MULTI-CASUALTY INCIDENT FIELD OPERATIONS
|
|
|
- Vanessa Garrett
- 9 years ago
- Views:
Transcription
1 California Governor s Office of Emergency Services REGION III MCI PLAN (Manual 1) MULTI-CASUALTY INCIDENT FIELD OPERATIONS Revised: April 26, 2015

2 TABLE OF CONTENTS SECTION 1: COMMAND & CONTROL... 3 A. SELECTION OF THE "TYPE" OF COMMAND... 4 B. FUNCTIONS OF THE INCIDENT COMMANDER... 5 SECTION 2: COMMUNICATIONS... 6 A. RADIO NETWORKS... 6 SECTION 3: EQUIPMENT & SUPPLIES... 7 SECTION 4: ACTIVATION/NOTIFICATION... 7 A. MOBILIZATION OF RESOURCES... 7 B. NOTIFICATION OF THE CONTROL FACILITY... 8 SECTION 5: INCIDENT OPERATIONS... 9 A. SCENE INITIATION OF ICS... 9 B. EMS FIELD MANAGEMENT PERSONNEL... 9 C. DESIGNATED AREAS D. TRIAGE E. TREATMENT F. EMS RESOURCE MANAGEMENT G TRANSPORTATION/PATIENT DISPERSAL H CONTAMINATION I. STANDING ORDERS SECTION 6: RESOURCES & ANCILLARY OPERATIONS A. DAY-TO-DAY MUTUAL AID B. MASTER MUTUAL AID C. ANCILLARY OPERATIONS SECTION 7: DOCUMENTATION A. TRIAGE TAGS B. FORMS C. MULTI-CASUALTY INCIDENT REVIEW/QUALITY IMPROVEMENT SECTION 8: TRAINING APPENDIX A: POSITION CHECKLISTS APPENDIX B: MEDICAL BRANCH MODULAR DEVELOPMENT APPENDIX C: S.T.A.R.T APPENDIX D: SAMPLE TRIAGE KIT APPENDIX E: FORMS APPENDIX F: GLOSSARY

3 PURPOSE OF THE FIELD OPERATIONS MANUAL The Field Operations Manual describes the response organization, personnel, equipment, resources, and procedures for field operations that are designed to be utilized by the thirteen counties which make up the Governor s Office of Emergency Services (OES) Region III. This plan is intended to establish a regional minimum standard. This does not prevent local agencies from developing additional protocols or procedures that do not conflict with this regional standard. The State approved Incident Command System (ICS) is used to provide the basic organizational structure for the following multi-casualty field operations manual. ICS was developed through a cooperative inter-agency (local, State and Federal) effort. The basic organizational structure of the ICS has been developed over time and is designed to coordinate the efforts of all involved agencies at the scene of a large, complex, emergency situation, as well as the small day-to-day situation. The organizational structure of ICS is designed to be developed and expanded in a modular fashion based upon the changing conditions and size/scope of the incident. Providers within this region shall be trained to the ICS 100 level, and are strongly encouraged to be trained to the ICS 200 level. This Field Operations Manual contains standardized position titles, procedures, checklists, forms, and tags in an effort to more efficiently and effectively utilize regional resources during a multicasualty incident. SEMS/NIMS Compliant Manual 1 concentrates on the field level and positions within the Standardized Emergency Management System (SEMS). In addition, this plan complies with the National Incident Management System (NIMS). 1
 is used to provide the basic organizational structure for the following multi-casualty field operations manual.")

4 INCIDENT COMMAND SYSTEM The ICS organization develops around five major functions that are required on any incident whether it is large or small. For some incidents, and in some applications, only a few of the organization's functional elements may be required. However, if there is a need to expand the organization, additional positions exist within the ICS framework to meet virtually any need. ICS establishes lines of supervisory authority and formal reporting relationships. There is complete unity of command as each position and person within the system has a designated supervisor. Direction and supervision follows established organizational lines at all times. 2

5 SECTION 1: COMMAND & CONTROL Within the ICS, the Incident Commander is that individual which holds overall responsibility for incident response and management, and shall be that individual present on scene representing the public service agency having primary investigatory authority or responsibility. Some examples are as follows: * HIGHWAY PATROL All freeways; all roadways in unincorporated areas to include right-of-way. (CVC 2454) * SHERIFF'S OFFICE Off-highway unincorporated areas, i.e., railroad right-of-ways, parks, private property, etc. (Local policy) * LOCAL FIRE/POLICE Specific areas of authority within their jurisdiction except freeways. * AIRPORT FIRE/POLICE Airports * U.S. MILITARY National Defense Area; a military reservation or an area with "military reservation status" that is temporarily under military control, e.g., military aircraft crash site. The Incident Commander has responsibility for coordination of all public and private agencies engaged at the incident site, and controls all responding agencies, such as medical, coroner staff, etc. The Incident Commander has the specific responsibility for establishing and identifying the Command Post (CP) for notifying county dispatch centers, requesting resources, and providing the initial field assessment to enable appropriate decisions regarding the level of response necessary. Jurisdictions where the City Council or other authority has assigned the function of Incident Commander to other than traffic law enforcement, i.e., fire service, that agency shall perform the incident command functions. 3
 * LOCAL FIRE/POLICE Specific areas of authority within their jurisdiction except freeways. * AIRPORT FIRE/POLICE Airports * U.S. MILITARY National Defense Area; a military reservation or an area with \"military reservation status\" that is temporarily under military control, e.")

6 A. SELECTION OF THE "TYPE" OF COMMAND The choice of type of command will usually be made based upon the number of jurisdictions involved, complexity, and size of the incident. Single Command: This is a system wherein a person determined by the impacted jurisdiction is given the lead role as Incident Commander. This person, initially, would be the most qualified official of the jurisdictional agency (ies) at the scene. In the ICS, as the incident progresses in size or scope, the incident command may be turned over to a higher ranking or more qualified official. Some incidents may require an advisory (liaison) staff to assist the Incident Commander. This will generally be comprised of officials of the major agencies involved such as fire, law enforcement, public works, and EMS. For large, complex incidents an EMS representative will be assigned by the Health Officer/EMS Medical Director or his/her designee and will normally be a member of the Health Department/Local EMS Agency or an ambulance service manager. Unified Command: This is a system where a group of officials from the major agencies involved share the lead responsibility. These officials may include fire, law enforcement, public works, and EMS. The EMS representative will again be determined by the Health Officer/EMS Medical Director or designee. 4

7 B. FUNCTIONS OF THE INCIDENT COMMANDER The Incident Commander shall be responsible for the following general functions: o Command: Overall management of the incident and setting of objectives. o Planning: The development of a procedure to deal with operational problems. o Logistics: The acquisition and distribution of resources. o Finance: Recording, for purposes of reimbursement, who and what was involved in the incident. o Operations: The direct control of tactical operations and the implementation of objectives. Depending on the size and duration of the incident, the Incident Commander may directly supervise operations or delegate this responsibility to an Operations Chief. The EMS Multi-Casualty Field Operations will fall within the responsibility of Operations. o The Incident Commander will determine when EMS personnel are no longer required and may be released from the incident, and will approve any information releases to the media. Personnel shall not release information to the media without approval. 5

8 SECTION 2: COMMUNICATIONS Communications at the incident are managed through the use of a common communications plan and an incident based communications center established solely for the use of tactical and support resources assigned to the incident. All communications between organizational elements at an incident should be in plain English or clear text. No codes should be used, and all communications should be confined only to essential messages. The Communications Unit is responsible for all communications planning at the incident. This will include incidentestablished radio networks, on-site telephone, public address, and off-incident telephone/microwave/radio systems. A. RADIO NETWORKS Radio networks for large incidents should be pre-designated, when possible, through a cooperative effort of all involved local agencies and will normally be organized as follows: Command Net - This net should link together: Incident Command, key staff members, Section Chiefs, Division and Group Supervisors. Tactical Nets - There may be several tactical nets. They may be established around agencies, departments, geographical areas, or even specific functions. The determination of how nets are set up should be a joint Planning/Operations function, and should be pre-designated whenever possible. The Communications Unit Leader will develop the plan in the event a pre-designated system is not in place. Support Nets - A support net will be established primarily to handle status-changing for resources as well as for support requests and certain other non-tactical or command functions. The scene-to-control Facility frequencies (Med-Net) fall under the categories of Support Net and, again, should be pre-designated. Ground to Air - A ground to air tactical frequency may be designated, or regular tactical nets may be used to coordinate ground to air traffic. Air to Air - Air to air nets will normally be pre-designated and assigned for use at the incident. 6

9 SECTION 3: EQUIPMENT & SUPPLIES It is imperative that all tools necessary for initial scene organization and patient triage are available to the first-in emergency response units. A Triage Kit (see Appendix D) and a minimum of two position (e.g. Triage Unit Leader & Medical Group Supervisor) vests should be carried on all initial response units. All remaining vests, Position Checklists, and the Medical Group Implementation Supplies should be carried in a supervisor/battalion vehicle which would be in the second wave dispatch to an MCI. SECTION 4: ACTIVATION/NOTIFICATION Activation of the Multi-Casualty Incident System consists of the mobilization of the necessary resources, notification of the Control Facility, and initiation of the ICS. The mobilization of resources and the notification of the Control Facility should be initiated as soon as possible to assure adequate time for the system to respond. It is not necessary to wait until emergency personnel have arrived on scene. As soon as it is determined that an emergency call may prove to be a multi-casualty incident, an additional response dispatch and Control Facility notification should occur. A. MOBILIZATION OF RESOURCES Three main categories of resources that should be considered are (E,M,T): Equipment and Supplies: - Medical Group Implementation Supplies - Medical Supply Caches/Disaster Trailers/Disaster Medical Supply Units - Rescue Equipment - Specialized Equipment Manpower: - ALS Personnel - BLS Personnel - Litter Bearers - Task Forces Transportation: - Ground Ambulances - Air Ambulances - Buses /Alternate Transport Vehicles (should be established prior to an incident, as part of an OA plan) - Ambulance Strike Teams (ALS or BLS) 7

10 B. NOTIFICATION OF THE CONTROL FACILITY Enroute The notification of the Control Facility (CF) should occur as soon as there is information that an MCI may exist. If this occurs at the time of dispatch or while responding to the incident, the CF should be contacted and advised of an "MCI Alert". Information concerning the location, approximate number of victims (if known), and a description of the incident should be given. The CF can be contacted by the dispatch center or prehospital responders. On Scene Immediately Upon Arrival (or upon confirmation of on-scene EMS first responders): Confirm or cancel MCI alert with CF. Identify location of MCI. Following Scene Size-up, Update CF on: Classification of Incident MCI Trauma Surgeon may be required for Immediate victims. MCI Medical e.g., chlorine gas inhalation or burns in which a surgeon would not be required at the receiving facility. MCI HazMat An incident requiring decontamination. Approximate number of victims. Name of incident Estimated time when triage will be completed. Following Triage, Update the CF on: Total number of patients by triage category and major injury, e.g., "A total of ten patients: 2 Immediate Heads, 4 Delayed, and 4 Minors." Number and description of transport units, e.g., "2 ALS ground ambulances, 1 BLS ground ambulance, and 1 ALS air ambulance. 8

11 SECTION 5: INCIDENT OPERATIONS A. SCENE INITIATION OF ICS Report to the IC and get permission to establish the medical group (or temporarily assume IC and establish the ICS), including: R esources: Ensure adequate resources have been ordered (Equipment, Manpower, Transportation), and clarify with IC the ordering process (i.e. can MGS order additional medical resources). Update ambulance dispatch and the Control Facility as soon as possible upon arrival. A ssignments: Assign Triage Unit Leader to begin triage. C ommunications: Determine medical tactical channel, command net, air ops (if any), etc. in cooperation with the IC. I ngress / Egress: Determine the best routes in and out of the incident with IC, and notify dispatch. N ame: Clarify incident name with IC, and notify dispatch. G eography: Quickly determine with the IC where incoming resources will stage, establish triage, treatment, transport areas. Note: The first in ambulance should generally be the last ambulance to leave the scene. Additionally, medical supplies from the first in ambulance should be used by triage/treatment units. B. EMS FIELD MANAGEMENT PERSONNEL At the time any of the following positions are assumed or assigned, it is imperative that the personnel being assigned be given: The appropriate vest for the position. The appropriate position checklist. Mode of communications to be utilized. 1. Medical Group Supervisor (MGS) This person is in charge of EMS Field Operations in an initial and reinforced level of response. While formal identification is not necessary on routine calls, on multi-casualty incidents, an identification vest will be used. The Medical Group Supervisor will report to the Incident Commander or designee. If an Incident Commander has not been established early in a multi-casualty incident, the Medical Group Supervisor will coordinate operations with fire and law enforcement until an Incident Commander is assigned. 9

