Substance Use Disorders and ASAM Patient Placement Criteria
|
|
|
- Jocelyn Daniel
- 8 years ago
- Views:
Transcription
1 Substance Use Disorders and ASAM Patient Placement Criteria Rochelle Head-Dunham, MD, FAPA Medical Director/Chief of Adult Services DHH/Office for Behavioral Health

2 Objectives 1. Discuss defining criteria for Substance Use Disorders 2. Highlight General Principles of the Neurobiology of Addiction 3. Review the American Society of Addiction Medicine s (ASAM) Patient Placement Criteria

3 SUBSTANCE USE DISORDERS 4

4 Terminology Dual-disorders vs Co-occurring Disorders Use vs Misuse vs Abuse Tolerance vs Physiological Dependence Physiological Dependence vs Addiction Pseudo-addiction Assessment vs Patient Placement Criteria 5

5 General Principles & Considerations Heterogeneity of the addiction populations Diagnosing with expectation not exception Holistic evaluations and comprehensive treatment planning Unique person-centered and family focused treatment approaches are required to enhance outcomes Significant predictors of treatment success are continuous, empathic relationships and coordination of care 6

6 Axis I: Axis II: Diagnostic Statistical Manual (DSM) Multi-Axial System Clinical Disorders (Mental Illness and Addictive Disorders) Other Conditions That may be a Focus of Clinical Attention Personality Disorders; Developmental Disabilities Axis III: General Medical Conditions Axis IV: Psychosocial and Environmental Problems ( Stressors ) Axis V: Global Assessment of Functioning (GAF) 7
 Axis V: Global Assessment of")
7 8
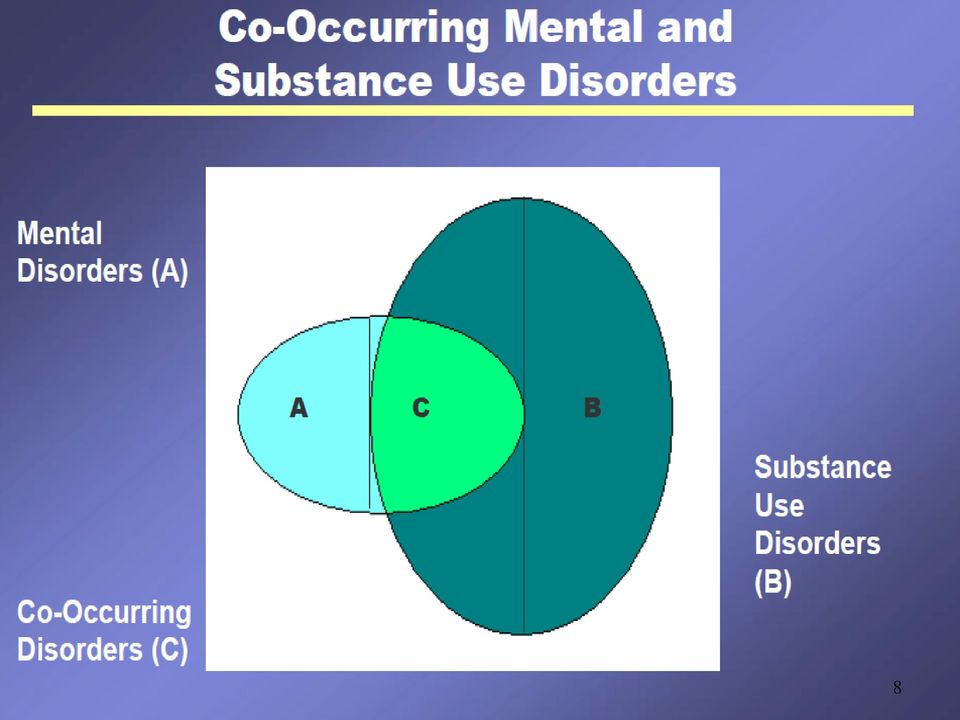
8 Interrelationship of Substance Use and Mental (Psychiatric) Disorders Psychiatric disorders and substance use disorders can evolve independently through different, unrelated processes Symptoms of psychiatric and substance use disorders can be expressed independently or simultaneously Both disorders can mimic or mask symptoms of the other, i.e., cocaine intoxication can mimic schizophrenic; depression can mimic cocaine induced mood disorder. A relapse of one disorder can precipitate acute symptoms of the other disorder. Psychiatric symptoms may emerge with cessation of alcohol/drug use (i.e., first break schizophrenic).
.")
9 Commonly Co-Occurring Mental Disorders (Axis I) 1. Mood Disorders are disorders that present with a disturbance in mood as a predominant feature; Major Depressive Disorders, Bipolar Disorders, substance Induced Mood Disorders, commonly co-occur with addictive disorders 2. Anxiety Disorders are disorders that present with anxiety (fear) as the predominant feature. Panic disorder, Social Anxiety Disorder, Generalized Anxiety Disorder, and Post-Traumatic Stress Disorder, commonly co-occur with addictive disorders. 3. Psychotic Disorders are disorders which typically present with psychosis or gross impairment in reality testing evidenced by delusional thinking, disorganized speech, or disorganized/ catatonic behavior. Schizophrenia, Schizoaffective disorder, and Delusional disorder, co-occur with addictive disorders. 10

10 Personality Disorders Co-occur with Substance Use (Axis II) A Personality Disorder is an enduring pattern of inner experience and behavior that deviates markedly from the expectations of the individual s culture, is pervasive and inflexible, has an onset in adolescence or early adulthood, is stable over time, and leads to distress or impairment, and is manifested in at least two of the following areas: Cognition, Affectivity, Interpersonal functioning or Impulse Control. DSM-IV TR

11 Medical Co-morbidity and Substance Use (Axis III) Inhalant use among year olds and depression are increasing; Patients in chemical dependency programs are 18 times more likely to have major psychosis, 15 times more likely to have depression and 9 times more likely to have an anxiety disorder; Substance use increases the risk for hypertension (x2), congestive heart failure (x9) and pneumonia (x12); HIV patients with a substance use disorder are more likely to be non-adherent; Medicaid patients with a substance use disorder are more likely to be readmitted to a hospital within 30 days; 12

12 Medical Co-morbidity and Substance Use (Axis III) Substance use creates increased rates of complications with hip replacements; Patients treated with medication for alcoholism had fewer detoxification, alcohol related inpatient days and emergency room visits; High cost Medicaid recipients with HIV had an average annual cost of $157,000, with 40% higher costs for treatment of co-morbid MH/SU disorders, the most common co-morbidities Treating patients with substance use related medical disorders in an integrated setting can achieve cost savings; 13

13 Definition of Substance Related Disorders Substance Related Disorders are disorders resulting from ingestion of a drug of abuse (including alcohol), along with the development of the side effects of a medication, or from toxin exposure. Substance can refer to a drug of abuse, a medication, or a toxin. Patterns of use have been researched for eleven substances: Alcohol, Amphetamine, Caffeine, Cannabis, Cocaine, Hallucinogens, Inhalants, Nicotine, Opioids, Phencyclidines and Sedative hypnotics/benzodiazepines.

14 Diagnoses Associated With Classes Of Substances Table 1. Diagnoses associated with class of substances Dependence Abuse Intoxication Withdrawal Intoxication Delirium Withdrawal Delirium Dementia Amnestic Disorder Psychotic Disorders Mood Disorders Anxiety Disorders Sexual Dysfunctions Sleep Disorders Alcohol x x x x I W P P I/W I/W I/W I I/W Amphetamines x x x x I I I/W I I I/W Caffeine x I I Cannabis x x x I I I Cocaine x x x x I I I/W I/W I I/W Hallucinogens x x x I I I I Inhalants x x x I P I I I Nicotine x x Opioids x x x x I I I I I/W Phencyclidine x x x I I I I Sedatives, hypnotics, or anxiolytics Polysubstance x x x x I W P P I/W I/W W I I/W x Other x x x x I W P P I/W I/W I/W I I/W *Also Hallucinogen Perception Disorder (Flashbacks). Note: X, I, W, I/W, or P indicates that the category is recognized in DSM-IV. In addition, I indicates that the specifier With Onset During Intoxication may be noted for the category (except for Intoxication Delirium); W indicates that the specifier With Onset During Withdrawal may be noted for the category (except for Withdrawal Delirium); and I/W indicates that either With Onset During Intoxication or With Onset During Withdrawal may be noted for the category. P indicates that the disorder is Persisting.

15 Diagnoses Associated With Classes Of Substances (Illustrated) Table 1. Diagnoses associated with class of substances Classes of Substances Dependence Abuse Intoxication Withdrawal Intoxication Delirium Withdrawal Delirium Dementia Amnestic Disorder Psychotic Disorders Mood Disorders Anxiety Disorders Sexual Dysfunctions Sleep Disorders Alcohol x x x x I W P P I/W I/W I/W I I/W Amphetamines x x x x I I I/W I I I/W I I x Caffeine Cannabis x x x I I I Cocaine x x x x I I I/W I/W I I/W Hallucinogens x x x I I I I Inhalants x x x I P I I I Nicotine x x Opioids x x x x I I I I I/W Phencyclidine x x x I I I I Sedatives, hypnotics, or anxiolytics x x x x I W P P I/W I/W W I I/W Polysubstance x Other x x x x I W P P I/W I/W I/W I I/W

16 Diagnostic Considerations DSM IV-TR The Diagnostic and Statistical Manual (DSM-IV) has established two broad categories for the distinction of Addictive Disorders: A. Use Disorders are those diagnostic states which name the substance of abuse and assign severity (i.e., alcohol abuse or dependence ) or acuity (cocaine intoxication or withdrawal). B. Induced Disorders are those diagnostic states which occur as a result of the psychological consequences of ingested chemicals (i.e.., cocaine induced psychosis, methamphetamine induced mood disorder ). 17
.")
17 Diagnostic Determinants Diagnostic determinants of Abuse versus Dependence, Withdrawal versus Intoxication are drug pharmacology and behavioral patterns/consequences of use Rationale for appropriate placement decisions must take into consideration, all of the above as determinants of severity and acuity.

