which other Integrated Care
Pulmonary Rehabilitation. Steve Crogan RRT Pulmonary Rehabilitation, University of Washington Medical Center Seattle, Washington 10/13/07
 Pulmonary Rehabilitation Steve Crogan RRT Pulmonary Rehabilitation, University of Washington Medical Seattle, Washington 10/13/07 Pulmonary Rehabilitation Created in the 1970 s Initially intended for COPD
Pulmonary Rehabilitation Steve Crogan RRT Pulmonary Rehabilitation, University of Washington Medical Seattle, Washington 10/13/07 Pulmonary Rehabilitation Created in the 1970 s Initially intended for COPD
COPD RESOURCE PACK SECTION 11. Fife Integrated COPD Care Pathways
 COPD RESOURCE PCK SECTION 11 Fife Integrated COPD Care Pathways In this section: 1. COPD Guidance treatment at each stage of the disease 2. Overview of Respiratory (COPD) Integrated Pathway 3. Chronic
COPD RESOURCE PCK SECTION 11 Fife Integrated COPD Care Pathways In this section: 1. COPD Guidance treatment at each stage of the disease 2. Overview of Respiratory (COPD) Integrated Pathway 3. Chronic
Co-morbiditeit associeert met respiratoire aandoeningen louter omwille van de leeftijd. COPD patiënten hebben veel meer kans op longkanker dan rokers
 Academisch centrum huisartsgeneeskunde Pneumologie Juni 2012 Prof W Janssens Co-morbiditeit associeert met respiratoire aandoeningen louter omwille van de leeftijd. COPD patiënten hebben veel meer kans
Academisch centrum huisartsgeneeskunde Pneumologie Juni 2012 Prof W Janssens Co-morbiditeit associeert met respiratoire aandoeningen louter omwille van de leeftijd. COPD patiënten hebben veel meer kans
COPD Intervention. Components:
 COPD Intervention 1. Primary disease education Member will have an increased understanding of chronic obstructive pulmonary disease, the causes, risks and complications. Explain COPD Explain how COPD is
COPD Intervention 1. Primary disease education Member will have an increased understanding of chronic obstructive pulmonary disease, the causes, risks and complications. Explain COPD Explain how COPD is
Asthma Intervention. An Independent Licensee of the Blue Cross and Blue Shield Association.
 Asthma Intervention 1. Primary disease education Member will have an increased understanding of asthma and the classification by severity, the risks and the complications. Define asthma Explain how lungs
Asthma Intervention 1. Primary disease education Member will have an increased understanding of asthma and the classification by severity, the risks and the complications. Define asthma Explain how lungs
Insights for Improvement: Advancing COPD Care Through Quality Measurement. An NCQA Insights for Improvement Publication
 2009 Insights for Improvement: Advancing COPD Care Through Quality Measurement An NCQA Insights for Improvement Publication Chronic obstructive pulmonary disease (COPD) includes chronic bronchitis, emphysema,
2009 Insights for Improvement: Advancing COPD Care Through Quality Measurement An NCQA Insights for Improvement Publication Chronic obstructive pulmonary disease (COPD) includes chronic bronchitis, emphysema,
Prof. Florian Gantner. Vice President Respiratory Diseases Research Boehringer Ingelheim
 Prof. Florian Gantner Vice President Respiratory Diseases Research Boehringer Ingelheim Research and Development in Practice: COPD Chronic Obstructive Pulmonary Disease (COPD) Facts Main cause of COPD
Prof. Florian Gantner Vice President Respiratory Diseases Research Boehringer Ingelheim Research and Development in Practice: COPD Chronic Obstructive Pulmonary Disease (COPD) Facts Main cause of COPD
Southwark Clinical Commissioning Group Lambeth Clinical Commissioning Group
 Getting the Vision Right: A multi-disciplinary approach to providing integrated care for respiratory patients Dr Noel Baxter, GP NHS Southwark CCG Dr Irem Patel, Integrated Consultant Respiratory Physician
Getting the Vision Right: A multi-disciplinary approach to providing integrated care for respiratory patients Dr Noel Baxter, GP NHS Southwark CCG Dr Irem Patel, Integrated Consultant Respiratory Physician
written by Harvard Medical School COPD It Can Take Your Breath Away www.patientedu.org/copd
 written by Harvard Medical School COPD It Can Take Your Breath Away www.patientedu.org/copd What Is COPD? COPD stands for chronic obstructive pulmonary disease. There are two major diseases included in
written by Harvard Medical School COPD It Can Take Your Breath Away www.patientedu.org/copd What Is COPD? COPD stands for chronic obstructive pulmonary disease. There are two major diseases included in
COPD. What is COPD? How many people have COPD in Canada? Who gets COPD?