12 Overall command of EMS field operations in a Full Branch Response would be delegated to the Medical Branch Director. Selection: The Medical Group Supervisor shall be the first qualified responder for the position on the scene and, in accordance with local policy, may be a law enforcement, fire department, or private provider personnel. The initial Medical Group Supervisor may be relieved or assisted by personnel more qualified for the position as they arrive. 10

13 11 FIRESCOPE- Multi-Casualty Organization Chart
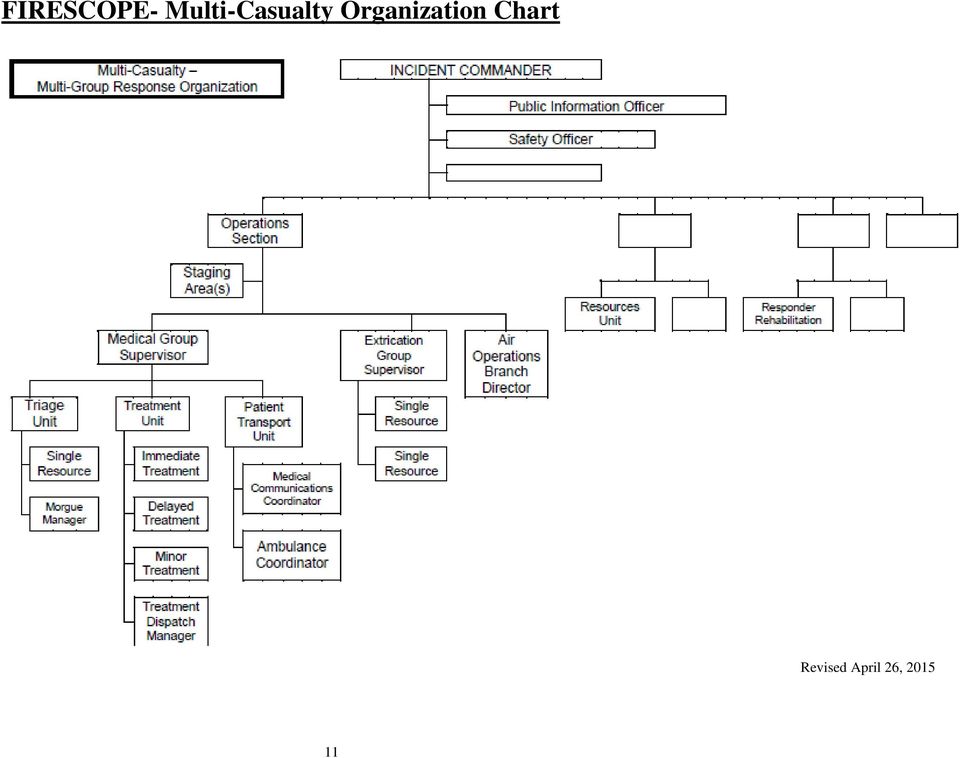
14 Function: The Medical Group Supervisor or Medical Branch Director if assigned, will be responsible for triage, treatment, and transportation in the multi-casualty incident, and should not be directly involved in patient care unless he/she is the only rescuer at the scene for extended lengths of time. The EMS field organization builds from the top down with responsibility and performance placed initially with the Medical Group Supervisor. The specific organizational structure established for any given incident will be based upon the management needs of the incident. If one individual can simultaneously manage all major functional areas, no further organization is required. If one or more of the areas require independent management, an individual should be named to be responsible for that area. In a small MCI, or in the early phases of a large MCI, the Medical Group Supervisor may also need to serve as the Triage, Treatment, and Transportation Unit Leader/Group Supervisor and coordinate communications with the Control Facility for patient dispersal. The Medical Branch Worksheet (ICS-MC-305), and the Position Checklists found in Appendix A, should be used any time it is appropriate. However, the Worksheet and Position Checklists must be used whenever more than two components of field operations have been assigned to other individuals. Personnel: The Medical Group Supervisor will appoint personnel depending upon the needs of the incident. Personnel can be placed in charge of several areas if this is the best utilization of available resources. Additional personnel may include, but are not limited to: o Triage Unit Leader o Treatment Unit Leader o Transportation Unit Leader/Group Supervisor o Medical Supply Coordinator o Medical Communications Coordinator 2. Triage Unit Leader The Triage Unit Leader (BLS level preferred) will coordinate the triage of all patients. After all patients have been triaged and tagged, this person will supervise the movement of patients to a treatment area. This person will remain at the triage area and will report to the Medical Group Supervisor. The Triage Unit Leader may assign as needed: o Triage Personnel o Morgue Manager 3. Treatment Unit Leader The Treatment Unit Leader, who reports to the Medical Group Supervisor, is responsible for on scene emergency medical care of victims in the treatment area. This person will be located at the treatment area and may assign Treatment Managers to the Immediate, Delayed, and Minor Treatment Areas as needed. The Treatment Unit Leader may also assign a Treatment Dispatch Manager to coordinate patient readiness with the Patient Transportation Unit Leader. Positions that may also be assigned are: o Treatment Dispatch Manager 12

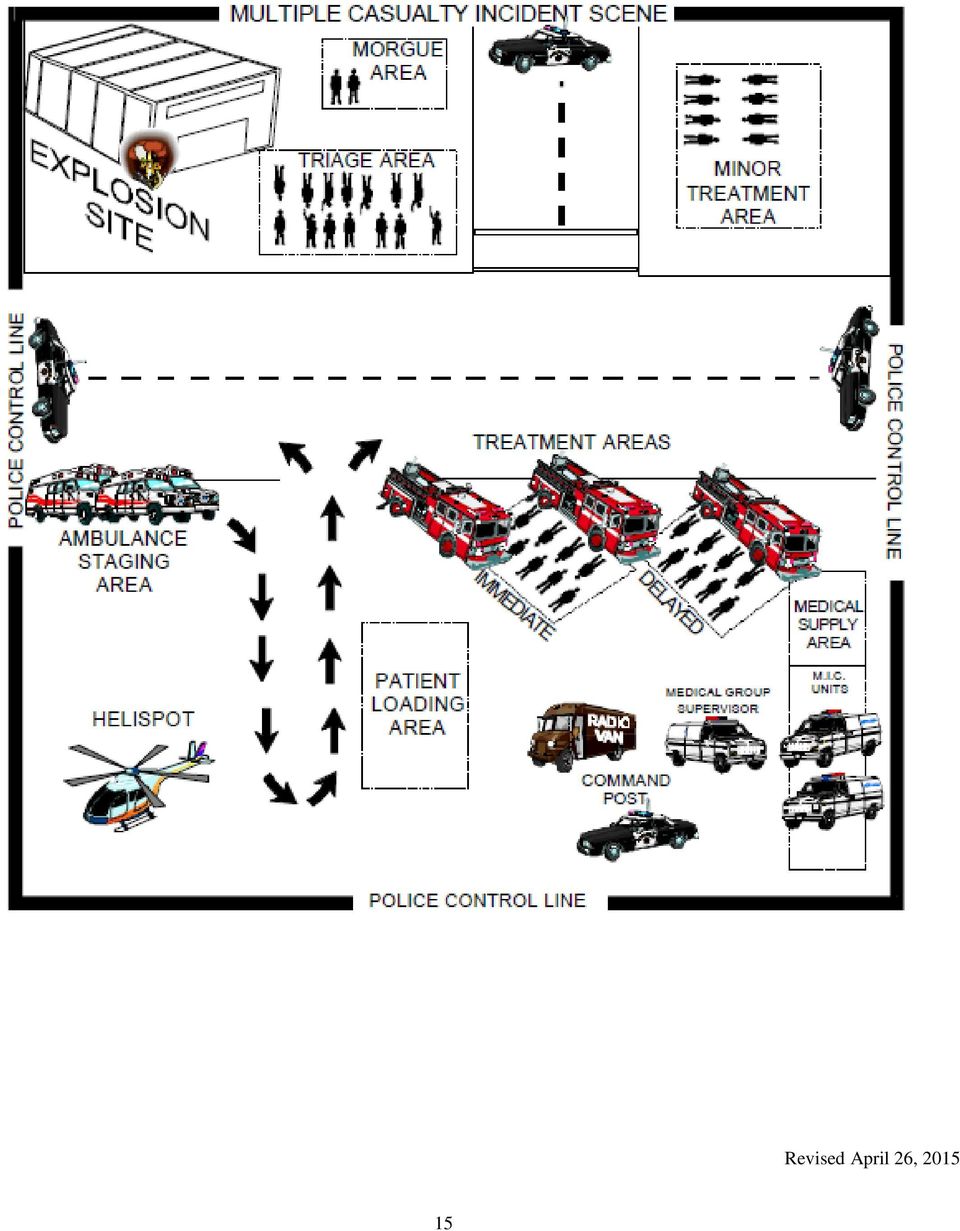
15 o Immediate Treatment Manager o Delayed Treatment Manager o Minor Treatment Manager 4. Patient Transportation Unit Leader/Group Supervisor (PTUL/PTGS) This position may be filled concurrently by the Medical Group Supervisor in the event there are not enough qualified personnel available. The Patient Transportation Unit Leader/Group Supervisor may assign the following personnel as necessary: o Medical Communications Coordinator o Ambulance Coordinator C. DESIGNATED AREAS Locations of designated areas, as detailed below shall be approved by the Incident Commander or designee. Once the location has been assigned to EMS, the Medical Group Supervisor or designee will oversee the organizing of specific areas within the agreed upon location. 1. Treatment Areas Treatment areas should be safely distanced from hazards, upwind from toxic fumes, including EMS vehicle exhaust, and allowance made for vehicle access to an adjacent loading area. There should be adequate space to lay the patients side-by-side/end-to-end and grouped by triage priority. In a small incident, if a treatment area needs to be established, a single treatment area is recommended for the Immediate and Delayed patients. The Minor patients should be grouped and treated away from all areas of active operations. In the case of large incidents or if problems with having only one treatment area develop, a treatment area may be designated for each triage category. The Immediate and Delayed treatment areas should be grouped close together and the Minor treatment area located a distance away. Remember, Immediate patients must be transported as soon as possible. Movement of these patients to a treatment area may be inappropriate if it unnecessarily delays transport. 2. EMS Staging Area This area will be the collection point for EMS personnel and equipment. A Staging Area Manager should be assigned by the IC or designee. Transport vehicles will be maintained in a one-way traffic pattern towards the loading area, if possible. Request law enforcement assistance through the Incident Commander, if a change of normal traffic pattern is necessary. If necessary, a supply cache will be established at the staging area. In a large incident, the staging area will include many other non-medical components. In this case, the Ambulance Coordinator will handle EMS resources and report to the person in charge of staging for the entire incident. EMS staging may be incorporated in a joint Staging Area if one has been established by the Operations Chief. 3. Loading Area 13

16 This area is for loading patients into transporting vehicles. The loading area should be adjacent to the treatment area(s) and in line with the one way traffic from the Staging Area. 4. Morgue Area Most MCI events may be considered crime scenes and the deceased should not be moved. A Morgue Area should be established only if it becomes necessary to remove deceased patients from the impact site, i.e., to gain access to salvageable patients. This area should be located away from the treatment area(s) and is the responsibility of the Coroner's Office/Law Enforcement. EMS personnel assistance may be required in the establishment of the field morgue. There may be instances in which it may be necessary to establish a second morgue area for victims that expire within the treatment areas if it is impractical to remove those casualties to the morgue area established at the impact site. 5. Triage Area Victims should usually be triaged where they lie. If this is not feasible due to physical or hazardous restraints, the victims may be removed to a safe area where the Triage Unit Leader or triage teams will triage, tag, or utilize optional flags. See Section 5.3 and direct litter bearers to the appropriate treatment area. 14
 and is the responsibility of the Coroner's Office/Law Enforcement.")

