Ovarian Cancer Treatment 2014 and beyond
|
|
|
- Leonard Daniels
- 8 years ago
- Views:
Transcription
1 Ovarian Cancer Treatment 2014 and beyond RK Potkul, MD, FACS, FACOG Mary Isabelle Caestecker Professor and Chair Department of Obstetrics and Gynecology Stritch School of Medicine Loyola University Chicago

2 The Impact of Ovarian Cancer Estimated incidence and mortality in the United States (2006) 1 20,810 new cases 15,310 deaths Approximately 6% of all cancer deaths in women Mortality Per 100,000 Women Uterine/Cervix Ovary 10-year survival: 8% 20%

3 Advanced Ovarian Cancer Study Agent Median Survival GOG GOG GOG GOG GOG GOG Ctxn, Doxo Ctxn, Doxo, CDDP (CAP) Paclitaxel, CDDP IP CDDP IP CDDP, IP Paclitaxel IP CDDP, IP Paclitaxel (Best Arm) 14.2 mo mo. 38 mo. 49 mo. 63 mo. 67 mo.
 14.2 mo. 19.7 mo. 38 mo. 49 mo. 63 mo.")
4 Management Points in Ovarian Cancer Progression Death Diagnosis Evaluation? SLL Secondary Surgery Symptoms Chemotherapy #1 Maintenance Chemo #2 Chemo #3+ Surgery Survivorship Supportive Care

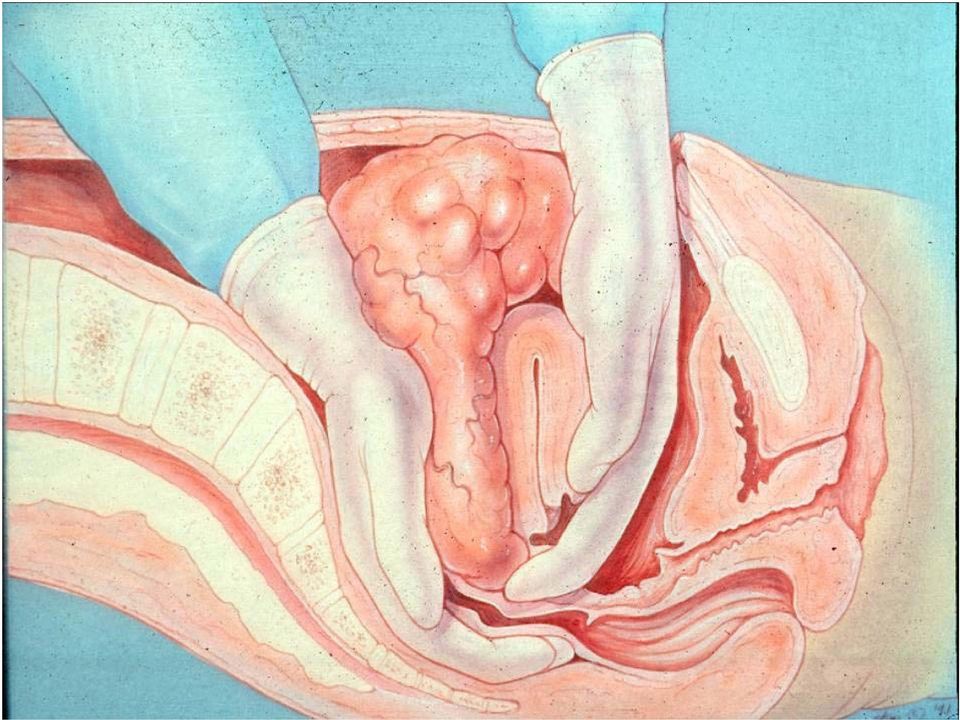
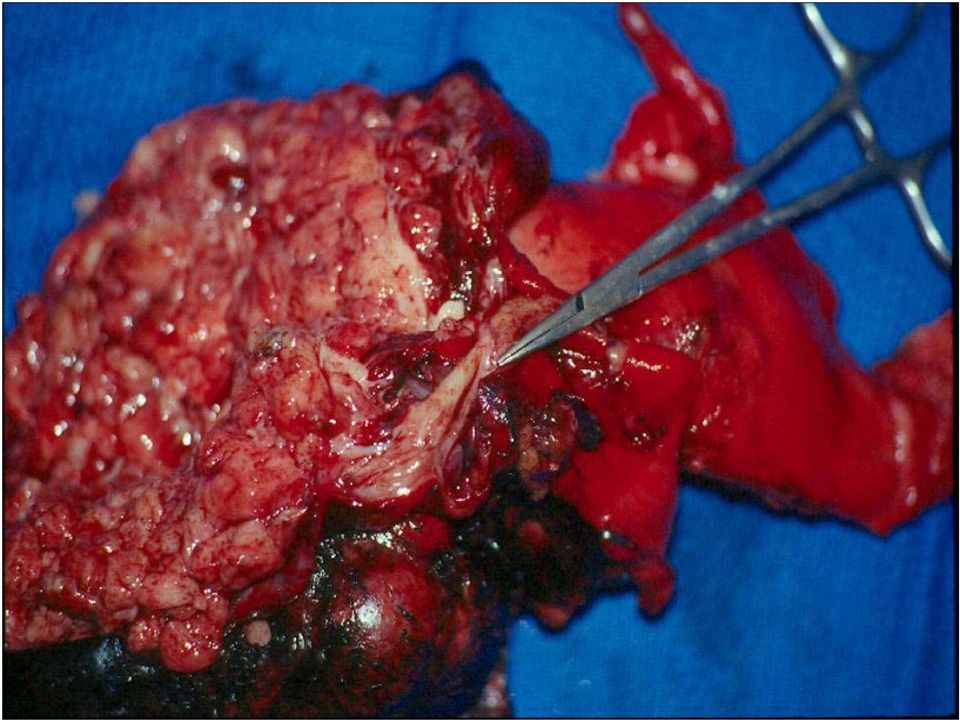
5 Opportunity #1 Optimal Tumor Debulking

6 Tumor Reductive Surgery Defined not by the surgery performed or the amount of tumor removed but by how large the residual disease is.

7

8

9

10

11

12

13
14
15

16

17 Ovarian Cancer: Survival by Residual Disease GOG Protocols (PR) 52 and 97
")
18 It s the Biology of the Disease If True, Then Patients Needing More Radical Surgery Should Do Worse Not Radical TAH BSO Omentectomy lymphadenectomy Radical Surgery = Radical TAH TAH and rectal resection splenectomy diaphragm surgery bowel resection extensive peritoneal stripping

19 IIIC and Carcinomatosis: Influence of Radical Surgery (N=144) Radical Surgery= Radical TAH TAH and rectal resection splenectomy diaphragm surgery bowel resection extensive peritoneal stripping

20 Management Points in Ovarian Cancer Progression Death Diagnosis Evaluation? SLL Secondary Surgery Symptoms Chemotherapy #1 Maintenance Chemo #2 Chemo #3+ Surgery Survivorship Supportive Care

