Abdominal Pain. Abdominal Pain
|
|
|
- Winfred Lucas
- 10 years ago
- Views:
Transcription
1 Abdominal Pain Melissa Kerg MD Howard Werman MD Abdominal Pain Can be a challenge to diagnose Personal biases Presumptive diagnosis hastily made Inefficient use of time and tests Delay in making actual diagnosis Mortality doubles with incorrect diagnosis 1

2 Introduction 10% of all undifferentiated patients presenting to ED have abdominal pain as a major complaint missed appendicitis and missed abdominal aortic aneurysm are among the leading causes of malpractice actions Abdominal Pain Pain Subjective No objective measures of pain Vital signs without sensitivity or specificity Pain Scales Ask the patient Useful to tract progress of treatment 2

3 Treat the Pain Goal is pain control not pain relief, there is a difference! Patients are very receptive to being told that we want to lessen the pain and make it tolerable but that its not realistic to remove it completely. Abdominal Pain It can be anything from the nipples to the pelvis Abdominal pain may not be associated with disease processes in the abdomen Abdominal pain may be associated with disease processes not in the abdomen 3

4 Abdominal Pain At least 5-10% of ED visits Up to 50% remain undiagnosed at discharge 5-10% of these have significant disease Small % of admitted patients are misdiagnosed Delays treatment Added morbidity and mortality Goals to identify any immediate lifethreatening causes of abdominal pain 15-30% of patients require immediate surgery to make an educated guess as to underlying medical condition most common dx: nonspecific abdominal pain (40-60% patients) 4

5 General Approach Rule out surgical pathology Look for non-surgical causes Referred pain Systemic illness Gut feelings are important and develop over a career Causes of Abdominal Pain within the Chest Angina/MI Pleuritic irritation Great vessels Aortic dissection Aortic aneurysm 5

6 Causes of Abdominal Pain Abdomen/Pelvic Organs Stomach Gastritis, PUD, gastroenteritis Intestines Appendicitis, SBO, diverticulitis, incarcerated hernia, ischemic gut, IBD Pancreas Pancreatitis, pseudocyst Liver Acute hepatitis, biliary tract disease Vessels AAA, Renal/splenic aneurysm Spleen: Splenic rupture Ureters Colic, stones, UTI Uterus PID, fibroids Ovaries and fallopian tubes (ruptured) ectopic, ovarian cyst, Mittelschmerz, torsion Prostate Prostatitis Testicles and associated structures Torsion, hydrocele, Retroperitoneal Kidneys Pyelonephritis, infarction Great Vessels AAA Muscles (psoas) 6

7 Miscellaneous Abdominal Wall Shingles Hernias Spontaneous Bacterial Peritonitis Acute Intermitent Porphyria Strep Throat (think pediatrics) Diabetes (DKA) Acute narrow angle glaucoma Black Widow Spider Bite History Many symptoms are neither sensitive or specific Few disease processes in abdomen have pathognomonic historical features The typical appendicitis occurs in only 33% of cases 7

8 But with that being said. Inadequate history most common feature of leading to a misdiagnosis History In assessing the patient with abdominal pain, a careful history will lead to a reasonable diagnosis in more than 80% of cases 8

9 History Suggestive of a surgical cause?? Sudden onset Lasting 1-2 days Subsequent peritoneal signs Anorexia History location: major factor in developing a differential diagnosis character radiation onset/chronology aggrevating/alleviating factors associated symptoms: anorexia, nausea, vomiting, bowel changes, urinary sx, vaginal sx 9

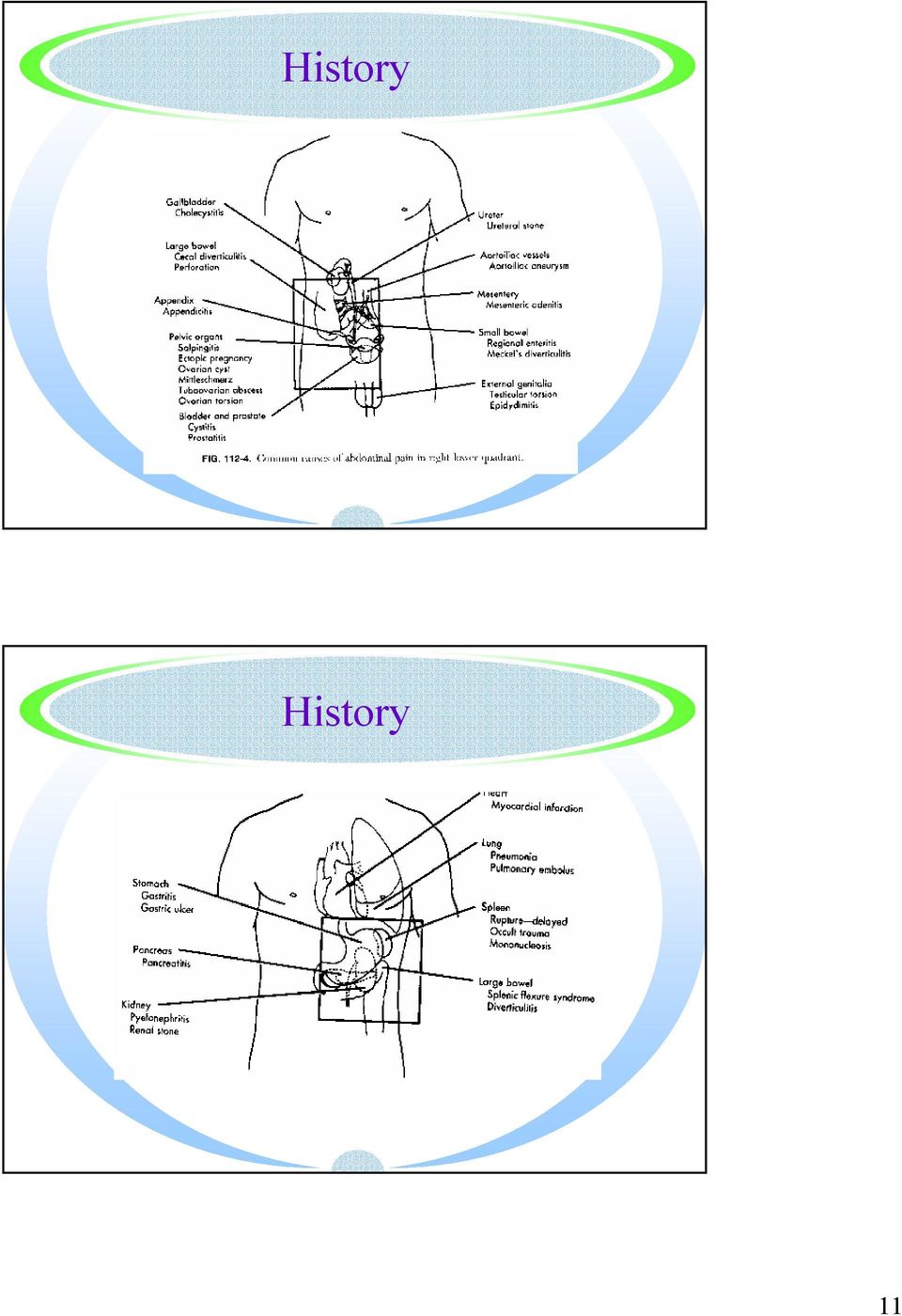
10 History Location of the pain major factor in developing a differential diagnosis History 10

11 History History 11
12 History History O onset P palliation/provocation Q quality R radiation S severity T time 12

13 How Fast Did It Start Sudden onset Perforated ulcer, mesenteric infarction, ruptured AAA, ruptured ectopic pregnancy, ovarian torsion, ruptured ovarian cyst, PE, AMI, testicular torsion Rapid onset (minutes to hours to max) Strangulated hernia, volvulus, intussuception, acute pancreatitis, biliary colic, diverticulitis, ureteral colic How Fast Did It Start Gradual Onset Appendicitis, chronic pancreatitis, PUD, inflammatory bowel diseases, mesenteric adenititis, uti, urinary retention, salpingitis, prostatitis 13

