By definition, medication means something that treats the symptoms of
|
|
|
- Jean Washington
- 8 years ago
- Views:
Transcription
1 Chapter 1 The Nurse s Role in Medication Reconciliation Authors Jennifer S. Johnson, R.N., C.M.A., charge nurse, telemetry unit; Paul Mollo, Pharm.D., director of Pharmacy; Caryl-Ann Mannino, R.N., O.C.N., director of Professional Practice and Oncology; Susan Hiza, M.B.A., management engineer; and Linda Miller, R.N., M.S., C.N.A.A., senior vice president for Nursing, Our Lady of Lourdes Memorial Hospital, Binghamton, New York By definition, medication means something that treats the symptoms of disease and reconciliation means the act of compliance or agreement. Together these two words, medication reconciliation, represent a process by which a complete list of each patient s current medications is obtained every time the patient enters the health care organization and is then communicated to subsequent providers in or out of the same health care organization. The goal of medication reconciliation is to prevent adverse drug events that could occur by allergic reactions, omissions, substitutions, and/or duplications. It is a necessary, yet simple, way of assessing what medications patients are currently taking. Medication reconciliation is necessary because a patient s medications can change at any point in time for any number of reasons (such as a newly diagnosed disease process, an age-related issue, an acute condition, a worsening chronic situation, a short-term need for antibiotics, patient altering medication regimens, or adding nonprescription, herbal, or other products to their regimen, or elective or emergency surgery) and because those medications can 11

2 The Nurse s Role in Medication Safety precipitate one or more allergic reactions, food and drug interactions, and/or drugdrug interactions. Medication reconciliation is an extremely important process that needs to take place every time a patient is involved with any health care system. Therefore, medication reconciliation was clearly an excellent choice when, in July 2004, Our Lady of Lourdes Memorial Hospital, Inc., Binghamton, New York (Lourdes Hospital), was asked by Ascension Health Ministries to participate in one of the eight Priority For Action Teams, whose goal was to have no preventable deaths by July 1, Medication reconciliation was one way to achieve that goal. The Adverse Drug Event (ADE) Priority for Action (PFA) Team selected by Lourdes Hospital was to be mostly composed of direct patient care nurses from all departments (from inpatient to outpatient) and management from various clinical and nonclinical backgrounds, including a pharmacist, a clinical nursing director, a physician, a management engineer, and the chief nursing officer. During the initial team meetings, a crystal clear definition of medication reconciliation was agreed upon so that the medication reconciliation task could be implemented across the organization. (See the box below for the definition of medication reconciliation as well as the language for National Patient Safety Goal 8, which pertains to medication reconciliation.) Because this particular chapter pertains to the nurse s role in medication reconciliation, it is presented in the nursing process format, wherein the nursing assess- Medication Reconciliation: The process of comparing a patient s medication orders (those newly prescribed) with all the medications the patient takes (previously prescribed as well as self-prescribed, including over-the-counter products such as herbals and supplements). 1 National Patient Safety Goal 8 Accurately and completely reconcile medications across the continuum of care. Requirement 8A: There is a process for comparing the patient s current medications with those ordered for the patient while under the care of the organization. Requirement 8B: A complete list of the patient s medications is communicated to the next provider of service when a patient is referred or transferred to another setting, service, practitioner, or level of care within or outside the organization. The complete list of medications is also provided to the patient on discharge from the facility. 12
, was asked by Ascension Health Ministries to participate in one of the eight Priority For Action Teams, whose goal was to have no preventable deaths by July")
3 Chapter 1: The Nurse s Role in Medication Reconciliation ment leads to the diagnosis of the problem, the planning of the goals and outcomes is followed by the implementation of the process, and subsequent evaluation and measurement dictate the success or failure of the process. Assessment Assessment of the issues involved with implementing medication reconciliation by using a pilot unit In September 2004, the organization chose the cardiac telemetry unit as a pilot unit in which to assess and introduce the idea and subsequent use of medication reconciliation. The first test of change for the new process included the following participants: One nurse (who was a member of the ADE team) One physician (who admitted a high number of patients to the pilot unit and would be amenable to change) One patient (who was typical of the patient population and had an accurate list of current medications) Prior to enacting the new process on the pilot unit, medication reconciliation was designed with the nurse, physician, and patient in mind. In the beginning, the hospital system considered several factors: change theory, adult-learner theory, additional paperwork, staffing crises, and the typically hectic, busy nature of a nursing unit. The nurse on the pilot unit as well as the selected physician had to be convinced that the benefit of medication reconciliation outweighed the burden of yet another change, more paperwork, and the potential for being overwhelmed. At first, the medication reconciliation process seemed complicated. Staff members perceived the additional paperwork as tedious. The nurses were naturally resistant and reluctant to embrace another change. They needed to know that the ADE team empathized with them and the ADE team needed the support of the nurses for the process to be successful. The process was to compare the patient s current medications with the medications that the physician ordered on admission to the hospital. That seemed simple enough; however, it was a change to the process and procedure, which created a new, time-consuming, detailed system that was absolutely necessary (and soon would be supported by policy). Fortunately, when the organization presented the process change to nurses from the perspective of patient safety, nurses recognized its importance. After the test of change on the pilot unit by the core individuals involved was successful, the idea was to spread the change. Nurses were beginning to incorporate and streamline medication reconciliation. The first test of change identified issues that the health care team had not considered, including the following: 13

4 The Nurse s Role in Medication Safety Nurses had to ask patients for lists of their current medications, which often were incomplete. Physicians had to order new medications that were pertinent to the hospital diagnosis as well as to the patient s current medication unless there was a duplication or an interaction. Pharmacists had to evaluate all the medications ordered for food and drug interactions and drug-drug interactions. Nurses were going to ask local pharmacies for pertinent information regarding patient s medications over the telephone. Family members would be involved to reconcile a patient s current medication. The goal was to first make medication reconciliation on admission successful on the pilot unit and then to spread the process to the emergency department (ED), then to the remainder of inpatient nursing units, followed by the outpatient areas, the off-site areas, and eventually on discharge from a hospital. Diagnosis Discussion of the current and potential problems for the patient and the nurse When the Lourdes Hospital system first introduced medication reconciliation, it was to include one nurse, one physician, and one patient. It was successful on the pilot unit because of the nature of the unit and the staff working on the unit, which included the following: An extremely dynamic cardiac telemetry unit where change is a daily thing Nurses who knew their unit is often chosen for some project or test of change A cardiologist whose patient population consisted of people with geriatric and cardiac issues who were taking several medications The hospital system initially chose the pilot unit for two reasons: One, a key member of the ADE team was a charge nurse on that unit, and two, that unit had (and still has) a highly collaborative relationship with the ED because of the number of admissions that occur on a daily basis. It only made sense to engage the ED next. And what a challenge it was. It took several revisions of the medication reconciliation process to meet the needs of the nurse, physician, and patient who entered the ED because patients seen belong to several categories, including the following: Those who are assessed, treated, and released within an hour Those who are assessed, treated, and released after some observation Those who are assessed, treated, and admitted Patients from all walks of life enter the ED: those with disabilities and those resulting from disasters, those with little or no familial or financial support, those from nursing homes, and those who are homeless all of whom need to have their 14

5 Chapter 1: The Nurse s Role in Medication Reconciliation medications reconciled when entering the ED. Very early in the formation of the ADE PFA team, a key component to the success of this diligent process was to have an energetic, persuasive ED nurse who regularly attends team meetings and who could drive change. She served not only as a resource person for the team but as a champion of medication reconciliation because she believed it to be an important patient safety issue. When presented to the ED, medication reconciliation was met with the predictable physician and nurse resistance because it was perceived as time consuming and difficult. At first, the ED nurses and physicians resisted having to bear the burden of yet another change and the possibility for more paperwork. (And, yes, the process was time consuming and difficult to accomplish, in the beginning.) When the test of change was spread to the ED, it was done on the first day by the one persuasive nurse team member with one optimistic physician and one patient with a simple diagnosis and few medications. The ADE PFA team was this nurse s committee (all nurses participate in committee membership at Lourdes Hospital) and her colleagues knew this. She believed in the importance of and accepted the challenge of medication reconciliation in the ED. Like anything that is repeated, the process became less complex with each new patient who came to the ED. And, if Lourdes Hospital s PFA was patient safety, then it needed to be done 100% of the time. That was the explanation this nurse team member had to repeat several times a day until her colleagues were convinced that medication reconciliation was the right thing to do (and until it would soon be supported by policy). One complication specific to the ED setting was the fact that patients medication information could be difficult to obtain. At times, the patient had more than one physician in the community. Some patients could not even begin to report what medications they took, when they had taken them, or why. Patients from nursing homes had their medication lists but those lists were quite extensive. Still other patients had detailed lists of medications and could reiterate exactly when they took their last dose medication reconciliation for those patients was relatively easy. In addition to the patients themselves, the nurses found they could rely on different sources of information to obtain accurate medication lists for their patients (for example, family members, local pharmacies, old charts, histories and physicals, and sometimes even the medication container labels). After the pilot unit and the ED adopted the process and after the ADE team provided intensive education for the nurses, pharmacists, and physicians, the process was very quickly spread to all inpatient and outpatient areas, including diagnostic imaging, perioperative services, ambulatory surgery, the GI laboratory, off-site physician offices, hospice, and home care. Essentially, the hospital system 15

