Kim-Thi Van-Dinh D.D.S.
|
|
|
- Pauline Arnold
- 8 years ago
- Views:
Transcription
1 Kim-Thi Van-Dinh D.D.S. EDUCATION University of Maryland School of Dentistry Baltimore, MD Candidate: Periodontics Certificate, Master of Science in Biomedical Sciences Graduation Date: June Present New York University College of Dentistry New York, NY Doctor of Dental Surgery Honors in Implant Dentistry Omicron Kappa Upsilon Member University of California Berkeley, CA Bachelor of Science in Bioengineering Areas of Concentration: Tissue Engineering and Biomechanics Graduated with Honors EXPERIENCE New York University Faculty Practice, New York, NY Senior selective residency at the Student Health Center; Comprehensive patient care. Implant Study Club NYU Department of Periodontics, New York, NY Attended lecture series on the biological considerations of the periodontium in regards to implant and restorative dentistry led by Dr. Dennis Tarnow Editor and Transcriber NYU Class Transcription Services, New York, NY Coordinated transcription services and payment of transcribers; Taped and edited lectures; Transcribed selected lectures. Dean s Summer Research Fellow NYU Department of Basic Science and Craniofacial Biology, New York, NY Studied the effect of the junction of premalignant and normal oral epithelial cells on the actin cytoskeleton; Presented at NYU s annual research day

2 ORGANIZATIONS AND ACTIVITIES Treasurer Curriculum Representative Secretary NYU College of Dentistry Class Council, New York, NY Editor-in-Chief NYU College of Dentistry Yearbook Committee, New York, NY HONORS AND AWARDS Omicron Kappa Upsilon Dental Honors Society New York University Dean s Research Award University of California Scholar Advanced Placement Scholar with Honors Bank of America Award for Excellence in Science and Mathematics Society of Women Engineers Certificate of Merit LICENSURE AND BOARD CERTIFICATION Northeast Regional Board Certification Invisalign, BLS, and ACLS Certifications MEMBERSHIPS IN PROFESSIONAL SOCIETIES American Dental Association Academy of Osseointegration American Academy of Periodontology Gerald Bowers Periodontal Study Club Maryland State Dental Association Omicron Kappa Upsilon

3 ABSTRACT: Maxillary Sinus Morphology: A Radiographic Retrospective Evaluation of Sinus Septa in Caucasian and African-American Subjects Kim-Thi Van-Dinh DDS, Masters of Science, 2012 Dissertation Directed by: Dr. Mark A. Reynolds DDS, PhD, Director and Chair of Postgraduate Periodontics Anatomic variations of maxillary sinus morphology including volume and septa impact the success of sinus augmentation procedures for dental implant placement. Anatomy has been investigated mainly with respect to age and gender; however, the effect of race has not been examined. The purpose of this study was to evaluate variations of maxillary septa sinus anatomy of African-American and Caucasian subjects, given differences significantly impact treatment success. This retrospective study examined consecutive computerized tomographic scans (CT) of patients scheduled for maxillary implant surgery at the University of Maryland School of Dentistry between 2009 to A total of 259 CT scans of 139 African-American and 120 Caucasian subjects were evaluated, of which, 62.5% of subjects (162/259) had identifiable septa. A total of 343 septa were identified in 518 sinuses (66.2%). Caucasians had more septa than African-Americans (1.56 compared to 1.09, p=0.006). The effect of gender was approaching significance (p=0.07). The adjusted mean number of sinus septa in female subjects was 1.48 compared to 1.17 in males. Sinuses were divided into three sections: anterior (premolars), middle (first and second molars), and posterior (third molar). In both the anterior and middle sections, race had a significant effect (p=0.033 and p=0.035). In the anterior, the adjusted mean number of septa for Caucasians was nearly

4 twice that of African-Americans (0.32 compared to 0.17). In the middle section, the adjusted mean for African-Americans was 0.57 compared to With respect to the posterior section, only gender had a significant effect (p=0.008). Women had an adjusted average of 0.51 septa compared to men with a 0.29 average. The majority of septa were found in the middle segment (51.3%, 176/343), and 17.5% (60/343) were identified in the anterior segment. Sinus septa complicate Schneiderian membrane elevation therefore increasing likelihood of membrane perforation, a common complication of sinus augmentation procedures. The dentally relevant sinus segments contain the majority of sinus septa (68.8%) and have a direct impact on clinicians performing sinus augmentation procedures. Both race and gender impact maxillary implant treatment planning with a greater frequency of detectable septa in Caucasians and females when compared to African-American males.

5 Maxillary Sinus Morphology: A Radiographic Retrospective Evaluation of Sinus Septa in Caucasian and African-American Subjects by Kim-Thi Van-Dinh Thesis submitted to the Faculty of the Graduate School of the University of Maryland, Baltimore in partial fulfillment of the requirements for the degree of Master of Science 2012

6 Copyright 2012 by Kim-Thi Van-Dinh All rights Reserved

7 ACKNOWLEDGEMENTS: This dissertation would not have been possible without the guidance and the help of Dr. Mark A. Reynolds and Dr. Mary-Beth Aichelmann-Reidy who contributed and extended their valuable assistance in the preparation and completion of this study. I would also like to thank my co-residents for their encouragement over the last three years. Lastly, I would like to thank my family and husband for all their love, support, and patience in dealing with my neuroticism. iii

8 TABLE OF CONTENTS: Chapter Acknowledgements. List of Tables.. List of Figures. I. INTRODUCTION... Page iii v vi 1 II. MATERIALS AND METHODS III. RESULTS. 18 IV. DISCUSSION V. CONCLUSION BIBLIOGRAPHY iv

9 LIST OF TABLES: Page Table 1. Summary of Septa Prevalence, Location, and Percentage of False Diagnosis according to Different Specimen Analysis Table 2. Number of Subjects included in the Investigation Table 3. Total Number of Septa Categorized by Race and Location 19 Table 4. Parameter Estimates for Number of Septa.. 19 Table 5. Adjusted Means Table for Race Table 6. Adjusted Means Table for Gender Table 7. Parameter Estimates for Septa Height Table 8. Parameter Estimates for Number of Septa in the Anterior Segment Table 9. Adjusted Means Table for Race in the Anterior Segment Table 10. Parameter Estimates for Number of Septa in the Middle Segment Table 11. Adjusted Means Table for Race in the Middle Segment Table 12. Parameter Estimates for Number of Septa in the Posterior Segment 21 Table 13. Adjusted Means Table for Gender in the Posterior Segment v

10 LIST OF FIGURES: Page Figure 1. Panoramic Reconstruction from a CT Scan... 4 Figure 2. Axial and Panoramic Views Figure 3. Sagittal, Axial, and Panoramic Views of a CT Scan.. 17 vi

11 I. INTRODUCTION: Maxillary molar teeth have some of the highest incidences of supporting bone loss and attrition due to anatomy and position in the arch. After loss of these molars, bone resorption results in decreased vertical and horizontal alveolar ridge dimension; progressive pneumatization of the sinuses also contributes to decreased ridge height. Sinus augmentation procedures have been widely utilized to restore patients with fixed prostheses by supplementing the alveolar ridge and allowing for dental implant placement even in the most severe cases of resorption. However, the presence of anatomic variations, such as septa, have been reported to increase the risk of membrane perforation during sinus floor augmentation procedures [1]. Also of concern is vascular damage, specifically to the posterior superior alveolar artery, upon accessing the sinus cavity through its lateral wall [2] as the maxillary blood supply is essential for preserving the vitality of the affected maxillary region, integration of the grafting material, and wound healing following sinus floor elevation [3]. In order to achieve a successful sinus augmentation for subsequent implant placement in patients, it is critical to appreciate any anatomical and morphological variation of the maxillary sinus between racial groups. The maxillary sinuses were first discovered and illustrated by Leonardo Da Vinci in 1489; however, British surgeon Nathaniel Highmore was the first to describe the air cavity of the maxilla. Subsequently it is often referred to as the antrum of Highmore [4]. The maxillary sinus is the largest of the paranasal sinuses and the first to develop. During the 12 th week of embryogenesis, it begins as an invagination of the ethmoid infundibulum in the middle meatus of the nasal cavity. At birth it expands by pneumatization into the developing alveolar process. Its growth rate parallels that of the 1

12 maxilla and the developing dentition [5]. Antrum height development depends on an equilibrium of forces; the pressure exerted by the eye on the thin orbital floor, the pull of muscles that attach to or originate from the maxilla, and the eruption of teeth all have an effect on the resulting size of the maxillary sinus [6]. Its size is insignificant until the eruption of the permanent teeth. As teeth erupt into the oral cavity, the sinus becomes pneumatized and drops down into the space once occupied by tooth buds. Typically expansion of the sinus halts once all the permanent teeth have erupted; however, the removal of maxillary posterior teeth can cause further pneumatization of the sinus. At twelve years of age, the floor of the sinus typically corresponds to the floor of the nasal cavity. In adults, the roots of maxillary posterior teeth may protrude into the sinus cavity [6]. The maxillary sinus is pyramidal in shape with its base at the nasal wall and the apex extending into the zygomatic arch. It is bordered medially by the nasal cavity, superiorly by the orbital floor, and laterally by the maxilla, alveolar process, and zygomatic arch. Blood supply is from the anterior, middle, and posterior superior alveolar arteries and to a lesser extent the greater palatine arteries, branches of the maxillary artery. Venous blood drainage is through the pterygoid plexus. It is innervated by the anterior, middle, and posterior superior alveolar nerves, branches of maxillary division of the Trigeminal cranial nerve (CN V). The antrum is an air filled cavity lined by respiratory epithelium known as the Schneiderian membrane. It is continuous with nasal epithelium through the semilunar hiatus in the middle meatus of the nasal cavity. Mucous is secreted by the epithelium and any foreign material present in the sinus is moved out by the beating of cilia. The function of the maxillary sinus is not clearly 2
![eruption of teeth all have an effect on the resulting size of the maxillary sinus [6]. Its size is insignificant until the eruption of the permanent teeth.](/docs-images/50/15342010/images/page_12.jpg "As teeth erupt into the oral cavity, the sinus becomes pneumatized and drops down into the space once occupied by tooth buds.")
13 defined. Many theories have been debated including decreasing the weight of the skull, protection against blows to the midface, phonetic resonance, warming and humidifying inspired air, and immunologic defense [4]. The floor of the sinus can contains one or more septa. Sinus septa were first described by Underwood in 1910; they are often referred to as Underwood s septa. He found that the sinus was frequently divided into 3 compartments that are often bordered by ridges corresponding to different periods of development of the dentition. The development of the anterior compartment occurs at the site of premolar eruption between 8 months and 2 years of age. The middle area corresponds to the location of the first and second permanent molars and growth occurs from 5 to 10 years of age. The posterior compartment develops during years of age and contains the third molar region. Sinus septa form between adjacent teeth because as the tooth develops and the roots form, the sinus cavity expands and the antral floor follows becoming more concave [7]. This type of septa development is now referred to as primary or congenital; it occurs during growth of the midface. Secondary septa development was first described by Vinter. They are typically incomplete septa resulting from tooth loss and caused by irregular atrophy of the alveolar process and pneumatization of the sinus leaving bony crests. The sinus floor anterior and posterior to a septum is often at different levels. Since premolar teeth are typically retained longer than molar teeth, septa formation could be promoted by different phases of maxillary sinus pneumatization [8]. Earlier loss of molars results in further expansion of the sinus and the floor reaches a deeper level than in the premolar region where loss usually occurs later as seen in Figure 1. A septum can remain between the two zones of regression. Septa function to reinforce the floor of the 3
![defense [4]. The floor of the sinus can contains one or more septa. Sinus septa were first described by Underwood in 1910; they are often referred to as Underwood s septa.](/docs-images/50/15342010/images/page_13.jpg "He found that the sinus was frequently divided into 3 compartments that are often bordered by ridges corresponding to different periods of development of the dentition.")
14 sinus and develop as a result of stress transfer within the bone [4]. They seem to slowly resorb when teeth are lost due to decreased forces on the maxilla [9]. Figure 1: Panoramic Reconstruction from a CT Scan. Reveals pathology in the left sinus and pneumatization of the antrum after the extraction of the maxillary left first molar. Compare the difference in the sinus floor between the left and right sinus. On the opposite side, the patient still has all the molars and the sinus floor is more or less at the same level. Although variations in septa prevalence have not been thoroughly examined in literature, skeletal differences between racial groups have been well documented. African-Americans have larger teeth but exhibit less crowding than Caucasians. Burris attributed this to the fact that African-American maxillas are larger in both size and shape. Arch perimeter was 8% greater and the cross-sectional area of the arch was 19% greater in African-Americans compared to Caucasians [10]. Differences in bone density between the two races have also been widely documented. After adjusting for body mass, Pollitzer et al. found that blacks have greater skeletal calcium content and total 4

