Esthetic Technique Clinical Case Studies and Technique Review
|
|
|
- Caitlin Johns
- 10 years ago
- Views:
Transcription
1 Vol. 1, No. 4, 2001 Esthetic Technique Clinical Case Studies and Technique Review Crown Considerations, Preparations, and Material Selection for Esthetic Metal-Ceramic Restorations Edward A. McLaren, DDS Greg Vigoren, DDS A Crown Preparation System That Produces Ideally Smooth Supragingival and Subgingival Margins Cary E. Goldstein, DMD Sponsored by Brasseler USA 2 Hours of Continuing Education Credit from Dental Learning Systems A Supplement to Contemporary Esthetics and Restorative Practice An MWC Publication Medical World Business Press, Inc.

2 Dental Learning Systems 241 Forsgate Drive, Jamesburg, NJ (800) Fax (732) ADVISORY BOARD Dear Reader: There has been a continuous increase in demand for more esthetic, or tooth-colored, restorations by the dental profession and the public over the past few decades. This demand has come about because of an increased public awareness of and desire for esthetic materials over metallic-based restorations, the introduction of new technologies by industry and the scientific community, and a growing population of clinicians who have elected a preference for enhancing the esthetics of their patients. It would be safe to assume that all clinicians would favor an esthetic restorative procedure as long as there was no significant compromise in health care delivery to their patients. Dr. McLaren and Dr. Vigoren have presented a comprehensive discussion of improving esthetics without compromising basic principles of ceramic crown restorations. Specifically, they focus their article on the proper use of the Captek technique of a metal-ceramic crown. Using a balance of science and personal experience, they are able to discuss in depth many of the basic guidelines and principles that can assist clinicians with achieving successful results when using this technology. They discuss important factors such as depth of preparations, indications for specifically designed burs or diamonds, type of core materials present, and single vs multiple units. The end result is a three-dimensional, integrated outline of the principles of ceramic crown restorations. Both the experienced and novice clinician will benefit from the authors experiences and knowledge. Dr. Goldstein reviews the use and significance of a series of diamond instruments that should assist clinicians when performing various esthtic procedures. Behind each procedural step are principles related to optimizing the final esthetic procedure. Dentists should find this information useful in developing a consistent approach to tooth preparation rather than relying on a history of inconsistent preparation routines that may not meet the demands of today s newer technologies. Dental Learning Systems would like to thank Brasseler USA for sponsoring this clinical series for the dental profession. Sincerely, Duke sig E. Steven Duke, DDS, MSD Professor and Chairman Department of Restorative Dentistry Indiana University School of Dentistry Nasser Barghi, DDS Edward A. McLaren, DDS John Kois, DMD, MSD Douglas A. Terry, DDS Bruce Crispin, DDS, MS Larry Rosenthal, DDS Gerard Kugel, DMD, MS Thomas F. Trinkner, DDS Dental Learning Systems is an ADA Recognized Provider Academy of General Dentistry Approved National Sponsor. FAGD/MAGD Credit 7/18/1990 to 12/31/2002 Lee Culp, CDT Howard Strassler, DMD Publisher and President, Daniel W. Perkins; Director of Publishing Operations, Ken Senerth; Vice President of Sales and Associate Publisher, Anthony Angelini; Editorial Director, Allison W. Walker; Associate Projects Editor, Lisa M. Neuman; Projects Director, Eileen R. Henry-Lewis; Copy Editors, Barbara Marino and Susan Costello; Design Director, Jennifer Kmenta; Design Director, Special Projects, Liz Arendt; Circulation Director, Jackie Hubler; Northeast Regional Sales Manager, Jeffery E. Gordon; West Coast Regional Sales Manager, Michael Gee; Executive and Advertising Offices, Dental Learning Systems, 241 Forsgate Drive, Jamesburg, NJ , Phone (732) , Fax (732) Postmaster: Send address changes to Contemporary Esthetics and Restorative Practice, Attn: Data Control, One Broad Avenue, Fairview, NJ Send correspondence regarding subscriptions or address changes to Data Control, One Broad Avenue, Fairview, NJ , or call (800) Periodicals postage paid at Monroe Township, NJ 08831, and at additional mailing entries. Contemporary Esthetics and Restorative Practice (ISSN , USPS ) is published 12 times a year by Dental Learning Systems, 241 Forsgate Drive, Jamesburg, NJ Copyright Medical World Business Press, Inc./A division of Medical World Communications, Inc. Printed in the USA. All rights reserved. No part of this issue may be reproduced in any form without written permission from the publisher. Contemporary Esthetics and Restorative Practice is a registered trademark of Medical World Business Press, Inc. Medical World Communications Corporate Officers: Chairman/CEO, John J. Hennessy; President, Curtis Pickelle; Chief Financial Officer, Steven J. Resnick; Vice President of Business Development, Robert Issler; Vice President of Manufacturing, Frank A. Lake. D452 The Esthetic Technique series is made possible through an educational grant from Brasseler USA. To order additional copies call , x180. D452

3 Crown Considerations, Preparations, and Material Selection for Esthetic Metal- Ceramic Restorations Edward A. McLaren, DDS Greg Vigoren, DDS Edward A. McLaren, DDS Director, Center for Esthetic Dentistry Director, School for Esthetic Dental Design School of Dentistry University of California at Los Angeles Los Angeles, California Greg Vigoren, DDS Adjunct Faculty Center for Esthetic Dentistry School of Dentistry University of California at Los Angeles Los Angeles, California Private Practice Newport Beach, California ABSTRACT In recent years, many dentists and patients have opted for metal-free restorations amid concerns regarding esthetics and potential metal toxicity. The use of a Captek substrate with a new-generation, lower-fusing porcelain has demonstrated excellent esthetic results, proving that it is possible to fabricate porcelain-fusedto-metal restorations that rival any all-ceramic restoration. This article will discuss the clinical considerations in the use of crown systems, and preparation guidelines for esthetic metal-ceramic restorations using Captek cores. LEARNING OBJECTIVES After reading this article, the reader should be able to: describe the preparation techniques for single- and multiple-crown situations. identify situations in which a core system should be used. discuss the clinical situations in which full-coverage crowns supported by a high-strength core should be considered. explain the difficulties in controlling proper tooth reduction in clinical situations where multiple crowns are necessary. Esthetic metal ceramics have seemed almost oxymoronic to many dentists and patients. The esthetic push in recent years has been for the metal-free restoration under the guise that superior esthetics can be obtained only without using metal substrates in crown restorations. Also, concerns over potential metal toxicity have led the public and many dentists to choose metal-free restorations. Many of these metal-free systems, marketed as alternatives to conventional porcelain-fused-to-metal (PFM) restorations, have little or no clinical or toxicity data to support their use. High-gold alloys have proven safe and are tolerated well by patients; it has been only the use of nonprecious alloys that have created toxic reactions in patients. 1 Porcelains have proven to be highly biocompatible, which favors a healthy gingival response, and are frequently used in restorations for veneers, metal-ceramic, or high-strength ceramic copings. 2 However, it is possible to fabricate PFM restorations that rival any all-ceramic restoration esthetically 3 with the proper use of new-generation porcelains and alloy systems. 4 Specifically, the use of a Captek,a substrate with Vita Omega 900 b, a new-generation, lower-fusing porcelain, has demonstrated excellent esthetic results (Figure 1). The specific framework design parameters for the esthetic fabrication of porcelain-veneered Captek crowns is dealt with elsewhere. 4,5 As critical as the design parameters are for the restoration to obtain an esthetic result, also critical is the proper tooth preparation to allow room for the esthetic material. CROWN CONSIDERATIONS Ideally, the least amount of tooth structure possible should be removed when preparing teeth for crown restorations. In situations where minimal tooth structure removal is required, a porcelain-bonded restoration is indicated, assuming it will satisfy the functional and esthetic requirements of the patient (Figures 2 and 3). 6 Excess tooth structure should never be mutilated to satisfy the requirements of a certain material when a more conservative approach will satisfy functional, biologic, and esthetic requirements. Clinical situations that require a conventional PFM are the same for a Captek - supported restoration. a Captek, Altamonte Springs, FL 32714; b Vita Zahnfabrik, Germany distributed in US by Vident, Brea, CA 92621; ESTHETIC TECHNIQUE VOL. 1, NO. 4,

4 Figure 1 Porcelain-fused-to-gold crowns on teeth Nos. 8 and 9 fabricated with a Captek substrate and Vita Omega 900, a new-generation, lowerfusing porcelain. Figure 2 Preoperative condition where the structural integrity of the remaining tooth was ideal for bonded porcelain. Figure 3 Postoperative view of bonded porcelain veneers on teeth Nos. 8 and 9. Note the esthetic integration of these very conservative, bonded porcelain restorations. Full-coverage crowns supported by a high-strength core should be considered in the following clinical situations: to replace an existing PFM restoration; when there is a compromised substrate (tooth); and when there is need for support for the porcelain. It is important to understand that porcelain gets its strength from being bonded to a high-strength substrate either enamel, metal, or ceramic core. If the substrate has only dentin or composite both of which are low modulus (flexible) materials then the less flexible and more brittle ceramic will absorb a disproportionate amount of stress under load, which increases the chance for brittle failure. 7 In a study that looked at the failure load of bonded, pressed ceramics to materials of different elastic moduli, it was concluded that the failure load was proportional to the flexibility of the substrate. 