14 History Where did it start? Migratory? Where is it at? What makes it worse or better? Movement, bumps, cough Eating How soon after Position Associated symptoms History PMH Have you ever had this before?? SH Alcohol Tobacco Recreational drugs 14

15 Abdominal Pain There are 2 types of abdominal pain Abdominal Pain Visceral Foregut, midgut, hindgut Autonomic nerves Innervates involuntary muscles, heart and glands Poorly localized Achy/colicky Intermittent Felt in the abdominal wall in the area of embryonic origin of the pain Somatic Typical pain and temperature fibers that innervate the skin Irritation of the parietal peritoneum or mesenteric root Intense and well localized Sharp Felt directly over area of inflammation 15

16 Abdominal Pain A 20 yo female OSU student presents with sharp RLQ abdominal pain. The patient reports that the pain began approximately 6 hours previously as a dull periumbilical pain which suddenly became localized 30 minutes ago. Can you explain? Abdominal Pain Referred pain: pain felt at a site distant from the involved abdominal organ due to a shared cutaneous sensory nerve 16

17 Abdominal Pain Vital Signs Vital signs Orthostatics---when would they not be useful? Fever When is it unreliable? Heart Rate Intra-peritoneal blood may be associated with a relative bradycardia (ectopics) Medications Respiratory Rate Vital signs do not correlate well with patients level of pain 17
 Medications Respiratory Rate Vital signs do not")
18 Physical Examination General Appearance May the most useful HEENT Cardiac Pulmonary Abdominal Rectal What will cause black, but heme negative stools? GU Check for hernias, especially in the pediatric population Physical Examination Observation What do I see? Look as you enter. Level of comfort Position Still vs active Diaphoresis Breathing pattern Distention Icterus 18

19 Physical Examination Auscultation-prior to palpation Bowel sounds Poor predictor of peritonitis People with peritonitis do have bowel sounds!! Listen for minutes-not practical in the ER rushes Bruits Physical Examination Palpation Masses, organomegaly If you don t think to check for it you will not find it Tenderness Abdominal pain with coughing or heal strike more sensitive than palpation or Rovsing s Guarding Voluntary Involuntary Unilateral always involuntary 25% of patients with rebound tenderness do not have surgical pathology 19