18 Diagnostic Determinants Use Disorders Intoxication and Withdrawal

19 Diagnoses Associated With Classes Of Substances: Use Disorders (Illustrated) Table 1. Diagnoses associated with class of substances Dependence Abuse Intoxication USE DISORDERS Withdrawal Intoxication Delirium Withdrawal Delirium Dementia Amnestic Disorder Psychotic Disorders Mood Disorders Anxiety Disorders Sexual Dysfunctions Sleep Disorders Alcohol x x x x I W P P I/W I/W I/W I I/W Amphetamines x x x x I I I/W I I I/W I I x Caffeine Cannabis x x x I I I Cocaine x x x x I I I/W I/W I I/W Hallucinogens x x x I I I I Inhalants x x x I P I I I Nicotine x x Opioids x x x x I I I I I/W Phencyclidine x x x I I I I Sedatives, hypnotics, or anxiolytics x x x x I W P P I/W I/W W I I/W Polysubstance x Other x x x x I W P P I/W I/W I/W I I/W

20 Diagnoses Associated With Classes Of Substances: Diagnostic Possibilities (Illustrated)

21 Diagnoses Associated With Classes Of Substances: Diagnostic Possibilities (Illustrated) Table 1. Diagnoses associated with class of substances Dependence Abuse Intoxication Withdrawal Intoxication Delirium Withdrawal Delirium Dementia Amnestic Disorder Psychotic Disorders Mood Disorders Anxiety Disorders Sexual Dysfunctions Sleep Disorders Alcohol x x x x I W P P I/W I/W I/W I I/W Amphetamines x x x x I I I/W I I I/W I I x Caffeine Cannabis x x x I I I Cocaine x x x x I I I/W I/W I I/W Hallucinogens x x x I I I I Inhalants x x x I P I I I Nicotine x x Opioids x x x x I I I I I/W Phencyclidine x x x I I I I Sedatives, hypnotics, or anxiolytics x x x x I W P P I/W I/W W I I/W Polysubstance x Other x x x x I W P P I/W I/W I/W I I/W
22 Medication Options Induced Disorders
23 Medication Considerations Medications and Induced States Drugs and Alcohol induce a complex array of symptoms which are very similar to mental disorders in those who do not use drugs and alcohol. Use of psychotropic medications is therefore indicated to manage the psychiatric symptoms, independent of the cause for their expression. (Some cautions are necessary.) 24
24 Diagnoses Associated With Classes Of Substances: Induced Disorders (Illustrated) Table 1. Diagnoses associated with class of substances Dependence Abuse Intoxication Withdrawal Intoxication Delirium Withdrawal Delirium Dementia Amnestic Disorder Psychotic Disorders Mood Disorders INDUCED DISORDERS Anxiety Disorders Sexual Dysfunctions Sleep Disorders Alcohol x x x x I W P P I/W I/W I/W I I/W Amphetamines x x x x I I I/W I I I/W I I x Caffeine Cannabis x x x I I I Cocaine x x x x I I I/W I/W I I/W Hallucinogens x x x I I I I Inhalants x x x I P I I I Nicotine x x Opioids x x x x I I I I I/W Phencyclidine x x x I I I I Sedatives, hypnotics, or anxiolytics x x x x I W P P I/W I/W W I I/W Polysubstance x Other x x x x I W P P I/W I/W I/W I I/W
25 DSM V Eliminates the Multi-Axial System Axis I, II, and III (all diagnosis) are combined Axis IV Stressors are eliminated, replaced by ICD-9-CM V codes ICD-10-CM Z codes after October 2014 Axis V GAF is eliminated-new options are World Health Organization Disability Assessment Schedule (WHO-DAS 2.0) 26
26 DSM-V Diagnostic Considerations Substance-Related and Addictive Disorders Substance Abuse and Substance Dependence now consolidated into Substance Use Disorder, with severity continuum of mild, moderate, or severe Legal consequences criterion removed and craving criterion added to Substance Use Disorder Tolerance and Withdrawal criteria are not counted if the substance is prescribed by a physician Gambling Disorder has been moved from the Impulse-Control Disorders chapter in DSM-IV to this chapter in DSM-5 27
27 NEUROBIOLOGY OF ADDICTION 28
28 What is Addiction? The repetitive compulsive use of anything in spite of adverse consequences and ineffectiveness. This is regardless of the drug or behavior used.
29 What are we Addicted to? Below the level of the cortex the brain has a reward center. This center is necessary for us to learn what we should do again. It is a necessary survival mechanism. It can go awry and when it does we can be addicted. The main neurotransmitter active at this site is DOPAMINE. Wetsman, 2007
30 The Dopamine Spike
31 Anatomy of the Reward System
32 Dopamine Spike Electrical stimulation of the MFB in humans Electrical self stimulation of the MFB in mammals Degree of reward varies with rate of rise Craving starts on the way down Everyone has enough at the peak Wetsman, 2007
33 The Reward System Non-selective and Indiscriminant
34 Addiction Definitions ASAM Impaired control Preoccupation with the drug Use despite adverse consequences Distortions in cognition (denial and others) APA Addiction can be defined as compulsive drug seeking and drug taking, with a loss of control over drug use. DSMIV Maladaptive pattern of use Significant impairment or distress Three or more of the following within any 12 month period: 35
35 Definitions DSMIV (cont d) Tolerance Withdrawal Broken limits Persistent desire or unsuccessful efforts Excessive time spent Important activities given up Use despite adverse consequences 36
36 Why Addiction, Not Dependence? History of the term Dependence and the APA. WHO and physically vs psychologically addicting. Addiction without physical dependence. Dependence without addiction. Dependence vs. Tolerance Wetsman, 2007
37 So What About Abuse? Addiction is a sick brain doing it s best to feel better. Abuse is a healthy brain doing stupid things with drugs. There is no evidence of one leading to the other. You can have one or the other first and then develop the other one. Wetsman, 2007
38 So What About Abuse Abuse is to won t -- as addiction is to can t. Abuse is a normal brain needing no medicines (other than for whatever else is wrong with it) and addiction is an ill brain that often needs medical help. Treatments for Abuse vs Dependence are Different! Wetsman, 2007
39 DSM IV-TR Abuse (Cont) Key Point: THE SYMPTOMS HAVE NEVER MET THE CRITERIA FOR SUBSTANCE DEPENDENCE FOR THIS CLASS OF SUBSTANCE. Wetsman, 2007
40 American Society of Addiction Medicine - Patient Placement Criteria (ASAM PPC) 41
41 What is happening in some programs in America? Clients are being referred to the wrong levels of care. Clients are often referred to, and treated in the agency conducting the assessment. Clinical Assessments do not justify the recommendations being made. Clinical Justifications are not required. If provided clinical justifications do not include clinical rationale / evidence supporting the recommendation. There are little to no policies or procedures that address the format and or quality of assessments, patient placement decisions, and clinical justifications 42
42 Why Do We Need to Improve Patient Placement and Clinical Justifications? Improved Performance and Treatment Outcomes Increase Initiation, Engagement & Retention Rates More Efficient & Effective Utilization of Resources Shift to Performance Based Contracting Positions Organizations for Medicaid and Private Insurance Reimbursement 43
43 Question QUESTION: How does this lack of consistency interpreting clinical information impact treatment? 44
44 Treatment Implications Answer: Client s receive the Wrong 1. Diagnosis or Diagnostic Impression 2. Level of Care Recommendation 3. Services and Interventions As a result, the client s chances of being successful in treatment are compromised right from the beginning of the treatment process. 45
45 Question QUESTION: What Does Research Say About Mismatching Clients to Treatment? 46
46 Treatment Implications ANSWER: Clients that are mismatched to treatment have lower retention rates and poorer outcomes. Less treatment is NOT Good. More treatment is NOT Good. One study found that No Treatment was better than the wrong treatment. (Knight, K., 2009) Louisiana Department of Health and 47
47 Uniform Patient Placement Criteria Defined Uniform Patient Placement Criteria (e.g., ASAM, LOCUS ) describe in detail the levels of care along the continuum of care, and provide specific guidelines for Patient Placement Decisions, a.k.a., Level of Care recommendations. General Components of UPPC Level of Care Continuum Dimensions of Assessment Criteria (e.g., admission, continued stay & discharge) 48
48 ASAM Dimensions ASAM Six (6)Dimensions: The client s risk status in each of the six dimensions collectively inform the patient placement decision. 1. Acute Intoxication and/or Withdrawal Potential. 2. Biomedical Conditions and Complications. 3. Emotional, Behavioral, or Cognitive Problems and Complications. 4. Readiness to Change. 5. Relapse, Continued Use, or Continued Problem Potential 6. Recovery Environment. 49
49 Benefits of UPPC Uniform Patient Placement Criteria: 1. Guides proper patient placement. 2. Promotes individualized care. 3. Identifies critical information to be collected during an assessment. 4. Influences multidimensional treatment planning. 5. Establishes a common language. 6. Identifies gaps in a continuum of care. 50
50 IMPORTANT!!! Criteria are NOT substitutes for GOOD Clinical Judgment. Tools, and Criteria s support, guide and enhance GOOD Clinical Judgment! 51
51 ASAM Historical and Theoretical Foundations The ASAM PPC 2 is published by the American Society of Addiction Medicine. Used as a clinical guide in matching patients to the correct level of care. Expands use of multidimensional assessments in developing objective patient placement decisions at various levels of care. Emphasis on intensities of along a continuum, in a variety of program types and levels of care ASAM PPC - 2R 52
