Rehabilitation s Role in Decreasing Returns to Acute Care
|
|
|
- George Woods
- 8 years ago
- Views:
Transcription
1 Rehabilitation s Role in Decreasing Returns to Acute Care Glenda Mack, PT, MSPT, MBA, CLT, CWS Division Vice President Clinical Operations, RehabCare

2 Objectives Participants will verbalize three primary reasons for skilled nursing facility patient s return to acute care hospitals. Participants will demonstrate understanding of the role of each therapy discipline in the treatment of patients with cardiac, pulmonary and other medical diagnoses. Participants will communicate a minimum of two strategies for engaging their rehabilitation staff in the care of their medically complex patient population. Participants will demonstrate knowledge of key Medicare guidelines for rehabilitation services for the care of patients with medically complex conditions. 2

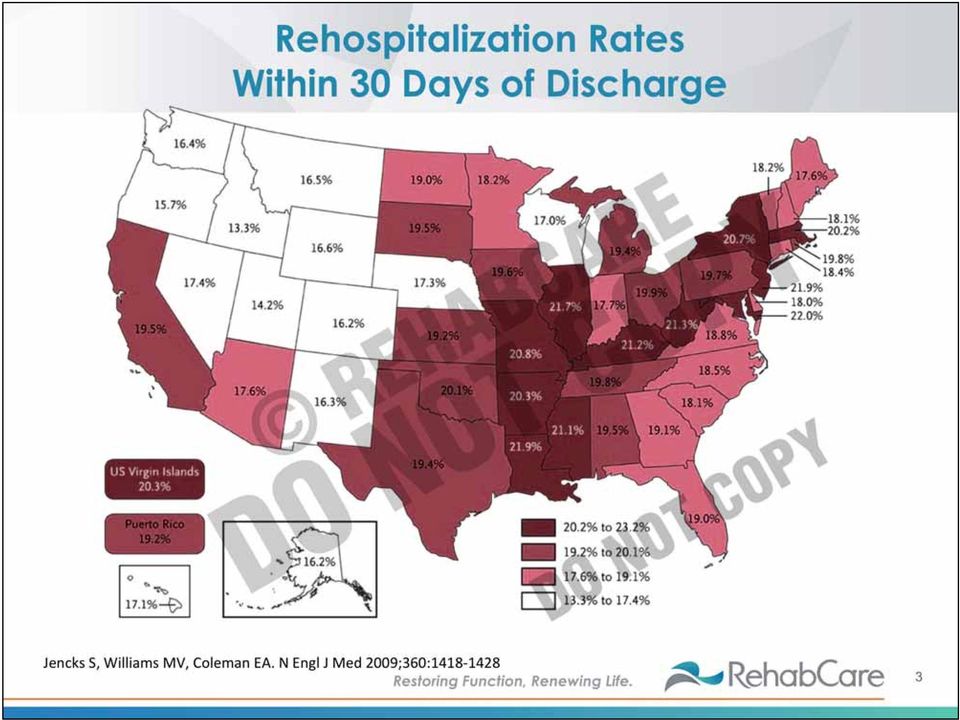
3 Rehospitalization Rates Within 30 Days of Discharge 3
4 Tremendous Opportunities Exist to Better Manage Patient Care After Discharge From Acute Care Hospitals 4

5 News by the Numbers 39.5 million hospital discharges per year = $329.2 billion 20% of all hospitalizations are rehospitalizations within 30 days 23% of patients older than 65 are discharged from the hospital to another institution 20% of Medicare patients readmitted within 30 days only half had a visit to a physician in the 30 days after discharge 5

6 Readmission Penalty CMS s Top Conditions Will Expand to Four in FY 2015 Pneumonia Heart attack Heart failure These three conditions made up 10% of hospital discharges in COPD (FY 2015) Elective lower extremity total joint replacement (Proposed rule for CY 2015) Coronary artery bypass graft Percutaneous transluminal coronary angioplasty Renal failure Urinary tract infection Sepsis Cerebral vascular accidents 6

7 Readmission STACHs D/C 40% AMI, HF, Pneumonia Patients to Post-Acute Care Advantage Care Positioning System 2009 Medicare, 100% Standard Analytic File claims data from CMS. Other = different acute hospital from original incident of care episode 7

8 SNFs Are Part of the Answer Treatment and stabilization of acute problem Medication management Management of secondary diagnosis or co-morbidity SNF and hospital need to be together on: Rehab Patient education Eventual patient D/C to home 8

9 PPACA Report Medicare Payment Advisory Commission (MedPAC) % of hospital admissions resulted in readmissions within 30 days of discharge 11.3% within 15 days 6.2% within 7 days Stephen F. Jencks, New England Journal of Medicine % of Medicare beneficiaries were readmitted to the hospital within 30 days 34.0% within 90 days 56.1% within one year of discharge MedPAC - readmissions within 30 days accounted for $15 billion of Medicare spending. 9

10 Quality Concerns with Readmissions Unplanned readmissions are stressful to patients and their families Unplanned readmissions are costly and resource intensive Potential adverse effects of rehospitalizations can include: Delirium Deconditioning Development of pressure ulcers Hospital acquired infections Unintentional weight loss/poor nutrition Use of restraints Urinary catheters 10

11 Rules of Successful Facility Living Differ from Outside World Fears and Anxieties Emerge: Nursing centers and hospitals viewed as prelude to death Failing health Institutionalization Increased dependence Financial uncertainty Separation from loved ones Feelings of rejection Loss of decision making 11

12 Facilities Key Areas to Assess Does Your Facility... Receive complete and accurate admission information from all disciplines from referral sources/sites? Have a process for referral to interdisciplinary team members? Communicate assessment results within interdisciplinary team with identification problem list or red flags? Utilize a patient discharge checklist outlining expectations and goals for safe discharge? Implement assessments to identify signs/symptoms, complications and possible resolutions prior to readmission to the hospital? Utilize a process to refer to hospital if a rehospitalization is required? 12

13 RAND Meta-Analysis of Studies Interventions That Led to a (Significant) Reduction in Readmissions Within One Month of Discharge Included: In-hospital daily visits by care coordinators and pharmacists, combined with post-discharge phone calls (proportion readmitted: 10 percent vs. 38 percent in usual care; p<0.05) (USA)61 Comprehensive geriatric assessment and multidisciplinary intervention (DEED II Study) (proportion readmitted: 61 percent vs. 82 percent in usual care; p<0.05) (Australia)62 Care transitions intervention with in-hospital visits, home visits and telephone follow-up by a transition coach (proportion readmitted: 8.3 percent vs percent in usual care; p<0.05) (USA)63 13
 (Australia)62 Care transitions intervention with in-hospital visits, home visits and telephone follow-up by a transition coach (proportion readmitted: 8.3 percent vs. 11.")
14 Why Are Patients Readmitted to the Hospital? Faulty care transitions Medication mismanagement Not taking prescribed dosage Polypharmacy Cost issues Communication between facility caregivers and physicians Exacerbation of primary disease Cognitive/physical dysfunction 14

15 TARGET Assessment Tool The 9Ps The BOOST Program Tool for Addressing Risk: a Geriatric Evaluation for Transitions Prior hospitalization Problem medications Psychological Principal diagnosis Polypharmacy Poor health literacy Patient support Palliative care Physical function 15

16 What Does the Research Say About Therapy? One unexpected finding was that a high level of usual physical activity was associated with a 46% reduction in the risk of admission. Identification of risk factors that were potentially amenable to modification showed that lack of rehabilitation and poor inhaler technique were the most frequent associations. 16

17 Key Elements of Rehab Roles Be familiar with sign/symptoms of disease process (decline) Proactive communication with nursing staff at all times Identifying appropriate admission Alerting nursing staff to issues Communicating with interdisciplinary team (IDT) members related to concerns ongoing D/C planning Ongoing patient education to prepare for D/C 17
 members related to concerns ongoing D/C planning Ongoing patient education to")
18 Coverage for Therapy Services in SNF Not diagnosis specific The determining issue is whether the skilled services of a health care professional are needed, not whether the beneficiary will improve. These services are provided by or under the supervision of skilled personnel and are covered by Medicare if the services are needed to maintain the individual s condition or prevent or slow his/her decline 18

19 Fundamentals of Therapy Intervention Standardized testing tools Ensure best practice /evidence-based care for each individual patient Individualized care/treatment Use of objective tests and measures baseline and outcome measures Ensure patient engagement 19

20 Therapy Partnership with Facility Team to Develop Diagnosis-Specific Protocols Medication management (cognitive assessment) Energy conservation/work simplification Specific protocols/standards of care Utilization of discharge checklists (ensure safety and knowledge transfer) Ensure patient engagement Structured and complete hand-off of care to other providers Include thorough and complete patient/family education throughout the episode of care and ensure understanding at and before D/C 20

21 Setting Expectations for Your Therapists At Evaluation Ensure knowledge of facility/site s initiatives and process Assess patient s readiness for change Assess patient s current knowledge and education needs (a patient education resource) Condition/disease Medication management Benefits of exercise/therapy and risks of non-compliance Safety Use objective tests and measures Establish patient s baseline and safe range for vitals and lab values Assess family involvement, knowledge, and support of patient 21
22 Setting Expectations for Your Therapists Developing the Plan of Care Frequency, intensity, duration matches patient medical status Includes formal patient education plan with handouts Condition/disease Medication management Benefits of exercise/therapy, risks of non-compliance Safety and when to contact the provider Measures to encourage patient/family engagement Designed to ensure thorough and continuous patient and family engagement and education Uses established protocols/evidence-based practice 22
23 Setting Expectations for Your Therapists Throughout Episode of Care and Before Discharge: Monitor vital signs before, during and after treatment Be alert for S&S of possible worsening or exacerbation of condition Try multiple interventions Ensure patient engagement Consider a home evaluation Ensure patient/family competence with education provided Assess executive functioning of the patient/family 23
24 At Discharge Prepare Formal Hand-Off Education/exercise handouts When to contact provider Date of your follow-up with patient/receiving facility Formal communication strategy with physician and next level caregivers on concerns and risks 24
25 Physical Therapy Scope of Practice Gait, locomotion, balance Mobility and transfers Pain management Aerobic capacity/ endurance Ventilation pulmonary Wound care including debridement Wheelchair seating and mobility Central nervous system assessment Environmental modification Orthotic, prosthetic and supportive devices Work integration/ reintegration Postural stability Electromodalities Assistive and adaptive equipment 25
26 Occupational Therapy Scope of Practice Cognitive assessment and treatment Self-care/activities of daily living and home management Motor and neurological assessment Work integration/ reintegration Functional mobility Assistive/adaptive equipment Environmental modification Postural assessment Wheelchair seating and mobility Sensory integration Therapeutic exercise Orthotic/prosthetic devices Electromodalities Oral dysphagia 26
27 Speech-Language Pathology Scope of Practice Comprehension Auditory and reading Communication Expressive and receptive skills (Aphasia), voice quality, fluency Cognition Dysphagia Pulmonary, oral, pharyngeal and esophageal phase, postural control Oral Motor assessment and treatment 27
28 Steps for Success Take inventory of rehab department materials and equipment to ensure appropriate tools and assessments are available. Vital signs: O2 saturation, blood pressure, heart rate, respiratory rate 6-minute walk test BORG rating of perceived exertion Edema measurement Manual muscle test Respiratory: posture, breathing pattern, cervical auscultation Activities of daily living assessment Cognition brief cognitive assessment tool Medication management forms and tools Energy conservation tools 28
29 Ensure the Relationships Are Strong Early Identification Therapists spend minutes with each patient Therapists may be the first to notice changes in the patient s physical or cognitive function Open dialog must be encouraged and rewarded: Small changes are addressed when observed Standard 24-hour communication process Clear feedback loops No-blame culture 29
30 Identify Strategic Opportunities Establish Who Partner for Key Clinical Focus Areas (Nursing and Therapy): Pulmonary Cardiac Wound care Medically complex 30
31 Identify Strategic Opportunities Partner With Key Physicians: Develop standardized protocols Promote standard feedback loops for physicians Identify key physician relationships to enhance patient outcomes 31
32 Therapists Value to Your Program Your Therapy Team Has Received Education On: Pharmacology Gross anatomy Pathophysiology of disease Functional implications of disease processes Central nervous system assessment and intervention Functional capacity and task segmentation Assessment of cognitive function Most therapists are able to synthesize information from multiple sources and develop an appropriate plan for the patient, and assist with risk assessment and mitigation. 32
33 Strengthen Your Strategy Integrating your therapy team into the rehospitalization strategy could be the missing link in many facilities. 33
34 Current vs. Future and the Roadblocks FFS Managed Managed FFS ACOs, bundle holders 34
35 Audience Questions and Participation We d like to open the floor to any questions you may have. Thank you for your time! 35
How Will Hospital Readmission Penalties Impact Skilled Nursing Facilities?
 How Will Hospital Readmission Penalties Impact Skilled Nursing Facilities? Patrick V. Trotta, CPA Director of ElderCare Provider Services Glass Jacobson patrick.trotta@glassjacobson.com 410 356 1000 Presentation
How Will Hospital Readmission Penalties Impact Skilled Nursing Facilities? Patrick V. Trotta, CPA Director of ElderCare Provider Services Glass Jacobson patrick.trotta@glassjacobson.com 410 356 1000 Presentation
Readmissions as an Enterprise Priority. Presenters 4/17/2014
 Readmissions as an Enterprise Priority April 24, 2014 Presenters Vincent A. Maniscalco, MPA, LNHA Administrator Middletown Park Rehabilitation and Health Care Center Vmaniscalco@parkmanorrehab.com Eileen
Readmissions as an Enterprise Priority April 24, 2014 Presenters Vincent A. Maniscalco, MPA, LNHA Administrator Middletown Park Rehabilitation and Health Care Center Vmaniscalco@parkmanorrehab.com Eileen
Preventing Readmissions
 Emerging Topics in Healthcare Reform Preventing Readmissions Janssen Pharmaceuticals, Inc. Preventing Readmissions The Patient Protection and Affordable Care Act (ACA) contains several provisions intended
Emerging Topics in Healthcare Reform Preventing Readmissions Janssen Pharmaceuticals, Inc. Preventing Readmissions The Patient Protection and Affordable Care Act (ACA) contains several provisions intended
Joan Carroll RN, CDMS, CCM Director of Care Transitions Lee Memorial Health System
 Joan Carroll RN, CDMS, CCM Director of Care Transitions Lee Memorial Health System 1 Explain how patients experience transitions of care Identify variables that affect transitions due to lack of patient
Joan Carroll RN, CDMS, CCM Director of Care Transitions Lee Memorial Health System 1 Explain how patients experience transitions of care Identify variables that affect transitions due to lack of patient
Outcomes Report through June 30, 2014
 Outcomes Report through June 0, 0 Contents Introduction... Haag Pavilion (Sub-Acute Unit)... Rehabilitation Outcomes... Rehospitalization Outcomes of Sub-Acute Patients... Center for Heart Health Outcomes...
Outcomes Report through June 0, 0 Contents Introduction... Haag Pavilion (Sub-Acute Unit)... Rehabilitation Outcomes... Rehospitalization Outcomes of Sub-Acute Patients... Center for Heart Health Outcomes...
Innovations@Home. Home Health Initiatives Reduce Avoidable Readmissions by Leveraging Innovation
 How Does CMS Measure the Rate of Acute Care Hospitalization (ACH)? Until January 2013, CMS measured Acute Care Hospitalization (ACH) through the Outcomes Assessment and Information Set (OASIS) reporting
How Does CMS Measure the Rate of Acute Care Hospitalization (ACH)? Until January 2013, CMS measured Acute Care Hospitalization (ACH) through the Outcomes Assessment and Information Set (OASIS) reporting
Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION
 Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION At the end of this session, you will be able to: Identify ways RT skills can be utilized for
Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION At the end of this session, you will be able to: Identify ways RT skills can be utilized for
Crucial Complications: Preventing Harm and Promoting Health
 Crucial Complications: Preventing Harm and Promoting Health MARCI RUEDIGER, PT, MS Agenda What puts patients at risk after acute care? How are these risks managed in rehab? How has the ACA changed the
Crucial Complications: Preventing Harm and Promoting Health MARCI RUEDIGER, PT, MS Agenda What puts patients at risk after acute care? How are these risks managed in rehab? How has the ACA changed the
How To Reduce Hospital Readmission
 Reducing Hospital Readmissions & The Affordable Care Act The Game Has Changed Drastically Reducing MSPB Measures Chuck Bongiovanni, MSW, MBA, NCRP, CSA, CFE Chuck Bongiovanni, MSW, MBA, NCRP, CSA, CFE
Reducing Hospital Readmissions & The Affordable Care Act The Game Has Changed Drastically Reducing MSPB Measures Chuck Bongiovanni, MSW, MBA, NCRP, CSA, CFE Chuck Bongiovanni, MSW, MBA, NCRP, CSA, CFE
Attachment A Minnesota DHS Community Service/Community Services Development
 Attachment A Minnesota DHS Community Service/Community Services Development Applicant Organization: First Plan of Minnesota Project Title: Implementing a Functional Daily Living Skills Assessment to Predict
Attachment A Minnesota DHS Community Service/Community Services Development Applicant Organization: First Plan of Minnesota Project Title: Implementing a Functional Daily Living Skills Assessment to Predict
Care Transitions: How Can You Help?
 Better Health: It s Your Health, Take Charge Transitions of Care: Coordination and Management Care Transitions: How Can You Help? presented by: Anne Elwell, RN, MPH Principal and Vice President, Qualidigm
Better Health: It s Your Health, Take Charge Transitions of Care: Coordination and Management Care Transitions: How Can You Help? presented by: Anne Elwell, RN, MPH Principal and Vice President, Qualidigm
SAM KARAS ACUTE REHABILITATION CENTER
 SAM KARAS ACUTE REHABILITATION CENTER 1 MEDICAL CARE Sam Karas Acute Rehabilitation The Sam Karas Acute Rehabilitation Center is a comprehensive and interdisciplinary inpatient unit. Medical care is directed
SAM KARAS ACUTE REHABILITATION CENTER 1 MEDICAL CARE Sam Karas Acute Rehabilitation The Sam Karas Acute Rehabilitation Center is a comprehensive and interdisciplinary inpatient unit. Medical care is directed
FINANCIAL IMPLICATIONS OF EXCESS HOSPITAL READMISSIONS JOSESPH B. HENDERSON, J.D.
 FINANCIAL IMPLICATIONS OF EXCESS HOSPITAL READMISSIONS JOSESPH B. HENDERSON, J.D. Executive MHA Candidate, 2013 University of Southern California Sol Price School of Public Policy Abstract A 2007 Medicare
FINANCIAL IMPLICATIONS OF EXCESS HOSPITAL READMISSIONS JOSESPH B. HENDERSON, J.D. Executive MHA Candidate, 2013 University of Southern California Sol Price School of Public Policy Abstract A 2007 Medicare
Stroke Rehab Across the Continuum of Care in Quinte Region
 Stroke Rehab Across the Continuum of Care in Quinte Region Adrienne Bell Smith Manager of Rehab Therapies QHC Karen Brown Manger Client Services, Hospital Access South East CCAC Disclosure of Potential
Stroke Rehab Across the Continuum of Care in Quinte Region Adrienne Bell Smith Manager of Rehab Therapies QHC Karen Brown Manger Client Services, Hospital Access South East CCAC Disclosure of Potential
Health Care Leader Action Guide to Reduce Avoidable Readmissions
 Health Care Leader Action Guide to Reduce Avoidable Readmissions January 2010 TRANSFORMING HEALTH CARE THROUGH RESEARCH AND EDUCATION Osei-Anto A, Joshi M, Audet AM, Berman A, Jencks S. Health Care Leader
Health Care Leader Action Guide to Reduce Avoidable Readmissions January 2010 TRANSFORMING HEALTH CARE THROUGH RESEARCH AND EDUCATION Osei-Anto A, Joshi M, Audet AM, Berman A, Jencks S. Health Care Leader
A Project to Reengineer Discharges Reduces 30-Day Hospital Readmission Rates. April 11, 2014
 A Project to Reengineer Discharges Reduces 30-Day Hospital Readmission Rates April 11, 2014 About the QIO Program Leading rapid, large-scale change in health quality: Goals are bolder. The patient is at
A Project to Reengineer Discharges Reduces 30-Day Hospital Readmission Rates April 11, 2014 About the QIO Program Leading rapid, large-scale change in health quality: Goals are bolder. The patient is at
GENERAL ADMISSION CRITERIA INPATIENT REHABILITATION PROGRAMS
 Originator: Case Management Original Date: 9/94 Review/Revision: 6/96, 2/98, 1/01, 4/02, 8/04, 3/06, 03/10, 3/11, 3/13 Stakeholders: Case Management, Medical Staff, Nursing, Inpatient Therapy GENERAL ADMISSION
Originator: Case Management Original Date: 9/94 Review/Revision: 6/96, 2/98, 1/01, 4/02, 8/04, 3/06, 03/10, 3/11, 3/13 Stakeholders: Case Management, Medical Staff, Nursing, Inpatient Therapy GENERAL ADMISSION
Medicare Savings and Reductions in Rehospitalizations Associated with Home Health Use
 Medicare Savings and Reductions in Rehospitalizations Associated with Home Health Use June 23, 2011 Avalere Health LLC Avalere Health LLC The intersection of business strategy and public policy Table of
Medicare Savings and Reductions in Rehospitalizations Associated with Home Health Use June 23, 2011 Avalere Health LLC Avalere Health LLC The intersection of business strategy and public policy Table of
Doctor of Physical Therapy Degree Curriculum:
 Doctor of Physical Therapy Degree Curriculum: SUMMER SEMESTER 1 st YEAR (BOTH SESSIONS) DPT 744 Gross Human Anatomy I 2 credits DPT 744L Gross Human Anatomy I Lab 1 credit DPT 745 Gross Human Anatomy II
Doctor of Physical Therapy Degree Curriculum: SUMMER SEMESTER 1 st YEAR (BOTH SESSIONS) DPT 744 Gross Human Anatomy I 2 credits DPT 744L Gross Human Anatomy I Lab 1 credit DPT 745 Gross Human Anatomy II
Risk Tools in Predicting Rehospitalization from Home Care. VNAA Best Practice for Home Health
 Risk Tools in Predicting Rehospitalization from Home Care VNAA Best Practice for Home Health Learning objectives The participant will be able to: Discuss the need for risk assessment for home health patients
Risk Tools in Predicting Rehospitalization from Home Care VNAA Best Practice for Home Health Learning objectives The participant will be able to: Discuss the need for risk assessment for home health patients
RT AS PROJECT MANAGER:
 RT AS PROJECT MANAGER: IMPROVING CARE TRANSITIONS DECREASES UNPLANNED READMISSIONS TAMMY JARNAGIN, BHS, RRT DIRECTOR CARDIOPULMONARY SERVICES, NEURODIAGNOSTICS, HOME MEDICAL EQUIPMENT Objectives Recognize
RT AS PROJECT MANAGER: IMPROVING CARE TRANSITIONS DECREASES UNPLANNED READMISSIONS TAMMY JARNAGIN, BHS, RRT DIRECTOR CARDIOPULMONARY SERVICES, NEURODIAGNOSTICS, HOME MEDICAL EQUIPMENT Objectives Recognize
PL 111-148 and Amendments: Impact on Post-Acute Care for Health Care Systems
 PL 111-148 and Amendments: Impact on Post-Acute Care for Health Care Systems By Kathleen M. Griffin, PhD. There are three key provisions of the law that will have direct impact on post-acute care needs
PL 111-148 and Amendments: Impact on Post-Acute Care for Health Care Systems By Kathleen M. Griffin, PhD. There are three key provisions of the law that will have direct impact on post-acute care needs
Reducing Readmissions with Predictive Analytics
 Reducing Readmissions with Predictive Analytics Conway Regional Health System uses analytics and the LACE Index from Medisolv s RAPID business intelligence software to identify patients poised for early
Reducing Readmissions with Predictive Analytics Conway Regional Health System uses analytics and the LACE Index from Medisolv s RAPID business intelligence software to identify patients poised for early
RE: CMS-3819-P; Medicare and Medicaid Programs; Conditions of Participation for Home Health Agencies
 January 6, 2015 Marilyn Tavenner Administrator Centers for Medicare & Medicaid Services Department of Health and Human Services Room 445 G Attention: CMS-3819-P Hubert H. Humphrey Building, 200 Independence
January 6, 2015 Marilyn Tavenner Administrator Centers for Medicare & Medicaid Services Department of Health and Human Services Room 445 G Attention: CMS-3819-P Hubert H. Humphrey Building, 200 Independence
Waterloo Wellington Rehabilitative Care System Integrated Care Pathway for COPD Stream of Care (short version)
") Waterloo Wellington Rehabilitative Care System Integrated Care Pathway for COPD Stream of Care (short version) Care Setting ACUTE Activity Confirmation of COPD diagnoses: If time and the patient s condition
Waterloo Wellington Rehabilitative Care System Integrated Care Pathway for COPD Stream of Care (short version) Care Setting ACUTE Activity Confirmation of COPD diagnoses: If time and the patient s condition
To provide standardized Supervised Exercise Programs across the province.
 TITLE ALBERTA HEALTHY LIVING PROGRAM SUPERVISED EXERCISE PROGRAM DOCUMENT # HCS-67-01 APPROVAL LEVEL Executive Director Primary Health Care SPONSOR Senior Consultant Central Zone, Primary Health Care CATEGORY
TITLE ALBERTA HEALTHY LIVING PROGRAM SUPERVISED EXERCISE PROGRAM DOCUMENT # HCS-67-01 APPROVAL LEVEL Executive Director Primary Health Care SPONSOR Senior Consultant Central Zone, Primary Health Care CATEGORY
1. Executive Summary Problem/Opportunity: Evidence: Baseline Data: Intervention: Results:
 A Clinical Nurse Leader led multidisciplinary Heart Failure Program: Integrating best practice across the care continuum to reduce avoidable 30 day readmissions. 1. Executive Summary Problem/Opportunity:
A Clinical Nurse Leader led multidisciplinary Heart Failure Program: Integrating best practice across the care continuum to reduce avoidable 30 day readmissions. 1. Executive Summary Problem/Opportunity:
Physician Guide to Home Health Care Certification for Medicare Enrollees Steve Landers MD, MPH (landers@ccf.org) Director, Cleveland Clinic at Home
 Director, Cleveland Clinic at Home") Physician Guide to Home Health Care Certification for Medicare Enrollees Steve Landers MD, MPH (landers@ccf.org) Director, Cleveland Clinic at Home January 2011 Background Helping patients succeed at home
Physician Guide to Home Health Care Certification for Medicare Enrollees Steve Landers MD, MPH (landers@ccf.org) Director, Cleveland Clinic at Home January 2011 Background Helping patients succeed at home
University of Maine at Presque Isle 181 Main Street Presque Isle, ME 04769 COURSE SYLLABUS CLINICAL EDUCATION EXPERIENCE III
 University of Maine at Presque Isle 181 Main Street Presque Isle, ME 04769 COURSE SYLLABUS CLINICAL EDUCATION EXPERIENCE III CURRICULUM AND COURSE NUMBER: PTA 225 DEPARTMENT: Professional programs/pta
University of Maine at Presque Isle 181 Main Street Presque Isle, ME 04769 COURSE SYLLABUS CLINICAL EDUCATION EXPERIENCE III CURRICULUM AND COURSE NUMBER: PTA 225 DEPARTMENT: Professional programs/pta
Avoiding Rehospitalizations in LTC Chris Osterberg, RN BSN Pathway Health Services
 Avoiding Rehospitalizations in LTC Chris Osterberg, RN BSN Pathway Health Services Objectives Understand the new consequences to hospitals for discharged clients being re-admitted within selected time
Avoiding Rehospitalizations in LTC Chris Osterberg, RN BSN Pathway Health Services Objectives Understand the new consequences to hospitals for discharged clients being re-admitted within selected time
Henry Ford Health System Care Coordination and Readmissions Update
 Henry Ford Health System Care Coordination and Readmissions Update September 2013 BACKGROUND Most hospital readmissions are viewed as avoidable, costly, and in some cases as a potential marker of poor
Henry Ford Health System Care Coordination and Readmissions Update September 2013 BACKGROUND Most hospital readmissions are viewed as avoidable, costly, and in some cases as a potential marker of poor
How To Help A Nursing Home And Hospital Collaborate
 Continuum of Care Bridging the Gap between the Hospital and Nursing Home Scott Wells, RN MSN Tiffany Noller, RN MSN Objectives Name key members involved in hospital/nursing home collaborative Identify
Continuum of Care Bridging the Gap between the Hospital and Nursing Home Scott Wells, RN MSN Tiffany Noller, RN MSN Objectives Name key members involved in hospital/nursing home collaborative Identify
CENTER OF EXCELLENCE IN REHABILITATION SERVICES. Policies Standards Survey Process
 CENTER OF EXCELLENCE IN REHABILITATION SERVICES Policies Standards Survey Process INTRODUCTION The CIHQ Center of Excellence in Rehabilitation Services program recognizes specialized inpatient rehabilitation
CENTER OF EXCELLENCE IN REHABILITATION SERVICES Policies Standards Survey Process INTRODUCTION The CIHQ Center of Excellence in Rehabilitation Services program recognizes specialized inpatient rehabilitation
NAVIGATING THE MEDICARE MAZE OF REHABILITATIVE SERVICES
 NAVIGATING THE MEDICARE MAZE OF REHABILITATIVE SERVICES NAVIGATING THE COMPLEXITY OF INSURANCE COVERAGE. Fox Rehabilitation is a private practice of physical, occupational, and speech therapists who specialize
NAVIGATING THE MEDICARE MAZE OF REHABILITATIVE SERVICES NAVIGATING THE COMPLEXITY OF INSURANCE COVERAGE. Fox Rehabilitation is a private practice of physical, occupational, and speech therapists who specialize
ISSUED BY: TITLE: ISSUED BY: TITLE: President
 CLINICAL PRACTICE GUIDELINE PROFESSIONAL PRACTICE TITLE: Stroke Care Rehabilitation Unit DATE OF ISSUE: 2005, 05 PAGE 1 OF 7 NUMBER: CPG 20-3 SUPERCEDES: New ISSUED BY: TITLE: Chief of Medical Staff ISSUED
CLINICAL PRACTICE GUIDELINE PROFESSIONAL PRACTICE TITLE: Stroke Care Rehabilitation Unit DATE OF ISSUE: 2005, 05 PAGE 1 OF 7 NUMBER: CPG 20-3 SUPERCEDES: New ISSUED BY: TITLE: Chief of Medical Staff ISSUED
How To Cover Occupational Therapy
 Guidelines for Medical Necessity Determination for Occupational Therapy These Guidelines for Medical Necessity Determination (Guidelines) identify the clinical information MassHealth needs to determine
Guidelines for Medical Necessity Determination for Occupational Therapy These Guidelines for Medical Necessity Determination (Guidelines) identify the clinical information MassHealth needs to determine
Plenary Session 1. Health Dimensions Group. 2010 Health Dimensions Group
 Plenary Session 1 Kathleen M. Griffin, PhD Health Dimensions Group March 31, 2011 Hospital, Post Acute and Long-Term Care Collaboration in Health Care Reform: Critical Success Factors National Summit:
Plenary Session 1 Kathleen M. Griffin, PhD Health Dimensions Group March 31, 2011 Hospital, Post Acute and Long-Term Care Collaboration in Health Care Reform: Critical Success Factors National Summit:
PURPOSE OF THE SELF-ASSESSMENT TOOLS:
 Geriatric Rehab Definitions Framework Self-Assessment Tool Outpatient/Ambulatory Geriatric Rehab INTRODUCTION: In response to a changing rehab landscape in which rehabilitation is offered in many different
Geriatric Rehab Definitions Framework Self-Assessment Tool Outpatient/Ambulatory Geriatric Rehab INTRODUCTION: In response to a changing rehab landscape in which rehabilitation is offered in many different
The Cost-Effectiveness of Homecare
 The Cost-Effectiveness of Homecare Homecare Reduces Costs by 37 Percent for Heart Failure Patients The May 2004 Journal of the American Geriatrics Society reports a study conducted at six Philadelphia
The Cost-Effectiveness of Homecare Homecare Reduces Costs by 37 Percent for Heart Failure Patients The May 2004 Journal of the American Geriatrics Society reports a study conducted at six Philadelphia
Post discharge tariffs in the English NHS
 Post discharge tariffs in the English NHS Martin Campbell Department of Health 4th June 2013 Contents Rationale and objectives Non payment for avoidable readmissions Development of post discharge tariffs
Post discharge tariffs in the English NHS Martin Campbell Department of Health 4th June 2013 Contents Rationale and objectives Non payment for avoidable readmissions Development of post discharge tariffs
Comprehensive Cardiac Care Program
 PrograM Comprehensive Cardiac Care Program Empowering you to strengthen your heart. Trust In Our Care. Trust in Our Care The Comprehensive Cardiac Care Program is physician directed and focused on assisting
PrograM Comprehensive Cardiac Care Program Empowering you to strengthen your heart. Trust In Our Care. Trust in Our Care The Comprehensive Cardiac Care Program is physician directed and focused on assisting
Understanding Care Transitions as a Patient Safety Issue
 Article reprinted from Patient Safety & Quality Healthcare, May/June 2011 Understanding Care Transitions as a Patient Safety Issue By Sara Butterfield RN, BSN, CPHQ, CCM; Christine Stegel, RN, MS, CPHQ;
Article reprinted from Patient Safety & Quality Healthcare, May/June 2011 Understanding Care Transitions as a Patient Safety Issue By Sara Butterfield RN, BSN, CPHQ, CCM; Christine Stegel, RN, MS, CPHQ;
Division of Physical Therapy Education
 Division of Physical Therapy Education University of Nebraska Medical Center School of Allied Health Professions Essential Functions The functions are presented in two sections: 1) Physical Therapy knowledge,
Division of Physical Therapy Education University of Nebraska Medical Center School of Allied Health Professions Essential Functions The functions are presented in two sections: 1) Physical Therapy knowledge,
30 DAY COPD READMISSIONS AND PULMONARY REHAB
 30 DAY COPD READMISSIONS AND PULMONARY REHAB Trina M. Limberg, Bs, RRT, FAARC, MAACVPR Director, Preventative Pulmonary and Rehabilitation Services UC San Diego Health System OVERVIEW The Impact of COPD
30 DAY COPD READMISSIONS AND PULMONARY REHAB Trina M. Limberg, Bs, RRT, FAARC, MAACVPR Director, Preventative Pulmonary and Rehabilitation Services UC San Diego Health System OVERVIEW The Impact of COPD
High Desert Medical Group Connections for Life Program Description
 High Desert Medical Group Connections for Life Program Description POLICY: High Desert Medical Group ("HDMG") promotes patient health and wellbeing by actively coordinating services for members with multiple
High Desert Medical Group Connections for Life Program Description POLICY: High Desert Medical Group ("HDMG") promotes patient health and wellbeing by actively coordinating services for members with multiple
5/10/13 HEALTH CARE REFORM LONGITUDINAL CARE COORDINATION HEALTH CARE REFORM WHY = VALUE WHY WHAT HOW WHEN WHO WHY WHAT HOW WHEN WHO
 TRANSITION CARE TRANSITION CARE WHY WHAT HOW WHEN WHO HEALTH CARE REFORM HEALTH CARE REFORM WHY = VALUE WHY WHAT HOW WHEN WHO Cost/Quality equation Higher cost care has not/does not equate with higher
TRANSITION CARE TRANSITION CARE WHY WHAT HOW WHEN WHO HEALTH CARE REFORM HEALTH CARE REFORM WHY = VALUE WHY WHAT HOW WHEN WHO Cost/Quality equation Higher cost care has not/does not equate with higher
Medicare Part A. Pulmonary Rehab Program Services Web-Based Training February 25, 2010 - Q & As
 Pulmonary Rehab Program Services Web-Based Training February 25, 2010 - Q & As The following are the question and answers from the Pulmonary Rehabilitation Program Services web-based training which was
Pulmonary Rehab Program Services Web-Based Training February 25, 2010 - Q & As The following are the question and answers from the Pulmonary Rehabilitation Program Services web-based training which was
Value-Based Purchasing
 Emerging Topics in Healthcare Reform Value-Based Purchasing Janssen Pharmaceuticals, Inc. Value-Based Purchasing The Patient Protection and Affordable Care Act (ACA) established the Hospital Value-Based
Emerging Topics in Healthcare Reform Value-Based Purchasing Janssen Pharmaceuticals, Inc. Value-Based Purchasing The Patient Protection and Affordable Care Act (ACA) established the Hospital Value-Based
Transmittal 55 Date: MAY 5, 2006. SUBJECT: Changes Conforming to CR3648 for Therapy Services
 CMS Manual System Pub 100-03 Medicare National Coverage Determinations Department of Health & Human Services (DHHS) Centers for Medicare & Medicaid Services (CMS) Transmittal 55 Date: MAY 5, 2006 Change
CMS Manual System Pub 100-03 Medicare National Coverage Determinations Department of Health & Human Services (DHHS) Centers for Medicare & Medicaid Services (CMS) Transmittal 55 Date: MAY 5, 2006 Change
Guidelines for Medical Necessity Determination for Speech and Language Therapy
 Guidelines for Medical Necessity Determination for Speech and Language Therapy These Guidelines for Medical Necessity Determination (Guidelines) identify the clinical information MassHealth needs to determine
Guidelines for Medical Necessity Determination for Speech and Language Therapy These Guidelines for Medical Necessity Determination (Guidelines) identify the clinical information MassHealth needs to determine
Pulmonary Rehab Definitions Framework Self-Assessment Tool outpatient/ambulatory care Rehab Survey for Pulmonary Rehab
 Pulmonary Rehab s Framework Self-Assessment Tool outpatient/ambulatory care Rehab Survey for Pulmonary Rehab INTRODUCTION: In response to a changing rehab landscape in which rehabilitation is offered in
Pulmonary Rehab s Framework Self-Assessment Tool outpatient/ambulatory care Rehab Survey for Pulmonary Rehab INTRODUCTION: In response to a changing rehab landscape in which rehabilitation is offered in
May 7, 2012. Submitted Electronically
 May 7, 2012 Submitted Electronically Secretary Kathleen Sebelius Department of Health and Human Services Office of the National Coordinator for Health Information Technology Attention: 2014 edition EHR
May 7, 2012 Submitted Electronically Secretary Kathleen Sebelius Department of Health and Human Services Office of the National Coordinator for Health Information Technology Attention: 2014 edition EHR
Use and Value of Data Analytics. Comparative Effectiveness Study Inpatient Rehab Hospital (IRH) vs. Skilled Nursing Facility (SNF)
 vs. Skilled Nursing Facility (SNF)") Use and Value of Data Analytics Comparative Effectiveness Study Inpatient Rehab Hospital (IRH) vs. Skilled Nursing Facility (SNF) Ryan Wilson Vice President of Managed Care HealthSouth Corporation Gerry
Use and Value of Data Analytics Comparative Effectiveness Study Inpatient Rehab Hospital (IRH) vs. Skilled Nursing Facility (SNF) Ryan Wilson Vice President of Managed Care HealthSouth Corporation Gerry
M Y H O M E C A R E B I Z
 IT S COMPETITIVE OUT THERE Do you want more business? You need an edge Also Medicare will be providing financial bonuses to HHAs for good care IT S COMPETITIVE OUT THERE MAINE In Maine 25,000 Medicare
IT S COMPETITIVE OUT THERE Do you want more business? You need an edge Also Medicare will be providing financial bonuses to HHAs for good care IT S COMPETITIVE OUT THERE MAINE In Maine 25,000 Medicare
NICHE: Innovations and Nursing Practice
 NICHE: Innovations and Nursing Practice nicheprogram.org Linda Bub MSN, RN, GCNS-BC Director of Education and Program Development, NICHE Objectives Describe the NICHE program and the impact on nursing
NICHE: Innovations and Nursing Practice nicheprogram.org Linda Bub MSN, RN, GCNS-BC Director of Education and Program Development, NICHE Objectives Describe the NICHE program and the impact on nursing
Clinical Coverage Criteria Extended Care Facility
 Clinical Coverage Criteria Extended Care Facility Document Number: 018 Commercial MassHealth* Commonwealth Care Authorization required X X X Notification within 24 hours of service or next business day
Clinical Coverage Criteria Extended Care Facility Document Number: 018 Commercial MassHealth* Commonwealth Care Authorization required X X X Notification within 24 hours of service or next business day
Chapter Seven Value-based Purchasing
 Chapter Seven Value-based Purchasing Value-based purchasing (VBP) is a pay-for-performance program that affects a significant and growing percentage of Medicare reimbursement for medical providers. It
Chapter Seven Value-based Purchasing Value-based purchasing (VBP) is a pay-for-performance program that affects a significant and growing percentage of Medicare reimbursement for medical providers. It
Life Care Plan vs. Medical Cost Projection: Claims Management Tools
 Life Care Plan vs. Medical Cost Projection: Claims Management Tools Nurse Case Manager Life Care Planner Lynn works for: Stubbe & Associates Miller Park Crain Accident Life Care Plans What is a life care
Life Care Plan vs. Medical Cost Projection: Claims Management Tools Nurse Case Manager Life Care Planner Lynn works for: Stubbe & Associates Miller Park Crain Accident Life Care Plans What is a life care
3/16/2016. Preventing Readmissions Through Compliant Patient Transitions. Transition of Care Statistics. Care Transitions The Regulatory Environment
 Preventing Readmissions Through Compliant Patient Transitions Deborah L. Carlino, RN, MBA, CHC, CHRC Director of Healthcare Compliance and Audit - Rutgers, The State University of New Jersey Melanie A.
Preventing Readmissions Through Compliant Patient Transitions Deborah L. Carlino, RN, MBA, CHC, CHRC Director of Healthcare Compliance and Audit - Rutgers, The State University of New Jersey Melanie A.
Patient s Handbook. Provincial Rehabilitation Unit ONE ISLAND HEALTH SYSTEM ONE ISLAND FUTURE 11HPE41-30364
 Patient s Handbook Provincial Rehabilitation Unit ONE ISLAND FUTURE ONE ISLAND HEALTH SYSTEM 11HPE41-30364 REHABILITATION EQUIPMENT USED ON UNIT 7 During a patient s stay on Unit 7, various pieces of
Patient s Handbook Provincial Rehabilitation Unit ONE ISLAND FUTURE ONE ISLAND HEALTH SYSTEM 11HPE41-30364 REHABILITATION EQUIPMENT USED ON UNIT 7 During a patient s stay on Unit 7, various pieces of
Rehabilitation After Debilitation. James Inzerillo MD Physiatrist
 Rehabilitation After Debilitation James Inzerillo MD Physiatrist What Happens to Me If I m I m Not Able to Take Care of Myself? Rehabilitation Options Self-Rehabilitation Outpatient Rehab At Home Rehab
Rehabilitation After Debilitation James Inzerillo MD Physiatrist What Happens to Me If I m I m Not Able to Take Care of Myself? Rehabilitation Options Self-Rehabilitation Outpatient Rehab At Home Rehab
Nancy L. Wilson Department of Medicine-Geriatrics Houston Center for Quality of Care& Utilization Studies Texas Consortium of Geriatric Education
 1 Nancy L. Wilson Department of Medicine-Geriatrics Houston Center for Quality of Care& Utilization Studies Texas Consortium of Geriatric Education Centers Care for Elders Governing Council Acknowledge
1 Nancy L. Wilson Department of Medicine-Geriatrics Houston Center for Quality of Care& Utilization Studies Texas Consortium of Geriatric Education Centers Care for Elders Governing Council Acknowledge
Community Care of North Carolina
 Community Care of North Carolina CCNC Transitional Care Management Jennifer Cockerham, RN, BSN, CDE Director, Chronic Care Programs & Quality Management 1 Chronic Care Population Within the NC Medicaid
Community Care of North Carolina CCNC Transitional Care Management Jennifer Cockerham, RN, BSN, CDE Director, Chronic Care Programs & Quality Management 1 Chronic Care Population Within the NC Medicaid
Chapter 4 Health Care Management Unit 1: Care Management
 Chapter 4 Health Care Unit 1: Care In This Unit Topic See Page Unit 1: Care Care 2 6 Emergency 7 4.1 Care Healthcare Healthcare (HMS), Highmark Blue Shield s medical management division, is responsible
Chapter 4 Health Care Unit 1: Care In This Unit Topic See Page Unit 1: Care Care 2 6 Emergency 7 4.1 Care Healthcare Healthcare (HMS), Highmark Blue Shield s medical management division, is responsible
Care Transitions. Provide Your Patients with Effective Transitional Care Without Changing Your Operating Model. Share This
 Care Transitions Provide Your Patients with Effective Transitional Care Without Changing Your Operating Model Brought to you by Amedisys: Architects of a leading patient-centered Care Transitions network.
Care Transitions Provide Your Patients with Effective Transitional Care Without Changing Your Operating Model Brought to you by Amedisys: Architects of a leading patient-centered Care Transitions network.
Care Coordination and Transitions in Behavioral Health
 Care Coordination and Transitions in Behavioral Health Pam Pietruszewski Integrated Health Consultant The National Council for Behavioral Health This product is supported by the Florida Department of Children
Care Coordination and Transitions in Behavioral Health Pam Pietruszewski Integrated Health Consultant The National Council for Behavioral Health This product is supported by the Florida Department of Children
AGS REHABILITATION/ POST-HOSPITAL CARE OF THE GERIATRIC FRACTURE PATIENT. Egan Allen, MD University of Rochester
 AGS REHABILITATION/ POST-HOSPITAL CARE OF THE GERIATRIC FRACTURE PATIENT Egan Allen, MD University of Rochester THE AMERICAN GERIATRICS SOCIETY Geriatrics Health Professionals. Leading change. Improving
AGS REHABILITATION/ POST-HOSPITAL CARE OF THE GERIATRIC FRACTURE PATIENT Egan Allen, MD University of Rochester THE AMERICAN GERIATRICS SOCIETY Geriatrics Health Professionals. Leading change. Improving
3/11/15. COPD Disease Management Tackling the Transition. Objectives. Describe the multidisciplinary approach to inpatient care for COPD patients
 Faculty Disclosures COPD Disease Management Tackling the Transition Dr. Cappelluti has no actual or potential conflicts of interest associated with this presentation. Jane Reardon has no actual or potential
Faculty Disclosures COPD Disease Management Tackling the Transition Dr. Cappelluti has no actual or potential conflicts of interest associated with this presentation. Jane Reardon has no actual or potential
INTERACT VERSION 3.0 and Beyond
 INTERACT VERSION 3.0 and Beyond Nancy Henry, GNP-BC, PhD Florida Atlantic University Boca Raton, Florida The 4 th National Readmissions Summit The Leading Forum on Hospital Readmissions and Strategies
INTERACT VERSION 3.0 and Beyond Nancy Henry, GNP-BC, PhD Florida Atlantic University Boca Raton, Florida The 4 th National Readmissions Summit The Leading Forum on Hospital Readmissions and Strategies
Aiming for Fewer Hospital U-turns: The Medicare Hospital Readmission Reduction Program
 Aiming for Fewer Hospital U-turns: The Medicare Hospital Readmission Reduction Program Cristina Boccuti and Giselle Casillas For Medicare patients, hospitalizations can be stressful; even more so when
Aiming for Fewer Hospital U-turns: The Medicare Hospital Readmission Reduction Program Cristina Boccuti and Giselle Casillas For Medicare patients, hospitalizations can be stressful; even more so when
Improvement in Dyspnea Implementing Pulmonary Rehabilitation in the Home
 Improvement in Dyspnea Implementing Pulmonary Rehabilitation in the Home Mary Cesarz MS, PT Lisa Gorski MS, APRN, BC, FAAN Wheaton Franciscan Home Health & Hospice Milwaukee, WI Objectives To identify
Improvement in Dyspnea Implementing Pulmonary Rehabilitation in the Home Mary Cesarz MS, PT Lisa Gorski MS, APRN, BC, FAAN Wheaton Franciscan Home Health & Hospice Milwaukee, WI Objectives To identify
Patients Receive Recommended Care for Community-Acquired Pneumonia
 Patients Receive Recommended Care for Community-Acquired Pneumonia For New Jersey to be a state in which all people live long, healthy lives. DSRIP LEARNING COLLABORATIVE PRESENTATION The Care you Trust!
Patients Receive Recommended Care for Community-Acquired Pneumonia For New Jersey to be a state in which all people live long, healthy lives. DSRIP LEARNING COLLABORATIVE PRESENTATION The Care you Trust!
Concept Series Paper on Disease Management
 Concept Series Paper on Disease Management Disease management is the concept of reducing health care costs and improving quality of life for individuals with chronic conditions by preventing or minimizing
Concept Series Paper on Disease Management Disease management is the concept of reducing health care costs and improving quality of life for individuals with chronic conditions by preventing or minimizing
COPD 30 Day Readmission Project SAINT THOMAS RUTHERFORD MURFREESBORO, TN SEPTEMBER 15, 2015 DAVID M. SELLERS, MD, MBA
 COPD 30 Day Readmission Project SAINT THOMAS RUTHERFORD MURFREESBORO, TN SEPTEMBER 15, 2015 DAVID M. SELLERS, MD, MBA USA COPD Data 24 Million Americans under the age of 65 with COPD Almost 20% readmit
COPD 30 Day Readmission Project SAINT THOMAS RUTHERFORD MURFREESBORO, TN SEPTEMBER 15, 2015 DAVID M. SELLERS, MD, MBA USA COPD Data 24 Million Americans under the age of 65 with COPD Almost 20% readmit
Coordinating Transitions of Care: It Takes a Village
 Coordinating Transitions of Care: It Takes a Village Ken Laube RN, BSN, MBA: Vice President Clinical Excellence Situation/Background Patients face significant challenges when moving from one health care
Coordinating Transitions of Care: It Takes a Village Ken Laube RN, BSN, MBA: Vice President Clinical Excellence Situation/Background Patients face significant challenges when moving from one health care
Goals and Objectives
 Care Transitions from the Skilled Nursing Facility Perspective: What Hospitals Need to Know Lessons Learned from working in a Skilled Nursing Facility Presented by: Pat Sutton, LSCW, ACM Goals and Objectives
Care Transitions from the Skilled Nursing Facility Perspective: What Hospitals Need to Know Lessons Learned from working in a Skilled Nursing Facility Presented by: Pat Sutton, LSCW, ACM Goals and Objectives
Performance Measurement for the Medicare and Medicaid Eligible (MME) Population in Connecticut Survey Analysis
 Population in Connecticut Survey Analysis") Performance Measurement for the Medicare and Medicaid Eligible (MME) Population in Connecticut Survey Analysis Methodology: 8 respondents The measures are incorporated into one of four sections: Highly
Performance Measurement for the Medicare and Medicaid Eligible (MME) Population in Connecticut Survey Analysis Methodology: 8 respondents The measures are incorporated into one of four sections: Highly
2009 QUALITY AND SOCIAL RESPONSIBILITY REPORT
 2009 QUALITY AND SOCIAL RESPONSIBILITY REPORT Each year, more than 8.5 million people 23,000 a day are discharged from short-term acute care hospitals and require some form of post-acute care. CONTENTS
2009 QUALITY AND SOCIAL RESPONSIBILITY REPORT Each year, more than 8.5 million people 23,000 a day are discharged from short-term acute care hospitals and require some form of post-acute care. CONTENTS
Basic Training: Home Health Edition. Defining and Documenting, Medical Necessity. March 28, 2013
 Basic Training: Home Health Edition Defining and Documenting, Medical Necessity March 28, 2013 Presented by: Nancy Buseth, RN, PT, BS, Senior Consultant Fazzi Associates, Inc. 243 King Street, Suite 246
Basic Training: Home Health Edition Defining and Documenting, Medical Necessity March 28, 2013 Presented by: Nancy Buseth, RN, PT, BS, Senior Consultant Fazzi Associates, Inc. 243 King Street, Suite 246
The Rehab Program At Stillwater Medical Center Disclosure Statement January 1 2014 December 31-2014. Patient Name.
 Patient Name Mission Statement The mission of Stillwater Medical Center/ Rehab Center is: to provide an intensive, interdisciplinary rehabilitation program of the highest quality that will result in the
Patient Name Mission Statement The mission of Stillwater Medical Center/ Rehab Center is: to provide an intensive, interdisciplinary rehabilitation program of the highest quality that will result in the
Good Samaritan Inpatient Rehabilitation Program
 Good Samaritan Inpatient Rehabilitation Program Living at your full potential. Welcome When people are sick or injured, our goal is their maximum recovery. We help people live to their full potential.
Good Samaritan Inpatient Rehabilitation Program Living at your full potential. Welcome When people are sick or injured, our goal is their maximum recovery. We help people live to their full potential.
2013 ACO Quality Measures
 ACO 1-7 Patient Satisfaction Survey Consumer Assessment of HealthCare Providers Survey (CAHPS) 1. Getting Timely Care, Appointments, Information 2. How well Your Providers Communicate 3. Patient Rating
ACO 1-7 Patient Satisfaction Survey Consumer Assessment of HealthCare Providers Survey (CAHPS) 1. Getting Timely Care, Appointments, Information 2. How well Your Providers Communicate 3. Patient Rating
Identifying High-Risk Medicare Beneficiaries with Predictive Analytics
 Identifying High-Risk Medicare Beneficiaries with Predictive Analytics September 2014 Until recently, with the passage of the Affordable Care Act (ACA), Medicare Fee-for-Service (FFS) providers had little
Identifying High-Risk Medicare Beneficiaries with Predictive Analytics September 2014 Until recently, with the passage of the Affordable Care Act (ACA), Medicare Fee-for-Service (FFS) providers had little
National Stroke Association s Guide to Choosing Stroke Rehabilitation Services
 National Stroke Association s Guide to Choosing Stroke Rehabilitation Services Rehabilitation, often referred to as rehab, is an important part of stroke recovery. Through rehab, you: Re-learn basic skills
National Stroke Association s Guide to Choosing Stroke Rehabilitation Services Rehabilitation, often referred to as rehab, is an important part of stroke recovery. Through rehab, you: Re-learn basic skills
APPENDIX 1: INTERDISCIPLINARY APPROACH TO PREVENTION AND MANAGEMENT OF DIABETIC FOOT COMPLICATIONS
 APPENDIX 1: INTERDISCIPLINARY APPROACH TO PREVENTION AND MANAGEMENT OF DIABETIC FOOT COMPLICATIONS Template: Regional Foot Programs should develop a list of available health professionals in the following
APPENDIX 1: INTERDISCIPLINARY APPROACH TO PREVENTION AND MANAGEMENT OF DIABETIC FOOT COMPLICATIONS Template: Regional Foot Programs should develop a list of available health professionals in the following
Using Predictive Analytics to Reduce COPD Readmissions
 Using Predictive Analytics to Reduce COPD Readmissions Agenda Information about PinnacleHealth Today s Environment PinnacleHealth Case Study Questions? PinnacleHealth System Non-profit, community teaching
Using Predictive Analytics to Reduce COPD Readmissions Agenda Information about PinnacleHealth Today s Environment PinnacleHealth Case Study Questions? PinnacleHealth System Non-profit, community teaching
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services. Discharge Planning
 DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services ICN 908184 October 2014 This booklet was current at the time it was published or uploaded onto the web. Medicare policy
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services ICN 908184 October 2014 This booklet was current at the time it was published or uploaded onto the web. Medicare policy
NEW YORK STATE MEDICAID PROGRAM REHABILITATION SERVICES POLICY GUIDELINES
 NEW YORK STATE MEDICAID PROGRAM REHABILITATION SERVICES POLICY GUIDELINES Version 2015-1 Page 1 of 11 Table of Contents SECTION I REQUIREMENTS FOR PARTICIPATION IN MEDICAID 3 QUALIFIED PRACTITIONERS. 3
NEW YORK STATE MEDICAID PROGRAM REHABILITATION SERVICES POLICY GUIDELINES Version 2015-1 Page 1 of 11 Table of Contents SECTION I REQUIREMENTS FOR PARTICIPATION IN MEDICAID 3 QUALIFIED PRACTITIONERS. 3
Basic Standards for Residency Training in Physical Medicine and Rehabilitation
 Basic Standards for Residency Training in Physical Medicine and Rehabilitation American Osteopathic Association and American Osteopathic College of Physical Medicine and Rehabilitation COPT/R-88 Rev. BOT,
Basic Standards for Residency Training in Physical Medicine and Rehabilitation American Osteopathic Association and American Osteopathic College of Physical Medicine and Rehabilitation COPT/R-88 Rev. BOT,
SUBCHAPTER 48C - SCOPE OF PHYSICAL THERAPY PRACTICE SECTION.0100 - PHYSICAL THERAPISTS
 SUBCHAPTER 48C - SCOPE OF PHYSICAL THERAPY PRACTICE SECTION.0100 - PHYSICAL THERAPISTS 21 NCAC 48C.0101 PERMITTED PRACTICE (a) Physical therapy is presumed to include any acts, tests, procedures, modalities,
SUBCHAPTER 48C - SCOPE OF PHYSICAL THERAPY PRACTICE SECTION.0100 - PHYSICAL THERAPISTS 21 NCAC 48C.0101 PERMITTED PRACTICE (a) Physical therapy is presumed to include any acts, tests, procedures, modalities,
The Role of Telemedicine in Home Monitoring and Long Term Care June 7, 2012. Penny S. Milanovich President UPMC Visiting Nurses Association
 The Role of Telemedicine in Home Monitoring and Long Term Care June 7, 2012 Penny S. Milanovich President UPMC Visiting Nurses Association Cost of Chronic Conditions An average of 40-50% of healthcare
The Role of Telemedicine in Home Monitoring and Long Term Care June 7, 2012 Penny S. Milanovich President UPMC Visiting Nurses Association Cost of Chronic Conditions An average of 40-50% of healthcare
105 CMR 143.000: STANDARDS GOVERNING CARDIAC REHABILITATION TREATMENT
 105 CMR 143.000: STANDARDS GOVERNING CARDIAC REHABILITATION TREATMENT Section 143.001: Purpose and Scope 143.002: Authority 143.003: Citation 143.004: Definitions 143.005: General Requirements for Cardiac
105 CMR 143.000: STANDARDS GOVERNING CARDIAC REHABILITATION TREATMENT Section 143.001: Purpose and Scope 143.002: Authority 143.003: Citation 143.004: Definitions 143.005: General Requirements for Cardiac
What to know if Medicare denies coverage
 What to know if Medicare denies coverage What Medicare covers Necessary post-hospital extended care for up to 100 days Extended care: nursing care and rehab provided to a Medicare beneficiary who is an
What to know if Medicare denies coverage What Medicare covers Necessary post-hospital extended care for up to 100 days Extended care: nursing care and rehab provided to a Medicare beneficiary who is an
T- 09 Up Up and Away with Mediocre Therapy Documentation
 T- 09 Up Up and Away with Mediocre Therapy Documentation Carol Ashdown M. A. CCC-SLP RAC-CT CHC Carol Ashdown is a Regional Vice President of Consulting for Exponential Consulting Services specializing
T- 09 Up Up and Away with Mediocre Therapy Documentation Carol Ashdown M. A. CCC-SLP RAC-CT CHC Carol Ashdown is a Regional Vice President of Consulting for Exponential Consulting Services specializing
Stakeholder s Report. 2525 SW 75 th Ave Miami, Florida 33155 305.262.6800 www.westgablesrehabhospital.com
 212 Stakeholder s Report 2525 SW 75 th Ave Miami, Florida 33155 35.262.68 www.westgablesrehabhospital.com PROFILE REPORT For more than 25 years, West Gables Rehabilitation Hospital has made a mission of
212 Stakeholder s Report 2525 SW 75 th Ave Miami, Florida 33155 35.262.68 www.westgablesrehabhospital.com PROFILE REPORT For more than 25 years, West Gables Rehabilitation Hospital has made a mission of
Discharge Planning. Home Care 1. Objectives. Where are they Going?
 Discharge Planning Heidi White, MD Associate Professor of Medicine Yvonne Spurney, RN Associate Chief Nurse Cristina C. Hendrix, DNS, GNP-BC Associate Professor of Nursing Objectives Describe challenges
Discharge Planning Heidi White, MD Associate Professor of Medicine Yvonne Spurney, RN Associate Chief Nurse Cristina C. Hendrix, DNS, GNP-BC Associate Professor of Nursing Objectives Describe challenges
The Centers for Medicare & Medicaid Services (CMS) Acute Care Hospital Fiscal Year (FY) 2018 Quality Improvement Program Measures
 Acute Care Hospital Fiscal Year (FY) 2018 Quality Improvement Program Measures") ID Me asure Name NQF # - (HRRP) ID Me asure Name NQF # - (HRRP) ID Me asure Name NQF # - (HRRP) CMS Measures Fiscal Year 2018 The Centers for Medicare & Medicaid Services (CMS) Acute Care Fiscal Year (FY)
ID Me asure Name NQF # - (HRRP) ID Me asure Name NQF # - (HRRP) ID Me asure Name NQF # - (HRRP) CMS Measures Fiscal Year 2018 The Centers for Medicare & Medicaid Services (CMS) Acute Care Fiscal Year (FY)
Improving Transitions & Reducing Readmissions from Skilled Nursing Facilities. Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies
 Improving Transitions & Reducing Readmissions from Skilled Nursing Facilities Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies Agenda Why this is so important What we know: a review of the
Improving Transitions & Reducing Readmissions from Skilled Nursing Facilities Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies Agenda Why this is so important What we know: a review of the
Section 2. Physical Therapy and Occupational Therapy Services
 Division of Medicaid and Health Financing Updated July 2015 Section 2 Table of Contents 1 General Information... 2 1-1 General Policy... 2 1-2 Fee-For-Service or Managed Care... 3 1-3 Definitions... 3
Division of Medicaid and Health Financing Updated July 2015 Section 2 Table of Contents 1 General Information... 2 1-1 General Policy... 2 1-2 Fee-For-Service or Managed Care... 3 1-3 Definitions... 3
Outpatient/Ambulatory Rehab. Dedicated Trans-disciplinary Team (defined within Annotated References)
") CARDIAC The delivery of Cardiac Rehab is unlike most other rehab populations. The vast majority of patients receive their rehab in outpatient or community settings and only a small subset requires an inpatient
CARDIAC The delivery of Cardiac Rehab is unlike most other rehab populations. The vast majority of patients receive their rehab in outpatient or community settings and only a small subset requires an inpatient