Chiropractors & Physiotherapists
|
|
|
- Anabel Eaton
- 7 years ago
- Views:
Transcription
1 A Support Package for Chiropractors & Physiotherapists Treating Injured Workers Published by Saskatchewan Workers Compensation Board 2011
2 TABLE OF CONTENTS 1. Preface Integrated Partnership Model Synopsis The Workers Compensation System Cost of Health Care for Injured Workers Benefits for Injured Workers 4 5. The WCB s Health Care Program Integrated Model of Recovery and Return To Work The WCB s Philosophy of Care WCB Services to Care Providers Levels of Care 5 6. Standards and Requirements Accreditation 6.2 WCB Standards Authorization to Treat 8 7. The Role of the Chiropractor and Physiotherapist Assessment and Diagnosis Explain the Benefits of Functional Rehabilitation and Early Return to Work Treatment Evaluate Any Risks Involved in Return to Work Communicate Functional Abilities Report to the WCB Monitor Return to Work Advanced Assessment and Treatment Multidisciplinary Assessment Arranging Advanced Treatment Return to Work Employers Have a Duty to Accommodate Return to Work Process Return to Work with Permanent Impairment Preventive Job Change Factors Affecting RTW/Function Symptoms of Increased Risk of Chronic Disability Employment and Personal Factors Permanent Functional Impairment (PFI)... 24
3 12. Workers With Injury-Related Disability Conclusion Appendices Appendix I: Compensation Benefits for Injured Workers 1 Appendix II: Appealing a WCB decision 2 Appendix III: Chiropractor s Initial Report (CHI) & User Manual 3 Appendix IV: Chiropractor s Progress/Discharge Report (CHP) & User Manual 7 Appendix V: Physiotherapist s Initial Report (PTI) & User Manual 11 Appendix VI: Physiotherapist s Progress/Discharge Report (PTP) & User Manual 15 Appendix VII: Practitioner s Return to Work Report (PRTW) 19 Appendix VIII: Risk Factors for Chronic Disability 21 Appendix IX: Lower Extremity Functional Scale (LEFS) 22 Appendix X: Neck Disability Index (NDI) 24 Appendix XI: Quick Dash and Work Module for Upper Extremities 29 Appendix XII: Roland Morris For Backs 32 Appendix XIII: Reporting Fees - Chiropractors 33 Appendix XIV: Reporting Fees - Physical Therapists 37 Appendix XV: Positive and Negative Factors for RTW/Function 40 Appendix XVI: Glossary and Abbreviations 42 Appendix XVII: WCB Contact Information 42
4 1. Preface The Saskatchewan Workers Compensation Board (WCB) recognizes the important role chiropractors and physical therapists play in diagnosing and treating, and assisting injured workers in safe and timely return to work. For this reason, the WCB has signed relationship agreements with the Saskatchewan Physiotherapy Association and the Chiropractor s Association of Saskatchewan that defines how the agencies and the WCB can work together. In addition, both associations hold seats on the WCB s Health Care Advisory Committee, which advises the WCB on health related issues. The committee also includes an injured worker, an employer, and representatives from physician, chiropractor, physical therapist and occupational therapist care provider groups. The WCB also employs two chiropractic and two physical therapy consultants to assist in file review, liaise with practitioners and provide input for program and policy development. The WCB encourages use of its Integrated Partnership Model, for the treatment and return to work of injured workers. This model (shown on the next page) requires all partners in the return to work process primary and other care providers, the injured worker, the employer, and the WCB to work together to promote recovery and return to work. This support package was prepared with input from the SPA and CAS to help practicing physical therapists and chiropractors manage a worker s recovery and return to work following an injury or illness. The package can also be used as a resource by health care students and residents in postgraduate programs to answer specific questions they will encounter when treating injured workers. As a companion to this Support Package, a quick reference Desk Card is now available. The card features: a quick reference to treating injured workers a convenient dictionary of occupational titles functional categories WCB contact information Chiropractors and physical therapists can order a laminated copy or download and print a paper copy by visiting
5 2. Integrated Partnership Model Returning an injured worker to work requires open, ongoing communication and cooperation by all the partners the primary and other care providers, the injured worker, the employer and the WCB and awareness of the role each plays in the process. 2
6 3. Synopsis The following is a summary of the steps in this document that will help chiropractors and physical therapists manage the care and return to work of injured workers: 1. Post a sign in your reception area asking patients who have been injured on the job to identify themselves to your office staff. 2. Compile a detailed history of the present injury and past history, make a diagnosis and establish a treatment plan. Explain the benefits of the functional rehabilitation model and early return to work if appropriate. 3. Report the injury to the WCB within 3 days of the initial visit using the appropriate Initial Report form (CHI or PTI). 4. Give the worker a prognosis for recovery and expected amount of time before the worker can return to full work. 5. Evaluate the risks to co-workers and the public if the worker returns to work with restrictions. 6. Initiate the return to work process during the first visit(s) by listing the functional abilities the injured worker has. Make contact with the employer to discuss the injured worker s functional abilities and a potential return-to-work plan. Send a copy of the return-to-work plan to the WCB, and inform the primary care provider (if other than yourself) of your plan for return to work. 7. Make and maintain detailed notes on the worker s condition. 8. Encourage a positive attitude to return to work and recovery. 9. Monitor the worker s progress and return to work on a regular basis as conditions warrant. 10. Monitor for any risk factors for chronic disability. If initial treatments do not appear to be the right care for the worker, complete a Progress Report form, and indicate in the comments section that an assessment or alternate form of treatment needs to be considered. 11. Expedite appointments for advanced diagnostic tests, assessments and treatment based on your professional judgment and clinical findings present. If you are the primary care provider, you can contact the WCB to initiate the request. If not, you must forward your request to the primary care provider. 12. Advise the WCB (and the primary care provider, if not you) whenever you think multidisciplinary assessment or treatment is needed. WCB staff will also consider this as part of their regularly scheduled file review. 3
7 4. The Workers Compensation System The Saskatchewan Workers Compensation Act, 1979 provides no-fault coverage for Saskatchewan workers in case of workplace related injury. A work injury is one that: occurs at work, on company property or on company business; requires the attention of a health care provider; and may or may not need time away from work. The WCB uses premiums it collects from employers to provide health care and benefits to injured workers, and promote safety and injury prevention in Saskatchewan workplaces. Workers do not pay for the benefits and protection they receive under the Act, and employers are protected against lawsuits. Care providers are required to report all work injuries to the WCB. After reviewing the care provider s report, along with reports from the employer and the worker, the WCB decides whether or not to accept the claim based on established WCB policy. If an injured worker disagrees with a WCB decision involving a claim, a request can be made to have that decision reviewed. Health care information is a vital part of many appeals. For more information on the review and appeal process, see Appendix II: Appealing a WCB Decision. 4.1 Cost of Health Care for Injured Workers The WCB pays all health care costs for injured workers because they are exempt from the Canada Health Act, and are not covered by Saskatchewan Health. The service fees paid to care providers by the WCB are negotiated with their respective professional associations. The WCB s mission is, in part, to provide the right service, at the right time, and be costeffective in our processes. To accomplish this, the WCB must ensure injured workers receive prompt, continuing, effective health care so they can return to work as soon as it is medically safe. 4.2 Benefits for Injured Workers In addition to medical costs, the WCB may also compensate injured workers for: wages lost due to their injuries; health care supplies; cost of travel to health care appointments in excess of usual employment travel costs; and additional support may be available if the worker is permanently impaired. For more information on WCB benefits, see Appendix I: Compensation Benefits for Injured Workers or visit the benefits section under Worker Services on the WCB website. 4
8 5. The WCB s Health Care Program 5.1 Integrated Model of Recovery and Return to Work WCB has adopted an integrated partnership model within which, injured workers, employers, all care providers, union representatives and the WCB employ strategies that: ensure adequate and timely health care; support the timely recovery of injured workers; integrate return-to-work programs in the work place with appropriate and timely health care, and claims management processes; hold all partners accountable for their roles of returning injured workers to safe and sustained employment; and encourage active treatment at the primary level, with timely access to secondary and tertiary services where required. 5.2 The WCB s Philosophy of Care The WCB supports the functional rehabilitation model, which uses the restoration of function as a very important measure of treatment success. There is a significant body of evidence-based literature to support this model. The model encourages care providers and injured workers to recognize that successful long-term recovery is associated with return to function, even in the presence of increasing symptoms where there are no objective signs of harm. The symptomatic model of care is discouraged in this model because it uses passive care to ease symptoms. Studies show this type of care may contribute to the development of chronic disability. 5.3 WCB Services to Care Providers Upon request, the WCB provides the following support to care providers treating injured workers: arranging expedited services such as specialist consultations in some specialties. MRIs, CT scans, diagnostic ultrasound, EMG or other diagnostics, and expedited day surgeries; arranging advanced multidisciplinary assessment and treatment; and hosting conferences and workshops to foster common understanding and efficient processes for treatment and return to work for injured workers. When a partner in the integrated partnership indicates an injured worker has certain functional abilities, the WCB will help the employer arrange appropriate accommodations, if requested. 5.4 Levels of Care The WCB s functional rehabilitation model allows for assessment and treatment to be delivered at three levels (primary, secondary, and tertiary) differentiated by complexity, scope and resources. 5
9 Primary Assessment and Treatment Following an injury, treatment is generally provided by a physician, chiropractor or physical therapist. Concurrent primary services by other allied health provider groups are sometimes utilized. Treatment is often delivered by a single service provider, although concurrent care providers can be involved. Global conditioning and functional conditioning are rarely required. The injured worker is often able to return to the workplace in a timely fashion using a graduated return-to-work program. Guidelines for the care of soft tissue injuries at the primary level have been developed by the WCB, in conjunction with the Saskatchewan Physiotherapy and Chiropractic Associations. These can be found at Approximately 90% of workplace injuries are resolved at the primary level. Secondary Treatment Secondary treatment programs are designed for injured workers who: have not made a timely recovery within typical primary timeframes; but can be expected to return to the duties they performed at the time of their injury without permanent disability. Treatment is provided by a multidisciplinary team of health care professionals. Increased resources are required to initiate global and functional conditioning in order to better prepare the injury for the typical stresses associated within the workplace. Additional time and treatment are required to assist with tissue accommodation prior to returning to work. Tertiary Treatment Tertiary treatment programs are designed for injured workers who may require: a wider range of treatment; additional conditioning or education; return to work planning and monitoring; and management of psychosocial and pain management issues. Treatment is provided by a multidisciplinary team of health care professionals with expertise in the management of injuries. These injuries may have permanent sequelae or significant associated psychosocial and pain management issues. The recovery process is more intense due to a range of associated issues or the severity of the injury. A coordinated multidisciplinary approach is required to ensure all injuryrelated issues are addressed. 6
10 6. Standards and Requirements 6.1 Accreditation Chiropractors Chiropractors are automatically accredited with the WCB through the Saskatchewan Medical Services Branch (MSB.) Chiropractors use their MSB billing number to bill the WCB for service to injured workers. Physiotherapists Physical therapists must be a member in good standing with the Saskatchewan College of Physical Therapists and the Saskatchewan Physiotherapy Association (via the Canadian Physiotherapy Association). Therapists must also be accredited by the WCB before they can provide physical therapy to WCB clients. Physiotherapists bill the WCB directly for those services. To apply for accreditation with the WCB: read the WCB Physical Therapy Practice Standards carefully; complete the Accreditation Request Primary Level Service form, print and sign it; Attach to your form: o evidence of your educational credentials; o o evidence of current licensure with your licensing body; evidence of additional educational credentials if you are applying for aerobic assessment and treatment accreditation; and mail the completed form and attached documents to the WCB Health Care Services department. Please note: The WCB cannot process incomplete applications. The WCB's Health Care Services department will: review your credentials against the requirement listed in the WCB Physical Therapy Practice Standards; notify you by mail as to whether your accreditation request has been accepted or rejected; and if accepted: o o add your name to the WCB's Approved Providers List mail to you a WCB billing number that allows you to bill the WCB directly for your services to injured workers. Accreditation Is Specific to Clinics Your WCB accreditation is non-transferable. The WCB will accredit you for work in all the clinics you listed on your application. The WCB cannot issue payment for care at a clinic where the provider is not accredited prior to that care being provided. If you add a clinic to your portfolio or if your clinic changes location, you must submit a separate accreditation request. 7
11 6.2 WCB Standards When treating WCB clients, health care providers assume certain roles and responsibilities. The WCB relies on all health care providers to ensure that: all workplace injuries requiring health care are reported promptly; all treatment is necessary and consistent with established agreements; all invoices are appropriate. When treating WCB clients, the WCB asks that you: familiarize yourself and comply with the practice standards and fee schedule established by the WCB with your professional associations, and all requirements of your licensing body; demonstrate ethical practice standards on a day-to-day basis, including disclosure to any perspective WCB client of any business relationship you may have with their employer (This allows the worker to make an informed decision regarding their choice of care provider); refrain from using your affiliation with the WCB in any advertising. Compliance Surveys If you supply physical therapy services to injured workers you will be required to participate in compliance surveys to ensure that practice standards and fee schedules are being followed. Treatment centers, clinics and individual practitioners will be notified two weeks before the survey is sent. You can prepare for the survey by reviewing the survey form and guidelines in advance. Surveys take approximately 1.5 hours and will be conducted by physical therapists or WCB representatives. 6.3 Authorization to Treat As a licensed chiropractor and an accredited physical therapist, injured workers have direct access to treatment. Please note: Referrals do not constitute authorization to treat. If you refer WCB clients to certain allied health care providers, such as massage therapists or exercise therapists, the providers must contact the WCB for authorization to treat the referred clients on a case-by-case basis. The WCB uses a negative-response system to confirm funding of chiropractic or physical therapy care: Within three days of your initial assessment of a client requesting work injury related treatment, you need to forward an Initial Report (CHI or PTI) detailing your initial findings and Functional Outcome Measures (FOM) scores. If the injury claim is disallowed or benefits terminated, you will be notified that the WCB cannot pay for further assessment or treatment. You will be paid for: o the intake assessment; o the initial report and any treatment given up to the date of notification of noncoverage; o any reporting fees to date of notice. 8
12 Until WCB advises of non-coverage, do not bill the Provincial Medical Services Plan, other insurers, and/or the worker for any treatment or portion of treatment. If the injured worker's recovery does not progress, contact the worker's primary care provider who can request advanced assessment and treatment, or expedited appointments. See also: Disability Duration Guidelines under Care Provider Services on the WCB website. Generally, return to work should be part of each worker's treatment plan. For more information, see our Recovery and Return to Work brochure. 9
13 7. The Role of the Chiropractor and Physiotherapist Standards of care for chiropractors and physical therapists are developed with input from the Chiropractor s Association of Saskatchewan and Saskatchewan Physiotherapy Association. These standards underscore the importance of evidence-based care that uses a functional rehabilitation approach. The fees that the WCB negotiates with the chiropractic and physical therapy associations reflect the level of service required to help a worker not only recover from a work injury, but also return to work as quickly as is safely possible in either a modified capacity or gradual progression to full function. Recovery is best achieved by active treatment at the primary level, integrated with return to work as soon as appropriate, and timely access to secondary and tertiary services where required. In addition to the assessment and treatment of the work injury, a chiropractor or physical therapist would normally complete an evaluation of the injured worker s current functional abilities. This evaluation is typically completed by history taking and by questioning or talking with the worker. This evaluation will be the basis of the return to work component of the treatment plan. The extra responsibility this places on chiropractors and physical therapists is balanced by the assistance available from the WCB and employer. As the injured worker s chiropractor or physical therapist, you have a responsibility to maintain communication with the worker and the WCB about the extent of the worker s injury and the expected recovery timeline. Within the first couple of appointments, please submit information about the worker s current functional abilities as they relate to their pre-injury work requirements to: the WCB; the primary care provider (if other than yourself); the employer (via the worker or directly to the employer). In almost all circumstances, functional abilities should be provided as soon as possible, unless the worker is hospitalized or housebound. The list of functional abilities allows the employer to identify if appropriate work is available for the worker while the worker recovers. The onus is on the employer to match work to the functional abilities identified by the care provider. The initial determination of these functional abilities is typically made through history taking, questioning the worker about specifics of the job and evaluating the clinical objective findings in relation to this information. If there is substantial discrepancy with the perceived functional abilities that the worker reports and the practitioner s expectations based on the clinical examination, a functional abilities evaluation may be required. This is typically only done on one occasion. Recovery can best be achieved by active treatment at the primary level integrated with a return to work as soon as appropriate, and timely access to secondary and tertiary services, where required. 10