6 The Nurse s Role in Medication Safety implemented medication reconciliation from admission to discharge to avoid any confusion with nursing and physician documentation, especially because documentation, by its nature, is ever-changing. National Patient Safety Goal 8 was reiterated throughout the organization. The words medication reconciliation were incorporated into most meeting agendas and discussed in most conversations. Planning Statement of the specific goals, action plans, and outcomes for patient safety National Patient Safety Goal 8 defines the purpose of medication reconciliation, which is to avoid errors of transcription, omission, duplication of therapy, and drug-drug and drug-disease interactions. The Joint Commission answers the question as to who is supposed to complete the medication reconciliation process in its Frequently Asked Questions, which are posted on its Web site. 2 According to the Joint Commission, there are the following two models: 1. The physician completes the medication reconciliation process when he or she writes the orders. 2. The pharmacist or nurse completes the medication reconciliation process before preparing or administering the medications, and then notifies physicians if any concerns arise. The team decided that throughout the Lourdes Hospital system every nurse will ask each one of his or her patients, on admission to the patient care unit, for a list of the medications they are currently taking and will fill out a medication reconciliation form accordingly, with a good faith effort to obtain as complete a list as possible, within 24 hours or less. 1 Besides the actual medication, the nurses will include the following information: dose, route, frequency, reasons for taking the medication, and the time of the last dose taken. Creating the Medication Reconciliation Form The hospital system designed the medication reconciliation form to be used as a physician order form. (See the Medication Reconciliation/Physician Initial Medication Order Form in Figure 1-1 on page 17.) After the physician indicates whether he or she wants the same medications to be continued or stopped, or if the medications have been ordered by the physician elsewhere on previous order sheets, the form can be used as an official physician order form. In addition, the form contains language that indicates how to use the form and that herbals/naturals and supplements will not be dispensed to inpatients. It references Lourdes Hospital s Patient Care Services Policy #29, which states that all products not regulated by the Food and Drug Administration (for example, 16

7 Chapter 1: The Nurse s Role in Medication Reconciliation herbal/natural products) will not be made available to hospital patients. A multidisciplinary team made this decision to prevent adverse drug events, and the director of the pharmacy and the Lourdes Hospital Patient Care Services Policy Figure 1-1: Medication Reconciliation/Physician Initial Medication Form NKA, no known allergies; US, unit secretary; RN, nurse; MD, physician; Pt, patient. 17

8 The Nurse s Role in Medication Safety and Procedure Committee approved the form in October To promote safe decision making, the form included information on allergies and intolerances, height, and weight for all patients. Check boxes indicated where nurses could or would obtain information to complete the form (for example, the patient, their medication list, the family, the outpatient pharmacy). For the form to be used as a physician order form, the licensed independent practitioner with prescription privileges was required to sign and date it. Only then was the hospital pharmacist authorized to prepare the medications for the nurses to administer. Every patient who entered the hospital s portals, for any reason, was to have the medication reconciliation form initiated and completed in 24 hours or less. From the ADE team s perspective, the process sounded very simple and straightforward. But after several tests of change on the pilot unit, the team found it necessary to accommodate the nurses and physicians who were actually going to use this form on an hourly basis. Suggestions for change came fast and furiously from the staff, and each week for many weeks the form was changed. The ADE team continually readjusted, rearranged, reconfigured, reconsidered, redesigned, reformatted, and revised the form to meet the safety needs of the patients and staff members. Creating a Master Medication List As the need for medication reconciliation spread throughout the organization, the team determined that nurses and physicians caring for outpatients (in the primary care network) needed access to a form with a design similar to the medication reconciliation form to easily transfer medication information if those patients were admitted to the hospital. The hospital system charged a small task force of nurses with designing the Master Medication List that primary care physicians and their nurses could use each and every time a patient came for an office visit. This form facilitates the process of looking at the list when new medications are ordered and updating the list to reflect any changes in the medication regimen. 1 And nurses can keep one copy of the list in the patient s chart, record any changes to the patient s record and the patient s copy, and return the list to the patient. (See Figure 1-2 on page 19 for the Master Medication List.) To increase physician compliance, task force members emphasized the benefits to staff nurses and physicians over and over again, which include the following: If the medications are listed, the physician only has to circle or check the same medications and/or add new ones. The physician or nurse does not have to handwrite the very long list of their patient s medications in the chart or at each visit. 18

9 Chapter 1: The Nurse s Role in Medication Reconciliation There will be fewer transcription errors. The nurse and the patient can discuss exactly what medications are still prescribed and what medications are no longer necessary. Figure 1-2: Master Medication List DOB, date of birth; MD, physician. 19

10 The Nurse s Role in Medication Safety If and when the patient ever needs to be hospitalized, the updated medication list from the primary care chart can be used with ease as the medication reconciliation/physician initial medication order form in the hospital chart. The only items required will be the physician signature, date, and time at the bottom of the list, and they can be included in the admission paperwork as medications reconciled and medications ordered, thus saving time and steps and ensuring each patient s medication safety. Creating Medication Cards for Patients While one task force of nurses was formatting the Master Medication List, another small task force of nurses from the primary care network was designing a medication card for patients. The hospital system trialed several tests of change in one outpatient setting. Once again, it was necessary to enlist the help of a multidisciplinary team composed of nurses, physicians, and patients (who were going to be using this medication card). Not only did the medication card list the patient s demographics and the primary care physician s name and telephone number, it contained a section for the patient s brief medical history, a place to denote allergies/intolerances, and a grid in which to list current medications (including herbals and supplements and over-the-counter drugs) that the patient was currently taking. The grid also included a place to list the dose (by simply asking, How much? ), the route, the frequency (by asking, How often? ), and the reason why. (The language used was basic to facilitate teaching and learning.) This grid on the patient s medication card was designed exactly like the columns on the inpatient medication reconciliation form. Soon, all patients who entered the outpatient arena would be given instructions on how to fill out their medication cards. They were also instructed to bring these cards with them each time they had an office visit so that their medication lists could and would be updated, ensuring their safety. (See the medication card for patients in Figure 1-3 on pages ) For those patients who have not received a medication card from the outpatient setting, a blank card is included in the paperwork for all patients who are admitted and discharged from the hospital. Often nurses on these units assist patients or their families with filling out the medication cards. Nurses encourage patients to update their medication cards at discharge. The Lourdes system has found that it only takes a few moments for a nurse to teach a patient about the importance of the right drug, dose, route, and the reason for their medications. At the same time, nurses can give medication-information teaching sheets to patients and their family members. These sheets describe any new medication initiated as well as dosage, administration, side effects, and contraindications. This is not a new 20

11 Chapter 1: The Nurse s Role in Medication Reconciliation Figure 1-3: Medication Card for Patients Continued on next page 21

12 The Nurse s Role in Medication Safety Figure 1-3: Medication Card for Patients (continued) 22

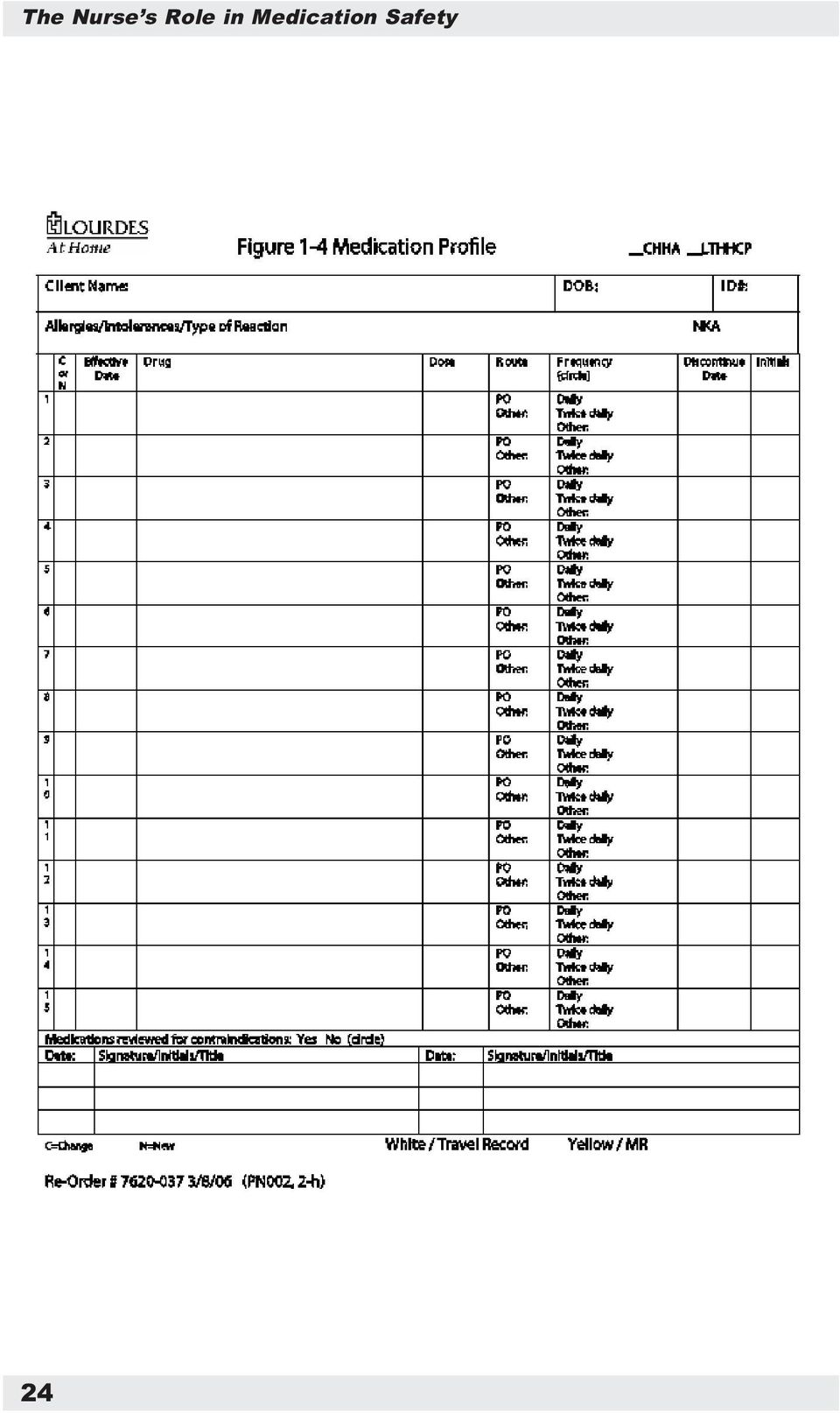
13 Chapter 1: The Nurse s Role in Medication Reconciliation practice because pharmacies across the nation are compelled to provide medicationinformation teaching sheets for any drug that is dispensed. Medication Reconciliation in Home Care and Hospice Another area of concern for appropriate medication reconciliation was within home care and hospice. To ascertain that every patient in the system would have their medications reconciled, Lourdes s home care agency, Lourdes at Home (LAH), and the Lourdes Hospice Program were included in the medication reconciliation process. LAH nurses reconciled their patients medications using a slightly different form (see Figure 1-4 on page 24). Every single time an LAH nurse entered a patient s home, the nurse reconciled medications in the following ways: By discussion with the patient or the family By the discharge paperwork from the hospital With any new prescriptions filled or unfilled From the actual medication bottles in the home By calling the patient s primary care physician or local pharmacy These nurse home care visits created several opportunities for teaching and learning, while at the same time maintaining patient safety as a top priority. Similarly, Lourdes Hospice nurses relied mostly on families for the medication reconciliation, as well as on the primary care physician and local pharmacy. The hospice forms are simpler, but two strong statements at the bottom of the forms alert the patient to disclose any and all medications including herbals, supplements, and vitamins they are currently taking so that any possible interactions could be discussed. (See the hospice care forms in Figures 1-5 on pages and Figure 1-6 on pages ) Implementation Including tasks in the process and documenting observations Now that the medication reconciliation forms were somewhat finalized across the system it was time to implement the process from the point of entry to the point of exit. On the inpatient side of the hospital system, each patient s current medication list is computer generated every night at midnight. The nurses medication administration records (MARs) for their patients are also computer generated every night at midnight. During the day shift, patients (or their family members if patients are unable to comprehend it) receive their current medication list. The patient copy of the list (entitled Postop/Transfer Medication Reconciliation Record ) is similar in 23
.")
14 The Nurse s Role in Medication Safety 24
15 The Nurse s Role in Medication Safety Figure 1-5: Hospice Medication Flow Sheet As-Needed Medications 26

