Spine Trauma. Vertebral Column Injuries
|
|
|
- Christiana Burns
- 8 years ago
- Views:
Transcription
1 Spine Trauma Vertebral Column Injuries Srinivas Prasad, MS, MD Assistant Professor Neurologic and Orthopedic Surgery Thomas Jefferson University Staff Neurosurgeon St. Mary s Medical Center

2 Presentation Overview Spinal Anatomy Incidence Cervical fractures Thoracolumbar fractures

3 Spine Anatomy Overview Two Components Spinal Column Stack of blocks called vertebral bodies 24 vertebral bodies 3 Zones Cervical Thoracic Lumbar Neural Elements

4 Spine Anatomy Overview Two Components Spinal Column Neural Elements Spinal Cord Starts at the brainstem Ends around L1 Spinal Nerves Exit spine at each level Numbered according to level of spinal column they come out of

5 Spine Anatomy Spinal Column Overall 24 mobile vertebral bodies 3 Zones Cervical Spine 7 Vertebral Bodies Thoracic Spine 12 Vertebral Bodies Lumbar Spine 5 Vertebral Bodies



6 Spine Anatomy Spinal Column Vertebral Body Vertebral Bodies Body Pedicle Transverse Process Facet Joints Spinous Process

7 Spine Anatomy Intervertebral Disc Nucleus Pulposus: 70-90% water Annulus fibrosis: Concentric, oblique, overlapping lamellae Largest Avasular Structure in the Human Body

8 Spine Anatomy Alignment and Balance Lordosis Curved backwards Normal in: Cervical Lumbar Kyphosis Curved Forward Normal in Thoracic Aging is kyphogenic



9 Spine Anatomy Alignment and Balance Local Malalignment Causes compensatory changes May cause global Malalignment Sagittal Balance Very Important Coronal Balance Less Important

10 Spine Anatomy Spinal Column Protects nervous structures Supports the head: Vision Ambulation Respiration Stability Anterior column: Load-bearing Posterior column: Tension band

11 Spine Anatomy Occiput-C2 Complex OCC-C2 50% Flex/Ext 50% Rotation Transverse Atlanto- Axial Ligament Atlanto-Alar portion of Alar Ligament Apical Ligament C2 to clivus

12 Spine Anatomy Cervical Range of Motion Flexion-Extension C C C C C7-T1 4-7 White and Panjabi, Clinical Biomechanics of the Spine

13 Spine Anatomy Thoracic Spine 12 Vertebra Unique topography T1 to T9 T10-T12 Rib cage Increases stiffness 400% Facets Coronal plane



14 Concentrates at apex Spine Anatomy Thoracic and Thoracolumbar Biomechanics usually T6 T8 fracture focus Change in loading patterns thoracic = anterior lumbar = posterior thoracolumbar = middle

15 Spine Anatomy Lumbar Anatomy and Biomechanics 5 vertebrae kidney shaped Sagittal facet joints Increased loads No spinal cord

16 Neurological Exam C 5 C 6 C 7 C 8 MOTOR Deltoid/ Biceps Wrist Extensor/ Biceps Triceps/ Wrist Flexors Intrinsics/grasp REFLEX Biceps Brachioradialis Triceps Ø SENSORY DEFICIT Shoulder Thumb/ Index Long 4 th /5 th

17 Spinal Cord Injury

18 Spinal Cord Injury Demographics

19 Spinal Cord Injury Demographics

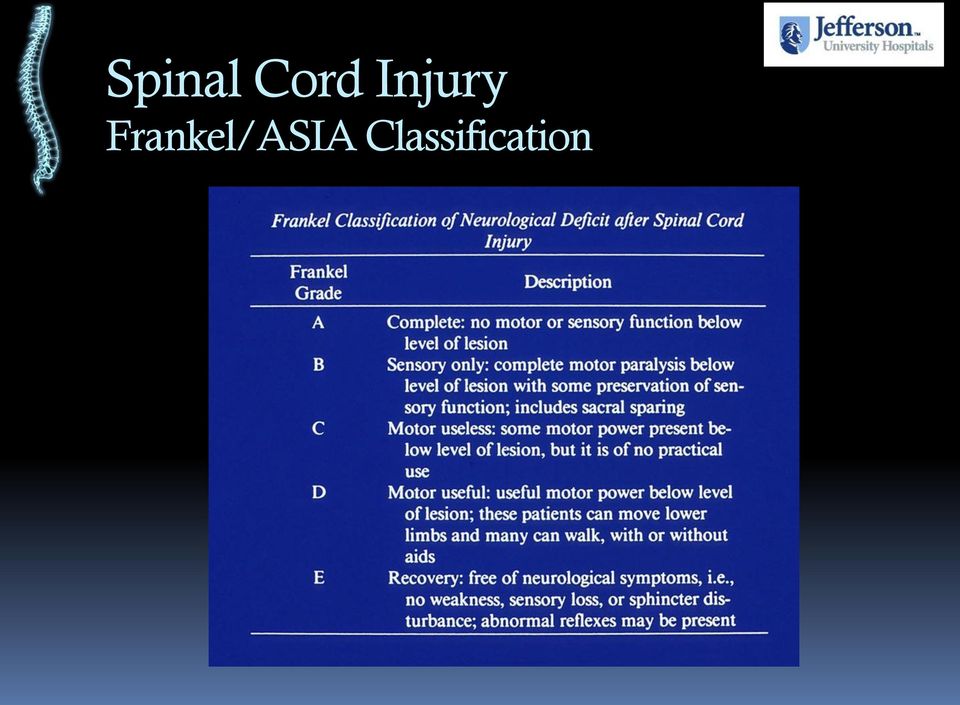
20 Spinal Cord Injury Frankel/ASIA Classification
21 Initial Mechanical Injury (Primary Injury) Acute Pathophysiologic Responses (Secondary Injury) -local ischemia -electrolyte imbalances -free radical formation/lipid peroxidation -inflammation/immunologic response -necrotic & apoptotic cell death Chronic Neuropathology -disrupted/demyelinated axons -glial scar & cystic cavitation
22 Spinal Cord Injury Timing of Decompression Animal Model 0 hr 2 hr 6 hr 24 hr improved neurorecovery 72 hr Dimar, et al. The influence of spinal canal narrowing & timing of decompression on neurologic recovery after Spinal cord contusion in a rat model. Spine 1999
23 Spinal Cord Injury Practice Patterns Timing of Surgery in Acute SCI Tator, Fehlings, et al, J Neurosurg, North American Centers 585 pts % of patients <24h 25-48h 48-96h >5 days Time to surgery
24 Spinal Cord Injury Clinical Studies ( ) Timing of Surgery Author No. Patients (level) Timing of intervention Study design (class of evidence) Conclusions McKinley (2004) 779(all):603 decompressed, 176 nonop 73 underwent decompression <24h Retrospective case series (III) Early (<72h) decomp did not improve neuro recov, but decreases complications/hosp stay LaRosa (2004) 1683(all):793 decompressed, 890 nonop 226 underwent decompression <24h Systematic lit review uo to 2000 (II) Early decomp improves neuro recov in incomplete injuries Pollard/Apple (2005) 412 (cervical) incomplete injuries Retrospective case series;baseline neuro assess NA in 51% of cases (III) Early decomp (<24h) not assoc w/ improved recovery: incomplete baseline and f/u assessments limit utility Papadopoulos (2002) 91 (cervical):66 decompressed, 25 nonoperative 34 underwent surgical decompression <10h Prospective, nonrandomized (II) Early decomp feasible, may improve neuro recov and decreases hosp stay Pointillart (2000) 106 (levels): 58 (cervical) 49 underwent surgical decompression <8h Prospective, nonrandomized (II) Early surgery did not improve neuro recovery
 Prospective cohort study Cervical Trauma with SCI and Cord Compression")

25 Spinal Cord Injury STASCIS Surgical Trial in Acute SCI Study PI: Michael Fehlings (U of T) Alex Vaccaro (TJU) Prospective cohort study Cervical Trauma with SCI and Cord Compression Multivariate analysis to examine affect of timing of decompression on outcome after SCI Krembil Foundation American Spinal Injury Association AANS/CNS Section on Neurotrauma and Critical Care

26 Spinal Cord Injury STASCIS Early vs Delayed Surgery Potential Covariates ISS Scores; Charleston Comorbidity Index: NSD

