Bile Leaks After Laparoscopic Cholecystectomy. Kings County Hospital Center Eliana A. Soto, MD
|
|
|
- Byron Ralf Roberts
- 7 years ago
- Views:
Transcription
1 Bile Leaks After Laparoscopic Cholecystectomy Kings County Hospital Center Eliana A. Soto, MD

2 Biliary Injuries during Cholecystectomy In the 1990s, high rate of biliary injury was due in part to learning curve effect. In reviews by Strasberg et al. and Roslyn et al., the incidence of biliary injury during open cholecystectomy was found to be %. The review by Strasberg et al. in 1995 of more than 124,000 laparoscopic cholecystectomies reported in the literature found the incidence of major bile duct injury to be 0.5%.

3 As surgeons passed through learning curve, have reached steady-state and there has been no significant improvement in the incidence of biliary duct injuries.

4 Incidence of biliary injury when laparoscopic cholecystectomy is performed for acute cholecystitis is three times greater than that for elective laparoscopic cholecystectomy and twice as high as open cholecystectomy for acute cholecystitis.

5 The aberrant right hepatic duct anomaly is the most common problem. The most dangerous variant is when the cystic duct joins a low-lying aberrant right sectional duct. These injuries are underreported since occlusion of an aberrant duct may be asymptomatic and even unrecognized.

6 Causes of Laparoscopic Biliary Injury Failure to properly occlude cystic duct. Injury to ducts in the liver bed is caused by entering a plane deep to the fascial plate on which the gallbladder rests. Misuse of cautery may cause serious bile duct injuries with loss of ductal tissue due to thermal necrosis. Pulling forcefully up on the gallbladder when clipping the cystic duct causing a tenting injury in which the junction of the common bile duct and hepatic duct is occluded.

7 In 1995, Strasberg and Soper modified the Bismuth classification of bile duct injuries: Type A- bile leak from a minor duct still in continuity with the common bile duct.these leaks occur at the cystic duct or from the liver bed. Type B- occlusion of part of the biliary tree. Usually the result of an injury to an aberrant right hepatic duct.in 2% of patients, the cystic duct enters a right hepatic duct rather than the common bile duct-common hepatic duct junction. The aberrant duct may be a segmental duct, a sectoral duct (the right anterior or posterior duct), or even

8 Type C- bile leak from duct not in communication with common bile duct. Usually diagnosed in early postoperative period as an intraperitoneal bile collection. Type D- lateral injury to extrahepatic bile ducts. May involve the common bile duct, common hepatic duct, or the right or left bile duct. Type E- circumferential injury of major bile ducts. This type of injury causes separation of hepatic parenchyma from the lower ducts and duodenum. May be treated by percutaneous or endoscopic techniques depending on length of stenosis or if

9 Classification of Biliary Duct Injuries:

10 Misidentification injuries: 2 main types. 1) common duct is mistaken for cystic duct and is clipped and divided. 2) the segment of an aberrant right hepatic duct, between entry of the cystic duct and junction of the common hepatic, is mistaken to be the cystic duct.
 the segment of an aberrant right hepatic duct, between entry of")
11 Routine intraoperative cholangiography-fletcher et al. in 1999 found that intraoperative cholangiography had a protective effect for complications of cholecystectomy in a retrospective study of 19,000 cholecystectomies. Operative cholangiography is best at detecting misidentification of the common bile duct as the cystic duct and will prevent excisional injuries of bile ducts if the cholangiogram is correctly interpreted. Poor at detecting aberrant right ducts, which unite with the cystic duct before joining the common

12 Management of Bile Leak post Laparoscopic Cholecystectomy Intraoperative conversion of biliary injury is usually an indication for conversion. Simple type D injuries are repaired by closure of the defect using fine absorbable sutures over a T- tube and placement of a closed suction drain in the vicinity of the repair. Type D injuries that are thermal in origin or that are complex are best repaired by hepaticojejunostomy.

13 Significant postoperative bile leaks occur in up to 1% of patients undergoing laparoscopic cholecystectomy compared to 0.5% in open cholecystectomy. Usually present within first week but can manifest up to 30 days after surgery.

14 Diagnosis of Bile Leaks Clinical manifestations of bile leaks include abdominal tenderness, generalized malaise and anorexia. Bile drainage from drains placed at the initial operation. Diagnosis of bile leak should be suspected whenever persistent bloating and anorexia last for more than a few days; failure to recover as smoothly as expected is the most common early symptom of an intraabdominal bile collection.

15 Minor bile leakage is common after open or laparoscopic cholecystectomy and is often related to disruption of small branches of the right intrahepatic duct entering the gallbladder bed. These leaks, usually from the liver, occurred in 25% of 105 patients prospectively evaluated with ultrasonography by Elboim et al. Such leaks may require no therapy, surgical placement of a drain at the time of the original procedure, or subsequent placement of a percutaneous drain for symptomatic bilomas that are recognized postoperatively.

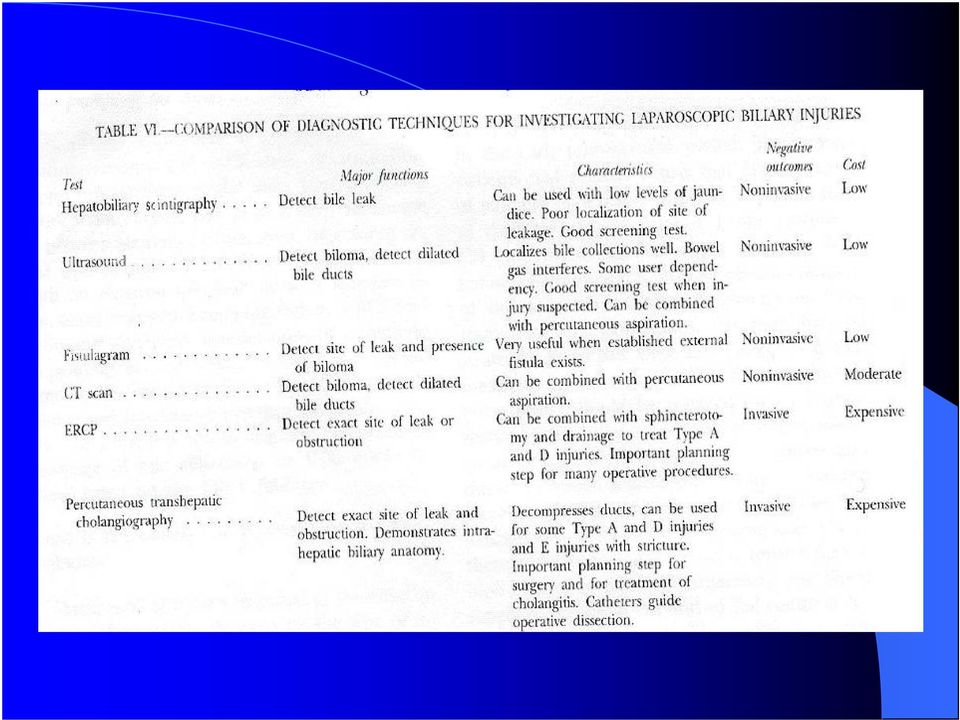
16 Noninvasive imaging (US/CT scan) is essential to define biloma that may require percutaneous or surgical drainage. HIDA scan may show presence of an active bile leak and general anatomic site of leakage. MRCP also provides imaging of the biliary tract, demonstrating dilation or stenosis of the biliary tract, and stones in the cystic duct remnant, the pancreas, and the pancreatic ducts; however, it does not allow concomitant therapeutic measures or physiologic assessment of bile flow (so cannot detect if a leak is active).

17 ERCP and percutaneous transhepatic cholangiography (PTC) can provide an exact anatomical diagnosis of bile duct leak, while at the same time allowing for treatment of the leak by appropriate decompression of the biliary tree.