8 The more flexible the substrate, the lower the failure load. Thus, thin teeth or extremely broken-down teeth, especially those with a large (and flexible) composite buildup, should not be considered for bonded porcelain restorations that have no core support. In these clinical situations, a crown should be placed that uses a high-strength core. A core system should also be used in situations where porcelain would be subjected to high shear and tensile stresses. Porcelain can extend several millimeters occlusally or incisally in situations where the stresses placed on it will be primarily compressive in nature and the substrate is stiff. It is possible to fabricate PFM restorations that rival any allceramic restoration esthetically with the proper use of newgeneration porcelains and alloy systems. PREPARATIONS The correct reduction for the room necessary for the esthetic fabrication of a Captek or, for that matter, any PFM restoration is paramount. Evaluation of more than 700 Captek restorations in which the primary author performed all clinical and ceramic procedures has led to the determination that 1.2 mm of overall labial crown thickness was the minimum ideal dimension for predictable esthetics. All of those 700-plus restorations were documented and measured for final crown dimensions before cementation, and subjective analysis was made as to the esthetic success of the cemented restorations. It was determined that a 1.2-mm facial crown dimension allowed predictable shape reproduction and subjective esthetic success. Thus, it is recommended to reduce facially to allow for a final restoration with a facial dimension of 1.2 mm. This may not mean that 1.2 mm of tooth structure needs to be removed facially. Esthetic and functional requirements will dictate whether more or less tooth should be removed, because labializing or lingualizing the facial surface may need to be accomplished. The correct reduction for a single crown is fairly easy, but the correct reduction for multiple-crown situations is much more complex. SINGLE-CROWN SITUATIONS Reduction for single crowns is generally dictated by the adjacent teeth, which is easy to visualize and compare. It is sometimes necessary to build up the tooth to the desired final shape before initiating the preparation process to better visualize the correct amount of reduction necessary for the final restoration. Before crown preparation, caries and old restoration removal with concomitant foundation restoration placement should be accomplished. Small carious lesions or old restorations can be removed during the gross reduction steps of the crown preparation. Figure 4 dem- 4 VOL. 1, NO. 4, 2001 ESTHETIC TECHNIQUE

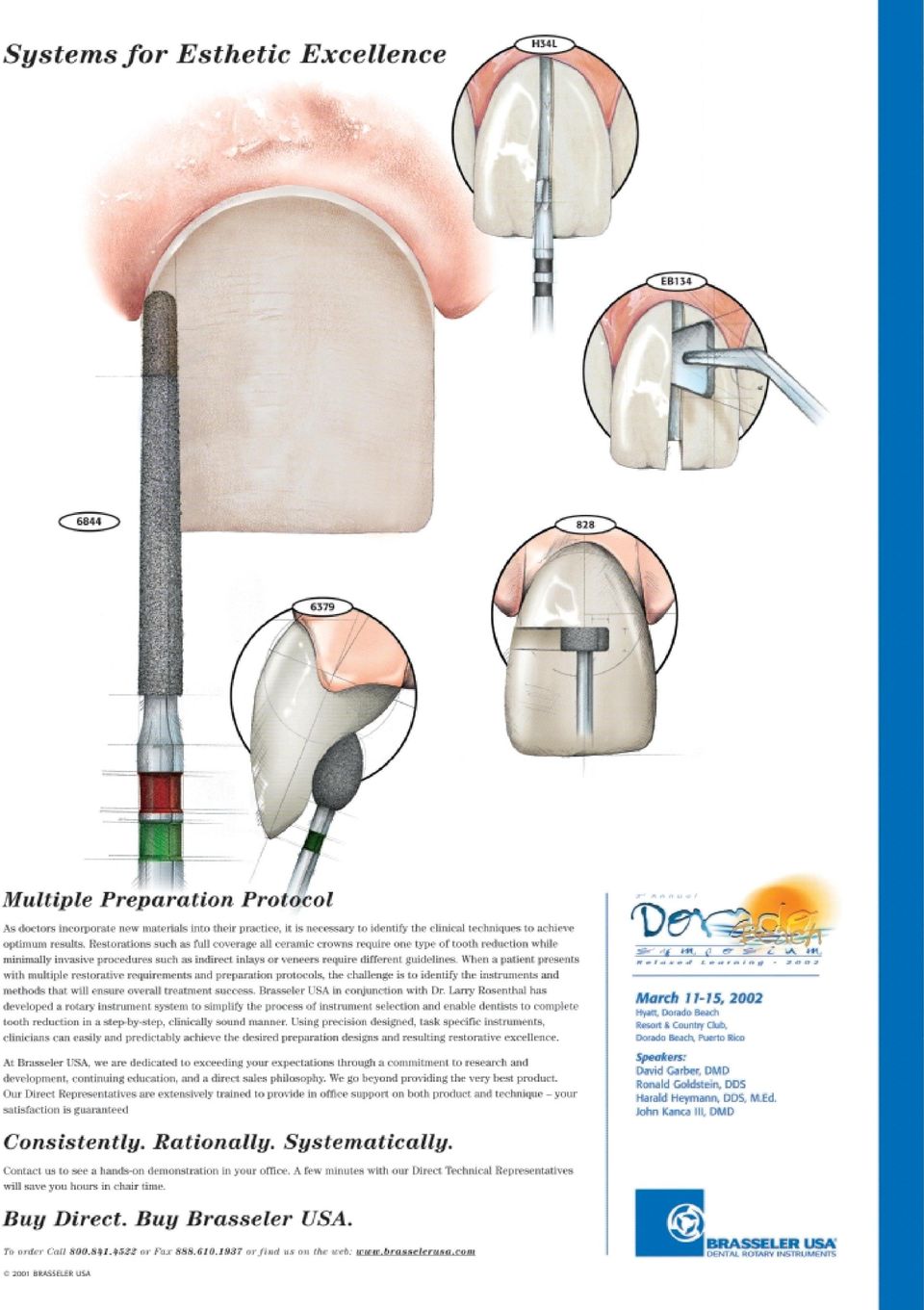
5 onstrates the UCLA Center for Esthetic Dentistry Metal-Ceramic and All-Ceramic Preparation Kit ( ) by Dr. McLaren c. The first step in the process is to break contact with the adjacent teeth (Figure 5) using the coarse diamond (# c ). The marginal area is prepared next with either a KS1 c or KS2 c diamond (Figures 6A and 6B). The marginal preparation is done right to the level of the gingiva (Figure 7). The marginal area is the most critical area when preparing for a PFM with a porcelain margin or an all-ceramic crown, and experience has shown that a 360-degree, 1- mm shoulder preparation with a 90- degree exit angle and rounded internal line angles is ideal for these restorations (Figure 8). c Brasseler USA, Savannah, GA 31419; All other areas of the preparation can be altered on the worked die by the ceramist if necessary to create more room, and can subsequently be adjusted intraorally by the dentist. An underprepared An underprepared marginal area is impossible to compensate for in the laboratory. marginal area is impossible to compensate for in the laboratory and would require repreparation and reimpressioning, hence the rationale for preparing the margin early in the preparation process. Axial reduction is next, and can be controlled by a number of techniques. Classically, it is recommended to use depth cuts to gauge the amount of reduction. This technique works only if the amount of tooth structure removal is the same as the amount of tooth structure that will be replaced. It does not work if the labial position of the tooth is being altered in the final restoration. Depth grooves generally allow the correct reduction in single-crown situations where the final restoration will follow the contour of adjacent teeth. Depth grooves are placed with a KS1, KS2, or KS3 c diamond (Figure 9) depending on the necessary reduction. The same diamond used for the depth cuts is used to remove the remaining tooth structure to the desired depth (Figure 10). The goal for a Captek Figure 4 The UCLA Center for Esthetic Dentistry Metal-Ceramic and All-Ceramic Preparation Kit by Dr. McLaren. Figure 5 Breaking contact with the # diamond on a demonstration model in which natural teeth are mounted. Figure 6A Profile view of initial margin placement done with either the KS1 or KS2 diamond. Figure 6B Facial view of margin placement done with either the KS1 or KS2 diamond. Figure 7 Initial margin placement is done right to the level of the gingiva facially and interproximally. Interproximally, a KS1 is used so as not to damage adjacent teeth. Figure 8 Shoulder margin with rounded axial-gingival line angle. ESTHETIC TECHNIQUE VOL. 1, NO. 4,

6 Figure 9 Depth grooves are placed with either a KS1 or KS2 diamond. Figure 10 Axial reduction is completed using the same KS diamond used for the depth cuts. Figure 11 Incisal edge reduction using the KS3 diamond. Figure 12 Using the 2-mm Reduction Guide to check the occlusal reduction on tooth No. 30. Figure 13 Lingual reduction is accomplished on anterior teeth with the egg-shaped KS4-024 diamond. Figure 14 Lingual reduction for posterior teeth is done with a KS2 or KS3 diamond. restoration should be to allow for 1.2 mm of space labially. Incisal or occlusal reduction is initiated with a KS3 diamond. Incisal edge reduction of 2 mm is adequate for good esthetics. The diameter of the KS3 is 1.6 mm, so going slightly deeper gives the necessary 2-mm reduction (Figure 11). The adjacent incisal edge can also be gauged as Figure 15 A clinical case with Ultrapak #000 cord placed to obtain initial gingival retraction so that the margins can be finished. The margin was prepared to the level of the retraction cord. d KerrLab, Orange, CA 92867; Figure 16 The apical position of the margin is placed with either a KS1, KS2, or, as shown, a KS6 diamond. a reduction guide. Posteriorly, it is necessary to have 2.5 mm of occlusal reduction for both esthetic metal-ceramic and all-ceramic restorations, especially if natural, unworn occlusal anatomy is desired in the final restoration. The best aid the authors have found to accomplish this reduction is the 2-mm Reduction Guide d. If the 2-mm guide passes with only slight binding through the occluded opposing arches, then there is close to 2.5 mm of interocclusal space (Figure 12). Lingual reduction is done with the KS4-024 c diamond for anterior teeth (Figure 13) and a KS2 or KS3 for posterior teeth (Figure 14) to allow for at least 0.7 mm of crown thickness for anterior teeth and 1.0 mm thickness for posterior teeth. Before finishing the preparation, one layer of Ultrapack #000 e is placed in the sulcus (Figure 15). This generally gives 0.5 mm of gingival displacement. The margin is apically positioned 0.5 mm with either a KS1 or KS2 (Figure 16) diamond or, in cases with excessively scalloped gingival margins, the KS6 c. The depth to which the margin should be placed in the sulcus is a complex issue and affect- e Ultradent Products, Inc, South Jordan, UT 84095; VOL. 1, NO. 4, 2001 ESTHETIC TECHNIQUE

7 Figure 17 Final margin finishing is completed with either the #8845KR-018 or #8845KR-025 fine diamond. Figure 18 The finishing carbide bur H can also be used to finish the margin. Figure 19 Axial contours are finished with either the # or #8856L-020 fine diamond. Figure 20 Using a polypropylene matrix to gauge gross reduction. Figure 21 A clinical case in which all maxillary teeth are to receive allceramic crowns. In these situations where adjacent teeth are prepared, the contact is broken using either the KS1 or KS2 diamond. Figure 22A Rough preparations immediately after old restoration removal. ed by many variables. 9,10 The ultimate goal of margin placement is to have an esthetic restoration/gingival interface without biologic complications (ie, violation of biologic width). The marginal area is then finished with either the #8845KR-018 c or #8845KR-025 c finishing diamonds, or the H c carbide finishing bur (Figures 17 and 18). Axial contours are finished with the # c or #8856L-020 c fine diamonds (Figure 19). For all-ceramic crowns, it is critical to round all internal line angles with one of the fine diamonds. This minimizes stress concentrations in the ceramic crown by eliminating sharp angles. PREPARATIONS FOR MULTIPLE CROWNS Clinical situations in which multiple crowns are necessary The depth to which the margin should be placed in the sulcus is a complex issue and affected by many variables. present extreme difficulties in controlling proper tooth reduction. Often, old crowns are being removed or the three-dimensional shape of the tooth is going to be altered significantly. In these situations, axial depth grooves are of limited value. It has generally been recommended to make a polypropylene vacuum-formed matrix to be used intraorally to control tooth reduction (Figure 20). While this is a useful adjunct, it is fraught with potential problems. When placed over the teeth, it is difficult to judge if the changes in tooth form that are incorporated into the matrix are in fact correct esthetically and functionally. Also, it is easy to displace the matrix in one direction or another up to almost 1 mm without knowing it. All of the above conditions could easily lead to overprepared or underprepared teeth. McLean described a technique where the prototype (temporary) is completed on the prepared teeth and then measured with a caliper to gauge proper tooth reduction. 11 Although this is the best method, two or three relines may be necessary to finalize the reduction amount, which is not very practical. One problem with this technique is that acrylic monomers left on the prepared tooth will inhibit the set of ESTHETIC TECHNIQUE VOL. 1, NO. 4,

8 Figure 22B A shell prototype is tried over the rough prepared teeth to assess esthetic and functional acceptance of the desired anatomical changes. Figure 23A The shell prototype is altered as necessary for esthetics and function. The prototype is then relined with a fast-set PVS bite registration material. Figure 23B The prototype is measured for optimal thickness, and appropriate adjustments are made to the preparation to obtain the ideal reduction. Figures 24A and 24B Two views of the final preparations on the master casts, demonstrating ideal reduction for Captek restorations. Figure 25A View of the seated, final Captek crowns. polyvinyl siloxane (PVS) impression materials. Therefore, an alternative technique will be discussed to control axial reduction. Preparations for multiplecrown situations begin by either removing the old crowns or breaking contact (Figures 21 and 22A). Contact is broken in the same manner as for a single crown, but larger diamonds can be used if the adjacent tooth is going to be prepared. The margins for all the teeth being prepared are placed second using either the KS1 or KS2 diamond. The margins are placed at this juncture following the same rationale as stated for single crowns. Gross axial reduction is done using the clear vacuum matrix as a guide, but should not be relied on for the final reduction for the reasons stated previously. Final reduction is accomplished using an alternative and very efficient technique that the authors have used for years. After gross reduction, a preformed shell prototype made from the preoperative cast or a diagnostic wax-up is placed over the prepared teeth (Figure 22B). This prototype is then evaluated for esthetics and altered as necessary for esthetic Clinical situations in which multiple crowns are necessary present extreme difficulties in controlling proper tooth reduction. acceptance. The prototype can then be relined with a fast-set PVS bite registration material (Figure 23A) and measured to verify reduction (Figure 23B). The tooth is then reduced as necessary with any of the KS diamonds. Another benefit of this technique is that debris is cleaned off the prepared teeth before final impressioning. One layer of Ultrapack #000 is then placed in the sulcus to obtain the initial tissue displacement. The final finishing steps and diamonds used are exactly the same as for single-crown situations (Figures 24A and 24B). Figures 25A through 25C represent a completed case of Captek -supported PFM restorations using the preparation protocol presented in this article. SUMMARY Many different criteria are involved in choosing the correct material or technique to treat a clinical situation. The authors presented a clinical rationale for choosing a crown system with a high-strength core of metal or ceramic vs an unsupported porcelain. Metal-ceramic restorations can rival all-ceramic restorations if 8 VOL. 1, NO. 4, 2001 ESTHETIC TECHNIQUE

