WMAS Clinical Guidelines CLN PRO 026 I Version - 4
|
|
|
- Juliet Hodges
- 9 years ago
- Views:
Transcription
1 WMAS Clinical Guidelines CLN PRO 026 I Version - 4 Guideline ID CLN PRO 026 Version Four Title WMAS Resuscitation Guidelines 2015 Approved by Clinical Steering Date Issued 4 May 2016 Review Date May 2019 Directorate Clinical and Quality Emergency Care Assistant X Student Paramedic X Technician X Critical Care Paramedic X Authorised Staff Advanced Technician X Nurse X Paramedic X Doctor X Specialist Paramedic - Urgent Care X Clinical Category Green Deviation permissible for registered healthcare professionals with application of clinical judgement 1 Scope 1.1 These guidelines are written to support clinicians management of patients requiring resuscitation from West Midlands Ambulance Service NHS Foundation Trust responders. 2 Background 2.1 The information contained within these clinical guidelines are provided to support clinicians utilising the UK Resuscitation Council Guidelines 2015 and provides information regarding the localisation of the guidelines for the West Midlands in order to provide a coordinated and seamless response.

2 3 Guidelines 3.1 Preventing Cardiac Arrest In many cases the ambulance service is only called following a patient s collapse, thus the first contact with many cardiac arrest patients is after the arrest has occurred. However, some patients may suffer a cardiac arrest in the presence of the ambulance crew. Therefore staff must be vigilant for clinical signs of deterioration and be aware of the measures to be taken to reduce the likelihood of cardiac arrest. The commonest clinical abnormalities witnessed before cardiac arrest are breathing problems, an increase in heart rate and fall in cardiac output. This may manifest itself as hypotension, confusion, restlessness, lethargy or a falling level of consciousness. Breathing difficulties are suggested by shortness of breath, an increase in respiratory rate, and a fall in oxygen saturation (SpO2). A fall in cardiac output should be suspected if the patient is cold, pale, clammy or cyanosed, or if their pulse is weak or impalpable. Any deterioration in mental status is usually secondary to inadequate cerebral perfusion as a result of diminished cardiac output. Wherever possible ambulance staff should initiate supportive treatment, for example oxygen therapy for those patients who are hypoxic, and, if indicated, administer treatments to correct the underlying cause, for example thrombolysis for AMI or nitrates and diuretics for acute cardiogenic pulmonary oedema. Prompt access to expert medical support and appropriate facilities such as those available in the emergency department, intensive care unit, high dependency unit or coronary care unit, is likely to decrease overall mortality, therefore ambulance staff must be conscious of minimising on scene delays so as to expedite transfer to definitive care Every emergency ambulance and response care is equipped to enable clinicians to deliver advance life support In so far as is possible, equipment is standardised across the trust. Ambulance staff are responsible for checking the resuscitation equipment on their ambulance or response car and thus ensuring that they are able to deliver advanced life support where needed In the case of a vehicle or response bag being pre-checked and tagged by ambulance fleet assistants the lead clinician is responsible for checking the intact tag and date of the green first response bag and red ALS bag and check the defibrillator

3 3.2.4 The minimum equipment required to attempt resuscitation is as follows: Suction unit Airway adjuncts Bag valve mask (BVM) Monitor with defibrillator This may be supplemented with additional equipment/procedures dependent on the skill level of the clinician or availability of the equipment: Supraglottic airway insertion Endotracheal intubation Mechanical ventilation Intravenous/intraosseous access (EZ-IO) Advanced life support medications A device for monitoring End Tidal CO2 Mechanical chest compression device The continued availability of resuscitation equipment for each station is managed through the Distribution Centre, stations have minimum list of consumable equipment and where they reach this more equipment is urgently ordered by the Operational Manager from the Distribution Centre The availability of resuscitation equipment on each Emergency Ambulance or Rapid Response Vehicle is the responsibility of the Area Manager and is delegated to the Ambulance Fleet Assistant. If the deployment site for the vehicle is not a make ready site then the senior clinician is responsible for that vehicle and all equipment should be checked and replenished from the station stores, where this is not possible or where the minimum/essential equipment is found to be defective this should be reported immediately to the Emergency Operations Centre to remove the vehicle from operational response until the vehicle has the minimum resuscitation equipment (see 3.2.4) Basic life support (BLS) is the foundation of resuscitation and must be expertly delivered to improve outcomes and should be performed in line with UK Resuscitation Council BLS Guidelines. It is important to note however that the UK Resuscitation Council BLS guidelines are generally written for laypersons and that healthcare professionals are expected to perform some additional assessments.

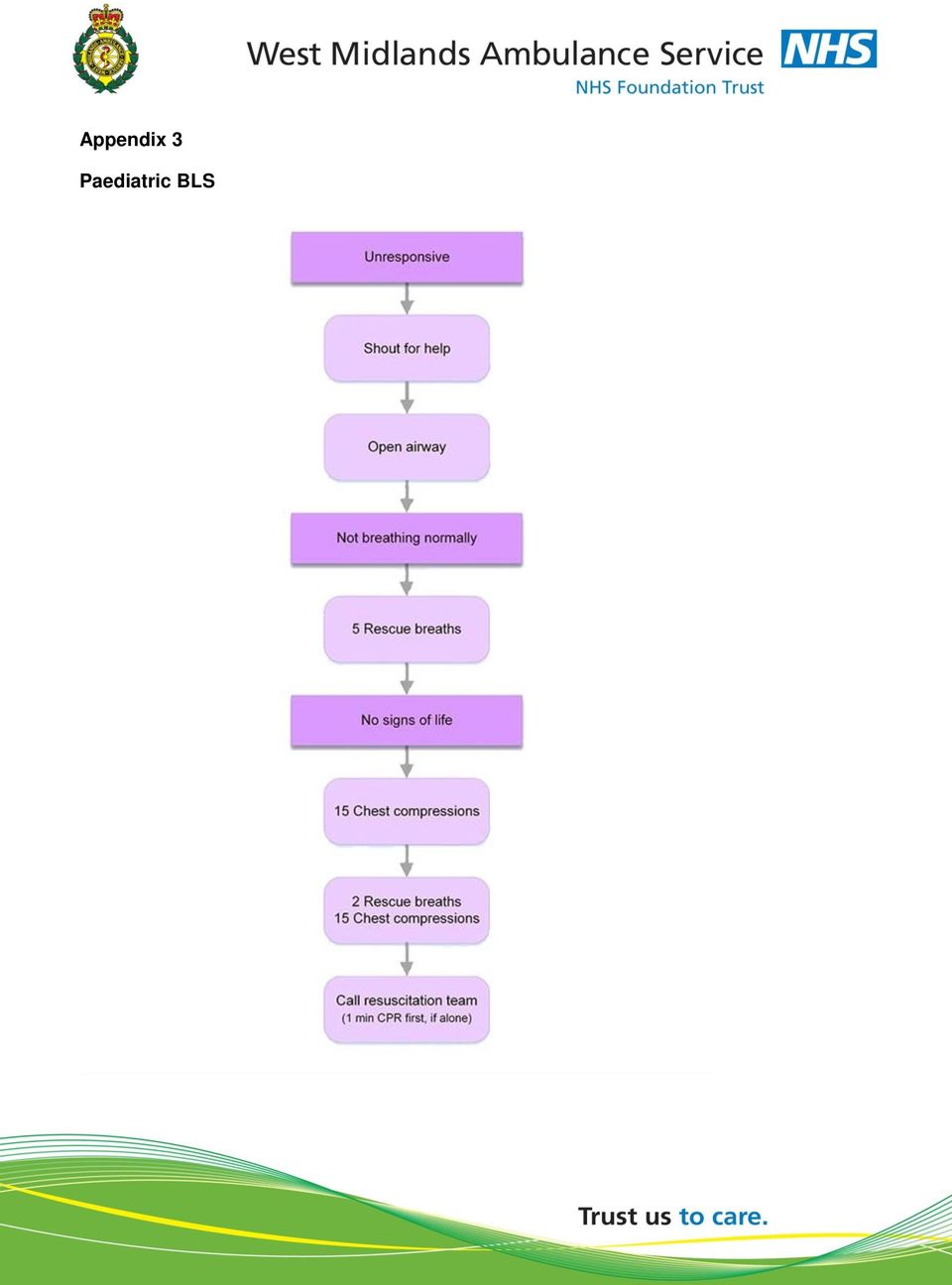
4 3.3.2 Provided the environment and surroundings are safe, BLS for healthcare professionals commences with an assessment of level of consciousness on the AVPU scale. A patient who does not respond to the clinician s arrival at their side is not alert. The clinician must then assess for responsiveness to voice and pain, however these must not occur simultaneously, but rather in succession starting with response to voice and proceeding to pain. A patient who does not respond to voice or pain stimuli is unresponsive If the patient is deemed to be unresponsive, then assessment of the airway is the next priority. Clinicians should quickly assess the facial bones before opening the mouth for visual inspection. Obstructions e.g. vomit should be removed under direct vision and the head positioned with the head-tilt-chin-lift manoeuver provided there is no suspicion of cervical spine injury. Where spinal injury is suspected the head-tilt-chin-lift manoeuvre should be avoided if at all possible, and a jaw thrust manoeuvre used in preference. An appropriate airway adjunct should be inserted The next stage includes assessment of not just breathing but also signs of life. The presence of breathing does not rule out the possibility of cardiac arrest. Agonal respirations immediately before and shortly after cardiac arrest are common. Patients with a regular breathing pattern are unlikely to be in cardiac arrest, and if they are in cardiac arrest they will not retain this pattern for long. In addition to assessing breathing, ambulance clinicians should also seek other signs of life including checking for pulses, looking for movement of limbs, listening for gagging sounds or noting low level reflexes such as blinking or coughing. Patients with abnormal breathing and absent signs of life are deemed to be in cardiac arrest If the ambulance clinician is a solo responder: Ensure further assistance is en route Attach the defibrillator and if the rhythm is shockable; Press charge on the monitor Recommence CPR Safety checks should occur whilst the defibrillator is charging Once the defibrillator is charged advise any bystanders to stand clear and deliver the shock to the patient Immediately recommence CPR do not undertake pulse checks or rhythm analysis If the rhythm is non shock able continue CPR immediately

5 If part of an ambulance crew: One member immediately commences CPR whilst the other crew member attaches the defibrillator pads As soon as a reliable ECG rhythm is seen CPR should stop to allow analysis to occur If a shock is indicated CPR must continue whilst the defibrillator is charging; safety checks should occur in tandem whilst the defibrillator is charging Once the defibrillator is charged advise any bystanders to stand clear and deliver the shock to the patient Immediately recommence CPR do not undertake pulse checks or rhythm analysis. For patients under 12 years of age: ALL shocks to be delivered at 4J per kg, regardless of type or manufacturer of defibrillator Compression to Ventilation Ratios and Compression Depth Age Group New Born* Infant/Child Between new born and puberty First Action Dry and Stimulate 5 Inflation Breaths 5 Rescue Breaths Ratio Compressions: Ventilations Rate Compressions per minute 3: : Depth At least 1/3 of the depth of the chest At least 1/3 of the depth of the chest Adult 30 Compressions 30: cm *New born babies are defined as patients during the transition from birth to successfully breathing once separated from the placenta.