21 2006 meta-analysis included 60 trials in women (n=15,609) with EOC A platinum-based combination was better than platinum monotherapy (hazard ratio [HR] favoring the combination 1.16, 95% CI ) A platinum-taxane combination was better than a platinum plus non-taxane combination (HR favoring platinum plus taxane 1.28, 95% CI ) J Natl Cancer Inst 2006; 98:1655.
22 International Study / GOG182 New Drugs, More Drugs, and New Sequences to avoid emerging drug resistance. Regimen I (control) Paclitaxel 175 mg/m 2 IV (3 h) d 1 Carboplatin AUC 6 IV d 1 Regimen II (triplet A) Paclitaxel 135 mg/m 2 IV (3 h) d 1 Carboplatin AUC 5 IV d 1 Gemcitabine 800 mg/m 2 /d IV d 1, 8 Randomization All patients Equal proportions on each regimen Primary end points: PFI,OS, RR Regimen III (triplet B) Paclitaxel 135 mg/m 2 IV (3 h) d 1 Carboplatin AUC 5 IV d 1 Doxil 30 mg/m 2 IV d 1 Every other cycle Regimen IV (sequential module A) Carboplatin AUC 5 IV d 3 Topotecan 1.5 mg/m 2 /d IV d 1-3 Regimen IV (sequential module B) Paclitaxel 175 mg/m 2 IV (3 h) d 1 Carboplatin AUC 6 IV d 1 Regimen V (sequential module A) Carboplatin AUC 6 IV d 8 Gemcitabine 1000 mg/m 2 /d IV d 1, 8 Regimen V (sequential module B) Paclitaxel 175 mg/m 2 IV (3 h) d 1 Carboplatin AUC 6 IV d 1 Regimens I and II: 8 cycles, 21-d cycle interval. Regimens IV and V: 4 cycles, 21-d cycle interval.
23 Drug Delivery for Ovarian Cancer: Intraperitoneal Therapy 1950 s: First use of IP for malignant ascites 1968: Long-term peritoneal access device 1978: Demonstration of slow peritoneal clearance of some drugs 1984: Feasibility of intermittent large volume intraperitoneal therapy 1996: First report of a survival benefit for IP vs. IV chemotherapy in advanced ovarian cancer
24 Assumption: IP Provides Pharmacological Benefit Drug Peak AUC Cisplatin Carboplatin Melphalan Adriamycin FU MTX Paclitaxel --- 1,000 Misleading Measure AUC of drug in dialysate to plasma Should be tumor to plasma Tumor penetration is superficial (1-2 mm) Efficacy requires good distribution
25 Intraperitoneal Chemotherapy Median PFS (mo) HR Median OS (mo) HR IV IP IV IP GOG 104 Alberts GOG 114 Markman (P = 0.02) (P = 0.01) (P = 0.05)
26 Ovarian Cancer: IP Chemotherapy
27 GOG-172 Survival IV: 18 mos IP: 24 mos HR: 0.80, P= 0.05 IV: 50 mos IP: 66 mos HR: 0.75, P= 0.03 Armstrong. N Engl J Med. 354:34, 2006
28
29 GOG 172: Toxicity Non-Hematologic IV IP GI Renal Fatigue Pain Metabolic Neuro Hematologic IV IP PLT Infection WBC
30 Quality of Life: GOG Pretreatment 4th Cycle Post-treatment 3-6 wks IV P = 0.03 P < P = P = NS IP Post-treatment 12 mos
31 Number of IP Courses Completed % Received Courses Completed Walker, Gynecol Oncol. 100:27, 2006
32
33
34 JAPANESE GOG Advanced stage ovarian cancer Conventional Regimen Six cycles paclitaxel (180 mg/m2, 3-h IV) plus carboplatin (AUC 6), given on day 1 of a 21- day cycle Dose-dense Regimen Six cycles paclitaxel (80 mg/m2; 1-h IV) given on days 1, 8, and 15 plus carboplatin given on day 1 of a 21-day cycle
35 JAPANESE GOG 631 total Dose-dense regimen, 312 Conventional regimen, 319 Toxicity Dose-dense regimen group n=113 Conventional regimen group n=69 Neutropenia dose-dense regimen, 286 [92%] of 312 conventional regimen, 276 [88%] of 314) Grade 3 and 4 anemia Dose-dense treatment group (214 [69%]) Conventional treatment group (137 [44%] p<0.0001
36 JAPANESE GOG Advanced stage ovarian cancer Conventional Regimen Six cycles paclitaxel (180 mg/m2, 3-h IV) plus carboplatin (AUC 6), given on day 1 of a 21- day cycle Dose-dense Regimen Six cycles paclitaxel (80 mg/m2; 1-h IV) given on days 1, 8, and 15 plus carboplatin given on day 1 of a 21-day cycle PFS 17.2m 3 YR SURVIVAL 65.1% PFS 28.0m* 3 YR SURVIVAL 72.1%* Katsumata N, Yasuda M, Takahashi FLancet Oct 17;374(9698):1303 5
37 GOG 262 Advanced stage ovarian cancer suboptimal Conventional Regimen Six cycles paclitaxel (175 mg/m2, 3-h IV) plus carboplatin (AUC 6), given on day 1 of a 21- day cycle Dose-dense Regimen Six cycles paclitaxel (80 mg/m2; 1-h IV) given on days 1, 8, and 15 plus carboplatin given on day 1 of a 21-day cycle
38 GOG #252 OPTIMAL & SUBOPTIMAL STAGE III & IV STANDARD IP IV TAXOL 135MG/M2 X3HRS DOSE DENSE IV COMBINATION
39 Incorporation of angiogenesis inhibitors GOG #218 STAGE III OR IV WITH GROSS RESIDUAL TUMOR CARBO AUC 6 TAXOL 175MG/M2 PLACEBO CARBO AUC 6 TAXOL 175MG/M2 BEVACIZUMAB PLACEBO PLACEBO BEVACIZUMAB 9/05 8/09
40 GOG #218 At a median followup of 17 months, there was no difference in PFS between group II and group I (median PFS, 10 and 11 months, respectively). Compared to group I, there was a significant increase in the median PFS in group III (14 months). There was no improvement in OS; median OS across all arms was approximately 39 months. The incidence of GI perforation or fistula formation was 3 percent in both bevacizumab containing arms versus 1 percent in the chemotherapy alone arm. N Engl J Med Dec;365(26):
41 Incorporation of angiogenesis inhibitors the National Comprehensive Cancer Network (NCCN) does not recomend bevacizumab routinely as part of the initial adjuvant therapy or as maintenance therapy following adjuvant therapy of advanced stage EOC Although actual cost data were not collected in GOG- 218, a subsequent modeled cost-effectiveness analysis using the available data on PFS and OS concluded that the cost-effectiveness ratio for the addition of bevacizumab to standard chemotherapy was unfavorable NCCN Guidelines Version
42 GOG #3001 Angiopoietin 1,2 AMG 386 Toxicity profile distinct from VEGF
43 Management Points in Ovarian Cancer Progression Death Diagnosis Evaluation? SLL Secondary Surgery Symptoms Chemotherapy #1 Maintenance Chemo #2 Chemo #3+ Surgery Survivorship Supportive Care
44 Management Points in Ovarian Cancer Progression Death Diagnosis Evaluation? SLL Secondary Surgery Symptoms Chemotherapy #1 Maintenance Chemo #2 Chemo #3+ Surgery Survivorship Supportive Care
45 Why Maintenance? Recurrence after clinical CR: 50-80% Recurrence after pathological CR: 40-60% Prognostic factors for recurrence: Tumor burden = residual disease Response to therapy = biology Unknowns Cure after Recurrence: Rare
46 Maintenance Therapy: Ovarian Cancer Progression Death Diagnosis Evaluation? SLL Secondary Surgery Symptoms Chemotherapy #1 Maintenance Chemo #2 Chemo #3+ Surgery Options: Radiation Immunotherapy Extension of first-line therapy Novel agents High-Dose (stem cell) Intraperitoneal (chemotherapy, radiation, immunotherapy, etc) vaccine Supportive Care
47 Consolidation or Maintainence chemotherapy What has been shown in clinical trials that appears to help: Oral altretamine IV Taxol monthly What has not helped : Five day topotecan as consolidation Ovarex Interferon Whole Abdomen Radiation. 12 cycles instead of 6 High dose chemotherapy 32 P
48 SWOG-9701 /GOG 178 Consolidation Trial: Schema Eligibility: Stage III-IV Clinically NED following platinum/paclitaxel No 2nd-look surgery R A N D O M I Z E Paclitaxel 135 mg/m 2 over 3 hrs Q 28 D x 3 cycles Paclitaxel 135 mg/m 2 over 3 hrs Q 28 D x 12 cycles Closed at Interim Analysis November 2001 by DSMB because the PFI for the 3 cycle arm was 21mos vs 28mos for the 12cycle arm with HR of 2.3 and p=.0035
49 Oregovomab (Ovarex ) Ovarian Cancer Clinical CR Normal CA125 Placebo Ovarex Outcome: TTP, OS Berek J Clin Oncol 22:3507, 2004
50 Interferon- Maintenance Hall, Br J Cancer 91: 621, 2004
51 Interferon- Maintenance Hall, Br J Cancer 91: 621, 2004
52 Vaccination Strategy Using Treg Depletion ± Ontak
53 Management Points in Ovarian Cancer Progression Death Diagnosis Evaluation? SLL Secondary Surgery Symptoms Chemotherapy #1 Maintenance Chemo #2 Chemo #3+ Surgery Survivorship Supportive Care
54 Recurrent Ovarian Cancer: Definition of Disease Sensitivity P R E V I O U S Refractory Time to Recurrence, Months X T R E A T M E N T Resistant Sensitive Really, Really Sensitive
55 The challenges to studying recurrent ovarian cancer Treatment (platinum) free interval predicts response more than which agent is used. Unique activity is best established in platinum resistant disease where a RR>20% is exciting. For third line platinum resistant pt 10%RR suggests activity. The end point should be PFS, very difficult to study OS when more tx to follow
56 Secondary Response to Platinum N = 176 pts Accrual: Responders = 125/211 regimens (55%) TFI 1 is related to response but not predictive individually TFI 2 < TFI 1 (N = 114, 97%) 3/4 exceptions received different chemo agents with platinum Duration of Prior Response & Secondary Response <12 mos 12 to to mos Markman. J Clin Oncol. 22:3120, 2004
57 Treatment-Free Interval and Survival N = 583 pts Phase II/III GINECO trials RECIST criteria of response Independent response effects (no prediction of response on the basis of prior drug or response to regimen) Days Platinum-Resistant Platinum-Sensitive Percent Prog 0-3 Non PD 3 to to PFS OS Response Lauraine, Proc ASCO #829, 2002
58 Therapeutic Options for Docetaxel Doxil Etoposide Gemcitabine Paclitaxel Platinum Topotecan Vinorelbine Ovarian Cancer Response Rate (%) Drug Platinum-Resistant Platinum-Sensitive 10% 25% 20% 55%
