Federal Breach Notification Decision Tree and Tools
|
|
|
- Jeffrey Martin
- 9 years ago
- Views:
Transcription
1 Federal Breach Notification and Tools Disclaimer This document is copyright 2013 by the Long Term Care Consortium (LTCC). These materials may be reproduced and used only by long-term health care providers and their health care affiliates for their internal use, in connection with their efforts to comply with relevant legal rules and regulations. All other reproduction, transfer and use is prohibited without the express written consent of the LTCC. Neither the LTCC nor its members make any representation that use of these materials will ensure other legal compliance. LTCC Mission Statement To provide leadership and guidance to the long term care profession utilizing the member organizations collective knowledge, expertise and information resources to improve overall compliance efforts and reduce the overall burden of compliance through collaboration on important initiatives that are common to the profession. Breach Notification Overview On August 24, 2009, the Department of Health & Human Services Breach Notification for Unsecured Protected Health Information Interim Final Rule (Federal Breach Notification Rule) was published in the Federal Register as required by the American Recovery & Reinvestment Act of On January 25, 2013, the Final Rule was published to the Federal Register. The federal breach reporting requirements apply to HIPAA covered entities and their business associates. It requires covered entities to notify individuals whose unsecured protected health information (PHI) has been accessed, acquired or disclosed because of a breach, which is defined as the unauthorized acquisition, access, use or disclosure of PHI. The rule also outlines a few exceptions to the definition of a breach. Breaches of PHI are reportable unless covered entities and business associates perform a risk assessment which demonstrates there is a low probability that the PHI has been compromised. After a breach has been discovered, affected residents must be notified of the breach without unreasonable delay and no later than 60 days from the date of discovery. Breaches affecting more than 500 residents must be reported immediately to HHS and the media. Breaches affecting less than 500 residents are logged and reported to HHS on an annual basis. When calculating the number of Page 1 of 16

2 affected residents, take into consideration the structure of the organization all reporting is at the covered entity level. The rule provides updated guidance specifying the technologies and methodologies that render protected health information (PHI) unusable, unreadable, or indecipherable to unauthorized individuals and therefore not subject to the notification requirements because the information does not meet the unsecured protected health information criteria. Using the and Tools This document serves as a guide to determine if an incident involves a breach of PHI in a manner that requires notification of the affected residents and what method of notification is required under the federal breach regulation. This document does not address state security breach notification requirements. Each decision references additional information on subsequent pages which may be useful throughout the assessment of an incident. You will need to document your assessment process to support your conclusions. Though you may conclude that notification is not required under federal law, you should review any applicable state laws as well as your organization s policies and procedures to assess whether it is prudent to proceed with notification even though it may not be required. Sample notification letters to affected residents and the media are available on the LTCC site for your reference. Page 2 of 16

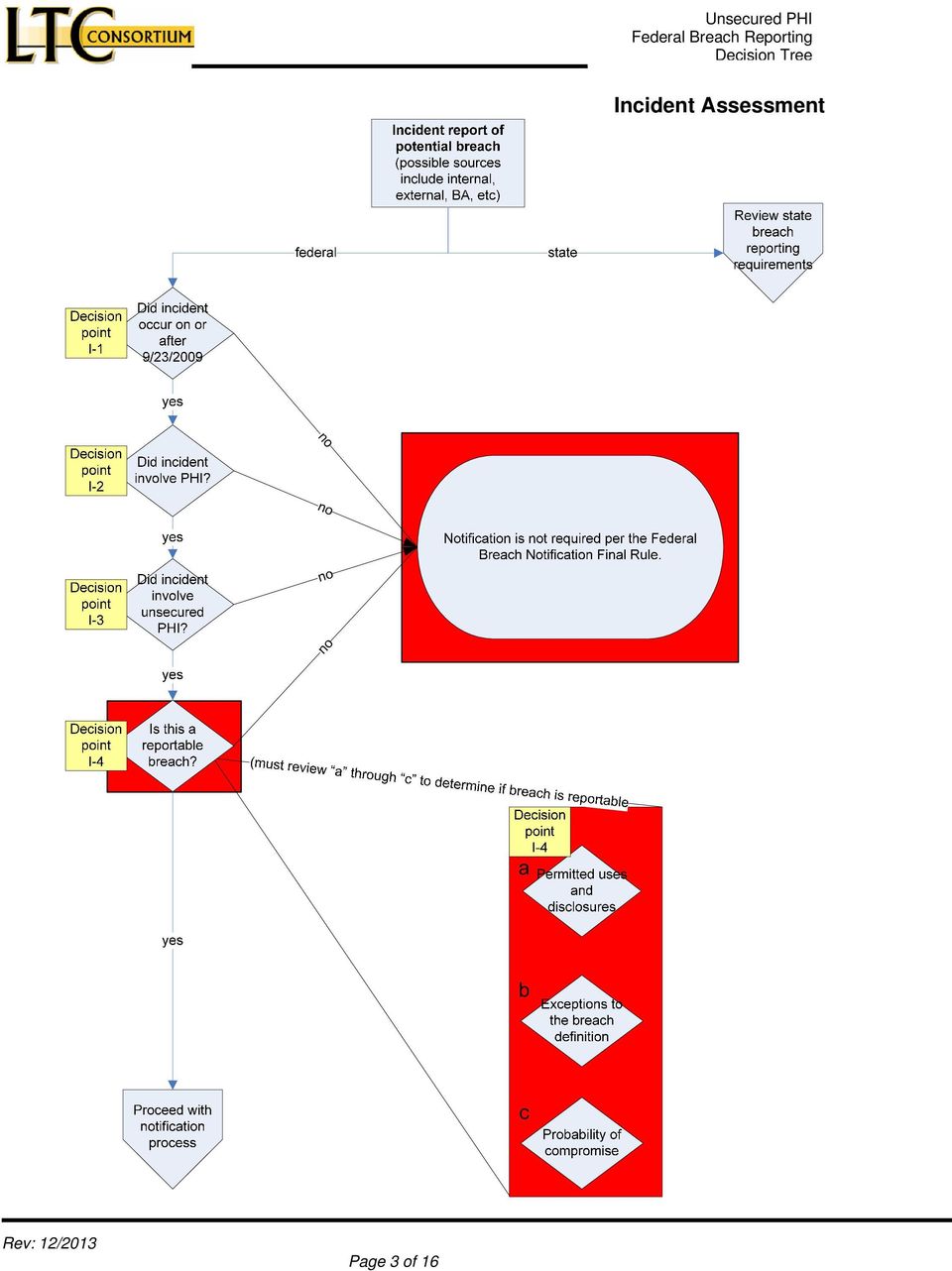
3 Incident Assessment no Page 3 of 16
4 Identification of PHI breach which requires federal notification (refer to incident assessment decision tree) Notification Process N-1 Has law enforcement requested a notification delay? yes N-2 What is the method of the request? written Delay notification for the time period specified, then proceed. verbal no Delay notification for up to 30 days, then proceed. Deliver notification to affected parties (see sample letter for notification requirements) Written notice to be delivered via firstclass mail to last known address or electronic notice via if agreed upon N-3 Does urgency exist because of possible imminent misuse? no yes Provide additional notice, such as by telephone These notifications must be delivered without unreasonable delay and in no case later than 60 days after breach discovery by the covered entity. In some instances, it may be unreasonable to wait 60 days. N-4 Is there out of date contact info for 10 or more individuals? yes Deliver substitute notice on CE website or media no N-5 Did breach involve more than 500 individuals? yes N-6 Did breach affect more than 500 residents from a state or jurisdication? yes no Track incident in breach log no Provide notice to Secretary HHS via website (insert link) Within 60 days of end of calendar year, deliver notification to Secretary, HHS for breaches discovered during preceding calendar year Provide notice to Secretary HHS via website Deliver notification to prominent media outlet for state or jurisdiction. (See sample press release) Page 4 of 16