18
19 Treatment of Bile Leaks The principle of treatment is to reestablish a pressure gradient that will favor the flow of bile into the duodenum and not out of the leak site. This means removing any physiological or pathological obstruction such as the normal sphincter of Oddi pressure or a retained bile duct stone.

20 In cases where there is a bile duct stone, removal of the stone with sphincterotomy is treatment of choice. If there is no stone, then internal stenting with or without sphincterotomy has shown to be effective in treating bile leaks. A retrospective study by De Palma et al. in 2002 showed that sphincterotomy alone was highly effective in producing closure of bile fistulas by reducing endobiliary pressure.

21 Endoscopic internal stenting is currently procedure of choice for treating bile duct leaks (usually types A, C and D). 7Fr and 10 Fr stents can be inserted without sphincterotomy. A prompt therapeutic response with cessation of bile extravasation in 70-95% of cases within a period of 1-7 days.
22 In the past, nasobiliary drains were used because they did not require sphincterotomy, and removal did not require second endoscopic procedure. However, nasobiliary drains are poorly tolerated and they are not able to transport more than onethird of daily bile production which makes them less effective than internal stents.
23 Another method of non-surgical treatment of bile leak is PTC drainage. However, bile ducts are usually of normal caliber when there is leakage, which makes the procedure difficult. PTC is usually reserved for instances when ERCP is unsuccessful or in preparation for surgical repair.
24 Intrahepatic bile duct injuries are not easily accessible by the retrograde route. In certain instances, the distal part of the injured bile duct may be closed and ERCP, therefore, may fail to reveal any contrast extravasation. Bile can thus continue to leak from the proximal part of the injury, and response to endoscopic treatment will be lacking. In this case, PTC may be useful, or repair surgically.
25 Experimental Histoacryl glue approved in Europe for the sealing of biliary fistulae; and botulinum toxin injection to sphincter of Oddi successful in canine models.
Biliary Stone Disease
 Biliary Stone Disease Delivering the best in care UHB is a no smoking Trust To see all of our current patient information leaflets please visit www.uhb.nhs.uk/patient-information-leaflets.htm You have
Biliary Stone Disease Delivering the best in care UHB is a no smoking Trust To see all of our current patient information leaflets please visit www.uhb.nhs.uk/patient-information-leaflets.htm You have
Gallbladder - gallstones and surgery
 Gallbladder - gallstones and surgery Summary Gallstones are small stones made from cholesterol, bile pigment and calcium salts, which form in a person s gall bladder. Medical treatment isn t necessary
Gallbladder - gallstones and surgery Summary Gallstones are small stones made from cholesterol, bile pigment and calcium salts, which form in a person s gall bladder. Medical treatment isn t necessary
Bile Leak after Laparoscopic Cholecystectomy. Sybile Val MD Long Island College Hospital September 22, 2006
 Bile Leak after Laparoscopic Cholecystectomy Sybile Val MD Long Island College Hospital September 22, 2006 History and Physical Chief Complaint: Severe abdominal pain x one day HPI: Patient is a xx year
Bile Leak after Laparoscopic Cholecystectomy Sybile Val MD Long Island College Hospital September 22, 2006 History and Physical Chief Complaint: Severe abdominal pain x one day HPI: Patient is a xx year
Pathway for the Management of Acute Gallstone Diseases
 Pathway for the Management of Acute Gallstone Diseases What s in this document? Pathways to encourage safer, faster and more cost effective management of acute gallstone (GS) disease by stratification
Pathway for the Management of Acute Gallstone Diseases What s in this document? Pathways to encourage safer, faster and more cost effective management of acute gallstone (GS) disease by stratification
ERCP in Post Surgical Anatomy
 ERCP in Post Surgical Anatomy ACG Western Regional Course, 2013 John G. Lee, MD Division of Gastroenterology University of California, Irvine Medical Center Common surgical alterations Intact pancreaticobiliary
ERCP in Post Surgical Anatomy ACG Western Regional Course, 2013 John G. Lee, MD Division of Gastroenterology University of California, Irvine Medical Center Common surgical alterations Intact pancreaticobiliary
WHAT S WRONG WITH MY GALL BLADDER? GALL BLADDER POLYPS
 WHAT S WRONG WITH MY GALL BLADDER? GALL BLADDER POLYPS This is a patient information booklet providing specific practical information about gall bladder polyps in brief. Its aim is to provide the patient
WHAT S WRONG WITH MY GALL BLADDER? GALL BLADDER POLYPS This is a patient information booklet providing specific practical information about gall bladder polyps in brief. Its aim is to provide the patient
Preoperative Diagnosis and Efficacy of Laparoscopic Procedures in the Treatment of Mirizzi Syndrome
 Preoperative Diagnosis and Efficacy of Laparoscopic Procedures in the Treatment of Mirizzi Syndrome A-Hon Kwon, MD, Hiroaki Inui, MD BACKGROUND: STUDY DESIGN: RESULTS: CONCLUSIONS: The role of laparoscopic
Preoperative Diagnosis and Efficacy of Laparoscopic Procedures in the Treatment of Mirizzi Syndrome A-Hon Kwon, MD, Hiroaki Inui, MD BACKGROUND: STUDY DESIGN: RESULTS: CONCLUSIONS: The role of laparoscopic
USE OF STENTS FOR UPPER GI DISASTERS. Michael Talbot. The St George Hospital, Sydney
 USE OF STENTS FOR UPPER GI DISASTERS Michael Talbot. The St George Hospital, Sydney Disclosures Educational grants by Coviden, Applied Medical, Endogastric Solutions and Allergan in the last 3 years Clinical
USE OF STENTS FOR UPPER GI DISASTERS Michael Talbot. The St George Hospital, Sydney Disclosures Educational grants by Coviden, Applied Medical, Endogastric Solutions and Allergan in the last 3 years Clinical
Colocutaneous Fistula. Disclosures
 Colocutaneous Fistula Madhulika G. Varma MD Associate Professor Chief, Colorectal Surgery University of California, San Francisco Honoraria Applied Medical Covidien Disclosures 1 Colocutaneous Fistula
Colocutaneous Fistula Madhulika G. Varma MD Associate Professor Chief, Colorectal Surgery University of California, San Francisco Honoraria Applied Medical Covidien Disclosures 1 Colocutaneous Fistula
Gary M. Annuniziata, D.O., F.A.C.P. Anh T. Duong, M.D. Jonathan C. Lin, M.D., MPH. Preparation for EGD, ERCP, Peg Placement.
 Gary M. Annuniziata, D.O., F.A.C.P. Anh T. Duong, M.D. Jonathan C. Lin, M.D., MPH Phone- (760) 321-2500 Fax- (760) 321-5720 Preparation for EGD, ERCP, Peg Placement Patient Name- Procedure Date and Time-
Gary M. Annuniziata, D.O., F.A.C.P. Anh T. Duong, M.D. Jonathan C. Lin, M.D., MPH Phone- (760) 321-2500 Fax- (760) 321-5720 Preparation for EGD, ERCP, Peg Placement Patient Name- Procedure Date and Time-
A Guide for Patients Living with a Biliary Metal Stent
 A Guide for Patients Living with a Biliary Metal Stent What is a biliary metal stent? A biliary metal stent (also known as a bile duct stent ) is a flexible metallic tube specially designed to hold your