14 WCB Consultants The WCB employs chiropractor and physiotherapy consultants who: provide input into WCB programs; provide information to their peers via WCB-funded conferences and newsletters; are available for file-specific discussions. WCB consultants may contact you if an injured worker s progress does not appear to be occurring. As professionals, you will review the situation, discuss the problem, and identify possible treatment(s) that offer the best progress to return the injured worker to their pre-injury functional levels. Quality Assurance Program In consultation with provincial chiropractic and physical therapy associations, the WCB developed a review process which demonstrates accountability to injured workers, employers who fund the recovery, and chiropractors and physiotherapists. The Primary Care Provider Review allows health care providers to compare their treatment outcomes with the average of their peers. 7.1 Assessment and Diagnosis It is important to identify injured workers during their first visit. Post a sign in your waiting room asking patients to identify that they have a work related injury. Carefully document the worker s condition at the first visit and throughout recovery, and completely fill out all WCB report forms. This information is valuable to the WCB, other health care professionals, and to the worker. Prompt reporting allows for: timely WCB decisions; timely access to treatment; prompt payment of benefits. A thorough and accurate initial assessment and diagnosis is extremely important for full and successful recovery. Extra care is needed at the initial visit(s) to ensure that the injured worker has an accurate understanding of the prognosis for recovery. 7.2 Explain the Benefits of Functional Rehabilitation and Early Return to Work During an injured worker s initial visit(s), you can prevent many worries the worker may have about their condition by: stressing the importance of being as active as possible with the functional abilities the worker may have; reassuring the worker that discomfort from recommended activity is a normal part of the recovery process. 11
15 7.3 Treatment The WCB has adopted an integrated partnership model to treat injured workers that requires timely and appropriate communication between the WCB, the injured worker, the employer, and health care providers. See Section 2: Integrated Partnership Model for information about this model. The functional rehabilitation model supported by the WCB requires all partners to work together in order to facilitate the recovery of the injured worker based on his physical abilities. This model is based on evidence and adheres to the best practice guidelines known for treating soft tissue injuries that occur in the workplace. More information about the functional rehabilitation model is found in Section 5.2: WCB s Philosophy of Care. The WCB will support evidence-based treatment protocols provided by chiropractors and physical therapists. Functional restoration of the injured worker requires the health care provider to encourage the worker to return to typical daily living and work-related activities in a timely fashion. This return to activity is based on the stages of soft tissue healing and not on the worker s subjective reports of pain and symptoms. In its service contracts, the WCB has a provision for the use of concurrent therapies such as conditioning therapy. The use of the concurrent therapies needs to be evidencebased. For example, to improve an injured worker s overall fitness level, global conditioning is supported after four weeks off work from the time of injury. The evidence would not support loss of fitness levels if the worker is able to maintain some meaningful work. Only 10% of workplace injuries require advanced assessment and treatment. However, when an injured worker s recovery does not proceed as expected, the WCB can support care providers by arranging for advanced assessment, treatment, referrals, and other special requests. Assessment Team Reviews There is little benefit in continuing a current level of treatment when the injured worker is not improving; however, requesting an Assessment Team Review to identify and suggest more comprehensive treatment(s) or investigations have proven effective and efficient. Where improvement of a specific injury does not occur and more resources are required to resolve the injury, the WCB, or you (as the primary care provider) may request an Assessment Team review. The review will identify and suggest more comprehensive treatment or if further investigation is required. If you are not the primary care provider, talk to the worker s primary care provider to determine if further diagnostics or specialist consultations are required. Additional information about Assessment Teams can be found in Section 8: Advanced Assessment and Treatment. Specialists, Diagnostic Services, and Expedited Appointments If you - as the primary care provider - determine specialist and diagnostic services are required, you can contact the WCB to request help in arranging diagnostic services, specialist appointments or advanced treatment. If there is waiting list for the health service required by the injured worker (e.g., MRI, CT scan or other diagnostic; day surgery; and some types of specialist appointments), the WCB can often help arrange expedited service. 12
16 If you are not the primary care provider, the WCB will forward your request to the primary care provider to be completed. Additional information about specialists, diagnostic services and expedited appointments can be found in Section 8.2: Arranging Advanced Treatment. Referrals The WCB respects the knowledge and diagnostic acumen of health care providers who provide service to injured workers. Any health care practitioner who has privileges to request a specialist referral to arrange MRIs, CT scans or other diagnostic tests may do so. If you do not have these privileges, please contact the injured worker s physician to request the diagnostic or consultant referral. Special Requests Requests for unusual devices, treatment or diagnostic tests by any care provider may require discussion with a WCB Health Care Consultant. The WCB and WCB Health Care Consultants try to ensure that the approval of special requests are supported by sound clinical reasoning, or evidence supporting the use of the device to reach the goal of returning the injured worker to their pre-injury functional levels. For example, there is no evidence presently for the use of lumbar supports to treat acute low back pain. Therefore, these devices are not paid for by the WCB. 7.4 Evaluate Any Risks Involved in Return to Work In most cases, returning to accommodated work has a positive impact on the worker s recovery. However, sometimes a worker s injury or illness, or the effects of medication prescribed for the injury or illness, may impair judgment or balance and pose a safety risk to the worker or others. Chiropractors and physiotherapists should consider such impairments when identifying the functional abilities of a worker. 7.5 Communicate Functional Abilities In addition to the normal information about the recommended course of treatment and the expected recovery time, you will need to advise injured workers about their current functional abilities (also known as restrictions.) The primary care provider (if not you) should be aware of, and in agreement with, the worker s functional abilities. Usually, injured workers can return to work in some capacity if they are not hospitalized or housebound. Rather than authorizing absence from work, you should provide the injured worker with a list of current functional abilities that can be safely performed while taking into account the injury. This list of functional abilities should be shared with the employer (either talking directly with the employer or via the worker.) You should always assume that employers can and will accommodate the functional abilities of their injured worker. The list of functional abilities will be based, as much as possible, on objective clinical findings, the client s perception and the practitioner s expertise. Occasionally, objective measurement of the functional abilities is required. 13
17 The list should include: the frequency, duration and intensity (pounds, steps, length, etc.) of the activity; the postural positions the activity can be performed in; and the approximate period of time for which accommodated duties will be required. During primary treatment, the functional abilities are often determined by your knowledge of the injured tissue and what typical stresses the injury will be able to handle. As well, the injured worker s perception of their own functional abilities will add information to help you make appropriate decisions. Functional Testing Functional testing may be required to educate the worker, and ensure the recommended functional abilities are safe, when the worker s perception significantly differs from the conclusions that you came to as a result of physical examination and history. In situations where more than one component of functional testing is required to progress return to work, you should consider whether the resources available at the primary level are enough to resolve the injury. The injured worker may benefit from an Assessment Team review and access to more resources at a higher level of treatment. Return to work If the worker s employer has a return-to-work program in place, the injured worker may bring a copy of a return to work form to be filled out. This form may be used, but the WCB Practitioner s Return to Work (PRTW) form is preferred. Forward copies of the PRTW form, or the list of the worker s functional abilities to: the employer (via the worker or directly to the employer); the WCB; and the primary care provider (if not you). You may find that a telephone call to the employer at this time can clarify or answer any questions the employer has, which in turn, helps ensure all members of the integrated partnership are involved. Once the injured worker, or the practitioner, provides the employer with a PRTW or list of functional abilities, the employer can consult with the worker, care provider (if necessary), and union (if any) to determine if the worker s duties can be modified or other accommodations made to allow return to work. If the employer cannot accommodate the worker s functional abilities, then absence from work may be the only option (even though return to the workplace in any capacity has been shown to have positive effects on recovery). During each visit, you should review the list of functional abilities. As the worker s condition improves, you should: discuss any changes to these abilities with the worker; update the PRTW form or list of functional abilities, and provide this to the employer directly, or through the worker; forward a copy of these documents to the primary care provider (if not you) and the WCB. Injured workers are encouraged to forward copies of their PRTW or list of functional abilities to their employer because it encourages both parties to keep the dialogue open regarding accommodation. Continuing communication between the care provider, worker and employer is a vital part of successful recovery and return to work. 14
18 7.6 Report to the WCB Every work injury that needs health care must be reported to the WCB. Reports can be submitted by mail, fax or online. Under Section of the Saskatchewan Workers' Compensation Act, 1979, care providers do not require a signed release from the injured worker to submit reports to the WCB. Early and regular care provider reports are important to the worker and the WCB for two reasons: the WCB requires client health records to process claims and appeals; and the WCB may need to provide copies of reports to other health care providers (i.e., Assessment Teams, Treatment Centres and specialists) to help obtain the best possible assessments and treatments for injured workers. Questions that may arise from the injured worker, in regards to access of their health records by other parties, such as employers, in the event of an appeal, should be directed to the case manager. Submit reports online If you have a WCB billing number, you can apply for a business account that will allow you to access and submit WCB forms over the internet. To apply for an online business account or access forms: go to click on the icon on the home page following the instructions to either request an account or to access forms Please make sure your notes are typewritten if you use paper forms. See the appendices for paper copies of WCB reporting forms. Report Forms Use the following forms to provide information about treatment, functional recovery, and response to treatment. Please fill out reports completely and fax them to WCB as quickly as possible. The WCB cannot pay for illegible or incomplete reports. Self Reported Functional Outcome Measures (FOM) Administer the appropriate self reported Functional Outcome Measures (FOM) tests to WCB clients as soon as possible to help identify those who may be at risk for prolonged recovery and who would benefit from more intensive treatment. These tests include: o o o o Lower Extremity Functional Scale (LEFS) Neck Disability Index (NDI) Quick Dash and Work Module for upper extremities Roland Morris for backs Only the client's FOM score should be submitted to the WCB, not the form itself. The score is to be reported on the Initial Report form and Progress/Discharge Report form described on the next page. 15
19 Initial Report You are required to submit an Initial Report (either CHI for chiropractors or PTI for physiotherapists). The report should include the appropriate FOM score for all injuries, including those that do not result in time off work. Where the injured worker loses time from work because of an injury, the Initial Report provides confirmation of disability, which allows the WCB to arrange timely payment of benefits to injured workers. Prompt reporting is important to prevent financial hardship for the injured worker and family. See appendices for forms and relevant User Manuals. Progress and Discharge Reports A Progress Report (either CHP for chiropractors or PTP for physiotherapists), which includes the appropriate updated FOM score, should be completed after each block of treatments (six treatments for chiropractors and ten treatments for physical therapists) unless the worker has been discharged. If the injured worker has been discharged, the PTP should be completed within 7 days. See appendices for forms and relevant User Manuals. Return to Work Report Once a return-to-work plan has been agreed upon, submit a Practitioner's Return to Work Report (PRTW) to the WCB with copies to the injured worker, employer, and the primary care provider (if not you). The report confirms the hours of work and current functional abilities. Other Reports Copies of special reports (diagnostic, operative, etc.) should always be forwarded to the WCB. These reports provide the WCB with relevant information, and save the attending practitioner from preparing a separate report. Reporting Schedule Chiropractors are to complete a CHP report after every six treatments; physical therapists are to complete a PHP report after every ten treatments. Failure to report: can seriously delay an injured worker's claims process; may increase costs to employers; may result in delays or non-payment to the provider; and can negatively affect the implementation of treatment plans and ultimately delay the recovery of the injured worker. Reporting fees The WCB issues payment when the care provider invoices the appropriate fee (See Appendix XIII: Reporting Fees - Chiropractors and Appendix XIV: Reporting Fees Physical Therapists). There is a two-tier fee for Initial and Progress reports: fee for reports that include FOM scores (both professional associations deem FOM scores to be extremely helpful in ensuring the worker is progressing); a lower fee for those that do not include FOM scores. If more than one report is received for the same day, only one report fee is paid. Note: WCB reports and phone inquiries are billable items for WCB claims. 16
20 7.7 Monitor Return To Work (RTW) As the injured worker s condition improves, the chiropractor or physiotherapist should: revise the worker s functional abilities and convey this information in progress reports or subsequent return to work reports to: o o o the employer; the primary care provider (if not you); and the WCB. reassure the injured worker that some increase in discomfort is normal and expected during return to work (unless there are objective clinical signs to suggest injury progression;) discuss modifications to the return-to-work plan with other involved health care professionals; modify return-to-work plan if necessary, but do not stop return to work unless continuing presents a clear danger to the injured worker (rest from return to work rarely leads to improvement except immediately after acute injuries). 17
21 8. Advanced Assessment and Treatment You, as the primary care provider, or the WCB may ask for an Assessment Team review where: the worker is not working and has no confirmed return to work date; the expected recovery date has been exceeded; significant risk factors for chronic disability have been identified (See Appendix VIII); the worker continues in employment but has not returned to full duties and/or full hours of work after the work injury; an active treatment plan is not in place. The WCB established the following administration guidelines to help identify injured workers in need of advanced assessment and treatment. The WCB may automatically refer the injured worker for assessment when these time frames have been exceeded and the worker has not returned to work. Type of Injury Soft Tissue Injury (STI) Non-STI - Neck and Spine (fractures/surgeries) Non-STI - Upper Extremity (includes non arthroscopic surgery) Non-STI - Others (includes all non arthroscopic surgery) All arthroscopic surgeries Lower Extremity (fractures/surgeries) All other complex/multiple fractures Amputation (lower or complex) Spinal fusion Psychological Referral to Assessment 7 weeks 12 weeks 12 weeks 12 weeks 6 weeks 16 weeks 16 weeks 26 weeks 26 weeks 4 weeks Disability Duration Guidelines are available at under Care Provider Services. The WCB, in conjunction with the physiotherapy and chiropractic associations, have developed a guide for treatment of soft tissue injuries at the primary level. The guidelines within this document outline the typical number of treatment sessions, the duration of treatment and the parameters for when a worker should be referred for advanced assessment and possible treatment. The Soft Tissue Guidelines are available at under Care Provider Services. 8.1 Multidisciplinary Assessment The Assessment Team will confirm diagnosis and make recommendations appropriate to the worker s condition such as: further primary treatment (in rare cases), secondary or tertiary care; specialist and diagnostics services to occur consecutively or concurrently with other treatment; timeline for return-to-work planning, which may include an immediate return to work; an indication of whether the worker has pathology to permanently preclude their return to the job they held at the time of the injury. 18
22 Assessment Teams Assessment Teams are composed of multidisciplinary health care professionals at both secondary and tertiary levels. The WCB selects the appropriate Assessment Team based on the length of time the worker has been away from regular job duties and/or the presence of psychosocial and pain management issues. The WCB may add specialists to the Assessment Teams if there are issues involved that are beyond the scope of practice of the typical team (i.e., physician, chiropractor and physiotherapist). Mental health assessments are also arranged by the WCB, when appropriate. Assessment Reports The Assessment Team will forward: a summary report, within two days for secondary assessments and four days for tertiary assessments, of the assessment to the primary care provider, the chiropractor or physiotherapist (even if not acting as the primary provider), and to the WCB; a comprehensive report, within two weeks, of the assessment to the primary care provider, surgeon and the WCB only. The Assessment Team and the WCB will tell the worker that all reports have been sent to the primary care provider. The injured worker should arrange an appointment with the primary care provider to discuss the Assessment Team s report and any recommended changes to treatment and/or return to work. If the worker has not contacted the primary care provider (if not you) in the days immediately following the assessment, you should urge the worker to do so. 8.2 Arranging Advanced Treatment If you, as the primary care provider, agree to a recommendation for secondary or tertiary treatment, you may either: make a direct referral to a WCB approved clinic; and ask the WCB to make a referral or appointment on your behalf. Where specialist/diagnostic appointments are recommended, the WCB will offer to arrange these. You should encourage the injured worker to consider advanced treatment as similar to work, and that his or her full effort, promptness and attendance are expected. When a referral is made to a treatment centre, the centre will contact the worker to: arrange for intake within one week of referral date; and advise the worker of the daily time commitment required (most secondary programs involve three to five hours of treatment per day while tertiary programs require four to six hours. here the work site can be used to make functional progressions, less treatment centre time may be indicated). 19