9 Figure 25B View of the final Captek crowns. Note the esthetic match with the adjacent natural teeth. the proper materials and design criteria are followed. Captek restorations require 1.2 mm of facial reduction for a predictable esthetic outcome, which is less than what is generally required for conventional metal-ceramics. Proper preparation techniques are of primary importance for esthetic success with metal-ceramic restorations. Figure 25C Full-face view of the same case. This is an excellent esthetic result for a patient in his late 60s. Authors Note: All clinical and laboratory procedures were performed by Dr. McLaren. REFERENCES 1. Schuster GS, LeFebvre CA, Watana JC, et al: Biocompatibility of posterior restorative materials. J Calif Dent Assoc 24(9):17-31, Survey of Dental Restorations. In: Survey of Dental Services Chicago, ADA Survey Center, Winter RR: Achieving esthetic ceramic restorations. J Calif Dent Assoc 18(9):21-24, McLaren EA: Utilization of advanced metalceramic technology: clinical and laboratory procedures for a lower-fusing porcelain. Pract Periodontics Aesthet Dent 10(7): , McLaren EA: Forward to the past: a renaissance in ceramometal technology. Contemp Esthet Rest Pract 2(suppl 6):6-13, Goldstein RE: Diagnostic dilemma: to bond, laminate or crown? Int J Periodontics Restorative Dent 7(5):8-29, McLaren EA: All-ceramic alternatives to conventional metal-ceramic restorations. Compend Contin Educ Dent 19(3): , Scherrer SS, de Rijk WG: The fracture resistance of all-ceramic crowns on supporting structures with different elastic moduli. Int J Prosthodont 6(5): , Kois JC: Altering gingival levels: the restorative connection, part I: biologic variables. J Esthet Dent 6(1):3-9, Kois JC: New paradigms for anterior tooth preparation: rationale and technique. Contemp Esthet Dent 2(1):1-8, McLean JW: The Science and Art of Dental Ceramics. Chicago, Quintessence Publishing Co, pp , Dental Learning Systems is an ADA Recognized Provider Academy of General Dentistry Approved National Sponsor FAGD/MAGD Credit 7/18/1990 to 12/31/2002 ESTHETIC TECHNIQUE VOL. 1, NO. 4,

10 A Crown Preparation System That Produces Ideally Smooth Supragingival and Subgingival Margins Cary E. Goldstein, DMD Cary E. Goldstein, DMD Private Practice Atlanta, Georgia ABSTRACT Crown preparation design kits can be quite complex. The technique described in this article offers simplicity and consistently accurate preparations for both anterior and posterior restorations. Depth cuts with the round 1.5-mm diamond ensure precise reduction for porcelain adaptation and proper esthetics. Nine instruments and a technique guide will lead the clinician through any crown design. a Brasseler USA, Savannah, GA 31419; In developing the Goldstein Crown Design Kit,a, the goal was to provide a selection of diamonds and stones that simplify crown preparation procedures in a variety of situations. Containing only nine instruments, the kit is designed to permit the dentist to address the esthetic requirements of anterior or posterior crown cases for patients with high or low lip lines. The kit s diamond selection was designed to accommodate all porcelain crowns, aluminous-core porcelain crowns, porcelain-fused-to-metal (PFM) crowns, or those fabricated from gold. Smooth-finished, precise margins free of jagged enamel edges can be produced supragingivally or subgingivally, according to specific case requirements, enhancing the adaptation of the restoration to the tooth. Impressions made after preparation with the kit components reveal exceptional detail and facilitate accurate laboratory communications. This article describes the multiple approaches to anterior preparations offered by the Goldstein Crown Design Kit. TOOTH PREPARATION Tooth preparation begins with depth reduction, using the 1.5-mm measured reduction, round diamond bur (# a ). This round diamond serves as the key to the success of the kit and the corresponding technique selected. The round diamond provides the precise dimensions needed to create the ideal preparation. Because the bur is round, it can be used on any surface of the tooth, a concept developed by Dr. Robert Stein and then popularized by Dr. Ronald Goldstein. 1 Using the round diamond bur, a 1.5-mm depth guide is scribed around the cervical to initiate creation of the margin (Figure 1). Sufficient reduction in the marginal Figure 1 Scribing a 1.5-mm diameter depth cut around the cervical with the # coarse round diamond. Figure 2 Using the same diamond to create precise, 1.5-mm depth reductions up the facial aspect of the tooth. Figure 3 Continuing over the incisal edge, down the lingual, and around the cervical with the same depth-reduction diamond. 10 VOL. 1, NO. 4, 2001 ESTHETIC TECHNIQUE

11 Figure 4 Depending on the size of the tooth, the small # or the large # barrel-shaped, tapered, coarse bulk-reduction diamond removes the incisal enamel. Figure 5 Using either the # or # diamond to remove the interproximal enamel. Figure 6 Removing the facial enamel down to the level of the initial depth guide with either the # or # diamond. area permits ideal adaptation of either an all-ceramic crown or a PFM crown with a large enough porcelain margin to obscure the metal. Although some clinicians may prefer a depth reduction measuring less than 1.5 mm, the maximum depth produced by the bur yields a margin of ideal thickness, particularly from the laboratory technician s perspective, because space is sufficient to develop an esthetic margin. Containing only nine instruments, the kit is designed to permit the dentist to address the esthetic requirements of anterior or posterior crown cases for patients with high or low lip lines. After the initial depth-reduction procedure, the same diamond is applied up the facial aspect of the tooth, producing an exact 1.5-mm facial trough (Figure 2). The same round depth-reduction diamond can next be used over the incisal edge, swept down onto the lingual aspect of the tooth, and then used to scribe a 1.5-mm line around the cervical of the lingual (Figure 3). The next diamond employed in this technique is either the small (# a ) or large (# a ) barrel-shaped, tapered, coarse bulk-reduction diamond. For a small tooth, such as a lateral incisor, the small barrel-shaped diamond should be selected. For a larger tooth, such as a molar or central incisor, the larger diamond is an ideal choice. First, the incisal edge (or occlusal surface for a molar) is reduced (Figure 4). Next, the same diamond removes the interproximal (Figure 5) and facial enamel (Figure 6) down to the extent of the depth grooves. Note that the coarse, coneshaped diamond is used to open tight interproximal contacts and to place bevels for extra retention. Finally, this same diamond removes the lingual wall of enamel (Figure 7). The next diamond in the sequence, the football-shaped diamond (# a ) (Figure 8), can be used to shape the lingual concavity. For all crowns, the healthiest margin that is, the least invasive is placed above the gingiva; therefore, analysis of the patient s lip line is critical whether it is high, medium, or low before undertaking tooth preparation and before the patient is anesthetized. A patient with a low lip line can have any margin including a facial collar of metal or a bevel as long as the patient understands this and accepts it. For the clinician who wishes to continue, for example, to develop a porcelain margin for either an allporcelain or PFM crown, the steps S mooth-finished, precise margins free of jagged enamel edges can be produced supragingivally or subgingivally, according to specific case requirements, enhancing the adaptation of the restoration to the tooth. described below produce an ideally smooth, polished margin with no exposed enamel prisms, thus allowing optimal adaptation of the porcelain to the preparation. SUPRAGINGIVAL MARGIN POLISHING To develop a smooth, polished supragingival margin, two smooth diamond burs that correspond in size to the coarse, barrel-shaped diamonds initially used are provided in the kit. The small, smooth, barrelshaped diamond (# a ) corresponds to the small, coarse, barrelshaped diamond (# ); the large, smooth, barrel-shaped dia- ESTHETIC TECHNIQUE VOL. 1, NO. 4,