27 Spinal Cord Injury STASCIS One Year Outcomes AIS N=118; 1 yr f/u Poisson regression p<0.005
28 Spinal Cord Injury STASCIS One Year Outcomes AIS There was a trend for higher complications rates (46%) in the late group compared to the early group (36%) main difference: reduction in ventilator associated pneumonia Complications Prior to Discharge by Time to Decompression Were there any complications prior to discharge? Yes No Total Time to Decompression Early Late Total Count Column N % Count Column N % Count Column N % % % % % % % % % %
29 Spinal Cord Injury Spinal Instability Difficult to define Anatomic disruption Spinal malalignment
30 Thoracolumbar Trauma White-Panjabi Definition of Stability Definition the ability of the spine under physiologic loads to prevent initial or additional neurologic damage, severe intractable pain, and gross deformity White and Panjabi, Clinical Biomechanics of the Spine 1990
31 Routine Trauma Workup
32 Routine Trauma Protocols C-Spine Clearance Algorithms NEXUS criteria (No Films): 1. No neurologic abnormalities 2. No evidence of intoxication 3. No posterior midline cervical spine tenderness 4. No other distracting injuries Dynamic flex/ext (Timing?) Unconscious patient Static bump induced flexion views Dynamic fluoroscopic exam-timing? Eastern Association for the Surgery of Trauma c-spine clearance guidelines Schenarts PJ. J Trauma. Oct 2001.?
33 Routine Trauma Protocols C-Spine Plain Film Landmarks ADI < 3 mm in adult < 5 mm in children Soft tissue retropharyngeal space C2 < 6 mm Retrotracheal space C6 < 22 mm in adult < 14 mm in children
 Final discharge diagnosis based: clinical data MCT Plain films Sixty of 667 (9%) sustained acute c-spine injuries")
34 Prospective unblinded c-spine evaluation 667 trauma patients (Blunt trauma 99%) Average age was 35.4 years and 70% were male Cervical three-view plain films Multidetector CT scan (MCT) Final discharge diagnosis based: clinical data MCT Plain films Sixty of 667 (9%) sustained acute c-spine injuries MCT had a sensitivity of 100% and specificity of 99.5% Plain films had a sensitivity of 45% and specificity of 97.4% Plain radiography missed 15 of 27 (55.5%) clinically significant c-spine injuries. J Trauma: Vol 62(6), 2007
:2079-84 34 patients with thoracolumbar spinal fractures evaluated Palpation of the interspinous gap, Plain radiography MRI before operation with fat-suppressed T2-weighted sequence")
35 Reliability of magnetic resonance imaging in detecting posterior ligament complex injury in thoracolumbar spinal fractures Lee HM, et al: Spine Aug 15;25(16): patients with thoracolumbar spinal fractures evaluated Palpation of the interspinous gap, Plain radiography MRI before operation with fat-suppressed T2-weighted sequence Wide interspinous gap was palpated in 14 patients Plain radiography noted 21 patients MRI suspected injury Supraspinous ligament - 27 patients Interspinous ligament - 30 patients Ligamentum flavum - 9 patients Operative findings 28 supraspinous ligament injuries 29 interspinous ligament injuries 7 ligamentum flavum injuries
36 Spine Trauma Injury Patterns and Management
37 Spine Injury Management Management Principles Goals of treatment Maximize neurologic recovery Prevent decline and deformities (i.e. stabilize spine) Maximize pain relief Instability Mechanical Neurologic Both Mechanical and Neurologic
38 Pre-hospital and Emergency Room Care
39 Non-Operative Treatment Immobilization Collars and Braces
40 Non-Operative Treatment Immobilization Collars and Braces
41 Non-Operative Treatment Immobilization Halo Vest
42 Operative Treatment Surgical Approach Posterior (Dorsal) Anterior (Ventral) Combined
43 Operative Treatment Factors affecting Surgical Approach Column(s) disrupted Site of neural compression Upper cervical vs subaxial Spinal deformity Degree of spinal instability
44 Operative Treatment The Role of Instrumentation Instrumentation provides for maturation of fusion
45 Common Injury Patterns and Management

46 Atlanto-Occipital Dislocation Occipito-Cervical Fusion
47 Jefferson (C1) Fracture Axial load injury Jefferson G, Br J Surg, 7:407, 1920.
48 Atlanto-Axial Instability
49 Odontoid Fractures 10-15% of all cervical fractures Flexion > extension injury Estimated 25-40% fatality Anderson and D Alonzo classification Crockard HA et al., J Neurosurg, 78: , 1993.
50 Odontoid Fractures Type I Fractures Rare Upper tip of dens Avulsion of alar ligament Stable fracture by itself? May be a manifestation of atlanto-occipital dislocation. Scott EW, et al., J Neurosurg, 72:488-92, 1990.
51 Odontoid Fractures Type II Fractures Type II Lower half of dens Unstable fracture High non-union rate Type II a 3% of type II fractures Comminuted fracture Free fracture fragments Hadley MN, et al., Neurosurgery, 22:67-71, 1988.
52 Odontoid Fractures Type III Fractures Not a true odontoid fracture Fracture through body of C2 Greater/large surface area Cancellous bone Better vascular supply Usually heal non-operatively
53 Odontoid Fractures General Treatment Considerations Type I stable? Type II surgery vs external immobilization Age of patient (>40-55) Age of fracture (> 2weeks) Displacement of Dens (>4 6 mm) Posterior displaced Tobacco use Type IIa Type III - surgery vs external immobilization Displacement of Dens
54 82 y/o female with posterior displaced odontoid fracture s/p fall
55 Odontoid Fractures Surgical Management Odontoid Screw
56 Odontoid Fractures Surgical Management Posterior C1-2 Fusion
57 Hangman s Fractures Fracture through C2 isthmus Judicial Distraction and shearing Accidental vary by type Neurological Intact Effendi B, J Bone Joint Surg, 63-B(3):319-27, 1981.
58 Hangman s Fractures Controversial treatment Type I collar Type II halo for 3-5mm subluxation with <10º angulation Operative fixation if > 5mm or > 10º Type IIa halo vest with compression Type III require surgical intervention Francis WR, et al., J Bone Joint Surg, 63B:313-18, 1981.
59 Central Cord Syndrome Incomplete Spinal Cord Injury
60 Central Cord Syndrome Incomplete Spinal Cord Injury
61 Central Cord Syndrome Surgical Management
62 Cervical Burst Fracture Potential for Spinal Cord Injury
63 Cervical Burst Fracture Surgical Management
64 Cervical Burst Fracture Surgical Management
65 Cervical Facet Dislocation Fracture Morphology
66 Unilateral Facet Dislocation Fracture Morphology 25% Subluxation of vertebrae
67 Bilateral Facet Dislocation Fracture Morphology
68 Closed Reduction Techniques Prerequisites Awake, cooperative patient Experienced physicians Dedicated radiology technician Complete cervical spine series No evidence of skull fracture Vaccaro, Spine 1999
69 Closed Reduction Techniques Early Closed Reduction Reduction < 8 hrs post injury Greater Neuro recovery compared to age, injury matched controls Cotler, NASS 92

70 Thoracolumbar Fractures Denis Classification Major injuries divided into four categories: Compression fractures Burst fractures Seat belt-type injuries Fracture-dislocations 16 Subtypes 3-5 Subtypes each Denis, Spine, 1983
71 Thoracic Compression Fractures Kyphoplasty Pre-operative Post Vertebral Kyphoplasty Augmentation