59 Gem/Carbo vs. Carbo: Design Recurrent Ov Ca 6+ mos after platinum Strata: PFI (6-12, > 12 mos) 1st-line therapy (Platinum +/- Paclitaxel) Measurable vs. Evaluable Primary Endpoint = PFS R A N D O M I Z A T I O N Gemcitabine 1000 mg/m2 d 1+8 Carboplatin AUC 4 d 1 q 21 x 6 (-10) Carboplatin AUC 5 d 1 q 21 x 6 (-10) (* Ann Oncol 2001; 12:1115) * Pfisterer, ASCO 2004, #5005
60 Progression-Free Survival HR = 0.72 (95% CI ) 0.8 Log-rank p-value = Progression-Free Probability Median = 5.8m ( m) Median = 8.6m ( m) Cb 178 pts / 162 evts GCb 178 pts / 163 evts months Pts at risk Cb GCb ASCO 04 #5005
61 Overall Survival Survival Probability HR = 0.96 (95% CI ) Log-rank p-value = Med = 17.3m ( m) Med = 18.0m ( m) Cb 178 pts / 126 evts GCb 178 pts / 127 evts Trial not powered for OS months Pts at risk Cb GCb ASCO 04 #5005
62 ICON IV: Schema Relapsed ovarian or primary Peritoneal requiring chemotherapy Previous platinum-based chemotherapy Prior chemotherapy: Carboplatin (34%) Cisplatin (30%) Paclitaxel/platinum (36%) TFI: >12 mos for 75% R A N D O M I Z E Conventional platinum-based chemotherapy Paclitaxel plus platinum Chemotherapy Ledermann JA, Lancet. 361:2099, 2003
63 ICON IV: Survival Median PFI: 9 vs. 12 mos Median OS: 24 vs. 29 mos Median Follow-up: 42 mos OR: 54 vs. 66% (P = 0.06)
64 Platinum Combinations: Summary Combination strategies appear to produce superior response rates and PFS Overall survival is the bar Unclear if sequential administration will reach the same endpoint QoL and toxicity are mandatory secondary endpoints
65 Neoadjuvant Chemotherapy giving pts 3-4 cycles of chemotherapy prior to debulking surgery Easier surgery Less hospital days Survival data mixed
66 EORTC/NCIC Neoadjuvant Chemotherapy 670 women with stage IIIC/IV EOC No difference in progression-free survival (PFS, 12 months in both groups) Similar overall survival in the neoadjuvant treatment group compared to those who underwent initial surgery (29 and 30 months) Lower rate of complications as compared to initial surgery N Engl J Med. 2010;363(10):943
67 SEER Databse and Neoadjuvant Chemotherapy 6844 women in this retrospective trial Significantly fewer ostomies placed (7.8 vs 19.2 percent), less small bowel resections (3.8 versus 6.3 percent), and less large bowel resections (11.1 versus 20.6 percent). Significant reduction in postoperative complications Among women with stage III disease, the risk of death at two years was higher following neoadjuvant chemotherapy [RR] 1.16 For women with stage IV EOC, there was a reduction in the risk of death at two years associated with neoadjuvant chemotherapy [RR] 0.85 Gynecol Oncol. 2011;123(3):461
68 In vitro chemosensitivity and resistance assays Chemo-FX assay or the Extreme Drug Resistance (EDR) assay ASCO concluded that the evidence is insufficient to justify the routine use of any of these assays oncologists should make chemotherapy treatment recommendations on the basis of published clinical trial reports J Clin Oncol. 2011;29(24):3328
69 PARP INHIBITORS Inhibitors of poly ADP ribose polymerase PARP1-protein important in repairing SS breaks-when these are not repaired DS breaks are formed with replication PARP inhibitors-cause multiple double strand breaks and tumors that have BRCA 1, BRCA 2 mutations cannot repair these and causes cell death Other cells sensitive to PARP inhibitors include tumors with PTEN mutations, PLAB2, radio sensitizer
70 Role of CA-125 surveillance Medical Research Council (MRC) 05 trial. In this study, 1442 women had their CA-125 levels checked every three months asymptomatic but whose CA-125 levels exceeded twice the upper limit of normal (n =527) were randomly assigned to immediate treatment or to treatment at the time of a clinical or symptomatic recurrence
71 Role of CA-125 surveillance Medical Research Council (MRC) 05 trial. In this study, 1442 women had their CA-125 levels checked every three months asymptomatic but whose CA-125 levels exceeded twice the upper limit of normal (n =527) were randomly assigned to immediate treatment or to treatment at the time of a clinical or symptomatic recurrence Second-line chemotherapy was started a median of five months earlier this did not contribute to improved survival immediate treatment had an adverse impact on quality of life
72 Role of CA-125 surveillance Following patients longitudinally by CA-125 may help identify patients for surgical treatment at recurrence a shorter time to surgery measured from the initial rise in CA-125 was associated with improved surgical outcome; the time from initial CA-125 elevation to surgery was five weeks in those optimally cytoreduced versus 16 weeks for those who were not Gynecol Oncol. 2011;121(2):249
73 DFS Stage I & % Stage III optimal 40% Stage III sub optimal 5-10% Stage IV 5-10%
74 Screening Unknown precancer condition Low detection High mortality No screening has yet proven to be effective
75 Prevention OCP Tubal Ligation Prophylactic Oophorectomy
76 OCP 6 years of use 60% Reduction Tubal Ligation Risk in General Population BRCA1.39 (.22.70) Both TL + OCP.28 (.15.50)
77 Risk of Ovarian Cancer General Population 1.4% BRCA % BRCA %
78 Prophylactic Salpingo-Oophorectomy 551 Women w/ BRCA1 or 2 mutation 292 Control Group - 58 Cancers - 6/58 Stage I (11%) 259 PO - 6 Stage I Ovarian Ca - 2 Additional Peritoneal Ca Risk Decreased from 20% to < 1% RR Breast CA.45 ( ) Rebbeck NEJM 2002
79 3 Unanswered Issues: 1) Optimal Time 2) Should Hysterectomy be included 3) Role of HRT
80 Optimal Time Deferred until childbearing complete BRCA 1 patients 11-21% CA risk by age 50 Defer till > 40 may lose breast protection 2-4 % rate of occult invasive carcinoma
81 Hysterectomy No consensus Should include bilateral salpingectomy Argue portion of tube in uterus is at theoretical risk Uterine cancer not over represented in BRCA2 Uterine cancer may be increased in BRCA1 (1-2%) Increase morbidity
82 Estrogens I just don t know what to think
83 HRT Effect on Breast Cancer Reduction Cohort of never users RR 0.42 Cohort of users & nonusers RR 0.53
84 HRT Effect on Breast Cancer Reduction Cohort of never users RR 0.42 Cohort of users & nonusers RR 0.53
85
86
87
88
89 Drug A Summary of Phase III Single Agent Trials: Recurrent Ovarian Cancer Drug B N TTP (wks) P OS (wks) P Comment Topotecan Paclitaxel vs 14 NS 61 vs. 43 NS Cross-over confirmed in 50% Paclitaxel (bolus) Paclitaxel (weekly) vs 26 NS 64 vs. 59 NS Less toxicity (wkly), no diff HSR Oxaliplatin Paclitaxel vs. 14 NS 42 vs. 37 NS 74% of cohort Platresistant PLD PLD Topotecan PLD Topotecan Paclitaxel Treosulfan Gemcitabine SGO vs vs vs vs 13 NS NS NS 60 vs vs vs. 48 PEND Cross-over Design NS NS % Plat-resist; PLD OS benefit in plat-sensitive subgroup All patients taxane-naïve 2nd-3rd line, Topo more heme All Plat-resistant Gr 3/4 PPE, mucositis (PLD), Gr 3/4 Heme
Chemotherapy in Ovarian Cancer. Dr R Jones Consultant Medical Oncologist South Wales Gynaecological Oncology Group
 Chemotherapy in Ovarian Cancer Dr R Jones Consultant Medical Oncologist South Wales Gynaecological Oncology Group Adjuvant chemotherapy for early stage EOC Fewer than 30% women present with FIGO stage
Chemotherapy in Ovarian Cancer Dr R Jones Consultant Medical Oncologist South Wales Gynaecological Oncology Group Adjuvant chemotherapy for early stage EOC Fewer than 30% women present with FIGO stage
U.S. Food and Drug Administration
 U.S. Food and Drug Administration Notice: Archived Document The content in this document is provided on the FDA s website for reference purposes only. It was current when produced, but is no longer maintained
U.S. Food and Drug Administration Notice: Archived Document The content in this document is provided on the FDA s website for reference purposes only. It was current when produced, but is no longer maintained
Maintenance therapy in in Metastatic NSCLC. Dr Amit Joshi Associate Professor Dept. Of Medical Oncology Tata Memorial Centre Mumbai
 Maintenance therapy in in Metastatic NSCLC Dr Amit Joshi Associate Professor Dept. Of Medical Oncology Tata Memorial Centre Mumbai Definition of Maintenance therapy The U.S. National Cancer Institute s
Maintenance therapy in in Metastatic NSCLC Dr Amit Joshi Associate Professor Dept. Of Medical Oncology Tata Memorial Centre Mumbai Definition of Maintenance therapy The U.S. National Cancer Institute s
OI PARP ΑΝΑΣΤΟΛΕΙΣ ΣΤΟΝ ΚΑΡΚΙΝΟ ΤΟΥ ΜΑΣΤΟΥ ΝΙΚΟΛΑΙΔΗ ΑΔΑΜΑΝΤΙΑ ΠΑΘΟΛΟΓΟΣ-ΟΓΚΟΛΟΓΟΣ Β ΟΓΚΟΛΟΓΙΚΗ ΚΛΙΝΙΚΗ ΝΟΣ. ΜΗΤΕΡΑ
 OI PARP ΑΝΑΣΤΟΛΕΙΣ ΣΤΟΝ ΚΑΡΚΙΝΟ ΤΟΥ ΜΑΣΤΟΥ ΝΙΚΟΛΑΙΔΗ ΑΔΑΜΑΝΤΙΑ ΠΑΘΟΛΟΓΟΣ-ΟΓΚΟΛΟΓΟΣ Β ΟΓΚΟΛΟΓΙΚΗ ΚΛΙΝΙΚΗ ΝΟΣ. ΜΗΤΕΡΑ Study Overview Inhibition of poly(adenosine diphosphate [ADP]-ribose) polymerase
OI PARP ΑΝΑΣΤΟΛΕΙΣ ΣΤΟΝ ΚΑΡΚΙΝΟ ΤΟΥ ΜΑΣΤΟΥ ΝΙΚΟΛΑΙΔΗ ΑΔΑΜΑΝΤΙΑ ΠΑΘΟΛΟΓΟΣ-ΟΓΚΟΛΟΓΟΣ Β ΟΓΚΟΛΟΓΙΚΗ ΚΛΙΝΙΚΗ ΝΟΣ. ΜΗΤΕΡΑ Study Overview Inhibition of poly(adenosine diphosphate [ADP]-ribose) polymerase
Management of stage III A-B of NSCLC. Hamed ALHusaini Medical Oncologist
 Management of stage III A-B of NSCLC Hamed ALHusaini Medical Oncologist Global incidence, CA cancer J Clin 2011;61:69-90 Stage III NSCLC Includes heterogeneous group of patients with differences in the
Management of stage III A-B of NSCLC Hamed ALHusaini Medical Oncologist Global incidence, CA cancer J Clin 2011;61:69-90 Stage III NSCLC Includes heterogeneous group of patients with differences in the
First-line chemotherapy for the treatment of women with epithelial ovarian cancer