A Guide for Patients Living with a Biliary Metal Stent What is a biliary metal stent? A biliary metal stent (also known as a bile duct stent ) is a flexible metallic tube specially designed to hold your
Long-term follow-up after biliary stent placement for postoperative bile duct stenosis
 Long-term follow-up after biliary stent placement for postoperative bile duct stenosis Jacques J. G. H. M. Bergman, MD, Lotje Burgemeister, MD, Marco J. Bruno, MD, Erik A. J. Rauws, MD, Dirk J. Gouma,
Long-term follow-up after biliary stent placement for postoperative bile duct stenosis Jacques J. G. H. M. Bergman, MD, Lotje Burgemeister, MD, Marco J. Bruno, MD, Erik A. J. Rauws, MD, Dirk J. Gouma,
Laparoscopic Gallbladder Removal (Cholecystectomy) Patient Information from SAGES
 Patient Information from SAGES") Laparoscopic Gallbladder Removal (Cholecystectomy) Patient Information from SAGES Gallbladder removal is one of the most commonly performed surgical procedures. Gallbladder removal surgery is usually performed
Laparoscopic Gallbladder Removal (Cholecystectomy) Patient Information from SAGES Gallbladder removal is one of the most commonly performed surgical procedures. Gallbladder removal surgery is usually performed
Journal Name: International Journal of Hepatobiliary and Pancreatic Diseases (IJHPD)
") ACCEPTED MAN U SCRIPT EARLY VIEW ARTICLE Early View Article: Online published version of an accepted article before inclusion in an issue of International Journal of Hepatobiliary and Pancreatic Diseases
ACCEPTED MAN U SCRIPT EARLY VIEW ARTICLE Early View Article: Online published version of an accepted article before inclusion in an issue of International Journal of Hepatobiliary and Pancreatic Diseases
PATIENT CONSENT TO PROCEDURE - ROUX-EN-Y GASTRIC BYPASS
 As a patient you must be adequately informed about your condition and the recommended surgical procedure. Please read this document carefully and ask about anything you do not understand. Please initial
As a patient you must be adequately informed about your condition and the recommended surgical procedure. Please read this document carefully and ask about anything you do not understand. Please initial
11/10/2014. I have nothing to Disclose. Covered Stents discussed are NOT FDA approved for the indications covered in my presentation
 I have nothing to Disclose Ramsey Dallal, MD, FACS Vice Chair Department of Surgery Chief Bariatric i and Minimally i Invasive Surgery Einstein Healthcare Network Nemacolin, PA 2014 Covered Stents discussed
I have nothing to Disclose Ramsey Dallal, MD, FACS Vice Chair Department of Surgery Chief Bariatric i and Minimally i Invasive Surgery Einstein Healthcare Network Nemacolin, PA 2014 Covered Stents discussed
Acute Abdominal Pain following Bariatric Surgery. Disclosure. Objectives 8/17/2015. I have nothing to disclose
 Acute Abdominal Pain following Bariatric Surgery Kathy J. Morris, DNP, APRN, FNP C, FAANP University of Nebraska Medical Center College of Nursing Disclosure I have nothing to disclose Objectives Pathophysiology
Acute Abdominal Pain following Bariatric Surgery Kathy J. Morris, DNP, APRN, FNP C, FAANP University of Nebraska Medical Center College of Nursing Disclosure I have nothing to disclose Objectives Pathophysiology
CPT COD1NG UPDATES Gastroenterology CPT Advisors
 2014 CPT COD1NG UPDATES Gastroenterology CPT Advisors Joel V. Brill, MD, AGA CPT Advisor Daniel C. DeMarco, MD, ACG CPT Advisor Glenn D. Littenberg, MD, ASGE CPT Advisor The American College of Gastroenterology
2014 CPT COD1NG UPDATES Gastroenterology CPT Advisors Joel V. Brill, MD, AGA CPT Advisor Daniel C. DeMarco, MD, ACG CPT Advisor Glenn D. Littenberg, MD, ASGE CPT Advisor The American College of Gastroenterology
Clinical Anatomy of the Biliary Apparatus: Relations & Variations
 Clinical Anatomy of the Biliary Apparatus: Relations & Variations Handout download: http://www.oucom.ohiou.edu/dbms-witmer/gs-rpac.htm 24 January 2012 Lawrence M. Witmer, PhD Professor of Anatomy Department
Clinical Anatomy of the Biliary Apparatus: Relations & Variations Handout download: http://www.oucom.ohiou.edu/dbms-witmer/gs-rpac.htm 24 January 2012 Lawrence M. Witmer, PhD Professor of Anatomy Department
A GUIDE TO HAVING PERCUTANEOUS TRANSHEPATIC CHOLANGIOGRAM (PTC) AND BILIARY DRAIN/DILATATION/STENTING
 AND BILIARY DRAIN/DILATATION/STENTING") A GUIDE TO HAVING PERCUTANEOUS TRANSHEPATIC CHOLANGIOGRAM (PTC) AND BILIARY DRAIN/DILATATION/STENTING WHAT IS PERCUTANEOUS TRANSHEPATIC CHOLANGIOGRAM (PTC) AND BILIARY DRAIN/ DILATATION/STENTING? A percutaneous
A GUIDE TO HAVING PERCUTANEOUS TRANSHEPATIC CHOLANGIOGRAM (PTC) AND BILIARY DRAIN/DILATATION/STENTING WHAT IS PERCUTANEOUS TRANSHEPATIC CHOLANGIOGRAM (PTC) AND BILIARY DRAIN/ DILATATION/STENTING? A percutaneous
Steven B. Goldin, MD, PhD University of South Florida Dimitrios Stefanidis, MD, PhD
 RUQ Abdominal Pain Steven B. Goldin, MD, PhD University of South Florida Dimitrios Stefanidis, MD, PhD Mrs. Stone 41 year-old woman in the ER presenting with 12 hours duration of progressively worsening
RUQ Abdominal Pain Steven B. Goldin, MD, PhD University of South Florida Dimitrios Stefanidis, MD, PhD Mrs. Stone 41 year-old woman in the ER presenting with 12 hours duration of progressively worsening
The Whipple Procedure. Sally Hodges, Ph.D.(c) Given the length and difficulty of the procedure, regardless of the diagnosis, certain
 Given the length and difficulty of the procedure, regardless of the diagnosis, certain") The Whipple Procedure Sally Hodges, Ph.D.(c) Preoperative procedures Given the length and difficulty of the procedure, regardless of the diagnosis, certain assurances must occur prior to offering a patient
The Whipple Procedure Sally Hodges, Ph.D.(c) Preoperative procedures Given the length and difficulty of the procedure, regardless of the diagnosis, certain assurances must occur prior to offering a patient
Endoscopy and infection: Prevention of infection during endoscopy Treatment of infection by endoscopy. M. Arvanitakis SRBG June 2009
 Endoscopy and infection: Prevention of infection during endoscopy Treatment of infection by endoscopy M. Arvanitakis SRBG June 2009 Outline Antibiotic prophylaxis during endoscopy Upper GI endoscopy Lower
Endoscopy and infection: Prevention of infection during endoscopy Treatment of infection by endoscopy M. Arvanitakis SRBG June 2009 Outline Antibiotic prophylaxis during endoscopy Upper GI endoscopy Lower
SOD (Sphincter of Oddi Dysfunction)
") SOD (Sphincter of Oddi Dysfunction) SOD refers to the mechanical malfunctioning of the Sphincter of Oddi, which is the valve muscle that regulates the flow of bile and pancreatic juice into the duodenum.
SOD (Sphincter of Oddi Dysfunction) SOD refers to the mechanical malfunctioning of the Sphincter of Oddi, which is the valve muscle that regulates the flow of bile and pancreatic juice into the duodenum.
Lenox Hill Hospital Department of Surgery General Surgery Goals and Objectives
 Lenox Hill Hospital Department of Surgery General Surgery Goals and Objectives Medical Knowledge and Patient Care: Residents must demonstrate knowledge and application of the pathophysiology and epidemiology