6 3.4 Defibrillation All emergency and urgent ambulance clinicians and primary responders must be trained and equipped to provide defibrillation where indicated. Defibrillation is the delivery of electrical current to the myocardium in order to depolarise a critical mass of myocardial cells, to terminate ventricular fibrillation (VF) or pulseless ventricular tachycardia (VT). Ventricular fibrillation is a life threatening arrhythmia characterised by electrical and mechanical chaos. Pulseless ventricular tachycardia is characterised by organised electrical activity without palpable cardiac output. Both arrhythmias are most commonly associated with cardiac disease but may also occur due to electrolyte or acid base disturbance, drug toxicity and electrocution. The only effective treatment for VF or pulseless VT is defibrillation WMAS NHS Trust uses a number of defibrillators across Automated External Defibrillators (AEDs) Cardiac Science Zoll AED Pro Manual Defibrillators Zoll M-series (biphasic) Zoll E-series (biphasic) Zoll X-series (biphasic) Lifepak 15 (biphasic) Automated External Defibrillators (AEDs) Automated External Defibrillators (AEDs) are deployed throughout the trust in its buildings and are used by certain individuals who respond on behalf of the service e.g. Community First Responders. All AED s used throughout the trust are biphasic and the energy settings are programmed into the AED s. Clinicians will not be able to adjust the energy settings on AEDs, however they may override the embedded ECG analysis software and decide for themselves whether or not shocks are indicated. No formal training is required for these devices although an awareness where a single device is used is supported during training.

7 The UK Resuscitation Council indicates that: AEDs should not be used on patients under 1 year of age. Paediatric attenuated pads SHOULD be used for patients aged 1 to 8 years of age. Adult pads may only be used in this age range if paediatric attenuated pads are not available. Adult pads should be used for all patients over 8 years of age. If ambulance clinicians are responded to a cardiac arrest where an AED is in use then: In cases of paediatric cardiac arrest, the AED must be replaced with a manual defibrillator as soon as one is available, this will allow the clinician to set an age/weight appropriate energy setting for defibrillation. In cases of adult cardiac arrest, it is advisable to replace any AED with a manual defibrillator as soon as it is practicable. This ensures that the clinician can obtain an accurate reading of the ECG and can print copies of the ECG if required. Where an AED is in use by a trained responder that does not have a screen to display the underlying rhythm, then the AED should be replaced with a WMAS manual defibrillator as soon as it is practicable. Replacement of the AED with a WMAS defibrillator allows the ambulance clinician to view and print the ECG Manual Defibrillators WMAS NHS Trust primarily uses Zoll manual defibrillators. All recently acquired defibrillators are biphasic in nature; however crews may encounter a limited number of legacy defibrillators that are monophasic. The energy setting for shocks can vary between type of defibrillator (monophasic vs. biphasic) and manufacturer (Zoll vs. Physio control). Below describes the energy settings used by the different manual defibrillators: For adult patients (12 years of age and over): If a monophasic defibrillator is used, then all shocks should be delivered at 360J. If a Zoll biphasic defibrillator is used then an escalating energy shock sequence is used. The first shock is delivered at 120J, the second at 150J and all subsequent shocks delivered at 200J.

8 If a manual biphasic defibrillator is not manufactured by Zoll then the first shock should be delivered at 150J, with all subsequent shocks being delivered at 200J. For patients under 12 years of age: ALL shocks delivered at 4J per kg regardless of type of defibrillator or manufacturer. WMAS NHS Trust primarily uses Zoll manual defibrillators. All recently acquired defibrillators are biphasic in nature; however crews may encounter a limited number of legacy defibrillators that are monophasic. The energy setting for shocks can vary between type of defibrillator (monophasic vs. biphasic) and manufacturer (Zoll vs. Physio control). Below describes the energy settings used by the different manual defibrillators: For adult patients (12 years of age and over): If a monophasic defibrillator is used, then all shocks should be delivered at 360J. If a Zoll biphasic defibrillator is used then an escalating energy shock sequence is used. The first shock is delivered at 120J, the second at 150J and all subsequent shocks delivered at 200J. If a manual biphasic defibrillator is not manufactured by Zoll then the first shock should be delivered at 150J, with all subsequent shocks being delivered at 200J. For patients under 12 years of age: ALL shocks delivered at 4J per kg regardless of type of defibrillator or manufacturer Defibrillation: Safety Issues Wherever possible, safety issues should be addressed and appropriate plans made while chest compressions are being performed, before a shock is considered. Prior to delivering a shock: Ensure no one is touching the patient either directly or indirectly. Ensure the electrodes are firmly adhered to the patient s chest and only make contact with skin. Ensure the chest is not wet. Ensure high flow O2 is not in the zone of defibrillation (Bag valve mask respirators should be moved at least 1 meter from the patient). Ensure defibrillator pads are not placed over any pacemaker. Remove any medication patches (especially GTN) from the patient. Remove any jewellery in proximity to the defibrillator pads
 and manufacturer (Zoll vs. Physio control).")
9 3.4.6 In general, the likelihood of successful defibrillation decreases by 7-10% per minute from the time of arrest. Consequently, the timely delivery of defibrillation shocks is essential improve outcomes If the patient is being monitored through defibrillation pads and subsequently arrests in front of the ambulance clinician, then defibrillation should be attempted immediately (if indicated) before CPR commences. If the patient is not being monitored through defibrillation pads and subsequently arrests in front of the ambulance clinician, then a precordial thump should be attempted. While CPR is in progress, defibrillation should be attempted every 2 minutes if indicated. It is critical to minimise the delay between stopping chest compressions and delivering the shock. Where a shock is indicated ambulance clinicians should aim to deliver the shock within 10 seconds of stopping CPR as every 5 second delay reduces the likelihood of successful defibrillation by approximately 50%. If there are delays caused by difficulties in rhythm analysis or if individuals are still in contact with the patient, chest compressions should be restarted whilst plans are made to decide what to do when compressions are next stopped. Chest compressions should be resumed immediately following the delivery of a shock do not wait to see if the rhythm has changed or assess for the presence of a pulse. Resume CPR immediately. Pulse checks should only be undertaken when a previously lifeless patient shows signs of life, e.g. movement, or if coordinated electrical activity is noted on the monitor or in the case of sudden improvement of End Tidal Capnograph readings Pulse checks should only be undertaken when a previously lifeless patient shows signs of life, e.g. movement, or if coordinated electrical activity is noted on the monitor or in the case of sudden improvement of End Tidal Capnograph readings 3.5 Advanced Life Support (ALS) Advanced Life Support (ALS) involves advanced airway management where indicated, and the delivery of resuscitation medications to supplement BLS and defibrillation. Research indicates that ALS does not significantly improve outcomes. The only interventions shown to improve outcomes in cardiac arrest are BLS, oxygen therapy and defibrillation. Consequently ALS must never be initiated at the expense of either BLS or defibrillation; ALS must always be deferred to ensure quality BLS and timely defibrillation.

10 3.5.2 ALS requires a minimum of two providers, one to deliver BLS and another to deliver the various elements of ALS for this reason it is not normally possible for a solo responder to deliver ALS. Where resources allow, ALS should occur in parallel with BLS, but should not interrupt BLS in any way. In particular, BLS must not be interrupted to perform cannulation, intubation or drug delivery. Refer to the UK Clinical Practice Guidelines and UK Resuscitation Council ALS guidelines for further detail regarding the delivery of advanced life support (ALS). 3.6 Reversible Causes Hypoxia Hypovolaemia Hypothermia/Hyperthermia Hypo-/hyperkalaemia/metabolic Tension pneumothorax Toxins Tamponade Cardiac Thrombosis Coronary or pulmonary Advance Directives / Living Wills An Advance Directive is produced by a patient and identifies what treatment a patient is willing to receive in the future should they lack capacity at that time; they may be written by an individual with capacity and in whom a resuscitation attempt may have a good chance of success. It is well established both in law and in ethics that adults with capacity have the right to refuse any medical treatment, even if that refusal results in their death. Consequently, for an Advance Directive to be valid, the patient must have capacity at the time the advance directive is produced. Any Advance Directive produced where capacity is lacking is not legally binding. Advance Directives usually relate to specific treatments such as: Intubation Mechanical ventilation External chest compressions Defibrillation Administration of certain drugs (usually resuscitation drugs) Administration of food substitutes It is important to note that these treatment restrictions apply to all health care related issues i.e. the same restrictions apply regardless of whether or not the patient chokes on a piece of food, suffers a heart attack, is poisoned or is injured in a road traffic accident. In England and Wales, the Mental Capacity Act 2005 provides the legal framework for Advance Directives. The Act confirms that an advance decision refusing resuscitation will be valid, and therefore legally binding on the healthcare team, provided that: The patient was 18 years old or over and had autonomy, capacity and competency when the decision was made

11 The decision is in writing, signed and witnessed It includes a statement that the Advance Decision is to apply even if the patient s life is at risk The Advance Decision has not been withdrawn The patient has not, since the Advance Decision was made, appointed a welfare attorney to make decisions about CPR on their behalf The patient has not done anything clearly inconsistent with its terms The circumstances that have arisen match those envisaged in the Advance Decision. If an Advance Decision does not meet these criteria but appears to set out a clear indication of the patient s wishes, it will not be legally binding but should be taken into consideration in determining the patient s best interests. Although a valid Advance Directive must be respected, it is incumbent upon the patient to ensure that the Advance Directive is communicated to the treating health care professionals. In an emergency, if there is no time to investigate further and confirm that the patient has made a prior and specific request to refuse treatment, the presumption should be in favour of resuscitation if this has a realistic chance of prolonging life and staff should continue to provide all clinical care in the normal way, until such time as evidence is produced. If a WMAS clinician determines that the Advance Directive does not fulfill the criteria listed in then the reasons why it is considered invalid or not applicable must be documented Do Not Attempt Cardiopulmonary Resuscitation (DNACPR) When a patient is in the final stages of an incurable illness and death is expected within a few days, CPR is very unlikely to be clinically successful. In some cases it may prolong or increase suffering and subject the patient to traumatic and undignified death. In these circumstances, most patients want a natural death without unnecessary interventions that most consider to be undignified. Ambulance clinicians thus have an ethical and moral obligation to ensure that the patient s best interests are being served Do Not Attempt Cardiopulmonary Resuscitation (DNACPR) is usually produced by the senior clinician in charge of a patient s medical care; however this task may be delegated to another competent clinician. There is no legal requirement for the DNACPR to be communicated to either the patient or their relatives however it is considered good practice, that wherever possible the patient, and if need be their family, are involved in the decision making process. It is important to note that patient capacity is not a prerequisite for a DNACPR to be valid.