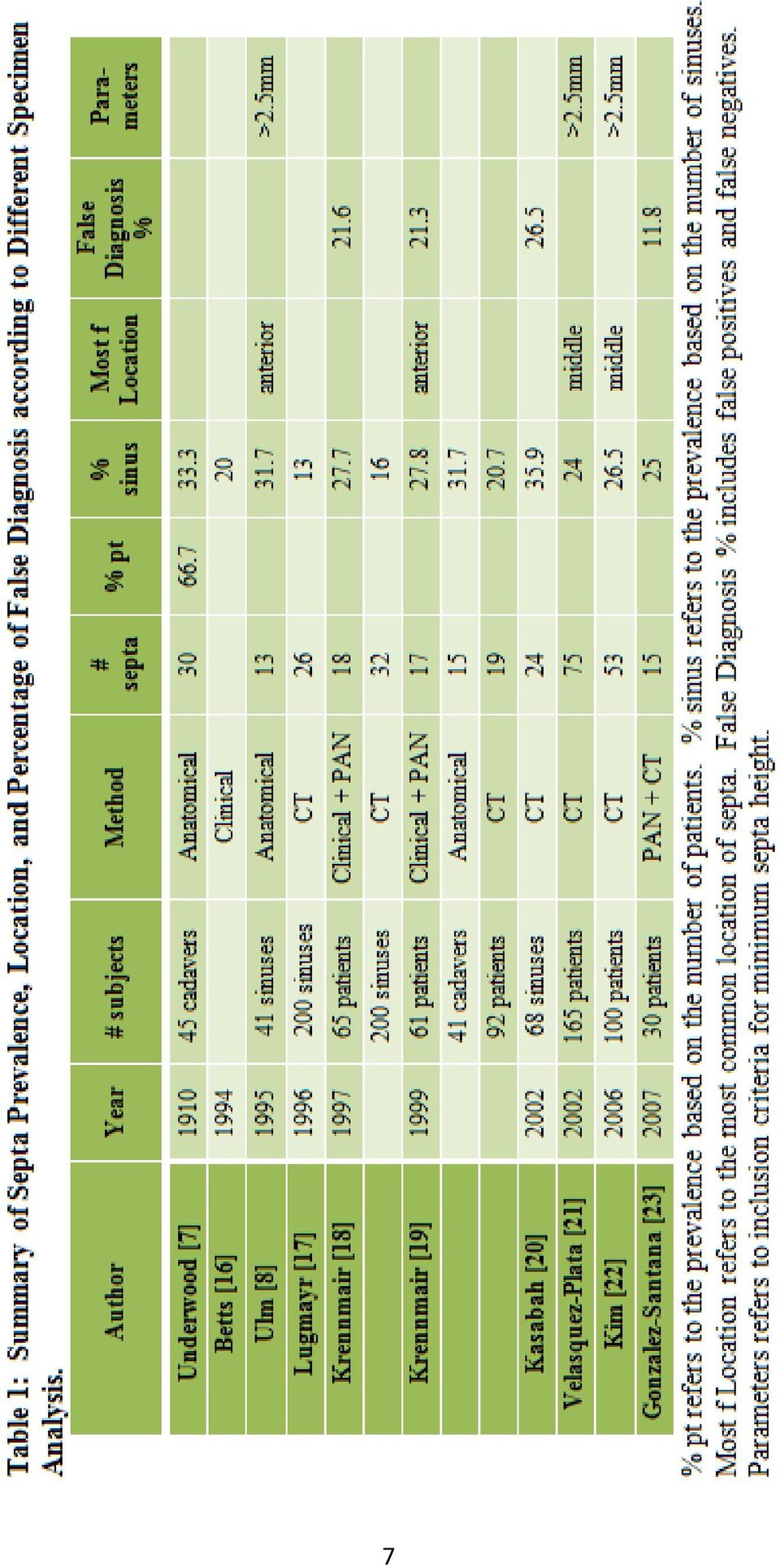
15 body potassium. He attributed differences in body mass to be related to ethnicity [11]. Ettinger examined whether racial differences could be due to differences in bone metabolism and lifestyle and found that differences in bone mineral density could not be accounted for by clinical or biochemical variables. Adjusted bone density measurements were % higher for black than white men and were % higher for black then for white women [12]. Though these other skeletal differences have been demonstrated, differences in maxillary sinus morphology and anatomy between African-Americans and Caucasians of European decent have remained largely underreported in the literature. In previous studies, anatomy and morphology of the maxillary sinus have been investigated, mainly with respect to age and gender, with the purpose of elucidating potential complications during augmentation and implant surgery. Anatomic variations including septa and size of the maxillary sinus have an effect on the success of sinus augmentation procedures. In Underwood s classic paper, he examined 45 dry skulls of European descent and found that 33.3% contained septa (30 septa found in 45 paired sinuses). A smaller number of maxillary sinuses in skulls originating from the Congo were evaluated and 3.8% of them contained septa (2 septa found in 26 paired sinuses). In a review by Maestre-Ferrin et al. 2010, the frequency of septa varied between 13 to 35% in all populations studied [13]. The prevalence of sinus septa reported has been as high as 69% in a study by van Zyl [14]. Table 1 summarizes a review of the literature with regards to septa prevalence using different methodology. Panoramic imaging has been used in the past to identify the presence of septa; however reported false diagnosis percentages range from %. Summarizing studies that use CT imaging for identification, % of sinuses contain septa. The majority of studies evaluate 5
![biochemical variables. Adjusted bone density measurements were 4.5-16.1% higher for black than white men and were 1.2-7.3% higher for black then for white women [12].](/docs-images/50/15342010/images/page_15.jpg "Though these other skeletal differences have been demonstrated, differences in maxillary sinus morphology and anatomy between African-Americans and Caucasians of European decent have remained largely")
16 prevalence in subjects of Caucasian descent; there have been no reported studies on the differences between African-Americans and Caucasians. In addition to evaluations of sinus septa, sinus volume has also been investigated. Fernandes examined computed tomography scans of dried skulls of Zulu and European descent and found that European crania had significantly larger antral volumes than Zulu crania [15]. There is an inherent difference in the morphology of the maxillary sinus in African-Americans and Caucasians. 6


17 7

18 8

19 In addition to variations in the maxillary sinus as a result of racial differences, pathologic changes of the maxillary alveolus can occur as due to tooth loss, infection, trauma, and tumors or cysts. Following a posterior extraction in the maxilla, atrophy related changes cause the buccal plate to resorb more than the palatal bone. The amount of tissue resorption is greatest in the edentulous molar region compared to incisor and premolar regions [16]. Pneumatization of the maxillary sinus has been previously described as part of normal development; however, it can also be considered a pathological process when occurring after extractions. Once a maxillary posterior tooth is removed, the sinus expands occupying the space where the roots used to be. Resorption occurs both vertically and horizontally leading to inadequate bone height and width for the future placement of an endosseous dental implant [17]. Bone loss following extractions is attributed to osteoclastic activity of the sinus membrane and the loss of marginal bone. Changes due to chronic sinus infections include thickening of the Schneiderian membrane, a decrease in antral volume, and an increase in the bone thickness of the lateral wall [18]. Trauma related changes include those that occur as a result of midface fractures and unsuccessful extractions where the tooth is lodged in the sinus cavity. Rapidly growing tumors or cysts in the sinus cavity can expand beyond the bony confines of the sinus and invade adjacent structures like the orbit, nose, cheek, infratemporal fossa, and mouth [19]. Sinus morphology can be different within the same individual due to pathologic changes and depend on the resorption of the sinus floor due to premature tooth loss. 9
![The amount of tissue resorption is greatest in the edentulous molar region compared to incisor and premolar regions [16].](/docs-images/50/15342010/images/page_19.jpg "Pneumatization of the maxillary sinus has been previously described as part of normal development; however, it can also be considered a pathological process when occurring after extractions.")
20 Restoring teeth lost in the posterior maxilla is challenging because of lack of bone volume and poorer bone quality. Numerous techniques for increasing the height of the maxillary posterior bone for the placement of dental implants have been described. Sinus augmentation, ridge onlay grafting procedures, distraction osteogenesis, and extrusion of teeth have been utilized to rebuild bone loss following extractions or due to periodontal disease. Although ridge onlay grafting can increase the maxillary bone height, there is also a decrease in the interarch distance. This procedure cannot be utilized in some patients. In those instances, gain in bone height from the apical aspect of the atrophic alveolar ridge would be ideal. Boyne and James first described the Caldwell-Luc sinus augmentation procedure in A window was created in the anterior wall to access the maxillary sinus floor. Graft material and autogenous marrow were utilized, and the ultimate goal was the placement of a blade type of implant [20]. Summers described another method of augmenting the maxillary bone height through a crestal approach with the use of osteotomes and bone [21]. This technique requires at least 5-6mm of remaining bone at the crest of the alveolus. Minimal drilling is needed and osteotomes are used to gradually widen the osteotomy. The objective is to conserve bone in the site and to selectively displace it upwards into the sinus. Often bone is added prior to infracturing the sinus floor with the osteotome. This method is believed to be less invasive than the traditional Caldwell-Luc approach since instruments never touch the membrane itself. Pressure is used to elevate the Schneiderian membrane. The resulting site will have increased bone density and height. Contraindications for this procedure include sinuses with an angled floor or septa. These situations make it more difficult to infracture the sinus floor because the osteotomes tend to be deflected from the 10