17 15
18 D. TRIAGE Once it has been established that the scene is safe from hazards, an initial walk through may be necessary to provide a baseline estimate of casualty figures. Initially Triage will be conducted by the first-in medical personnel. The Triage Unit leader will assign the personnel to conduct triage as needed by the size and complexity of the incident. Treatment prior to triage of all patients shall be restricted to airway establishment and hemorrhage control. CPR generally should not be initiated unless an overabundance of ALS personnel, equipment, transport units, and immediate receiving facilities exist. The Medical Group Supervisor or Triage Unit Leader is responsible for stopping CPR when not appropriate in multi-casualty situations. Initial triage should take 30 seconds or less per patient. Initial triage should be performed utilizing the S.T.A.R.T. method (see Appendix C). All providers in OES Region III should be utilizing the DMS All Risk Triage Tags. Adjustments may be necessary during re-triage and when triage is being done by higher trained personnel. Triage of patients should occur where they lie only if the area is safe. If a hazard exists, patients should be moved to a safe triage area. Patients should be triaged and tagged prior to leaving the triage area. Do not wait to triage patients until they are placed in a treatment area. This will cause confusion as the patients will have to be rearranged into triage categories. Providers may utilize triage ribbon as part of their initial triage. The appropriate ribbon color must be clearly displayed on the patient. It is recommended that providers use strips of ribbon that are approximately 2 (two) feet long, comfortably tied on an uninjured extremity. Triage Tags must be placed on all patients either when placed in the appropriate treatment area or prior to transport to ensure proper patient tracking. Triage personnel will return unused tags to the Medical Group Supervisor or Triage Unit Leader and will, at that time, be reassigned as appropriate. 1. Triage Categories Note: These can be very dynamic. A patient s condition may rapidly worsen and change categories. START is designed to be a rapid, but not thorough evaluation technique. o IMMEDIATE: (Critical, life-threatening) These patients require immediate intervention and definitive medical care. (Target field to facility transport time: within thirty (30) minutes) o DELAYED: (Serious, may be life threatening) These patients have serious injuries, and should be observed closely for decompensation. (Target field to facility transport time: within 2 hours) o MINOR: (Walking wounded, non-life or limb threatening injuries) These patients do not demonstrate serious injuries, but should be observed for changes in their 16

19 condition. (Target field to facility transport time: within 6 hours or as soon as practical) o DECEASED: (Mortally injured) These patients are deceased or not expected to survive. They may receive expectant/palliative care. E. TREATMENT Once all patients have been triaged, the Immediate patients must be transported as soon as possible. If there is going to be a delay in transport due to a lack of transportation units or a high number of victims, patients should be moved to a treatment area. The Treatment Area will be supervised by the Treatment Unit Leader (if assigned). The Treatment Unit Leader may in turn assign supervision of the various treatment areas to Treatment Manager(s). o Assign EMS personnel to specific patients or groups of patients, ensuring adequate BLS/ALS coverage to the extent possible (priority to immediate and delayed patients). Volunteer medical personnel must report to the staging area. The Transportation/Ambulance Provider will advise the Air/Ground Ambulance Coordinator, as to assignment of personnel. EMTs and EMRs should be assigned to the minor treatment area. o CPR should not be initiated unless staffing allows for immediate treatment of all immediate and delayed patients. o Re-triage every fifteen (15) minutes, if possible. If staffing allows, re-triage should be more precise than the initial S.T.A.R.T. method. 1. Immediate Once in the treatment area, a set of vital signs should be taken, vital signs recorded on the triage tag, and patients prepared for transportation. Treatment should not delay transporting immediate patients. As with all critical trauma patients, the emphasis is on the ABCs and early transport. 2. Delayed These patients should be re-triaged (assessment and vital signs) as often as manpower allows. Delayed patients may require ALS and/or BLS treatment while waiting for transportation. 3. Minor Minor patients should be kept away from all areas of active operations, including other treatment areas, morgue, and impact area (inner perimeter). These patients should receive an assessment and have vital signs taken and have triage tags applied. BLS treatment should be performed as necessary. 4. Deceased Deceased patients should be left in the position they are found, if possible. Do not separate patient from identification. If it is necessary to move deceased patients, a field morgue will be established away from the other areas and under the direction of the Coroner or Law Enforcement. Movement of deceased 17
. The Treatment Unit Leader may in turn assign supervision of the various treatment areas to Treatment Manager(s).")
20 patients shall be done only after consultation with the Coroner's Office or Law Enforcement, if possible. F. EMS RESOURCE MANAGEMENT EMS resources shall be requested through the Incident Commander/Designee or Logistic Section if developed. In a small incident, the Medical Group Supervisor and Patient Transportation Unit Leader may be allowed to directly request EMS resources, but this should not be assumed. A procedure for requesting resources should be arranged with the Incident Commander. In an incident with expanded ICS activation, resources are the responsibility of Logistics. EMS resources will be supervised by the Medical Group Supervisor. Supervision of a medical staging area may be assigned by the Incident Commander to the Patient Transportation Unit Leader/ Patient Transportation Group Supervisor, who may assign an Air/Ground Ambulance Coordinator. o All EMS personnel, equipment, and supplies shall be directed to the staging area. o Resources (personnel, equipment, etc.) will be assigned or distributed to specific tasks. They will be dispatched by the Ambulance Coordinator or the Patient Transportation Unit Leader/Group Supervisor at the request of the Medical Group Supervisor. o Transport vehicles will be maintained in a one way traffic pattern adjacent to the loading area. The Patient Transportation Unit Leader or Ground Ambulance Coordinator if assigned, may request law enforcement assistance through the Incident Commander or his/her designee if necessary to assist with traffic flow. o If possible, keep a driver with each vehicle. If drivers are needed for triage or treatment, KEYS MUST BE LEFT IN VEHICLE. o Remove equipment not necessary for transport. Create a field inventory at the staging area which can be rapidly moved to treatment area(s) as needed, e.g., backboards, stretchers, splints, oxygen, solutions, etc. G. TRANSPORTATION/PATIENT DISPERSAL Once transporting vehicles are available, patients will be moved from the treatment area to the loading area. The Patient Transportation Unit Leader/Group Supervisor will request transport vehicles from the Ambulance Coordinator as patients are ready for transport. o Vehicle loading should be maximized without jeopardizing patient care. Unless it is the only option, two immediate patients should not be transported in the same ambulance. Instead, an immediate may be transported with a delayed patient to better assure that pre-hospital staff can adequately care for patients during transport. Each patient transported must be registered in the Patient Transportation Summary Worksheet (MCM-403). See sample below. 18