16 Chapter 1: The Nurse s Role in Medication Reconciliation Figure 1-5: Hospice Medication Flow Sheet As-Needed Medications (continued) 27

17 The Nurse s Role in Medication Safety Figure 1-6: Hospice Medication Flow Sheet Routine Medications 28

18 Chapter 1: The Nurse s Role in Medication Reconciliation Figure 1-6: Hospice Medication Flow Sheet Routine Medications (continued) 29

19 The Nurse s Role in Medication Safety assessed and initially treated, the primary nurse in the ED asks for her current list of medications. The patient produces a Lourdes Hospital medication card from her wallet that contains an up-to-date list of her medications, the doses in milligrams, the times she takes them, and why. Her primary care physician s name and telephone number and an emergency contact and telephone number are also on the card, as well as a brief summary of her health history, her allergies, and a list of questions to ask about herself. Because she is alert and oriented and has been initially treated for dyspnea, the patient is able to tell the ED nurse exactly what medication she has already taken today and what medication she still needs. This information is then put on the medication reconciliation form that stays with her chart for the entire hospitalization. When her admitting physician arrives to evaluate the patient, he can use this form (by simply circling the appropriate words) to continue the same medications and/or stop other medications and/or order new medications. By signing the medication reconciliation form at the bottom, the medication reconciliation form becomes a physician initial medication order form and is faxed to the pharmacy. At this time, the pharmacy is authorized to prepare the medications for the nurses to administer. The ED nurse gives a face-to-face report to the receiving nurse on the telemetry unit together with all that he/she knows about this patient, including the medication reconciliation information. By the time the patient arrives on the telemetry unit, her current medications have been ordered and reconciled, the MAR has been printed, and the medications that the patient did not already take today are ready to be administered. If there are any new medications ordered or current medications stopped, the nurse can incorporate this information into the initial plan of care. Example 2: A woman in her forties is brought into the ED by paramedics because she was found wandering a residential neighborhood at 3:00 A.M. She knows who she is and knows that yesterday was her birthday. She says she was celebrating and her blood alcohol content on arrival was 0.29%. After she is assessed and treated, the ED nurse attempts to ask her about her health history. The patient continues to alternate between dozing off and repeating incomprehensible words. The ED physician decides to admit the patient. The ED nurse cannot possibly complete the medication reconciliation form, there are no family members present, and the hospital pharmacy is closed because a 24-hour pharmacy does not exist at Lourdes Hospital yet. Any retail pharmacy would also be closed at this time of night and the hospitalist assigned to this admission does not know the patient at all. When giving the report to the receiving unit, the ED nurse apologizes for the 30

20 Chapter 1: The Nurse s Role in Medication Reconciliation incomplete medication reconciliation form and asks the receiving nurse to make a good faith effort in the morning toward reconciling this patient s medications. The next morning, the patient is more coherent and is questioned about any and all medications that she may have been taking prior to her admission to the hospital. At this time, the patient is able to state to her nurse what she takes but does not know the doses and she cannot remember anything about the day before. She uses a local pharmacy and has given the nurse permission to contact the pharmacy to obtain the medications and doses she takes. The nurse on the medical unit to which the patient is assigned places a call to the pharmacy, and identifies herself and the reason for her call. The local pharmacist asks for the patient s demographics and then gives the nurse the requested information as to her patient s medications and dosages. The nurse now places a call to the patient s physician to request the current medications and appropriate dosages for the patient. (She is taking escitalopram oxalate, metoprolol, ciprofloxacin, a nicotine patch, and ibuprofen.) Her medications are reconciled and she is started back on her same drug regimen except for the over-the-counter ibuprofen. (To prevent any potential gastric reflux or ulcers, the ibuprofen was discontinued and pantoprazole sodium was ordered, as well as folic acid, thiamine, vitamins, and diazepam to move her safely through alcohol withdrawal.) These two examples are at opposite ends of the spectrum when considering medication reconciliation, but, as stated previously, it is the primary goal of keeping patients safe that compels nurses to continue toward completing the medication reconciliation process, regardless of how difficult this is to accomplish, at every portal of the system. Most of the time, medication reconciliation is successful because of the initial steps the nurses take. There has been remarkable success in reducing adverse drug events with the incorporation of medication reconciliation at Lourdes Hospital as evidenced by the evaluation and measurement described below. Evaluation and Measurement Note success or failure across the system and adopt, amend, or abandon By August 2005, the goal of medication reconciliation (to reduce nonreconciled medications to <50%) on admission for all inpatients and, on admission and on discharge for all ED patients and, at each visit in the primary care setting had been met for the past six months. By August 2006, the goal of medication reconciliation (to reduce nonreconciled medications to <6.25%) on admission for all inpatients and all sites (inpatient, ED, ambulatory surgery, primary care) and on transfer and discharge had been met for the past 16 months. As evidenced by the statis- 31

