Basics. Hair Follicle. Adult human has 5 million follicles All are present at birth About 1 million on head and 100,000 alone on scalp
|
|
|
- Merry Daniels
- 8 years ago
- Views:
Transcription
1

2 Basics Hair Follicle Adult human has 5 million follicles All are present at birth About 1 million on head and 100,000 alone on scalp

3 Hair Follicle: cycling Each hair follicle perpetually cycles through three stages Cycling is independent, not synchronous Many molecular signals orchestrate the transition of these stages

4 Hair physiology With each hair cycle, remodeling of the follicle below the isthmus occurs (impermanent portion) Reservoir of pluripotent cells responsible for regeneration reside in the bulge region near the site of arrector pili attachment Langerhans cells are concentrated in the infundibular epithelium, bulge and sebaceous epithelium and initiate immune response When inflammation is limited to the lower follicle as in non scarring alopecias, the potential to regrow hair remains intact When inflammation affects the upper portion of the hair follicle, permanent functional disruption of the bulge area results in permanent alopecia

5 Hair Follicle: cycling Anagen (90%) Growth phase 2-6 years hair grows approximately 0.35 mm/day longer anagen phase= longer hair Initiation: insulin like growth factor 1 Fibroblast growth factor 7 Androgen??? Cessation: Fibroblast growth factor 5

6 Hair Follicle: cycling Catagen (<1%) Involution phase Lasts 2-3 weeks Apoptosis of follicular keratinocytes Dermal papillae condenses and rises to the bulge

7 Hair Follicle: cycling Telogen (10%) Resting/ shedding phase Lasts 2-3 months scalp hairs per day

8 Hair Cycles

9 Evaluating Hair Loss Tests: Hair pull Hair pluck Hair analysis (microscope) Hair collection and count Hair shave window Scalp biopsy: Vertical Horizontal DIF

10

11 Androgenetic Alopecia Pathogenesis Androgen dependent Increased 5 alpha reductase activity on testosterone/ DHEA --> increased DHT--> TGFbeta 1 production from dermal papilla cells which mediates hair growth suppression Higher levels of 5 alpha reductase and androgen receptors in frontal hair follicles vs occipital follicles Progressive miniaturization (terminal--> vellus) decrease dermal papilla size, decrease in size of hair matrix, decrease in hair shaft diameter, decrease in anagen phase, more rapid cycling, follicle becomes more superficial with finer, shorter, less pigmented hair

12 Histology Androgenetic Alopecia Decrease in anagen and increase in telogen follicles Miniaturized follicles and shaft diameter variability Vascular or fibromucinous fibrous tract remnant below miniaturized or telogen follicles

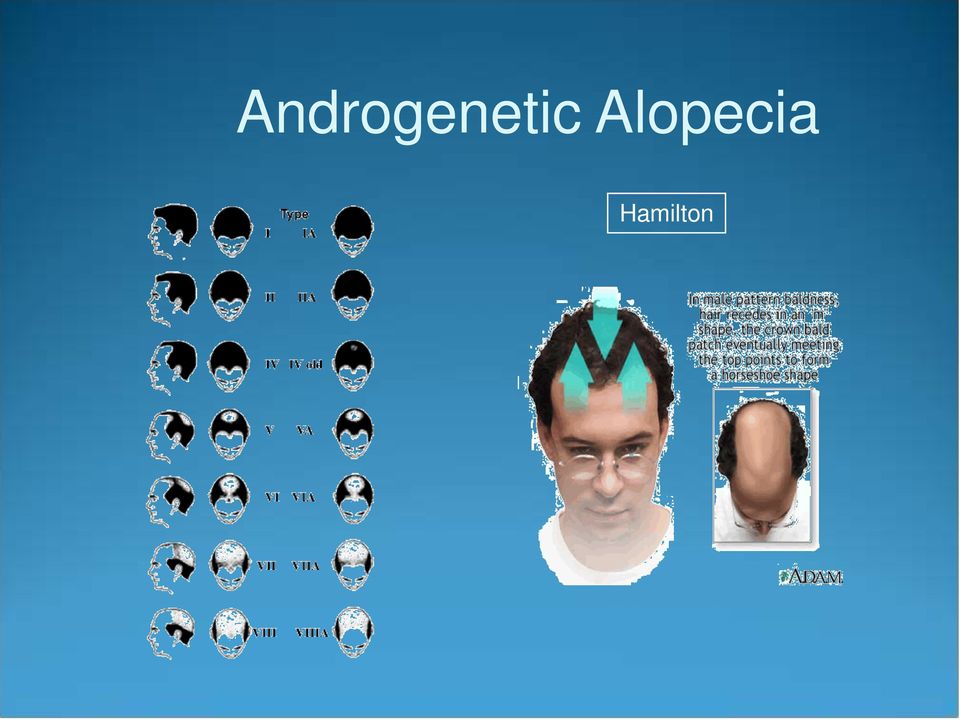
13 Androgenetic Alopecia (Male Pattern Baldness) Clinical Begins in the teens, 20s or early 30s Thought to be autosomal dominant with incomplete penetrance and polygenic inheritance affects 50% of men Exam Whisker or kinky hair may be the first sign Most frequent pattern is bitemporal recession and vertex balding Anterior hairline recedes on each side in the Geheimratswinkeln ( professor angles ) Normal hair pull
 Normal")
14 Androgenetic Alopecia Hamilton
15 Male Androgenetic Alopecia Treatment Topical minoxidil promotes survival of dermal papilla cells, induces and prolongs anagen phase, and results in enlargement of shaft diameter (vellus-->terminal hairs) Finasteride (men aged 18-41) Type 2 5-alpha reductase inhibitor Prolongs anagen phase 1 mg daily can prevent further hair loss and increase hair counts hair patterning on the temples is not improved Hair transplantation of occipital hair follicles to anterior scalp

16 Female Androgenetic Alopecia (Female Pattern Hair Loss) History Gradual, may begin anytime after puberty with peaks in the 20s and 40s, perimenopausally, or at times of hormone change Clinical Diffuse thinning over frontoparietal scalp with preserved frontal hairline Christmas tree pattern midline part - widest anteriorly Subset with male type pattern of bitemporal recession more common in postmenopausal women Part width on crown > occiput Hair pull test may be negative or positive Trichodynia common symptom

17 Female Androgenetic Alopecia Ludwig s classification

18 Female Androgenetic Alopecia Workup Determined by signs and symptoms Consider TSH, T3, T4, ferritin, DHEA-S, free testosterone and total testosterone Most have normal androgen levels

19 Female Androgenetic Alopecia Treatment Topical minoxidil Oral antiandrogens spironolactone cyproterone acetate more effective than minoxidil when when signs of hyperandrogenism, hypersoberhhea, menstrual abnormalities and high body mass index Finasteride in subset with temporal recession Hair transplantation, wigs, interwoven hair

20 Telogen Effluvium Clinical Increased shedding of club hairs with diffuse hair loss from the roots May lose per day Trichodynia common symptom and often coexist with signs of depression, obsessive personality disorder and anxiety Acute TE- Often triggering event 2-5 months before onset i.e. illness, parturition, operation, hospitalization, loss of loved one, divorce, medications change, crash diet self limited usually within 6-12 months Chronic TE- insidious onset or acute TE that never resolves lasts 6 months to years continuous or fluctuating hair loss