20 Physical Examination Hernia Ventral, inguinal, femoral, umbilical Rectal Pelvic Carnett s Test Straight leg raise or have patient lift head and tightened abdominal muscles and palpate If the pain increases - abdominal wall Rectal Examination Only useful to check guaiac or for local phenomena (perirectal abscess) Will not/can not help with the diagnosis of appendicitis/diverticulitis 20
 Will not/can not help with the diagnosis of")
21 Signs Carnett s Murphy s 50% specific (less in elderly) Presence or absence should not preclude diagnosis Ultrasonic (radiographic) murphy s sign Psoas Not specific but sensitive Obturators and Rovsing s Not predictive of anything good or bad What are we trying to diagnosis? Bad stuff!! Ruptured viscus AAA Ischemic bowel Appendicitis Strangulated hernia Ectopic pregnancy Need to go to OR! Gallbladder disease Pancreatitis Bowel obstruction PID Torsions 21
22 The Rest Could be the early presentation of more serious disease Usually nonspecific self limiting diseases Follow up is going to be important Diagnostic Approach Prior to ordering any tests you should have a reasonably short differential to act on In a significant minority of patients with abdominal pain, no tests are needed other than a u/a (and pregnancy test in females) 22
23 The Tests What is needed? We over-utilize every test we can CBC, AAS, Amylase, LFT s Pregnancy Tests may be under-utilized But. Always consider an ECG on patients with upper abdominal pain or nonspecific symptoms in their coronary years Consider a Chest x-ray on young children Consider glucose testing (DKA) 23
24 Blood WBC Not sensitive, not specific, not predictive Can be misleading Amylase Not specific, > 3 times upper level of normal Lipase More specific and sensitive Rises as quickly as the amylase but stays elevated 2x longer Blood LFT s Abnormal in only 50% of acute cholecytitis Just a ALT and urine bilirubin to screen for hepatitis Full battery if patient icteric Chem 7 Why??? Only needed for protracted vomiting or dehydration. BUN/Creatinine is needed prior to IV contrast Lactate-late finding Type and screen vs type and cross 24
25 Urinalysis Up to 33% of patients with appendicitis have blood or WBC s in the urine 50% with ruptured appy have wbc s 33-67% of AAA have blood in their urine Urine pregnancy Radiology AAS No role in undifferentiated abd pain Obstruction, perforation, or foreign body The patient needs to be upright for 10 minutes to increase sensitivity 25
26 26
27 Radiology Ultrasound Not useful in undifferentiated abd pain Wonderful for directed exams Screening exam for most diagnoses by EP Sensitive for AAA but not for dissection 27
28 Radiology CT scan Know what you are looking for 28
29 Special Considerations Elderly Higher prevalence of disease Up to 40% require surgery Majority have co-morbid illnesses Longer delay to presentations (2X) Less likely to have a fever Higher morbidity and mortality Higher atypical cholecystitis incidence Special Considerations Steroids Blunt inflammatory response No peritonitis possible Children Transfer to a higher level of care if you are not comfortable with children, especially the infants Intussusception Typical: male, 5-10 months old, involves ileocecal valve Colicy pain, bloody stool or mucus within several hours 29
30 The Most Common Causes of Children Presenting with Acute Abdominal Pain URI/OM 18.6% Pharyngitis 16.6% Viral Syndrome 16% Abdominal Pain? Etiology 15.6% Gastroenteritis 10.9% Acute Febrile Illness 7.8% Bronchitis/Asthma 2.6% Pneumonia 2.3% Constipation 2.0% UTI 1.6% Appendicitis 0.9% Gastroenteritis Vomiting (Gastro) and diarrhea (enteritis) Frequently used as diagnosis Appendicitis malpractice issue 30
31 It s not simple Frustrating to patient, family, staff and you at times Don t forget repeat exams If ever in doubt, obtain second opinion CLEAR discharge instructions Problem could not be identified Repeat evaluation in 8-12 hours Precautions Discharge Instructions write all discharge instructions in language understandable to the patient avoid medical abbreviations carefully describe any therapies prescribed identify clear follow-up for each patient list the signs and symptoms for which the patient should immediately return for evaluation 31
32 Cases 35 y/o female with upper abdominal pain Vitals: Temp 97.5, BP 122/70, HR 92, RR 18 Hx: Pain, some nausea, no vomiting. Radiates to back PHx: S/P cesarean 6 weeks ago, known gallstones PE: RUQ tenderness, soft elsewhere Test? Labs? Medications? Continued WBC 14.5, LFTs normal Ultrasound shows: Gallstones, gallbladder wall is not thick, no pericholic edema. Common bile duct is 1.5cm diameter Disposition of patient? 32
33 Case 2 79 y/o female from ECF with Abdominal pain Vitals: Temp 99.4, BP 110/66, HR 60, RR 20 Hx: Little ostomy output today, urinated once today, feels bloated PHx: Colon Ca 1999 s/p partial colectomy, SBO, UTI, Mild dementia, Renal insufficiency, HTN PE: Diffuse tenderness, worse in the RLQ, mild distention. Rectal: no stool. Thin liquid in ostomy bag Case 2 Labs? X-rays? Medications? Differential diagnosis? 33
34 Case 2 WBC 19.9 BUN 43, Creatinine 2.7 (baseline 1.6) AAS: Mildly dilated small bowel, possible ileus vs. PSBO What is the next step? Case 2 CT without IV contrast: Diverticulitis of the right colon Disposition? 34
35 Case 3 82 y/o male with left side pain Vitals: Temp 98.5, BP 188/110, HR 105, RR 22 Hx: Intermittent sharp pain, hurts to the back, no pain now PHx: Mass in the abdomen, told to keep a watch on it (this was 5 years ago), kidney stone >40ys ago, HTN, CAD PE: RRR, CTA, Abd soft, NT, pulsatile mass midline, pulses equal Case 3 Differential Diagnosis? Labs? Medications? X-rays? 35
36 Case 3 WBC nl, Hgb 10.8 PT/PTT nl UA: 1+ blood BUN and Creatinine of 30 and 3.0 Diagnostic dilemma? Disposition? Case 3 Follow up: Pt was admitted with BP control. Surgical repair of 7cm AAA performed, however pt died of post-op complications. 36
37 Case 4 13 y/o girl arrives 6:30Am with RLQ pain Mom talks 99% fo the time Vitals: All normal Hx: Similar pains in the past, never lasting more than 1 hour at a time. This time non-stop since 8PM. Sharp pain, sudden onset. Now has N/V PHs: Menarche 11 y/o, never regular; never had a pelvic before. Soc: Never sexually active, Started OCPs 4 days ago by PMD to help regulate her cycle and stop the pains. PE: Flat abd, slender, keeps knees and hips flexed. Severely tender in RLQ and suprapubic areas (pelvic deferred until pain meds) Case 4 Differential Diagnosis? Labs? Medications? X-rays? 37
38 Case 4 After pain meds and antiemetics pelvic reveals pain and fullness of the right adnexa Pregnancy test is negative, WBC 17 Differential diagnosis further narrowed? Case 4 Ultrasound: right ovarian torsion Pt went to surgery and the ovary was saved Pt had numerous cysts 38
39 Case 5 44 y/o male complains of abd pain Vitals: Temp 99.2, BP 90/66, HR 120, RR 28 Hx: Sharp, constant pain epigastic area, some N/V PHx: Similar pain in the past, never this intense, told of elevated BR in the past Soc: Drinks significant ETOH whenever possible, homeless PE: Dry mouth, tachy, CTA, scaphoid abdomen, tender in the epigastric area Case 5 Differential diagnosis? Labs? Meds? X-rays? 39
40 Case 5 Rectal: little stool, heme positive AAS: no free air WBC 14, Hgb 9 Lipase 120 LFTs: AST and Alk Phos are elevated Why are these elevated? NG: positive for dark blood.>200cc Management? Summary/Conclusions abdominal pain is a common presenting complaint goal is to identify immediately lifethreatening (surgical) problems and make an educated guess as to other causes identify the toxic patient the history is most important is establishing the diagnosis give clear discharge instructions 40
The Acute Abdomen. Dr. Ed Snyder Dr. Melanie Walker Huntington Memorial Hospital
 The Acute Abdomen Dr. Ed Snyder Dr. Melanie Walker Huntington Memorial Hospital Causes of the Acute Abdomen Hemorrhage in the GI tract Blood vessel GU tract Perforation of the GI tract Ulcer Infection
The Acute Abdomen Dr. Ed Snyder Dr. Melanie Walker Huntington Memorial Hospital Causes of the Acute Abdomen Hemorrhage in the GI tract Blood vessel GU tract Perforation of the GI tract Ulcer Infection
ABDOMINAL PAIN. 2. Name the most common abdominal emergencies for each of the major anatomic areas of the abdomen
 ABDOMINAL PAIN Objectives: 1. Distinguish between somatic and referred pain 2. Name the most common abdominal emergencies for each of the major anatomic areas of the abdomen 3. Understand age-related differences
ABDOMINAL PAIN Objectives: 1. Distinguish between somatic and referred pain 2. Name the most common abdominal emergencies for each of the major anatomic areas of the abdomen 3. Understand age-related differences
Abdominal Pain. Charles Henley, DO, MPH Department of Family Medicine. OSU College of Osteopathic Medicine (Revised 9/2002)