21 The Nurse s Role in Medication Safety tics above, medication reconciliation is a process that is performed, primarily by nurses, with success. The goal for 2007 is to sustain improvement in the percentage of nonreconciled medications on admission to <5%. The above goals have been and will continue to be met in several ways. Nurses and other members of the ADE team complete retrospective and concurrent chart reviews on a regular basis. Staff nurses from each unit are required to review one chart a month. A section of the eight-page chart review pertains to physician order forms and has included questions about medication reconciliation. All the data is collected, compiled, reported, and discussed at weekly ADE team meetings. The continued success of medication reconciliation is incumbent primarily on nurses, then pharmacists and physicians. Its progress is periodically monitored and evaluated. It is also measured by the reduction in ADEs reported each month and compared to ADE rates before and after the process was initiated. Currently, there is ongoing research and investigation across the organization where nurses are involved in administering medications. This is to ensure that medication reconciliation is being conducted and is successful for all patients in all areas. The research has highlighted some unique patient areas such as Youth Services, the Breast Care Center, the Coumadin Clinic, and Cardiac Rehabilitation where advance practice nurses can prescribe and staff nurses administer medications. These areas are not exempt from completing medication reconciliation for their particular patients 100% of the time. If at any step in the process, nurses (or pharmacists or physicians) devise a more efficient or user-friendly way of performing medication reconciliation, they are encouraged to and are welcome to present their findings and suggestions to the ADE team. From its inception, the medication reconciliation form has been revised primarily because of input from the staff nurse. In fact, several times (more than 50 at present) the medication reconciliation form has been amended as a result of suggestions from the nurses using it across the continuum of care. How the Nurse Improves the Medication Reconciliation Process Nurses are essential to creating, improving, and implementing the medication reconciliation process. Their position and skills benefit medication reconciliation in the following ways: Medication reconciliation is an arduous process that takes time to plan, design, and test. It is necessary to promote patient safety and prevent ADEs. It cannot be performed without input and buy-in from nurses. 32
22 Chapter 1: The Nurse s Role in Medication Reconciliation The trusted nurse-patient relationship yields improved outcomes and a plan of care that can be instituted when medication reconciliation and subsequent medication safety prevail. Nurses are usually the first caregivers whom patients see when entering a health care system. Medication reconciliation as well as patient teaching takes place at this time. Nurses are usually the last caregivers whom patients see when exiting a health care system. Medication reconciliation as well as patient teaching takes place at this time. Nurses may use any and all resources to make a good faith effort to ensure that a patient s medications are reconciled appropriately. Their perseverance is necessary at this juncture. Nurses may design and use different forms unique to their departments while staying within the guidelines of medication reconciliation. Their creativity is helpful at this juncture. Nurses perform chart reviews and serve on committees where data is gathered and where suggestions for changes to the medication reconciliation process are welcomed. Looking to the Future The future design includes using the electronic medical record to record the patient s medication history, height, weight, and allergies, with alerts to all members of the health care team if any of this information is unavailable. The pharmacist will receive alerts for potential allergic reactions, drug-drug interactions, and drugfood interactions, as well as alerts based on laboratory results or other patient information. The system will alert caregivers when medications are scheduled to be given and will document medication administration in the electronic medication administration record. These capabilities will also support computerized provider order entry. References 1. Miller L., Mannino C.A.: Taking the Lead in Medication Reconciliation. The Cerner Quarterly 2(2):40 47, The Joint Commission: FAQ s for the 2006 National Patient Safety Goals. commission.org/nr/rdonlyres/7c116d6d-ae82-449e-ba45-1de49d2a0a34/ 0/06_npsg_faq.pdf (accessed Jan. 22, 2006; site now discontinued). 33
UNIVERSITY OF WISCONSIN HOSPITAL AND CLINICS DEPARTMENT OF PHARMACY SCOPE OF PATIENT CARE SERVICES FY 2014 October 1 st, 2014
 UNIVERSITY OF WISCONSIN HOSPITAL AND CLINICS DEPARTMENT OF PHARMACY SCOPE OF PATIENT CARE SERVICES FY 2014 October 1 st, 2014 Department Name: Department of Pharmacy Department Director: Steve Rough, MS,
UNIVERSITY OF WISCONSIN HOSPITAL AND CLINICS DEPARTMENT OF PHARMACY SCOPE OF PATIENT CARE SERVICES FY 2014 October 1 st, 2014 Department Name: Department of Pharmacy Department Director: Steve Rough, MS,
Medicines reconciliation on admission and discharge from hospital policy April 2013. WHSCT medicines reconciliation policy 1
 Medicines reconciliation on admission and discharge from hospital policy April 2013 WHSCT medicines reconciliation policy 1 Policy Title Policy Reference Number Medicines reconciliation on admission and
Medicines reconciliation on admission and discharge from hospital policy April 2013 WHSCT medicines reconciliation policy 1 Policy Title Policy Reference Number Medicines reconciliation on admission and
Health Professions Act BYLAWS SCHEDULE F. PART 2 Hospital Pharmacy Standards of Practice. Table of Contents
 Health Professions Act BYLAWS SCHEDULE F PART 2 Hospital Pharmacy Standards of Practice Table of Contents 1. Application 2. Definitions 3. Drug Distribution 4. Drug Label 5. Returned Drugs 6. Drug Transfer
Health Professions Act BYLAWS SCHEDULE F PART 2 Hospital Pharmacy Standards of Practice Table of Contents 1. Application 2. Definitions 3. Drug Distribution 4. Drug Label 5. Returned Drugs 6. Drug Transfer
Medication error is the most common
 Medication Reconciliation Transfer of medication information across settings keeping it free from error. By Jane H. Barnsteiner, PhD, RN, FAAN Medication error is the most common type of error affecting
Medication Reconciliation Transfer of medication information across settings keeping it free from error. By Jane H. Barnsteiner, PhD, RN, FAAN Medication error is the most common type of error affecting
Health Professions Act BYLAWS SCHEDULE F. PART 3 Residential Care Facilities and Homes Standards of Practice. Table of Contents
 Health Professions Act BYLAWS SCHEDULE F PART 3 Residential Care Facilities and Homes Standards of Practice Table of Contents 1. Application 2. Definitions 3. Supervision of Pharmacy Services in a Facility
Health Professions Act BYLAWS SCHEDULE F PART 3 Residential Care Facilities and Homes Standards of Practice Table of Contents 1. Application 2. Definitions 3. Supervision of Pharmacy Services in a Facility
TABLE OF CONTENTS CHAPTER 9 PATIENT COUNSELING AND PROSPECTIVE DRUG USE REVIEW REGULATIONS
 TABLE OF CONTENTS CHAPTER 9 PATIENT COUNSELING AND PROSPECTIVE DRUG USE REVIEW REGULATIONS Section 1. Authority 9-1 Section 2. Definitions 9-1 Section 3. Patient Profile Records 9-1 Section 4. Prospective
TABLE OF CONTENTS CHAPTER 9 PATIENT COUNSELING AND PROSPECTIVE DRUG USE REVIEW REGULATIONS Section 1. Authority 9-1 Section 2. Definitions 9-1 Section 3. Patient Profile Records 9-1 Section 4. Prospective
Agency # 070.00 REGULATION 9 PHARMACEUTICAL CARE/PATIENT COUNSELING
 Agency # 070.00 REGULATION 9 PHARMACEUTICAL CARE/PATIENT COUNSELING 09-00: PATIENT COUNSELING 09-00-0001--PATIENT INFORMATION, DRUG USE EVALUATION, AND PATIENT COUNSELING The intent of this regulation
Agency # 070.00 REGULATION 9 PHARMACEUTICAL CARE/PATIENT COUNSELING 09-00: PATIENT COUNSELING 09-00-0001--PATIENT INFORMATION, DRUG USE EVALUATION, AND PATIENT COUNSELING The intent of this regulation
Welcome to Your Personal Health Record
 Welcome to Your Personal Health Record What is the Shared Care Plan? The Shared Care Plan is a free, easy-to-use, Personal Health Record that lets you keep track of vital health information in case of
Welcome to Your Personal Health Record What is the Shared Care Plan? The Shared Care Plan is a free, easy-to-use, Personal Health Record that lets you keep track of vital health information in case of
Medication Reconciliation Technician Standard Workflow
 Process Description: Medication Reconciliation is the process of making a good faith attempt to obtain a patients prior to admission medication history, which is eventually reconciled against a patients
Process Description: Medication Reconciliation is the process of making a good faith attempt to obtain a patients prior to admission medication history, which is eventually reconciled against a patients
Measure #130 (NQF 0419): Documentation of Current Medications in the Medical Record National Quality Strategy Domain: Patient Safety
: Documentation of Current Medications in the Medical Record National Quality Strategy Domain: Patient Safety") Measure #130 (NQF 0419): Documentation of Current Medications in the Medical Record National Quality Strategy Domain: Patient Safety 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS, REGISTRY DESCRIPTION:
Measure #130 (NQF 0419): Documentation of Current Medications in the Medical Record National Quality Strategy Domain: Patient Safety 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS, REGISTRY DESCRIPTION:
Correctional Treatment CenterF
 0BCHAPTER 15 F 1BI. POLICY The California Department of Corrections and Rehabilitation (CDCR) shall maintain s (CTC) to house inmate-patients who do not require general acute care level of services but
0BCHAPTER 15 F 1BI. POLICY The California Department of Corrections and Rehabilitation (CDCR) shall maintain s (CTC) to house inmate-patients who do not require general acute care level of services but
Medication Reconciliation Training Packet. Legacy Health System
 Medication Reconciliation Training Packet Legacy Health System 1 Objectives To identify the key elements of the medication reconciliation process To describe the role of the nurse in the medication reconciliation