Lenox Hill Hospital Department of Surgery General Surgery Goals and Objectives Medical Knowledge and Patient Care: Residents must demonstrate knowledge and application of the pathophysiology and epidemiology
Red Flags. Whether you handle malpractice. in General Surgical Malpractice Cases
 10 Red Flags in General Surgical Malpractice Cases Whether you handle malpractice cases regularly or you have a general personal injury practice, at some point you likely will need to evaluate a general
10 Red Flags in General Surgical Malpractice Cases Whether you handle malpractice cases regularly or you have a general personal injury practice, at some point you likely will need to evaluate a general
To Whipple or Not to Whipple, that is the Question: Evaluating the Resectability of Pancreatic Adenocarcinoma
 August 2009 To Whipple or Not to Whipple, that is the Question: Evaluating the Resectability of Pancreatic Adenocarcinoma Christina Ramirez, Harvard Medical School Year III Gillian Lieberman, MD Agenda
August 2009 To Whipple or Not to Whipple, that is the Question: Evaluating the Resectability of Pancreatic Adenocarcinoma Christina Ramirez, Harvard Medical School Year III Gillian Lieberman, MD Agenda
Acute abdominal conditions Key Points
 7 Acute abdominal conditions Key Points 7.1 ASSESSMENT AND DIAGNOSIS Referred abdominal pain Fore gut pain (stomach, duodenum, gall bladder) is referred to the upper abdomen Mid gut pain (small intestine,
7 Acute abdominal conditions Key Points 7.1 ASSESSMENT AND DIAGNOSIS Referred abdominal pain Fore gut pain (stomach, duodenum, gall bladder) is referred to the upper abdomen Mid gut pain (small intestine,
Muskegon Surgical Associates, P.L.C. www.msapc.com
 GALLBLADDER SURGERY Muskegon Surgical Associates, P.L.C. www.msapc.com Mercy Drive Office 1316 Mercy Drive Muskegon, Michigan 49444 231-739-9461 1-888-874-5892 (Toll Free) Grand Haven Office 1445 Sheldon,
GALLBLADDER SURGERY Muskegon Surgical Associates, P.L.C. www.msapc.com Mercy Drive Office 1316 Mercy Drive Muskegon, Michigan 49444 231-739-9461 1-888-874-5892 (Toll Free) Grand Haven Office 1445 Sheldon,
Surgery and other procedures to control symptoms
 Surgery and other procedures to control symptoms This fact sheet is for people diagnosed with inoperable pancreatic cancer who will be having surgery or another interventional procedure to relieve symptoms
Surgery and other procedures to control symptoms This fact sheet is for people diagnosed with inoperable pancreatic cancer who will be having surgery or another interventional procedure to relieve symptoms
restricted to certain centers and certain patients, preferably in some sort of experimental trial format.
 Managing Pancreatic Cancer, Part 4: Pancreatic Cancer Surgery, Complications, & the Importance of Surgical Volume Dr. Matthew Katz, Surgeon, MD Anderson Cancer Center, Houston, TX I m going to talk a little
Managing Pancreatic Cancer, Part 4: Pancreatic Cancer Surgery, Complications, & the Importance of Surgical Volume Dr. Matthew Katz, Surgeon, MD Anderson Cancer Center, Houston, TX I m going to talk a little
How to Effectively Code for Endoscopic Procedures in Gastroenterology
 How to Effectively Code for Endoscopic Procedures in Gastroenterology Ariwan Rakvit, MD Associate Professor Interim Chief, Division of Gastroenterology Texas Tech University Health Science Center All rights
How to Effectively Code for Endoscopic Procedures in Gastroenterology Ariwan Rakvit, MD Associate Professor Interim Chief, Division of Gastroenterology Texas Tech University Health Science Center All rights
IN THE CIRCUIT COURT OF THE STATE OF OREGON FOR THE COUNTY OF [COUNTY]
![IN THE CIRCUIT COURT OF THE STATE OF OREGON FOR THE COUNTY OF [COUNTY]](/thumbs/26/8837397.jpg "IN THE CIRCUIT COURT OF THE STATE OF OREGON FOR THE COUNTY OF [COUNTY]") IN THE CIRCUIT COURT OF THE STATE OF OREGON FOR THE COUNTY OF [COUNTY] [PLAINTIFF], CASE NO. Plaintiff, (Negligence Medical Malpractice v. Claim Not Subject to Mandatory Arbitration [NAMES] (Prayer Amount
IN THE CIRCUIT COURT OF THE STATE OF OREGON FOR THE COUNTY OF [COUNTY] [PLAINTIFF], CASE NO. Plaintiff, (Negligence Medical Malpractice v. Claim Not Subject to Mandatory Arbitration [NAMES] (Prayer Amount
Biliary stenting: Indications, choice of stents and results: European Society of Gastrointestinal Endoscopy (ESGE) clinical guideline
 clinical guideline") Guideline 277 Biliary stenting: Indications, choice of stents and results: European Society of Gastrointestinal Endoscopy (ESGE) clinical guideline Authors J.-M. Dumonceau 1, A. Tringali 2, D. Blero 3,
Guideline 277 Biliary stenting: Indications, choice of stents and results: European Society of Gastrointestinal Endoscopy (ESGE) clinical guideline Authors J.-M. Dumonceau 1, A. Tringali 2, D. Blero 3,
2016 Quick Reference Coding Chart
 43197 Trans nasal esophagoscopy 43198 Biospy Trans Nasal Esophagoscopy Esophagoscopy 43200 Esophagoscopy Includes collection of specimen(s) by brushing or washing, when performed. 43201 Submucosal injection
43197 Trans nasal esophagoscopy 43198 Biospy Trans Nasal Esophagoscopy Esophagoscopy 43200 Esophagoscopy Includes collection of specimen(s) by brushing or washing, when performed. 43201 Submucosal injection
Gallstones. National Digestive Diseases Information Clearinghouse
 Gallstones National Digestive Diseases Information Clearinghouse National Institute of Diabetes and Digestive and Kidney Diseases NATIONAL INSTITUTES OF HEALTH U.S. Department of Health and Human Services
Gallstones National Digestive Diseases Information Clearinghouse National Institute of Diabetes and Digestive and Kidney Diseases NATIONAL INSTITUTES OF HEALTH U.S. Department of Health and Human Services
Treatment of Hepatic Neoplasm
 I. Policy University Health Alliance (UHA) will reimburse for treatment of hepatic neoplasm outside of systemic chemotherapy alone when determined to be medically necessary and within the medical criteria
I. Policy University Health Alliance (UHA) will reimburse for treatment of hepatic neoplasm outside of systemic chemotherapy alone when determined to be medically necessary and within the medical criteria
Open Ventral Hernia Repair
 Ventral Hernias Open Ventral Hernia Repair UCSF Postgraduate Course in General Surgery Maui, HI March 21, 2011 Hobart W. Harris, MD, MPH Ventral Hernias: National Experience Occur following 11-23% of laparotomies,
Ventral Hernias Open Ventral Hernia Repair UCSF Postgraduate Course in General Surgery Maui, HI March 21, 2011 Hobart W. Harris, MD, MPH Ventral Hernias: National Experience Occur following 11-23% of laparotomies,
Your Map of the ICD-9 to ICD-10 PCS Conversion
 Your Map of the ICD-9 to ICD-10 PCS Conversion Table of Contents Disclaimer 3 Endoscopy 4 Interventional Cardiology 20 Neuromodulation 34 Peripheral Interventions 35 Rhythm Management and Electrophysiology
Your Map of the ICD-9 to ICD-10 PCS Conversion Table of Contents Disclaimer 3 Endoscopy 4 Interventional Cardiology 20 Neuromodulation 34 Peripheral Interventions 35 Rhythm Management and Electrophysiology
EAES course on Advanced Laparoscopic GI Surgery Course. Riyadh, Saudi Arabia 10-14 January 2015
 EAES course on Advanced Laparoscopic GI Surgery Course Riyadh, Saudi Arabia 10-14 January 2015 The European Association for Endoscopic Surgery and King Khalid University Hospital, Riyadh, Saudi Arabia