") Abdominal Pain Charles Henley, DO, MPH Department of Family Medicine OSU College of Osteopathic Medicine (Revised 9/2002) Common Causes of Abdominal Pain Infants - colic, gastroenteritis, constipation,
Abdominal Pain Charles Henley, DO, MPH Department of Family Medicine OSU College of Osteopathic Medicine (Revised 9/2002) Common Causes of Abdominal Pain Infants - colic, gastroenteritis, constipation,
Acute Abdominal Pain: Other causes
 Acute Abdominal Pain: Other causes Vishal Gupta, MCh Associate Professor Deptt Surg. Gastroenterology KGMU Definition Acute abdominal pain: Presentation of previously undiagnosed abdominal pain Lasting
Acute Abdominal Pain: Other causes Vishal Gupta, MCh Associate Professor Deptt Surg. Gastroenterology KGMU Definition Acute abdominal pain: Presentation of previously undiagnosed abdominal pain Lasting
Introduction. Physiology of the Abdomen. Anatomy & Physiology. Abdominal Pain Introduction (2 of 2) Gastrointestional and Urologic Emergencies
 Gastrointestional and Urologic Emergencies") Gastrointestional and Urologic Emergencies Introduction Abdominal pain is a common complaint. Cause of abdominal pain is often difficult to determine. As an EMT: You do not need to determine exact cause.
Gastrointestional and Urologic Emergencies Introduction Abdominal pain is a common complaint. Cause of abdominal pain is often difficult to determine. As an EMT: You do not need to determine exact cause.
Constipation in Adults. Abdominal Pain, Acute
 1 Constipation in Adults Abdominal Pain, Acute Abdominal pain is common and often inconsequential. Acute and severe abdominal pain, however, is almost always a symptom of intraabdominal disease. It may
1 Constipation in Adults Abdominal Pain, Acute Abdominal pain is common and often inconsequential. Acute and severe abdominal pain, however, is almost always a symptom of intraabdominal disease. It may
Steven B. Goldin, MD, PhD University of South Florida Dimitrios Stefanidis, MD, PhD
 RUQ Abdominal Pain Steven B. Goldin, MD, PhD University of South Florida Dimitrios Stefanidis, MD, PhD Mrs. Stone 41 year-old woman in the ER presenting with 12 hours duration of progressively worsening
RUQ Abdominal Pain Steven B. Goldin, MD, PhD University of South Florida Dimitrios Stefanidis, MD, PhD Mrs. Stone 41 year-old woman in the ER presenting with 12 hours duration of progressively worsening
Guide to Abdominal or Gastroenterological Surgery Claims
 What are the steps towards abdominal surgery? Investigation and Diagnosis It is very important that all necessary tests are undertaken to investigate the patient s symptoms appropriately and an accurate
What are the steps towards abdominal surgery? Investigation and Diagnosis It is very important that all necessary tests are undertaken to investigate the patient s symptoms appropriately and an accurate
Differential diagnosis of abdominal pain. Lakatos Péter László
 Differential diagnosis of abdominal pain Lakatos Péter László Precise anamnesis Physical examination are prognosticated to the cause of the pain Anamnesis Sudden pain Perforation Mesenteric infarction
Differential diagnosis of abdominal pain Lakatos Péter László Precise anamnesis Physical examination are prognosticated to the cause of the pain Anamnesis Sudden pain Perforation Mesenteric infarction
Appendicitis National Digestive Diseases Information Clearinghouse
 Appendicitis National Digestive Diseases Information Clearinghouse National Institute of Diabetes and Digestive and Kidney Diseases NATIONAL INSTITUTES OF HEALTH The appendix is a small, tube-like structure
Appendicitis National Digestive Diseases Information Clearinghouse National Institute of Diabetes and Digestive and Kidney Diseases NATIONAL INSTITUTES OF HEALTH The appendix is a small, tube-like structure
Laparoscopic Repair of Hernias. A simple guide to help answer your questions
 Laparoscopic Repair of Hernias A simple guide to help answer your questions What is a hernia? A hernia is defined as a hole or defect in the abdominal (belly) wall. A hernia can either be congenital (a
Laparoscopic Repair of Hernias A simple guide to help answer your questions What is a hernia? A hernia is defined as a hole or defect in the abdominal (belly) wall. A hernia can either be congenital (a
Diseases of peritoneum Lect. Al Qassim University, Faculty of Medicine Phase II Year III, CMD 332 Pathology Department 31-32
 Diseases of peritoneum Lect Al Qassim University, Faculty of Medicine Phase II Year III, CMD 332 Pathology Department 31-32 Describe the etiology, pathogenesis and types of peritonitis Define ascites and
Diseases of peritoneum Lect Al Qassim University, Faculty of Medicine Phase II Year III, CMD 332 Pathology Department 31-32 Describe the etiology, pathogenesis and types of peritonitis Define ascites and
Advanced Practice Provider Academy
 (+)Dean T. Harrison, MPAS,PA C,DFAAPA Director of Mid Level Practitioners; Assistant Medical Director Clinical Evaluation Unit, Division of Emergency Medicine, Department of Surgery, Duke University Medical
(+)Dean T. Harrison, MPAS,PA C,DFAAPA Director of Mid Level Practitioners; Assistant Medical Director Clinical Evaluation Unit, Division of Emergency Medicine, Department of Surgery, Duke University Medical
Acute abdominal conditions Key Points
 7 Acute abdominal conditions Key Points 7.1 ASSESSMENT AND DIAGNOSIS Referred abdominal pain Fore gut pain (stomach, duodenum, gall bladder) is referred to the upper abdomen Mid gut pain (small intestine,
7 Acute abdominal conditions Key Points 7.1 ASSESSMENT AND DIAGNOSIS Referred abdominal pain Fore gut pain (stomach, duodenum, gall bladder) is referred to the upper abdomen Mid gut pain (small intestine,
Emergencies in Post- Bariatric Surgery Patients
 Emergencies in Post- Patients Disclosures Dr. Birnbaumer has no financial disclosures Diane M. Birnbaumer, M.D., FACEP Professor of Medicine University of California, Los Angeles Senior Clinical Educator
Emergencies in Post- Patients Disclosures Dr. Birnbaumer has no financial disclosures Diane M. Birnbaumer, M.D., FACEP Professor of Medicine University of California, Los Angeles Senior Clinical Educator
Bile Duct Diseases and Problems
 Bile Duct Diseases and Problems Introduction A bile duct is a tube that carries bile between the liver and gallbladder and the intestine. Bile is a substance made by the liver that helps with digestion.
Bile Duct Diseases and Problems Introduction A bile duct is a tube that carries bile between the liver and gallbladder and the intestine. Bile is a substance made by the liver that helps with digestion.
X-Plain Inguinal Hernia Repair Reference Summary
 X-Plain Inguinal Hernia Repair Reference Summary Introduction Hernias are common conditions that affect men and women of all ages. Your doctor may recommend a hernia operation. The decision whether or
X-Plain Inguinal Hernia Repair Reference Summary Introduction Hernias are common conditions that affect men and women of all ages. Your doctor may recommend a hernia operation. The decision whether or
Abdominal Pain. Learning Objectives:
 Abdominal Pain Learning Objectives: Knowledge At the end of the subinternship, the subinterns should be able to: Describe the common causes of abdominal pain in hospitalized patient including o Intestinal
Abdominal Pain Learning Objectives: Knowledge At the end of the subinternship, the subinterns should be able to: Describe the common causes of abdominal pain in hospitalized patient including o Intestinal
Laparoscopic Colectomy. What do I need to know about my laparoscopic colorectal surgery?
 Laparoscopic Colectomy What do I need to know about my laparoscopic colorectal surgery? Traditionally, colon & rectal surgery requires a large, abdominal and/or pelvic incision, which often requires a
Laparoscopic Colectomy What do I need to know about my laparoscopic colorectal surgery? Traditionally, colon & rectal surgery requires a large, abdominal and/or pelvic incision, which often requires a
Preoperative Laboratory and Diagnostic Studies
 Preoperative Laboratory and Diagnostic Studies Preoperative Labratorey and Diagnostic Studies The concept of standardized testing in all presurgical patients regardless of age or medical condition is no
Preoperative Laboratory and Diagnostic Studies Preoperative Labratorey and Diagnostic Studies The concept of standardized testing in all presurgical patients regardless of age or medical condition is no
Evaluation of Acute Abdominal Pain in Adults
 Evaluation of Acute Abdominal Pain in Adults Sarah L. Cartwright, MD, and Mark P. Knudson, MD, MSPH Wake Forest University School of Medicine, Winston-Salem, North Carolina Acute abdominal pain can represent
Evaluation of Acute Abdominal Pain in Adults Sarah L. Cartwright, MD, and Mark P. Knudson, MD, MSPH Wake Forest University School of Medicine, Winston-Salem, North Carolina Acute abdominal pain can represent