23 Once the worker is in treatment, secondary and tertiary treatment centres will: deliver the treatment recommended by the Assessment Team; provide reports to the primary care provider regarding progress, including functional gains; establish a return-to-work plan using functional testing as one indicator of ability. advise the primary care provider of the details of the plan; monitor the return-to-work plan, working closely with the worker, employer, WCB and primary care provider; provide a Physical/Functional Capacity Evaluation (PFCE) that catalogues residual capacities and guides re-employment planning where permanent restrictions to the pre-injury job exist. Successful outcomes are achieved where all care providers support the functional rehabilitation approach even in the presence of subjective complaints. 20
24 9. Return to Work (RTW) Total disability is rare. Most injured workers benefit from transitional return to work (see below) while they recover. Being at work: helps maintain their self-esteem and connection with the workplace; helps alleviate concerns about job security; allows continuing contributions to workplace benefit and pension plans; provides activity that enhances the healing process (See: Recovery and Return to Work for Injured Workers brochure). 9.1 Employers Have a Duty to Accommodate Saskatchewan Human Rights legislation requires all employers to accommodate injured workers to allow them to return to work as soon as medically safe. However, in the absence of a collective agreement, the Saskatchewan Labour Standards only protects a worker s employment for 26 weeks of absence due to work injury. The list of functional abilities you supply is crucial to the employer s ability to accommodate the injured workers as soon as possible to avoid job loss and other negative consequences of absence from the workplace. 9.2 Return to Work Process Early return to work helps maintain the injured worker s link to the workplace and serves a therapeutic role. Return to work should be incorporated into the treatment plan as soon as possible by completing a Practitioner s Return to Work Report (PRTW) to define the worker s abilities, so the employer can arrange for modified duties. There are three return-to-work plans that can be used and adapted as the worker s condition improves: Return-to-Work Plan (RTW) This program is the documented, planned process implemented by the employer for managing work absences due to injury/illness related disabilities. It can include modified jobs, tasks, equipment, hours of work, and work schedule based on medical recommendations and work requirements. The program is designed to assist the employee s rehabilitation. Transitional Return-to-Work Plan (TRTW) This plan includes any combination of a gradual increase in hours of work and/or work activities designed to return the disabled worker to the job they had at the time of their injury. Where appropriate, TRTW is followed by full return to the job the worker held at the time of the injury. This plan may involve two components often referred to as Transitional Return to Work (first component) and Graduated Return to Work (second component): o Transitional Return to Work The first component, usually implemented as soon as possible after the injury, typically does not progress the worker s duties in the work place. This initial component of the plan is to ensure the worker returns to the workplace to help maintain their self-esteem and connection with the workplace, help alleviate concerns about job security, and allow continuing contributions to workplace benefit and pension plans. 21
25 o Graduated Return to Work The second component is designed to progressively increase the worker s duties and/or capacity in the workplace. This component uses the functional activities within the workplace to increase the stress on the injured tissue, thus allowing for continual rehabilitation of the injury. At the primary level, it is unusual for this component to take longer than four weeks. Typically, it can be completed in a much shorter time frame, dependant on the injury and the pathology to the injured tissue. Maintenance Return-to-Work Plan This plan includes any combination of hours of work and/or work activities designed to maintain the function of a disabled worker awaiting treatment and/or surgery. 9.3 Return to Work with Permanent Impairment Full return-to-work planning will normally involve the employer, injured worker, and a union representative if requested by the worker. This generally occurs within a tertiary treatment program and involves a Physical/Functional Capacity Evaluation (PFCE). The tertiary treatment team will establish and monitor a RTW plan, progressing up to and including permanent return to accommodated work. Vocational assistance may be available for injured workers who cannot return to their previous jobs. The goal is to return the injured worker to their previous earning capacity. The WCB is not responsible for finding jobs for workers with permanent restrictions resulting from work injuries, but may help with job searches, resumes and training. 9.4 Preventive Job Change Regardless of the risk of re-injury, the WCB s responsibilities end when the worker has recovered from the work injury sufficiently to return to the job they had before their injury. Preventative job change is beyond the mandate of the WCB and is a point of discussion for the worker and employer. 22
26 10. Factors Affecting RTW/Function There are many factors that may affect the worker s return to work/function. Some factors may be related to the nature of the injury, others are not. For a worker whose disability is not explained by the nature of the injury, an extended recovery time may be the first sign of chronic disability. Timely health care, return to work and vocational services are vital to the prevention of chronic disability. The first few months are critical; the risk of an injured worker becoming chronically disabled increases rapidly with time unrelated to the nature of the injury. WCB treatment programs are available for injured workers at increased risk of prolonged recovery or chronic disability. The following may help care providers identify those workers who may need these services Symptoms of Increased Risk of Chronic Disability The following symptoms may help you identify those workers who may show an increased risk of chronic disability: diminished or no interest in actively participating in their recovery; a negative attitude about returning to work; believe they are disabled and that they are entitled to financial benefits, whether they are receiving them or not; or complaints that cannot be verified, and that are out of proportion to the nature or severity of their injury. Experienced health care professionals will often have intuitive concerns about their patients. These gut feelings should not be ignored even in the absence of other risk factors. These concerns should be reported to the WCB as early as possible so arrangement for advanced assessment and treatment can be made. For more information on the risk factors for chronic disability, see Appendix VIII: Risk Factors for Chronic Disability. See Section 8: Advanced Assessment and Treatment for information on the services available for workers at increased risk Employment and Personal Factors For a list of positive and negative employment and personal factors that may affect an injured workers return to work, see Appendix XV: Positive and Negative Factors for RTW/Function. 23
27 11. Permanent Functional Impairment (PFI) When an injured worker has reached maximum improvement (MMI) and a part of their body still does not function as it did before the injury, they may be entitled to a permanent functional impairment (PFI) award. PFI Award A PFI award is a monetary payment based on a percent of whole body impairment. The award s dollar amount is a percentage of amounts established under The Workers Compensation Act, The rating is done by WCB Medical Professionals based on the AMA s Guides to the Evaluation of Permanent Impairment. The rating is a percentage determined by review of the file, including all medical records and examination findings provided by the injured worker s community-based caregivers. Please note that an impairment rating is different than a disability rating: A functional impairment is a deviation from normal in a body part or system and its functioning. Disability arises out of the interaction between impairment and external requirements such as the capacity to meet personal, social or occupational demands, or statutory or regulatory requirements. A PFI payment does not affect any wage-loss, vocational or other benefits the worker may receive. Independence Allowance The WCB may also provide an allowance to help qualified impaired workers live independently. This allowance may cover expenses such as lawn care, snow shovelling and transportation. 12. Workers with Injury-Related Disability Permanent impairments can lead to disabilities that have serious implications for injured workers and their families. To minimize the effects of these disabilities, you (as the primary care provider) should encourage injured workers to: accept accommodated employment with the employer, as established and monitored by the treatment team; cooperate with WCB vocational services in cases where the employer cannot accommodate. 24
28 13. Conclusion In addition to the enormous economic and social impact, work-related illness/injury can devastate individuals, their families, and their workplace. To be an effective health advocate for the injured worker, and to lessen the burden of work injuries to society, the treating chiropractor or physical therapist will need to address many modifiable factors to assist in an early and safe return to-work/function. Integrating return to work with clinical care is of primary importance in returning injured workers to work/function and overall well being. 25
29 14. Appendices Appendix I: Compensation Benefits for Injured Workers Appendix II: Appealing a WCB decision Appendix III: Chiropractor s Initial Report (CHI) & User Manual Appendix IV: Chiropractor s Progress/Discharge Report (CHP) & User Manual Appendix V: Physiotherapist s Initial Report (PTI) & User Manual Appendix VI: Physiotherapist s Progress/Discharge Report (PTP) & User Manual Appendix VII Practitioner s Return to Work Report (PRTW) Appendix VIII: Risk Factors for Chronic Disability Appendix IX: Lower Extremity Functional Scale (LEFS) Appendix X: Neck Disability Index (ND) Appendix XI: Quick Dask and Work Module for Upper Extremities Appendix XII: Roland Morris for Backs Appendix XIII: Reporting Fees Chiropractors Appendix XIV: Reporting Fees Physiotherapists Appendix XV: Positive and Negative Factors for RTW/Function Appendix XVI: Glossary and Abbreviations Appendix XVII: WCB Contact Information 26
30 Appendix I: Compensation Benefits for Injured Workers When the WCB accepts a worker s injury claim that worker may be entitled to a variety of benefits as set out in WCB legislation and policy. These benefits may include: Wage Loss Workers, who are injured at work and off work beyond the day they were injured, may be entitled to receive wage-loss benefits. In most cases, this benefit may be equal to 90 per cent of their probable take-home pay. Benefit payments usually begin on the day of first wage loss after the date of injury, with the initial payment normally made in 14 days or less. Permanent Impairment If a work injury results in a permanent impairment such as the loss of a limb, the worker may receive a lump sum payment. This payment is in addition to wage-loss compensation, if applicable, or in some cases, even if there was no wage- loss. The lump sum is dependent on a percentage of impairment. If a work injury results in a severe functional impairment, the WCB may also provide an annual independence allowance to assist in maintaining an independent lifestyle. Long-Term Benefits Wage-loss benefits may continue for as long as the worker experiences total or partial loss of earning capacity due to the injury. Benefits usually end at age 65. To protect wage-loss benefits from the effects of inflation, they are reviewed annually based on changes in the Consumer Price Index. Death Benefits In cases where a worker dies on the job, the WCB makes an immediate lump sum burial payment, and may pay the cost of transportation of the deceased to their home within Canada. In addition, the WCB pays compensation benefits to the surviving spouse and any dependent children. Benefits to Surviving Spouse A dependent spouse receives monthly benefits equal to 90 per cent of the deceased worker's probable net earnings. These benefits are payable for five years, or until the youngest child reaches age 16, regardless of other earnings. If there is a dependent child in full-time attendance at a secondary or post-secondary educational institution, benefit payments continue until that child is 18. Benefits for Dependent Children At age 18, each dependent child who is in full-time attendance at a secondary or post-secondary school will be eligible to receive a monthly allowance plus an amount equal to the cost of tuition, books and other required educational fees. The WCB will pay a dependent child s educational fees, plus allowance and other expenses as specified above, for a maximum of three years between the ages of 18 and 25. Compensation to survivors may be extended beyond the above time period, depending on individual circumstances. Relocation WCB benefits, health care and rehabilitation may be affected if the worker relocates. View the Voluntary Relocation Outside Canada Fact Sheet, available from under Publications.
31 Appendix II: Appealing a WCB decision Both workers and employers can ask for a review or appeal of any WCB decision. Worker Appeals If an injured worker disagrees with a WCB decision on a claim, they can: ask the WCB staff member who made the decision to review their file(many disputes can be resolved at this point); contact the WCB s Fair Practices Officer, who will review the file and may make recommendations; contact the Saskatchewan Office of the Worker s Advocate for assistance. The WCB also provides an appeal process for workers. There are three levels of appeal that must be accessed consecutively: Appeal Department Review The worker can ask that the Appeals Department review their claim file. The Appeals Department should provide a decision within 30 days. The WCB Operations Division must follow the instructions outlined in the appeal decision. Appeals Officers will review the claim file and gather any additional information they feel is necessary to come to a fair and reasonable resolution. Board Member Review If the worker disagrees with the decision of the Appeals Officer, they may request a further review by the WCB Board Members, giving reasons for the review and documentation to support the request. In most cases, this is the final level of appeal. Medical Review Panel When a bona fide health care question exists, the worker may request a review by a Medical Review Panel. (A bona fide health care question exists when a physician or chiropractor disagrees with a position taken by the WCB. This results in two conflicting health care positions). A Medical Review Panel consists of a Chair selected by the WCB, and the worker s choice of either: o two specialists o a specialist and a chiropractor The decision of the Medical Review Panel is final and binding on all parties. To initiate a Medical Review Panel, the worker s primary physician or a chiropractor must sign an enabling certificate outlining which of WCB s medical positions the care provider disagrees with and setting out the reasons why. Enabling certificates are available from the WCB's Medical Services or Board Services departments. Employer Appeals Employers who disagree with a WCB decision on a worker s injury claim can: ask the WCB staff member who made the decision to review the file (many disputes can be resolved at this point); contact the WCB s Fair Practices Officer, who will review the file and may make recommendations; follow an appeal process for employers, which is similar to the process described for workers above. There are two levels of appeal that can be accessed consecutively, the Appeal Department Review and Board Members Review.
32 Appendix III: Chiropractor s Initial Report (CHI) & User Manual The Chiropractor s Initial Report (CHI) and CHI User Manual are found on the following pages. The screen shot of the interactive CHI form is one page long; the CHI User Manual is two pages long. NOTE: If you wish to download or access the interactive CHI form, please go to Forms & Publications tab at
33
34 CHI USER MANUAL Chiropractor s Initial Report WCB Claim # Clinic # Chiro # Personal Health # Phone # Fax # Date of Birth Phone # Chiropractor s Name, Address, Postal code Employer Name Worker Name, Address, Postal Code Print/stamp/sticker Clinic Name Print/stamp/sticker (The employer to be included in above should be the pre-injury employer. It is understood that there may be some instances where the current employer is different from the pre-injury employer. It is requested that this section only include the pre-injury employer) 1. Date of injury: d/m/y 2. Date of initial Exam: d/m/y 3. Part of Body Injured: ( i.e. Shoulder, neck, leg) 4. Diagnosis: (Be specific i.e. Grade 2 LBP) 5. Mechanism of injury: (Where possible please be as specific as possible) 6. Subjective complaints: (Include quantifiable measures where possible i.e. Numeric pain scale rating) 7. Objective Findings: (Include quantifiable measures where possible i.e. Range of motion, straight leg raise testing, manual muscle testing, deep tendon reflex testing.) 8. Investigations ordered: xray other ( If previous pertinent diagnostic reports are available attach to CHI or CHP) 9. Assessment of recovery status (0-10): 0 = none, 10 = preinjury (The assessment of recovery is a measure that asks the provider to summarize available information to provide an estimate of the expectation of recovery within typical primary timelines. The clinician is asked to incorporate clinical findings, self-report measure change, objective functional change where testing is appropriate as well as possible psychosocial issues. A score between 0 and 10 representing no recovery and 10 representing recovery to pre-injury status is established. This score will represent the practitioners assessment of the complexity of this worker on initial presentation and potential for recovery.) 10. Intensity Score: 0 1 (An Intensity score is the Chiropractor s clinical opinion based on the case history and physical examination whether given a normal primary treatment program the injured worker will make a successful recovery = 0. A high intensity or complex case which may require more multidisciplinary or comprehensive primary treatment for a successful recovery = 1). 11. Treatment Plan: Physical Therapist* Massage* Specialist* Hospitalized* Education Biomechanical Electrophysical Regional conditioning, Supervised Home Supervised global conditioning Transitional RTW *Please name(med., caregiver) (This section is meant to communicate services that you have included in your treatment plan. Also, please identify if you are aware of other caregivers who are involved in the care of the worker even if you didn t refer to these practitioners.) 12. Frequency of treatment: per week 13. Expected number of weeks to discharge (This should represent the total expected number of weeks to discharge) 14. Have you advised the patient to be off work due to the injury Yes No (if yes, complete #15 22) If NO, is the patient to be working with restrictions Yes No (if yes, complete #15 22) 15. Are you aware of previous injury/treatment for this area No Yes Date(s): (This is dependant on the worker s recall of previous injuries. Therefore, the year of injury is satisfactory. Please include details of his/her previous injuries in the comments section including time loss, type and length of treatment.)