21 Exam Telogen Effluvium Normal scalp, diffuse thinning, part width of crown = occiput Positive hair pull test- grasp 40 hairs firmly and pull slowly >4-6 club hairs is positive Other tests if hair pull test not positive daily hair shed counts collect all hairs lost during pre shampoo 1 minute combing session (back to front) x 3 consecutive days (10-15 normal, >50 common in TE) clip test trichogram evaluation Normal telogen hairs-depigmented club shaped bulb, no sheath Hair often appears to be of normal thickness (perceptibly thin hair more common with preexisting pattern alopecia) Shorter regrowing hairs in frontal and bitemporal areas
22
23 Telogen Effluvium Genetics no known genetic cause Histology Normal follicles without inflammation Active phase- >12-15% of terminal follicles in telogen Associations Iron deficiencey, thyroid disease, and medications (beta blockers, some antihyperlipemics, NSAIDS, HRT, anticoagulants)
24 Telogen Effluvium Types 1 Immediate anagen release- Premature conversion of many anagen hairs through catagen to telogen induced by stressor (e.g. drugs, high fever, starvation/dieting) 2 Delayed anagen release- Prolonged anagen phase secondary to pregnancy hormones with large shift to telogen once hormonal drive removed 3 Short anagen- shorter hair which traverses the hair cycle more quickly and is shed more often- chronic TE and androgenetic alopeica 4 Immediate telogen release- can occur with topical minoxidil 5 Delayed telogen release- no known clinical correlate 6 Chronic
25 Telogen Effluvium Evaluation Iron and thyroid labs if history suggestive or if course prolonged scalp biopsy if diagnosis unclear Treatment Address any coexisting scalp disease Iron replacement 5% Minoxidil
26 Anagen Effluvium History Abrupt loss of all growing hairs (90%) secondary to hair shaft fracture 1-2 months following chemotherapy/trigger Exam Diffuse alopecia, no scalp irritation Histology Normal
27
28 Anagen Effluvium Pathogenesis It is always abnormal to shed anagen hairs Mitotic inhibition temporarily shuts down the rapidly dividing hair matrix cells resulting in tapering of the shaft (Pohl-Pinkus constrictions) and breakage of the hair when this thin portion reaches the surface Treatment Drug cessation Re-growth begins a few weeks after insult May have different color or texture Pressure cuff around scalp during chemo and scalp hypothermia may prevent Minoxidil may shorten period of baldness by 50 days
29 Alopecia Areata Clinical Rapid, complete loss of hair in patches Types diffuse (least common)- widespread thinning totalis universalis ophiasis (bandlike along peripheral temporal and occipital scalp) sisaipho (loss of hair on entire scalp except for temporal and occipital) generally presents as an anagen effluvium, with an inflammatory insult to the hair matrix resulting in tapering of the hair shaft and fracture of anagen hairs migratory poliosis
30 Alopecia Areata Exam Bald, circumscribed patches Exclamation point hairs at periphery (distal end broader than proximal end) White re-growth If active, positive hair pull at periphery associated nail findings uniform pitting, trachyonychia, onychomadesis, red or spotted lunulae
31
32 Alopecia Areata Epidemiology M=F increased risk with other autoimmune conditions (vitiligo, DM, lupus erythematosus, RA, thyroiditis, myasthenia gravis) atopic dermatitis, Down syndrome, lichen planus Genetics 25% with positive family history Family history strongest in early onset disease (<30 y/o) early onset severe familial disease associated with HLA DR4, DR11, and DQ7
33 Alopecia Areata Pathogenesis T cell directed autoimmune attack on hair follicle target= follicular melanocytes (white hair rarely affected, regrowing hair often depigmented) collapse of immune privilege? normal anagen hair bulb lacks MHC I and II HLA expressed in AA allowing interaction of cytotoxic T cells with matrix cells
34 Alopecia Areata Histology swarm of bees : T-cell infiltrate around anagen hair bulbs miniaturization of follicles fibrous tract remnants beneath miniaturized bulbs contain lymphoid cells, eos, and melanin pigment Work up thyroid function tests if suggestive signs or symptoms or if strong family history of thyroid disease Prognosis high rate of spontaneous recovery in postpubertal onset poor prognosis with atopic dermatitis, childhood onset, widespread involvement, ophiasis, duration longer than 5 years, onychodystrophy
35
36 Alopecia Areata Treatment IL steroids treatment of choice for localized cosmeticdally conspicuous patches high strength topical steroids Immunomodulators Squaric acid dibutyl ester, DNCB, diphencyprone in refractory cases (blockade of leukocyte trafficking and extravasation) PUVA SCAT topical minoxidil
37 History: Trichotillomania Often presents in childhood, F>M Patient unaware of own behavior; presents with hair loss May elicit history of stress/anxiety when hair loss began may relate history of localized follicular pain relieved with plucking Exam: irregularly shaped patches hairs of various lengths Normal hair pull test Hair re-growth in shaved windows Pathogenesis: Self-induced plucking or breaking of hair Manifestation of an obsessive-compulsive disorder/ anxiety/ depression
38 Trichotillomania
39 Trichotillomania Histology: empty anagen follicles increased catagen hairs pigment casts within infundibulum trichomalacia hemorrhage Treatment: Psychiatric evaluation SSRIs
40 Trichotillomania
41 Clinical Traction Alopecia African Americans, Japanese women, and Sikh men in India Children and young adults Hair won t grow along the periphery of scalp Usually complain of itching and dandruff Exam Bilateral hair loss along periphery, especially temples and above the ears Initially, pruritus, perifollicular erythema, and hyperkeratosis may be present, creating a seborrheic picture abundance of broken hairs scale and pustules may have positive hair pull test persistent traction--> follicular atrophy --> fine, short hair
42 Traction Alopecia
43 Pathogenesis Prolonged tension on hair causes increased release from roots and can lead to secondary inflammation Excessive traction for prolonged periods leads to conversion of the anagen phase to the telogen phase Histology Increased telogen count Late development of fibrous tracts Treatment Traction Alopecia Prevention- process is reversible early
44
45 Scarring Alopecias Diagnostic hallmarks are visible loss of follicular ostia and destruction of the hair follicle on histopathologic examination Primary Target of destruction is the hair follicle Secondary Nonfollicular disease indirectly causes follicular destruction e.g. sarcoid, morphea, leprosy many scarring alopecias begin as nonscarring inflammation typically affects upper portion of follicle
46 Scarring alopecias Treatment should be managed as a trichologic emergency during initial nonscarring phase Topical minoxidil if coexistent AGA- may improve cosmesis by enlarging miniaturized hairs (1 ml of 5% sol n bid x at least 1 year) wig, hair color-matched powder hair transplantation and scalp reduction once completely burned out sun protection
47 Proposed NAHRS working classification of primary cicatricial alopecia Lymphocytic Chronic cutaneous lupus erythematosus Lichen planopilaris Classic Frontal fibrosing alopecia Graham- Little syndrome Central centrifugal cicatricial alopecia Alopecia mucinosa Keratosis follicularis spinulosa decalvans Neutrophilic Folliculitis decalvans Dissecting cellulitis Mixed Acne keloidalis Acne necrotica Erosive pustular dermatosis Nonspecific
48
49 Discoid Lupus Clinical females>males onset between 20 and 40 years of age Patients complain of hair loss, pruritus, stinging, burning, scalp tenderness Exam Well-circumscribed, coin shaped erythematous, atrophic plaque with mottled hyper- and hypopigmentation Plugged follicular ostia ( carpet tacking ) Pull test often yields anagen hairs May show other rash of DLE Pathogenesis Autoimmune UV light possible antigenic stimulus
50
51 Discoid Lupus Course Spontaneous remission in 1/3 to 1/2 within 4 years 5-10% of adults ad 26-31% of children and adolescents --> SLE course of systemic disease often severe with renal or neurologic involvement unless SLE predates DLE Complications disfigurement ulceration SCC- 31% metastasis rate
52 Discoid Lupus Histology hyperkeratosis, follicular plugging, vacuolar interface dermatitis, BMZ thickening, dermal mucin, pigment incontinence patchy perivascular and periadnexal inflammation perifollicular lymphoid infiltrates involve the isthmus inflammation of fibrous tract remnants creates dense vertical columns of lymphocytes scarring of follicular units and intervening dermis DIF- full house -continuous granular IgG, IgM, IgA, and C3 at D-E junction
53 Discoid Lupus Follicular plugging Perivascular hyalinization Follicular lichenoid infiltrate Thick, hyalinized BMZ Dermal mucinosis.
54 Discoid Lupus Treatment Sun avoidance Limited active disease class I or II steroids topically or intralesional steroids or both Reports of calcineurin inhibitors, imiquimod, tazorac Rapidly progressive or extensive disease antimalarials Oral prednisone as temporizing measure if severe Oral retinoids if resistance to antimalarials Dapsone, thalidomide, sulfasalazine, mycophenolate mofetil, and methotrexate also been reported Low threshold to biopsy persistent treatment resistant hyperkeratotic or ulcerated foci
55 Lichen Planopilaris A follicular variant of lichen planus Hair is a necessary cofactor 3 forms Classic lichen planopilaris, Frontal fibrosing alopecia, and Graham- Little syndrome
56 Lichen Planopilaris Pathogenesis Similar to LP Postulated that an antigenic trigger (i.e certain medications) initiates disease and ultimately elicits lesional expression of keratinocyte autoantigens with an ensuant CD 8+ T-cell mediated lichenoid response with destruction of follicular basilar epitehelium Implicated medications include gold, atabrine, quinacrine, hepatitis B vaccine associated with Hepatitis C