12 Figure 7 The # or # diamond is used to create the lingual wall reduction. Figure 8 Shaping the lingual concavity with the # football diamond. Figure 9 The red smooth diamond is used to round off all preparation line angles and to refine the margins. This is the finished supragingival preparation. mond (# a ) corresponds to the larger coarse diamond (# ). The smooth diamonds round off any sharp line angles in the preparation, and they also smooth the margins. After the fine, barrel-shaped diamond has been used to smooth and round the line angles, the white stone (# a ), included in the kit, should be applied around the margin one last time to produce a polished surface. Figure 9 shows a finished supragingival preparation that is ready for impression. The burs in the crown design kit used to this point provide two types of preparations: one, a very rapid preparation for metal margins that require minimal smoothness; the other, a smooth, polished margin to meet the requirements for porcelain restorations. The instruments in the kit, however, also yield exceptional subgingival margins. SUPRAGINGIVAL PREPARATION If a subgingival margin is desired in an esthetic case involving a patient with a medium to high lip line, retraction cord (such as the purple Number 1 Ultrapak cord b, which packs dry) would be placed after the coarse barrel-shaped diamond is used. Cord packing should b Ultradent Products, Inc, South Jordan, UT 84095; begin from the midfacial surface of the preparation, and the cord would be packed circumferentially around the tooth until it abuts perfectly at the facial surface, right in the center of the tooth. For each tooth being prepared, the cord is packed very gently into the sulcus and left in place for 3 to 5 minutes, allowing the tissue to retract. Apatient with a low lip line can have any margin including a facial collar of metal or a bevel as long as the patient understands this and accepts it. With the retraction cord left in place, the coarse, barrel-shaped diamond is used to drop the margin circumferentially all the way around the tooth to the height of the retracted tissue (Figure 10). The corresponding fine, barrelshaped diamond is used to produce a smooth surface at the margin. Because the margin is extended subgingivally, the next bur used in the sequence should be the tissue-protecting-end (TPE) cutting diamond (# a ), which features diamond grit only at the very tip of the instrument (Figure 11). Because no diamond grit is on the sides of the bur, and because of its beveled configuration, the diamond-tipped end can be placed precisely on the edge of the tooth, and moved circumferentially around the margin. The beveled configuration of the diamond essentially pushes the tissue out of the way and prevents tissue laceration when the instrument is placed close to the gingiva, even when working subgingivally. The instrument is applied around the edge of the tooth to completely smooth any jagged enamel prisms. After the smoothing procedure with the TPE diamond, the white stone (# a ) is used for further finishing and polishing of the margin (Figure 12). IMPRESSION PROCEDURE To make an impression at this point, a white Number 1 GingiGel cord c is placed circumferentially around the tooth on top of the purple retraction cord (previously placed) and left in place for 3 to 5 minutes (Figure 13). The site should be washed, making certain the white cord is wet. The white cord is then removed, and the preparation is thoroughly dried and evaluated. If all margins are clearly visible, the impression c Van R Dental Inc, Oxnard, CA 93033; VOL. 1, NO. 4, 2001 ESTHETIC TECHNIQUE
, included in the kit, should be applied around the margin one last time to")
13 Figure 10 For a subgingival margin, a single-size #0 or #1 cord is placed, and the original bulk-reduction diamond is used to lower the preparation margin to the height of the retracted tissue. The margin is refined with the smooth red diamond. Figure 11 The TPE diamond, # , is used to remove any jagged enamel prisms left at the margin. Figure 12 Finally, the white stone, # , produces a fine polish to the entire margin. This key step ensures excellent marginal adaptation with the final restoration. Figure 13 The finished preparation, with two cords placed for ideal retraction. should be taken with the purple cord still in place. The purple cord should remain in place throughout the entire preparation and impression procedure because it acts as a gasket between the sulcus and the tooth, stopping crevicular flow or hemorrhage. This double-cord technique can produce a perfect impression because it eliminates any fluids at the preparation site. Because the impression extends subgingivally, the laboratory technician can perfectly visualize the margins for die trimming and provide a proper emergence angle for the final restorations. The Goldstein Crown Design Kit offers exceptional versatility in its applications, allowing the clinician to address virtually any crown preparation requirements with speed and precision. Using the instruments in the appropriate sequence produces smooth, finished margins that can be accurately recorded during impression making, thus facilitating laboratory communications and reducing the likelihood of remakes and returns. REFERENCE 1. Goldstein RE: In: Esthetics in Dentistry. London, England: Quintessence; p395, WARNING: Reading an article in Esthetic Technique does not necessarily qualify you to integrate new techniques or procedures into your practice. Dental Learning Systems expects its readers to rely on their judgment regarding their clinical expertise and recommends further education when necessary before trying to implement any new procedure. The views and opinions expressed in the article appearing in this publication are those of the author(s) and do not necessarily reflect the views or opinions of the editors, the editorial board, or the publisher. As a matter of policy, the editors, the editorial board, the publisher, and the university affiliate do not endorse any products, medical techniques, or diagnoses, and publication of any material in this journal should not be construed as such an endorsement. ESTHETIC TECHNIQUE VOL. 1, NO. 4,

14 CE QUIZ Dental Learning Systems provides 2 hours of Continuing Education credit for those who wish to document their continuing education endeavors. Participants are urged to contact their state registry boards for special CE requirements. To receive credit, complete the enclosed answer form, and mail with a check for $20, payable to Dental Learning Systems, to Dental Learning Systems CE Dept., 405 Glenn Drive, Suite 4, Sterling, VA Program #: D In situations where minimal tooth structure removal is required, what restoration is indicated? a. full crown b. three-quarters crown c. porcelain-bonded d. amalgam 2. Full-coverage crowns supported by a highstrength core should be considered in which clinical situation? a. bonding b. brittle c. feldspar d. sintering 3. In one study, 7 the failure load of bonded, pressed ceramics to materials of different elastic moduli was: a. proportional to the flexibility of the substrate. b. inversely proportional to the flexibility of the substrate. c. logarithmically proportional to the flexibility of the substrate. d. not proportional to the flexibility of the substrate. 4. A core system should be used in situations where porcelain would be subjected to: a. high shear and high tensile stresses. b. low shear and low tensile stresses. c. high shear and low tensile stresses. d. low shear and high tensile stresses. 5. How many millimeters of overall labial crown thickness was the minimum ideal dimension for predictable esthetics? a. 0.6 mm b. 1.2 mm c. 1.8 mm d. 2.4 mm 6. What was subsequently employed for the fabrication of the provisional restorations? a. matrix b. copper tube c. no provisional was used d. alginate impression 7. It is sometimes necessary to build up the tooth to the desired final shape before initiating the preparation process in order to: a. fabricate the temporary. b. check the occlusion. c. ensure pulpal clearance. d. visualize the correct amount of reduction. 8. For the marginal area of a PFM, experience has shown that what type of shoulder with rounded internal line angles is ideal for these restorations? a. 180 degrees, 1 mm b. 270 degrees, 1.5 mm c. 270 degrees, 0.5 mm d. 360 degrees, 1 mm 9. How much incisal edge reduction is adequate for good esthetics? a. 1 mm b. 1.5 mm c. 2 mm d. 2.5 mm 10. Posteriorly, it is necessary to have how much occlusal reduction? a. 2 mm b. 2.5 mm c. 3 mm d. 3.5 mm 14 VOL. 1, NO. 4, 2001 ESTHETIC TECHNIQUE

15 PREP STEPS New Instruments for Provisional Restorations Figure 1 UK cutters. Figure 2 Diamond disc. Figure 3 Vision Flex disc. Figure 4 Acrylic polisher. Figure 5 Diacomp point composite polisher. Adjusting and polishing are inevitable for any provisional restoration, whether it is composite or acrylic, laboratory-fabricated or office-made. These new Brasseler USA instruments can make adjusting temporaries faster, easier, and more precise. Trimming facial and lingual margins: The completely new blade geometry of the UK Universal tungsten carbide cutter (H ) facilitates fine shaping and contouring of tooth-colored materials. The clinician can control the desired material reduction and surface quality by varying the contact pressure high contact pressure yields high material reduction; low contact pressure yields a smooth, finished surface. New, specially staggered, UK-toothing tungsten carbide cutters are ideal for trimming facial and lingual cervical margins and facial embrasures (Figure 1). Trimming and identifying interproximal margins: The efficient and long-lasting diamond disc (6918B-220) makes interproximal cuts that define facial embrasures without tearing or folding. To prevent clogging of the diamond disc when working on composite material, it is helpful to rinse the temporary in alcohol to remove the oxygen-inhibited layer (Figure 2). Contouring interproximal forms, duplicating mamelon extensions, and personalizing provisional restorations: The new, open-meshed, diamond Vision Flex discs ( and ) help to quickly and precisely remove bulk composite and acrylic and restore perfect proximal contour. The numerous honeycombs make the finishing disc flexible without impairing its stability. A new version of this disc, the (Figure 3), has snap-on mounting with a precision-fit, quick-change sliding chuck, which stops the disc if it becomes engaged between the teeth. The and are available with a straight handpiece mandrel or slow speed for intraoral use. Polishing temporary restorations: The knife-edge acrylic polishers BRO3, BRO2, and BRO1 (Figure 4) allow the clinician to quickly restore a natural-appearing, lustrous surface. These polishers are autoclavable and, therefore, more hygienic and time-efficient than messy, wet, pumice polishing. For high-polish temporary composite restorations, use the autoclavable Diacomp points (DCH2DM and DCH2D) or Diacomp wheels (DCH8DM and DCH8M) (Figure 5). Temporization Kits are available with complete instrumentation and assembled in cooperation with several lecturing clinicians. This information is provided by Brasseler USA. ESTHETIC TECHNIQUE VOL. 1, NO. 4,
 facilitates fine shaping and contouring of tooth-colored materials.")
16
Universal Crown and Bridge Preparation
 Universal Crown and Bridge Preparation The All-Ceramic Crown Preparation Technique for Predictable Success According to Dr. Ronald E. Goldstein Expect the Best. Buy Direct. The Universal * Crown and Bridge
Universal Crown and Bridge Preparation The All-Ceramic Crown Preparation Technique for Predictable Success According to Dr. Ronald E. Goldstein Expect the Best. Buy Direct. The Universal * Crown and Bridge
Implants in your Laboratory: Abutment Design
 1/2 point CDT documented scientific credit. See Page 41. Implants in your Laboratory: Abutment Design By Leon Hermanides, CDT A patient s anatomical limitations have the greatest predictive value for successful
1/2 point CDT documented scientific credit. See Page 41. Implants in your Laboratory: Abutment Design By Leon Hermanides, CDT A patient s anatomical limitations have the greatest predictive value for successful
Full Crown Module: Learner Level 1
 Full Crown Module Restoration / Tooth # Full Gold Crown (FGC) / 30 Extensions: Porcelain Fused to Metal (PFM) / 12 All Ceramic / 8 Learner Level 1 Mastery of Tooth Preparation Estimated Set Up Time: 30
Full Crown Module Restoration / Tooth # Full Gold Crown (FGC) / 30 Extensions: Porcelain Fused to Metal (PFM) / 12 All Ceramic / 8 Learner Level 1 Mastery of Tooth Preparation Estimated Set Up Time: 30
CHAPTER 10 RESTS AND PREPARATIONS. 4. Serve as a reference point for evaluating the fit of the framework to the teeth.