21 o In a large MCI, the method of transportation for minor priority patients may be of a type that cannot be used for the transportation of Immediate and Delayed patients, i.e., buses with fixed seats. Loading of minor patients should not interfere with the loading of immediate or delayed patients and a separate loading area may be required. Minor patients can be transported in the front seat of ambulances transporting Immediate or Delayed patients if necessary. o Once prepared for transportation, the Treatment Unit Leader should notify the Patient Transportation Unit Leader/Group Supervisor of the number of patients, their triage categories, and a one word classification of their injuries, i.e., "one Immediate head and one Immediate chest." After receiving direction from the Control Facility, the Patient Transportation Unit Leader/Group Supervisor will advise the transporting units of the appropriate hospital destination. o The Patient Transportation Unit Leader/Group Supervisor should assign either the Ambulance Coordinator or a recorder to log patient names and/or triage tag numbers, unit numbers of transporting units, triage category, destination, time of transport, and ETA on a Patient Transportation Summary Worksheet as the patients are loaded for transport. H. CONTAMINATION Pre-hospital personnel must remain alert to the potential for toxic and hazardous materials at the scene of all incidents. Familiarization with the State document "Hazardous Materials Medical Management Protocols" and the Incident Command System document "Hazardous Materials Operational System Description (ICS-HM-120-1)" is essential to avoid further and unnecessary contamination of personnel/equipment. General guidelines include: o Contaminated patients and the entire area of contamination must be isolated from equipment and other personnel and the area labeled a "hot zone." An additional "warm zone" must be established around the periphery. Only personnel who have been trained in the proper use of self contained breathing apparatus and are equipped with appropriate suits should enter the hot zone. All designated areas must be established upwind from the hot zone and no one should be allowed to enter the area downwind of the hot zone unless they are equipped with self contained breathing apparatus and properly attired. Patients are usually received from the Contamination Reduction Corridor. o Accurate information on the identification and health effects of the substance and the appropriate pre-hospital evaluation and care of the victim must be obtained. o Initial decontamination must occur on scene by qualified personnel. Decontaminated patients must be properly packaged to prevent contamination of the transporting units and personnel and be transported by medical triage categories and not by level of contamination. NOTE: Transportation units other than ambulances may be needed to transport some victims with significant exposure to prevent secondary contamination and the subsequent removal from service of those ambulances. o The Control Facility should be advised of patient contamination as early as possible to assure that a properly equipped facility can accept them. 19
22 o Clearly indicate on the triage tag and field assessment form "CONTAMINATED", in addition to the specific identity of the contaminate, if known. I. STANDING ORDERS During an MCI, it is imperative that radio transmissions be kept to a minimum. Therefore, advanced life support and limited advanced life support personnel will function under standing orders. If Base Hospital contact is necessary due to extenuating circumstances, the following guidelines should be adhered to: o On-Scene: Contact should only be made following approval of the Medical Group Supervisor or Patient Transportation Unit Leader/Group Supervisor. o Enroute: o Updates with the receiving facilities should only be made if there is a clear frequency not being utilized for the incident. 20
23 SECTION 6: RESOURCES & ANCILLARY OPERATIONS A. DAY-TO-DAY MUTUAL AID During small incidents or in the initial phases of a large incident, resources should be requested utilizing the usual day-to-day mutual aid process. B. MASTER MUTUAL AID If the usual day-to-day mutual aid system will not provide adequate resources, the Master Medical Mutual Aid system should be accessed as soon as possible. Instructions for the activation of this system are outlined in CAL-EMA REGION III Medical/Health Mutual Aid Plan. C. ANCILLARY OPERATIONS Besides fire, EMS, and law enforcement agencies, the following is a list of ancillary services involved in EMS Field operations and should be involved in any local multi-casualty incident planning and training. o Dispatch Centers o Control Facilities o Receiving Facility o Local Emergency Medical Services Agencies o Local Office of Emergency Services o Local Military Establishments o Local Red Cross o Local H.A.M. Operators 21
24 SECTION 7: DOCUMENTATION Original ICS-MC & MCM FORMS for use with this manual are found in Appendix E. An Index is provided listing the most recent form number and date for each form. Position Checklist forms are found in Appendix A. A. TRIAGE TAGS Note:.OA s should utilize the DMS (Disaster Medical Services) All Risk Triage Tags to ensure uniformity across the region and improve mutual aid MCI operations Fire and EMS personnel upon arrival at the scene, will distribute tags to qualified triage personnel. The number of tags distributed should be noted to better assess the actual number of patients. 1. Triage Personnel should: o initially tag patients with the S.T.A.R.T. triage method; o attach triage tags directly to the patient, and not clothing; in a readily visible location for other responders, and avoid injured areas; o report to the Medical Group Supervisor or designee; o return unused tags and ask for further assignment. 2. Treatment Personnel should: o when the victims arrive in the treatment areas, indicate the time, date of triage, and briefly the chief complaint/major injuries; o document vital signs and times obtained on Part I of the tag; o list treatment and time administered on Part II of the tag; o assign non-medical personnel to complete patient identification section of the triage tag (name, address, phone, sex, age, weight) if possible. Re-evaluate triage as necessary. If the initial triage was categorically incorrect or is full of information, DO NOT REMOVE. Obtain a second tag, detach and discard all numbered tabs, and mark through all tag numbers on second tag. Leave all remaining tabs on the original tag. The original tag number shall remain as the patient number until the victim is hospitalized. Note on the second tag the time and reason it was attached. Once the destination facility has been determined, it will be written on the tag. The Patient Transportation Unit Leader/Group Supervisor will note the tag number on a Patient Transportation Summary Worksheet (MCM-403). Transporting personnel will note the triage tag number on the patient care record/field assessment form. This will enable information to be obtained at a later time and permit a rapid return to the incident scene. Hospital admitting personnel will use the triage tag number in the admitting process in such a means that patient information and medical records may be retrieved rapidly by the use of the triage tag number. 22
25 B. FORMS 1. Field Pre-Hospital Care Records Pre-hospital Care Records should be completed according to local policy. 2. Medical Branch Worksheet The Medical Branch Worksheet (MCM-402) is used by the Medical Group Supervisor as an organizational aid. This worksheet is an abbreviated flow chart that provides space for names of persons filling positions and a checklist for other resources to be considered. The Medical Group Supervisor must use this form whenever more than one component has been delegated to other individuals. 3. Patient Transportation Summary Worksheet This worksheet (see instructions, Appendix E) may be used by the Patient Transportation Unit Leader/Group Supervisor, Medical Communications Coordinator, Treatment Unit Leader, and Air/Ground Ambulance Coordinators to maintain an accurate status list of patients as they are moved through the system. It is used by the Medical Communications Coordinator (if assigned) to record information from the Treatment Unit regarding the status of patients ready for transport as well as to record patient destination information as directed by the Control Facility (CF). The Worksheet is also utilized by the Patient Transportation Unit Leader/Group Supervisor (PTUS/PTGS) and Ambulance Coordinator to record the transport of patients from the scene. In the event that Medical Communications Coordinator or Air/Ground Ambulance Coordinator has not been assigned, a single worksheet can be utilized by the Patient Transportation Unit Leader/Group Supervisor to record all of the above information. 4. Ambulance Staging Resource Status This status worksheet (MCM-404) should be maintained by the Ground Ambulance Coordinator to track ambulance availability and activities. Space is provided for the agency name and unit identification number, as well as their time in and out of staging. 5. Supply Receipt & Inventory Form This status form (ICS-MC-312) is used by the Medical Supply Coordinator to document supplies and equipment obtained from response agency vehicles for allocation to medical group units. C. MULTI-CASUALTY INCIDENT REVIEW/QUALITY IMPROVEMENT Copies of all multi-casualty incident forms will be forwarded to the local EMS agency by the Medical Group Supervisor within forty-eight (48) hours after the incident. The local EMS Agency may conduct an "all agency critique" of a multi-casualty incident for the purpose of improving future coordination and/or performance. An "all agency critique" will be conducted with incidents involving ten (10) or more immediate patients or a combination of fifteen (15) or more immediate and delayed patients. At 23
26 least one all-agency critique of a multi-casualty incident will be conducted every six (6) months. SECTION 8: TRAINING All providers in OES Region III should conduct regular MCI training. This training should include: Scene size up and CF notification procedures (CF notification should include incident location, incident name, type of MCI and approximate number of victims Triage Training, review of START triage procedures, RPM. This training may include regularly scheduled Triage Training Days where providers utilize Triage Tags for a certain period of time, triaging regular patient contacts Patient Tracking, ensuring all response vehicles have the appropriate Patient Tracking forms. Triage Training should incorporate patient tracking. Disaster Drills or Planned Events. These events allow MCI planning objectives to be practiced with local providers and the Control Facility. Please refer to your LEMSA MCI Plan for reporting and documentation requirements. 24
27 APPENDIX A: POSITION CHECKLISTS MEDICAL GROUP SUPERVISOR (MGS) Resources: assess need for additional resources: o Equipment: medical supplies (e.g. medical caches, backboards, litters, cots). o Manpower: FRs, EMTs, paramedics o Transportation: air/ground, vans, buses Assignments: o Establish Medical Group, assign personnel. o Direct and/or supervise on-scene personnel from agencies such as Coroner's Office, Red Cross, ambulance, etc. Communications: o Participate in Medical Branch/Operations Section planning activities. o Ensure notification of the Control Facility. Ingress/Egress: Report staging area and transport routes to dispatch. Name: Confer with IC/Ops Chief to determine incident name, report to dispatch / Control Facility. Geography: Designate Treatment Area locations. o Isolate Morgue and Minor Treatment Area from Immediate/ Delayed Treatment Areas. o Request proper security, traffic control, and access for the Medical Group work areas. TRIAGE UNIT LEADER Develop organization sufficient to handle assignment. Inform Medical Group Supervisor of resource needs. Implement triage process. o Ensure triage tags are properly applied to each victim. Coordinate movement of patients from the Triage Area to the appropriate Treatment Area. Give periodic status reports to Medical Group Supervisor, including total victim counts by triage category. Maintain security and control of the Triage Area. Establish Morgue. Maintain Unit/Activity Log (ICS Form 214). Maintain Unit/Activity Log (ICS Form 214). TREATMENT UNIT LEADER Develop organization sufficient to handle assignment. Direct and supervise Treatment Dispatch, Immediate, Delayed, & Minor Treatment Areas. Coordinate movement of patients from Triage Area to Treatment Areas with Triage Unit Leader. Request sufficient medical caches and supplies as necessary. Establish communications and coordination with Patient Transportation Unit Leader. Ensure continual triage of patients throughout Treatment Areas. Direct movement of patients to ambulance loading area(s). Give periodic status reports to Medical Group Supervisor. Maintain Unit/Activity Log (ICS Form 214) PATIENT TRANSPORTATION UNIT LEADER Ensure the establishment of communications with the Control Facility. Designate Ambulance Staging Area(s). Direct patient destinations as reported by the Medical Communications Coordinator and Control Facility. Ensure patient information and destination are recorded on the Patient Transport Worksheet. Establish communications with the Ambulance Coordinator. Request additional ambulances as required. Notify Ambulance Coordinator of ambulance requests. Coordinate requests for air ambulance transportation through the Air Operations Branch Director. Coordinate the establishment of the Air Ambulance Helispots with the Medical Branch Director and Air Operations Branch Director (if assigned). Maintain Unit/Activity Log (ICS Form 214). 25
28 MEDICAL BRANCH DIRECTOR The Medical Branch Director is responsible for the implementation of the Incident Action Plan within the Medical Branch. The Branch Director reports to the Operations Section Chief and supervises the Medical Group(s) and the Patient Transportation function (Unit or Group). Patient Transportation may be upgraded from a Unit to a Group based on the size and complexity of the incident. Review Group Assignments for effectiveness of current operations and modify as needed. Provide input to Operations Section Chief for the Incident Action Plan. Supervise Branch activities. TREATMENT AREA MANAGER Request or establish Medical Teams as necessary. Assign treatment personnel to patients received in the Treatment Area. Ensure treatment of patients triaged to the Treatment Area. Assure that patients are prioritized for transportation. Coordinate transportation of patients with Treatment Dispatch Manager. Notify Treatment Dispatch Manager of patient readiness and priority for transportation. Report to Operations Section Chief on Branch activities. Ensure that appropriate patient information is recorded. Maintain Unit/Activity Log (ICS Form 214). Maintain Unit/Activity Log (ICS Form 214) MEDICAL COMMUNICATIONS COORDINATOR Establish communications with the Control Facility. Determine and maintain current status of hospital/medical facility availability and capability. Receive basic patient information and condition from Treatment Dispatch Manager. Coordinate patient destination with the hospital alert system. Communicate patient transportation needs to Ambulance Coordinator based upon requests from Treatment Dispatch Manager. Communicate patient air ambulance transportation needs to the Air Operations Branch Director based on requests from the Treatment Area Manager(s) or Treatment Dispatch Manager. Maintain Patient Transport Worksheet. Maintain Unit/Activity Log (ICS Form 214) AMBULANCE COORDINATOR Establish appropriate staging area for ambulances. Establish routes of travel for ambulances for incident operations. Establish and maintain communications with the Air Operations Branch Director regarding Air Ambulance Transportation assignments. Establish and maintain communications with the Medical Communications Coordinator and Treatment Dispatch Manager. Provide ambulances upon request from the Medical Communications Coordinator. Assure that necessary equipment is available in the ambulance for patient needs during transportation. Establish contact with ambulance providers at the scene. Request additional transportation resources as appropriate. Provide an inventory of medical supplies available at ambulance staging area for use at the scene. Maintain records as required and Unit/Activity Log (ICS Form 214) 26
29 MEDICAL SUPPLY COORDINATOR Acquire, distribute and maintain status inventory of medical equipment and supplies within the Medical Group*. Request additional medical supplies* TREATMENT DISPATCH MANAGER Establish communications with the Immediate, Delayed, and Minor Treatment Managers. Establish communications with the Patient Transportation Unit Leader. Distribute medical supplies to Treatment and Triage Units. Verify that patients are prioritized for transportation. Maintain Unit/Activity Log (ICS Form 214). *If the Logistics Section is established, this position would coordinate with the Logistics Section Chief or Supply Unit Leader. Advise Medical Communications Coordinator of patient readiness and priority for transport. Coordinate transportation of patients with Medical Communications Coordinator. Assure that appropriate patient tracking information is recorded. Coordinate ambulance loading with the Treatment Managers and ambulance personnel. Maintain Unit/Activity Log (ICS Form 214) MORGUE MANAGER Assess resource/supply needs and order as needed. Coordinate all Morgue Area activities. Keep area off limits to all but authorized personnel. Coordinate with law enforcement and assist the Coroner or Medical Examiner representative. Keep identity of deceased persons confidential. Maintain appropriate records. 27
30 APPENDIX B: MEDICAL BRANCH MODULAR DEVELOPMENT (THIS PAGE INTENTIONALLY LEFT BLANK) 28
31 29