57 Lichen Planopilaris Classic Clinical onset in middle age females> males 17%-28% with extracranial LP at presentation and 50% during course Common symptoms include hair loss, pruritus, scaling, burning, and scalp tenderness
58 Lichen Planopilaris Exam Classic Active disease marked by follicular hyperkeratosis and perifollicular erythema Burnt out disease marked by depigmented shiny patches typically multifocal and central hair loss and scarring after months disease activity limited to hair bearing periphery of cicatrized alopecia (vs DLE, alopecia mucinosa) pull test positive for anagen hairs
59
60 Lichen Planopilaris Pathology Classic D-E junction of the upper follicle (infundibulum in particular) obscured by lichenoid lymphocytic infiltrate Follicular destruction and foreign body hair shaft granulomas with evolution wedge shaped superficial dermal scar DIF- patchy or shaggy fibrinogen and clumped IgM along the follicular BMZ
61 Lichen Planopilaris
62 Lichen Planopilaris Classic Evaluation drug history hep C status if eroded or ulcerated scalp lesions Treatment local disease topical moderate or high potency topical steroids, intralesional steroids, or both steroid refractory, rapidly progressive, or extensive active or symptomatic disease low dose oral retinoids antimalarials reports of griseofulvin, cyclosporine, and low molecular weight heparin
63 Lichen Planopilaris Frontal fibrosing alopecia A patterned variant of LPP that primarily affects postmenopausal women Clinical shiny, uniformly pale, bandlike zone of incomplete hair loss 1-8 cm in width affecting frontotemporal hairline new hairline with perifollicular erythema and hyperkeratosis thinned to absent eyebrows nonscarring axillary and extremity hair loss may also have classic LPP or extracranial LP
64 Lichen Planopilaris Frontal fibrosing alopecia Pathology Indistinguishable from classic LPP Treatment twice daily midpotency topical steroids may lead to stabilization oral prednisone or chloroquine may be tried for rapidly progressive disease
65 Lichen Planopilaris Frontal fibrosing alopecia
66 Lichen Planopilaris Graham-Little syndrome AKA Graham- Little- Piccardi- Lassuer syndrome Clinical adults patchy cicatricial alopecia of the scalp with follicular hyperkeratosis or erythema nonscarring alopecia of axillae and pubis Grouped spinous follicular papules that resemble lichen spinulosus or KP on the trunk and extremities Pathology features of LPP or keratosis pilaris atrophicans Treatment reports of topical, intralesional, or oral steroids, cyclosporine
67 Lichen Planopilaris Graham- Little syndrome
68 Pseudopelade of Brocq Named for its likeness to alopecia areata (la pelade) AKA alopecia cicatrisata distinct entity vs variant of certain primary cicatricial alopecias (LPP and DLE) vs common final stage of several cicatricial alopecias Clinical chronic, insidious onset typically asymptomatic
69 Pseudopelade of Brocq Exam confetti like, coin sized, hypopigmented or flesh colored, atrophic oval to round plaques of noninflamed cicatricial alopecia ( footprints in the snow ) commonly involves the vertex no pustules, crusts or broken off hairs never has an inflammatory stage pull test positive for anagen hairs
70 Pseudopelade of Brocq Histology no pathognomonic features described absent epidermal atrophy and interface changes DIF usually negative Treatment reported success with topical steroids, intralesional steroids, prednisone, hydroxychloroquine, isotretinoin the disease usually reaches an inactive endpoint after many years
71
72 Central Centrifugal Cicatricial Alopecia Encompasses the terms hot comb alopecia, follicular degeneration syndrome, pseudopelade in African Americans, and central elliptical pseudopelade in Caucasians Unique entity vs common morphologic pattern shared by different disorders Clinical Slowly progressive, symmetric, noninflammatory cicatricial alopecia of the central scalp Most commonly seen in African American females May have islands of unaffected hair within areas of scar Frequently asymptomatic, but pins and needles sensation, pruritus and tenderness also common
73 Central Centrifugal Cicatricial Alopecia Pathophysiology Unclear whether due to intrinsic defect in inner root sheath desquamation or exogenous factors such as various hair styling procedures Pathology Premature inner root sheath desquamation, perifollicular lymphocytic infiltrate surrounding upper follicle, follicular fibrosis in end stage disease Treatment Discontinue traumatic hair grooming practices Success reported with daily potent topical steroid and tetracycline 500 mg bid
74
75 Alopecia Mucinosa Inflammatory condition of the pilosebaceous unit that can result in nonscarring and scarring alopecia Alopecia mucinosa = disease process Follicular mucinosis= histologic features Skin limited vs associated with follicular MF Clinical All ages Lesional pruritus, sensory dissociation, anhidrosis Exam Classically involves head and neck hypopigmented or erythematous, scaly or eczematous plaques, or plaques composed of flesh colored follicular papules May see black dot sign because affected hair shafts prone to breakage
76
77 Alopecia Mucinosa Associated malignancy No reliable clinical criteria for differentiation of benign from malignancy associated disease Adults- MF reported to occur in 9-60% Children and young adults- Hodgkin s lymphoma Can present as a paraneoplastic phenomenon Follicular MF is more refractory to treatment and has a worse prognosis than classic CTCL Pathology Lesional T cell clonality is common but doesn t connote malignancy or predict progression to lymphoma mucin (hyaluronic acid) within cells of sebaceous gland and outer root sheath No concentric lamellar fibrosis vs other primary cicatricial alopecias
78
79 Alopecia Mucinosa Treatment Regular examinations with lymph node palpation Serial biopsies with disease progression Topical, intralesional, and oral steroids, minocycline, anti staph antibiotics if staph culture positive, topical and oral retinoids, dapsone, topical and oral indomethacin, topical nitrogen mustard, phototherapy, excision, PUVA
80 Keratosis Follicularis Spinulosa Decalvans AKA keratosis pilaris decalvans, Siemens-1 syndrome Characterized by cicatricial alopecia of the scalp, widespread KP followed by atrophy, and photophobia Morphologically similar to ulerythema ophryogenes and atrophoderma vermiculata defect on gene for spermidine/spermine N(1)- acetyltransferase in one X linked form
81 Keratosis Follicularis Spinulosa Decalvans Clinical onset in infancy or early childhood with follicular hyperkeratosis first on the face with eventual widespread distribution then develop patchy scalp, eyebrow, and eyelash alopecia followed by scarring onset of photophobia coincides with cutaneous disease and is marked by corneal dystrophy with punctate defects
82 Keratosis Follicularis Spinulosa Decalvans Pathology compact hyperkeratosis and hypergranulosis of the upper follicular epithelium early sparse perivascular and perifollicular mononuclear cell infiltrate with mucin and loose connective tissue around the upper follicle with advancing disease granulomatous inflammation with follicular destruction, concentric perifollicular and horizontal adventitial lamellar fibrosis, and scarred follicular tracts late Treatment sustained topical and intralesional steroids oral retionoids baseline and routine ophthalmologic exams
83
84 Folliculitis Decalvans A destructive suppurative folliculitis Clinical young and middle aged adults typically affects scalp periodic crops of painful or pruritic follicular pustules or papules that coalesce and eventually form atrophic areas of scarring alopecia active disease continues peripherally as a marginated perifollicular pustules and tufted folliculitis chronic and slowly progressive
85 Folliculitis Decalvans
86 Folliculitis Decalvans Pathogenesis S aureus usually isolated from pustules and thought to be etiologic antigen by some Postulated that follicular destruction secondary to abnormal suppurative immune response likely incited by staph and other organisms vs chronic staph infection
87 Folliculitis Decalvans Histology intra- and peri- follicular neutrophilic infiltrate affecting upper and middle parts of follicle wedge shaped superficial dermal scar Treatment if other symptoms of immunodeficiency, evaluate accordingly culture pustules anti-staph antibiotic the combination of rifampin + clindamycin, fusidic acid (alternatively topical mupirocin or topical erythromycin) and oral zinc sulfate have resulted in remission for months to years
88 Tufted Folliculitis Pattern of scarring alopecia seen in a wide range of scarring alopecias presents with doll s hair like bundling of follicular units 5-20 hairs emerge from common dilated follicular orifice
89 Dissecting Cellulitis AKA Perifolliculitis capitis abscedens et suffodiens Thought to be result of abnormal keratinization leading to obstruction, secondary bacterial infection, and follicular destruction Clinical >80% black males 18 to 40 years old vertex and occiput are sites of predilection follicular inflammatory nodules suppurate and undermine to form intercommunicating sinuses initially develop a nonscarring alopecia over nodules which eventually becomes scarring ~ 1/3 have coexisting acne conglobata or hidradenitis suppuritiva and at risk for HLA B27 negative spondyloarthropathy
90
91 Dissecting Cellulitis Histology intra- and peri- follicular neutrophilic infiltration with follicular perforation, develop abscesses in perifollicular mid to deep dermis and superficial fat Inflammation replaced by fibrosis Treatment isotretionoin first line 1 mg/kg/d x 4 months minimum followed by mg/kg/d x 5-7 months intralesional steroids oral antibiotics oral zinc I and D or excisional CO2 laser with secondary intention healing/ marsupialization
92