72 Thoracic Compression Fractures Kyphoplasty Pre-operative Post Vertebral Kyphoplasty Augmentation
73 Thoracolumbar Burst Fractures Fracture Morphology
74 Thoracolumbar Burst Fractures Conservative Management = 4 5
75 Thoracolumbar Burst Fractures SCI Surgical Management L1 Burst Fracture Conus Injury T12 Body L2 Body
76 Thoracolumbar Burst Fractures Progressive Kyphosis Surgical Management 8 26 A B
77 Thoracolumbar Burst Fracture Surgical Management Anterior Approach Visualization of pathology & more consistent decompression of spinal cord Reconstruction of anterior column
78 Thoracolumbar Burst Fracture Surgical Management Anterior Approach
79 Thoracolumbar Burst Fracture Surgical Management Anterior Approach
80 Thoracolumbar Burst Fracture Surgical Management Anterior Approach
81 Thoracolumbar Burst Fracture Surgical Management Anterior Approach Plate Dura
82 Thoracolumbar Burst Fracture Surgical Management Anterior Approach Screws 45 and 40mm Bicortical Screws No coronal abnormality Plate Flate Graft in position Screws not in the canal End plates parallel
83 Thoracolumbar Burst Fracture Surgical Management Posterior Approach
84 Thoracolumbar Burst Fracture Surgical Management Posterior Approach
85 Thoracolumbar Burst Fracture Surgical Management Anterior & Posterior
86 Conclusions Spine Trauma is common and increasing in incidence Prompt immobilization is essential until comprehensive workup is complete Fracture Morphology and Neurological status are central factors in management Hospital care makes a big difference in minimizing secondary injury
87 Thanks!
Evaluation and Treatment of Spine Fractures. Lara C. Portmann, MSN, ACNP-BC
 Evaluation and Treatment of Spine Fractures Lara C. Portmann, MSN, ACNP-BC Nurse Practitioner, Neurosurgery, Trauma Services, Intermountain Medical Center; Salt Lake City, Utah Objectives: Identify the
Evaluation and Treatment of Spine Fractures Lara C. Portmann, MSN, ACNP-BC Nurse Practitioner, Neurosurgery, Trauma Services, Intermountain Medical Center; Salt Lake City, Utah Objectives: Identify the
Objectives. Spinal Fractures: Classification Diagnosis and Treatment. Level of Fracture. Neuro exam Muscle Grading
 Objectives Spinal Fractures: Classification Diagnosis and Treatment Johannes Bernbeck,, MD Review and apply the understanding of incidence and etiology of VCF. Examine conservative and operative management
Objectives Spinal Fractures: Classification Diagnosis and Treatment Johannes Bernbeck,, MD Review and apply the understanding of incidence and etiology of VCF. Examine conservative and operative management
Instability concept. Symposium- Cervical Spine. Barcelona, February 2014
 Instability concept Guillem Saló Bru, MD, Phd AOSpine Principles Symposium- Cervical Spine Orthopaedic Depatment. Spine Unit. Hospital del Mar. Barcelona. Associated Professor UAB Barcelona, February 2014
Instability concept Guillem Saló Bru, MD, Phd AOSpine Principles Symposium- Cervical Spine Orthopaedic Depatment. Spine Unit. Hospital del Mar. Barcelona. Associated Professor UAB Barcelona, February 2014
Thoracolumbar Spine Fractures. Outline. Outline. Holmes Criteria. Disclosure:
 Thoracolumbar Spine Fractures C. Craig Blackmore, MD, MPH Department of Radiology Virginia Mason Medical Center Affiliate Professor, University of Washington Disclosure: Book Royalties, Springer-Verlag
Thoracolumbar Spine Fractures C. Craig Blackmore, MD, MPH Department of Radiology Virginia Mason Medical Center Affiliate Professor, University of Washington Disclosure: Book Royalties, Springer-Verlag
Spine Trauma: When to Transfer. Alexander Ching, MD Director, Orthopaedic Spine Trauma OHSU
 Spine Trauma: When to Transfer Alexander Ching, MD Director, Orthopaedic Spine Trauma OHSU Disclosures Depuy Spine Consultant (teaching and courses) Department education and research funds Atlas Spine
Spine Trauma: When to Transfer Alexander Ching, MD Director, Orthopaedic Spine Trauma OHSU Disclosures Depuy Spine Consultant (teaching and courses) Department education and research funds Atlas Spine
Vivian Gonzalez Gillian Lieberman, MD. January 2002. Lumbar Spine Trauma. Vivian Gonzalez, Harvard Medical School Year III Gillian Lieberman, MD
 January 2002 Lumbar Spine Trauma Vivian Gonzalez, Harvard Medical School Year III Agenda Anatomy and Biomechanics of Lumbar Spine Three-Column Concept Classification of Fractures Our Patient Imaging Modalities
January 2002 Lumbar Spine Trauma Vivian Gonzalez, Harvard Medical School Year III Agenda Anatomy and Biomechanics of Lumbar Spine Three-Column Concept Classification of Fractures Our Patient Imaging Modalities
C-Spine Injuries. Trauma Rounds
 C-Spine Injuries Trauma Rounds OUTLINE Introduction: Incidence, Importance Normal C-spine Anatomy Clinical Criteria for C-Spine X-rays Imaging Evaluation & Interpretation Fractures: Mechanism, Types, Management
C-Spine Injuries Trauma Rounds OUTLINE Introduction: Incidence, Importance Normal C-spine Anatomy Clinical Criteria for C-Spine X-rays Imaging Evaluation & Interpretation Fractures: Mechanism, Types, Management
Clearing the C Spine
 1. Introduction 2. Clinical Presentation 3. History 4. Physical Exam 5. Diagnosis 6. Investigations 7. Evaluation 8. Management 9. Reference 10. Acknowledgents Clearing the C Spine 1. Introduction: Injury
1. Introduction 2. Clinical Presentation 3. History 4. Physical Exam 5. Diagnosis 6. Investigations 7. Evaluation 8. Management 9. Reference 10. Acknowledgents Clearing the C Spine 1. Introduction: Injury
.org. Fractures of the Thoracic and Lumbar Spine. Cause. Description
 Fractures of the Thoracic and Lumbar Spine Page ( 1 ) Spinal fractures can vary widely in severity. While some fractures are very serious injuries that require emergency treatment, other fractures can
Fractures of the Thoracic and Lumbar Spine Page ( 1 ) Spinal fractures can vary widely in severity. While some fractures are very serious injuries that require emergency treatment, other fractures can
Compression Fractures
 September 2006 Compression Fractures Eleanor Adams Harvard Medical School Year IV Overview Spine Anatomy Thoracolumbar Fractures Cases Compression Fractures, Ddx Radiologic Tests of Choice Treatment Options
September 2006 Compression Fractures Eleanor Adams Harvard Medical School Year IV Overview Spine Anatomy Thoracolumbar Fractures Cases Compression Fractures, Ddx Radiologic Tests of Choice Treatment Options
III./8.4.2: Spinal trauma. III./8.4.2.1 Injury of the spinal cord
 III./8.4.2: Spinal trauma Introduction Causes: motor vehicle accidents, falls, sport injuries, industrial accidents The prevalence of spinal column trauma is 64/100,000, associated with neurological dysfunction
III./8.4.2: Spinal trauma Introduction Causes: motor vehicle accidents, falls, sport injuries, industrial accidents The prevalence of spinal column trauma is 64/100,000, associated with neurological dysfunction
Thoracolumbar Fratures R1: 胡 家 瑞 指 导 老 师 : 吴 轲 主 任
 Thoracolumbar Fratures R1: 胡 家 瑞 指 导 老 师 : 吴 轲 主 任 Patient Data Name: 苏 XX Gender: Female Age:47 years old Admission date: 2010.06.09 Chief complaint Fell down from 4-54 5 meter tree and lead to lumbosacral
Thoracolumbar Fratures R1: 胡 家 瑞 指 导 老 师 : 吴 轲 主 任 Patient Data Name: 苏 XX Gender: Female Age:47 years old Admission date: 2010.06.09 Chief complaint Fell down from 4-54 5 meter tree and lead to lumbosacral
Cervical Spondylotic Myelopathy Associated with Kyphosis or Sagittal Sigmoid Alignment: Outcome after Anterior or Posterior Decompression
 Cervical Spondylotic Myelopathy Associated with Kyphosis or Sagittal Sigmoid Alignment: Outcome after Anterior or Posterior Decompression 1 Journal of Neurosurgery: Spine November 2009, Volume 11, pp.
Cervical Spondylotic Myelopathy Associated with Kyphosis or Sagittal Sigmoid Alignment: Outcome after Anterior or Posterior Decompression 1 Journal of Neurosurgery: Spine November 2009, Volume 11, pp.
Upper Cervical Spine - Occult Injury and Trigger for CT Exam
 Upper Cervical Spine - Occult Injury and Trigger for CT Exam Bakman M, Chan K, Bang C, Basu A, Seo G, Monu JUV Department of Imaging Sciences University of Rochester Medical Center, Rochester, NY Introduction
Upper Cervical Spine - Occult Injury and Trigger for CT Exam Bakman M, Chan K, Bang C, Basu A, Seo G, Monu JUV Department of Imaging Sciences University of Rochester Medical Center, Rochester, NY Introduction