12 There are no legal requirements concerning DNACPR, only good practice recommendations. As such the presentation of DNACPR varies considerably; there is no uniform template. Ideally a DNACPR should: Explicitly identify the patient Explicitly identify the circumstances in which the DNACPR applies Identify if the patient and their family are aware of the DNACPR Identify who produced the DNACPR Identify when the DNACPR was produced A DNACPR decision applies solely to cardiopulmonary resuscitation. All other treatment and care that a patient requires is not precluded or influenced by a DNACPR decision e.g. provision of analgesia. Where a DNACPR is in place, a patient or their family cannot demand that health care professionals provide resuscitation health care professionals do however have an ethical, moral and professional responsibility to clinically justify withholding resuscitation. 3.8 Relatives witnessing resuscitation attempts There is an increasing appreciation of the desire of close relatives to be present at resuscitation attempts. It is now agreed that such presence can reassure relatives that all necessary therapeutic steps were taken and can aid the process of bereavement. This practice has been routine for many years in paediatric medicine and is now relatively common in Emergency Departments around the country. Ambulance Clinicians should consider these facts when undertaking resuscitation in the presence of family members Relatives who wish to remain with the patient during resuscitation attempts should be allowed to do so unless their presence interferes with the resuscitation attempt. No relative should feel under any pressure to be present during CPR, and should be allowed to leave the vicinity of the resuscitation attempt if they so wish. Where resources allow (i.e. at least 4 ambulance staff are in attendance), it is best practice to appoint a single member of the resuscitation team to look after the relative and answer any questions that the relative may have. Reasonable efforts should be made to accommodate relatives requests; however clinical needs of the patient must take priority. The presence of relatives should be allowed provided that:

13 There is no reason to believe that the patient has already refused permission for relatives to be present if they require resuscitation. There is sufficient space to accommodate the presence of the relative without impact on the resuscitation effort. The presence of a relative will not compromise the potential success of the resuscitation attempt e.g. by asking questions that distract the clinicians or interfering with resuscitation attempts. No member of the resuscitation team objects to the presence of the relative. (If a member of the team does object, they must provide adequate justification as to why the relatives presence will compromise the resuscitation attempt before the relative is excluded) The relative must be informed that if at any time during the resuscitation attempt it is believed that their continued presence compromises the best interest of the patient then they will be politely asked to leave. If relatives are prohibited from witnessing a resuscitation attempt for any of the preceding reasons then the team leader of the resuscitation should always confer with the relative afterwards, answering any questions they may have If the resuscitation attempt is successful, the surviving patient should be informed that their relative was present during the resuscitation attempt. 3.9 Outcome of Cardiac Arrest Recognition of Life Extinct Refer to Recognition of Life Extinct procedure Return of Spontaneous Circulation (ROSC) Refer to Return of Spontaneous Circulation (ROSC) procedure (appendix 8) Ongoing resuscitation attempt continued into hospital Resuscitation consistent with indicated guideline should continue. Continuous consideration of the safety of patient and rescuers and continue to dynamically assess and adapt to any risks that are identified. Pre-alert hospital to ensure that the hospital resuscitation team is on standby Following ROSC the patient should continue to be assessed as per Patients that fit following ROSC can be due to reperfusion episodes, patients should only receive diazepam after 5 minutes of continuous fitting. The method for the movement of a patient immediately following ROSC should be carefully considered. The myocardium has a level of dysfunction following cardiac arrest which leaves the heart susceptible to further arrhythmia and reduced cardiac output which can lead to subsequent cardiac arrest if not handled appropriately.

14 3.10 Ambulance Quality Indicators (AQIs) Requirements The current national Ambulance Quality Indicators (AQIs) require Ambulance Trusts to report the following outcomes: ROSC at time of arrival at hospital Overall ROSC at time of arrival at hospital - Utstein Comparator Group Survival to discharge Overall survival rate Survival to discharge Utstein Comparator Group survival rate These are then compared against each other to identify achievement against the standard References Resus.org.uk, (2016). Resuscitation guidelines. [online] Available at: [Accessed 9 Feb. 2016]. Mental Capacity Act 2005 (c.9) London. OPSI
. Resuscitation guidelines. [online] Available at: https://www.resus.org.uk/resuscitation-guidelines/ [Accessed 9 Feb. 2016].")
15 Appendix 1 Adult BLS and AED

16 Appendix 2 Adult Choking Algorithm

17 Appendix 3 Paediatric BLS
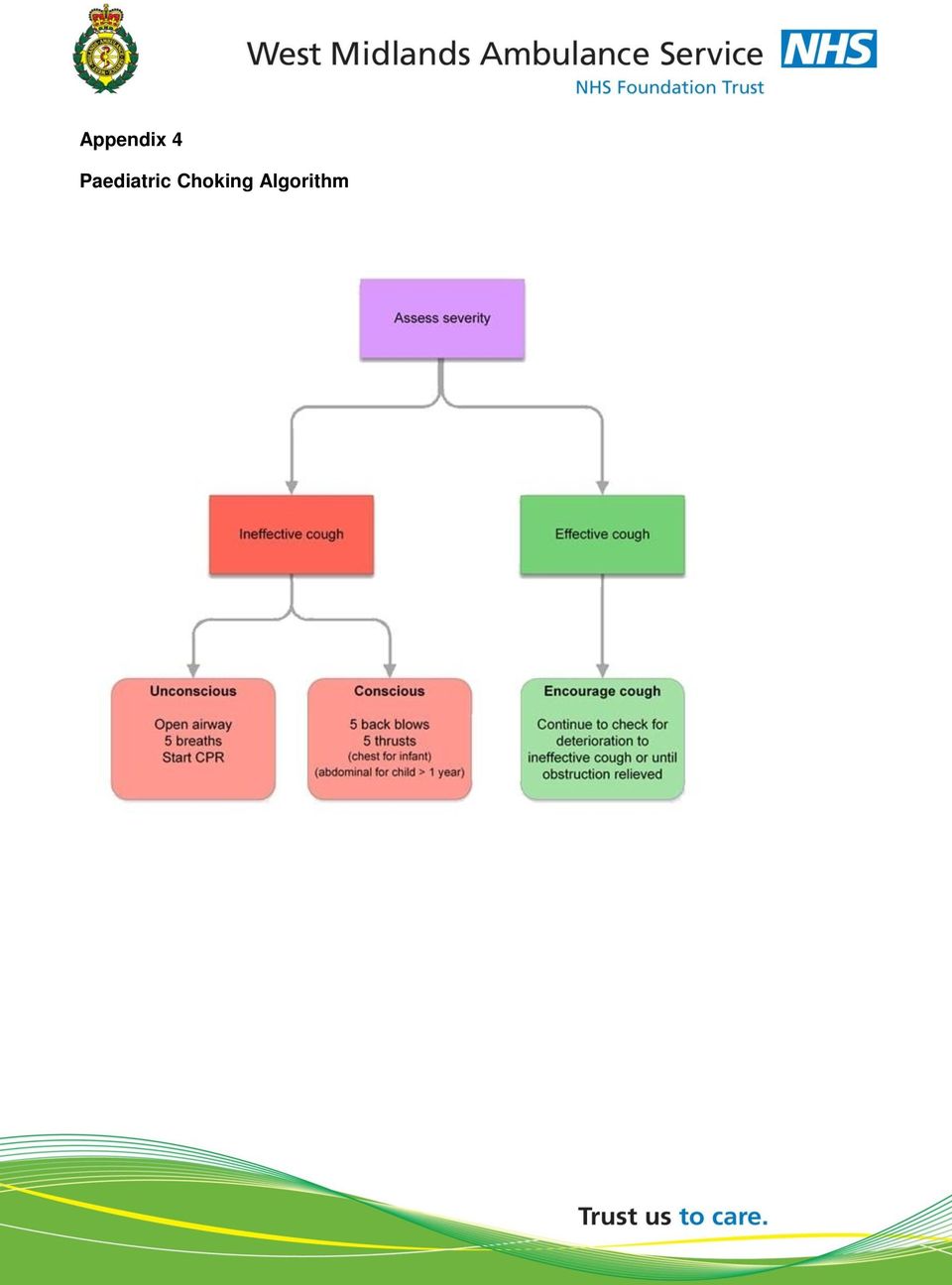
18 Appendix 4 Paediatric Choking Algorithm
19 Appendix 5 Adult ALS Algorithm (Medical)