EAES course on Advanced Laparoscopic GI Surgery Course Riyadh, Saudi Arabia 10-14 January 2015 The European Association for Endoscopic Surgery and King Khalid University Hospital, Riyadh, Saudi Arabia
Biliary Injury in Laparoscopic Surgery: Part 1. Processes Used in Determination of Standard of Care in Misidentification Injuries
 EDUCATION Biliary Injury in Laparoscopic Surgery: Part 1. Processes Used in Determination of Standard of Care in Misidentification Injuries Steven M Strasberg, MD, FACS Biliary injury is a major cause
EDUCATION Biliary Injury in Laparoscopic Surgery: Part 1. Processes Used in Determination of Standard of Care in Misidentification Injuries Steven M Strasberg, MD, FACS Biliary injury is a major cause
Ultrasound versus liver function tests for diagnosis of common bile duct stones (Review)
") Ultrasound versus liver function tests for diagnosis of common bile duct stones (Review) Gurusamy KS, Giljaca V, Takwoingi Y, Higgie D, Poropat G, Štimac D, Davidson BR This is a reprint of a Cochrane
Ultrasound versus liver function tests for diagnosis of common bile duct stones (Review) Gurusamy KS, Giljaca V, Takwoingi Y, Higgie D, Poropat G, Štimac D, Davidson BR This is a reprint of a Cochrane
Guidelines for the Clinical Application of Laparoscopic Biliary Tract Surgery
 Guidelines for the Clinical Application of Laparoscopic Biliary Tract Surgery I. PREAMBLE Laparoscopic cholecystectomy has become the standard of care for patients requiring the removal of the gallbladder.
Guidelines for the Clinical Application of Laparoscopic Biliary Tract Surgery I. PREAMBLE Laparoscopic cholecystectomy has become the standard of care for patients requiring the removal of the gallbladder.
Bile Duct Diseases and Problems
 Bile Duct Diseases and Problems Introduction A bile duct is a tube that carries bile between the liver and gallbladder and the intestine. Bile is a substance made by the liver that helps with digestion.
Bile Duct Diseases and Problems Introduction A bile duct is a tube that carries bile between the liver and gallbladder and the intestine. Bile is a substance made by the liver that helps with digestion.
Cholangiocarcinoma (Bile Duct Cancer) Patient Information Booklet
 Patient Information Booklet") Cholangiocarcinoma (Bile Duct Cancer) Patient Information Booklet Delivering the best in care UHB is a no smoking Trust To see all of our current patient information leaflets please visit www.uhb.nhs.uk/patient-information-leaflets.htm
Cholangiocarcinoma (Bile Duct Cancer) Patient Information Booklet Delivering the best in care UHB is a no smoking Trust To see all of our current patient information leaflets please visit www.uhb.nhs.uk/patient-information-leaflets.htm
Gallbladder Diseases and Problems
 Gallbladder Diseases and Problems Introduction Your gallbladder is a pear-shaped organ under your liver. It stores bile, a fluid made by your liver to digest fat. There are many diseases and problems that
Gallbladder Diseases and Problems Introduction Your gallbladder is a pear-shaped organ under your liver. It stores bile, a fluid made by your liver to digest fat. There are many diseases and problems that
Laparoscopic Cholecystectomy
 Laparoscopic Cholecystectomy Gallbladder removal is one of the most commonly performed surgical procedures in the United States. Today,gallbladder surgery is performed laparoscopically. The medical name
Laparoscopic Cholecystectomy Gallbladder removal is one of the most commonly performed surgical procedures in the United States. Today,gallbladder surgery is performed laparoscopically. The medical name
Secretin Enhanced Imaging of the Pancreas
 Secretin Enhanced Imaging of the Pancreas Pablo R. Ros, MD University Hospitals Case Medical Center Case Western Reserve University SCBT-MR Boston, MA October, 2012 Pablo.Ros@UHhospitals.org Disclosures
Secretin Enhanced Imaging of the Pancreas Pablo R. Ros, MD University Hospitals Case Medical Center Case Western Reserve University SCBT-MR Boston, MA October, 2012 Pablo.Ros@UHhospitals.org Disclosures
Marginal Ulcers. Marginal Ulcers. Gastric Remnant Ulcers. Double Balloon Enteroscopy. Marginal Ulcer. Gastrojejunal Stricture.
 Upper Abdominal Pain in the Bariatric Surgery Patient Martin L. Freeman, M.D., FASGE,FACG Professor of Medicine Director, Pancreaticobiliary Endoscopy Fellowship Interim Director, Division of GI, Hepatology
Upper Abdominal Pain in the Bariatric Surgery Patient Martin L. Freeman, M.D., FASGE,FACG Professor of Medicine Director, Pancreaticobiliary Endoscopy Fellowship Interim Director, Division of GI, Hepatology
Laparoscopic Cholecystectomy (Removal of the Gallbladder)
") Laparoscopic Cholecystectomy (Removal of the Gallbladder) The gall bladder is a small pear-shaped organ that lies in the right upper quadrant of your abdomen under your liver (under your ribs). The liver
Laparoscopic Cholecystectomy (Removal of the Gallbladder) The gall bladder is a small pear-shaped organ that lies in the right upper quadrant of your abdomen under your liver (under your ribs). The liver
PANCREATIC AND PERIAMPULLARY TUMORS: PANCREATICODUODENECTOMY. Dr. Shailesh V. Shrikhande
 PANCREATIC AND PERIAMPULLARY TUMORS: PANCREATICODUODENECTOMY Dr. Shailesh V. Shrikhande Associate Professor & Consultant Surgeon GI and HPB Surgical Oncology Tata Memorial Hospital, Mumbai INDIA HELICAL
PANCREATIC AND PERIAMPULLARY TUMORS: PANCREATICODUODENECTOMY Dr. Shailesh V. Shrikhande Associate Professor & Consultant Surgeon GI and HPB Surgical Oncology Tata Memorial Hospital, Mumbai INDIA HELICAL
Surgery and cancer of the pancreas
 Surgery and cancer of the pancreas This information is an extract from the booklet Understanding cancer of the pancreas. You may find the full booklet helpful. We can send you a free copy see page 8. Introduction
Surgery and cancer of the pancreas This information is an extract from the booklet Understanding cancer of the pancreas. You may find the full booklet helpful. We can send you a free copy see page 8. Introduction
Cholecystectomy for acute gallstone pancreatitis: early vs delayed approach
 Scandinavian Journal of Surgery 99: 81 85, 2010 Cholecystectomy for acute gallstone pancreatitis: early vs delayed approach C. T. Wilson, M. A. de Moya Department of Trauma, Emergency Surgery, and Critical
Scandinavian Journal of Surgery 99: 81 85, 2010 Cholecystectomy for acute gallstone pancreatitis: early vs delayed approach C. T. Wilson, M. A. de Moya Department of Trauma, Emergency Surgery, and Critical
A Patient s Guide to. Pancreatic Cysts. University of Michigan Comprehensive Cancer Center
 A Patient s Guide to Pancreatic Cysts University of Michigan Comprehensive Cancer Center Staff of the Comprehensive Cancer Center s Multidisciplinary Pancreatic Cancer Program provided information for
A Patient s Guide to Pancreatic Cysts University of Michigan Comprehensive Cancer Center Staff of the Comprehensive Cancer Center s Multidisciplinary Pancreatic Cancer Program provided information for
Quality indicators, including complications, of ERCP in a community setting: a prospective study
 ORIGINAL ARTICLE: Clinical Endoscopy Quality indicators, including complications, of ERCP in a community setting: a prospective study Joshua B. Colton, MD, Colleen C. Curran, MS St. Paul, Minnesota, USA
