Jeffrey Summers, M.D. Director, Interventional Pain Division NewSouth NeuroSpine Flowood, MS
|
|
|
- Ginger Beverley Shelton
- 8 years ago
- Views:
Transcription
1 Jeffrey Summers, M.D. Director, Interventional Pain Division NewSouth NeuroSpine Flowood, MS

2 Partial ownership in a medical service company that primarily sells DME, none of which has pain management applications. Includes compounding pharmaceutical services which produce topical analgesic creams.

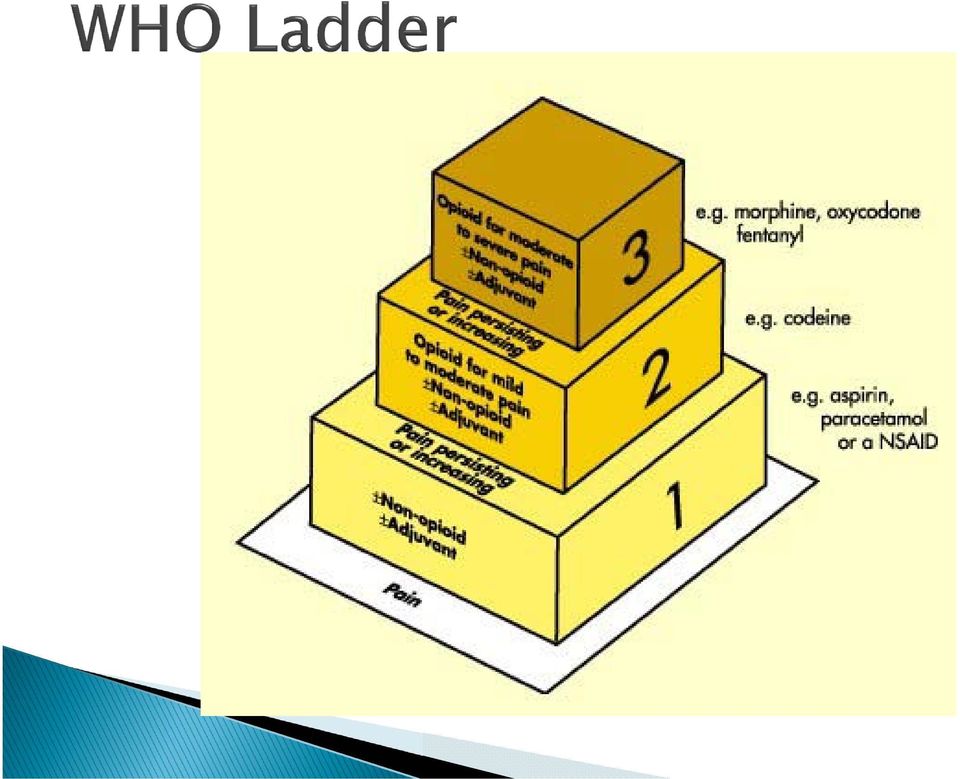
3 WHO ladder Chronic Opiod therapy Non-Opiod pain management Pharmacological p.o. topical Injections Physical Medicine Surgical options Implantable devices

4
5 Scope of the Problem

6 Number of people with chronic pain exceeds that of diabetes, heart disease and cancer COMBINED Institute of Medicine million people with chronic pain in the US but only 4000 pain specialists

7 American Pain Foundation 50% of patients with severe pain are under treated American Academy of Pain Medicine 80% of people in nursing homes have under treated pain World Health Organization (WHO) Under treatment of pain is the #1 health problem in the US
 Under treatment of pain is the #1 health")
8 But it s NOT because we aren t prescribing enough narcotics

9 United States has 4.6% of the world s population United States consumes over 80% of the world s opioid (narcotic) pain medication The milligram per person use of prescription narcotics in the United States increased 402%, between 1997 and 2007.

10 Average annual per capita consumption of morphine North America (US and Canada) 75mg 750x India (0.1 mg) 375x Nepal (0.2mg) 12x worldwide (6mg) India and Nepal are the major supplies of opium to the U.S.
 12x worldwide (6mg) India and Nepal are the")
11 Narcotics are now the most widely prescribed group of drugs in the USA (passing, antidepressants). 15% to 20% of the meetings between a doctor and a patient in the USA result in a prescription of narcotics.

12 aka Lorcet, Lortab, Vicoden, Norco Hydrocodone is the #1 prescribed pain medicine in the U.S. Hydrocodone is the #1 prescribed drug of any kind in the U.S. 99% of the hydrocodone produced in the world is consumed in the U.S.

13 81 medications in the U.S. contain hydrocodone The U.S. population in 2011 was 311 million In 2011, hydrocodone was Rx to 47 million different patients in the U.S.

14 40% Primary Care physicians 10% by Dentists 3% by Anesthesiologists specializing in treatment of pain

15 Musculoskeletal and connective tissue-26% Respiratory- 21% Fractures, sprains, contusions, injuries 19%

16 Fact: Good doctors prescribe narcotics What about the patients with chronic pain who need narcotics? Who does need chronic narcotics? What do narcotics do?

17 They do not treat the cause of the pain They attach to specific receptors in the brain, spinal cord and gastrointestinal tract Interfere with and prevent the transmission of pain signals to the brain Alter the brain s perception of pain But do they work???

18 Comprehensive literature review 2011 Evaluate the clinical effectiveness of narcotics in chronic non-cancer pain Manchikanti L, Pain Physician 2011;14;E133-E156

19 90% of patients who present to pain centers are taking opiods Paucity of literature for multiple drugs and multiple conditions of non-cancer pain Evidence weak for pain relief with improvement in functional status Only drug with high level evidence of effectiveness: Tramadol for arthritis Conclusion: There is a lack of literature on longterm therapy; thus, opioid therapy should be provided with great restraint and caution