Complications in Adult Deformity Surgery
 Complications in Adult Deformity Surgery Proximal Junctional Kyphosis: Thoracolumbar and Cervicothoracic Sigurd Berven, MD Professor in Residence UC San Francisco Disclosures Research/Institutional Support:
Complications in Adult Deformity Surgery Proximal Junctional Kyphosis: Thoracolumbar and Cervicothoracic Sigurd Berven, MD Professor in Residence UC San Francisco Disclosures Research/Institutional Support:
Spine and Spinal Cord Injuries. William Schecter, MD
 Spine and Spinal Cord Injuries William Schecter, MD Anatomy of the Spine http://education.yahoo.com/reference/gray/fig/387.html Anatomy of the spine 7 cervical vertebrae 12 thoracic vertebrae 5 lumbar
Spine and Spinal Cord Injuries William Schecter, MD Anatomy of the Spine http://education.yahoo.com/reference/gray/fig/387.html Anatomy of the spine 7 cervical vertebrae 12 thoracic vertebrae 5 lumbar
Assessment & Treatment of Fractures and Dislocations of the Thoracic and Lumbar Spine. Brian Drew, MD
 Assessment & Treatment of Fractures and Dislocations of the Thoracic and Lumbar Spine Brian Drew, MD Introduction Mechanism of injuries to the thoracolumbar spine Assessment of spinal stability Treatment
Assessment & Treatment of Fractures and Dislocations of the Thoracic and Lumbar Spine Brian Drew, MD Introduction Mechanism of injuries to the thoracolumbar spine Assessment of spinal stability Treatment
Cervical-Spine Injuries: Catastrophic Injury to Neck Sprain. Seth Cheatham, MD
 Cervical-Spine Injuries: Catastrophic Injury to Neck Sprain Seth Cheatham, MD 236 Seth A. Cheatham, MD VCU Sports Medicine I have no financial disclosures Contact sports, specifically football, places
Cervical-Spine Injuries: Catastrophic Injury to Neck Sprain Seth Cheatham, MD 236 Seth A. Cheatham, MD VCU Sports Medicine I have no financial disclosures Contact sports, specifically football, places
Maricopa Integrated Health System: Administrative Policy & Procedure
 Maricopa Integrated Health System: Administrative Policy & Procedure Effective Date: 03/05 Reviewed Dates: 09/05, 9/08 Revision Dates: Policy #: 64500 S Policy Title: Cervical & Total Spine Clearance and
Maricopa Integrated Health System: Administrative Policy & Procedure Effective Date: 03/05 Reviewed Dates: 09/05, 9/08 Revision Dates: Policy #: 64500 S Policy Title: Cervical & Total Spine Clearance and
Thoracolumbar and Lumbar Burst Fractures. Sussan Salas, MD Thomas Jefferson University Hospital Department of Neurological Surgery
 Thoracolumbar and Lumbar Burst Fractures Sussan Salas, MD Thomas Jefferson University Hospital Department of Neurological Surgery Thoracolumbar/Lumbar Burst Fractures: Overview Epidemiology Anatomy Initial
Thoracolumbar and Lumbar Burst Fractures Sussan Salas, MD Thomas Jefferson University Hospital Department of Neurological Surgery Thoracolumbar/Lumbar Burst Fractures: Overview Epidemiology Anatomy Initial
Cervical Conditions: Diagnosis and Treatments
 Cervical Conditions: Diagnosis and Treatments Mark R Mikles, M.D. Cervical Conditions: Diagnosis and Treatment Cervical conditions Neck Pain Radiculopathy Myelopathy 1 Cervical Conditions: Diagnosis and
Cervical Conditions: Diagnosis and Treatments Mark R Mikles, M.D. Cervical Conditions: Diagnosis and Treatment Cervical conditions Neck Pain Radiculopathy Myelopathy 1 Cervical Conditions: Diagnosis and
Cervical Spine Imaging
 March 20, 2006 Cervical Spine Imaging Johannes Kratz, Harvard Medical School Year IV 1 Overview Background Clinical Cases Diagnostic Tests and a Decision-Tree Algorithm Examples of Cervical Spine Evaluations
March 20, 2006 Cervical Spine Imaging Johannes Kratz, Harvard Medical School Year IV 1 Overview Background Clinical Cases Diagnostic Tests and a Decision-Tree Algorithm Examples of Cervical Spine Evaluations
Minimally Invasive Spine Surgery For Your Patients
 Minimally Invasive Spine Surgery For Your Patients Lukas P. Zebala, M.D. Assistant Professor Orthopaedic and Neurological Spine Surgery Department of Orthopaedic Surgery Washington University School of
Minimally Invasive Spine Surgery For Your Patients Lukas P. Zebala, M.D. Assistant Professor Orthopaedic and Neurological Spine Surgery Department of Orthopaedic Surgery Washington University School of
If you or a loved one have suffered because of a negligent error during spinal surgery, you will be going through a difficult time.
 If you or a loved one have suffered because of a negligent error during spinal surgery, you will be going through a difficult time. You may be worried about your future, both in respect of finances and
If you or a loved one have suffered because of a negligent error during spinal surgery, you will be going through a difficult time. You may be worried about your future, both in respect of finances and
Return to same game if sx s resolve within 15 minutes. Return to next game if sx s resolve within one week Return to Competition
 Assessment Skills of the Spine on the Field and in the Clinic Ron Burke, MD Cervical Spine Injuries Sprains and strains Stingers Transient quadriparesis Cervical Spine Injuries Result in critical loss
Assessment Skills of the Spine on the Field and in the Clinic Ron Burke, MD Cervical Spine Injuries Sprains and strains Stingers Transient quadriparesis Cervical Spine Injuries Result in critical loss
Spinal Fractures Classification System
 Spinal Fractures Classification System an AOSpine Knowledge Forum initiative Cervical Spine Fractures Thoracolumbar Spine Fractures Sacral Spine Fractures AOSpine the leading global academic community
Spinal Fractures Classification System an AOSpine Knowledge Forum initiative Cervical Spine Fractures Thoracolumbar Spine Fractures Sacral Spine Fractures AOSpine the leading global academic community
Patient Information. Anterior Cervical Discectomy and Fusion Surgery (ACDF).
.") Patient Information. Anterior Cervical Discectomy and Fusion Surgery (ACDF). Understanding your spine Disc Between each pair of vertebrae there is a disc that acts as a cushion to protect the vertebra,
Patient Information. Anterior Cervical Discectomy and Fusion Surgery (ACDF). Understanding your spine Disc Between each pair of vertebrae there is a disc that acts as a cushion to protect the vertebra,
Whiplash injuries can be visible by functional magnetic resonance imaging. Pain Research and Management Autumn 2006; Vol. 11, No. 3, pp.
 Whiplash injuries can be visible by functional magnetic resonance imaging 1 Bengt H Johansson, MD FROM ABSTRACT: Pain Research and Management Autumn 2006; Vol. 11, No. 3, pp. 197-199 Whiplash trauma can
Whiplash injuries can be visible by functional magnetic resonance imaging 1 Bengt H Johansson, MD FROM ABSTRACT: Pain Research and Management Autumn 2006; Vol. 11, No. 3, pp. 197-199 Whiplash trauma can
Patient Information. Lateral Lumbar Interbody Fusion Surgery (LLIF).
.") Patient Information. Lateral Lumbar Interbody Fusion Surgery (LLIF). Understanding your spine Disc Between each pair of vertebrae there is a disc that acts as a cushion to protect the vertebra, allows
Patient Information. Lateral Lumbar Interbody Fusion Surgery (LLIF). Understanding your spine Disc Between each pair of vertebrae there is a disc that acts as a cushion to protect the vertebra, allows
Study on Structural Behaviour of Human Vertebral Column Using Staad.Pro
 Study on Structural Behaviour of Human Vertebral Column Using Staad.Pro Healtheephan alexis. S Post graduate student, Government College of Technology, Coimbatore 641 013 healtheephan@yahoo.com ABSTRACT
Study on Structural Behaviour of Human Vertebral Column Using Staad.Pro Healtheephan alexis. S Post graduate student, Government College of Technology, Coimbatore 641 013 healtheephan@yahoo.com ABSTRACT
Cervical Spine Trauma: Pearls and Pitfalls
 Cervical Spine Trauma: Pearls and Pitfalls Mark P. Bernstein 1, Alexander B. Baxter Accurate diagnosis of acute cervical spine injury requires cooperation between clinician and radiologist, a reliable
Cervical Spine Trauma: Pearls and Pitfalls Mark P. Bernstein 1, Alexander B. Baxter Accurate diagnosis of acute cervical spine injury requires cooperation between clinician and radiologist, a reliable
Spinal Instability as Defined by the Three-column Spine Concept in Acute Spinal Trauma
 Spinal Instability as Defined by the Three-column Spine Concept in Acute Spinal Trauma FRANCIS DENIS, M.D., F.R.C.S.(C.), F.A.C.S.* This article is a presentation of the concept of the three-column spine.
Spinal Instability as Defined by the Three-column Spine Concept in Acute Spinal Trauma FRANCIS DENIS, M.D., F.R.C.S.(C.), F.A.C.S.* This article is a presentation of the concept of the three-column spine.
Cervical Spine Surgery. Orthopaedic Nursing Seminar. Dr Michelle Atkinson. Friday October 21 st 2011. Cervical Disc Herniation
 Cervical Spine Surgery Dr Michelle Atkinson The Sydney and Dalcross Adventist Hospitals Orthopaedic Nursing Seminar Friday October 21 st 2011 Cervical disc herniation The most frequently treated surgical
Cervical Spine Surgery Dr Michelle Atkinson The Sydney and Dalcross Adventist Hospitals Orthopaedic Nursing Seminar Friday October 21 st 2011 Cervical disc herniation The most frequently treated surgical
CERVICAL SPINE CLEARANCE
 DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
Biomechanics of the Lumbar Spine
 Biomechanics of the Lumbar Spine Biomechanics of the Spine 6 degrees of freedom Extension & Flexion Translation Rotation Compression & Distraction The disc/annulus/all/pll complex is the major restraint
Biomechanics of the Lumbar Spine Biomechanics of the Spine 6 degrees of freedom Extension & Flexion Translation Rotation Compression & Distraction The disc/annulus/all/pll complex is the major restraint
ANTERIOR CERVICAL DISCECTOMY AND FUSION. Basic Anatomical Landmarks: Anterior Cervical Spine
 Anterior In the human anatomy, referring to the front surface of the body or position of one structure relative to another Cervical Relating to the neck, in the spine relating to the first seven vertebrae
Anterior In the human anatomy, referring to the front surface of the body or position of one structure relative to another Cervical Relating to the neck, in the spine relating to the first seven vertebrae
Cervical Spine Injuries in Hockey. Joel L. Boyd, MD Minnesota Wild
 Cervical Spine Injuries in Hockey Joel L. Boyd, MD Minnesota Wild DISCLOSURES Case example: Hey, doc. My neck hurts. 30 yo NFL lineman involved in head-tohead collision during a preseason game Player continued
Cervical Spine Injuries in Hockey Joel L. Boyd, MD Minnesota Wild DISCLOSURES Case example: Hey, doc. My neck hurts. 30 yo NFL lineman involved in head-tohead collision during a preseason game Player continued
INJURIES OF THE HAND AND WRIST By Derya Dincer, M.D.
 05/05/2007 INJURIES OF THE HAND AND WRIST By Derya Dincer, M.D. Hand injuries, especially the fractures of metacarpals and phalanges, are the most common fractures in the skeletal system. Hand injuries
05/05/2007 INJURIES OF THE HAND AND WRIST By Derya Dincer, M.D. Hand injuries, especially the fractures of metacarpals and phalanges, are the most common fractures in the skeletal system. Hand injuries
Pediatric Cervical Spine Trauma. When Is Cross-sectional Imaging Needed? Susan D. John, M.D.
 Pediatric Cervical Spine Trauma When Is Cross-sectional Imaging Needed? Susan D. John, M.D. Spine Fractures in Children Uncommon 1-3% of pediatric trauma patients 60-80% spine fxs in children involve C-spine,
Pediatric Cervical Spine Trauma When Is Cross-sectional Imaging Needed? Susan D. John, M.D. Spine Fractures in Children Uncommon 1-3% of pediatric trauma patients 60-80% spine fxs in children involve C-spine,
DUKE ORTHOPAEDIC SURGERY GOALS AND OBJECTIVES SPINE SERVICE
 GOALS AND OBJECTIVES PATIENT CARE Able to perform a complete musculoskeletal and neurologic examination on the patient including cervical spine, thoracic spine, and lumbar spine. The neurologic examination
GOALS AND OBJECTIVES PATIENT CARE Able to perform a complete musculoskeletal and neurologic examination on the patient including cervical spine, thoracic spine, and lumbar spine. The neurologic examination
Thoracic Spine Anatomy
 A Patient s Guide to Thoracic Spine Anatomy 228 West Main, Suite C Missoula, MT 59802 Phone: info@spineuniversity.com DISCLAIMER: The information in this booklet is compiled from a variety of sources.
A Patient s Guide to Thoracic Spine Anatomy 228 West Main, Suite C Missoula, MT 59802 Phone: info@spineuniversity.com DISCLAIMER: The information in this booklet is compiled from a variety of sources.
Upper Cervical Spine Fusion
 1 Surgical Indications and Considerations Upper Cervical Spine Fusion Anatomical Considerations: The occiput-c1 articulations primarily allow for flexion and extension movements and the C1-C2 articulations
1 Surgical Indications and Considerations Upper Cervical Spine Fusion Anatomical Considerations: The occiput-c1 articulations primarily allow for flexion and extension movements and the C1-C2 articulations
Contents. Introduction 1. Anatomy of the Spine 1. 2. Spinal Imaging 7. 3. Spinal Biomechanics 23. 4. History and Physical Examination of the Spine 33
 Contents Introduction 1. Anatomy of the Spine 1 Vertebrae 1 Ligaments 3 Intervertebral Disk 4 Intervertebral Foramen 5 2. Spinal Imaging 7 Imaging Modalities 7 Conventional Radiographs 7 Myelography 9
Contents Introduction 1. Anatomy of the Spine 1 Vertebrae 1 Ligaments 3 Intervertebral Disk 4 Intervertebral Foramen 5 2. Spinal Imaging 7 Imaging Modalities 7 Conventional Radiographs 7 Myelography 9
Minimally Invasive Lumbar Fusion
 Minimally Invasive Lumbar Fusion Biomechanical Evaluation (1) coflex-f screw Biomechanical Evaluation (1) coflex-f intact Primary Stability intact Primary Stability Extension Neutral Position Flexion Coflex
Minimally Invasive Lumbar Fusion Biomechanical Evaluation (1) coflex-f screw Biomechanical Evaluation (1) coflex-f intact Primary Stability intact Primary Stability Extension Neutral Position Flexion Coflex
NEW YORK STATE IN-HOSPITAL CERVICAL SPINE CLEARANCE GUIDELINES IN BLUNT TRAUMA
 Page 1 of 5 NEW YORK STATE IN-HOSPITAL CERVICAL SPINE CLEARANCE GUIDELINES IN BLUNT TRAUMA STAC Evaluation Subcommittee Authors: Jamie S. Ullman, MD FACS, Matthew Bank, MD, FACS, Nelson Rosen, MD, FACS,
Page 1 of 5 NEW YORK STATE IN-HOSPITAL CERVICAL SPINE CLEARANCE GUIDELINES IN BLUNT TRAUMA STAC Evaluation Subcommittee Authors: Jamie S. Ullman, MD FACS, Matthew Bank, MD, FACS, Nelson Rosen, MD, FACS,
CERVICAL DISC HERNIATION
 CERVICAL DISC HERNIATION Most frequent at C 5/6 level but also occur at C 6 7 & to a lesser extent at C4 5 & other levels In relatively younger persons soft disk protrusion is more common than hard disk
CERVICAL DISC HERNIATION Most frequent at C 5/6 level but also occur at C 6 7 & to a lesser extent at C4 5 & other levels In relatively younger persons soft disk protrusion is more common than hard disk
Abstract. Introduction. Case Report. imedpub Journals http://www.imedpub.com/
 Case Report imedpub Journals http://www.imedpub.com/ Unusual 2-Stages Posterior Approach Surgical Treatment for Complete Fracture Dislocation of the Upper Thoracic Spine without Neurologic Deficit: A Case
Case Report imedpub Journals http://www.imedpub.com/ Unusual 2-Stages Posterior Approach Surgical Treatment for Complete Fracture Dislocation of the Upper Thoracic Spine without Neurologic Deficit: A Case
1 REVISOR 5223.0070. (4) Pain associated with rigidity (loss of motion or postural abnormality) or
 Pain associated with rigidity (loss of motion or postural abnormality) or") 1 REVISOR 5223.0070 5223.0070 MUSCULOSKELETAL SCHEDULE; BACK. Subpart 1. Lumbar spine. The spine rating is inclusive of leg symptoms except for gross motor weakness, bladder or bowel dysfunction, or sexual
1 REVISOR 5223.0070 5223.0070 MUSCULOSKELETAL SCHEDULE; BACK. Subpart 1. Lumbar spine. The spine rating is inclusive of leg symptoms except for gross motor weakness, bladder or bowel dysfunction, or sexual
Lumbar Back Pain in Young Athletes
 Lumbar Back Pain in Young Athletes MS CAQ in Sports Medicine Blair Orthopedics Altoona, PA OMED 2012 San Diego CA AOASM Tuesday October 9 th 1:00pm Lumbar Back Pain in Learning ObjecKves Epidemiology Anatomy
Lumbar Back Pain in Young Athletes MS CAQ in Sports Medicine Blair Orthopedics Altoona, PA OMED 2012 San Diego CA AOASM Tuesday October 9 th 1:00pm Lumbar Back Pain in Learning ObjecKves Epidemiology Anatomy
CERVICAL SPONDYLOSIS
 CERVICAL SPONDYLOSIS Dr. Sahni B.S Dy. Chief Medical Officer, ONGC Hospital Panvel-410221,Navi Mumbai,India Introduction The cervical spine consists of the top 7 vertebrae of the spine. These are referred
CERVICAL SPONDYLOSIS Dr. Sahni B.S Dy. Chief Medical Officer, ONGC Hospital Panvel-410221,Navi Mumbai,India Introduction The cervical spine consists of the top 7 vertebrae of the spine. These are referred
Airway Management in Adults after Cervical Spine Trauma Edward T. Crosby, M.D., F.R.C.P.C.*
 REVIEW ARTICLE David C. Warltier, M.D., Ph.D., Editor Anesthesiology 2006; 104:1293 318 2006 American Society of Anesthesiologists, Inc. Lippincott Williams & Wilkins, Inc. Airway Management in Adults
REVIEW ARTICLE David C. Warltier, M.D., Ph.D., Editor Anesthesiology 2006; 104:1293 318 2006 American Society of Anesthesiologists, Inc. Lippincott Williams & Wilkins, Inc. Airway Management in Adults
visualized. The correct level is then identified again. With the use of a microscope and
 SURGERY FOR SPINAL STENOSIS Laminectomy A one inch (or longer for extensive stenosis) incision is made in the middle of the back over the effected region of the spine. The muscles over the bone are moved
SURGERY FOR SPINAL STENOSIS Laminectomy A one inch (or longer for extensive stenosis) incision is made in the middle of the back over the effected region of the spine. The muscles over the bone are moved
Spinal Cord Injury Education. An Overview for Patients, Families, and Caregivers
 Spinal Cord Injury Education An Overview for Patients, Families, and Caregivers Spinal Cord Anatomy A major component of the Central Nervous System (CNS) It is 15 to 16 inches long, and weighs 1 to 2 ounces
Spinal Cord Injury Education An Overview for Patients, Families, and Caregivers Spinal Cord Anatomy A major component of the Central Nervous System (CNS) It is 15 to 16 inches long, and weighs 1 to 2 ounces
Advances In Spine Care. James D. Bruffey M.D. Scripps Clinic Division of Orthopaedic Surgery Section of Spinal Surgery
 Advances In Spine Care James D. Bruffey M.D. Scripps Clinic Division of Orthopaedic Surgery Section of Spinal Surgery Introduction The Spine - A common source of problems Back pain is the #2 presenting
Advances In Spine Care James D. Bruffey M.D. Scripps Clinic Division of Orthopaedic Surgery Section of Spinal Surgery Introduction The Spine - A common source of problems Back pain is the #2 presenting
Spinal Cord Injury. North American Spine Society Public Education Series
 Spinal Cord Injury North American Spine Society Public Education Series What Is a Spinal Cord Injury? A spinal cord injury is a condition that results from damage or trauma to the nerve tissue of the spine.
Spinal Cord Injury North American Spine Society Public Education Series What Is a Spinal Cord Injury? A spinal cord injury is a condition that results from damage or trauma to the nerve tissue of the spine.
Cervical Spinal Injuries
 Cervical Spinal Injuries Common mechanism is extension or axial compression with buckling into extension. Structures most often injured are discs & facets. Disc & facet injuries are equally frequent. Major
Cervical Spinal Injuries Common mechanism is extension or axial compression with buckling into extension. Structures most often injured are discs & facets. Disc & facet injuries are equally frequent. Major
Case Report Chronic Neck Pain Associated with an Old Odontoid Fracture: A Rare Presentation
 Case Reports in Emergency Medicine Volume 2013, Article ID 372723, 4 pages http://dx.doi.org/10.1155/2013/372723 Case Report Chronic Neck Pain Associated with an Old Odontoid Fracture: A Rare Presentation
Case Reports in Emergency Medicine Volume 2013, Article ID 372723, 4 pages http://dx.doi.org/10.1155/2013/372723 Case Report Chronic Neck Pain Associated with an Old Odontoid Fracture: A Rare Presentation
Nonoperative Management of Herniated Cervical Intervertebral Disc With Radiculopathy. Spine Volume 21(16) August 15, 1996, pp 1877-1883
 August 15, 1996, pp 1877-1883") Nonoperative Management of Herniated Cervical Intervertebral Disc With Radiculopathy 1 Spine Volume 21(16) August 15, 1996, pp 1877-1883 Saal, Joel S. MD; Saal, Jeffrey A. MD; Yurth, Elizabeth F. MD FROM
Nonoperative Management of Herniated Cervical Intervertebral Disc With Radiculopathy 1 Spine Volume 21(16) August 15, 1996, pp 1877-1883 Saal, Joel S. MD; Saal, Jeffrey A. MD; Yurth, Elizabeth F. MD FROM
WHIPLASH INJURIES By Prof RP Grabe, Department of Orthopaedics, University of Pretoria
 1 WHIPLASH INJURIES By Prof RP Grabe, Department of Orthopaedics, University of Pretoria In a recent publication in Spine the Quebec task force mentions that very little is available in the literature
1 WHIPLASH INJURIES By Prof RP Grabe, Department of Orthopaedics, University of Pretoria In a recent publication in Spine the Quebec task force mentions that very little is available in the literature
Spine & Nervous System Trauma
 Spine & Nervous System Trauma Andrea L. Williams PhD, RN Emergency Education Specialist Clinical Associate Professor University of Wisconsin School of Nursing http://www.youtube.com/watch?v=g2tdp_7q3n4
Spine & Nervous System Trauma Andrea L. Williams PhD, RN Emergency Education Specialist Clinical Associate Professor University of Wisconsin School of Nursing http://www.youtube.com/watch?v=g2tdp_7q3n4
How To Understand The Anatomy Of A Lumbar Spine
 Sciatica: Low back and Leg Pain Diagnosis and Treatment Options Presented by Devesh Ramnath, MD Orthopaedic Associates Of Dallas Baylor Spine Center Sciatica Compression of the spinal nerves in the back
Sciatica: Low back and Leg Pain Diagnosis and Treatment Options Presented by Devesh Ramnath, MD Orthopaedic Associates Of Dallas Baylor Spine Center Sciatica Compression of the spinal nerves in the back
Cervical Spine: Postmortem Assessment of Accident Injuries Comparison of Radiographic, MR Imaging, Anatomic, and Pathologic Findings
 Cervical Spine: Postmortem Assessment of Accident Injuries Comparison of Radiographic, MR Imaging, Anatomic, and Pathologic Findings 1 Radiology, November, 2001;221:340-346. Axel Stäbler, MD, Jurik Eck,
Cervical Spine: Postmortem Assessment of Accident Injuries Comparison of Radiographic, MR Imaging, Anatomic, and Pathologic Findings 1 Radiology, November, 2001;221:340-346. Axel Stäbler, MD, Jurik Eck,
Spine Anatomy and Spine General The purpose of the spine is to help us stand and sit straight, move, and provide protection to the spinal cord.
 Spine Anatomy and Spine General The purpose of the spine is to help us stand and sit straight, move, and provide protection to the spinal cord. Normal List Kyphosis The human spine has 7 Cervical vertebra
Spine Anatomy and Spine General The purpose of the spine is to help us stand and sit straight, move, and provide protection to the spinal cord. Normal List Kyphosis The human spine has 7 Cervical vertebra
Burst fracture of the fifth lumbar vertebra: results of posterior internal fixation and transpedicular bone grafting
 Eur Spine J (2002) 11 :435 440 DOI 10.1007/s00586-002-0390-1 ORIGINAL ARTICLE A. Kaminski E. J. Müller G. Muhr Burst fracture of the fifth lumbar vertebra: results of posterior internal fixation and transpedicular
Eur Spine J (2002) 11 :435 440 DOI 10.1007/s00586-002-0390-1 ORIGINAL ARTICLE A. Kaminski E. J. Müller G. Muhr Burst fracture of the fifth lumbar vertebra: results of posterior internal fixation and transpedicular
Introduction. Incomplete Cord Injury. Primer for Emergency Medicine Students
 Introduction Radiographic Evaluation of Cervical Spine Injury The single most important treatment for those suspected of having incurred a cervical spine injury is immobilization. Soft cervical collar
Introduction Radiographic Evaluation of Cervical Spine Injury The single most important treatment for those suspected of having incurred a cervical spine injury is immobilization. Soft cervical collar
Spinal Surgery Functional Status and Quality of Life Outcome Specifications 2015 (01/01/2013 to 12/31/2013 Dates of Procedure) September 2014
 September 2014") Description Methodology For patients ages 18 years and older who undergo a lumbar discectomy/laminotomy or lumbar spinal fusion procedure during the measurement year, the following measures will be calculated:
Description Methodology For patients ages 18 years and older who undergo a lumbar discectomy/laminotomy or lumbar spinal fusion procedure during the measurement year, the following measures will be calculated:
Human Anatomy & Physiology
 PowerPoint Lecture Slides prepared by Barbara Heard, Atlantic Cape Community College Ninth Edition Human Anatomy & Physiology C H A P T E R 7 The Skeleton: Part B Annie Leibovitz/Contact Press Images Vertebral
PowerPoint Lecture Slides prepared by Barbara Heard, Atlantic Cape Community College Ninth Edition Human Anatomy & Physiology C H A P T E R 7 The Skeleton: Part B Annie Leibovitz/Contact Press Images Vertebral
The multitude of symptoms following a whiplash injury has given rise to much discussion because of the lack of objective radiological findings.
 HELPFUL PERSONAL INJURY INFORMATION COURTESY OF RIVERVIEW CHIROPRACTIC FROM ABSTRACT: Dynamic kine magnetic resonance imaging in whiplash patients Pain Research and Management 2009 Nov-Dec 2009;Vol. 14,
HELPFUL PERSONAL INJURY INFORMATION COURTESY OF RIVERVIEW CHIROPRACTIC FROM ABSTRACT: Dynamic kine magnetic resonance imaging in whiplash patients Pain Research and Management 2009 Nov-Dec 2009;Vol. 14,
SPINAL FUSION. North American Spine Society Public Education Series
 SPINAL FUSION North American Spine Society Public Education Series WHAT IS SPINAL FUSION? The spine is made up of a series of bones called vertebrae ; between each vertebra are strong connective tissues
SPINAL FUSION North American Spine Society Public Education Series WHAT IS SPINAL FUSION? The spine is made up of a series of bones called vertebrae ; between each vertebra are strong connective tissues
TRAUMA OF THE SPINE AND SPINAL CORD
 TRAUMA OF THE SPINE AND SPINAL CORD Mauricio Castillo, M.D., F.A.C.R. Professor of Radiology and Chief of Neuroradiology University of North Carolina School of Medicine, Chapel Hill, NC Editor-in-Chief,
TRAUMA OF THE SPINE AND SPINAL CORD Mauricio Castillo, M.D., F.A.C.R. Professor of Radiology and Chief of Neuroradiology University of North Carolina School of Medicine, Chapel Hill, NC Editor-in-Chief,
Treating Bulging Discs & Sciatica. Alexander Ching, MD
 Treating Bulging Discs & Sciatica Alexander Ching, MD Disclosures Depuy Spine Teaching and courses K2 Spine Complex Spine Study Group Disclosures Take 2 I am a spine surgeon I like spine surgery I believe
Treating Bulging Discs & Sciatica Alexander Ching, MD Disclosures Depuy Spine Teaching and courses K2 Spine Complex Spine Study Group Disclosures Take 2 I am a spine surgeon I like spine surgery I believe
SPINE ANATOMY AND PROCEDURES. Tulsa Spine & Specialty Hospital 6901 S. Olympia Avenue Tulsa, Oklahoma 74132
 SPINE ANATOMY AND PROCEDURES Tulsa Spine & Specialty Hospital 6901 S. Olympia Avenue Tulsa, Oklahoma 74132 SPINE ANATOMY The spine consists of 33 bones called vertebrae. The top 7 are cervical, or neck
SPINE ANATOMY AND PROCEDURES Tulsa Spine & Specialty Hospital 6901 S. Olympia Avenue Tulsa, Oklahoma 74132 SPINE ANATOMY The spine consists of 33 bones called vertebrae. The top 7 are cervical, or neck
Case Studies Updated 10.24.11
 S O L U T I O N S Case Studies Updated 10.24.11 Hill DT Solutions Cervical Decompression Case Study An 18-year-old male involved in a motor vehicle accident in which his SUV was totaled suffering from
S O L U T I O N S Case Studies Updated 10.24.11 Hill DT Solutions Cervical Decompression Case Study An 18-year-old male involved in a motor vehicle accident in which his SUV was totaled suffering from
BODY BODY PEDICLE PEDICLE TRANSVERSE TRANSVERSE PROCESS PROCESS
 Learning Objective Radiology Anatomy of the Spine and Upper Extremity Identify anatomic structures of the spine and upper extremities on standard radiographic and cross-sectional images Timothy J. Mosher,
Learning Objective Radiology Anatomy of the Spine and Upper Extremity Identify anatomic structures of the spine and upper extremities on standard radiographic and cross-sectional images Timothy J. Mosher,
GUIDELINES FOR ASSESSMENT OF SPINAL STABILITY THE CHRISTIE, GREATER MANCHESTER & CHESHIRE. CP57 Version: V3
 GUIDELINES FOR ASSESSMENT OF SPINAL STABILITY THE CHRISTIE, GREATER MANCHESTER & CHESHIRE Procedure Reference: Document Owner: CP57 Version: V3 Dr V. Misra Accountable Committee: Acute Oncology Group Network
GUIDELINES FOR ASSESSMENT OF SPINAL STABILITY THE CHRISTIE, GREATER MANCHESTER & CHESHIRE Procedure Reference: Document Owner: CP57 Version: V3 Dr V. Misra Accountable Committee: Acute Oncology Group Network
R/F. Applications and Present Issues of Tomosynthesis in Spine Surgery. 87th Annual Meeting of the Japanese Orthopaedic Association Evening Seminar 4
 R/F Applications and Present Issues of Tomosynthesis in Spine Surgery 87th Annual Meeting of the Japanese Orthopaedic Association Evening Seminar 4 Professor and Chairman Department of Orthopaedic Surgery
R/F Applications and Present Issues of Tomosynthesis in Spine Surgery 87th Annual Meeting of the Japanese Orthopaedic Association Evening Seminar 4 Professor and Chairman Department of Orthopaedic Surgery
DIAGNOSING SCAPHOID FRACTURES. Anthony Hewitt
 DIAGNOSING SCAPHOID FRACTURES Anthony Hewitt Introduction Anatomy of the scaphoid Resembles a deformed peanut Articular cartilage covers 80% of the surface It rests in a plane 45 degrees to the longitudinal
DIAGNOSING SCAPHOID FRACTURES Anthony Hewitt Introduction Anatomy of the scaphoid Resembles a deformed peanut Articular cartilage covers 80% of the surface It rests in a plane 45 degrees to the longitudinal
Clinical guidance for MRI referral
 MRI for cervical radiculopathy Referral by a medical practitioner (excluding a specialist or consultant physician) for a scan of spine for a patient 16 years or older for suspected: cervical radiculopathy
MRI for cervical radiculopathy Referral by a medical practitioner (excluding a specialist or consultant physician) for a scan of spine for a patient 16 years or older for suspected: cervical radiculopathy
X Stop Spinal Stenosis Decompression
 X Stop Spinal Stenosis Decompression Am I a candidate for X Stop spinal surgery? You may be a candidate for the X Stop spinal surgery if you have primarily leg pain rather than mostly back pain and your
X Stop Spinal Stenosis Decompression Am I a candidate for X Stop spinal surgery? You may be a candidate for the X Stop spinal surgery if you have primarily leg pain rather than mostly back pain and your
Low Back Injury in the Industrial Athlete: An Anatomic Approach
 Low Back Injury in the Industrial Athlete: An Anatomic Approach Earl J. Craig, M.D. Assistant Professor Indiana University School of Medicine Department of Physical Medicine and Rehabilitation Epidemiology
Low Back Injury in the Industrial Athlete: An Anatomic Approach Earl J. Craig, M.D. Assistant Professor Indiana University School of Medicine Department of Physical Medicine and Rehabilitation Epidemiology
Whiplash and Whiplash- Associated Disorders
 Whiplash and Whiplash- Associated Disorders North American Spine Society Public Education Series What Is Whiplash? The term whiplash might be confusing because it describes both a mechanism of injury and
Whiplash and Whiplash- Associated Disorders North American Spine Society Public Education Series What Is Whiplash? The term whiplash might be confusing because it describes both a mechanism of injury and
Management of spinal cord compression
 Management of spinal cord compression (SUMMARY) Main points a) On diagnosis, all patients should receive dexamethasone 10mg IV one dose, then 4mg every 6h. then switched to oral dose and tapered as tolerated
Management of spinal cord compression (SUMMARY) Main points a) On diagnosis, all patients should receive dexamethasone 10mg IV one dose, then 4mg every 6h. then switched to oral dose and tapered as tolerated
The Petrylaw Lawsuits Settlements and Injury Settlement Report
 The Petrylaw Lawsuits Settlements and Injury Settlement Report BACK INJURIES How Minnesota Juries Decide the Value of Pain and Suffering in Back Injury Cases The Petrylaw Lawsuits Settlements and Injury
The Petrylaw Lawsuits Settlements and Injury Settlement Report BACK INJURIES How Minnesota Juries Decide the Value of Pain and Suffering in Back Injury Cases The Petrylaw Lawsuits Settlements and Injury
On Cervical Zygapophysial Joint Pain After Whiplash. Spine December 1, 2011; Volume 36, Number 25S, pp S194 S199
 On Cervical Zygapophysial Joint Pain After Whiplash 1 Spine December 1, 2011; Volume 36, Number 25S, pp S194 S199 Nikolai Bogduk, MD, PhD FROM ABSTRACT Objective To summarize the evidence that implicates
On Cervical Zygapophysial Joint Pain After Whiplash 1 Spine December 1, 2011; Volume 36, Number 25S, pp S194 S199 Nikolai Bogduk, MD, PhD FROM ABSTRACT Objective To summarize the evidence that implicates
The goals of modern spinal surgery are to maximize
 SPRING 2013 Robot-Guided Spine Surgery Christopher R. Good, M.D., F.A.C.S. and Blair K. Snyder, P.A.-C. The goals of modern spinal surgery are to maximize patient function and accelerate a return to a
SPRING 2013 Robot-Guided Spine Surgery Christopher R. Good, M.D., F.A.C.S. and Blair K. Snyder, P.A.-C. The goals of modern spinal surgery are to maximize patient function and accelerate a return to a
Anatomy of the Spine. Figure 1. (left) The spine has three natural curves that form an S-shape; strong muscles keep our spine in alignment.
 The spine has three natural curves that form an S-shape; strong muscles keep our spine in alignment.") 1 2 Anatomy of the Spine Overview The spine is made of 33 individual bony vertebrae stacked one on top of the other. This spinal column provides the main support for your body, allowing you to stand upright,
1 2 Anatomy of the Spine Overview The spine is made of 33 individual bony vertebrae stacked one on top of the other. This spinal column provides the main support for your body, allowing you to stand upright,
Spine Trauma. Seamus Looby, MD*, Adam Flanders, MD. radiologic.theclinics.com KEYWORDS OVERVIEW OF SPINE TRAUMA. Spine Trauma Cervical Thoracic Lumbar
 Spine Trauma Seamus Looby, MD*, Adam Flanders, MD KEYWORDS Spine Trauma Cervical Thoracic Lumbar Spine trauma is a devastating event with a high morbidity and mortality and many additional medical, psychological,
Spine Trauma Seamus Looby, MD*, Adam Flanders, MD KEYWORDS Spine Trauma Cervical Thoracic Lumbar Spine trauma is a devastating event with a high morbidity and mortality and many additional medical, psychological,
Musculoskeletal Trauma of the Wrist
 September 2000 Musculoskeletal Trauma of the Wrist Murat Akalin, Harvard Medical School, Year- IV Gillian Lieberman, MD The Wrist Most common site of injury in entire skeleton Distal radius and ulna fractures
September 2000 Musculoskeletal Trauma of the Wrist Murat Akalin, Harvard Medical School, Year- IV Gillian Lieberman, MD The Wrist Most common site of injury in entire skeleton Distal radius and ulna fractures
Anatomy and Terminology of the Spine. Bones of the Spine (Vertebrae)
") Anatomy and Terminology of the Spine The spine, also called the spinal column, vertebral column or backbone, consists of bones, intervertebral discs, ligaments, and joints. In addition, the spine serves
Anatomy and Terminology of the Spine The spine, also called the spinal column, vertebral column or backbone, consists of bones, intervertebral discs, ligaments, and joints. In addition, the spine serves
Title: Interspinous Process Decompression with the X-Stop Device for Lumbar Spinal Stenosis: A Retrospective Review. Authors: Jennifer R.
 Title: Interspinous Process Decompression with the X-Stop Device for Lumbar Spinal Stenosis: A Retrospective Review. Authors: Jennifer R. Madonia-Barr, MS, PA-C and David L. Kramer, MD Institution: Connecticut
Title: Interspinous Process Decompression with the X-Stop Device for Lumbar Spinal Stenosis: A Retrospective Review. Authors: Jennifer R. Madonia-Barr, MS, PA-C and David L. Kramer, MD Institution: Connecticut
THE LUMBAR SPINE (BACK)
") THE LUMBAR SPINE (BACK) At a glance Chronic back pain, especially in the area of the lumbar spine (lower back), is a widespread condition. It can be assumed that 75 % of all people have it sometimes or
THE LUMBAR SPINE (BACK) At a glance Chronic back pain, especially in the area of the lumbar spine (lower back), is a widespread condition. It can be assumed that 75 % of all people have it sometimes or
A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH)
") A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH) Introduction Diffuse Idiopathic Skeletal Hyperostosis (DISH) is a phenomenon that more commonly affects older males. It is associated
A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH) Introduction Diffuse Idiopathic Skeletal Hyperostosis (DISH) is a phenomenon that more commonly affects older males. It is associated
IMPAIRMENT RATING 5 TH EDITION MODULE II
 IMPAIRMENT RATING 5 TH EDITION MODULE II THE SPINE AND ALTERATION OF MOTION SEGMENT INTEGRITY (AOMSI) PRESENTED BY: RONALD J. WELLIKOFF, D.C., FACC, FICC In conjuction with: The chapter on the spine includes
IMPAIRMENT RATING 5 TH EDITION MODULE II THE SPINE AND ALTERATION OF MOTION SEGMENT INTEGRITY (AOMSI) PRESENTED BY: RONALD J. WELLIKOFF, D.C., FACC, FICC In conjuction with: The chapter on the spine includes
Spine Injury and Back Pain in Sports
 Spine Injury and Back Pain in Sports DAVID W. GRAY, MD 1 Back Pain Increases with Age Girls>Boys in Teenage years Anywhere from 15 to 80% of children and adolescents have back pain depending on the studies
Spine Injury and Back Pain in Sports DAVID W. GRAY, MD 1 Back Pain Increases with Age Girls>Boys in Teenage years Anywhere from 15 to 80% of children and adolescents have back pain depending on the studies
Imaging of Lisfranc Injury
 November 2011 Imaging of Lisfranc Injury Greg Cvetanovich, Harvard Medical School Year IV Agenda Case Presentation Introduction Anatomy Lisfranc Injury Classification Imaging Treatment 2 Case Presentation
November 2011 Imaging of Lisfranc Injury Greg Cvetanovich, Harvard Medical School Year IV Agenda Case Presentation Introduction Anatomy Lisfranc Injury Classification Imaging Treatment 2 Case Presentation
CERVICAL PROCEDURES PHYSICIAN CODING
 CERVICAL PROCEDURES PHYSICIAN CODING Anterior Cervical Discectomy with Interbody Fusion (ACDF) Anterior interbody fusion, with discectomy and decompression; cervical below C2 22551 first interspace 22552
CERVICAL PROCEDURES PHYSICIAN CODING Anterior Cervical Discectomy with Interbody Fusion (ACDF) Anterior interbody fusion, with discectomy and decompression; cervical below C2 22551 first interspace 22552
A Patient s Guide to the Disorders of the Cervical and Upper Thoracic Spine
 A Patient s Guide to the Disorders of the Cervical and Upper Thoracic Spine General Anatomy of the Spine The spine can be divided into four regions based on vertebral shape and sagittal plane curve.» CERVICAL:
A Patient s Guide to the Disorders of the Cervical and Upper Thoracic Spine General Anatomy of the Spine The spine can be divided into four regions based on vertebral shape and sagittal plane curve.» CERVICAL:
SCAPULAR FRACTURES. Jai Relwani, Shoulder Fellow, Reading Shoulder Unit, Reading.
 SCAPULAR FRACTURES Jai Relwani, Shoulder Fellow, Reading Shoulder Unit, Reading. Aims Anatomy Incidence/Importance Mechanism Classification Principles of treatment Specific variations Conclusion Anatomy
SCAPULAR FRACTURES Jai Relwani, Shoulder Fellow, Reading Shoulder Unit, Reading. Aims Anatomy Incidence/Importance Mechanism Classification Principles of treatment Specific variations Conclusion Anatomy
Adult Spine Rotation Specific Evaluation Orthopaedic Surgery Training Program School of Medicine, Queen s University
 Adult Spine Rotation Specific Evaluation Orthopaedic Surgery Training Program School of Medicine, Queen s University CanMEDS Roles / Competencies Name: PGY Rotation Dates: s s Exceeds N/A Attending Staff:
Adult Spine Rotation Specific Evaluation Orthopaedic Surgery Training Program School of Medicine, Queen s University CanMEDS Roles / Competencies Name: PGY Rotation Dates: s s Exceeds N/A Attending Staff:
HOW TO CITE THIS ARTICLE:
 POST TRAUMATIC INSTABILITY OF SUB-AXIAL CERVICAL SPINE - REDUCTION AND INTERNAL FIXATION BY LATERAL MASS SCREWS A LONG TERM FOLLOW-UP STUDY Godagu Bhaskar 1, Ambarapu Mastan Reddy 2, Akyam Lakshman Rao
POST TRAUMATIC INSTABILITY OF SUB-AXIAL CERVICAL SPINE - REDUCTION AND INTERNAL FIXATION BY LATERAL MASS SCREWS A LONG TERM FOLLOW-UP STUDY Godagu Bhaskar 1, Ambarapu Mastan Reddy 2, Akyam Lakshman Rao