35 16. Self Report (score) Roland Morris Quick Dash QD Work module NDI LEFS (The self-report measures have been developed based on instruments that were reviewed at the WCB Outcome Measures Workshop. The instruments chosen are based on body parts involved i.e. Roland Morris for thoracic and lumbar spine, Quick Dash for upper quadrant, and NDI for cervical spine and LEFS for lower quadrant injuries. It is mandatory to use the instruments described above. Please include the raw score for the initial measure when providing the information about the self-report measure) 17. Estimated physical restrictions include lifting (~ # of lbs.) pushing/pulling (~ # of lbs) reaching overhead reaching turning walking stairs ladders standing (~ # of hrs) sitting (~ # of hrs) environment other (Provide the restrictions based on best clinical judgment and available information i.e. functional testing where appropriate. It does not ask for confirmed capacities but asks the practitioner to provide functional levels based on available information so that return to work parameters can be established. ) 18. Effects of the injury may affect work activity for: # of days < RTW Date (Based on your examination and management/treatment plan when would the worker be capable of Transitional or RTW) 19. Has transitional RTW been discussed with the worker Yes No the employer Yes No 20. Has a transitional RTW been arranged Yes, TRTW start date No (Explain barriers in Comments) 21. Are there any specific safety or medication concerns in a TRTW No Yes (If Yes, explain in Comments) 22. Comments (Please use the comments section to include any concerns with the severity of injury, treatment, psychosocial or work issues which may delay recovery). Signature Date: Copy to Revised
36 Appendix IV: Chiropractor s Progress/Discharge Report (CHP) & User Manual The Chiropractor s Progress/Discharge Report (CHP) form and CHP User Manual start on the next page. The screen shot of the interactive CHP form is one page long. The CHP User Manual is two pages long. NOTE: If you wish to download or access the interactive CHP form, please go to Forms & Publications tab at
37
38 CHP USER MANUAL Chiropractor s Progress/Discharge Report WCB Claim # Clinic # DC # Personal Health # Phone # Fax # Date of Birth Phone # Chiropractor s Name, Address, Postal code Employer Name Worker Name, Address, Postal Code Print/stamp/sticker Clinic Name Print/stamp/sticker (Please note: All sections need to be filled out to insure reimbursement.) REQUEST FOR EXTENSION DENIED CES/CM Date (Note that case management in consultation with the Chiropractic Consultant when appropriate will be considering assessment of recovery and duration, frequency of treatments as well as other clinical features in approving further treatment at a primary level or if a decision will be made to proceed with a multi-disciplinary assessment.) 1. Examination date: d m y 2. Current Diagnosis: (Be as specific as possible) 3. Body areas currently being treated (List body areas presently under treatment and related to the compensable injuries) 4. Subjective Complaints: (Use quantifiable measures where possible i.e. Numeric pain scale rating) 5. Objective Findings: (Use quantifiable measures where possible( i.e. Range of motion, straight leg raise testing, manual muscle testing, deep tendon reflex testing.) 6. Results of diagnostics since previous report: (Please attach all pertinent diagnostic reports to the form if not already done) 7. Assessment of recovery (0-10): initial current 0 = No recovery, 10 = recovered to preinjury Explain any delay in recovery: (The assessment of recovery is a measure that asks the provider to summarize available information to provide an estimate of the expectation of recovery within typical primary timelines. The clinician is asked to incorporate clinical findings, self-report measure change, objective functional change where testing is appropriate as well as possible psychosocial issues. A score between 0 and 10 representing no recovery and 10 representing recovery to pre-injury status is established. This score will represent the practitioners assessment of the complexity of this primary patient s presentation and potential for recovery.) 8. Have you advised the patient to be off work due to the injury: yes no (if yes, complete #10 21) If no, is the patient to be working with restrictions yes no (if yes, complete #10 21) 9. Discharged: Yes DD MM YY (Include the date of discharge) no, requires a Request for Extension of Treatment (complete #10 21).
39 10. Self Report (initial/current) Roland Morris / Quick Dash / QD Work module / NDI / LEFS / (The self-report measures have been developed based on instruments that were established at the Outcome Measures Workshop. The instruments chosen are based on body parts involved i.e. Roland Morris for thoracic and lumbar spine, Quick Dash for upper quadrant, and NDI for cervical spine and LEFS for lower quadrant injuries. It is mandatory to use the instruments described above. Please include the raw score for the initial and the current measure when providing the information about the self-report measure.) 11. Treatment Plan: physical Therapist* massage* specialist* hospitalized* education biomechanical electrophysical regional conditioning, supervised home supervised global conditioning transitional RTW *Please name(med., caregiver) (This section is meant to communicate services that you have included in your treatment plan. Also, please identify if you are aware of other caregivers who are involved in the care of the worker even if you didn t refer to these practitioners.) 12. Frequency of treatment: per week 13. Expected number of weeks to discharge: 14. Would you like WCB to arrange/expedite diagnostic specialist assessment type/name (In the comments section specify type of diagnostic or specialist that you are requesting. Also secondary or tertiary assessment.) 15. Are you aware of other health or non-health factors affecting recovery no yes (if yes, add to comments) (Are there any red flags - diabetes, arthritis, cardiovascular disease or yellow flags - depression, family issues, monetary which may affect recovery.) 16. Estimated restrictions include lifting (# of lbs.) pushing/pulling (# of lbs) reaching overhead reaching turning walking stairs ladders standing (# of hrs) sitting (# of hrs) environment other (Provide the restrictions based on best clinical judgment and available information i.e. functional testing where appropriate. It does not ask for confirmed capacities but asks the practitioner to provide functional levels based on available information so that return to work parameters can be established. ) 17. The effects of the injury may affect activity for: # of days if < 8 days RTW Date (Based on your examination and management/treatment plan when the worker would be capable of Transitional or RTW.) 18. Has transitional RTW been discussed with the worker: Yes No the employer Yes No 19. Has a transitional RTW been arranged: Yes TRTW start date No (Explain barriers as to why the worker could not start transitional work in comments section.) 20. Are there any specific safety or medication concerns in a TRTW No Yes (If yes, explain in comments) 21. Comments: (Please use the comments section to include any concerns with the severity of injury, treatment, psychosocial or work issues which may delay recovery.) Signature: Date Copy to Revised 02/08
40 Appendix V: Physiotherapist s Initial Report (PTI) & User Manual The Physiotherapist s Initial Report (PTI) and PTI User Manual start on the next page. The screen shot of the interactive PTI form is one page long. The PTI User Manual is two pages long. NOTE: If you wish to download or access the interactive PTI form, please go to Forms & Publications tab at
41
42 PTI USER MANUAL Physiotherapist s Initial Report WCB Claim No Clinic # PT s # Personal Health # Phone # Fax # Date of Birth Phone # Employer Name Physiotherapist s Name, Address, Postal Code Worker Name, Address, Postal Code Print/stamp/sticker Clinic Name Print/stamp/sticker (The physical therapist will not have an individual number. Leave this blank. The clinic billing number should be filled in. The employer to be included in above should be the pre-injury employer. It is understood that there may be some instances where the current employer is different from the pre-injury employer. It is requested that this section only include the pre-injury employer) 1. Date of injury: dd/mm/yy 2. Date of initial Exam dd/mm/yy 3. Part of Body Injured 4. Diagnosis 5. Mechanism of injury (Where possible please be as specific as possible) 6. Subjective complaints (Include quantifiable measures where possible i.e. Numeric pain scale rating) 7. Objective Findings (Include quantifiable measures where possible i.e. Range of motion, straight leg raise testing, manual muscle testing, deep tendon reflex testing.) 8. Treatment goals (Please use goals that are functional including return to work) 9. Assessment of recovery status (0-10) (0= no recovery, 10=recovered to preinjury) (The assessment of recovery is a measure that asks the provider to summarize available information to provide an estimate of the expectation of recovery within typical primary timelines. The clinician is asked to incorporate clinical findings, self-report measure change, objective functional change where testing is appropriate as well as possible psychosocial issues. A score between 0 and 10 representing no recovery and 10 representing recovery to pre-injury status is established. This score will represent the practitioners assessment of the complexity of this primary worker s presentation and potential for recovery.) 10. Intensity Score: (0= An injured worker who displays medical and psychological factors that will allow successful outcome with average treatment resources. 1: An injured worker who requires a high level of complex treatment programming to achieve a successful outcome with average treatment resources.) 11. Treatment Plan Chiropractic Massage Biomechanical Electrophysical Regional conditioning, Supervised Home Supervised global conditioning Transitional RTW Other (This section is meant to communicate services that you understand to be part of the current treatment plan. Also, please identify if you are aware of other caregivers who are involved in the care of the worker even if you didn t refer to these practitioners.) 12. Frequency of treatment: per week 13. Expected number of treatments to discharge (This should represent the total expected number of treatments to discharge) 14. Have you advised the patient to be off work due to the injury Yes No If NO, is the patient to be working with restrictions Yes No 15. Are you aware of previous injury/treatment for this area No Yes Date(s): (This is dependent on the worker s recall of previous injuries. Therefore, the year of injury is satisfactory.)
43 16. Self Report (score) Roland Morris Quick Dash QD Work module NDI LEFS (The self-report measures have been developed based on instruments that were reviewed at the Outcome Measures Workshop in May The instruments chosen are based on body parts involved i.e. Roland Morris for thoracic and lumbar spine, Quick Dash for upper quadrant, and NDI for cervical spine and LEFS for lower quadrant injuries. It is mandatory to use the instruments described above. Please include the raw score for the initial measure when providing the information about the self-report measure) 17. Restrictions Subjective Measured lifting (# of lbs.) pushing/pulling (# of lbs) reaching overhead reaching turning walking stairs ladders standing (# of hrs) sitting (# of hrs) environment other Client and practitioner agreed Yes No (Explain in comments) (Use the boxes above to indicate if the restrictions that are provided are based on functional testing (where appropriate) or by client perception of function in combination with clinical judgment. If you have already advised that the worker is not suitable for work of any kind at this time (question 14), then the restriction sections should be left blank. Your rationale for indicating the worker s inappropriateness for return to work of any kind should be included in the comments section.) 18. Effects of the injury may affect work activity for: # of days < RTW Date 19. Has a RTW been discussed with the worker Yes No the employer Yes No 19. Has a transitional RTW been arranged Yes, TRTW start date No (Explain barriers in the comments section) 20. Are there any specific safety concerns in a TRTW No Yes (If Yes, explain in the comments section. If there are concerns expressed by the physical therapist regarding medication, a discussion between the physical therapist and physician regarding return to work issues should be initiated and should be commented on in the comments section below) 21. Comments 22. Signature Date: Copy to Revised 02/2008
44 Appendix VI: Physiotherapist s Progress/Discharge Report (PTP) & User Manual The Physiotherapist s Progress/Discharge Report (PTP) and PTP User Manual start on the next page. The screen shot of the interactive PTP form is one page long. The PTP User Manual is two pages long. NOTE: If you wish to download or access the interactive PTP form, please go to Forms & Publications tab at
45
46 PTP USER MANUAL Physiotherapist s Progress/Discharge Report WCB Claim No Clinic # PT s # Personal Health # Phone # Fax # Date of Birth Phone # Employer Name Physiotherapist s Name, Address, Postal Code Worker Name, Address, Postal Code Print/stamp/sticker Clinic Name Print/stamp/sticker (Please note: All sections need to be filled out where appropriate to insure reimbursement for the PTP form.) REQUEST FOR EXTENSION DENIED CES/CM Date (Note that case management will be considering assessment of recovery and duration, frequency of treatments as well as other features of recovery in approving further treatment at a primary level or if a decision will be made to proceed with a multi-disciplinary assessment.) 1. Current Diagnosis (Be as specific as possible) 2. Body areas being treated (Be as specific as possible) 3. Subjective Complaints (Use quantifiable measures where possible i.e. Numeric pain scale rating) 4. Objective Findings (Use quantifiable measures where possible i.e. Range of motion, straight leg raise testing, manual muscle testing, deep tendon reflex testing.) 5. Assessment of recovery (0-10) 0 = No recovery, 10 = recovered to preinjury Explain any delay in recovery (The assessment of recovery is a measure that asks the provider to summarize available information to provide an estimate of the expectation of recovery within typical primary timelines. The clinician is asked to incorporate clinical findings, self-report measure change, objective functional change where testing is appropriate as well as possible psychosocial issues. A score between 0 and 10 representing no recovery and 10 representing recovery to pre-injury status is established. This score will represent the practitioners assessment of the complexity of this primary patient s presentation and potential for recovery.) 6. Discharged date: (Include the final date of treatment. There is no longer a discharge report that is separate from the progress report.) 7. Restrictions Subjective Measured lifting (# of lbs.) pushing/pulling (# of lbs) Reaching overhead reaching turning walking stairs ladders standing (# of hrs) sitting (# of hrs) environment Other (Use the boxes above to indicate if the restrictions that are provided are based on functional testing (where appropriate) or by client perception of function in combination with clinical judgment. If it is your clinical opinion that the worker is not suitable for work of any kind at this time, then the restriction sections should be left blank. Your rationale for indicating the worker s inappropriateness for return to work of any kind should be included in the comments section) 8. Have you advised the patient to be off work due to injury Yes No (If Yes, complete #9-18) If NO, is the patient to be working with restrictions Yes No (If Yes, complete #9-18)
47 9. Self Report (initial/current) Roland Morris / Quick Dash / QD Work module / NDI / LEFS / (The self-report measures have been developed based on instruments that were established at the Outcome Measures Workshop in May The instruments chosen are based on body parts involved i.e. Roland Morris for thoracic and lumbar spine, Quick Dash for upper quadrant, and NDI for cervical spine and LEFS for lower quadrant injuries. It is mandatory to use the instruments described above. Please include the raw score for the initial and the current measure when providing the information about the self-report measure.) 10. Treatment Plan Chiropractic Massage Biomechanical Electrophysical Regional conditioning, Supervised Home Supervised global conditioning RTW Other 11. Frequency of treatment: per week 12. Expected number of week to discharge. 13. Are you aware of other health or non-health factors affecting recovery No Yes (If Yes, add to Comments) 14. The effects of the injury may affect activity for: # of days < RTW Date (The expectation is for an estimation based on the available information at the time of the progress report) 15. Has a return to work plan been discussed with the worker Yes No the employer Yes No 16. Has a return to work plan been arranged: Yes RTW start date No (Explain barriers in Comments) 17. Are there any specific safety concerns in a RTW No Yes (If yes, explain in comments) 18. Comments (This section is included to expand on issues related to the return to work, i.e. work place issues, psychosocial issues or non-compensable issues delaying recovery, concerns regarding safety related to medications). Signature: Date Copy to Revised 02/2008