20 Focused Review Chronic non-cancer pain treatment with narcotics Manchikanti et al, Pain Physician, 2011;14;E103-E117

21 Transient exacerbation of pain experienced by individuals who have relatively stable and adequately controlled baseline cancer pain Literature for breakthrough pain in chronic non-cancer pain including its terminology, prevalence, relevance, characteristics, and treatments, has been poorly described
22 There is no significant evidence for any type of breakthrough pain in chronic non-cancer pain based on available literature, methodology utilized, and response to opioids in chronic non-cancer pain.
23 Why has there been an explosion in the use and abuse of prescription pain medicine?
24 Changes by the medical community in the pharmacological approach to chronic pain resulted in increased acceptance of the use of controlled substances in the management of pain Changes in State law allowed improved freedom to prescribe controlled substances These same laws made it easier to prescribe controlled substances for illicit purposes
25 Previously rogue internet pharmacies were the prime source of improperly obtained prescription pill medicine. Abusers could contact a pharmacy who would connect them with an internet doctor who could diagnose and treat (with controlled substances) without ever seeing or examining the patient
26 The epidemic of rogue free standing pain clinics ( Pill Mills ) started after the Ryan Haight Act legislation in 2008 made it illegal for a doctor to prescribe medication to a patient without at least one face to face meeting.
27 WHEN IS A PAIN CLINIC PILL MILL?
28 Goal is functional restoration Treatment that is unsuccessful is discontinued Multiple consultations if goals not met The cause of the pain is treated Legit Clinics Goal is pain relief Treatment that is unsuccessful is increased No outside consultation The symptom of pain is treated Pill Mills
29 Multiple Specialists Anesthesiologists Neurologists Physical Medicine Psychology/psychiatry Multiple treatments Physical therapy Injection therapy Surgery Pharmacological Real Clinics Often one specialty or multiple specialties that have no specific training in the management of chronic pain Treatment is exclusively pharmacological Pill Mills
30 The physicians in your clinic are a pediatrician, radiologist, pathologist and two allergists that specialize in the treatment of chronic pain The cars in your parking lot have twice as many out-of-state tags as in state ones
31 the Hybrid Pill Mill
32 Pill Mill Hybrid Pill Mill All pills, all the time Cash only Gives pills to keep customers coming back for other treatment-injections, physical therapy etc. Will take insurance for treatments, but if you want pills, you better have your deductible and co-payments met
33 Pills not the primary form of treatment, but are used to keep patients coming back--and paying bills Often numerous, expensive treatments, such as injections-often dozens if not hundredsthat never help or never help for long. BUT--if you want pills, you have to be willing to participate with other treatments or you are refusing the physician s recommendations and may be drug seeking.
34 Starting a Sonic Drive-In or a fully operational pain clinic?
35 Building up to code Employer ID Number (EIN) Vendor s License Annual inspections by State Department of Health Franchise License Seller s Permit Food Service License Sign Permit Music License
36 The image part with relationship ID rid2 was not found in the file. : If operating out of a clinic: Building Permit: Yes EIN: Yes CON-None Facility credentialing-none
37 Pain Management Specialists
38 M.D. or D.O. degree Additional requirements NOTHING!!
39 M.D. or D.O. degree Victims!! BUT--Neurosurgeons can only operate in a hospital, which requires hospital privileges Pain clinics do not require a hospital or ASM, because in most states they can operate in a office setting.
40 ABMS has recognized an Added Qualifications in Pain Management certification since 1992 MUST have a primary Board certification in: Anesthesiology Physical Medicine and Rehabilitation Neurology Psychiatry Written exam, certification must be renewed every 10 years You DO NOT need a board certification in anything to call yourself a pain specialist
41 PAIN SPECIALTISTS
42 Your waiting room is so full, and you have a line of patients that snakes into the parking lot You have armed security personnel guarding your clinic.
43 Consider the Side effects
44 Overdose/death Addiction Dependence Endocrine dysfunction Immunosuppression Infectious disease Opioid-induced hyperalgesia
45 Acute Unresponsive to non-narcotics Progressive
46 Review of 45,432 patients (IARS) who underwent colon surgery, GB removal, hysterectomy, hip replacement Studied patients experiencing opiod-related side effects (nausea/vomiting, itching, urinary retention, constipation, respiratory depression) Are the side effects minor? Are there significant consequences?
47 Costs increased from $17,281 to $18,309 per stay Length of stay increased from 4.1 days to 5.2 days
48 Low Tes Loss of libido, infertility, erectile dysfunction, fatigue, depression, anxiety, loss of muscle strength/mass, osteoporosis, compression fractures More likely with continuous release preparations (OxyContin, Fentanyl patch, Oramorph, Exalgo, ER, XR, XL, CR, MR $$$) Katz. Clin J Pain 2008
49 The Risks A higher risk of the pain becoming chronic A higher risk of long-term disability Higher medical costs overall A greater risk of surgery being conducted on the patient A greater risk of narcotics being used later in the patient s life.
50 5 th Liver disease/cirrhosis 4 th COPD 3 rd Accidental injury (MVA) 2 nd Heart disease 1 st Cancer azdh.gov 2000
51 5 th COPD 4 rd Accidental injury (MVA) 3 nd Heart disease 2 st Cancer 1 st Accidental drug overdose (up 390%) CDC
52 Defined as a state of pain receptor sensitization caused by exposure to opiods Paradoxical response whereby a patient receiving opioids for the treatment of pain becomes more sensitive to certain painful stimuli Lee et al, A comprehensive review of opioid-induced hyperalgesia, Pain Physician 2011 Mar-Apr;14(2):145-61
53 Paradoxical effect of opiods causing a centralized increase in the level of pain experienced Higher doses of opioids may stimulate rather than inhibit the central nervous system Characterized by increasing pain causing doctors to escalating narcotic doses, which results in a worsening of the patients pain and condition Mercadante S Hyperalgesia: An Emerging Iatrogenic Syndrome, J Pain Symptom Manage 2003 Aug;26(2):769-75
54 Opioid treatment's effect seems to wane in the absence of disease progression Unexplained pain reports or diffuse allodynia (pain from a stimulus that normally does not cause pain) unassociated with the original pain Increased levels of pain with increasing dosages.
55 Detoxification Reduction of narcotic dose Narcotic rotation Treat with NMDA receptor antagonists (Meperidine, Methadone, Tramadol, Ketamine, Dextromethorphan, phencyclidine (PCP) Sublingual buprenorphine (Suboxone)
56 No consensus Most teaching centers consider the evidence to be strong that narcotics can be effective in the management of chronic pain.
57
58 Research What is the goal/purpose? What are the inclusion and exclusion criteria? What are the methods? What are the results? Discussion
59 Goals Reduction of pain Improvement in function Inclusion/exclusion criteria Patient s baseline health, co-morbidities History of addiction, etc Methods What drugs did you use and in what amounts
60 Results Is the pain better? Can they do more? Discussion Does the patient know the risks? Does the patient know how you expect them to take the drugs (opiod maintenance agreement)? Is there an endpoint?
61 Is the patient having side effects? Is the patient reporting less pain? Does increasing the dose lower the pain? MOST IMPORTANTLY Can they do more when they take the drug?
62 Pharmacological Physical medicine Active PT (stretching, conditioning, strengthening, etc) Passive PT(heat/cold, ultrasound, TENS, massage, etc) Injections Spinal (epidural, caudal, facet) Joints Sympathetic (RSD, causalgia, CRPS)
63 NSAIDs Anti-Epileptic drugs (AEDs) Anti-Depressant drugs (ADs) Local Anesthetics Neuroleptics
64 Nociceptive pain due to tissue damage Intact nervous system is doing its job Neuropathic pain Pain propagated by damage or injury to the nervous system (radiculopathy, diabetic neuropathy, post herpetic neuralgia) Pain maintained by abnormal activity in the nervous system (CRPS aka RSD)
65 Narcotics are most effective for treatment of nociceptive pain Least effective (in typical therapeutic doses) for neuropathic pain
66 Adjuvant medications are indicated as front line drugs for the treatment of neuropathic pain Anti epileptic drugs Anti-depressant drugs Local anesthetics (injected, topical, p.o.)
67 Act via suppression of ectopic pain impulses at the spinal cord level Decreasing conductance in Na+ channels and inhibiting ectopic discharges Prevent neuroplastic changes Neuroplasticity- pathophysiological and biochemical changes in the nervous system to adapt morphologically and functionally to external stimuli as a result of an injury. Plays a crucial role in the onset and maintenance of pain symptoms. Tremont-Lukats Drugs Nov;60(5):