93 Acne Keloidalis Clinical predominantly affects the nuchal hairline of young black, Hispanic or Asian postpubertal males A unique race related property of the pilosebaceous unit, hair shaft, or scalp skin has been postulated to underlie disease evolution Flesh colored to reddish brown smooth firm follicular papules May enlarge and coalesce into a large keloidal plaque Proposed precipitants include mechanical trauma (shirt collar, excoriation), infection (demodex, bacteria), and autoimmunity Drug induced reports in white males diphenylhydantoin + carbamazepine (1) cyclosporine (4)
94 Acne Keloidalis Pathology follicular dilatation and peri infundibular mixed infiltrate eventual follicular rupture with granuloma or microabscess formation around extruded hair shaft fragments no keloidal collagen Treatment topical and intralesional steroids topical retinoids topical and oral antibiotics surgical excision
95 Acne Keloidalis
96 Acne Necrotica 2 forms acne necrotica miliaris nonscarring superficial folliculitis that possibly represents variant of same disease process with individual host response responsible for clinical expression acne necrotica varioliformis necrotizing follicular disorder that heals with varioliform scars proposed causes: abnormal response to S aureus or P acnes, excoriation of underlying folliculiltis, and rosacea like genesis
97 Acne Necrotica Clinical (varioliformis) chronic relapsing disorder of adults commonly involves anterior hairline, also seborrheic face and chest crops of pruritic, tender red-brown papules or pustules that umbilicate and undergo central necrosis leaving varioliform scars Pathology confluent necrosis of follicular epithelium and adjacent epidermis containing fragmented bits of hair Treatment culture directed antibiotics oral tetracyclines (if culture negative) topical or intralesional steroids if refractory isotretinoin in culture proven P acnes or intractable cases doxepin
98 Erosive pustular dermatosis Idiopathic, chronic sterile pustular dermatosis of scalp resulting in scarring alopecia Often history of trauma (sunburn, zoster, abrasion, radiation, topical 5-FU, cryotherapy, topical tretinoin, chronic actinic damage) Clinical usually elderly female predominance large, asymptomatic, boggy, superficially crusted plaque that when unroofed reveals a beefy red exudative erosion with flaccid pustules episodic pustular flares with slow enlargement
99 Pathology Erosive pustular dermatosis nonspecific Treatment typically improves rapidly with class I and II topical steroids BID, requires maintenance antibiotics topical calcipotriol 0.005% cream BID x 2 months zinc sulfate
STOP HAIR LOSS DR JOYCE LIM DERMATOLOGIST PARAGON MEDICAL CENTRE #11-16/20
 STOP HAIR LOSS DR JOYCE LIM DERMATOLOGIST PARAGON MEDICAL CENTRE #11-16/20 HAIR LOSS Types of Hair loss What causes them What are the solutions HAIR LOSS PATCHY HAIR LOSS PATCHY HAIR LOSS Single/ Multiple
STOP HAIR LOSS DR JOYCE LIM DERMATOLOGIST PARAGON MEDICAL CENTRE #11-16/20 HAIR LOSS Types of Hair loss What causes them What are the solutions HAIR LOSS PATCHY HAIR LOSS PATCHY HAIR LOSS Single/ Multiple
www.healthoracle.org 1
 How does hair grow and should it recycle? A single hair follicle grows its hair strand over a period of four to six years (the anagen phase). It then rests for two to four months (the telogen phase), after
How does hair grow and should it recycle? A single hair follicle grows its hair strand over a period of four to six years (the anagen phase). It then rests for two to four months (the telogen phase), after
Oxford University Hospitals. NHS Trust. Dermatology Department Frontal Fibrosing Alopecia. Information for patients
 Oxford University Hospitals NHS Trust Dermatology Department Frontal Fibrosing Alopecia Information for patients What is Frontal Fibrosing Alopecia (FFA)? FFA is a condition which causes hair loss, mainly
Oxford University Hospitals NHS Trust Dermatology Department Frontal Fibrosing Alopecia Information for patients What is Frontal Fibrosing Alopecia (FFA)? FFA is a condition which causes hair loss, mainly
B. Disorders of sebaceous glands
 Go Back to the Top To Order, Visit the Purchasing Page for Details B. Disorders of sebaceous glands 1. Acne vulgaris It most frequently occurs on the face of adolescent men and women. Comedones, folliculitis,
Go Back to the Top To Order, Visit the Purchasing Page for Details B. Disorders of sebaceous glands 1. Acne vulgaris It most frequently occurs on the face of adolescent men and women. Comedones, folliculitis,
X-Plain Alopecia Reference Summary
 X-Plain Alopecia Reference Summary Introduction Hair loss is very common in both men and women. You or someone you love may be experiencing hair loss. Hair follicle Learning about normal hair growth is
X-Plain Alopecia Reference Summary Introduction Hair loss is very common in both men and women. You or someone you love may be experiencing hair loss. Hair follicle Learning about normal hair growth is
Acne. Sofia Chaudhry M.D. Histology of an inflamed comedo. Bolognia, 2008.
 Acne Sofia Chaudhry M.D. Histology of an inflamed comedo. Bolognia, 2008. Acne Vulgaris (Common Acne) Multifactorial disorder of pilosebaceous unit Affects 40-50 million individuals annually in U.S. alone
Acne Sofia Chaudhry M.D. Histology of an inflamed comedo. Bolognia, 2008. Acne Vulgaris (Common Acne) Multifactorial disorder of pilosebaceous unit Affects 40-50 million individuals annually in U.S. alone
What is androgenetic alopecia?
 What is androgenetic alopecia? Androgenetic alopecia is also called male pattern alopecia. It refers to a symptom that develops after puberty, influenced by the androgen, where thinning and/or loss of
What is androgenetic alopecia? Androgenetic alopecia is also called male pattern alopecia. It refers to a symptom that develops after puberty, influenced by the androgen, where thinning and/or loss of
Pathogenesis 10/04/2015. Acne
 Deepani Rathnayake MBBS, MD, FACD Acne Affects >80% of adolescents >40% of adults Associated with Disfigurement Loss of confidence Depression Affects quality of life Pathogenesis i) increased sebum production,
Deepani Rathnayake MBBS, MD, FACD Acne Affects >80% of adolescents >40% of adults Associated with Disfigurement Loss of confidence Depression Affects quality of life Pathogenesis i) increased sebum production,
Smoothbeam Laser Treatment of Acne Vulgaris. Emerging Applications
 Smoothbeam Laser Treatment of Acne Vulgaris Emerging Applications About Acne Vulgaris Very common - Affects 80% of population Almost every person experiences acne Most common reason to visit dermatologist
Smoothbeam Laser Treatment of Acne Vulgaris Emerging Applications About Acne Vulgaris Very common - Affects 80% of population Almost every person experiences acne Most common reason to visit dermatologist
Hair Chemistry. Chapter 1. Hair Relaxers Science, Design, and Application www.alluredbooks.com
 Hair Relaxers Science, Design, and Application www.alluredbooks.com Chapter 1 Hair Chemistry We all know that the hair on our head is dead, but underneath the scalp, within the hair follicle, is a surprisingly
Hair Relaxers Science, Design, and Application www.alluredbooks.com Chapter 1 Hair Chemistry We all know that the hair on our head is dead, but underneath the scalp, within the hair follicle, is a surprisingly
X-Plain Acne Reference Summary
 X-Plain Acne Reference Summary Introduction Nearly 17 million people in the United States have acne, making it one of the most common skin diseases in the USA. Although acne is not a serious health threat,
X-Plain Acne Reference Summary Introduction Nearly 17 million people in the United States have acne, making it one of the most common skin diseases in the USA. Although acne is not a serious health threat,
Acne Vulgaris: Basic Facts
 Acne 1 Module Instructions The following module contains hyperlinked information which serves to offer more information on topics you may or may not be familiar with. We encourage that you read all the
Acne 1 Module Instructions The following module contains hyperlinked information which serves to offer more information on topics you may or may not be familiar with. We encourage that you read all the
HAIR LOSS IN WOMEN. by DAVID SALINGER. www.hair-loss-centre.com.au
 HAIR LOSS IN WOMEN by DAVID SALINGER HAIR LOSS IN WOMEN Loss of hair does worry people and when you realise that so many factors can be responsible for hair loss, you can appreciate that it is important
HAIR LOSS IN WOMEN by DAVID SALINGER HAIR LOSS IN WOMEN Loss of hair does worry people and when you realise that so many factors can be responsible for hair loss, you can appreciate that it is important
Spongiotic reaction pattern Spongiosis = Intercellular edema Elongation of bridges vesiculation, bullae?mechanism unclear Fluid comes from dermis Impo
 Spongiotic Reaction Pattern and review Nathan C. Walk, M.D. Spongiotic reaction pattern Spongiosis = Intercellular edema Elongation of bridges vesiculation, bullae?mechanism unclear Fluid comes from dermis
Spongiotic Reaction Pattern and review Nathan C. Walk, M.D. Spongiotic reaction pattern Spongiosis = Intercellular edema Elongation of bridges vesiculation, bullae?mechanism unclear Fluid comes from dermis
Proceeding of the NAVC North American Veterinary Conference Jan. 8-12, 2005, Orlando, Florida
 Proceeding of the NAVC North American Veterinary Conference Jan. 8-12, 2005, Orlando, Florida Reprinted in the IVIS website with the permission of the NAVC http:/// Small Animal - Dermatology CLINICAL
Proceeding of the NAVC North American Veterinary Conference Jan. 8-12, 2005, Orlando, Florida Reprinted in the IVIS website with the permission of the NAVC http:/// Small Animal - Dermatology CLINICAL
PROPERTIES OF THE HAIR AND SCALP
 PROPERTIES OF THE HAIR AND SCALP 1. The scientific study of hair, its diseases and care is called: a. dermatology c. biology b. trichology d. cosmetology 2. The two parts of a mature hair strand are the
PROPERTIES OF THE HAIR AND SCALP 1. The scientific study of hair, its diseases and care is called: a. dermatology c. biology b. trichology d. cosmetology 2. The two parts of a mature hair strand are the
Hair Loss. The medical term for hair loss is alopecia and there are many types. What is the normal cycle of hair growth and loss?