Medication Reconciliation Training Packet Legacy Health System 1 Objectives To identify the key elements of the medication reconciliation process To describe the role of the nurse in the medication reconciliation
LOUISIANA STATE UNIVERSITY HEALTH SCIENCES CENTER - SHREVEPORT MEDICAL RECORDS CONTENT/DOCUMENTATION
 LOUISIANA STATE UNIVERSITY HEALTH SCIENCES CENTER - SHREVEPORT MEDICAL RECORDS CONTENT/DOCUMENTATION Hospital Policy Manual Purpose: To define the components of the paper and electronic medical record
LOUISIANA STATE UNIVERSITY HEALTH SCIENCES CENTER - SHREVEPORT MEDICAL RECORDS CONTENT/DOCUMENTATION Hospital Policy Manual Purpose: To define the components of the paper and electronic medical record
NEWFOUNDLAND AND LABRADOR PHARMACY BOARD Standards of Pharmacy Practice. Standards for Hospital Pharmacies
 NEWFOUNDLAND AND LABRADOR PHARMACY BOARD Standards of Pharmacy Practice Standards for Hospital Pharmacies Approved by the Newfoundland and Labrador Pharmacy Board January 11, 1998 Updated: June 16, 2007
NEWFOUNDLAND AND LABRADOR PHARMACY BOARD Standards of Pharmacy Practice Standards for Hospital Pharmacies Approved by the Newfoundland and Labrador Pharmacy Board January 11, 1998 Updated: June 16, 2007
HIPAA Notice of Privacy Practices
 HIPAA Notice of Privacy Practices THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. This Notice
HIPAA Notice of Privacy Practices THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. This Notice
Truth or Consequences, Best Medication List Practices to Deliver Best Care. Leaning & Action Network Session
 Truth or Consequences, Best Medication List Practices to Deliver Best Care Leaning & Action Network Session Introduction David Cook (5 minutes) Housekeeping: - In event of a fire? - Restrooms? David R.
Truth or Consequences, Best Medication List Practices to Deliver Best Care Leaning & Action Network Session Introduction David Cook (5 minutes) Housekeeping: - In event of a fire? - Restrooms? David R.
Medication Error. Medication Errors. Transitions in Care: Optimizing Intern Resources
 Transitions in Care: Optimizing Intern Resources DeeDee Hu PharmD, MBA Clinical Specialist Critical Care and Cardiology PGY1 Program Director Memorial Hermann Memorial City Medical Center Medication Error
Transitions in Care: Optimizing Intern Resources DeeDee Hu PharmD, MBA Clinical Specialist Critical Care and Cardiology PGY1 Program Director Memorial Hermann Memorial City Medical Center Medication Error
Clinical Information System Downtime (Cerner PowerChart, FirstNet, SurgiNet)
") Clinical Information System Downtime (Cerner PowerChart, FirstNet, SurgiNet) Preparing for Downtime A. 60 Minutes prior 1. No additional electronic orders are entered. 2. For any new lab orders, begin
Clinical Information System Downtime (Cerner PowerChart, FirstNet, SurgiNet) Preparing for Downtime A. 60 Minutes prior 1. No additional electronic orders are entered. 2. For any new lab orders, begin
B. Clinical Data Management
 B. Clinical Data Management The purpose of the applications of this group is to support the clinical needs of care providers including maintaining accurate medical records. Ideally, a clinical data management
B. Clinical Data Management The purpose of the applications of this group is to support the clinical needs of care providers including maintaining accurate medical records. Ideally, a clinical data management
MARY T. INC. PROGRAM POLICY MANUAL
 MARY T. INC. PROGRAM POLICY MANUAL POLICY Safe Medication Assistance and SECTION: 2-2C TITLE: Administration Policy REVISED BY: Jane Strobel, RN PAGE: 1of 6 APPLIES TO: All Services Operating Under Rule
MARY T. INC. PROGRAM POLICY MANUAL POLICY Safe Medication Assistance and SECTION: 2-2C TITLE: Administration Policy REVISED BY: Jane Strobel, RN PAGE: 1of 6 APPLIES TO: All Services Operating Under Rule
Reducing Medical Errors with an Electronic Medical Records System
 Reducing Medical Errors with an Electronic Medical Records System A recent report by the Institute of Medicine estimated that as many as 98,000 people die in any given year from medical errors in hospitals
Reducing Medical Errors with an Electronic Medical Records System A recent report by the Institute of Medicine estimated that as many as 98,000 people die in any given year from medical errors in hospitals
Plum Borough School District Nursing Services Department
 Information Regarding the Student with an Allergy Student s Name Grade Homeroom Date Physician s Name Physician s Phone # Type of Allergy (Food, Bee, Wasp, Latex, Other: Specify): Type of Reaction: For
Information Regarding the Student with an Allergy Student s Name Grade Homeroom Date Physician s Name Physician s Phone # Type of Allergy (Food, Bee, Wasp, Latex, Other: Specify): Type of Reaction: For
East & South East England Specialist Pharmacy Services Medicines Use and Safety Division Community Health Services Transcribing
 East & outh East England pecialist Pharmacy ervices East of England, London, outh Central & outh East Coast Medicines Use and afety Division Community Health ervices Transcribing Guidance to support the
East & outh East England pecialist Pharmacy ervices East of England, London, outh Central & outh East Coast Medicines Use and afety Division Community Health ervices Transcribing Guidance to support the
Stroke/VTE Quality Measure Build for Meaningful Use Stage 1
 Stroke/VTE Quality Measure Build for Meaningful Use Stage 1 Presented by Susan Haviland, BSN RN Senior Consult, Santa Rosa Consulting Meaningful Use Quality Measures Centers for Medicare and Medicaid Services
Stroke/VTE Quality Measure Build for Meaningful Use Stage 1 Presented by Susan Haviland, BSN RN Senior Consult, Santa Rosa Consulting Meaningful Use Quality Measures Centers for Medicare and Medicaid Services
Medication Reconciliation Process; Reducing Prescribing Errors
 Medication Reconciliation Process; Reducing Prescribing Errors Amjed Abu Alburak, RN, BSN, ACCPC CRN, Nursing Administration Medication Safety Program KAMC- CR, Kingdom of Saudi Arabia abualburaka@ngha.med.sa
Medication Reconciliation Process; Reducing Prescribing Errors Amjed Abu Alburak, RN, BSN, ACCPC CRN, Nursing Administration Medication Safety Program KAMC- CR, Kingdom of Saudi Arabia abualburaka@ngha.med.sa
Custodial Procedures Manual Table of Contents
 Custodial Procedures Manual Table of Contents Page 1. Drug Policies and Procedures 1 A. Procurement of Prescription Drugs 1 i. Prescription drugs may only be accepted from 1 pharmacies and or practitioners.
Custodial Procedures Manual Table of Contents Page 1. Drug Policies and Procedures 1 A. Procurement of Prescription Drugs 1 i. Prescription drugs may only be accepted from 1 pharmacies and or practitioners.
Frequently Asked Questions (FAQs) Treatment Authorization Request (TAR) Restriction on Antipsychotic Medications for the 0-17 Population
 Treatment Authorization Request (TAR) Restriction on Antipsychotic Medications for the 0-17 Population") Frequently Asked Questions (FAQs) Treatment Authorization Request (TAR) Restriction on Antipsychotic Medications for the 0-17 Population Prescriber FAQs Update January 22, 2015 1. What information is needed
Frequently Asked Questions (FAQs) Treatment Authorization Request (TAR) Restriction on Antipsychotic Medications for the 0-17 Population Prescriber FAQs Update January 22, 2015 1. What information is needed
HIM Frequently Asked Questions
 Suspension Process Why am I on suspension? HIM Frequently Asked Questions You have delinquent records records which have not been completed in the time frame outlined in our governance documents and by
Suspension Process Why am I on suspension? HIM Frequently Asked Questions You have delinquent records records which have not been completed in the time frame outlined in our governance documents and by
GUIDELINES ON PREVENTING MEDICATION ERRORS IN PHARMACIES AND LONG-TERM CARE FACILITIES THROUGH REPORTING AND EVALUATION
 GUIDELINES GUIDELINES ON PREVENTING MEDICATION ERRORS IN PHARMACIES AND LONG-TERM CARE FACILITIES THROUGH REPORTING AND EVALUATION Preamble The purpose of this document is to provide guidance for the pharmacist
GUIDELINES GUIDELINES ON PREVENTING MEDICATION ERRORS IN PHARMACIES AND LONG-TERM CARE FACILITIES THROUGH REPORTING AND EVALUATION Preamble The purpose of this document is to provide guidance for the pharmacist
Compliance Tip Sheet CMS FY 2010 TOP TEN HOSPICE SURVEY DEFICIENCIES COMPLIANCE RECOMMENDATIONS CMS TOP TEN HOSPICE SURVEY DEFICIENCIES
 Compliance Tip Sheet National Hospice and Palliative Care Organization www.nhpco.org/regulatory CMS FY 2010 TOP TEN HOSPICE SURVEY DEFICIENCIES COMPLIANCE RECOMMENDATIONS INTRODUCTION The Centers for Medicare
Compliance Tip Sheet National Hospice and Palliative Care Organization www.nhpco.org/regulatory CMS FY 2010 TOP TEN HOSPICE SURVEY DEFICIENCIES COMPLIANCE RECOMMENDATIONS INTRODUCTION The Centers for Medicare
RIH Transitions of Care Collaboration with Coastal Medical To Improve Transitions for Patients Discharged Hospital To Home
 RIH Transitions of Care Collaboration with Coastal Medical To Improve Transitions for Patients Discharged Hospital To Home Sergio Petrillo, PharmD Clinical Pharmacist Specialist, Rhode Island Hospital
RIH Transitions of Care Collaboration with Coastal Medical To Improve Transitions for Patients Discharged Hospital To Home Sergio Petrillo, PharmD Clinical Pharmacist Specialist, Rhode Island Hospital
Revised: X Date: 04/07/14. 1. All medication orders shall be reviewed, signed, or co-signed by a Registered Nurse (RN).
.") Vermont Psychiatric Care Hospital Procedure Revised: X Date: 04/07/14 I. Medication Orders 1. All medication orders shall be reviewed, signed, or co-signed by a Registered Nurse (RN). 2. Medication orders
Vermont Psychiatric Care Hospital Procedure Revised: X Date: 04/07/14 I. Medication Orders 1. All medication orders shall be reviewed, signed, or co-signed by a Registered Nurse (RN). 2. Medication orders
Community Center Readiness Guide Additional Resource #17 Protocol for Physician Assistants and Advanced Practice Nurses
 Community Center Readiness Guide Additional Resource #17 Protocol for Physician Assistants and Advanced Practice Nurses PROTOCOL FOR PHYSICIAN ASSISTANTS AND ADVANCED PRACTICE NURSES 1. POLICY Advanced
Community Center Readiness Guide Additional Resource #17 Protocol for Physician Assistants and Advanced Practice Nurses PROTOCOL FOR PHYSICIAN ASSISTANTS AND ADVANCED PRACTICE NURSES 1. POLICY Advanced