68 Carbamazepine (Tegretol) Gabapentin (Neurontin) Pregabalin (Lyrica) Topiramate (Topomax) Valproic Acid (Depakote) Lamotrigine (Lamictal) Levetiracetam (Keppra) Oxcarbazepine (Trileptal)
69 First anticonvulsant studied in clinical trials Probably alleviates pain by decreasing conductance in Na+ channels and inhibiting ectopic discharges. Results from clinical trials have been positive in the treatment of trigeminal neuralgia, painful diabetic neuropathy and postherpetic neuralgia
70 Haplotype testing recommended for Asians due to the risk of Stevens-Johnson Syndrome/toxic epidermal necrolysis. Aplastic anemia Leukopenia WBC monitoring recommended
71 Has the most clearly demonstrated analgesic effect for the treatment of neuropathic pain. Studies demonstrate efficacy in the treatment of painful diabetic neuropathy and postherpetic neuralgia. Based on the positive results of clinical studies and its favorable adverse effect profile, gabapentin should be considered the first choice of therapy for neuropathic pain.
72 Not metabolized, so no enzyme induction, or development of tolerance Minimal drug interactions Renal elimination Overdose potential limited by inability of gut to absorb more than 1200 mg per dose Side effects usually mild and reversible Sedation Nausea, diarrhea, constipation Loss of balance or coordination Blurred vision Peripheral edema
73 Do NOT affect GABA receptor nor GABA production Binds to alpha2delta receptor Decrease release of neurotransmitters Glutamate Norepinephrine Substance P Calcitonin GRP
74 Profile similar to gabapentin May have an earlier onset of analgesia (at lower blood levels) than gabapentin Negligible metabolism, enzyme induction or tolerance Drugs interactions potentiation of sedation with CNS depressants For neuropathic pain (not fibro) try gabapentin first due to cost considerations Schedule V
75 Studies showed it was ineffective for Tx of HIV associated peripheral neuropathy Pregabalin is also used off-label for the treatment of Perioperative pain Migraine Used in lieu of benzodiazepines for somatic anxiety symptoms
76 Studies have demonstrated effectiveness in the treatment of neuropathic pain related to diabetic peripheral neuropathy and postherpetic neuralgia June 2007 became the first drug approved by FDA for treatment of fibromyalgia
77 Update product labeling to include a warning about an increased risk of suicidal thoughts or actions Develop a Medication Guide to help patients understand this risk. These changes affect all approved AEDs except those indicated only for short-term use All patients who currently are taking or starting on any antiepileptic drug for any indication should be monitored for notable changes in behavior that could indicate the emergence or worsening of suicidal thoughts or behavior or depression.
78 Studied extensively in the treatment of chronic pain, particularly neuropathic pain Have an analgesic effect independent of their anti-depressant properties Analgesic benefit earlier onset than anti depressant effect Effective analgesic dose is usually lower than the anti-depressant dose Analgesic effect related to inhibition of uptake of neurotranmitters (seritonin, norepinephrine, dopamine) in the descending (pain) inhibitory tracts of the brain and spinal cord
79 Tricyclic antidepressants SSRI (selective serotonin reuptake inhibitors) SNRI (serotonin norepinephrine reuptake inhibitors) SARIs (serotonin antagonist and reuptake inhibitors) NDRIs (norepineprine-dopamine reuptake inhibitors) MAOIs (monamine oxidase inhibitors) TeCAs (tetracyclic antidepressants)
80 Best studied of the ADs for the treatment of chronic pain Work on seritonin, norepinephrine and dopamine Significant anti-cholinergic effects Studies suggests effectiveness in multiple pain states Neuropathic pain (PHN, DPN) Fibromyalgia Headache
81 Amitriptyline, Nortriptyline, Desipramine Imipramine Affect DA, NE and serotonin levels
82 Multiple drug interactions Sedation Cardiac conduction abnormalities Orthostatic hypotension (falls) Tachycardia Weight gain amitriptyline 20 mg dose ave 3.6kg wt gain Amitriptyline contraindicated in elderly
83 The dirtier (DA, NE, 5 HT) the more analgesic benefit The dirtier the more side effects Tricyclics have good evidence of efficacy, but have high SA profiles SSRIs weak evidence of efficacy, low SA profiles SNRIs-better efficacy, lower SA, good starting point
84 Duloxetine (Cymbalta) Venlafaxine (Effexor) Desvenlafaxine (Pristiq) Milnacipran (Sevella) Tramadol (Ultram)
85 The only piece of medical equipment in your office is a scale. Your office is in a strip mall in which the largest building is your pharmacy.
86 Side effects: GI Renal CVA? MI? Route oral, IV, topical
87 Diclofenac-biochemical profile favorable for local absorption Available as: Gel (Voltaren, Selaraze) Drops (Pennsaid) Patch (Flector)
88 Bioavailability: 5-10% of oral route Plasma concentration: 15-25% of oral drug Oral NSAID: 15+% incidence of GI side effects Topical: <8% incidence of GI issues same as placebo
89 Carisoprodol (Soma) Cyclobenzaprine (Flexeril) Metaxalone (Skelaxin) Chlorzoxazone (Parafon Forte ) Methocarbamol (Robaxin) McIntosh G, Hall H (2008). Low back pain (acute), May BMJ Clinical Evidence
90 Half your patients spend the night before their appointment sleeping in their car in your parking lot. You ve prescribed for the Hydrocodone + Xanax + SOMA combination so much your pharmacy dispenses it as a Party Pack.
91 Local anesthetic Nerve blocks Sympathetic blocks Trigger point injections Steroid Epidural Joint Limbs Spine (Facets, Sacroiliac)
92 Generally poor evidence of long term efficacy with joint injections regardless of region injected (shoulder, hip, knee, spine) Paucity of studies investigating efficacy for intra-spinal (epidural) injections involving the cervical or thoracic spines. Generally low level evidence of long term benefit with intralaminar epidural injections Good evidence of efficacy with transforaminal epidural injections
93 Surgery sparing effect Analgesia often wanes with time requirement repeat procedures Frequency of repeat procedures ultimately defines if the procedures are indicated
94 You see 80 new patients on a slow day None of the doctors in your clinic are listed on the sign in front of the clinic
95 Neurodestructive procedures Rhizotomy Dorsal root entry zone lesions (DREZ) Cingulotomy Cordotomy Implantable Devices Continuous infusion pump Spinal cord/dorsal column stimulator
96 Indications Radiculopathy CRPS Peripheral neuropathy Phantom limb pain Post herpetic neuralgia Headaches Axial back/neck pain
97 Radiating leg (or arm) pain from nerve injury Vascular disease (RSD/CRPS), angina Ischemic peripheral vascular disease Neuropathy Phantom pain syndrome Failed back surgery syndrome Axial back pain (on the spine non radiating) Pelvic/visceral pain
98 North et al, SCS for neuropathic LBP 2.3 year follow up after device implanted Rigid exclusion criteria
99 Neurogenic back pain Constant No association with movement No association with position Not coming from pain sensors (nociceptors) but from the injured nerves themselves Not for mechanical low back pain (muscles, facets, sacroiliac joint, sprain/strain)
100 Physiologic contraindication (mechanical LBP) Abnormal Pain Behavior Unresolved psychiatric illness Unresolved issues of secondary gain Inappropriate medication use
101 Pain improvement- 53% had 50+% relief 12% increased pain Side effects Decreased sense of touch 47% Decreased strength/coordination 53% Bladder/bowel control problems 12%
102 Use of medicine 41% decreased pain medicine use 53% increased medicine use Return to work 40% working before SCS 35% working after SCS i.e., 15% of workers who received SCS did not RTW after implantation
103 HAVE Radiating leg pain from nerve injury Vascular disease (RSD/CRPS), Angina Ischemic peripheral vascular disease Neuropathy DON T HAVE Axial (non-radiating pain) Psyche issues Secondary gain
104 The contents in the 4 pockets of your white doctor s coat are a prescription pad, two Montblanc pens, 6 Powerball tickets and a Glock The delivery vehicle for your in office pharmacy is a Brinks Armored Car
105 Your patients take so much hydrocodone, they ask you if the pre-starch binder in the pills could be the reason they ve gained so much weight on their Low Carb diet Your business model for choosing analgesic drug therapies is based on Burger King s Have it your way campaign.
106 You practice in the South but there are twice as many vans or buses in the parking lot than pick-up trucks or SUVs Your follow-up appointment cards for existing patients say: First come, first served.
107 On your office s new patient intake forms the block for the accepted insurance plans lists only: Cash
108 THANK YOU!
Medications for chronic pain
 Medications for chronic pain When it comes to treating chronic pain with medications, there are many to choose from. Different types of pain medications are used for different pain conditions. You may
Medications for chronic pain When it comes to treating chronic pain with medications, there are many to choose from. Different types of pain medications are used for different pain conditions. You may
POST-TEST Pain Resource Professional Training Program University of Wisconsin Hospital & Clinics
 POST-TEST University of Wisconsin Hospital & Clinics True/False/Don't Know - Circle the correct answer T F D 1. Changes in vital signs are reliable indicators of pain severity. T F D 2. Because of an underdeveloped