 First-line chemotherapy for the treatment of women with epithelial ovarian cancer Recommendations for the use of first-line chemotherapy for the treatment of women with epithelial ovarian cancer June 2014
First-line chemotherapy for the treatment of women with epithelial ovarian cancer Recommendations for the use of first-line chemotherapy for the treatment of women with epithelial ovarian cancer June 2014
New Developments in the Treatment of Recurrent Ovarian Cancer and Evolving New Therapies
 New Developments in the Treatment of Recurrent Ovarian Cancer and Evolving New Therapies Alexi Wright, MD Dana-Farber Cancer Institute Harvard Medical School Email: alexi_wright@dfci.harvard.edu 617-632-3857
New Developments in the Treatment of Recurrent Ovarian Cancer and Evolving New Therapies Alexi Wright, MD Dana-Farber Cancer Institute Harvard Medical School Email: alexi_wright@dfci.harvard.edu 617-632-3857
Management of Platinum-Sensitive Recurrent Ovarian Cancer
 Management of Platinum-Sensitive Jacobus Pfisterer a and Jonathan A. Ledermann b The majority of patients with ovarian cancer will relapse despite state-of-the-art first-line surgery and chemotherapy.
Management of Platinum-Sensitive Jacobus Pfisterer a and Jonathan A. Ledermann b The majority of patients with ovarian cancer will relapse despite state-of-the-art first-line surgery and chemotherapy.
The role of PARP inhibitors in high grade serous ovarian cancers
 The role of PARP inhibitors in high grade serous ovarian cancers Jonathan Ledermann UCL Cancer Institute University College London ANZGOG-ASGO, Canberra, March 214 Cancer Research UK UCL Centre DNA Repair
The role of PARP inhibitors in high grade serous ovarian cancers Jonathan Ledermann UCL Cancer Institute University College London ANZGOG-ASGO, Canberra, March 214 Cancer Research UK UCL Centre DNA Repair
Latest developments in management. Gianfilippo Bertelli Consultant Medical Oncologist Swansea
 Latest developments in management Gianfilippo Bertelli Consultant Medical Oncologist Swansea Optimizing management of ovarian cancer in South Wales Diagnosis and referral pathways: Role of GPs, gynaecologists,
Latest developments in management Gianfilippo Bertelli Consultant Medical Oncologist Swansea Optimizing management of ovarian cancer in South Wales Diagnosis and referral pathways: Role of GPs, gynaecologists,
Selecting Second Line Treatment for Relapsing Epithelial Ovarian Cancer. Dr. Rebecca Kristeleit Prof. Jonathan Ledermann UCL, London, UK
 Selecting Second Line Treatment for Relapsing Epithelial Ovarian Cancer Dr. Rebecca Kristeleit Prof. Jonathan Ledermann UCL, London, UK Overview of Presentation This presentation will discuss the management
Selecting Second Line Treatment for Relapsing Epithelial Ovarian Cancer Dr. Rebecca Kristeleit Prof. Jonathan Ledermann UCL, London, UK Overview of Presentation This presentation will discuss the management
Clinical Trial Endpoints for Regulatory Approval First-Line Therapy for Advanced Ovarian Cancer
 Clinical Trial Endpoints for Regulatory Approval First-Line Therapy for Advanced Ovarian Cancer Elizabeth Eisenhauer MD FRCPC Options for Endpoints First-Line Trials in Advanced OVCA Overall Survival:
Clinical Trial Endpoints for Regulatory Approval First-Line Therapy for Advanced Ovarian Cancer Elizabeth Eisenhauer MD FRCPC Options for Endpoints First-Line Trials in Advanced OVCA Overall Survival:
Lenalidomide (LEN) in Patients with Transformed Lymphoma: Results From a Large International Phase II Study (NHL-003)
 in Patients with Transformed Lymphoma: Results From a Large International Phase II Study (NHL-003)") Lenalidomide (LEN) in Patients with Transformed Lymphoma: Results From a Large International Phase II Study (NHL-003) Reeder CB et al. Proc ASCO 2010;Abstract 8037. Introduction > Patients (pts) with low-grade
Lenalidomide (LEN) in Patients with Transformed Lymphoma: Results From a Large International Phase II Study (NHL-003) Reeder CB et al. Proc ASCO 2010;Abstract 8037. Introduction > Patients (pts) with low-grade
Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
 Efficacy Results from the ToGA Trial: A Phase III Study of Trastuzumab Added to Standard Chemotherapy in First-Line HER2- Positive Advanced Gastric Cancer Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
Efficacy Results from the ToGA Trial: A Phase III Study of Trastuzumab Added to Standard Chemotherapy in First-Line HER2- Positive Advanced Gastric Cancer Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
CHEMOTHERAPY FOR ADVANCED UROTHELIAL CANCER OF THE BLADDER. Walter Stadler, MD University of Chicago
 CHEMOTHERAPY FOR ADVANCED UROTHELIAL CANCER OF THE BLADDER Walter Stadler, MD University of Chicago Chemotherapy Doctor Terms Drugs used to treat cancer Will attack cancer no matter where it is located
CHEMOTHERAPY FOR ADVANCED UROTHELIAL CANCER OF THE BLADDER Walter Stadler, MD University of Chicago Chemotherapy Doctor Terms Drugs used to treat cancer Will attack cancer no matter where it is located
Prior Authorization Guideline
 Prior Authorization Guideline Guideline: PS Inj - Alimta Therapeutic Class: Antineoplastic Agents Therapeutic Sub-Class: Antifolates Client: PS Inj Approval Date: 8/2/2004 Revision Date: 12/5/2006 I. BENEFIT
Prior Authorization Guideline Guideline: PS Inj - Alimta Therapeutic Class: Antineoplastic Agents Therapeutic Sub-Class: Antifolates Client: PS Inj Approval Date: 8/2/2004 Revision Date: 12/5/2006 I. BENEFIT
Pancreatic Cancer: FDA Approved Treatments and Clinical Trials
 Pancreatic Cancer: FDA Approved Treatments and Clinical Trials Vincent J Picozzi MD MMM Virginia Mason Medical Center Seattle WA 1 Pancreatic cancer is the hardest cancer of all to treat 2 Pancreatic cancer:
Pancreatic Cancer: FDA Approved Treatments and Clinical Trials Vincent J Picozzi MD MMM Virginia Mason Medical Center Seattle WA 1 Pancreatic cancer is the hardest cancer of all to treat 2 Pancreatic cancer:
First-line chemotherapy for women with epithelial ovarian cancer
 First-line chemotherapy for women with epithelial ovarian cancer A systematic review July 2013 First line chemotherapy for women with epithelial ovarian cancer: a systematic review was prepared and produced
First-line chemotherapy for women with epithelial ovarian cancer A systematic review July 2013 First line chemotherapy for women with epithelial ovarian cancer: a systematic review was prepared and produced
Integrating Chemotherapy and Liver Surgery for the Management of Colorectal Metastases
 I Congresso de Oncologia D Or July 5-6, 2013 Integrating Chemotherapy and Liver Surgery for the Management of Colorectal Metastases Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University
I Congresso de Oncologia D Or July 5-6, 2013 Integrating Chemotherapy and Liver Surgery for the Management of Colorectal Metastases Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University
Adjuvant Therapy Non Small Cell Lung Cancer. Sunil Nagpal MD Director, Thoracic Oncology Jan 30, 2015
 Adjuvant Therapy Non Small Cell Lung Cancer Sunil Nagpal MD Director, Thoracic Oncology Jan 30, 2015 No Disclosures Number of studies Studies Per Month 12 10 8 6 4 2 0 1 2 3 4 5 6 7 8 9 10 11 12 1 2 3
Adjuvant Therapy Non Small Cell Lung Cancer Sunil Nagpal MD Director, Thoracic Oncology Jan 30, 2015 No Disclosures Number of studies Studies Per Month 12 10 8 6 4 2 0 1 2 3 4 5 6 7 8 9 10 11 12 1 2 3
Cancer Treatments Subcommittee of PTAC Meeting held 18 September 2015. (minutes for web publishing)
") Cancer Treatments Subcommittee of PTAC Meeting held 18 September 2015 (minutes for web publishing) Cancer Treatments Subcommittee minutes are published in accordance with the Terms of Reference for the
Cancer Treatments Subcommittee of PTAC Meeting held 18 September 2015 (minutes for web publishing) Cancer Treatments Subcommittee minutes are published in accordance with the Terms of Reference for the
Advances In Chemotherapy For Hormone Refractory Prostate Cancer. TAX 327 study results & SWOG 99-16 study results presented at ASCO 2004
 Ronald de Wit Rotterdam Cancer Institute The Netherlands Advances In Chemotherapy For Hormone Refractory Prostate Cancer TAX 327 study results & SWOG 99-16 study results presented at Slide 1 Prostate Cancer
Ronald de Wit Rotterdam Cancer Institute The Netherlands Advances In Chemotherapy For Hormone Refractory Prostate Cancer TAX 327 study results & SWOG 99-16 study results presented at Slide 1 Prostate Cancer
Hereditary Ovarian cancer: BRCA1 and BRCA2. Karen H. Lu MD September 22, 2013
 Hereditary Ovarian cancer: BRCA1 and BRCA2 Karen H. Lu MD September 22, 2013 Outline Hereditary Breast and Ovarian Cancer (HBOC) BRCA1/2 genes How to identify What it means to you What it means to your
Hereditary Ovarian cancer: BRCA1 and BRCA2 Karen H. Lu MD September 22, 2013 Outline Hereditary Breast and Ovarian Cancer (HBOC) BRCA1/2 genes How to identify What it means to you What it means to your
Treatment results with Bortezomib in multiple myeloma
 Treatment results with Bortezomib in multiple myeloma Prof. Dr. Orhan Sezer Hamburg University Medical Center Circulating proteasome levels are an independent prognostic factor in MM 1.0 Probability of