32 30
33 31
34 APPENDIX C: S.T.A.R.T 32
35 APPENDIX D: SAMPLE TRIAGE KIT The following list is a recommended inventory of MCI supplies to be carried on each first response vehicle, including fire fighting vehicles, ambulances and where appropriate, law enforcement vehicles. Equipment should be kept in a readily accessible location within the vehicle, preferably accessible from the cab. 2 ea MCI position vests for Triage and Medical Group Supervisor positions 1ea 30ea 2ea 1ea 1ea 1ea 1roll 2ea 1ea 1ea Position Checklist for the following positions Medical Group Supervisor Medical Communications Coordinator Triage Unit Leader Treatment Area Leader Patient Transportation Unit Leader Medical Supply Coordinator DMS All Risk START Triage Tags (must meet OA/LEMSA requirement for content and quantity) Grease pencils, ball point pins Trauma Shears Clipboard (consider small dry erase clipboard with markers) START Triage reference sheet Barrier Tape Glow Sticks Folio or gear bag for contents CF Communications Plan 2 ea Forms: Medical Branch Worksheet Patient Transportation Summary Worksheet Ambulance Staging Resources Medical Supply Receipt/Inventory 33
36 APPENDIX E: FORMS (THIS PAGE INTENTIONALLY LEFT BLANK) 34
37 MEDICAL BRANCH WORKSHEET INCIDENT NAME DATE TIME INCIDENT COMMANDER MEDICAL BRANCH DIRECTOR MEDICAL GROUP/ DIVISION SUPERVISOR MEDICAL SUPPLY COORDINATOR TRIAGE UNIT LEADER TRIAGE PERSONNEL TREATMENT UNIT LEADER IMMEDIATE TREATMENT MANAGER TRANSPORT UNIT LEADER MEDICAL COMMUNICATIONS COORDINATOR MORGUE MANAGER DELAYED TREATMENT MANAGER AMBULANCE COORDINATOR MINOR TREATMENT MANAGER TREATMENT DISPATCH MANAGER OTHER MEDICAL CACHES AIR AMBULANCES LAW ENFORCEMENT RADIO FREQUENCIES CORONER RED CROSS CHAPLAIN BUSES MENTAL HEALTH ICS-MC
38 AMBULANCE STAGING RESOURCES STATUS 1. INCIDENT NAME 2. DATE PREPARED AGENCY UNIT NUMBER TIME IN STAGING AREA 3. TIME PREPARED TIME OUT STAGING AREA ALS BLS : : ALS BLS : : ALS BLS : : ALS BLS : : ALS BLS : : ALS BLS : : ALS BLS : : ALS BLS : : ALS BLS : : ALS BLS : : ALS BLS : : ALS BLS : : ALS BLS : : ALS BLS : : ALS BLS : : ALS BLS : : 36
39 MEDICAL SUPPLY RECEIPT AND INVENTORY FORM INCIDENT NAME INCIDENT NUMBER INCIDENT COMMANDER MEDICAL BRANCH DIRECTOR A. Supplies / Equipment received from: DATE: / / Agency: Unit I.D. Name: (whenever possible, use masking tape and markers to identify all equipment) B. Supplies / Equipment received by: NAME: INCIDENT POSITION: No. Item Description (PRINT all entries) Unit* Amount *Unit - list a measurable description of the item (gauge, gm, ml, bag, doz., etc.) Form distribution: Original - Medical Supply Coordinator, Copy - Source of Supply INCIDENT RE-IMBURSEMENT OF ANY SUPPLIES/EQUIPMENT WILL BE BASED ONLY UPON ORIGINAL FORM LISTINGS. I-MC
40 38
41 APPENDIX F: GLOSSARY MULTI-CASUALTY OPERATIONS GLOSSARY ALS (Advanced Life Support) - Allowable procedures and techniques utilized by PARAMEDIC and Advanced EMT- personnel to stabilize critically sick and injured patient(s) which exceed Basic Life Support procedures. BLS (Basic Life Support) - Basic non-invasive first-aid procedures and techniques utilized by PARAMEDIC, Advanced EMT, EMT, and EMR personnel to stabilize critically sick and injured patient(s). Delayed Treatment - Second priority in patient treatment. These people require rapid aid, but injuries are less severe than immediate victims. EMR- Emergency Medical Responder - An individual trained in Basic Life Support and who has a current and valid EMR certificate in the State of California. EMT (Emergency Medical Technician) - An individual trained in Basic Life Support according to the standards prescribed by the Health and Safety Code and who has a current and valid EMT certificate in the State of California issued pursuant to the Health and Safety Code. AEMT (Advanced Emergency Medical Technician) - An individual with additional training in limited Advanced Life Support according to the standards prescribed by the Health and Safety Code and who has a current and valid certificate issued pursuant to the Health and Safety Code. Paramedic - An individual who has received additional training in Advanced Life Support according to the Health and Safety Code and who has a current and valid State Paramedic License issued pursuant to the Health and Safety Code. Hospital Alert System - A communications system between medical facilities and on-incident medical personnel, which provides available hospital patient receiving capability and/or medical control. Hospital Emergency Response Teams (HERT) - Prearranged hospital teams that respond to the incident upon request. Immediate Treatment - A patient who requires rapid assessment and medical intervention for survival. Qualified - A person meeting the certification and/or requirements established by the agency that has jurisdiction over the incident. Team - Combinations of medical trained personnel who are responsible for on scene patient treatment. Supply Cache - A cache consists of standardized medical supplies and equipment stored in a predetermined location for dispatch to incidents. MICU - Mobile Intensive Care Unit refers to a paramedic equipped vehicle. It would include drugs, medications, cardiac monitors and telemetry, and other specialized emergency medical equipment. Minor Treatment - These patients injuries require simple rudimentary first-aid, and are ambulatory. Morgue (Temporary on Incident) - Area designated for temporary placement of the dead. The Morgue is the responsibility of the Coroner's Office when a Coroner's representative is on scene. 39
42 Multi-Casualty Incident - The combination of numbers of injured personnel and type of injuries going beyond capability of an entity's normal first response. Patient Transportation Recorder - Supervised by the Patient Transportation Unit Leader/Group Supervisor. Responsible for recording pertinent information regarding off-incident transportation of patients. START - S.T.A.R.T. - Acronym for Simple Triage And Rapid Treatment. This is the initial triage system that has been adopted for use by the California Fire Chiefs' Association. Standing Orders - Policies and Procedures approved by the local EMS Agency for use by an EMT, Advanced EMT, or PARAMEDIC in situations where direct voice contact with a Base Hospital cannot be established or maintained. Triage - The screening and classification of sick, wounded, or injured persons to determine priority needs in order to ensure the efficient use of medical manpower, equipment, and facilities. Triage Personnel - Personnel responsible for performing triage on patients at the scene of an incident, and assigning them to an appropriate Treatment Area. Triage Tag - A tag used by triage personnel to identify and document the patient's medical condition. 40
Marin County EMS Agency. Attachment B Position Checklists
 Marin County EMS Agency Multiple Patient Management Plan Attachment B s Excellent Care Every Patient, Every Time April 2015 *Denotes Marin Specific Additions Medical Group Incident Commander "IC" Operations
Marin County EMS Agency Multiple Patient Management Plan Attachment B s Excellent Care Every Patient, Every Time April 2015 *Denotes Marin Specific Additions Medical Group Incident Commander "IC" Operations
STANDARD OPERATING PROCEDURES. Rapidly establish triage, treatment and transportation of multiple field casualties.
 EMERGENCY MEDICAL SERVICE SOP #: Category: Mass Casualty Incidents Date: January 1, 2010 I. Purpose: STANDARD OPERATING PROCEDURES Rapidly establish triage, treatment and transportation of multiple field
EMERGENCY MEDICAL SERVICE SOP #: Category: Mass Casualty Incidents Date: January 1, 2010 I. Purpose: STANDARD OPERATING PROCEDURES Rapidly establish triage, treatment and transportation of multiple field
SAN LUIS OBISPO COUNTY EMERGENCY MEDICAL SERVICES AGENCY PREHOSPITAL POLICY
 SAN LUIS OBISPO COUNTY EMERGENCY MEDICAL SERVICES AGENCY PREHOSPITAL POLICY Policy Reference No: 214 [01/10/2013] Formerly Policy No: 126 Effective Date: 03/01/2013 Supersedes: 10/01/2008 Review Date:
SAN LUIS OBISPO COUNTY EMERGENCY MEDICAL SERVICES AGENCY PREHOSPITAL POLICY Policy Reference No: 214 [01/10/2013] Formerly Policy No: 126 Effective Date: 03/01/2013 Supersedes: 10/01/2008 Review Date:
COUNTY OF LOS ANGELES FIRE DEPARTMENT CONTEXT TRAINING PROGRAM MULTI-CASUALTY INCIDENT OPERATIONAL PLAN
 3 INTRODUCTION MULTI-CASUALTY INCIDENT OPERATIONAL PLAN It is the intent of this plan to provide a system for managing large number of patients at a Multi-Casualty Incident (MCI). The main focus of the
3 INTRODUCTION MULTI-CASUALTY INCIDENT OPERATIONAL PLAN It is the intent of this plan to provide a system for managing large number of patients at a Multi-Casualty Incident (MCI). The main focus of the
TABLE OF CONTENTS 19. ANNEX M... 19-1
 TABLE OF CONTENTS 19. ANNEX M... 19-1 19.1 PURPOSE...19-1 19.2 SITUATION AND ASSUMPTIONS...19-1 19.2.1 SITUATION...19-1 19.2.2 ASSUMPTIONS...19-1 19.3 GENERAL PROCEDURES AND RESPONSIBILITIES... 19-1 19.3.1
TABLE OF CONTENTS 19. ANNEX M... 19-1 19.1 PURPOSE...19-1 19.2 SITUATION AND ASSUMPTIONS...19-1 19.2.1 SITUATION...19-1 19.2.2 ASSUMPTIONS...19-1 19.3 GENERAL PROCEDURES AND RESPONSIBILITIES... 19-1 19.3.1
MASS CASUALTY INCIDENT PLAN
 MASS CASUALT INCIDENT PLAN Adopted by the Marion County Fire Defense Board April 2001 CONTENTS A. Introduction 1 B. Procedures 1. Incident Command 1 2. Hazmat Exposure 2 3. Medical Resource Hospital 3
MASS CASUALT INCIDENT PLAN Adopted by the Marion County Fire Defense Board April 2001 CONTENTS A. Introduction 1 B. Procedures 1. Incident Command 1 2. Hazmat Exposure 2 3. Medical Resource Hospital 3
MODOC OPERATIONAL AREA MULTI-CASUALTY AND MEDICAL EMERGENCY PLAN
 MODOC OPERATIONAL AREA MULTI-CASUALTY AND MEDICAL EMERGENCY PLAN Prepared by E. Dan Bouse and Nancy C. Ballard Modoc County Office of Emergency Services In cooperation with the Modoc County Disaster Council
MODOC OPERATIONAL AREA MULTI-CASUALTY AND MEDICAL EMERGENCY PLAN Prepared by E. Dan Bouse and Nancy C. Ballard Modoc County Office of Emergency Services In cooperation with the Modoc County Disaster Council
SIERRA-SACRAMENTO VALLEY EMS AGENCY PROGRAM POLICY REFERENCE NO. 450
 SIERRA-SACRAMENTO VALLEY EMS AGENCY PROGRAM POLICY REFERENCE NO. 450 PURPOSE: To establish minimum standards for the integration of EMS aircraft and flight personnel into the EMS prehospital patient transport
SIERRA-SACRAMENTO VALLEY EMS AGENCY PROGRAM POLICY REFERENCE NO. 450 PURPOSE: To establish minimum standards for the integration of EMS aircraft and flight personnel into the EMS prehospital patient transport
MODULE III PLANNING &TRIAGE
 MODULE III PLANNING &TRIAGE PLANNING By failing to prepare, you are preparing to fail Benjamin Franklin OBJECTIVES Discuss the components of disaster planning Review the levels of planning Discuss the
MODULE III PLANNING &TRIAGE PLANNING By failing to prepare, you are preparing to fail Benjamin Franklin OBJECTIVES Discuss the components of disaster planning Review the levels of planning Discuss the
SEMS/NIMS MANAGEMENT SYSTEM REVISED SEPTEMBER 2007
 SEMS/NIMS MANAGEMENT SYSTEM REVISED SEPTEMBER 2007 SEMS/NIMS - SYSTEM (ICS) is the model tool for command, control, and coordination of a response and provides a means to coordinate the efforts of individual
SEMS/NIMS MANAGEMENT SYSTEM REVISED SEPTEMBER 2007 SEMS/NIMS - SYSTEM (ICS) is the model tool for command, control, and coordination of a response and provides a means to coordinate the efforts of individual
Mass Causality Incident Response Plan
 Robert McMahon Commissioner Putnam County BUREAU OF EMERGENCY SERVICES Adam B. Stiebeling Deputy Commissioner Thomas C. Lannon, Sr., Director Emergency Management Robert Cuomo, Director Emergency Medical
Robert McMahon Commissioner Putnam County BUREAU OF EMERGENCY SERVICES Adam B. Stiebeling Deputy Commissioner Thomas C. Lannon, Sr., Director Emergency Management Robert Cuomo, Director Emergency Medical
SOUTH WORCESTER COUNTY COMMUNICATIONS CENTER PUBLIC SAFETY TELECOMMUNICATOR POSITION DESCRIPTION
 SOUTH WORCESTER COUNTY COMMUNICATIONS CENTER PUBLIC SAFETY TELECOMMUNICATOR POSITION DESCRIPTION POSITION: PUBLIC SAFETY TELECOMMUNICATOR DISPATCHER JOB STATUS: CIVILIAN EMPLOYEE GENERAL STATEMENT OF DUTIES
SOUTH WORCESTER COUNTY COMMUNICATIONS CENTER PUBLIC SAFETY TELECOMMUNICATOR POSITION DESCRIPTION POSITION: PUBLIC SAFETY TELECOMMUNICATOR DISPATCHER JOB STATUS: CIVILIAN EMPLOYEE GENERAL STATEMENT OF DUTIES
M.I.E.M.S.S. REGION V ALERT STATUS SYSTEM
 M.I.E.M.S.S. REGION V ALERT STATUS SYSTEM Approved by the Maryland Region V EMS Advisory Council January 28, 1999 Amended November 16, 2000 Reprinted with Corrections January 16, 2001 Note: Patients destined