POST-TEST University of Wisconsin Hospital & Clinics True/False/Don't Know - Circle the correct answer T F D 1. Changes in vital signs are reliable indicators of pain severity. T F D 2. Because of an underdeveloped
Drug Class Review Neuropathic Pain
 Drug Class Review Neuropathic Pain Final Update 1 Report June 2011 The Agency for Healthcare Research and Quality has not yet seen or approved this report The purpose of the is to summarize key information
Drug Class Review Neuropathic Pain Final Update 1 Report June 2011 The Agency for Healthcare Research and Quality has not yet seen or approved this report The purpose of the is to summarize key information
What alternatives are there to the use of opioid analgesics in the treatment of chronic pain in light of existing evidence and its limitations?
 What alternatives are there to the use of opioid analgesics in the treatment of chronic pain in light of existing evidence and its limitations? Michael C. Rowbotham, MD Scientific Director California Pacific
What alternatives are there to the use of opioid analgesics in the treatment of chronic pain in light of existing evidence and its limitations? Michael C. Rowbotham, MD Scientific Director California Pacific
Best Practices for Patients With Pain. Commonly Used Over the Counter (OTC) Pain Relievers 5/15/2015
 Pain Relievers 5/15/2015") Faculty Best Practices for Patients With Pain Nancy Bishop, RPh Assistant State Pharmacy Director Alabama Department of Public Health Satellite Conference and Live Webcast Wednesday, May 20, 2015 2:00
Faculty Best Practices for Patients With Pain Nancy Bishop, RPh Assistant State Pharmacy Director Alabama Department of Public Health Satellite Conference and Live Webcast Wednesday, May 20, 2015 2:00
Got Pain? 11/19/2013. Pain Kill Beyond The Pill. Yet it is often inadequately treated.
 Pain Kill Beyond The Pill An Innovative & Personalized Approach to Pain Treatment MAZEN BAISA, PharmD, RPh., MBA, ABAAHP, FAARM, CPE Director of Clinical Services BioMed Specialty Pharmacy Pain Kill Beyond
Pain Kill Beyond The Pill An Innovative & Personalized Approach to Pain Treatment MAZEN BAISA, PharmD, RPh., MBA, ABAAHP, FAARM, CPE Director of Clinical Services BioMed Specialty Pharmacy Pain Kill Beyond
Acute Pain Management in the Opioid Dependent Patient. Maripat Welz-Bosna MSN, CRNP-BC
 Acute Pain Management in the Opioid Dependent Patient Maripat Welz-Bosna MSN, CRNP-BC Relieving Pain in America (IOM) More then 116 Million Americans have pain the persists for weeks to years $560-635
Acute Pain Management in the Opioid Dependent Patient Maripat Welz-Bosna MSN, CRNP-BC Relieving Pain in America (IOM) More then 116 Million Americans have pain the persists for weeks to years $560-635
Test Content Outline Effective Date: June 9, 2014. Pain Management Nursing Board Certification Examination
 Pain Management Nursing Board Certification Examination There are 175 questions on this examination. Of these, 150 are scored questions and 25 are pretest questions that are not scored. Pretest questions
Pain Management Nursing Board Certification Examination There are 175 questions on this examination. Of these, 150 are scored questions and 25 are pretest questions that are not scored. Pretest questions
Lora McGuire MS, RN Educator and Consultant lmcguire@jjc.edu. Barriers to effective pain relief
 Lora McGuire MS, RN Educator and Consultant lmcguire@jjc.edu Barriers to effective pain relief Freedom from pain is a basic human right -WHO Pain is whatever the experiencing person says it is and exists
Lora McGuire MS, RN Educator and Consultant lmcguire@jjc.edu Barriers to effective pain relief Freedom from pain is a basic human right -WHO Pain is whatever the experiencing person says it is and exists
Why are antidepressants used to treat IBS? Some medicines can have more than one action (benefit) in treating medical problems.
 in treating medical problems.") The Use of Antidepressants in the Treatment of Irritable Bowel Syndrome and Other Functional GI Disorders Christine B. Dalton, PA-C Douglas A. Drossman, MD What are functional GI disorders? There are more
The Use of Antidepressants in the Treatment of Irritable Bowel Syndrome and Other Functional GI Disorders Christine B. Dalton, PA-C Douglas A. Drossman, MD What are functional GI disorders? There are more
Pain Management in Palliative and Hospice Care
 Pain Management in Palliative and Hospice Care Donna Butler, MSN, ANP-BC, OCN, ACHPN, FAAPM Current Status of Pain Cancer patients at EOL- 54% have pain AIDS with prognosis < 6mons- intense pain Less research
Pain Management in Palliative and Hospice Care Donna Butler, MSN, ANP-BC, OCN, ACHPN, FAAPM Current Status of Pain Cancer patients at EOL- 54% have pain AIDS with prognosis < 6mons- intense pain Less research
Clinical Algorithm & Preferred Medications to Treat Pain in Dialysis Patients
 Clinical Algorithm & Preferred Medications to Treat Pain in Dialysis Patients Developed by the Mid Atlantic Renal Coalition and the Kidney End of Life Coalition September 2009 This project was supported,
Clinical Algorithm & Preferred Medications to Treat Pain in Dialysis Patients Developed by the Mid Atlantic Renal Coalition and the Kidney End of Life Coalition September 2009 This project was supported,
Opioid Prescribing for Chronic Pain: Guidelines for Marin County Clinicians
 Opioid Prescribing for Chronic Pain: Guidelines for Marin County Clinicians Although prescription pain medications are intended to improve the lives of people with pain, their increased use and misuse
Opioid Prescribing for Chronic Pain: Guidelines for Marin County Clinicians Although prescription pain medications are intended to improve the lives of people with pain, their increased use and misuse
PARTNERSHIP HEALTHPLAN RECOMMENDATIONS For Safe Use of Opioid Medications
 PARTNERSHIP HEALTHPLAN RECOMMENDATIONS For Safe Use of Opioid Medications Primary Care & Specialist Prescribing Guidelines Introduction Partnership HealthPlan is a County Organized Health System covering
PARTNERSHIP HEALTHPLAN RECOMMENDATIONS For Safe Use of Opioid Medications Primary Care & Specialist Prescribing Guidelines Introduction Partnership HealthPlan is a County Organized Health System covering
Naltrexone Pellet Treatment for Opiate, Heroin, and Alcohol Addiction. Frequently Asked Questions
 Naltrexone Pellet Treatment for Opiate, Heroin, and Alcohol Addiction Frequently Asked Questions What is Naltrexone? Naltrexone is a prescription drug that effectively blocks the effects of heroin, alcohol,
Naltrexone Pellet Treatment for Opiate, Heroin, and Alcohol Addiction Frequently Asked Questions What is Naltrexone? Naltrexone is a prescription drug that effectively blocks the effects of heroin, alcohol,
BENZODIAZEPINE CONSIDERATIONS IN WORKERS COMPENSATION: IMPLICATIONS FOR WORK DISABILITY AND CLAIM COSTS By: Michael Erdil MD, FACOEM
 3 rd Quarter 2015 BENZODIAZEPINE CONSIDERATIONS IN WORKERS COMPENSATION: IMPLICATIONS FOR WORK DISABILITY AND CLAIM COSTS By: Michael Erdil MD, FACOEM Introduction Benzodiazepines, sometimes called "benzos",
3 rd Quarter 2015 BENZODIAZEPINE CONSIDERATIONS IN WORKERS COMPENSATION: IMPLICATIONS FOR WORK DISABILITY AND CLAIM COSTS By: Michael Erdil MD, FACOEM Introduction Benzodiazepines, sometimes called "benzos",
Review of Pharmacological Pain Management
 Review of Pharmacological Pain Management CHAMP Activities are possible with generous support from The Atlantic Philanthropies and The John A. Hartford Foundation The WHO Pain Ladder The World Health Organization
Review of Pharmacological Pain Management CHAMP Activities are possible with generous support from The Atlantic Philanthropies and The John A. Hartford Foundation The WHO Pain Ladder The World Health Organization
Fact Sheet. Queensland Spinal Cord Injuries Service. Pain Management Following Spinal Cord Injury for Health Professionals
 Pain Management Following Injury for Health Professionals and Introduction Pain is a common problem following SCI. In the case where a person with SCI does have pain, there are treatments available that
Pain Management Following Injury for Health Professionals and Introduction Pain is a common problem following SCI. In the case where a person with SCI does have pain, there are treatments available that
THE COMMONWEALTH OF MASSACHUSETTS Department of Industrial Accidents
 THE COMMONWEALTH OF MASSACHUSETTS Department of Industrial Accidents 1 Congress Street, Suite 100 Boston, Massachusetts 02114-2017 DEVAL L. PATRICK Governor PHILIP L. HILLMAN Director TIMOTHY P. MURRAY
THE COMMONWEALTH OF MASSACHUSETTS Department of Industrial Accidents 1 Congress Street, Suite 100 Boston, Massachusetts 02114-2017 DEVAL L. PATRICK Governor PHILIP L. HILLMAN Director TIMOTHY P. MURRAY
Lumbar Fusion. Reference Guide for PACU CLINICAL PATHWAY. All patient variances to the pathway are to be circled and addressed in the progress notes.
 Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
Appendix to Tennessee Department of Health: Tennessee Clinical Practice Guidelines for Outpatient Management of Chronic Non- Malignant Pain
 Appendix to Tennessee Department of Health: Tennessee Clinical Practice Guidelines for Outpatient Management of Chronic Non- Malignant Pain Division of Workers Compensation 04.01.2015 Background Opioids