5 Incident Assessment Points The effective date of this rule is September 23, Notification requirements apply to breaches that occurred on or after September 23, The HIPAA Rules define protected health information as the individually identifiable health information held or transmitted in any form or medium by HIPAA covered entities and business associates. Excluded from the definition of PHI is de-identified information as defined in the HIPAA Privacy Rule and listed below: De-identified health information: Health information that does not identify an individual and with respect to which there is no reasonable basis to believe that the information can be used to identify an individual is not individually identifiable health information (see section (a) or glossary). Page 5 of 16

6 I-3 Did incident involve unsecured PHI? Due to the variations in each entity s environment, no uniform standards exist for secured Protected Health Information. Each covered entity must perform a risk assessment to determine if PHI is secured. The Final Rule applies to unsecured PHI. The generally accepted definition of secured PHI is PHI that is rendered unusable, unreadable, or indecipherable to unauthorized individuals. Notification is not required for PHI that is considered secure. The Final Rule contains guidance specifying the technologies and methodologies that render PHI secure. PHI is rendered unusable, unreadable, or indecipherable to unauthorized individuals if one or more of the following applies: 1. Electronic PHI has been encrypted as specified in the HIPAA Security Rule by the use of a(n) process to transform data into a form in which there is a low probability of assigning meaning (to the data) without use of a confidential process or key (45 CFR definition of encryption) and such confidential process or key that might enable decryption has not been breached. To avoid a breach of the confidential process or key, these decryption tools should be stored on a device or at a location separate from the data that they are used to encrypt or decrypt. The encryption processes identified below have been tested by the National Institute of Standards and Technology (NIST) and judged to meet this standard. These publications were cited as potentially valuable resources, although not required by CMS, for technical personnel having knowledge of the covered entity s IT environment with specific questions and concerns about securing PHI. (i) Valid encryption processes for data at rest are consistent with NIST Special Publication , Guide to Storage Encryption Technologies for End User Devices. 1 (ii) Valid encryption processes for data in motion are those which comply, as appropriate, with NIST Special Publications , Guidelines for the Selection and Use of Transport Layer Security (TLS) Implementations 1 ; , Guide to IPsec VPNs; or , Guide to SSL VPNs 1, or others which are Federal Information Processing Standards (FIPS) validated. 1 ( Page 6 of 16

7 2. The media on which the PHI is stored or recorded has been destroyed in one of the following ways: (i) Paper, film, or other hard copy media have been shredded or destroyed such that the PHI cannot be read or otherwise cannot be reconstructed. Redaction is specifically excluded as a means of destruction. (ii) Electronic media have been cleared, purged, or destroyed consistent with NIST Special Publication , Guidelines for Media Sanitization 1 such that the PHI cannot be retrieved. In order for a use or disclosure of resident information to be considered a breach, the acquisition, use or disclosure of the PHI must be in violation of the HIPAA Privacy Rule. Permissible uses and disclosure under the Privacy Rule must fall into one of the categories below. The following are questions you must ask and answer as you document your efforts in confirming a breach or validating a permissible use or disclosure. PERMITTED USES AND DISCLOSURES 1. Was the PHI accessed, acquired, used or disclosed for treatment, payment or healthcare operations purposes (refer to your notice of privacy practices)? If No, go to question #2 If Yes, and the purpose was for treatment, it is not a breach. Page 7 of 16

8 If Yes, and the purpose was for payment or healthcare operations, was the PHI the minimum necessary amount for the given task? If Yes, it is not a breach. If No, go to the section Probability of Compromise. 2. Was the PHI acquired, used or disclosed incidental to a permitted use or disclosure? In order for a use or disclosure to be considered incidental, it must be related to a use or disclosure that is either permitted or required under the Privacy Rule and the amount of information must have been the minimum necessary for the intended purpose and reasonable safeguards must have been taken to keep the information confidential. For example, the following practices are permissible under the Privacy Rule, if reasonable precautions were taken to minimize the chance of incidental disclosures to others who may be nearby: a. Health care staff may orally coordinate services at nursing stations. b. Nurses or other health care professionals may discuss a resident s condition over the phone with a provider or legal representative. c. A health care professional may discuss lab test results with a resident or other provider in a joint treatment area. d. A physician may discuss a residents condition or treatment regimen in the resident s semi-private room. If Yes, it is not a breach. If No, go to question Was the PHI disclosed pursuant to and in compliance with a HIPAA-compliant authorization? If Yes, it is not a breach. If No, go to question Was the PHI accessed, acquired, used or disclosed for facility directory purposes in compliance with (a)? If Yes, it is not a breach. If No, go to question Was the PHI accessed, acquired, used or disclosed for involvement in the resident s care and notification purposes in compliance with (b)? Page 8 of 16

9 If Yes, it is not a breach. If No, go to question Was the PHI accessed, acquired, used or disclosed pursuant to uses and disclosures for which an authorization or opportunity to agree or object is not required? Was it: a. required by law, b. for public health activities, c. about victims of abuse, neglect or domestic violence, d. for health oversight activities, e. for judicial and administrative proceedings, f. for law enforcement purposes, g. about decedents, h. for cadaveric organ, eye or tissue donation purposes, i. for research purposes, j. to avert a serious threat to health or safety, k. for specialized government functions, OR l. for workers compensation purposes, AND m. in compliance with the requirements outlined in ? If Yes, it is not a breach. If No, go to question 7. EXCEPTIONS TO THE BREACH DEFINITION Corresponds to Section 1 of Breach Risk Tool Does the impermissible access, acquisition, use or disclosure fall under one of the following exceptions? 7. Was it an incidental access, use or disclosure by a workforce member of the covered entity or business associate: a. While acting under the organization s authority, and b. Made in good faith, and c. Within their scope of authority, and d. Does not result in a further use or disclosure? i. For example, a billing employee receives and opens an containing protected health information about a patient which a nurse mistakenly sent to the billing employee. The billing employee notices that he is not the intended recipient, alerts the nurse of the misdirected , and then deletes it. The billing employee unintentionally accessed protected health information to which he was not authorized to have access. However, the billing employee s Page 9 of 16