M.I.E.M.S.S. REGION V ALERT STATUS SYSTEM Approved by the Maryland Region V EMS Advisory Council January 28, 1999 Amended November 16, 2000 Reprinted with Corrections January 16, 2001 Note: Patients destined
MASS CASUALTY INCIDENT (MCI)
") MASS CASUALTY INCIDENT (MCI) AN OVERVIEW Atlanta bus crash (internet photo) wikimedia.org Jim Thomas, Captain EMT-B, EMSI, FF2, FSI, FI As emergency responders, we all respond to hundreds of emergency
MASS CASUALTY INCIDENT (MCI) AN OVERVIEW Atlanta bus crash (internet photo) wikimedia.org Jim Thomas, Captain EMT-B, EMSI, FF2, FSI, FI As emergency responders, we all respond to hundreds of emergency
SPU SHOOTING MCI. 3467 3 Avenue W. Incident #14-0058018 June 5, 2014. Incident # 14-0058018
 SPU SHOOTING MCI 3467 3 Avenue W. Incident #14-0058018 June 5, 2014 Incident # 14-0058018 This page intentionally left blank. Incident # 14-0058018 2 From the Desk of the Assistant Chief of Operations
SPU SHOOTING MCI 3467 3 Avenue W. Incident #14-0058018 June 5, 2014 Incident # 14-0058018 This page intentionally left blank. Incident # 14-0058018 2 From the Desk of the Assistant Chief of Operations
INCIDENT COMMAND SYSTEM MULTI-CASUALTY POSITION MANUAL AIR AMBULANCE COORDINATOR ICS-MC-222-9. December, 1991
 INCIDENT COMMAND SYSTEM MULTI-CASUALTY POSITION MANUAL AIR AMBULANCE COORDINATOR December, 1991 Revised March, 1993 CONTENTS 1.1 CHECKLIST USE...1 1.2 AIR AMBULANCE COORDINATOR S CHECKLIST...1 2.1 RESPONSIBILITIES...2
INCIDENT COMMAND SYSTEM MULTI-CASUALTY POSITION MANUAL AIR AMBULANCE COORDINATOR December, 1991 Revised March, 1993 CONTENTS 1.1 CHECKLIST USE...1 1.2 AIR AMBULANCE COORDINATOR S CHECKLIST...1 2.1 RESPONSIBILITIES...2
H Functional Annex Emergency Medical Services Resource Management
 H Functional Annex Emergency Medical Services Resource Management Approved (April 20, 2007) This page left blank intentionally Table of Contents 1 Purpose... 3 2 Situation and Assumptions... 3 2.1 Situation...
H Functional Annex Emergency Medical Services Resource Management Approved (April 20, 2007) This page left blank intentionally Table of Contents 1 Purpose... 3 2 Situation and Assumptions... 3 2.1 Situation...
INCIDENT COMMAND SYSTEM MULTI-CASUALTY POSITION MANUAL PATIENT TRANSPORTATION GROUP SUPERVISOR ICS-MC-222-2 DECEMBER, 1989
 INCIDENT COMMAND SYSTEM MULTI-CASUALTY POSITION MANUAL PATIENT TRANSPORTATION GROUP SUPERVISOR DECEMBER, 1989 Revised March, 1993 CONTENTS Page 1.1 CHECKLIST USE...1 1.2 PATIENT TRANSPORTATION GROUP SUPERVISOR'S
INCIDENT COMMAND SYSTEM MULTI-CASUALTY POSITION MANUAL PATIENT TRANSPORTATION GROUP SUPERVISOR DECEMBER, 1989 Revised March, 1993 CONTENTS Page 1.1 CHECKLIST USE...1 1.2 PATIENT TRANSPORTATION GROUP SUPERVISOR'S
TEPP Planning Products Model Procedure
 TEPP Planning Products e for Properly Handling and Packaging Potentially Radiologically 02B00215-13.p65 Prepared for the Department of Energy Office of Transportation and Emergency Management table of
TEPP Planning Products e for Properly Handling and Packaging Potentially Radiologically 02B00215-13.p65 Prepared for the Department of Energy Office of Transportation and Emergency Management table of
BROOME COUNTY EMERGENCY MEDICAL SERVICES SYSTEM HAZARDOUS MATERIALS INCIDENT RESPONSE PLAN
 BROOME COUNTY EMERGENCY MEDICAL SERVICES SYSTEM HAZARDOUS MATERIALS INCIDENT RESPONSE PLAN Revised: December 2008 I. Introduction Hazardous materials in Broome County are found both at fixed facilities,
BROOME COUNTY EMERGENCY MEDICAL SERVICES SYSTEM HAZARDOUS MATERIALS INCIDENT RESPONSE PLAN Revised: December 2008 I. Introduction Hazardous materials in Broome County are found both at fixed facilities,
FIRE AND RESCUE DEPARTMENTS OF NORTHERN VIRGINIA FIREFIGHTING AND EMERGENCY OPERATIONS MANUAL. EMS Multiple Casualty Incident Manual.
 FIRE AND RESCUE DEPARTMENTS OF NORTHERN VIRGINIA FIREFIGHTING AND EMERGENCY OPERATIONS MANUAL EMS Multiple Casualty Incident Manual Second Edition Issued: August 2008 Revised: May 2013 ACKNOWLEDGEMENTS
FIRE AND RESCUE DEPARTMENTS OF NORTHERN VIRGINIA FIREFIGHTING AND EMERGENCY OPERATIONS MANUAL EMS Multiple Casualty Incident Manual Second Edition Issued: August 2008 Revised: May 2013 ACKNOWLEDGEMENTS
Administrative Policy 5201
 Administrative Policy 5201 Effective April 1, 2015 Expires March 31, 2016 Policy: EMS Aircraft Operations, Equipment, and... Approval: REMSA Medical Director Daved van Stralen, MD Signed Applies To: FR,
Administrative Policy 5201 Effective April 1, 2015 Expires March 31, 2016 Policy: EMS Aircraft Operations, Equipment, and... Approval: REMSA Medical Director Daved van Stralen, MD Signed Applies To: FR,
Module Two: EMS Systems. Wisconsin EMS Medical Director s Course
 : EMS Systems Wisconsin EMS Medical Director s Course Objectives List the components of EMS systems Outline organizational and design options for EMS systems Outline system staffing and response configurations
: EMS Systems Wisconsin EMS Medical Director s Course Objectives List the components of EMS systems Outline organizational and design options for EMS systems Outline system staffing and response configurations
Chisholm Trail Fire/Rescue First Responder Organization Standard Operating Procedures/Guidelines
 Chisholm Trail Fire/Rescue First Responder Organization Standard Operating Procedures/Guidelines Mission: Respond to emergency requests to provide prehospital care to the sick and injured. Personnel: Shall
Chisholm Trail Fire/Rescue First Responder Organization Standard Operating Procedures/Guidelines Mission: Respond to emergency requests to provide prehospital care to the sick and injured. Personnel: Shall
COUNTY OF KERN EMERGENCY MEDCAL SERVICES DEPARTMENT. EMS Aircraft Dispatch-Response-Utilization Policies & Procedures
 COUNTY OF KERN EMERGENCY MEDCAL SERVICES DEPARTMENT Final - May 2, 2002 Russ Blind Interim Director Robert Barnes, M.D. Medical Director TABLE OF CONTENTS Section: Topic: Page #: I. Definitions 3-4 II.
COUNTY OF KERN EMERGENCY MEDCAL SERVICES DEPARTMENT Final - May 2, 2002 Russ Blind Interim Director Robert Barnes, M.D. Medical Director TABLE OF CONTENTS Section: Topic: Page #: I. Definitions 3-4 II.
Operations Modified On:Nov 24, 2010 12:37
 NOTE: EMS Aircraft utilized in Alameda County for prehospital emergency care will meet the qualifications specified in Title 22, Chapter 8. 1. DEFINITIONS 1.1 "EMS Aircraft" any aircraft utilized for the
NOTE: EMS Aircraft utilized in Alameda County for prehospital emergency care will meet the qualifications specified in Title 22, Chapter 8. 1. DEFINITIONS 1.1 "EMS Aircraft" any aircraft utilized for the
Search & Rescue Merit Badge
 FEMA Course IS-100b Introduction to the Incident Command System for Search & Rescue Merit Badge Visual 1.1 Search & Rescue Merit Badge (requirement #5) Complete the training for ICS-100, Introduction to
FEMA Course IS-100b Introduction to the Incident Command System for Search & Rescue Merit Badge Visual 1.1 Search & Rescue Merit Badge (requirement #5) Complete the training for ICS-100, Introduction to
Submitted By Dutchess County Emergency Response Coordinator John Murphy Date:
 THE DUTCHESS COUNTY OFFICE OF EMERGENCY RESPONSE FIRE ~ RESCUE ~ EMS MUTUAL AID PLAN FOR THE COUNTY OF DUTCHESS RECOMMENDED FOR ADOPTION BY: DUTCHESS COUNTY FIRE AND SAFETY ADVISORY BOARD ORIGINAL DATED
THE DUTCHESS COUNTY OFFICE OF EMERGENCY RESPONSE FIRE ~ RESCUE ~ EMS MUTUAL AID PLAN FOR THE COUNTY OF DUTCHESS RECOMMENDED FOR ADOPTION BY: DUTCHESS COUNTY FIRE AND SAFETY ADVISORY BOARD ORIGINAL DATED
EMERGENCY MANAGEMENT ORGANIZATION
 VI. EMERGENCY MANAGEMENT ORGANIZATION General 1. The overall responsibility for emergency preparedness rests with government on all levels, including all agencies of state, county and city in coordination
VI. EMERGENCY MANAGEMENT ORGANIZATION General 1. The overall responsibility for emergency preparedness rests with government on all levels, including all agencies of state, county and city in coordination
BOSTON MEDFLIGHT HELICOPTER CRASH INCIDENT
 I. PURPOSE BOSTON MEDFLIGHT HELICOPTER CRASH INCIDENT To provide guidance and procedures for emergency response to a Boston MedFlight helicopter crash at Boston University Medical Center. II. SITUATION
I. PURPOSE BOSTON MEDFLIGHT HELICOPTER CRASH INCIDENT To provide guidance and procedures for emergency response to a Boston MedFlight helicopter crash at Boston University Medical Center. II. SITUATION
ICS 100 Intro to Incident Command System. Crawford County Volunteer Unit Training Session
 ICS 100 Intro to Incident Command System Crawford County Volunteer Unit Training Session Course Objective Demonstrate basic knowledge of the Incident Command System (ICS) What is ICS? A standardized, on
ICS 100 Intro to Incident Command System Crawford County Volunteer Unit Training Session Course Objective Demonstrate basic knowledge of the Incident Command System (ICS) What is ICS? A standardized, on
INCIDENT COMMAND SYSTEM MULTI-CASUALTY POSITION MANUAL GROUND AMBULANCE COORDINATOR ICS-MC-222-8 DECEMBER, 1991
 INCIDENT COMMAND SYSTEM MULTI-CASUALTY POSITION MANUAL GROUND AMBULANCE COORDINATOR DECEMBER, 1991 Revised March, 1993 CONTENTS 1.1 CHECKLIST USE...1 1.2 GROUND AMBULANCE COORDINATOR'S CHECKLIST...1 2.1
INCIDENT COMMAND SYSTEM MULTI-CASUALTY POSITION MANUAL GROUND AMBULANCE COORDINATOR DECEMBER, 1991 Revised March, 1993 CONTENTS 1.1 CHECKLIST USE...1 1.2 GROUND AMBULANCE COORDINATOR'S CHECKLIST...1 2.1
Part III. Supporting Documents. Standardized Emergency Management System (SEMS) Glossary of Terms
 Glossary of Terms") Standardized Emergency Management System (SEMS) Glossary of Terms INTRODUCTION The Glossary contains definitions of terms commonly used in the Standardized Emergency Management System (SEMS). The Glossary
Standardized Emergency Management System (SEMS) Glossary of Terms INTRODUCTION The Glossary contains definitions of terms commonly used in the Standardized Emergency Management System (SEMS). The Glossary
ARKANSAS STATE BOARD OF HEALTH DIVISION OF EMERGENCY MEDICAL SERVICES AND TRAUMA SYSTEMS RULES AND REGULATIONS FOR MASS CASUALTY INCIDENTS
 ARKANSAS STATE BOARD OF HEALTH DIVISION OF EMERGENCY MEDICAL SERVICES AND TRAUMA SYSTEMS RULES AND REGULATIONS FOR MASS CASUALTY INCIDENTS Promulgated Under the Authority of Act 1255 OF 1997 Effective
ARKANSAS STATE BOARD OF HEALTH DIVISION OF EMERGENCY MEDICAL SERVICES AND TRAUMA SYSTEMS RULES AND REGULATIONS FOR MASS CASUALTY INCIDENTS Promulgated Under the Authority of Act 1255 OF 1997 Effective
Typed Resource Definitions Emergency Medical Services Resources
 Typed Resource Definitions Emergency Medical Services Resources FEMA 508-3 (March 2009) Background Resource Typing Web Site Supersedure Changes The National Mutual Aid and Resource Management Initiative
Typed Resource Definitions Emergency Medical Services Resources FEMA 508-3 (March 2009) Background Resource Typing Web Site Supersedure Changes The National Mutual Aid and Resource Management Initiative
San Benito County Emergency Medical Services Agency
 San Benito County Emergency Medical Services Agency Policy : 1060 Effective : May 1, 2014 Reviewed : April 1, 2014 Air Medical Services I. Purpose To authorize a standard of operation for Air Medical Services
San Benito County Emergency Medical Services Agency Policy : 1060 Effective : May 1, 2014 Reviewed : April 1, 2014 Air Medical Services I. Purpose To authorize a standard of operation for Air Medical Services
The Massachusetts Emergency Medical Services (EMS) Mass Casualty Incident (MCI) Plan
 Mass Casualty Incident (MCI) Plan") The Massachusetts Emergency Medical Services (EMS) Mass Casualty Incident (MCI) Plan January 11, 2016 1 Contact for Questions Please direct any questions about this MCI Plan to: Department of Public Health
The Massachusetts Emergency Medical Services (EMS) Mass Casualty Incident (MCI) Plan January 11, 2016 1 Contact for Questions Please direct any questions about this MCI Plan to: Department of Public Health
ICS ORIENTATION Saskatchewan
 INCIDENT COMMAND SYSTEM Canadian Version CANADIAN NATIONAL TRAINING CURRICULUM ICS ORIENTATION Saskatchewan Module 1 I - 100 INCIDENT COMMAND SYSTEM Canadian Version CANADIAN TRAINING CURRICULUM MODULE
INCIDENT COMMAND SYSTEM Canadian Version CANADIAN NATIONAL TRAINING CURRICULUM ICS ORIENTATION Saskatchewan Module 1 I - 100 INCIDENT COMMAND SYSTEM Canadian Version CANADIAN TRAINING CURRICULUM MODULE
EVACUATION/TRANSFER PROCEDURES
 EVACUATION/TRANSFER PROCEDURES MISSION: Every effort will be made by all staff to maintain the highest quality care through but not limited to continuity of: Care Plan/Medical Records- The Care Plan will