52 ASAM Historical and Theoretical Foundations The continuing development and refinement of the criteria continue a shift from: Uni-dimensional to multidimensional assessment. Program-driven to clinically driven treatment. Fixed length of service to variable length of service. A limited number of discrete levels of care to a continuum of care. ASAM PPC - 2R 53
53 Theoretical Foundations of the Goals of Treatment: ASAM PPC Tailored to individuals needs (length, choice) Guided by individualized treatment plan. Client directed treatment plan. Based on comprehensive bio-psychosocial assessment of person and when possible, family. Should list problems, strengths, priorities, goals, methods or strategies. Safety first ASAM PPC - 2R 54
54 ASAM Placement Considerations Placement decisions are determined based upon consideration of: Level of Service/Care most appropriate to meet the clinical needs Dimensional Assessments Primary and Secondary Determinants Louisiana Department of Health and Hospitals 55
55 Exceptions to PPC There are 3 exceptions which override the PPC match: Lack of the availability of the appropriate selected care. Failure of a patient to progress at a given level of care so as to warrant a reassessment of the treatment plan with a view to modification of the treatment approach. State laws regulating requiring different criteria. ASAM PPC - 2R 56
56 ASAM Levels of Service Levels of Care: Level 0.5 Level I Level II Level III Level IV Early Intervention Outpatient Treatment Intensive Outpatient / Partial Hospitalization Residential/Inpatient Treatment Medically Managed Intensive Hospital/Inpatient Treatment (Note:.1 to.9 represents graduated intensity within an existing level of care.) ASAM PPC - 2R 57
57 Levels of Care ASAM PPC - 2R Levels 0.5 Early Intervention Prevention Focus Staffing (Essential) Partnerships Individuals at risk for developing substance-related problems or Those without sufficient information to document a substance use disorder. Licensed Prevention Professionals Department of Education
58 Levels of Care ASAM PPC - 2R Levels I Outpatient Care (<9hrs/week Adults <6hrs/week Adols) Staffing (Essential) Organized services delivered in a wide variety of outpatient settings. Prescriptive services, regularly scheduled sessions, a defined set of policies and procedures or medical protocols. Accommodates high severity D4, unmotivated mandated persons; expanded for COD MD, Nurse, Clinicians/ Counselors, Care Coordinator, Peer Mentors (strongly recommended)
59 Levels of Care ASAM PPC - 2R Level II Intensive Outpatient/Partial Hospitalization (>9hrs/wk) Staffing (Essential) Partial 9-20hrs/wk; IOP 20hrs/</wk Organized, clinically intensive services delivered during the day, before or after work/school, in the evening or on weekends. Provides essential education and treatment components while allowing patients to apply their newly acquired skills within real world environments. MD, Nurse, Clinicians/ Counselors, Care Coordinator, Peer Mentors (strongly recommended
60 Levels of Care ASAM PPC - 2R Level III Residential/Inpatient Treatment Organized, 24hr services, staffed by trained medical and counseling staff to stabilize multidimensional problems, as prep for outpatient treatment. Defined set of policies and procedures foster reliance on the treatment community as a therapeutic agents. Designed to treat person who have significant social and psychological problems Staffing (Essential) MD(s), Nurse(s), Psych Techs Clinicians/ Counselors, Care Coordinator Staffing (Optional) Psychologist, Occupational Therapist, Peer Mentors Housed in or affiliated with permanent residential facilities. Generally provide access to on-site self-help meetings.
61 Levels of Care ASAM PPC - 2R Level III. 7D Residential Medically Monitored/Supported Detox Staffing (Essential) Staffing (Optional) Organized 24 hour nursing care and daily physician care for severe, unstable problems in Dimensions 1, 2 or 3. Counselors available. Appropriate for patients whose subacute biomedical, emotional, behavioral and cognitive problems are so severe that they require residential care not a full service hospital. MD(s) (AD Psych/Primary Care w/ ASAM); APRN/NP/RN; Psych Techs; Clinicians/ Counselors, Care Coordinator, Peer Mentor
62 Levels of Care ASAM PPC - 2R Level IV.D Medically Managed Intensive Hospital/ Inpatient Treatment Organized 24 hour nursing care and daily physician care for severe, unstable problems in Dimensions 1, 2 or 3. Counselors available. Appropriate for patients whose acute biomedical, emotional, behavioral and cognitive problems are so severe that they require primary medical and nursing care Full resources of a general acute care psychiatric hospital are available. Staffing (Essential) MD(s) (AD Psych/Primary Care w/ ASAM); APRN/NP/RN; Psych Techs; Clinicians/ Counselors, Care Coordinator, Staffing (Optional) Peer Mentor
63 Levels of Care ASAM PPC - 2R Opioid Maintenance Therapy Staffing (Essential) Best conceptualized as a separate service that can be provided at any level of care but typically, Level I Outpatient in an ambulatory setting. Daily or several times weekly opioid medication and counseling available to maintain multidimensional stability for those with opioid dependency. MD, Nurse, Clinician or Counselor
64 Dimensional Criteria ASAM s 6 assessment dimensions allow for multidimensional considerations in the determination of best level of care placements. Primary Determinants Acute Detox Medical Complications Psychiatric Difficulties Secondary Determinants Change readiness Relapse, continued use, continued problem potential Recovery/Living Environment
65 Summary Addiction populations are heterogeneous Neurobiology of addiction supports a chronic, relapsing condition and the disease concept Diagnose with expectation not exception Holistic evaluations and comprehensive treatment planning with care coordination are critical Appropriate dosing of care is critical to successful outcomes Unique person-centered, family focused empathic treatment approaches are required to enhance outcomes 66
66 References American Psychiatric Association, Diagnostic and Statistical manual of Mental Disorders, Fourth Edition, Text Revision. Washington DC, American Psychiatric Association, Carroll, K.M. Methodological issues and problems in the assessment of substance use. Psychological Assessment 7: , Donovan, D.M., and Marlatt, G.A., eds. Assessment of Addictive Behaviors. New York: Guilford Press, McLellan, A.T.; Kushner, H.; Metzger, D.; Peters, R.; Smith, I.; Grissom, G.; Pettinati, H.; and Argeriou, M. The fifth edition of the Addiction Severity Index. J Substance Abuse Treat 9: , 1992b. Louisiana Department of Health and Hospitals 67
67 References Mee-Lee, D.; Shulman, G.D.; Fishman, M.; Gastfriend, D.R.; and Grifith, J.H. Patient Placement Criteria for the Treatment of Substance-Related Disorders. 2d ed., rev. Chevy Chase, MD: American Society of Addiction Medicine, Meyers, A. Thomas McLellan, J. Jaeger, H. Pettinati,The development of the comprehensive addiction severity index for adolescents (CASI-A) An interview for assessing multiple problems of adolescents. Journal of Substance Abuse Treatment, Volume 12, Issue 3, Pages K. Spitzer, R.L., Williams, J.B.W., Gibbon, M. & First, M.B. Structured Clinical Interview for DSM- III-R-Patient Version. New York: New York State Psychiatric Institute, Biometrics Research Department, Sheehan, D.V., Lecrubier, Y., Sheehan, K.H., Amorim, P., Janavs, J., Weiller, E., Hergueta, T., Baker, R., & Dunbar, G.C. The mini-international neuropsychiatric interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-1V and ICD-10. Journal of Clinical Psychiatry, 59 (suppl. 20), Louisiana Department of Health and Hospitals 68
68 Questions and Discussion Rochelle Head-Dunham, MD
69
ADVANCED BEHAVIORAL HEALTH, INC. Clinical Level of Care Guidelines - 2015
 The Clinical Level of Care Guidelines contained on the following pages have been developed as a guide to assist care managers, physicians and providers in making medical necessity decisions about the least
The Clinical Level of Care Guidelines contained on the following pages have been developed as a guide to assist care managers, physicians and providers in making medical necessity decisions about the least
DSM-5 and its use by chemical dependency professionals
 + DSM-5 and its use by chemical dependency professionals Greg Bauer Executive Director Alpine Recovery Services Inc. President Chemical Dependency Professionals Washington State (CDPWS) NAADAC 2014 Annual
+ DSM-5 and its use by chemical dependency professionals Greg Bauer Executive Director Alpine Recovery Services Inc. President Chemical Dependency Professionals Washington State (CDPWS) NAADAC 2014 Annual
THE OFFICE OF SUBSTANCE ABUSE SERVICES REQUIREMENTS FOR THE PROVISION OF RESIDENTIAL DETOXIFICATION SERVICES BY PROVIDERS FUNDED WITH DBHDS RESOURCES
 THE OFFICE OF SUBSTANCE ABUSE SERVICES REQUIREMENTS FOR THE PROVISION OF RESIDENTIAL DETOXIFICATION SERVICES BY PROVIDERS FUNDED WITH DBHDS RESOURCES PURPOSE: The goal of this document is to describe the
THE OFFICE OF SUBSTANCE ABUSE SERVICES REQUIREMENTS FOR THE PROVISION OF RESIDENTIAL DETOXIFICATION SERVICES BY PROVIDERS FUNDED WITH DBHDS RESOURCES PURPOSE: The goal of this document is to describe the
SCREENING FOR CO-OCCURRING DISORDERS USING THE MODIFIED MINI SCREEN (MMS) USER S GUIDE. (Rev. 6/05)
 USER S GUIDE. (Rev. 6/05)") SCREENING FOR CO-OCCURRING DISORDERS USING THE MODIFIED MINI SCREEN (MMS) USER S GUIDE (Rev. 6/05) ACKNOWLEDGEMENTS This user guide was developed by the NYS Practice Improvement Collaborative (PIC) under