 CHAPTER 10 RESTS AND DEFINITIONS A REST is any rigid part of an RPD framework which contacts a properly prepared surface of a tooth. A REST PREPARATION or REST SEAT is any portion of a tooth or restoration
CHAPTER 10 RESTS AND DEFINITIONS A REST is any rigid part of an RPD framework which contacts a properly prepared surface of a tooth. A REST PREPARATION or REST SEAT is any portion of a tooth or restoration
porcelain fused to metal crown
 Lectur.5 Dr.Adel F.Ibraheem porcelain fused to metal crown the most widely used fixed restoration,it is full metal crown having facial surface (or all surfaces) covered by ceramic material. It consist
Lectur.5 Dr.Adel F.Ibraheem porcelain fused to metal crown the most widely used fixed restoration,it is full metal crown having facial surface (or all surfaces) covered by ceramic material. It consist
How to Achieve Shade Harmony With Different Restorations
 Procera Alumina vs. Feldspathic Porcelain How to Achieve Shade Harmony With Different Restorations Luke S. Kahng, CDT Key Words: Stump shade, Feldspathic Porcelain, Zirconia, Alumina, LSK Treatment Plan
Procera Alumina vs. Feldspathic Porcelain How to Achieve Shade Harmony With Different Restorations Luke S. Kahng, CDT Key Words: Stump shade, Feldspathic Porcelain, Zirconia, Alumina, LSK Treatment Plan
WAX-UP AND CERAMIC EXTENSIVE COURSE Dr. Dario Adolfi Dr. Ivan Ronald Huanca
 WAX-UP AND CERAMIC EXTENSIVE COURSE Dr. Dario Adolfi Dr. Ivan Ronald Huanca Duration: 6 meses STEP 1: WAX-UP OF FOUR UPPER POSTERIOR TEETH with Dr. Ivan Ronald Huanca The objective of this course s step
WAX-UP AND CERAMIC EXTENSIVE COURSE Dr. Dario Adolfi Dr. Ivan Ronald Huanca Duration: 6 meses STEP 1: WAX-UP OF FOUR UPPER POSTERIOR TEETH with Dr. Ivan Ronald Huanca The objective of this course s step
Jacket crown. Advantage : Crown and Bridge
 Crown and Bridge Lecture 1 Dr.Nibras AL-Kuraine Jacket crown It is a type of crown that is formed by a tooth colored material. It is mainly used as a single unit in the anterior quadrant of the mouth.
Crown and Bridge Lecture 1 Dr.Nibras AL-Kuraine Jacket crown It is a type of crown that is formed by a tooth colored material. It is mainly used as a single unit in the anterior quadrant of the mouth.
Class I and II Indirect Tooth-Colored Restorations
 Class I and II Indirect Tooth-Colored Restorations Most indirect restorations are made on a replica of the prepared tooth in a dental laboratory by a trained technician. Tooth-colored indirect systems
Class I and II Indirect Tooth-Colored Restorations Most indirect restorations are made on a replica of the prepared tooth in a dental laboratory by a trained technician. Tooth-colored indirect systems
ATLANTIS abutments design guide CAD/CAM patient-specific abutments
 ATLANTIS abutments design guide CAD/CAM patient-specific abutments Contents Introduction 4 This manual helps you to explore all the benefits of ATLANTIS CAD/CAM patient-specific abutments. It gives you
ATLANTIS abutments design guide CAD/CAM patient-specific abutments Contents Introduction 4 This manual helps you to explore all the benefits of ATLANTIS CAD/CAM patient-specific abutments. It gives you
Implant Replacement of the Maxillary Central Incisor Utilizing a Modified Ceramic Abutment (Thommen SPI ART) and Ceramic Restoration
 and Ceramic Restoration") Implant Replacement of the Maxillary Central Incisor Utilizing a Modified Ceramic Abutment (Thommen SPI ART) and Ceramic Restoration ROBERT SCHNEIDER, DDS, MS* ABSTRACT The prosthetic restoration of a
Implant Replacement of the Maxillary Central Incisor Utilizing a Modified Ceramic Abutment (Thommen SPI ART) and Ceramic Restoration ROBERT SCHNEIDER, DDS, MS* ABSTRACT The prosthetic restoration of a
Tooth preparation J. C. Davenport, 1 R. M. Basker, 2 J. R. Heath, 3 J. P. Ralph, 4 P-O. Glantz, 5 and P. Hammond, 6
 12 5 Tooth preparation J. C. Davenport, 1 R. M. Basker, 2 J. R. Heath, 3 J. P. Ralph, 4 P-O. Glantz, 5 and P. Hammond, 6 This final article in the series describes the modification of teeth to improve
12 5 Tooth preparation J. C. Davenport, 1 R. M. Basker, 2 J. R. Heath, 3 J. P. Ralph, 4 P-O. Glantz, 5 and P. Hammond, 6 This final article in the series describes the modification of teeth to improve
Composite artistry- speedy mock up
 Case Report: Composite artistry- speedy mock up Dr.Shikha Kanodia*, Dr.Manjit Kaur**, Dr.Girish J. Parmar*** * Asst. Professor, **Post Graduate Part 3, ***Head and Dean, Department of Conservative Dentistry
Case Report: Composite artistry- speedy mock up Dr.Shikha Kanodia*, Dr.Manjit Kaur**, Dr.Girish J. Parmar*** * Asst. Professor, **Post Graduate Part 3, ***Head and Dean, Department of Conservative Dentistry
Another Implant Option for Missing Teeth with Challenging Symmetry Patrick Gannon, DDS and Luke Kahng, CDT
 Another Implant Option for Missing Teeth with Challenging Symmetry Patrick Gannon, DDS and Luke Kahng, CDT Introduction A 58 year old male had been missing teeth #7=12 for approximately 28 years. During
Another Implant Option for Missing Teeth with Challenging Symmetry Patrick Gannon, DDS and Luke Kahng, CDT Introduction A 58 year old male had been missing teeth #7=12 for approximately 28 years. During
CLASSIFICATION OF CARIOUS LESIONS AND TOOTH PREPARATION.
 CLASSIFICATION OF CARIOUS LESIONS AND TOOTH PREPARATION. ١ G.V. BLACK who is known as the father of operative dentistry,he classified carious lesions into groups according to their locations in permanent
CLASSIFICATION OF CARIOUS LESIONS AND TOOTH PREPARATION. ١ G.V. BLACK who is known as the father of operative dentistry,he classified carious lesions into groups according to their locations in permanent
Replacement of the upper left central incisor with a Straumann Bone Level Implant and a Straumann Customized Ceramic Abutment
 Replacement of the upper left central incisor with a Straumann Bone Level Implant and a Straumann Customized Ceramic Abutment by Dr. Ronald Jung and Master Dental Technician Xavier Zahno Initial situation
Replacement of the upper left central incisor with a Straumann Bone Level Implant and a Straumann Customized Ceramic Abutment by Dr. Ronald Jung and Master Dental Technician Xavier Zahno Initial situation
priti crown Your patients deserve you
 priti crown Your patients deserve you 3 and you deserve the priti crown So close to nature priti crown is a high-tech solution for making perfect crown and bridge restorations using state-of-the-art CAD/CAM
priti crown Your patients deserve you 3 and you deserve the priti crown So close to nature priti crown is a high-tech solution for making perfect crown and bridge restorations using state-of-the-art CAD/CAM
FABRICATING CUSTOM ABUTMENTS
 FABRICATING CUSTOM ABUTMENTS LUC AND PATRICK RUTTEN How much should a Dental Technician know about the clinical aspects of implantology? The answer is clear: as much as possible. This is the distinction
FABRICATING CUSTOM ABUTMENTS LUC AND PATRICK RUTTEN How much should a Dental Technician know about the clinical aspects of implantology? The answer is clear: as much as possible. This is the distinction
Restorative Guidelines
 Restorative Guidelines Contents Restorative Guidelines 4.1 Neoss Implant System 4.2 4.2 Esthetiline Solution 4.3 4.3 Provisional Abutments 4.8 4.4 Impression Techniques Implant Level 4.12 4.5 NeoLink
Restorative Guidelines Contents Restorative Guidelines 4.1 Neoss Implant System 4.2 4.2 Esthetiline Solution 4.3 4.3 Provisional Abutments 4.8 4.4 Impression Techniques Implant Level 4.12 4.5 NeoLink
Clinical and Laboratory Procedures for Fixed Margin Implant Abutments
 Clinical and Laboratory Procedures for Fixed Margin Implant Abutments Dr. Carl Drago DDS, MS, American Board of Prosthodontics Director, Dental Research BIOMET 3i, Adjunct Faculty Department of Prosthodontics,
Clinical and Laboratory Procedures for Fixed Margin Implant Abutments Dr. Carl Drago DDS, MS, American Board of Prosthodontics Director, Dental Research BIOMET 3i, Adjunct Faculty Department of Prosthodontics,
PROSTHETIC PROCEDURE. for HG IMPLANT SYSTEM
 PROSTHETIC PROCEDURE for HG IMPLANT SYSTEM PROSTHETIC PROCEDURE for HG IMPLANT SYSTEM HG Implant System Contents Cement retained restoration Rigid abutment When abutment reduction is unnecessary When abutment
PROSTHETIC PROCEDURE for HG IMPLANT SYSTEM PROSTHETIC PROCEDURE for HG IMPLANT SYSTEM HG Implant System Contents Cement retained restoration Rigid abutment When abutment reduction is unnecessary When abutment
Chapter 8--Fixed Prosthodontics
 Overview Introduction --Fixed Prosthodontics Many excellent crown and bridge tests and courses are available, with some of them expressing seemingly contradictory opinions and approaches. This chapter
Overview Introduction --Fixed Prosthodontics Many excellent crown and bridge tests and courses are available, with some of them expressing seemingly contradictory opinions and approaches. This chapter
American Academy of Cosmetic Dentistry. Laboratory Technician Clinical Case Type II. One or Two Indirect Restorations
 American Academy of Cosmetic Dentistry Laboratory Technician Clinical Case Type II One or Two Indirect Restorations AACD Member ID # 00000 EXAMPLE REPORT Treatment List #8, #9 All Ceramic Crowns Restorative
American Academy of Cosmetic Dentistry Laboratory Technician Clinical Case Type II One or Two Indirect Restorations AACD Member ID # 00000 EXAMPLE REPORT Treatment List #8, #9 All Ceramic Crowns Restorative
by Stephen M. Phelan, DDS, AAACD
 Co n s e r vat i v e Po r c e l a i n Veneer Te c h n i q u e s Guided By Three Different Preparation Stents Restorative Dentistry by Stephen M. Phelan, DDS, AAACD Oakville, ON, Canada www.smiletoremember.com
Co n s e r vat i v e Po r c e l a i n Veneer Te c h n i q u e s Guided By Three Different Preparation Stents Restorative Dentistry by Stephen M. Phelan, DDS, AAACD Oakville, ON, Canada www.smiletoremember.com
Removing fixed prostheses using the ATD automatic crown and bridge remover
 Removing fixed prostheses using the ATD automatic crown and bridge remover By Dr. Ian E. Shuman, Baltimore, MD. Information provided by J. Morita USA When removing cemented provisionals and final fixed
Removing fixed prostheses using the ATD automatic crown and bridge remover By Dr. Ian E. Shuman, Baltimore, MD. Information provided by J. Morita USA When removing cemented provisionals and final fixed
CUSTOMIZED PROVISIONAL ABUTMENT AND PROVISIONAL RESTORATION FOR AN IMMEDIATELY-PLACED IMPLANT
 CONTINUING EDUCATION 1 4 CUSTOMIZED PROVISIONAL ABUTMENT AND PROVISIONAL RESTORATION FOR AN IMMEDIATELY-PLACED IMPLANT Gerard J. Lemongello, Jr, DMD* LEMONGELLO 19 7 AUGUST The use of immediate implant
CONTINUING EDUCATION 1 4 CUSTOMIZED PROVISIONAL ABUTMENT AND PROVISIONAL RESTORATION FOR AN IMMEDIATELY-PLACED IMPLANT Gerard J. Lemongello, Jr, DMD* LEMONGELLO 19 7 AUGUST The use of immediate implant
portion of the tooth such as 3/4 Crown, 7/8Crown.