20 Appendix 6 Adult ALS Algorithm (Trauma)

21 Appendix 7 Paediatric Advanced Life Support
22 Appendix 8 ROSC Procedure This procedure is to be undertaken following any case of Return of Spontaneous Circulation: Haemorrhage Control Continue to monitor effectiveness of haemorrhage control Airway Assess and manage using a stepwise approach Suction as required Breathing Monitor respiratory rate and maintain SPO2 at 95-98% Ventilation if required should undertaking using 10-15litres of O2 If available monitor ETCO2 and maintain at 3-5Kpa (Capnography) Circulation Undertake 12 Lead ECG If diagnostic of a STEMI discuss direct transfer with PPCI Centre Assess BP and remove patient keeping them as flat as possible Aim for mmhg. (250ml boluses of fluids) Treat Symptomatic Bradycardia Disability Assess and record AVPU Do not actively re-warm patients that are unresponsive to pain Undertake a BM and treat hypoglycaemia In a combative patient consider Hypoxaemia and Hypoglycaemia in the first instance Secondly consider Rapid Sequence Induction (RSI) Evacuate Optimise cerebral perfusion utilise SUPINE position, FEET FIRST when down a stairs Consider head end of body raised 30 degrees (return to flat if further arrest occurs) Continue ABCDE on route to hospital. Provide a pre-alert message and convey to the appropriate centre of care Constantly monitor and treat any reversible cause: Hypoxia Tension pneumothorax Hypovolaemia Tamponade (Cardiac) Hypothermia Toxins Hypo/Hyperkalaemia/BM Thromboembolic
23 Date Change Authorised by Jan 2010 DRAFT Mike Smyth Medical Director Feb 2010 Reviewed and Amended - Matthew Ward Medical Director May 2010 Amended following external review Director of Nursing June 10 Approved Staff Side Policy Group July 10 Approved Clinical Governance Committee Nov 10 March 12 Amended following 2010 Resus Guidelines Reviewed by Head of Cardiac and Stroke Management Medical Director Medical Director July 13 Reviewed by Head of Cardiac and Stroke Management Medical Director Dec 13 Reviewed by Head of Clinical Practice, Research Paramedic and CPGM Medical Director 28 Jan 14 Approved by Clinical Steering Group Medical Director 04 May 2016 Approved Clinical Steering Group
ACLS Provider Manual Comparison Sheet Based on 2010 AHA Guidelines for CPR and ECC. BLS Changes
 ACLS Provider Manual Comparison Sheet Based on 2010 AHA Guidelines for CPR and ECC CPR Chest compressions, Airway, Breathing (C-A-B) BLS Changes New Old Rationale New science indicates the following order:
ACLS Provider Manual Comparison Sheet Based on 2010 AHA Guidelines for CPR and ECC CPR Chest compressions, Airway, Breathing (C-A-B) BLS Changes New Old Rationale New science indicates the following order:
Michigan Adult Cardiac Protocols CARDIAC ARREST GENERAL. Date: May 31, 2012 Page 1 of 5
 Date: May 31, 2012 Page 1 of 5 Cardiac Arrest General This protocol should be followed for all adult cardiac arrests. Medical cardiac arrest patients undergoing attempted resuscitation should not be transported
Date: May 31, 2012 Page 1 of 5 Cardiac Arrest General This protocol should be followed for all adult cardiac arrests. Medical cardiac arrest patients undergoing attempted resuscitation should not be transported
In-hospital resuscitation. Superseded by
 6 In-hospital resuscitation Introduction These guidelines are aimed primarily at healthcare professionals who are first to respond to an in-hospital cardiac arrest and may also be applicable to healthcare
6 In-hospital resuscitation Introduction These guidelines are aimed primarily at healthcare professionals who are first to respond to an in-hospital cardiac arrest and may also be applicable to healthcare
American Heart Association
 American Heart Association Basic Life Support for Healthcare Providers Pretest April 2006 This examination to be used only as a PRECOURSE TEST For BLS for Healthcare Providers Courses 2006 American Heart
American Heart Association Basic Life Support for Healthcare Providers Pretest April 2006 This examination to be used only as a PRECOURSE TEST For BLS for Healthcare Providers Courses 2006 American Heart
Question-and-Answer Document 2010 AHA Guidelines for CPR & ECC As of October 18, 2010
 Question-and-Answer Document 2010 AHA Guidelines for CPR & ECC As of October 18, 2010 Q: What are the most significant changes in the 2010 AHA Guidelines for CPR & ECC? A: Major changes for all rescuers,
Question-and-Answer Document 2010 AHA Guidelines for CPR & ECC As of October 18, 2010 Q: What are the most significant changes in the 2010 AHA Guidelines for CPR & ECC? A: Major changes for all rescuers,
CPR/AED for Professional Rescuers and Health Care Providers HANDBOOK
 CPR/AED for Professional Rescuers and Health Care Providers HANDBOOK TABLE OF CONTENTS SECTION 1: THE PROFESSIONAL RESCUER The Duty to Respond 2 Preventing the Spread of Bloodborne Pathogens 3 Taking Action
CPR/AED for Professional Rescuers and Health Care Providers HANDBOOK TABLE OF CONTENTS SECTION 1: THE PROFESSIONAL RESCUER The Duty to Respond 2 Preventing the Spread of Bloodborne Pathogens 3 Taking Action
Cardiac Arrest Pediatric Ventricular Fibrillation / Pulseless Ventricular Tachycardia Protocol revised October 2008
 Cardiac Arrest Pediatric Ventricular Fibrillation / Pulseless Ventricular Tachycardia Protocol revised October 2008 Preamble In contrast to cardiac arrest in adults, cardiopulmonary arrest in pediatric
Cardiac Arrest Pediatric Ventricular Fibrillation / Pulseless Ventricular Tachycardia Protocol revised October 2008 Preamble In contrast to cardiac arrest in adults, cardiopulmonary arrest in pediatric
ACLS Study Guide BLS Overview CAB
 ACLS Study Guide The ACLS Provider exam is 50-mutiple choice questions. Passing score is 84%. Student may miss 8 questions. For students taking ACLS for the first time or renewing students with a current
ACLS Study Guide The ACLS Provider exam is 50-mutiple choice questions. Passing score is 84%. Student may miss 8 questions. For students taking ACLS for the first time or renewing students with a current
Update on Small Animal Cardiopulmonary Resuscitation (CPR)- is anything new?
- is anything new?") Update on Small Animal Cardiopulmonary Resuscitation (CPR)- is anything new? DVM, DACVA Objective: Update on the new Small animal guidelines for CPR and a discussion of the 2012 Reassessment Campaign on
Update on Small Animal Cardiopulmonary Resuscitation (CPR)- is anything new? DVM, DACVA Objective: Update on the new Small animal guidelines for CPR and a discussion of the 2012 Reassessment Campaign on
It is recommended that the reader review each medical directive presented in this presentation along with the actual PCP Core medical directive.
 It is recommended that the reader review each medical directive presented in this presentation along with the actual PCP Core medical directive. This presentation will highlight the changes and any new
It is recommended that the reader review each medical directive presented in this presentation along with the actual PCP Core medical directive. This presentation will highlight the changes and any new
Oxygen - update April 2009 OXG
 PRESENTATION Oxygen (O 2 ) is a gas provided in compressed form in a cylinder. It is also available in liquid form, in a system adapted for ambulance use. It is fed via a regulator and flow meter to the
PRESENTATION Oxygen (O 2 ) is a gas provided in compressed form in a cylinder. It is also available in liquid form, in a system adapted for ambulance use. It is fed via a regulator and flow meter to the
Cardiac Arrest - Ventricular Fibrillation / Pulseless Ventricular Tachycardia Protocol revised October 2008
 Cardiac Arrest - Ventricular Fibrillation / Pulseless Ventricular Tachycardia Protocol revised October 2008 Preamble Survival from cardiorespiratory arrest for patients who present with ventricular fibrillation
Cardiac Arrest - Ventricular Fibrillation / Pulseless Ventricular Tachycardia Protocol revised October 2008 Preamble Survival from cardiorespiratory arrest for patients who present with ventricular fibrillation
Adult, Child, and Infant Written Exam CPR Pro for the Professional Rescuer
 Adult, Child, and Infant Written Exam CPR Pro for the Professional Rescuer Instructions: Read each of the following questions carefully and then place an X over the correct answer on the separate answer
Adult, Child, and Infant Written Exam CPR Pro for the Professional Rescuer Instructions: Read each of the following questions carefully and then place an X over the correct answer on the separate answer
The American Heart Association released new resuscitation science and treatment guidelines on October 19, 2010.
 ACLS Study Guide The American Heart Association released new resuscitation science and treatment guidelines on October 19, 2010. Please read the below information carefully This letter is to confirm your
ACLS Study Guide The American Heart Association released new resuscitation science and treatment guidelines on October 19, 2010. Please read the below information carefully This letter is to confirm your
Northwestern Health Sciences University. Basic Life Support for Healthcare Providers
 Northwestern Health Sciences University Basic Life Support for Healthcare Providers Pretest May 2005 This examination to be used only as a PRECOURSE TEST for BLS for Healthcare Providers Courses Based
Northwestern Health Sciences University Basic Life Support for Healthcare Providers Pretest May 2005 This examination to be used only as a PRECOURSE TEST for BLS for Healthcare Providers Courses Based
Oxygen Therapy. Oxygen therapy quick guide V3 July 2012.
 PRESENTATION Oxygen (O 2 ) is a gas provided in a compressed form in a cylinder. It is also available in a liquid form. It is fed via a regulator and flow meter to the patient by means of plastic tubing