SCREENING FOR CO-OCCURRING DISORDERS USING THE MODIFIED MINI SCREEN (MMS) USER S GUIDE (Rev. 6/05) ACKNOWLEDGEMENTS This user guide was developed by the NYS Practice Improvement Collaborative (PIC) under
Assessment and Diagnosis of DSM-5 Substance-Related Disorders
 Assessment and Diagnosis of DSM-5 Substance-Related Disorders Jason H. King, PhD (listed on p. 914 of DSM-5 as a Collaborative Investigator) j.king@lecutah.com or 801-404-8733 www.lecutah.com D I S C L
Assessment and Diagnosis of DSM-5 Substance-Related Disorders Jason H. King, PhD (listed on p. 914 of DSM-5 as a Collaborative Investigator) j.king@lecutah.com or 801-404-8733 www.lecutah.com D I S C L
LEVEL I SA: OUTPATIENT INDIVIDUAL THERAPY - Adult
 LEVEL I SA: OUTPATIENT INDIVIDUAL THERAPY - Adult Definition The following is based on the Adult Criteria of the Patient Placement Criteria for the Treatment of Substance-Related Disorders of the American
LEVEL I SA: OUTPATIENT INDIVIDUAL THERAPY - Adult Definition The following is based on the Adult Criteria of the Patient Placement Criteria for the Treatment of Substance-Related Disorders of the American
The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5)
") The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) Cardwell C Nuckols, PhD cnuckols@elitecorp1.com Cardwell C. Nuckols, PhD www.cnuckols.com SECTION I-BASICS DSM-5 Includes
The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) Cardwell C Nuckols, PhD cnuckols@elitecorp1.com Cardwell C. Nuckols, PhD www.cnuckols.com SECTION I-BASICS DSM-5 Includes
How To Know If You Can Get Help For An Addiction
 2014 FLORIDA SUBSTANCE ABUSE LEVEL OF CARE CLINICAL CRITERIA SUBSTANCE ABUSE LEVEL OF CARE CLINICAL CRITERIA Overview Psychcare strives to provide quality care in the least restrictive environment. An
2014 FLORIDA SUBSTANCE ABUSE LEVEL OF CARE CLINICAL CRITERIA SUBSTANCE ABUSE LEVEL OF CARE CLINICAL CRITERIA Overview Psychcare strives to provide quality care in the least restrictive environment. An
-- No equivalent DSM-IV code disorders 303 Alcohol dependence syndrome -- No equivalent DSM-IV code 303.9 [0-3]*
![-- No equivalent DSM-IV code disorders 303 Alcohol dependence syndrome -- No equivalent DSM-IV code 303.9 [0-3]*](/thumbs/26/8764864.jpg "-- No equivalent DSM-IV code disorders 303 Alcohol dependence syndrome -- No equivalent DSM-IV code 303.9 [0-3]*") Substance Use Disorder Covered Diagnoses ICD-9 DSM-IV Alcohol Use Disorders 291 Alcohol-induced mental -- No equivalent DSM-IV code s 303 Alcohol syndrome -- No equivalent DSM-IV code 303.9 [0-3]* Other
Substance Use Disorder Covered Diagnoses ICD-9 DSM-IV Alcohol Use Disorders 291 Alcohol-induced mental -- No equivalent DSM-IV code s 303 Alcohol syndrome -- No equivalent DSM-IV code 303.9 [0-3]* Other
AN INTRODUCTION ASAM
 AN INTRODUCTION ASAM 2013 Ray Caesar LPC, LADC-MH Director of Addiction Specialty Programs ODMHSAS (405)522-3870 rcaesar@odmhsas.org AMERICAN SOCIETY OF ADDICTON MEDICINE ASAM ASAM is a professional organization
AN INTRODUCTION ASAM 2013 Ray Caesar LPC, LADC-MH Director of Addiction Specialty Programs ODMHSAS (405)522-3870 rcaesar@odmhsas.org AMERICAN SOCIETY OF ADDICTON MEDICINE ASAM ASAM is a professional organization
PHENOTYPE PROCESSING METHODS.
 PHENOTYPE PROCESSING METHODS. We first applied exclusionary criteria, recoding diagnosed individuals as phenotype unknown in the presence of: all dementias, amnestic and cognitive disorders; unknown/unspecified
PHENOTYPE PROCESSING METHODS. We first applied exclusionary criteria, recoding diagnosed individuals as phenotype unknown in the presence of: all dementias, amnestic and cognitive disorders; unknown/unspecified
Behavioral Health Medical Necessity Criteria
 Behavioral Health Medical Necessity Criteria Revised: 7/14/05 2 nd Revision: 9/14/06 3 rd Revision: 8/23/07 4 th Revision: 8/28/08; 11/20/08 5 th Revision: 8/27/09 Anthem Blue Cross and Blue Shield 2 Gannett
Behavioral Health Medical Necessity Criteria Revised: 7/14/05 2 nd Revision: 9/14/06 3 rd Revision: 8/23/07 4 th Revision: 8/28/08; 11/20/08 5 th Revision: 8/27/09 Anthem Blue Cross and Blue Shield 2 Gannett
LEVEL III.5 SA: SHORT TERM RESIDENTIAL - Adult (DUAL DIAGNOSIS CAPABLE)
") LEVEL III.5 SA: SHT TERM RESIDENTIAL - Adult (DUAL DIAGNOSIS CAPABLE) Definition The following is based on the Adult Criteria of the Patient Placement Criteria for the Treatment of Substance-Related Disorders
LEVEL III.5 SA: SHT TERM RESIDENTIAL - Adult (DUAL DIAGNOSIS CAPABLE) Definition The following is based on the Adult Criteria of the Patient Placement Criteria for the Treatment of Substance-Related Disorders
Phenotype Processing Algorithm
 Phenotype Processing Algorithm 1. Each individual has three associated variables which will be used for diagnostic classification. The variables are SZ, SA, and BS, which correspond to affection status
Phenotype Processing Algorithm 1. Each individual has three associated variables which will be used for diagnostic classification. The variables are SZ, SA, and BS, which correspond to affection status
OUTPATIENT SUBSTANCE USE DISORDER SERVICES FEE-FOR-SERVICE
 OUTPATIENT SUBSTANCE USE DISORDER SERVICES FEE-FOR-SERVICE Brief Coverage Statement Outpatient Substance Use Disorder (SUD) Fee-For-Service (FFS) Treatment Services are available for the treatment of substance
OUTPATIENT SUBSTANCE USE DISORDER SERVICES FEE-FOR-SERVICE Brief Coverage Statement Outpatient Substance Use Disorder (SUD) Fee-For-Service (FFS) Treatment Services are available for the treatment of substance
DSM-5 Do Not Use ICD -10 Codes
 DSM-5 Do Not Use ICD -10 Codes There are ICD-10 codes that DSM 5 is not compatible with. This spreadsheet details the ICD-10 codes that are NOT compatible with DSM 5. ICD10_DX_CD ICD10_DX_DESC F03.90 Unspecified
DSM-5 Do Not Use ICD -10 Codes There are ICD-10 codes that DSM 5 is not compatible with. This spreadsheet details the ICD-10 codes that are NOT compatible with DSM 5. ICD10_DX_CD ICD10_DX_DESC F03.90 Unspecified
GAIN and DSM. Presentation Objectives. Using the GAIN Diagnostically
 GAIN and DSM GAIN National Clinical Training Team 2011 Version 2 Materials Presentation Objectives Understand which DSM diagnoses are generated by GAIN ABS for the GAIN reports and which ones must be added
GAIN and DSM GAIN National Clinical Training Team 2011 Version 2 Materials Presentation Objectives Understand which DSM diagnoses are generated by GAIN ABS for the GAIN reports and which ones must be added
Topics In Addictions and Mental Health: Concurrent disorders and Community resources. Laurence Bosley, MD, FRCPC
 Topics In Addictions and Mental Health: Concurrent disorders and Community resources Laurence Bosley, MD, FRCPC Overview Understanding concurrent disorders. Developing approaches to treatment Definitions
Topics In Addictions and Mental Health: Concurrent disorders and Community resources Laurence Bosley, MD, FRCPC Overview Understanding concurrent disorders. Developing approaches to treatment Definitions
American Society of Addiction Medicine
 American Society of Addiction Medicine Public Policy Statement on Treatment for Alcohol and Other Drug Addiction 1 I. General Definitions of Addiction Treatment Addiction Treatment is the use of any planned,
American Society of Addiction Medicine Public Policy Statement on Treatment for Alcohol and Other Drug Addiction 1 I. General Definitions of Addiction Treatment Addiction Treatment is the use of any planned,
EXHIBIT D, COVERED BEHAVIORAL HEALTH DIAGNOSES
 EXHIBIT D, COVERED BEHAVIORAL HEALTH DIAGNOSES Part I- Mental Health Covered Diagnoses 295-298.9 295 Schizophrenic s (the following fifth-digit sub-classification is for use with category 295) 0 unspecified
EXHIBIT D, COVERED BEHAVIORAL HEALTH DIAGNOSES Part I- Mental Health Covered Diagnoses 295-298.9 295 Schizophrenic s (the following fifth-digit sub-classification is for use with category 295) 0 unspecified
ICD- 9 Source Description ICD- 10 Source Description
 291.0 Alcohol withdrawal delirium F10.121 Alcohol abuse with intoxication delirium 291.0 Alcohol withdrawal delirium F10.221 Alcohol dependence with intoxication delirium 291.0 Alcohol withdrawal delirium
291.0 Alcohol withdrawal delirium F10.121 Alcohol abuse with intoxication delirium 291.0 Alcohol withdrawal delirium F10.221 Alcohol dependence with intoxication delirium 291.0 Alcohol withdrawal delirium
UNDERSTANDING CO-OCCURRING DISORDERS. Frances A. Campbell MSN, PMH CNS-BC, CARN Michael Beatty, LCSW, NCGC-1 Bridge To Hope November 18, 2015
 UNDERSTANDING CO-OCCURRING DISORDERS Frances A. Campbell MSN, PMH CNS-BC, CARN Michael Beatty, LCSW, NCGC-1 Bridge To Hope November 18, 2015 CO-OCCURRING DISORDERS What does it really mean CO-OCCURRING
UNDERSTANDING CO-OCCURRING DISORDERS Frances A. Campbell MSN, PMH CNS-BC, CARN Michael Beatty, LCSW, NCGC-1 Bridge To Hope November 18, 2015 CO-OCCURRING DISORDERS What does it really mean CO-OCCURRING
WORKERS COMPENSATION PROTOCOLS WHEN PRIMARY INJURY IS PSYCHIATRIC/PSYCHOLOGICAL
 WORKERS COMPENSATION PROTOCOLS WHEN PRIMARY INJURY IS PSYCHIATRIC/PSYCHOLOGICAL General Guidelines for Treatment of Compensable Injuries Patient must have a diagnosed mental illness as defined by DSM-5
WORKERS COMPENSATION PROTOCOLS WHEN PRIMARY INJURY IS PSYCHIATRIC/PSYCHOLOGICAL General Guidelines for Treatment of Compensable Injuries Patient must have a diagnosed mental illness as defined by DSM-5
WCHO PIHP/CA POLICY for the LIVINGSTON- WASHTENAW COORDINATING AGENCY Department: Coordinating Agency Author: Marci Scalera Approval Date 4/17/12