21 desired direction. Regardless of the technique, maxillary sinus augmentation is a very predictable procedure. Various techniques have been described involving modifications in the lateral window, and various bone grafting materials have been utilized. The 1996 Consensus Conference on Maxillary Sinus Bone Grafting concluded that allografts, alloplasts, and xenografts, alone or in combination with autogenous bone, can be effective as bone substitute graft materials for sinus bone augmentation. They found a 90% success rate for implants placed in grafted sinuses and in function at least 3 years [22]. There are numerous approaches to maxillary sinus augmentation which require knowledge of sinus anatomy and variations to avoid any possible complications. The most common complications include perforation of the Schneiderian membrane, infection, and bleeding problems. Perforations during sinus augmentation procedures have been reported to be as high as 60% (45/75) [23]. Sinus septa have been reported to cause complications in elevating the membrane [20], but there are also studies that show the opposite. In a 2003 study, Kashabah and colleagues found that there was no relationship observed between the perforation and the presence of sinus septa. In all of the 118 subjects studied, no sinusitis or infections of the graft material were found despite perforations in 56% of the cases [24]. Contrastingly, Schwartz-Arad and colleagues found that 10% of sinus augmentation procedures had post operative complications including cyst formation and infection. They concluded that although membrane perforations correlated strongly with post operative complications, no associations were found between perforations and implant survival [25]. Typically if the perforation is small, a repair procedure can be performed. Fibrin and resorbable membranes have been 11
22 utilized. If the perforation is large, block grafts have been considered in the past [9]. However in most cases with large perforations, the procedure is aborted and re-entered at a later date [6]. In addition to perforations, post operative infections can occur. The occurrence of post operative sinusitis is not related to membrane perforations but limited to patients with a history of preoperative sinusitis [26]. In is imperative to inform these patients of the increased risks; these patients require close follow up. Absolute contraindications for sinus augmentation procedures include maxillary sinus infection, severe chronic sinusitis, and tumors or pathologic growths in the sinus [27]. Relative contraindications include sinus floor convolutions, sinus septa, transient mucosa swelling, and narrow sinuses [9]. Bleeding problems during surgical procedures is another complication that can be avoided by identifying intraosseous vasculature in the lateral wall in CT scans. Large diameter vessels can be ligated to avoid intra and post operative complications [28]. Although sinus perforations are common, infections and other post operative complications are rare and can be avoided with careful surgical planning, ideal imaging, and detailed knowledge of sinus morphology. The success of a sinus augmentation procedure is not solely dependent on avoiding post operative complications; success is related to consolidation of graft materials and osteointegration of implants. Since graft consolidation relies on adequate angiogenesis and migration of osteogenic cells from native bone, the remaining height of the alveolar ridge and buccopalatal dimension may have an effect on the therapeutic outcomes. Avila-Ortiz studied the relationship between the remaining alveolar bone height and the proportion of vital bone formation. Twenty-one sinuses were grafted with allograft material and core biopsies were taken at the time of implant surgery. They 12
23 found no significant correlation between residual bone height and percentage of vital bone formation [29]. Avila also evaluated the relationship between the distance from the lateral to medial wall of the maxillary sinus and percentage of vital bone formation. Twenty-five subjects were treated and core biopsies were taken at the time of implant placement. A strong negative correlation was found; the percentage of vital bone formation after sinus augmentation procedures with allograft is inversely proportional to the buccal-palatal dimension of the sinus [30]. Although septa create difficulties in elevating the membrane, they can serve as an additional source of blood supply. Rough surfaced implants have a higher success rate than machined surfaced implants in grafted sinuses. Implants placed in particulate grafts had a higher survival rate than those placed in sinuses augmented with block grafts. Grafting entirely with autogenous bone or including autogenous bone as part of a composite graft did not affect implant survival. The survival rate of implants placed in sinuses augmented through the lateral window technique ranged from %, with an average of 91.8% [31]. Reported success rates are similar or better for implants in grafted sites compared to non-grafted maxillary bone [22]. Sinus augmentation procedures have frequently been utilized to restore patients with fixed prosthesis even in cases of severe resorption. The presence of anatomic variations, such has septa, have been reported to increase the risk of membrane perforation during sinus floor augmentation procedures. Differences in the morphology of the maxillary sinus between African-Americans and Caucasians of European decent have remained largely underreported in the literature; the purpose of the study is to evaluate the variations in anatomy of the maxillary sinus between African-American and 13
24 Caucasian patients, given that differences sinus morphology can significantly impact treatment planning as well as treatment outcome. 14
25 II. MATERIALS AND METHODS: This retrospective study examined CT scans obtained on patients presenting for maxillary implant surgery at the University of Maryland School of Dentistry from 2009 to Records were reviewed based on treatment codes for maxillary computerized tomographic scans (D0310.0) and a total of 259 scans were identified on 139 African- American and 120 Caucasian patients. Since there were more female patients imaged than male patients, consecutively imaged patients were screened until a total number of 54 males of each race were identified. Subjects had undergone maxillary CT imaging prior to implant placement to replace lost or missing teeth due to caries or periodontal disease. Charts were accessed and reviewed to determine the race, age, and sex of the subject and to verify the presence of a pre-operative CT scan. CT scans were taken with 5-14mA and kV, and viewed with 1mm cross-sections. Data was analyzed from reformatted CT scans using Romexis software. CT images were examined for the presence, location, and height of antral septa using axial planes as shown in Figure 2. The presence of septa was evaluated in axial cross-sections, and panoramic reconstructions were used to determine the height of septa (Figure 3). A baseline was drawn connecting the lowest mesial and distal points of the septum. The height of the septa was measured from the baseline to the highest peak of the sinus. The sinus cavity was divided into three parts consisting of an anterior (mesial to distal aspect of second premolar), middle (distal to second premolar to distal aspect of second molar), and posterior (distal aspect of second molar region). The prevalence of septa in each section was evaluated. 15
26 The scans were reviewed by two independent calibrated examiners to confirm findings. The primary dependent measure was the number of sinus septa. Secondary measures included the spatial location and height of septa. Data was submitted to statistical analysis using JMP software to do an analysis of variance. Figure 2: Axial and Panoramic Views. The axial view reveals that the left sinus is divided into three compartments by two sinus septa. At the same axial level, only one of the two septa on the right can be seen. The lateral septa on the left and right are in the third molar area and designated part of the posterior segment. The medial septa on the subject s right is found between the second premolar and the first molar; it is part of the middle segment. The medial septa on the left is in the premolar region thus part of the anterior segment. 16
27 Figure 3: Sagittal, Axial, and Panoramic Views of a CT Scan. Axial and panoramic sections were evaluated for the presence of septa. The axial section reveals pathology associated with the right sinus. There are 2 septa on the subject s right and 3 septa on the left. The heights of the septa were determined by creating a baseline from the most apical aspects medially and laterally and measuring at a right angle from the baseline to the highest peak. 17
28 III. RESULTS: CT scans from 259 subjects were evaluated for the presence, location, and height of septa. The age range for Caucasian subjects was years old with a mean age of African-American subjects ranged from years old with a mean age of Caucasian males comprised 45.0% (54/120) of the subjects, and African-American males comprised 38.9% (54/139). Table 2 summarizes the number of subjects in each group. Table 2: Number of Subjects included in the Investigation. Males Females Total Caucasian African-American Total Of the 259 investigated subjects, 37.5% (97/259) showed no septa and 62.5% (162/259) had at least 1 septa. A total of 343 septa were found in 518 sinuses (66.2%). A summary of the findings is presented in Table 3. Caucasian patients had 186 septa; 37 in the anterior area comprising of the premolars, 95 in the middle area comprising the first and second molars, 54 in the posterior area comprising of the area of the third molars. There were less septa found in African-American subjects with a total of 157; 23 in the anterior, 81 in the middle, and 53 in the posterior. In both races, women had more septa than men; 111 compared to 75 in Caucasians and 108 compared to 49 in African- Americans. 18
29 Table 3: Total Number of Septa Categorized by Race and Location. Caucasian Anterior Middle Posterior Total Male (40.3%) Female (59.7%) Total 37 (19.9%) 95 (51.1%) 54 (29.0%) 186 African-American Anterior Middle Posterior Total Male (31.2%) Female (68.8%) Total 23 (14.6%) 81 (51.6%) 53 (33.8%) 157 Statistical analysis of variance revealed a significant difference with respect to the presence of septa related to subject race (p=0.0061). The effect of gender was approaching significance. The combined effect of gender and race was not significant (Table 4). Caucasians were more likely to have sinus septa than African-Americans; the adjusted mean number was 1.56 compared to 1.09 (Table 5). Adjusted means were reported since there were a disproportionate number of subjects in each category. Although not statistically significant (p=0.07), women were more likely to have septa than men, the adjusted mean number was 1.46 compared to 1.17 (Table 6). When evaluating the septa height, there was no significant relationship with respect to gender, race, or the combined effect of race and gender (Table 7). Table 4: Parameter Estimates for Number of Septa. Term Estimate Std Error t Ratio Prob> t Race[AA] * Gender[F] Race[AA]*Gender[F] Statistically significant results are indicated with an asterisk (*). There was a statistically significant difference in the number of sinus septa with respect to race. The effect of gender was only nearing significance. 19
30 Table 5: Adjusted Means Number of Sinus Septa by Race. Level Adjusted Mean Std Error Mean AA C The adjusted mean number of sinus septa in African-Americans (AA) is 1.09 compared to 1.56 in Caucasians (C). Table 6: Adjusted Mean Number of Sinus Septa by Gender. Level Adjusted Mean Std Error Mean F M The adjusted mean number of sinus septa in female subjects is 1.48 compared to 1.17 in males. Table 7: Parameter Estimates for Septa Height. Term Estimate Std Error t Ratio Prob> t Race[AA] Gender[F] Race[AA]*Gender[F] Results from statistical analysis revealing that neither race or gender were statistically significant. When evaluating solely the anterior zone, there were significant differences only with respect to race (p=0.03). Caucasians had more septa in the premolar region; 0.32 compared to 0.17 septa found in African-Americans (Table 9). Gender and the combined effect of race and gender had no effect on the number of septa (Table 8). Analysis of the middle section revealed that there was a significant difference based on race (Table 10). Caucasians had more septa in the first and second molar region; 0.79 compared to 0.57 septa found in African-Americans (Table 11). The posterior section showed a significant difference only with respect to gender. Females had more septa in the third molar area than males; 0.51 for females and 0.29 in males (Tables 12-13). 20