SafetyFirst Alert. Errors in Transcribing and Administering Medications
 SafetyFirst Alert Massachusetts Coalition for the Prevention of Medical Errors January 2001 This issue of Safety First Alert is a publication of the Massachusetts Coalition for the Prevention of Medical
SafetyFirst Alert Massachusetts Coalition for the Prevention of Medical Errors January 2001 This issue of Safety First Alert is a publication of the Massachusetts Coalition for the Prevention of Medical
LEGISLATURE OF THE STATE OF IDAHO Sixty-third Legislature Second Regular Session - 2016 IN THE SENATE SENATE BILL NO. 1322
 LEGISLATURE OF THE STATE OF IDAHO Sixty-third Legislature Second Regular Session - IN THE SENATE SENATE BILL NO. BY HEALTH AND WELFARE COMMITTEE 0 0 AN ACT RELATING TO EPINEPHRINE AUTO-INJECTORS; AMENDING
LEGISLATURE OF THE STATE OF IDAHO Sixty-third Legislature Second Regular Session - IN THE SENATE SENATE BILL NO. BY HEALTH AND WELFARE COMMITTEE 0 0 AN ACT RELATING TO EPINEPHRINE AUTO-INJECTORS; AMENDING
Understanding Alberta s Drug Schedules
 Understanding Alberta s Drug Schedules Preface In May 2002, the provincial drug schedules to the Pharmaceutical Profession Act were amended. In April 2007, the Alberta Regulation 66/2007 to the Pharmacy
Understanding Alberta s Drug Schedules Preface In May 2002, the provincial drug schedules to the Pharmaceutical Profession Act were amended. In April 2007, the Alberta Regulation 66/2007 to the Pharmacy
www.sequelmed.com 800.965.2728 www.sequelmed.com
 Practice Management Document Management Medical Records e-prescribe e-health Patient Portal One Integrated Solution Our practice has been working with Sequel Systems for many years and is extremely satisfied.
Practice Management Document Management Medical Records e-prescribe e-health Patient Portal One Integrated Solution Our practice has been working with Sequel Systems for many years and is extremely satisfied.
National Patient Safety Goals Effective January 1, 2015
 National Patient Safety Goals Goal 1 Nursing are enter ccreditation Program Improve the accuracy of patient and resident identification. NPSG.01.01.01 Use at least two patient or resident identifiers when
National Patient Safety Goals Goal 1 Nursing are enter ccreditation Program Improve the accuracy of patient and resident identification. NPSG.01.01.01 Use at least two patient or resident identifiers when
Intake / Admissions Processes
 Intake / Admissions Processes Now that the elements of providing quality customer service have been reviewed, the intake and admission processes will be covered. Some homecare companies make a distinction
Intake / Admissions Processes Now that the elements of providing quality customer service have been reviewed, the intake and admission processes will be covered. Some homecare companies make a distinction
Standards of Practice for Pharmacists and Pharmacy Technicians
 Standards of Practice for Pharmacists and Pharmacy Technicians Introduction These standards are made under the authority of Section 133 of the Health Professions Act. They are one component of the law
Standards of Practice for Pharmacists and Pharmacy Technicians Introduction These standards are made under the authority of Section 133 of the Health Professions Act. They are one component of the law
TITLE: Processing Provider Orders: Inpatient and Outpatient
 POLICY and PROCEDURE TITLE: Processing Provider Orders: Inpatient and Outpatient Number: 13211 Version: 13211.3 Type: Patient Care Author: Janice Dinner; Provider Order Policy Committee Effective Date:
POLICY and PROCEDURE TITLE: Processing Provider Orders: Inpatient and Outpatient Number: 13211 Version: 13211.3 Type: Patient Care Author: Janice Dinner; Provider Order Policy Committee Effective Date:
HealthCare Partners of Nevada. Heart Failure
 HealthCare Partners of Nevada Heart Failure Disease Management Program 2010 HF DISEASE MANAGEMENT PROGRAM The HealthCare Partners of Nevada (HCPNV) offers a Disease Management program for members with
HealthCare Partners of Nevada Heart Failure Disease Management Program 2010 HF DISEASE MANAGEMENT PROGRAM The HealthCare Partners of Nevada (HCPNV) offers a Disease Management program for members with
PHYSICIAN ORDER POLICY
 PURPOSE: To clarify requirements and assure all physician orders are complete and valid for safe patient care SUPPORTIVE DATA: Medication: Prescribing and Ordering Procedure #790.25 RCW 18.164.011 and
PURPOSE: To clarify requirements and assure all physician orders are complete and valid for safe patient care SUPPORTIVE DATA: Medication: Prescribing and Ordering Procedure #790.25 RCW 18.164.011 and
CCNC Care Management Standardized Plan
 Standardization & Reporting: Why is standardization important? Community Care Networks are responsible for the delivery of targeted care management services that will improve quality of care while containing
Standardization & Reporting: Why is standardization important? Community Care Networks are responsible for the delivery of targeted care management services that will improve quality of care while containing
National Patient Safety Goals Effective January 1, 2015
 National Patient Safety Goals Effective January 1, 2015 Goal 1 Improve the accuracy of resident identification. NPSG.01.01.01 Long Term are ccreditation Program Medicare/Medicaid ertification-based Option
National Patient Safety Goals Effective January 1, 2015 Goal 1 Improve the accuracy of resident identification. NPSG.01.01.01 Long Term are ccreditation Program Medicare/Medicaid ertification-based Option
September 2013 EHR Integration Patient Care Storyboard Page 1 of 5
 EHR Integration in Point of Service Systems: Patient Care Storyboard The Patient Medication Profile The Pharmaceutical Information Network (PIN) is one component of the EHR; it is the central repository
EHR Integration in Point of Service Systems: Patient Care Storyboard The Patient Medication Profile The Pharmaceutical Information Network (PIN) is one component of the EHR; it is the central repository
Script/Notes for PowerPoint Presentation. Medication Use Safety Training for Seniors (MUST for Seniors)
") Script/Notes for PowerPoint Presentation Medication Use Safety Training for Seniors (MUST for Seniors) Instructions: You can use the following script to help you prepare your remarks to your organization
Script/Notes for PowerPoint Presentation Medication Use Safety Training for Seniors (MUST for Seniors) Instructions: You can use the following script to help you prepare your remarks to your organization
*The Medicare Hospice Conditions of Participation (2008) (CoPs) contain the federal regulations that govern all Medicare-certified hospice programs.
 (CoPs) contain the federal regulations that govern all Medicare-certified hospice programs.") Compliance Tip Sheet National Hospice and Palliative Care Organization www.nhpco.org/regulatory CMS TOP TEN HOSPICE SURVEY DEFICIENCIES COMPLIANCE RECOMMENDATIONS INTRODUCTION The Centers for Medicare
Compliance Tip Sheet National Hospice and Palliative Care Organization www.nhpco.org/regulatory CMS TOP TEN HOSPICE SURVEY DEFICIENCIES COMPLIANCE RECOMMENDATIONS INTRODUCTION The Centers for Medicare
Mayo Clinic College of Medicine Pharmacy Services. Rotation Summary
 Mayo Clinic College of Medicine Pharmacy Services Rotation Summary Rotation Title: PGY-2 Pediatric Hematology-Oncology Rotation Length: 3-6 weeks Primary Preceptor Name: Amanda Kuper, PharmD, BPCS, Ron
Mayo Clinic College of Medicine Pharmacy Services Rotation Summary Rotation Title: PGY-2 Pediatric Hematology-Oncology Rotation Length: 3-6 weeks Primary Preceptor Name: Amanda Kuper, PharmD, BPCS, Ron
Reconciling the Differences. Karen Lippett B.Sc.Phm Humber River Regional Hospital Renal Dialysis Unit
 Reconciling the Differences Karen Lippett B.Sc.Phm Humber River Regional Hospital Renal Dialysis Unit Objectives 1. Review the medication discharge counselling process in the renal dialysis program 2.
Reconciling the Differences Karen Lippett B.Sc.Phm Humber River Regional Hospital Renal Dialysis Unit Objectives 1. Review the medication discharge counselling process in the renal dialysis program 2.
Unity Point Health PROBLEM LISTS IN THE ELECTRONIC HEALTH RECORD
 Unity Point Health PROBLEM LISTS IN THE ELECTRONIC HEALTH RECORD Introduction The problem list is a critical part of electronic documentation and serves as a communication tool between all care providers.
Unity Point Health PROBLEM LISTS IN THE ELECTRONIC HEALTH RECORD Introduction The problem list is a critical part of electronic documentation and serves as a communication tool between all care providers.
Administrative Policies and Procedures for MOH hospitals /PHC Centers. TITLE: Organization & Management Of Medication Use APPLIES TO: Hospital-wide
 Administrative Policies and Procedures for MOH hospitals /PHC Centers TITLE: Organization & Management Of Medication Use APPLIES TO: Hospital-wide NO. OF PAGES: ORIGINAL DATE: REVISION DATE : السیاسات
Administrative Policies and Procedures for MOH hospitals /PHC Centers TITLE: Organization & Management Of Medication Use APPLIES TO: Hospital-wide NO. OF PAGES: ORIGINAL DATE: REVISION DATE : السیاسات
Regulatory Compliance Policy No. COMP-RCC 4.03 Title:
 I. SCOPE: Regulatory Compliance Policy No. COMP-RCC 4.03 Page: 1 of 10 This policy applies to (1) Tenet Healthcare Corporation and its wholly-owned subsidiaries and affiliates (each, an Affiliate ); (2)
I. SCOPE: Regulatory Compliance Policy No. COMP-RCC 4.03 Page: 1 of 10 This policy applies to (1) Tenet Healthcare Corporation and its wholly-owned subsidiaries and affiliates (each, an Affiliate ); (2)
WHEREAS updates are required to the Compensation Plan for Pharmacy Services;
 M.O. 23/2014 WHEREAS the Minister of Health is authorized pursuant to section 16 of the Regional Health Authorities Act to provide or arrange for the provision of health services in any area of Alberta
M.O. 23/2014 WHEREAS the Minister of Health is authorized pursuant to section 16 of the Regional Health Authorities Act to provide or arrange for the provision of health services in any area of Alberta
c. determine the factors that will facilitate/limit physician utilization of pharmacists for medication management services.
 Consumer, Physician, and Payer Perspectives on Primary Care Medication Management Services with a Shared Resource Pharmacists Network Marie Smith, PharmD and Michlle Breland, PhD University of Connecticut,