 WCHO PIHP/CA POLICY for the LIVINGSTON- WASHTENAW COORDINATING AGENCY Department: Coordinating Agency Author: Marci Scalera Approval Date 4/17/12 Policy and Procedure Residential Treatment Services Policy
WCHO PIHP/CA POLICY for the LIVINGSTON- WASHTENAW COORDINATING AGENCY Department: Coordinating Agency Author: Marci Scalera Approval Date 4/17/12 Policy and Procedure Residential Treatment Services Policy
Exploring and Understanding DSM-5. Neal Adams, MD, MPH, Deputy Director, CiMH Victor Kogler, Executive Director, ADPI
 Exploring and Understanding DSM-5 Neal Adams, MD, MPH, Deputy Director, CiMH Victor Kogler, Executive Director, ADPI 1 Disclosure Information Exploring and Understanding: DSM-5 Neal Adams, MD, MPH Victor
Exploring and Understanding DSM-5 Neal Adams, MD, MPH, Deputy Director, CiMH Victor Kogler, Executive Director, ADPI 1 Disclosure Information Exploring and Understanding: DSM-5 Neal Adams, MD, MPH Victor
ICD 9 to ICD 10 Code Conversions Based on 2014 GEMs Alcohol and Drug Abuse Programs Approved ICD 10 Codes 3/21/2014
 291 Alcohol induced mental disorders 291.0 Alcohol withdrawal delirium F10.231 Alcohol dependence with withdrawal delirium F10.121 Alcohol abuse with intoxication delirium F10.221 Alcohol dependence with
291 Alcohol induced mental disorders 291.0 Alcohol withdrawal delirium F10.231 Alcohol dependence with withdrawal delirium F10.121 Alcohol abuse with intoxication delirium F10.221 Alcohol dependence with
THE DISEASE OF ADDICTION: A Primer. The 10 th Annual Kinship Conference for Grandparents and Relatives South Burlington, Vermont 9 September 2014
 THE DISEASE OF ADDICTION: A Primer The 10 th Annual Kinship Conference for Grandparents and Relatives South Burlington, Vermont 9 September 2014 3 BASIC QUESTIONS AT THE KITCHEN TABLE 1. Why don t they
THE DISEASE OF ADDICTION: A Primer The 10 th Annual Kinship Conference for Grandparents and Relatives South Burlington, Vermont 9 September 2014 3 BASIC QUESTIONS AT THE KITCHEN TABLE 1. Why don t they
LEVEL II.1 SA: INTENSIVE OUTPATIENT - Adult
 LEVEL II.1 SA: INTENSIVE OUTPATIENT - Adult Definition The following is based on the Adult Criteria of the Patient Placement Criteria for the Treatment of Substance- Related Disorders of the American Society
LEVEL II.1 SA: INTENSIVE OUTPATIENT - Adult Definition The following is based on the Adult Criteria of the Patient Placement Criteria for the Treatment of Substance- Related Disorders of the American Society
OUTPATIENT SUBSTANCE USE DISORDER SERVICES FEE-FOR-SERVICE
 OUTPATIENT SUBSTANCE USE DISORDER SERVICES FEE-FOR-SERVICE BRIEF COVERAGE STATEMENT This benefit coverage standard describes outpatient Substance Use Disorder services (known as SUD Fee-For-Service (FFS)
OUTPATIENT SUBSTANCE USE DISORDER SERVICES FEE-FOR-SERVICE BRIEF COVERAGE STATEMENT This benefit coverage standard describes outpatient Substance Use Disorder services (known as SUD Fee-For-Service (FFS)
New York State Office of Alcoholism & Substance Abuse Services Addiction Services for Prevention, Treatment, Recovery
 New York State Office of Alcoholism & Substance Abuse Services Addiction Services for Prevention, Treatment, Recovery USING THE 48 HOUR OBSERVATION BED USING THE 48 HOUR OBSERVATION BED Detoxification
New York State Office of Alcoholism & Substance Abuse Services Addiction Services for Prevention, Treatment, Recovery USING THE 48 HOUR OBSERVATION BED USING THE 48 HOUR OBSERVATION BED Detoxification
Medical Necessity Criteria
 Medical Necessity Criteria 2015 Updated 03/04/2015 Appendix B Medical Necessity Criteria Purpose: In order to promote consistent utilization management decisions, all utilization and care management staff
Medical Necessity Criteria 2015 Updated 03/04/2015 Appendix B Medical Necessity Criteria Purpose: In order to promote consistent utilization management decisions, all utilization and care management staff
These changes are prominent in individuals with severe disorders, but also occur at the mild or moderate level.
 Substance-Related Disorders DSM-V Many people use words like alcoholism, drug dependence and addiction as general descriptive terms without a clear understanding of their meaning. What does it really mean
Substance-Related Disorders DSM-V Many people use words like alcoholism, drug dependence and addiction as general descriptive terms without a clear understanding of their meaning. What does it really mean
Appendix D. Behavioral Health Partnership. Adolescent/Adult Substance Abuse Guidelines
 Appendix D Behavioral Health Partnership Adolescent/Adult Substance Abuse Guidelines Handbook for Providers 92 ASAM CRITERIA The CT BHP utilizes the ASAM PPC-2R criteria for rendering decisions regarding
Appendix D Behavioral Health Partnership Adolescent/Adult Substance Abuse Guidelines Handbook for Providers 92 ASAM CRITERIA The CT BHP utilizes the ASAM PPC-2R criteria for rendering decisions regarding
Behavioral Health Medical Necessity Criteria
 Behavioral Health Medical Necessity Criteria Effective January 1, 2011 Revised and approved on 8/19/2010 The Office of Medical Policy and Technological Assessment (OMPTA) has developed policies that serve
Behavioral Health Medical Necessity Criteria Effective January 1, 2011 Revised and approved on 8/19/2010 The Office of Medical Policy and Technological Assessment (OMPTA) has developed policies that serve
Overview of the ASAM Patient Placement Criteria, Second Edition Revised (ASAM PPC-2R)
") SAMHSA s Co-occurring Center for Excellence (COCE) Overview of the ASAM Patient Placement Criteria, Second Edition Revised (ASAM PPC-2R) David Mee-Lee, M.D. Chief Editor, ASAM PPC-2R www.dmlmd.com June
SAMHSA s Co-occurring Center for Excellence (COCE) Overview of the ASAM Patient Placement Criteria, Second Edition Revised (ASAM PPC-2R) David Mee-Lee, M.D. Chief Editor, ASAM PPC-2R www.dmlmd.com June
CO-OCCURRING DISORDERS. Michaelene Spence MA LADC 8/8/12
 CO-OCCURRING DISORDERS Michaelene Spence MA LADC 8/8/12 Activity Chemical Health? Mental Health? Video- What is Addiction HBO Terminology MI/CD: Mental Illness/Chemical Dependency IDDT: Integrated Dual
CO-OCCURRING DISORDERS Michaelene Spence MA LADC 8/8/12 Activity Chemical Health? Mental Health? Video- What is Addiction HBO Terminology MI/CD: Mental Illness/Chemical Dependency IDDT: Integrated Dual
hepatolenticular degeneration (E83.0) human immunodeficiency virus [HIV] disease (B20) hypercalcemia (E83.52) hypothyroidism, acquired (E00-E03.
![hepatolenticular degeneration (E83.0) human immunodeficiency virus [HIV] disease (B20) hypercalcemia (E83.52) hypothyroidism, acquired (E00-E03.](/thumbs/30/13936427.jpg "hepatolenticular degeneration (E83.0) human immunodeficiency virus [HIV] disease (B20) hypercalcemia (E83.52) hypothyroidism, acquired (E00-E03.") ICD-10-CM Codes for Mental, Behavioral and Neurodevelopmental Disorders Chapter 5 Mental, Behavioral and Neurodevelopmental disorders (F01-F99) Includes: disorders of psychological development Excludes2:
ICD-10-CM Codes for Mental, Behavioral and Neurodevelopmental Disorders Chapter 5 Mental, Behavioral and Neurodevelopmental disorders (F01-F99) Includes: disorders of psychological development Excludes2:
TREATMENT POLICY #10. Residential Treatment Continuum of Services
 Michigan Department of Community Health, Behavioral Health and Developmental Disabilities Administration BUREAU OF SUBSTANCE ABUSE AND ADDICTION SERVICES TREATMENT POLICY #10 SUBJECT: Residential Treatment
Michigan Department of Community Health, Behavioral Health and Developmental Disabilities Administration BUREAU OF SUBSTANCE ABUSE AND ADDICTION SERVICES TREATMENT POLICY #10 SUBJECT: Residential Treatment
Behavioral Health Medical Necessity Criteria
 Behavioral Health Medical Necessity Criteria Effective January 1, 2013 Revised and approved on 8/09/2012 Anthem Blue Cross 21555 Oxnard St. Woodland Hills, CA 91365 Toll free: 1-800-274-7767 The Office
Behavioral Health Medical Necessity Criteria Effective January 1, 2013 Revised and approved on 8/09/2012 Anthem Blue Cross 21555 Oxnard St. Woodland Hills, CA 91365 Toll free: 1-800-274-7767 The Office
CHAPTER 5 MENTAL, BEHAVIOR AND NEURODEVELOPMENT DISORDERS (F01-F99) March 2014. 2014 MVP Health Care, Inc.
 March 2014. 2014 MVP Health Care, Inc.") CHAPTER 5 MENTAL, BEHAVIOR AND NEURODEVELOPMENT DISORDERS (F01-F99) March 2014 2014 MVP Health Care, Inc. CHAPTER 5 CHAPTER SPECIFIC CATEGORY CODE BLOCKS F01-F09 Mental disorders due to known physiological
CHAPTER 5 MENTAL, BEHAVIOR AND NEURODEVELOPMENT DISORDERS (F01-F99) March 2014 2014 MVP Health Care, Inc. CHAPTER 5 CHAPTER SPECIFIC CATEGORY CODE BLOCKS F01-F09 Mental disorders due to known physiological
Level of Care Criteria Psychiatric Criteria
 LEVEL OF CARE AND TREATMENT CRITERIA Level of Care Criteria Psychiatric Criteria Adult Half Day Partial Hospital Treatment Adult Psychiatric Home Care Child and Adolescent Half Day Partial Hospital Treatment
LEVEL OF CARE AND TREATMENT CRITERIA Level of Care Criteria Psychiatric Criteria Adult Half Day Partial Hospital Treatment Adult Psychiatric Home Care Child and Adolescent Half Day Partial Hospital Treatment
Psychiatric Comorbidity in Methamphetamine-Dependent Patients
 Psychiatric Comorbidity in Methamphetamine-Dependent Patients Suzette Glasner-Edwards, Ph.D. UCLA Integrated Substance Abuse Programs August11 th, 2010 Overview Comorbidity in substance users Risk factors