PRESENTATION Oxygen (O 2 ) is a gas provided in a compressed form in a cylinder. It is also available in a liquid form. It is fed via a regulator and flow meter to the patient by means of plastic tubing
Purpose To guide registered nurses who may manage clients experiencing sudden or unexpected life-threatening cardiac emergencies.
 Emergency Cardiac Care: Decision Support Tool #1 RN-Initiated Emergency Cardiac Care Without Cardiac Monitoring/Manual Defibrillator or Emergency Cardiac Drugs Decision support tools are evidence-based
Emergency Cardiac Care: Decision Support Tool #1 RN-Initiated Emergency Cardiac Care Without Cardiac Monitoring/Manual Defibrillator or Emergency Cardiac Drugs Decision support tools are evidence-based
BASIC LIFE SUPPORT - ADULT
 BASIC LIFE SUPPORT - ADULT First Issued by/date BKW PCT May 2003 Issue Version Purpose of Issue/Description of Change 3 Policy reviewed. No changes in procedure or legislation since policy revised 12 months
BASIC LIFE SUPPORT - ADULT First Issued by/date BKW PCT May 2003 Issue Version Purpose of Issue/Description of Change 3 Policy reviewed. No changes in procedure or legislation since policy revised 12 months
National Registry of Emergency Medical Technicians Emergency Medical Responder Psychomotor Examination PATIENT ASSESSMENT/MANAGEMENT TRAUMA
 PATIENT ASSESSMENT/MANAGEMENT TRAUMA Scenario # Note: Areas denoted by ** may be integrated within sequence of Primary Survey/Resuscitation SCENE SIZE-UP Determines the mechanism of injury/nature of illness
PATIENT ASSESSMENT/MANAGEMENT TRAUMA Scenario # Note: Areas denoted by ** may be integrated within sequence of Primary Survey/Resuscitation SCENE SIZE-UP Determines the mechanism of injury/nature of illness
CHAPTER 2 APPROACH TO THE INCIDENT
 CHAPTER 2 APPROACH TO THE INCIDENT Reassuring the casualty is very important in first aid and the best reassurance for both casualty and bystanders is a confident first aider taking decisive action. In
CHAPTER 2 APPROACH TO THE INCIDENT Reassuring the casualty is very important in first aid and the best reassurance for both casualty and bystanders is a confident first aider taking decisive action. In
Official Online ACLS Exam
 \ Official Online ACLS Exam Please fill out this form before you take the exam. Name : Email : Phone : 1. Hypovolemia initially produces which arrhythmia? A. PEA B. Sinus tachycardia C. Symptomatic bradyarrhythmia
\ Official Online ACLS Exam Please fill out this form before you take the exam. Name : Email : Phone : 1. Hypovolemia initially produces which arrhythmia? A. PEA B. Sinus tachycardia C. Symptomatic bradyarrhythmia
Procedure 17: Cardiopulmonary Resuscitation
 Cardiopulmonary Resuscitation 349 Procedure 17: Cardiopulmonary Resuscitation Introduction Cardiopulmonary arrest (CPA) occurs when a patient s heart and lungs stop functioning. In children, CPA usually
Cardiopulmonary Resuscitation 349 Procedure 17: Cardiopulmonary Resuscitation Introduction Cardiopulmonary arrest (CPA) occurs when a patient s heart and lungs stop functioning. In children, CPA usually
American Heart Association. Basic Life Support for Healthcare Providers
 American Heart Association Basic Life Support for Healthcare Providers Pretest February 2001 This examination to be used only as a PRECOURSE TEST for BLS for Healthcare Providers Courses 2001 American
American Heart Association Basic Life Support for Healthcare Providers Pretest February 2001 This examination to be used only as a PRECOURSE TEST for BLS for Healthcare Providers Courses 2001 American
404 Section 5 Shock and Resuscitation. Scene Size-up. Primary Assessment. History Taking
 404 Section 5 and Resuscitation Scene Size-up Scene Safety Mechanism of Injury (MOI)/ Nature of Illness (NOI) Ensure scene safety and address hazards. Standard precautions should include a minimum of gloves
404 Section 5 and Resuscitation Scene Size-up Scene Safety Mechanism of Injury (MOI)/ Nature of Illness (NOI) Ensure scene safety and address hazards. Standard precautions should include a minimum of gloves
National Registry of Emergency Medical Technicians Emergency Medical Technician Psychomotor Examination BLEEDING CONTROL/SHOCK MANAGEMENT
 BLEEDING CONTROL/SHOCK MANAGEMENT Candidate: Examiner: Date: Signature: Possible Applies direct pressure to the wound 1 NOTE: The examiner must now inform the candidate that the wound continues to bleed.
BLEEDING CONTROL/SHOCK MANAGEMENT Candidate: Examiner: Date: Signature: Possible Applies direct pressure to the wound 1 NOTE: The examiner must now inform the candidate that the wound continues to bleed.
2015 Interim Resources for HeartCode ACLS
 2015 Interim Resources for HeartCode ACLS Original Release: November 25, 2015 Starting in 2016, new versions of American Heart Association online courses will be released to reflect the changes published
2015 Interim Resources for HeartCode ACLS Original Release: November 25, 2015 Starting in 2016, new versions of American Heart Association online courses will be released to reflect the changes published
Cardiac Arrest: General Considerations
 Andrea Gabrielli, MD, FCCM Cardiac Arrest: General Considerations Cardiopulmonary resuscitation (CPR) is described as a series of assessments and interventions performed during a variety of acute medical
Andrea Gabrielli, MD, FCCM Cardiac Arrest: General Considerations Cardiopulmonary resuscitation (CPR) is described as a series of assessments and interventions performed during a variety of acute medical
2015 Interim Resources for BLS
 2015 Interim Resources for BLS Original Release: November 25, 2015 Starting in 2016, new versions of American Heart Association online courses will be released to reflect the changes published in the 2015
2015 Interim Resources for BLS Original Release: November 25, 2015 Starting in 2016, new versions of American Heart Association online courses will be released to reflect the changes published in the 2015
National Registry of Emergency Medical Technicians Emergency Medical Responder Psychomotor Examination BVM VENTILATION OF AN APNEIC ADULT PATIENT
 BVM VENTILATION OF AN APNEIC ADULT PATIENT Candidate: Examiner: Date: Signature: Possible Points Checks responsiveness NOTE: After checking responsiveness and breathing for at least 5 but no 1 Checks breathing
BVM VENTILATION OF AN APNEIC ADULT PATIENT Candidate: Examiner: Date: Signature: Possible Points Checks responsiveness NOTE: After checking responsiveness and breathing for at least 5 but no 1 Checks breathing
EMS SKILL CARDIAC EMERGENCY: AUTOMATED EXTERNAL DEFIBRILLATION (AED)
") EMS SKILL CARDIAC EMERGENCY: AUTOMATED EXTERNAL DEFIBRILLATION (AED) PERFORMANCE OBJECTIVE Demonstrate competency in assessing signs of cardiopulmonary arrest and performing defibrillation using a semi-automated
EMS SKILL CARDIAC EMERGENCY: AUTOMATED EXTERNAL DEFIBRILLATION (AED) PERFORMANCE OBJECTIVE Demonstrate competency in assessing signs of cardiopulmonary arrest and performing defibrillation using a semi-automated
Success Manual and Cheat Sheet Notes to Pass Your Basic Life Support (BLS) Course
 Course") Success Manual and Cheat Sheet Notes to Pass Your Basic Life Support (BLS) Course Written by: Jay Snaric, MS And Kimberly Hickman, RN CPR St. Louis 44 Meramec Valley Plaza St. Louis MO 63088 www.stlcpr.com
Success Manual and Cheat Sheet Notes to Pass Your Basic Life Support (BLS) Course Written by: Jay Snaric, MS And Kimberly Hickman, RN CPR St. Louis 44 Meramec Valley Plaza St. Louis MO 63088 www.stlcpr.com
DEBRIEFING GUIDE. The key components of an optimal code response: 1. Early recognition that the patient is deteriorating or has become unresponsive.
 DEBRIEFING GUIDE I N T R O D U C T I O N Debriefing has been shown to improve clinical behavior during cardiac resuscitation and, as such, has become a recommended procedure in the 2010 American Heart
DEBRIEFING GUIDE I N T R O D U C T I O N Debriefing has been shown to improve clinical behavior during cardiac resuscitation and, as such, has become a recommended procedure in the 2010 American Heart
National Registry Skill Sheets
 Bleeding Control/Shock Management BVM Ventilation of an Apneic Adult Patient Cardiac Arrest Management/AED Joint Immobilization Long Bone Immobilization Oxygen Administration By Non-Rebreather Mask Patient
Bleeding Control/Shock Management BVM Ventilation of an Apneic Adult Patient Cardiac Arrest Management/AED Joint Immobilization Long Bone Immobilization Oxygen Administration By Non-Rebreather Mask Patient
NATIONAL AMBULANCE SERVICE ONE LIFE PROJECT
 February 2015 NATIONAL AMBULANCE SERVICE ONE LIFE PROJECT Improving patient outcomes from Out Of Hospital Cardiac Arrest David Hennelly AP MSc Jan 2015 THE ONE LIFE PROJECT IS BEING LED BY THE NATIONAL
February 2015 NATIONAL AMBULANCE SERVICE ONE LIFE PROJECT Improving patient outcomes from Out Of Hospital Cardiac Arrest David Hennelly AP MSc Jan 2015 THE ONE LIFE PROJECT IS BEING LED BY THE NATIONAL
Heart information. CPR cardiopulmonary resuscitation
 Heart information CPR cardiopulmonary resuscitation Contents 3 What is CPR? 3 What is cardiac arrest? 4 Heart attack and cardiac arrest 4 Cardiopulmonary resuscitation (CPR) 5 Danger 6 Response 7 Send
Heart information CPR cardiopulmonary resuscitation Contents 3 What is CPR? 3 What is cardiac arrest? 4 Heart attack and cardiac arrest 4 Cardiopulmonary resuscitation (CPR) 5 Danger 6 Response 7 Send
ACLS PRE-TEST ANNOTATED ANSWER KEY
 ACLS PRE-TEST ANNOTATED ANSWER KEY June, 2011 Question 1: Question 2: There is no pulse with this rhythm. Question 3: Question 4: Question 5: Question 6: Question 7: Question 8: Question 9: Question 10:
ACLS PRE-TEST ANNOTATED ANSWER KEY June, 2011 Question 1: Question 2: There is no pulse with this rhythm. Question 3: Question 4: Question 5: Question 6: Question 7: Question 8: Question 9: Question 10:
PEDIATRIC TREATMENT GUIDELINES
 P1 Pediatric Patient Care P2 Cardiac Arrest Initial Care and CPR P3 Neonatal Resuscitation P4 Ventricular Fibrillation / Ventricular Tachycardia P5 PEA / Asystole P6 Symptomatic Bradycardia P7 Tachycardia
P1 Pediatric Patient Care P2 Cardiac Arrest Initial Care and CPR P3 Neonatal Resuscitation P4 Ventricular Fibrillation / Ventricular Tachycardia P5 PEA / Asystole P6 Symptomatic Bradycardia P7 Tachycardia
BLS for Healthcare Providers Study Guide and Pretest
 BLS for Healthcare Providers Study Guide and Pretest Adult CPR 1-Rescuer CPR Sequence check for responsiveness if no response, activate 911 and get the AED open the airway look, listen, & feel for breathing
BLS for Healthcare Providers Study Guide and Pretest Adult CPR 1-Rescuer CPR Sequence check for responsiveness if no response, activate 911 and get the AED open the airway look, listen, & feel for breathing
EMERGENCY MEDICAL RESPONDER (EMR) PRACTICAL SKILLS EXAMINATION REPORT State Form 54407 (R / 5-13)
 PRACTICAL SKILLS EXAMINATION REPORT State Form 54407 (R / 5-13)") EMERGENCY MEDICAL RESPONDER (EMR) PRACTICAL SKILLS EXAMINATION REPT State Form 54407 (R / 5-3) INDIANA DEPARTMENT OF HOMELAND SECURITY EMERGENCY MEDICAL SERVICES CERTIFICATION 302 West Washington Street,
EMERGENCY MEDICAL RESPONDER (EMR) PRACTICAL SKILLS EXAMINATION REPT State Form 54407 (R / 5-3) INDIANA DEPARTMENT OF HOMELAND SECURITY EMERGENCY MEDICAL SERVICES CERTIFICATION 302 West Washington Street,
Southern Stone County Fire Protection District Emergency Medical Protocols
 TITLE Pediatric Medical Assessment PM 2.4 Confirm scene safety Appropriate body substance isolation procedures Number of patients Nature of illness Evaluate the need for assistance B.L.S ABC s & LOC Focused
TITLE Pediatric Medical Assessment PM 2.4 Confirm scene safety Appropriate body substance isolation procedures Number of patients Nature of illness Evaluate the need for assistance B.L.S ABC s & LOC Focused
Team Leader. Ensures high-quality CPR at all times Assigns team member roles Ensures that team members perform well. Bradycardia Management
 ACLS Megacode Case 1: Sinus Bradycardia (Bradycardia VF/Pulseless VT Asystole Out-of-Hospital Scenario You are a paramedic and arrive on the scene to find a 57-year-old woman complaining of indigestion.
ACLS Megacode Case 1: Sinus Bradycardia (Bradycardia VF/Pulseless VT Asystole Out-of-Hospital Scenario You are a paramedic and arrive on the scene to find a 57-year-old woman complaining of indigestion.
How you can help save lives
 How you can help save lives Through Life Support Training Courses with THE INTERNATIONAL LIFE SUPPORT TRAINING CENTER (ILSTC) TABLE OF CONTENTS Introduction Page 3 Basic Life Support for Healthcare Provider
How you can help save lives Through Life Support Training Courses with THE INTERNATIONAL LIFE SUPPORT TRAINING CENTER (ILSTC) TABLE OF CONTENTS Introduction Page 3 Basic Life Support for Healthcare Provider
Cardiac Arrest VF/Pulseless VT Learning Station Checklist
 Cardiac Arrest VF/Pulseless VT Learning Station Checklist VF/VT 00 American Heart Association Adult Cardiac Arrest Shout for Help/Activate Emergency Response Epinephrine every - min Amiodarone Start CPR
Cardiac Arrest VF/Pulseless VT Learning Station Checklist VF/VT 00 American Heart Association Adult Cardiac Arrest Shout for Help/Activate Emergency Response Epinephrine every - min Amiodarone Start CPR
PRO-CPR. 2015 Guidelines: PALS Algorithm Overview. (Non-AHA supplementary precourse material)
") PRO-CPR 2015 Guidelines: PALS Algorithm Overview (Non-AHA supplementary precourse material) Please reference Circulation (from our website), the ECC Handbook, or the 2015 ACLS Course Manual for correct
PRO-CPR 2015 Guidelines: PALS Algorithm Overview (Non-AHA supplementary precourse material) Please reference Circulation (from our website), the ECC Handbook, or the 2015 ACLS Course Manual for correct
Management of Adult Cardiac Arrest
 73991_CH27_page68-73.qxd 6/6/11 3:54 PM Page 68 27.68 Section 5 Medical Guidelines for Performing a 12-Lead ECG The only way to learn how to obtain a 12-lead ECG is to practice with the equipment itself.
73991_CH27_page68-73.qxd 6/6/11 3:54 PM Page 68 27.68 Section 5 Medical Guidelines for Performing a 12-Lead ECG The only way to learn how to obtain a 12-lead ECG is to practice with the equipment itself.
19.109 AUTOMATED EXTERNAL DEFIBRILLATOR
 19.109 AUTOMATED EXTERNAL DEFIBRILLATOR References: American Heart Association Healthcare Provider (CPR/AED) Ohio Revised Code Chapter 2305.235 Immunity of Person Involved with Providing Automated External
19.109 AUTOMATED EXTERNAL DEFIBRILLATOR References: American Heart Association Healthcare Provider (CPR/AED) Ohio Revised Code Chapter 2305.235 Immunity of Person Involved with Providing Automated External
Emergency Medical Services Agency. Report to the Local Agency Formation Commission
 Emergency Medical Services Agency August 8, 2012 Report to the Local Agency Formation Commission The Relationship of Fire First Response to Emergency Medical Services On September 26, 2011, the Contra
Emergency Medical Services Agency August 8, 2012 Report to the Local Agency Formation Commission The Relationship of Fire First Response to Emergency Medical Services On September 26, 2011, the Contra
First Responder (FR) and Emergency Medical Responder (EMR) Progress Log
 and Emergency Medical Responder (EMR) Progress Log") First Responder (FR) and Emergency Medical Responder (EMR) Progress Log Note: Those competencies that are for EMR only are denoted by boldface type. For further details on the National Occupational Competencies
First Responder (FR) and Emergency Medical Responder (EMR) Progress Log Note: Those competencies that are for EMR only are denoted by boldface type. For further details on the National Occupational Competencies
BLS: basic cardiac life support. ACLS: advanced cardiac life support. PALS: paediatric advanced life support. VF: ventricular fibrillation
 RN-Initiated Emergency Cardiac Care: Decision Support Tool #2 Emergency Cardiac Care in Areas Using Cardiac Monitoring, Defibrillation and Emergency Cardiac Drugs Decision support tools are evidenced-based
RN-Initiated Emergency Cardiac Care: Decision Support Tool #2 Emergency Cardiac Care in Areas Using Cardiac Monitoring, Defibrillation and Emergency Cardiac Drugs Decision support tools are evidenced-based
2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care
 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Presenter Name Disclosures
2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Presenter Name Disclosures
The management of cardiac arrest
 CHAPTER 6 The management of cardiac arrest LEARNING OBJECTIVES In this chapter you will learn: How to assess the cardiac arrest rhythm and perform advanced life support 6.1. INTRODUCTION Cardiac arrest
CHAPTER 6 The management of cardiac arrest LEARNING OBJECTIVES In this chapter you will learn: How to assess the cardiac arrest rhythm and perform advanced life support 6.1. INTRODUCTION Cardiac arrest
Anatomy and Physiology: Understanding the Importance of CPR
 Anatomy and Physiology: Understanding the Importance of CPR Overview This document gives you more information about the body s structure (anatomy) and function (physiology). This information will help
Anatomy and Physiology: Understanding the Importance of CPR Overview This document gives you more information about the body s structure (anatomy) and function (physiology). This information will help
BLS TREATMENT GUIDELINES - CARDIAC
 BLS TREATMENT GUIDELINES - CARDIAC CARDIOPULMONARY ARREST - NON-TRAUMATIC (SJ-B101) effective 07/01/99 Defibrillation CPR Apply S-AED and assess rhythm as trained. Defib as indicated Simultaneous OXYGEN:
BLS TREATMENT GUIDELINES - CARDIAC CARDIOPULMONARY ARREST - NON-TRAUMATIC (SJ-B101) effective 07/01/99 Defibrillation CPR Apply S-AED and assess rhythm as trained. Defib as indicated Simultaneous OXYGEN:
(Organization s Name)
") 2 1 6 W A K E M A N P L A C E B R O O K L Y N, N E W Y O R K 1 1 2 2 0 W W W. A F O R U M F O R L I F E. O R G P H O N E 7 1 8 7 5 9 9 0 1 3 F A X 4 3 7 4 9 7 4 0 2 9 In association with the PROPOSAL FIRST
2 1 6 W A K E M A N P L A C E B R O O K L Y N, N E W Y O R K 1 1 2 2 0 W W W. A F O R U M F O R L I F E. O R G P H O N E 7 1 8 7 5 9 9 0 1 3 F A X 4 3 7 4 9 7 4 0 2 9 In association with the PROPOSAL FIRST
Community Ambulance Service of Minot ALS Standing Orders Legend
 Legend Indicates General Information and Guidelines Indicates Procedures Indicates Medication Administration Indicates Referral to Other Protocol Indicates Referral to Online Medical Direction Pediatric
Legend Indicates General Information and Guidelines Indicates Procedures Indicates Medication Administration Indicates Referral to Other Protocol Indicates Referral to Online Medical Direction Pediatric
ROC CONTINUOUS CHEST COMPRESSIONS STUDY (CCC): MEDICAL CARDIAC ARREST MEDICAL DIRECTIVE
: MEDICAL CARDIAC ARREST MEDICAL DIRECTIVE") ROC CONTINUOUS CHEST COMPRESSIONS STUDY (CCC): MEDICAL CARDIAC ARREST MEDICAL DIRECTIVE An Advanced Care Paramedic will provide the treatment based on the randomization scheme and as prescribed in this
ROC CONTINUOUS CHEST COMPRESSIONS STUDY (CCC): MEDICAL CARDIAC ARREST MEDICAL DIRECTIVE An Advanced Care Paramedic will provide the treatment based on the randomization scheme and as prescribed in this
EMBARGOED FOR RELEASE
 Systems of Care and Continuous Quality Improvement Universal elements of a system of care have been identified to provide stakeholders with a common framework with which to assemble an integrated resuscitation
Systems of Care and Continuous Quality Improvement Universal elements of a system of care have been identified to provide stakeholders with a common framework with which to assemble an integrated resuscitation