ORIGINAL ARTICLE: Clinical Endoscopy Quality indicators, including complications, of ERCP in a community setting: a prospective study Joshua B. Colton, MD, Colleen C. Curran, MS St. Paul, Minnesota, USA
Laparoscopic Cholecystectomy
 Laparoscopic Cholecystectomy Removal of Gall Bladder Page 12 Patient Information Further Information We endeavour to provide an excellent service at all times, but should you have any concerns please,
Laparoscopic Cholecystectomy Removal of Gall Bladder Page 12 Patient Information Further Information We endeavour to provide an excellent service at all times, but should you have any concerns please,
The digestive system. Medicine and technology. Normal structure and function Diagnostic methods Example diseases and therapies
 The digestive system Medicine and technology Normal structure and function Diagnostic methods Example diseases and therapies The digestive system An overview (1) Oesophagus Liver (hepar) Biliary system
The digestive system Medicine and technology Normal structure and function Diagnostic methods Example diseases and therapies The digestive system An overview (1) Oesophagus Liver (hepar) Biliary system
Pancreatic Cancer Understanding your diagnosis
 Pancreatic Cancer Understanding your diagnosis Let s Make Cancer History 1 888 939-3333 cancer.ca Pancreatic Cancer Understanding your diagnosis When you first hear that you have cancer you may feel alone
Pancreatic Cancer Understanding your diagnosis Let s Make Cancer History 1 888 939-3333 cancer.ca Pancreatic Cancer Understanding your diagnosis When you first hear that you have cancer you may feel alone
Cancer Surgery Volume Study: ICD-9 and CPT Codes
 This paper contains the ICD-9 diagnostic and procedure codes and the CPT procedure codes used by researchers for a project of the California HealthCare Foundation (CHCF) and the California Office of Statewide
This paper contains the ICD-9 diagnostic and procedure codes and the CPT procedure codes used by researchers for a project of the California HealthCare Foundation (CHCF) and the California Office of Statewide
David R. DeHaas, Jr. MD Sacred Heart Medical Center at RiverBend
 David R. DeHaas, Jr. MD Sacred Heart Medical Center at RiverBend 1. To review the surgical history of the Whipple procedure for periampullary tumors. 2. To review the differential diagnosis for patients
David R. DeHaas, Jr. MD Sacred Heart Medical Center at RiverBend 1. To review the surgical history of the Whipple procedure for periampullary tumors. 2. To review the differential diagnosis for patients
Basic Laparoscopy and Lap. Suturing and Stapling course Course Contents
 Online Courses on Laparoscopic GI Surgery for GISurgery.info Lap Skills course Harshad Soni 1. Basic Laparoscopy and Lap. Suturing and Stapling course H. Soni 2. Laparoscopic UGI Surgery Course J Mistry
Online Courses on Laparoscopic GI Surgery for GISurgery.info Lap Skills course Harshad Soni 1. Basic Laparoscopy and Lap. Suturing and Stapling course H. Soni 2. Laparoscopic UGI Surgery Course J Mistry
State of Tennessee Health Care Innovation Initiative Executive Summary
 State of Tennessee Health Care Innovation Initiative Executive Summary Outpatient and Non-acute Inpatient Cholecystectomy Episode OVERVIEW OF AN OUTPATIENT AND NON-ACUTE INPATIENT CHOLECYSTECTOMY EPISODE
State of Tennessee Health Care Innovation Initiative Executive Summary Outpatient and Non-acute Inpatient Cholecystectomy Episode OVERVIEW OF AN OUTPATIENT AND NON-ACUTE INPATIENT CHOLECYSTECTOMY EPISODE
What will the doctor do?
 Information about Pancreatic Cancer www.corecharity.org.uk What are the symptoms? What are the causes? Pancreatic Cancer explained When should I consult a doctor? What will the doctor do? How should I
Information about Pancreatic Cancer www.corecharity.org.uk What are the symptoms? What are the causes? Pancreatic Cancer explained When should I consult a doctor? What will the doctor do? How should I
Laparoscopic Hernia Repair. Hernia Repair. Laparoscopic Ventral. Several Different Types of Hernia
 Laparoscopic Hernia Repair David B Renton, MD Assistant Professor Department of Surgery The Ohio State University Advantages of Laparoscopic Ventral vs. Open Hernia Repair Lower wound infection rate: 2.6%
Laparoscopic Hernia Repair David B Renton, MD Assistant Professor Department of Surgery The Ohio State University Advantages of Laparoscopic Ventral vs. Open Hernia Repair Lower wound infection rate: 2.6%
When, Why, and How to Revise a Failed Sleeve Gastrectomy
 When, Why, and How to Revise a Failed Sleeve Gastrectomy Jin S. Yoo M.D. Assistant Professor of Surgery Duke University Medical Center April 6, 2013 When and Why Already Covered Let s Talk About How Overview
When, Why, and How to Revise a Failed Sleeve Gastrectomy Jin S. Yoo M.D. Assistant Professor of Surgery Duke University Medical Center April 6, 2013 When and Why Already Covered Let s Talk About How Overview
Case 1. 79 y old woman Medical history: Diabetes insuline treatment Hypertension Obesity CABG + Pacemaker Ilocolic resection for T2 colonadenoca 2009
 Cholangitis Difficult stone management D. De Wulf AZ Delta Roeselare UZ Gent Case 1 79 y old woman Medical history: Diabetes insuline treatment Hypertension Obesity CABG + Pacemaker Ilocolic resection
Cholangitis Difficult stone management D. De Wulf AZ Delta Roeselare UZ Gent Case 1 79 y old woman Medical history: Diabetes insuline treatment Hypertension Obesity CABG + Pacemaker Ilocolic resection
Guide to Abdominal or Gastroenterological Surgery Claims
 What are the steps towards abdominal surgery? Investigation and Diagnosis It is very important that all necessary tests are undertaken to investigate the patient s symptoms appropriately and an accurate
What are the steps towards abdominal surgery? Investigation and Diagnosis It is very important that all necessary tests are undertaken to investigate the patient s symptoms appropriately and an accurate
CEU Update. Pancreatic Cancer
 CEU Update A semi-annual publication of the National Association for Health Professionals June 2015 Issue #0615 Pancreatic Cancer The Pancreatic Cancer Action Network, Inc. (PanCAN), established in 1999,
CEU Update A semi-annual publication of the National Association for Health Professionals June 2015 Issue #0615 Pancreatic Cancer The Pancreatic Cancer Action Network, Inc. (PanCAN), established in 1999,
Billing Guideline. Subject: Colorectal Cancer Screening Exams (Invasive Procedures) Effective Date: 1/1/2012 Last Update Effective: 4/16
 Effective Date: 1/1/2012 Last Update Effective: 4/16") Subject: Colorectal Cancer Screening Exams (Invasive Procedures) Effective Date: 1/1/2012 Last Update Effective: 4/16 Billing Guideline Background Health First administers benefit packages with full coverage
Subject: Colorectal Cancer Screening Exams (Invasive Procedures) Effective Date: 1/1/2012 Last Update Effective: 4/16 Billing Guideline Background Health First administers benefit packages with full coverage
Surgical Treatment of Various GI Tract Cancers
 Surgical Treatment of Various GI Tract Cancers By James Ouellette, DO, FACS, Surgical Oncology, Hepatobiliary Surgery Surgical treatment for most gastrointestinal (GI) cancers requires multidisciplinary
Surgical Treatment of Various GI Tract Cancers By James Ouellette, DO, FACS, Surgical Oncology, Hepatobiliary Surgery Surgical treatment for most gastrointestinal (GI) cancers requires multidisciplinary
Gallstone Ileus. Audrey C. Durrant,, M.D. SUNY Downstate Medical Center May 20, 2005
 Gallstone Ileus Audrey C. Durrant,, M.D. SUNY Downstate Medical Center May 20, 2005 Gallstone Ileus Diagnosis and Management Background Misnomer coined by Bartolin in 1654 Not a true ileus True mechanical
Gallstone Ileus Audrey C. Durrant,, M.D. SUNY Downstate Medical Center May 20, 2005 Gallstone Ileus Diagnosis and Management Background Misnomer coined by Bartolin in 1654 Not a true ileus True mechanical
Endoscopic therapy for obesity and complications of bariatric surgery
 Endoscopic therapy for obesity and complications of bariatric surgery Jacques Devière, MD, PhD Erasme University Hospital Brussels Belgium jacques.deviere@erasme.ulb.ac.be Obesity Affects 300 millions
Endoscopic therapy for obesity and complications of bariatric surgery Jacques Devière, MD, PhD Erasme University Hospital Brussels Belgium jacques.deviere@erasme.ulb.ac.be Obesity Affects 300 millions
GASTROENTEROLOGY FELLOWSHIP PANCREATICOBILARY CONSULTATION SERVICE GOALS AND OBJECTIVES University of Toledo
 GASTROENTEROLOGY FELLOWSHIP PANCREATICOBILARY CONSULTATION SERVICE GOALS AND OBJECTIVES University of Toledo Educational Purpose: The Pancreaticobiliary Service at UTMC introduces the fellow to inpatient
GASTROENTEROLOGY FELLOWSHIP PANCREATICOBILARY CONSULTATION SERVICE GOALS AND OBJECTIVES University of Toledo Educational Purpose: The Pancreaticobiliary Service at UTMC introduces the fellow to inpatient
A Patient s Guide to. Pancreatic Cancer
 A Patient s Guide to Pancreatic Cancer Staff of the Comprehensive Cancer Center s Multidisciplinary Pancreatic Cancer Program provided information for this handbook GI Oncology Program, Patient Education
A Patient s Guide to Pancreatic Cancer Staff of the Comprehensive Cancer Center s Multidisciplinary Pancreatic Cancer Program provided information for this handbook GI Oncology Program, Patient Education
Gallbladder Cancer. What is gallbladder cancer? About the gallbladder
 Gallbladder Cancer What is gallbladder cancer? Cancer starts when cells in the body begin to grow out of control. Cells in nearly any part of the body can become cancer, and can spread to other areas of
Gallbladder Cancer What is gallbladder cancer? Cancer starts when cells in the body begin to grow out of control. Cells in nearly any part of the body can become cancer, and can spread to other areas of
ATLAS FOR THE DELINEATION OF THE POSTOPERATIVE TREATMENT OF PANCREATIC CANCER
 CONSENSUS PANEL CONTOURING ATLAS FOR THE DELINEATION OF THE CLINICAL TARGET VOLUME IN THE POSTOPERATIVE TREATMENT OF PANCREATIC CANCER Collaborators Ross A. Abrams, M.D. 1, William F. Regine, M.D. 2, Karyn
CONSENSUS PANEL CONTOURING ATLAS FOR THE DELINEATION OF THE CLINICAL TARGET VOLUME IN THE POSTOPERATIVE TREATMENT OF PANCREATIC CANCER Collaborators Ross A. Abrams, M.D. 1, William F. Regine, M.D. 2, Karyn
GIANT HERNIA REPAIR MY EXPERIENCE
 GIANT HERNIA REPAIR MY EXPERIENCE Giorgobiani G. Department of Surgery at Tbilisi State Medical University. The AVERSI Clinic.Tbilisi, Georgia. If we could artificially produce tissue of the density and
GIANT HERNIA REPAIR MY EXPERIENCE Giorgobiani G. Department of Surgery at Tbilisi State Medical University. The AVERSI Clinic.Tbilisi, Georgia. If we could artificially produce tissue of the density and
Pancreatic Cancer. The Killer that must be discovered early. Dr Alfred Kow Wei Chieh
 Pancreatic Cancer The Killer that must be discovered early 27 th June 2015 Dr Alfred Kow Wei Chieh Consultant Department of Surgery Division of HPB Surgery & Liver Transplantation & Assistant Dean (Education)
Pancreatic Cancer The Killer that must be discovered early 27 th June 2015 Dr Alfred Kow Wei Chieh Consultant Department of Surgery Division of HPB Surgery & Liver Transplantation & Assistant Dean (Education)
Diagnosis and management of iatrogenic endoscopic perforations: European Society of Gastrointestinal Endoscopy (ESGE) Position Statement
 Position Statement") Diagnosis and management of iatrogenic endoscopic perforations: European Society of Gastrointestinal Endoscopy (ESGE) Position Statement Authors Gregorios A. Paspatis 1, Jean-Marc Dumonceau 2, Marc Barthet
Diagnosis and management of iatrogenic endoscopic perforations: European Society of Gastrointestinal Endoscopy (ESGE) Position Statement Authors Gregorios A. Paspatis 1, Jean-Marc Dumonceau 2, Marc Barthet
MODIFIER 59 ARTICLE. The CPT Manual defines modifier 59 as follows:
 MODIFIER 59 ARTICLE The Medicare National Correct Coding Initiative (NCCI) includes Procedure-to-Procedure (PTP) edits that define when two Healthcare Common Procedure Coding System (HCPCS)/ Current Procedural
MODIFIER 59 ARTICLE The Medicare National Correct Coding Initiative (NCCI) includes Procedure-to-Procedure (PTP) edits that define when two Healthcare Common Procedure Coding System (HCPCS)/ Current Procedural
Dept. of Medical Imaging University of Ottawa
 ED Visits Related to Bariatric Surgery: Review of Normal Post-Surgical Anatomy as Well as Complications Dept. of Medical Imaging University of Ottawa Disclosures Background Roux-en-Y Gastric Bypass Surgery
ED Visits Related to Bariatric Surgery: Review of Normal Post-Surgical Anatomy as Well as Complications Dept. of Medical Imaging University of Ottawa Disclosures Background Roux-en-Y Gastric Bypass Surgery
An External Audit of Laparoscopic Cholecystectomy Performed
 ANNALS OF SURGERY Vol. 220, No. 5,626-634 A 1994 J. B. Lippincott Company An External Audit of Laparoscopic Cholecystectomy Performed in Medical Treatment Facilities of the Department of Defense David
ANNALS OF SURGERY Vol. 220, No. 5,626-634 A 1994 J. B. Lippincott Company An External Audit of Laparoscopic Cholecystectomy Performed in Medical Treatment Facilities of the Department of Defense David
SPINAL STENOSIS Information for Patients WHAT IS SPINAL STENOSIS?
 SPINAL STENOSIS Information for Patients WHAT IS SPINAL STENOSIS? The spinal canal is best imagined as a bony tube through which nerve fibres pass. The tube is interrupted between each pair of adjacent
SPINAL STENOSIS Information for Patients WHAT IS SPINAL STENOSIS? The spinal canal is best imagined as a bony tube through which nerve fibres pass. The tube is interrupted between each pair of adjacent
Endoscopic drainage of pancreatic pseudocysts
 ANNALS OF GASTROENTEROLOGY 2005, 18(4):445-450 Case report Endoscopic drainage of pancreatic pseudocysts E. Christoforidis, K. Bluchos, T. Tsahalis, K. Tsalis, D. Betsis SUMMARY Pancreatic pseudocysts
ANNALS OF GASTROENTEROLOGY 2005, 18(4):445-450 Case report Endoscopic drainage of pancreatic pseudocysts E. Christoforidis, K. Bluchos, T. Tsahalis, K. Tsalis, D. Betsis SUMMARY Pancreatic pseudocysts
Laparoscopic Sleeve gastrectomy
 Restrictive procedure Laparoscopic Sleeve gastrectomy Dr. R. Peterli Professional Education 1 2 Introduction Gastric sleeve resection is the restrictive part of the biliopancreatic diversion duodenal switch,