 Hair Loss By Eamonn Brady (MPSI) The medical term for hair loss is alopecia and there are many types. What is the normal cycle of hair growth and loss? Hair is composed of protein called keratin. Keratin
Hair Loss By Eamonn Brady (MPSI) The medical term for hair loss is alopecia and there are many types. What is the normal cycle of hair growth and loss? Hair is composed of protein called keratin. Keratin
Psoriasis. Psoriasis. Mark A. Bechtel, M.D. Director of Dermatology The Ohio State University College of Medicine
 Psoriasis Mark A. Bechtel, M.D. Director of Dermatology The Ohio State University College of Medicine Psoriasis Psoriasis is a chronic skin disorder resulting from a polygenic predisposition combined with
Psoriasis Mark A. Bechtel, M.D. Director of Dermatology The Ohio State University College of Medicine Psoriasis Psoriasis is a chronic skin disorder resulting from a polygenic predisposition combined with
FastTest. You ve read the book... ... now test yourself
 FastTest You ve read the book...... now test yourself To ensure you have learned the key points that will improve your patient care, read the authors questions below. Please refer back to relevant sections
FastTest You ve read the book...... now test yourself To ensure you have learned the key points that will improve your patient care, read the authors questions below. Please refer back to relevant sections
Psoriasis. Student's Name. Institution. Date of Submission
 Running head: PSORIASIS Psoriasis Student's Name Institution Date of Submission PSORIASIS 1 Abstract Psoriasis is a non-contagious chronic skin disease that is characterized by inflammatory and multiplying
Running head: PSORIASIS Psoriasis Student's Name Institution Date of Submission PSORIASIS 1 Abstract Psoriasis is a non-contagious chronic skin disease that is characterized by inflammatory and multiplying
X-Plain Psoriasis Reference Summary
 X-Plain Psoriasis Reference Summary Introduction Psoriasis is a long-lasting skin disease that causes the skin to become inflamed. Patches of thick, red skin are covered with silvery scales. It affects
X-Plain Psoriasis Reference Summary Introduction Psoriasis is a long-lasting skin disease that causes the skin to become inflamed. Patches of thick, red skin are covered with silvery scales. It affects
Treatment of Hair Loss
 Treatment of Hair Loss Prof.Dr. Hoda Rasheed Professor of dermatology Faculty of medicine Cairo University Causes of hair loss Androgens Aging of the follicles Decreased blood supply Decresed thickness
Treatment of Hair Loss Prof.Dr. Hoda Rasheed Professor of dermatology Faculty of medicine Cairo University Causes of hair loss Androgens Aging of the follicles Decreased blood supply Decresed thickness
How To Treat Fd With Tolmao
 Clinical trial Treatment of folliculitis decalvans with tacrolimus ointment Jesús Bastida, MD, Pedro Valerón-Almazán, MD, Néstor Santana-Molina, MD, Carolina Medina-Gil, MD, and Gregorio Carretero-Hernández,
Clinical trial Treatment of folliculitis decalvans with tacrolimus ointment Jesús Bastida, MD, Pedro Valerón-Almazán, MD, Néstor Santana-Molina, MD, Carolina Medina-Gil, MD, and Gregorio Carretero-Hernández,
HIRSUTISM. What are the aims of this leaflet?
 HIRSUTISM What are the aims of this leaflet? This leaflet has been written to help you understand more about hirsutism. It tells you what it is, what causes it, what can be done about it, and provides
HIRSUTISM What are the aims of this leaflet? This leaflet has been written to help you understand more about hirsutism. It tells you what it is, what causes it, what can be done about it, and provides
acne Dr. M. Goeteyn Dermatologie AZ Sint-Jan Brugge-Oostende AV marleen.goeteyn@azsintjan.be
 acne Dr. M. Goeteyn Dermatologie AZ Sint-Jan Brugge-Oostende AV marleen.goeteyn@azsintjan.be Why should you treat acne? -Impact on the quality of life -scarring What is acne? Acne is an inflammatory disease
acne Dr. M. Goeteyn Dermatologie AZ Sint-Jan Brugge-Oostende AV marleen.goeteyn@azsintjan.be Why should you treat acne? -Impact on the quality of life -scarring What is acne? Acne is an inflammatory disease
 no!no! Thermicon: A Novel, Home-based Hair Removal Device Dr. Mira Barki Yavne, Israel Introduction Lasers and intense pulsed light sources have become a popular method for long-term removal of unwanted
no!no! Thermicon: A Novel, Home-based Hair Removal Device Dr. Mira Barki Yavne, Israel Introduction Lasers and intense pulsed light sources have become a popular method for long-term removal of unwanted
Diffuse hair loss: Its triggers and management
 REVIEW CME CREDIT EDUCATIONAL OBJECTIVE: Readers will recognize when hair loss may be the result of a trigger disrupting the normal cycle of hair growth Shannon Harrison, MBBS, MMed Clinical Research Fellow,
REVIEW CME CREDIT EDUCATIONAL OBJECTIVE: Readers will recognize when hair loss may be the result of a trigger disrupting the normal cycle of hair growth Shannon Harrison, MBBS, MMed Clinical Research Fellow,
ACNE. Nisakorn Saewan, Ph.D.
 ACNE, Ph.D. Contents Definition Cause of acne Type of acne Acne grades Acne treatments Objectives To explain the definition of acne To elucidate cause of acne To identify type and grade of acne To explain
ACNE, Ph.D. Contents Definition Cause of acne Type of acne Acne grades Acne treatments Objectives To explain the definition of acne To elucidate cause of acne To identify type and grade of acne To explain
The Integumentary System Dr. Ali Ebneshahidi
 The Integumentary System Dr. Ali Ebneshahidi The Skin The integument system consists of the skin (cutaneous membrane) and its accessory organs. The skin is composed of three layers of tissue: the outer
The Integumentary System Dr. Ali Ebneshahidi The Skin The integument system consists of the skin (cutaneous membrane) and its accessory organs. The skin is composed of three layers of tissue: the outer
Mane Australia. FAQs. General Questions
 Mane Australia There is no guaranteed cure for hair loss, but with Mane you can have instantly thicker, natural looking hair in seconds; without the need for expensive clinical treatments, drugs or painful
Mane Australia There is no guaranteed cure for hair loss, but with Mane you can have instantly thicker, natural looking hair in seconds; without the need for expensive clinical treatments, drugs or painful
Hair Loss (Alopecia) Alopecia. Anatomy and Physiology of Hair. The Active Follicle
 Alopecia. Anatomy and Physiology of Hair. The Active Follicle") Dr. Sahni BS DHMS Hons, PGRT (BOM), FF Hom Deputy Chief Medical Officer (H), ONGC Hospital Panvel-410221, Navi Mumbai, INDIA Hair Loss (Alopecia) Website: http://www.homoeopathyclinic.com Email: drsahnibs@vsnl.com
Dr. Sahni BS DHMS Hons, PGRT (BOM), FF Hom Deputy Chief Medical Officer (H), ONGC Hospital Panvel-410221, Navi Mumbai, INDIA Hair Loss (Alopecia) Website: http://www.homoeopathyclinic.com Email: drsahnibs@vsnl.com
Acne (Acne Vulgaris) A common type of bacteria that lives on the skin, known as Propionibacterium acnes, sometimes
 A common type of bacteria that lives on the skin, known as Propionibacterium acnes, sometimes") Acne (Acne Vulgaris) Acne, clinically known as acne vulgaris, is the most common skin disease. It affects 85% of teenagers, some as young as 12, and often continues into adulthood. It is also called pimples,
Acne (Acne Vulgaris) Acne, clinically known as acne vulgaris, is the most common skin disease. It affects 85% of teenagers, some as young as 12, and often continues into adulthood. It is also called pimples,
Before you know about your future see your past before improving your future hair see what has been and is the state of your hair now Ravi Bhanot
 Chapter 1 All you need to know about hair almost Before you know about your future see your past before improving your future hair see what has been and is the state of your hair now Ravi Bhanot Typically
Chapter 1 All you need to know about hair almost Before you know about your future see your past before improving your future hair see what has been and is the state of your hair now Ravi Bhanot Typically
Getting to the Root of Hair Loss
 26 March 2012 MP3 at voaspecialenglish.com Getting to the Root of Hair Loss Reuters An example of male pattern baldness SHIRLEY GRIFFITH: This is SCIENCE IN THE NEWS in VOA Special English. I'm Shirley
26 March 2012 MP3 at voaspecialenglish.com Getting to the Root of Hair Loss Reuters An example of male pattern baldness SHIRLEY GRIFFITH: This is SCIENCE IN THE NEWS in VOA Special English. I'm Shirley
MANAGING ACNE IN PHARMACY
 MANAGING ACNE IN PHARMACY ACNE PREVALENCE Acne is the most common of skin diseases, affecting 85 per cent of Australians aged 15-24 years old. Very few people manage to escape their teenage and young adult
MANAGING ACNE IN PHARMACY ACNE PREVALENCE Acne is the most common of skin diseases, affecting 85 per cent of Australians aged 15-24 years old. Very few people manage to escape their teenage and young adult
All About Human Hair and Hair Loss. 1. Story
 All About Human Hair and Hair Loss 1. Story Hair has always been an important sign of beauty. This is especially true for women. Next to the face, hair is one of the main qualities people look for when
All About Human Hair and Hair Loss 1. Story Hair has always been an important sign of beauty. This is especially true for women. Next to the face, hair is one of the main qualities people look for when
Melanoma The Skin Understanding Cancer
 Melanoma A form of cancer that begins in melanocytes (cells that make the pigment melanin). It may begin in a mole (skin melanoma), but can also begin in other pigmented tissues, such as in the eye or
Melanoma A form of cancer that begins in melanocytes (cells that make the pigment melanin). It may begin in a mole (skin melanoma), but can also begin in other pigmented tissues, such as in the eye or
family study of seven male cases and six female