WMAS Clinical Guidelines CLN PRO - 027 I Version - 4
 WMAS Clinical Guidelines CLN PRO - 027 I Version - 4 Guideline ID CLN PRO - 027 Version Version 4 Title WMAS Stroke Guidelines Approved by Clinical Steering Group Date Issued 4 May 2016 Review Date May
WMAS Clinical Guidelines CLN PRO - 027 I Version - 4 Guideline ID CLN PRO - 027 Version Version 4 Title WMAS Stroke Guidelines Approved by Clinical Steering Group Date Issued 4 May 2016 Review Date May
AMERICAN HEART ASSOCIATION 2010 ACLS GUIDELINES: WHAT EVERY CLINICIAN NEEDS TO KNOW
 AMERICAN HEART ASSOCIATION 2010 ACLS GUIDELINES: WHAT EVERY CLINICIAN NEEDS TO KNOW Joseph Heidenreich, MD Texas A&M Health Science Center Scott & White Memorial Hospital Scott & White Memorial Hospital
AMERICAN HEART ASSOCIATION 2010 ACLS GUIDELINES: WHAT EVERY CLINICIAN NEEDS TO KNOW Joseph Heidenreich, MD Texas A&M Health Science Center Scott & White Memorial Hospital Scott & White Memorial Hospital
First Aid as a Life Skill. Training Requirements for Quality Provision of Unit Standard-based First Aid Training
 First Aid as a Life Skill Training Requirements for Quality Provision of Unit Standard-based First Aid Training New Zealand Qualifications Authority 2010 2 Index Introduction 3 Section One: Framework outline
First Aid as a Life Skill Training Requirements for Quality Provision of Unit Standard-based First Aid Training New Zealand Qualifications Authority 2010 2 Index Introduction 3 Section One: Framework outline
AUTOMATED EXTERNAL DEFIBRILLATORS (AEDs)
") UNIVERSITY of NORTH DAKOTA FINANCE & OPERATIONS POLICY LIBRARY AUTOMATED EXTERNAL DEFIBRILLATORS (AEDs) Policy 6.15, Automated External Defibrillators (AED) Responsible Executive: VP Finance & Operations
UNIVERSITY of NORTH DAKOTA FINANCE & OPERATIONS POLICY LIBRARY AUTOMATED EXTERNAL DEFIBRILLATORS (AEDs) Policy 6.15, Automated External Defibrillators (AED) Responsible Executive: VP Finance & Operations
Pediatric Airway Management
 Pediatric Airway Management Dec 2003 Dr. Shapiro I., PICU Adult Chain of Survival EMS CPR ALS Early Defibrillation Pediatric Chain of Survival Prevention CPR EMS ALS Out-of-Hospital Cardiac Arrest SIDS
Pediatric Airway Management Dec 2003 Dr. Shapiro I., PICU Adult Chain of Survival EMS CPR ALS Early Defibrillation Pediatric Chain of Survival Prevention CPR EMS ALS Out-of-Hospital Cardiac Arrest SIDS
CARDIOPULMONARY RESUSCITATION (CPR)
") Alert the Emergency Team Algorithm ABC Assess & Manage Defibrillation Medications Disability Exposure Secondary Survey Emergency Team Roles Medical Emergency Team Roles - Nursing Role in Wards Post-Resuscitation
Alert the Emergency Team Algorithm ABC Assess & Manage Defibrillation Medications Disability Exposure Secondary Survey Emergency Team Roles Medical Emergency Team Roles - Nursing Role in Wards Post-Resuscitation
EMERGENCY MEDICAL RESPONDER (EMR) PRACTICAL SKILLS EXAMINATION REPORT
 PRACTICAL SKILLS EXAMINATION REPORT") Reset Form EMERGENCY MEDICAL RESPONDER (EMR) PRACTICAL SKILLS EXAMINATION REPT INDIANA DEPARTMENT OF HOMELAND SECURITY EMERGENCY MEDICAL SERVICES CERTIFICATION 302 West Washington Street, Room E239 Indianapolis,
Reset Form EMERGENCY MEDICAL RESPONDER (EMR) PRACTICAL SKILLS EXAMINATION REPT INDIANA DEPARTMENT OF HOMELAND SECURITY EMERGENCY MEDICAL SERVICES CERTIFICATION 302 West Washington Street, Room E239 Indianapolis,
STATE OF CONNECTICUT
 STATE OF CONNECTICUT DEPARTMENT OF PUBLIC HEALTH June 7, 2010 The Following Will Be Policy For Emergency Medical Service Care Providers: GUIDELINES FOR EMR, EMT, AEMT, and Paramedic DETERMINATION OF DEATH/DISCONTINUATION
STATE OF CONNECTICUT DEPARTMENT OF PUBLIC HEALTH June 7, 2010 The Following Will Be Policy For Emergency Medical Service Care Providers: GUIDELINES FOR EMR, EMT, AEMT, and Paramedic DETERMINATION OF DEATH/DISCONTINUATION
National Registry of EMTs Continued Competency Program. (NREMT Recertification Requirements) BETA Version 2
 BETA Version 2") National Registry of EMTs Continued Competency Program (NREMT Recertification Requirements) BETA Version 2 Massachusetts providers Issue date: 5/1/2013 The Four Principles of Continued Competency Professional
National Registry of EMTs Continued Competency Program (NREMT Recertification Requirements) BETA Version 2 Massachusetts providers Issue date: 5/1/2013 The Four Principles of Continued Competency Professional
Policy: B4 Basic Life Support Policy
 Policy: B4 Basic Life Support Policy Version: B4/04 Ratified by: Trust Management Team Date ratified: 15 th April 2015 Name and Title of Author: Director of Primary Care Accountable Director Medical Director
Policy: B4 Basic Life Support Policy Version: B4/04 Ratified by: Trust Management Team Date ratified: 15 th April 2015 Name and Title of Author: Director of Primary Care Accountable Director Medical Director
Module Two: EMS Systems. Wisconsin EMS Medical Director s Course
 : EMS Systems Wisconsin EMS Medical Director s Course Objectives List the components of EMS systems Outline organizational and design options for EMS systems Outline system staffing and response configurations
: EMS Systems Wisconsin EMS Medical Director s Course Objectives List the components of EMS systems Outline organizational and design options for EMS systems Outline system staffing and response configurations
2015 AHA /ECC updates for BLS: Compression rate and depth - how to perform and monitor
 2015 AHA /ECC updates for BLS: Compression rate and depth - how to perform and monitor 范 文 林 醫 師 2016/04/10 Reinforced Chest compressions are the key component of effective CPR. Characteristics of chest
2015 AHA /ECC updates for BLS: Compression rate and depth - how to perform and monitor 范 文 林 醫 師 2016/04/10 Reinforced Chest compressions are the key component of effective CPR. Characteristics of chest
Seven steps to patient safety The full reference guide. Second print August 2004
 Seven steps to patient safety The full reference guide Second print August 2004 National Patient Safety Agency Seven steps to patient safety 113 Appendix Four F Examples of events according to severity
Seven steps to patient safety The full reference guide Second print August 2004 National Patient Safety Agency Seven steps to patient safety 113 Appendix Four F Examples of events according to severity
RGN JOY LAUDE WATFORD GENERAL HOSPITAL, ENGLAND
 RGN JOY LAUDE WATFORD GENERAL HOSPITAL, ENGLAND Monitor patient on the ward to detect trends in vital signs and to manage accordingly To recognise deteriorating trends and request relevant medical/out
RGN JOY LAUDE WATFORD GENERAL HOSPITAL, ENGLAND Monitor patient on the ward to detect trends in vital signs and to manage accordingly To recognise deteriorating trends and request relevant medical/out
New Approaches for Prehospital Cardiac Arrest Management 2010 NCEMSF Conference
 New Approaches for Prehospital Cardiac Arrest Management 2010 NCEMSF Conference Mark E. Pinchalk, MS, EMT-P Paramedic Crew Chief City of Pittsburgh EMS Out of Hospital Cardiac Arrest Poor outcomes: Arizona
New Approaches for Prehospital Cardiac Arrest Management 2010 NCEMSF Conference Mark E. Pinchalk, MS, EMT-P Paramedic Crew Chief City of Pittsburgh EMS Out of Hospital Cardiac Arrest Poor outcomes: Arizona
Guideline Health Service Directive
 Guideline Health Service Directive Guideline QH-HSDGDL-025-3:2014 Effective Date: 17 January 2014 Review Date: 17 January 2016 Supersedes: qh-hsdptl-025-3:2012 Patient Access and Flow Health Service Directive
Guideline Health Service Directive Guideline QH-HSDGDL-025-3:2014 Effective Date: 17 January 2014 Review Date: 17 January 2016 Supersedes: qh-hsdptl-025-3:2012 Patient Access and Flow Health Service Directive
Levels of Critical Care for Adult Patients
 LEVELS OF CARE 1 Levels of Critical Care for Adult Patients STANDARDS AND GUIDELINES LEVELS OF CARE 2 Intensive Care Society 2009 All rights reserved. No reproduction, copy or transmission of this publication
LEVELS OF CARE 1 Levels of Critical Care for Adult Patients STANDARDS AND GUIDELINES LEVELS OF CARE 2 Intensive Care Society 2009 All rights reserved. No reproduction, copy or transmission of this publication
MLFD Standard Operating Guidelines SOG# 12-22 Subject: Patient Transfer of Care Initiated 1/30/2013
 MLFD Standard Operating Guidelines SOG# 12-22 Subject: Patient Transfer of Care Initiated 1/30/2013 Approved: Revised PURPOSE It is the purpose of this SOG to provide and ensure the highest level of patient
MLFD Standard Operating Guidelines SOG# 12-22 Subject: Patient Transfer of Care Initiated 1/30/2013 Approved: Revised PURPOSE It is the purpose of this SOG to provide and ensure the highest level of patient
American Red Cross CPR Adult EXAMPLE ANSWER SHEET
 American Red Cross CPR Adult IMPORTANT: Read all instructions before beginning the exam. INSTRUCTIONS: Do not write on this exam. Mark all answers in pencil on the separate answer sheet as directed by
American Red Cross CPR Adult IMPORTANT: Read all instructions before beginning the exam. INSTRUCTIONS: Do not write on this exam. Mark all answers in pencil on the separate answer sheet as directed by
American Heart Association. BLS Instructor Course. Written Examination. July 2003
 American Heart Association BLS Instructor Course Written Examination July 2003 Basic Life Support Instructor Exam Part I Please do not mark on this examination. Record the best answer on the separate answer
American Heart Association BLS Instructor Course Written Examination July 2003 Basic Life Support Instructor Exam Part I Please do not mark on this examination. Record the best answer on the separate answer
Emergency Action Plans
 Emergency Action Plans Clearly the most effective way to deal with an injury- emergency is to plan ahead and to practice the appropriate procedures. An emergency action plan is a written plan of action