EVACUATION/TRANSFER PROCEDURES MISSION: Every effort will be made by all staff to maintain the highest quality care through but not limited to continuity of: Care Plan/Medical Records- The Care Plan will
Position Description
 Position Description Job Title: Ambulance Strike Team Leader Date: April 2013 Department: Operations & Office of Emergency Management Status: Non-exempt or Exempt Reports To: Ambulance Task Force Leader
Position Description Job Title: Ambulance Strike Team Leader Date: April 2013 Department: Operations & Office of Emergency Management Status: Non-exempt or Exempt Reports To: Ambulance Task Force Leader
Decontamination of the victim. Protection of medical personnel. Disposing of contaminated protective equipment and wash solutions.
 Decontamination: Standard Operating Procedure This procedure should be followed in the event of an emergency where a victim or equipment should need to be decontaminated due to a chemical, biological,
Decontamination: Standard Operating Procedure This procedure should be followed in the event of an emergency where a victim or equipment should need to be decontaminated due to a chemical, biological,
1.20.2 Definitions. The following definitions are applicable to this OG:
 Blackwood Fire Company Operating Guidelines 1.20 Water Rescue and Recovery Operations 1.20.1 Scope This Operating Guideline (OG) will apply to all incidents (except swimming pools) where victims require
Blackwood Fire Company Operating Guidelines 1.20 Water Rescue and Recovery Operations 1.20.1 Scope This Operating Guideline (OG) will apply to all incidents (except swimming pools) where victims require
How To Handle A Train Accident In Whitefish
 Drawing by Marty Two Bulls BAKKEN OIL SURE HAS US LOOKING AT OUR DISASTER PLANNING We can t say, Not in our backyard! We can t say rail accidents don t happen here in Whitefish area. Derailment in Olney
Drawing by Marty Two Bulls BAKKEN OIL SURE HAS US LOOKING AT OUR DISASTER PLANNING We can t say, Not in our backyard! We can t say rail accidents don t happen here in Whitefish area. Derailment in Olney
Template Policy on Healthcare Facility Patient Evacuation and Shelter-in Place
 Template Policy on Healthcare Facility Patient Evacuation and Shelter-in Place Policy: It is the policy of the healthcare facility to have defined procedures to protect the life and safety of both patients1
Template Policy on Healthcare Facility Patient Evacuation and Shelter-in Place Policy: It is the policy of the healthcare facility to have defined procedures to protect the life and safety of both patients1
07/14/2014 REVIEWED/REVISED: DATE TO BE REVIEWED: 01/31/2016 EMERGENCY MEDICAL SERVICES ELECTRONIC PATIENT CARE REPORT DOCUMENTATION - EPCR
 POLICY NO: 701 DATE ISSUED: 08/2000 DATE 07/14/2014 REVIEWED/REVISED: DATE TO BE REVIEWED: 01/31/2016 EMERGENCY MEDICAL SERVICES I. PURPOSE: To define the use of standardized records to be used by Emergency
POLICY NO: 701 DATE ISSUED: 08/2000 DATE 07/14/2014 REVIEWED/REVISED: DATE TO BE REVIEWED: 01/31/2016 EMERGENCY MEDICAL SERVICES I. PURPOSE: To define the use of standardized records to be used by Emergency
CHESTER COUNTY EMS COUNCIL, INC. Policies and Procedures Air Ambulance Utilization. Air Ambulance Utilization for Patients in Chester County.
 CHESTER COUNTY EMS COUNCIL, INC. Policies and Procedures Air Ambulance Utilization TITLE: PURPOSE: POLICY: Air Ambulance Utilization for Patients in Chester County. The utilization of air ambulances for
CHESTER COUNTY EMS COUNCIL, INC. Policies and Procedures Air Ambulance Utilization TITLE: PURPOSE: POLICY: Air Ambulance Utilization for Patients in Chester County. The utilization of air ambulances for
Automatic External Defibrillator Program
 Automatic External Defibrillator Program 1.0 Introduction This policy serves as guidance to outline the availability, maintenance, and proper use of Automated External Defibrillators (AEDs) at the University
Automatic External Defibrillator Program 1.0 Introduction This policy serves as guidance to outline the availability, maintenance, and proper use of Automated External Defibrillators (AEDs) at the University
HE MANTRA SAYS IT: Practice makes perfect.
 T HE MANTRA SAYS IT: Practice makes perfect. Perhaps nowhere is this more important than emergency preparation, and that s absolutely critical at airports. So we at Salt Lake City International Airport
T HE MANTRA SAYS IT: Practice makes perfect. Perhaps nowhere is this more important than emergency preparation, and that s absolutely critical at airports. So we at Salt Lake City International Airport
Multiple Aircraft Scene Response
 Multiple Aircraft Scene Response Developed by Missouri State Advisory Council on EMS Air Ambulance Sub Committee In cooperation with Missouri Association of Air Medical Services Objectives n Identify
Multiple Aircraft Scene Response Developed by Missouri State Advisory Council on EMS Air Ambulance Sub Committee In cooperation with Missouri Association of Air Medical Services Objectives n Identify
Emergency Incident Management Systems
 Emergency Incident Management Systems Fundamentals and Applications LOUIS N. MOLINO, Sr.,WILEY- INTERSCIENCE A JOHN WILEY & SONS, INC., PUBLICATION CONTENTS Acknowledgments, vii About the Author, ix Preface,
Emergency Incident Management Systems Fundamentals and Applications LOUIS N. MOLINO, Sr.,WILEY- INTERSCIENCE A JOHN WILEY & SONS, INC., PUBLICATION CONTENTS Acknowledgments, vii About the Author, ix Preface,
County of Sutter. Emergency Operations Plan
 County of Sutter Emergency Operations Plan Sutter Operational Area Annex 2 Emergency Operations Center Handbook and Checklists February 2015 BLANK PAGE TABLE OF CONTENTS Section 1 INTRODUCTION Page 1 Emergency
County of Sutter Emergency Operations Plan Sutter Operational Area Annex 2 Emergency Operations Center Handbook and Checklists February 2015 BLANK PAGE TABLE OF CONTENTS Section 1 INTRODUCTION Page 1 Emergency
5.8 Staging Area: The location where incident personnel and equipment are assigned on immediately available status.
 KING COUNTY FIRE MODEL PROCEDURE Section 21 King County Rehab Guidelines Adopted 06/24/09 Revised 5/21/15 REHABILITATION AND MONITORING ON THE FIRE GROUND 1.0 PURPOSE: Provide rehabilitation & medical
KING COUNTY FIRE MODEL PROCEDURE Section 21 King County Rehab Guidelines Adopted 06/24/09 Revised 5/21/15 REHABILITATION AND MONITORING ON THE FIRE GROUND 1.0 PURPOSE: Provide rehabilitation & medical
County of Santa Clara Emergency Medical Services System
 County of Santa Clara Emergency Medical Services System Policy #611: EMS Air Resource Utilization EMS AIR RESOURCE UTILIZATION Effective: Feburary 12, 2015 Replaces: May 5, 2008 Review: November 12, 2108
County of Santa Clara Emergency Medical Services System Policy #611: EMS Air Resource Utilization EMS AIR RESOURCE UTILIZATION Effective: Feburary 12, 2015 Replaces: May 5, 2008 Review: November 12, 2108
TEPP Planning Products Model Procedure
 TEPP Planning Products Model Procedure for First Responder Initial Response to Radiological Transportation Accidents 02B00215-13.p65 Prepared for the Department of Energy Office of Transportation and Emergency
TEPP Planning Products Model Procedure for First Responder Initial Response to Radiological Transportation Accidents 02B00215-13.p65 Prepared for the Department of Energy Office of Transportation and Emergency
Procedure: Hazardous Materials Medical Support and Rehabilitation Functions
 Procedure: HAZARDOUS MATERIALS MEDICAL SUPPORT Purpose: This standard operating procedure requires that a medical support function be designated to the Hazardous Materials Group during all operations within
Procedure: HAZARDOUS MATERIALS MEDICAL SUPPORT Purpose: This standard operating procedure requires that a medical support function be designated to the Hazardous Materials Group during all operations within
ESCAMBIA COUNTY FIRE-RESCUE 3105.005
 Patrick T Grace, Fire Chief Page 1 of 13 PURPOSE: Escambia County Fire-Rescue responds to a wide range of emergency incidents. In order to effectively manage personnel and resources and to provide for
Patrick T Grace, Fire Chief Page 1 of 13 PURPOSE: Escambia County Fire-Rescue responds to a wide range of emergency incidents. In order to effectively manage personnel and resources and to provide for
PUBLIC SAFETY FIRE. Functional Coordinator: Fire Chiefs
 Option for Public Safety or Tasks can be combined with Law Enforcement depending on jurisdiction PUBLIC SAFETY FIRE Functional Coordinator: Fire Chiefs Purpose This function provides procedures for preparedness,
Option for Public Safety or Tasks can be combined with Law Enforcement depending on jurisdiction PUBLIC SAFETY FIRE Functional Coordinator: Fire Chiefs Purpose This function provides procedures for preparedness,
TOWN OF WAYLAND POSITION DESCRIPTION
 TOWN OF WAYLAND POSITION DESCRIPTION Title: Department: Appointing Authority: Affiliation: Assistant Fire Chief Fire Fire Chief Non-Union Grade: N-9 Personnel Board Approved: 02/29/16 Summary of Duties
TOWN OF WAYLAND POSITION DESCRIPTION Title: Department: Appointing Authority: Affiliation: Assistant Fire Chief Fire Fire Chief Non-Union Grade: N-9 Personnel Board Approved: 02/29/16 Summary of Duties
County of Santa Clara Emergency Medical Services System
 County of Santa Clara Emergency Medical Services System Policy #611: EMS Air Resource Utilization EMS AIR RESOURCE UTILIZATION Effective: May 5, 2008TBD Replaces: January 22, 2007 May 5, 2008 Review: TBD
County of Santa Clara Emergency Medical Services System Policy #611: EMS Air Resource Utilization EMS AIR RESOURCE UTILIZATION Effective: May 5, 2008TBD Replaces: January 22, 2007 May 5, 2008 Review: TBD
Emergency Quick Reference Guide
 Township of Rideau Lakes - Emergency Response Plan 1 Emergency Quick Reference Guide Upon the arrival of three or more members, the Community Control Group (CCG) may initiate its function. Ensure that
Township of Rideau Lakes - Emergency Response Plan 1 Emergency Quick Reference Guide Upon the arrival of three or more members, the Community Control Group (CCG) may initiate its function. Ensure that
Communications Unit Leader All-Hazards (COML) Task Book
 Task Book") Communications Unit Leader All-Hazards (CML) Task Book Version 03_08 VERFCATN / CERTFCATN F CMPLETED TASK BK FR THE PSTN F Type CML (All-Hazards) FNAL EVALUATR S VERFCATN verify that all tasks have been
Communications Unit Leader All-Hazards (CML) Task Book Version 03_08 VERFCATN / CERTFCATN F CMPLETED TASK BK FR THE PSTN F Type CML (All-Hazards) FNAL EVALUATR S VERFCATN verify that all tasks have been
Emergency Medical Services Division. AMBULANCE-BASED ALS FIRST RESPONDER AND ASSESSMENT UNIT POLICIES AND PROCEDURES December 1, 2015
 Emergency Medical Services Division AMBULANCE-BASED ALS FIRST RESPONDER AND ASSESSMENT UNIT POLICIES AND PROCEDURES December 1, 2015 June 1, 2010 Edward Hill EMS Director Kristopher Lyon, M.D. Medical
Emergency Medical Services Division AMBULANCE-BASED ALS FIRST RESPONDER AND ASSESSMENT UNIT POLICIES AND PROCEDURES December 1, 2015 June 1, 2010 Edward Hill EMS Director Kristopher Lyon, M.D. Medical
[This page is intentionally left blank]
![[This page is intentionally left blank]](/thumbs/27/11307501.jpg "[This page is intentionally left blank]") Drill #3 [This page is intentionally left blank] CERT DRILLS AND EXERCISES: DRILL #3 Table of Contents CERT Drills and Exercises... 1 What is a Drill?... 1 Exercise Overview... 2 For Exercise Staff...
Drill #3 [This page is intentionally left blank] CERT DRILLS AND EXERCISES: DRILL #3 Table of Contents CERT Drills and Exercises... 1 What is a Drill?... 1 Exercise Overview... 2 For Exercise Staff...
California Code of Regulations Title 22. Social Security Division 9. Prehospital Emergency Medical Services Chapter 8. Prehospital EMS Air Regulations
 California Code of Regulations Title 22. Social Security Division 9. Prehospital Emergency Medical Services Chapter 8. Prehospital EMS Air Regulations 100276. Advanced Life Support. Article 1. Definitions
California Code of Regulations Title 22. Social Security Division 9. Prehospital Emergency Medical Services Chapter 8. Prehospital EMS Air Regulations 100276. Advanced Life Support. Article 1. Definitions
CENTRAL CALIFORNIA EMERGENCY MEDICAL SERVICES A Division of the Fresno County Department of Public Health
 CENTRAL CALIFORNIA EMERGENCY MEDICAL SERVICES A Division of the Fresno County Department of Public Health Manual Emergency Medical Services Administrative Policies and Procedures Policy Subject Helicopter
CENTRAL CALIFORNIA EMERGENCY MEDICAL SERVICES A Division of the Fresno County Department of Public Health Manual Emergency Medical Services Administrative Policies and Procedures Policy Subject Helicopter