 What is COPD? COPD stands for Chronic Obstructive Pulmonary Disease. It is a long-term lung disease that makes it difficult for air to move into and out of the lungs. COPD is used to describe a few lung
What is COPD? COPD stands for Chronic Obstructive Pulmonary Disease. It is a long-term lung disease that makes it difficult for air to move into and out of the lungs. COPD is used to describe a few lung
Exploratory data: COPD and blood eosinophils. David Price: 9.23-9.35am
 Exploratory data: COPD and blood eosinophils David Price: 9.23-9.35am Blood Eosinophilia in COPD The reliability and utility of blood eosinophils as a marker of disease burden, healthcare resource utilisation
Exploratory data: COPD and blood eosinophils David Price: 9.23-9.35am Blood Eosinophilia in COPD The reliability and utility of blood eosinophils as a marker of disease burden, healthcare resource utilisation
Prevention of Acute Exacerbations of COPD American College of Chest Physicians and Canadian Thoracic Society Guideline
 [ Evidence-Based Medicine ] Prevention of Acute Exacerbations of COPD American College of Chest Physicians and Canadian Thoracic Society Guideline Gerard J. Criner, MD, FCCP ; Jean Bourbeau, MD, FCCP ;
[ Evidence-Based Medicine ] Prevention of Acute Exacerbations of COPD American College of Chest Physicians and Canadian Thoracic Society Guideline Gerard J. Criner, MD, FCCP ; Jean Bourbeau, MD, FCCP ;
Position Statement from the Irish Thoracic Society on the treatment of Idiopathic Pulmonary Fibrosis
 BACKGROUND Position Statement from the Irish Thoracic Society on the treatment of Idiopathic Pulmonary Fibrosis Idiopathic Pulmonary Fibrosis (IPF) is a rare, chronic and fatal disease characterised by
BACKGROUND Position Statement from the Irish Thoracic Society on the treatment of Idiopathic Pulmonary Fibrosis Idiopathic Pulmonary Fibrosis (IPF) is a rare, chronic and fatal disease characterised by
Compare the physiologic responses of the respiratory system to emphysema, chronic bronchitis, and asthma
 Chapter 31 Drugs Used to Treat Lower Respiratory Disease Learning Objectives Describe the physiology of respirations Compare the physiologic responses of the respiratory system to emphysema, chronic bronchitis,
Chapter 31 Drugs Used to Treat Lower Respiratory Disease Learning Objectives Describe the physiology of respirations Compare the physiologic responses of the respiratory system to emphysema, chronic bronchitis,
Objectives COPD. Chronic Obstructive Pulmonary Disease (COPD) 4/19/2011
 4/19/2011") Objectives Discuss assessment findings and treatment for: Chronic Obstructive Pulmonary Disease Bronchitis Emphysema Asthma Anaphylaxis Other respiratory issues Provide some definitions Chronic Obstructive
Objectives Discuss assessment findings and treatment for: Chronic Obstructive Pulmonary Disease Bronchitis Emphysema Asthma Anaphylaxis Other respiratory issues Provide some definitions Chronic Obstructive
Adult Home Oxygen Therapy. Purpose To provide guidance on the requirements for and procedures relating to domiciliary oxygen therapy.
 Contents Purpose... 1 Scope/Audience... 1 Categories for Home Oxygen Therapy... 2 Assessment for Home Oxygen Therapy... 3 Investigations... 3 Requests for home oxygen... 3 Provision of Home Oxygen... 4
Contents Purpose... 1 Scope/Audience... 1 Categories for Home Oxygen Therapy... 2 Assessment for Home Oxygen Therapy... 3 Investigations... 3 Requests for home oxygen... 3 Provision of Home Oxygen... 4
Original Article COPD and Hospital Stay Pak Armed Forces Med J 2014; 64 (1): 46-50. Ahmed Raza, Mahmood Iqbal Malik*, Yousaf Jamal**
: 46-50. Ahmed Raza, Mahmood Iqbal Malik*, Yousaf Jamal**") Original Article COPD and Hospital Stay Pak Armed Forces Med J 2014; 64 (1): 46-50 COMPARISON OF NIPPV WITH STANDARD TREATMENT IN PATIENTS WITH ACUTE EXACERBATIONS OF COPD IN TERMS OF IMPROVEMENT IN ABGS
Original Article COPD and Hospital Stay Pak Armed Forces Med J 2014; 64 (1): 46-50 COMPARISON OF NIPPV WITH STANDARD TREATMENT IN PATIENTS WITH ACUTE EXACERBATIONS OF COPD IN TERMS OF IMPROVEMENT IN ABGS
COPD. (Chronic Obstructive Pulmonary Disease) (Emphysema) (Chronic Bronchitis) Education For Our Community
 (Emphysema) (Chronic Bronchitis) Education For Our Community") COPD (Chronic Obstructive Pulmonary Disease) (Emphysema) (Chronic Bronchitis) Education For Our Community Chronic Obstructive Pulmonary Disease (COPD) Definition Chronic obstructive pulmonary disease (COPD)
COPD (Chronic Obstructive Pulmonary Disease) (Emphysema) (Chronic Bronchitis) Education For Our Community Chronic Obstructive Pulmonary Disease (COPD) Definition Chronic obstructive pulmonary disease (COPD)
Chronic obstructive pulmonary disease: Management of adults with chronic obstructive pulmonary disease in primary and secondary care
 Chronic obstructive pulmonary disease: Management of adults with chronic obstructive pulmonary disease in primary and secondary care NICE guideline First draft for consultation, September 2003 If you wish
Chronic obstructive pulmonary disease: Management of adults with chronic obstructive pulmonary disease in primary and secondary care NICE guideline First draft for consultation, September 2003 If you wish
Stanley J. Szefler, MD National Jewish Medical and Research Center
 New Asthma Guidelines: Special Attention to Infant Wheezers Stanley J. Szefler, MD Helen Wohlberg & Herman Lambert Chair in Pharmacokinetics, & Professor of Pediatrics and Pharmacology, University of Colorado
New Asthma Guidelines: Special Attention to Infant Wheezers Stanley J. Szefler, MD Helen Wohlberg & Herman Lambert Chair in Pharmacokinetics, & Professor of Pediatrics and Pharmacology, University of Colorado
medicineupdate to find out more about this medicine
 medicineupdate Asking the right questions about new medicines Seretide for chronic obstructive pulmonary disease What this medicine is 1 What this medicine treats 2 Other medicines available for this condition
medicineupdate Asking the right questions about new medicines Seretide for chronic obstructive pulmonary disease What this medicine is 1 What this medicine treats 2 Other medicines available for this condition
These factors increase your chance of developing emphysema. Tell your doctor if you have any of these risk factors:
 Emphysema Pronounced: em-fiss-see-mah by Debra Wood, RN En Español (Spanish Version) Definition Emphysema is a chronic obstructive disease of the lungs. The lungs contain millions of tiny air sacs called
Emphysema Pronounced: em-fiss-see-mah by Debra Wood, RN En Español (Spanish Version) Definition Emphysema is a chronic obstructive disease of the lungs. The lungs contain millions of tiny air sacs called
Idiopathic Pulmonary Fibrosis
