SHOULDER INJURIES IN SPORT
|
|
|
- Lesley Barber
- 7 years ago
- Views:
Transcription

1 SHOULDER INJURIES IN SPORT DR. ANDREW POTTER SPORTS & EXERCISE MEDICINE PHYSICIAN

2 SHOULDER INJURIES 4 joints - sternoclavicular acromioclavicular glenohumeral scapulothoracic Designed for mobility Balance MOBILITY v STABILITY Stability - passive - ligamentous active - muscular rotator cuff scapular stabilisers

3 ASSESSMENT Handedness HISTORY Activity, sport Acute - mechanism of injury Chronic - duration of symptoms changes to training habits Instability - dislocation and reduction, subluxation, dead arm Previous injury Other conditions cervical spine polyarthropathy systemic symptoms

4 INVESTIGATIONS Plain x-ray - AP with ER = greater tuberosity AP with IR = Hill-Sachs Lateral Axillary Ultrasound scan - subacromial bursa rotator cuff biceps tendon CT (arthrography) - bony injury labral tears rotator cuff tear (full thickness) Nuclear bone scan - bony injury (stress fractures) MRI(A) - rotator cuff tears labral, capsular tears
 MRI(A) - rotator cuff tears labral,")
5 MANAGEMENT Medical, Physiotherapy, Surgical Rest - maintain fitness Modalities - ice, heat, U/S, IFT, MFT Medication - analgaesics, NSAIDs, corticosteroid Maintain movement, flexibility within pain limits Strengthen muscles - isometric, concentric resistance, eccentric movers, stabilisers Dynamic exercises Check technique Graded return to sport

6 SHOULDER INJURIES ACUTE TRAUMATIC Contact or collision sports Fractures - clavicle humerus acromion Joint injury - glenohumeral acromioclavicular sternoclavicular Soft tissue contusion


7 SHOULDER INJURIES CHRONIC OVERUSE Overhead sports Repetitive, fast Disruption of mobility stability balance Young - glenohumeral instability labral tears impingement tendonitis rotator cuff Older - degenerative changes to joints degenerative tendonosis rotator cuff tears


8 CLAVICLE FRACTURES Common - 5% of adult fractures 80% in middle third, 15% distally Direct blow, fall onto outstretched hand Pain, dysfunction, tenderness, deformity Associated injuries direct violence 1 st rib, sternoclavicular, acromioclavicular joints lung neurovascular structures

9 CLAVICULAR FRACTURES TREATMENT NON-OPERATIVE Sling or brace? Less discomfort with sling Alignment, cosmetic, functional results identical Non union 0.9 4% Good results with excellent remodelling Healing 6-12 weeks in adults (less in children) Return to contact sport after 8 weeks (minimum)

10 CLAVICULAR FRACTURES TREATMENT INDICATIONS OPERATIVE Open fractures Associated neurovascular injuries Displaced fractures of midshaft, distal 1/3 High risk of dysfunction displacement, shortening < 5 mm acceptable > 20 mm higher risk of non-union, poor function Rapid return to sport

11 CLAVICULAR FRACTURES TREATMENT OPERATIVE Plate fixation Large scar Hardware prominence 5 23 % complication rate (loosening, malunion, infection) Intramedullary Fixation Large threaded cannulated screws Less secure Wires increased risk of migration Recommended removal of fixation later

12 CLAVICULAR FRACTURES MANAGEMENT Governed by pain, complications, activity Sling for comfort Pendulum exercise as tolerated Active range of movement when out of sling Return to sport skills as tolerated Contact sport later


13 ACROMIOCLAVICULAR INJURIES Collision, fall onto lateral shoulder Damage - joint capsule ligaments meniscus / fibrous disc Pain, swelling, local tenderness, deformity X-ray - separation fracture distal clavicle weighted views little value

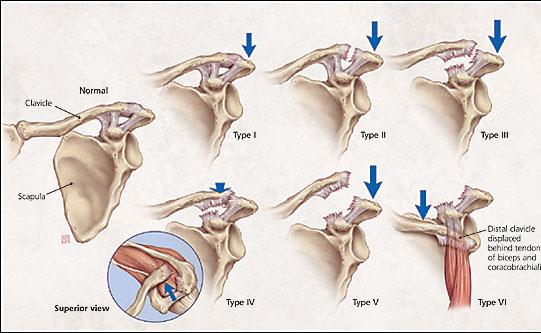
14 ACROMIOCLAVICULAR INJURIES

15 Symptomatic Ice Rest in collar & cuff Analgaesics, NSAIDs ACROMIOCLAVICULAR INJURIES GRADE 1 & 2 Physiotherapy - modalities movement muscle strengthening trapezius rotator cuff deltoid scapular stabilisers Return to sport when full pain-free movement, full strength 2 4 weeks Risk of degenerative arthropathy Damage to joint disc, surfaces

16 ACROMIOCLAVICULAR INJURIES GRADE 3 Operative v conservative? No differences in outcomes (retrospective studies) Conservative return to sport earlier Management Sling for support Range of movement Strengthening exercises Return to sport 6 12 weeks Operative Repetitive heavy lifting Use of arms above 90 degrees abduction Thin, prominent distal clavicle Cosmesis

17 Grades 4,5 Mostly operative ACROMIOCLAVICULAR INJURIES OPERATIVE MANAGEMENT Grade 6 Usually unstable Anchor clavicle to coracoid process plaited suture screw stay sutures? Excision of distal clavicle Reconstruction of acromio-clavicular ligament

18 OSTEOLYSIS OF DISTAL CLAVICLE Bony resorption of distal clavicle, (acromion) Atraumatic medical conditions rheumatoid arthritis infection sceloderma hyperparathyroidism multiple myeloma Traumatic recurrent heavy lifting overhead weight training Pain, tenderness of a/c joint pushups, dips, bench press, throwing



19 OSTEOLYSIS OF DISTAL CLAVICLE Plain X-ray weeks to months to appear loss of subarticular cortex demineralisation of clavicular tip erosion of distal clavicle (5 to 30 mm) Nuclear Bone Scan increased uptake in distal clavicle (acromion)


20 OSTEOLYSIS OF DISTAL CLAVICLE MANAGEMENT Rest from pain producing activities NSAIDs, physiotherapy Reparative process 4-6 months remineralisation of distal clavicle joint widening may persist Excision of distal cavicle for persistent symptoms

21 STERNOCLAVICULAR JOINT INJURIES Collision injury - lateral force to shoulder Posterior is surgical emergency neurovascular impingement Anterior displacement of clavicle more common in sport subluxation capsular ligament sprain avulsion fracture posteriorly on CT Local pain, swelling, prominence, tenderness worse with shoulder movements Management - soft tissue injury ice, heat, analgaesia, NSAIDs, physiotherapy modalities rest injured area pain free movement graded return to sport
22 GLENOHUMERAL DISLOCATION Serious injury with significant disability M > F < 25 years recurrence rate % - less as older Anterior 95% - abduction + external rotation + extension fall, direct force Posterior - adduction + internal rotation + extension epilepsy Inferior - abduction + inferior force wrestling, fall on top of shoulder
23 GLENOHUMERAL DISLOCATION Pain, disability, deformity Serious injury with damage - capsule, ligaments glenoid labrum humerus Bankart lesion in 90% - anterior glenoid labrum detachment anterior inferior glenohumeral ligament disruption HAGL humeral end of anterior GHL Capsular laxity - plastic deformation prior to failure Hill-Sachs lesion - compression fracture of posterolateral humeral head impact with anteroinferior glenoid rim


24 GLENOHUMERAL DISLOCATION PLAIN X-RAY
25 Hill Sachs Bankart
26 GLENOHUMERAL DISLOCATION MANAGEMENT Reduction as soon as possible check for neurovascular, fracture (x-ray) analgaesics Method of reduction - prone traction Post reduction x-ray Analgaesics? Conservative or operative
27 GLENOHUMERAL DISLOCATION MANAGEMENT NON-OPERATIVE IMMOBILISE Fibroblastic response to damaged tissue reattachment of labrum, tightening of anterior ligaments Sling = adduction + IR for 3 6 weeks Brace in ER better aposition of Bankart lesion to glenoid neck REST IN SLING Comfort Active movement as tolerated No difference in recurrence rates Rehab program
28 GLENOHUMERAL DISLOCATION MANAGEMENT ACUTE OPERATIVE Within 10 days of injury Arthroscopic Bankart repair re-attachment of labrum to glenoid Less recurrence than non-operative management Longer recovery - > 3 months return to sport RECURRENT Open Bankart repair + capsular shift Lower recurrence than arthroscopic repair Loss of external rotation - beware throwers 6 months return to sport Require 4 6 weeks immobilisation in sling + rehab program
29 GLENOHUMERAL DISLOCATION REHABILITATION Isometric contractions for IR and ER Pain free active movement - during/after immobilisation Increase range of movement avoiding extremes ER, Abduction Strengthen - dynamic stabilisers - IR, ADDUCTORS rotator cuff + scapular stabilisers concentric & eccentric Sport specific activities - graded Return to sport when - pain free full mobility & strength 8 12 weeks for non-operative management continuing rehab program
30 CHRONIC GLENOHUMERAL INSTABILITY Recurrent dislocations Recurrent subluxations - initial acute injury repeated weakening of stabilisers Labral tears - chronic repetitive stresses with overhead activity Rotator cuff dysfunction (subacromial impingement) Adolescents with generalised ligament laxity
31 CHRONIC GLENOHUMERAL INSTABILITY Symptoms - pain, weakness, reduced function episodes of going out momentary dead arm mechanical catching Signs - muscle wasting scapular dysrhythmia apprehension with stressing pain with stressing frank instability to direction testing
32 GLENOHUMERAL INSTABILITY MANAGEMENT CONSERVATIVE prolonged rehab program maintain full mobility muscle balance for stability of glenohumeral joint strengthen rotator cuff concentric + eccentric modify activity to avoid aggravation SURGICAL arthroscopic or open re-attach labrum debride labral tears tighten anterior capsule continue rehab program RETURN to sport 3 6 months reduced external rotation
33 SLAP LESIONS Superior attachment of glenoid labrum and biceps tendon Affect stability extra strain on IGHLs increased translation due to destabilised biceps tendon Poor vascular supply Acute, chronic Traction - overhead athletes with chronic repetitive overload throwers, swimmers, tennis, weight training Compression fall on outstretched hand in ER

34 SLAP LESIONS Poorly localised shoulder pain overhead, behind the back activities Mechanical catching, popping, grinding Tenderness over anterosuperior aspect of shoulder Pain with resisted biceps contraction Specific tests stress superior labrum variable reliability O Brien s Crank compression-rotation

35 SLAP LESIONS MRA CT ARTHROGRAM


36 SLAP LESIONS MANAGEMENT NON-OPERATIVE Analgaesics NSAIDs Stabilising exercises OPERATIVE Failure of rehab program Arthroscopic surgery stable - debridement unstable - reattachment of labrum Continuing stabilising rehab
37 SUBACROMIAL IMPINGEMENT CYCLICAL INJURY Repetitive overhead activity tennis, swimming, weights, throwing impingement on RC tendon, bursa maximal at degrees ADD more with flexion + IR Pressure - irritation, inflammation Weakness of dynamic shoulder stabilisers Superior migration of humeral head Further damage to RC tendon Eventual degenerative change partial RC tears Acute full thickness tears through areas of degeneration
38 ACUTE IMPINGEMENT Young age group Tendonitis & bursitis Recent onset of acute constant pain aggravated by overhead activities Local tenderness in subacromial space, anterior & lateral painful arc degrees adduction, active & passive often painful internal rotation behind back Positive impingement sign Pain with resisted contraction (supraspinatus) Relief of pain with subacromial anaesthetic
39 ACUTE IMPINGEMENT Investigation usually not required Rest shoulder from aggravating activity MANAGEMENT Local ice, heat, physiotherapy modalities maintain aerobic fitness with alternate exercise Analgaesics, oral NSAIDs, corticosteroid injection Maintain movement of shoulder joints Maintain muscle strength in RC & scapular stabilisers
40 ACUTE IMPINGEMENT SWIMMERS Posture accentuates impingement - muscle imbalance strong, tight IR, adductors protracted scapulae cervical lordosis Impingement in pull-through phase of freestyle, butterfly, breast stroke Rehab includes - stretch tight adductors, IRs, anterior capsule strengthen abductors, ERs Technique correction - body roll bilateral breathing early recovery from pull-through Graded return to swimming
41 SHOULDER REHABILITATION
42 CHRONIC IMPINGEMENT Older age group Long history of overhead activities Chronic bursitis & degenerative tendonosis Prolonged symptoms - local pain referred to upper arm & cervical spine weakness, disability Signs of impingement + muscle wasting reduced movement
43 CHRONIC IMPINGEMENT IMAGING Plain x-ray - narrowed subacromial space bony impingement from acromion, a-c joint calcific tendonopathy sclerosis at greater tuberosity of humerus Ultrasound scan - bursitis degenerative changes in RC tendons partial, full-thickness tears CT Arthrogram - full-thickness and inferior surface RC tears MRI - best soft tissue imaging
44 ROTATOR CUFF INJURIES Part of clinical picture of subacromial impingement YOUNGER acute subacomial bursitis acute tendonitis (supraspinatus) acute tendon tears OLDER chronic overuse injuries degenerative changes in tendons and bursa degenerative bony impingement of subacromial space thickening of coraco-acromial ligament calcific tendonitis tears of rotator cuff tendons adhesive capsulitis
45 CHRONIC IMPINGEMENT COMPLICATIONS ROTATOR CUFF TEAR partial common - exercise program complete - acute event loss of active adduction drop arm sign in acute phase compensation with progress return of some function surgical repair for prolonged symptoms
46 CHRONIC IMPINGEMENT ADHESIVE CAPSULITIS Follows shoulder pathology diabetics, antibiotics Prolonged course Residual loss of movement & function MANAGEMENT Control pain Analgaesics NSAIDs Corticosteroids Distension arthrogram with corticosteroid Rehab program - movement, stabiliser strength Surgical MUA, arthroscopic debridement
47 SUPRASCAPULAR NERVE IMPINGEMENT Supplies supraspinatus & infraspinatus Repetitive overhead activities - tennis, volleyball 2 Sites Irritation at suprascapular notch - affects both muscles posterior, lateral shoulder pain tenderness over notch wasting of both muscles weakness of abduction, external rotation Irritation at spinoglenoid notch - labral tear & cyst/ganglion affects infraspinatus wasting of infraspinatus weakness of external rotation

48 SUPRASCAPULAR NERVE IMPINGEMENT MANAGEMENT Rest from overhead activity Mobility & strengthening exercises Surgical decompression

49 THANK YOU
A Simplified Approach to Common Shoulder Problems
 A Simplified Approach to Common Shoulder Problems Objectives: Understand the basic categories of common shoulder problems. Understand the common patient symptoms. Understand the basic exam findings. Understand
A Simplified Approach to Common Shoulder Problems Objectives: Understand the basic categories of common shoulder problems. Understand the common patient symptoms. Understand the basic exam findings. Understand
Shoulder Injuries. Why Bother? QAS Injury Prevalence. Screening Injury 29.2% 12 month cumulative injury prevalence. Dr Simon Locke
 Shoulder Injuries Dr Simon Locke Why Bother? Are shoulder and upper limb injuries common? Some anatomy What, where, what sports? How do they happen? Treatment, advances? QAS Injury Prevalence Screening
Shoulder Injuries Dr Simon Locke Why Bother? Are shoulder and upper limb injuries common? Some anatomy What, where, what sports? How do they happen? Treatment, advances? QAS Injury Prevalence Screening
Rotator Cuff Tears in Football
 Disclosures Rotator Cuff Tears in Football Roger Ostrander, MD Consultant: Mitek Consultant: On-Q Research Support: Arthrex Research Support: Breg Research Support: Arthrosurface 2 Anatomy 4 major muscles:
Disclosures Rotator Cuff Tears in Football Roger Ostrander, MD Consultant: Mitek Consultant: On-Q Research Support: Arthrex Research Support: Breg Research Support: Arthrosurface 2 Anatomy 4 major muscles:
Refer to Specialist. The Diagnosis and Management of Shoulder Pain 1. SLAP lesions, types 1 through 4
 The Diagnosis Management of Shoulder Pain 1 Significant Hisry -Age -Extremity Dominance -Hisry of trauma, dislocation, subluxation -Weakness, numbness, paresthesias -Sports participation -Past medical
The Diagnosis Management of Shoulder Pain 1 Significant Hisry -Age -Extremity Dominance -Hisry of trauma, dislocation, subluxation -Weakness, numbness, paresthesias -Sports participation -Past medical
.org. Shoulder Pain and Common Shoulder Problems. Anatomy. Cause
 Shoulder Pain and Common Shoulder Problems Page ( 1 ) What most people call the shoulder is really several joints that combine with tendons and muscles to allow a wide range of motion in the arm from scratching
Shoulder Pain and Common Shoulder Problems Page ( 1 ) What most people call the shoulder is really several joints that combine with tendons and muscles to allow a wide range of motion in the arm from scratching
9/7/14. I do not have a financial relationship with any orthopedic manufacturing organization
 I do not have a financial relationship with any orthopedic manufacturing organization Timothy M. Geib, MD Oklahoma Sports & Orthopedic Institute September 27, 2014 Despite what you may have heard, I am
I do not have a financial relationship with any orthopedic manufacturing organization Timothy M. Geib, MD Oklahoma Sports & Orthopedic Institute September 27, 2014 Despite what you may have heard, I am
Notice of Independent Review Decision DESCRIPTION OF THE SERVICE OR SERVICES IN DISPUTE:
 Notice of Independent Review Decision DATE OF REVIEW: 12/10/10 IRO CASE #: NAME: DESCRIPTION OF THE SERVICE OR SERVICES IN DISPUTE: Determine the appropriateness of the previously denied request for right
Notice of Independent Review Decision DATE OF REVIEW: 12/10/10 IRO CASE #: NAME: DESCRIPTION OF THE SERVICE OR SERVICES IN DISPUTE: Determine the appropriateness of the previously denied request for right
Hand and Upper Extremity Injuries in Outdoor Activities. John A. Schneider, M.D.
 Hand and Upper Extremity Injuries in Outdoor Activities John A. Schneider, M.D. Biographical Sketch Dr. Schneider is an orthopedic surgeon that specializes in the treatment of hand and upper extremity
Hand and Upper Extremity Injuries in Outdoor Activities John A. Schneider, M.D. Biographical Sketch Dr. Schneider is an orthopedic surgeon that specializes in the treatment of hand and upper extremity
A Patient s Guide to Shoulder Pain
 A Patient s Guide to Shoulder Pain Part 2 Evaluating the Patient James T. Mazzara, M.D. Shoulder and Elbow Surgery Sports Medicine Occupational Orthopedics Patient Education Disclaimer This presentation
A Patient s Guide to Shoulder Pain Part 2 Evaluating the Patient James T. Mazzara, M.D. Shoulder and Elbow Surgery Sports Medicine Occupational Orthopedics Patient Education Disclaimer This presentation
Arthroscopic Shoulder Procedures. David C. Neuschwander MD. Shoulder Instability. Allegheny Health Network Orthopedic Associates of Pittsburgh
 Arthroscopic Shoulder Procedures David C. Neuschwander MD Allegheny Health Network Orthopedic Associates of Pittsburgh Shoulder Instability Anterior Instability Posterior Instability Glenohumeral Joint
Arthroscopic Shoulder Procedures David C. Neuschwander MD Allegheny Health Network Orthopedic Associates of Pittsburgh Shoulder Instability Anterior Instability Posterior Instability Glenohumeral Joint
Rotator Cuff Pathophysiology. treatment program that will effectively treat it. The tricky part about the shoulder is that it is a ball and
 Rotator Cuff Pathophysiology Shoulder injuries occur to most people at least once in their life. This highly mobile and versatile joint is one of the most common reasons people visit their health care
Rotator Cuff Pathophysiology Shoulder injuries occur to most people at least once in their life. This highly mobile and versatile joint is one of the most common reasons people visit their health care
Rotator cuff tears Acute or chronic? Mary Obele ANZSOM September 2012 Acknowledgement: ACC
 Rotator cuff tears Acute or chronic? Mary Obele ANZSOM September 2012 Acknowledgement: ACC Anatomy Epidemiology Asymptomatic rotator cuff tears: prevalence is 35% (5) 15% full thickness and 20% partial
Rotator cuff tears Acute or chronic? Mary Obele ANZSOM September 2012 Acknowledgement: ACC Anatomy Epidemiology Asymptomatic rotator cuff tears: prevalence is 35% (5) 15% full thickness and 20% partial
Ms. Ruth Delaney ROTATOR CUFF DISEASE Orthopaedic Surgeon, Shoulder Specialist
 WHAT DOES THE ROTATOR CUFF DO? WHAT DOES THE ROTATOR CUFF DO? WHO GETS ROTATOR CUFF TEARS? HOW DO I CLINICALLY DIAGNOSE A CUFF TEAR? WHO NEEDS AN MRI? DOES EVERY CUFF TEAR NEED TO BE FIXED? WHAT DOES ROTATOR
WHAT DOES THE ROTATOR CUFF DO? WHAT DOES THE ROTATOR CUFF DO? WHO GETS ROTATOR CUFF TEARS? HOW DO I CLINICALLY DIAGNOSE A CUFF TEAR? WHO NEEDS AN MRI? DOES EVERY CUFF TEAR NEED TO BE FIXED? WHAT DOES ROTATOR
TOWN CENTER ORTHOPAEDIC ASSOCIATES P.C. Labral Tears
 Labral Tears The shoulder is your body s most flexible joint. It is designed to let the arm move in almost any direction. But this flexibility has a price, making the joint prone to injury. The shoulder
Labral Tears The shoulder is your body s most flexible joint. It is designed to let the arm move in almost any direction. But this flexibility has a price, making the joint prone to injury. The shoulder
SHOULDER INSTABILITY. E. Edward Khalfayan, MD
 SHOULDER INSTABILITY E. Edward Khalfayan, MD Instability of the shoulder can occur from a single injury or as the result of repetitive activity such as overhead sports. Dislocations of the shoulder are
SHOULDER INSTABILITY E. Edward Khalfayan, MD Instability of the shoulder can occur from a single injury or as the result of repetitive activity such as overhead sports. Dislocations of the shoulder are
Shoulder Instability. Fig 1: Intact labrum and biceps tendon
 Shoulder Instability What is it? The shoulder joint is a ball and socket joint, with the humeral head (upper arm bone) as the ball and the glenoid as the socket. The glenoid (socket) is a shallow bone
Shoulder Instability What is it? The shoulder joint is a ball and socket joint, with the humeral head (upper arm bone) as the ball and the glenoid as the socket. The glenoid (socket) is a shallow bone
THE SHOULDER. Shoulder Pain. Fractures. Instability and Dislocations of the Shoulder
 THE SHOULDER Shoulder Pain 1. Fractures 2. Sports injuries 3. Instability/Dislocations 4. Rotator Cuff Disease and Tears 5. Arthritis Fractures The shoulder is made up of three primary bones, the clavicle,
THE SHOULDER Shoulder Pain 1. Fractures 2. Sports injuries 3. Instability/Dislocations 4. Rotator Cuff Disease and Tears 5. Arthritis Fractures The shoulder is made up of three primary bones, the clavicle,
.org. Rotator Cuff Tears. Anatomy. Description
 Rotator Cuff Tears Page ( 1 ) A rotator cuff tear is a common cause of pain and disability among adults. In 2008, close to 2 million people in the United States went to their doctors because of a rotator
Rotator Cuff Tears Page ( 1 ) A rotator cuff tear is a common cause of pain and disability among adults. In 2008, close to 2 million people in the United States went to their doctors because of a rotator
J F de Beer, K van Rooyen, D Bhatia. Rotator Cuff Tears
 1 J F de Beer, K van Rooyen, D Bhatia Rotator Cuff Tears Anatomy The shoulder consists of a ball (humeral head) and a socket (glenoid). The muscles around the shoulder act to elevate the arm. The large
1 J F de Beer, K van Rooyen, D Bhatia Rotator Cuff Tears Anatomy The shoulder consists of a ball (humeral head) and a socket (glenoid). The muscles around the shoulder act to elevate the arm. The large
Shoulder Impingement/Rotator Cuff Tendinitis
 Copyright 2011 American Academy of Orthopaedic Surgeons Shoulder Impingement/Rotator Cuff Tendinitis One of the most common physical complaints is shoulder pain. Your shoulder is made up of several joints
Copyright 2011 American Academy of Orthopaedic Surgeons Shoulder Impingement/Rotator Cuff Tendinitis One of the most common physical complaints is shoulder pain. Your shoulder is made up of several joints
Shoulder Injury Prevention and Rehabilitation for Health & Fitness Professionals
 s EDUCATION WORKSHOPS Shoulder Injury Prevention and Rehabilitation for Health & Fitness Professionals with B.App.Sc (Physio), Dip.Ed (P.E.) CONTENTS Topic Page 1. Functional Anatomy 3 2. Scapulohumeral
s EDUCATION WORKSHOPS Shoulder Injury Prevention and Rehabilitation for Health & Fitness Professionals with B.App.Sc (Physio), Dip.Ed (P.E.) CONTENTS Topic Page 1. Functional Anatomy 3 2. Scapulohumeral
1 of 6 1/22/2015 10:06 AM
 1 of 6 1/22/2015 10:06 AM 2 of 6 1/22/2015 10:06 AM This cross-section view of the shoulder socket shows a typical SLAP tear. Injuries to the superior labrum can be caused by acute trauma or by repetitive
1 of 6 1/22/2015 10:06 AM 2 of 6 1/22/2015 10:06 AM This cross-section view of the shoulder socket shows a typical SLAP tear. Injuries to the superior labrum can be caused by acute trauma or by repetitive
Shoulder MRI for Rotator Cuff Tears. Conor Kleweno,, Harvard Medical School Year III Gillian Lieberman, MD
 Shoulder MRI for Rotator Cuff Tears Conor Kleweno,, Harvard Medical School Year III Goals of Presentation Shoulder anatomy Function of rotator cuff MRI approach to diagnose cuff tear Anatomy on MRI images
Shoulder MRI for Rotator Cuff Tears Conor Kleweno,, Harvard Medical School Year III Goals of Presentation Shoulder anatomy Function of rotator cuff MRI approach to diagnose cuff tear Anatomy on MRI images
SHOULDER INSTABILITY IN PATIENTS WITH EDS
 EDNF 2012 CONFERENCE LIVING WITH EDS SHOULDER INSTABILITY IN PATIENTS WITH EDS Keith Kenter, MD Associate Professor Sports Medicine & Shoulder Reconstruction Director, Orthopaedic Residency Program Department
EDNF 2012 CONFERENCE LIVING WITH EDS SHOULDER INSTABILITY IN PATIENTS WITH EDS Keith Kenter, MD Associate Professor Sports Medicine & Shoulder Reconstruction Director, Orthopaedic Residency Program Department
Rehabilitation Guidelines for Arthroscopic Capsular Shift
 Rehabilitation Guidelines for Arthroscopic Capsular Shift The anatomic configuration of the shoulder joint (glenohumeral joint) is often compared to a golf ball on a tee. This is because the articular
Rehabilitation Guidelines for Arthroscopic Capsular Shift The anatomic configuration of the shoulder joint (glenohumeral joint) is often compared to a golf ball on a tee. This is because the articular
Knee Injuries What are the ligaments of the knee?
 As sporting participants or observers, we often hear a variety of terms used to describe sport-related injuries. Terms such as sprains, strains and tears are used to describe our aches and pains following
As sporting participants or observers, we often hear a variety of terms used to describe sport-related injuries. Terms such as sprains, strains and tears are used to describe our aches and pains following
Injuries to Upper Limb
 Injuries to Upper Limb 1 The following is a list of common sporting conditions and injuries. The severity of each condition may lead to different treatment protocols and certainly varying levels of intervention.
Injuries to Upper Limb 1 The following is a list of common sporting conditions and injuries. The severity of each condition may lead to different treatment protocols and certainly varying levels of intervention.
Rehabilitation Guidelines for Anterior Shoulder Reconstruction with Arthroscopic Bankart Repair
 Rehabilitation Guidelines for Anterior Shoulder Reconstruction with Arthroscopic Bankart Repair The anatomic configuration of the shoulder joint (glenohumeral joint) is often compared to a golf ball on
Rehabilitation Guidelines for Anterior Shoulder Reconstruction with Arthroscopic Bankart Repair The anatomic configuration of the shoulder joint (glenohumeral joint) is often compared to a golf ball on
28% have partial tear of the rotator cuff.
 ROTATOR CUFF TENDON RUPTURE Anatomy: 1. Rotator cuff consists of: Subscapularis anteriorly, Supraspinatus superiorly and Infraspinatus and Teres minor posteriorly. 2 Biceps tendon is present in the rotator
ROTATOR CUFF TENDON RUPTURE Anatomy: 1. Rotator cuff consists of: Subscapularis anteriorly, Supraspinatus superiorly and Infraspinatus and Teres minor posteriorly. 2 Biceps tendon is present in the rotator
Diagnosis of Acromioclavicular Joint Injuries
 PO Box 15 Rocky Hill, CT 06067 (860) 463-9003 Chiroeducation@aol.com www.chirocredit.com ChiroCredit.com is proud to present a section from one of our continuing education programs: Physical Diagnosis
PO Box 15 Rocky Hill, CT 06067 (860) 463-9003 Chiroeducation@aol.com www.chirocredit.com ChiroCredit.com is proud to present a section from one of our continuing education programs: Physical Diagnosis
Shoulder Arthropathies. Crystal Skovly, PA-C Orthopedic Institute Yankton, SD
 Shoulder Arthropathies Crystal Skovly, PA-C Orthopedic Institute Yankton, SD Covered Glenohumeral Arthritis Impingement Syndrome Rotator Cuff Tears Rupture of the Long Head Biceps Tendon Shoulder Instability
Shoulder Arthropathies Crystal Skovly, PA-C Orthopedic Institute Yankton, SD Covered Glenohumeral Arthritis Impingement Syndrome Rotator Cuff Tears Rupture of the Long Head Biceps Tendon Shoulder Instability
Sports Medicine. Assessing and Diagnosing Shoulder Injuries in Pediatric and Adolescent Patients
 Sports Medicine Assessing and Diagnosing Shoulder Injuries in Pediatric and Adolescent Patients Sports Medicine at Nationwide Children s Hospital Nationwide Children s Hospital Sports Medicine includes
Sports Medicine Assessing and Diagnosing Shoulder Injuries in Pediatric and Adolescent Patients Sports Medicine at Nationwide Children s Hospital Nationwide Children s Hospital Sports Medicine includes
SHOULDER ACROMIOPLASTY/ SHOULDER DECOMPRESSION
 ORTHOPAEDIC WARD: 01-293 8687 /01-293 6602 BEACON CENTRE FOR ORTHOPAEDICS: 01-2937575 PHYSIOTHERAPY DEPARTMENT: 01-2936692 GUIDELINES FOR PATIENTS HAVING A SHOULDER ACROMIOPLASTY/ SHOULDER DECOMPRESSION
ORTHOPAEDIC WARD: 01-293 8687 /01-293 6602 BEACON CENTRE FOR ORTHOPAEDICS: 01-2937575 PHYSIOTHERAPY DEPARTMENT: 01-2936692 GUIDELINES FOR PATIENTS HAVING A SHOULDER ACROMIOPLASTY/ SHOULDER DECOMPRESSION
Dr. Benjamin Hewitt. Shoulder Stabilisation
 Please contactmethroughthegoldcoasthospitaswityouhaveanyproblemsafteryoursurgery. Dr. Benjamin Hewitt Orthopaedic Surgeon Shoulder Stabilisation The shoulder is the most flexible joint in the body, allowing
Please contactmethroughthegoldcoasthospitaswityouhaveanyproblemsafteryoursurgery. Dr. Benjamin Hewitt Orthopaedic Surgeon Shoulder Stabilisation The shoulder is the most flexible joint in the body, allowing
Rehabilitation Guidelines for Shoulder Arthroscopy
 Rehabilitation Guidelines for Shoulder Arthroscopy Front View Long head of bicep Acromion Figure 1 Shoulder anatomy Supraspinatus Image Copyright 2010 UW Health Sports Medicine Center. Short head of bicep
Rehabilitation Guidelines for Shoulder Arthroscopy Front View Long head of bicep Acromion Figure 1 Shoulder anatomy Supraspinatus Image Copyright 2010 UW Health Sports Medicine Center. Short head of bicep
Internal Impingement in the Overhead Athlete: A Correlation of Findings on MRI and Arthroscopic Evaluation
 Internal Impingement in the Overhead Athlete: A Correlation of Findings on MRI and Arthroscopic Evaluation Lee D Kaplan, MD J Towers, MD PJ McMahon, MD CH Harner,, MD RW Rodosky,, MD Thrower s shoulder
Internal Impingement in the Overhead Athlete: A Correlation of Findings on MRI and Arthroscopic Evaluation Lee D Kaplan, MD J Towers, MD PJ McMahon, MD CH Harner,, MD RW Rodosky,, MD Thrower s shoulder
5/7/2009 SHOULDER) CONDITIONS OF THE SHOULDER NOW IT TIME TO TEST YOU ICD-9 SKILLS: PLEASE APPEND THE APPROPRIATE DIAGNOSIS CODE FOR EACH:
 CONDITIONS OF THE SHOULDER NOW IT TIME TO TEST YOU ICD-9 SKILLS: PLEASE APPEND THE APPROPRIATE DIAGNOSIS CODE FOR EACH:") SHOULDER CONDITIONS OF THE SHOULDER AND THEIR TREATMENT Presented by Kevin Solinsky, CPC,CPC-I,CEDC, CEMC The is a major joint and plays a large part in daily life, particularly for athletes and those
SHOULDER CONDITIONS OF THE SHOULDER AND THEIR TREATMENT Presented by Kevin Solinsky, CPC,CPC-I,CEDC, CEMC The is a major joint and plays a large part in daily life, particularly for athletes and those
Shoulder Examination
 Shoulder Examination Summary Inspection Palpation Movement Special Tests Neurological examination Introduction Shoulder disorders are can be broadly classified into the following types: Pain Stiffness
Shoulder Examination Summary Inspection Palpation Movement Special Tests Neurological examination Introduction Shoulder disorders are can be broadly classified into the following types: Pain Stiffness
10/16/2012. Marc J Breslow, MD Illinois Bone and Joint Institute Morton Grove, Des Plaines
 Orthopaedic Management of Shoulder Pathology Marc J Breslow, MD Illinois Bone and Joint Institute Morton Grove, Des Plaines Opening Statements IBJI Began fall 2007 9000 Waukegan Rd, Morton Grove 900 Rand
Orthopaedic Management of Shoulder Pathology Marc J Breslow, MD Illinois Bone and Joint Institute Morton Grove, Des Plaines Opening Statements IBJI Began fall 2007 9000 Waukegan Rd, Morton Grove 900 Rand
X-Ray Rounds: (Plain) Radiographic Evaluation of the Shoulder
 Radiographic Evaluation of the Shoulder") X-Ray Rounds: (Plain) Radiographic Evaluation of the Shoulder Anatomy 3 Bones Humerus Scapula Clavicle 3 Joints Glenohumeral Acromioclavicular Sternoclavicular 1 Articulation Scapulothoracic Anatomy Humerus
X-Ray Rounds: (Plain) Radiographic Evaluation of the Shoulder Anatomy 3 Bones Humerus Scapula Clavicle 3 Joints Glenohumeral Acromioclavicular Sternoclavicular 1 Articulation Scapulothoracic Anatomy Humerus
Upper limb injuries. Traumatology RHS 231 Dr. Einas Al-Eisa
 Upper limb injuries Traumatology RHS 231 Dr. Einas Al-Eisa Pain in the limbs: May be classified under 4 headings: 1. Joint pain 2. Soft tissue pain 3. Neurogenic pain 4. Orthopaedic causes (fractures,
Upper limb injuries Traumatology RHS 231 Dr. Einas Al-Eisa Pain in the limbs: May be classified under 4 headings: 1. Joint pain 2. Soft tissue pain 3. Neurogenic pain 4. Orthopaedic causes (fractures,
SHOULDER PAIN. Procedures: Subacromial, Glenohumeral and Acromioclavicular Injections Nonprocedural Treatments
 SHOULDER PAIN Anatomy Conditions: Muscular Spasm Pinched Nerve Rotator Cuff Tendonitis Procedures: Subacromial, Glenohumeral and Acromioclavicular Injections Nonprocedural Treatments Surgery: Rotator Cuff
SHOULDER PAIN Anatomy Conditions: Muscular Spasm Pinched Nerve Rotator Cuff Tendonitis Procedures: Subacromial, Glenohumeral and Acromioclavicular Injections Nonprocedural Treatments Surgery: Rotator Cuff
Musculoskeletal: Acute Lower Back Pain
 Musculoskeletal: Acute Lower Back Pain Acute Lower Back Pain Back Pain only Sciatica / Radiculopathy Possible Cord or Cauda Equina Compression Possible Spinal Canal Stenosis Red Flags Initial conservative
Musculoskeletal: Acute Lower Back Pain Acute Lower Back Pain Back Pain only Sciatica / Radiculopathy Possible Cord or Cauda Equina Compression Possible Spinal Canal Stenosis Red Flags Initial conservative
CAPPAGH NATIONAL ORTHOPAEDIC HOSPITAL, FINGLAS, DUBLIN 11. The Sisters of Mercy. Rotator Cuff Repair
 1.0 Policy Statement... 2 2.0 Purpose... 2 3.0 Scope... 2 4.0 Health & Safety... 2 5.0 Responsibilities... 2 6.0 Definitions and Abbreviations... 3 7.0 Guideline... 3 7.1 Pre-Operative... 3 7.2 Post-Operative...
1.0 Policy Statement... 2 2.0 Purpose... 2 3.0 Scope... 2 4.0 Health & Safety... 2 5.0 Responsibilities... 2 6.0 Definitions and Abbreviations... 3 7.0 Guideline... 3 7.1 Pre-Operative... 3 7.2 Post-Operative...
Bankart Repair using the Smith & Nephew BIORAPTOR 2.9 Suture Anchor
 Shoulder Series Technique Guide *smith&nephew BIORAPTOR 2.9 Suture Anchor Bankart Repair using the Smith & Nephew BIORAPTOR 2.9 Suture Anchor Gary M. Gartsman, M.D. Introduction Arthroscopic studies of
Shoulder Series Technique Guide *smith&nephew BIORAPTOR 2.9 Suture Anchor Bankart Repair using the Smith & Nephew BIORAPTOR 2.9 Suture Anchor Gary M. Gartsman, M.D. Introduction Arthroscopic studies of
INJURIES OF THE HAND AND WRIST By Derya Dincer, M.D.
 05/05/2007 INJURIES OF THE HAND AND WRIST By Derya Dincer, M.D. Hand injuries, especially the fractures of metacarpals and phalanges, are the most common fractures in the skeletal system. Hand injuries
05/05/2007 INJURIES OF THE HAND AND WRIST By Derya Dincer, M.D. Hand injuries, especially the fractures of metacarpals and phalanges, are the most common fractures in the skeletal system. Hand injuries
Rehabilitation Guidelines For SLAP Lesion Repair
 Rehabilitation Guidelines For SLAP Lesion Repair The anatomic configuration of the shoulder joint (glenohumeral joint) is often compared to a golf ball on a tee. This is because the articular surface of
Rehabilitation Guidelines For SLAP Lesion Repair The anatomic configuration of the shoulder joint (glenohumeral joint) is often compared to a golf ball on a tee. This is because the articular surface of
Shoulder Tendonitis. Brett Sanders, MD Center For Sports Medicine and Orthopaedic 2415 McCallie Ave. Chattanooga, TN (423) 624-2696
 624-2696") Shoulder Tendonitis Brett Sanders, MD Center For Sports Medicine and Orthopaedic 2415 McCallie Ave. Chattanooga, TN (423) 624-2696 Shoulder tendinitis is a common overuse injury in sports (such as swimming,
Shoulder Tendonitis Brett Sanders, MD Center For Sports Medicine and Orthopaedic 2415 McCallie Ave. Chattanooga, TN (423) 624-2696 Shoulder tendinitis is a common overuse injury in sports (such as swimming,
ACL plastik, erfarenheter av. tidig kirurgisk behandling. tidig kirurgisk behandling 6/12/2013
 in sports Per Renström, MD, PhD Professor emeritus,,, Sweden Member ATP and ITF Sports Science and Medical Committees Physician Swedish Football Association Presentation at the IOC Advanced team physician
in sports Per Renström, MD, PhD Professor emeritus,,, Sweden Member ATP and ITF Sports Science and Medical Committees Physician Swedish Football Association Presentation at the IOC Advanced team physician
Anterior Capsular Repair Rehabilitation Program Methodist Sports Medicine Center, Indianapolis, IN Department of Physical Therapy
 Anterior Capsular Repair Rehabilitation Program Methodist Sports Medicine Center, Indianapolis, IN Department of Physical Therapy Anterior Capsule reconstruction is a surgical procedure utilized for anterior
Anterior Capsular Repair Rehabilitation Program Methodist Sports Medicine Center, Indianapolis, IN Department of Physical Therapy Anterior Capsule reconstruction is a surgical procedure utilized for anterior
MRI shoulder: troubleshooting the cuff and instability. Phil Hughes Plymouth
 MRI shoulder: troubleshooting the cuff and instability Phil Hughes Plymouth Shoulder Pathways Pain (subacromial/cuff) Stiffness (Frozen shoulder/oa) Weakness (Query cuff tear) Instability General Practice
MRI shoulder: troubleshooting the cuff and instability Phil Hughes Plymouth Shoulder Pathways Pain (subacromial/cuff) Stiffness (Frozen shoulder/oa) Weakness (Query cuff tear) Instability General Practice
Clients w/ Orthopedic, Injury and Rehabilitation Concerns. Chapter 21
 Clients w/ Orthopedic, Injury and Rehabilitation Concerns Chapter 21 Terminology Macrotrauma A specific, sudden episode of overload injury to a given tissue, resulting in disrupted tissue integrity (Acute)
Clients w/ Orthopedic, Injury and Rehabilitation Concerns Chapter 21 Terminology Macrotrauma A specific, sudden episode of overload injury to a given tissue, resulting in disrupted tissue integrity (Acute)
Rehabilitation Guidelines for Posterior Shoulder Reconstruction with or without Labral Repair
 Rehabilitation Guidelines for Posterior Shoulder Reconstruction with or without Labral Repair The anatomic configuration of the shoulder joint (glenohumeral joint) is often compared to a golf ball on a
Rehabilitation Guidelines for Posterior Shoulder Reconstruction with or without Labral Repair The anatomic configuration of the shoulder joint (glenohumeral joint) is often compared to a golf ball on a
Rotator Cuff Repair and Rehabilitation
 1 Rotator Cuff Repair and Rehabilitation Surgical Indications and Considerations Anatomical Considerations: The rotator cuff complex is comprised of four tendons from four muscles: supraspinatus, infraspinatus,
1 Rotator Cuff Repair and Rehabilitation Surgical Indications and Considerations Anatomical Considerations: The rotator cuff complex is comprised of four tendons from four muscles: supraspinatus, infraspinatus,
Arthroscopic Labral Repair Protocol-Type II, IV, and Complex Tears:
 Department of Rehabilitation Services Physical Therapy This protocol has been adopted from Brotzman & Wilk, which has been published in Brotzman SB, Wilk KE, Clinical Orthopeadic Rehabilitation. Philadelphia,
Department of Rehabilitation Services Physical Therapy This protocol has been adopted from Brotzman & Wilk, which has been published in Brotzman SB, Wilk KE, Clinical Orthopeadic Rehabilitation. Philadelphia,
THE SHOULDER JOINT T H E G L E N O H U M E R A L ( G H ) J O I N T
 J O I N T") THE SHOULDER JOINT T H E G L E N O H U M E R A L ( G H ) J O I N T CLARIFICATION OF TERMS Shoulder girdle = scapula and clavicle Shoulder joint (glenohumeral joint) = scapula and humerus Lippert, p115
THE SHOULDER JOINT T H E G L E N O H U M E R A L ( G H ) J O I N T CLARIFICATION OF TERMS Shoulder girdle = scapula and clavicle Shoulder joint (glenohumeral joint) = scapula and humerus Lippert, p115
UHealth Sports Medicine
 UHealth Sports Medicine Rehabilitation Guidelines for Arthroscopic Rotator Cuff Repair Type 2 Repairs with Bicep Tenodesis (+/- subacromial decompression) The rehabilitation guidelines are presented in
UHealth Sports Medicine Rehabilitation Guidelines for Arthroscopic Rotator Cuff Repair Type 2 Repairs with Bicep Tenodesis (+/- subacromial decompression) The rehabilitation guidelines are presented in
SLAP Repair Protocol Arthroscopic Labral Repair Protocols (Type II, IV and Complex Tears)
") SLAP Repair Protocol Arthroscopic Labral Repair Protocols (Type II, IV and Complex Tears) This protocol has been modified and is being used with permission from the BWH Sports and Shoulder Service. The
SLAP Repair Protocol Arthroscopic Labral Repair Protocols (Type II, IV and Complex Tears) This protocol has been modified and is being used with permission from the BWH Sports and Shoulder Service. The
Abstract Objective: To review the mechanism, surgical procedures, and rehabilitation techniques used with an athlete suffering from chronic anterior
 Abstract Objective: To review the mechanism, surgical procedures, and rehabilitation techniques used with an athlete suffering from chronic anterior glenohumeral instability and glenoid labral tear. Background:
Abstract Objective: To review the mechanism, surgical procedures, and rehabilitation techniques used with an athlete suffering from chronic anterior glenohumeral instability and glenoid labral tear. Background:
ARTHROSCOPIC (KEY-HOLE) SHOULDER SURGERY
 SHOULDER SURGERY") ARTHROSCOPIC (KEY-HOLE) SHOULDER SURGERY Information Leaflet Your Health. Our Priority. Page 2 of 8 What is arthroscopic ( key-hole ) surgery? Key-hole surgery is the technique of performing surgery though
ARTHROSCOPIC (KEY-HOLE) SHOULDER SURGERY Information Leaflet Your Health. Our Priority. Page 2 of 8 What is arthroscopic ( key-hole ) surgery? Key-hole surgery is the technique of performing surgery though
Rotator Cuff Tears. Anatomy
 Copyright 2011 American Academy of Orthopaedic Surgeons Rotator Cuff Tears A rotator cuff tear is a common cause of pain and disability among adults. In 2008, close to 2 million people in the United States
Copyright 2011 American Academy of Orthopaedic Surgeons Rotator Cuff Tears A rotator cuff tear is a common cause of pain and disability among adults. In 2008, close to 2 million people in the United States
Biceps Tenodesis Protocol
 Department of Rehabilitation Services Physical Therapy The intent of this protocol is to provide the clinician with a guideline of the postoperative rehabilitation course of a patient that has undergone
Department of Rehabilitation Services Physical Therapy The intent of this protocol is to provide the clinician with a guideline of the postoperative rehabilitation course of a patient that has undergone
Chapter 5. The Shoulder Joint. The Shoulder Joint. Bones. Bones. Bones
 Copyright The McGraw-Hill Companies, Inc. Reprinted by permission. Chapter 5 The Shoulder Joint Structural Kinesiology R.T. Floyd, Ed.D, ATC, CSCS Structural Kinesiology The Shoulder Joint 5-1 The Shoulder
Copyright The McGraw-Hill Companies, Inc. Reprinted by permission. Chapter 5 The Shoulder Joint Structural Kinesiology R.T. Floyd, Ed.D, ATC, CSCS Structural Kinesiology The Shoulder Joint 5-1 The Shoulder
Imaging of Sports Injuries
 Imaging of Sports Injuries Capable of tremendous mobility Paradox Must be loose enough to function but stable enough to prevent symptoms Shoulder injuries occur when the balance between stability & mobility
Imaging of Sports Injuries Capable of tremendous mobility Paradox Must be loose enough to function but stable enough to prevent symptoms Shoulder injuries occur when the balance between stability & mobility
.org. Rotator Cuff Tears: Surgical Treatment Options. When Rotator Cuff Surgery is Recommended. Surgical Repair Options
 Rotator Cuff Tears: Surgical Treatment Options Page ( 1 ) The following article provides in-depth information about surgical treatment for rotator cuff injuries, and is a continuation of the article Rotator
Rotator Cuff Tears: Surgical Treatment Options Page ( 1 ) The following article provides in-depth information about surgical treatment for rotator cuff injuries, and is a continuation of the article Rotator
SCAPULAR FRACTURES. Jai Relwani, Shoulder Fellow, Reading Shoulder Unit, Reading.
 SCAPULAR FRACTURES Jai Relwani, Shoulder Fellow, Reading Shoulder Unit, Reading. Aims Anatomy Incidence/Importance Mechanism Classification Principles of treatment Specific variations Conclusion Anatomy
SCAPULAR FRACTURES Jai Relwani, Shoulder Fellow, Reading Shoulder Unit, Reading. Aims Anatomy Incidence/Importance Mechanism Classification Principles of treatment Specific variations Conclusion Anatomy
The Shoulder Complex & Shoulder Girdle
 The Shoulder Complex & Shoulder Girdle The shoulder complex 4 articulations involving The sternum The clavicle The ribs The scapula and The humerus Bony Landmarks provide attachment points for muscles
The Shoulder Complex & Shoulder Girdle The shoulder complex 4 articulations involving The sternum The clavicle The ribs The scapula and The humerus Bony Landmarks provide attachment points for muscles
Shoulder Impingement Syndrome
 Shoulder Impingement Syndrome Causes The shoulder joint is stabilized and moved mainly by the four tendons of the socalled rotator cuff. These tendons are situated in a narrow bony canal between the ball
Shoulder Impingement Syndrome Causes The shoulder joint is stabilized and moved mainly by the four tendons of the socalled rotator cuff. These tendons are situated in a narrow bony canal between the ball
North Shore Shoulder Dr.Robert E. McLaughlin II 1-855-SHOULDER 978-969-3624 Fax: 978-921-7597 www.northshoreshoulder.com
 North Shore Shoulder Dr.Robert E. McLaughlin II 1-855-SHOULDER 978-969-3624 Fax: 978-921-7597 www.northshoreshoulder.com Physical Therapy Protocol for Patients Following Shoulder Surgery -Rotator Cuff
North Shore Shoulder Dr.Robert E. McLaughlin II 1-855-SHOULDER 978-969-3624 Fax: 978-921-7597 www.northshoreshoulder.com Physical Therapy Protocol for Patients Following Shoulder Surgery -Rotator Cuff
Combined SLAP with Arthroscopic Rotator Cuff Repair Large to Massive Tears = or > 3 cm
 Combined SLAP with Arthroscopic Rotator Cuff Repair Large to Massive Tears = or > 3 cm *It is the treating therapist s responsibility along with the referring physician s guidance to determine the actual
Combined SLAP with Arthroscopic Rotator Cuff Repair Large to Massive Tears = or > 3 cm *It is the treating therapist s responsibility along with the referring physician s guidance to determine the actual
What is a Sports Physician?
 What is a Sports Physician? Dr Mike Bundy MBBS MRCGP Dip Sports Med FFSEM Consultant in Sport and Exercise Medicine Medical Director at Pure Sports Medicine Ex-England Rugby senior team Doctor www.puresportsmed.com
What is a Sports Physician? Dr Mike Bundy MBBS MRCGP Dip Sports Med FFSEM Consultant in Sport and Exercise Medicine Medical Director at Pure Sports Medicine Ex-England Rugby senior team Doctor www.puresportsmed.com
COMMON ROWING INJURIES
 COMMON ROWING INJURIES Prevention and Treatment Jo A. Hannafin, MD, PhD Professor of Orthopaedic Surgery Hospital for Special Surgery, Cornell University Medical College Team Physician, US Rowing FISA
COMMON ROWING INJURIES Prevention and Treatment Jo A. Hannafin, MD, PhD Professor of Orthopaedic Surgery Hospital for Special Surgery, Cornell University Medical College Team Physician, US Rowing FISA
 ROTATOR CUFF SYNDROME Arbejds- og Miljømedicinsk Årsmøde 2008 ROTATOR CUFF SYNDROME = SHOULDER PAIN Steen Bo Kalms, Shoulder- and Elbow Surgeon ROTATOR CUFF SYNDROME VERY COMMON DIAGNOSIS ON REFERRED PTT
ROTATOR CUFF SYNDROME Arbejds- og Miljømedicinsk Årsmøde 2008 ROTATOR CUFF SYNDROME = SHOULDER PAIN Steen Bo Kalms, Shoulder- and Elbow Surgeon ROTATOR CUFF SYNDROME VERY COMMON DIAGNOSIS ON REFERRED PTT
POSTERIOR LABRAL (BANKART) REPAIRS
 REPAIRS") LOURDES MEDICAL ASSOCIATES Sean Mc Millan, DO Director of Orthopaedic Sports Medicine & Arthroscopy 2103 Burlington-Mount Holly Rd Burlington, NJ 08016 (609) 747-9200 (office) (609) 747-1408 (fax) http://orthodoc.aaos.org/drmcmillan
LOURDES MEDICAL ASSOCIATES Sean Mc Millan, DO Director of Orthopaedic Sports Medicine & Arthroscopy 2103 Burlington-Mount Holly Rd Burlington, NJ 08016 (609) 747-9200 (office) (609) 747-1408 (fax) http://orthodoc.aaos.org/drmcmillan
SLAP repair. An information guide for patients. Delivering the best in care. UHB is a no smoking Trust
 SLAP repair An information guide for patients Delivering the best in care UHB is a no smoking Trust To see all of our current patient information leaflets please visit www.uhb.nhs.uk/patient-information-leaflets.htm
SLAP repair An information guide for patients Delivering the best in care UHB is a no smoking Trust To see all of our current patient information leaflets please visit www.uhb.nhs.uk/patient-information-leaflets.htm
10/1/2007. Philosophy. Pune Shoulder Rehabilitation Programme (PSRP) 9 th Annual TRAC meeting, Budapest. Principles -I. Design. Study-I.
 9 th Annual TRAC meeting, Budapest. Principles -I. Design. Study-I.") Dr. Ashish Babhulkar D.Orth., DNB(Orth.), MCh.Orth.(Liverpool,UK.),FRCS(Tr. & Orth.) Shoulder & Joint Replacement Surgeon Pune, India Pune Shoulder Rehabilitation Programme (PSRP) Philosophy Design an
Dr. Ashish Babhulkar D.Orth., DNB(Orth.), MCh.Orth.(Liverpool,UK.),FRCS(Tr. & Orth.) Shoulder & Joint Replacement Surgeon Pune, India Pune Shoulder Rehabilitation Programme (PSRP) Philosophy Design an
Completing the Loop: Management of the Adolescent Sports Injury. Adam Thomas, PT, DPT, ATC
 : Management of the Adolescent Sports Injury Adam Thomas, PT, DPT, ATC https://www.youtube.com/watch?v=vbufpo 8s3As On field assessment can be the most efficient when the health care provider has observed
: Management of the Adolescent Sports Injury Adam Thomas, PT, DPT, ATC https://www.youtube.com/watch?v=vbufpo 8s3As On field assessment can be the most efficient when the health care provider has observed
.org. Clavicle Fracture (Broken Collarbone) Anatomy. Description. Cause. Symptoms
 Anatomy. Description. Cause. Symptoms") Clavicle Fracture (Broken Collarbone) Page ( 1 ) A broken collarbone is also known as a clavicle fracture. This is a very common fracture that occurs in people of all ages. Anatomy The collarbone (clavicle)
Clavicle Fracture (Broken Collarbone) Page ( 1 ) A broken collarbone is also known as a clavicle fracture. This is a very common fracture that occurs in people of all ages. Anatomy The collarbone (clavicle)
ROTATOR CUFF TEARS SMALL
 LOURDES MEDICAL ASSOCIATES Sean Mc Millan, DO Director of Orthopaedic Sports Medicine & Arthroscopy 2103 Burlington-Mount Holly Rd Burlington, NJ 08016 (609) 747-9200 (office) (609) 747-1408 (fax) http://orthodoc.aaos.org/drmcmillan
LOURDES MEDICAL ASSOCIATES Sean Mc Millan, DO Director of Orthopaedic Sports Medicine & Arthroscopy 2103 Burlington-Mount Holly Rd Burlington, NJ 08016 (609) 747-9200 (office) (609) 747-1408 (fax) http://orthodoc.aaos.org/drmcmillan
Orthopaedic and Spine Institute 21 Spurs Lane, Suite 245, San Antonio, TX 78240 www.saspine.com Tel# 210-487-7463
 Phase I Passive Range of Motion Phase (postop week 1-2) Minimize shoulder pain and inflammatory response Achieve gradual restoration of gentle active range of motion Enhance/ensure adequate scapular function
Phase I Passive Range of Motion Phase (postop week 1-2) Minimize shoulder pain and inflammatory response Achieve gradual restoration of gentle active range of motion Enhance/ensure adequate scapular function
Arthroscopic Labrum Repair of the Shoulder (SLAP)
") Anatomy Arthroscopic Labrum Repair of the Shoulder (SLAP) The shoulder joint involves three bones: the scapula (shoulder blade), the clavicle (collarbone) and the humerus (upper arm bone). The humeral
Anatomy Arthroscopic Labrum Repair of the Shoulder (SLAP) The shoulder joint involves three bones: the scapula (shoulder blade), the clavicle (collarbone) and the humerus (upper arm bone). The humeral
Radiology Corner. The Superior Labrum, Anterior-to-Posterior SLAP Lesion
 Radiology Corner The Superior Labrum, Anterior-to-Posterior SLAP Lesion The Superior Labrum, Anterior-to-Posterior SLAP Lesion Guarantor: Col Timothy G. Sanders, MC, USAF (Ret.) 1 Contributors: Col Timothy
Radiology Corner The Superior Labrum, Anterior-to-Posterior SLAP Lesion The Superior Labrum, Anterior-to-Posterior SLAP Lesion Guarantor: Col Timothy G. Sanders, MC, USAF (Ret.) 1 Contributors: Col Timothy
Postoperative Protocol For Posterior Labral Repair/ Capsular Plication-- Dr. Trueblood
 Postoperative Protocol For Posterior Labral Repair/ Capsular Plication-- Dr. Trueblood Indications: Posterior shoulder instability is a relatively uncommon finding in normal adult shoulders. The most common
Postoperative Protocol For Posterior Labral Repair/ Capsular Plication-- Dr. Trueblood Indications: Posterior shoulder instability is a relatively uncommon finding in normal adult shoulders. The most common
Rehabilitation Guidelines for Biceps Tenodesis
 UW Health Sports Rehabilitation Rehabilitation Guidelines for Biceps Tenodesis The shoulder has two primary joints. One part of the shoulder blade, called the glenoid fossa forms a flat, shallow surface.
UW Health Sports Rehabilitation Rehabilitation Guidelines for Biceps Tenodesis The shoulder has two primary joints. One part of the shoulder blade, called the glenoid fossa forms a flat, shallow surface.
Physical Therapy for Shoulder. Joseph Lorenzetti PT, DPT, MTC Catholic Health Athleticare Kenmore 1495 Military Road Kenmore, NY 14217
 Physical Therapy for Shoulder and Knee Pain Joseph Lorenzetti PT, DPT, MTC Catholic Health Athleticare Kenmore 1495 Military Road Kenmore, NY 14217 Physical Therapy for Shoulder and Knee Pain GOALS: Explain
Physical Therapy for Shoulder and Knee Pain Joseph Lorenzetti PT, DPT, MTC Catholic Health Athleticare Kenmore 1495 Military Road Kenmore, NY 14217 Physical Therapy for Shoulder and Knee Pain GOALS: Explain
Sports Injuries of the Foot and Ankle. Dr. Travis Kieckbusch August 7, 2014
 Sports Injuries of the Foot and Ankle Dr. Travis Kieckbusch August 7, 2014 Foot and Ankle Injuries in Athletes Lateral ankle sprains Syndesmosis sprains high ankle sprain Achilles tendon injuries Lisfranc
Sports Injuries of the Foot and Ankle Dr. Travis Kieckbusch August 7, 2014 Foot and Ankle Injuries in Athletes Lateral ankle sprains Syndesmosis sprains high ankle sprain Achilles tendon injuries Lisfranc
Outcome of Arthroscopic Repair of Type II SLAP Lesions in Worker_s Compensation Patients
 HSSJ (2007) 3: 58 62 DOI 10.1007/s11420-006-9023-2 ORIGINAL ARTICLE Outcome of Arthroscopic Repair of Type II SLAP Lesions in Worker_s Compensation Patients Nikhil N. Verma, MD & Ralph Garretson, MD &
HSSJ (2007) 3: 58 62 DOI 10.1007/s11420-006-9023-2 ORIGINAL ARTICLE Outcome of Arthroscopic Repair of Type II SLAP Lesions in Worker_s Compensation Patients Nikhil N. Verma, MD & Ralph Garretson, MD &
Dr Doron Sher MB.BS. MBiomedE, FRACS(Orth)
") Dr Doron Sher MB.BS. MBiomedE, FRACS(Orth) Knee, Shoulder, Elbow Surgery PATIENT NOTES ARTHROSCOPIC SHOULDER SURGERY I have suggested that you consider an Arthroscopic procedure to assess and treat your
Dr Doron Sher MB.BS. MBiomedE, FRACS(Orth) Knee, Shoulder, Elbow Surgery PATIENT NOTES ARTHROSCOPIC SHOULDER SURGERY I have suggested that you consider an Arthroscopic procedure to assess and treat your
Arthritis of the Shoulder
 Arthritis of the Shoulder In 2011, more than 50 million people in the United States reported that they had been diagnosed with some form of arthritis, according to the National Health Interview Survey.
Arthritis of the Shoulder In 2011, more than 50 million people in the United States reported that they had been diagnosed with some form of arthritis, according to the National Health Interview Survey.
Elbow Injuries and Disorders
 Elbow Injuries and Disorders Introduction Your elbow joint is made up of bone, cartilage, ligaments and fluid. Muscles and tendons help the elbow joint move. There are many injuries and disorders that
Elbow Injuries and Disorders Introduction Your elbow joint is made up of bone, cartilage, ligaments and fluid. Muscles and tendons help the elbow joint move. There are many injuries and disorders that
Shoulder Dyslexia: The Alphabet Soup. Alison Nguyen 4/13/06
 Shoulder Dyslexia: The Alphabet Soup Alison Nguyen 4/13/06 Mystery Cases Case 1 Case 2 Case 3 Case 4 Shoulder Dyslexia: The Alphabet Soup Shoulder dyslexia: addressing the endless alphabet soup Ant-inf
Shoulder Dyslexia: The Alphabet Soup Alison Nguyen 4/13/06 Mystery Cases Case 1 Case 2 Case 3 Case 4 Shoulder Dyslexia: The Alphabet Soup Shoulder dyslexia: addressing the endless alphabet soup Ant-inf
Rehabilitation Guidelines for Post-Operative Stiff Shoulder
 Rehabilitation Guidelines for Post-Operative Stiff Shoulder Please note that this is advisory information only. Your experiences may differ from those described. A fully qualified Physiotherapist must
Rehabilitation Guidelines for Post-Operative Stiff Shoulder Please note that this is advisory information only. Your experiences may differ from those described. A fully qualified Physiotherapist must
Temple Physical Therapy
 Temple Physical Therapy A General Overview of Common Neck Injuries For current information on Temple Physical Therapy related news and for a healthy and safe return to work, sport and recreation Like Us
Temple Physical Therapy A General Overview of Common Neck Injuries For current information on Temple Physical Therapy related news and for a healthy and safe return to work, sport and recreation Like Us
SLAP Repair Protocol
 SLAP Repair Protocol Anatomy and Biomechanics The shoulder is a wonderfully complex joint that is made up of the ball and socket connection between the humerus (ball) and the glenoid portion of the scapula
SLAP Repair Protocol Anatomy and Biomechanics The shoulder is a wonderfully complex joint that is made up of the ball and socket connection between the humerus (ball) and the glenoid portion of the scapula
ARTHROSCOPIC ROTATOR CUFF REPAIR PROTOCOL (DR. ROLF)
") ARTHROSCOPIC ROTATOR CUFF REPAIR PROTOCOL (DR. ROLF) Phase I Immediate Post Surgical Phase (Weeks 1-4): Maintain integrity of repair Diminish pain and inflammation Prevent muscular inhibition Independent
ARTHROSCOPIC ROTATOR CUFF REPAIR PROTOCOL (DR. ROLF) Phase I Immediate Post Surgical Phase (Weeks 1-4): Maintain integrity of repair Diminish pain and inflammation Prevent muscular inhibition Independent
Dr. Benjamin Hewitt. Subacramial Decompression & Rotator Cuff Repair
 Please contactmethroughthegoldcoasthospitaswityouhaveanyproblemsafteryoursurgery. Dr. Benjamin Hewitt Orthopaedic Surgeon Subacramial Decompression & Rotator Cuff Repair The Rotator Cuff consists of four
Please contactmethroughthegoldcoasthospitaswityouhaveanyproblemsafteryoursurgery. Dr. Benjamin Hewitt Orthopaedic Surgeon Subacramial Decompression & Rotator Cuff Repair The Rotator Cuff consists of four
THE REVERSE SHOULDER REPLACEMENT
 THE REVERSE SHOULDER REPLACEMENT The Reverse Shoulder Replacement is a newly approved implant that has been used successfully for over ten years in Europe. It was approved by the FDA for use in the U.S.A.
THE REVERSE SHOULDER REPLACEMENT The Reverse Shoulder Replacement is a newly approved implant that has been used successfully for over ten years in Europe. It was approved by the FDA for use in the U.S.A.
Open Rotator Cuff Repair Rehabilitation Program Methodist Sports Medicine Center, Indianapolis, IN Department of Physical Therapy
 Open Rotator Cuff Repair Rehabilitation Program Methodist Sports Medicine Center, Indianapolis, IN Department of Physical Therapy Rotator Cuff Repair is a surgical procedure utilized for a tear in the
Open Rotator Cuff Repair Rehabilitation Program Methodist Sports Medicine Center, Indianapolis, IN Department of Physical Therapy Rotator Cuff Repair is a surgical procedure utilized for a tear in the
Treatment Guide Wave Goodbye to Shoulder Pain
 Treatment Guide Wave Goodbye to Shoulder Pain Shoulder pain and injuries are extremely common whether due to exercise, age, overuse injuries or trauma. In fact, they account for nearly 20 percent of visits
Treatment Guide Wave Goodbye to Shoulder Pain Shoulder pain and injuries are extremely common whether due to exercise, age, overuse injuries or trauma. In fact, they account for nearly 20 percent of visits
Cigna Medical Coverage Policies Musculoskeletal Shoulder Surgery Arthroscopic and Open Procedures
 Cigna Medical Coverage Policies Musculoskeletal Shoulder Surgery Arthroscopic and Open Procedures Effective January 1, 2016 Instructions for use The following coverage policy applies to health benefit
Cigna Medical Coverage Policies Musculoskeletal Shoulder Surgery Arthroscopic and Open Procedures Effective January 1, 2016 Instructions for use The following coverage policy applies to health benefit