 Lecture.1 Dr.Adel F.Ibraheem Crown and Bridge: It s a branch of dental science that deals with restoration of damaged teeth with artificial crown replacing the missing natural teeth by a cast prosthesis
Lecture.1 Dr.Adel F.Ibraheem Crown and Bridge: It s a branch of dental science that deals with restoration of damaged teeth with artificial crown replacing the missing natural teeth by a cast prosthesis
Accurate Transfer of Peri-implant Soft Tissue Emergence Profile from the Provisional Crown to the Final Prosthesis Using an Emergence Profile Cast
 ccurate Transfer of Peri-implant Soft Tissue Emergence Profile from the Provisional Crown to the Final Prosthesis Using an Emergence Profile Cast NICOLS ELIN, DDS* GERRD TOURIN, DDS, MS ZID N. JLOUT, DDS
ccurate Transfer of Peri-implant Soft Tissue Emergence Profile from the Provisional Crown to the Final Prosthesis Using an Emergence Profile Cast NICOLS ELIN, DDS* GERRD TOURIN, DDS, MS ZID N. JLOUT, DDS
Prosthetic Manual. Implant System. Contact Us: Smarter thinking. Simpler design. Phone: 866-902-9272 781-328-3490. Fax: 866-903-9272 781-328-3400
 Contact Us: Implant System Phone: 866-902-9272 781-328-3490 Fax: 866-903-9272 781-328-3400 Prosthetic Manual Mail: Keystone Dental, Inc. 144 Middlesex Turnpike Burlington, MA 01803 USA www.keystonedental.com
Contact Us: Implant System Phone: 866-902-9272 781-328-3490 Fax: 866-903-9272 781-328-3400 Prosthetic Manual Mail: Keystone Dental, Inc. 144 Middlesex Turnpike Burlington, MA 01803 USA www.keystonedental.com
Zirconium Abutments for Improved Esthetics in Anterior Restorations
 Zirconium Abutments for Improved Esthetics in Anterior Restorations by Luke S., C.D.T. Mr. is the founder and owner of Capital Dental Technology Laboratory, Inc., in Naperville, Illinois. The laboratory
Zirconium Abutments for Improved Esthetics in Anterior Restorations by Luke S., C.D.T. Mr. is the founder and owner of Capital Dental Technology Laboratory, Inc., in Naperville, Illinois. The laboratory
Taking the Mystique out of Implant Dentistry. Dr. Michael Weinberg B.Sc., DDS, FICOI
 Taking the Mystique out of Implant Dentistry Dr. Michael Weinberg B.Sc., DDS, FICOI What is Restorative Implant Dentistry? Restorative implant dentistry involves taking a few simple mechanical principles
Taking the Mystique out of Implant Dentistry Dr. Michael Weinberg B.Sc., DDS, FICOI What is Restorative Implant Dentistry? Restorative implant dentistry involves taking a few simple mechanical principles
Nobel Clinician - Quick Guide
 1220 E. Birch St. #201 Brea, CA 92821 (800)750-5004 Haupt Dental Lab Inc. Nobel Clinician - Quick Guide Step #1 - Diagnostics Make impressions of both the upper and lower arches using custom trays. Care
1220 E. Birch St. #201 Brea, CA 92821 (800)750-5004 Haupt Dental Lab Inc. Nobel Clinician - Quick Guide Step #1 - Diagnostics Make impressions of both the upper and lower arches using custom trays. Care
CLASS II AMALGAM. Design Principles
 CLASS II AMALGAM Design Principles CLASS II Class II cavitated caries lesions Class II cavitated caries lesions opaque white haloes identify areas of enamel undermining and decalcification from within
CLASS II AMALGAM Design Principles CLASS II Class II cavitated caries lesions Class II cavitated caries lesions opaque white haloes identify areas of enamel undermining and decalcification from within
Anterior crowns used in children
 Anterior crowns used in children Objectives of this session Discuss strip crowns, temporary crown use and acrylic jacket crowns. Discuss the possible use of porcelain jacket crowns in paediatric dental
Anterior crowns used in children Objectives of this session Discuss strip crowns, temporary crown use and acrylic jacket crowns. Discuss the possible use of porcelain jacket crowns in paediatric dental
Prosthodontist s Perspective
 Unless otherwise noted, the content of this course material is licensed under a Creative Commons Attribution - Non-Commercial - Share Alike 3.0 License. Copyright 2008, Dr. Jeff Shotwell. The following
Unless otherwise noted, the content of this course material is licensed under a Creative Commons Attribution - Non-Commercial - Share Alike 3.0 License. Copyright 2008, Dr. Jeff Shotwell. The following
In the Spring of 2010, the American Academy of Cosmetic
 Greetings to the members of the American Academy of Cosmetic Dentistry (AACD). As you know, a sisterhood agreement was concluded between the AACD and the Japan Academy of Esthetic Dentistry (JAED) at a
Greetings to the members of the American Academy of Cosmetic Dentistry (AACD). As you know, a sisterhood agreement was concluded between the AACD and the Japan Academy of Esthetic Dentistry (JAED) at a
Advances in All Ceramic Restorations. Alaa AlQutub Umm AlQura University, Faculty of Dentistry
 Advances in All Ceramic Restorations Alaa AlQutub Umm AlQura University, Faculty of Dentistry Types of materials used in esthetic zone I. Metal ceramic restoration: Metal ceramic alloy features : Produce
Advances in All Ceramic Restorations Alaa AlQutub Umm AlQura University, Faculty of Dentistry Types of materials used in esthetic zone I. Metal ceramic restoration: Metal ceramic alloy features : Produce
Porcelain Veneers for Children and Teens. By Fred S. Margolis, D.D.S., F.I.C.D., F.A.C.D., F.A.D.I. Abstract
 Porcelain Veneers for Children and Teens By Fred S. Margolis, D.D.S., F.I.C.D., F.A.C.D., F.A.D.I. Abstract This article will discuss the advantages of providing our young patients and their parents an
Porcelain Veneers for Children and Teens By Fred S. Margolis, D.D.S., F.I.C.D., F.A.C.D., F.A.D.I. Abstract This article will discuss the advantages of providing our young patients and their parents an
ATLANTIS abutments as individual as your patients
 ATLANTIS abutments as individual as your patients ATLANTIS the freedom of unlimited possibilities Discover why ATLANTIS CAD/CAM abutments are the natural choice for patientspecific, cement-retained implant
ATLANTIS abutments as individual as your patients ATLANTIS the freedom of unlimited possibilities Discover why ATLANTIS CAD/CAM abutments are the natural choice for patientspecific, cement-retained implant
IMMEDIATE CUSTOM IMPLANT PROVISIONALIZATION: A PROSTHETIC TECHNIQUE
 IMMEDIATE CUSTOM IMPLANT PROVISIONALIZATION: A PROSTHETIC TECHNIQUE Gerard J. Lemongello, Jr, DMD* LEMONGELLO 19 5 JUNE Surgical and restorative techniques that can reduce the loss of hard and soft tissues
IMMEDIATE CUSTOM IMPLANT PROVISIONALIZATION: A PROSTHETIC TECHNIQUE Gerard J. Lemongello, Jr, DMD* LEMONGELLO 19 5 JUNE Surgical and restorative techniques that can reduce the loss of hard and soft tissues
IPS. Special Edition. Press-on-Metal Ceramic. Harald Gritsch Max Wörishofer Christoph Zobler
 InLine PoM Press-on-Metal Ceramic IPS Special Edition Harald Gritsch Max Wörishofer Christoph Zobler Press-on technique on metal frameworks Combining the widely known casting technique and press technique
InLine PoM Press-on-Metal Ceramic IPS Special Edition Harald Gritsch Max Wörishofer Christoph Zobler Press-on technique on metal frameworks Combining the widely known casting technique and press technique
your talent. our technology. the perfect fit.
 your talent. our technology. the perfect fit. itero - exclusively distributed in Europe by The digital revolution Changing the Face of Dentistry Digital technology ensures a more accurate impression from
your talent. our technology. the perfect fit. itero - exclusively distributed in Europe by The digital revolution Changing the Face of Dentistry Digital technology ensures a more accurate impression from
In 1999, more than 1 million people in
 Clinical SHOWCASE Slip-and-Fall Injuries Causing Dental Trauma Morley S. Rubinoff, DDS, Cert Prosth Clinical Showcase is a series of pictorial essays that focus on the technical art of clinical dentistry.
Clinical SHOWCASE Slip-and-Fall Injuries Causing Dental Trauma Morley S. Rubinoff, DDS, Cert Prosth Clinical Showcase is a series of pictorial essays that focus on the technical art of clinical dentistry.