Appendix to Tennessee Department of Health: Tennessee Clinical Practice Guidelines for Outpatient Management of Chronic Non- Malignant Pain Division of Workers Compensation 04.01.2015 Background Opioids
Information for Pharmacists
 Page 43 by 42 CFR part 2. A general authorization for the release of medical or other information is NOT sufficient for this purpose. Information for Pharmacists SUBOXONE (buprenorphine HCl/naloxone HCl
Page 43 by 42 CFR part 2. A general authorization for the release of medical or other information is NOT sufficient for this purpose. Information for Pharmacists SUBOXONE (buprenorphine HCl/naloxone HCl
Treatment of Opioid Dependence with Buprenorphine/Naloxone (Suboxone )
") Treatment of Opioid Dependence with Buprenorphine/Naloxone (Suboxone ) Elinore F. McCance-Katz, M.D., Ph.D. Professor and Chair, Addiction Psychiatry Virginia Commonwealth University Neurobiology of Opiate
Treatment of Opioid Dependence with Buprenorphine/Naloxone (Suboxone ) Elinore F. McCance-Katz, M.D., Ph.D. Professor and Chair, Addiction Psychiatry Virginia Commonwealth University Neurobiology of Opiate
PROTOCOL SYNOPSIS Evaluation of long-term opioid efficacy for chronic pain
 P a g e 1 PROTOCOL SYNOPSIS Evaluation of long-term opioid efficacy for chronic pain Clinical Phase 4 Study Centers Study Period 25 U.S. sites identified and reviewed by the Steering Committee and Contract
P a g e 1 PROTOCOL SYNOPSIS Evaluation of long-term opioid efficacy for chronic pain Clinical Phase 4 Study Centers Study Period 25 U.S. sites identified and reviewed by the Steering Committee and Contract
1. Which of the following would NOT be an appropriate choice for postoperative pain. C. Oral oxycodone 5 mg po every 4 to 6 hours as needed for pain
 Pain Management 1 Chapter 34. Pain Management, Self-Assessment Questions 1. Which of the following would NOT be an appropriate choice for postoperative pain management in a patient dependent on opioids?
Pain Management 1 Chapter 34. Pain Management, Self-Assessment Questions 1. Which of the following would NOT be an appropriate choice for postoperative pain management in a patient dependent on opioids?
Guidelines for Cancer Pain Management in Substance Misusers Dr Jane Neerkin, Dr Chi-Chi Cheung and Dr Caroline Stirling
 Guidelines for Cancer Pain Management in Substance Misusers Dr Jane Neerkin, Dr Chi-Chi Cheung and Dr Caroline Stirling Patients with a substance misuse history are at increased risk of receiving inadequate
Guidelines for Cancer Pain Management in Substance Misusers Dr Jane Neerkin, Dr Chi-Chi Cheung and Dr Caroline Stirling Patients with a substance misuse history are at increased risk of receiving inadequate
Guidance on competencies for management of Cancer Pain in adults
 Guidance on competencies for management of Cancer Pain in adults Endorsed by: Contents Introduction A: Core competencies for practitioners in Pain Medicine B: Competencies for practitioners in Pain Medicine
Guidance on competencies for management of Cancer Pain in adults Endorsed by: Contents Introduction A: Core competencies for practitioners in Pain Medicine B: Competencies for practitioners in Pain Medicine
Care Manager Resources: Common Questions & Answers about Treatments for Depression
 Care Manager Resources: Common Questions & Answers about Treatments for Depression Questions about Medications 1. How do antidepressants work? Antidepressants help restore the correct balance of certain
Care Manager Resources: Common Questions & Answers about Treatments for Depression Questions about Medications 1. How do antidepressants work? Antidepressants help restore the correct balance of certain
SAFE PAIN MEDICATION PRESCRIBING GUIDELINES
 Prescription drug abuse has been declared an epidemic by the Centers for Disease Control. According to 2012 San Diego Medical Examiner data, the number one cause of non-natural death is due to drug overdoses
Prescription drug abuse has been declared an epidemic by the Centers for Disease Control. According to 2012 San Diego Medical Examiner data, the number one cause of non-natural death is due to drug overdoses
DOLORE CRONICO NELL ANZIANO
 DOLORE CRONICO NELL ANZIANO Vecchie e nuove strategie terapeutiche: sicurezza ed efficacia Walter Gianni INRCA, Ircss Sede di Roma Let s start.. Older person s reflection about pain I feel like a dog thrown
DOLORE CRONICO NELL ANZIANO Vecchie e nuove strategie terapeutiche: sicurezza ed efficacia Walter Gianni INRCA, Ircss Sede di Roma Let s start.. Older person s reflection about pain I feel like a dog thrown
3/10/2015. SPEAKER NAME AND CREDENTIALS: Roberta Goff, MSN Ed, RN-BC, ACNS-BC, ONC
 GOAL OF PROGRAM: To gain understanding about caring for different pain populations and keeping them safe. SUCCESSFUL COMPLETION: To receive contact hours, participants must attend the entire program. Please
GOAL OF PROGRAM: To gain understanding about caring for different pain populations and keeping them safe. SUCCESSFUL COMPLETION: To receive contact hours, participants must attend the entire program. Please
Hospice and Palliative Medicine
 Hospice and Palliative Medicine Maintenance of Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills
Hospice and Palliative Medicine Maintenance of Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills
Ultram (tramadol), Ultram ER (tramadol extended-release tablets); Conzip (tramadol extended-release capsules), Ultracet (tramadol / acetaminophen)
, Ultram ER (tramadol extended-release tablets); Conzip (tramadol extended-release capsules), Ultracet (tramadol / acetaminophen)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.02.35 Subject: Tramadol Acetaminophen Page: 1 of 8 Last Review Date: September 18, 2015 Tramadol Acetaminophen
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.02.35 Subject: Tramadol Acetaminophen Page: 1 of 8 Last Review Date: September 18, 2015 Tramadol Acetaminophen
Prior Authorization Guideline
 Prior Authorization Guideline Guideline: CSD - Suboxone Therapeutic Class: Central Nervous System Agents Therapeutic Sub-Class: Analgesics and Antipyretics (Opiate Partial Agonists) Client: County of San
Prior Authorization Guideline Guideline: CSD - Suboxone Therapeutic Class: Central Nervous System Agents Therapeutic Sub-Class: Analgesics and Antipyretics (Opiate Partial Agonists) Client: County of San
Frequently asked questions
 Naltrexone Pellet Treatment for Opiate, Heroin, and Alcohol Addiction Frequently asked questions What is Naltrexone? Naltrexone is a prescription drug that completely blocks the effects of all opioid drugs
Naltrexone Pellet Treatment for Opiate, Heroin, and Alcohol Addiction Frequently asked questions What is Naltrexone? Naltrexone is a prescription drug that completely blocks the effects of all opioid drugs
UNIT VIII NARCOTIC ANALGESIA
 UNIT VIII NARCOTIC ANALGESIA Objective Review the definitions of Analgesic, Narcotic and Antagonistic. List characteristics of Opioid analgesics in terms of mechanism of action, indications for use and
UNIT VIII NARCOTIC ANALGESIA Objective Review the definitions of Analgesic, Narcotic and Antagonistic. List characteristics of Opioid analgesics in terms of mechanism of action, indications for use and
Cervical Spondylosis (Arthritis of the Neck)
") Copyright 2009 American Academy of Orthopaedic Surgeons Cervical Spondylosis (Arthritis of the Neck) Neck pain is extremely common. It can be caused by many things, and is most often related to getting
Copyright 2009 American Academy of Orthopaedic Surgeons Cervical Spondylosis (Arthritis of the Neck) Neck pain is extremely common. It can be caused by many things, and is most often related to getting
Pain Management after Surgery Patient Information Booklet
 Pain Management after Surgery Patient Information Booklet PATS 509-15-05 Your Health Care Be Involved Be involved in your healthcare. Speak up if you have questions or concerns about your care. Tell a
Pain Management after Surgery Patient Information Booklet PATS 509-15-05 Your Health Care Be Involved Be involved in your healthcare. Speak up if you have questions or concerns about your care. Tell a
NEW PATIENTS' INFORMATION SHEET
 NEW PATIENTS' INFORMATION SHEET Please print clearly. Please complete all information so that your claim can be processed quickly and efficiently. Thank you! PATIENT INFORMATION (First) (MI) (Last) Name
NEW PATIENTS' INFORMATION SHEET Please print clearly. Please complete all information so that your claim can be processed quickly and efficiently. Thank you! PATIENT INFORMATION (First) (MI) (Last) Name
Abstral Prescriber and Pharmacist Guide
 Abstral Prescriber and Pharmacist Guide fentanyl citrate sublingual tablets Introduction The Abstral Prescriber and Pharmacist Guide is designed to support healthcare professionals in the diagnosis of
Abstral Prescriber and Pharmacist Guide fentanyl citrate sublingual tablets Introduction The Abstral Prescriber and Pharmacist Guide is designed to support healthcare professionals in the diagnosis of
Depression is a common biological brain disorder and occurs in 7-12% of all individuals over
 Depression is a common biological brain disorder and occurs in 7-12% of all individuals over the age of 65. Specific groups have a much higher rate of depression including the seriously medically ill (20-40%),
Depression is a common biological brain disorder and occurs in 7-12% of all individuals over the age of 65. Specific groups have a much higher rate of depression including the seriously medically ill (20-40%),