 36 J Med Genet 1992; 29: 36-40 Keratosis follicularis spinulosa decalvans: a family study of seven male cases and six female carriers Loes D M van Osch, Arnold P Oranje, Frank M Keukens, Pieter C van Voorst
36 J Med Genet 1992; 29: 36-40 Keratosis follicularis spinulosa decalvans: a family study of seven male cases and six female carriers Loes D M van Osch, Arnold P Oranje, Frank M Keukens, Pieter C van Voorst
MEDICAL POLICY No. 91456-R13 SKIN CONDITIONS I. POLICY/CRITERIA
 SKIN CONDITIONS MEDICAL POLICY Effective Date: June 2, 2014 Review Dates: 8/02, 2/03, 8/03, 7/04, 7/05, 6/06, 2/07, 8/07, 2/08, 2/09, 10/09, 4/10, 4/11, 4/12, 4/13, 5/14, 5/15 Date Of Origin: August 28,
SKIN CONDITIONS MEDICAL POLICY Effective Date: June 2, 2014 Review Dates: 8/02, 2/03, 8/03, 7/04, 7/05, 6/06, 2/07, 8/07, 2/08, 2/09, 10/09, 4/10, 4/11, 4/12, 4/13, 5/14, 5/15 Date Of Origin: August 28,
ACNE AND ROSACEA. Disclosure. Distribution of Acne 6/12/2014. NJAFP 2014 Summer Celebration & Scientific Assembly 1
 ACNE AND ROSACEA Everett Schlam, MD Assistant Director, Mountainside Hospital Family Medicine Residency Program, Verona, NJ Disclosure Dr. Schlam has indicated that he has nothing to disclose relevant
ACNE AND ROSACEA Everett Schlam, MD Assistant Director, Mountainside Hospital Family Medicine Residency Program, Verona, NJ Disclosure Dr. Schlam has indicated that he has nothing to disclose relevant
where hair grows Hair Restoration NO SCARS NO PAIN NO STRIPS It s your Hair - 100% Natural Results
 where hair grows Hair Restoration NO SCARS NO PAIN NO STRIPS It s your Hair - 100% Natural Results GOING BALD? HAIR LOSS? THINNING? NO MORE! - HAIR RESTORATION FROM FUECLINICS Hair transplantation involves
where hair grows Hair Restoration NO SCARS NO PAIN NO STRIPS It s your Hair - 100% Natural Results GOING BALD? HAIR LOSS? THINNING? NO MORE! - HAIR RESTORATION FROM FUECLINICS Hair transplantation involves
Inflammation and Healing. Review of Normal Defenses. Review of Normal Capillary Exchange. BIO 375 Pathophysiology
 Inflammation and Healing BIO 375 Pathophysiology Review of Normal Defenses Review of Normal Capillary Exchange 1 Inflammation Inflammation is a biochemical and cellular process that occurs in vascularized
Inflammation and Healing BIO 375 Pathophysiology Review of Normal Defenses Review of Normal Capillary Exchange 1 Inflammation Inflammation is a biochemical and cellular process that occurs in vascularized
NURS 821 Alterations in the Musculoskeletal System. Rheumatoid Arthritis. Type III Hypersensitivity Response
 NURS 821 Alterations in the Musculoskeletal System Margaret H. Birney PhD, RN Lecture 12 Part 2 Joint Disorders (cont d) Rheumatoid Arthritis Definition: Autoimmune disorder occurring in genetically sensitive
NURS 821 Alterations in the Musculoskeletal System Margaret H. Birney PhD, RN Lecture 12 Part 2 Joint Disorders (cont d) Rheumatoid Arthritis Definition: Autoimmune disorder occurring in genetically sensitive
Not Your Father s Hair Restoration: The Latest Clinical Advancements from Lasers to Robots in Treating in Men and Women
 Not Your Father s Hair Restoration: The Latest Clinical Advancements from Lasers to Robots in Treating in Men and Women Robert T. Leonard, Jr., DO, FAACS, FISHRS Founder and Chief Surgeon Leonard Hair
Not Your Father s Hair Restoration: The Latest Clinical Advancements from Lasers to Robots in Treating in Men and Women Robert T. Leonard, Jr., DO, FAACS, FISHRS Founder and Chief Surgeon Leonard Hair
Vesiculobullous Diseases Non-Infectious Etiology. Vesiculobullous Diseases. Infectious Etiology
 Vesicles and Pustules in the Newborn Julian Trevino, M.D. Associate Professor Boonshoft School of Medicine Department of Dermatology Vesicles and Pustules in the Newborn Represent wide spectrum of disorders
Vesicles and Pustules in the Newborn Julian Trevino, M.D. Associate Professor Boonshoft School of Medicine Department of Dermatology Vesicles and Pustules in the Newborn Represent wide spectrum of disorders
Hair loss? I ve got a grip on it! Brochure for women on hair loss and its treatment. Dependably effective against hair loss
 Hair loss? I ve got a grip on it! Brochure for women on hair loss and its treatment Dependably effective against hair loss Hair is part of a woman s natural beauty. Hair loss is more than a medical problem
Hair loss? I ve got a grip on it! Brochure for women on hair loss and its treatment Dependably effective against hair loss Hair is part of a woman s natural beauty. Hair loss is more than a medical problem
Cutaneous Lymphoma FAST FACTS
 Cutaneous Lymphoma FAST FACTS What is Cutaneous Lymphoma? Cutaneous lymphomas are types of non-hodgkin s lymphomas (NHL) that originate in the lymphocytes (white blood cells). Unlike most other types of
Cutaneous Lymphoma FAST FACTS What is Cutaneous Lymphoma? Cutaneous lymphomas are types of non-hodgkin s lymphomas (NHL) that originate in the lymphocytes (white blood cells). Unlike most other types of
Acne Vulgaris: Pathophysiology, diagnosis, and treatment of a common dermatologic condition
 Acne Vulgaris: Pathophysiology, diagnosis, and treatment of a common dermatologic condition Latasha Weeks, B.A., B.S. Doctor of Pharmacy Candidate, 2007 University of Maryland School of Pharmacy Learning
Acne Vulgaris: Pathophysiology, diagnosis, and treatment of a common dermatologic condition Latasha Weeks, B.A., B.S. Doctor of Pharmacy Candidate, 2007 University of Maryland School of Pharmacy Learning
Summary Acne vulgaris is a chronic, treatable disease but response to treatment may be delayed.
 TREATMENT OF ACNE VULGARIS Summary Acne vulgaris is a chronic, treatable disease but response to treatment may be delayed. Topical agents are useful as monotherapy for mild acne and in combination with
TREATMENT OF ACNE VULGARIS Summary Acne vulgaris is a chronic, treatable disease but response to treatment may be delayed. Topical agents are useful as monotherapy for mild acne and in combination with
MEDICAL MANAGEMENT POLICY
 TITLE: Scar Revision/Keloid PAGE: 1of 9 This Medical policy is not a guarantee of benefits or coverage, nor should it be deemed as medical advice. In the event of any conflict concerning benefit coverage,
TITLE: Scar Revision/Keloid PAGE: 1of 9 This Medical policy is not a guarantee of benefits or coverage, nor should it be deemed as medical advice. In the event of any conflict concerning benefit coverage,
Common Dermatologic Problems in Medicine
 Common Dermatologic Problems in Medicine Toby Maurer, MD University of California, San Francisco Psoriasis-What is it? Fast growing skin-takes 3 days to come to surface and desquamate Normal rate is 28
Common Dermatologic Problems in Medicine Toby Maurer, MD University of California, San Francisco Psoriasis-What is it? Fast growing skin-takes 3 days to come to surface and desquamate Normal rate is 28
F r e q u e n t l y A s k e d Q u e s t i o n s
 Acne who specializes in treating skin problems) about how you can help prevent acne and if treatment would help you. Q: What is acne? A: Acne is a disorder that causes outbreaks of skin lesions commonly
Acne who specializes in treating skin problems) about how you can help prevent acne and if treatment would help you. Q: What is acne? A: Acne is a disorder that causes outbreaks of skin lesions commonly
Informed Consent For Laser Hair Removal
 Informed Consent For Laser Hair Removal INSTRUCTIONS This informed-consent document has been prepared to help inform you about laser procedures, its risks, as well as alternative treatment(s). It is important
Informed Consent For Laser Hair Removal INSTRUCTIONS This informed-consent document has been prepared to help inform you about laser procedures, its risks, as well as alternative treatment(s). It is important
A t f e t r e r th t is s lec e t c u t re r e t h t e e st s u t den e t t sh s ould b e e a b a le e t o t :
 Dermatopharmacology Prof Werner Sinclair Department of Dermatology University of the Free State Outcomes for this Lecture After this lecture the student should be able to: Name the most important characteristics
Dermatopharmacology Prof Werner Sinclair Department of Dermatology University of the Free State Outcomes for this Lecture After this lecture the student should be able to: Name the most important characteristics
What is Psoriasis? Common Areas Affected. Type Who Does it Affect Characteristics
 What is? is a term derived from the Greek word psōra which means itch and is a common, long lasting, inflammatory skin condition which affects 1-3% of the UK population and about 80 million people worldwide.
What is? is a term derived from the Greek word psōra which means itch and is a common, long lasting, inflammatory skin condition which affects 1-3% of the UK population and about 80 million people worldwide.
Two main classes: Epithelial Connective (synovial) Epithelial. Cutaneous Mucous Serous
 Epithelial. Cutaneous Mucous Serous") Two main classes: Epithelial Connective (synovial) Epithelial Cutaneous Mucous Serous Epithelial Membranes = sheet of epithelia + connective tissue base 1. Cutaneous membrane: outer skin layer (stratified
Two main classes: Epithelial Connective (synovial) Epithelial Cutaneous Mucous Serous Epithelial Membranes = sheet of epithelia + connective tissue base 1. Cutaneous membrane: outer skin layer (stratified
Thyroid Eye Disease. Anatomy: There are 6 muscles that move your eye.
 Thyroid Eye Disease Your doctor thinks you have thyroid orbitopathy. This is an autoimmune condition where your body's immune system is producing factors that stimulate enlargement of the muscles that
Thyroid Eye Disease Your doctor thinks you have thyroid orbitopathy. This is an autoimmune condition where your body's immune system is producing factors that stimulate enlargement of the muscles that
FastTest. You ve read the book... ... now test yourself
 FastTest You ve read the book...... now test yourself To ensure you have learned the key points that will improve your patient care, read the authors questions below. The answers will refer you back to