Treatment results with Bortezomib in multiple myeloma Prof. Dr. Orhan Sezer Hamburg University Medical Center Circulating proteasome levels are an independent prognostic factor in MM 1.0 Probability of
National Horizon Scanning Centre. Vandetanib (Zactima) for advanced or metastatic non-small cell lung cancer. December 2007
 for advanced or metastatic non-small cell lung cancer. December 2007") Vandetanib (Zactima) for advanced or metastatic non-small cell lung cancer December 2007 This technology summary is based on information available at the time of research and a limited literature search.
Vandetanib (Zactima) for advanced or metastatic non-small cell lung cancer December 2007 This technology summary is based on information available at the time of research and a limited literature search.
New Treatment Options for Breast Cancer
 New Treatment Options for Breast Cancer Brandon Vakiner, PharmD., BCOP Clinical Pharmacy Specialist - Oncology The University of Iowa Hospitals and Clinics Assistant Professor (Clinical) University of
New Treatment Options for Breast Cancer Brandon Vakiner, PharmD., BCOP Clinical Pharmacy Specialist - Oncology The University of Iowa Hospitals and Clinics Assistant Professor (Clinical) University of
Everolimus plus exemestane for second-line endocrine treatment of oestrogen receptor positive metastatic breast cancer
 LONDON CANCER NEWS DRUGS GROUP RAPID REVIEW Everolimus plus exemestane for second-line endocrine treatment of oestrogen receptor positive metastatic breast cancer Everolimus plus exemestane for second-line
LONDON CANCER NEWS DRUGS GROUP RAPID REVIEW Everolimus plus exemestane for second-line endocrine treatment of oestrogen receptor positive metastatic breast cancer Everolimus plus exemestane for second-line
Avastin in breast cancer: Summary of clinical data
 Avastin in breast cancer: Summary of clinical data Worldwide, over one million people are diagnosed with breast cancer every year 1. It is the most frequently diagnosed cancer in women 1,2, and the leading
Avastin in breast cancer: Summary of clinical data Worldwide, over one million people are diagnosed with breast cancer every year 1. It is the most frequently diagnosed cancer in women 1,2, and the leading
January 2013 LONDON CANCER NEW DRUGS GROUP RAPID REVIEW. Summary. Contents
 LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Paclitaxel albumin (Abraxane ) as a substitute for docetaxel/paclitaxel for cancer Paclitaxel albumin (Abraxane ) as a substitute for docetaxel/ paclitaxel for
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Paclitaxel albumin (Abraxane ) as a substitute for docetaxel/paclitaxel for cancer Paclitaxel albumin (Abraxane ) as a substitute for docetaxel/ paclitaxel for
Frequency of NHL Subtypes in Adults
 Chemotherapy Options Stephanie A. Gregory, M.D. The Elodia Kehm Professor of Medicine Director, Section of Hematology Rush University Medical Center Chicago, Illinois Frequency of NHL Subtypes in Adults
Chemotherapy Options Stephanie A. Gregory, M.D. The Elodia Kehm Professor of Medicine Director, Section of Hematology Rush University Medical Center Chicago, Illinois Frequency of NHL Subtypes in Adults
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_stem-cell_transplantation_for_epithelial_ovarian_cancer 2/2001 11/2015 11/2016 11/2015 Description
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_stem-cell_transplantation_for_epithelial_ovarian_cancer 2/2001 11/2015 11/2016 11/2015 Description
PARP Inhibitors in Lung Cancer. Primo N. Lara, Jr., MD Professor of Medicine UC Davis Comprehensive Cancer Center
 PARP Inhibitors in Lung Cancer Primo N. Lara, Jr., MD Professor of Medicine UC Davis Comprehensive Cancer Center Poly (ADP-ribose) Polymerase (PARP): Mechanism of Action PARPs: family of enzymes that repair
PARP Inhibitors in Lung Cancer Primo N. Lara, Jr., MD Professor of Medicine UC Davis Comprehensive Cancer Center Poly (ADP-ribose) Polymerase (PARP): Mechanism of Action PARPs: family of enzymes that repair
Role of taxanes in the treatment of advanced NHL patients: A randomized study of 87 cases
 Role of taxanes in the treatment of advanced NHL patients: A randomized study of 87 cases R. Shraddha, P.N. Pandit Radium Institute, Patna Medical College and Hospital, Patna, India Abstract NHL is a highly
Role of taxanes in the treatment of advanced NHL patients: A randomized study of 87 cases R. Shraddha, P.N. Pandit Radium Institute, Patna Medical College and Hospital, Patna, India Abstract NHL is a highly
GUIDELINES FOR THE MANAGEMENT OF LUNG CANCER
 GUIDELINES FOR THE MANAGEMENT OF LUNG CANCER BY Ali Shamseddine, MD (Coordinator); as04@aub.edu.lb Fady Geara, MD Bassem Shabb, MD Ghassan Jamaleddine, MD CLINICAL PRACTICE GUIDELINES FOR THE TREATMENT
GUIDELINES FOR THE MANAGEMENT OF LUNG CANCER BY Ali Shamseddine, MD (Coordinator); as04@aub.edu.lb Fady Geara, MD Bassem Shabb, MD Ghassan Jamaleddine, MD CLINICAL PRACTICE GUIDELINES FOR THE TREATMENT
NCCN Non-Small Cell Lung Cancer V.1.2011 Update Meeting 07/09/10
 Guideline Page and Request NSCL-3 Stage IA, margins positive delete the recommendation for chemoradiation. Stage IB, IIA, margins positive delete the recommendation for chemoradiation + Stage IIA, Stage
Guideline Page and Request NSCL-3 Stage IA, margins positive delete the recommendation for chemoradiation. Stage IB, IIA, margins positive delete the recommendation for chemoradiation + Stage IIA, Stage
New Directions in Treatment of Ovarian Cancer. Amit M. Oza Princess Margaret Hospital University of Toronto
 New Directions in Treatment of Ovarian Cancer Amit M. Oza Princess Margaret Hospital University of Toronto Newly diagnosed: scenario Ist line Surgery chemotherapy Cure If can t cure can we turn into chronic
New Directions in Treatment of Ovarian Cancer Amit M. Oza Princess Margaret Hospital University of Toronto Newly diagnosed: scenario Ist line Surgery chemotherapy Cure If can t cure can we turn into chronic
New developments and controversies in breast cancer treatment: PARP Inhibitors: a breakthrough?
 New developments and controversies in breast cancer treatment: PARP Inhibitors: a breakthrough? F. Cardoso, MD Champalimaud Cancer Center Lisbon, Portugal BBM 2010 Thank you to A Tutt & PRIME Oncology
New developments and controversies in breast cancer treatment: PARP Inhibitors: a breakthrough? F. Cardoso, MD Champalimaud Cancer Center Lisbon, Portugal BBM 2010 Thank you to A Tutt & PRIME Oncology
Adiuwantowe i neoadiuwantowe leczenie chorych na zaawansowanego raka żołądka
 Adiuwantowe i neoadiuwantowe leczenie chorych na zaawansowanego raka żołądka Neoadiuvant and adiuvant therapy for advanced gastric cancer Franco Roviello, IT Neoadjuvant and adjuvant therapy for advanced
Adiuwantowe i neoadiuwantowe leczenie chorych na zaawansowanego raka żołądka Neoadiuvant and adiuvant therapy for advanced gastric cancer Franco Roviello, IT Neoadjuvant and adjuvant therapy for advanced
La Chemioterapia Adiuvante Dose-Dense. Lo studio GIM 2. Alessandra Fabi
 La Chemioterapia Adiuvante Dose-Dense Lo studio GIM 2 Alessandra Fabi San Antonio Breast Cancer Symposium -December 10-14, 2013 GIM 2 study Epirubicin and Cyclophosphamide (EC) followed by Paclitaxel (T)
La Chemioterapia Adiuvante Dose-Dense Lo studio GIM 2 Alessandra Fabi San Antonio Breast Cancer Symposium -December 10-14, 2013 GIM 2 study Epirubicin and Cyclophosphamide (EC) followed by Paclitaxel (T)
What is the optimal sequence of anti-her2 therapy in metastatic breast cancer?
 What is the optimal sequence of anti-her2 therapy in metastatic breast cancer? David Miles Mount Vernon Cancer Centre Northwood Middlesex UKBCM mee)ng: London 2013 Herceptin plus a taxoid extends survival
What is the optimal sequence of anti-her2 therapy in metastatic breast cancer? David Miles Mount Vernon Cancer Centre Northwood Middlesex UKBCM mee)ng: London 2013 Herceptin plus a taxoid extends survival
Management of low grade glioma s: update on recent trials
 Management of low grade glioma s: update on recent trials M.J. van den Bent The Brain Tumor Center at Erasmus MC Cancer Center Rotterdam, the Netherlands Low grades Female, born 1976 1 st seizure 2005,
Management of low grade glioma s: update on recent trials M.J. van den Bent The Brain Tumor Center at Erasmus MC Cancer Center Rotterdam, the Netherlands Low grades Female, born 1976 1 st seizure 2005,
Drug/Drug Combination: Bevacizumab in combination with chemotherapy
 AHFS Final Determination of Medical Acceptance: Off-label Use of Bevacizumab in Combination with Chemotherapy for the Treatment of Metastatic Breast Cancer Previously Treated with Cytotoxic Chemotherapy
AHFS Final Determination of Medical Acceptance: Off-label Use of Bevacizumab in Combination with Chemotherapy for the Treatment of Metastatic Breast Cancer Previously Treated with Cytotoxic Chemotherapy
Ovarian Cancer Genetic Testing: Why, When, How?
 Ovarian Cancer Genetic Testing: Why, When, How? Jeffrey Dungan, MD Associate Professor Division of Clinical Genetics Department of Obstetrics & Gynecology Northwestern University Feinberg School of Medicine
Ovarian Cancer Genetic Testing: Why, When, How? Jeffrey Dungan, MD Associate Professor Division of Clinical Genetics Department of Obstetrics & Gynecology Northwestern University Feinberg School of Medicine
Ovarian Cancer and Modern Immunotherapy: Regulatory Strategies for Drug Development
 Ovarian Cancer and Modern Immunotherapy: Regulatory Strategies for Drug Development Sanjeeve Bala, MD, MPH Ovarian Cancer Endpoints Workshop FDA White Oak September 3, 2015 Overview Immune agents from
Ovarian Cancer and Modern Immunotherapy: Regulatory Strategies for Drug Development Sanjeeve Bala, MD, MPH Ovarian Cancer Endpoints Workshop FDA White Oak September 3, 2015 Overview Immune agents from
NATIONAL CANCER DRUG FUND PRIORITISATION SCORES
 NATIONAL CANCER DRUG FUND PRIORITISATION SCORES Drug Indication Regimen (where appropriate) BORTEZOMIB In combination with dexamethasone (VD), or with dexamethasone and thalidomide (VTD), is indicated
NATIONAL CANCER DRUG FUND PRIORITISATION SCORES Drug Indication Regimen (where appropriate) BORTEZOMIB In combination with dexamethasone (VD), or with dexamethasone and thalidomide (VTD), is indicated
COMMISSIONING. for ULTRA-RADICAL SURGERY ADVANCED OVARIAN CANCER
 COMMISSIONING for ULTRA-RADICAL SURGERY in ADVANCED OVARIAN CANCER WHY THIS MUST HAPPEN PERSPECTIVE COMMISSIONING FOR WHO, FOR WHAT? Biological Basis Surgical Basis International and national standards
COMMISSIONING for ULTRA-RADICAL SURGERY in ADVANCED OVARIAN CANCER WHY THIS MUST HAPPEN PERSPECTIVE COMMISSIONING FOR WHO, FOR WHAT? Biological Basis Surgical Basis International and national standards
EPITHELIAL OVARIAN CANCER
 EPITHELIAL OVARIAN CANCER Executive Summary Epithelial ovarian cancer is the most common type of ovarian cancer and the most aggressive gynecological malignancy. Approximately 70% of patients are diagnosed
EPITHELIAL OVARIAN CANCER Executive Summary Epithelial ovarian cancer is the most common type of ovarian cancer and the most aggressive gynecological malignancy. Approximately 70% of patients are diagnosed
Clinical Trial Design. Sponsored by Center for Cancer Research National Cancer Institute
 Clinical Trial Design Sponsored by Center for Cancer Research National Cancer Institute Overview Clinical research is research conducted on human beings (or on material of human origin such as tissues,
Clinical Trial Design Sponsored by Center for Cancer Research National Cancer Institute Overview Clinical research is research conducted on human beings (or on material of human origin such as tissues,
Anti-PD1 Agents: Immunotherapy agents in the treatment of metastatic melanoma. Claire Vines, 2016 Pharm.D. Candidate
 + Anti-PD1 Agents: Immunotherapy agents in the treatment of metastatic melanoma Claire Vines, 2016 Pharm.D. Candidate + Disclosure I have no conflicts of interest to disclose. + Objectives Summarize NCCN
+ Anti-PD1 Agents: Immunotherapy agents in the treatment of metastatic melanoma Claire Vines, 2016 Pharm.D. Candidate + Disclosure I have no conflicts of interest to disclose. + Objectives Summarize NCCN
Avastin in breast cancer: Summary of clinical data
 Avastin in breast cancer: Summary of clinical data Worldwide, over one million people are diagnosed with breast cancer every year 1. It is the most frequently diagnosed cancer in women 1,2, and the leading
Avastin in breast cancer: Summary of clinical data Worldwide, over one million people are diagnosed with breast cancer every year 1. It is the most frequently diagnosed cancer in women 1,2, and the leading
Treatment of Metastatic Non-Small Cell Lung Cancer: A Systematic Review of Comparative Effectiveness and Cost Effectiveness
 Treatment of Metastatic Non-Small Cell Lung Cancer: A Systematic Review of Comparative Effectiveness and Cost Effectiveness Investigators: Paul G. Shekelle, MD, PhD, Director Alicia R. Maher, MD Clinical
Treatment of Metastatic Non-Small Cell Lung Cancer: A Systematic Review of Comparative Effectiveness and Cost Effectiveness Investigators: Paul G. Shekelle, MD, PhD, Director Alicia R. Maher, MD Clinical
Come è cambiata la storia naturale della malattia
 Malattia Metastatica del Carcinoma del Grosso Intestino Tecniche e terapie Innovative Come è cambiata la storia naturale della malattia Antonio Frassoldati Oncologia Clinica - Ferrara 29 ottobre 2011 Colorectal
Malattia Metastatica del Carcinoma del Grosso Intestino Tecniche e terapie Innovative Come è cambiata la storia naturale della malattia Antonio Frassoldati Oncologia Clinica - Ferrara 29 ottobre 2011 Colorectal
PARP INHIBITORS IN OVARIAN CANCER. A 2011 PERSPECTIVE
 PARP INHIBITORS IN OVARIAN CANCER. A 2011 PERSPECTIVE Prof S.B. Kaye Royal Marsden Hospital, London MD Anderson Cancer Centre December 2011 DISCLOSURES Received honoraria as member of Advisory Boards to
PARP INHIBITORS IN OVARIAN CANCER. A 2011 PERSPECTIVE Prof S.B. Kaye Royal Marsden Hospital, London MD Anderson Cancer Centre December 2011 DISCLOSURES Received honoraria as member of Advisory Boards to
Columbia University Mesothelioma Applied Research Foundation - 2009 - www.curemeso.org. Mesothelioma Center www.mesocenter.org
 Columbia University Mesothelioma Center www.mesocenter.org Multimodal clinical trials, treatment (surgery, radiation, chemotherapy) Peritoneal mesothelioma program Immunotherapy translational, experimental
Columbia University Mesothelioma Center www.mesocenter.org Multimodal clinical trials, treatment (surgery, radiation, chemotherapy) Peritoneal mesothelioma program Immunotherapy translational, experimental
Treatment of Metastatic Breast Cancer: Endocrine Therapies. Robert W. Carlson, M.D. Professor of Medicine Stanford University
 Treatment of Metastatic Breast Cancer: Endocrine Therapies Robert W. Carlson, M.D. Professor of Medicine Stanford University MDACC Experience with FAC in Chemotherapy-Naive MBC Greenberg et al, J Clin
Treatment of Metastatic Breast Cancer: Endocrine Therapies Robert W. Carlson, M.D. Professor of Medicine Stanford University MDACC Experience with FAC in Chemotherapy-Naive MBC Greenberg et al, J Clin
Carcinoma of the Cervix. Kathleen M. Schmeler, MD Associate Professor Department of Gynecologic Oncology
 Carcinoma of the Cervix Kathleen M. Schmeler, MD Associate Professor Department of Gynecologic Oncology Cervical Cancer Treatment Treatment Microinvasive (Stage IA1): Simple (extrafascial) hysterectomy/cone
Carcinoma of the Cervix Kathleen M. Schmeler, MD Associate Professor Department of Gynecologic Oncology Cervical Cancer Treatment Treatment Microinvasive (Stage IA1): Simple (extrafascial) hysterectomy/cone
Background. t 1/2 of 3.7 4.7 days allows once-daily dosing (1.5 mg) with consistent serum concentration 2,3 No interaction with CYP3A4 inhibitors 4
 with consistent serum concentration 2,3 No interaction with CYP3A4 inhibitors 4") Abstract No. 4501 Tivozanib versus sorafenib as initial targeted therapy for patients with advanced renal cell carcinoma: Results from a Phase III randomized, open-label, multicenter trial R. Motzer, D.
Abstract No. 4501 Tivozanib versus sorafenib as initial targeted therapy for patients with advanced renal cell carcinoma: Results from a Phase III randomized, open-label, multicenter trial R. Motzer, D.
Re irradiation Using HDR Interstitial Brachytherapy for Locally Recurrent. Disclosure
 Re irradiation Using HDR Interstitial Brachytherapy for Locally Recurrent Cervical lcancer Yasuo Yoshioka, MD Department of Radiation Oncology Osaka University Graduate School of Medicine Osaka, Japan
Re irradiation Using HDR Interstitial Brachytherapy for Locally Recurrent Cervical lcancer Yasuo Yoshioka, MD Department of Radiation Oncology Osaka University Graduate School of Medicine Osaka, Japan
What is the reference cytotoxic regimen in advanced gastric cancer?
 What is the reference cytotoxic regimen in advanced gastric cancer? Florian Lordick Professor of Oncology Director of the University Cancer Center Leipzig (UCCL) Germany What we know from clinical research.
What is the reference cytotoxic regimen in advanced gastric cancer? Florian Lordick Professor of Oncology Director of the University Cancer Center Leipzig (UCCL) Germany What we know from clinical research.
SMALL CELL LUNG CANCER
 Protocol for Planning and Treatment The process to be followed in the management of: SMALL CELL LUNG CANCER Patient information given at each stage following agreed information pathway 1. DIAGNOSIS New
Protocol for Planning and Treatment The process to be followed in the management of: SMALL CELL LUNG CANCER Patient information given at each stage following agreed information pathway 1. DIAGNOSIS New
the standard of care 2009 5/1/2009 Mesothelioma: The standard of care take home messages PILC 2006 Jan.vanmeerbeeck@ugent.be Brussels, March 7, 2009
 Mesothelioma: The standard of care Jan.vanmeerbeeck@ugent.be Brussels, March 7, 2009 take home messages PILC 2006 All patients should receive adequate palliation of dyspnea and pain before starting chemotherapy
Mesothelioma: The standard of care Jan.vanmeerbeeck@ugent.be Brussels, March 7, 2009 take home messages PILC 2006 All patients should receive adequate palliation of dyspnea and pain before starting chemotherapy
Trials in Elderly Melanoma Patients (with a focus on immunotherapy)
") Trials in Elderly Melanoma Patients (with a focus on immunotherapy) Where we were Immunotherapy Trials: past and present Relevance for real world practice Where we are SIOG October 2012 James Larkin FRCP
Trials in Elderly Melanoma Patients (with a focus on immunotherapy) Where we were Immunotherapy Trials: past and present Relevance for real world practice Where we are SIOG October 2012 James Larkin FRCP
STEM CELL TRANSPLANTATION IN MULTIPLE MYELOMA
 STEM CELL TRANSPLANTATION IN MULTIPLE MYELOMA Sundar Jagannath MD Professor of Medicine St. Vincent s Comprehensive Cancer Center New York, NY Where is transplant today in the management of Myeloma? Autologous
STEM CELL TRANSPLANTATION IN MULTIPLE MYELOMA Sundar Jagannath MD Professor of Medicine St. Vincent s Comprehensive Cancer Center New York, NY Where is transplant today in the management of Myeloma? Autologous
Malignant Mesothelioma State of the Art
 Malignant Mesothelioma State of the Art Paul Baas The Netherlands Cancer Institute August 12, 2011, Carlsbad, CA Summary Diagnosis; epithelial type subdivided Pleiomorphic vs other Staging: IASLC-IMIG
Malignant Mesothelioma State of the Art Paul Baas The Netherlands Cancer Institute August 12, 2011, Carlsbad, CA Summary Diagnosis; epithelial type subdivided Pleiomorphic vs other Staging: IASLC-IMIG
THE SECRETS OF OUR SUCCESS
 THE SECRETS OF OUR SUCCESS QUALITY OF LIFE STUDIES OF THE NCIC Andrea Bezjak, MDCM, MSc,, FRCPC Chair, NCIC CTG QOL Committee Outline of the Presentation Can we consider NCIC CTG QOL activities a success?
THE SECRETS OF OUR SUCCESS QUALITY OF LIFE STUDIES OF THE NCIC Andrea Bezjak, MDCM, MSc,, FRCPC Chair, NCIC CTG QOL Committee Outline of the Presentation Can we consider NCIC CTG QOL activities a success?
Multiple Myeloma: Novel Agents. Robert A. Kyle, M.D. Germany June 28, 2008. Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida
 Multiple Myeloma: Novel Agents Robert A. Kyle, M.D. Germany June 28, 2008 Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida Multiple Myeloma Untreated Initial Therapy Transplant eligible Multiple
Multiple Myeloma: Novel Agents Robert A. Kyle, M.D. Germany June 28, 2008 Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida Multiple Myeloma Untreated Initial Therapy Transplant eligible Multiple
with ovarian cancer exhibit an initial response. 5 In addition, the majority of
 Research ONCOLOGY Impact of a chemoresponse assay on treatment costs for recurrent ovarian cancer Laura J. Havrilesky, MD, MHSc; Thomas C. Krivak, MD; John W. Mucenski, PharmD; Evan R. Myers, MD, MPH OBJECTIVE:
Research ONCOLOGY Impact of a chemoresponse assay on treatment costs for recurrent ovarian cancer Laura J. Havrilesky, MD, MHSc; Thomas C. Krivak, MD; John W. Mucenski, PharmD; Evan R. Myers, MD, MPH OBJECTIVE:
Management of Peritoneal Metastases (PM) from colorectal cancers: New Perspectives. Dominique ELIAS
 from colorectal cancers: New Perspectives. Dominique ELIAS") Management of Peritoneal Metastases (PM) from colorectal cancers: New Perspectives Dominique ELIAS Declaration of interest BOARDS Congress and teaching 0 Merck 0 Ipsen Novartis Sanofi Trials The peritoneum
Management of Peritoneal Metastases (PM) from colorectal cancers: New Perspectives Dominique ELIAS Declaration of interest BOARDS Congress and teaching 0 Merck 0 Ipsen Novartis Sanofi Trials The peritoneum
Recommendation Strength Strong, supported by the evidence and expert consensus. Recommendation Benefit/Harm Evidence Quality
 CHEMO- AND TARGETED THERAPY FOR WOMEN WITH HER2 NEGATIVE (OR UNKNOWN) ADVANCED BREAST Benefit/Harm Evidence Quality 1: Endocrine therapy, rather than chemotherapy, should be offered as the standard firstline
CHEMO- AND TARGETED THERAPY FOR WOMEN WITH HER2 NEGATIVE (OR UNKNOWN) ADVANCED BREAST Benefit/Harm Evidence Quality 1: Endocrine therapy, rather than chemotherapy, should be offered as the standard firstline
Non-small cell lung cancer, advanced or metastatic, switch-therapy after gemcitabine/carboplatin
 COMPENDIA TRANSPARENCY TRACKING FORM DRUG: Docetaxel INDICATION: Non-small cell lung cancer, advanced or metastatic, switch-therapy after gemcitabine/carboplatin COMPENDIA TRANSPARENCY REQUIREMENTS 1 Provide
COMPENDIA TRANSPARENCY TRACKING FORM DRUG: Docetaxel INDICATION: Non-small cell lung cancer, advanced or metastatic, switch-therapy after gemcitabine/carboplatin COMPENDIA TRANSPARENCY REQUIREMENTS 1 Provide
Is the third-line chemotherapy feasible for non-small cell lung cancer? A retrospective study
 Turkish Journal of Cancer Volume 34, No.1, 2004 19 Is the third-line chemotherapy feasible for non-small cell lung cancer? A retrospective study MUSTAFA ÖZDO AN, MUSTAFA SAMUR, HAKAN BOZCUK, ERKAN ÇOBAN,
Turkish Journal of Cancer Volume 34, No.1, 2004 19 Is the third-line chemotherapy feasible for non-small cell lung cancer? A retrospective study MUSTAFA ÖZDO AN, MUSTAFA SAMUR, HAKAN BOZCUK, ERKAN ÇOBAN,
7. Prostate cancer in PSA relapse
 7. Prostate cancer in PSA relapse A patient with prostate cancer in PSA relapse is one who, having received a primary treatment with intent to cure, has a raised PSA (prostate-specific antigen) level defined
7. Prostate cancer in PSA relapse A patient with prostate cancer in PSA relapse is one who, having received a primary treatment with intent to cure, has a raised PSA (prostate-specific antigen) level defined
Metastatic Breast Cancer 201. Carolyn B. Hendricks, MD October 29, 2011
 Metastatic Breast Cancer 201 Carolyn B. Hendricks, MD October 29, 2011 Overview Is rebiopsy necessary at the time of recurrence or progression of disease? How dose a very aggressive treatment upfront compare
Metastatic Breast Cancer 201 Carolyn B. Hendricks, MD October 29, 2011 Overview Is rebiopsy necessary at the time of recurrence or progression of disease? How dose a very aggressive treatment upfront compare
Future Directions in Clinical Research. Karen Kelly, MD Associate Director for Clinical Research UC Davis Cancer Center
 Future Directions in Clinical Research Karen Kelly, MD Associate Director for Clinical Research UC Davis Cancer Center Outline 1. Status of Cancer Treatment 2. Overview of Clinical Research at UCDCC 3.
Future Directions in Clinical Research Karen Kelly, MD Associate Director for Clinical Research UC Davis Cancer Center Outline 1. Status of Cancer Treatment 2. Overview of Clinical Research at UCDCC 3.
Cytotoxic Therapy in Metastatic Breast Cancer
 Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Cytotoxic Therapy in Metastatic Breast Cancer Cytotoxic Therapy in Metastatic Breast Cancer Version 2002: von Minckwitz Versions
Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Cytotoxic Therapy in Metastatic Breast Cancer Cytotoxic Therapy in Metastatic Breast Cancer Version 2002: von Minckwitz Versions
Chemotherapy or Not? Anthracycline or Not? Taxane or Not? Does Density Matter? Chemotherapy in Luminal Breast Cancer: Choice of Regimen.
 Chemotherapy in Luminal Breast Cancer: Choice of Regimen Andrew D. Seidman, MD Attending Physician Breast Cancer Medicine Service Memorial Sloan Kettering Cancer Center Professor of Medicine Weill Cornell
Chemotherapy in Luminal Breast Cancer: Choice of Regimen Andrew D. Seidman, MD Attending Physician Breast Cancer Medicine Service Memorial Sloan Kettering Cancer Center Professor of Medicine Weill Cornell
New Trends & Current Research in the Treatment of Lung Cancer, Pt. II
 New Trends & Current esearch in the Treatment of Lung Cancer, Pt. II Howard (Jack) West, MD President & CEO, GACE Medical Director, Thoracic Oncology Program Swedish Cancer Institute Seattle, WA Cancer
New Trends & Current esearch in the Treatment of Lung Cancer, Pt. II Howard (Jack) West, MD President & CEO, GACE Medical Director, Thoracic Oncology Program Swedish Cancer Institute Seattle, WA Cancer
New Targets and Treatments for Follicular Lymphoma. Disclosures
 Winship Cancer Institute of Emory University New Targets and Treatments for Follicular Lymphoma Jonathon B. Cohen, MD, MS Assistant Professor Div of BMT, Emory University Disclosures Consulting fees from:
Winship Cancer Institute of Emory University New Targets and Treatments for Follicular Lymphoma Jonathon B. Cohen, MD, MS Assistant Professor Div of BMT, Emory University Disclosures Consulting fees from:
What is the Optimal Front-Line Treatment for mrcc? Michael B. Atkins, MD Deputy Director, Georgetown-Lombardi Comprehensive Cancer Center
 What is the Optimal Front-Line Treatment for mrcc? Michael B. Atkins, MD Deputy Director, Georgetown-Lombardi Comprehensive Cancer Center The Case for Immunotherapy in mrcc 1. Achieves patient s goal 2.
What is the Optimal Front-Line Treatment for mrcc? Michael B. Atkins, MD Deputy Director, Georgetown-Lombardi Comprehensive Cancer Center The Case for Immunotherapy in mrcc 1. Achieves patient s goal 2.
Corso Integrato di Clinica Medica ONCOLOGIA MEDICA AA 2010-2011 LUNG CANCER. VIII. THERAPY. V. SMALL CELL LUNG CANCER Prof.
 Corso Integrato di Clinica Medica ONCOLOGIA MEDICA AA 2010-2011 LUNG CANCER. VIII. THERAPY. V. SMALL CELL LUNG CANCER Prof. Alberto Riccardi SMALL CELL LUNG CARCINOMA Summary of treatment approach * limited
Corso Integrato di Clinica Medica ONCOLOGIA MEDICA AA 2010-2011 LUNG CANCER. VIII. THERAPY. V. SMALL CELL LUNG CANCER Prof. Alberto Riccardi SMALL CELL LUNG CARCINOMA Summary of treatment approach * limited
Hematopoietic Stem-Cell Transplantation for Epithelial Ovarian Cancer
 Hematopoietic Stem-Cell Transplantation for Epithelial Ovarian Cancer Policy Number: Original Effective Date: MM.07.014 04/01/2008 Line(s) of Business: Current Effective Date: HMO; PPO 01/23/2015 Section:
Hematopoietic Stem-Cell Transplantation for Epithelial Ovarian Cancer Policy Number: Original Effective Date: MM.07.014 04/01/2008 Line(s) of Business: Current Effective Date: HMO; PPO 01/23/2015 Section:
Progress and Prospects in Ovarian Cancer Screening and Prevention
 Progress and Prospects in Ovarian Cancer Screening and Prevention Rebecca Stone, MD MS Assistant Professor Kelly Gynecologic Oncology Service The Johns Hopkins Hospital 1 No Disclosures 4/12/2016 2 Ovarian
Progress and Prospects in Ovarian Cancer Screening and Prevention Rebecca Stone, MD MS Assistant Professor Kelly Gynecologic Oncology Service The Johns Hopkins Hospital 1 No Disclosures 4/12/2016 2 Ovarian
Ovarian Cancer (Event Driven)
") Brochure More information from http://www.researchandmarkets.com/reports/2367241/ Ovarian Cancer (Event Driven) Description: Owing to the lack of screening programs across the markets under study, ovarian
Brochure More information from http://www.researchandmarkets.com/reports/2367241/ Ovarian Cancer (Event Driven) Description: Owing to the lack of screening programs across the markets under study, ovarian
Intraperitoneal chemotherapy for the initial management of primary epithelial ovarian cancer (Review)
") Intraperitoneal chemotherapy for the initial management of primary epithelial ovarian cancer (Review) Jaaback K, Johnson N, Lawrie TA This is a reprint of a Cochrane review, prepared and maintained by
Intraperitoneal chemotherapy for the initial management of primary epithelial ovarian cancer (Review) Jaaback K, Johnson N, Lawrie TA This is a reprint of a Cochrane review, prepared and maintained by
Ching-Yao Yang, Yu-Wen Tien
 Ching-Yao Yang, Yu-Wen Tien Division of General Surgery, Department of Surgery, National Taiwan University Hospital Oct-30-2010 Pancreatic NET have poorer prognosis when presence of liver metastases at
Ching-Yao Yang, Yu-Wen Tien Division of General Surgery, Department of Surgery, National Taiwan University Hospital Oct-30-2010 Pancreatic NET have poorer prognosis when presence of liver metastases at
SAKK Lung Cancer Group. Current activities and future projects
 SAKK Lung Cancer Group Current activities and future projects SAKK Lung Cancer Group Open group of physicians interested in lung cancer Mostly Medical Oncologists, but also Thoracic Surgeons Radiation
SAKK Lung Cancer Group Current activities and future projects SAKK Lung Cancer Group Open group of physicians interested in lung cancer Mostly Medical Oncologists, but also Thoracic Surgeons Radiation
Treatment Paradigm in NSCLC Treatment
 Treatment Paradigm in NSCLC Treatment Era of Targeted Therapy Aumkhae Sookprasert, MD Medicine Department, KKU Which factors taken to be account in NSCLC treatment? 1. Staging 2. ECOG performance status
Treatment Paradigm in NSCLC Treatment Era of Targeted Therapy Aumkhae Sookprasert, MD Medicine Department, KKU Which factors taken to be account in NSCLC treatment? 1. Staging 2. ECOG performance status
Should we use Docetaxel in hormone- naïve prostate cancer? Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France
 Should we use Docetaxel in hormone- naïve prostate cancer? Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation to advisory boards/honorarium from: Amgen, Astellas,
Should we use Docetaxel in hormone- naïve prostate cancer? Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation to advisory boards/honorarium from: Amgen, Astellas,
Progress in Treating Advanced Triple Negative Breast Cancer
 Progress in Treating Advanced Triple Negative Breast Cancer Lisa A. Carey, M.D. University of North Carolina at Chapel Hill Lineberger Comprehensive Cancer Center Triple Negative Breast Cancer by Subtype
Progress in Treating Advanced Triple Negative Breast Cancer Lisa A. Carey, M.D. University of North Carolina at Chapel Hill Lineberger Comprehensive Cancer Center Triple Negative Breast Cancer by Subtype
Treatment of Metastatic Non-Small Cell Lung Cancer: A Systematic Review of Comparative Effectiveness and Cost-Effectiveness
 Department of Veterans Affairs Health Services Research & Development Service Treatment of Metastatic Non-Small Cell Lung Cancer: A Systematic Review of Comparative Effectiveness and Cost-Effectiveness
Department of Veterans Affairs Health Services Research & Development Service Treatment of Metastatic Non-Small Cell Lung Cancer: A Systematic Review of Comparative Effectiveness and Cost-Effectiveness
Activity of pemetrexed in thoracic malignancies
 Activity of pemetrexed in thoracic malignancies Results of phase III clinical studies of pemetrexed in malignant pleural mesothelioma and non-small cell lung cancer show benefit P emetrexed (Alimta) is
Activity of pemetrexed in thoracic malignancies Results of phase III clinical studies of pemetrexed in malignant pleural mesothelioma and non-small cell lung cancer show benefit P emetrexed (Alimta) is
Scottish Medicines Consortium
 Scottish Medicines Consortium pemetrexed 500mg infusion (Alimta ) No. (192/05) Eli Lilly 8 July 2005 The Scottish Medicines Consortium has completed its assessment of the above product and advises NHS
Scottish Medicines Consortium pemetrexed 500mg infusion (Alimta ) No. (192/05) Eli Lilly 8 July 2005 The Scottish Medicines Consortium has completed its assessment of the above product and advises NHS
2010 Gynecologic Cancer InterGroup (GCIG) Consensus Statement on Clinical Trials in Ovarian Cancer
 Consensus Statement on Clinical Trials in Ovarian Cancer") REVIEW ARTICLE 2010 Gynecologic Cancer InterGroup (GCIG) Consensus Statement on Clinical Trials in Ovarian Cancer Report From the Fourth Ovarian Cancer Consensus Conference Gavin C.E. Stuart, MD, FRCSC,*
REVIEW ARTICLE 2010 Gynecologic Cancer InterGroup (GCIG) Consensus Statement on Clinical Trials in Ovarian Cancer Report From the Fourth Ovarian Cancer Consensus Conference Gavin C.E. Stuart, MD, FRCSC,*
Ovarian Cancer 101 Jessica McAlpine, MD
 Ovarian Cancer 101 Jessica McAlpine, MD Different types of ovarian cancer: Outline: Ovarian Cancer Presentation, behavior, site of origin Primary treatment: surgery, chemo, +/-radiation Role of genetics
Ovarian Cancer 101 Jessica McAlpine, MD Different types of ovarian cancer: Outline: Ovarian Cancer Presentation, behavior, site of origin Primary treatment: surgery, chemo, +/-radiation Role of genetics
MOH Policy for dispensing NEOPLASTIC DISEASES DRUGS
 MOH Policy for dispensing NEOPLASTIC DISEASES DRUGS All prescriptions for antineoplastic drugs must be accompanied by the MOH special form. All the attachments mentioned on this form shall be submitted
MOH Policy for dispensing NEOPLASTIC DISEASES DRUGS All prescriptions for antineoplastic drugs must be accompanied by the MOH special form. All the attachments mentioned on this form shall be submitted
Jennifer Diamond M.D. Assistant Professor Developmental Therapeutics and Breast Oncology University of Colorado Anschutz Medical Campus SUMO Fall
 Jennifer Diamond M.D. Assistant Professor Developmental Therapeutics and Breast Oncology University of Colorado Anschutz Medical Campus SUMO Fall Meeting September 26, 2015 To understand the biology and
Jennifer Diamond M.D. Assistant Professor Developmental Therapeutics and Breast Oncology University of Colorado Anschutz Medical Campus SUMO Fall Meeting September 26, 2015 To understand the biology and
Controversies in Management of. Inoperable NSCLC. Inoperable NSCLC. Introduction:
 Inoperable NSCLC Controversies in Management of Inoperable NSCLC Introduction: It is difficult to overemphasize the magnitude of lung cancer as Public Health Problem in our society. - In US, Lung cancer
Inoperable NSCLC Controversies in Management of Inoperable NSCLC Introduction: It is difficult to overemphasize the magnitude of lung cancer as Public Health Problem in our society. - In US, Lung cancer
Summary ID# 13095. Clinical Study Summary: Study H3E-EW-B012
 Page 1 Summary ID# 13095 Clinical Study Summary: Study H3E-EW-B012 First-line Treatment of Non-Small Cell Lung Cancer under Routine Conditions: Observational Study on Overall Survival Date summary electronically
Page 1 Summary ID# 13095 Clinical Study Summary: Study H3E-EW-B012 First-line Treatment of Non-Small Cell Lung Cancer under Routine Conditions: Observational Study on Overall Survival Date summary electronically
How To Compare The Effects Of A Hysterectomy And A Hysterectomy
 A RANDOMIZED TRIAL COMPARING RADICAL HYSTERECTOMY AND PELVIC NODE DISSECTION VS SIMPLE HYSTERECTOMY AND PELVIC NODE DISSECTION IN PATIENTS WITH LOW RISK EARLY STAGE CERVICAL CANCER A Gynecologic Cancer
A RANDOMIZED TRIAL COMPARING RADICAL HYSTERECTOMY AND PELVIC NODE DISSECTION VS SIMPLE HYSTERECTOMY AND PELVIC NODE DISSECTION IN PATIENTS WITH LOW RISK EARLY STAGE CERVICAL CANCER A Gynecologic Cancer
Avastin in Metastatic Breast Cancer
 Non-interventional study Avastin in Metastatic Breast Cancer ML 21165 / 2007 Clinical Study Report Synopsis ROCHE ML21165 / WiSP Project RH09 / V. 1.0 / 24.06.2013 ROCHE ML21165-2 - Name of Sponsor Roche
Non-interventional study Avastin in Metastatic Breast Cancer ML 21165 / 2007 Clinical Study Report Synopsis ROCHE ML21165 / WiSP Project RH09 / V. 1.0 / 24.06.2013 ROCHE ML21165-2 - Name of Sponsor Roche