6/3/2011. High Prevalence and Incidence. Low back pain is 5 th most common reason for all physician office visits in the U.S.
 High Prevalence and Incidence Prevalence 85% of Americans will experience low back pain at some time in their life. Incidence 5% annual Timothy C. Shen, M.D. Physical Medicine and Rehabilitation Sub-specialty
High Prevalence and Incidence Prevalence 85% of Americans will experience low back pain at some time in their life. Incidence 5% annual Timothy C. Shen, M.D. Physical Medicine and Rehabilitation Sub-specialty
Clinical Anatomy of the Biliary Apparatus: Relations & Variations
 Clinical Anatomy of the Biliary Apparatus: Relations & Variations Handout download: http://www.oucom.ohiou.edu/dbms-witmer/gs-rpac.htm 24 January 2012 Lawrence M. Witmer, PhD Professor of Anatomy Department
Clinical Anatomy of the Biliary Apparatus: Relations & Variations Handout download: http://www.oucom.ohiou.edu/dbms-witmer/gs-rpac.htm 24 January 2012 Lawrence M. Witmer, PhD Professor of Anatomy Department
Marginal Ulcers. Marginal Ulcers. Gastric Remnant Ulcers. Double Balloon Enteroscopy. Marginal Ulcer. Gastrojejunal Stricture.
 Upper Abdominal Pain in the Bariatric Surgery Patient Martin L. Freeman, M.D., FASGE,FACG Professor of Medicine Director, Pancreaticobiliary Endoscopy Fellowship Interim Director, Division of GI, Hepatology
Upper Abdominal Pain in the Bariatric Surgery Patient Martin L. Freeman, M.D., FASGE,FACG Professor of Medicine Director, Pancreaticobiliary Endoscopy Fellowship Interim Director, Division of GI, Hepatology
Pediatric Upper GI Series New Patient
 Pediatric Upper GI Series New Patient Upper GI Series Thought to be malrotation, no evidence of midgut volvulus Needed to repeat UGI Series WHY? Repeat UGI Series Repeat UGI Series Repeat UGI Series No
Pediatric Upper GI Series New Patient Upper GI Series Thought to be malrotation, no evidence of midgut volvulus Needed to repeat UGI Series WHY? Repeat UGI Series Repeat UGI Series Repeat UGI Series No
Abdominal Pain in Adults
 1 Abdominal Pain in Adults Abdominal pain is the most common complaint seen in emergency departments in the United States and one of the 10 most common complaints in family medicine outpatient settings.
1 Abdominal Pain in Adults Abdominal pain is the most common complaint seen in emergency departments in the United States and one of the 10 most common complaints in family medicine outpatient settings.
PATIENT CONSENT TO PROCEDURE - ROUX-EN-Y GASTRIC BYPASS
 As a patient you must be adequately informed about your condition and the recommended surgical procedure. Please read this document carefully and ask about anything you do not understand. Please initial
As a patient you must be adequately informed about your condition and the recommended surgical procedure. Please read this document carefully and ask about anything you do not understand. Please initial
Understanding. Pancreatic Cancer
 Understanding Pancreatic Cancer Understanding Pancreatic Cancer The Pancreas The pancreas is an organ that is about 6 inches long. It s located deep in your belly between your stomach and backbone. Your
Understanding Pancreatic Cancer Understanding Pancreatic Cancer The Pancreas The pancreas is an organ that is about 6 inches long. It s located deep in your belly between your stomach and backbone. Your
Abdominal Wall Pain. What is Abdominal Wall Pain?
 Abdominal Wall Pain What is Abdominal Wall Pain? Abdominal Wall Pain is a syndrome (an experience) of abdominal pain that can occur at any time of life and is not unique to children. It is diagnosed by
Abdominal Wall Pain What is Abdominal Wall Pain? Abdominal Wall Pain is a syndrome (an experience) of abdominal pain that can occur at any time of life and is not unique to children. It is diagnosed by
Streptococcal Infections
 Streptococcal Infections Introduction Streptococcal, or strep, infections cause a variety of health problems. These infections can cause a mild skin infection or sore throat. But they can also cause severe,
Streptococcal Infections Introduction Streptococcal, or strep, infections cause a variety of health problems. These infections can cause a mild skin infection or sore throat. But they can also cause severe,
Prevention of Medical Errors
 Prevention of Medical Errors FS 456.013(7) Florida Chapter of American College of Physicians St. Petersburg Beach, Florida October 5, 2013 Cliff Rapp, LHRM Regional Vice President Patient Safety Course
Prevention of Medical Errors FS 456.013(7) Florida Chapter of American College of Physicians St. Petersburg Beach, Florida October 5, 2013 Cliff Rapp, LHRM Regional Vice President Patient Safety Course
Total Abdominal Hysterectomy
 What is a total abdominal hysterectomy? Is the removal of the uterus and cervix through an abdominal incision (either an up and down or bikini cut). Removal of the ovaries and tubes depends on the patient.
What is a total abdominal hysterectomy? Is the removal of the uterus and cervix through an abdominal incision (either an up and down or bikini cut). Removal of the ovaries and tubes depends on the patient.
Women s Health Laparoscopy Information for patients
 Women s Health Laparoscopy Information for patients This leaflet is for women who have been advised to have a laparoscopy. It outlines the common reasons doctors recommend this operation, what will happen
Women s Health Laparoscopy Information for patients This leaflet is for women who have been advised to have a laparoscopy. It outlines the common reasons doctors recommend this operation, what will happen
Is it really so? : Varying Presentations for ACS among Elderly, Women and Diabetics. Yen Tibayan, M.D. Division of Cardiovascular Medicine
 Is it really so? : Varying Presentations for ACS among Elderly, Women and Diabetics Yen Tibayan, M.D. Division of Cardiovascular Medicine Case Presentation 69 y.o. woman calls 911 with the complaint of
Is it really so? : Varying Presentations for ACS among Elderly, Women and Diabetics Yen Tibayan, M.D. Division of Cardiovascular Medicine Case Presentation 69 y.o. woman calls 911 with the complaint of
Surgical removal of fibroids through an abdominal incision-either up and down or bikini cut. The uterus and cervix are left in place.
 What is an abdominal myomectomy? Surgical removal of fibroids through an abdominal incision-either up and down or bikini cut. The uterus and cervix are left in place. When is this surgery used? Treatment
What is an abdominal myomectomy? Surgical removal of fibroids through an abdominal incision-either up and down or bikini cut. The uterus and cervix are left in place. When is this surgery used? Treatment
THE KIDNEY. Bulb of penis Abdominal aorta Scrotum Adrenal gland Inferior vena cava Urethra Corona glandis. Kidney. Glans penis Testicular vein
 29 THE KIDNEY 9. Recurrent urinary tract infections Recurrent urinary tract infections The urinary tract consists of the urethra, the bladder, the ureters, the kidneys and in men the prostate gland. An
29 THE KIDNEY 9. Recurrent urinary tract infections Recurrent urinary tract infections The urinary tract consists of the urethra, the bladder, the ureters, the kidneys and in men the prostate gland. An
SOD (Sphincter of Oddi Dysfunction)
") SOD (Sphincter of Oddi Dysfunction) SOD refers to the mechanical malfunctioning of the Sphincter of Oddi, which is the valve muscle that regulates the flow of bile and pancreatic juice into the duodenum.
SOD (Sphincter of Oddi Dysfunction) SOD refers to the mechanical malfunctioning of the Sphincter of Oddi, which is the valve muscle that regulates the flow of bile and pancreatic juice into the duodenum.
Urinary Diversion: Ileovesicostomy/Ileal Loop/Colon Loop
 Urinary Diversion: Ileovesicostomy/Ileal Loop/Colon Loop Why do I need this surgery? A urinary diversion is a surgical procedure that is performed to allow urine to safely pass from the kidneys into a
Urinary Diversion: Ileovesicostomy/Ileal Loop/Colon Loop Why do I need this surgery? A urinary diversion is a surgical procedure that is performed to allow urine to safely pass from the kidneys into a
Gallbladder Diseases and Problems
 Gallbladder Diseases and Problems Introduction Your gallbladder is a pear-shaped organ under your liver. It stores bile, a fluid made by your liver to digest fat. There are many diseases and problems that
Gallbladder Diseases and Problems Introduction Your gallbladder is a pear-shaped organ under your liver. It stores bile, a fluid made by your liver to digest fat. There are many diseases and problems that
Laparoscopic Cholecystectomy
 Laparoscopic Cholecystectomy Removal of Gall Bladder Page 12 Patient Information Further Information We endeavour to provide an excellent service at all times, but should you have any concerns please,