31 Table 8: Parameter Estimates for Number of Septa in the Anterior Segment. Term Estimate Std Error t Ratio Prob> t Race[AA] * Gender[F] Race[AA]*Gender[F] Results from statistical analysis revealed significant difference in the number of septa in the anterior region with respect to race. Table 9: Adjusted Means Table for Race in the Anterior Segment. Level Adjusted Mean Std Error Mean AA C The adjusted mean number of sinus septa in the anterior segment in African-Americans (AA) is 0.17 compared to 0.32 in Caucasians (C). Table 10: Parameter Estimates for Number of Septa in the Middle Segment. Term Estimate Std Error t Ratio Prob> t Race[AA] * Gender[F] Race[AA]*Gender[F] Statistically significant results are indicated with an asterisk (*); There is significant difference in the number of septa in the middle region with respect to race. Table 11: Adjusted Means Table for Race in the Middle Segment. Level Adjusted Mean Std Error Mean AA C The adjusted mean number of sinus septa in the middle segment in African-Americans (AA) was 0.57 compared to 0.79 in Caucasians (C). Table 12: Parameter Estimates for Number of Septa in the Posterior Segment. Term Estimate Std Error t Ratio Prob> t Race[AA] Gender[F] * Race[AA]*Gender[F] Statistically significant results are indicated with an asterisk (*); There is significant difference in the number of septa in the posterior region with respect to gender. 21
32 Table 13: Adjusted Means Table for Gender in the Posterior Segment. Level Adjusted Mean Std Error Mean F M The adjusted mean number of sinus septa in the posterior segment in female subjects is 0.51 compared to 0.29 in males. 22
33 IV. DISCUSSION: This retrospective study examined the prevalence, location, and height of maxillary sinus septa in 259 consecutive scans of Caucasian and African-American patients obtained for the surgical planning of dental implants. Previous studies have utilized panoramic radiographs for the detection of sinus septa and found the prevalence to range from % [32-35]. However, the percentage of false diagnosis has been reported to be as high as 44.1% [24, 32, 33, 36, 37]. Studies utilizing CT scans for positive identification of septa show the prevalence to be between 13% and 66.7% (Table 1). For accurate diagnosis and proper treatment planning, CT scans are useful for identifying maxillary sinus septa and for evaluating pathology in the sinuses. The prevalence of sinus septa in the current study for all subjects was 66.2%. The percentage of patients with at least one septa was 62.5%. Similarly, van Zyl utilized 3- dimensional reconstructions for the identification of septa with no minimum exclusion criteria, and found that the prevalence was 66% [14]. The prevalence of sinus septa in studies which excluded septa less than 2.5mm-4mm in height ranged between 24-39% [8, 34, 38-41]. The current study reported a higher prevalence than previous reports. This difference may be attributable to dissimilar inclusion criteria. In addition, CT scans enabled more accurate identification of sinus septa compared to panoramic images. Clinically, Zijderveld found sinus septa in 48% of subjects treated [42]. There is a large range of reported findings across all methods used. Methodology can influence the identification of sinus septa. In this study, Caucasians were more likely than African-Americans to have septa in the sinus floor. Caucasian subjects had a prevalence of 77.5% and African-Americans 23
34 had a prevalence of 56.5%. Statistical analysis revealed that the mean number of septa for Caucasians was 1.56 compared to 1.09 in African-Americans (p=0.006). The effect of gender was nearing significance (p=0.07). The data revealed a trend that women were more likely than men to have maxillary sinus septa. The adjusted mean number of sinus septa in female subjects was 1.48 compared to 1.17 in males. Since septa function to reinforce the floor of the sinus and develop as a result of stress transfer, one can surmise that prevalence is related to bone density. Ettinger found that black men and women had higher adjusted bone mineral densities than their Caucasian counterparts [12]. In addition, Caucasian and Asian women were most likely to have osteoporosis. Traditionally, Caucasians have lower bone density when compared to African-Americans and women have lower bone density than men. In this study, a higher prevalence of maxillary sinus septa was found for Caucasians and women. Future studies can examine the relationship of bone density to the presence of septa. In both the anterior and middle sections, race had a significant effect on the number of sinus septa identified (p=0.033 and p=0.035). In the anterior, the adjusted mean number of septa for Caucasians was nearly twice that of African-Americans; 0.32 compared to 0.17 (Tables 8-9). In the middle section, the adjusted mean for African- Americans was 0.57 compared to 0.79 (Tables 10-11). The effect of gender or the combined effect of race and gender did not have a significant effect on the number of sinus septa found in the anterior and middle sections (Tables 8, 10). Bone density difference between races and premature loss of molar teeth may have affected the study results. 24
35 With respect to the posterior section, only gender had a significant effect (p=0.0083); there was no effect for race or combined effect of race and gender. Women had more septa than men: 0.51 septa in the posterior zone compared to men with a 0.29 average (Tables 12-13). It is unclear why the anterior and middle sections were affected by race while the posterior section was affected only by gender. When looking at the overall differences, gender was approaching statistical significance. It is only in the posterior section that it reached statistical significance. Premature loss of third molars may not largely influence the site since many are removed or impacted. Primary septa are typically associated with the roots of teeth, and secondary septa result from premature loss of teeth. Septa in edentulous areas can be either primary or secondary in nature. Septa develop as a result of stress transfer on the bone, and occlusal forces in the posterior zone are much heavier than forces in the anterior and middle. That may explain why gender differences are only found in the posterior zone. Again, bone density and occlusal force differences could influence the number of septa that develop. The majority of septa were found in the middle segment (51.3%, 176/343) which supports the findings of Velasquez-Plata, Kim, Lee, Neugebauer, Park, and Rosano. Ulm and Krennmair found that septa were most frequently present in the anterior segment. Variations in study subjects and differences in inclusion criteria, measurement methods, and imaging modalities may have caused the diverse findings across studies. There may also be some variation between edentulous and fully dentate patients. 68.8% of septa were found in the anterior and middle sections (236/343) which impacts clinicians since that is the area most often involved in sinus augmentation procedures. Perforations of the Schneiderian membrane during sinus augmentation procedures are the most common 25
36 complication. The presence of septa can make elevation of the membrane more difficult. Septa in the anterior region can be managed by creating two windows and elevating the membrane separately in the two compartments. Septa in the middle region are often fractured to enable elevation of the membrane more posteriorly. Although perforations have not been shown to influence the osteointegration of dental implants, large perforations can delay treatment if the procedure needs to be aborted. Smaller tears can be repaired which will not increase treatment time, but will increase material costs to the surgical procedure. Contrastingly, septa may have a slight advantage to sinus augmentation and implant placement because they are mainly composed of cortical bone and implant placement can engage denser bone and have increased primary stability. In addition, septa can act as an additional source of blood supply allowing for faster bone formation and consolidation of graft materials. Limitations of the current investigation include a disproportionate amount of female subjects. Subjects were selected based on treatment codes of consecutively imaged patients which resulted in the inclusion of higher numbers of females in both Caucasians and African-Americans. In addition, information regarding smoking status and systemic diseases was incomplete. Smoking is more likely to have an effect on the thickness of the Schneiderian membrane rather than the presence of septa but diseases such as osteoporosis and hyperparathyroidism can affect bone density and may have an effect on septa formation. There are also limitations associated with Romexis imaging software. Measurements of septa heights were made from a baseline to the highest point and depending on the sharpness of the structures on the CT scan, there may be some measurement errors. Furthermore, there was no information on when teeth were lost; 26
37 therefore, no correlations could be made regarding time elapsed since tooth loss and heights of septa. 27
38 V. CONCLUSION: Differences in the morphology of the maxillary sinus between African-Americans and Caucasians of European decent have remained largely underreported in the literature. The purpose of the study was to evaluate the variations in anatomy of the maxillary sinus between African-American and Caucasian patients, given that differences in sinus morphology can significantly impact treatment planning as well as treatment outcome. A total of 343 septa were identified in 518 maxillary sinuses (66.2%) which corresponded to 62.5% of subjects (162/259). The prevalence in African-Americans was 56.5% compared to 77.5% in Caucasians. Caucasians had more septa than African-Americans (1.56 compared to 1.09, p=0.006). The effect of gender was approaching significance (p=0.07); women tended to have more septa than men. The adjusted mean number of sinus septa in female subjects was 1.48 compared to 1.17 in males. In the both the anterior and middle sections, race had a significant effect (p=0.033 and p=0.035). In the anterior, the adjusted mean number of septa for Caucasians was nearly twice that of African-Americans (0.32 compared to 0.17). In the middle section, the adjusted mean for African-Americans was 0.57 compared to With respect to the posterior section, only gender had a significant effect (p=0.008). Women had an adjusted average of 0.51 septa compared to men with a 0.29 average. The majority of septa were found in the middle segment (51.3%, 176/343) and 17.5% (60/343) were found in the anterior. Thus, 68.8% of all sinus septa were found in the area most often involved in sinus augmentation procedures. It is important to obtain 3-dimensional imaging for proper surgical planning since panoramic images can have false diagnoses up to 44%. Perforations of the Schneiderian membrane are the most common complications 28
39 encountered; sinus septa can make elevation of the membrane more difficult. Appropriate pre-surgical treatment planning requires an in depth knowledge of the anatomy and morphology of the sinus with CT scan imaging to prevent surgical complications due to aberrant structures in the sinus. This investigation confirms the existence of regional differences in maxillary sinus floor morphology. Both race and gender impact maxillary implant treatment planning with a greater frequency of detectable septa in Caucasians and females when compared to African-American males. 29