FastTest You ve read the book...... now test yourself To ensure you have learned the key points that will improve your patient care, read the authors questions below. The answers will refer you back to
Acne breakouts vulgaris is one of the commonest skin conditions, which dermatologists treat and it
 Introduction Acne breakouts vulgaris is one of the commonest skin conditions, which dermatologists treat and it mostly impacts teens, though it might appear at any sort of age. Acne breakouts cause necessarily
Introduction Acne breakouts vulgaris is one of the commonest skin conditions, which dermatologists treat and it mostly impacts teens, though it might appear at any sort of age. Acne breakouts cause necessarily
Potulaca (Portulaca oleracea) detergent and other formulations that disrupt the active anthraquinones by regulating the Nitric
 detergent and other formulations that disrupt the active anthraquinones by regulating the Nitric") Natural effective support for acne, oily and inflamed skin care At the heart of Frutarom's TopicRange for oily and acne skin problems, we focus Z-Care - a botanical blend based on traditions of Chinese
Natural effective support for acne, oily and inflamed skin care At the heart of Frutarom's TopicRange for oily and acne skin problems, we focus Z-Care - a botanical blend based on traditions of Chinese
F REQUENTLY A SKED Q UESTIONS
 Acne ogist (a doctor who specializes in treating skin problems) about how you can help prevent acne and if treatment would help you. page 1 Q: What is acne? Q: What are the different types of A: Acne is
Acne ogist (a doctor who specializes in treating skin problems) about how you can help prevent acne and if treatment would help you. page 1 Q: What is acne? Q: What are the different types of A: Acne is
CHAPTER 6: INTEGUMENTARY SYSTEM. 1. Explain why the skin is called the cutaneous membrane.
 OBJECTIVES: 1. Explain why the skin is called the cutaneous membrane. 2. Name the layers of the skin, describe the structure (tissues) of each, and name a general function of each. 3. Discuss the four
OBJECTIVES: 1. Explain why the skin is called the cutaneous membrane. 2. Name the layers of the skin, describe the structure (tissues) of each, and name a general function of each. 3. Discuss the four
PSORIASIS. -Multi factorial. -Papulosquamous disorder. -Genetically determined (few) -Chronic Scaly lesions. -Seasonal variations
 -Chronic Scaly lesions. -Seasonal variations") PSORIASIS -Multi factorial -Papulosquamous disorder -Genetically determined (few) -Chronic Scaly lesions -Seasonal variations -Recurrences & remissions Etiology & Pathogenesis T-cell mediated autoimmune
PSORIASIS -Multi factorial -Papulosquamous disorder -Genetically determined (few) -Chronic Scaly lesions -Seasonal variations -Recurrences & remissions Etiology & Pathogenesis T-cell mediated autoimmune
Rheumatoid Arthritis. Nicole Klett,, M.D.
 Rheumatoid Arthritis Nicole Klett,, M.D. Rheumatoid Arthritis Systemic Chronic Inflammatory Primarily targets the synovium of diarthrodial joints Etiology likely combination genetic and environmental Diarthrodial
Rheumatoid Arthritis Nicole Klett,, M.D. Rheumatoid Arthritis Systemic Chronic Inflammatory Primarily targets the synovium of diarthrodial joints Etiology likely combination genetic and environmental Diarthrodial
History and Physical Examination for Rheumatic Disease for MUSC Students
 History and Physical Examination for Rheumatic Disease for MUSC Students Inflammatory vs. non-inflammatory arthritis Inflammatory Prolonged stiffness after rest Stiffness improved with use Warmth Prolonged
History and Physical Examination for Rheumatic Disease for MUSC Students Inflammatory vs. non-inflammatory arthritis Inflammatory Prolonged stiffness after rest Stiffness improved with use Warmth Prolonged
Thank you for downloading this free report!
 Thank you for downloading this free report! Feel free to share this report with other people! Marthine B. Green www.acnebuzz.com 2 Page The Truth About Acne There are so many misconceptions about what
Thank you for downloading this free report! Feel free to share this report with other people! Marthine B. Green www.acnebuzz.com 2 Page The Truth About Acne There are so many misconceptions about what
Welcome to the Hair and Nail Clinic 2008
 Welcome to the Hair and Nail Clinic 2008 The expectations for each resident rotating through the Hair & Nail Clinic are outlined below. HAIR AND NAIL CLINIC Goals and Objectives for First Year Residents
Welcome to the Hair and Nail Clinic 2008 The expectations for each resident rotating through the Hair & Nail Clinic are outlined below. HAIR AND NAIL CLINIC Goals and Objectives for First Year Residents
Thymus Cancer. This reference summary will help you better understand what thymus cancer is and what treatment options are available.
 Thymus Cancer Introduction Thymus cancer is a rare cancer. It starts in the small organ that lies in the upper chest under the breastbone. The thymus makes white blood cells that protect the body against
Thymus Cancer Introduction Thymus cancer is a rare cancer. It starts in the small organ that lies in the upper chest under the breastbone. The thymus makes white blood cells that protect the body against
Most skin diseases occur in people of
 treating skin of color NATIONALLY-RECOGNIZED DERMATOLOGIST CHARLES E CRUTCHFIELD III MD DISCUSSES SOME COMMON SKIN DISORDERS OBSERVED IN SKIN OF COLOR. Most skin diseases occur in people of all nationalities,
treating skin of color NATIONALLY-RECOGNIZED DERMATOLOGIST CHARLES E CRUTCHFIELD III MD DISCUSSES SOME COMMON SKIN DISORDERS OBSERVED IN SKIN OF COLOR. Most skin diseases occur in people of all nationalities,
1. ACNE 1. Lisa Schmidt, MPH, Eve A. Kerr, MD, and Kenneth Clark, MD
 1. ACNE 1 Lisa Schmidt, MPH, Eve A. Kerr, MD, and Kenneth Clark, MD The general approach to summarizing the key literature on acne was to review relevant sections of two medical text books (Vernon and
1. ACNE 1 Lisa Schmidt, MPH, Eve A. Kerr, MD, and Kenneth Clark, MD The general approach to summarizing the key literature on acne was to review relevant sections of two medical text books (Vernon and
Other Noninfectious Diseases. Chapter 31 Lesson 3
 Other Noninfectious Diseases Chapter 31 Lesson 3 Diabetes Diabetes- a chronic disease that affects the way body cells convert food into energy. Diabetes is the seventh leading cause of death by disease
Other Noninfectious Diseases Chapter 31 Lesson 3 Diabetes Diabetes- a chronic disease that affects the way body cells convert food into energy. Diabetes is the seventh leading cause of death by disease
LASER HAIR REMOVAL: SCIENTIFIC PRINCIPLES AND PRACTICAL ASPECTS
 LASER HAIR REMOVAL: SCIENTIFIC PRINCIPLES AND PRACTICAL ASPECTS ABSTRACT Christine C. Dierickx, M.D. Visiting Research Scientist Wellman Laboratories of Photomedicine Harvard Medical School The use of
LASER HAIR REMOVAL: SCIENTIFIC PRINCIPLES AND PRACTICAL ASPECTS ABSTRACT Christine C. Dierickx, M.D. Visiting Research Scientist Wellman Laboratories of Photomedicine Harvard Medical School The use of
Highlights on Clinical Picture of Psoriasis
 Highlights on Clinical Picture of Psoriasis PROF DR DOAA MAHGOUB CAIRO UNIVERSITY 1 Chronic Plaque Psoriasis Symmetric distribution of sharply defined, erythematous, scaly plaques. The scalp, elbows, knees
Highlights on Clinical Picture of Psoriasis PROF DR DOAA MAHGOUB CAIRO UNIVERSITY 1 Chronic Plaque Psoriasis Symmetric distribution of sharply defined, erythematous, scaly plaques. The scalp, elbows, knees
Notes on Hair Analysis
 Notes on Hair Analysis I have found local veterinarians very uncooperative when trying to get samples of dog and cat fur. I have found neighbors, friends and relatives a much better source of fur. There
Notes on Hair Analysis I have found local veterinarians very uncooperative when trying to get samples of dog and cat fur. I have found neighbors, friends and relatives a much better source of fur. There
Dermatology Dr. Faraidoon Lecture 1 Hair Disorders
 Dermatology Dr. Faraidoon Lecture 1 Hair Disorders Hair is a filamentous (threadlike) biomaterial, that grows from follicles found in the dermis. Is composed of protein, notably keratin. Hair is one of
Dermatology Dr. Faraidoon Lecture 1 Hair Disorders Hair is a filamentous (threadlike) biomaterial, that grows from follicles found in the dermis. Is composed of protein, notably keratin. Hair is one of
Common Breast Complaints:
 : Palpable mass Abnormal mammogram with normal physical exam Vague thickening or nodularity Nipple Discharge Breast pain Breast infection or inflammation The physician s goal is to determine whether the
: Palpable mass Abnormal mammogram with normal physical exam Vague thickening or nodularity Nipple Discharge Breast pain Breast infection or inflammation The physician s goal is to determine whether the
Management in the pre-hospital setting
 Management in the pre-hospital setting Inflammation of the joints Two main types: Osteoarthritis - cartilage loss from wear and tear Rheumatoid arthritis - autoimmune disorder Affects all age groups,
Management in the pre-hospital setting Inflammation of the joints Two main types: Osteoarthritis - cartilage loss from wear and tear Rheumatoid arthritis - autoimmune disorder Affects all age groups,
Common Skin Conditions in Children. Liz Moore and Emma King Dermatology Nurse Consultants
 Common Skin Conditions in Children Liz Moore and Emma King Dermatology Nurse Consultants Diagnosis? Nummular Dermatitis Disc pattern rash (discoid eczema) Clearly demarcated edges Occurs at any age Can
Common Skin Conditions in Children Liz Moore and Emma King Dermatology Nurse Consultants Diagnosis? Nummular Dermatitis Disc pattern rash (discoid eczema) Clearly demarcated edges Occurs at any age Can
Countless medications, nutrients, herbs, and chemicals have
 9Drugs That Grow Hair Countless medications, nutrients, herbs, and chemicals have been claimed to stop or reverse hair loss, however when tested scientifically in well controlled, double-blind clinical