Psychiatric Comorbidity in Methamphetamine-Dependent Patients Suzette Glasner-Edwards, Ph.D. UCLA Integrated Substance Abuse Programs August11 th, 2010 Overview Comorbidity in substance users Risk factors
Attachment A. Code Beginning Review
 Attachment A ICD-10-CM Mental Disorders Diagnosis Codes and s Subject to Certification of Admission/Concurrent/Continued Stay Review Based on the Admitting Diagnosis Code This list contains principal diagnosis
Attachment A ICD-10-CM Mental Disorders Diagnosis Codes and s Subject to Certification of Admission/Concurrent/Continued Stay Review Based on the Admitting Diagnosis Code This list contains principal diagnosis
Martha Brewer, MS, LPC,LADC. Substance Abuse and Treatment
 Martha Brewer, MS, LPC,LADC Substance Abuse and Treatment What is a substance use disorder? Long-term and chronic illness Can affect anyone: rich or poor, male or female, employed or unemployed, young
Martha Brewer, MS, LPC,LADC Substance Abuse and Treatment What is a substance use disorder? Long-term and chronic illness Can affect anyone: rich or poor, male or female, employed or unemployed, young
Washington State Regional Support Network (RSN)
") Access to Care Standards 11/25/03 Eligibility Requirements for Authorization of Services for Medicaid Adults & Medicaid Older Adults Please note: The following standards reflect the most restrictive authorization
Access to Care Standards 11/25/03 Eligibility Requirements for Authorization of Services for Medicaid Adults & Medicaid Older Adults Please note: The following standards reflect the most restrictive authorization
Co-Occurring Disorders
 Presented by Pamela Messore LICSW, LCDP Co-Occurring Disorder - formerly Dual Diagnosis - was once a challenge to providers. Historically, clients were treated in separate modalities - even separate agencies.
Presented by Pamela Messore LICSW, LCDP Co-Occurring Disorder - formerly Dual Diagnosis - was once a challenge to providers. Historically, clients were treated in separate modalities - even separate agencies.
Co-Occurring Disorders
 Co-Occurring Disorders PACCT 2011 CAROLYN FRANZEN Learning Objectives List common examples of mental health problems associated with substance abuse disorders Describe risk factors that contribute to the
Co-Occurring Disorders PACCT 2011 CAROLYN FRANZEN Learning Objectives List common examples of mental health problems associated with substance abuse disorders Describe risk factors that contribute to the
What s New in DSM-5 and the New ASAM Criteria? Implications in an Era of Healthcare Reform
 March 2014 ATTC Messenger What s New in DSM-5 and the New ASAM Criteria? Implications in an Era of Healthcare Reform David Mee-Lee, M.D. Chief Editor, The ASAM Criteria Senior Vice President The Change
March 2014 ATTC Messenger What s New in DSM-5 and the New ASAM Criteria? Implications in an Era of Healthcare Reform David Mee-Lee, M.D. Chief Editor, The ASAM Criteria Senior Vice President The Change
Inpatient Behavioral Health and Inpatient Substance Abuse Treatment: Aligning Care Efficiencies with Effective Treatment
 Inpatient Behavioral Health and Inpatient Substance Abuse Treatment: Aligning Care Efficiencies with Effective Treatment BHM Healthcare Solutions 2013 1 Presentation Objectives Attendees will have a thorough
Inpatient Behavioral Health and Inpatient Substance Abuse Treatment: Aligning Care Efficiencies with Effective Treatment BHM Healthcare Solutions 2013 1 Presentation Objectives Attendees will have a thorough
Psychiatric Residential Treatment Facility (PRTF): Aligning Care Efficiencies with Effective Treatment. BHM Healthcare Solutions 2013 1
: Aligning Care Efficiencies with Effective Treatment. BHM Healthcare Solutions 2013 1") Psychiatric Residential Treatment Facility (PRTF): Aligning Care Efficiencies with Effective Treatment 1 Presentation Objectives Attendees will have a thorough understanding of Psychiatric Residential
Psychiatric Residential Treatment Facility (PRTF): Aligning Care Efficiencies with Effective Treatment 1 Presentation Objectives Attendees will have a thorough understanding of Psychiatric Residential
The Department of Children and Families Substance Abuse Program
 The Department of Children and Families Substance Abuse Program Florida Supplement To the American Society of Addiction Medicine Patient Placement Criteria For the Treatment of Substance-Related Disorders
The Department of Children and Families Substance Abuse Program Florida Supplement To the American Society of Addiction Medicine Patient Placement Criteria For the Treatment of Substance-Related Disorders
Column1 Substance Abuse Diagnosis Exclusion Codes ICD-9: Description 291.0 Alcohol withdrawal delirium 291.1 Alcohol-induced persisting amnestic
 Column1 Substance Abuse Diagnosis Exclusion Codes ICD-9: Code Description 291.0 Alcohol withdrawal delirium 291.1 Alcohol-induced persisting amnestic disorder 291.2 Alcohol-induced persisting dementia
Column1 Substance Abuse Diagnosis Exclusion Codes ICD-9: Code Description 291.0 Alcohol withdrawal delirium 291.1 Alcohol-induced persisting amnestic disorder 291.2 Alcohol-induced persisting dementia
Procedure/ Revenue Code. Billing NPI Required. Rendering NPI Required. Service/Revenue Code Description. Yes No No
 Procedure/ Revenue Code Service/Revenue Code Description Billing NPI Rendering NPI Attending/ Admitting NPI 0100 Inpatient Services Yes No Yes 0114 Room & Board - private psychiatric Yes No Yes 0124 Room
Procedure/ Revenue Code Service/Revenue Code Description Billing NPI Rendering NPI Attending/ Admitting NPI 0100 Inpatient Services Yes No Yes 0114 Room & Board - private psychiatric Yes No Yes 0124 Room
Addiction Billing. Kimber Debelak, CMC, CMOM, CMIS Director, Recovery Pathways
 Addiction Billing Kimber Debelak, CMC, CMOM, CMIS Director, Recovery Pathways Objectives Provide overview of addiction billing contrasting E&M vs. behavioral health codes Present system changes in ICD-9
Addiction Billing Kimber Debelak, CMC, CMOM, CMIS Director, Recovery Pathways Objectives Provide overview of addiction billing contrasting E&M vs. behavioral health codes Present system changes in ICD-9
Substance Abuse Diagnosis DUG 8.0
 Substance Abuse Diagnosis DUG 8.0 ICD-10 Code ICD-10 Description F10. Alcohol Related Disorders F10.1 Alcohol Abuse F10.10 Alcohol Abuse, Uncomplicated F10.12 Alcohol Abuse With Intoxication F10.120 Alcohol
Substance Abuse Diagnosis DUG 8.0 ICD-10 Code ICD-10 Description F10. Alcohol Related Disorders F10.1 Alcohol Abuse F10.10 Alcohol Abuse, Uncomplicated F10.12 Alcohol Abuse With Intoxication F10.120 Alcohol
information for service providers Schizophrenia & Substance Use
 information for service providers Schizophrenia & Substance Use Schizophrenia and Substance Use Index 2 2 3 5 6 7 8 9 How prevalent are substance use disorders among people with schizophrenia? How prevalent
information for service providers Schizophrenia & Substance Use Schizophrenia and Substance Use Index 2 2 3 5 6 7 8 9 How prevalent are substance use disorders among people with schizophrenia? How prevalent
Core Competencies for Addiction Medicine, Version 2
 Core Competencies for Addiction Medicine, Version 2 Core Competencies, Version 2, was approved by the Directors of the American Board of Addiction Medicine (ABAM) Foundation March 6, 2012 Core Competencies
Core Competencies for Addiction Medicine, Version 2 Core Competencies, Version 2, was approved by the Directors of the American Board of Addiction Medicine (ABAM) Foundation March 6, 2012 Core Competencies
DSM-5: A Comprehensive Overview
 1) The original DSM was published in a) 1942 b) 1952 c) 1962 d) 1972 DSM-5: A Comprehensive Overview 2) The DSM provides all the following EXCEPT a) Guidelines for the treatment of identified disorders
1) The original DSM was published in a) 1942 b) 1952 c) 1962 d) 1972 DSM-5: A Comprehensive Overview 2) The DSM provides all the following EXCEPT a) Guidelines for the treatment of identified disorders
Addiction Medicine for FP / GP. Dr. Francisco Ward, DABPMR/PM SetonPainRehab.com setonpr@gmail.com
 Addiction Medicine for FP / GP Dr. Francisco Ward, DABPMR/PM SetonPainRehab.com setonpr@gmail.com S Disease of Chemical Addiction Short Definition of Addiction (ASAM): Addiction is a primary, chronic disease
Addiction Medicine for FP / GP Dr. Francisco Ward, DABPMR/PM SetonPainRehab.com setonpr@gmail.com S Disease of Chemical Addiction Short Definition of Addiction (ASAM): Addiction is a primary, chronic disease
Mental Health 101 for Criminal Justice Professionals David A. D Amora, M.S.
 Mental Health 101 for Criminal Justice Professionals David A. D Amora, M.S. Director, National Initiatives, Council of State Governments Justice Center Today s Presentation The Behavioral Health System
Mental Health 101 for Criminal Justice Professionals David A. D Amora, M.S. Director, National Initiatives, Council of State Governments Justice Center Today s Presentation The Behavioral Health System
Med-QUEST Division Behavioral Health Protocol
 Attachment F Med-QUEST Division Behavioral Health Protocol I. OVERVIEW The Med-QUEST Division (MQD) is responsible for providing behavioral health to all its beneficiaries. MQD provides standard behavioral
Attachment F Med-QUEST Division Behavioral Health Protocol I. OVERVIEW The Med-QUEST Division (MQD) is responsible for providing behavioral health to all its beneficiaries. MQD provides standard behavioral
DSM IV TR Diagnostic Codes. (In Numeric Order) DSM IV Codes: Through revisions on 10.01.1996 and 10.01.2005. Code Description Code Description