Consumer, Physician, and Payer Perspectives on Primary Care Medication Management Services with a Shared Resource Pharmacists Network Marie Smith, PharmD and Michlle Breland, PhD University of Connecticut,
Mona Osman MD, MPH, MBA
 Mona Osman MD, MPH, MBA Objectives To define an Electronic Medical Record (EMR) To demonstrate the benefits of EMR To introduce the Lebanese Society of Family Medicine- EMR Reality Check The healthcare
Mona Osman MD, MPH, MBA Objectives To define an Electronic Medical Record (EMR) To demonstrate the benefits of EMR To introduce the Lebanese Society of Family Medicine- EMR Reality Check The healthcare
How To Write A Nursing Home Self Assessment Survey On Patient Transitions And Family Caregivers
 How Are We Doing? A Nursing Home Self Assessment Survey on Patient Transitions and Family Caregivers Well-planned and managed transitions are essential for high quality care and patient safety. Transitions
How Are We Doing? A Nursing Home Self Assessment Survey on Patient Transitions and Family Caregivers Well-planned and managed transitions are essential for high quality care and patient safety. Transitions
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES
 Facility Name: Facility ID: Date: Surveyor Name: Resident Name: Resident ID: Initial Admission Date: Interviewable: Yes No Resident Room: Care Area(s): Use Use this protocol for a sampled resident receiving
Facility Name: Facility ID: Date: Surveyor Name: Resident Name: Resident ID: Initial Admission Date: Interviewable: Yes No Resident Room: Care Area(s): Use Use this protocol for a sampled resident receiving
Patient Advocate Checklist For:
 Today s Date Patient Advocate Checklist For: Name of Patient An advocate is not a Health Care Proxy and can not make decisions for the patient. The advocate should know who the Health Care Proxy is and
Today s Date Patient Advocate Checklist For: Name of Patient An advocate is not a Health Care Proxy and can not make decisions for the patient. The advocate should know who the Health Care Proxy is and
Cedars Sinai Medical Center (CSMC) Learning Objectives. Why Medication Reconciliation?
 Learning Objectives. Why Medication Reconciliation?") Management Case Study: Transitions Trifecta Calibrating the Severity of Drug Related Problems, dherence, and Literacy in a High Risk Population Tuesday, December 10, 2013 2:00 p.m. 2:30 p.m. Management
Management Case Study: Transitions Trifecta Calibrating the Severity of Drug Related Problems, dherence, and Literacy in a High Risk Population Tuesday, December 10, 2013 2:00 p.m. 2:30 p.m. Management
Electronic Medication Administration Record (emar) (For Cerner Sites Only)
 (For Cerner Sites Only)") POLICY NO. 1009 Approved: 12/05 Effective: 12/05 Reviewed: 9/10; 5/12 1. Purpose: Electronic Medication Administration Record (emar) (For Cerner Sites Only) To provide direction for the transcription and
POLICY NO. 1009 Approved: 12/05 Effective: 12/05 Reviewed: 9/10; 5/12 1. Purpose: Electronic Medication Administration Record (emar) (For Cerner Sites Only) To provide direction for the transcription and
Prior Authorization, Pharmacy and Health Case Management Information. Prior Authorization. Pharmacy Information. Health Case Management
 Prior Authorization, Pharmacy and Health Case Management Information The purpose of this information sheet is to provide you with details on how Great-West Life will be assessing and managing your claim
Prior Authorization, Pharmacy and Health Case Management Information The purpose of this information sheet is to provide you with details on how Great-West Life will be assessing and managing your claim
Concept Series Paper on Disease Management
 Concept Series Paper on Disease Management Disease management is the concept of reducing health care costs and improving quality of life for individuals with chronic conditions by preventing or minimizing
Concept Series Paper on Disease Management Disease management is the concept of reducing health care costs and improving quality of life for individuals with chronic conditions by preventing or minimizing
Department of Veterans Affairs VHA HANDBOOK 1108.11. Washington, DC 20420 July 1, 2015 CLINICAL PHARMACY SERVICES
 Department of Veterans Affairs VHA HANDBOOK 1108.11 Veterans Health Administration Transmittal Sheet Washington, DC 20420 July 1, 2015 CLINICAL PHARMACY SERVICES 1. REASON FOR ISSUE: This Veterans Health
Department of Veterans Affairs VHA HANDBOOK 1108.11 Veterans Health Administration Transmittal Sheet Washington, DC 20420 July 1, 2015 CLINICAL PHARMACY SERVICES 1. REASON FOR ISSUE: This Veterans Health
Wellness Consultation Policies. HIPAA Notice of Privacy Practices
 Wellness Consultation Policies Cancellation Policy: There is a $50 charge for cancellations of less than 24 hours or failure to show up for a scheduled appointment. Email Policy: Email may be used for
Wellness Consultation Policies Cancellation Policy: There is a $50 charge for cancellations of less than 24 hours or failure to show up for a scheduled appointment. Email Policy: Email may be used for
Addressing forecasted oncologist shortage: A Cancer Education Program for Pharmacy Students (CEPPS)
") Addressing forecasted oncologist shortage: A Cancer Education Program for Pharmacy Students (CEPPS) Dr. Department of Pharmacy Practice State University of New York School of Pharmacy and Pharmaceutical
Addressing forecasted oncologist shortage: A Cancer Education Program for Pharmacy Students (CEPPS) Dr. Department of Pharmacy Practice State University of New York School of Pharmacy and Pharmaceutical
IN-HOME QUALITY IMPROVEMENT MEDICATION MANAGEMENT BE SAFE & TAKE
 IN-HOME QUALITY IMPROVEMENT MEDICATION MANAGEMENT BE SAFE & TAKE NURSE ENRICHMENT PROGRAM 1 Medication Management Be Safe & Take Nurse Enrichment Program Purpose: 1) To provide consistent instruction to
IN-HOME QUALITY IMPROVEMENT MEDICATION MANAGEMENT BE SAFE & TAKE NURSE ENRICHMENT PROGRAM 1 Medication Management Be Safe & Take Nurse Enrichment Program Purpose: 1) To provide consistent instruction to
PHARMACEUTICAL MANAGEMENT PROCEDURES
 PHARMACEUTICAL MANAGEMENT PROCEDURES THE FORMULARY The purpose of Coventry Health Care s formulary is to encourage use of the most cost-effective drugs. The formulary is necessary because the cost of prescription
PHARMACEUTICAL MANAGEMENT PROCEDURES THE FORMULARY The purpose of Coventry Health Care s formulary is to encourage use of the most cost-effective drugs. The formulary is necessary because the cost of prescription
Overview of emar Electronic Medication Administration Record
 Overview of emar Electronic Medication Administration Record March 2006 WHAT IS emar? emar Electronic Medication Administration Record - Replaces the paper MAR MAK Medication Administration Check (Siemens)
Overview of emar Electronic Medication Administration Record March 2006 WHAT IS emar? emar Electronic Medication Administration Record - Replaces the paper MAR MAK Medication Administration Check (Siemens)
Electronic Health Records
 What Do Electronic Health Records Mean for Our Practice? What are Electronic Health Records? Electronic Health Records (EHRs) are computer systems that medical practices use instead of paper charts. All
What Do Electronic Health Records Mean for Our Practice? What are Electronic Health Records? Electronic Health Records (EHRs) are computer systems that medical practices use instead of paper charts. All
Andrew C. Bledsoe, MBA, CHPA, PCMH CCE Executive Director. Northeast KY Regional Health Information Organization. www.nekyrhio.org
 Andrew C. Bledsoe, MBA, CHPA, PCMH CCE Executive Director Northeast KY Regional Health Information Organization www.nekyrhio.org NCQA Program Setup Standards Six Standards Outline Program Elements Six
Andrew C. Bledsoe, MBA, CHPA, PCMH CCE Executive Director Northeast KY Regional Health Information Organization www.nekyrhio.org NCQA Program Setup Standards Six Standards Outline Program Elements Six
Interviewable: Yes No Resident Room: Initial Admission Date: Care Area(s): Use
: Use") Facility Name: Facility ID: Date: Surveyor Name: Resident Name: Resident ID: Initial Admission Date: Care Area(s): Interviewable: Yes No Resident Room: Use Use this protocol for a sampled resident receiving
Facility Name: Facility ID: Date: Surveyor Name: Resident Name: Resident ID: Initial Admission Date: Care Area(s): Interviewable: Yes No Resident Room: Use Use this protocol for a sampled resident receiving
APP PRIVILEGES IN ORTHOPEDICS
 APP PRIVILEGES IN ORTHOPEDICS Education/Training Licensure (Initial and Reappointment) Required Successful completion of a PA or NP program Current Licensure as a PA or RN in the state of CA Current certification
APP PRIVILEGES IN ORTHOPEDICS Education/Training Licensure (Initial and Reappointment) Required Successful completion of a PA or NP program Current Licensure as a PA or RN in the state of CA Current certification
MODULE 11: Developing Care Management Support
 MODULE 11: Developing Care Management Support In this module, we will describe the essential role local care managers play in health care delivery improvement programs and review some of the tools and
MODULE 11: Developing Care Management Support In this module, we will describe the essential role local care managers play in health care delivery improvement programs and review some of the tools and
MEANINGFUL USE. Community Center Readiness Guide Additional Resource #13 Meaningful Use Implementation Tracking Tool (Template) CONTENTS:
 CONTENTS:") Community Center Readiness Guide Additional Resource #13 Meaningful Use Implementation Tracking Tool (Template) MEANINGFUL USE HITECH s goal is not adoption alone but meaningful use of EHRs that is, their
Community Center Readiness Guide Additional Resource #13 Meaningful Use Implementation Tracking Tool (Template) MEANINGFUL USE HITECH s goal is not adoption alone but meaningful use of EHRs that is, their
a) Each facility shall have a medical record system that retrieves information regarding individual residents.
 Each facility shall have a medical record system that retrieves information regarding individual residents.") TITLE 77: PUBLIC HEALTH CHAPTER I: DEPARTMENT OF PUBLIC HEALTH SUBCHAPTER c: LONG-TERM CARE FACILITIES PART 300 SKILLED NURSING AND INTERMEDIATE CARE FACILITIES CODE SECTION 300.1810 RESIDENT RECORD REQUIREMENTS
TITLE 77: PUBLIC HEALTH CHAPTER I: DEPARTMENT OF PUBLIC HEALTH SUBCHAPTER c: LONG-TERM CARE FACILITIES PART 300 SKILLED NURSING AND INTERMEDIATE CARE FACILITIES CODE SECTION 300.1810 RESIDENT RECORD REQUIREMENTS