ADA Insurance Codes for Laboratory Procedures:
 ADA Insurance Codes for Laboratory Procedures: Inlay/Onlay Restorations D2510 Inlay - metallic - one surface D2520 Inlay - metallic - two surfaces D2530 Inlay - metallic - three or more surfaces D2542
ADA Insurance Codes for Laboratory Procedures: Inlay/Onlay Restorations D2510 Inlay - metallic - one surface D2520 Inlay - metallic - two surfaces D2530 Inlay - metallic - three or more surfaces D2542
Structur. Structur 2 SC / Structur Premium EXCELLENT TEMPORARIES WITH STRUCTUR
 Structur Structur 2 SC / Structur Premium EXCELLENT TEMPORARIES WITH STRUCTUR Simple to use Reliable products are required to provide your patients with prosthetic treatments, especially with regard to
Structur Structur 2 SC / Structur Premium EXCELLENT TEMPORARIES WITH STRUCTUR Simple to use Reliable products are required to provide your patients with prosthetic treatments, especially with regard to
Increasing. VDO and the Use of CAD/CAM. Prosthodontic Principles and the Full-Mouth Reconstruction. 86 Summer 2013 Volume 29 Number 2
 Increasing VDO and the Use of CAD/CAM Prosthodontic Principles and the Full-Mouth Reconstruction Jonathan L. Ferencz, DDS, FACP Abstract This article describes the treatment of a young adult female with
Increasing VDO and the Use of CAD/CAM Prosthodontic Principles and the Full-Mouth Reconstruction Jonathan L. Ferencz, DDS, FACP Abstract This article describes the treatment of a young adult female with
Projecting a new smile from a facial photograph:
 I special _ digital smile design Projecting a new smile from a facial photograph: A new way to plan multidisciplinarydental treatments Authors_ Drs Marco Del Corso, Italy, & Alain Méthot, Canada without
I special _ digital smile design Projecting a new smile from a facial photograph: A new way to plan multidisciplinarydental treatments Authors_ Drs Marco Del Corso, Italy, & Alain Méthot, Canada without
Taking a Custom Shade, Step by Step: A Technician s Viewpoint
 Members Pearls Taking a Custom Shade, Step by Step: A Technician s Viewpoint Ka h n g by Luke S. Khang, C.D.T. Naperville, IL [email protected] In t r o d u c t i o n Have you ever struggled with the selection
Members Pearls Taking a Custom Shade, Step by Step: A Technician s Viewpoint Ka h n g by Luke S. Khang, C.D.T. Naperville, IL [email protected] In t r o d u c t i o n Have you ever struggled with the selection
Many roads lead to a perfect impression...
 Comprecord Stay-put Tissue Contouring System Magic FoamCord Retracto Many roads lead to a perfect impression... with the Gingiva Management System from Coltène/Whaledent The Gingiva Management System lays
Comprecord Stay-put Tissue Contouring System Magic FoamCord Retracto Many roads lead to a perfect impression... with the Gingiva Management System from Coltène/Whaledent The Gingiva Management System lays
In contemporary restorative dentistry, there are several ways
 Case Report Hybrid Combination REStoRAtion Vonlays: A Conservative Esthetic Alternative to Full-Coverage Crowns Edward A. McLaren, DDS, MDC; Johan Figueira, DDS; and Ronald E. Goldstein, DDS Abstract:
Case Report Hybrid Combination REStoRAtion Vonlays: A Conservative Esthetic Alternative to Full-Coverage Crowns Edward A. McLaren, DDS, MDC; Johan Figueira, DDS; and Ronald E. Goldstein, DDS Abstract:
Press Abutment Solutions
 Press Abutment Solutions Efficiency and esthetics redefined all ceramic all you need More press ceramic options... Press ceramics have been synonymous with the ideal combination of accuracy of fit, shape
Press Abutment Solutions Efficiency and esthetics redefined all ceramic all you need More press ceramic options... Press ceramics have been synonymous with the ideal combination of accuracy of fit, shape
Treatment planning for the class 0, 1A, 1B dental arches
 Treatment planning for the class 0, 1A, 1B dental arches Dr.. Peter Hermann Dr Reminder: Torquing movement on tooth supported denture : no movement Class 1 movement in one direction (depression) Class
Treatment planning for the class 0, 1A, 1B dental arches Dr.. Peter Hermann Dr Reminder: Torquing movement on tooth supported denture : no movement Class 1 movement in one direction (depression) Class
Renaissance of One-Piece Implants
 2 EDI Minimally invasive and patient-friendly treatment concepts using one-piece implants Renaissance of One-Piece Implants Hannes Thurm-Meyer, dentist, Bremen, Germany, Thomas Horn, master dental technician,
2 EDI Minimally invasive and patient-friendly treatment concepts using one-piece implants Renaissance of One-Piece Implants Hannes Thurm-Meyer, dentist, Bremen, Germany, Thomas Horn, master dental technician,
Dentist and Lab Communication: Key to better Restorations.
 Dentist and Lab Communication: Key to better Restorations. 1 Dr. Ajit S. Jankar, 2 Dr. yogesh J.Kale Abstract: Dental professionals must consider the health of surrounding soft tissues, reproduce the size,
Dentist and Lab Communication: Key to better Restorations. 1 Dr. Ajit S. Jankar, 2 Dr. yogesh J.Kale Abstract: Dental professionals must consider the health of surrounding soft tissues, reproduce the size,
In the past decade, there has been a remarkable
 TECHNO BYTES Principles of cosmetic dentistry in orthodontics: Part 1. Shape and proportionality of anterior teeth David M. Sarver, DMD, MS Vestavia Hills, Ala In the past decade, there has been a remarkable
TECHNO BYTES Principles of cosmetic dentistry in orthodontics: Part 1. Shape and proportionality of anterior teeth David M. Sarver, DMD, MS Vestavia Hills, Ala In the past decade, there has been a remarkable
The course of time in dental morphology
 The course of time in dental morphology Author_ Daniele Rondoni, Italy Figs. 1 3_Pressure die cast ceramic. The restoration must be perfectly integrated both morphologically and chromatically. The perfect
The course of time in dental morphology Author_ Daniele Rondoni, Italy Figs. 1 3_Pressure die cast ceramic. The restoration must be perfectly integrated both morphologically and chromatically. The perfect
Dental Updates. Excerpted Article e-mail: [email protected]. Why Implant Screws Loosen Part 1. Richard Erickson, MS, DDS
 ¼ ½ ¾ µ mw/cm 2 Volume 17; 2007 Dental Updates "CUTTING EDGE INFORMATION FOR THE DENTAL PROFESSIONAL " 200 SEMINARS AND 30 JOURNALS REVIEWED YEARLY FOR THE LATEST, CUTTING EDGE INFORMATION Excerpted Article
¼ ½ ¾ µ mw/cm 2 Volume 17; 2007 Dental Updates "CUTTING EDGE INFORMATION FOR THE DENTAL PROFESSIONAL " 200 SEMINARS AND 30 JOURNALS REVIEWED YEARLY FOR THE LATEST, CUTTING EDGE INFORMATION Excerpted Article
Do s and Don ts of Porcelain Laminate Veneers
 Do s and Don ts of Porcelain Laminate Veneers Chad J. Anderson, MS, DMD; Gerard Kugel, DMD, MS, PhD; Shradha Sharma, BDS, DMD Continuing Education Units: 2 hours Online Course: www.dentalcare.com/en-us/dental-education/continuing-education/ce333/ce333.aspx
Do s and Don ts of Porcelain Laminate Veneers Chad J. Anderson, MS, DMD; Gerard Kugel, DMD, MS, PhD; Shradha Sharma, BDS, DMD Continuing Education Units: 2 hours Online Course: www.dentalcare.com/en-us/dental-education/continuing-education/ce333/ce333.aspx
Indirect Ceramic Restorations, Hands-on Course
 Indirect Ceramic Restorations, Hands-on Course October 22, 2016 Guest Lecturer John West, DDS, MSD Presented by Augusta University (formerly: Georgia Regents University) Department of Oral Rehabilitation
Indirect Ceramic Restorations, Hands-on Course October 22, 2016 Guest Lecturer John West, DDS, MSD Presented by Augusta University (formerly: Georgia Regents University) Department of Oral Rehabilitation
Flexible dentures an alternate for rigid dentures? Volume 1 Issue 1
 Flexible dentures an alternate for rigid dentures? Dr. Sunitha N Shamnur 1, Dr. Jagadeesh KN 1, Dr. Kalavathi SD 1, Dr. Kashinath KR 2 1 Senior Lecturer, 2 Professor & Head, Department of Prosthodontics,
Flexible dentures an alternate for rigid dentures? Dr. Sunitha N Shamnur 1, Dr. Jagadeesh KN 1, Dr. Kalavathi SD 1, Dr. Kashinath KR 2 1 Senior Lecturer, 2 Professor & Head, Department of Prosthodontics,
Use of variable torque brackets to enhance treatment outcomes
 Use of variable torque brackets to enhance treatment outcomes Ralph Nicassio DDS Many clinicians performing Orthodontics for their patients are missing an opportunity to get better results because they
Use of variable torque brackets to enhance treatment outcomes Ralph Nicassio DDS Many clinicians performing Orthodontics for their patients are missing an opportunity to get better results because they
Removable Partial Dentures 101 Back to the Basics. Luther A. Ison, CDT University of Minnesota School of Dentistry
 Removable Partial Dentures 101 Back to the Basics Luther A. Ison, CDT University of Minnesota School of Dentistry Anterior-Posterior Palatal Strap Major connector Lingual Bar Major Connector, Kennedy Class
Removable Partial Dentures 101 Back to the Basics Luther A. Ison, CDT University of Minnesota School of Dentistry Anterior-Posterior Palatal Strap Major connector Lingual Bar Major Connector, Kennedy Class
THE VOICE OF TECHNO-CLINICAL DENTISTRY
 May 2009 Vol. 3, No. 2 THE VOICE OF TECHNO-CLINICAL DENTISTRY The Enhanced Restoration of Removables Jim Collis, CDT Patients with existing full or partial dentures often report that they would like to
May 2009 Vol. 3, No. 2 THE VOICE OF TECHNO-CLINICAL DENTISTRY The Enhanced Restoration of Removables Jim Collis, CDT Patients with existing full or partial dentures often report that they would like to
PROSTHETICS. Crown and bridge restorations with the synocta prosthetic system. www.straumann.com
 PROSTHETICS Crown and bridge restorations with the synocta prosthetic system www.straumann.com Straumann is the exclusive industrial partner of the ITI (International Team for Implantology) in the areas
PROSTHETICS Crown and bridge restorations with the synocta prosthetic system www.straumann.com Straumann is the exclusive industrial partner of the ITI (International Team for Implantology) in the areas
The Successful Crown Delivery
 The Successful Crown Delivery Understanding Occlusal and Contact Problems in Crown and Bridge Robert R. Cowie, DDS, FAGD 1/2 point CDT or RG documented scientiþc credit. See Page 44. 38 hen I talk with
The Successful Crown Delivery Understanding Occlusal and Contact Problems in Crown and Bridge Robert R. Cowie, DDS, FAGD 1/2 point CDT or RG documented scientiþc credit. See Page 44. 38 hen I talk with
STEP-BY-STEP INSTRUCTIONS ON THE PROSTHETIC PROCEDURES. Straumann Anatomic IPS e.max Abutment
 STEP-BY-STEP INSTRUCTIONS ON THE PROSTHETIC PROCEDURES Straumann Anatomic IPS e.max Abutment The ITI (International Team for Implantology) is academic partner of Institut Straumann in the areas of research
STEP-BY-STEP INSTRUCTIONS ON THE PROSTHETIC PROCEDURES Straumann Anatomic IPS e.max Abutment The ITI (International Team for Implantology) is academic partner of Institut Straumann in the areas of research
HEALTH SERVICES POLICY & PROCEDURE MANUAL. SUBJECT: Types of Dental Treatments Provided EFFECTIVE DATE: July 2014 SUPERCEDES DATE: January 2014
 PAGE 1 of 5 References Related ACA Standards 4 th Edition Standards for Adult Correctional Institutions 4-4369, 4-4375 PURPOSE To provide guidelines for determining appropriate levels of care and types
PAGE 1 of 5 References Related ACA Standards 4 th Edition Standards for Adult Correctional Institutions 4-4369, 4-4375 PURPOSE To provide guidelines for determining appropriate levels of care and types
Implant Abutments and Crowns on your CEREC. Welcome
 Welcome Welcome Welcome Robert Marcus D.M.D. UConn Dental 1993 Poway (SD) office since 1997 CEREC user since 2004 CEREC Mentor and Trainer Founder of Kick Your Apps, Inc. Control Freak Welcome Many thanks
Welcome Welcome Welcome Robert Marcus D.M.D. UConn Dental 1993 Poway (SD) office since 1997 CEREC user since 2004 CEREC Mentor and Trainer Founder of Kick Your Apps, Inc. Control Freak Welcome Many thanks
Encode Restorative System Procedure & Laboratory Manual
 Procedure & Laboratory Manual Encode Virtual Abutment Encode Abutment Blank Encode Abutment 1/2 Milled Encode Abutment Completed ENCODE RESTORATIVE SYSTEM Simply Impressive With the introduction of the
Procedure & Laboratory Manual Encode Virtual Abutment Encode Abutment Blank Encode Abutment 1/2 Milled Encode Abutment Completed ENCODE RESTORATIVE SYSTEM Simply Impressive With the introduction of the
by Michael J. Morgan, DDS
 Ex t r e m e Class IV Co m p o s i t e s: Th e Ne x t Best Thing to Cloning Restorative Dentistry by Michael J. Morgan, DDS Hinsdale, IL www.smilesbymorgan.com Ab s t r ac t The restoration of a large
Ex t r e m e Class IV Co m p o s i t e s: Th e Ne x t Best Thing to Cloning Restorative Dentistry by Michael J. Morgan, DDS Hinsdale, IL www.smilesbymorgan.com Ab s t r ac t The restoration of a large
Contents. Cement retained restoration. Screw retained restoration. Overdenture retained restoration. TS Implant System. 70 ComOcta Gold Abutment
 Contents TS Implant System Cement retained restoration Screw retained restoration 06 Cement-retained bridges with the Solid abutment system (non- 72 Screw retained crown with the ComOcta Gold abutment
Contents TS Implant System Cement retained restoration Screw retained restoration 06 Cement-retained bridges with the Solid abutment system (non- 72 Screw retained crown with the ComOcta Gold abutment
Chart 1. Chart 2. How to Use the Following Charts. Be sure to follow the legal requirements to perform dental radiographic procedures.