April 16, 2007. From the EMS Perspective. Captain Matthew Johnson Lieutenant William Booker
 April 16, 2007 From the EMS Perspective Captain Matthew Johnson Lieutenant William Booker Virginia Tech Rescue Squad Established in 1969 by four VT students Received the EMS Service of the Year, 1988 Received
April 16, 2007 From the EMS Perspective Captain Matthew Johnson Lieutenant William Booker Virginia Tech Rescue Squad Established in 1969 by four VT students Received the EMS Service of the Year, 1988 Received
MLFD Standard Operating Guidelines SOG# 12-22 Subject: Patient Transfer of Care Initiated 1/30/2013
 MLFD Standard Operating Guidelines SOG# 12-22 Subject: Patient Transfer of Care Initiated 1/30/2013 Approved: Revised PURPOSE It is the purpose of this SOG to provide and ensure the highest level of patient
MLFD Standard Operating Guidelines SOG# 12-22 Subject: Patient Transfer of Care Initiated 1/30/2013 Approved: Revised PURPOSE It is the purpose of this SOG to provide and ensure the highest level of patient
SAN FRANCISCO INTERNATIONAL AIRPORT - PARAMEDIC FIRST RESPONDER PROGRAM
 SAN FRANCISCO INTERNATIONAL AIRPORT - PARAMEDIC FIRST RESPONDER PROGRAM APPROVED: EMS Medical Director EMS Administrator 1. Purpose 1.1 To establish policy and procedures for paramedic first response and
SAN FRANCISCO INTERNATIONAL AIRPORT - PARAMEDIC FIRST RESPONDER PROGRAM APPROVED: EMS Medical Director EMS Administrator 1. Purpose 1.1 To establish policy and procedures for paramedic first response and
EMERGENCY RESPONSE TEAMS AND INCIDENT MANAGEMENT SYSTEMS
 GAP.1.7.0.2 A Publication of Global Asset Protection Services LLC EMERGENCY RESPONSE TEAMS AND INCIDENT MANAGEMENT SYSTEMS INTRODUCTION A key part of an emergency response system is to create the necessary
GAP.1.7.0.2 A Publication of Global Asset Protection Services LLC EMERGENCY RESPONSE TEAMS AND INCIDENT MANAGEMENT SYSTEMS INTRODUCTION A key part of an emergency response system is to create the necessary
CAMS CRITICAL INCIDENT RESPONSE. This document is dated 4 March 2015 it consists of 16 pages
 CAMS CRITICAL INCIDENT RESPONSE This document is dated 4 March 2015 it consists of 16 pages Critical Incident Response Procedures for Club Motor Sport Events Note: This document has two discrete parts:
CAMS CRITICAL INCIDENT RESPONSE This document is dated 4 March 2015 it consists of 16 pages Critical Incident Response Procedures for Club Motor Sport Events Note: This document has two discrete parts:
Hospital Emergency Operations Plan
 Hospital Emergency Operations Plan I-1 Emergency Management Plan I PURPOSE The mission of University Hospital of Brooklyn (UHB) is to improve the health of the people of Kings County by providing cost-effective,
Hospital Emergency Operations Plan I-1 Emergency Management Plan I PURPOSE The mission of University Hospital of Brooklyn (UHB) is to improve the health of the people of Kings County by providing cost-effective,
Standard Operating Guideline for
 MABAS DIVISION 5 Standard Operating Guideline SUBJECT: Emergency Incident Rehabilitation S.O.G. REHAB 2009 Approved: December 16, 2009 Revised: Standard Operating Guideline for Emergency Incident Rehabilitation
MABAS DIVISION 5 Standard Operating Guideline SUBJECT: Emergency Incident Rehabilitation S.O.G. REHAB 2009 Approved: December 16, 2009 Revised: Standard Operating Guideline for Emergency Incident Rehabilitation
4 Best Practices for. Active Shooter. Lessons Learned from 10 Active Shooter Exercises with the University of North Florida. www.c3pathways.
 4 Best Practices for Active Shooter Incident Managment Lessons Learned from 10 Active Shooter Exercises with the University of North Florida www.c3pathways.com contents contents 01 Assume Command Quickly
4 Best Practices for Active Shooter Incident Managment Lessons Learned from 10 Active Shooter Exercises with the University of North Florida www.c3pathways.com contents contents 01 Assume Command Quickly
EMS Aircraft Operations
 Page 1 Policy: Field Care Patient Management EMS Aircraft Operations I. AUTHORITY California Code of Regulations, Title 22, Division 9, Chapter 8, Articles 1-5 II. PURPOSE A. To establish guidelines for
Page 1 Policy: Field Care Patient Management EMS Aircraft Operations I. AUTHORITY California Code of Regulations, Title 22, Division 9, Chapter 8, Articles 1-5 II. PURPOSE A. To establish guidelines for
INCIDENT COMMAND SYSTEM. For Fire Department Structure Fire Operations ICS-SF
 INCIDENT COMMAND SYSTEM For Fire Department Structure Fire Operations FIrefighting RESources of California Organized for Potential Emergencies Revised November 1, 1994 This document contains information
INCIDENT COMMAND SYSTEM For Fire Department Structure Fire Operations FIrefighting RESources of California Organized for Potential Emergencies Revised November 1, 1994 This document contains information
FEDERAL EMERGENCY MANAGEMENT AGENCY (FEMA) INDEPENDENT STUDY COURSE INTRO TO INCIDENT COMMAND SYSTEM FOR FEDERAL WORKERS (IS-100.
 INDEPENDENT STUDY COURSE INTRO TO INCIDENT COMMAND SYSTEM FOR FEDERAL WORKERS (IS-100.") This Study Guide has been created to provide an overview of the course content presented in the Federal Emergency Management Agency (FEMA) Independent Study Course titled IS-100.FWA Intro to Incident Command
This Study Guide has been created to provide an overview of the course content presented in the Federal Emergency Management Agency (FEMA) Independent Study Course titled IS-100.FWA Intro to Incident Command
Lesson 1: What Is the National Incident Management System (NIMS)? Summary of Lesson Content
? Summary of Lesson Content") Lesson 1: What Is the National Incident Management System (NIMS)? Lesson Overview On February 28, 2003, President Bush issued Homeland Security Presidential Directive 5. HSPD 5 directed the Secretary of
Lesson 1: What Is the National Incident Management System (NIMS)? Lesson Overview On February 28, 2003, President Bush issued Homeland Security Presidential Directive 5. HSPD 5 directed the Secretary of
UFF Position Statement: Fire and Smoke as a Weapon
 UFF Position Statement: Fire and Smoke as a Weapon According to the United States Department of Homeland Security, international terrorist groups and violent extremists have shown interest in using fire
UFF Position Statement: Fire and Smoke as a Weapon According to the United States Department of Homeland Security, international terrorist groups and violent extremists have shown interest in using fire
Emergency Medical Services Agency. Report to the Local Agency Formation Commission
 Emergency Medical Services Agency August 8, 2012 Report to the Local Agency Formation Commission The Relationship of Fire First Response to Emergency Medical Services On September 26, 2011, the Contra
Emergency Medical Services Agency August 8, 2012 Report to the Local Agency Formation Commission The Relationship of Fire First Response to Emergency Medical Services On September 26, 2011, the Contra
MEDICAL UNIVERSITY OF SOUTH CAROLINA DEPARTMENT OF PUBLIC SAFETY. of Prisoners
 MEDICAL UNIVERSITY OF SOUTH CAROLINA DEPARTMENT OF PUBLIC SAFETY SUBJECT: Searching and Transportation of Prisoners EFFECTIVE DATE: 1 January 1999 PAGE 1 OF 10 REVIEW DATE: 30 November 2015 APPROVED: CHANGE
MEDICAL UNIVERSITY OF SOUTH CAROLINA DEPARTMENT OF PUBLIC SAFETY SUBJECT: Searching and Transportation of Prisoners EFFECTIVE DATE: 1 January 1999 PAGE 1 OF 10 REVIEW DATE: 30 November 2015 APPROVED: CHANGE
2014 TRANSPORTATION SAFETY SUMMIT LOUISIANA STATE POLICE & LADOTD TIM INITIATIVE
 2014 TRANSPORTATION SAFETY SUMMIT LOUISIANA STATE POLICE & LADOTD TIM INITIATIVE PROJECT SUMMARY & PRESENTATION LAW ENFORCEMENT FIRE EMS TRANSPORTATION TOWING & RECOVERY COMMUNICATIONS What is Traffic
2014 TRANSPORTATION SAFETY SUMMIT LOUISIANA STATE POLICE & LADOTD TIM INITIATIVE PROJECT SUMMARY & PRESENTATION LAW ENFORCEMENT FIRE EMS TRANSPORTATION TOWING & RECOVERY COMMUNICATIONS What is Traffic
MARYLAND REGION IV ALERT STATUS SYSTEM
 MARYLAND REGION IV ALERT STATUS SYSTEM Revised September 20, 2011 - NOTE - Patients destined for specialty referral centers would not be governed by these policies and should be transported to facilities
MARYLAND REGION IV ALERT STATUS SYSTEM Revised September 20, 2011 - NOTE - Patients destined for specialty referral centers would not be governed by these policies and should be transported to facilities
S.T.A.R.T SIMPLE TRIAGE AND RAPID TREATMENT
 S.T.A.R.T SIMPLE TRIAGE AND RAPID TREATMENT Incidents which produce multiple human casualties are somewhat rare but do occur and must be planned for. A multiple or mass casualty incident can be defined
S.T.A.R.T SIMPLE TRIAGE AND RAPID TREATMENT Incidents which produce multiple human casualties are somewhat rare but do occur and must be planned for. A multiple or mass casualty incident can be defined
DEVELOPING THE EMERGENCY PLAN By: Robert Sheffield INTRODUCTION. Overview
 DEVELOPING THE EMERGENCY PLAN By: Robert Sheffield INTRODUCTION Overview The Emergency Plan can never be tested until there an emergency occurs. The incident range can extend from a minor or simple impairment
DEVELOPING THE EMERGENCY PLAN By: Robert Sheffield INTRODUCTION Overview The Emergency Plan can never be tested until there an emergency occurs. The incident range can extend from a minor or simple impairment
Contractor s Injury Management Toolbox RISK CONTROL
 Contractor s Injury Management Toolbox managing job site accidents and injuries RISK CONTROL Your Role in Workplace Safety As a superintendent or foreman, you play an important role in helping our company
Contractor s Injury Management Toolbox managing job site accidents and injuries RISK CONTROL Your Role in Workplace Safety As a superintendent or foreman, you play an important role in helping our company
Tuolumne County Emergency Medical Services Agency EMS System Policies and Procedures. Creation Date: 2-25-99
 Tuolumne County Emergency Medical Services Agency EMS System Policies and Procedures Policy: EMS Aircraft Classification and Authorization Creation Date: 2-25-99 #442.00 Medical Director: Revision Date:
Tuolumne County Emergency Medical Services Agency EMS System Policies and Procedures Policy: EMS Aircraft Classification and Authorization Creation Date: 2-25-99 #442.00 Medical Director: Revision Date:
Geographic Area Command
 Geographic Area Command Appendix to: Georgia Emergency Operations Plan- ( Georgia Hurricane Plan ) 2013 Purpose INTRODUCTION Geographic Area Command shall be established to oversee the management of an
Geographic Area Command Appendix to: Georgia Emergency Operations Plan- ( Georgia Hurricane Plan ) 2013 Purpose INTRODUCTION Geographic Area Command shall be established to oversee the management of an
North Carolina Burn Disaster Program Carolina Hospital Burn Surge Plan Template
 North Carolina Burn Disaster Program Carolina Hospital Burn Surge Plan Template Developed by: UNC School of Medicine North Carolina Jaycee Burn Center North Carolina Office of EMS NC Burn Disaster Program
North Carolina Burn Disaster Program Carolina Hospital Burn Surge Plan Template Developed by: UNC School of Medicine North Carolina Jaycee Burn Center North Carolina Office of EMS NC Burn Disaster Program
Classification Appeal Decision Under Section 5112 of Title 5, United States Code
 U.S. Office of Personnel Management Office of Merit Systems Oversight and Effectiveness Classification Appeals and FLA. Programs San Francisco Oversight Division 120 Howard Street, Room 760 San Francisco,
U.S. Office of Personnel Management Office of Merit Systems Oversight and Effectiveness Classification Appeals and FLA. Programs San Francisco Oversight Division 120 Howard Street, Room 760 San Francisco,
The Instructional Guidelines in this section include all the topics and material at the AEMT level.
 Principles of Safely Operating a Ground Ambulance The Instructional Guidelines in this section include all the topics and material at the AEMT level. The intent of this section is to give an overview of
Principles of Safely Operating a Ground Ambulance The Instructional Guidelines in this section include all the topics and material at the AEMT level. The intent of this section is to give an overview of
B E F O R E T H E E M E R G E N C Y
 B E F O R E T H E E M E R G E N C Y RESPONSIBILITY / LIABILITY for Homeland Security / Emergency Management Duty of Care - Counties and Cities ARE responsible for the safety of their citizens. Following
B E F O R E T H E E M E R G E N C Y RESPONSIBILITY / LIABILITY for Homeland Security / Emergency Management Duty of Care - Counties and Cities ARE responsible for the safety of their citizens. Following