 DSM IV Codes: Through revisions on 10.01.1996 and 10.01.2005. Code Description Code Description") 290.0 Dementia of the Alzheimer's type, with late onset, uncomplicated NO DSM IV TR 290 code / See codes [294.10 294.1x] 290.10A Dementia due to Creutzfeldt Jakob disease NO DSM IV TR 290.10 code / See
290.0 Dementia of the Alzheimer's type, with late onset, uncomplicated NO DSM IV TR 290 code / See codes [294.10 294.1x] 290.10A Dementia due to Creutzfeldt Jakob disease NO DSM IV TR 290.10 code / See
opiates alcohol 27 opiates and alcohol 30 April 2016 drug addiction signs 42 Ranked #1 123 Drug Rehab Centers in New Jersey 100 Top 10 380
 opiates alcohol 27 opiates and alcohol 30 April 2016 drug addiction signs 42 ed #1 123 Drug Rehab Centers in New Jersey 100 Top 10 380 effects of alcohol in the brain 100 Top 30 698 heroin addiction 100
opiates alcohol 27 opiates and alcohol 30 April 2016 drug addiction signs 42 ed #1 123 Drug Rehab Centers in New Jersey 100 Top 10 380 effects of alcohol in the brain 100 Top 30 698 heroin addiction 100
Dual diagnosis: working together
 Dual diagnosis: working together Tom Carnwath RCGP conference Birmingham 2007 DSM-IV & cocaine Cocaine intoxication Cocaine withdrawal Cocaine-induced sleep disorder Cocaine-induced sexual dysfunction
Dual diagnosis: working together Tom Carnwath RCGP conference Birmingham 2007 DSM-IV & cocaine Cocaine intoxication Cocaine withdrawal Cocaine-induced sleep disorder Cocaine-induced sexual dysfunction
SUBSTANCE USE DISORDER SOCIAL DETOXIFICATION SERVICES [ASAM LEVEL III.2-D]
![SUBSTANCE USE DISORDER SOCIAL DETOXIFICATION SERVICES [ASAM LEVEL III.2-D]](/thumbs/27/9667060.jpg "SUBSTANCE USE DISORDER SOCIAL DETOXIFICATION SERVICES [ASAM LEVEL III.2-D]") SUBSTANCE USE DISORDER SOCIAL DETOXIFICATION SERVICES [ASAM LEVEL III.2-D] I. Definitions: Detoxification is the process of interrupting the momentum of compulsive drug and/or alcohol use in an individual
SUBSTANCE USE DISORDER SOCIAL DETOXIFICATION SERVICES [ASAM LEVEL III.2-D] I. Definitions: Detoxification is the process of interrupting the momentum of compulsive drug and/or alcohol use in an individual
Prescription Drug Abuse
 Prescription Drug Abuse Introduction Most people take medicines only for the reasons their health care providers prescribe them. But millions of people around the world have used prescription drugs for
Prescription Drug Abuse Introduction Most people take medicines only for the reasons their health care providers prescribe them. But millions of people around the world have used prescription drugs for
DSM 5 Opioid Related Disorders. Dr. Phil O Dwyer Oakland University Brookfield Clinics
 DSM 5 Opioid Related Disorders Dr. Phil O Dwyer Oakland University Brookfield Clinics Cead Mile Failte Opioids A classification of drugs derived from the opium plant. Common opioids: Morphine Heroin Codeine
DSM 5 Opioid Related Disorders Dr. Phil O Dwyer Oakland University Brookfield Clinics Cead Mile Failte Opioids A classification of drugs derived from the opium plant. Common opioids: Morphine Heroin Codeine
Clinical Criteria 4.201 Inpatient Medical Withdrawal Management 4.201 Substance Use Inpatient Withdrawal Management (Adults and Adolescents)
") 4.201 Inpatient Medical Withdrawal Management 4.201 Substance Use Inpatient Withdrawal Management (Adults and Adolescents) Description of Services: Inpatient withdrawal management is comprised of services
4.201 Inpatient Medical Withdrawal Management 4.201 Substance Use Inpatient Withdrawal Management (Adults and Adolescents) Description of Services: Inpatient withdrawal management is comprised of services
RULES OF THE TENNESSEE DEPARTMENT OF MENTAL HEALTH AND DEVELOPMENTAL DISABILITIES
 RULES OF THE TENNESSEE DEPARTMENT OF MENTAL HEALTH AND DEVELOPMENTAL DISABILITIES CHAPTER 0940-05-47 MINIMUM PROGRAM REQUIREMENTS FOR ALCOHOL AND DRUG OUTPATIENT DETOXIFICATION TREATMENT FACILITIES TABLE
RULES OF THE TENNESSEE DEPARTMENT OF MENTAL HEALTH AND DEVELOPMENTAL DISABILITIES CHAPTER 0940-05-47 MINIMUM PROGRAM REQUIREMENTS FOR ALCOHOL AND DRUG OUTPATIENT DETOXIFICATION TREATMENT FACILITIES TABLE
Transitioning to ICD-10 Behavioral Health
 Transitioning to ICD-10 Behavioral Health Jeri Leong, R.N., CPC, CPC-H, CPMA Healthcare Coding Consultants of Hawaii LLC 1 Course Objectives Review of new requirements to ICD-10-CM Identify the areas of
Transitioning to ICD-10 Behavioral Health Jeri Leong, R.N., CPC, CPC-H, CPMA Healthcare Coding Consultants of Hawaii LLC 1 Course Objectives Review of new requirements to ICD-10-CM Identify the areas of
CRITERIA CHECKLIST. Serious Mental Illness (SMI)
") Serious Mental Illness (SMI) SMI determination is based on the age of the individual, functional impairment, duration of the disorder and the diagnoses. Adults must meet all of the following five criteria:
Serious Mental Illness (SMI) SMI determination is based on the age of the individual, functional impairment, duration of the disorder and the diagnoses. Adults must meet all of the following five criteria:
Comprehensive Behavioral Care, Inc. Level of Care Guidelines Substance Abuse Children/Adolescents
 Medical Necessity In considering the appropriateness of any level of care, the four basic elements of Medical Necessity should be met: 1. A diagnosis as defined by standard diagnosis nomenclatures (DSM
Medical Necessity In considering the appropriateness of any level of care, the four basic elements of Medical Necessity should be met: 1. A diagnosis as defined by standard diagnosis nomenclatures (DSM
How To Know If You Should Be Treated
 Comprehensive ehavioral Care, Inc. delivery system that does not include sufficient alternatives to a particular LOC and a particular patient. Therefore, CompCare considers at least the following factors
Comprehensive ehavioral Care, Inc. delivery system that does not include sufficient alternatives to a particular LOC and a particular patient. Therefore, CompCare considers at least the following factors
Evidence Based Approaches to Addiction and Mental Illness Treatment for Adults
 Evidence Based Practice Continuum Guidelines The Division of Behavioral Health strongly encourages behavioral health providers in Alaska to implement evidence based practices and effective program models.
Evidence Based Practice Continuum Guidelines The Division of Behavioral Health strongly encourages behavioral health providers in Alaska to implement evidence based practices and effective program models.
Residential Sub-Acute Detoxification Guidelines
 I. Background Information A. Definition of Detoxification Residential Sub-Acute Detoxification Guidelines SAMSA s TIP #45, Detoxification and Substance Abuse Treatment: Treatment Improvement Protocols
I. Background Information A. Definition of Detoxification Residential Sub-Acute Detoxification Guidelines SAMSA s TIP #45, Detoxification and Substance Abuse Treatment: Treatment Improvement Protocols
Addiction Psychiatry Fellowship Rotation Goals & Objectives
 Addiction Psychiatry Fellowship Rotation Goals & Objectives Table of Contents University Neuropsychiatric Institute (UNI) Training Site 2 Inpatient addiction psychiatry rotation.....2 Outpatient addiction
Addiction Psychiatry Fellowship Rotation Goals & Objectives Table of Contents University Neuropsychiatric Institute (UNI) Training Site 2 Inpatient addiction psychiatry rotation.....2 Outpatient addiction
Handout for. A Videotaped Lecture Produced by:
 Handout for DUAL DIAGNOSIS: An Integrated Model for the Treatment of People with Co-occurring Psychiatric and Substance Disorders in Managed Care Systems Kenneth Minkoff, M.D. A Videotaped Lecture Produced
Handout for DUAL DIAGNOSIS: An Integrated Model for the Treatment of People with Co-occurring Psychiatric and Substance Disorders in Managed Care Systems Kenneth Minkoff, M.D. A Videotaped Lecture Produced
ICD-10 Update* Mental and Behavioral Health ICD-10-CM Codes Blue Cross Blue Shield of Michigan 2014
 ICD-10 Update* Mental and Behavioral Health ICD-10-CM Codes Blue Cross Blue Shield of Michigan 2014 *NOTE: The information in this document is not intended to impart legal advice. This overview is intended
ICD-10 Update* Mental and Behavioral Health ICD-10-CM Codes Blue Cross Blue Shield of Michigan 2014 *NOTE: The information in this document is not intended to impart legal advice. This overview is intended
seeking the certification education requirements as an Addiction Counselor through either the
 180-Hour Training Series: Addiction Counselor Program The Addiction Certification Program is designed to provide the coursework necessary for those Evidence-Based & Best Practices seeking the certification
180-Hour Training Series: Addiction Counselor Program The Addiction Certification Program is designed to provide the coursework necessary for those Evidence-Based & Best Practices seeking the certification
Chapter 7. Screening and Assessment
 Chapter 7 Screening and Assessment Screening And Assessment Starting the dialogue and begin relationship Each are sizing each other up Information gathering Listening to their story Asking the questions
Chapter 7 Screening and Assessment Screening And Assessment Starting the dialogue and begin relationship Each are sizing each other up Information gathering Listening to their story Asking the questions
What s New in DSM-5 and the New ASAM Criteria?: Implications in an Era of Healthcare Reform
 What s New in DSM-5 and the New ASAM Criteria?: Implications in an Era of Healthcare Reform David Mee-Lee, M.D. Chief Editor, The ASAM Criteria Senior Vice President The Change Companies Carson City, NV