Laparoscopic Cholecystectomy Removal of Gall Bladder Page 12 Patient Information Further Information We endeavour to provide an excellent service at all times, but should you have any concerns please,
Ovarian Cyst. Homoeopathy Clinic. Introduction. Types of Ovarian Cysts. Contents. Case Reports. 21 August 2002
 Case Reports 21 August 2002 Ovarian Cyst Homoeopathy Clinic Check Yourself If you have any of the following symptoms call your doctor. Sense of fullness or pressure or a dull ache in the abdomen Pain during
Case Reports 21 August 2002 Ovarian Cyst Homoeopathy Clinic Check Yourself If you have any of the following symptoms call your doctor. Sense of fullness or pressure or a dull ache in the abdomen Pain during
Advanced Practice Provider Academy
 (+)Dean T. Harrison, MPAS,PA C,DFAAPA Director of Mid Level Practitioners; Assistant Medical Director Clinical Evaluation Unit, Division of Emergency Medicine, Department of Surgery, Duke University Medical
(+)Dean T. Harrison, MPAS,PA C,DFAAPA Director of Mid Level Practitioners; Assistant Medical Director Clinical Evaluation Unit, Division of Emergency Medicine, Department of Surgery, Duke University Medical
Abdominal Pain. Learning Objectives:
 Abdominal Pain Learning Objectives: Knowledge At the end of the subinternship, the subinterns should be able to: Describe the common causes of abdominal pain in hospitalized patient including o Intestinal
Abdominal Pain Learning Objectives: Knowledge At the end of the subinternship, the subinterns should be able to: Describe the common causes of abdominal pain in hospitalized patient including o Intestinal
 More information >>> HERE
More information >>> HERE Amylase and Lipase Tests
 Amylase and Lipase Tests Also known as: Amy Formal name: Amylase Related tests: Lipase The Test The blood amylase test is ordered, often along with a lipase test, to help diagnose and monitor acute or
Amylase and Lipase Tests Also known as: Amy Formal name: Amylase Related tests: Lipase The Test The blood amylase test is ordered, often along with a lipase test, to help diagnose and monitor acute or
Informed Consent for Laparoscopic Vertical Sleeve Gastrectomy. Patient Name
 Informed Consent for Laparoscopic Vertical Sleeve Gastrectomy Patient Name Please read this form carefully and ask about anything you may not understand. I consent to have a laparoscopic Vertical Sleeve
Informed Consent for Laparoscopic Vertical Sleeve Gastrectomy Patient Name Please read this form carefully and ask about anything you may not understand. I consent to have a laparoscopic Vertical Sleeve
It s A Gut Feeling: Abdominal Pain in Children. David Deutsch, MD Pediatric Gastroenterology Rockford Health Physicians
 It s A Gut Feeling: Abdominal Pain in Children David Deutsch, MD Pediatric Gastroenterology Rockford Health Physicians Introduction Common Symptom Affects 10-15% of school-aged children Definition (Dr.
It s A Gut Feeling: Abdominal Pain in Children David Deutsch, MD Pediatric Gastroenterology Rockford Health Physicians Introduction Common Symptom Affects 10-15% of school-aged children Definition (Dr.
Laparoscopic Bilateral Salpingo-Oophorectomy
 Laparoscopic Bilateral Salpingo-Oophorectomy What is a? This is a surgery where your doctor uses a thin, lighted camera and small surgical tool placed through a small (1/2 inch) incision usually in the
Laparoscopic Bilateral Salpingo-Oophorectomy What is a? This is a surgery where your doctor uses a thin, lighted camera and small surgical tool placed through a small (1/2 inch) incision usually in the
Total Vaginal Hysterectomy
 What is a total vaginal hysterectomy? Is the removal of the uterus and cervix through the vagina. Removal of the ovaries and tubes depends on the patient. Why is this surgery used? To treat disease of
What is a total vaginal hysterectomy? Is the removal of the uterus and cervix through the vagina. Removal of the ovaries and tubes depends on the patient. Why is this surgery used? To treat disease of
Care and Problems of the Digestive System. Chapter 18 Lesson 2
 Care and Problems of the Digestive System Chapter 18 Lesson 2 Care of the Digestive System Good eating habits are the best way to avoid or minimize digestive system problems. Eat a variety of foods Avoid
Care and Problems of the Digestive System Chapter 18 Lesson 2 Care of the Digestive System Good eating habits are the best way to avoid or minimize digestive system problems. Eat a variety of foods Avoid
Aehlert: Paramedic Practice Today PowerPoint Lecture Notes Chapter 50: Abdominal Trauma
 Aehlert: Paramedic Practice Today PowerPoint Lecture Notes Chapter 50: Abdominal Trauma Chapter 50 Abdominal Trauma 1 Describe the epidemiology, including morbidity, mortality rates, and prevention strategies,
Aehlert: Paramedic Practice Today PowerPoint Lecture Notes Chapter 50: Abdominal Trauma Chapter 50 Abdominal Trauma 1 Describe the epidemiology, including morbidity, mortality rates, and prevention strategies,
New England Pain Management Consultants At New England Baptist Hospital
 New England Pain Management Consultants At New England Baptist Hospital Pain Management Center Health Assessment Dear New Pain Management Patient, Welcome to the New England Pain Management Consultants
New England Pain Management Consultants At New England Baptist Hospital Pain Management Center Health Assessment Dear New Pain Management Patient, Welcome to the New England Pain Management Consultants
 More details >>> HERE
More details >>> HERE Radiation Therapy for Prostate Cancer
 Radiation Therapy for Prostate Cancer Introduction Cancer of the prostate is the most common form of cancer that affects men. About 240,000 American men are diagnosed with prostate cancer every year. Your
Radiation Therapy for Prostate Cancer Introduction Cancer of the prostate is the most common form of cancer that affects men. About 240,000 American men are diagnosed with prostate cancer every year. Your
Abdomen X-Ray (AXR) Collimation is ideally from diaphragms to lower border of the symphysis pubis and the lateral skin margins.
 Collimation is ideally from diaphragms to lower border of the symphysis pubis and the lateral skin margins.") Abdomen X-Ray (AXR) Collimation is ideally from diaphragms to lower border of the symphysis pubis and the lateral skin margins. LMP of child-bearing age female patients should be checked. 1. Acute abdomen
Abdomen X-Ray (AXR) Collimation is ideally from diaphragms to lower border of the symphysis pubis and the lateral skin margins. LMP of child-bearing age female patients should be checked. 1. Acute abdomen
Chronic abdominal pain of childhood
 Chronic abdominal pain of childhood Sandra I. Escalera, M.D. ProHealth Physicians Associate Clinical Professor Department of Pediatrics Yale University School of Medicine Objectives Brief overview of approach
Chronic abdominal pain of childhood Sandra I. Escalera, M.D. ProHealth Physicians Associate Clinical Professor Department of Pediatrics Yale University School of Medicine Objectives Brief overview of approach
Guide to Claims against General Practitioners (GPs)
") Patients often build up a relationship of trust with their GP over a number of years. It can be devastating when a GP fails in his or her duty to a patient. Our medical negligence solicitors understand
Patients often build up a relationship of trust with their GP over a number of years. It can be devastating when a GP fails in his or her duty to a patient. Our medical negligence solicitors understand
Abdominal Pain in a Pregnant Patient
 January 2007 Abdominal Pain in a Pregnant Patient Megan Browning, Harvard Medical School Year III 1 HPI Ms.O is a 21yo pregnant female (23+6 weeks gestation) Woke with 5/10 crampy abdominal pain followed
January 2007 Abdominal Pain in a Pregnant Patient Megan Browning, Harvard Medical School Year III 1 HPI Ms.O is a 21yo pregnant female (23+6 weeks gestation) Woke with 5/10 crampy abdominal pain followed
Ovarian Cystectomy / Oophorectomy
 Cystectomy and Ovarian Cysts Ovarian cysts are sacs filled with fluids or pockets located on or in an ovary. In some cases, these cysts need to be removed surgically. Types of Cysts Ovarian cysts are quite
Cystectomy and Ovarian Cysts Ovarian cysts are sacs filled with fluids or pockets located on or in an ovary. In some cases, these cysts need to be removed surgically. Types of Cysts Ovarian cysts are quite
PATIENT REGISTRATION
 PATIENT REGISTRATION Patient s Last Name: Patient s First Name: MI: Address: City, State Zip code: Patient s Date of Birth: Patient s Social Security: Best Number to contact: Secondary Number: Marital
PATIENT REGISTRATION Patient s Last Name: Patient s First Name: MI: Address: City, State Zip code: Patient s Date of Birth: Patient s Social Security: Best Number to contact: Secondary Number: Marital