40 BIBLIOGRAPHY: 1. Shibli, J.A., et al., Prevalence of maxillary sinus septa in 1024 subjects with edentulous upper jaws: a retrospective study. J Oral Implantol, (5): p Rosano, G., et al., Maxillary sinus vascular anatomy and its relation to sinus lift surgery. Clin Oral Implants Res, (7): p Solar, P., et al., Blood supply to the maxillary sinus relevant to sinus floor elevation procedures. Clin Oral Implants Res, (1): p Misch, C.E., Contemporary Implant Dentistry, 3rd Edition. 2008, Mosby. 5. Hupp, J.R., Contemporary Oral and Maxillofacial Surgery, 5th Edition. 2008, Mosby. 6. Chanavaz, M., Maxillary sinus: anatomy, physiology, surgery, and bone grafting related to implantology--eleven years of surgical experience ( ). J Oral Implantol, (3): p Underwood, A.S., An Inquiry into the Anatomy and Pathology of the Maxillary Sinus. J Anat Physiol, (Pt 4): p Ulm, C.W., et al., Incidence and suggested surgical management of septa in sinus-lift procedures. Int J Oral Maxillofac Implants, (4): p van den Bergh, J.P., et al., Anatomical aspects of sinus floor elevations. Clin Oral Implants Res, (3): p Burris, B.G. and E.F. Harris, Maxillary arch size and shape in American blacks and whites. Angle Orthod, (4): p Pollitzer, W.S. and J.J. Anderson, Ethnic and genetic differences in bone mass: a review with a hereditary vs environmental perspective. Am J Clin Nutr, (6): p Ettinger, B., et al., Racial differences in bone density between young adult black and white subjects persist after adjustment for anthropometric, lifestyle, and biochemical differences. J Clin Endocrinol Metab, (2): p Maestre-Ferrin, L., et al., Maxillary sinus septa: a systematic review. Med Oral Patol Oral Cir Bucal, (2): p. e van Zyl, A.W. and W.F. van Heerden, A retrospective analysis of maxillary sinus septa on reformatted computerised tomography scans. Clin Oral Implants Res, (12): p Fernandes, C.L., Volumetric analysis of maxillary sinuses of Zulu and European crania by helical, multislice computed tomography. J Laryngol Otol, (11): p Pietrokovski, J. and M. Massler, Alveolar ridge resorption following tooth extraction. J Prosthet Dent, (1): p Ulm, C.W., et al., The edentulous maxillary alveolar process in the region of the maxillary sinus--a study of physical dimension. Int J Oral Maxillofac Surg, (4): p Cho, S.H., et al., Factors for maxillary sinus volume and craniofacial anatomical features in adults with chronic rhinosinusitis. Arch Otolaryngol Head Neck Surg, (6): p Du Tolt, D.F. and C. Nortje, The maxillae: integrated and applied anatomy relevant to dentistry. SADJ, (8): p Boyne, P.J. and R.A. James, Grafting of the maxillary sinus floor with autogenous marrow and bone. J Oral Surg, (8): p Summers, R.B., A new concept in maxillary implant surgery: the osteotome technique. Compendium, (2): p. 152, 154-6, 158 passim; quiz Jensen, O.T., et al., Report of the Sinus Consensus Conference of Int J Oral Maxillofac Implants, Suppl: p
41 23. Raghoebar, G.M., et al., Morbidity and complications of bone grafting of the floor of the maxillary sinus for the placement of endosseous implants. Mund Kiefer Gesichtschir, Suppl 1: p. S Kasabah, S., et al., Can we predict maxillary sinus mucosa perforation? Acta Medica (Hradec Kralove), (1): p Schwartz-Arad, D., R. Herzberg, and E. Dolev, The prevalence of surgical complications of the sinus graft procedure and their impact on implant survival. J Periodontol, (4): p Manor, Y., et al., Late signs and symptoms of maxillary sinusitis after sinus augmentation. Oral Surg Oral Med Oral Pathol Oral Radiol Endod, (1): p. e Newman, M.G., Carranza's Clinical Periodontology, 10th Edition. 2006, Saunders Book Company. 28. Testori, T., et al., Ligation of an unusually large vessel during maxillary sinus floor augmentation. A case report. Eur J Oral Implantol, (3): p Avila-Ortiz, G., et al., Analysis of the influence of residual alveolar bone height on sinus augmentation outcomes. Clin Oral Implants Res, Avila, G., et al., The influence of the bucco-palatal distance on sinus augmentation outcomes. J Periodontol, (7): p Wallace, S.S. and S.J. Froum, Effect of maxillary sinus augmentation on the survival of endosseous dental implants. A systematic review. Ann Periodontol, (1): p Krennmair, G., C. Ulm, and H. Lugmayr, Maxillary sinus septa: incidence, morphology and clinical implications. J Craniomaxillofac Surg, (5): p Gonzalez-Santana, H., et al., A study of the septa in the maxillary sinuses and the subantral alveolar processes in 30 patients. J Oral Implantol, (6): p Naitoh, M., et al., Assessment of maxillary sinus septa using cone-beam computed tomography: etiological consideration. Clin Implant Dent Relat Res, Suppl 1: p. e Maestre-Ferrin, L., et al., Prevalence, location, and size of maxillary sinus septa: panoramic radiograph versus computed tomography scan. J Oral Maxillofac Surg, (2): p Krennmair, G., et al., The incidence, location, and height of maxillary sinus septa in the edentulous and dentate maxilla. J Oral Maxillofac Surg, (6): p ; discussion Park, Y.B., et al., Analysis of the anatomy of the maxillary sinus septum using 3- dimensional computed tomography. J Oral Maxillofac Surg, (4): p Velasquez-Plata, D., et al., Maxillary sinus septa: a 3-dimensional computerized tomographic scan analysis. Int J Oral Maxillofac Implants, (6): p Kim, M.J., et al., Maxillary sinus septa: prevalence, height, location, and morphology. A reformatted computed tomography scan analysis. J Periodontol, (5): p Ella, B., et al., Septa within the sinus: effect on elevation of the sinus floor. Br J Oral Maxillofac Surg, (6): p Lee, W.J., S.J. Lee, and H.S. Kim, Analysis of location and prevalence of maxillary sinus septa. J Periodontal Implant Sci, (2): p Zijderveld, S.A., et al., Anatomical and surgical findings and complications in 100 consecutive maxillary sinus floor elevation procedures. J Oral Maxillofac Surg, (7): p
Oftentimes, as implant surgeons, we are
 CLINICAL AVOIDING INJURY TO THE INFERIOR ALVEOLAR NERVE BY ROUTINE USE OF INTRAOPERATIVE RADIOGRAPHS DURING IMPLANT PLACEMENT Jeffrey Burstein, DDS, MD; Chris Mastin, DMD; Bach Le, DDS, MD Injury to the
CLINICAL AVOIDING INJURY TO THE INFERIOR ALVEOLAR NERVE BY ROUTINE USE OF INTRAOPERATIVE RADIOGRAPHS DURING IMPLANT PLACEMENT Jeffrey Burstein, DDS, MD; Chris Mastin, DMD; Bach Le, DDS, MD Injury to the
Resorptive Changes of Maxillary and Mandibular Bone Structures in Removable Denture Wearers
 Resorptive Changes of Maxillary and Mandibular Bone Structures in Removable Denture Wearers Dubravka KnezoviÊ-ZlatariÊ Asja»elebiÊ Biserka LaziÊ Department of Prosthodontics School of Dental Medicine University
Resorptive Changes of Maxillary and Mandibular Bone Structures in Removable Denture Wearers Dubravka KnezoviÊ-ZlatariÊ Asja»elebiÊ Biserka LaziÊ Department of Prosthodontics School of Dental Medicine University
LATERAL BONE EXPANSION FOR IMMEDIATE PLACEMENT OF ENDOSSEOUS DENTAL IMPLANTS
 LATERAL BONE EXPANSION FOR IMMEDIATE PLACEMENT OF ENDOSSEOUS DENTAL IMPLANTS Department of Oral Maxillofacial Surgery, Chisinau Abstract: The study included 10 using the split control expansion technique
LATERAL BONE EXPANSION FOR IMMEDIATE PLACEMENT OF ENDOSSEOUS DENTAL IMPLANTS Department of Oral Maxillofacial Surgery, Chisinau Abstract: The study included 10 using the split control expansion technique
Anatomic limitations in the maxilla provide challenges
 Osteotome Single-Stage Dental Implant Placement With and Without Sinus Elevation: A Clinical Report Orest G. Komarnyckyj, DDS*/Robert M. London, DDS** Forty-three sites in 16 patients were selected for
Osteotome Single-Stage Dental Implant Placement With and Without Sinus Elevation: A Clinical Report Orest G. Komarnyckyj, DDS*/Robert M. London, DDS** Forty-three sites in 16 patients were selected for
Maxillary Sinus. (Antrum of Higmore)
") Maxillary Sinus (Antrum of Higmore) The maxillary sinus is a pneumatic space. It is the largest bilateral air sinus located in the body of the maxilla and opens in the middle nasal meatus of the nasal
Maxillary Sinus (Antrum of Higmore) The maxillary sinus is a pneumatic space. It is the largest bilateral air sinus located in the body of the maxilla and opens in the middle nasal meatus of the nasal
The Clinical Significance of Sinus Membrane Perforation During Augmentation of the Maxillary Sinus
 DENTAL IMPLANTS The Clinical Significance of Sinus Membrane Perforation During Augmentation of the Maxillary Sinus Leon Ardekian, DDS,* Efrat Oved-Peleg, DMD, Eli E. Mactei, DMD, and Micha Peled, DMD,
DENTAL IMPLANTS The Clinical Significance of Sinus Membrane Perforation During Augmentation of the Maxillary Sinus Leon Ardekian, DDS,* Efrat Oved-Peleg, DMD, Eli E. Mactei, DMD, and Micha Peled, DMD,
Restoration of the Edentulous Maxilla: The Case for the Zygomatic Implants
 CLINICAL CONTROVERSIES IN ORAL AND MAXILLOFACIAL SURGERY: PART ONE J Oral Maxillofac Surg 62:1418-1422, 2004 Restoration of the Edentulous Maxilla: The Case for the Zygomatic Implants Eric D. Ferrara,
CLINICAL CONTROVERSIES IN ORAL AND MAXILLOFACIAL SURGERY: PART ONE J Oral Maxillofac Surg 62:1418-1422, 2004 Restoration of the Edentulous Maxilla: The Case for the Zygomatic Implants Eric D. Ferrara,
Department of Periodontology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
 Location of maxillary intraosseous vascular anastomosis based on the tooth position and height of the residual alveolar bone: computed tomographic analysis Seung-Min Yang*, Seung-Beom Kye Department of
Location of maxillary intraosseous vascular anastomosis based on the tooth position and height of the residual alveolar bone: computed tomographic analysis Seung-Min Yang*, Seung-Beom Kye Department of
Healing Abutment Selection. Perio Implant Part I. Implant Surface Characteristics. Single Tooth Restorations. Credit and Thanks for Lecture Material
 Healing Abutment Selection Perio Implant Part I Credit and Thanks for Lecture Material Implant Surface Characteristics!CAPT Robert Taft!CAPT Greg Waskewicz!Periodontal Residents NPDS and UMN!Machined Titanium!Tiunite!Osseotite
Healing Abutment Selection Perio Implant Part I Credit and Thanks for Lecture Material Implant Surface Characteristics!CAPT Robert Taft!CAPT Greg Waskewicz!Periodontal Residents NPDS and UMN!Machined Titanium!Tiunite!Osseotite
Current Concepts in American Dentistry: Advances in Implantology and Oral Rehabilitation
 2009 New York University College Of Dentistry Linhart Continuing Dental Education Program Presents Current Concepts in American Dentistry: Advances in Implantology and Oral Rehabilitation International
2009 New York University College Of Dentistry Linhart Continuing Dental Education Program Presents Current Concepts in American Dentistry: Advances in Implantology and Oral Rehabilitation International
Supervisors: Dr. Farhan Raza Khan
 1 Presenter: Dr. Sana Ehsen Supervisors: Dr. Farhan Raza Khan 2 A dental implant (also known as an endosseous implant or fixture) is a surgical component that interfaces with the bone of the jaw to support
1 Presenter: Dr. Sana Ehsen Supervisors: Dr. Farhan Raza Khan 2 A dental implant (also known as an endosseous implant or fixture) is a surgical component that interfaces with the bone of the jaw to support
1 The Single Tooth Implant. The Ultimate Aesthetic Challenge
 1 The Single Tooth Implant The Ultimate Aesthetic Challenge by Daniel G. Pompa, D.D.S. 2 Before starting any Maxillary Anterior Single Implant, or any case in the esthetic zone: TAKE A PHOTO OF YOUR PATIENT
1 The Single Tooth Implant The Ultimate Aesthetic Challenge by Daniel G. Pompa, D.D.S. 2 Before starting any Maxillary Anterior Single Implant, or any case in the esthetic zone: TAKE A PHOTO OF YOUR PATIENT
IMPLANT DENTISTRY EXAM BANK
 IMPLANT DENTISTRY EXAM BANK 1. Define osseointegration. (4 points, 1/4 2. What are the critical components of an acceptable clinical trial? (10 points) 3. Compare the masticatory performance of individuals
IMPLANT DENTISTRY EXAM BANK 1. Define osseointegration. (4 points, 1/4 2. What are the critical components of an acceptable clinical trial? (10 points) 3. Compare the masticatory performance of individuals
Histologic comparison of biologic width around teeth versus implants: The effect on bone preservation
 Clinical Histologic comparison of biologic width around teeth versus implants: The effect on bone preservation Kazuto Makigusa 1 Abstract Histological analysis of the biological width surrounding primate
Clinical Histologic comparison of biologic width around teeth versus implants: The effect on bone preservation Kazuto Makigusa 1 Abstract Histological analysis of the biological width surrounding primate
MAIN LINE DENTAL IMPLANT CENTER
 1257 Lancaster Ave Berwyn, PA 19312 Tel: 610-722-5542 CHIUN-LIN (STEVEN), LIU D.D.S., D.M.D. School of Dental Medicine CURRICULUM VITAE Summer, 2012 Education: 1987-1993 D.D.S. Kaohsiung Medical University
1257 Lancaster Ave Berwyn, PA 19312 Tel: 610-722-5542 CHIUN-LIN (STEVEN), LIU D.D.S., D.M.D. School of Dental Medicine CURRICULUM VITAE Summer, 2012 Education: 1987-1993 D.D.S. Kaohsiung Medical University
BioHorizons Education Programme 2015
 BioHorizons Education Programme 2015 SPMP14328GB Rev A November 2014 Contents The Role of Implants in Restorative Dentistry An Introduction to Contemporary Implant Prosthodontics Sinus Elevation Socket
BioHorizons Education Programme 2015 SPMP14328GB Rev A November 2014 Contents The Role of Implants in Restorative Dentistry An Introduction to Contemporary Implant Prosthodontics Sinus Elevation Socket
Replacing Hopeless Retained Deciduous Teeth in Adults Utilizing Dental Implants: Concepts and Case Presentation
 Replacing Hopeless Retained Deciduous Teeth in Adults Utilizing Dental Implants: Concepts and Case Presentation by Michael Tischler, DDS Published: Dentistry Today November 2005 Photos at end of article
Replacing Hopeless Retained Deciduous Teeth in Adults Utilizing Dental Implants: Concepts and Case Presentation by Michael Tischler, DDS Published: Dentistry Today November 2005 Photos at end of article
Long-term success of osseointegrated implants