48 Appendix VII: Practitioner s Return to Work Report (PRTW) The Practitioner s Return to Work Report starts on the next page. The screen shot of the interactive PRTW form is one page long. The PRTW User Manual is two pages long. NOTE: If you wish to download or access the interactive PRTW form, please go to Forms & Publications tab at

49
50 Scarth Street Phone: Toll Free: Regina SK S4P 4L1 Fax: Toll Free: User Manual for Practitioner s Return to Work Report (PRTW) Return to work (RTW) is a documented plan/strategy to accommodate an injured worker with temporary restrictions while receiving treatment or rehabilitation. The return-to-work plan is a collaboration between the worker, the employer, the care provider and the WCB. The return to work will be monitored and progressed by the care providers based on objective clinical findings. It should have a defined start and end point that may include a combination of a gradual increase in hours of work and/or work activities designed to return the injured worker to the pre-injury job. It is expected that the majority of RTW programs will be less than four weeks in duration, unless there are unusual circumstances such as unusual shift length, heavy to very heavy industrial DOT, a highly repetitive job or a post-surgical worker. A RTW Plan should include: The week it should start, the total hours of work, the days, and a list of restrictions to job duties; and Any comments or concerns regarding job duties in the comments section. A RTW may exceed four weeks on occasion. After the four weeks have been completed, the practitioner should: Submit the remainder of the RTW for the final stages; If a graduated RTW of greater than 4 weeks is required, provide a rationale in the restrictions section below; and Provide an anticipated end date. When a RTW plan exceeds 4 weeks, please indicate the actual week when the worker can be expected to return to work, i.e., week 5, 6, 7. This is particularly important when the return to work is exceeding 4 weeks because the worker s case manager uses this information for payment of wage loss. Practitioner s Return to Work Report WCB Claim No.: Clinic # Billing # Personal Health # Phone # Fax # Date of Birth Phone # Practitioner s Name, Address, Postal Code Clinic Name Employer Name Worker Name, Address, Postal Code Memo to: (employer/primary practitioner/wcb) Please forward any requests for changes to the RTW plan to the therapist, who will monitor the worker s progress, evaluate any suggested changes, adjust the RTW plan if required, and forward amendments to all parties. The WCB will also adjust the level of income replacement as the worker s duties and hours of work change. Return to Work Start Date: DD/MM/YY Anticipated End Date: DD/MM/YY Employer Contact Name: Contact Phone # Cont d
51 Calendar of Hours and Restrictions Month Sunday Monday Tuesday Wednesday Thursday Friday Saturday Week Date 21/10/07 One Hrs Restrictions: Mr. Smith should avoid lifting greater than 25 lbs. and above shoulder activity. Comments: Mr. Smith requires alternate modified work than his construction job as a framer. He should be accommodated in the shop until he begins his GRTW. Week Two Date 28/10/07 Hrs Restrictions: Mr. Smith can begin lifting above shoulder while under treatment. Comments: Continue accommodation in the shop while under treatment. Week Three Date Hours Restrictions: Comments: Please explain need for RTW longer than 2 weeks Week Four Date Hrs Restrictions: Comments: Please explain need for RTW longer than 2 weeks Signatures: Care provider may sign all three as verification that all parties are aware of, and have agreed to, the RTW plan. Revised 02/08 22
52 Appendix VIII: Risk Factors for Chronic Disability Injured Worker Age older workers may have difficulty finding jobs because of their age. Place of residence rural workers may have more difficulty finding other employment if they are unable to return to their pre-injury jobs. Education jobs with fewer educational requirements usually involve more physical activity. Language English as a second language may limit their ability to find work. Lack of mobility if their spouse has a job in the community, or if they have lived there a long time, they may not want to move and this will limit their ability to find work. Opinion as to the degree of disability is out of proportion to the nature of the injury. History of drug or alcohol abuse. Financial problems reduce the ability to focus on return to work as a priority. Family problems such as separation, divorce, serious illness or death. Injured worker cannot be reached when Case Manager calls or tries to arrange a meeting. Injured worker relies on a third party (spouse or parent) to communicate with the WCB. Injured worker has a significant number of prior claims with the WCB. Employment Employment history length of employment with employer of record, seasonal work, issued a layoff, uncertainly about having a job to return to. Nature of employment no light duties available, employer small in size. History of poor performance on the job employer doesn t want worker to return to work. Excuses for not returning to work no transportation, unreasonable demand for light duties. Little or no contact with employer after injury. Rate of compensation provides a sense of security, especially if pre-injury income was uncertain, sporadic or seasonal. Dissatisfaction with the job. Lack of job opportunities because of economic conditions within usual field of employment. Health Period of disability exceeds expected recovery time for the injury. Injured worker has other health problems at the same time as the injury. Lack of physical findings on health care reports to support a delay in returning to work. Injured worker frequently changes primary care providers. Past related problems in same body area of the injury. Expansion or change in location of symptoms from those of the original injury. Injured worker does not participate in treatment, misses appointments, makes excuses for nonattendance, and has only vague recollection of primary care provider s advice. 23
53 Appendix IX: Lower Extremity Functional Scale (LEFS) Go to the next page to see the Lower Extremity Functional Scale, which you can print off to use with a patient. The Lower Extremity Functional Scale is one page long. 24
54 THE LOWER EXTREMITY FUNCTIONAL SCALE We are interested in knowing whether you are having any difficulty at all with the activities listed below because of your lower limb problem for which you are currently seeking attention. Please provide an answer for each activity. Today, do you or would you have any difficulty at all with: (circle one number on each line) ACTIVITIES a. Any of your usual work, housework, or school activities. b. Your usual hobbies, recreational or sporting activities. Extreme Difficulty or Unable to Perform Activity Quite a Bit of Difficulty Moderate Difficulty A Little Bit of Difficulty No Difficulty c. Getting into or out of the bath d. Walking between rooms e. Putting on your shoes or socks f. Squatting g. Lifting an object, like a bag of groceries from the floor. h. Performing light activities around your home. i. Performing heavy activities around your home j. Getting into or out of a car k. Walking 2 blocks l. Walking a mile m. Going up or down 10 stairs (about 1 flight of stairs). n. Standing for 1 hour o. Sitting for 1 hour p. Running on even ground q. Running on uneven ground r. Making sharp turns while running fast s. Hopping t. Rolling over in bed Column Totals: Score: / 80 25
55 Appendix X: Neck Disability Index (NDI) THE NECK DISABILITY INDEX (NDI) An informal blurb from the author Howard Vernon, D.C. The Neck Disability Index (NDI) was developed in 1989 by Howard Vernon. The Index was developed as a modification of the Oswestry Low Back Pain Disability Index with the permission of the original author (J. Fairbank, 1980). In 1991, Vernon and Mior published the results of a study of reliability and validity in the Journal of Manipulative and Physiologic Therapeutics. Since then, approximately ten articles have appeared in the indexed literature on the NDI. All of these studies have confirmed the original reports of a high level of reliability and validity. We currently know that the NDI consists of one factor physical disability although NDI scores correlate well with the SF-36 mental component scores as well. We know that the minimum detectable score and the minimal clinically important difference amounts to the same figure 5 NDI points. The NDI has become a standard instrument for measuring self-rated disability due to neck pain and is used by clinicians and researchers alike. Each of the 10 items is scored from 0 5. The maximum score is therefore 50. The obtained score can be multiplied by 2 to produce a percentage score. Occasionally, a respondent will not complete one question or another. The average of all other items is then added to the completed items. The original report provided scoring intervals for interpretation, as follows: 0 4 = no disability 5 14 = mild = moderate = severe Above 34 = complete. Please note: The means out of 50 (the RAW SCORE) equates with moderate disability. It is recommended that the NDI be used at baseline and for every 2 weeks thereafter within the treatment program to measure progress. As noted above, at least a 5-point change is required to be clinically meaningful. Patients often do not score the items as zero, once they are in treatment. In other words, it is common to find that patients will continue to score between 5 15 despite having made excellent recovery (i.e., they may be back to work now). The practitioner should avoid the trap of treating till zero, as this is not supportable based on current evidence. 26
56 THIS QUESTIONNAIRE IS DESIGNED TO HELP US BETTER UNDERSTAND HOW YOUR NECK PAIN AFFECTS YOUR ABILITY TO MANAGE EVERYDAY LIFE ACTIVITIES. PLEASE MARK IN EACH SECTION THE ONE BOX THAT APPLIES TO YOU. ALTHOUGH YOU MAY CONSIDER THAT TWO OF THE STATEMENTS IN ANY ONE SECTION RELATE TO YOU, PLEASE MAKRE THE BOX THAT MOST CLOSELY DESCRIBES YOUR PRESENT DAY SITUATION. Section 1 Pain Intensity I have no pain at the moment. The pain is very mild at the moment. The pain is moderate at the moment. The pain is fairly severe at the moment. The pain is very severe at the moment. The pain is the worst pain imaginable at the moment. Section 2 Personal Care I can look after myself normally without causing extra pain. I can look after myself normally, but it causes extra pain. It is painful to look after myself, and I am slow and careful. I need some help but manage most of my personal care. I need help every day in most aspects of self-care. I do not get dressed. I wash with difficulty and stay in bed. Section 3 Lifting I can lift heavy weights without causing extra pain. I can lift heavy weights but it gives me extra pain. Pain prevents me from lifting heavy weights off the floor, but I can manage items if they are conveniently positioned, ie on a table. I can lift only very light weights. I cannot lift or carry anything at all. Section 4 Work I can do as much work as I want. I can only do my usual work, but no more. I can do most of my usual work, but no more. I can t do my usual work. I can hardly do any work at all. I can t do any work at all. Section 5 Headaches I have no headaches at all. I have slight headaches that come infrequently. I have moderate headaches that come infrequently. I have moderate headaches that come frequently. I have severe headaches that come frequently. I have headaches almost all the time. Section 6 Concentration I can concentrate fully without difficulty. I can concentrate fully with slight difficulty. I have a fair degree of difficulty concentrating. I have a lot of difficulty concentrating. I have a great deal of difficulty concentrating. I can t concentrate at all. Section 7 Sleeping I have no trouble sleeping. My sleep is slightly disturbed for less than 1 hour. My sleep is mildly disturbed for up to 1 2 hours. My sleep is moderately disturbed for up to 2-3 hours. My sleep is greatly disturbed for up to 3-5 hours My sleep is completely disturbed for up to 5-7 hours. Section 8 Driving I can drive my car without neck pain. I can drive as long as I want with slight neck pain. I can drive as long as I want with moderate neck pain. I can t drive as long as I want because of moderate neck pain. I can hardly drive at all because of severe neck pain. I can t drive my car at all because of neck pain. Section 9 Reading I can read as much as I want with no neck pain. I can read as much as I want with slight neck pain. I can read as much as I want with moderate neck pain. I can t read as much as I want because of moderate neck pain. I can t read as much as I want because of severe neck pain. I can t read at all. Section 10 Recreation I have no neck pain during all recreational activities. I have some neck pain with all recreational activities. I have some neck pain with a few recreational activities. I have neck pain with most recreational activities. I can hardly do recreational activities due to neck pain. I can t do any recreational activities due to neck pain. Patient Name Date Score (50) Benchmark -5 + Name Date Case # 27
57 Please check the one box in each section that most closely describes your condition. Section 1 Pain Intensity I have no pain at the moment. The pain is very mild at the moment. The pain is moderate at the moment. The pain is fairly severe at the moment. The pain is very severe at the moment. The pain is the worst imaginable at the moment. Section 2 Personal Care (Washing, Dressing, etc) I can look after myself normally without causing extra pain. I can look after myself normally but it causes extra pain. Section 3 Lifting Section 4 Reading It is painful to look after myself and I am slow and careful. I need some help but manage most of my personal care. I need help every day in most aspects of self-care. I do not get dressed, I wash with difficulty and stay in bed. I can lift heavy weights without extra pain. I can lift heavy weights but it gives me extra pain. Pain prevents me from lifting heavy weights off the floor, but I can manage if they are conveniently positioned, for example on a table. Pain prevents me from lifting heavy weights off the floor, but I can manage light to medium weights if they are conveniently positioned. I can lift very light weights. I cannot lift or carry anything at all. I can read as much as I want to with no pain in my neck. I can read as much as I want to with slight pain in my neck. I can read as much as I want to with moderate pain in my neck. I can t read as much as I want because of moderate pain in my neck. 28
58 I can hardly read at all because of moderate pain in my neck. I cannot read at all. Section 5 Headaches I have no headaches at all. I have slight headaches which come infrequently. I have moderate headaches which come infrequently. I have moderate headaches which come frequently. I have severe headaches which come frequently. I have headaches almost all the time. Section 6 Concentration I can concentrate fully when I want to with no difficulty. I can concentrate fully when I want to with slight difficulty. I have a fair degree of difficulty in concentration when I want to. I have a lot of difficulty in concentrating when I want to. I have a great deal of difficulty in concentrating when I want to. I cannot concentrate at all. Section 7 Work I can do as much work as I want to. I can only do my usual work, but no more. I can do most of my usual work, but no more. I cannot do my usual work. I can hardly do any work at all. I can t do any work at all. Section 8 Driving I can drive my car without any neck pain. I can drive my car as long as I want with slight neck pain. I can drive my car as long as I want with moderate neck pain. 29
59 Section 9 Sleeping I can t drive my car as long as I want because of moderate pain in my neck. I can hardly drive at all because of severe pain in my neck. I can t drive my car at all. Section 10 Recreation I have no trouble sleeping. My sleep is slightly disturbed (less than 1 hour sleepless). My sleep is mildly disturbed (1 2 hours sleepless). My sleep is moderately disturbed (2 3 hours sleepless). My sleep is greatly disturbed (3 5 hours sleepless). My sleep is completely disturbed (5 7 hours sleepless). I am able to engage in all my recreation activities with no neck pain at all. I am able to engage in all my recreation activities, with some pain in my neck. I am able to engage in most, but not all of my usual recreation activities because of pain in my neck. I am able to engage in a few of my usual recreation activities because of pain in my neck. I can hardly do any recreation activities because of pain in my neck. I can t do any recreation activities at all. 30
60 Appendix XI: Quick Dash and Work Module for Upper Extremities 31
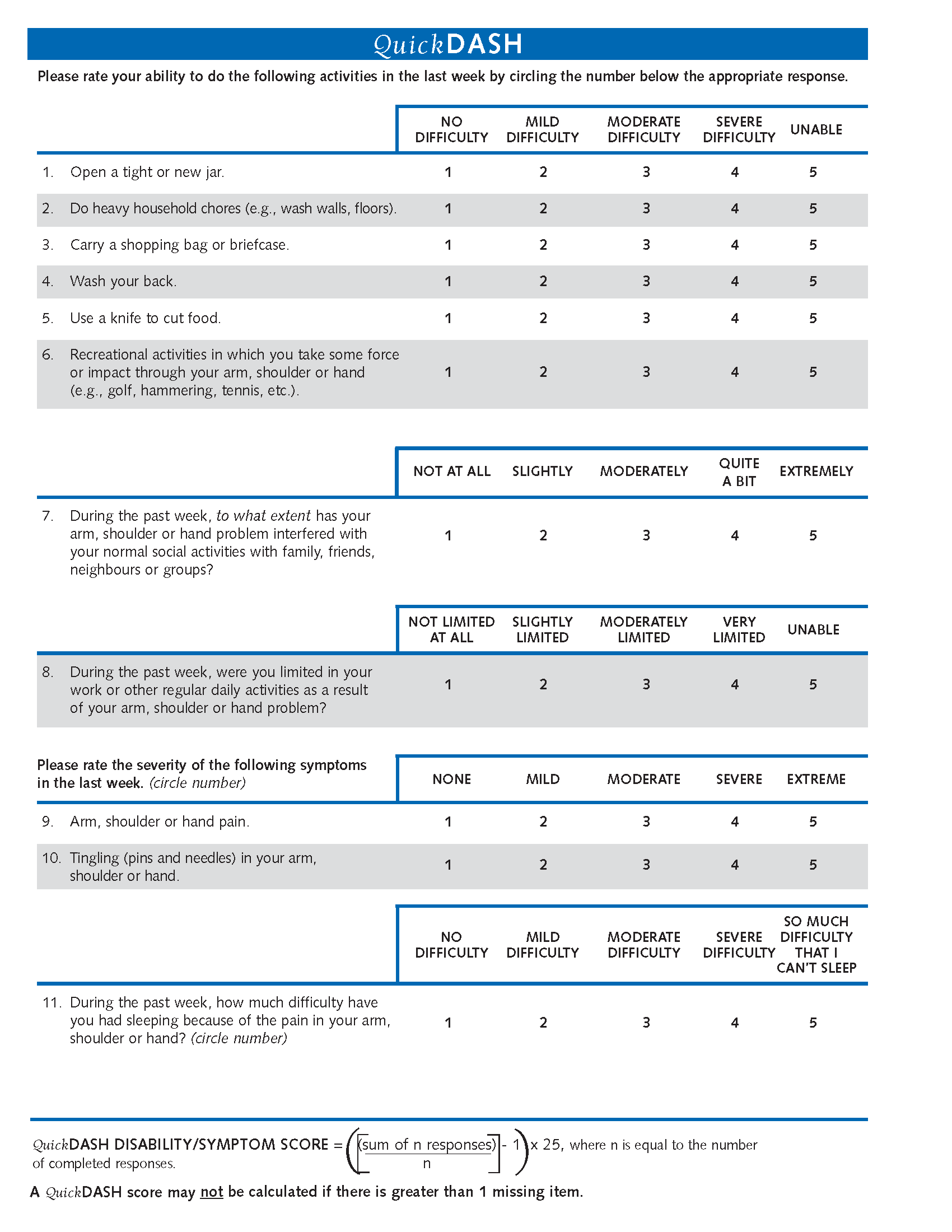
61 32

62 33
A Support Package for Physicians Treating Injured Workers
 A Support Package for Physicians Treating Injured Workers Published by Saskatchewan Workers Compensation Board Last updated: October 2010 TABLE OF CONTENTS 1. Preface...1 1.1 List of updates 2. Synopsis...2
A Support Package for Physicians Treating Injured Workers Published by Saskatchewan Workers Compensation Board Last updated: October 2010 TABLE OF CONTENTS 1. Preface...1 1.1 List of updates 2. Synopsis...2
Accreditation Standards and Service Provider Guidelines for Saskatchewan Workers Compensation Board. Primary Occupational Therapy Service Providers.