Cardiovascular diseases. pathology
 Cardiovascular diseases pathology Atherosclerosis Vascular diseases A disease that results in arterial wall thickens as a result of build- up of fatty materials such cholesterol, resulting in acute and
Cardiovascular diseases pathology Atherosclerosis Vascular diseases A disease that results in arterial wall thickens as a result of build- up of fatty materials such cholesterol, resulting in acute and
Borland-Groover Clinic PATIENT GENERATED MEDICAL HISTORY Name: DOB: Email: Primary Care Physician: Pharmacy: Pharmacy Phone #:
 PATIENT GENERATED MEDICAL HISTORY Name: DOB: Email: Primary Care Physician: Referring: Pharmacy: Pharmacy Phone #: Place Sticker Here Directions: Please circle any of the following you have personally
PATIENT GENERATED MEDICAL HISTORY Name: DOB: Email: Primary Care Physician: Referring: Pharmacy: Pharmacy Phone #: Place Sticker Here Directions: Please circle any of the following you have personally
Acute Abdominal Pain following Bariatric Surgery. Disclosure. Objectives 8/17/2015. I have nothing to disclose
 Acute Abdominal Pain following Bariatric Surgery Kathy J. Morris, DNP, APRN, FNP C, FAANP University of Nebraska Medical Center College of Nursing Disclosure I have nothing to disclose Objectives Pathophysiology
Acute Abdominal Pain following Bariatric Surgery Kathy J. Morris, DNP, APRN, FNP C, FAANP University of Nebraska Medical Center College of Nursing Disclosure I have nothing to disclose Objectives Pathophysiology
The degree of liver inflammation or damage (grade) Presence and extent of fatty liver or other metabolic liver diseases
 Presence and extent of fatty liver or other metabolic liver diseases") ilearning about your health Liver Biopsy www.cpmc.org/learning What is a Liver Biopsy? A liver biopsy is a procedure where a specially trained doctor (typically a hepatologist, radiologist, or gastroenterologist)
ilearning about your health Liver Biopsy www.cpmc.org/learning What is a Liver Biopsy? A liver biopsy is a procedure where a specially trained doctor (typically a hepatologist, radiologist, or gastroenterologist)
X-Plain Abdominal Aortic Aneurysm Vascular Surgery Reference Summary
 X-Plain Abdominal Aortic Aneurysm Vascular Surgery Reference Summary Ballooning of the aorta, also known as an "abdominal aortic aneurysm," can lead to life threatening bleeding. Doctors may recommend
X-Plain Abdominal Aortic Aneurysm Vascular Surgery Reference Summary Ballooning of the aorta, also known as an "abdominal aortic aneurysm," can lead to life threatening bleeding. Doctors may recommend
Colon and Rectal Cancer
 Colon and Rectal Cancer What is colon or rectal cancer? Colon or rectal cancer is the growth of abnormal cells in your large intestine, which is also called the large bowel. The colon is the last 5 feet
Colon and Rectal Cancer What is colon or rectal cancer? Colon or rectal cancer is the growth of abnormal cells in your large intestine, which is also called the large bowel. The colon is the last 5 feet
REVIEW OF SYSTEMS! HISTORY OF PRESENT ILLNESS! 4/1/14! Exertional Abdominal Pain in a Crew Athlete!
 Exertional Abdominal Pain in a Crew Athlete! Vanessa Lalley-DeMong DO Andrew Kusienski DO Melissa Tabor DO! HISTORY OF PRESENT ILLNESS! 19 year old Division II sophomore female crew athlete presents to
Exertional Abdominal Pain in a Crew Athlete! Vanessa Lalley-DeMong DO Andrew Kusienski DO Melissa Tabor DO! HISTORY OF PRESENT ILLNESS! 19 year old Division II sophomore female crew athlete presents to
Gastrointestinal Bleeding
 Gastrointestinal Bleeding Introduction Gastrointestinal bleeding is a symptom of many diseases rather than a disease itself. A number of different conditions can cause gastrointestinal bleeding. Some causes
Gastrointestinal Bleeding Introduction Gastrointestinal bleeding is a symptom of many diseases rather than a disease itself. A number of different conditions can cause gastrointestinal bleeding. Some causes
Incontinence. What is incontinence?
 Incontinence What is incontinence? Broadly speaking, the medical term incontinence refers to any involuntary release of bodily fluids, but many people associate it strongly with the inability to control
Incontinence What is incontinence? Broadly speaking, the medical term incontinence refers to any involuntary release of bodily fluids, but many people associate it strongly with the inability to control
Recognizing and Treating Fevers in Children with Complex Medical Issues by Susan Agrawal
 www.complexchild.com Recognizing and Treating Fevers in Children with Complex Medical Issues by Susan Agrawal Fevers can be some of the scariest symptoms we see in our children, but they are also some
www.complexchild.com Recognizing and Treating Fevers in Children with Complex Medical Issues by Susan Agrawal Fevers can be some of the scariest symptoms we see in our children, but they are also some
Application For Admission To The Non-Surgical Spinal Decompression Program At The Spinal Decompression Center of Long Beach
 Application For Admission To The Non-Surgical Spinal Decompression Program At The Spinal Decompression Center of Long Beach If you are reading this form, you have qualified for a consultation with Dr.
Application For Admission To The Non-Surgical Spinal Decompression Program At The Spinal Decompression Center of Long Beach If you are reading this form, you have qualified for a consultation with Dr.
Learning Objectives. Introduction to Medical Careers. Vocabulary: Chapter 16 FACTS. Functions. Organs. Digestive System Chapter 16
 Learning Objectives Introduction to Medical Careers Digestive System Chapter 16 Define at least 10 terms relating to the digestive Describe the four functions of the digestive Identify different structures
Learning Objectives Introduction to Medical Careers Digestive System Chapter 16 Define at least 10 terms relating to the digestive Describe the four functions of the digestive Identify different structures
OVARIAN CYSTS. Types of Ovarian Cysts There are many types of ovarian cysts and these can be categorized into functional and nonfunctional
 OVARIAN CYSTS Follicular Cyst Ovarian cysts are fluid-filled sacs that form within or on the ovary. The majority of these cysts are functional meaning they usually form during a normal menstrual cycle.
OVARIAN CYSTS Follicular Cyst Ovarian cysts are fluid-filled sacs that form within or on the ovary. The majority of these cysts are functional meaning they usually form during a normal menstrual cycle.
Section IV Diagnostic Coding and Reporting for Outpatient Services
 Section IV Diagnostic Coding and Reporting for Outpatient Services Section IV, here we come! Keep that book cracked open and let s go through Diagnostic Coding and Reporting Guidelines for Outpatient Services.
Section IV Diagnostic Coding and Reporting for Outpatient Services Section IV, here we come! Keep that book cracked open and let s go through Diagnostic Coding and Reporting Guidelines for Outpatient Services.
Acute Pancreatitis. Questionnaire. if yes: amount (cigarettes/day): since when (year): Drug consumption: yes / no if yes: type of drug:. amount:.
: since when (year): Drug consumption: yes / no if yes: type of drug:. amount:.") The physical examination has to be done AT ADMISSION! The blood for laboratory parameters has to be drawn AT ADMISSION! This form has to be filled AT ADMISSION! Questionnaire Country: 1. Patient personal
The physical examination has to be done AT ADMISSION! The blood for laboratory parameters has to be drawn AT ADMISSION! This form has to be filled AT ADMISSION! Questionnaire Country: 1. Patient personal
Consent for Treatment/Procedure Laparoscopic Sleeve Gastrectomy
 Patient's Name: Today's Date: / / The purpose of this document is to confirm, in the presence of witnesses, your informed request to have Surgery for obesity. You are asked to read the following document
Patient's Name: Today's Date: / / The purpose of this document is to confirm, in the presence of witnesses, your informed request to have Surgery for obesity. You are asked to read the following document
Laparoscopic Cholecystectomy
 Laparoscopic Cholecystectomy Gallbladder removal is one of the most commonly performed surgical procedures in the United States. Today,gallbladder surgery is performed laparoscopically. The medical name
Laparoscopic Cholecystectomy Gallbladder removal is one of the most commonly performed surgical procedures in the United States. Today,gallbladder surgery is performed laparoscopically. The medical name
10 Common Questions Answers SBO
 10 Common Questions Answers SBO 1 What is Small Bowel Obstruction (SBO)? After food passes through our stomach, it soon arrives in our intestines, starting at the small bowel. This tube-like organ meanders