9Drugs That Grow Hair Countless medications, nutrients, herbs, and chemicals have been claimed to stop or reverse hair loss, however when tested scientifically in well controlled, double-blind clinical
COSMETIC LASER AND AESTHETICS CENTER
 COSMETC LASER AND AESTHETCS CENTER LGHT SHEAR LASER HAR REMOVAL NFORMATON AND CONSENT understand that the purpose of this procedure is to reduce and/or remove unwanted hair. There are several alternatives
COSMETC LASER AND AESTHETCS CENTER LGHT SHEAR LASER HAR REMOVAL NFORMATON AND CONSENT understand that the purpose of this procedure is to reduce and/or remove unwanted hair. There are several alternatives
ELECTROLYSIS- INFORMATION AND FAQ s
 ELECTROLYSIS- INFORMATION AND FAQ s 1. How does Electrolysis work? A very fine sterilized filament is inserted into the hair follicle, which is a natural opening in the skin. The skin is not pierced or
ELECTROLYSIS- INFORMATION AND FAQ s 1. How does Electrolysis work? A very fine sterilized filament is inserted into the hair follicle, which is a natural opening in the skin. The skin is not pierced or
Systemic Lupus Erythematosus
 Harvard-MIT Division of Health Sciences and Technology HST.021: Musculoskeletal Pathophysiology, IAP 2006 Course Director: Dr. Dwight R. Robinson Systemic Lupus Erythematosus A multi-system autoimmune
Harvard-MIT Division of Health Sciences and Technology HST.021: Musculoskeletal Pathophysiology, IAP 2006 Course Director: Dr. Dwight R. Robinson Systemic Lupus Erythematosus A multi-system autoimmune
Acne Vulgaris: Pathophysiology, diagnosis, and treatment of a common dermatologic condition
 Acne Vulgaris: Pathophysiology, diagnosis, and treatment of a common dermatologic condition Dr. Mohamed Emam Lecturer in Clinical Pharmacy Department Faculty of Pharmacy Beni Suef University Hair Pilosebaceous
Acne Vulgaris: Pathophysiology, diagnosis, and treatment of a common dermatologic condition Dr. Mohamed Emam Lecturer in Clinical Pharmacy Department Faculty of Pharmacy Beni Suef University Hair Pilosebaceous
Juvenile Dermatomyositis Joseph Junewick, MD FACR
 Juvenile Dermatomyositis Joseph Junewick, MD FACR 10/11/2015 History Child with several month history of weakness, arthralgias and palpable abnormalities at the knee Diagnosis Juvenile Dermatomyositis
Juvenile Dermatomyositis Joseph Junewick, MD FACR 10/11/2015 History Child with several month history of weakness, arthralgias and palpable abnormalities at the knee Diagnosis Juvenile Dermatomyositis
Acne and Rosacea handout version. Dr Elizabeth Ogden Associate Specialist in Dermatology 25.4.13
 Acne and Rosacea handout version Dr Elizabeth Ogden Associate Specialist in Dermatology 25.4.13 Acne Acne is the most common skin disease Affecting all races and ages Acne is most common in teenagers and
Acne and Rosacea handout version Dr Elizabeth Ogden Associate Specialist in Dermatology 25.4.13 Acne Acne is the most common skin disease Affecting all races and ages Acne is most common in teenagers and
Lupus in Children and Teenagers. Arielle Hay, MD Pediatric Rheumatologist Nicklaus Children s Hospital
 Lupus in Children and Teenagers Arielle Hay, MD Pediatric Rheumatologist Nicklaus Children s Hospital Systemic Lupus Erythematosus (SLE) Chronic Illness What is lupus? Autoimmune Multisystem Antinuclear
Lupus in Children and Teenagers Arielle Hay, MD Pediatric Rheumatologist Nicklaus Children s Hospital Systemic Lupus Erythematosus (SLE) Chronic Illness What is lupus? Autoimmune Multisystem Antinuclear
 BISPHOSPHONATE RELATED OSTEONECROSIS OF THE JAW (BRONJ) BISPHOSPHONATES AND WHAT HAPPENS TO BONE VINCENT E. DIFABIO, DDS, MS MEMBER OF THE COMMITTEE ON HEALTHCARE AND ADVOCACY FROM THE AMERICAN ASSOCIATION
BISPHOSPHONATE RELATED OSTEONECROSIS OF THE JAW (BRONJ) BISPHOSPHONATES AND WHAT HAPPENS TO BONE VINCENT E. DIFABIO, DDS, MS MEMBER OF THE COMMITTEE ON HEALTHCARE AND ADVOCACY FROM THE AMERICAN ASSOCIATION
EL CAMINO MEDICAL CLINIC
 EL CAMINO MEDICAL CLINIC 1828 El Camino Real, Suite 706 Burlingame, CA 940101 Phone #: (650)777-9117 Acne Acne is a disorder resulting from the action of hormones and other substances on the skin's oil
EL CAMINO MEDICAL CLINIC 1828 El Camino Real, Suite 706 Burlingame, CA 940101 Phone #: (650)777-9117 Acne Acne is a disorder resulting from the action of hormones and other substances on the skin's oil
9/25/2012. Composed of three layers. Glands. Basic skin care Acne How to recognize How to treat. I have no conflict of interest
 By Theresa M. Schimmels, PA-C WAPA Fall CME 2012 Basic skin care Acne How to recognize How to treat I have no conflict of interest Composed of three layers epidermis dermis hypodermis or subcutaneous Glands
By Theresa M. Schimmels, PA-C WAPA Fall CME 2012 Basic skin care Acne How to recognize How to treat I have no conflict of interest Composed of three layers epidermis dermis hypodermis or subcutaneous Glands
Canine Lymphoma Frequently Asked Questions by Pet Owners
 Canine Lymphoma Frequently Asked Questions by Pet Owners What is lymphoma? The term lymphoma describes a diverse group of cancers in dogs that are derived from white blood cells called lymphocytes. Lymphocytes
Canine Lymphoma Frequently Asked Questions by Pet Owners What is lymphoma? The term lymphoma describes a diverse group of cancers in dogs that are derived from white blood cells called lymphocytes. Lymphocytes
page 1 HAIR LOSS TREATMENT: EFFICACY STUDY (6 months)
") page 1 HAIR LOSS TREATMENT: EFFICACY STUDY (6 months) page 2 HAIR LOSS TREATMENT: EFFICACY STUDY (6 months) Report nº: 07301-4 Study Managers: Auxiliary Staff: Client: Encarnación Gómez María Teresa Alcalde
page 1 HAIR LOSS TREATMENT: EFFICACY STUDY (6 months) page 2 HAIR LOSS TREATMENT: EFFICACY STUDY (6 months) Report nº: 07301-4 Study Managers: Auxiliary Staff: Client: Encarnación Gómez María Teresa Alcalde
COMMON BACTERIAL SKIN INFECTIONS IN GENERAL PRACTICE
 COMMON BACTERIAL SKIN INFECTIONS IN GENERAL PRACTICE The two most common bacteria to cause skin infections are staphylococcus aureus (staph aureus ) and streptococcus pyogenes ( strep) (see Table 1). Staphylococcus
COMMON BACTERIAL SKIN INFECTIONS IN GENERAL PRACTICE The two most common bacteria to cause skin infections are staphylococcus aureus (staph aureus ) and streptococcus pyogenes ( strep) (see Table 1). Staphylococcus
THYROID CANCER. I. Introduction
 THYROID CANCER I. Introduction There are over 11,000 new cases of thyroid cancer each year in the US. Females are more likely to have thyroid cancer than men by a ratio of 3:1, and it is more common in
THYROID CANCER I. Introduction There are over 11,000 new cases of thyroid cancer each year in the US. Females are more likely to have thyroid cancer than men by a ratio of 3:1, and it is more common in
LYMPHOMA. BACHIR ALOBEID, M.D. HEMATOPATHOLOGY DIVISION PATHOLOGY DEPARTMENT Columbia University/ College of Physicians & Surgeons
 LYMPHOMA BACHIR ALOBEID, M.D. HEMATOPATHOLOGY DIVISION PATHOLOGY DEPARTMENT Columbia University/ College of Physicians & Surgeons Normal development of lymphocytes Lymphocyte proliferation and differentiation:
LYMPHOMA BACHIR ALOBEID, M.D. HEMATOPATHOLOGY DIVISION PATHOLOGY DEPARTMENT Columbia University/ College of Physicians & Surgeons Normal development of lymphocytes Lymphocyte proliferation and differentiation:
COST-EFFECTIVE TREATMENT OF ACNE, ATOPIC DERMATITIS AND MOLLUSCUM. Jan Yusk, M.D.
 COST-EFFECTIVE TREATMENT OF ACNE, ATOPIC DERMATITIS AND MOLLUSCUM Jan Yusk, M.D. Conflicts of Interest I have no conflicts of interest to disclose. ACNE Pathogenesis Epidermis Dermis Hair Follicle Hair
COST-EFFECTIVE TREATMENT OF ACNE, ATOPIC DERMATITIS AND MOLLUSCUM Jan Yusk, M.D. Conflicts of Interest I have no conflicts of interest to disclose. ACNE Pathogenesis Epidermis Dermis Hair Follicle Hair
STATE OF THE ART SURGICAL TECHNIQUE: FOLLICULAR UNIT HAIR GRAFTING
 STATE OF THE ART SURGICAL TECHNIQUE: FOLLICULAR UNIT HAIR GRAFTING Author: Jeffrey S. Epstein, M.D., F.A.C.S. Clinical Professor, University of Miami Private Practice, Miami, FL 305.666.1774 305.666.6708
STATE OF THE ART SURGICAL TECHNIQUE: FOLLICULAR UNIT HAIR GRAFTING Author: Jeffrey S. Epstein, M.D., F.A.C.S. Clinical Professor, University of Miami Private Practice, Miami, FL 305.666.1774 305.666.6708
Psoriasis Can be Cured with Homoeopathy
 Homoeopathy Clinic http://www.homoeopathyclinic.com Psoriasis Can be Cured with Homoeopathy Case Report / General Information What you should Know about Psoriasis? It is not a contagious disease. Psoriasis
Homoeopathy Clinic http://www.homoeopathyclinic.com Psoriasis Can be Cured with Homoeopathy Case Report / General Information What you should Know about Psoriasis? It is not a contagious disease. Psoriasis
Malignant Lymphomas and Plasma Cell Myeloma
 Malignant Lymphomas and Plasma Cell Myeloma Dr. Bruce F. Burns Dept. of Pathology and Lab Medicine Overview definitions - lymphoma lymphoproliferative disorder plasma cell myeloma pathogenesis - translocations
Malignant Lymphomas and Plasma Cell Myeloma Dr. Bruce F. Burns Dept. of Pathology and Lab Medicine Overview definitions - lymphoma lymphoproliferative disorder plasma cell myeloma pathogenesis - translocations
A Free Guide to different Hair Removal Treatments
 A Free Guide to different Hair Removal Treatments 2 Introduction From peach-fuzz to long, dark, or coarse growth, both men and women have been doing battle with excess hair -and hair removal - for centuries.
A Free Guide to different Hair Removal Treatments 2 Introduction From peach-fuzz to long, dark, or coarse growth, both men and women have been doing battle with excess hair -and hair removal - for centuries.
Aggressive lymphomas. Michael Crump Princess Margaret Hospital
 Aggressive lymphomas Michael Crump Princess Margaret Hospital What are the aggressive lymphomas? Diffuse large B cell Mediastinal large B cell Anaplastic large cell Burkitt lymphoma (transformed lymphoma:
Aggressive lymphomas Michael Crump Princess Margaret Hospital What are the aggressive lymphomas? Diffuse large B cell Mediastinal large B cell Anaplastic large cell Burkitt lymphoma (transformed lymphoma: