SESSION 6. Progrès en chirurgie et endoscopie des cancers digestifs. Modérateur : Dr. François QUENET
|
|
|
- Sophia Catherine Parsons
- 8 years ago
- Views:
Transcription
1 SESSION 6 Progrès en chirurgie et endoscopie des cancers digestifs Modérateur : Dr. François QUENET

2 La chirurgie robotique Pr. Philippe ROUANET

3 La Chirurgie Robotique en cancérologie digestive Philippe Rouanet

4

5

6

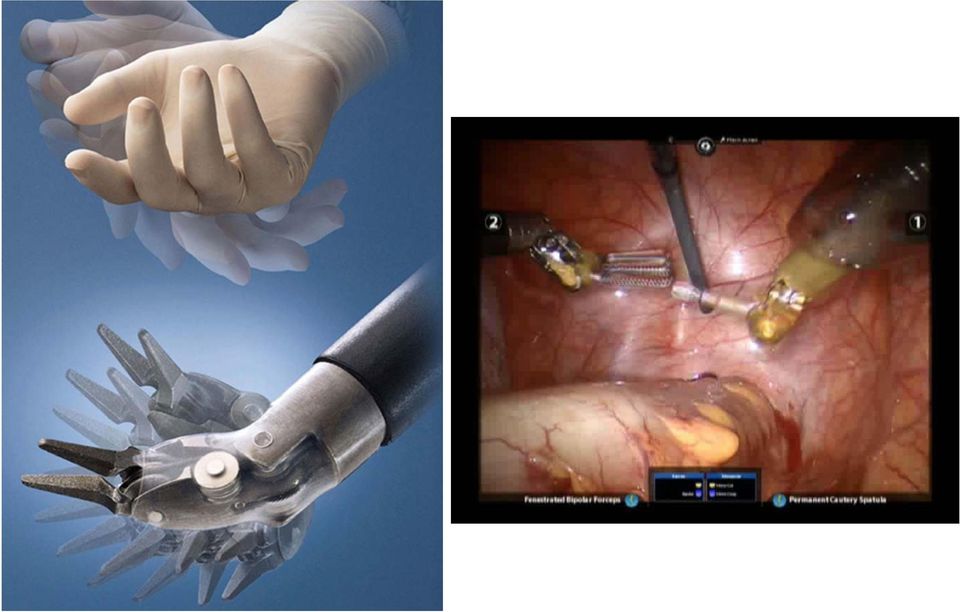
7 Chirurgie Robotique Contrôle «Intuitif» des instruments Contrôle de la Camera Vision 3D HD Instrumentation «EndoWrist» Ergonomie pour le chirurgien

8
9 Depuis Robotic Surgery 5999 Robotic oncologic surgery 446 Robotic digestive surgery 206

10 Robot assistance in liver surgery: a real advantage over a fully laparoscopic approach? Results of a comparative bi-institutional analysis. Troisi R & al. Int J Med Robot 2013 LAPR (Laparoscopic liver resection) vs ROBR (Robot assisted Liver Surgery) LAPR ROBR N Hépatectomie majeure 17% 0 Chirurgie segmentaire 34% 55% Lésions réséquées 1,57 1,97 Conversion 7,6% 20% Saignement 174 ml 330 ml

11 Major early complications following open, laparoscopic and robotic gastrectomy Kim KM & al. BJS 2012 Open Laparoscopic Robotic p n LNH 40* 37 40* <0,001 T1/4 (%) 48 / / 5 77 / 6 <0,001 R0 (%) 99,3 99,8 99,3 0,2 Hosp Stay 10,2 7,8* 7,5* <0,001 Temps Op <0,001 Morbidity 10,7 9,4 10,1 0,494 Leak (%) 1,1 2,1 2,3 0,017 Abscess 3,3 2,0 1,4 0,013 Reoperation 1 1 1,6 0,483 Mortality 0,5 0,3 0,5 1
 1,1 2,1 2,3 0,017 Abscess 3,3 2,0 1,4 0,013 Reoperation 1 1 1,6 0,483")
12

13 Cancer Control. 2013
14 Outcomes After Minimally Invasive Esophagectomy Review of Over 1000 Patients Luketich & al. Ann Surg 2012 MIE Neck McKeown MIE Chest Ivor-Lewis

15 The rise in minimally invasive esophagectomy publications in United States National Library of Medicine service, PubMed. Luketich & al. Ann Surg 2012

16 Notre démarche 2006 : Corum Montpellier Farid Gharagozloo, M.D. Washington Institute of Thoracic and Cardiovascular Surgery George Washington University 37 LS Robot avec anastomose intra thoracique 2012: University Medical Center Utrecht Robot-assisted minimally invasive thoraco-laparoscopic esophagectomy versus open transthoracic esophagectomy for resectable esophageal cancer, a randomized controlled trial (ROBOT trial) van der Sluis et al. Trials 2012, 13:230
 van der Sluis et")
17

18

19 Technical aspects and early results of robotic esophagectomy with chest anastomosis. Cerfolio RJ & al. J Thorac Cardiovasc Surg patients R0 100% LNH 18 BL 40 ml Anastomoses IT - 6 mécaniques morbidité 80% - 16 manuelles morbidité 0%

20
21
22 Robot-assisted laparoscopic surgery of the colon and rectum. Antoniou sa & al. Surg Endosc nonrandomized studies : 1012 patients 13 ileocaecal resections 220 Right colectomies Right C Left C AR APR Total C 190 Left Colectomies 440 Anterior resection 149 APR 11 Total colectomies 60% RC
23 Randomized clinical trial of robot-assisted versus standard laparoscopic right colectomy. Park JS & al. Br J Surg NCT patients : 35/35 Similar Hosp stay - Complications - post op pain blood loss - resection margin - LNH Conversion (0) Duration of surgery R > L (195/130 ; p:<0.0001) Hospital cost R > L (12.235$ / $ ; p:0.013) CCl: Robotic-assisted laparoscopic right colectomy was feasible but provided no benefit to justify the greater cost
24 Robotic versus laparoscopic anterior resection of Sigmoid colon cancer: comparative study of long-term oncologic outcomes. Lim DR & al. Surg Endosc sigmoid colon K: 34 R 146 L Operative technique: Anterior resection Operative time 252 / 217 p: Post op complications 10.3% / 5.9% p:0.28 OS3 92% / 93% p:0.723 CONCLUSION: In this study, R-AR showed safety and feasibility in terms of perioperative clinical and long-term oncologic outcomes. However, the advanced technologies of R-AR did not translate into better long-term oncologic outcomes compared with L-AR
25 Robotic Rectal Cancer
26 Effect of the plane of surgery achieved on local recurrence in patients with operable rectal cancer: a prospective study using data from the MRC CR07 and NCIC-CTG CO16 randomised clinical trial. P Quirke & al. Lancet 2009
27 RTME et Chirurgie conservatrice auteur type n durée Perte sang Spinoglio 2008 Choi 2009 Leong Pigazzi 2010 Zimmern 2010 Koh 2010 Baek 2010 Conv % Morbidité % DMS Nbre N Full % 14% ½ Full* 1 dock Full ISR Full hybrid % % % % % 41% % hybrid % 22% full % % Hybrid % 31% *: laparoscopic rectal section & anastomosis R1 %
28 KR: Robot vs Laparoscopie R L type Rob/ Lap durée Perte sang Conv % Morbidité % DMS Nbre N R1 % Bianchi Full R 75% Park 2010 Hyb % 7.3% Baek 2011 Hyb Patel Hyb * * Kwak Full R *
29 Meta-analysis of robotic and laparoscopic surgery for treatment of rectal cancer. Lin S & al. World J Gastroenterol études : 268 RTME / 393 LTME DS: Taux de conversion NS: Temps op / Saignement / Reprise transit / Hospit Complications / Nbre GGl / DM / CRM
30 The impact of robotic surgery for mid and low rectal cancer: a case-matched analysis of a 3-arm comparison - open, laparoscopic, and robotic surgery. Kang J & al. Ann Surg 2013 OS LS RS p n Op time <0.001 CS 89% 95% NS 99% 0.01 Conv - 1.8% 0.6% 0.62 NOTES - 4% 22% <0.01 ileostomy 32% 27% 22% 0.40 EBL <0.001 CRM+ 10.3% NS 6.7% % 0.09 LN harvested Fist 3.4% 11% 7.3% 0.04 Hosp lenght <0.001 NS
31 Cancer du rectum Notre pratique: OS LS TEM Robotic
32
33 Robotic and laparoscopic total mesorectal excision for conservative rectal surgery: a consecutive monocentric series of 120 patients. RTME n=60 LTME n= 60 p Age median (range) 62 (34 82) 60 (35 85) BMI median 25.8 ( ) 23.8 ( ) Gender M F 40 (66.7%) 20 (33.3%) 42 (70.0%) 18 (30.0%) ASA score (33.3%) 30 (50.0%) 9 (15.0%) 1 (1.7%) 18 (30.0%) 32 (53.3%) 10 (16.7%) 0 (0.0%) Tumor location Upper 11 Mid 6-10 Lower 5 8 (13.3%) 26 (43.3%) 26 (43.3%) 13 (21.7%) 21 (35.0%) 26 (43.3%) Pre op RCT 47 (78.3%) 39 (65.0%) 0.105
34 Robotic and laparoscopic total mesorectal excision for conservative rectal surgery: a consecutive monocentric series of 120 patients. RTME LTME p n=60 n= 60 Type of operation ULCRA PCAA DCAA LCAA 33(55.0%) 11 (18.3%) 8 (13.3%) 8 (13.3%) 30 (50.0%) 19 (31.7%) 11 (18.3%) 0 (0.0%) ISR Complete Partial Mucosectomie None 1 (1.7%) 25 (41.7%) 1 (1.7) 33 (55.0%) 0 (0.0%) 29 (48,4%) 0 (0.0%) 31 (51.7%) TAEP 1 (1.7%) 10 (16.7%) Median operation time (range) 274 min ( ) 228 min ( ) Diverting ileostomy 44 (73.3%) 35 (58.3%) Median EBL (range) 200 ml (0 1100) 100 ml (0 1700) Conversion 2 (3.2 %) 3 (4.8%) 0.661
35 Robotic and laparoscopic total mesorectal excision for conservative rectal surgery: a consecutive monocentric series of 120 patients. RTME (n=60) LTME (n=60) p Median DRM mm (range) 15.0 ( ) 10.0 ( ) Positive CRM 1 3 (6.4%) 4 (9.3%) Median HLN (range) 15 (1 71) 19 (3 68) Median POS (range) 12 (6 27) 11 (6 60) Severe Morbidity Fistula Colic necroses Occlusion Anastomotic abscess Other 17 (28.3%) 3 (5%) 4 (6%) 7 (11%) 1 (1.6%) 2 (3.2%) 12 (20.0%) 4 (6%) 0 (0%) 6 (10%) 2 (3.2%) 0 (0%) Early postop surgery 2 (3.3%) 4 (6.7%) Mortality 3 (5.0 %) 4 (6.8 %) (Log-rank test) Median follow-up 8 [ ] 19.9 [ ] Months (95% IC)
36 Robotic and laparoscopic total mesorectal excision for conservative rectal surgery: a consecutive monocentric series of 120 patients. Minutes Learning Curve First 30 patients patients Minutes
37 Randomized Trial on Robotic Assisted Resection for Rectal Cancer: ROLARR Robotic versus Laparoscopic Resection for Rectal cancer International, Multicentre, Prospective, Randomised controlled trial Total or hybrid procedure 400 patients / end date? Primary outcome: rate of conversion
38 Robot et chirurgie du KR? Dans la «course» entre Laparoscopie et Robotique, il n y a pas de vainqueur pour les cas «faciles» Aujourd hui, le Robot apporte un plus pour les cas difficiles: Homme gros à bassin étroit porteur de tumeur moyenne et basse, surtout antérieure. Mais demain,.?
39 Impact of Robotic Surgery on Sexual and Urinary Functions After Fully Robotic Nerve-Sparing Total Mesorectal Excision for Rectal Cancer. Luca F & al. Ann Surg /08 4/10 ; 74 RTME ; Prospective evaluation Urinary functions Sexual functions Results Urinary: Incontinence, at 1year, unchanged for both sexes Sexual function and General sexual satisfaction decreased 1 month after the surgery comparable at 1 year to those measured before surgery CONCLUSIONS: RTME allows for preservation of urinary and sexual functions. This is probably due to the superior movements of the wristed instruments that facilitate fine dissection, coupled with a stable and magnified view that helps in recognizing the inferior hypogastric plexus.
40
41 Robotic cancer surgery M. H. Sodergren and A. Darzi Institute of Global Health Innovation, Imperial College London. BJS 2013 Robotics is unlikely to displace the human element in the art of surgery, but, with adequate funding, resource allocation and market competition, robotic assistance will likely complement human surgical skills and significantly improve cancer surgery outcomes in the future.
42 Cœlio-chirurgie des cancers œsogastriques Pr. Christophe MARIETTE
43 Service de chirurgie digestive CHRU - Lille
44 Open resections involve significant risk of morbidity and death Purported advantages of MIO Reduced blood loss Reduced morbidity Reduced respiratory complications Less pain Shorter hospital stay Earlier functionnal recovery
45 Minimally invasive oesophagectomy techniques for oesophageal cancer WITH Thoracoscopic Approach Thoracoscopic AND Laparoscopic oesophagectomy with Cervical Anastomosis Thoracoscopic AND Laparoscopic oesophagectomy with Intra- Thoracic Anastomosis Thoracic oesophageal mobilisation with Open Laparotomy and Cervical Anastomosis MIO MIO Hybrid WITHOUT Thoracoscopic Approach Laparoscopic Gastric Mobilisation with Open Thoracotomy and Intra-Thoracic Anastomosis Total Laparoscopic Transhiatal Oesophagectomy Hybrid MIO
46 Mostly single institution case series Few studies report on comparisons with historical/concurrent/matched controls Various surgical techniques used Differences between Eastern and Western countries Differences according to the study period (Learning Curve)
47 Prospective Database Open surgery 64 Hybrid MIO 44 (Thoracoscopy / Laparotomy) Totally MIO 30 Survival curve comparing open (mean survival months ) and MIO (hybrid plus total MIO) (mean survival months) (p=0.501, n=137) World Journal of Surgery (2011) 35:
48 Oncological results... Decreased LOS Postoperative complications reduced significantly World Journal of Surgery (2011) 35:
49 University Hospital Vienna Case controlled pair matched study 31 consecutive patients undergoing MIO (laparoscopy and thoracoscopy) 31 consecutive open oesophagectomies
50
51 Retrospective Study Evaluation of outcomes in 1011 consecutive elective MIO Comparison of modified McKeown MIO to modified Ivor Lewis MIO Study period from with progression to Ivor Lewis MIO and intrathoracic stapled anastomosis in 2005
52
53
54 Less respiratory morbidity Review 31 Articles All of Level III evidence Single centre cohort and comparative studies Shorter Hospital Stay Lower 30 Day Mortality
55 TOTALLY MIO vs. Open Oesophagectomy
56 HYBRID MIO vs. Open Oesophagectomy
57 Comparison open vs. MIO Multi-centre RCT MIO 56 patients Open Resection 59pts Oesophageal Tumours including Siewert type I MIO Performed By - Thoracoscopy / Laparoscopy and cervical incision Open Resection - Right thoracotomy and intrathoracic anastomosis Primary Endpoints - Respiratory complications in first 2 weeks Secondary Endpoints - Operative / Postoperative / Oncological Data
58 Pulmonary infection defined clinical manifestation with confirmation on CXR or CT scan and positive culture
59 Positive results appear to validate MIO by thoracoscopy and laparoscopy... However... Many non-studies variables strongly affect the primary endpoint of TIME trial (malnutrition, smoking habits, pulmonary co-morbidity, performance status)... and small sample? non-equivalent repartition of these variables One lung ventilation only applicable to one group A longitudinal assessment of QoL No multivariate analysis to test independent effect of MIO on post-op course Pneumonia rate in open surgery group is high (34%) may be related to a high vocal cord paralysis rate (14%) in open group (2% in MIO group) Mariette C Lancet 2012
60 372 Ivor-Lewis procedures for cancer 140 consecutive laparoscopy HMIO Randomly matched for: 140 open resections Open group ASA score, age, gender, denutrition, tumoural location and stage, histological subtype, neoadjuvant CRT, epidural analgesia
61 Briez N, Mariette C et al BJS in press
62 HMIO Independent protective factor against major pulmonary complications
63 HMIO -> independent protective factor against major pulmonary complications Laparoscopic gastric mobilisation in OC could be a promising approach Easy, little learning curve Reproducible Do not compromise carcinologic resection significantly pulmonary complications = main source of morbidity after oesophagectomy Briez et al BJS 2012
64 Comparison open vs. MIO Multi-centre RCT Oesophageal Tumours Including Siewert I Surgical Procedure - Thoracotomy plus Laparoscopy Primary Endpoints - Major 30 day morbidity Secondary Endpoints - 30 day morbidity, mortality, pulmonary morbidity - DFS, OS, QOL, Medico-economic
65 Formidable technical challenge Increased complexity brings a higher potential for error Is it sufficiently safe to be offered selectively to patients with early disease? Concerns regarding gastric conduit vascularity and oncological resection Is the middle ground a hybrid procedure? Mariette C Recent Results Cancer Res 2012
66 Morbidité significative donc licite d évaluer place MIG Nombreuses publications qualité hétérogène Méta-analyse ayant inclus essais randomisés et études comparatives de qualité Vinuela F Ann Surg 2012
67 Vinuela F Ann Surg 2012
68 Vinuela F Ann Surg 2012
69 Vinuela F Ann Surg 2012
70 Vinuela F Ann Surg 2012
71 Vinuela F Ann Surg 2012
72 Vinuela F Ann Surg 2012
73 Laparoscopie pour cancer gastrique distal tx complications globales et médicales, durée d hospi, pertes sanguines Pas sur mortalité et complications majeures Moins de gg analysés Peu de données de survie Questions en suspend Sécurité oncologique? Learning curve En Occident? Faisabilité pour gastrectomie totale?
74 Faisabilité technique démontrée Centres entraînés Bénéfices à ce jour non majeurs Peu de données oncologiques à long terme Reproductibilité??? Résultats d essais randomisés à venir Certainement l avenir pour certains patients
75 Endoscopie interventionnelle Dr. Marc GIOVANNINI
76 CFOD, 5-7 SEPTEMBRE 2013
77 DEVELOPPEMENTS RECENTS DISSECTION SOUS-MUQUEUSE RADIOFREQUENCE OESOPHAGIENNE ECHO-ENDOSCOPIE THERAPEUTIQUE DRAINAGE BILIAIRE GUIDE PAR EE ABLATION TUMORALE GUIDEE PAR EE
78 ?
79 90-95% SM % IE
80 HD ENDOSCOPY
81 ESD Mark the lesion Local Injection Marginal Incision SM Dissection Dyeing Sprayer Marking Local Injection Injection Needle Marginal Incision Electro Surgical Knife Submucosal Dissection Hemostasis Marginal Incision, SM Dissection Post ESD for prevention of complication Hemostasis Device
82
83
84
85
86 ESD> EMR pour les cancers superficiels de l estomac (Gotoda, 2007) ESD>EMR pour les cancers superficiels de l oesophage ( Ishihara et al : GIE,2008) Taux de résection curative: 97% vs 71% Pas de différence en terme de complication EMR= lesion <15 mm, ESD=lesion>15 mm ESD>EMR pour les cancers superficiels du colon et rectum (Saito et al, Surg Endosc 2010) 145 CRT traités par ESD vs 228 traités par EMR Taux de récidive de 2% pour l ESD vs 14% pour l EMR (p<0.001) Taux de Perforation =6.2% pour ESD vs 1% pour EMR
87 ENDOSCOPIE TRADITIONNELLE A ECHOUE OU EST IMPOSSIBLE COLLECTIONS PANCREATIQUES ABCES PELVIENS DRAINAGE BILIAIRE DRAINAGE DU WIRSUNG ANASTOMOSE CHOLECYSTO- DUODENALE CHIRURGIE
88 10 F 8 F 6 F 19 G
89
90 QUELLE ALTERNATIVE SI ECHEC DE LA CPRE OU EN CAS DE MODIFICATION ANATOMIQUE? GASTRECTOMIE DPC RESECTION DE LA VBP ET ANASTOMOSE HEPATICO-JEJUNALE CHIRURGIE OU DRAINAGE PERCUTANE RADIOLOGIQUE
91
92
93
94
95
96
97
98 COMPLICATION RATE : 31% 4 DEATHS ( 1 Bile leakage, 1 perforation, 2 bleedings) Extra-Hepatic Intra-Hepatic p value Success 75/89 (84.3%) 132/146 (90.4%) 0.15 Complications 29/89 (32.6%) 52/146 (35.6%) 0.64 Perforation 1/89 (1.1%) 11/146 (7.5%) 0.03 Bile leakage 13/89 (14.6%) 14/146 (9.6%) 0.24 Cholangitis 4/89 (4.5%) 7/146 (4.8%) 0.92 Bleeding 8/89 (9.0%) 18/146 (12.3%) 0.42 Pain 1/89 (1.1%) 4/146 (2.7%) 0.41 Stent Obstruction 2/89 (2.3%) 0/146 (0%) 0.07
99
100
101 AETIOLOGIES K PANCREAS CCK META HILAIRE 8 NO FAILURE OF STENT INSERTION
102 YOUNG FEMALE OF 38 YEARS OLD WITH A LIVER MET OF OVARIAN CANCER STILL ALIVE AFTER 4 YEARS WITH 2 HEPATICO- GASTROSTOMIE AND 3 OTHER METALLIC STENTS IN THE RIGHT LOBE THIS KIND OF DRAINAGE WAS IMPOSSIBLE 10 YEAR AGO!!!!!
103 ENDOSCOPIE THERAPEUTIQUE OFFRE AUJOURD HUI UNE ALTERNATIVE A LA CHIRURGIE MAIS NECESSITE UNE SELECTION TRES PRECISE DES PATIENTS T SUPERFICIELLE DU TUBE DIGESTIF m3 ŒSOPHAGE-ESTOMAC Sm1 COLON-RECTUM ECHOENDOSCOPIE INTERVENTIONNELLE PERMET DES DRAINAGES BILIAIRES COMPLEXES
104
Bridging Techniques. What s between EMR and Traditional Surgery? Elisabeth C. McLemore, MD, FACS, FASCRS
 Bridging Techniques What s between EMR and Traditional Surgery? Elisabeth C. McLemore, MD, FACS, FASCRS Associate Professor of Surgery Assistant Program Director, General Surgery Residency Disclosures
Bridging Techniques What s between EMR and Traditional Surgery? Elisabeth C. McLemore, MD, FACS, FASCRS Associate Professor of Surgery Assistant Program Director, General Surgery Residency Disclosures
Facing a Hysterectomy? If you ve been diagnosed with early stage gynecologic cancer, learn about minimally invasive da Vinci Surgery
 Facing a Hysterectomy? If you ve been diagnosed with early stage gynecologic cancer, learn about minimally invasive da Vinci Surgery The Condition: Early Stage Gynecologic Cancer A variety of gynecologic
Facing a Hysterectomy? If you ve been diagnosed with early stage gynecologic cancer, learn about minimally invasive da Vinci Surgery The Condition: Early Stage Gynecologic Cancer A variety of gynecologic
ESD for colorectal lesions I am in favour. Alessandro Repici, MD Digestive Endoscopy Unit IRCCS Istituto Clinico Humanitas Milano, Italy
 ESD for colorectal lesions I am in favour Alessandro Repici, MD Digestive Endoscopy Unit IRCCS Istituto Clinico Humanitas Milano, Italy Surgery for early colonic lesions 51 pts referred for lap colectomy
ESD for colorectal lesions I am in favour Alessandro Repici, MD Digestive Endoscopy Unit IRCCS Istituto Clinico Humanitas Milano, Italy Surgery for early colonic lesions 51 pts referred for lap colectomy
How to treat early gastric cancer. Surgery
 How to treat early gastric cancer Surgery Mark I. van Berge Henegouwen Department of Surgery, AMC, Amsterdam Director upper GI surgical unit Academic Medical Center Upper GI surgery at AMC 100 oesophagectomies
How to treat early gastric cancer Surgery Mark I. van Berge Henegouwen Department of Surgery, AMC, Amsterdam Director upper GI surgical unit Academic Medical Center Upper GI surgery at AMC 100 oesophagectomies
Facing Pancreatic Surgery? Learn about minimally invasive da Vinci Surgery
 Facing Pancreatic Surgery? Learn about minimally invasive da Vinci Surgery The Condition: Pancreatitis/Pancreatic Cancer The pancreas is an organ that produces enzymes and hormones to help your body digest
Facing Pancreatic Surgery? Learn about minimally invasive da Vinci Surgery The Condition: Pancreatitis/Pancreatic Cancer The pancreas is an organ that produces enzymes and hormones to help your body digest
Basic Laparoscopy and Lap. Suturing and Stapling course Course Contents
 Online Courses on Laparoscopic GI Surgery for GISurgery.info Lap Skills course Harshad Soni 1. Basic Laparoscopy and Lap. Suturing and Stapling course H. Soni 2. Laparoscopic UGI Surgery Course J Mistry
Online Courses on Laparoscopic GI Surgery for GISurgery.info Lap Skills course Harshad Soni 1. Basic Laparoscopy and Lap. Suturing and Stapling course H. Soni 2. Laparoscopic UGI Surgery Course J Mistry
The Royal Marsden. Surgery for Gastric and GE Junction Cancer: primary palliative where and when? William Allum
 The Royal Marsden Surgery for Gastric and GE Junction Cancer: primary palliative where and when? William Allum Any surgeon can cure Surgeon - dependent No surgeon can cure EMR D2 GASTRECTOMY H N SN. WEDGE
The Royal Marsden Surgery for Gastric and GE Junction Cancer: primary palliative where and when? William Allum Any surgeon can cure Surgeon - dependent No surgeon can cure EMR D2 GASTRECTOMY H N SN. WEDGE
Robotic Radical Prostatectomy: What s s the Advantage? Matthew T. Gettman, M.D. Associate Professor Department of Urology
 Robotic Radical Prostatectomy: What s s the Advantage? Matthew T. Gettman, M.D. Associate Professor Department of Urology Prostate Cancer Epidemiology: 2009 Estimated new cases: 230,000 Estimated deaths:
Robotic Radical Prostatectomy: What s s the Advantage? Matthew T. Gettman, M.D. Associate Professor Department of Urology Prostate Cancer Epidemiology: 2009 Estimated new cases: 230,000 Estimated deaths:
Evidence tabel Lokaal palliatieve behandelingen
 Auteurs, jaartal Mate van bewijs Studie type Follow-up Populatie (incl. steekproef-grootte) Patienten kenmerken Interventie Controle Resultaten Conclusie Opmerkingen, commentaar Hartgrink, 2002 The Netherlands
Auteurs, jaartal Mate van bewijs Studie type Follow-up Populatie (incl. steekproef-grootte) Patienten kenmerken Interventie Controle Resultaten Conclusie Opmerkingen, commentaar Hartgrink, 2002 The Netherlands
Clinical Practice Assessment Robotic surgery
 Clinical Practice Assessment Robotic surgery Background: Surgery is by nature invasive. Efforts have been made over time to reduce complications and the trauma inherently associated with surgery through
Clinical Practice Assessment Robotic surgery Background: Surgery is by nature invasive. Efforts have been made over time to reduce complications and the trauma inherently associated with surgery through
9/26/14. Joel E. Rand, MPAS, PA-C DMU Luncheon May 1, 2014
 Joel E. Rand, MPAS, PA-C DMU Luncheon May 1, 2014 No financial relationship or commercial interest in any of the technologies discussed Not supporting any non-fda off label uses of any product or service
Joel E. Rand, MPAS, PA-C DMU Luncheon May 1, 2014 No financial relationship or commercial interest in any of the technologies discussed Not supporting any non-fda off label uses of any product or service
Endoscopic Resection for Barrett s Esophagus and Early Cancer 2014 Masters of Minimally Invasive Surgery
 Endoscopic Resection for Barrett s Esophagus and Early Cancer 2014 Masters of Minimally Invasive Surgery Matthew Hartwig, M.D. Duke Cancer Institute Case Presentation: Patient ER 51 y/o man with schizophrenia
Endoscopic Resection for Barrett s Esophagus and Early Cancer 2014 Masters of Minimally Invasive Surgery Matthew Hartwig, M.D. Duke Cancer Institute Case Presentation: Patient ER 51 y/o man with schizophrenia
PANCREATIC AND PERIAMPULLARY TUMORS: PANCREATICODUODENECTOMY. Dr. Shailesh V. Shrikhande
 PANCREATIC AND PERIAMPULLARY TUMORS: PANCREATICODUODENECTOMY Dr. Shailesh V. Shrikhande Associate Professor & Consultant Surgeon GI and HPB Surgical Oncology Tata Memorial Hospital, Mumbai INDIA HELICAL
PANCREATIC AND PERIAMPULLARY TUMORS: PANCREATICODUODENECTOMY Dr. Shailesh V. Shrikhande Associate Professor & Consultant Surgeon GI and HPB Surgical Oncology Tata Memorial Hospital, Mumbai INDIA HELICAL
Cancer of the Cardia/GE Junction: Surgical Options
 Cancer of the Cardia/GE Junction: Surgical Options Michael A Smith, MD Associate Chief Thoracic Surgery Center for Thoracic Disease St Joseph s Hospital and Medical Center Phoenix, AZ Michael Smith, MD
Cancer of the Cardia/GE Junction: Surgical Options Michael A Smith, MD Associate Chief Thoracic Surgery Center for Thoracic Disease St Joseph s Hospital and Medical Center Phoenix, AZ Michael Smith, MD
Surgery for oesophageal cancer
 Surgery for oesophageal cancer This information is an extract from the booklet Understanding oesophageal cancer (cancer of the gullet). You may find the full booklet helpful. We can send you a free copy
Surgery for oesophageal cancer This information is an extract from the booklet Understanding oesophageal cancer (cancer of the gullet). You may find the full booklet helpful. We can send you a free copy
How To Perform Da Vinci Surgery
 Facing a Hysterectomy? If you ve been diagnosed with early stage gynecologic cancer, learn about minimally invasive da Vinci Surgery The Condition: Early Stage Gynecologic Cancer A variety of gynecologic
Facing a Hysterectomy? If you ve been diagnosed with early stage gynecologic cancer, learn about minimally invasive da Vinci Surgery The Condition: Early Stage Gynecologic Cancer A variety of gynecologic
Endoscopic Therapy for Early Esophageal Cancer: EMR and ESD
 Endoscopic Therapy for Early Esophageal Cancer: EMR and ESD AATS Toronto April 26, 2014 Lorenzo Ferri MD PhD David S. Mulder Chair in Surgery Associate Professor of Surgery and Oncology Disclosures Olympus
Endoscopic Therapy for Early Esophageal Cancer: EMR and ESD AATS Toronto April 26, 2014 Lorenzo Ferri MD PhD David S. Mulder Chair in Surgery Associate Professor of Surgery and Oncology Disclosures Olympus
Cancer Surgery Volume Study: ICD-9 and CPT Codes
 This paper contains the ICD-9 diagnostic and procedure codes and the CPT procedure codes used by researchers for a project of the California HealthCare Foundation (CHCF) and the California Office of Statewide
This paper contains the ICD-9 diagnostic and procedure codes and the CPT procedure codes used by researchers for a project of the California HealthCare Foundation (CHCF) and the California Office of Statewide
Considering Endometriosis Surgery? Learn about minimally invasive da Vinci Surgery
 Considering Endometriosis Surgery? Learn about minimally invasive da Vinci Surgery The Condition: Endometriosis Endometriosis is a condition in which the tissue that lines your uterus (the endometrium)
Considering Endometriosis Surgery? Learn about minimally invasive da Vinci Surgery The Condition: Endometriosis Endometriosis is a condition in which the tissue that lines your uterus (the endometrium)
Endoscopic therapy for obesity and complications of bariatric surgery
 Endoscopic therapy for obesity and complications of bariatric surgery Jacques Devière, MD, PhD Erasme University Hospital Brussels Belgium jacques.deviere@erasme.ulb.ac.be Obesity Affects 300 millions
Endoscopic therapy for obesity and complications of bariatric surgery Jacques Devière, MD, PhD Erasme University Hospital Brussels Belgium jacques.deviere@erasme.ulb.ac.be Obesity Affects 300 millions
Considering Bariatric Surgery? Learn about minimally invasive da Vinci Surgery
 Considering Bariatric Surgery? Learn about minimally invasive da Vinci Surgery The Condition: Obesity Obesity is defined as having a body mass index (BMI) of 30 or greater. Obesity is a serious medical
Considering Bariatric Surgery? Learn about minimally invasive da Vinci Surgery The Condition: Obesity Obesity is defined as having a body mass index (BMI) of 30 or greater. Obesity is a serious medical
INTERVENTIONAL PROCEDURES PROGRAMME
 NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of radical laparoscopic hysterectomy for early stage cervical cancer Introduction This overview
NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of radical laparoscopic hysterectomy for early stage cervical cancer Introduction This overview
The lungs What is lung cancer? How common is it? Risks & symptoms Diagnosis & treatment options
 Why We re Here The lungs What is lung cancer? How common is it? Risks & symptoms Diagnosis & treatment options What Are Lungs? What Do They Do? 1 Located in the chest Allow you to breathe Provide oxygen
Why We re Here The lungs What is lung cancer? How common is it? Risks & symptoms Diagnosis & treatment options What Are Lungs? What Do They Do? 1 Located in the chest Allow you to breathe Provide oxygen
Endoscopy and infection: Prevention of infection during endoscopy Treatment of infection by endoscopy. M. Arvanitakis SRBG June 2009
 Endoscopy and infection: Prevention of infection during endoscopy Treatment of infection by endoscopy M. Arvanitakis SRBG June 2009 Outline Antibiotic prophylaxis during endoscopy Upper GI endoscopy Lower
Endoscopy and infection: Prevention of infection during endoscopy Treatment of infection by endoscopy M. Arvanitakis SRBG June 2009 Outline Antibiotic prophylaxis during endoscopy Upper GI endoscopy Lower
Bowel Preparation for Colon Resection. Eric Klein, M.D. SUNY Downstate Department of Surgery
 Bowel Preparation for Colon Resection Eric Klein, M.D. SUNY Downstate Department of Surgery Historical Perspective During World War II, failure to treat penetrating colon injuries with diversion could
Bowel Preparation for Colon Resection Eric Klein, M.D. SUNY Downstate Department of Surgery Historical Perspective During World War II, failure to treat penetrating colon injuries with diversion could
The Need for Accurate Lung Cancer Staging
 The Need for Accurate Lung Cancer Staging Peter Baik, DO Thoracic Surgery Cancer Treatment Centers of America Oklahoma Osteopathic Association 115th Annual Convention Financial Disclosures: None 2 Objectives
The Need for Accurate Lung Cancer Staging Peter Baik, DO Thoracic Surgery Cancer Treatment Centers of America Oklahoma Osteopathic Association 115th Annual Convention Financial Disclosures: None 2 Objectives
Facing Prostate Cancer Surgery? Learn about minimally invasive da Vinci Surgery
 Facing Prostate Cancer Surgery? Learn about minimally invasive da Vinci Surgery The Condition: Prostate Cancer Your prostate is a walnut-sized gland that is part of the male reproductive system. The prostate
Facing Prostate Cancer Surgery? Learn about minimally invasive da Vinci Surgery The Condition: Prostate Cancer Your prostate is a walnut-sized gland that is part of the male reproductive system. The prostate
Endoscopic Management of Strictures and Leaks. Prepared by Aurora D. Pryor, MD Presented by Dana Portenier, MD Duke University Medical Center
 Endoscopic Management of Strictures and Leaks Prepared by Aurora D. Pryor, MD Presented by Dana Portenier, MD Duke University Medical Center What can go wrong? Bleeding (2%) Sleeve too big Angulated Too
Endoscopic Management of Strictures and Leaks Prepared by Aurora D. Pryor, MD Presented by Dana Portenier, MD Duke University Medical Center What can go wrong? Bleeding (2%) Sleeve too big Angulated Too
Stadards in Abdominoperineal Resection
 Stadards in Abdominoperineal Resection Manuel Francisco T. Roxas, MD, FPCS, FPSCRS, FACS Clinical Associate Professor, University of the Philippines Chief, Section of Colorectal Surgery, Department of
Stadards in Abdominoperineal Resection Manuel Francisco T. Roxas, MD, FPCS, FPSCRS, FACS Clinical Associate Professor, University of the Philippines Chief, Section of Colorectal Surgery, Department of
GENERAL SUMMARY AND DISCUSSION
 GENERAL SUMMARY AND DISCUSSION In the last 30 years, abdominal surgery has progressed from the standard open approach to less invasive techniques such as laparoscopy and natural orifice translumenal endoscopic
GENERAL SUMMARY AND DISCUSSION In the last 30 years, abdominal surgery has progressed from the standard open approach to less invasive techniques such as laparoscopy and natural orifice translumenal endoscopic
Adiuwantowe i neoadiuwantowe leczenie chorych na zaawansowanego raka żołądka
 Adiuwantowe i neoadiuwantowe leczenie chorych na zaawansowanego raka żołądka Neoadiuvant and adiuvant therapy for advanced gastric cancer Franco Roviello, IT Neoadjuvant and adjuvant therapy for advanced
Adiuwantowe i neoadiuwantowe leczenie chorych na zaawansowanego raka żołądka Neoadiuvant and adiuvant therapy for advanced gastric cancer Franco Roviello, IT Neoadjuvant and adjuvant therapy for advanced
Understanding Laparoscopic Colorectal Surgery
 Understanding Laparoscopic Colorectal Surgery University Colon & Rectal Surgery A Problem with Your Colon Your doctor has told you that you have a colon problem. Now you ve learned that surgery is needed
Understanding Laparoscopic Colorectal Surgery University Colon & Rectal Surgery A Problem with Your Colon Your doctor has told you that you have a colon problem. Now you ve learned that surgery is needed
Thomas A. Kollmorgen, M.D. Oregon Urology Institute
 Thomas A. Kollmorgen, M.D. Oregon Urology Institute None 240,000 new diagnosis per year, and an estimated 28,100 deaths (2012) 2 nd leading cause of death from cancer in U.S.A. Approximately 1 in 6 men
Thomas A. Kollmorgen, M.D. Oregon Urology Institute None 240,000 new diagnosis per year, and an estimated 28,100 deaths (2012) 2 nd leading cause of death from cancer in U.S.A. Approximately 1 in 6 men
TITLE: Minimal Access Lobectomy for Lung Cancer Patients: A Review of the Clinical and Cost-Effectiveness
 TITLE: Minimal Access Lobectomy for Lung Cancer Patients: A Review of the Clinical and Cost-Effectiveness DATE: 02 February 2009 CONTEXT AND POLICY ISSUES: In Canada, lung cancer is the most common type
TITLE: Minimal Access Lobectomy for Lung Cancer Patients: A Review of the Clinical and Cost-Effectiveness DATE: 02 February 2009 CONTEXT AND POLICY ISSUES: In Canada, lung cancer is the most common type
restricted to certain centers and certain patients, preferably in some sort of experimental trial format.
 Managing Pancreatic Cancer, Part 4: Pancreatic Cancer Surgery, Complications, & the Importance of Surgical Volume Dr. Matthew Katz, Surgeon, MD Anderson Cancer Center, Houston, TX I m going to talk a little
Managing Pancreatic Cancer, Part 4: Pancreatic Cancer Surgery, Complications, & the Importance of Surgical Volume Dr. Matthew Katz, Surgeon, MD Anderson Cancer Center, Houston, TX I m going to talk a little
Acute Abdominal Pain following Bariatric Surgery. Disclosure. Objectives 8/17/2015. I have nothing to disclose
 Acute Abdominal Pain following Bariatric Surgery Kathy J. Morris, DNP, APRN, FNP C, FAANP University of Nebraska Medical Center College of Nursing Disclosure I have nothing to disclose Objectives Pathophysiology
Acute Abdominal Pain following Bariatric Surgery Kathy J. Morris, DNP, APRN, FNP C, FAANP University of Nebraska Medical Center College of Nursing Disclosure I have nothing to disclose Objectives Pathophysiology
SBRT (Elekta), 45 Gy in fractions of 3 Gy 3x/week for 5 weeks (N=22) vs.
, 45 Gy in fractions of 3 Gy 3x/week for 5 weeks (N=22) vs.") Uitgangsvraag 6: Wat is de plaats van stereotactische radiotherapiebehandeling (SBRT) bij HCC patiënten? Primaire studies I Study ID II Method III Patient characteristics IV Intervention(s) V Results primary
Uitgangsvraag 6: Wat is de plaats van stereotactische radiotherapiebehandeling (SBRT) bij HCC patiënten? Primaire studies I Study ID II Method III Patient characteristics IV Intervention(s) V Results primary
Facing Lung Cancer? Learn why da Vinci Surgery may be your best treatment option for lung cancer.
 Facing Lung Cancer? Learn why da Vinci Surgery may be your best treatment option for lung cancer. The Condition: Lung Cancer The lung is the organ that moves oxygen through your body. You have two lungs
Facing Lung Cancer? Learn why da Vinci Surgery may be your best treatment option for lung cancer. The Condition: Lung Cancer The lung is the organ that moves oxygen through your body. You have two lungs
Robotic Assisted Surgery
 WA Health Technology Assessment Robotic Assisted Surgery Health Technology Assessment Program UPDATED FINAL EVIDENCE REPORT May 3, 2012 Health Technology Assessment Program (HTA) Washington State Health
WA Health Technology Assessment Robotic Assisted Surgery Health Technology Assessment Program UPDATED FINAL EVIDENCE REPORT May 3, 2012 Health Technology Assessment Program (HTA) Washington State Health
Laparoscopic One Anastomosis Gastric Bypass (LOAGB) How I do it
 How I do it") CENTER OF EXCELLENCE FOR THE STUDY AND OBESITY TREATMENT Laparoscopic One Anastomosis Gastric Bypass (LOAGB) How I do it Concepts and Results in a series of 11-years experience with 2,200 patients Miguel-A.
CENTER OF EXCELLENCE FOR THE STUDY AND OBESITY TREATMENT Laparoscopic One Anastomosis Gastric Bypass (LOAGB) How I do it Concepts and Results in a series of 11-years experience with 2,200 patients Miguel-A.
Resection of Lung Cancer Invading the Mediastinum
 Resection of Lung Cancer Invading the Mediastinum Philippe G. Dartevelle MARIE-LANNELONGUE HOSPITAL GUSTAVE ROUSSY INSTITUTE INSTITUTE OF THORACIC ONCOLOGY PARIS SUD UNIVERSITY Mediastinal Invasion Superior
Resection of Lung Cancer Invading the Mediastinum Philippe G. Dartevelle MARIE-LANNELONGUE HOSPITAL GUSTAVE ROUSSY INSTITUTE INSTITUTE OF THORACIC ONCOLOGY PARIS SUD UNIVERSITY Mediastinal Invasion Superior
Evolution of Barrett s esophagus
 Endoscopic Treatment and Surveillance of Esophageal Cancer: GI Perspective Charles J. Lightdale, MD Columbia University New York, NY Evolution of Barrett s esophagus Squamous esophagus Chronic inflammation
Endoscopic Treatment and Surveillance of Esophageal Cancer: GI Perspective Charles J. Lightdale, MD Columbia University New York, NY Evolution of Barrett s esophagus Squamous esophagus Chronic inflammation
Preoperative drainage is always indicated in malignant CBD strictures PRO. Horst Neuhaus Evangelisches Krankenhaus Düsseldorf, Germany
 Preoperative drainage is always indicated in malignant CBD strictures PRO Horst Neuhaus Evangelisches Krankenhaus Düsseldorf, Germany Background Jaundice is associated with high perioperative morbidity
Preoperative drainage is always indicated in malignant CBD strictures PRO Horst Neuhaus Evangelisches Krankenhaus Düsseldorf, Germany Background Jaundice is associated with high perioperative morbidity
Management of Peritoneal Metastases (PM) from colorectal cancers: New Perspectives. Dominique ELIAS
 from colorectal cancers: New Perspectives. Dominique ELIAS") Management of Peritoneal Metastases (PM) from colorectal cancers: New Perspectives Dominique ELIAS Declaration of interest BOARDS Congress and teaching 0 Merck 0 Ipsen Novartis Sanofi Trials The peritoneum
Management of Peritoneal Metastases (PM) from colorectal cancers: New Perspectives Dominique ELIAS Declaration of interest BOARDS Congress and teaching 0 Merck 0 Ipsen Novartis Sanofi Trials The peritoneum
Benign Esophageal Perforations: Better Keep a Surgeon in the Toolkit
 Benign Esophageal Perforations: Better Keep a Surgeon in the Toolkit Bryan F. Meyers MD MPH Patrick and Joy Williamson Professor of Surgery Background Esophageal perforation is a difficult problem to characterize,
Benign Esophageal Perforations: Better Keep a Surgeon in the Toolkit Bryan F. Meyers MD MPH Patrick and Joy Williamson Professor of Surgery Background Esophageal perforation is a difficult problem to characterize,
Laparoscopic Repair of Incisional Hernia. Maria B. ALBUJA-CRUZ, MD University of Colorado Department of Surgery-Grand Rounds
 Laparoscopic Repair of Incisional Hernia Maria B. ALBUJA-CRUZ, MD University of Colorado Department of Surgery-Grand Rounds Overview Definition Advantages of Laparoscopic Repair Disadvantages of Open Repair
Laparoscopic Repair of Incisional Hernia Maria B. ALBUJA-CRUZ, MD University of Colorado Department of Surgery-Grand Rounds Overview Definition Advantages of Laparoscopic Repair Disadvantages of Open Repair
National Bowel Cancer Audit Report 2008 Public and Executive Summary
 National Bowel Cancer Audit Report 2008 Public and Executive Summary Prepared in association with: Healthcare Quality Improvement Partnership HQIP Association of Coloproctology of Great Britain and Ireland
National Bowel Cancer Audit Report 2008 Public and Executive Summary Prepared in association with: Healthcare Quality Improvement Partnership HQIP Association of Coloproctology of Great Britain and Ireland
Summa Health System. A Woman s Guide to Hysterectomy
 Summa Health System A Woman s Guide to Hysterectomy Hysterectomy A hysterectomy is a surgical procedure to remove a woman s uterus (womb). The uterus is the organ which shelters and nourishes a baby during
Summa Health System A Woman s Guide to Hysterectomy Hysterectomy A hysterectomy is a surgical procedure to remove a woman s uterus (womb). The uterus is the organ which shelters and nourishes a baby during
Sleeve gastrectomy or gastric bypass as revisional bariatric procedures: retrospective evaluation of outcomes. Abstract Background Methods:
 Sleeve gastrectomy or gastric bypass as revisional bariatric procedures: retrospective evaluation of outcomes. Mousa Khoursheed, Ibtisam Al-Bader, Ali Mouzannar, Abdulla Al-Haddad, Ali Sayed, Ali Mohammad,
Sleeve gastrectomy or gastric bypass as revisional bariatric procedures: retrospective evaluation of outcomes. Mousa Khoursheed, Ibtisam Al-Bader, Ali Mouzannar, Abdulla Al-Haddad, Ali Sayed, Ali Mohammad,
Results of Surgery in a New Lung Institute in South Texas Focused on the Treatment of Lung Cancer
 Results of Surgery in a New Lung Institute in South Texas Focused on the Treatment of Lung Cancer Lung cancer accounts for 13% of all cancer diagnoses and is the leading cause of cancer death in both males
Results of Surgery in a New Lung Institute in South Texas Focused on the Treatment of Lung Cancer Lung cancer accounts for 13% of all cancer diagnoses and is the leading cause of cancer death in both males
Richard M Peterson, MD MPH FACS Chief UT Medicine Center for Bariatric and Metabolic Surgery Director Christus Weight Loss Institute Assistant
 Richard M Peterson, MD MPH FACS Chief UT Medicine Center for Bariatric and Metabolic Surgery Director Christus Weight Loss Institute Assistant Professor of Surgery UTHSCSA None Laparoscopic adjustable
Richard M Peterson, MD MPH FACS Chief UT Medicine Center for Bariatric and Metabolic Surgery Director Christus Weight Loss Institute Assistant Professor of Surgery UTHSCSA None Laparoscopic adjustable
Mesothelioma. Malignant Pleural Mesothelioma
 Mesothelioma William G. Richards, PhD Brigham and Women s Hospital Malignant Pleural Mesothelioma 2,000-3,000 cases per year (USA) Increasing incidence Asbestos (50-80%, decreasing) 30-40 year latency
Mesothelioma William G. Richards, PhD Brigham and Women s Hospital Malignant Pleural Mesothelioma 2,000-3,000 cases per year (USA) Increasing incidence Asbestos (50-80%, decreasing) 30-40 year latency
Facing a Hernia Repair? Learn about minimally invasive da Vinci Surgery
 Facing a Hernia Repair? Learn about minimally invasive da Vinci Surgery The Condition: Hernia A hernia happens when part of an internal organ or tissue bulges through a hole or weak area in the belly wall
Facing a Hernia Repair? Learn about minimally invasive da Vinci Surgery The Condition: Hernia A hernia happens when part of an internal organ or tissue bulges through a hole or weak area in the belly wall
Overview of Bariatric Surgery
 Overview of Bariatric Surgery To better understand how weight loss surgery works, it is helpful to know how the normal digestive process works. As food moves along the digestive tract, special digestive
Overview of Bariatric Surgery To better understand how weight loss surgery works, it is helpful to know how the normal digestive process works. As food moves along the digestive tract, special digestive
The Link Between Obesity and Diabetes The Rapid Evolution and Positive Results of Bariatric Surgery
 The Link Between Obesity and Diabetes The Rapid Evolution and Positive Results of Bariatric Surgery Michael E. Farkouh, MD, MSc Peter Munk Chair in Multinational Clinical Trials Director, Heart and Stroke
The Link Between Obesity and Diabetes The Rapid Evolution and Positive Results of Bariatric Surgery Michael E. Farkouh, MD, MSc Peter Munk Chair in Multinational Clinical Trials Director, Heart and Stroke
L Lang-Lazdunski, A Bille, S Marshall, R Lal, D Landau, J Spicer
 Pleurectomy/decortication, hyperthermic pleural lavage with povidone-iodine and systemic chemotherapy in malignant pleural mesothelioma. A 10-year experience. L Lang-Lazdunski, A Bille, S Marshall, R Lal,
Pleurectomy/decortication, hyperthermic pleural lavage with povidone-iodine and systemic chemotherapy in malignant pleural mesothelioma. A 10-year experience. L Lang-Lazdunski, A Bille, S Marshall, R Lal,
Weight loss surgery more than just a gastric band
 Weight loss surgery more than just a gastric band Presented by Ms Beth Murgatroyd Honorary Bariatric Nurse Practitioner Mr Ameet G Patel Consultant Surgeon Director of Bariatric Surgery at King s College
Weight loss surgery more than just a gastric band Presented by Ms Beth Murgatroyd Honorary Bariatric Nurse Practitioner Mr Ameet G Patel Consultant Surgeon Director of Bariatric Surgery at King s College
THE SURGICAL TREATMENT OF ESOPHAGEAL CANCER. INDICATIONS, COMPARATIVE ANALYSIS OF SURGICAL TECHNIQUES.
 UNIVERSITY OF MEDICINE AND PHARMACY OF CRAIOVA FACULTY OF MEDICINE THE SURGICAL TREATMENT OF ESOPHAGEAL CANCER. INDICATIONS, COMPARATIVE ANALYSIS OF SURGICAL TECHNIQUES. Scientific coordinator : Prof.
UNIVERSITY OF MEDICINE AND PHARMACY OF CRAIOVA FACULTY OF MEDICINE THE SURGICAL TREATMENT OF ESOPHAGEAL CANCER. INDICATIONS, COMPARATIVE ANALYSIS OF SURGICAL TECHNIQUES. Scientific coordinator : Prof.
da Vinci Prostatectomy Information Guide (Robotically-Assisted Radical Prostatectomy)
") da Vinci Prostatectomy Information Guide (Robotically-Assisted Radical Prostatectomy) Prostate Cancer Overview Prostate cancer is a disease in which malignant (cancer) cells form in the tissues of the
da Vinci Prostatectomy Information Guide (Robotically-Assisted Radical Prostatectomy) Prostate Cancer Overview Prostate cancer is a disease in which malignant (cancer) cells form in the tissues of the
How To Compare The Effects Of A Hysterectomy And A Hysterectomy
 A RANDOMIZED TRIAL COMPARING RADICAL HYSTERECTOMY AND PELVIC NODE DISSECTION VS SIMPLE HYSTERECTOMY AND PELVIC NODE DISSECTION IN PATIENTS WITH LOW RISK EARLY STAGE CERVICAL CANCER A Gynecologic Cancer
A RANDOMIZED TRIAL COMPARING RADICAL HYSTERECTOMY AND PELVIC NODE DISSECTION VS SIMPLE HYSTERECTOMY AND PELVIC NODE DISSECTION IN PATIENTS WITH LOW RISK EARLY STAGE CERVICAL CANCER A Gynecologic Cancer
Rehabilitation and Lung Cancer Resection. Roberto Benzo MD MS Mindful Breathing Laboratory Division of Pulmonary & CCM Mayo Clinic
 Rehabilitation and Lung Cancer Resection Roberto Benzo MD MS Mindful Breathing Laboratory Division of Pulmonary & CCM Mayo Clinic Disclosure Funded by the National Cancer Institute NIH for Preoperative
Rehabilitation and Lung Cancer Resection Roberto Benzo MD MS Mindful Breathing Laboratory Division of Pulmonary & CCM Mayo Clinic Disclosure Funded by the National Cancer Institute NIH for Preoperative
How TARGIT Intra-operative Radiotherapy can help Older Patients with Breast cancer
 How TARGIT Intra-operative Radiotherapy can help Older Patients with Breast cancer Jeffrey S Tobias, Jayant S Vaidya, Frederik Wenz and Michael Baum, University College Hospital, London, UK - on behalf
How TARGIT Intra-operative Radiotherapy can help Older Patients with Breast cancer Jeffrey S Tobias, Jayant S Vaidya, Frederik Wenz and Michael Baum, University College Hospital, London, UK - on behalf
Considering Surgery for Fibroids? Learn about minimally invasive da Vinci Surgery
 Considering Surgery for Fibroids? Learn about minimally invasive da Vinci Surgery The Condition: Uterine Fibroid (Fibroid Tumor) A uterine fibroid is a benign (non-cancerous) tumor that grows in the uterine
Considering Surgery for Fibroids? Learn about minimally invasive da Vinci Surgery The Condition: Uterine Fibroid (Fibroid Tumor) A uterine fibroid is a benign (non-cancerous) tumor that grows in the uterine
Types of Bariatric Procedures. Tejal Brahmbhatt, MD General Surgery Teaching Conference April 18, 2012
 Types of Bariatric Procedures Tejal Brahmbhatt, MD General Surgery Teaching Conference April 18, 2012 A Brief History of Bariatric Surgery First seen in pts with short bowel syndrome weight loss First
Types of Bariatric Procedures Tejal Brahmbhatt, MD General Surgery Teaching Conference April 18, 2012 A Brief History of Bariatric Surgery First seen in pts with short bowel syndrome weight loss First
The outcome of rectal cancer after early salvage surgery following transanal endoscopic microsurgery seems promising
 The outcome of rectal cancer after early salvage surgery following transanal endoscopic microsurgery seems promising Katarina Levic, Orhan Bulut, Peter Hesselfeldt & Steffen Bülow ABSTRACT INTRODUCTION:
The outcome of rectal cancer after early salvage surgery following transanal endoscopic microsurgery seems promising Katarina Levic, Orhan Bulut, Peter Hesselfeldt & Steffen Bülow ABSTRACT INTRODUCTION:
INSTEAD at 5-year follow-up shifts the expectations for endovascular treatment
 INSTEAD at 5-year follow-up shifts the expectations for endovascular treatment Christoph A. Nienaber, MD, FACC University Heart Center Rostock Department of Medicine I - Cardiology christoph.nienaber@med.uni-rostock.de
INSTEAD at 5-year follow-up shifts the expectations for endovascular treatment Christoph A. Nienaber, MD, FACC University Heart Center Rostock Department of Medicine I - Cardiology christoph.nienaber@med.uni-rostock.de
Learning Luncheon 7: Endoscopic Mucosal Resection: When, Where and How?
 Endoscopic Mucosal Resection (EMR): When, Where, and Charles J. Lightdale, MD Columbia University New York, NY Endoscopic Mucosal Resection (EMR) EMR developed for removal of sessile or flat neoplasms
Endoscopic Mucosal Resection (EMR): When, Where, and Charles J. Lightdale, MD Columbia University New York, NY Endoscopic Mucosal Resection (EMR) EMR developed for removal of sessile or flat neoplasms
A Practical Guide to Advances in Staging and Treatment of NSCLC
 A Practical Guide to Advances in Staging and Treatment of NSCLC Robert J. Korst, M.D. Director, Thoracic Surgery Medical Director, The Blumenthal Cancer Center The Valley Hospital Objectives Revised staging
A Practical Guide to Advances in Staging and Treatment of NSCLC Robert J. Korst, M.D. Director, Thoracic Surgery Medical Director, The Blumenthal Cancer Center The Valley Hospital Objectives Revised staging
SURGICAL PREAMBLE SPECIFIC ELEMENTS SURGICAL SERVICES WHICH ARE NOT LISTED AS A "Z" CODE
 Surgical PreambleApril 1, 2015 PREAMBLE SPECIFIC ELEMENTS In addition to the common elements, all surgical services include the following specific elements. A. Supervising the preparation of and/or preparing
Surgical PreambleApril 1, 2015 PREAMBLE SPECIFIC ELEMENTS In addition to the common elements, all surgical services include the following specific elements. A. Supervising the preparation of and/or preparing
Accelerated hemithoracic radiation followed by extrapleural pneumonectomy for malignant pleural mesothelioma
 Accelerated hemithoracic radiation followed by extrapleural pneumonectomy for malignant pleural mesothelioma Marc de Perrot, Ronald Feld, Natasha B Leighl, Andrew Hope, Thomas K Waddell, Shaf Keshavjee,
Accelerated hemithoracic radiation followed by extrapleural pneumonectomy for malignant pleural mesothelioma Marc de Perrot, Ronald Feld, Natasha B Leighl, Andrew Hope, Thomas K Waddell, Shaf Keshavjee,
Neoadjuvant therapy are we doing it right? Short course and chemoradiation
 Neoadjuvant therapy are we doing it right? Short course and chemoradiation Rob Glynne-Jones Mount Vernon Cancer Centre Relevant Endpoints in rectal cancer Local recurrence Disease-free survival Overall
Neoadjuvant therapy are we doing it right? Short course and chemoradiation Rob Glynne-Jones Mount Vernon Cancer Centre Relevant Endpoints in rectal cancer Local recurrence Disease-free survival Overall
Use of stents in esophageal cancer" Hans Gerdes, M.D. Director, GI Endoscopy Unit Memorial Sloan-Kettering Cancer Center
 Use of stents in esophageal cancer" Hans Gerdes, M.D. Director, GI Endoscopy Unit Memorial Sloan-Kettering Cancer Center Features of esophageal cancer Esophageal cancer is an abnormal growth that arises
Use of stents in esophageal cancer" Hans Gerdes, M.D. Director, GI Endoscopy Unit Memorial Sloan-Kettering Cancer Center Features of esophageal cancer Esophageal cancer is an abnormal growth that arises
Endoscopic gastric pouch plication - a novel endoluminal incision free approach to revisional bariatric surgery
 Endoscopic gastric pouch plication - a novel endoluminal incision free approach to revisional bariatric surgery Authors: Chiranjiv S Virk, I Michael Leitman and Elliot R Goodman. Location: Beth Israel
Endoscopic gastric pouch plication - a novel endoluminal incision free approach to revisional bariatric surgery Authors: Chiranjiv S Virk, I Michael Leitman and Elliot R Goodman. Location: Beth Israel
Sur les nouveaux médicaments et les perspectives qu ils offrent (traitement à la carte et survie longue)
") Sur les nouveaux médicaments et les perspectives qu ils offrent (traitement à la carte et survie longue) Professeur Jean Trédaniel Unité de cancérologie thoracique Hôpital Saint-Louis Comparison of Four
Sur les nouveaux médicaments et les perspectives qu ils offrent (traitement à la carte et survie longue) Professeur Jean Trédaniel Unité de cancérologie thoracique Hôpital Saint-Louis Comparison of Four
Informed Consent for Laparoscopic Vertical Sleeve Gastrectomy. Patient Name
 Informed Consent for Laparoscopic Vertical Sleeve Gastrectomy Patient Name Please read this form carefully and ask about anything you may not understand. I consent to have a laparoscopic Vertical Sleeve
Informed Consent for Laparoscopic Vertical Sleeve Gastrectomy Patient Name Please read this form carefully and ask about anything you may not understand. I consent to have a laparoscopic Vertical Sleeve
Surgical & Nutritional Complications of Bariatric Surgery: What Every GI Doc Needs to Know Brian R. Smith, MD, FACS Associate Clinical Professor of
 Surgical & Nutritional Complications of Bariatric Surgery: What Every GI Doc Needs to Know Brian R. Smith, MD, FACS Associate Clinical Professor of Surgery & Associate Residency Program Director UC Irvine
Surgical & Nutritional Complications of Bariatric Surgery: What Every GI Doc Needs to Know Brian R. Smith, MD, FACS Associate Clinical Professor of Surgery & Associate Residency Program Director UC Irvine
Considering a Hysterectomy?
 Considering a Hysterectomy? Learn more about virtually scarless surgery using da Vinci Single-Site technology { {Symptoms & Conditions: Chronic Pain, Heavy Bleeding, Fibroids, Endometriosis, Pelvic Prolapse
Considering a Hysterectomy? Learn more about virtually scarless surgery using da Vinci Single-Site technology { {Symptoms & Conditions: Chronic Pain, Heavy Bleeding, Fibroids, Endometriosis, Pelvic Prolapse
Management of Chest Tubes and Air Leaks after Lung Resection
 Management of Chest Tubes and Air Leaks after Lung Resection Emily Kluck PA-C The Johns Hopkins Hospital Baltimore, MD AATS 2014, Toronto, CAN April 2014 Management of Chest Tubes 1 Overview Review the
Management of Chest Tubes and Air Leaks after Lung Resection Emily Kluck PA-C The Johns Hopkins Hospital Baltimore, MD AATS 2014, Toronto, CAN April 2014 Management of Chest Tubes 1 Overview Review the
Emerging Concepts in Bariatric Surgery
 Emerging Concepts in Bariatric Surgery C Y N T H I A L. L O N G, M D, F A C S S I N A I H O S P I T A L O F B A L T I M O R E D E P A R T M E N T O F S U R G E R Y D I V I S I O N O F M I N I M A L L Y
Emerging Concepts in Bariatric Surgery C Y N T H I A L. L O N G, M D, F A C S S I N A I H O S P I T A L O F B A L T I M O R E D E P A R T M E N T O F S U R G E R Y D I V I S I O N O F M I N I M A L L Y
RESEARCH ARTICLE. Abstract. Introduction. Materials and Methods
 DOI:http://dx.doi.org/10.7314/APJCP.2015.16.13.5483 Perioperative and Oncologic Outcomes with Laparotomy, and Laparoscopic, and Robotic Surgery for Endometrial Cancer RESEARCH ARTICLE Comparison of Perioperative
DOI:http://dx.doi.org/10.7314/APJCP.2015.16.13.5483 Perioperative and Oncologic Outcomes with Laparotomy, and Laparoscopic, and Robotic Surgery for Endometrial Cancer RESEARCH ARTICLE Comparison of Perioperative
The Whipple Procedure. Sally Hodges, Ph.D.(c) Given the length and difficulty of the procedure, regardless of the diagnosis, certain
 Given the length and difficulty of the procedure, regardless of the diagnosis, certain") The Whipple Procedure Sally Hodges, Ph.D.(c) Preoperative procedures Given the length and difficulty of the procedure, regardless of the diagnosis, certain assurances must occur prior to offering a patient
The Whipple Procedure Sally Hodges, Ph.D.(c) Preoperative procedures Given the length and difficulty of the procedure, regardless of the diagnosis, certain assurances must occur prior to offering a patient
Bariatric i Surgery: Optimalizing Outcome Results. Dr. B. Dillemans AZ Sint-Jan AV Brugge-Oostende BARIATRIC SURGERY
 Bariatric i Surgery: Optimalizing i Outcome Results Dr. B. Dillemans AZ Sint-Jan AV Brugge-Oostende THE OBESE PATIENT : A CHALLENGE FOR ANAESTHESIA, Ostend,14/11/09 BARIATRIC SURGERY 50 s : First Reported
Bariatric i Surgery: Optimalizing i Outcome Results Dr. B. Dillemans AZ Sint-Jan AV Brugge-Oostende THE OBESE PATIENT : A CHALLENGE FOR ANAESTHESIA, Ostend,14/11/09 BARIATRIC SURGERY 50 s : First Reported
COMMISSIONING. for ULTRA-RADICAL SURGERY ADVANCED OVARIAN CANCER
 COMMISSIONING for ULTRA-RADICAL SURGERY in ADVANCED OVARIAN CANCER WHY THIS MUST HAPPEN PERSPECTIVE COMMISSIONING FOR WHO, FOR WHAT? Biological Basis Surgical Basis International and national standards
COMMISSIONING for ULTRA-RADICAL SURGERY in ADVANCED OVARIAN CANCER WHY THIS MUST HAPPEN PERSPECTIVE COMMISSIONING FOR WHO, FOR WHAT? Biological Basis Surgical Basis International and national standards
Roux-en-y gastric bypass - clinical perspectives
 Roux-en-y gastric bypass - clinical perspectives Tom Mala Consultant surgeon Department of Gastroenterologic Surgery Oslo University Hospital Bariatric surgery weight loss Sjøstrøm L, JAMA 2012 Five-year
Roux-en-y gastric bypass - clinical perspectives Tom Mala Consultant surgeon Department of Gastroenterologic Surgery Oslo University Hospital Bariatric surgery weight loss Sjøstrøm L, JAMA 2012 Five-year
Technical Aspects of Bariatric Surgical Procedures. Robert O. Carpenter, MD, MPH, FACS Department of Surgery Scott & White Memorial Hospital
 Technical Aspects of Bariatric Surgical Procedures Robert O. Carpenter, MD, MPH, FACS Department of Surgery Scott & White Memorial Hospital Disclosures Allergan, Inc. (Past) Faculty Member Educational
Technical Aspects of Bariatric Surgical Procedures Robert O. Carpenter, MD, MPH, FACS Department of Surgery Scott & White Memorial Hospital Disclosures Allergan, Inc. (Past) Faculty Member Educational
Considering a Hysterectomy?
 Considering a Hysterectomy? Learn more about virtually scarless surgery using da Vinci Single-Site technology { {Symptoms & Conditions: Chronic Pain, Heavy Bleeding, Fibroids, Endometriosis, Adenomyosis,
Considering a Hysterectomy? Learn more about virtually scarless surgery using da Vinci Single-Site technology { {Symptoms & Conditions: Chronic Pain, Heavy Bleeding, Fibroids, Endometriosis, Adenomyosis,
Principles of Radiation Therapy A Bapsi Chakravarthy, MD Associate e P rofessor Professor Radiation Oncology
 Principles of Radiation Therapy A Bapsi Chakravarthy, MD Associate Professor Radiation Oncology Disclosure Information I have no financial relationships to disclose relevant to the conten of this presentation.
Principles of Radiation Therapy A Bapsi Chakravarthy, MD Associate Professor Radiation Oncology Disclosure Information I have no financial relationships to disclose relevant to the conten of this presentation.
Thoracoabdominal aortic aneurysm
 Thoracoabdominal aortic aneurysm Patient (1) - 69 PMH: 2013 - MVP, aortic root replacement with biological valve (Perimount) and subtotal aortic arch replacement Analysis for oppressive chest complaints
Thoracoabdominal aortic aneurysm Patient (1) - 69 PMH: 2013 - MVP, aortic root replacement with biological valve (Perimount) and subtotal aortic arch replacement Analysis for oppressive chest complaints
PATIENT CONSENT TO PROCEDURE - ROUX-EN-Y GASTRIC BYPASS
 As a patient you must be adequately informed about your condition and the recommended surgical procedure. Please read this document carefully and ask about anything you do not understand. Please initial
As a patient you must be adequately informed about your condition and the recommended surgical procedure. Please read this document carefully and ask about anything you do not understand. Please initial
Surgical Treatment of Obesity: A Surgeon s View
 Surgical Treatment of Obesity: A Surgeon s View Jenny J. Choi, MD Director of Bariatrics Associate Director of Clinical Affairs Assistant Professor of Surgery Albert Einstein School of Medicine Montefiore
Surgical Treatment of Obesity: A Surgeon s View Jenny J. Choi, MD Director of Bariatrics Associate Director of Clinical Affairs Assistant Professor of Surgery Albert Einstein School of Medicine Montefiore
Dept. of Medical Imaging University of Ottawa
 ED Visits Related to Bariatric Surgery: Review of Normal Post-Surgical Anatomy as Well as Complications Dept. of Medical Imaging University of Ottawa Disclosures Background Roux-en-Y Gastric Bypass Surgery
ED Visits Related to Bariatric Surgery: Review of Normal Post-Surgical Anatomy as Well as Complications Dept. of Medical Imaging University of Ottawa Disclosures Background Roux-en-Y Gastric Bypass Surgery
A PATIENT S GUIDE TO ABLATION THERAPY
 A PATIENT S GUIDE TO ABLATION THERAPY THE DIVISION OF VASCULAR/INTERVENTIONAL RADIOLOGY THE ROBERT WOOD JOHNSON UNIVERSITY HOSPITAL Treatment options for patients with cancer continue to expand, providing
A PATIENT S GUIDE TO ABLATION THERAPY THE DIVISION OF VASCULAR/INTERVENTIONAL RADIOLOGY THE ROBERT WOOD JOHNSON UNIVERSITY HOSPITAL Treatment options for patients with cancer continue to expand, providing
Surgery and cancer of the pancreas
 Surgery and cancer of the pancreas This information is an extract from the booklet Understanding cancer of the pancreas. You may find the full booklet helpful. We can send you a free copy see page 8. Introduction
Surgery and cancer of the pancreas This information is an extract from the booklet Understanding cancer of the pancreas. You may find the full booklet helpful. We can send you a free copy see page 8. Introduction
Data Management, Audit and Outcomes of the NHS
 Data Management, Audit and Outcomes Providing Accurate Outcomes and Activity Data The Trust has in place robust mechanisms for capturing and reporting on all oesophago-gastric cancer surgery activity and
Data Management, Audit and Outcomes Providing Accurate Outcomes and Activity Data The Trust has in place robust mechanisms for capturing and reporting on all oesophago-gastric cancer surgery activity and
Scott A. Shikora, MD, FACS. Sleeve Gastrectomy. Sleeve Gastrectomy. Sleeve Gastrectomy 11/8/2013
 DISCLOSURE Scott A. Shikora, MD, FACS Scott A. Shikora, MD, FACS Associate Professor of Surgery Harvard Medical School Director, Center for Metabolic and Bariatric Surgery Brigham and Women s Hospital
DISCLOSURE Scott A. Shikora, MD, FACS Scott A. Shikora, MD, FACS Associate Professor of Surgery Harvard Medical School Director, Center for Metabolic and Bariatric Surgery Brigham and Women s Hospital
SUNY DOWNSTATE MEDICAL CENTER SURGERY GRAND ROUNDS February 28, 2013 VERENA LIU, MD ROSEANNA LEE, MD
 SUNY DOWNSTATE MEDICAL CENTER SURGERY GRAND ROUNDS February 28, 2013 VERENA LIU, MD ROSEANNA LEE, MD Case Presentation 35 year old male referred from PMD with an asymptomatic palpable right neck mass PMH/PSH:
SUNY DOWNSTATE MEDICAL CENTER SURGERY GRAND ROUNDS February 28, 2013 VERENA LIU, MD ROSEANNA LEE, MD Case Presentation 35 year old male referred from PMD with an asymptomatic palpable right neck mass PMH/PSH:
Endoskopische Venenentnahme der V. saphena in der koronaren Bypasschirurgie - Aktuelle Datenlage - Dr. med. Stefanie Reutter
 Endoskopische Venenentnahme der V. saphena in der koronaren Bypasschirurgie - Aktuelle Datenlage - Dr. med. Stefanie Reutter Endoskopische Venenentnahme (EVH) - Einführung 1979 Tevaearai und Kollegen haben
Endoskopische Venenentnahme der V. saphena in der koronaren Bypasschirurgie - Aktuelle Datenlage - Dr. med. Stefanie Reutter Endoskopische Venenentnahme (EVH) - Einführung 1979 Tevaearai und Kollegen haben
ERBEJET 2. The versatility of waterjet surgery: ERBEJET 2 with hybrid instruments WATERJET SURGERY
 ERBEJET 2 The versatility of waterjet surgery: ERBEJET 2 with hybrid instruments WATERJET SURGERY Gentle interventions in surgery and endoscopy Waterjet surgery with hybrid technology Waterjet surgery
ERBEJET 2 The versatility of waterjet surgery: ERBEJET 2 with hybrid instruments WATERJET SURGERY Gentle interventions in surgery and endoscopy Waterjet surgery with hybrid technology Waterjet surgery
Current Status of Esophageal Cancer Treatment
 Cancer Current Status of Esophageal Cancer Treatment JMAJ 46(11): 497 503, 2003 Hiroyasu MAKUUCHI Professor and Chairman, Department of Surgery, Tokai University School of Medicine Abstract: The diagnosis
Cancer Current Status of Esophageal Cancer Treatment JMAJ 46(11): 497 503, 2003 Hiroyasu MAKUUCHI Professor and Chairman, Department of Surgery, Tokai University School of Medicine Abstract: The diagnosis
Facing Gallbladder Surgery? Learn why Single-Site da Vinci Surgery may be your best option for virtually scarless results.
 Facing Gallbladder Surgery? Learn why Single-Site da Vinci Surgery may be your best option for virtually scarless results. The Condition: Gallstones and Gallbladder Diseases Your gallbladder is a pear-shaped
Facing Gallbladder Surgery? Learn why Single-Site da Vinci Surgery may be your best option for virtually scarless results. The Condition: Gallstones and Gallbladder Diseases Your gallbladder is a pear-shaped