10 Common Questions Answers SBO 1 What is Small Bowel Obstruction (SBO)? After food passes through our stomach, it soon arrives in our intestines, starting at the small bowel. This tube-like organ meanders
ENDOSCOPIC ULTRASOUND (EUS)
") ENDOSCOPIC ULTRASOUND (EUS) What you need to know before your procedure Your Doctor has decided that an EUS is necessary for further evaluation and treatment of your condition. This information sheet has
ENDOSCOPIC ULTRASOUND (EUS) What you need to know before your procedure Your Doctor has decided that an EUS is necessary for further evaluation and treatment of your condition. This information sheet has
Excision of Vaginal Mesh
 What is excision of vaginal mesh? This procedure is done to remove mesh from the vagina. When is this surgery used? If mesh has eroded into the vagina, bladder, urethra, or bowel If there is pain associated
What is excision of vaginal mesh? This procedure is done to remove mesh from the vagina. When is this surgery used? If mesh has eroded into the vagina, bladder, urethra, or bowel If there is pain associated
Urinary Tract Infections
 1 Infections in the urinary tract are relatively common. These infections are often referred to as bladder infections. They are also known as UTI s or urinary tract infections. When an infection is confined
1 Infections in the urinary tract are relatively common. These infections are often referred to as bladder infections. They are also known as UTI s or urinary tract infections. When an infection is confined
NEURO-OPHTHALMIC QUESTIONNAIRE NAME: AGE: DATE OF EXAM: CHART #: (Office Use Only)
") PAGE 1 NEURO-OPHTHALMIC QUESTIONNAIRE NAME: AGE: DATE OF EXAM: CHART #: (Office Use Only) 1. What is the main problem that you are having? (If additional space is required, please use the back of this
PAGE 1 NEURO-OPHTHALMIC QUESTIONNAIRE NAME: AGE: DATE OF EXAM: CHART #: (Office Use Only) 1. What is the main problem that you are having? (If additional space is required, please use the back of this
Quality Measures for Long-stay Residents Percent of residents whose need for help with daily activities has increased.
 Quality Measures for Long-stay Residents Percent of residents whose need for help with daily activities has increased. This graph shows the percent of residents whose need for help doing basic daily tasks
Quality Measures for Long-stay Residents Percent of residents whose need for help with daily activities has increased. This graph shows the percent of residents whose need for help doing basic daily tasks
MEDICAL HISTORY AND SCREENING FORM
 MEDICAL HISTORY AND SCREENING FORM The purpose of preventive exams is to screen for potential health problems and provide education to promote optimal health. It is best practice for chronic health problems
MEDICAL HISTORY AND SCREENING FORM The purpose of preventive exams is to screen for potential health problems and provide education to promote optimal health. It is best practice for chronic health problems
ABDOMINAL PAIN. Epigastric Pain. Right Upper Quadrant Pain. Location Work-up Acute pain syndromes Chronic pain syndromes
 ABDOMINAL PAIN Location Work-up Acute pain syndromes Chronic pain syndromes Epigastric Pain PUD GERD MI AAA- abdominal aortic aneurysm Pancreatic pain Gallbladder and common bile duct obstruction Right
ABDOMINAL PAIN Location Work-up Acute pain syndromes Chronic pain syndromes Epigastric Pain PUD GERD MI AAA- abdominal aortic aneurysm Pancreatic pain Gallbladder and common bile duct obstruction Right
RENAL ANGIOMYOLIPOMA EMBOLIZATION
 RENAL ANGIOMYOLIPOMA EMBOLIZATION The information about renal angiomyolipomas on the next several pages includes questions commonly asked about the embolization procedure. Please take a few moments to
RENAL ANGIOMYOLIPOMA EMBOLIZATION The information about renal angiomyolipomas on the next several pages includes questions commonly asked about the embolization procedure. Please take a few moments to
Spinal Cord and Bladder Management Male: Intermittent Catheter
 Spinal Cord and Bladder Management Male: Intermittent Catheter The 5 parts of the urinary system work together to get rid of waste and make urine. Urine is made in your kidneys and travels down 2 thin
Spinal Cord and Bladder Management Male: Intermittent Catheter The 5 parts of the urinary system work together to get rid of waste and make urine. Urine is made in your kidneys and travels down 2 thin
Open the Flood Gates Urinary Obstruction and Kidney Stones. Dr. Jeffrey Rosenberg Dr. Emilio Lastarria Dr. Richard Kasulke
 Open the Flood Gates Urinary Obstruction and Kidney Stones Dr. Jeffrey Rosenberg Dr. Emilio Lastarria Dr. Richard Kasulke Nephrology vs. Urology Nephrologist a physician who has been trained in the diagnosis
Open the Flood Gates Urinary Obstruction and Kidney Stones Dr. Jeffrey Rosenberg Dr. Emilio Lastarria Dr. Richard Kasulke Nephrology vs. Urology Nephrologist a physician who has been trained in the diagnosis
San Luis Dermatology & Laser Clinic, Inc.
 San Luis Dermatology & Laser Clinic, Inc. Patient Name: Pharmacy Name: LOCATION Health History Intake Form The federal government has defined a complete electronic medical record (EMR) or electronic health
San Luis Dermatology & Laser Clinic, Inc. Patient Name: Pharmacy Name: LOCATION Health History Intake Form The federal government has defined a complete electronic medical record (EMR) or electronic health
Chest Pain. Acute Myocardial Infarction: Differential Diagnosis and Patient Management. Common complaint in ED. Wide range of etiologies
 Acute Myocardial Infarction: Differential Diagnosis and Patient Management Presented By: Barbara Furry, RN-BC, MS, CCRN, FAHA Director The Center of Excellence in Education Director of HERO Chest Pain
Acute Myocardial Infarction: Differential Diagnosis and Patient Management Presented By: Barbara Furry, RN-BC, MS, CCRN, FAHA Director The Center of Excellence in Education Director of HERO Chest Pain
Surgical Emergency Unit Abdominal Pain
 Oxford University Hospitals NHS Trust Surgical Emergency Unit Abdominal Pain Information for Patients What is abdominal pain? Abdominal pain usually refers to cramps or a dull ache in the abdomen. It is
Oxford University Hospitals NHS Trust Surgical Emergency Unit Abdominal Pain Information for Patients What is abdominal pain? Abdominal pain usually refers to cramps or a dull ache in the abdomen. It is
Figure 9-2. Abdominal and Genitourinary. Internal Anatomy. Deep Internal Anatomy. Abdominal Anatomy & Physiology. Abdominal Surface Landmarks
 Figure 9-2. Abdominal and Genitourinary Abdominal Surface Landmarks Myung-Hee Pak, RN, MSN, CNS Internal Anatomy Deep Internal Anatomy Pat Thomas, 2006. Pat Thomas, 2006. Abdominal Anatomy & Organs of
Figure 9-2. Abdominal and Genitourinary Abdominal Surface Landmarks Myung-Hee Pak, RN, MSN, CNS Internal Anatomy Deep Internal Anatomy Pat Thomas, 2006. Pat Thomas, 2006. Abdominal Anatomy & Organs of
Palm Beach Obstetrics & Gynecology, PA
 Palm Beach Obstetrics & Gynecology, PA 4671 S. Congress Avenue, Lake Worth, FL 33461 561.434.0111 4631 N. Congress Avenue, Suite 102, West Palm Beach, FL 33407 Urinary Tract Infection About one of every
Palm Beach Obstetrics & Gynecology, PA 4671 S. Congress Avenue, Lake Worth, FL 33461 561.434.0111 4631 N. Congress Avenue, Suite 102, West Palm Beach, FL 33407 Urinary Tract Infection About one of every
A.P. Chen, MD Director, Developmental Therapeutics Clinic Division of Cancer Treatment and Diagnosis National Cancer Institute
 A.P. Chen, MD Director, Developmental Therapeutics Clinic Division of Cancer Treatment and Diagnosis National Cancer Institute Click to view Biosketch and Presentation Abstract or page down to review presentation
A.P. Chen, MD Director, Developmental Therapeutics Clinic Division of Cancer Treatment and Diagnosis National Cancer Institute Click to view Biosketch and Presentation Abstract or page down to review presentation
Chemotherapy Side Effects Worksheet
 Page 1 of 6 Chemotherapy Side Effects Worksheet Medicines or drugs that destroy cancer cells are called cancer chemotherapy. It is sometimes the first choice for treating many cancers. Chemotherapy differs
Page 1 of 6 Chemotherapy Side Effects Worksheet Medicines or drugs that destroy cancer cells are called cancer chemotherapy. It is sometimes the first choice for treating many cancers. Chemotherapy differs
ABThera Open Abdomen Negative Pressure Therapy for Active Abdominal Therapy. Case Series
 ABThera Open Abdomen Negative Pressure Therapy for Active Abdominal Therapy Case Series Summary of Cases: USER EXPERIENCE The ABThera OA NPT system was found by surgeons to be a convenient and effective
ABThera Open Abdomen Negative Pressure Therapy for Active Abdominal Therapy Case Series Summary of Cases: USER EXPERIENCE The ABThera OA NPT system was found by surgeons to be a convenient and effective