Drug and non-drug treatments for chronic pain related to vascular disease. Gregory Chernish, MD, CIME
 Drug and non-drug treatments for chronic pain related to vascular disease 1 Greg Chernish MD Assistant Professor, Family Medicine U of M Chengdu College of Traditional Chinese Medicine 1990 Certified Independent
Drug and non-drug treatments for chronic pain related to vascular disease 1 Greg Chernish MD Assistant Professor, Family Medicine U of M Chengdu College of Traditional Chinese Medicine 1990 Certified Independent
The Pharmacological Management of Cancer Pain in Adults. Clinical Audit Tool
 The Pharmacological Management of Cancer Pain in Adults Clinical Audit Tool 2015 This clinical audit tool accompanies the Pharmacological Management of Cancer Pain in Adults NCEC National Clinical Guideline
The Pharmacological Management of Cancer Pain in Adults Clinical Audit Tool 2015 This clinical audit tool accompanies the Pharmacological Management of Cancer Pain in Adults NCEC National Clinical Guideline
6/3/2011. High Prevalence and Incidence. Low back pain is 5 th most common reason for all physician office visits in the U.S.
 High Prevalence and Incidence Prevalence 85% of Americans will experience low back pain at some time in their life. Incidence 5% annual Timothy C. Shen, M.D. Physical Medicine and Rehabilitation Sub-specialty
High Prevalence and Incidence Prevalence 85% of Americans will experience low back pain at some time in their life. Incidence 5% annual Timothy C. Shen, M.D. Physical Medicine and Rehabilitation Sub-specialty
How To Treat Anorexic Addiction With Medication Assisted Treatment
 Medication Assisted Treatment for Opioid Addiction Tanya Hiser, MS, LPC Premier Care of Wisconsin, LLC October 21, 2015 How Did We Get Here? Civil War veterans and women 19th Century physicians cautious
Medication Assisted Treatment for Opioid Addiction Tanya Hiser, MS, LPC Premier Care of Wisconsin, LLC October 21, 2015 How Did We Get Here? Civil War veterans and women 19th Century physicians cautious
Opioids and the Injured Worker Tools for Successful Outcomes
 Opioids and the Injured Worker Tools for Successful Outcomes Tim Pokorney, RPh Director, Clinical Express Scripts Workers' Compensation Division Goals and Objectives Alarming statistics for narcotic utilization,
Opioids and the Injured Worker Tools for Successful Outcomes Tim Pokorney, RPh Director, Clinical Express Scripts Workers' Compensation Division Goals and Objectives Alarming statistics for narcotic utilization,
After seeing a patient on a Diversion Alert installment..
 After seeing a patient on a Diversion Alert installment.. Recommendations from Dr. James Berry of Mercy Recovery Center OVERVIEW OF DIVERSION Manufacture Distribution Pharmacy Patient End -user OPPORTUNITIES
After seeing a patient on a Diversion Alert installment.. Recommendations from Dr. James Berry of Mercy Recovery Center OVERVIEW OF DIVERSION Manufacture Distribution Pharmacy Patient End -user OPPORTUNITIES
Drug Class Review Drugs for Fibromyalgia
 Drug Class Review Drugs for Fibromyalgia Final Original Report April 2011 The Agency for Healthcare Research and Quality has not yet seen or approved this report. The purpose of the is to summarize key
Drug Class Review Drugs for Fibromyalgia Final Original Report April 2011 The Agency for Healthcare Research and Quality has not yet seen or approved this report. The purpose of the is to summarize key
Update and Review of Medication Assisted Treatments
 Update and Review of Medication Assisted Treatments for Opiate and Alcohol Use Disorders Richard N. Whitney, MD Medical Director Addiction Services Shepherd Hill Newark, Ohio Medication Assisted Treatment
Update and Review of Medication Assisted Treatments for Opiate and Alcohol Use Disorders Richard N. Whitney, MD Medical Director Addiction Services Shepherd Hill Newark, Ohio Medication Assisted Treatment
Submitted via email to chronic_care@finance.senate.gov. June 22, 2015
 Submitted via email to chronic_care@finance.senate.gov June 22, 2015 Chronic Care Working Group Senate Finance Committee United States Senate 219 Dirksen Senate Office Building Washington, D.C. 20510 Re:
Submitted via email to chronic_care@finance.senate.gov June 22, 2015 Chronic Care Working Group Senate Finance Committee United States Senate 219 Dirksen Senate Office Building Washington, D.C. 20510 Re:
03/20/12. Recognize the right of patients to appropriate assessment and management of pain
 Narcotic Bowel Syndrome Alvin Zfass M.D. M.D. Professor of Medicine Toufic Kachaamy M.D. GI Fellow Chronic Pain 110 million Americans suffer from chronic pain according to the NIH Cost of untreated t or
Narcotic Bowel Syndrome Alvin Zfass M.D. M.D. Professor of Medicine Toufic Kachaamy M.D. GI Fellow Chronic Pain 110 million Americans suffer from chronic pain according to the NIH Cost of untreated t or
Neurotransmitters Made Easy: The Mood Teeter-Totter
 Neurotransmitters Made Easy: The Mood Brad Lander PhD, LICDC Clinical Director / Psychologist Talbot Hall - Addiction Medicine at The Ohio State University Wexner Medical Center Key Point #1 Thinking and
Neurotransmitters Made Easy: The Mood Brad Lander PhD, LICDC Clinical Director / Psychologist Talbot Hall - Addiction Medicine at The Ohio State University Wexner Medical Center Key Point #1 Thinking and
MQAC Rules for the Management of Chronic Non-Cancer Pain
 MQAC Rules for the Management of Chronic Non-Cancer Pain Effective January 2, 2012 246-919-850 Pain management Intent. These rules govern the use of opioids in the treatment of patients for chronic noncancer
MQAC Rules for the Management of Chronic Non-Cancer Pain Effective January 2, 2012 246-919-850 Pain management Intent. These rules govern the use of opioids in the treatment of patients for chronic noncancer
Pharmacologic management of neuropathic pain: Evidence-based recommendations
 Pain 132 (2007) 237 251 Review and recommendations Pharmacologic management of neuropathic pain: Evidence-based recommendations Robert H. Dworkin a, *, Alec B. O Connor a, Miroslav Backonja b, John T.
Pain 132 (2007) 237 251 Review and recommendations Pharmacologic management of neuropathic pain: Evidence-based recommendations Robert H. Dworkin a, *, Alec B. O Connor a, Miroslav Backonja b, John T.
How To Write An Opiate Prescription Guideline
 Guidelines for Prescription of Opioid Medications for Acute and Chronic Pain developed and adopted by the Physician Advisory Committee Adopted by the Administrator of the Oklahoma Workers' Compensation
Guidelines for Prescription of Opioid Medications for Acute and Chronic Pain developed and adopted by the Physician Advisory Committee Adopted by the Administrator of the Oklahoma Workers' Compensation
A Guide to pain relief medicines For patients receiving Palliative Care
 A Guide to pain relief medicines For patients receiving Palliative Care 1 Which pain medicines are you taking? Contents Page No. Amitriptyline 8 Codeine 9 Co-codamol 10 Co-dydramol 11 Diclofenac (Voltarol
A Guide to pain relief medicines For patients receiving Palliative Care 1 Which pain medicines are you taking? Contents Page No. Amitriptyline 8 Codeine 9 Co-codamol 10 Co-dydramol 11 Diclofenac (Voltarol
Options in Pain Management Alice Looney ANP-C Kreisberg Family Pain Management Center Saint Luke s Cornwall Hospital
 Options in Pain Management Alice Looney ANP-C Kreisberg Family Pain Management Center Saint Luke s Cornwall Hospital To decrease pain To improve lifestyle To decrease the need for drugs (including narcotics
Options in Pain Management Alice Looney ANP-C Kreisberg Family Pain Management Center Saint Luke s Cornwall Hospital To decrease pain To improve lifestyle To decrease the need for drugs (including narcotics
Narcotic drugs used for pain treatment Version 4.3
 Narcotic drugs used for pain treatment Version 4.3 Strategy to restrict the pack sizes or the type of packaging available in public pharmacies. 1. Introduction The document describing the strategy of the
Narcotic drugs used for pain treatment Version 4.3 Strategy to restrict the pack sizes or the type of packaging available in public pharmacies. 1. Introduction The document describing the strategy of the
CLINICAL PRACTICE GUIDELINES FOR MANAGEMENT OF LOW BACK PAIN
 CLINICAL PRACTICE GUIDELINES FOR MANAGEMENT OF LOW BACK PAIN Low back pain is very common, up to 90+% of people are affected by back pain at some time in their lives. Most often back pain is benign and
CLINICAL PRACTICE GUIDELINES FOR MANAGEMENT OF LOW BACK PAIN Low back pain is very common, up to 90+% of people are affected by back pain at some time in their lives. Most often back pain is benign and
Questions and answers on breast cancer Guideline 10: The management of persistent pain after breast cancer treatment
 Questions and answers on breast cancer Guideline 10: The management of persistent pain after breast cancer treatment I ve had breast cancer treatment, and now I m having pain. Does this mean the cancer
Questions and answers on breast cancer Guideline 10: The management of persistent pain after breast cancer treatment I ve had breast cancer treatment, and now I m having pain. Does this mean the cancer
Nurses Self Paced Learning Module on Pain Management