 Against All Odds A No Bone Solution Long-term success of osseointegrated implants depends on the length of the implants used and the quality and quantity of bone surrounding these implants. As surgical
Against All Odds A No Bone Solution Long-term success of osseointegrated implants depends on the length of the implants used and the quality and quantity of bone surrounding these implants. As surgical
An adequate amount of bone, in
 CASE REPORT Immediate Loading of Dental Implant After Sinus Floor Elevation With Osteotome Technique: A Clinical Report and Preliminary Radiographic Results Mario Santagata, MD* Luigi Guariniello, MD,
CASE REPORT Immediate Loading of Dental Implant After Sinus Floor Elevation With Osteotome Technique: A Clinical Report and Preliminary Radiographic Results Mario Santagata, MD* Luigi Guariniello, MD,
Bone augmentation procedure without wound closure
 THE CREATION OF ATTACHED GINGIVA IMMEDIATELY AFTER EXTRACTION Bone augmentation procedure without wound closure One of the characteristics of wound healing after an extraction is that the alveolar process
THE CREATION OF ATTACHED GINGIVA IMMEDIATELY AFTER EXTRACTION Bone augmentation procedure without wound closure One of the characteristics of wound healing after an extraction is that the alveolar process
Appropriate soft tissue closure represents a critical
 Periosteoplasty for Soft Tissue Closure and Augmentation in Preprosthetic Surgery: A Surgical Report Albino Triaca, Dr Med, Dr Med Dent 1 /Roger Minoretti, Dr Med, Dr Med Dent 1 / Mauro Merli, DMD 2 /Beat
Periosteoplasty for Soft Tissue Closure and Augmentation in Preprosthetic Surgery: A Surgical Report Albino Triaca, Dr Med, Dr Med Dent 1 /Roger Minoretti, Dr Med, Dr Med Dent 1 / Mauro Merli, DMD 2 /Beat
Replacement of the upper left central incisor with a Straumann Bone Level Implant and a Straumann Customized Ceramic Abutment
 Replacement of the upper left central incisor with a Straumann Bone Level Implant and a Straumann Customized Ceramic Abutment by Dr. Ronald Jung and Master Dental Technician Xavier Zahno Initial situation
Replacement of the upper left central incisor with a Straumann Bone Level Implant and a Straumann Customized Ceramic Abutment by Dr. Ronald Jung and Master Dental Technician Xavier Zahno Initial situation
Updated: February 2014. 1986-1990 Highland General Hospital, Certificate of Completion Oral & Maxillofacial Surgery Residency
 Edmond Bedrossian DDS, FACD, FACOMS, FAO Diplomate, American Board of Oral & Maxillofacial Surgery Director, Implant Surgery, Alameda Medical Center & UOP School of Dentistry Professor, Department of Oral
Edmond Bedrossian DDS, FACD, FACOMS, FAO Diplomate, American Board of Oral & Maxillofacial Surgery Director, Implant Surgery, Alameda Medical Center & UOP School of Dentistry Professor, Department of Oral
Key words maxillary sinus, posterior teeth roots. Introduction. Tikrit Journal for Dental Sciences 1(2012)81-88
81-88") Tikrit Journal for Dental Sciences 1(2012)81-88 The Relation of Maxillary Posterior Teeth Roots to the Maxillary Sinus Floor Using Panoramic and Computed Tomography Imaging in a Sample of Kurdish People
Tikrit Journal for Dental Sciences 1(2012)81-88 The Relation of Maxillary Posterior Teeth Roots to the Maxillary Sinus Floor Using Panoramic and Computed Tomography Imaging in a Sample of Kurdish People
Adramatic increase in the number of dental practitioners
 Risk Management Aspects of Implant Dentistry Navot Givol, DMD 1 /Shlomo Taicher, DMD 2 /Talia Halamish-Shani, LLB 3 /Gavriel Chaushu, DMD, MSc 4 Purpose: To categorize and review complications related
Risk Management Aspects of Implant Dentistry Navot Givol, DMD 1 /Shlomo Taicher, DMD 2 /Talia Halamish-Shani, LLB 3 /Gavriel Chaushu, DMD, MSc 4 Purpose: To categorize and review complications related
Saudi Fellowship In Dental Implant (SF-DI)
") Saudi Fellowship In Dental Implant (SF-DI) Prepared and Updated by Dr. Arwa AL-Sayed Consultant Periodontics and Dental Implants M E M B E R S Dr. Arwa AL-Sayed Dr. Abdulhadi Abanmy Dr. Ali AL-Ghamdi Dr.
Saudi Fellowship In Dental Implant (SF-DI) Prepared and Updated by Dr. Arwa AL-Sayed Consultant Periodontics and Dental Implants M E M B E R S Dr. Arwa AL-Sayed Dr. Abdulhadi Abanmy Dr. Ali AL-Ghamdi Dr.
Advances in bone augmentation to enable dental implant placement: Consensus Report of the Sixth European Workshop on Periodontology
 J Clin Periodontol 2008; 35 (Suppl. 8): 168 172 doi: 10.1111/j.1600-051X.2008.01268.x Advances in bone augmentation to enable dental implant placement: Consensus Report of the Sixth European Workshop on
J Clin Periodontol 2008; 35 (Suppl. 8): 168 172 doi: 10.1111/j.1600-051X.2008.01268.x Advances in bone augmentation to enable dental implant placement: Consensus Report of the Sixth European Workshop on
PREPARATION OF MOUTH FOR REMOVABLE PARTIAL DENTURES Dr. Mazen kanout
 PREPARATION OF MOUTH FOR REMOVABLE PARTIAL DENTURES Dr. Mazen kanout Mouth preparation includes procedures in four categories: 1. Oral Surgical Preparation. 2. Conditioning of Abused and Irritated Tissue.
PREPARATION OF MOUTH FOR REMOVABLE PARTIAL DENTURES Dr. Mazen kanout Mouth preparation includes procedures in four categories: 1. Oral Surgical Preparation. 2. Conditioning of Abused and Irritated Tissue.
Don t Let Life Pass You By Because Of Oral Bone Loss
 Don t Let Life Pass You By Because Of Oral Bone Loss Ask For Dental Implant Solutions From BIOMET 3i Scan With Your Smartphone! In order to scan QR codes, your mobile device must have a QR code reader
Don t Let Life Pass You By Because Of Oral Bone Loss Ask For Dental Implant Solutions From BIOMET 3i Scan With Your Smartphone! In order to scan QR codes, your mobile device must have a QR code reader
A. DEVELOPMENT OF THE DENTAL ORGAN (ENAMEL ORGAN):
:") A. DEVELOPMENT OF THE DENTAL ORGAN (ENAMEL ORGAN): AS EARLY AS THE SECOND MONTH OF FETAL LIFE, THE DEVELOPMENT OF THE DECIDUOUS TEETH MAY FIRST BECOME EVIDENT. 1. Dental lamina and Bud stage At about six
A. DEVELOPMENT OF THE DENTAL ORGAN (ENAMEL ORGAN): AS EARLY AS THE SECOND MONTH OF FETAL LIFE, THE DEVELOPMENT OF THE DECIDUOUS TEETH MAY FIRST BECOME EVIDENT. 1. Dental lamina and Bud stage At about six
Powertome Assisted Atraumatic Tooth Extraction
 Powertome Assisted Atraumatic Tooth Extraction White et al Jason White, DDS 1 2 3 Abstract Background: While traditional dental extraction techniques encourage minimal trauma, luxated elevation and forceps
Powertome Assisted Atraumatic Tooth Extraction White et al Jason White, DDS 1 2 3 Abstract Background: While traditional dental extraction techniques encourage minimal trauma, luxated elevation and forceps
DEVELOPMENT AND GROWTH OF THE MANDIBLE
 2012-2013 ORAL BIOLOGY DEVELOPMENT AND GROWTH OF THE MANDIBLE Ass. Prof. Dr. Heba M. Elsabaa Development and Growth of the Mandible DEVELOPMENT OF THE MANDIBLE The Mandible Is the largest and strongest
2012-2013 ORAL BIOLOGY DEVELOPMENT AND GROWTH OF THE MANDIBLE Ass. Prof. Dr. Heba M. Elsabaa Development and Growth of the Mandible DEVELOPMENT OF THE MANDIBLE The Mandible Is the largest and strongest
TRI Product NewsFlash. December 2015
 TRI Product NewsFlash December 2015 Study Overview 2015 Dear Partners Year in, year out, we are screening all major scientific journals to ensure that our TRI Performance Concept still reflects the latest
TRI Product NewsFlash December 2015 Study Overview 2015 Dear Partners Year in, year out, we are screening all major scientific journals to ensure that our TRI Performance Concept still reflects the latest
Dental Updates. Excerpted Article e-mail: re777@comcast.net. Why Implant Screws Loosen Part 1. Richard Erickson, MS, DDS
 ¼ ½ ¾ µ mw/cm 2 Volume 17; 2007 Dental Updates "CUTTING EDGE INFORMATION FOR THE DENTAL PROFESSIONAL " 200 SEMINARS AND 30 JOURNALS REVIEWED YEARLY FOR THE LATEST, CUTTING EDGE INFORMATION Excerpted Article
¼ ½ ¾ µ mw/cm 2 Volume 17; 2007 Dental Updates "CUTTING EDGE INFORMATION FOR THE DENTAL PROFESSIONAL " 200 SEMINARS AND 30 JOURNALS REVIEWED YEARLY FOR THE LATEST, CUTTING EDGE INFORMATION Excerpted Article
What Dental Implants Can Do For You!
 What Dental Implants Can Do For You! Putting Smiles into Motion About Implants 01. What if a Tooth is Lost and the Area is Left Untreated? 02. Do You Want to Restore Confidence in Your Appearance? 03.
What Dental Implants Can Do For You! Putting Smiles into Motion About Implants 01. What if a Tooth is Lost and the Area is Left Untreated? 02. Do You Want to Restore Confidence in Your Appearance? 03.
UNMH Oral and Maxillofacial Surgery Clinical Privileges
 All new applicants must meet the following requirements as approved by the UNMH Board of Trustees effective: 09/26/2014 INSTRUCTIONS Applicant: Check off the "Requested" box for each privilege requested.
All new applicants must meet the following requirements as approved by the UNMH Board of Trustees effective: 09/26/2014 INSTRUCTIONS Applicant: Check off the "Requested" box for each privilege requested.
Warm Regards, Tony Fiorello and the Tatum Surgical Staff
 Volume 4, Issue 2 June, 2011 4500 140th Avenue North, Suite 112 Phone: 888-360-5550 Clearwater, Florida 33762 Fax: 727-531-6005 tatumimplants@verizon.net The Tatum Times INSIDE THIS ISSUE: A Simple and
Volume 4, Issue 2 June, 2011 4500 140th Avenue North, Suite 112 Phone: 888-360-5550 Clearwater, Florida 33762 Fax: 727-531-6005 tatumimplants@verizon.net The Tatum Times INSIDE THIS ISSUE: A Simple and
Ideal treatment of the impaired
 RESEARCH IMPLANTS AS ANCHORAGE IN ORTHODONTICS: ACLINICAL CASE REPORT Dale B. Herrero, DDS KEY WORDS External anchorage Pneumatized Often, in dental reconstruction, orthodontics is required for either
RESEARCH IMPLANTS AS ANCHORAGE IN ORTHODONTICS: ACLINICAL CASE REPORT Dale B. Herrero, DDS KEY WORDS External anchorage Pneumatized Often, in dental reconstruction, orthodontics is required for either
E. Richard Hughes, D.D.S.
 E. Richard Hughes, D.D.S. Docket No. FDA-2012-N-0677 Blade Form Endosseous Dental Implants E. Richard Hughes, D.D.S. 46440 Benedict Dr.,# 201 Sterling, Va. 20164 USA 703-444-1152 erhughesdds@aol.com Diplomate,
E. Richard Hughes, D.D.S. Docket No. FDA-2012-N-0677 Blade Form Endosseous Dental Implants E. Richard Hughes, D.D.S. 46440 Benedict Dr.,# 201 Sterling, Va. 20164 USA 703-444-1152 erhughesdds@aol.com Diplomate,
How To Plan A Dental Implant With A 3D Image Based Program
 J Oral Maxillofac Surg 62:41-47, 2004, Suppl 2 Interactive Imaging for Implant Planning, Placement, and Prosthesis Construction Stephen M. Parel, DDS,* and R. Gilbert Triplett, DDS, PhD Purpose: This review
J Oral Maxillofac Surg 62:41-47, 2004, Suppl 2 Interactive Imaging for Implant Planning, Placement, and Prosthesis Construction Stephen M. Parel, DDS,* and R. Gilbert Triplett, DDS, PhD Purpose: This review
BIOMECHANICAL ANALYSIS OF NORMAL AND IMPLANTED TOOTH USING BITING FORCE MEASUREMENT
 BIOMECHANICAL ANALYSIS OF NORMAL AND IMPLANTED TOOTH USING BITING FORCE MEASUREMENT B K Biswas 1 S Bag 2 & S Pal 3 1. Dept. of Dental Surgery, Associate Professor, KPC Medical College & Hospital, Kolkata,
BIOMECHANICAL ANALYSIS OF NORMAL AND IMPLANTED TOOTH USING BITING FORCE MEASUREMENT B K Biswas 1 S Bag 2 & S Pal 3 1. Dept. of Dental Surgery, Associate Professor, KPC Medical College & Hospital, Kolkata,
Complications Associated with Tooth Extraction
 1 Complications Associated with Tooth Extraction Mark M. Smith, VMD, DACVS, DAVDC Center for Veterinary Dentistry and Oral Surgery 9041 Gaither Road Gaithersburg, MD 20877 Introduction Tooth extraction
1 Complications Associated with Tooth Extraction Mark M. Smith, VMD, DACVS, DAVDC Center for Veterinary Dentistry and Oral Surgery 9041 Gaither Road Gaithersburg, MD 20877 Introduction Tooth extraction
(970) 663-6878 WWW. REYNOLDSORALFACIAL. COM
 663-6878 WWW. REYNOLDSORALFACIAL. COM") (970) 663-6878 WWW. REYNOLDSORALFACIAL. COM Glossary Anterior-Posterior - Front-back Class I - Normal relationship of teeth Class II - Distal (posterior) relationship of mandibular teeth to maxillary teeth.
(970) 663-6878 WWW. REYNOLDSORALFACIAL. COM Glossary Anterior-Posterior - Front-back Class I - Normal relationship of teeth Class II - Distal (posterior) relationship of mandibular teeth to maxillary teeth.
Implants in your Laboratory: Abutment Design
 1/2 point CDT documented scientific credit. See Page 41. Implants in your Laboratory: Abutment Design By Leon Hermanides, CDT A patient s anatomical limitations have the greatest predictive value for successful
1/2 point CDT documented scientific credit. See Page 41. Implants in your Laboratory: Abutment Design By Leon Hermanides, CDT A patient s anatomical limitations have the greatest predictive value for successful
The Immediate Placement of Dental Implants Into Extraction Sites With Periapical Lesions: A Retrospective Chart Review
 IMPLANTS The Immediate Placement of Dental Implants Into Extraction Sites With Periapical Lesions: A Retrospective Chart Review Christopher Lincoln Bell,* David Diehl, Brian Michael Bell, and Robert E.