What s New in DSM-5 and the New ASAM Criteria?: Implications in an Era of Healthcare Reform David Mee-Lee, M.D. Chief Editor, The ASAM Criteria Senior Vice President The Change Companies Carson City, NV
Schizoaffective Disorder
 FACT SHEET 10 What Is? Schizoaffective disorder is a psychiatric disorder that affects about 0.5 percent of the population (one person in every two hundred). Similar to schizophrenia, this disorder is
FACT SHEET 10 What Is? Schizoaffective disorder is a psychiatric disorder that affects about 0.5 percent of the population (one person in every two hundred). Similar to schizophrenia, this disorder is
Optum By United Behavioral Health. 2015 Florida Medicaid Managed Medical Assistance (MMA) Level of Care Guidelines
 Level of Care Guidelines") Optum By United Behavioral Health 2015 Florida Medicaid Managed Medical Assistance (MMA) Level of Care Guidelines Therapeutic group care services are community-based, psychiatric residential treatment
Optum By United Behavioral Health 2015 Florida Medicaid Managed Medical Assistance (MMA) Level of Care Guidelines Therapeutic group care services are community-based, psychiatric residential treatment
CSAT s Knowledge Application Program. KAP Keys. For Clinicians
 The Role and Current Status of Patient Placement Criteria in the Treatment of Substance Use Disorders CSAT s Knowledge Application Program KAP Keys For Clinicians Based on TIP 13 The Role and Current Status
The Role and Current Status of Patient Placement Criteria in the Treatment of Substance Use Disorders CSAT s Knowledge Application Program KAP Keys For Clinicians Based on TIP 13 The Role and Current Status
Overview of DSM-5. With a Focus on Adult Disorders. Gordon Clark, MD
 Overview of DSM-5 With a Focus on Adult Disorders Gordon Clark, MD Sources include: 1. DSM-5: An Update D Kupfer & D Regier, ACP Annual Meeting, 2/21-22/13, Kauai 2. Master Course, DSM-5: What You Need
Overview of DSM-5 With a Focus on Adult Disorders Gordon Clark, MD Sources include: 1. DSM-5: An Update D Kupfer & D Regier, ACP Annual Meeting, 2/21-22/13, Kauai 2. Master Course, DSM-5: What You Need
JACKSON RECOVERY CENTERS Initial Substance Abuse Assessment Form. Substance used: Method: Age started: Last used: Frequency/progression of use:
 JACKSON RECOVERY CENTERS Initial Substance Abuse Assessment Form PRESENTING PROBLEM DRUGS OF CHOICE Substance used: Method: Age started: Last used: Frequency/progression of use: Indicators of Addiction:
JACKSON RECOVERY CENTERS Initial Substance Abuse Assessment Form PRESENTING PROBLEM DRUGS OF CHOICE Substance used: Method: Age started: Last used: Frequency/progression of use: Indicators of Addiction:
Department of Social and Health Services Division of Alcohol and Substance Abuse. WAC 388-805 Revision Recommendations Patient Placement Criteria
 Department of Social and Health Services Division of Alcohol and Substance Abuse WAC 388-805 Revision Recommendations Patient Placement Criteria April 2003 WAC 388-805 WAC 388-805-005 What definitions
Department of Social and Health Services Division of Alcohol and Substance Abuse WAC 388-805 Revision Recommendations Patient Placement Criteria April 2003 WAC 388-805 WAC 388-805-005 What definitions
Brief Review of Common Mental Illnesses and Treatment
 Brief Review of Common Mental Illnesses and Treatment Presentations to the Joint Subcommittee to Study Mental Health Services in the 21st Century September 9, 2014 Jack Barber, M.D. Medical Director Virginia
Brief Review of Common Mental Illnesses and Treatment Presentations to the Joint Subcommittee to Study Mental Health Services in the 21st Century September 9, 2014 Jack Barber, M.D. Medical Director Virginia
the Treatment Of Substance-Related Making it Real, Making it Work
 ASAM Patient Placement Criteria for the Treatment Of Substance-Related Disorders (ASAM PPC-IIr): Making it Real, Making it Work Terrence D. Walton, MSW, ICADC Director of Treatment Pretrial Services Agency
ASAM Patient Placement Criteria for the Treatment Of Substance-Related Disorders (ASAM PPC-IIr): Making it Real, Making it Work Terrence D. Walton, MSW, ICADC Director of Treatment Pretrial Services Agency
Complete List of DSM-IV Codes
 Complete List of DSM-IV Codes The following 2 tables give basic codes for all DSM-IV diagnoses. Note that the numbers are the least important part of the diagnoses: Additional verbiage, often not stated
Complete List of DSM-IV Codes The following 2 tables give basic codes for all DSM-IV diagnoses. Note that the numbers are the least important part of the diagnoses: Additional verbiage, often not stated
Conceptual Models of Substance Use
 Conceptual Models of Substance Use Different causal factors emphasized Different interventions based on conceptual models 1 Developing a Conceptual Model What is the nature of the disorder? Why causes
Conceptual Models of Substance Use Different causal factors emphasized Different interventions based on conceptual models 1 Developing a Conceptual Model What is the nature of the disorder? Why causes
DSM 5 SUBSTANCE USE DISORDERS. Ronald W. Kanwischer LCPC, CADC Professor Emeritus Department of Psychiatry SIU School of Medicine
 DSM 5 SUBSTANCE USE DISORDERS Ronald W. Kanwischer LCPC, CADC Professor Emeritus Department of Psychiatry SIU School of Medicine I have no financial relationships to disclose with regard to this presentation.
DSM 5 SUBSTANCE USE DISORDERS Ronald W. Kanwischer LCPC, CADC Professor Emeritus Department of Psychiatry SIU School of Medicine I have no financial relationships to disclose with regard to this presentation.
Professional Treatment Services in Facility-Based Crisis Program Children and Adolescents
 Professional Treatment Services in Facility-Based Crisis Program Children and Adolescents Medicaid and North Carolina Health Choice (NCHC) Billable Service WORKING DRAFT Revision Date: September 11, 2014
Professional Treatment Services in Facility-Based Crisis Program Children and Adolescents Medicaid and North Carolina Health Choice (NCHC) Billable Service WORKING DRAFT Revision Date: September 11, 2014
The purpose of this policy is to describe the criteria used by BHP in medical necessity determinations for inpatient CH treatment services.
 Page 1 of 5 Category: Code: Subject: Purpose: Policy: Utilization Management Inpatient (IP) Chemical Health (CH) Level of Care Guidelines The purpose of this policy is to describe the criteria used by
Page 1 of 5 Category: Code: Subject: Purpose: Policy: Utilization Management Inpatient (IP) Chemical Health (CH) Level of Care Guidelines The purpose of this policy is to describe the criteria used by
TRANSITIONING FROM ICD-9 to ICD-10 CODES. Presented by: Michael Langer, Office Chief, Behavioral Health and Prevention
 TRANSITIONING FROM ICD-9 to ICD-10 CODES Presented by: Michael Langer, Office Chief, Behavioral Health and Prevention September 25, 2015 2 TOPICS Coding and System Changes Understanding the ICD-10 Format
TRANSITIONING FROM ICD-9 to ICD-10 CODES Presented by: Michael Langer, Office Chief, Behavioral Health and Prevention September 25, 2015 2 TOPICS Coding and System Changes Understanding the ICD-10 Format
treatment effectiveness and, in most instances, to result in successful treatment outcomes.
 Key Elements of Treatment Planning for Clients with Co Occurring Substance Abuse and Mental Health Disorders (COD) [Treatment Improvement Protocol, TIP 42: SAMHSA/CSAT] For purposes of this TIP, co occurring
Key Elements of Treatment Planning for Clients with Co Occurring Substance Abuse and Mental Health Disorders (COD) [Treatment Improvement Protocol, TIP 42: SAMHSA/CSAT] For purposes of this TIP, co occurring
mental health-substance use
 mental health-substance use recognition and effective responses from General Practice Gary Croton Eastern Hume Dual Diagnosis Service www.dualdiagnosis.org.au This talk: 25 minutes The territory 5 minutes
mental health-substance use recognition and effective responses from General Practice Gary Croton Eastern Hume Dual Diagnosis Service www.dualdiagnosis.org.au This talk: 25 minutes The territory 5 minutes
Accessing Substance Abuse Treatment in Iowa
 Accessing Substance Abuse Treatment in Iowa Panel Discussion: Steve Estes, Fonda Frazier (MECCA) Lowell Yoder (UIHC) Overview What kinds of Substance Abuse treatment are available? How do we know who needs
Accessing Substance Abuse Treatment in Iowa Panel Discussion: Steve Estes, Fonda Frazier (MECCA) Lowell Yoder (UIHC) Overview What kinds of Substance Abuse treatment are available? How do we know who needs
Building the Evidence Based Intensive OP Service. Presenter: Thomas L. Moore Two Moons LLC LMSW, LLP, CAADC, CCS June 5 2015
 Building the Evidence Based Intensive OP Service Presenter: Thomas L. Moore Two Moons LLC LMSW, LLP, CAADC, CCS June 5 2015 # 33 Comprehensive Assessment # 30 Application of SUD Diagnosis to treatment
Building the Evidence Based Intensive OP Service Presenter: Thomas L. Moore Two Moons LLC LMSW, LLP, CAADC, CCS June 5 2015 # 33 Comprehensive Assessment # 30 Application of SUD Diagnosis to treatment
ALCOHOL RELATED DISORDERS Includes Alcohol Abuse and Alcohol Dependence; Does Not Include Alcohol Use Disorders
 1 MH 12 ALCOHOL RELATED DISORDERS Includes Alcohol Abuse and Alcohol Dependence; Does Not Include Alcohol Use Disorders Background This case definition was developed by the Armed Forces Health Surveillance
1 MH 12 ALCOHOL RELATED DISORDERS Includes Alcohol Abuse and Alcohol Dependence; Does Not Include Alcohol Use Disorders Background This case definition was developed by the Armed Forces Health Surveillance