 Idiopathic Pulmonary Fibrosis What is Idiopathic Pulmonary Fibrosis? Idiopathic pulmonary fibrosis (IPF) is a condition that causes persistent and progressive scarring of the tiny air sacs (alveoli) in
Idiopathic Pulmonary Fibrosis What is Idiopathic Pulmonary Fibrosis? Idiopathic pulmonary fibrosis (IPF) is a condition that causes persistent and progressive scarring of the tiny air sacs (alveoli) in
Value of Homecare: COPD and Long-Term Oxygen Therapy. A White Paper
 Value of Homecare: COPD and Long-Term Oxygen Therapy A White Paper Chronic Obstructive Pulmonary Disease (COPD) is the 4 th leading cause of death in the world and afflicts over 14 million Americans. The
Value of Homecare: COPD and Long-Term Oxygen Therapy A White Paper Chronic Obstructive Pulmonary Disease (COPD) is the 4 th leading cause of death in the world and afflicts over 14 million Americans. The
Medication and Devices for Chronic Obstructive Pulmonary Disease (COPD)
") Medication and Devices for Chronic Obstructive Pulmonary Disease (COPD) Patients with COPD take a wide variety of medicines to manage their symptoms these include: Inhaled Short Acting Bronchodilators
Medication and Devices for Chronic Obstructive Pulmonary Disease (COPD) Patients with COPD take a wide variety of medicines to manage their symptoms these include: Inhaled Short Acting Bronchodilators
understanding the professional guidelines
 SEVERE ASTHMA understanding the professional guidelines This guide includes information on what the European Respiratory Society (ERS) and the American Thoracic Society (ATS) have said about severe asthma.
SEVERE ASTHMA understanding the professional guidelines This guide includes information on what the European Respiratory Society (ERS) and the American Thoracic Society (ATS) have said about severe asthma.
Respiratory Care. A Life and Breath Career for You!
 Respiratory Care A Life and Breath Career for You! Respiratory Care Makes a Difference At 9:32 am, Lori Moreno brought a newborn baby struggling to breathe back to life What have you accomplished today?
Respiratory Care A Life and Breath Career for You! Respiratory Care Makes a Difference At 9:32 am, Lori Moreno brought a newborn baby struggling to breathe back to life What have you accomplished today?
How to use FENO-guided asthma control in routine clinical practice
 How to use FENO-guided asthma control in routine clinical practice Asthma is a chronic inflammatory disease of the airways. This has implications for the diagnosis, management and potential prevention
How to use FENO-guided asthma control in routine clinical practice Asthma is a chronic inflammatory disease of the airways. This has implications for the diagnosis, management and potential prevention
Breathe With Ease. Asthma Disease Management Program
 Breathe With Ease Asthma Disease Management Program MOLINA Breathe With Ease Pediatric and Adult Asthma Disease Management Program Background According to the National Asthma Education and Prevention Program
Breathe With Ease Asthma Disease Management Program MOLINA Breathe With Ease Pediatric and Adult Asthma Disease Management Program Background According to the National Asthma Education and Prevention Program
United Lung & Sleep Clinic Asbestos Questionnaire
 Date United Lung & Sleep Clinic Asbestos Questionnaire 1. Name,, Last First M.I. 2. Address 3. Home Phone: ( ) - Area Code,, City State Zip Code 4. Social Security # : - - 5. Birthdate: / / Month Day Year
Date United Lung & Sleep Clinic Asbestos Questionnaire 1. Name,, Last First M.I. 2. Address 3. Home Phone: ( ) - Area Code,, City State Zip Code 4. Social Security # : - - 5. Birthdate: / / Month Day Year
