Neonatal Drug Withdrawal. John Wareham, MD Department of Neonatology, St. Vincent Women s Hospital
|
|
|
- Felicia James
- 8 years ago
- Views:
Transcription
1 Neonatal Drug Withdrawal John Wareham, MD Department of Neonatology, St. Vincent Women s Hospital

2 Neonatal Drug Withdrawal What are we going to cover? Overview of the problem in neonates Opioid exposure/dependence (Newborn Abstinence Syndrome) Review a few other drugs THC, cocaine and other stimulants, Selective Serotonin Uptake Inhibitors (SSRIs) Current methods for drug screening newborns Long term outcome Selected topics
 Current methods for drug screening newborns")
3

4 2009 National Survey on Drug Use and Health Surveyed population 12 years or older. 8.7%, 23.7%, and 27.7%, respectively, reported recent use of illicit drugs, binge or heavy alcohol ingestion and use of tobacco products. 4.5% of pregnant women years of age reported recent use of illicit drugs (marijuana, cocaine, hallucinogens, heroin, methamphetamines, and nonmedical use of prescription drugs). Binge or heavy drinking in the first trimester was reported by 11.9% and recent tobacco use by 15.3%. In the year old range, the use of illicit drugs and smoking were higher in pregnant women than in those not pregnant.
. Binge or heavy drinking in the first trimester was reported by 11.9% and recent tobacco use by 15.3%.")
5 Discharge Data from Agency for Health Care Research and the Florida Department of Health Using ICD 9 code for neonatal withdrawal syndrome the number of infants coded at discharge increased from 7653 in 1995 to 11, 937 in In Florida, the number of newborns discharged with ICD 9 code increased from 0.4 to 4.4/1000 live births from 1995 to Part of this increase, though exactly how much is not known, is thought to be from the more liberal use of prescription opiates in pregnant women to help with pain from a number of etiologies.

6 St. Vincent Women s NICU Number 10 (8 outborn) Gestation al Age 37.4 weeks Birth weight Length of Stay kg 34.1 days Admitting diagnosis of Drug Withdrawal

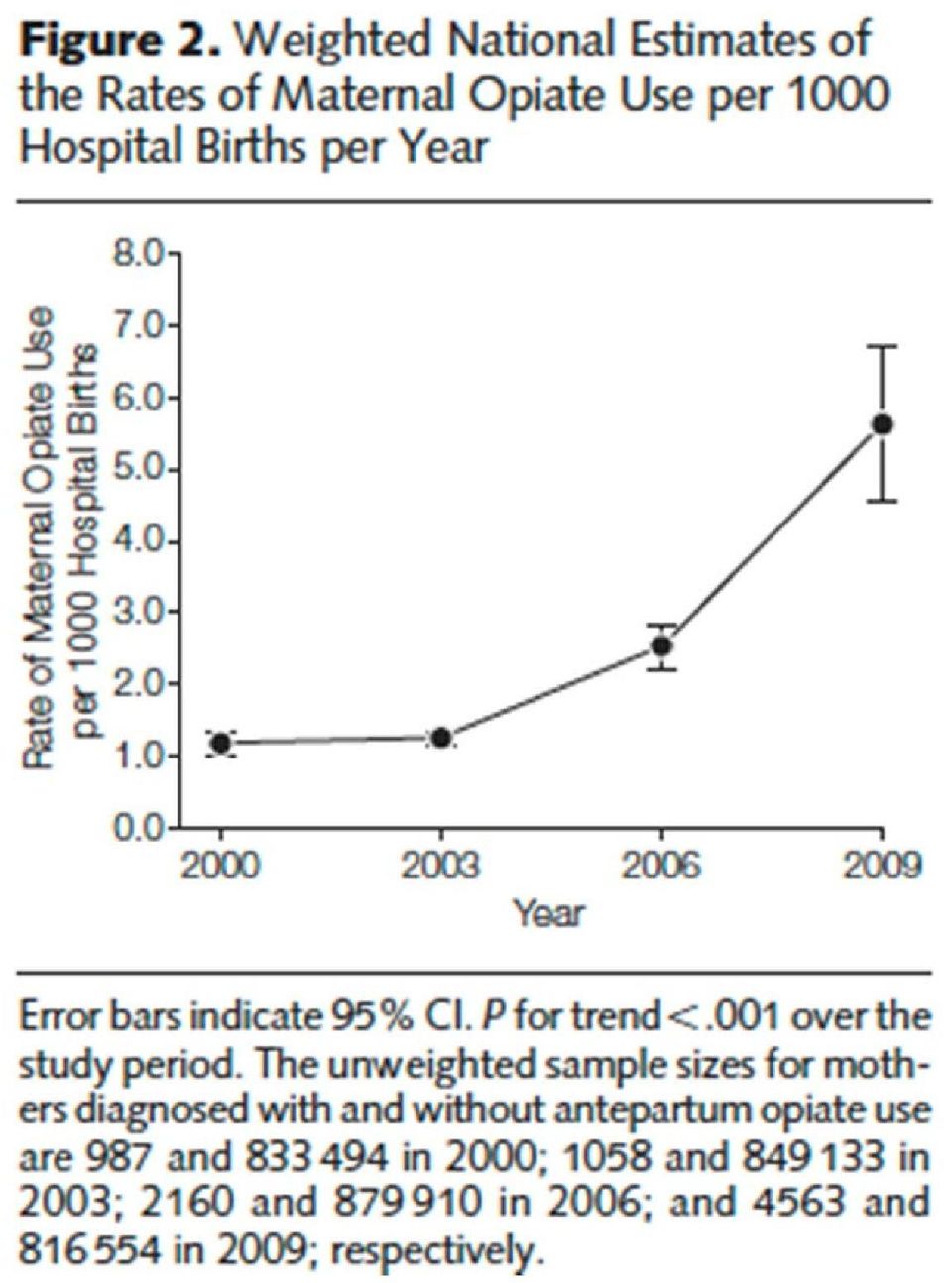
7 Neonatal Abstinence Syndrome and Associated Health Care Expenditures JAMA, May 9, 2012;307(18); This article was a retrospective cross sectional analysis of national samples using several large databases. Authors were from the University of Michigan. Infants with NAS were identified from a cross sectional analysis of pediatric discharges in 2000, 2003, 2006, and 2009 using the Healthcare Cost and Utilization Project s Kids Inpatient Database (KID). The database samples 80% of pediatric discharges and 10% of uncomplicated births. Using the KID, NAS patients were identified using the ICD 9 CM code of (drug withdrawal syndrome in a newborn). Using another database, the Nationwide Inpatient Sample (NIS), delivering mothers were identified by common delivery diagnosis related groups.
. The database samples 80% of pediatric discharges and 10% of uncomplicated births. Using the KID, NAS patients were identified using the ICD 9 CM code of 779.")
8 Neonatal Abstinence Syndrome and Associated Health Care Expenditures JAMA, May 9, 2012;307(18); Iatrogenic NAS was looked for by searching NICU discharge data for the diagnoses of very low birth weight, PVL, IVH, NEC, spontaneous bowel perforation, or BPD. Data would probably have been more accurate if search included pulmonary hypertension, ECMO, and congenital heart disease.

9

10
11

12

13 Conclusions Between 2000 and 2009 total hospital charges for NAS were estimated to have increased from 190 to 720 million dollars (includes inflation). The CDC found that the sales and deaths related to opiate pain relievers quadrupled between 1999 and The majority of costs related to NAS are shouldered by Medicaid. We are no better at getting infants with NAS home than we were in 2000.

14
15

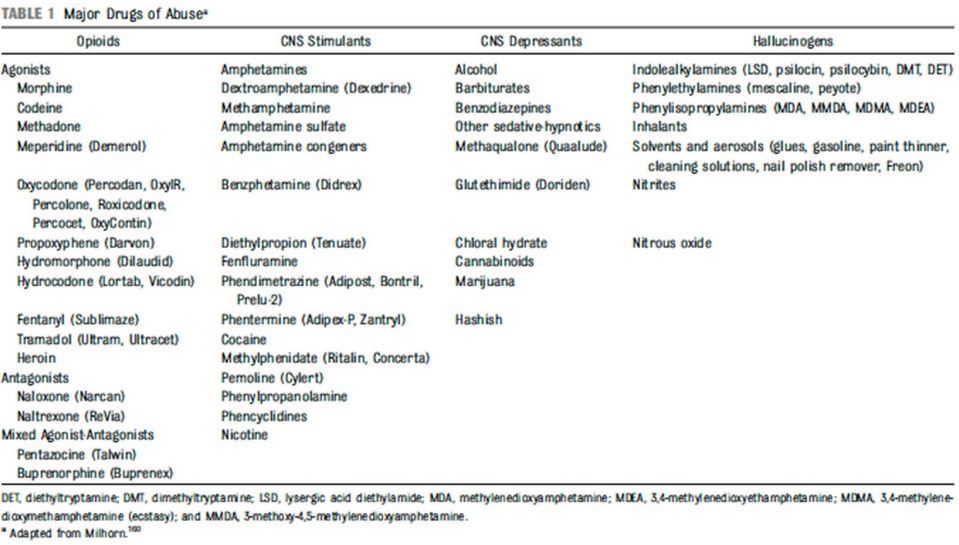
16 Neonatal Drug Withdrawal This is a nationwide problem. In Indiana, this is a problem in every county. The classic drugs of abuse that cause neonatal withdrawal are opioids such as heroin and morphine. Prescription pain medications such as oxycodone (Percocet), hydromorphone (Dilaudid), and propoxyphene (Darvon) are currently a hot issue. Stimulant drugs, such as cocaine and amphetamine, cause symptoms/signs and probably harm in neonates. Marijuana, the most common illicit drug detected on drug screens, still is a source of debate concerning withdrawal. Selective serotonin reuptake inhibitors (SSRIs) have become a problem because of their frequent prescription to pregnant women with depression and the emergence of a neonatal withdrawal syndrome. Also, complicating the use of SSRI s is their frequent prescription to mothers for postpartum depression. It is not clear that these drugs are safe for breast feeding.