IMPLANTS The Immediate Placement of Dental Implants Into Extraction Sites With Periapical Lesions: A Retrospective Chart Review Christopher Lincoln Bell,* David Diehl, Brian Michael Bell, and Robert E.
Retrospective study on the survival rate of IBS implant
 Retrospective study on the survival rate of IBS implant Date : 30. 05. 2013 Written by : Dr. Je Won Wang, Director of research Approved by : Prof. Min Seung Ki - Contents - 1. Purpose Of Study 2. Materials
Retrospective study on the survival rate of IBS implant Date : 30. 05. 2013 Written by : Dr. Je Won Wang, Director of research Approved by : Prof. Min Seung Ki - Contents - 1. Purpose Of Study 2. Materials
The Mandibular Two-Implant Overdenture First-Choice. Standard of Care for the Edentulous Denture Patient
 The Mandibular Two-Implant Overdenture First-Choice Standard of Care for the Edentulous Denture Patient Joseph R. Carpentieri, DDS Dennis P. Tarnow, DDS ii Preface Preface The prosthetic management of
The Mandibular Two-Implant Overdenture First-Choice Standard of Care for the Edentulous Denture Patient Joseph R. Carpentieri, DDS Dennis P. Tarnow, DDS ii Preface Preface The prosthetic management of
INFUSE Bone Graft (rhbmp-2/acs)
") 1 INFUSE Bone Graft (rhbmp-2/acs) For patients who need more bone to place dental implants Enjoy living with INFUSE Bone Graft. www.medtronic.com Medtronic Spinal and Biologics Business Worldwide Headquarters
1 INFUSE Bone Graft (rhbmp-2/acs) For patients who need more bone to place dental implants Enjoy living with INFUSE Bone Graft. www.medtronic.com Medtronic Spinal and Biologics Business Worldwide Headquarters
Modern Tooth Replacement Strategies & Digital Workflow
 Modern Tooth Replacement Strategies & Digital Workflow Case Studies by Dr Maurice Salama, DMD AS PUBLISHED BY Dentistry Today, June 2014 Complete Implant Restoration System FACTS: Implant Dentistry Has
Modern Tooth Replacement Strategies & Digital Workflow Case Studies by Dr Maurice Salama, DMD AS PUBLISHED BY Dentistry Today, June 2014 Complete Implant Restoration System FACTS: Implant Dentistry Has
Residency Competency and Proficiency Statements
 Residency Competency and Proficiency Statements 1. REQUEST AND RESPOND TO REQUESTS FOR CONSULTATIONS Identify needs and make referrals to appropriate health care providers for the treatment of physiologic,
Residency Competency and Proficiency Statements 1. REQUEST AND RESPOND TO REQUESTS FOR CONSULTATIONS Identify needs and make referrals to appropriate health care providers for the treatment of physiologic,
Understanding Dental Implants
 Understanding Dental Implants Comfort and Confidence Again A new smile It s no fun when you re missing teeth. You may not feel comfortable eating or speaking. You might even avoid smiling in public. Fortunately,
Understanding Dental Implants Comfort and Confidence Again A new smile It s no fun when you re missing teeth. You may not feel comfortable eating or speaking. You might even avoid smiling in public. Fortunately,
Molar Uprighting Dr. Margherita Santoro Division of Orthodontics School of Dental and Oral surgery. Consequences of tooth loss.
 Molar Uprighting Dr. Margherita Santoro Division of Orthodontics School of Dental and Oral surgery Molars The wide occlusal surface is designed for food grinding. The surface needs to be aligned with the
Molar Uprighting Dr. Margherita Santoro Division of Orthodontics School of Dental and Oral surgery Molars The wide occlusal surface is designed for food grinding. The surface needs to be aligned with the
IMPLANT CONSENT FORM WHAT ARE DENTAL IMPLANTS?
 IMPLANT CONSENT FORM WHAT ARE DENTAL IMPLANTS? Dental implants are a very successful and accepted treatment option to replace lost or missing teeth. A dental implant is essentially an artificial tooth
IMPLANT CONSENT FORM WHAT ARE DENTAL IMPLANTS? Dental implants are a very successful and accepted treatment option to replace lost or missing teeth. A dental implant is essentially an artificial tooth
The definitive implant restoration
 CASE REPORT Implant Bone Rings. One-Stage Three-Dimensional Bone Transplant Technique: A Case Report Mark R. Stevens, DDS 1 * Hany A. Emam, MS 2 Mahmoud E. L. Alaily, MS 3 Mohamed Sharawy, PhD 4 A variety
CASE REPORT Implant Bone Rings. One-Stage Three-Dimensional Bone Transplant Technique: A Case Report Mark R. Stevens, DDS 1 * Hany A. Emam, MS 2 Mahmoud E. L. Alaily, MS 3 Mohamed Sharawy, PhD 4 A variety
Straumann Bone Level Tapered Implant Peer-to-peer communication
 Straumann Bone Level Tapered Implant Peer-to-peer communication Clinical cases April, 2015 Clinical Cases Case No. Site 1 Single unit; Anterior Maxilla 2 Multi-unit; Anterior Maxilla Implant placement
Straumann Bone Level Tapered Implant Peer-to-peer communication Clinical cases April, 2015 Clinical Cases Case No. Site 1 Single unit; Anterior Maxilla 2 Multi-unit; Anterior Maxilla Implant placement
Prosthetic rehabilitation with dental implants after treatment of a keratocystic odontogenic tumor. case report
 Journal section: Oral Surgery Publication Types: Case Report doi:10.4317/jced.3.e360 Prosthetic rehabilitation with dental implants after treatment of a keratocystic odontogenic tumor. case report Amila
Journal section: Oral Surgery Publication Types: Case Report doi:10.4317/jced.3.e360 Prosthetic rehabilitation with dental implants after treatment of a keratocystic odontogenic tumor. case report Amila
CHAPTER 10 RESTS AND PREPARATIONS. 4. Serve as a reference point for evaluating the fit of the framework to the teeth.
 CHAPTER 10 RESTS AND DEFINITIONS A REST is any rigid part of an RPD framework which contacts a properly prepared surface of a tooth. A REST PREPARATION or REST SEAT is any portion of a tooth or restoration
CHAPTER 10 RESTS AND DEFINITIONS A REST is any rigid part of an RPD framework which contacts a properly prepared surface of a tooth. A REST PREPARATION or REST SEAT is any portion of a tooth or restoration
Comparison of Peri-Implant Bone Loss
 Original Article Comparison of Peri-Implant Bone Loss and Survival of Maxillary Intrasinus and Extrasinus Implants After 2 Years AR. Rokn 1,2, AAR. Rasouli Ghahroudi 3,4, S. Hemati 5, A. Soolari 6 1 Associate
Original Article Comparison of Peri-Implant Bone Loss and Survival of Maxillary Intrasinus and Extrasinus Implants After 2 Years AR. Rokn 1,2, AAR. Rasouli Ghahroudi 3,4, S. Hemati 5, A. Soolari 6 1 Associate
4-1-2005. Dental Clinical Criteria and Documentation Requirements
 4-1-2005 Dental Clinical Criteria and Documentation Requirements Table of Contents Dental Clinical Criteria Cast Restorations and Veneer Procedures... Pages 1-3 Crown Repair... Page 3 Endodontic Procedures...
4-1-2005 Dental Clinical Criteria and Documentation Requirements Table of Contents Dental Clinical Criteria Cast Restorations and Veneer Procedures... Pages 1-3 Crown Repair... Page 3 Endodontic Procedures...
Ando A., Nakamura Y., Kanbara R., Kumano H., Miyata T., Masuda T., Ohno Y. and Tanaka Y.
 11. The Effect of Abutment Tooth Connection with Extracoronal Attachment using the Three Dimensional Finite Element Method - Part 2. The Construction of Finite Element Model from CT Data - Ando A., Nakamura
11. The Effect of Abutment Tooth Connection with Extracoronal Attachment using the Three Dimensional Finite Element Method - Part 2. The Construction of Finite Element Model from CT Data - Ando A., Nakamura
Prosthetic treatment planning on the basis of scientific evidence.
 Prosthetic treatment planning on the basis of scientific evidence. Pjetursson BE, Lang NP. J Oral Rehabil. 2008 Jan;35 Suppl 1:72-9. Faculty of Odontology, University of Iceland, Reykjavik, Iceland, and
Prosthetic treatment planning on the basis of scientific evidence. Pjetursson BE, Lang NP. J Oral Rehabil. 2008 Jan;35 Suppl 1:72-9. Faculty of Odontology, University of Iceland, Reykjavik, Iceland, and
A Study of 25 Zygomatic Dental Implants with 11 to 49 Months Follow-up After Loading
 A Study of 25 Zygomatic Dental Implants with 11 to 49 Months Follow-up After Loading Fredrik Ahlgren, DDS, MSc 1 / Kjell Størksen, DDS 2 /Knut Tornes, DDS, PhD 3 Purpose: The purpose of this study was
A Study of 25 Zygomatic Dental Implants with 11 to 49 Months Follow-up After Loading Fredrik Ahlgren, DDS, MSc 1 / Kjell Størksen, DDS 2 /Knut Tornes, DDS, PhD 3 Purpose: The purpose of this study was
vitality meets bone volume around dental implants Straumann BoneCeramic
 vitality meets bone volume around dental implants Straumann BoneCeramic The vitality you need around your implants Bone volume restoration and preservation for the desired esthetic outcome Image by PD
vitality meets bone volume around dental implants Straumann BoneCeramic The vitality you need around your implants Bone volume restoration and preservation for the desired esthetic outcome Image by PD
Claims submission simplified for emergency dental procedure codes
 January 2002 No. 2002-02 PHC 1844 To: Dentists HMOs and Other Managed Care Programs Claims submission simplified for emergency dental procedure codes Effective immediately, both electronic and paper claims
January 2002 No. 2002-02 PHC 1844 To: Dentists HMOs and Other Managed Care Programs Claims submission simplified for emergency dental procedure codes Effective immediately, both electronic and paper claims
While the prosthetic rehabilitation of
 Restoring Mandibular Single Teeth with the Inclusive Tooth Replacement Solution Go online for in-depth content by Bradley C. Bockhorst, DMD While the prosthetic rehabilitation of full-arch cases provides
Restoring Mandibular Single Teeth with the Inclusive Tooth Replacement Solution Go online for in-depth content by Bradley C. Bockhorst, DMD While the prosthetic rehabilitation of full-arch cases provides
Don t Let Life Pass You By Because Of Missing Teeth
 Don t Let Life Pass You By Because Of Missing Teeth Ask For Dental Implant Solutions From BIOMET 3i Scan With Your Smartphone! In order to scan QR codes, your mobile device must have a QR code reader installed.
Don t Let Life Pass You By Because Of Missing Teeth Ask For Dental Implant Solutions From BIOMET 3i Scan With Your Smartphone! In order to scan QR codes, your mobile device must have a QR code reader installed.
Ridge Reconstruction for Implant Placement
 Volume 1, No. 5 July/August 2009 The Journal of Implant & Advanced Clinical Dentistry Ridge Reconstruction for Implant Placement 2 Hours of CE Credit Oral Implications of Cancer Chemotherapy Immediate
Volume 1, No. 5 July/August 2009 The Journal of Implant & Advanced Clinical Dentistry Ridge Reconstruction for Implant Placement 2 Hours of CE Credit Oral Implications of Cancer Chemotherapy Immediate
Implant rehabilitation in the edentulous jaw: the All-on-4 immediate function concept
 Implant rehabilitation in the edentulous jaw: the All-on-4 immediate function concept By Christopher CK Ho, BDS (Hons), Grad.Dip.Clin.Dent (Implants), M.Clin.Dent (Pros) The All-on-4 technique involves
Implant rehabilitation in the edentulous jaw: the All-on-4 immediate function concept By Christopher CK Ho, BDS (Hons), Grad.Dip.Clin.Dent (Implants), M.Clin.Dent (Pros) The All-on-4 technique involves
Dental Bone Grafting Options. A review of bone grafting options for patients needing more bone to place dental implants
 Dental Bone Grafting Options A review of bone grafting options for patients needing more bone to place dental implants Dental Bone Grafting Options What is bone grafting? Bone grafting options Bone from
Dental Bone Grafting Options A review of bone grafting options for patients needing more bone to place dental implants Dental Bone Grafting Options What is bone grafting? Bone grafting options Bone from
Introduction to Dental Anatomy
 Introduction to Dental Anatomy Vickie P. Overman, RDH, MEd Continuing Education Units: N/A This continuing education course is intended for dental students and dental hygiene students. Maintaining the
Introduction to Dental Anatomy Vickie P. Overman, RDH, MEd Continuing Education Units: N/A This continuing education course is intended for dental students and dental hygiene students. Maintaining the
Survival Analysis of Dental Implants. Abstracts
 Survival Analysis of Dental Implants Andrew Kai-Ming Kwan 1,4, Dr. Fu Lee Wang 2, and Dr. Tak-Kun Chow 3 1 Census and Statistics Department, Hong Kong, China 2 Caritas Institute of Higher Education, Hong
Survival Analysis of Dental Implants Andrew Kai-Ming Kwan 1,4, Dr. Fu Lee Wang 2, and Dr. Tak-Kun Chow 3 1 Census and Statistics Department, Hong Kong, China 2 Caritas Institute of Higher Education, Hong
Spedding Dental Clinic. 73 Warwick Road Carlisle CA1 1EB T: 01228 521889 www.speddingdental.co.uk
 DENTAL IMPLANTS Spedding Dental Clinic 73 Warwick Road Carlisle CA1 1EB T: 01228 521889 www.speddingdental.co.uk SPEDDING DENTAL CLINIC Jack Spedding is a partner in Spedding dental clinic. He is a highly