 1. Intent Accreditation Standards and Service Provider Guidelines for Saskatchewan Workers Compensation Board Primary Occupational Therapy Service Providers This document sets out the: accreditation standards,
1. Intent Accreditation Standards and Service Provider Guidelines for Saskatchewan Workers Compensation Board Primary Occupational Therapy Service Providers This document sets out the: accreditation standards,
Registered Nurse (Nurse Practitioner) Accreditation Standards and Service Provider Guidelines
 Accreditation Standards and Service Provider Guidelines") 1. Intent Registered Nurse (Nurse Practitioner) Accreditation Standards and Service Provider Guidelines The intent of this document is to set out the accreditation standards and the service provider guidelines
1. Intent Registered Nurse (Nurse Practitioner) Accreditation Standards and Service Provider Guidelines The intent of this document is to set out the accreditation standards and the service provider guidelines
SCHEDULE A Practice Guidelines for Psychologists
 SCHEDULE A Practice Guidelines for Psychologists 1. Introduction The intent of this document is to set out the WCB service provider guidelines for Psychologists providing the following services to WCB
SCHEDULE A Practice Guidelines for Psychologists 1. Introduction The intent of this document is to set out the WCB service provider guidelines for Psychologists providing the following services to WCB
THE MEDICAL TREATMENT GUIDELINES
 THE MEDICAL TREATMENT GUIDELINES I. INTRODUCTION A. About the Medical Treatment Guidelines. On December 1, 2010, the NYS Workers' Compensation Board is implementing new regulations and Medical Treatment
THE MEDICAL TREATMENT GUIDELINES I. INTRODUCTION A. About the Medical Treatment Guidelines. On December 1, 2010, the NYS Workers' Compensation Board is implementing new regulations and Medical Treatment
A guide for injured workers. Returning to work. April 2011
 A guide for injured workers Returning to work April 2011 Contents 1. Getting back to work 1 Ideas to help you return to work 2 Staying positive 2 Your employer s legal obligations 3 Anti-discrimination
A guide for injured workers Returning to work April 2011 Contents 1. Getting back to work 1 Ideas to help you return to work 2 Staying positive 2 Your employer s legal obligations 3 Anti-discrimination
Information for Workers. Information for Workers
 Information for Workers Information for Workers Revised March 2015 Contents Overview... 2 Workplace Injuries... 2 Worker Responsibilities... 2 Employer Responsibilities... 4 WCB Responsibilities... 4 Returning
Information for Workers Information for Workers Revised March 2015 Contents Overview... 2 Workplace Injuries... 2 Worker Responsibilities... 2 Employer Responsibilities... 4 WCB Responsibilities... 4 Returning
Physical Therapy Contract. Reference guide to understanding your contract
 Physical Therapy Contract Reference guide to understanding your contract Revised February 2011 HC-429 REV FEB 2011 Copyright 2009 at WCB Health Care Services Page 2 of 13 PHYSICAL THERAPY PROVIDER EXPECTATIONS
Physical Therapy Contract Reference guide to understanding your contract Revised February 2011 HC-429 REV FEB 2011 Copyright 2009 at WCB Health Care Services Page 2 of 13 PHYSICAL THERAPY PROVIDER EXPECTATIONS
AIG/HealthSmart Managed Health Care Plan
 AIG/HealthSmart Managed Health Care Plan Your Workers Compensation Medical Solution Employer Manual Contents AIG/HealthSmart Managed Health Care Plan Overview...2 Program Description and Objectives...3
AIG/HealthSmart Managed Health Care Plan Your Workers Compensation Medical Solution Employer Manual Contents AIG/HealthSmart Managed Health Care Plan Overview...2 Program Description and Objectives...3
California Provider Reference Manual Introduction and Overview of Medical Provider Networks (CA MPNs)
") California Provider Reference Manual Introduction and Overview of Medical Provider Networks (CA MPNs) Coventry/First Health has designed this manual for The Coventry/First Health Network providers participating
California Provider Reference Manual Introduction and Overview of Medical Provider Networks (CA MPNs) Coventry/First Health has designed this manual for The Coventry/First Health Network providers participating
Worker s Handbook. A guide to your workers compensation insurance. Nova Scotians safe and secure from workplace injury
 Worker s Handbook A guide to your workers compensation insurance Nova Scotians safe and secure from workplace injury Your Worker s Handbook at a glance Your care comes first: health care benefits.... 2
Worker s Handbook A guide to your workers compensation insurance Nova Scotians safe and secure from workplace injury Your Worker s Handbook at a glance Your care comes first: health care benefits.... 2
WORKPLACE INJURY INSURANCE: Worker s Handbook
 WORKPLACE INJURY INSURANCE: Worker s Handbook A GUIDE TO YOUR WORKERS COMPENSATION INSURANCE The following information is provided as a basic guide to your Workers Compensation Insurance. For more complete
WORKPLACE INJURY INSURANCE: Worker s Handbook A GUIDE TO YOUR WORKERS COMPENSATION INSURANCE The following information is provided as a basic guide to your Workers Compensation Insurance. For more complete
THE PHYSICIAN S ROLE IN HELPING PATIENTS RETURN TO WORK AFTER AN ILLNESS OR INJURY (UPDATE 2000)
") CMA POLICY THE PHYSICIAN S ROLE IN HELPING PATIENTS RETURN TO WORK AFTER AN ILLNESS OR INJURY (UPDATE 2000) This policy addresses the role of attending physicians in assisting their patients to return
CMA POLICY THE PHYSICIAN S ROLE IN HELPING PATIENTS RETURN TO WORK AFTER AN ILLNESS OR INJURY (UPDATE 2000) This policy addresses the role of attending physicians in assisting their patients to return
Injured Worker s Guide to. Best Practice Return to Work for a Stress Injury
 Injured Worker s Guide to Best Practice Return to Work for a Stress Injury The best practice return to work guidelines for a stress injury were developed by the Australian Services Union with the support
Injured Worker s Guide to Best Practice Return to Work for a Stress Injury The best practice return to work guidelines for a stress injury were developed by the Australian Services Union with the support
If you have opted out of the student plan, check with your other health plan to see if it covers chiropractic services.
 MacEwan Student Centre, Room 370 2500 University Drive NW Calgary, AB, Canada T2N 1N4 ucalgary.ca/wellnesscentre CHIROPRACTIC SERVICES FAQs How much does it cost? The SU Wellness Centre has very affordable
MacEwan Student Centre, Room 370 2500 University Drive NW Calgary, AB, Canada T2N 1N4 ucalgary.ca/wellnesscentre CHIROPRACTIC SERVICES FAQs How much does it cost? The SU Wellness Centre has very affordable
About us. Your injured worker s recovery and return to work is a team effort. It involves you, your WorkSafe Agent, your worker and their doctor.
 1. About us Your injured worker s recovery and return to work is a team effort. It involves you, your WorkSafe Agent, your worker and their doctor. About WorkSafe Victoria WorkSafe Victoria (WorkSafe)
1. About us Your injured worker s recovery and return to work is a team effort. It involves you, your WorkSafe Agent, your worker and their doctor. About WorkSafe Victoria WorkSafe Victoria (WorkSafe)
How To Manage A Return To Work
 Policy Number: CS-1302-2013 Policy Title: Return to Work Occupational & Non-Occupational Absences due to Medical Reasons Policy Policy Owner: Chief Human Resources Officer Effective Date: March 27, 2013
Policy Number: CS-1302-2013 Policy Title: Return to Work Occupational & Non-Occupational Absences due to Medical Reasons Policy Policy Owner: Chief Human Resources Officer Effective Date: March 27, 2013
A workers compensation guide for employers
 A workers compensation guide for employers When a worker is injured 1 C CONTENTS PURPOSE OF THIS GUIDE 4 NSW workers compensation system 4 Your obligations 5 The evidence for recovery at work 5 The benefits
A workers compensation guide for employers When a worker is injured 1 C CONTENTS PURPOSE OF THIS GUIDE 4 NSW workers compensation system 4 Your obligations 5 The evidence for recovery at work 5 The benefits
WORKERS GUIDE YUKON WORKERS COMPENSATION HEALTH AND SAFETY BOARD. working together WITH YUKON WORKERS AND EMPLOYERS
 WORKERS GUIDE YUKON WORKERS COMPENSATION HEALTH AND SAFETY BOARD working together WITH YUKON WORKERS AND EMPLOYERS workers compensation WORKERS COMPENSATION Workers compensation is an employer-funded insurance
WORKERS GUIDE YUKON WORKERS COMPENSATION HEALTH AND SAFETY BOARD working together WITH YUKON WORKERS AND EMPLOYERS workers compensation WORKERS COMPENSATION Workers compensation is an employer-funded insurance
Introduction and Overview of HCO Program
 Introduction and Overview of HCO Program To meet the requirements of Article 8 9771.70, First Health has designed this manual for The First Health Network providers participating in The First Health/CompAmerica
Introduction and Overview of HCO Program To meet the requirements of Article 8 9771.70, First Health has designed this manual for The First Health Network providers participating in The First Health/CompAmerica
Signed:... (worker or representative) Guidelines for Claiming Compensation Benefits September 2013 Page 46 of 46
 Guidelines for Claiming Compensation Benefits September 2013 Page 46 of 46") 8 October 2013 SPECIAL SUPPLEMENT 4385 Additional Reports or Documents Please list and provide copies of all further information, reports and documents in support of this application for review................
8 October 2013 SPECIAL SUPPLEMENT 4385 Additional Reports or Documents Please list and provide copies of all further information, reports and documents in support of this application for review................
A guide for injured workers. Introducing WorkSafe
 A guide for injured workers Introducing WorkSafe September July 2013 2011 Contents 1. About us 1 2. Weekly payments (income entitlements) 2 3. Services to help you get better 4 4. Getting back to work
A guide for injured workers Introducing WorkSafe September July 2013 2011 Contents 1. About us 1 2. Weekly payments (income entitlements) 2 3. Services to help you get better 4 4. Getting back to work
The Hartford s California Workers Compensation Medical Provider Network (MPN) Accessing Anthem Blue Cross Prudent Buyer PPO
 Accessing Anthem Blue Cross Prudent Buyer PPO") Employer Implementation Guide Topics Covered in the Guide: Workers Compensation MPN Networks in CA How It Works The Employer s Role Implementation Steps Dealing with Workplace Injuries Employee Rights
Employer Implementation Guide Topics Covered in the Guide: Workers Compensation MPN Networks in CA How It Works The Employer s Role Implementation Steps Dealing with Workplace Injuries Employee Rights
POLICY: 04-05 PART I Chapter: BENEFITS Subject: RETURN-TO-WORK SERVICES Authorization: BoD Resolution 2001/07/38 August 21, 2001
 REFERENCE: Workers Compensation Act, RSA 2000, Sections 1(1)(f), 54, 56, 63, 89, and 137.1 POLICY: When a work-related injury results in compensable work restrictions that impair a worker s employability
REFERENCE: Workers Compensation Act, RSA 2000, Sections 1(1)(f), 54, 56, 63, 89, and 137.1 POLICY: When a work-related injury results in compensable work restrictions that impair a worker s employability
Policy: Worker s Compensation/ On the Job Injury
 Worker s Compensation Policy Policy: Worker s Compensation/ On the Job Injury Policy Statement CITATION REFERENCE Official Title: Worker s Compensation / On the Job Injury Policy Abbreviated Title: Worker
Worker s Compensation Policy Policy: Worker s Compensation/ On the Job Injury Policy Statement CITATION REFERENCE Official Title: Worker s Compensation / On the Job Injury Policy Abbreviated Title: Worker
Injured Workers Handbook
 Injured Workers Handbook The Commission is responsible for keeping your personal information confidential and secure, and we take this responsibility very seriously. We collect, use and disclose only information
Injured Workers Handbook The Commission is responsible for keeping your personal information confidential and secure, and we take this responsibility very seriously. We collect, use and disclose only information
Workplace rehabilitation providers and WorkCover
 Workplace rehabilitation providers and WorkCover What to expect from your workplace rehabilitation provider This guide aims to provide workers and employers with information regarding the role of WorkCover
Workplace rehabilitation providers and WorkCover What to expect from your workplace rehabilitation provider This guide aims to provide workers and employers with information regarding the role of WorkCover
InformatIon for Workers
 InformatIon for Workers InformatIon for Workers Employers, workers, care providers and the WCB must work together to prevent work injuries and, when injuries happen, get injured workers back to work as
InformatIon for Workers InformatIon for Workers Employers, workers, care providers and the WCB must work together to prevent work injuries and, when injuries happen, get injured workers back to work as
Managing Workers Compensation Claims
 Managing Workers Compensation Claims A Presentation of The Office of the Employer Advisor Office of the Employer Advisor What is it? P Mandate in Sec. 85.(1) (b) of the Workers Compensation Act P Funded
Managing Workers Compensation Claims A Presentation of The Office of the Employer Advisor Office of the Employer Advisor What is it? P Mandate in Sec. 85.(1) (b) of the Workers Compensation Act P Funded
Saskatchewan Workers Compensation Act Committee of Review
 Submission to the Saskatchewan Workers Compensation Act Committee of Review Submitted by the 3420A Hill Avenue Regina, SK S4S 0W9 Phone: (306) 585-1411 - Fax: (306) 585-0685 E-mail: cas@saskchiropractic.ca
Submission to the Saskatchewan Workers Compensation Act Committee of Review Submitted by the 3420A Hill Avenue Regina, SK S4S 0W9 Phone: (306) 585-1411 - Fax: (306) 585-0685 E-mail: cas@saskchiropractic.ca
Guidelines for Employers. Return-to-Work. April 2003. WorkCover. Watching out for you.
 Guidelines for Employers Return-to-Work Programs April 2003 WorkCover. Watching out for you. Published by WorkCover NSW First published November 1987 Revised November 1993, December 1994, May 1997, March
Guidelines for Employers Return-to-Work Programs April 2003 WorkCover. Watching out for you. Published by WorkCover NSW First published November 1987 Revised November 1993, December 1994, May 1997, March
Facts & Tips about Long-term Disability (LTD)
") Facts & Tips about Long-term Disability (LTD) Revised June 2008 Please keep this document handy for reference It offers general information about LTD benefits under an insurance policy or contract. It
Facts & Tips about Long-term Disability (LTD) Revised June 2008 Please keep this document handy for reference It offers general information about LTD benefits under an insurance policy or contract. It
Rehabilitation of employees back to work after illness or injury Policy and Procedure
 Rehabilitation of employees back to work after illness or injury Policy and Procedure Document reference number HSAG 2011/3 Document developed by Revision number 4.13 Document approved by Approval date
Rehabilitation of employees back to work after illness or injury Policy and Procedure Document reference number HSAG 2011/3 Document developed by Revision number 4.13 Document approved by Approval date
Road to Recovery Rehabilitation following a motor vehicle accident
 Road to Recovery Rehabilitation following a motor vehicle accident If you have been injured in a motor vehicle accident, rehabilitation may help you recover and move on with your life. Queensland Compulsory
Road to Recovery Rehabilitation following a motor vehicle accident If you have been injured in a motor vehicle accident, rehabilitation may help you recover and move on with your life. Queensland Compulsory
Workers' Compensation in California: Questions & Answers
 Workers' Compensation in California: Questions & Answers prepared for the California Commission on Health and Safety and Workers' Compensation October 2006 Page 2 Introduction. How To Use This Booklet.....................................
Workers' Compensation in California: Questions & Answers prepared for the California Commission on Health and Safety and Workers' Compensation October 2006 Page 2 Introduction. How To Use This Booklet.....................................
A glossary for injured workers Who s who in the claims process
 A glossary for injured workers Who s who in the July 2013 Who s who in the A glossary for injured workers About us 1 Talking your language service 2 Key contacts during the 3 About the roles in the 4 Allied
A glossary for injured workers Who s who in the July 2013 Who s who in the A glossary for injured workers About us 1 Talking your language service 2 Key contacts during the 3 About the roles in the 4 Allied
UNISA INJURY/ILLNESS MANAGEMENT HANDBOOK A GUIDE FOR UNISA EMPLOYEES AND THEIR MANAGERS
 Introduction The University of South Australia, a self insured employer under the Return to Work Act 2014 (the Act), is committed to providing a sound injury/illness management program for all employees.
Introduction The University of South Australia, a self insured employer under the Return to Work Act 2014 (the Act), is committed to providing a sound injury/illness management program for all employees.
There are some specific guidelines provided in the rules and regulations for these lists:
 Health Care Provider Panels List Defined The PA Workers' Compensation Act gives employers the right to establish a list of designated health care providers. When the list is properly posted, injured workers
Health Care Provider Panels List Defined The PA Workers' Compensation Act gives employers the right to establish a list of designated health care providers. When the list is properly posted, injured workers
Workers' Compensation Act, 1981 (as amended), Sections 1(1)(d), 49,51,57, and 83
, Sections 1(1)(d), 49,51,57, and 83") 04-05 PART I REFERENCE : Workers' Compensation Act, 1981 (as amended), Sections 1(1)(d), 49,51,57, and 83 When a work-related injury results in compensable work restrictions that impair a worker's employability
04-05 PART I REFERENCE : Workers' Compensation Act, 1981 (as amended), Sections 1(1)(d), 49,51,57, and 83 When a work-related injury results in compensable work restrictions that impair a worker's employability
Employer s Guide to. Best Practice Return to Work for a Stress Injury
 Employer s Guide to Best Practice Return to Work for a Stress Injury Employers Guide to Best Practice Return to Work for a Stress Injury 1. Early Intervention 2. Claim Lodged 3. Claim Acceptance 4. Return
Employer s Guide to Best Practice Return to Work for a Stress Injury Employers Guide to Best Practice Return to Work for a Stress Injury 1. Early Intervention 2. Claim Lodged 3. Claim Acceptance 4. Return
University Students Council of the University of Western Ontario EARLY AND SAFE RETURN TO WORK POLICY
 EFFECTIVE: 30 th October 2012 SUPERSEDES: 15 th November 2011 AUTHORITY: General Manager RATIFIED BY: Executive Council 30 th OCTOBER 2012 RELATED DOCUMENTS: PAGE 1 of 8 PURPOSE: This Policy is created
EFFECTIVE: 30 th October 2012 SUPERSEDES: 15 th November 2011 AUTHORITY: General Manager RATIFIED BY: Executive Council 30 th OCTOBER 2012 RELATED DOCUMENTS: PAGE 1 of 8 PURPOSE: This Policy is created
Reference Guide. Chiropractic Services Memorandum of Agreement. Date September 2014. Health Care Services. Prepared by
 Reference Guide Chiropractic Services Memorandum of Agreement Department Health Care Services Date Prepared by Health Care Services Phone: 604.232.7787 or 1.888.967.5377 (Local 7787) E-mail: HCSINQU@worksafebc.com
Reference Guide Chiropractic Services Memorandum of Agreement Department Health Care Services Date Prepared by Health Care Services Phone: 604.232.7787 or 1.888.967.5377 (Local 7787) E-mail: HCSINQU@worksafebc.com
Member Handbook. Regina Civic Employees Long Term Disability Plan
 Member Handbook Regina Civic Employees Long Term Disability Plan Table of Contents About the Plan.. Eligibility and Enrollment.... Contributions Definition of Disability.. Applying for Benefits... Qualifying
Member Handbook Regina Civic Employees Long Term Disability Plan Table of Contents About the Plan.. Eligibility and Enrollment.... Contributions Definition of Disability.. Applying for Benefits... Qualifying
annual report 2012 Fair Practices office An independent office working to promote fair practices at the Workers Compensation Board of Saskatchewan
 annual report 2012 Fair Practices office An independent office working to promote fair practices at the Workers Compensation Board of Saskatchewan Table of contents MESSAGE FROM THE FAIR PRACTICES OFFICER
annual report 2012 Fair Practices office An independent office working to promote fair practices at the Workers Compensation Board of Saskatchewan Table of contents MESSAGE FROM THE FAIR PRACTICES OFFICER
DECS REHABILITATION RETURN TO WORK POLICY PROCEDURES
 DECS REHABILITATION & RETURN TO WORK POLICY & PROCEDURES FOREWORD The Department of Education and Children s Services (DECS) is committed to safe work practices that support the wellbeing of all employees.
DECS REHABILITATION & RETURN TO WORK POLICY & PROCEDURES FOREWORD The Department of Education and Children s Services (DECS) is committed to safe work practices that support the wellbeing of all employees.
Constituent Union HSPBA Enhanced Disability Management Program: Overview
 Constituent Union HSPBA Enhanced Disability Management Program: Overview The EDMP is a collaborative holistic program between the employer, employee and union. All regular employees must be referred to
Constituent Union HSPBA Enhanced Disability Management Program: Overview The EDMP is a collaborative holistic program between the employer, employee and union. All regular employees must be referred to
LOW BACK INJURIES PROGRAM OF CARE PROGRAM OF CARE 4TH EDITION 2014
 LOW BACK INJURIES PROGRAM OF CARE PROGRAM OF CARE 4TH EDITION 2014 GUIDE Acknowledgements Acknowledgements The WSIB would like to acknowledge the significant contributions of the following regulated Health
LOW BACK INJURIES PROGRAM OF CARE PROGRAM OF CARE 4TH EDITION 2014 GUIDE Acknowledgements Acknowledgements The WSIB would like to acknowledge the significant contributions of the following regulated Health
RETURN-TO-WORK SERVICES
 RETURN-TO-WORK SERVICES TABLE OF CONTENTS Early Intervention...2 Creating A Return-To-Work Program...3 Keep in Mind...3 Five Steps for Creating an Effective Return-To-Work Policy...4 Situations to Avoid
RETURN-TO-WORK SERVICES TABLE OF CONTENTS Early Intervention...2 Creating A Return-To-Work Program...3 Keep in Mind...3 Five Steps for Creating an Effective Return-To-Work Policy...4 Situations to Avoid
Working together. The role of the TAC. Your role
 Returning to work Current from 1 July 2014 A Working together Your role The most important person in your return to work is you. A large part of recovering from your accident and getting on with your life
Returning to work Current from 1 July 2014 A Working together Your role The most important person in your return to work is you. A large part of recovering from your accident and getting on with your life
Best Practices in Return to Work For Federal Employees Who Sustain Workplace Injury or Illness: A Guide for Agencies
 Best Practices in Return to Work For Federal Employees Who Sustain Workplace Injury or Illness: A Guide for Agencies Introduction The Department of Labor (DOL) initiated a study to identify strategies
Best Practices in Return to Work For Federal Employees Who Sustain Workplace Injury or Illness: A Guide for Agencies Introduction The Department of Labor (DOL) initiated a study to identify strategies
A Guide for Self-Employed Registered Nurses
 A Guide for Self-Employed Registered Nurses 2014 (new format inserted) First printing (1997) Revisions (2003, 2014) 2014, Suite 4005 7071 Bayers Road, Halifax, NS B3L 2C2 info@crnns.ca www.crnns.ca All
A Guide for Self-Employed Registered Nurses 2014 (new format inserted) First printing (1997) Revisions (2003, 2014) 2014, Suite 4005 7071 Bayers Road, Halifax, NS B3L 2C2 info@crnns.ca www.crnns.ca All
Berkshire Hathaway GUARD Insurance Companies. Medical Provider Network
 Berkshire Hathaway GUARD Insurance Companies Medical Provider Network Site Coordinator Guide Created 11/9/04 Revised 7/7/08 Table of Contents SITE COORDINATOR GUIDE Page 1 Background Your MPN contact When
Berkshire Hathaway GUARD Insurance Companies Medical Provider Network Site Coordinator Guide Created 11/9/04 Revised 7/7/08 Table of Contents SITE COORDINATOR GUIDE Page 1 Background Your MPN contact When
 Appendix 1 July 5th, 2012 Process Guide for xxx Catholic District School Board Advice to Pay Program Preparation Date: June 28, 2012 Effective Date of Services: xxxxxx 1 Acronyms, Abbreviations and Definitions...
Appendix 1 July 5th, 2012 Process Guide for xxx Catholic District School Board Advice to Pay Program Preparation Date: June 28, 2012 Effective Date of Services: xxxxxx 1 Acronyms, Abbreviations and Definitions...
The County of Scotland Transitional Duty Policy
 The County of Scotland Transitional Duty Policy A. PURPOSE This policy defines the County of Scotland s Transitional Duty Program for employees who are injured on the job. B. POLICY/MISSION STATEMENT It
The County of Scotland Transitional Duty Policy A. PURPOSE This policy defines the County of Scotland s Transitional Duty Program for employees who are injured on the job. B. POLICY/MISSION STATEMENT It
Ambulance Victoria Position Description
 Ambulance Victoria Position Description Position Title: Claims Management Coordinator Reports To: Injury & Claims Management Team Leader Division: People & Community Department: Health, Safety & Wellbeing
Ambulance Victoria Position Description Position Title: Claims Management Coordinator Reports To: Injury & Claims Management Team Leader Division: People & Community Department: Health, Safety & Wellbeing
MAIC GUIDELINES FOR COMPULSORY THIRD PARTY (CTP) REHABILITATION PROVIDERS. Revised and updated 2012
 REHABILITATION PROVIDERS. Revised and updated 2012") MAIC GUIDELINES FOR COMPULSORY THIRD PARTY (CTP) REHABILITATION PROVIDERS Revised and updated 2012 MOTOR ACCIDENT INSURANCE COMMISSION (MAIC) GUIDELINES FOR COMPULSORY THIRD PARTY (CTP) REHABILITATION
MAIC GUIDELINES FOR COMPULSORY THIRD PARTY (CTP) REHABILITATION PROVIDERS Revised and updated 2012 MOTOR ACCIDENT INSURANCE COMMISSION (MAIC) GUIDELINES FOR COMPULSORY THIRD PARTY (CTP) REHABILITATION
POLICIES FOR CHIROPRACTIC SPECIALTY COLLEGES Approved by the CFCREAB Board November 26, 2011
 POLICIES FOR CHIROPRACTIC SPECIALTY COLLEGES Approved by the CFCREAB Board November 26, 2011 SECTION I - INTRODUCTION 1. The CFCREAB The Canadian Federation of Chiropractic Regulatory & Educational Accrediting
POLICIES FOR CHIROPRACTIC SPECIALTY COLLEGES Approved by the CFCREAB Board November 26, 2011 SECTION I - INTRODUCTION 1. The CFCREAB The Canadian Federation of Chiropractic Regulatory & Educational Accrediting
Supplementary services table of costs Effective 1 July 2010
 Effective 1 July 2010 Service Insurer prior approval required 1 Communication Case conference Consult list of exclusions before using this item Communication between practitioners and stakeholders (insurer,
Effective 1 July 2010 Service Insurer prior approval required 1 Communication Case conference Consult list of exclusions before using this item Communication between practitioners and stakeholders (insurer,
PERSONAL INJURIES. If needed, we may be able to tell you of professionals in your area whom you can consider.
 PERSONAL INJURIES There are three main aspects to dealing with the results of personal injury: medical treatment, employment, and recovery of proper compensation. MEDICAL TREA TMEN T Coordinatinq Doctor
PERSONAL INJURIES There are three main aspects to dealing with the results of personal injury: medical treatment, employment, and recovery of proper compensation. MEDICAL TREA TMEN T Coordinatinq Doctor
Guidelines. for developing an Injury Management Program. Licensed Insurers and Self-Insurers:
 Licensed Insurers and Self-Insurers: Guidelines for developing an Injury Management Program VERSION 2 Effective 1 July 2014 and to apply to all injury management activities regardless of when the injury
Licensed Insurers and Self-Insurers: Guidelines for developing an Injury Management Program VERSION 2 Effective 1 July 2014 and to apply to all injury management activities regardless of when the injury
CIRCULAR HEAD COUNCIL
 CIRCULAR HEAD COUNCIL RETURN TO WORK AND REHABILITATION MANAGEMENT PLAN RETURN TO WORK & REHABILITATION MANAGEMENT PLAN 1 TABLE OF CONTENTS RETURN TO WORK & REHABILITATION POLICY... 3 DEFINITIONS... 4
CIRCULAR HEAD COUNCIL RETURN TO WORK AND REHABILITATION MANAGEMENT PLAN RETURN TO WORK & REHABILITATION MANAGEMENT PLAN 1 TABLE OF CONTENTS RETURN TO WORK & REHABILITATION POLICY... 3 DEFINITIONS... 4
Comparative Review of Workers Compensation Systems in Select Jurisdictions SASKATCHEWAN
 of Workers Compensation Systems in Select Jurisdictions JURISDICTION: SASKATCHEWAN ENVIRONMENT Population Size Labour Force Demographic and Economic Indicators 1,015,600 (1995, Stats Canada) 494,000 (1995,
of Workers Compensation Systems in Select Jurisdictions JURISDICTION: SASKATCHEWAN ENVIRONMENT Population Size Labour Force Demographic and Economic Indicators 1,015,600 (1995, Stats Canada) 494,000 (1995,
Workcover Guidelines on Injury Management Consultants
 4210 SPECIAL SUPPLEMENT 28 September 2012 Workcover Guidelines on Injury Management Consultants Workplace Injury Management and Workers Compensation Act 1998 I, Julie Newman, the Acting Chief Executive
4210 SPECIAL SUPPLEMENT 28 September 2012 Workcover Guidelines on Injury Management Consultants Workplace Injury Management and Workers Compensation Act 1998 I, Julie Newman, the Acting Chief Executive
SGEU Recommendations to Workers' Compensation Board 2006 Committee of Review
 SGEU Recommendations to Workers' Compensation Board 2006 Committee of Review The Saskatchewan Government and General Employees Union (SGEU) represents some 22,000 public sector workers in the province.
SGEU Recommendations to Workers' Compensation Board 2006 Committee of Review The Saskatchewan Government and General Employees Union (SGEU) represents some 22,000 public sector workers in the province.
Avoiding 10 Common Workers Compensation Pitfalls. Presented by Peter P. Greaney, M.D. Medical Director and CEO, WorkCare, Inc.
 Avoiding 10 Common Workers Compensation Pitfalls Presented by Peter P. Greaney, M.D. Medical Director and CEO, WorkCare, Inc. Session Overview Improve understanding of workers comp Identify/correct weaknesses
Avoiding 10 Common Workers Compensation Pitfalls Presented by Peter P. Greaney, M.D. Medical Director and CEO, WorkCare, Inc. Session Overview Improve understanding of workers comp Identify/correct weaknesses
Workplace Health, Safety & Compensation Review Division
 Workplace Health, Safety & Compensation Review Division WHSCRD Case No: 13252-11 WHSCC Claim No.(s): 604016, 611050, 672511 705910, 721783, 731715, 753775, 784014, 831110 Decision Number: 14189 Marlene
Workplace Health, Safety & Compensation Review Division WHSCRD Case No: 13252-11 WHSCC Claim No.(s): 604016, 611050, 672511 705910, 721783, 731715, 753775, 784014, 831110 Decision Number: 14189 Marlene
Policy and Procedures Date: May 21, 2010
 Virginia Polytechnic Institute and State University No. 4420 Rev.: 3 Policy and Procedures Date: May 21, 2010 Subject: Return to Work Policy 1. Purpose... 1 2. Policy... 1 2.1 Occupational Injuries or
Virginia Polytechnic Institute and State University No. 4420 Rev.: 3 Policy and Procedures Date: May 21, 2010 Subject: Return to Work Policy 1. Purpose... 1 2. Policy... 1 2.1 Occupational Injuries or
Occupational Management Services
 Occupational Services Managing workplace injuries for better outcomes GROUP BENEFITS Keeping employees safe and productive at work is important to a company s success. Typically, Group disability and absence
Occupational Services Managing workplace injuries for better outcomes GROUP BENEFITS Keeping employees safe and productive at work is important to a company s success. Typically, Group disability and absence
California Workers Compensation Medical Provider Network Employee Notification & Guide
 California Workers Compensation Medical Provider Network Employee Notification & Guide In partnership with We are pleased to introduce the California workers compensation medical provider network (MPN)
California Workers Compensation Medical Provider Network Employee Notification & Guide In partnership with We are pleased to introduce the California workers compensation medical provider network (MPN)
Workplace Safety and Insurance Board (WSIB)
") Workplace Safety and Insurance Board (WSIB) Dr. L. Grbac March 25, 2013 1 ASSESSMENT AND TREATMENT RESOURCES Programs of Care Specialty Clinics Low Back Expert Physician Examiner Assessments Regional Evaluation
Workplace Safety and Insurance Board (WSIB) Dr. L. Grbac March 25, 2013 1 ASSESSMENT AND TREATMENT RESOURCES Programs of Care Specialty Clinics Low Back Expert Physician Examiner Assessments Regional Evaluation
AGENCY FOR HEALTH CARE ADMINISTRATION HEALTH QUALITY ASSURANCE BUREAU OF MANAGED HEALTH CARE 2727 Mahan Drive Tallahassee Florida 32308
 AGENCY FOR HEALTH CARE ADMINISTRATION HEALTH QUALITY ASSURANCE BUREAU OF MANAGED HEALTH CARE 2727 Mahan Drive Tallahassee Florida 32308 WORKERS COMPENSATION MANAGED CARE ARRANGEMENT SURVEY REPORT NAME
AGENCY FOR HEALTH CARE ADMINISTRATION HEALTH QUALITY ASSURANCE BUREAU OF MANAGED HEALTH CARE 2727 Mahan Drive Tallahassee Florida 32308 WORKERS COMPENSATION MANAGED CARE ARRANGEMENT SURVEY REPORT NAME
Service Provision and Service Descriptions (standards) for Approved Workplace Rehabilitation Providers
 for Approved Workplace Rehabilitation Providers") Service Provision and (standards) for Approved Providers Service Provision and (standards) for Approved Workplace Rehabilitation Providers Service delivery requirements for Providers relating to the principles
Service Provision and (standards) for Approved Providers Service Provision and (standards) for Approved Workplace Rehabilitation Providers Service delivery requirements for Providers relating to the principles
The Hartford s California Workers Compensation Medical Provider Network (MPN)
") Employer Notification Guide Topics Covered are: Workers Compensation MPN Networks in CA New MPN Employee Notification Documents and Processes How It Works The Employer s Role Notification Steps Dealing
Employer Notification Guide Topics Covered are: Workers Compensation MPN Networks in CA New MPN Employee Notification Documents and Processes How It Works The Employer s Role Notification Steps Dealing
GIO Workers Compensation Australian Capital Territory
 GIO Workers Compensation Australian Capital Territory Injury Management Program ACT Injury Management Program This document is a guide for employers and workers to understand the framework of Injury Management
GIO Workers Compensation Australian Capital Territory Injury Management Program ACT Injury Management Program This document is a guide for employers and workers to understand the framework of Injury Management
An Injured Workers Guide to the Workers Compensation Process Table of Contents
 An Injured Workers Guide to the Workers Compensation Process Table of Contents I. Claim Information A. General Information 1. What is workers compensation? 2. How do I know if I qualify for Workers Compensation?
An Injured Workers Guide to the Workers Compensation Process Table of Contents I. Claim Information A. General Information 1. What is workers compensation? 2. How do I know if I qualify for Workers Compensation?
Risk Management Workers Compensation Program Designated Medical Provider Program
 Risk Management Workers Compensation Program Designated Medical Provider Program Benefits of an effective Workers Compensation Designated Medical Provider Program 1 August, 2008 INTRODUCTION Your employer,
Risk Management Workers Compensation Program Designated Medical Provider Program Benefits of an effective Workers Compensation Designated Medical Provider Program 1 August, 2008 INTRODUCTION Your employer,
Zurich Handbook. Managed Care Arrangement program summary
 Zurich Handbook Managed Care Arrangement program summary A Managed Care Arrangement (MCA) is being used to ensure that employees receive timely and proper medical treatment with respect to work-related
Zurich Handbook Managed Care Arrangement program summary A Managed Care Arrangement (MCA) is being used to ensure that employees receive timely and proper medical treatment with respect to work-related
This policy applies to job applicants, Bargaining Unit Staff, Management / Excluded Staff, Casual Staff and Contractors at Yukon College.
 INTRODUCTION This policy applies to job applicants, Bargaining Unit Staff, Management / Excluded Staff, Casual Staff and Contractors at Yukon College. DUTY TO ACCOMMODATE: The Yukon Human Rights Act requires
INTRODUCTION This policy applies to job applicants, Bargaining Unit Staff, Management / Excluded Staff, Casual Staff and Contractors at Yukon College. DUTY TO ACCOMMODATE: The Yukon Human Rights Act requires
CHUBB GROUP OF INSURANCE COMPANIES
 CHUBB GROUP OF INSURANCE COMPANIES Dear Insured, Attached please find an informational letter which is being sent to your treating provider outlining the processes and procedures for Precertification and
CHUBB GROUP OF INSURANCE COMPANIES Dear Insured, Attached please find an informational letter which is being sent to your treating provider outlining the processes and procedures for Precertification and
ALBERTA INSURANCE REFORM LEGISLATION
 ALBERTA INSURANCE REFORM LEGISLATION INSURANCE LITIGATION LEGAL ALERT October, 2004 A Review of Bill 53, the INSURANCE AMENDMENT ACT, 2003 (No. 2), S.A. 2003, c.40 In November of 2003 the Provincial Government
ALBERTA INSURANCE REFORM LEGISLATION INSURANCE LITIGATION LEGAL ALERT October, 2004 A Review of Bill 53, the INSURANCE AMENDMENT ACT, 2003 (No. 2), S.A. 2003, c.40 In November of 2003 the Provincial Government
CANBI. Work Injury Rehabilitation. Canadian Back Institute. The Basics. Canadian vs Hong Kong Experience. www.cbi.ca
 Work Injury Rehabilitation Canadian vs Hong Kong Experience Canadian Back Institute www.cbi.ca Specialists in the prevention and treatment of back and neck pain Founded in 1974 as an education facility
Work Injury Rehabilitation Canadian vs Hong Kong Experience Canadian Back Institute www.cbi.ca Specialists in the prevention and treatment of back and neck pain Founded in 1974 as an education facility
PSYCHOLOGY SERVICES TABLE OF COSTS
 PSYCHOLOGY SERVICES TABLE OF COSTS 1. INTRODUCTION This document outlines the procedures and conditions and fees payable for the delivery of psychology services by registered psychologists for workers
PSYCHOLOGY SERVICES TABLE OF COSTS 1. INTRODUCTION This document outlines the procedures and conditions and fees payable for the delivery of psychology services by registered psychologists for workers
WORKER S COMPENSATION TREATMENT AUTHORIZATION FORM
 FLORIDA TECH EMPLOYEE ACCIDENT/ INJURY REPORT Contact Financial Affairs @ 674-7297 OR 8885 IMMEDIATELY regarding an Employee's Injury. Employee AND Supervisor must complete this report. EMPLOYEE INFORMATION
FLORIDA TECH EMPLOYEE ACCIDENT/ INJURY REPORT Contact Financial Affairs @ 674-7297 OR 8885 IMMEDIATELY regarding an Employee's Injury. Employee AND Supervisor must complete this report. EMPLOYEE INFORMATION
Important Information about Medical Care if you have a Work-Related Injury or Illness
 Important Information about Medical Care if you have a Work-Related Injury or Illness Initial Written Employee Notification Re: Medical Provider Network (Title 8, California Code of Regulations, section
Important Information about Medical Care if you have a Work-Related Injury or Illness Initial Written Employee Notification Re: Medical Provider Network (Title 8, California Code of Regulations, section
Occupational Rehab table of costs Effective 1 July 2015
 Occupational Rehab table of costs Effective 1 July 2015 Service Descriptor Insurer prior approval required 1 Communication - less than 10 Mins Communication - 11 to 20 mins Consult list of exclusions before
Occupational Rehab table of costs Effective 1 July 2015 Service Descriptor Insurer prior approval required 1 Communication - less than 10 Mins Communication - 11 to 20 mins Consult list of exclusions before
Behavioral Health and Human Services Licensing Board
 Behavioral Health and Human Services Licensing Board SOCIAL WORKERS, MARRIAGE AND FAMILY THERAPISTS, MENTAL HEALTH COUNSELORS, AND ADDICTION COUNSELORS A compilation of the Indiana Code and Indiana Administrative
Behavioral Health and Human Services Licensing Board SOCIAL WORKERS, MARRIAGE AND FAMILY THERAPISTS, MENTAL HEALTH COUNSELORS, AND ADDICTION COUNSELORS A compilation of the Indiana Code and Indiana Administrative
Dr Ina Diener Physiotherapy Clinician in Private Practice Lecturer in OMT Stellenbosch, South Africa
 Dr Ina Diener Physiotherapy Clinician in Private Practice Lecturer in OMT Stellenbosch, South Africa Invitation... 2 Invitation... To present evidence for the effectiveness of direct access and service
Dr Ina Diener Physiotherapy Clinician in Private Practice Lecturer in OMT Stellenbosch, South Africa Invitation... 2 Invitation... To present evidence for the effectiveness of direct access and service
How To Cover Occupational Therapy
 Guidelines for Medical Necessity Determination for Occupational Therapy These Guidelines for Medical Necessity Determination (Guidelines) identify the clinical information MassHealth needs to determine
Guidelines for Medical Necessity Determination for Occupational Therapy These Guidelines for Medical Necessity Determination (Guidelines) identify the clinical information MassHealth needs to determine
How to complete workers compensation medical certificates correctly
 How to complete workers compensation medical certificates correctly How to complete workers compensation medical certificates correctly Purpose The purpose of this publication is to help the primary treating
How to complete workers compensation medical certificates correctly How to complete workers compensation medical certificates correctly Purpose The purpose of this publication is to help the primary treating
Directory of Records. Workers Compensation Board Alberta
 Directory of Records Workers Compensation Board Alberta Last updated: May 2005 Table of Contents WCB Mandate...3 Organization...3 Introduction...4 How the Directory is Organized...4 Access Point...4 Business
Directory of Records Workers Compensation Board Alberta Last updated: May 2005 Table of Contents WCB Mandate...3 Organization...3 Introduction...4 How the Directory is Organized...4 Access Point...4 Business
InformatIon for employers
 InformatIon for employers InformatIon for Employers Employers, workers, care providers and the WCB must work together to prevent work injuries and, when injuries happen, get injured workers back to work
InformatIon for employers InformatIon for Employers Employers, workers, care providers and the WCB must work together to prevent work injuries and, when injuries happen, get injured workers back to work
RE: CMS-3819-P; Medicare and Medicaid Programs; Conditions of Participation for Home Health Agencies
 January 6, 2015 Marilyn Tavenner Administrator Centers for Medicare & Medicaid Services Department of Health and Human Services Room 445 G Attention: CMS-3819-P Hubert H. Humphrey Building, 200 Independence
January 6, 2015 Marilyn Tavenner Administrator Centers for Medicare & Medicaid Services Department of Health and Human Services Room 445 G Attention: CMS-3819-P Hubert H. Humphrey Building, 200 Independence
Workers Compensation Claims Services Favorable Outcomes for Employers and Employees
 Workers Compensation Claims Services Favorable Outcomes for Employers and Employees Medical Case Management Resources Preferred Medical Provider Networks Nurse Case Managers Pharmacy Benefit Management
Workers Compensation Claims Services Favorable Outcomes for Employers and Employees Medical Case Management Resources Preferred Medical Provider Networks Nurse Case Managers Pharmacy Benefit Management
WORK HARDENING/WORK CONDITIONING TREATMENT GUIDELINES
 WORK HARDENING/WORK CONDITIONING TREATMENT GUIDELINES recommended by the PHYSICIAN ADVISORY COMMITTEE (Adopted by the Admilustrator of the Oklahoma Workers' Compensation Collrt on August 1,2001) Effective
WORK HARDENING/WORK CONDITIONING TREATMENT GUIDELINES recommended by the PHYSICIAN ADVISORY COMMITTEE (Adopted by the Admilustrator of the Oklahoma Workers' Compensation Collrt on August 1,2001) Effective
Return to Work/Injury Management Plan
 Return to Work/Injury Management Plan (Incorporating initial assessment and subsequent reviews of RTW or IM Plans) Type of plan please 4 Return to Work Plan (RTWP) Injury Management Plan (IMP) Worker details
Return to Work/Injury Management Plan (Incorporating initial assessment and subsequent reviews of RTW or IM Plans) Type of plan please 4 Return to Work Plan (RTWP) Injury Management Plan (IMP) Worker details