Meaningful Use. Goals and Principles
 Meaningful Use Goals and Principles 1 HISTORY OF MEANINGFUL USE American Recovery and Reinvestment Act, 2009 Two Programs Medicare Medicaid 3 Stages 2 ULTIMATE GOAL Enhance the quality of patient care
Meaningful Use Goals and Principles 1 HISTORY OF MEANINGFUL USE American Recovery and Reinvestment Act, 2009 Two Programs Medicare Medicaid 3 Stages 2 ULTIMATE GOAL Enhance the quality of patient care
Compensation Plan for Pharmacy Services
 Compensation Plan for Pharmacy Services Attachment A Section 1 - Definitions ABC Pharmacy Agreement means an agreement between ABC and a Community Pharmacy as described in Schedule 2.1 of the Alberta Blue
Compensation Plan for Pharmacy Services Attachment A Section 1 - Definitions ABC Pharmacy Agreement means an agreement between ABC and a Community Pharmacy as described in Schedule 2.1 of the Alberta Blue
105 CMR: DEPARTMENT OF PUBLIC HEALTH 105 CMR 210.000: THE ADMINISTRATION OF PRESCRIPTION MEDICATIONS IN PUBLIC AND PRIVATE SCHOOLS
 105 CMR 210.000: THE ADMINISTRATION OF PRESCRIPTION MEDICATIONS IN PUBLIC AND PRIVATE SCHOOLS Section 210.001: Purpose 210.002: Definitions 210.003: Policies Governing the Administration of Prescription
105 CMR 210.000: THE ADMINISTRATION OF PRESCRIPTION MEDICATIONS IN PUBLIC AND PRIVATE SCHOOLS Section 210.001: Purpose 210.002: Definitions 210.003: Policies Governing the Administration of Prescription
How To Prevent Medication Errors
 The Academy of Managed Care Pharmacy s Concepts in Managed Care Pharmacy Medication Errors Medication errors are among the most common medical errors, harming at least 1.5 million people every year. The
The Academy of Managed Care Pharmacy s Concepts in Managed Care Pharmacy Medication Errors Medication errors are among the most common medical errors, harming at least 1.5 million people every year. The
NH Medicaid Managed Care Supplemental Issue
 Empowering and informing families and professionals caring for children with special health care needs and disabilities from birth to adulthood. NH Medicaid Managed Care Supplemental Issue In 2011 the
Empowering and informing families and professionals caring for children with special health care needs and disabilities from birth to adulthood. NH Medicaid Managed Care Supplemental Issue In 2011 the
Prior Authorization, Pharmacy and Health Case Management Information. Prior Authorization. Pharmacy Information. Health Case Management
 Prior Authorization, Pharmacy and Health Case Management Information The purpose of this information sheet is to provide you with details on how Great-West Life will be assessing and managing your claim
Prior Authorization, Pharmacy and Health Case Management Information The purpose of this information sheet is to provide you with details on how Great-West Life will be assessing and managing your claim
Ch. 109 NURSING SERVICES 28 CHAPTER 109. NURSING SERVICES GENERAL PROVISIONS
 Ch. 109 NURSING SERVICES 28 CHAPTER 109. NURSING SERVICES GENERAL PROVISIONS Sec. 109.1. Principle. 109.2. Director of nursing services. 109.3. Assistants to director of nursing services. 109.4. Professional
Ch. 109 NURSING SERVICES 28 CHAPTER 109. NURSING SERVICES GENERAL PROVISIONS Sec. 109.1. Principle. 109.2. Director of nursing services. 109.3. Assistants to director of nursing services. 109.4. Professional
High Desert Medical Group Connections for Life Program Description
 High Desert Medical Group Connections for Life Program Description POLICY: High Desert Medical Group ("HDMG") promotes patient health and wellbeing by actively coordinating services for members with multiple
High Desert Medical Group Connections for Life Program Description POLICY: High Desert Medical Group ("HDMG") promotes patient health and wellbeing by actively coordinating services for members with multiple
CHAPTER 27 THE SCOPE OF PROFESSIONAL NURSING PRACTICE AND ARNP AND CNM PROTOCOLS
 I. INTRODUCTION CHAPTER 27 THE SCOPE OF PROFESSIONAL NURSING PRACTICE AND ARNP AND CNM PROTOCOLS Advance registered nurse practitioners (ARNPs) and clinical nurse practitioners (CNPs) have their scope
I. INTRODUCTION CHAPTER 27 THE SCOPE OF PROFESSIONAL NURSING PRACTICE AND ARNP AND CNM PROTOCOLS Advance registered nurse practitioners (ARNPs) and clinical nurse practitioners (CNPs) have their scope
Managing Your Medications
 Managing Your Medications Table of Contents Managing Your Medications Handout 1 Personal health goals & medications... 4 Handout 2 Pharmacists can help you... 6 Handout 3 Managing your medications... 7
Managing Your Medications Table of Contents Managing Your Medications Handout 1 Personal health goals & medications... 4 Handout 2 Pharmacists can help you... 6 Handout 3 Managing your medications... 7
Special Topics in Vendor- Specific Systems. Outline. Results Review. Unit 4 EHR Functionality. EHR functionality. Results Review
 Special Topics in Vendor- Specific Systems Unit 4 EHR Functionality EHR functionality Results Review Outline Computerized Provider Order Entry (CPOE) Documentation Billing Messaging 2 Results Review Laboratory
Special Topics in Vendor- Specific Systems Unit 4 EHR Functionality EHR functionality Results Review Outline Computerized Provider Order Entry (CPOE) Documentation Billing Messaging 2 Results Review Laboratory
Medical Records Training Manual for EMR
 Medical Records Training Manual for EMR ENTERPRISE MEDICAL RECORD (EMR) The MEDITECH Enterprise Medical Record (EMR) collects, stores, and displays clinical data such as lab results, transcribed reports,
Medical Records Training Manual for EMR ENTERPRISE MEDICAL RECORD (EMR) The MEDITECH Enterprise Medical Record (EMR) collects, stores, and displays clinical data such as lab results, transcribed reports,
HIMSS Electronic Health Record Definitional Model Version 1.0
 HIMSS Electronic Health Record Definitional Model Version 1.0 Prepared by HIMSS Electronic Health Record Committee Thomas Handler, MD. Research Director, Gartner Rick Holtmeier, President, Berdy Systems
HIMSS Electronic Health Record Definitional Model Version 1.0 Prepared by HIMSS Electronic Health Record Committee Thomas Handler, MD. Research Director, Gartner Rick Holtmeier, President, Berdy Systems
FLORIDA MEDICAL CLINIC, P.A. NOTICE OF PRIVACY PRACTICES
 FLORIDA MEDICAL CLINIC, P.A. NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW
FLORIDA MEDICAL CLINIC, P.A. NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW
Section II When you are finished with this section, you will be able to: Define medication (p 2) Describe how medications work (p 3)
 Describe how medications work (p 3)") Section II When you are finished with this section, you will be able to: Define medication (p 2) Describe how medications work (p 3) List the different medication effects (p5) List the ways that medications
Section II When you are finished with this section, you will be able to: Define medication (p 2) Describe how medications work (p 3) List the different medication effects (p5) List the ways that medications
KENTUCKY ADMINISTRATIVE REGULATIONS TITLE 201. GENERAL GOVERNMENT CABINET CHAPTER 9. BOARD OF MEDICAL LICENSURE
 KENTUCKY ADMINISTRATIVE REGULATIONS TITLE 201. GENERAL GOVERNMENT CABINET CHAPTER 9. BOARD OF MEDICAL LICENSURE 201 KAR 9:260. Professional standards for prescribing and dispensing controlled substances.
KENTUCKY ADMINISTRATIVE REGULATIONS TITLE 201. GENERAL GOVERNMENT CABINET CHAPTER 9. BOARD OF MEDICAL LICENSURE 201 KAR 9:260. Professional standards for prescribing and dispensing controlled substances.
BC PALLIATIVE CARE BENEFITS PRESCRIBER GUIDE
 BC PALLIATIVE CARE BENEFITS PRESCRIBER GUIDE VERSION 2.5 OCTOBER 29, 2015 BC PALLIATIVE CARE BENEFITS PRESCRIBER GUIDE CHANGE RECORD DATE VERSION CHANGE DETAILS Dec 1, 2009 1.0 Original version Jun 21,
BC PALLIATIVE CARE BENEFITS PRESCRIBER GUIDE VERSION 2.5 OCTOBER 29, 2015 BC PALLIATIVE CARE BENEFITS PRESCRIBER GUIDE CHANGE RECORD DATE VERSION CHANGE DETAILS Dec 1, 2009 1.0 Original version Jun 21,
Medication Utilization. Understanding Potential Medication Problems of the Elderly
 Medication Utilization Understanding Potential Medication Problems of the Elderly NICE - National Initiative for the Care of the Elderly WHAT ARE MEDICATION UTILIZATION PROBLEMS AMONG THE ELDERLY? A useful
Medication Utilization Understanding Potential Medication Problems of the Elderly NICE - National Initiative for the Care of the Elderly WHAT ARE MEDICATION UTILIZATION PROBLEMS AMONG THE ELDERLY? A useful
Pharmacy and Nursing Collaborate to Improve the Patient Experience Communication about Medications
 Learning Points 1. Explain why pharmacists are highly qualified and motivated to improve patient education on newly prescribed medications. 2. Illustrate how to create memorable education through design,
Learning Points 1. Explain why pharmacists are highly qualified and motivated to improve patient education on newly prescribed medications. 2. Illustrate how to create memorable education through design,
Cerner PowerChart/FirstNet Home Medication History
 Cerner PowerChart/FirstNet Home Medication History Training Script Training and Education Services, IST Division Table of Contents INTRODUCTION...5 ICONS...6 TERMINOLOGY...6 SIGNING IN...8 OPENING THE
Cerner PowerChart/FirstNet Home Medication History Training Script Training and Education Services, IST Division Table of Contents INTRODUCTION...5 ICONS...6 TERMINOLOGY...6 SIGNING IN...8 OPENING THE
Unstoppable Report Removing a Barrier to Patient Flow by Nursing Process Redesign
 Unstoppable Report Removing a Barrier to Patient Flow by Nursing Process Redesign 17th Annual Society for Health Systems Management Engineering Forum February 12-13, 2005 Dallas, Texas Norwalk Hospital
Unstoppable Report Removing a Barrier to Patient Flow by Nursing Process Redesign 17th Annual Society for Health Systems Management Engineering Forum February 12-13, 2005 Dallas, Texas Norwalk Hospital
Liberty Union High School District Administrative Regulation
 Page 1 of 7 Definitions Authorized health care provider means an individual who is licensed by the State of California to prescribe or order medication, including, but not limited to, a physician or physician
Page 1 of 7 Definitions Authorized health care provider means an individual who is licensed by the State of California to prescribe or order medication, including, but not limited to, a physician or physician