Emergency Action Plans Clearly the most effective way to deal with an injury- emergency is to plan ahead and to practice the appropriate procedures. An emergency action plan is a written plan of action
If you do not wish to print the entire pre-test you may print Page 2 only to write your answers, score your test, and turn in to your instructor.
 This is a SAMPLE of the pretest you can access with your AHA PALS Course Manual at Heart.org/Eccstudent using your personal code that comes with your PALS Course Manual The American Heart Association strongly
This is a SAMPLE of the pretest you can access with your AHA PALS Course Manual at Heart.org/Eccstudent using your personal code that comes with your PALS Course Manual The American Heart Association strongly
GWAS Competency Mapping Levels of Medical Support Within GWAS
 GWAS Competency Mapping Levels of Medical Support Within GWAS Great Western Ambulance Service NHS Trust is pleased to be able to work with a range of doctors in delivering effective pre-hospital care.
GWAS Competency Mapping Levels of Medical Support Within GWAS Great Western Ambulance Service NHS Trust is pleased to be able to work with a range of doctors in delivering effective pre-hospital care.
Patient Schematic. Perkins GD et al The Lancet, 385, 2015, 947-955
 Lancet March 2015 Patient Schematic Perkins GD et al The Lancet, 385, 2015, 947-955 Background Adequate CPR is critical for survival for CA patients Maintenance of high-quality compressions during OHCA
Lancet March 2015 Patient Schematic Perkins GD et al The Lancet, 385, 2015, 947-955 Background Adequate CPR is critical for survival for CA patients Maintenance of high-quality compressions during OHCA
Cardio-Pulmonary Resuscitation (CPR): A Decision Aid For. KGH Patients And Their Families
: A Decision Aid For. KGH Patients And Their Families") Cardio-Pulmonary Resuscitation (CPR): A Decision Aid For KGH Patients And Their Families The goal of this pamphlet is to provide information about cardiopulmonary resuscitation (CPR) so you can be adequately
Cardio-Pulmonary Resuscitation (CPR): A Decision Aid For KGH Patients And Their Families The goal of this pamphlet is to provide information about cardiopulmonary resuscitation (CPR) so you can be adequately
Present : PGY 王 淳 峻 Supervisor: F1 王 德 皓 991109
 Present : PGY 王 淳 峻 Supervisor: F1 王 德 皓 991109 Interventions to prevent cardiac arrest + Airway management + Ventilation support + Treatment of bradyarrhythmias & Tachyarrhythmias Treat cardiac arrest
Present : PGY 王 淳 峻 Supervisor: F1 王 德 皓 991109 Interventions to prevent cardiac arrest + Airway management + Ventilation support + Treatment of bradyarrhythmias & Tachyarrhythmias Treat cardiac arrest
American Heart Association. Basic Life Support for Healthcare Providers
 American Heart Association Basic Life Support for Healthcare Providers Pretest ANNOTATED ANSWER KEY February 2001 This examination to be used only as a PRECOURSE TEST for BLS for Healthcare Providers Courses
American Heart Association Basic Life Support for Healthcare Providers Pretest ANNOTATED ANSWER KEY February 2001 This examination to be used only as a PRECOURSE TEST for BLS for Healthcare Providers Courses
Intro Who should read this document 2 Key Messages 2 Background 2
 Classification: Policy Lead Author: Nathan Griffiths, Consultant Nurse Paediatric Emergency Medicine Additional author(s): N/A Authors Division: Salford Healthcare Unique ID: DDCPan04(14) Issue number:
Classification: Policy Lead Author: Nathan Griffiths, Consultant Nurse Paediatric Emergency Medicine Additional author(s): N/A Authors Division: Salford Healthcare Unique ID: DDCPan04(14) Issue number:
Emergency Medical Services Advanced Level Competency Checklist
 Emergency Services Advanced Level Competency Checklist EMS Service: Current License in State of Nebraska: # (Copy of license kept in file at station) Date of joining EMS Service: EMS Service Member Name:
Emergency Services Advanced Level Competency Checklist EMS Service: Current License in State of Nebraska: # (Copy of license kept in file at station) Date of joining EMS Service: EMS Service Member Name:
A. Policy Statement. B. Principles. (1) Phases of Emergency Medical Services (EMS)
 Phases of Emergency Medical Services (EMS)") A. Policy Statement B. Principles Each State-operated psychiatric inpatient facility is responsible for ensuring the provision of appropriate emergency medical care to patients, visitors and employees
A. Policy Statement B. Principles Each State-operated psychiatric inpatient facility is responsible for ensuring the provision of appropriate emergency medical care to patients, visitors and employees
NORTH WALES CRITICAL CARE NETWORK
 NORTH WALES CRITICAL CARE NETWORK LEVELS OF CRITICAL CARE FOR ADULT PATIENTS Throughout the work of the North Wales Critical Care Network reference to Levels of Care for the critically ill are frequently
NORTH WALES CRITICAL CARE NETWORK LEVELS OF CRITICAL CARE FOR ADULT PATIENTS Throughout the work of the North Wales Critical Care Network reference to Levels of Care for the critically ill are frequently
How To Treat A Heart Attack
 13 Resuscitation and preparation for anaesthesia and surgery Key Points 13.1 MANAGEMENT OF EMERGENCIES AND CARDIOPULMONARY RESUSCITATION ESSENTIAL HEALTH TECHNOLOGIES The emergency measures that are familiar
13 Resuscitation and preparation for anaesthesia and surgery Key Points 13.1 MANAGEMENT OF EMERGENCIES AND CARDIOPULMONARY RESUSCITATION ESSENTIAL HEALTH TECHNOLOGIES The emergency measures that are familiar
Ohio s Do-Not-Resuscitate Law
 Ohio s Do-Not-Resuscitate Law Copied from Choices: Living Well at the End of Life developed in collaboration with the Ohio Hospice and Palliative Care Organization, the Ohio State Medical Association,
Ohio s Do-Not-Resuscitate Law Copied from Choices: Living Well at the End of Life developed in collaboration with the Ohio Hospice and Palliative Care Organization, the Ohio State Medical Association,
trust clinical guideline
 CG04 VERSION 1.0 1/5 Guideline ID CG04 Version 1.0 Title Approved by Allergic Reactions Clinical Effectiveness Group Date Issued 01/01/2013 Review Date 31/12/2016 Directorate Authorised Staff Clinical
CG04 VERSION 1.0 1/5 Guideline ID CG04 Version 1.0 Title Approved by Allergic Reactions Clinical Effectiveness Group Date Issued 01/01/2013 Review Date 31/12/2016 Directorate Authorised Staff Clinical
Orientation Guide www.lucas-cpr.com a product by JOLIFE 900080-00 RevB JOLIFE 2012
 Orientation Guide www.lucas-cpr.com a product by JOLIFE 900080-00 RevB JOLIFE 2012 Refer to the Instructions for Use for complete directions for use, indications, contraindications, warnings, precautions
Orientation Guide www.lucas-cpr.com a product by JOLIFE 900080-00 RevB JOLIFE 2012 Refer to the Instructions for Use for complete directions for use, indications, contraindications, warnings, precautions
AHA/AAP Neonatal Resuscitation Guidelines 2010: Summary of Major Changes and Comment on its Utility in Resource-Limited Settings
 AHA/AAP Neonatal Resuscitation Guidelines 2010: Summary of Major Changes and Comment on its Utility in Resource-Limited Settings Resuscitation step Recommendations (2005) Recommendations (2010) Comments/LOE
AHA/AAP Neonatal Resuscitation Guidelines 2010: Summary of Major Changes and Comment on its Utility in Resource-Limited Settings Resuscitation step Recommendations (2005) Recommendations (2010) Comments/LOE
Early Warning Scores (EWS) Clinical Sessions 2011 By Bhavin Doshi
 Clinical Sessions 2011 By Bhavin Doshi") Early Warning Scores (EWS) Clinical Sessions 2011 By Bhavin Doshi What is EWS? After qualifying, junior doctors are expected to distinguish between the moderately sick patients who can be managed in the
Early Warning Scores (EWS) Clinical Sessions 2011 By Bhavin Doshi What is EWS? After qualifying, junior doctors are expected to distinguish between the moderately sick patients who can be managed in the
Basic life support (BLS) Techniques
 Techniques") module Basic life support (BLS) Techniques 1 01 04. Basic Cardio Pulmonary Resuscitation (CPR) 08. Adult basic life support sequence, according to European Resuscitation Guidelines 12. Recognition of cardiorespiratory
module Basic life support (BLS) Techniques 1 01 04. Basic Cardio Pulmonary Resuscitation (CPR) 08. Adult basic life support sequence, according to European Resuscitation Guidelines 12. Recognition of cardiorespiratory
Automated External Defibrillator
 Automated External Defibrillator 1. INTRODUCTION An automated external defibrillator (AED) is used to treat victims who experience sudden cardiac arrest. It must only be applied to victims who are unconscious,
Automated External Defibrillator 1. INTRODUCTION An automated external defibrillator (AED) is used to treat victims who experience sudden cardiac arrest. It must only be applied to victims who are unconscious,
Target groups: Paramedics, nurses, respiratory therapists, physicians, and others who manage respiratory emergencies.
 Overview Estimated scenario time: 10 15 minutes Estimated debriefing time: 10 minutes Target groups: Paramedics, nurses, respiratory therapists, physicians, and others who manage respiratory emergencies.
Overview Estimated scenario time: 10 15 minutes Estimated debriefing time: 10 minutes Target groups: Paramedics, nurses, respiratory therapists, physicians, and others who manage respiratory emergencies.
Health Care Directive
 PATIENT EDUCATION Health Care Directive Honoring Choices My Health Care Directive I created this document with much thought to give my treatment choices and personal preferences if I cannot communicate
PATIENT EDUCATION Health Care Directive Honoring Choices My Health Care Directive I created this document with much thought to give my treatment choices and personal preferences if I cannot communicate