Chronic Obstructive Pulmonary Disease (COPD) Admission Order Set
 Admission Order Set") Patient Name: PHN: Page 1/1 Admit to Dr: Notified Consult: Dr: Family Dr: Precautions: Contact Droplet Enhanced Droplet Airborne - Reason: _ Code Status: Full Resuscitation or Consults: Reason: Dietician
Patient Name: PHN: Page 1/1 Admit to Dr: Notified Consult: Dr: Family Dr: Precautions: Contact Droplet Enhanced Droplet Airborne - Reason: _ Code Status: Full Resuscitation or Consults: Reason: Dietician
PCOM Letterhead [Substitute same from participating institution and, of course, change Department, PI, and Co-Investigators]
![PCOM Letterhead [Substitute same from participating institution and, of course, change Department, PI, and Co-Investigators]](/thumbs/26/2087522.jpg "PCOM Letterhead [Substitute same from participating institution and, of course, change Department, PI, and Co-Investigators]") PCOM Letterhead [Substitute same from participating institution and, of course, change Department, PI, and Co-Investigators] Department of Neuroscience, Physiology and Pharmacology 215-871-6880 PATIENT
PCOM Letterhead [Substitute same from participating institution and, of course, change Department, PI, and Co-Investigators] Department of Neuroscience, Physiology and Pharmacology 215-871-6880 PATIENT
Diagnosis and Treatment
 Sleep Apnea: Diagnosis and Treatment Sleep Apnea Sleep Apnea is Common Dangerous Easily recognized Treatable Types of Sleep Disordered Breathing Apnea Cessation of airflow > 10 seconds Hypopnea Decreased
Sleep Apnea: Diagnosis and Treatment Sleep Apnea Sleep Apnea is Common Dangerous Easily recognized Treatable Types of Sleep Disordered Breathing Apnea Cessation of airflow > 10 seconds Hypopnea Decreased
Better Breathing with COPD
 Better Breathing with COPD People with Chronic Obstructive Pulmonary Disease (COPD) often benefit from learning different breathing techniques. Pursed Lip Breathing Pursed Lip Breathing (PLB) can be very
Better Breathing with COPD People with Chronic Obstructive Pulmonary Disease (COPD) often benefit from learning different breathing techniques. Pursed Lip Breathing Pursed Lip Breathing (PLB) can be very
The. Treating patients with COPD with medications
 Treating patients with COPD with medications Gilbert E. D Alonzo Jr, MS, DO, FACOI; Fredric Jaffe, DO, FCCP; Samuel L. Krachman, DO SHUTTERSTOCK.COM The management treatment of chronic obstructive pulmonary
Treating patients with COPD with medications Gilbert E. D Alonzo Jr, MS, DO, FACOI; Fredric Jaffe, DO, FCCP; Samuel L. Krachman, DO SHUTTERSTOCK.COM The management treatment of chronic obstructive pulmonary
Objectives. Asthma Management
 Objectives Asthma Management BREATHE Conference Allergy and Asthma Specialists PC Christine Malloy MD March 22, 2013 Review the role of inflammation in asthma Discuss the components of the EPR-3 management
Objectives Asthma Management BREATHE Conference Allergy and Asthma Specialists PC Christine Malloy MD March 22, 2013 Review the role of inflammation in asthma Discuss the components of the EPR-3 management
Annotated from the NAEPP/NHLBI Updated Asthma Guidelines and Developed Through Expert Consensus
 Asthma Pocket Guide for Primary Care Annotated from the NAEPP/NHLBI Updated Asthma Guidelines and Developed Through Expert Consensus POSITION STATEMENT Despite advances in therapy, asthma remains a disease
Asthma Pocket Guide for Primary Care Annotated from the NAEPP/NHLBI Updated Asthma Guidelines and Developed Through Expert Consensus POSITION STATEMENT Despite advances in therapy, asthma remains a disease