 Nurses Self Paced Learning Module on Pain Management Dominican Santa Cruz Hospital Santa Cruz, California Developed by: Strategic Planning Committee Dominican Santa Cruz Hospital 1555 Soquel Drive Santa
Nurses Self Paced Learning Module on Pain Management Dominican Santa Cruz Hospital Santa Cruz, California Developed by: Strategic Planning Committee Dominican Santa Cruz Hospital 1555 Soquel Drive Santa
PAIN MANAGEMENT. Louise Smith Clinical Nurse Specialist
 PAIN MANAGEMENT Louise Smith Clinical Nurse Specialist Objectives To understand:- The concept of Total Pain The types of Physical Pain Holistic assessment Pain management; pharmaceutical & non pharmaceutical
PAIN MANAGEMENT Louise Smith Clinical Nurse Specialist Objectives To understand:- The concept of Total Pain The types of Physical Pain Holistic assessment Pain management; pharmaceutical & non pharmaceutical
Blueprint for Prescriber Continuing Education Program
 CDER Final 10/25/11 Blueprint for Prescriber Continuing Education Program I. Introduction: Why Prescriber Education is Important Health care professionals who prescribe extended-release (ER) and long-acting
CDER Final 10/25/11 Blueprint for Prescriber Continuing Education Program I. Introduction: Why Prescriber Education is Important Health care professionals who prescribe extended-release (ER) and long-acting
PAIN MANAGEMENT AT UM/SYLVESTER
 PAIN MANAGEMENT AT UM/SYLVESTER W HAT IS THE PURPOSE OF THIS BROCHURE? We created this brochure for patients receiving care from the University of Miami Sylvester Comprehensive Cancer Center and their
PAIN MANAGEMENT AT UM/SYLVESTER W HAT IS THE PURPOSE OF THIS BROCHURE? We created this brochure for patients receiving care from the University of Miami Sylvester Comprehensive Cancer Center and their
Physician Coding and Payment Guide 2015
 Targeted Drug Delivery Physician Coding and Payment Guide 2015 Flowonix Medical has compiled this coding information for your convenience. This information is gathered from third party sources and is subject
Targeted Drug Delivery Physician Coding and Payment Guide 2015 Flowonix Medical has compiled this coding information for your convenience. This information is gathered from third party sources and is subject
Depression in Older Persons
 Depression in Older Persons How common is depression in later life? Depression affects more than 6.5 million of the 35 million Americans aged 65 or older. Most people in this stage of life with depression
Depression in Older Persons How common is depression in later life? Depression affects more than 6.5 million of the 35 million Americans aged 65 or older. Most people in this stage of life with depression
PSYCHOPHARMACOLOGY AND WORKING WITH PSYCHIATRY PROVIDERS. Juanaelena Garcia, MD Psychiatry Director Institute for Family Health
 PSYCHOPHARMACOLOGY AND WORKING WITH PSYCHIATRY PROVIDERS Juanaelena Garcia, MD Psychiatry Director Institute for Family Health Learning Objectives Learn basics about the various types of medications that
PSYCHOPHARMACOLOGY AND WORKING WITH PSYCHIATRY PROVIDERS Juanaelena Garcia, MD Psychiatry Director Institute for Family Health Learning Objectives Learn basics about the various types of medications that
OPIOIDS. Petros Levounis, MD, MA Chair Department of Psychiatry Rutgers New Jersey Medical School
 OPIOIDS Petros Levounis, MD, MA Chair Department of Psychiatry Rutgers New Jersey Medical School Rutgers New Jersey Medical School Fundamentals of Addiction Medicine Summer Series Newark, NJ July 24, 2013
OPIOIDS Petros Levounis, MD, MA Chair Department of Psychiatry Rutgers New Jersey Medical School Rutgers New Jersey Medical School Fundamentals of Addiction Medicine Summer Series Newark, NJ July 24, 2013
Treatments for Major Depression. Drug Treatments The two (2) classes of drugs that are typical antidepressants are:
 classes of drugs that are typical antidepressants are:") Treatments for Major Depression Drug Treatments The two (2) classes of drugs that are typical antidepressants are: 1. 2. These 2 classes of drugs increase the amount of monoamine neurotransmitters through
Treatments for Major Depression Drug Treatments The two (2) classes of drugs that are typical antidepressants are: 1. 2. These 2 classes of drugs increase the amount of monoamine neurotransmitters through
Prescription Drugs: Abuse and Addiction
 EAP Drug Free Workplace Newsletter March 2014 Prescription Drugs: Abuse and Addiction What are some of the commonly abused prescription drugs? Although many prescription drugs can be abused or misused,
EAP Drug Free Workplace Newsletter March 2014 Prescription Drugs: Abuse and Addiction What are some of the commonly abused prescription drugs? Although many prescription drugs can be abused or misused,
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS
 GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: Frenchay 0117 340 6692 Southmead 0117 323
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: Frenchay 0117 340 6692 Southmead 0117 323
MEDICATION ABUSE IN OLDER ADULTS
 MEDICATION ABUSE IN OLDER ADULTS Clifford Milo Singer, MD Adjunct Professor, University of Maine, Orono ME Chief, Division of Geriatric Mental Health and Neuropsychiatry The Acadia Hospital and Eastern
MEDICATION ABUSE IN OLDER ADULTS Clifford Milo Singer, MD Adjunct Professor, University of Maine, Orono ME Chief, Division of Geriatric Mental Health and Neuropsychiatry The Acadia Hospital and Eastern
Downers/Depressants (pages 40-50)
") Downers/Depressants (pages 40-50) Read pages 49-54, 59-60, and 78-79 of the booklet, Street Drugs. Pages 40-50 of the text. Narcotics: Prescription Origin: Southeast Asia, Southwest Asia, and in the Western
Downers/Depressants (pages 40-50) Read pages 49-54, 59-60, and 78-79 of the booklet, Street Drugs. Pages 40-50 of the text. Narcotics: Prescription Origin: Southeast Asia, Southwest Asia, and in the Western
MANAGEMENT OF CHRONIC NON MALIGNANT PAIN
 MANAGEMENT OF CHRONIC NON MALIGNANT PAIN Introduction The Manitoba Prescribing Practices Program (MPPP) recognizes the important role served by physicians in relieving pain and suffering and acknowledges
MANAGEMENT OF CHRONIC NON MALIGNANT PAIN Introduction The Manitoba Prescribing Practices Program (MPPP) recognizes the important role served by physicians in relieving pain and suffering and acknowledges
Benzodiazepines: A Model for Central Nervous System (CNS) Depressants
 Depressants") Benzodiazepines: A Model for Central Nervous System (CNS) Depressants Objectives Summarize the basic mechanism by which benzodiazepines work in the brain. Describe two strategies for reducing and/or eliminating
Benzodiazepines: A Model for Central Nervous System (CNS) Depressants Objectives Summarize the basic mechanism by which benzodiazepines work in the brain. Describe two strategies for reducing and/or eliminating
Topical Pain Creams for Management of Acute, Chronic, and Neuropathic Pain
 2825 W. Andrew Johnson Hwy. Morristown, TN 37814 phone: 423-307-5757 fax: 423-307-5241 www.fountainplazapharmacy.com Topical Pain Creams for Management of Acute, Chronic, and Neuropathic Pain Pain is one
2825 W. Andrew Johnson Hwy. Morristown, TN 37814 phone: 423-307-5757 fax: 423-307-5241 www.fountainplazapharmacy.com Topical Pain Creams for Management of Acute, Chronic, and Neuropathic Pain Pain is one
Non medical use of prescription medicines existing WHO advice
 Non medical use of prescription medicines existing WHO advice Nicolas Clark Management of Substance Abuse Team WHO, Geneva Vienna, June 2010 clarkn@who.int Medical and Pharmaceutical role Recommendations
Non medical use of prescription medicines existing WHO advice Nicolas Clark Management of Substance Abuse Team WHO, Geneva Vienna, June 2010 clarkn@who.int Medical and Pharmaceutical role Recommendations
DIFFERENTIAL DIAGNOSIS OF LOW BACK PAIN. Arnold J. Weil, M.D., M.B.A. Non-Surgical Orthopaedics, P.C. Atlanta, GA
 DIFFERENTIAL DIAGNOSIS OF LOW BACK PAIN Arnold J. Weil, M.D., M.B.A. Non-Surgical Orthopaedics, P.C. Atlanta, GA MEDICAL ALGORITHM OF REALITY LOWER BACK PAIN Yes Patient will never get better until case
DIFFERENTIAL DIAGNOSIS OF LOW BACK PAIN Arnold J. Weil, M.D., M.B.A. Non-Surgical Orthopaedics, P.C. Atlanta, GA MEDICAL ALGORITHM OF REALITY LOWER BACK PAIN Yes Patient will never get better until case
Ambulatory Surgery Center Coding and Payment Guide 2015
 Targeted Drug Delivery Ambulatory Surgery Center Coding and Payment Guide 2015 Flowonix Medical has compiled this coding information for your convenience. This information is gathered from third party
Targeted Drug Delivery Ambulatory Surgery Center Coding and Payment Guide 2015 Flowonix Medical has compiled this coding information for your convenience. This information is gathered from third party
Opioid Analgesics. Week 19
 Opioid Analgesics Week 19 Analgesic Vocabulary Analgesia Narcotic Opiate Opioid Agonist Antagonist Narcotic Analgesics Controlled substances Opioid analgesics derived from poppy Opiates include morphine,
Opioid Analgesics Week 19 Analgesic Vocabulary Analgesia Narcotic Opiate Opioid Agonist Antagonist Narcotic Analgesics Controlled substances Opioid analgesics derived from poppy Opiates include morphine,
Guidelines for the Use of Controlled Substances in the Treatment of Pain Adopted by the New Hampshire Medical Society, July 1998
 Guidelines for the Use of Controlled Substances in the Treatment of Pain Adopted by the New Hampshire Medical Society, July 1998 Section I: Preamble The New Hampshire Medical Society believes that principles