DENTAL IMPLANTS Spedding Dental Clinic 73 Warwick Road Carlisle CA1 1EB T: 01228 521889 www.speddingdental.co.uk SPEDDING DENTAL CLINIC Jack Spedding is a partner in Spedding dental clinic. He is a highly
INTERNATIONAL MEDICAL COLLEGE
 INTERNATIONAL MEDICAL COLLEGE Joint Degree Master Program: Implantology and Dental Surgery (M.Sc.) Basic modules: List of individual modules Basic Module 1 Basic principles of general and dental medicine
INTERNATIONAL MEDICAL COLLEGE Joint Degree Master Program: Implantology and Dental Surgery (M.Sc.) Basic modules: List of individual modules Basic Module 1 Basic principles of general and dental medicine
Course Curriculum for the Master Degree in Dentistry/Orthodontics
 Jordan University of Science and Technology Faculty of Graduate Studies Course Curriculum for the Master Degree in Dentistry/Orthodontics The Master Degree in Dentistry/ Orthodontics is awarded by the
Jordan University of Science and Technology Faculty of Graduate Studies Course Curriculum for the Master Degree in Dentistry/Orthodontics The Master Degree in Dentistry/ Orthodontics is awarded by the
Teeth and Dental Implants: When to save, and when to extract.
 Teeth and Dental Implants: When to save, and when to extract. One of the most difficult decisions a restorative dentist has to make is when to refer a patient for extraction and placement of dental implants.
Teeth and Dental Implants: When to save, and when to extract. One of the most difficult decisions a restorative dentist has to make is when to refer a patient for extraction and placement of dental implants.
Retrospective analysis of factors influencing the eruption of delayed permanent incisors after supernumerary tooth removal
 Retrospective analysis of factors influencing the eruption of delayed permanent incisors after supernumerary tooth removal R.A.E. BRYAN*, B.O.I. COLE**, R.R. WELBURY* ABSTRACT. Aim This was to assess the
Retrospective analysis of factors influencing the eruption of delayed permanent incisors after supernumerary tooth removal R.A.E. BRYAN*, B.O.I. COLE**, R.R. WELBURY* ABSTRACT. Aim This was to assess the
Periodontal surgery report for crown lengthening of tooth number 24,25
 411 PDS Periodontal surgery report for crown lengthening of tooth number -Course director : Dr. Nahid Ashri - instructor: Dr.Fatin Awaratani - - Student Name: Hanadi Alyami Computer Number: K S U - D E
411 PDS Periodontal surgery report for crown lengthening of tooth number -Course director : Dr. Nahid Ashri - instructor: Dr.Fatin Awaratani - - Student Name: Hanadi Alyami Computer Number: K S U - D E
More than a fixed rehabilitation.
 More than a fixed rehabilitation. A reason to smile. In combination with: Patient expectations drive dental treatments for fixed edentulous immediate restorations. Patients today have increasingly high
More than a fixed rehabilitation. A reason to smile. In combination with: Patient expectations drive dental treatments for fixed edentulous immediate restorations. Patients today have increasingly high
Improving Esthetics with Sequential Treatment Planning and Implant-Retained Dentures
 Improving Esthetics with Sequential Treatment Planning and Implant-Retained Dentures by Timothy F. Kosinski, DDS, MAGD While oral function is the primary concern for most patients, the importance of esthetics
Improving Esthetics with Sequential Treatment Planning and Implant-Retained Dentures by Timothy F. Kosinski, DDS, MAGD While oral function is the primary concern for most patients, the importance of esthetics
Dental Implants and Esthetics
 Dental Implants and Esthetics Charles J. Goodacre, DDS, MSD; Chad J. Anderson, MS, DMD Continuing Education Units: 1 hour Online Course: www.dentalcare.com/en-us/dental-education/continuing-education/ce203/ce203.aspx
Dental Implants and Esthetics Charles J. Goodacre, DDS, MSD; Chad J. Anderson, MS, DMD Continuing Education Units: 1 hour Online Course: www.dentalcare.com/en-us/dental-education/continuing-education/ce203/ce203.aspx
Congenital absence of mandibular second premolars
 CLINICIAN S CORNER Congenitally missing mandibular second premolars: Clinical options Vincent G. Kokich a and Vincent O. Kokich b Seattle, Wash Introduction: Congenital absence of mandibular second premolars
CLINICIAN S CORNER Congenitally missing mandibular second premolars: Clinical options Vincent G. Kokich a and Vincent O. Kokich b Seattle, Wash Introduction: Congenital absence of mandibular second premolars
Human, Male, White. Bone Clones Osteological Evaluation Report. Product Number: 1 intact mandible. General observations:
 Human, Male, White Product Number: Specimen Evaluated: Skeletal Inventory: BC-107 Bone Clones replica 1 intact cranium 1 intact mandible General observations: In general, the molding process has preserved
Human, Male, White Product Number: Specimen Evaluated: Skeletal Inventory: BC-107 Bone Clones replica 1 intact cranium 1 intact mandible General observations: In general, the molding process has preserved
Dental Implant Options in Atrophic Jaws
 Dental Implant Options in Atrophic Jaws Orthopedic Application Jay B. Reznick, D.M.D., M.D. Diplomate, American Board of Oral and Maxillofacial Surgery Tarzana, CA Endopore Dental Implant System Screw-Type
Dental Implant Options in Atrophic Jaws Orthopedic Application Jay B. Reznick, D.M.D., M.D. Diplomate, American Board of Oral and Maxillofacial Surgery Tarzana, CA Endopore Dental Implant System Screw-Type
Classification of Malocclusion
 Classification of Malocclusion What s going on here? How would you describe this? Dr. Robert Gallois REFERENCE: Where Do We Begin? ESSENTIALS FOR ORTHODONTIC PRACTICE By Riolo and Avery Chapter 6 pages
Classification of Malocclusion What s going on here? How would you describe this? Dr. Robert Gallois REFERENCE: Where Do We Begin? ESSENTIALS FOR ORTHODONTIC PRACTICE By Riolo and Avery Chapter 6 pages
Dental Implant Treatment after Improvement of Oral Environment by Orthodontic Therapy
 Dental implant treatment after impr Title environment by orthodontic therapy. Sekine, H; Miyazaki, H; Takanashi, Author(s) Matsuzaki, F; Taguchi, T; Katada, H Journal Bulletin of Tokyo Dental College,
Dental implant treatment after impr Title environment by orthodontic therapy. Sekine, H; Miyazaki, H; Takanashi, Author(s) Matsuzaki, F; Taguchi, T; Katada, H Journal Bulletin of Tokyo Dental College,
Straumann Dental Implant System. Implant Selection Guide.
 Straumann Dental Implant System. Implant Selection Guide. STRAUMANN's IMPLANT PORTFOLIO The Straumann Dental Implant System offers two implant lines with diverse body and neck designs ranging from the
Straumann Dental Implant System. Implant Selection Guide. STRAUMANN's IMPLANT PORTFOLIO The Straumann Dental Implant System offers two implant lines with diverse body and neck designs ranging from the
Outcomes of Placing Short Dental Implants in the Posterior Mandible: A Retrospective Study of 124 Cases
 DENTAL IMPLANTS J Oral Maxillofac Surg 67:713-717, 2009 Outcomes of Placing Short Dental in the Posterior Mandible: A Retrospective Study of 124 Cases Bao-Thy N. Grant, DDS,* Franklin X. Pancko, DDS, and
DENTAL IMPLANTS J Oral Maxillofac Surg 67:713-717, 2009 Outcomes of Placing Short Dental in the Posterior Mandible: A Retrospective Study of 124 Cases Bao-Thy N. Grant, DDS,* Franklin X. Pancko, DDS, and
Alveolar Width Distraction Osteogenesis for Early Implant Placement
 J Oral Maxillofac Surg 63:1724-1730, 2005 Alveolar Width Distraction Osteogenesis for Early Implant Placement Zvi Laster, DDS,* Adi Rachmiel, DDS, and Ole T. Jensen, DDS, MS Distraction osteogenesis for
J Oral Maxillofac Surg 63:1724-1730, 2005 Alveolar Width Distraction Osteogenesis for Early Implant Placement Zvi Laster, DDS,* Adi Rachmiel, DDS, and Ole T. Jensen, DDS, MS Distraction osteogenesis for
DENTAL IMPLANTS DR JEBIN,MDS.,D.ICOI
 Good Morning DENTAL IMPLANTS DR JEBIN,MDS.,D.ICOI What is implant? A dental implant is an artificial root that replaces the natural tooth root. Crown Gum Implant Tooth Root Jawbone Parts of implant Cover
Good Morning DENTAL IMPLANTS DR JEBIN,MDS.,D.ICOI What is implant? A dental implant is an artificial root that replaces the natural tooth root. Crown Gum Implant Tooth Root Jawbone Parts of implant Cover
2016 Buy Up Dental Care Plan Procedure List
 * This is in addition to the embedded Preventive Plan (see procedure list at deltadentalco.com/kp_preventive. BASIC SERVICES Minor Restorative Services D2140 Amalgam 1 surface, primary or permanent D2150
* This is in addition to the embedded Preventive Plan (see procedure list at deltadentalco.com/kp_preventive. BASIC SERVICES Minor Restorative Services D2140 Amalgam 1 surface, primary or permanent D2150
Dr. Park's Publications
 Dr. Park's Publications Jae Hyun Park, D.M.D., M.S.D., M.S., Ph.D. Diplomate, American Board of Orthodontics Editor-in-Chief, Pacific Coast Society of Orthodontists Chief Editor, Computed Tomography: New
Dr. Park's Publications Jae Hyun Park, D.M.D., M.S.D., M.S., Ph.D. Diplomate, American Board of Orthodontics Editor-in-Chief, Pacific Coast Society of Orthodontists Chief Editor, Computed Tomography: New
Periapical radiography
 8 Periapical radiography Periapical radiography describes intraoral techniques designed to show individual teeth and the tissues around the apices. Each film usually shows two to four teeth and provides
8 Periapical radiography Periapical radiography describes intraoral techniques designed to show individual teeth and the tissues around the apices. Each film usually shows two to four teeth and provides
Luigi Vito Stefanelli,D.Eng.,DDS
 LYON, 27-28/09/2013 Luigi Vito Stefanelli,D.Eng.,DDS Assistant Researcher, Department of Oral Sciences, Sapienza University of Rome, Italy, School of Dentistry. Private practitioner dental office Stasi
LYON, 27-28/09/2013 Luigi Vito Stefanelli,D.Eng.,DDS Assistant Researcher, Department of Oral Sciences, Sapienza University of Rome, Italy, School of Dentistry. Private practitioner dental office Stasi
Single anterior tooth replacement: clinical approaches
 Single anterior tooth replacement: clinical approaches Paul Swanson examines the role of implant design in approaching a range of treatment protocols for replacing a single tooth Case 1 Figure 1: Patient
Single anterior tooth replacement: clinical approaches Paul Swanson examines the role of implant design in approaching a range of treatment protocols for replacing a single tooth Case 1 Figure 1: Patient
Cone Beam Imaging Why all the Fuss about the X-ray Dose? D.A. Miles BA, DDS, MS, FRCD(C) Dip. ABOM, Dip. ABOMR. Introduction
 Dip. ABOM, Dip. ABOMR. Introduction") Cone Beam Imaging Why all the Fuss about the X-ray Dose? D.A. Miles BA, DDS, MS, FRCD(C) Dip. ABOM, Dip. ABOMR Introduction The newest imaging modality to become available to dentists is making its impact
Cone Beam Imaging Why all the Fuss about the X-ray Dose? D.A. Miles BA, DDS, MS, FRCD(C) Dip. ABOM, Dip. ABOMR Introduction The newest imaging modality to become available to dentists is making its impact
Coding and Payment Guide for Dental Services. A comprehensive coding, billing, and reimbursement resource for dental services
 Coding and Payment Guide for Dental Services A comprehensive coding, billing, and reimbursement resource for dental services 2011 Contents Introduction...1 Coding Systems... 1 Claim Forms... 2 Contents
Coding and Payment Guide for Dental Services A comprehensive coding, billing, and reimbursement resource for dental services 2011 Contents Introduction...1 Coding Systems... 1 Claim Forms... 2 Contents
Maxillary sinusitis of odontogenic origin: cone-beam volumetric computerized tomography aided diagnosis
 Maxillary sinusitis of odontogenic origin: cone-beam volumetric computerized tomography aided diagnosis Umadevi P. Nair, DMD, MDS, a and Madhu K. Nair, DMD, MS, PhD, b Gainesville, Florida UNIVERSITY OF
Maxillary sinusitis of odontogenic origin: cone-beam volumetric computerized tomography aided diagnosis Umadevi P. Nair, DMD, MDS, a and Madhu K. Nair, DMD, MS, PhD, b Gainesville, Florida UNIVERSITY OF
Friday 29 th April 2016
 8.00 9.00 Registration and coffee/bread 9.00 9.45 1. Status of Dental Traumatology worldwide. Is prevention realistic? Lars Andersson Presently almost all countries have published data on the dental trauma
8.00 9.00 Registration and coffee/bread 9.00 9.45 1. Status of Dental Traumatology worldwide. Is prevention realistic? Lars Andersson Presently almost all countries have published data on the dental trauma
CPD Article ISSUE 15. Proud of our History, Looking Forward to the Future
 CPD Article ISSUE 15 Proud of our History, Looking Forward to the Future BIDST CPD This learning session has been judged as being equivalent to one hour of verifiable CPD. To claim your verifiable CPD
CPD Article ISSUE 15 Proud of our History, Looking Forward to the Future BIDST CPD This learning session has been judged as being equivalent to one hour of verifiable CPD. To claim your verifiable CPD