10 If Yes, there is no breach. If No, go to question 8. use of the information was done in good faith and within the scope of authority, and therefore, would not constitute a breach and notification would not be required, provided the employee did not further use or disclose the information accessed in a manner not permitted by the Privacy Rule. 8. Was it an inadvertent disclosure: a. By a person who is authorized to access protected health information at a covered entity or business associate, b. To another person authorized to access protected health information at the same covered entity or business associate, or organized health care arrangement in which the covered entity participates, and c. The information received as a result of such disclosure is not further used or disclosed in a manner not permitted by the Privacy Rule? i. For example, a nurse calls a doctor who provides medical information on a resident in response to the inquiry. It turns out the information was for the wrong resident and the information was not further used or disclosed by the doctor. If Yes, there is no breach. If No, go to question Was it a disclosure of protected health information where a covered entity or business associate has a good faith belief that an unauthorized person to whom the disclosure was made would not reasonably have been able to retain such information? i. For example, a medical records clerk hands a resident a copy of a medical record, but quickly realizes that it was another resident s record and requests the return of the record. In this case, if the medical records clerk can reasonably conclude that the resident could not have read or otherwise retained the information, then providing the medical record to the wrong resident does not constitute a breach. If Yes, there is no breach. If No, proceed to question 10. PROBABILITY OF COMPROMISE Page 10 of 16

11 Corresponds to Section 2 of Breach Risk Tool 10. Was the PHI accessed, acquired, used or disclosed by another entity governed by the HIPAA Privacy and Security Rules or a Federal Agency obligated to comply with the Privacy Act of 1974 and Federal Information Security Management Act (FISMA) of 2002? If Yes, were immediate steps taken to mitigate the impermissible use/disclosure/acquisition? For example: a. Was the recipient contacted and were satisfactory assurances obtained assuring that the PHI would not be further used or disclosed or would be destroyed? Or b. Was the PHI not accessed, opened, altered, transferred or otherwise compromised? For example, a mailing is returned unopened or through analysis it is determined that information on a laptop or computer was not accessed. If Yes, the probability of compromise is low. If No, go to question Do the circumstances of the PHI disclosure result in a low probability of compromise? a. What is the nature and extent of the protected health information involved, including the types of identifiers and the likelihood of re-identification? i. Was only minimal PHI acquired, accessed, used or disclosed such as just the patient name and the fact that services were received? ii. Did the PHI include the resident s name and type of services received? For example: were services from a specialized facility such as an infectious disease clinic or substance abuse provider? iii. Did the PHI include high risk information that could be used for identity theft such as name, social security number, date of birth, financial or credit card account numbers, driver's license number or state-issued identification card number or maiden name? iv. Did the PHI include only a limited data set as defined by the Privacy Rule and the likelihood of re-identification is low? For example, if the information included the zip code for a metropolitan city vs. a rural location. b. Who was the unauthorized person who used the protected health information or to whom the disclosure was made? c. Was the protected health information actually acquired or viewed? d. What is the extent to which the risk to the protected health information has been mitigated? Page 11 of 16

12 If the circumstances of the PHI disclosure indicate there is a low probability of compromise, no breach has occurred. Otherwise, there is a breach. Proceed with notification. Continue the investigation and document your decision. Page 12 of 16

13 Notification Process Points N-1 Has law enforcement requested a notification delay? If a law enforcement official states to a covered entity or business associate that a notification, notice, or posting would impede a criminal investigation, or cause damage to national security, notification should be delayed. See decision N-2 to determine the length of the delay. Law enforcement requests are accepted in two formats: written statement or oral statement. If the type of request is oral, the covered entity should delay notification for a period of up to 30 days, then proceed with the notification process. If the request is written, the request should specify a time frame for the delay. The covered entity should honor the request and delay notice as specified. Page 13 of 16

14 In any case deemed by the covered entity to require urgency because of possible imminent misuse of unsecured PHI, the covered entity may provide information to individuals by telephone or other means, as appropriate, in addition to the standard notice. In the case where there is insufficient or out-of-date contact information for ten or more affected individuals, a substitute notice is required. This substitute notice must be provided in the form of a media announcement or conspicuous posting for a period of 90 days on the covered entity s web site home page. N-5 Did breach involve more than 500 individuals? Based upon the number of individuals affected by the breach, additional notice may be required. If a breach affects 500 or more residents, a covered entity must provide the Secretary with notice of the breach without unreasonable delay and in no case later than 60 days from discovery of the breach. If the breach affects more than 500 residents from a state or jurisdiction, see decision N-6. Page 14 of 16

15 Where a breach affects more than 500 residents from a state or jurisdiction, additional notice is required. In that case, the covered entity shall notify prominent media outlets serving the state or jurisdiction. This media notice is in addition to, not a substitute for, individual notice. Notification to prominent media outlets should occur without unreasonable delay and in no case later than 60 calendar days after discovery of the breach. Page 15 of 16

16 REFERENCES American Recovery and Reinvestment Act of 2009 (ARRA): Final text of legislation (HITECH = Title VIII) Federal Breach Notification Rule: General information html Interim final rule Federal Register Final Rule Breach notification guidance erbreachrfi.pdf Guidance for securing PHI ance.html o Encryption of data at rest NIST o Encryption of data in motion (TLS) NIST o Encryption of data in motion (VPN) NIST o Guidelines for media sanitation NIST o Cryptographic security FIPS Instructions for submitting notice to the secretary: html Page 16 of 16

POLICY AND PROCEDURE MANUAL
 Pennington Biomedical POLICY NO. 412.22 POLICY AND PROCEDURE MANUAL Origin Date: 02/04/2013 Impacts: ALL PERSONNEL Effective Date: 03/17/2014 Subject: HIPAA BREACH NOTIFICATION Last Revised: Source: LEGAL
Pennington Biomedical POLICY NO. 412.22 POLICY AND PROCEDURE MANUAL Origin Date: 02/04/2013 Impacts: ALL PERSONNEL Effective Date: 03/17/2014 Subject: HIPAA BREACH NOTIFICATION Last Revised: Source: LEGAL
BREACH NOTIFICATION FOR UNSECURED PROTECTED HEALTH INFORMATION
 BREACH NOTIFICATION FOR UNSECURED PROTECTED HEALTH INFORMATION Summary November 2009 On August 24, 2009, the Department of Health and Human Services (HHS) published an interim final rule (the Rule ) that
BREACH NOTIFICATION FOR UNSECURED PROTECTED HEALTH INFORMATION Summary November 2009 On August 24, 2009, the Department of Health and Human Services (HHS) published an interim final rule (the Rule ) that
UNDERSTANDING THE HIPAA/HITECH BREACH NOTIFICATION RULE 2/25/14
 UNDERSTANDING THE HIPAA/HITECH BREACH NOTIFICATION RULE 2/25/14 RULES Issued August 19, 2009 Requires Covered Entities to notify individuals of a breach as well as HHS without reasonable delay or within
UNDERSTANDING THE HIPAA/HITECH BREACH NOTIFICATION RULE 2/25/14 RULES Issued August 19, 2009 Requires Covered Entities to notify individuals of a breach as well as HHS without reasonable delay or within
This presentation focuses on the Healthcare Breach Notification Rule. First published in 2009, the final breach notification rule was finalized in
 This presentation focuses on the Healthcare Breach Notification Rule. First published in 2009, the final breach notification rule was finalized in the HIPAA Omnibus Rule of 2013. As part of the American
This presentation focuses on the Healthcare Breach Notification Rule. First published in 2009, the final breach notification rule was finalized in the HIPAA Omnibus Rule of 2013. As part of the American
Barnes & Thornburg LLP HIPAA Update: HITECH Act Breach Notification Rule
 HEALTHCARE October 2009 Barnes & Thornburg LLP HIPAA Update: HITECH Act Breach Notification Rule This HIPAA Update provides a detailed description of the new breach notification requirements for HIPAA
HEALTHCARE October 2009 Barnes & Thornburg LLP HIPAA Update: HITECH Act Breach Notification Rule This HIPAA Update provides a detailed description of the new breach notification requirements for HIPAA
Data Breach, Electronic Health Records and Healthcare Reform
 Data Breach, Electronic Health Records and Healthcare Reform (This presentation is for informational purposes only and it is not intended, and should not be relied upon, as legal advice.) Overview of HIPAA
Data Breach, Electronic Health Records and Healthcare Reform (This presentation is for informational purposes only and it is not intended, and should not be relied upon, as legal advice.) Overview of HIPAA
Breach Notification Policy
 1. Breach Notification Team. Breach Notification Policy Ferris State University ( Ferris State ), a hybrid entity with health care components, has established a Breach Notification Team, which consists
1. Breach Notification Team. Breach Notification Policy Ferris State University ( Ferris State ), a hybrid entity with health care components, has established a Breach Notification Team, which consists
M E M O R A N D U M. Definitions
 M E M O R A N D U M DATE: November 10, 2011 TO: FROM: RE: Krevolin & Horst, LLC HIPAA Obligations of Business Associates In connection with the launch of your hosted application service focused on practice
M E M O R A N D U M DATE: November 10, 2011 TO: FROM: RE: Krevolin & Horst, LLC HIPAA Obligations of Business Associates In connection with the launch of your hosted application service focused on practice
The ReHabilitation Center. 1439 Buffalo Street. Olean. NY. 14760
 Procedure Name: HITECH Breach Notification The ReHabilitation Center 1439 Buffalo Street. Olean. NY. 14760 Purpose To amend The ReHabilitation Center s HIPAA Policy and Procedure to include mandatory breach
Procedure Name: HITECH Breach Notification The ReHabilitation Center 1439 Buffalo Street. Olean. NY. 14760 Purpose To amend The ReHabilitation Center s HIPAA Policy and Procedure to include mandatory breach
HIPAA BREACH RESPONSE POLICY
 http://dhmh.maryland.gov/sitepages/op02.aspx (OIG) DHMH POLICY 01.03.07 Effective Date: July 22, 2014 I. EXECUTIVE SUMMARY The Department of Health and Mental Hygiene (DHMH) is committed to protecting
http://dhmh.maryland.gov/sitepages/op02.aspx (OIG) DHMH POLICY 01.03.07 Effective Date: July 22, 2014 I. EXECUTIVE SUMMARY The Department of Health and Mental Hygiene (DHMH) is committed to protecting
Five Rivers Medical Center, Inc. 2801 Medical Center Drive Pocahontas, AR 72455. Notification of Security Breach Policy
 Five Rivers Medical Center, Inc. 2801 Medical Center Drive Pocahontas, AR 72455 Notification of Security Breach Policy Purpose: This policy has been adopted for the purpose of complying with the Health
Five Rivers Medical Center, Inc. 2801 Medical Center Drive Pocahontas, AR 72455 Notification of Security Breach Policy Purpose: This policy has been adopted for the purpose of complying with the Health
ADMINISTRATIVE REGULATION EFFECTIVE DATE: 1/1/2016
 Page 1 of 9 CITY OF CHESAPEAKE, VIRGINIA NUMBER: 2.62 ADMINISTRATIVE REGULATION EFFECTIVE DATE: 1/1/2016 SUPERCEDES: N/A SUBJECT: HUMAN RESOURCES DEPARTMENT CITY OF CHESAPEAKE EMPLOYEE/RETIREE GROUP HEALTH
Page 1 of 9 CITY OF CHESAPEAKE, VIRGINIA NUMBER: 2.62 ADMINISTRATIVE REGULATION EFFECTIVE DATE: 1/1/2016 SUPERCEDES: N/A SUBJECT: HUMAN RESOURCES DEPARTMENT CITY OF CHESAPEAKE EMPLOYEE/RETIREE GROUP HEALTH
Everett School Employee Benefit Trust. Reportable Breach Notification Policy HIPAA HITECH Rules and Washington State Law
 Everett School Employee Benefit Trust Reportable Breach Notification Policy HIPAA HITECH Rules and Washington State Law Introduction The Everett School Employee Benefit Trust ( Trust ) adopts this policy
Everett School Employee Benefit Trust Reportable Breach Notification Policy HIPAA HITECH Rules and Washington State Law Introduction The Everett School Employee Benefit Trust ( Trust ) adopts this policy
FEDERAL AND STATE BREACH NOTIFICATION LAWS FOR CALIFORNIA
 APPENDIX PR 12-A FEDERAL AND STATE BREACH NOTIFICATION LAWS FOR CALIFORNIA LEGAL CITATION California Civil Code Section 1798.82 California Health and Safety (H&S) Code Section 1280.15 42 U.S.C. Section
APPENDIX PR 12-A FEDERAL AND STATE BREACH NOTIFICATION LAWS FOR CALIFORNIA LEGAL CITATION California Civil Code Section 1798.82 California Health and Safety (H&S) Code Section 1280.15 42 U.S.C. Section
COMPLIANCE ALERT 10-12
 HAWAII HEALTH SYSTEMS C O R P O R A T I O N "Touching Lives Every Day COMPLIANCE ALERT 10-12 HIPAA Expansion under the American Recovery and Reinvestment Act of 2009 The American Recovery and Reinvestment
HAWAII HEALTH SYSTEMS C O R P O R A T I O N "Touching Lives Every Day COMPLIANCE ALERT 10-12 HIPAA Expansion under the American Recovery and Reinvestment Act of 2009 The American Recovery and Reinvestment
HIPAA and the HITECH Act Privacy and Security of Health Information in 2009
 HIPAA and the HITECH Act Privacy and Security of Health Information in 2009 What is HIPAA? Health Insurance Portability & Accountability Act of 1996 Effective April 13, 2003 Federal Law HIPAA Purpose:
HIPAA and the HITECH Act Privacy and Security of Health Information in 2009 What is HIPAA? Health Insurance Portability & Accountability Act of 1996 Effective April 13, 2003 Federal Law HIPAA Purpose:
NOTICE OF THE NATHAN ADELSON HOSPICE PRIVACY PRACTICES
 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION PLEASE REVIEW IT CAREFULLY. DEFINITIONS PROTECTED HEALTH INFORMATION (PHI):
THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION PLEASE REVIEW IT CAREFULLY. DEFINITIONS PROTECTED HEALTH INFORMATION (PHI):
AVE MARIA UNIVERSITY HIPAA PRIVACY NOTICE
 AVE MARIA UNIVERSITY HIPAA PRIVACY NOTICE This Notice of Privacy Practices describes the legal obligations of Ave Maria University, Inc. (the plan ) and your legal rights regarding your protected health
AVE MARIA UNIVERSITY HIPAA PRIVACY NOTICE This Notice of Privacy Practices describes the legal obligations of Ave Maria University, Inc. (the plan ) and your legal rights regarding your protected health
Business Associates and Breach Reporting Under HITECH and the Omnibus Final HIPAA Rule
 Business Associates and Breach Reporting Under HITECH and the Omnibus Final HIPAA Rule Patricia D. King, Esq. Associate General Counsel Swedish Covenant Hospital Chicago, IL I. Business Associates under
Business Associates and Breach Reporting Under HITECH and the Omnibus Final HIPAA Rule Patricia D. King, Esq. Associate General Counsel Swedish Covenant Hospital Chicago, IL I. Business Associates under
STANDARD ADMINISTRATIVE PROCEDURE
 STANDARD ADMINISTRATIVE PROCEDURE 16.99.99.M0.26 Investigation and Response to Breach of Unsecured Protected Health Information (HITECH) Approved October 27, 2014 Next scheduled review: October 27, 2019
STANDARD ADMINISTRATIVE PROCEDURE 16.99.99.M0.26 Investigation and Response to Breach of Unsecured Protected Health Information (HITECH) Approved October 27, 2014 Next scheduled review: October 27, 2019
New HIPAA Breach Notification Rule: Know Your Responsibilities. Loudoun Medical Group Spring 2010
 New HIPAA Breach Notification Rule: Know Your Responsibilities Loudoun Medical Group Spring 2010 Health Information Technology for Economic and Clinical Health Act (HITECH) As part of the Recovery Act,
New HIPAA Breach Notification Rule: Know Your Responsibilities Loudoun Medical Group Spring 2010 Health Information Technology for Economic and Clinical Health Act (HITECH) As part of the Recovery Act,
NCHICA HITECH Act Breach Notification Risk Assessment Tool. Prepared by the NCHICA Privacy, Security & Legal Officials Workgroup
 NCHICA HITECH Act Breach Notification Risk Assessment Tool Prepared by the NCHICA Privacy, Security & Legal Officials Workgroup NORTH CAROLINA HEALTHCARE INFORMATION AND COMMUNICATIONS ALLIANCE, INC August
NCHICA HITECH Act Breach Notification Risk Assessment Tool Prepared by the NCHICA Privacy, Security & Legal Officials Workgroup NORTH CAROLINA HEALTHCARE INFORMATION AND COMMUNICATIONS ALLIANCE, INC August
HIPPA and HITECH NOTIFICATION Effective Date: September 23, 2013
 HIPPA and HITECH NOTIFICATION Effective Date: September 23, 2013 Orchard Creek Health Care is required by law to maintain the privacy of protected health information (PHI) of our residents. If you feel
HIPPA and HITECH NOTIFICATION Effective Date: September 23, 2013 Orchard Creek Health Care is required by law to maintain the privacy of protected health information (PHI) of our residents. If you feel
REPRODUCTIVE ASSOCIATES OF DELAWARE (RAD) NOTICE OF PRIVACY PRACTICES PLEASE REVIEW IT CAREFULLY.
 NOTICE OF PRIVACY PRACTICES PLEASE REVIEW IT CAREFULLY.") REPRODUCTIVE ASSOCIATES OF DELAWARE (RAD) NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW PROTECTED HEALTH INFORMATION (PHI) ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS
REPRODUCTIVE ASSOCIATES OF DELAWARE (RAD) NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW PROTECTED HEALTH INFORMATION (PHI) ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS
Model Business Associate Agreement
 Model Business Associate Agreement Instructions: The Texas Health Services Authority (THSA) has developed a model BAA for use between providers (Covered Entities) and HIEs (Business Associates). The model
Model Business Associate Agreement Instructions: The Texas Health Services Authority (THSA) has developed a model BAA for use between providers (Covered Entities) and HIEs (Business Associates). The model
IDAHO STATE UNIVERSITY POLICIES AND PROCEDURES (ISUPP) HIPAA Privacy - Data Breach Notification Policy 10240
 HIPAA Privacy - Data Breach Notification Policy 10240") IDAHO STATE UNIVERSITY POLICIES AND PROCEDURES (ISUPP) HIPAA Privacy - Data Breach Notification Policy 10240 POLICY INFORMATION Major Functional Area (MFA): MFA X - Office of General Counsel & Compliance
IDAHO STATE UNIVERSITY POLICIES AND PROCEDURES (ISUPP) HIPAA Privacy - Data Breach Notification Policy 10240 POLICY INFORMATION Major Functional Area (MFA): MFA X - Office of General Counsel & Compliance
Checklist for HITECH Breach Readiness
 Checklist for HITECH Breach Readiness Checklist for HITECH Breach Readiness Figure 1 describes a checklist that may be used to assess for breach preparedness for the organization. It is based on published
Checklist for HITECH Breach Readiness Checklist for HITECH Breach Readiness Figure 1 describes a checklist that may be used to assess for breach preparedness for the organization. It is based on published
NACHC Issue Brief Changes to the Health Insurance Portability and Accountability Act Included in ARRA. March 2010
 NACHC Issue Brief Changes to the Health Insurance Portability and Accountability Act Included in ARRA March 2010 Prepared By: Marisa Guevara and Marcie H. Zakheim Feldesman Tucker Leifer Fidell, LLP 2001
NACHC Issue Brief Changes to the Health Insurance Portability and Accountability Act Included in ARRA March 2010 Prepared By: Marisa Guevara and Marcie H. Zakheim Feldesman Tucker Leifer Fidell, LLP 2001
Identity Theft Prevention and Security Breach Notification Policy. Purpose:
 Identity Theft Prevention and Security Breach Notification Policy Purpose: Lahey Clinic is committed to protecting the privacy of the Personal Health Information ( PHI ) of our patients and the Personal
Identity Theft Prevention and Security Breach Notification Policy Purpose: Lahey Clinic is committed to protecting the privacy of the Personal Health Information ( PHI ) of our patients and the Personal
HIPAA Compliance: Are you prepared for the new regulatory changes?
 HIPAA Compliance: Are you prepared for the new regulatory changes? Baker Tilly CARIS Innovation, Inc. April 30, 2013 Baker Tilly refers to Baker Tilly Virchow Krause, LLP, an independently owned and managed
HIPAA Compliance: Are you prepared for the new regulatory changes? Baker Tilly CARIS Innovation, Inc. April 30, 2013 Baker Tilly refers to Baker Tilly Virchow Krause, LLP, an independently owned and managed
Health Information Privacy Refresher Training. March 2013
 Health Information Privacy Refresher Training March 2013 1 Disclosure There are no significant or relevant financial relationships to disclose. 2 Topics for Today State health information privacy law Federal
Health Information Privacy Refresher Training March 2013 1 Disclosure There are no significant or relevant financial relationships to disclose. 2 Topics for Today State health information privacy law Federal
FACT SHEET: Ransomware and HIPAA
 FACT SHEET: Ransomware and HIPAA A recent U.S. Government interagency report indicates that, on average, there have been 4,000 daily ransomware attacks since early 2016 (a 300% increase over the 1,000
FACT SHEET: Ransomware and HIPAA A recent U.S. Government interagency report indicates that, on average, there have been 4,000 daily ransomware attacks since early 2016 (a 300% increase over the 1,000
BUSINESS ASSOCIATE AGREEMENT. Business Associate. Business Associate shall mean.
 BUSINESS ASSOCIATE AGREEMENT This Business Associate Agreement is made as of the day of, 2010, by and between Methodist Lebonheur Healthcare, on behalf of itself and all of its affiliates ( Covered Entity
BUSINESS ASSOCIATE AGREEMENT This Business Associate Agreement is made as of the day of, 2010, by and between Methodist Lebonheur Healthcare, on behalf of itself and all of its affiliates ( Covered Entity
Updated HIPAA Regulations What Optometrists Need to Know Now. HIPAA Overview
 Updated HIPAA Regulations What Optometrists Need to Know Now The U.S. Department of Health & Human Services Office for Civil Rights recently released updated regulations regarding the Health Insurance
Updated HIPAA Regulations What Optometrists Need to Know Now The U.S. Department of Health & Human Services Office for Civil Rights recently released updated regulations regarding the Health Insurance
HIPAA Data Breaches: Managing Them Internally and in Response to Civil/Criminal Investigations
 HIPAA Data Breaches: Managing Them Internally and in Response to Civil/Criminal Investigations Health Care Litigation Webinar Series March 22, 2012 Spence Pryor Paula Stannard Jason Popp 1 HIPAA/HITECH
HIPAA Data Breaches: Managing Them Internally and in Response to Civil/Criminal Investigations Health Care Litigation Webinar Series March 22, 2012 Spence Pryor Paula Stannard Jason Popp 1 HIPAA/HITECH
HIPAA Omnibus Rule Practice Impact. Kristen Heffernan MicroMD Director of Prod Mgt and Marketing
 HIPAA Omnibus Rule Practice Impact Kristen Heffernan MicroMD Director of Prod Mgt and Marketing 1 HIPAA Omnibus Rule Agenda History of the Rule HIPAA Stats Rule Overview Use of Personal Health Information
HIPAA Omnibus Rule Practice Impact Kristen Heffernan MicroMD Director of Prod Mgt and Marketing 1 HIPAA Omnibus Rule Agenda History of the Rule HIPAA Stats Rule Overview Use of Personal Health Information
Table of Contents INTRODUCTION AND PURPOSE 1
 HEALTH INSURANCE PORTABILITY AND ACCOUNTABILITY ACT OF 1996 ( HIPAA ) COMPLIANCE PROGRAM Adopted December 2008: Revised February 2009, May, 2012, and August 2013 Table of Contents INTRODUCTION AND PURPOSE
HEALTH INSURANCE PORTABILITY AND ACCOUNTABILITY ACT OF 1996 ( HIPAA ) COMPLIANCE PROGRAM Adopted December 2008: Revised February 2009, May, 2012, and August 2013 Table of Contents INTRODUCTION AND PURPOSE
How To Notify Of A Security Breach In Health Care Records
 CHART YOUR HIPAA COURSE... HHS ISSUES SECURITY BREACH NOTIFICATION RULES PUBLISHED IN FEDERAL REGISTER 8/24/09 EFFECTIVE 9/23/09 The Department of Health and Human Services ( HHS ) has issued interim final
CHART YOUR HIPAA COURSE... HHS ISSUES SECURITY BREACH NOTIFICATION RULES PUBLISHED IN FEDERAL REGISTER 8/24/09 EFFECTIVE 9/23/09 The Department of Health and Human Services ( HHS ) has issued interim final
Name of Other Party: Address of Other Party: Effective Date: Reference Number as applicable:
 PLEASE NOTE: THIS DOCUMENT IS SUBMITTED AS A SAMPLE, FOR INFORMATIONAL PURPOSES ONLY TO ABC ORGANIZATION. HIPAA SOLUTIONS LC IS NOT ENGAGED IN THE PRACTICE OF LAW IN ANY STATE, JURISDICTION, OR VENUE OF
PLEASE NOTE: THIS DOCUMENT IS SUBMITTED AS A SAMPLE, FOR INFORMATIONAL PURPOSES ONLY TO ABC ORGANIZATION. HIPAA SOLUTIONS LC IS NOT ENGAGED IN THE PRACTICE OF LAW IN ANY STATE, JURISDICTION, OR VENUE OF
12/19/2014. HIPAA More Important Than You Realize. Administrative Simplification Privacy Rule Security Rule
 HIPAA More Important Than You Realize J. Ira Bedenbaugh Consulting Shareholder February 20, 2015 This material was used by Elliott Davis Decosimo during an oral presentation; it is not a complete record
HIPAA More Important Than You Realize J. Ira Bedenbaugh Consulting Shareholder February 20, 2015 This material was used by Elliott Davis Decosimo during an oral presentation; it is not a complete record
HHS Finalizes HIPAA Privacy and Data Security Rules, Including Stricter Rules for Breaches of Unsecured PHI
 January 23, 2013 HHS Finalizes HIPAA Privacy and Data Security Rules, Including Stricter Rules for Breaches of Unsecured PHI Executive Summary HHS has issued final regulations that address recent legislative
January 23, 2013 HHS Finalizes HIPAA Privacy and Data Security Rules, Including Stricter Rules for Breaches of Unsecured PHI Executive Summary HHS has issued final regulations that address recent legislative
HIPAA Omnibus Rule Overview. Presented by: Crystal Stanton MicroMD Marketing Communication Specialist
 HIPAA Omnibus Rule Overview Presented by: Crystal Stanton MicroMD Marketing Communication Specialist 1 HIPAA Omnibus Rule - Agenda History of the Omnibus Rule What is the HIPAA Omnibus Rule and its various
HIPAA Omnibus Rule Overview Presented by: Crystal Stanton MicroMD Marketing Communication Specialist 1 HIPAA Omnibus Rule - Agenda History of the Omnibus Rule What is the HIPAA Omnibus Rule and its various
CREATIVE SOLUTIONS IN HEALTHCARE, INC. Privacy Policy
 CREATIVE SOLUTIONS IN HEALTHCARE, INC. Privacy Policy Amended as of February 12, 2010 on the authority of the HIPAA Privacy Officer for Creative Solutions in Healthcare, Inc. TABLE OF CONTENTS ARTICLE
CREATIVE SOLUTIONS IN HEALTHCARE, INC. Privacy Policy Amended as of February 12, 2010 on the authority of the HIPAA Privacy Officer for Creative Solutions in Healthcare, Inc. TABLE OF CONTENTS ARTICLE
HEALTH INSURANCE PORTABILITY & ACCOUNTABILITY ACT OF 1996 HIPAA
 TRAINING MANUAL HEALTH INSURANCE PORTABILITY & ACCOUNTABILITY ACT OF 1996 HIPAA Table of Contents INTRODUCTION 3 What is HIPAA? Privacy Security Transactions and Code Sets What is covered ADMINISTRATIVE
TRAINING MANUAL HEALTH INSURANCE PORTABILITY & ACCOUNTABILITY ACT OF 1996 HIPAA Table of Contents INTRODUCTION 3 What is HIPAA? Privacy Security Transactions and Code Sets What is covered ADMINISTRATIVE
SAMPLE BUSINESS ASSOCIATE AGREEMENT
 SAMPLE BUSINESS ASSOCIATE AGREEMENT THIS AGREEMENT IS TO BE USED ONLY AS A SAMPLE IN DEVELOPING YOUR OWN BUSINESS ASSOCIATE AGREEMENT. ANYONE USING THIS DOCUMENT AS GUIDANCE SHOULD DO SO ONLY IN CONSULT
SAMPLE BUSINESS ASSOCIATE AGREEMENT THIS AGREEMENT IS TO BE USED ONLY AS A SAMPLE IN DEVELOPING YOUR OWN BUSINESS ASSOCIATE AGREEMENT. ANYONE USING THIS DOCUMENT AS GUIDANCE SHOULD DO SO ONLY IN CONSULT
Heather L. Hughes, J.D. HIPAA Privacy Officer U.S. Legal Support, Inc. [email protected] www.uslegalsupport.com
 Heather L. Hughes, J.D. HIPAA Privacy Officer U.S. Legal Support, Inc. [email protected] www.uslegalsupport.com HIPAA Privacy Rule Sets standards for confidentiality and privacy of individually
Heather L. Hughes, J.D. HIPAA Privacy Officer U.S. Legal Support, Inc. [email protected] www.uslegalsupport.com HIPAA Privacy Rule Sets standards for confidentiality and privacy of individually
HIPAA Business Associate Agreement
 HIPAA Business Associate Agreement User of any Nemaris Inc. (Nemaris) products or services including but not limited to Surgimap Spine, Surgimap ISSG, Surgimap SRS, Surgimap Office, Surgimap Ortho, Surgimap
HIPAA Business Associate Agreement User of any Nemaris Inc. (Nemaris) products or services including but not limited to Surgimap Spine, Surgimap ISSG, Surgimap SRS, Surgimap Office, Surgimap Ortho, Surgimap
The HIPAA privacy rule established federal law to help protect the use and disclosure of patient information. The privacy rule prohibits a covered
 The HIPAA privacy rule established federal law to help protect the use and disclosure of patient information. The privacy rule prohibits a covered entity from using or disclosing protected health information
The HIPAA privacy rule established federal law to help protect the use and disclosure of patient information. The privacy rule prohibits a covered entity from using or disclosing protected health information
HIPAA PRIVACY AND SECURITY RULES BUSINESS ASSOCIATE AGREEMENT BETWEEN. Stewart C. Miller & Co., Inc. (Business Associate) AND
 AND") HIPAA PRIVACY AND SECURITY RULES BUSINESS ASSOCIATE AGREEMENT BETWEEN Stewart C. Miller & Co., Inc. (Business Associate) AND City of West Lafayette Flexible Spending Plan (Covered Entity) TABLE OF CONTENTS
HIPAA PRIVACY AND SECURITY RULES BUSINESS ASSOCIATE AGREEMENT BETWEEN Stewart C. Miller & Co., Inc. (Business Associate) AND City of West Lafayette Flexible Spending Plan (Covered Entity) TABLE OF CONTENTS
SaaS. Business Associate Agreement
 SaaS Business Associate Agreement This Business Associate Agreement ( BA Agreement ) becomes effective pursuant to the terms of Section 5 of the End User Service Agreement ( EUSA ) between Customer ( Covered
SaaS Business Associate Agreement This Business Associate Agreement ( BA Agreement ) becomes effective pursuant to the terms of Section 5 of the End User Service Agreement ( EUSA ) between Customer ( Covered
Use & Disclosure of Protected Health Information by Business Associates
 Applicability: Policy Title: Policy Number: Use & Disclosure of Protected Health Information by Business Associates PP-12 Superseded Policy(ies) or Entity Policy: N/A Date Established: January 31, 2003
Applicability: Policy Title: Policy Number: Use & Disclosure of Protected Health Information by Business Associates PP-12 Superseded Policy(ies) or Entity Policy: N/A Date Established: January 31, 2003
Disclaimer: Template Business Associate Agreement (45 C.F.R. 164.308)
") HIPAA Business Associate Agreement Sample Notice Disclaimer: Template Business Associate Agreement (45 C.F.R. 164.308) The information provided in this document does not constitute, and is no substitute
HIPAA Business Associate Agreement Sample Notice Disclaimer: Template Business Associate Agreement (45 C.F.R. 164.308) The information provided in this document does not constitute, and is no substitute
HIPAA PRIVACY AND SECURITY TRAINING P I E D M O N T COMMUNITY H EA LT H P L A N
 HIPAA PRIVACY AND SECURITY TRAINING P I E D M O N T COMMUNITY H EA LT H P L A N 1 COURSE OVERVIEW This course is broken down into 4 modules: Module 1: HIPAA Omnibus Rule - What you need to know to remain
HIPAA PRIVACY AND SECURITY TRAINING P I E D M O N T COMMUNITY H EA LT H P L A N 1 COURSE OVERVIEW This course is broken down into 4 modules: Module 1: HIPAA Omnibus Rule - What you need to know to remain
BUSINESS ASSOCIATE AGREEMENT Tribal Contract
 DEPARTMENT OF HEALTH SERVICES Division of Enterprise Services F-00714 (08/2013) STATE OF WISCONSIN BUSINESS ASSOCIATE AGREEMENT Tribal Contract This Business Associate Agreement is made between the Wisconsin
DEPARTMENT OF HEALTH SERVICES Division of Enterprise Services F-00714 (08/2013) STATE OF WISCONSIN BUSINESS ASSOCIATE AGREEMENT Tribal Contract This Business Associate Agreement is made between the Wisconsin
Effective Date: March 23, 2016
 AIG COMPANIES Effective Date: March 23, 2016 HIPAA NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION.
AIG COMPANIES Effective Date: March 23, 2016 HIPAA NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION.
HIPAA for Business Associates
 HIPAA for Business Associates February 11, 2015 Teresa D. Locke This presentation is similar to any other legal education materials designed to provide general information on pertinent legal topics. The
HIPAA for Business Associates February 11, 2015 Teresa D. Locke This presentation is similar to any other legal education materials designed to provide general information on pertinent legal topics. The
Breach Notification Decision Process 1/1/2014
 WEDI Strategic National Implementation Process (SNIP) Privacy and Security Workgroup Breach Risk Assessment Issue Brief Breach Notification Decision Process 1/1/2014 Workgroup for Electronic Data Interchange
WEDI Strategic National Implementation Process (SNIP) Privacy and Security Workgroup Breach Risk Assessment Issue Brief Breach Notification Decision Process 1/1/2014 Workgroup for Electronic Data Interchange
This form may not be modified without prior approval from the Department of Justice.
 This form may not be modified without prior approval from the Department of Justice. Delete this header in execution (signature) version of agreement. HIPAA BUSINESS ASSOCIATE AGREEMENT This Business Associate
This form may not be modified without prior approval from the Department of Justice. Delete this header in execution (signature) version of agreement. HIPAA BUSINESS ASSOCIATE AGREEMENT This Business Associate
Reproductive Medicine Associates of New Jersey, LLC
 NOTICE OF PRIVACY PRACTICES Effective Date: September 20, 2013 Last Modified: May 12, 2013 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO
NOTICE OF PRIVACY PRACTICES Effective Date: September 20, 2013 Last Modified: May 12, 2013 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO
BUSINESS ASSOCIATE AGREEMENT TERMS
 BUSINESS ASSOCIATE AGREEMENT TERMS This Addendum ( Addendum ) is incorporated into and made part of the Agreement between SIGNATURE HEALTHCARE CORPORATION ("Covered Entity ) and ( Business Associate"),
BUSINESS ASSOCIATE AGREEMENT TERMS This Addendum ( Addendum ) is incorporated into and made part of the Agreement between SIGNATURE HEALTHCARE CORPORATION ("Covered Entity ) and ( Business Associate"),
Privacy Notice Document (HIPAA)
") Privacy Notice Document (HIPAA) THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. This Privacy
Privacy Notice Document (HIPAA) THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. This Privacy
G REATER H OUSTON H EALTHCONNECT. HIPAA/HITECH Privacy Compliance Manual
 G REATER H OUSTON H EALTHCONNECT HIPAA/HITECH Privacy Compliance Manual Adopted by the Board of Directors on December 14, 2011and amended on September 12, 2012 and February 27, 2013 TABLE OF CONTENTS Page
G REATER H OUSTON H EALTHCONNECT HIPAA/HITECH Privacy Compliance Manual Adopted by the Board of Directors on December 14, 2011and amended on September 12, 2012 and February 27, 2013 TABLE OF CONTENTS Page
GLENN COUNTY HEALTH AND HUMAN SERVICES AGENCY. HIPAA Policies and Procedures 06/30/2014
 GLENN COUNTY HEALTH AND HUMAN SERVICES AGENCY HIPAA Policies and Procedures 06/30/2014 Glenn County Health and Human Services Agency HIPAA Policies and Procedures TABLE OF CONTENTS HIPAA Policy Number
GLENN COUNTY HEALTH AND HUMAN SERVICES AGENCY HIPAA Policies and Procedures 06/30/2014 Glenn County Health and Human Services Agency HIPAA Policies and Procedures TABLE OF CONTENTS HIPAA Policy Number
NOTICE OF HEALTH INFORMATION PRIVACY PRACTICES (HIPAA)
") NOTICE OF HEALTH INFORMATION PRIVACY PRACTICES (HIPAA) THIS NOTICE OF PRIVACY PRACTICES DESCRIBES HOW HEALTH INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION.
NOTICE OF HEALTH INFORMATION PRIVACY PRACTICES (HIPAA) THIS NOTICE OF PRIVACY PRACTICES DESCRIBES HOW HEALTH INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION.
My Docs Online HIPAA Compliance
 My Docs Online HIPAA Compliance Updated 10/02/2013 Using My Docs Online in a HIPAA compliant fashion depends on following proper usage guidelines, which can vary based on a particular use, but have several
My Docs Online HIPAA Compliance Updated 10/02/2013 Using My Docs Online in a HIPAA compliant fashion depends on following proper usage guidelines, which can vary based on a particular use, but have several
Policies and Procedures Audit Checklist for HIPAA Privacy, Security, and Breach Notification
 Policies and Procedures Audit Checklist for HIPAA Privacy, Security, and Breach Notification Type of Policy and Procedure Comments Completed Privacy Policy to Maintain and Update Notice of Privacy Practices
Policies and Procedures Audit Checklist for HIPAA Privacy, Security, and Breach Notification Type of Policy and Procedure Comments Completed Privacy Policy to Maintain and Update Notice of Privacy Practices
UNITED CEREBRAL PALSY OF NORTHWEST MISSOURI NOTICE OF PRIVACY PRACTICES EFFECTIVE DATE: OCTOBER 22, 2014
 UNITED CEREBRAL PALSY OF NORTHWEST MISSOURI NOTICE OF PRIVACY PRACTICES EFFECTIVE DATE: OCTOBER 22, 2014 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN
UNITED CEREBRAL PALSY OF NORTHWEST MISSOURI NOTICE OF PRIVACY PRACTICES EFFECTIVE DATE: OCTOBER 22, 2014 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN
HIPAA BUSINESS ASSOCIATE AGREEMENT
 HIPAA BUSINESS ASSOCIATE AGREEMENT This HIPAA Business Associate Agreement ("BA AGREEMENT") supplements and is made a part of any and all agreements entered into by and between The Regents of the University
HIPAA BUSINESS ASSOCIATE AGREEMENT This HIPAA Business Associate Agreement ("BA AGREEMENT") supplements and is made a part of any and all agreements entered into by and between The Regents of the University
FirstCarolinaCare Insurance Company Business Associate Agreement
 FirstCarolinaCare Insurance Company Business Associate Agreement THIS BUSINESS ASSOCIATE AGREEMENT ("Agreement"), is made and entered into as of, 20 (the "Effective Date") between FirstCarolinaCare Insurance
FirstCarolinaCare Insurance Company Business Associate Agreement THIS BUSINESS ASSOCIATE AGREEMENT ("Agreement"), is made and entered into as of, 20 (the "Effective Date") between FirstCarolinaCare Insurance
Data Breach Notification Burden Grows With First State Insurance Commissioner Mandate
 Privacy, Data Security & Information Use September 16, 2010 Data Breach Notification Burden Grows With First State Insurance Commissioner Mandate by John L. Nicholson and Meighan E. O'Reardon Effective
Privacy, Data Security & Information Use September 16, 2010 Data Breach Notification Burden Grows With First State Insurance Commissioner Mandate by John L. Nicholson and Meighan E. O'Reardon Effective