17 Neonatal Drug Withdrawal When talking about neonatal drug withdrawal, most people are referring to neonatal withdrawal from opiates, which is called the neonatal abstinence syndrome (NAS). The actual incidence of NAS is not known, but has probably increased. While there is a fair amount of information on the short term effects of drug exposure, the long term effects of fetal drug exposure (other than to drugs associated with teratogenicity and birth defects), in most instances, are unknown. Alcohol may be the exception. The optimal treatment for fetal drug exposure that results in withdrawal is not known. As an additional problem in NICU s, the use of narcotics and/or benzodiazepines to provide analgesia or sedation for hospitalized infants puts that population at risk for drug dependency and withdrawal. Is there a difference between a neonate withdrawing after a fetal exposure and a neonate withdrawing after a neonatal exposure?
, in most instances, are unknown. Alcohol may be the exception. The optimal treatment for fetal drug exposure that results in withdrawal is not known.")
18 Neonatal Drug Withdrawal Withdrawal or toxicity? Maternal use of certain drugs can cause transient neonatal signs consistent with withdrawal or acute toxicity or sustained signs consistent with a lasting drug effect. Opioid exposure of the fetus often causes withdrawal, cocaine exposure probably causes toxicity/drug effects, but not a true withdrawal. Signs and symptoms of withdrawal worsen as the drug level decreases, the signs and symptoms of acute toxicity improve as the drug level decreases.

19 Mechanisms of Drug Injury in the Fetus Early in gestation, during the embryonic stage, drugs can have teratogenic effects. During the fetal period, after the major structural development has been completed, drug effects are more subtle. These effects include abnormal growth and/or maturation, alterations in neurotransmitters and their receptors, and brain organization. Drugs of abuse mimic naturally occurring neurotransmitters marijuana acts as anandamides, opiates as endorphins, cocaine and stimulants act within the mesolimbic dopaminergic pathways to increase dopamine and serotonin within the synapses.

20 Mechanisms of Drug Injury Important indirect effects of drugs of abuse on the fetus are altered maternal health behaviors attributable to the mother s addiction. These altered behaviors include poor nutrition, decreased access to and compliance with health care, increased exposure to violence, and increased risk of mental illness and infection. Of all the mechanisms of injury, perhaps the most concerning is the chronic exposure of the developing nervous system to drugs that mimic the activity of neurotransmitters and their receptors. During fetal development neurotransmitters are very important in guiding the development of the brain.

21 Neonatal Drug Withdrawal Opiates By far, the most common neonatal drug withdrawal comes from intrauterine opioid exposure. The typical clinical findings associated with opioid withdrawal are called the Neonatal Abstinence Syndrome (NAS). Withdrawal signs develop in 55 94% of neonates exposed to opioids in utero. Neonatal withdrawal signs have also been described in infants exposed to benzodiazepines, barbiturates, SSRI s and alcohol.
22
23 Opioids Opioids are a class of natural, endogenous, and synthetic compounds that activate primarily mu opioid receptors in the CNS to produce supraspinal analgesia. Morphine is a natural opioid and is extracted from the opium poppy. Codeine, heroin, hydromorphone, fentanyl, and methadone are all synthetic opioids. Opioids acutely inhibit the release of noradrenaline at the synaptic terminals. With chronic opioid exposure, tolerance develops and the rate of noradrenaline release increases toward normal. Abrupt cessation of exogenous opioids results in a supranormal release of noradrenaline and produces the autonomic and behavioral signs characteristic of opioid withdrawal.
24 Opioid Abuse in Pregnancy Opioids are small lipophilic compounds that freely cross the placenta and blood brain barrier. Maternal detoxification may be associated with increased risk of fetal distress and fetal loss. Maintenance programs with methadone for pregnant women sustain opioid concentrations in the mother and fetus in ranges that minimize opioid craving, suppress abstinence symptomatology, block heroin induced euphoria, and prevent fetal stress. Unfortunately, because of its addictive properties, the use of methadone makes detoxification after delivery unlikely and produces a longer course of NAS than with heroin exposure.
25 Opioid Withdrawal Since the opioid receptors are concentrated in the CNS and GI tract, you get the signs and symptoms seen in the previous chart. Excess environmental stimuli and hunger exacerbate the perceived severity of NAS. Hence, frequent feeds and a quiet room are part of the treatment of withdrawal. Signs of neonatal withdrawal often begin in the first 24 hours after birth with heroin. In methadone, the withdrawal tends to begin between 24 and 72 hours. However, for both opioids, withdrawal has been reported to take up to 5 7 days to develop.
26 Opioid Withdrawal For buprenorphine, withdrawal onset peaks at 40 hours, is at its worst at 70 hours. The different time courses reflect variations in the half lives of drug elimination. The incidence and severity of NAS are greater in infants exposed to methadone compared with infants exposed to heroin or buprenorphine. However, up to 50% of infants exposed to buprenorphine may withdraw. Daily maternal methadone dose has not been consistently correlated with the incidence or severity of NAS. Maternal methadone metabolism is probably a more important determinant than the actual daily dose.
27 Preterm Opioid Withdrawal Preterm infants do not withdraw as frequently or as severely. It is not known whether that is due to the less mature nervous system or being exposed to a lower total dose of narcotic or both. Preterm infants also have less body fat and opiates are lipophilic.
28 Deciding When to Treat the Newborn with NAS Once a newborn becomes symptomatic, you must decide how to manage the withdrawal. First line of treatment is nonpharmacologic using frequent feedings, a quiet environment, comforting techniques, etc. If the nonpharmacologic approach is not successful, then medication may be required. In deciding when to move to medication, a withdrawal scoring system is helpful. There are two frequently used, the Lipsitz tool and Finnegan s Neonatal Abstinence Scoring Tool. The Finnegan Tool (not modified!!) is probably the most utilized.
29 Neonatal Abstinence Scoring Tool
30 Pharmacologic Therapy of NAS The optimal screening scores for the initiation of pharmacologic therapy by any published abstinence scoring system are unknown. If nonpharmacologic treatment fails, then the drugs of choice are oral morphine or methadone (94% first choice in UK, 83% first choice in US). Paregoric is no longer used because it contains multiple other opioids as well as camphor, anise oil, alcohol, and benzoic acid. Tincture of opium contains a 25 fold higher concentration of morphine than currently available oral morphine preparations making accidental overdose a concern. When a second drug is needed, phenobarbital is commonly picked. However, clonidine may be taking it s place.
31 Clonidine Clonidine is an alpha 2 adrenergic receptor agonist that is being used with an opioid or other drug to reduce withdrawal symptoms. It s more common uses are in hypertension, ADHD, anxiety disorders and certain pain conditions. Clonidine reduces CNS sympathetic outflow and moderates symptoms of autonomic over activity such as tachycardia, hypertension, sweating, restlessness and diarrhea. Cessation of clonidine treatment can result in a rebound of autonomic activity, so it must be weaned. NICU s are starting to use it in infants with more severe symptoms or those difficult to wean off methadone or morphine.
32 Other Drugs Marijuana Cocaine and other stimulants SSRIs Aquired drug dependency (in the NICU and PICU) Alcohol and cigarette smoke
33 Marijuana Marijuana is the most common drug of abuse found in newborn drug tests in our practice. The main chemical compound in marijuana, 9 tetrahydrocannabinol (THC), crosses the placenta. The major metabolite, 11 nor 9 carboxy THC does not. In animal species, it appears that the placenta limits the passage of THC with fetal concentrations being below the maternal concentrations. There is still debate about the existence of a withdrawal syndrome. Long term, studies have suggested that there may be effects on attention and impulsivity in children exposed to marijuana during pregnancy. There is also the suggestion that prenatal marijuana exposure decreases academic achievement, especially in the areas of reading and spelling.
34 Cocaine and Other Stimulants Both cocaine and methamphetamine increase the risk of preterm birth, placental abruption, fetal distress, and IUGR in pregnant women. A true abstinence syndrome after exposure to CNS stimulants such as cocaine and amphetamine has not been defined. The neurobehavioral abnormalities that occur frequently 2 3 days after birth in neonates with intrauterine exposure include irritability, hyperactivity, tremors, high pitched cry, and excessive sucking. Since cocaine and its metabolites may be detected in exposed infants for up to 7 days after birth, the signs may relate more to drug effect than withdrawal.
35 Selective Serotonin Reuptake Inhibitors (SSRIs) This class of antidepressant medications became available for widespread use in They are now the most frequently used drugs to treat depression. Included are such well known names as Prozac (fluoxetine), Zoloft (sertraline), Lexaprol (escitalopram), and Paxil (paroxetine). SSRIs block the reuptake of serotonin into the presynaptic neuron thereby increasing the concentration of serotonin in the presynaptic cleft available to bind to serotonin receptors on the postsynaptic neuron.
36 SSRIs Third trimester use of SSRIs can produce neonatal signs that include continuous crying, irritability, jitteriness, shivering, fever, tremors, hypertonia, tachypnea, feeding difficulty, sleep disturbance, hypoglycemia, and seizures. The onset of signs varies from several hours to several days after birth. Signs typically resolve within 1 2 weeks. Again, it is unknown whether this is a withdrawal syndrome or serotonin syndrome (serotonin overload). Clinical course is frequently one of a slow resolution of signs, which may be more consistent with a hyperserotonergic condition rather than withdrawal. Only paroxetine (Paxil) produces a ratio of infant to maternal plasma concentration that is consistently low (<0.1) with breast feeding.
37 Aquired Opioid and/or Benzodiazepine Dependency This refers to drug dependency generated in sick neonates from the use of opioids and benzodiazepines. ECMO patients are heavily represented in this patient population. Most of the data comes from Peds ICUs, not NICUs. Drug infusions, such as with fentanyl and midazolam, are especially good at generating dependency. Withdrawal signs and symptoms from the two drugs overlap, making it hard to separate the two in weaning. This issue leads to significant prolongation of hospital courses.
38 Aquired Opioid and/or Benzodiazepine Dependency For those infants who receive prolonged cumulative exposure to these two classes of drugs, the AAP offers some guidelines. Each clinical unit needs to establish its own dose levels above which withdrawal is likely. As a rule for fentanyl infusions, a cumulative fentanyl exposure of >2 mg/kg or >7 days duration predicts a likelihood of dependency of over 50%, but less than 100%. These infants should go into a weaning schedule over weeks. Infants who do not reach the cumulative exposure to either opioids or benzodiazepines can be weaned rapidly. In such cases, many of the infants will not withdraw (BUT, some will). If withdrawal occurs after a rapid wean, it is usually within 24 hours of the last dose.
39 Aquired Opioid and/or Benzodiazepine Dependency As previously mentioned, withdrawal from benzodiazepines overlaps the signs and symptoms of NAS. Once weaning has been established, iv benzodiazepines can be converted to oral lorazepam. The weaning duration will be proportional to the length of treatment with the iv benzodiazepine.
40 Alcohol and Cigarette Smoke These are legal drugs that are frequently used in pregnancy. Maternal smoking exposes the fetus to more than 4000 compounds. Of these, about 30 have been associated with adverse health outcomes. The best known is nicotine. Nicotine concentrations are higher in the placenta, amniotic fluid and fetus than in the maternal serum. Exact mechanisms by which nicotine causes harm to the fetus are unknown, but likely includes hypoxia, undernourishment of the fetus and direct vasoconstrictor effects on the placental and umbilical vessels. Nicotine has also been shown to have direct negative effects on brain development.
41 Alcohol and Cigarette Smoke Ethanol readily crosses the placenta with significant concentrations identified in amniotic fluid and maternal and fetal blood. Possible mechanisms of injury include direct teratogenic effects during the embryonic and fetal stages of development, toxic effects on the placenta, altered prostaglandin and protein synthesis, hormonal alterations, nutritional effects, altered neurotransmitter levels in the brain, altered brain morphology and neuronal development, and hypoxia.
42 Lab Screening Urine testing of the mother and infant has the advantage of short turn around time, but a brief window of time screened. Meconium screening of the newborn has the advantage of a much longer screening window, but the testing is messy and requires 1 2 weeks for results. The infant has often been discharged prior to the results. Testing of umbilical cord samples is relatively new and comparable to meconium testing in accuracy. Results can be available in 2 3 days.
43
44 Long Term Outcome The long term neurodevelopmental outcome of infants who withdraw is really not known. It is very difficult to tease out the drug effects from the family/social issues. The available data tends to be reassuring, at least as far as marked impairment in intelligence. Whether it is looking at infants who seize secondary to opioid withdrawal or drug toxicity from cocaine, most of the infants appear to do OK cognitively. With opiates and other drugs, long term problems in the neurobehavioral and learning areas may be the most common. The fact that infants exposed to opiates, cocaine, etc. are not routinely devastated as older children doesn t mean they achieve to the degree they would have without a drug exposure. In this area the data is pretty sparse.
45
46
47 Methadone Dosing and the NAS Studies comparing maternal methadone dose and the risk of withdrawal have been contradictory. For every study showing a link, another study shows there is not. There are a number of reasons for this lack of correlation: Variation in study design studies where the mothers received higher doses tended to find no relationship, studies finding a relationship tended to use lower doses. Variability in maternal methadone metabolism even using a similar daily dose, fetuses will see different total doses of methadone based on their mothers ability to metabolize the drug.
48 Methadone Dosing and the NAS There are better ways to predict the chance of withdrawal in neonates born to mothers on methadone, but they are not as easily obtained as the total daily dose of methadone. Cord and serum methadone value at 48 hours of age as well as the rate of decline are better predictors. The lower the cord value of methadone and the more rapid the decline in serum value, the more severe withdrawal is likely to be.
49 Buprenorphine Because of the negative aspects of methadone use synthetic opioids have been developed as alternatives. Buprenorphine, a partial mu receptor agonist, was approved in 2002 by the FDA for the treatment of opioid dependence. Buprenorphine alone (Subutex) or in combination with naloxone (Suboxone) has been used as a first line treatment of heroin addiction and as a replacement drug for methadone. Neither methadone nor buprenorphine is approved by the FDA for use in pregnancy. There is some data that buprenorphine may produce less withdrawal in neonates and that the withdrawal, when it occurs, is shorter. However, the data is not extensive. Unfortunately, pregnant women on methadone tend to comply with their narcotic management more consistently than with buprenorphine. Conversion from methadone to buprenorphine during pregnancy requires hospitalization for it to be done safely (for the mother and fetus).
50 Management of NAS at the Community Hospital Referral of withdrawing newborns to a tertiary care hospital/nicu has advantages and disadvantages. The major advantages are care in a setting where infants with drug withdrawal are fairly frequent and resources for care are extensive. There are significant negatives however: The geographic distance between the parents home and the tertiary care hospital can be a significant roadblock to parental visitation. Families with a drug issue often have significant financial and transportation constraints. The infant is removed from the county where he/she will reside. That means the CPS office that may already be familiar with the family is working from afar.
51 Length of Hospitalization for Observation after Birth The length of observation in the hospital is dependent on the mother s history and the type and amount of drug being taken. Heroin withdrawal usually begins in the first 24 hours after birth, methadone withdrawal usually starts between 24 and 72 hours of age. However, both drugs have resulted in delayed withdrawal at 5 7 days of age. The peak onset of withdrawal in fetuses exposed to buprenorphine is ~40 hours. The AAP recommends that infants born to mothers who used a shorter acting opiate, such as hydrocodone, be observed for 3 days. Infants born to mothers using a long acting opiate such as methadone should be observed for 5 7 days.
52 Breast Feeding Breastfeeding has been associated with less severe NAS presents later and less often requires drug intervention. Breast feeding, safety wise, requires that the mother be in a supervised drug treatment program and that the mother be HIV negative. Generally, that means a methadone program. Methadone is excreted into breast milk, but at a low level. Dose range has been estimated at from 0.01 to 0.15 mg/day in the first 30 days of life. Maternal use of street drugs is a contraindication to breast feeding, with the possible exception of marijuana.
53 Breastfeeding Oral narcotic pain relievers, for the most part, should not be used in lactating mothers. Butorphanol, morphine, and hydromorphone are relatively safe, but still should be used in the lowest possible doses. In the case of SSRI s, all but Paxil (paroxetine) have case reports showing significant intake by breast feeding. The long term effects of this class of drugs is unknown, but serotonin is an important neurotransmitter and it s levels are manipulated in the CNS of developing infants by exposure to SSRI s.
54 Summary Every nursery should develop a protocol that defines indications and procedures for screening for maternal substance abuse. Additionally, a standardized plan should be in place for evaluating and treating infants at risk for or showing signs of withdrawal or drug effect. Infants with known intrauterine exposure to opioids and benzodiazepines should be observed in the hospital for 4 7 days. Outpatient follow up should be early. Breastfeeding, if safely possible, may help reduce the risk of withdrawal. However, the mothers must be closely supervised and HIV negative.
55 Summary There are not nearly enough drug dependency and pain management programs/professionals available to treat the need. Methadone treatment programs have not emphasized weaning off of opioids and have been uneasy with pregnancy. There is a paucity of data on best treatment and long term outcome.
56 Based on national data comparing 50 states and the District of Columbia, Indiana ranks 28th in preterm births* (12.4%) * less than 37 completed weeks gestation 29th in low birth weight* (8.3%) * less than 2,500 grams 18th in deliveries via cesarean section (30%) 39th on 1st trimester entry into prenatal care (63.3%) 39th in infant mortality (7.8) 36th in percent of babies who are ever breastfed (70.5%) Indiana received a grade of C on the March of Dimes 2011 Premature Birth Report Cards
57 References Sachs HC and the Committee on Drugs. The Transfer of Drugs and Therapeutics Into Human Breast Milk: An Update on Selected Topics. Pediatrics. 2013; 132(3): e Behnke M, Smith VC, the Committee on Substance Abuse and the Committee on the Fetus and Newborn. Prenatal Substance Abuse: Short and Long term Effects on the Exposed Fetus. Pediatrics. 2013; 131(3): e1009 e1024 Hudak ML, Tan RC, the Committee on Drugs and the Committee on the Fetus and the Newborn. Neonatal Drug Withdrawal. Pediatrics. 2012;129(2): e540 e560 Patrick SW, Schumacher RE, Benneyworth BD, Krans EE, McAllister JM and Davis MM. Neonatal Abstinence Syndrome and Associated Health Care Expenditures, United States JAMA. 2012; 307(18):
NEONATAL ABSTINENCE SYNDROME. Osama Naga, M.D. PGY2
 NEONATAL ABSTINENCE SYNDROME Osama Naga, M.D. PGY2 Objective: Describe the common causes of NAS Clinical Presentation Diagnosis Identify the different scoring system for pharmacologic therapy Minimize
NEONATAL ABSTINENCE SYNDROME Osama Naga, M.D. PGY2 Objective: Describe the common causes of NAS Clinical Presentation Diagnosis Identify the different scoring system for pharmacologic therapy Minimize
NEONATAL ABSTINENCE SYNDROME AND SCORING SYSTEM
 VIDANT MEDICAL CENTER PATIENT CARE _ SUBJECT: Abstinence Scoring NUMBER: A-1 PAGE: 1 OF: 5 _ NEONATAL ABSTINENCE SYNDROME AND SCORING SYSTEM POLICY: A thorough evaluation of the infant is required in order
VIDANT MEDICAL CENTER PATIENT CARE _ SUBJECT: Abstinence Scoring NUMBER: A-1 PAGE: 1 OF: 5 _ NEONATAL ABSTINENCE SYNDROME AND SCORING SYSTEM POLICY: A thorough evaluation of the infant is required in order
Identifying Neonatal Abstinence Syndrome (NAS) and Treatment Guidelines University of Iowa Children s Hospital -2/11/13
 and Treatment Guidelines University of Iowa Children s Hospital -2/11/13") Identifying Neonatal Abstinence Syndrome (NAS) and Treatment Guidelines University of Iowa Children s Hospital -// What is Neonatal Abstinence Syndrome? Neonatal withdrawal after intrauterine exposure
Identifying Neonatal Abstinence Syndrome (NAS) and Treatment Guidelines University of Iowa Children s Hospital -// What is Neonatal Abstinence Syndrome? Neonatal withdrawal after intrauterine exposure
Medication Assisted Treatment
 Medication Assisted Treatment Tanya Hiser, MS, LPC State Opioid Treatment Authority Bureau Of Prevention, Treatment, & Recovery State of Wisconsin Elizabeth Collier, MSW, CSAC, ICS, LCSW TANF Best Practice
Medication Assisted Treatment Tanya Hiser, MS, LPC State Opioid Treatment Authority Bureau Of Prevention, Treatment, & Recovery State of Wisconsin Elizabeth Collier, MSW, CSAC, ICS, LCSW TANF Best Practice
Current Trends In Identifying And Treating Newborns With Withdrawal Syndromes 6/24/2010
 Current Trends In Identifying And Treating Newborns With Withdrawal Syndromes 6/24/2010 Substance Exposed Newborns Alcohol Tobacco Caffeine Amphetamines Cocaine Barbituates Selective Serotonin Re-uptake
Current Trends In Identifying And Treating Newborns With Withdrawal Syndromes 6/24/2010 Substance Exposed Newborns Alcohol Tobacco Caffeine Amphetamines Cocaine Barbituates Selective Serotonin Re-uptake
Management of Neonatal Abstinence Syndrome and Iatrogenic Drug Withdrawal
 Management of Neonatal Abstinence Syndrome and Iatrogenic Drug Withdrawal Kirsten H. Ohler, Pharm.D., BCPS Clinical Assistant Professor Neonatal / Pediatric Clinical Pharmacist University of Illinois at
Management of Neonatal Abstinence Syndrome and Iatrogenic Drug Withdrawal Kirsten H. Ohler, Pharm.D., BCPS Clinical Assistant Professor Neonatal / Pediatric Clinical Pharmacist University of Illinois at
Introduction to Neonatal Abstinence Syndrome
 Introduction to Neonatal Abstinence Syndrome Cara Christ, MD Director, Arizona Department of Health Services Learning Objectives 1.Define Neonatal Abstinence Syndrome 2.Describe Neonatal Abstinence Syndrome
Introduction to Neonatal Abstinence Syndrome Cara Christ, MD Director, Arizona Department of Health Services Learning Objectives 1.Define Neonatal Abstinence Syndrome 2.Describe Neonatal Abstinence Syndrome
Substance Abuse During Pregnancy: Moms on Meds. Jennifer Anderson Maddron, M.D LeConte Womens Healthcare Associates
 Substance Abuse During Pregnancy: Moms on Meds Jennifer Anderson Maddron, M.D LeConte Womens Healthcare Associates 2010 National Survey on Drug Use and Health An estimated 4.4% of pregnant women reported
Substance Abuse During Pregnancy: Moms on Meds Jennifer Anderson Maddron, M.D LeConte Womens Healthcare Associates 2010 National Survey on Drug Use and Health An estimated 4.4% of pregnant women reported
What is Methadone? Opioid Treatment Programs Today. Is Methadone Safe? Pain Clinics. Wisconsin OTPs. Methadone Maintenance Treatment 5/6/2013
 Methadone Maintenance Treatment Tanya Hiser, MS, LPC State Opioid Treatment Authority April 22, 2013 What is Methadone? Schedule II pharmaceutical opioid similar to Oxycodone or morphine. Binds to the
Methadone Maintenance Treatment Tanya Hiser, MS, LPC State Opioid Treatment Authority April 22, 2013 What is Methadone? Schedule II pharmaceutical opioid similar to Oxycodone or morphine. Binds to the
Opioid/Opiate Dependent Pregnant Women
 Opioid/Opiate Dependent Pregnant Women The epidemic, safety, stigma, and how to help. Presented by Lisa Ramirez MA,LCDC & Kerby Stewart MD The prescription painkiller epidemic is killing more women than
Opioid/Opiate Dependent Pregnant Women The epidemic, safety, stigma, and how to help. Presented by Lisa Ramirez MA,LCDC & Kerby Stewart MD The prescription painkiller epidemic is killing more women than
Substance Abuse lifestyle Concern for mother - fetus - and - neonate
 OBJECTIVES Learn about types of opioids and associated withdrawal symptoms Learn what medications are available to treat opioid addiction Understand the pros and cons associated with each medication Understand
OBJECTIVES Learn about types of opioids and associated withdrawal symptoms Learn what medications are available to treat opioid addiction Understand the pros and cons associated with each medication Understand
Magee-Womens Hospital
 Magee-Womens Hospital Magee Pregnancy Recovery Program: History Pregnancy Recovery Center A Medical Home Model Approach to Strengthen Families Bawn Maguire, MSN, RN Programmatic Nurse Specialist Stephanie
Magee-Womens Hospital Magee Pregnancy Recovery Program: History Pregnancy Recovery Center A Medical Home Model Approach to Strengthen Families Bawn Maguire, MSN, RN Programmatic Nurse Specialist Stephanie
CHILDREN S SERVICES. Neonatal Abstinence Syndrome
 CHILDREN S SERVICES Neonatal Abstinence Syndrome Background Neonatal Abstinence Syndrome (NAS) is a combination of behavioural and physiological signs and symptoms that occur in newborns going through
CHILDREN S SERVICES Neonatal Abstinence Syndrome Background Neonatal Abstinence Syndrome (NAS) is a combination of behavioural and physiological signs and symptoms that occur in newborns going through
3/31/2015. Objectives. Alcohol. Long term effects. Substance abuse increases the risk of: Substance Abuse in Pregnancy
 Objectives Substance Abuse in Pregnancy Basics of screening and counseling Minako Watabe, MD Obstetrics and Gynecology Ventura County Medical Center 1) Discuss the risks of alcohol, tobacco, and drug use
Objectives Substance Abuse in Pregnancy Basics of screening and counseling Minako Watabe, MD Obstetrics and Gynecology Ventura County Medical Center 1) Discuss the risks of alcohol, tobacco, and drug use
Heroin. How is Heroin Abused? What Other Adverse Effects Does Heroin Have on Health? How Does Heroin Affect the Brain?
 Heroin Heroin is a synthetic opiate drug that is highly addictive. It is made from morphine, a naturally occurring substance extracted from the seed pod of the Asian opium poppy plant. Heroin usually appears
Heroin Heroin is a synthetic opiate drug that is highly addictive. It is made from morphine, a naturally occurring substance extracted from the seed pod of the Asian opium poppy plant. Heroin usually appears
Management of Pregnancy. Opioid Addiction Treatment
 Management of Pregnancy Opioid Addiction Treatment Perinatal Opioid Addiction Pharmacotherapy and co-ordination of care are essential elements in the comprehensive care of pregnant patients with opioid
Management of Pregnancy Opioid Addiction Treatment Perinatal Opioid Addiction Pharmacotherapy and co-ordination of care are essential elements in the comprehensive care of pregnant patients with opioid
(peak at 2 days 6 wks)
") Perinatal Manual of Southwestern Ontario A collaboration between the Regional Perinatal Outreach Program of Southwestern Ontario & the Southwestern Ontario Perinatal Partnership (SWOPP) Chapter 46 NEONATAL
Perinatal Manual of Southwestern Ontario A collaboration between the Regional Perinatal Outreach Program of Southwestern Ontario & the Southwestern Ontario Perinatal Partnership (SWOPP) Chapter 46 NEONATAL
Neonatal Abstinence Syndrome: Indian Health Service (IHS) Best Practices Guidelines
 Best Practices Guidelines") Neonatal Abstinence Syndrome: Indian Health Service (IHS) Best Practices Guidelines 1. Neonatal Drug Withdrawal Intrauterine exposure to certain drugs and medications can cause clinical symptoms in the
Neonatal Abstinence Syndrome: Indian Health Service (IHS) Best Practices Guidelines 1. Neonatal Drug Withdrawal Intrauterine exposure to certain drugs and medications can cause clinical symptoms in the
Identifying and Managing Substance Use During Pregnancy
 Identifying and Managing Substance Use During Pregnancy Joseph B. Landwehr, Jr., MD Director, Perinatal Center IU Health Ball Memorial Hospital OBJECTIVES Overview of illicit drug use in pregnant women
Identifying and Managing Substance Use During Pregnancy Joseph B. Landwehr, Jr., MD Director, Perinatal Center IU Health Ball Memorial Hospital OBJECTIVES Overview of illicit drug use in pregnant women
Welcome. How Do I Ask Questions? Agenda. Thank you for joining us today. The webinar will begin in a few moments.
 Welcome How Do I Ask Questions? Thank you for joining us today. The webinar will begin in a few moments. If you are experiencing technical problems with the GoToWebinar program, contact the GoToWebinar
Welcome How Do I Ask Questions? Thank you for joining us today. The webinar will begin in a few moments. If you are experiencing technical problems with the GoToWebinar program, contact the GoToWebinar
Presentation to Senate Health and Human Services Committee: Prescription Drug Abuse in Texas
 Presentation to Senate Health and Human Services Committee: Prescription Drug Abuse in Texas David Lakey, MD Commissioner, Department of State Health Services Lauren Lacefield Lewis Assistant Commissioner,
Presentation to Senate Health and Human Services Committee: Prescription Drug Abuse in Texas David Lakey, MD Commissioner, Department of State Health Services Lauren Lacefield Lewis Assistant Commissioner,
Heroin. How Is Heroin Abused? How Does Heroin Affect the Brain? What Other Adverse Effects Does Heroin Have on Health?
 Heroin Heroin is an opiate drug that is synthesized from morphine, a naturally occurring substance extracted from the seed pod of the Asian opium poppy plant. Heroin usually appears as a white or brown
Heroin Heroin is an opiate drug that is synthesized from morphine, a naturally occurring substance extracted from the seed pod of the Asian opium poppy plant. Heroin usually appears as a white or brown
Downers/Depressants (pages 40-50)
") Downers/Depressants (pages 40-50) Read pages 49-54, 59-60, and 78-79 of the booklet, Street Drugs. Pages 40-50 of the text. Narcotics: Prescription Origin: Southeast Asia, Southwest Asia, and in the Western
Downers/Depressants (pages 40-50) Read pages 49-54, 59-60, and 78-79 of the booklet, Street Drugs. Pages 40-50 of the text. Narcotics: Prescription Origin: Southeast Asia, Southwest Asia, and in the Western
Children s Specialized Hospital Neonatal Abstinence Syndrome (NAS)
") Children s Specialized Hospital Neonatal Abstinence Syndrome (NAS) A Pharmacologic and Rehabilitation Program that Promotes Narcotic Weaning and Autonomic Regulation Necessary for Infant Development Sharon
Children s Specialized Hospital Neonatal Abstinence Syndrome (NAS) A Pharmacologic and Rehabilitation Program that Promotes Narcotic Weaning and Autonomic Regulation Necessary for Infant Development Sharon
Methadone and Pregnancy
 Methadone and Pregnancy Methadone 101/Hospitalist Workshop Launette Rieb, MD, MSc, CCFP, CCSAM, FCFP Clinical Associate Professor, Dept. Family Practice, UBC American Board of Addiction Medicine Certified
Methadone and Pregnancy Methadone 101/Hospitalist Workshop Launette Rieb, MD, MSc, CCFP, CCSAM, FCFP Clinical Associate Professor, Dept. Family Practice, UBC American Board of Addiction Medicine Certified
Considerations in Medication Assisted Treatment of Opiate Dependence. Stephen A. Wyatt, D.O. Dept. of Psychiatry Middlesex Hospital Middletown, CT
 Considerations in Medication Assisted Treatment of Opiate Dependence Stephen A. Wyatt, D.O. Dept. of Psychiatry Middlesex Hospital Middletown, CT Disclosures Speaker Panels- None Grant recipient - SAMHSA
Considerations in Medication Assisted Treatment of Opiate Dependence Stephen A. Wyatt, D.O. Dept. of Psychiatry Middlesex Hospital Middletown, CT Disclosures Speaker Panels- None Grant recipient - SAMHSA
10/19/15. Stephen Loyd, M.D., F.A.C.P Healthy Kingsport Meadowview Convention Center Kingsport, Tennessee October 17, 2015
 Stephen Loyd, M.D., F.A.C.P Healthy Kingsport Meadowview Convention Center Kingsport, Tennessee October 17, 2015 Receives no commercial support, in any form, from pharmaceutical companies or anyone else
Stephen Loyd, M.D., F.A.C.P Healthy Kingsport Meadowview Convention Center Kingsport, Tennessee October 17, 2015 Receives no commercial support, in any form, from pharmaceutical companies or anyone else
Heroin. How Is Heroin Abused? How Does Heroin Affect the Brain? What Other Adverse Effects Does Heroin Have on Health?
 Heroin Heroin is an opiate drug that is synthesized from morphine, a naturally occurring substance extracted from the seed pod of the Asian opium poppy plant. Heroin usually appears as a white or brown
Heroin Heroin is an opiate drug that is synthesized from morphine, a naturally occurring substance extracted from the seed pod of the Asian opium poppy plant. Heroin usually appears as a white or brown
NNEPQIN Guideline for the Management of Labor, Delivery and the Newborn in the Opioid Dependent Pregnancy. March 2014
 The following guidelines are intended only as a general educational resource for hospitals and clinicians, and are not intended to reflect or establish a standard of care or to replace individual clinician
The following guidelines are intended only as a general educational resource for hospitals and clinicians, and are not intended to reflect or establish a standard of care or to replace individual clinician
1. According to recent US national estimates, which of the following substances is associated
 1 Chapter 36. Substance-Related, Self-Assessment Questions 1. According to recent US national estimates, which of the following substances is associated with the highest incidence of new drug initiates
1 Chapter 36. Substance-Related, Self-Assessment Questions 1. According to recent US national estimates, which of the following substances is associated with the highest incidence of new drug initiates
How To Treat A Drug Addiction
 1 About drugs Drugs are substances that change a person s physical or mental state. The vast majority of drugs are used to treat medical conditions, both physical and mental. Some, however, are used outside
1 About drugs Drugs are substances that change a person s physical or mental state. The vast majority of drugs are used to treat medical conditions, both physical and mental. Some, however, are used outside
Substance Use Guideline 4B PERINATAL OPIOID EXPOSURE, CARE OF THE NEWBORN
 British Columbia Reproductive Care Program Substance Use Guideline 4B PERINATAL OPIOID EXPOSURE, CARE OF THE NEWBORN INTRODUCTION During the antenatal period, the opportunity exists for the primary care
British Columbia Reproductive Care Program Substance Use Guideline 4B PERINATAL OPIOID EXPOSURE, CARE OF THE NEWBORN INTRODUCTION During the antenatal period, the opportunity exists for the primary care
Addressing Substance Use in Pregnancy
 Addressing Substance Use in Pregnancy Stefan Maxwell, MD Director, NICU, CAMC Women and Children s Hospital Chair, Drug Use in Pregnancy Committee West Virginia Perinatal Partnership July 31, 2013 WV Early
Addressing Substance Use in Pregnancy Stefan Maxwell, MD Director, NICU, CAMC Women and Children s Hospital Chair, Drug Use in Pregnancy Committee West Virginia Perinatal Partnership July 31, 2013 WV Early
Established in 1974 Non-Profit Federal Block Grant recipient Accept Medicaid, Private Insurance, and Self-Pay.
 Established in 1974 Non-Profit Federal Block Grant recipient Accept Medicaid, Private Insurance, and Self-Pay. Patients are not denied treatment if they do not have the ability to pay for services Schedule
Established in 1974 Non-Profit Federal Block Grant recipient Accept Medicaid, Private Insurance, and Self-Pay. Patients are not denied treatment if they do not have the ability to pay for services Schedule
From the street to the NICU. Richard Christensen, PA, CAS
 From the street to the NICU Richard Christensen, PA, CAS Treatment works Truths Disconnect with pregnant women seeking treatment Disconnect between community and science Medication is not a stand-alone
From the street to the NICU Richard Christensen, PA, CAS Treatment works Truths Disconnect with pregnant women seeking treatment Disconnect between community and science Medication is not a stand-alone
Massachusetts Department of Public Health Guidelines for Community Standard for Maternal/Newborn Screening For Alcohol/Substance Use
 The Commonwealth of Massachusetts Executive Office of Health and Human Services Department of Public Health 250 Washington Street, Boston, MA 02108-4619 DEVAL L. PATRICK GOVERNOR TIMOTHY P. MURRAY LIEUTENANT
The Commonwealth of Massachusetts Executive Office of Health and Human Services Department of Public Health 250 Washington Street, Boston, MA 02108-4619 DEVAL L. PATRICK GOVERNOR TIMOTHY P. MURRAY LIEUTENANT
Neonatal Abstinence Syndrome
 Neonatal Abstinence Syndrome Effective Prevention Strategies Division of Prevention and Health Promotion Injury Prevention Program Objectives Characterize PDA as a public health problem Detail the impact
Neonatal Abstinence Syndrome Effective Prevention Strategies Division of Prevention and Health Promotion Injury Prevention Program Objectives Characterize PDA as a public health problem Detail the impact
Developing Human Fetus
 Period Date LAB. DEVELOPMENT OF A HUMAN FETUS After a human egg is fertilized with human sperm, the most amazing changes happen that allow a baby to develop. This amazing process, called development, normally
Period Date LAB. DEVELOPMENT OF A HUMAN FETUS After a human egg is fertilized with human sperm, the most amazing changes happen that allow a baby to develop. This amazing process, called development, normally
V11.2 NPIC/QAS. Special Quarterly Report: Linked Analysis Neonatal Abstinence Syndrome
 V11.2 NPIC/QAS Special Quarterly Report: Linked Analysis Neonatal Abstinence Syndrome I. Background The use of drugs and alcohol during pregnancy has been shown in several studies to affect the health
V11.2 NPIC/QAS Special Quarterly Report: Linked Analysis Neonatal Abstinence Syndrome I. Background The use of drugs and alcohol during pregnancy has been shown in several studies to affect the health
BABIES BORN TO ADDICTED MOTHERS
 BABIES BORN TO ADDICTED MOTHERS PATRICA M. MESSERLE LICENSED CLINICAL PSYCHOLOGIST, M.A., ABSNP LICENSED SCHOOL PSYCHOLOGIST DIPLOMATE OF THE AMERICAN BOARD OF SCHOOL- NEUROPSYCHOLOGY 1 Signs and Symptoms
BABIES BORN TO ADDICTED MOTHERS PATRICA M. MESSERLE LICENSED CLINICAL PSYCHOLOGIST, M.A., ABSNP LICENSED SCHOOL PSYCHOLOGIST DIPLOMATE OF THE AMERICAN BOARD OF SCHOOL- NEUROPSYCHOLOGY 1 Signs and Symptoms
Like cocaine, heroin is a drug that is illegal in some areas of the world. Heroin is highly addictive.
 Heroin Introduction Heroin is a powerful drug that affects the brain. People who use it can form a strong addiction. Addiction is when a drug user can t stop taking a drug, even when he or she wants to.
Heroin Introduction Heroin is a powerful drug that affects the brain. People who use it can form a strong addiction. Addiction is when a drug user can t stop taking a drug, even when he or she wants to.
The CCB Science 2 Service Distance Learning Program
 S2S 2055 DETOXIFICATION Module 1 Post-Test 1. A common use of a biochemical marker is. a. to support or refute other information that leads to proper diagnosis b. for forensic purposes c. in detecting
S2S 2055 DETOXIFICATION Module 1 Post-Test 1. A common use of a biochemical marker is. a. to support or refute other information that leads to proper diagnosis b. for forensic purposes c. in detecting
10/18/2012. The Impact of Substance Use on Newborns. Objectives. Do Infants Exposed to Maternal Opioids Have Drug Addiction?
 Objectives The Impact of Substance Use on Newborns Pamela Harris-Haman, CRNP, NNP-BC 1. Discuss the incidence of drug use in pregnancy and the percentage of infants that have abstinence syndrome. 2. Review
Objectives The Impact of Substance Use on Newborns Pamela Harris-Haman, CRNP, NNP-BC 1. Discuss the incidence of drug use in pregnancy and the percentage of infants that have abstinence syndrome. 2. Review
March of Dimes. FAQ on Drug Use and Pregnancy. November 2006. <http://www.marchofdimes.com/14332_1169.asp>. [accessed February 2010]
![March of Dimes. FAQ on Drug Use and Pregnancy. November 2006. <http://www.marchofdimes.com/14332_1169.asp>. [accessed February 2010]](/thumbs/27/11703693.jpg "March of Dimes. FAQ on Drug Use and Pregnancy. November 2006. <http://www.marchofdimes.com/14332_1169.asp>. [accessed February 2010]") March of Dimes. FAQ on Drug Use and Pregnancy. November 2006. . [accessed February 2010] After delivery, babies who were exposed to amphetamines before birth
March of Dimes. FAQ on Drug Use and Pregnancy. November 2006. . [accessed February 2010] After delivery, babies who were exposed to amphetamines before birth
Dependence and Addiction. Marek C. Chawarski, Ph.D. Yale University David Metzger, Ph.D. University of Pennsylvania
 Dependence and Addiction Marek C. Chawarski, Ph.D. Yale University David Metzger, Ph.D. University of Pennsylvania Overview Heroin and other opiates The disease of heroin addiction or dependence Effective
Dependence and Addiction Marek C. Chawarski, Ph.D. Yale University David Metzger, Ph.D. University of Pennsylvania Overview Heroin and other opiates The disease of heroin addiction or dependence Effective
Algorithm for Initiating Antidepressant Therapy in Depression
 Algorithm for Initiating Antidepressant Therapy in Depression Refer for psychotherapy if patient preference or add cognitive behavioural office skills to antidepressant medication Moderate to Severe depression
Algorithm for Initiating Antidepressant Therapy in Depression Refer for psychotherapy if patient preference or add cognitive behavioural office skills to antidepressant medication Moderate to Severe depression
Ethical Issues Related to Long-Term Consequences of Neonatal Abstinence Syndrome (NAS) Christopher Church, Ph.D.
 Christopher Church, Ph.D.") Ethical Issues Related to Long-Term Consequences of Neonatal Abstinence Syndrome (NAS) Christopher Church, Ph.D. Content and Objectives Content: Describe common ethical issues related to caring for babies
Ethical Issues Related to Long-Term Consequences of Neonatal Abstinence Syndrome (NAS) Christopher Church, Ph.D. Content and Objectives Content: Describe common ethical issues related to caring for babies
We re glad you are here! Agenda for the Day Breaks Lunch Q&A and note cards Phones
 We re glad you are here! Agenda for the Day Breaks Lunch Q&A and note cards Phones Learn about the history of opioid addiction and discuss what is happening today in Kentucky Learn about the disease of
We re glad you are here! Agenda for the Day Breaks Lunch Q&A and note cards Phones Learn about the history of opioid addiction and discuss what is happening today in Kentucky Learn about the disease of
Incidence. Substance Abuse. Care of the Drug Exposed Infant. 2010 National Survey on Drug Use and Health:
 Care of the Drug Exposed Infant Connie Anderson M.D. Assistant Professor of Pediatrics Saint Louis University School of Medicine Cardinal Glennon Children s Medical Center September 19,2012 Substance Abuse
Care of the Drug Exposed Infant Connie Anderson M.D. Assistant Professor of Pediatrics Saint Louis University School of Medicine Cardinal Glennon Children s Medical Center September 19,2012 Substance Abuse
Opiate Addiction in Ohio: An Update on Scope of Problem Ashland Ohio
 Governor s Cabinet Opiate Action Team Promoting Wellness and Recovery John R. Kasich, Governor Tracy J. Plouck, Director Opiate Addiction in Ohio: An Update on Scope of Problem Ashland Ohio November 14,
Governor s Cabinet Opiate Action Team Promoting Wellness and Recovery John R. Kasich, Governor Tracy J. Plouck, Director Opiate Addiction in Ohio: An Update on Scope of Problem Ashland Ohio November 14,
Treatment Approaches for Drug Addiction
 Treatment Approaches for Drug Addiction NOTE: This is a fact sheet covering research findings on effective treatment approaches for drug abuse and addiction. If you are seeking treatment, please call 1-800-662-HELP(4357)
Treatment Approaches for Drug Addiction NOTE: This is a fact sheet covering research findings on effective treatment approaches for drug abuse and addiction. If you are seeking treatment, please call 1-800-662-HELP(4357)
Naltrexone and Alcoholism Treatment Test
 Naltrexone and Alcoholism Treatment Test Following your reading of the course material found in TIP No. 28. Please read the following statements and indicate the correct answer on the answer sheet. A score
Naltrexone and Alcoholism Treatment Test Following your reading of the course material found in TIP No. 28. Please read the following statements and indicate the correct answer on the answer sheet. A score
PRESCRIPTION DRUG ABUSE: THE NATIONAL PERSPECTIVE
 PRESCRIPTION DRUG ABUSE: THE NATIONAL PERSPECTIVE May 19, 2012 National Association Boards of Pharmacy Annual Meeting Gil Kerlikowske, Director White House Office of National Drug Control Policy ONDCP
PRESCRIPTION DRUG ABUSE: THE NATIONAL PERSPECTIVE May 19, 2012 National Association Boards of Pharmacy Annual Meeting Gil Kerlikowske, Director White House Office of National Drug Control Policy ONDCP
Treatment Approaches for Drug Addiction
 Treatment Approaches for Drug Addiction [NOTE: This is a fact sheet covering research findings on effective treatment approaches for drug abuse and addiction. If you are seeking treatment, please call
Treatment Approaches for Drug Addiction [NOTE: This is a fact sheet covering research findings on effective treatment approaches for drug abuse and addiction. If you are seeking treatment, please call
Prescription Drugs: Abuse and Addiction
 EAP Drug Free Workplace Newsletter March 2014 Prescription Drugs: Abuse and Addiction What are some of the commonly abused prescription drugs? Although many prescription drugs can be abused or misused,
EAP Drug Free Workplace Newsletter March 2014 Prescription Drugs: Abuse and Addiction What are some of the commonly abused prescription drugs? Although many prescription drugs can be abused or misused,
1. The potential sites of action for sympathomimetics and the difference between a direct and indirect acting agonist.
 1 OBI 836 The Autonomic Nervous System-Sympathomimetics M.T. Piascik August 29, 2012 Learning Objectives Lecture II The student should be able to explain or describe 1. The potential sites of action for
1 OBI 836 The Autonomic Nervous System-Sympathomimetics M.T. Piascik August 29, 2012 Learning Objectives Lecture II The student should be able to explain or describe 1. The potential sites of action for
Antidepressants in Pregnancy D R S N E H A P A R G H I
 Antidepressants in Pregnancy D R S N E H A P A R G H I Overview Depression and its effects Antidepressants and their effects Birth defects Miscarriage Neonatal withdrawal Longterm consequences Breastfeeding
Antidepressants in Pregnancy D R S N E H A P A R G H I Overview Depression and its effects Antidepressants and their effects Birth defects Miscarriage Neonatal withdrawal Longterm consequences Breastfeeding
Care Management Council submission date: August 2013. Contact Information
 Clinical Practice Approval Form Clinical Practice Title: Acute use of Buprenorphine for the Treatment of Opioid Dependence and Detoxification Type of Review: New Clinical Practice Revisions of Existing
Clinical Practice Approval Form Clinical Practice Title: Acute use of Buprenorphine for the Treatment of Opioid Dependence and Detoxification Type of Review: New Clinical Practice Revisions of Existing
John R. Kasich, Governor Orman Hall, Director
 John R. Kasich, Governor Orman Hall, Director 2 3 Epidemics of unintentional drug overdoses in Ohio, 1979-2011 1,2,3 1800 1600 1400 1200 1000 800 Prescription drugs are causing a larger overdose epidemic
John R. Kasich, Governor Orman Hall, Director 2 3 Epidemics of unintentional drug overdoses in Ohio, 1979-2011 1,2,3 1800 1600 1400 1200 1000 800 Prescription drugs are causing a larger overdose epidemic
Death in the Suburbs: How Prescription Painkillers and Heroin Have Changed Treatment and Recovery
 Death in the Suburbs: How Prescription Painkillers and Heroin Have Changed Treatment and Recovery Marvin D. Seppala, MD Chief Medical Officer Hazelden Betty Ford Foundation This product is supported by
Death in the Suburbs: How Prescription Painkillers and Heroin Have Changed Treatment and Recovery Marvin D. Seppala, MD Chief Medical Officer Hazelden Betty Ford Foundation This product is supported by
This module reviews the following: Opioid addiction and the brain Descriptions and definitions of opioid agonists,
 BUPRENORPHINE TREATMENT: A Training For Multidisciplinary Addiction Professionals Module II Opioids 101 Goals for Module II This module reviews the following: Opioid addiction and the brain Descriptions
BUPRENORPHINE TREATMENT: A Training For Multidisciplinary Addiction Professionals Module II Opioids 101 Goals for Module II This module reviews the following: Opioid addiction and the brain Descriptions
Collaborative Care for Pregnant Women with Substance Use Disorders
 Collaborative Care for Pregnant Women with Substance Use Disorders Alane O Connor DNP Maine Dartmouth Family Medicine Residency MaineGeneral Medical Center Dartmouth Medical School Vanderbilt University
Collaborative Care for Pregnant Women with Substance Use Disorders Alane O Connor DNP Maine Dartmouth Family Medicine Residency MaineGeneral Medical Center Dartmouth Medical School Vanderbilt University
MAJOR DEPRESSION DURING CONCEPTION AND PREGNANCY: A Guide for Patients and Families
 MAJOR DEPRESSION DURING CONCEPTION AND PREGNANCY: A Guide for Patients and Families David A. Kahn, MD, Margaret L. Moline, PhD, Ruth W. Ross, MA, Lee S. Cohen, MD, and Lori L. Altshuler, MD www.womensmentalhealth.org
MAJOR DEPRESSION DURING CONCEPTION AND PREGNANCY: A Guide for Patients and Families David A. Kahn, MD, Margaret L. Moline, PhD, Ruth W. Ross, MA, Lee S. Cohen, MD, and Lori L. Altshuler, MD www.womensmentalhealth.org
Treatment of Opioid Dependence with Buprenorphine/Naloxone (Suboxone )
") Treatment of Opioid Dependence with Buprenorphine/Naloxone (Suboxone ) Elinore F. McCance-Katz, M.D., Ph.D. Professor and Chair, Addiction Psychiatry Virginia Commonwealth University Neurobiology of Opiate
Treatment of Opioid Dependence with Buprenorphine/Naloxone (Suboxone ) Elinore F. McCance-Katz, M.D., Ph.D. Professor and Chair, Addiction Psychiatry Virginia Commonwealth University Neurobiology of Opiate
Update on Buprenorphine: Induction and Ongoing Care
 Update on Buprenorphine: Induction and Ongoing Care Elizabeth F. Howell, M.D., DFAPA, FASAM Department of Psychiatry, University of Utah School of Medicine North Carolina Addiction Medicine Conference
Update on Buprenorphine: Induction and Ongoing Care Elizabeth F. Howell, M.D., DFAPA, FASAM Department of Psychiatry, University of Utah School of Medicine North Carolina Addiction Medicine Conference
Pregnancy and Substance Abuse
 Pregnancy and Substance Abuse Introduction When you are pregnant, you are not just "eating for two." You also breathe and drink for two, so it is important to carefully consider what you put into your
Pregnancy and Substance Abuse Introduction When you are pregnant, you are not just "eating for two." You also breathe and drink for two, so it is important to carefully consider what you put into your
Karol Kaltenbach, PhD Maternal Addiction Treatment Education and. Jefferson Medical College Thomas Jefferson University
 Benzodiazepines and the Pregnant Patient: Special Challenges Karol Kaltenbach, PhD Maternal Addiction Treatment Education and Research Jefferson Medical College Thomas Jefferson University Outline Introduction
Benzodiazepines and the Pregnant Patient: Special Challenges Karol Kaltenbach, PhD Maternal Addiction Treatment Education and Research Jefferson Medical College Thomas Jefferson University Outline Introduction
Substance-Exposed Newborns
 Substance-Exposed Newborns State of Oklahoma 2013 Substance-Exposed Newborns State of Oklahoma 2013 Legal Background Federal guidelines in the Child Abuse Prevention and Treatment Act (CAPTA) require states
Substance-Exposed Newborns State of Oklahoma 2013 Substance-Exposed Newborns State of Oklahoma 2013 Legal Background Federal guidelines in the Child Abuse Prevention and Treatment Act (CAPTA) require states
Medication Assisted Treatment as the Standard of Care for Opiate Dependent Pregnant Women
 Medication Assisted Treatment as the Standard of Care for Opiate Dependent Pregnant Women Jason B. Fields, MD Medical Director, DACCO This product is supported by Florida Department of Children and Families
Medication Assisted Treatment as the Standard of Care for Opiate Dependent Pregnant Women Jason B. Fields, MD Medical Director, DACCO This product is supported by Florida Department of Children and Families
Pharmacology of Opiates. Steve Hanson Associate Commissioner NYS OASAS
 Pharmacology of Opiates Steve Hanson Associate Commissioner NYS OASAS Neurotransmitter-receptor receptor interactions To transmit instructions to cells, neurotransmitters interact with their receptors.
Pharmacology of Opiates Steve Hanson Associate Commissioner NYS OASAS Neurotransmitter-receptor receptor interactions To transmit instructions to cells, neurotransmitters interact with their receptors.
New York State Office of Alcoholism & Substance Abuse Services Addiction Services for Prevention, Treatment, Recovery
 New York State Office of Alcoholism & Substance Abuse Services Addiction Services for Prevention, Treatment, Recovery USING THE 48 HOUR OBSERVATION BED USING THE 48 HOUR OBSERVATION BED Detoxification
New York State Office of Alcoholism & Substance Abuse Services Addiction Services for Prevention, Treatment, Recovery USING THE 48 HOUR OBSERVATION BED USING THE 48 HOUR OBSERVATION BED Detoxification
Alcohol and drugs Be proactive
 Alcohol and drugs Be proactive PREGNANCY: a critical time to take care of yourself and your future baby Pregnant women must often change certain daily habits and are bombarded with recommendations from
Alcohol and drugs Be proactive PREGNANCY: a critical time to take care of yourself and your future baby Pregnant women must often change certain daily habits and are bombarded with recommendations from
Medication-Assisted Addiction Treatment
 Medication-Assisted Addiction Treatment Molly Carney, Ph.D., M.B.A. Executive Director Evergreen Treatment Services Seattle, WA What is MAT? MAT is the use of medications, in combination with counseling
Medication-Assisted Addiction Treatment Molly Carney, Ph.D., M.B.A. Executive Director Evergreen Treatment Services Seattle, WA What is MAT? MAT is the use of medications, in combination with counseling
Substitution Therapy for Opioid Dependence The Role of Suboxone. Mandy Manak, MD, ABAM, CCSAM Methadone 101-Hospitalist Workshop, October 3, 2015
 Substitution Therapy for Opioid Dependence The Role of Suboxone Mandy Manak, MD, ABAM, CCSAM Methadone 101-Hospitalist Workshop, October 3, 2015 Objectives Recognize the options available in treating opioid
Substitution Therapy for Opioid Dependence The Role of Suboxone Mandy Manak, MD, ABAM, CCSAM Methadone 101-Hospitalist Workshop, October 3, 2015 Objectives Recognize the options available in treating opioid
Opiate Abuse and Mental Illness
 visited on Page 1 of 5 LEARN MORE (HTTP://WWW.NAMI.ORG/LEARN-MORE) FIND SUPPORT (HTTP://WWW.NAMI.ORG/FIND-SUPPORT) GET INVOLVED (HTTP://WWW.NAMI.ORG/GET-INVOLVED) DONATE (HTTPS://NAMI360.NAMI.ORG/EWEB/DYNAMICPAGE.ASPX?
visited on Page 1 of 5 LEARN MORE (HTTP://WWW.NAMI.ORG/LEARN-MORE) FIND SUPPORT (HTTP://WWW.NAMI.ORG/FIND-SUPPORT) GET INVOLVED (HTTP://WWW.NAMI.ORG/GET-INVOLVED) DONATE (HTTPS://NAMI360.NAMI.ORG/EWEB/DYNAMICPAGE.ASPX?
One example: Chapman and Huygens, 1988, British Journal of Addiction
 This is a fact in the treatment of alcohol and drug abuse: Patients who do well in treatment do well in any treatment and patients who do badly in treatment do badly in any treatment. One example: Chapman
This is a fact in the treatment of alcohol and drug abuse: Patients who do well in treatment do well in any treatment and patients who do badly in treatment do badly in any treatment. One example: Chapman
Alcoholism, Drug Addiction, and the Road to Recovery
 Alcoholism, Drug Addiction, and the Road to Recovery Life on the Edge Barry Stimmel, MD The Haworth Medical Press An Imprint of The Haworth Press, Inc. New York London Oxford CONTENTS Preface Acknowledgments
Alcoholism, Drug Addiction, and the Road to Recovery Life on the Edge Barry Stimmel, MD The Haworth Medical Press An Imprint of The Haworth Press, Inc. New York London Oxford CONTENTS Preface Acknowledgments
Policy Consideration and Collaborative Partnerships: Working with Opioid Dependent Pregnant and Parenting Women
 Policy Consideration and Collaborative Partnerships: Working with Opioid Dependent Pregnant and Parenting Women 2015 San Diego International Conference on Child and Family Maltreatment January 26-30, 2015
Policy Consideration and Collaborative Partnerships: Working with Opioid Dependent Pregnant and Parenting Women 2015 San Diego International Conference on Child and Family Maltreatment January 26-30, 2015
Karla Ramirez, LCSW Director, Outpatient Services Laurel Ridge Treatment Center
 Karla Ramirez, LCSW Director, Outpatient Services Laurel Ridge Treatment Center 1 in 4 Americans will have an alcohol or drug problems at some point in their lives. The number of alcohol abusers and addicts
Karla Ramirez, LCSW Director, Outpatient Services Laurel Ridge Treatment Center 1 in 4 Americans will have an alcohol or drug problems at some point in their lives. The number of alcohol abusers and addicts
WITHDRAWAL OF ANALGESIA AND SEDATION
 WITHDRAWAL OF ANALGESIA AND SEDATION Patients receiving analgesia and/or sedation for longer than 5-7 days may suffer withdrawal if these drugs are suddenly stopped. To prevent this happening drug doses
WITHDRAWAL OF ANALGESIA AND SEDATION Patients receiving analgesia and/or sedation for longer than 5-7 days may suffer withdrawal if these drugs are suddenly stopped. To prevent this happening drug doses
HEROIN AND RELATED OPIATES
 HEROIN AND RELATED OPIATES DAVID J. NUTT Psychopharmacology Unit, Bristol University Heroin is a derivative of morphine and both belong to a large family of drugs called the opiates, that were originally
HEROIN AND RELATED OPIATES DAVID J. NUTT Psychopharmacology Unit, Bristol University Heroin is a derivative of morphine and both belong to a large family of drugs called the opiates, that were originally
FRN Research Report January 2012: Treatment Outcomes for Opiate Addiction at La Paloma
 FRN Research Report January 2012: Treatment Outcomes for Opiate Addiction at La Paloma Background A growing opiate abuse epidemic has highlighted the need for effective treatment options. This study documents
FRN Research Report January 2012: Treatment Outcomes for Opiate Addiction at La Paloma Background A growing opiate abuse epidemic has highlighted the need for effective treatment options. This study documents
MEDICATION ASSISTED TREATMENT FOR OPIOID ADDICTION
 MEDICATION ASSISTED TREATMENT FOR OPIOID ADDICTION Mark Fisher Program Administrator State Opioid Treatment Adminstrator Kentucky Division of Behavioral Health OBJECTIVES Learn about types of opioids and
MEDICATION ASSISTED TREATMENT FOR OPIOID ADDICTION Mark Fisher Program Administrator State Opioid Treatment Adminstrator Kentucky Division of Behavioral Health OBJECTIVES Learn about types of opioids and
Important facts to remember
 Important facts to remember If you re pregnant or trying to get pregnant, or if you know someone who is, there are several important points to remember: See a healthcare professional regularly. Get plenty
Important facts to remember If you re pregnant or trying to get pregnant, or if you know someone who is, there are several important points to remember: See a healthcare professional regularly. Get plenty
DrugFacts: Treatment Approaches for Drug Addiction
 DrugFacts: Treatment Approaches for Drug Addiction NOTE: This is a fact sheet covering research findings on effective treatment approaches for drug abuse and addiction. If you are seeking treatment, please
DrugFacts: Treatment Approaches for Drug Addiction NOTE: This is a fact sheet covering research findings on effective treatment approaches for drug abuse and addiction. If you are seeking treatment, please
Advanced Treatment for Opioid & Alcohol Dependence. John Larson, M.D. Corporate Medical Director Gateway Foundation
 Advanced Treatment for Opioid & Alcohol Dependence John Larson, M.D. Corporate Medical Director Gateway Foundation Background 41 years practicing psychiatry Last 15 in addiction medicine I ve watched a
Advanced Treatment for Opioid & Alcohol Dependence John Larson, M.D. Corporate Medical Director Gateway Foundation Background 41 years practicing psychiatry Last 15 in addiction medicine I ve watched a
Disclosure. Objectives. ~History~ 5/11/2015. ~History~
 Disclosure Dr. Reilly has disclosed no relevant financial relationships with any commercial interests. 2015 Annual WAPC Conference Maureen Reilly DNP, NNP-BC bjectives At the conclusion of the session,
Disclosure Dr. Reilly has disclosed no relevant financial relationships with any commercial interests. 2015 Annual WAPC Conference Maureen Reilly DNP, NNP-BC bjectives At the conclusion of the session,
Naltrexone Pellet Treatment for Opiate, Heroin, and Alcohol Addiction. Frequently Asked Questions
 Naltrexone Pellet Treatment for Opiate, Heroin, and Alcohol Addiction Frequently Asked Questions What is Naltrexone? Naltrexone is a prescription drug that effectively blocks the effects of heroin, alcohol,
Naltrexone Pellet Treatment for Opiate, Heroin, and Alcohol Addiction Frequently Asked Questions What is Naltrexone? Naltrexone is a prescription drug that effectively blocks the effects of heroin, alcohol,
Understanding Addiction: The Intersection of Biology and Psychology
 Understanding Addiction: The Intersection of Biology and Psychology Robert Heimer, Ph.D. Yale University School of Public Health Center for Interdisciplinary Research on AIDS New Haven, CT, USA November
Understanding Addiction: The Intersection of Biology and Psychology Robert Heimer, Ph.D. Yale University School of Public Health Center for Interdisciplinary Research on AIDS New Haven, CT, USA November
Using Drugs to Treat Drug Addiction How it works and why it makes sense
 Using Drugs to Treat Drug Addiction How it works and why it makes sense Jeff Baxter, MD University of Massachusetts Medical School May 17, 2011 Objectives Biological basis of addiction Is addiction a chronic
Using Drugs to Treat Drug Addiction How it works and why it makes sense Jeff Baxter, MD University of Massachusetts Medical School May 17, 2011 Objectives Biological basis of addiction Is addiction a chronic
4/18/14. Background. Evaluation of a Morphine Weaning Protocol in Pediatric Intensive Care Patients. Background. Signs and Symptoms of Withdrawal
 Background 1 Evaluation of a Morphine Weaning Protocol in Pediatric Intensive Care Patients Alyssa Cavanaugh, PharmD PGY1 Pharmacy Resident Children s Hospital of Michigan **The speaker has no actual or
Background 1 Evaluation of a Morphine Weaning Protocol in Pediatric Intensive Care Patients Alyssa Cavanaugh, PharmD PGY1 Pharmacy Resident Children s Hospital of Michigan **The speaker has no actual or
The Clinical Content of Preconception Care: Alcohol, Tobacco, and Illicit Drug Exposures
 The Clinical Content of Preconception Care: Alcohol, Tobacco, and Illicit Drug Exposures by R. Louise Floyd, DSN, RN; Brian W. Jack, MD; Robert Cefalo, MD, PhD; Hani Atrash, MD, MPH; Jeanne Mahoney, BSN,
The Clinical Content of Preconception Care: Alcohol, Tobacco, and Illicit Drug Exposures by R. Louise Floyd, DSN, RN; Brian W. Jack, MD; Robert Cefalo, MD, PhD; Hani Atrash, MD, MPH; Jeanne Mahoney, BSN,
MEDICALLY MONITORED ACUTE TREATMENT SERVICES. Brief Guide for Providers
 MEDICALLY MONITORED ACUTE TREATMENT SERVICES Brief Guide for Providers Introduction: Pregnant women are a priority population for substance abuse treatment services. The Bureau of Substance Abuse Services
MEDICALLY MONITORED ACUTE TREATMENT SERVICES Brief Guide for Providers Introduction: Pregnant women are a priority population for substance abuse treatment services. The Bureau of Substance Abuse Services
OVERVIEW OF MEDICATION ASSISTED TREATMENT
 Sarah Akerman MD Assistant Professor of Psychiatry Director of Addiction Services Geisel School of Medicine/Dartmouth-Hitchcock Medical Center OVERVIEW OF MEDICATION ASSISTED TREATMENT Conflicts of Interest
Sarah Akerman MD Assistant Professor of Psychiatry Director of Addiction Services Geisel School of Medicine/Dartmouth-Hitchcock Medical Center OVERVIEW OF MEDICATION ASSISTED TREATMENT Conflicts of Interest
Evaluation of a Morphine Weaning Protocol in Pediatric Intensive Care Patients
 Evaluation of a Morphine Weaning Protocol in Pediatric Intensive Care Patients Jennifer Kuhns, Pharm.D. Pharmacy Practice Resident Children s Hospital of Michigan **The speaker has no actual or potential
Evaluation of a Morphine Weaning Protocol in Pediatric Intensive Care Patients Jennifer Kuhns, Pharm.D. Pharmacy Practice Resident Children s Hospital of Michigan **The speaker has no actual or potential
Update and Review of Medication Assisted Treatments
 Update and Review of Medication Assisted Treatments for Opiate and Alcohol Use Disorders Richard N. Whitney, MD Medical Director Addiction Services Shepherd Hill Newark, Ohio Medication Assisted Treatment
Update and Review of Medication Assisted Treatments for Opiate and Alcohol Use Disorders Richard N. Whitney, MD Medical Director Addiction Services Shepherd Hill Newark, Ohio Medication Assisted Treatment
FDA Presentation: Maternal Perspective on Opioid Medication Assisted Therapy
 FDA Presentation: Maternal Perspective on Opioid Medication Assisted Therapy Lorraine A. Milio, M.D. Obstetrical Director Center for Addiction and Pregnancy Assistant Professor Maternal-Fetal Medicine
FDA Presentation: Maternal Perspective on Opioid Medication Assisted Therapy Lorraine A. Milio, M.D. Obstetrical Director Center for Addiction and Pregnancy Assistant Professor Maternal-Fetal Medicine
Drug addiction. These factors increase the likelihood of your having an addiction to a legal or an illegal drug:
 Drug addiction You may be hooked emotionally and psychologically. You may have a physical dependence, too. If you're addicted to a drug whether it's legal or illegal you have intense cravings for it. You
Drug addiction You may be hooked emotionally and psychologically. You may have a physical dependence, too. If you're addicted to a drug whether it's legal or illegal you have intense cravings for it. You
Opioid Addiction and Methadone: Myths and Misconceptions. Nicole Nakatsu WRHA Practice Development Pharmacist
 Opioid Addiction and Methadone: Myths and Misconceptions Nicole Nakatsu WRHA Practice Development Pharmacist Learning Objectives By the end of this presentation you should be able to: Understand how opioids
Opioid Addiction and Methadone: Myths and Misconceptions Nicole Nakatsu WRHA Practice Development Pharmacist Learning Objectives By the end of this presentation you should be able to: Understand how opioids
opiates alcohol 27 opiates and alcohol 30 April 2016 drug addiction signs 42 Ranked #1 123 Drug Rehab Centers in New Jersey 100 Top 10 380
 opiates alcohol 27 opiates and alcohol 30 April 2016 drug addiction signs 42 ed #1 123 Drug Rehab Centers in New Jersey 100 Top 10 380 effects of alcohol in the brain 100 Top 30 698 heroin addiction 100
opiates alcohol 27 opiates and alcohol 30 April 2016 drug addiction signs 42 ed #1 123 Drug Rehab Centers in New Jersey 100 Top 10 380 effects of alcohol in the brain 100 Top 30 698 heroin addiction 100