Guidelines for the Use of Controlled Substances in the Treatment of Pain Adopted by the New Hampshire Medical Society, July 1998 Section I: Preamble The New Hampshire Medical Society believes that principles
UNM Pain Center: Addressing New Mexico s Public Health Crises of Pain, Addiction, and Unintentional Opioid Overdose Deaths
 UNM Pain Center: Addressing New Mexico s Public Health Crises of Pain, Addiction, and Unintentional Opioid Overdose Deaths Joanna G Katzman, M.D., M.S.P.H Director, UNM Pain Center Associate Professor,
UNM Pain Center: Addressing New Mexico s Public Health Crises of Pain, Addiction, and Unintentional Opioid Overdose Deaths Joanna G Katzman, M.D., M.S.P.H Director, UNM Pain Center Associate Professor,
The Outpatient Knee Replacement Program at Orlando Orthopaedic Center. Jeffrey P. Rosen, MD
 The Outpatient Knee Replacement Program at Orlando Orthopaedic Center Jeffrey P. Rosen, MD Anesthesia Pain Management Post-Op / Discharge Protocols The Orlando Orthopaedic Center Joint Replacement Team
The Outpatient Knee Replacement Program at Orlando Orthopaedic Center Jeffrey P. Rosen, MD Anesthesia Pain Management Post-Op / Discharge Protocols The Orlando Orthopaedic Center Joint Replacement Team
Death in the Suburbs: How Prescription Painkillers and Heroin Have Changed Treatment and Recovery
 Death in the Suburbs: How Prescription Painkillers and Heroin Have Changed Treatment and Recovery Marvin D. Seppala, MD Chief Medical Officer Hazelden Betty Ford Foundation This product is supported by
Death in the Suburbs: How Prescription Painkillers and Heroin Have Changed Treatment and Recovery Marvin D. Seppala, MD Chief Medical Officer Hazelden Betty Ford Foundation This product is supported by
m y f o u n d a t i o n i n f o s h e e t
 Pain and Myeloma m y f o u n d a t i o n i n f o s h e e t Pain is the most common symptom of myeloma and can greatly affect all areas of your life, especially if it is untreated or poorly managed. This
Pain and Myeloma m y f o u n d a t i o n i n f o s h e e t Pain is the most common symptom of myeloma and can greatly affect all areas of your life, especially if it is untreated or poorly managed. This
Recognition and Treatment of Depression in Parkinson s Disease
 Recognition and Treatment of Depression in Parkinson s Disease Web Ross VA Pacific Islands Health Care System What is depression? Depression is a serious medical condition that affects a person s feelings,
Recognition and Treatment of Depression in Parkinson s Disease Web Ross VA Pacific Islands Health Care System What is depression? Depression is a serious medical condition that affects a person s feelings,
Mitchell Freedman, DO
 The Treatment of Chronic lower back pain: The Good, the Bad and the Ugly Mitchell Freedman, DO Director of Physical Medicine and Rehabilitation at the Rothman Institute Associate Professor of Physical
The Treatment of Chronic lower back pain: The Good, the Bad and the Ugly Mitchell Freedman, DO Director of Physical Medicine and Rehabilitation at the Rothman Institute Associate Professor of Physical
Prescription Opioid Addiction and Chronic Pain: Non-Addictive Alternatives To Treatment and Management
 Prescription Opioid Addiction and Chronic Pain: Non-Addictive Alternatives To Treatment and Management Dr. Barbara Krantz Medical Director Diplomate American Board of Addiction Medicine 1 Learning Objectives
Prescription Opioid Addiction and Chronic Pain: Non-Addictive Alternatives To Treatment and Management Dr. Barbara Krantz Medical Director Diplomate American Board of Addiction Medicine 1 Learning Objectives
Prescribing and Tapering Benzodiazepines
 E-Resource October, 2014 Prescribing and Tapering Benzodiazepines The use of benzodiazepines has grown over time and evidence has shown that long term use of these drugs has very little benefit with many
E-Resource October, 2014 Prescribing and Tapering Benzodiazepines The use of benzodiazepines has grown over time and evidence has shown that long term use of these drugs has very little benefit with many
Objectives. Pain Management Knowing How To Help Yourself. Patients and Family Requirements. Your Rights As A Consumer
 Objectives Pain Management Knowing How To Help Yourself Jackie Carter, RN MSN CNS Become familiar with the definitions of pain Be aware of your rights to have your pain treated Become familiar with the
Objectives Pain Management Knowing How To Help Yourself Jackie Carter, RN MSN CNS Become familiar with the definitions of pain Be aware of your rights to have your pain treated Become familiar with the
02 DEPARTMENT OF PROFESSIONAL AND FINANCIAL REGULATION
 Effective June 13, 2010 02-313, 02-373, 02-380, 02-383, 02-396 Chapter 21 page 1 02 DEPARTMENT OF PROFESSIONAL AND FINANCIAL REGULATION 313 BOARD OF DENTAL EXAMINERS 373 BOARD OF LICENSURE IN MEDICINE
Effective June 13, 2010 02-313, 02-373, 02-380, 02-383, 02-396 Chapter 21 page 1 02 DEPARTMENT OF PROFESSIONAL AND FINANCIAL REGULATION 313 BOARD OF DENTAL EXAMINERS 373 BOARD OF LICENSURE IN MEDICINE
Chronic Headaches. David R. Greeley, MD, FAAN Northwest Neurological, PLLC October 23, 2015
 s David R. Greeley, MD, FAAN Northwest Neurological, PLLC October 23, 2015 Why is Headache Important? 36,000,000 people have migraine - more than asthma and diabetes combined 13,000,000 have chronic daily
s David R. Greeley, MD, FAAN Northwest Neurological, PLLC October 23, 2015 Why is Headache Important? 36,000,000 people have migraine - more than asthma and diabetes combined 13,000,000 have chronic daily
CHPN Review Course Pain Management Part 1 Hospice and Palliative Nurses Association
 CHPN Review Course Pain Management Part 1 Disclosures Bonnie Morgan has no real or perceived conflicts of interest that relate to this presentation. Copyright 2015 by the. HPNA has the exclusive rights
CHPN Review Course Pain Management Part 1 Disclosures Bonnie Morgan has no real or perceived conflicts of interest that relate to this presentation. Copyright 2015 by the. HPNA has the exclusive rights
Treatment of Chronic Pain: Our Approach
 Treatment of Chronic Pain: Our Approach Today s webinar was coordinated by the National Association of Community Health Centers, a partner with the SAMHSA-HRSA Center for Integrated Health Solutions SAMHSA
Treatment of Chronic Pain: Our Approach Today s webinar was coordinated by the National Association of Community Health Centers, a partner with the SAMHSA-HRSA Center for Integrated Health Solutions SAMHSA
New England Pain Management Consultants At New England Baptist Hospital
 New England Pain Management Consultants At New England Baptist Hospital Pain Management Center Health Assessment Dear New Pain Management Patient, Welcome to the New England Pain Management Consultants
New England Pain Management Consultants At New England Baptist Hospital Pain Management Center Health Assessment Dear New Pain Management Patient, Welcome to the New England Pain Management Consultants
Headaches in Children
 Children s s Hospital Headaches in Children Manikum Moodley, MD, FRCP Section of Pediatric Neurology The Cleveland Clinic Foundation Introduction Headaches are common in children Most headaches are benign
Children s s Hospital Headaches in Children Manikum Moodley, MD, FRCP Section of Pediatric Neurology The Cleveland Clinic Foundation Introduction Headaches are common in children Most headaches are benign
Protecting your employees, physicians and you.
 Protecting your employees, physicians and you. Opioid abuse is being talked about every day. Modern Medical has a solution - now with real outcomes. Opioids are the most common drugs prescribed in workers
Protecting your employees, physicians and you. Opioid abuse is being talked about every day. Modern Medical has a solution - now with real outcomes. Opioids are the most common drugs prescribed in workers
Medicines for Treating Depression. A Review of the Research for Adults
 Medicines for Treating Depression A Review of the Research for Adults Is This Information Right for Me? Yes, if: A doctor or other health care professional has told you that you have depression. Your doctor
Medicines for Treating Depression A Review of the Research for Adults Is This Information Right for Me? Yes, if: A doctor or other health care professional has told you that you have depression. Your doctor
Emergency and inpatient treatment of migraine: An American Headache Society
 Emergency and inpatient treatment of migraine: An American Headache Society survey. The objective of this study was to determine the practice preferences of AHS members for acute migraine treatment in
Emergency and inpatient treatment of migraine: An American Headache Society survey. The objective of this study was to determine the practice preferences of AHS members for acute migraine treatment in
ADVISORY OPINION THE USE OF CONTROLLED SUBSTANCES FOR THE TREATMENT OF CHRONIC PAIN
 Janice K. Brewer Governor Arizona State Board of Nursing 4747 North 7 th Street, Suite 200 Phoenix, AZ 85014-3655 Phone (602) 889-5150 Fax - (602) 889-5155 E-Mail: arizona@azbn.gov Home Page: http://www.azbn.gov
Janice K. Brewer Governor Arizona State Board of Nursing 4747 North 7 th Street, Suite 200 Phoenix, AZ 85014-3655 Phone (602) 889-5150 Fax - (602) 889-5155 E-Mail: arizona@azbn.gov Home Page: http://www.azbn.gov