Restrictive procedure Laparoscopic Sleeve gastrectomy Dr. R. Peterli Professional Education 1 2 Introduction Gastric sleeve resection is the restrictive part of the biliopancreatic diversion duodenal switch,
Chapter 6 Gastrointestinal Impairment
 Chapter 6 Gastrointestinal This chapter consists of 2 parts: Part 6.1 Diseases of the digestive system Part 6.2 Abdominal wall hernias and obesity PART 6.1: DISEASES OF THE DIGESTIVE SYSTEM Diseases of
Chapter 6 Gastrointestinal This chapter consists of 2 parts: Part 6.1 Diseases of the digestive system Part 6.2 Abdominal wall hernias and obesity PART 6.1: DISEASES OF THE DIGESTIVE SYSTEM Diseases of
Pancreaticoduodenectomy (Pylorus-Preserving Whipple Procedure)
") Pancreaticoduodenectomy (Pylorus-Preserving Whipple Procedure) Operative Indications: Pancreaticoduodenectomy, or the Whipple procedure, may be indicated for a variety of benign and malignant diseases.
Pancreaticoduodenectomy (Pylorus-Preserving Whipple Procedure) Operative Indications: Pancreaticoduodenectomy, or the Whipple procedure, may be indicated for a variety of benign and malignant diseases.
to appear yellow caused by excess bilirubin, a substance found in bile and can be elevated in liver disease.
 2 A Tale of Surgeries Non-Blood Surgical Care for Pancreatic Cancer and Small Bowel Obstruction Gail and Theodore McFarland, a married couple from Pottstown, PA, underwent serious and unexpected surgeries
2 A Tale of Surgeries Non-Blood Surgical Care for Pancreatic Cancer and Small Bowel Obstruction Gail and Theodore McFarland, a married couple from Pottstown, PA, underwent serious and unexpected surgeries
A New Hope For Patients with Mild Gallstone Pancreatitis
 RADOMIZED CONTROLLED TRIALS Early Cholecystectomy Safely Decreases Hospital Stay in Patients With Mild Gallstone Pancreatitis A Randomized Prospective Study Armen Aboulian, MD,* Tony Chan, MD,* Arezou
RADOMIZED CONTROLLED TRIALS Early Cholecystectomy Safely Decreases Hospital Stay in Patients With Mild Gallstone Pancreatitis A Randomized Prospective Study Armen Aboulian, MD,* Tony Chan, MD,* Arezou
Recurrent Varicose Veins
 Information for patients Recurrent Varicose Veins Sheffield Vascular Institute Northern General Hospital You have been diagnosed as having Varicose Veins that have recurred (come back). This leaflet explains
Information for patients Recurrent Varicose Veins Sheffield Vascular Institute Northern General Hospital You have been diagnosed as having Varicose Veins that have recurred (come back). This leaflet explains
MR imaging of primary sclerosing cholangitis (PSC) using the hepatobiliary specific contrast agent Gd-EOB-DTPA
 using the hepatobiliary specific contrast agent Gd-EOB-DTPA") MR imaging of primary sclerosing cholangitis (PSC) using the hepatobiliary specific contrast agent Gd-EOB-DTPA Poster No.: C-0019 Congress: ECR 2010 Type: Educational Exhibit Topic: Abdominal Viscera (Solid
MR imaging of primary sclerosing cholangitis (PSC) using the hepatobiliary specific contrast agent Gd-EOB-DTPA Poster No.: C-0019 Congress: ECR 2010 Type: Educational Exhibit Topic: Abdominal Viscera (Solid
ENDOSCOPIC ULTRASOUND (EUS)
") ENDOSCOPIC ULTRASOUND (EUS) What you need to know before your procedure Your Doctor has decided that an EUS is necessary for further evaluation and treatment of your condition. This information sheet has
ENDOSCOPIC ULTRASOUND (EUS) What you need to know before your procedure Your Doctor has decided that an EUS is necessary for further evaluation and treatment of your condition. This information sheet has
Intraoperative Prevention of Stenosis for Laparoscopic Sleeve Gastrectomy
 CASE REPORT Intraoperative Prevention of Stenosis for Laparoscopic Sleeve Gastrectomy Ramon Vilallonga, MD, PhD, Jacques Himpens, MD Division of Bariatric Surgery, AZ St. Blasius, Dendermonde, Belgium
CASE REPORT Intraoperative Prevention of Stenosis for Laparoscopic Sleeve Gastrectomy Ramon Vilallonga, MD, PhD, Jacques Himpens, MD Division of Bariatric Surgery, AZ St. Blasius, Dendermonde, Belgium
Insurer s Spin Defense to Bile Duct Transection
 Insurer s Spin Defense to Bile Duct Transection By: Thomas T. Dunbar All agree that a common bile duct transection arising from a gallbladder surgery can be a devastating injury, life-threatening, and
Insurer s Spin Defense to Bile Duct Transection By: Thomas T. Dunbar All agree that a common bile duct transection arising from a gallbladder surgery can be a devastating injury, life-threatening, and
Treatment Guide Pancreatic Disease CHOOSING YOUR CARE
 Treatment Guide Pancreatic Disease The pancreas is one of the body s great multi-taskers this dual-purpose organ is also a gland. Some people may not give much thought to the pancreas, especially those
Treatment Guide Pancreatic Disease The pancreas is one of the body s great multi-taskers this dual-purpose organ is also a gland. Some people may not give much thought to the pancreas, especially those
Hepatic resection (Removal of part of the liver)
") Hepatic resection (Removal of part of the liver) The liver is the largest solid organ in the body and is located in the upper right-quadrant of the abdomen under the rib cage. Functionally it is a major
Hepatic resection (Removal of part of the liver) The liver is the largest solid organ in the body and is located in the upper right-quadrant of the abdomen under the rib cage. Functionally it is a major
Informed Consent for Laparoscopic Vertical Sleeve Gastrectomy. Patient Name
 Informed Consent for Laparoscopic Vertical Sleeve Gastrectomy Patient Name Please read this form carefully and ask about anything you may not understand. I consent to have a laparoscopic Vertical Sleeve
Informed Consent for Laparoscopic Vertical Sleeve Gastrectomy Patient Name Please read this form carefully and ask about anything you may not understand. I consent to have a laparoscopic Vertical Sleeve
Demographics. MBSAQIP Case Number: IDN: ACS NSQIP Case Number:
 Demographics *LMRN: *DOB: / / *Gender: Male Female *Race: White Native Hawaiian/Other Pacific Islander Black or African American Asian American Indian or Alaska Native Unknown *Hispanic Ethnicity: Unknown
Demographics *LMRN: *DOB: / / *Gender: Male Female *Race: White Native Hawaiian/Other Pacific Islander Black or African American Asian American Indian or Alaska Native Unknown *Hispanic Ethnicity: Unknown
Understanding. Pancreatic Cancer
 Understanding Pancreatic Cancer Understanding Pancreatic Cancer The Pancreas The pancreas is an organ that is about 6 inches long. It s located deep in your belly between your stomach and backbone. Your
Understanding Pancreatic Cancer Understanding Pancreatic Cancer The Pancreas The pancreas is an organ that is about 6 inches long. It s located deep in your belly between your stomach and backbone. Your
COMPLICATIONS OF FISTULA REPAIR SURGERY. Sherif Mourad
 COMPLICATIONS OF FISTULA REPAIR SURGERY Sherif Mourad In the developing world, the true incidence of obstetric fistulas is unknown, as many patients with this condition suffer in silence and isolation.
COMPLICATIONS OF FISTULA REPAIR SURGERY Sherif Mourad In the developing world, the true incidence of obstetric fistulas is unknown, as many patients with this condition suffer in silence and isolation.