 These data are presented for informational purposes only and are not intended as a legal opinion regarding dental practice in any state. DANB confers with each state s dental board at least annually regarding
These data are presented for informational purposes only and are not intended as a legal opinion regarding dental practice in any state. DANB confers with each state s dental board at least annually regarding
62 Fall 2011 Volume 27 Number 3
 62 Fall 2011 Volume 27 Number 3 Ruiz/Christensen s vs. Realities State-of-the-Art Indirect Posterior Tooth-Colored Restorations Jose-Luis Ruiz, DDS Gordon J. Christensen, DDS, MSD, PhD The time of the
62 Fall 2011 Volume 27 Number 3 Ruiz/Christensen s vs. Realities State-of-the-Art Indirect Posterior Tooth-Colored Restorations Jose-Luis Ruiz, DDS Gordon J. Christensen, DDS, MSD, PhD The time of the
Ideal treatment of the impaired
 RESEARCH IMPLANTS AS ANCHORAGE IN ORTHODONTICS: ACLINICAL CASE REPORT Dale B. Herrero, DDS KEY WORDS External anchorage Pneumatized Often, in dental reconstruction, orthodontics is required for either
RESEARCH IMPLANTS AS ANCHORAGE IN ORTHODONTICS: ACLINICAL CASE REPORT Dale B. Herrero, DDS KEY WORDS External anchorage Pneumatized Often, in dental reconstruction, orthodontics is required for either
Improving your margins
 Clinical Improving your margins Philip Newsome and Siobhan Owen A restoration s margin marks the transition between the restoration itself and the finishing line of the adjacent tooth tissue. This is a
Clinical Improving your margins Philip Newsome and Siobhan Owen A restoration s margin marks the transition between the restoration itself and the finishing line of the adjacent tooth tissue. This is a
More than a fixed rehabilitation.
 More than a fixed rehabilitation. A reason to smile. In combination with: Patient expectations drive dental treatments for fixed edentulous immediate restorations. Patients today have increasingly high
More than a fixed rehabilitation. A reason to smile. In combination with: Patient expectations drive dental treatments for fixed edentulous immediate restorations. Patients today have increasingly high
A Review of Implant Abutments - Abutment Classification to Aid Prosthetic Selection
 A Review of Implant Abutments - Abutment Classification to Aid Prosthetic Selection Sanjay Karunagaran, B.D.S., D.D.S., M.S.D., Gregory J. Paprocki, D.D.S., Russell Wicks, D.D.S., M.S., Sony Markose, B.D.S.,
A Review of Implant Abutments - Abutment Classification to Aid Prosthetic Selection Sanjay Karunagaran, B.D.S., D.D.S., M.S.D., Gregory J. Paprocki, D.D.S., Russell Wicks, D.D.S., M.S., Sony Markose, B.D.S.,
Mail to: Mona Fine OR Fax to (585) 273-1235. Business Phone ( )... Fax ( )...
 273-1235. Business Phone ( )... Fax ( )...") Eastman Institute for Oral Health 2016 Continuing Dental Education Registration Mail to: Mona Fine OR Fax to (585) 273-1235 Eastman Institute for Oral Health OR Email to [email protected] Box
Eastman Institute for Oral Health 2016 Continuing Dental Education Registration Mail to: Mona Fine OR Fax to (585) 273-1235 Eastman Institute for Oral Health OR Email to [email protected] Box
One Abutment - One Time
 One Abutment - One Time A new treatment concept simple, innovative, easy to implement. Something so simple that does so much. What makes One Abutment - One Time a favorite among clinicians and patients
One Abutment - One Time A new treatment concept simple, innovative, easy to implement. Something so simple that does so much. What makes One Abutment - One Time a favorite among clinicians and patients
One of the hottest topics in the dental industry is the debate about which
 Pressed Ceramics Versus Layered Feldspathic Veneers: A Rationale for Modality Selection by John Haupt, M.D.T. John Haupt is the founder and president of Haupt Dental Lab, Inc. in Huntington Beach, CA.
Pressed Ceramics Versus Layered Feldspathic Veneers: A Rationale for Modality Selection by John Haupt, M.D.T. John Haupt is the founder and president of Haupt Dental Lab, Inc. in Huntington Beach, CA.
The One-Visit Smile Makeover: An Ultraconservative Approach
 The One-Visit Smile Makeover: An Ultraconservative Approach Oleg Borshch, DDS Private Practice Brooklyn, New York Phone: 718.376.8656 Email: [email protected] Web site: www.omnidentalcare.com [QA:
The One-Visit Smile Makeover: An Ultraconservative Approach Oleg Borshch, DDS Private Practice Brooklyn, New York Phone: 718.376.8656 Email: [email protected] Web site: www.omnidentalcare.com [QA:
WIPE AND GO! No more time-consuming polishing of your provisionals. Structur 3. Structur 3
 WIPE AND GO! Structur 3 No more time-consuming polishing of your provisionals Structur 3 NANO-FILLED, QUICK SETTING, STRONG TEMPORARY CROWN & BRIDGE MATERIAL WITH WIPE & GO TECHNOLOGY Structur 3 NANO-FILLED,
WIPE AND GO! Structur 3 No more time-consuming polishing of your provisionals Structur 3 NANO-FILLED, QUICK SETTING, STRONG TEMPORARY CROWN & BRIDGE MATERIAL WITH WIPE & GO TECHNOLOGY Structur 3 NANO-FILLED,
ATLANTIS crown abutment. Patient-specific CAD/CAM abutments for single-tooth, screw-retained restorations
 ATLANTIS crown abutment Patient-specific CAD/CAM abutments for single-tooth, screw-retained restorations Excellent results every time For all major implant systems DENTSPLY Implants now offers the appreciated
ATLANTIS crown abutment Patient-specific CAD/CAM abutments for single-tooth, screw-retained restorations Excellent results every time For all major implant systems DENTSPLY Implants now offers the appreciated
Section 16 Dental Laboratories
 Section 16 Dental Laboratories TABLE OF CONTENTS Policies and Procedures for Central Dental Laboratory Services 1 Purpose 1 Scope 1 Laboratory Hours and Information 1 Procedures 1 Patient Accounts 2 Selection
Section 16 Dental Laboratories TABLE OF CONTENTS Policies and Procedures for Central Dental Laboratory Services 1 Purpose 1 Scope 1 Laboratory Hours and Information 1 Procedures 1 Patient Accounts 2 Selection
prosthetic technique manual
 prosthetic technique manual TABLE OF CONTENTS Introduction 1 Treatment Planning 2-5 Restorative Options Implant-level Cement-retained Restorations Implant-level Screw-retained Restorations Abutment-level
prosthetic technique manual TABLE OF CONTENTS Introduction 1 Treatment Planning 2-5 Restorative Options Implant-level Cement-retained Restorations Implant-level Screw-retained Restorations Abutment-level
20TDNH 214. Course Description:
 Revised: Fall 2015 20TDNH 214 20TPractical Materials for Dental Hygiene Course Description: 37TStudies the current technologic advances, expanded functions, and clinical/laboratory materials used in dental
Revised: Fall 2015 20TDNH 214 20TPractical Materials for Dental Hygiene Course Description: 37TStudies the current technologic advances, expanded functions, and clinical/laboratory materials used in dental
The Lower Free End Saddle (distal extension saddle)
") Giles Perryer 1997 I The Lower Free End Saddle (distal extension saddle) Free end saddle dentures move Excessive movement of the denture can cause pain, tissue damage, and complaints of instability and
Giles Perryer 1997 I The Lower Free End Saddle (distal extension saddle) Free end saddle dentures move Excessive movement of the denture can cause pain, tissue damage, and complaints of instability and
4-1-2005. Dental Clinical Criteria and Documentation Requirements
 4-1-2005 Dental Clinical Criteria and Documentation Requirements Table of Contents Dental Clinical Criteria Cast Restorations and Veneer Procedures... Pages 1-3 Crown Repair... Page 3 Endodontic Procedures...
4-1-2005 Dental Clinical Criteria and Documentation Requirements Table of Contents Dental Clinical Criteria Cast Restorations and Veneer Procedures... Pages 1-3 Crown Repair... Page 3 Endodontic Procedures...
Full Crown Module: Learner Level 3
 Full Crown Module Restoration / Tooth # Full Gold Crown (FGC) / mesially tilted 30 Extensions: Porcelain Fused to Metal (PFM) / lingually 21 All Ceramic / rotated 12 Learner Level 3 Preparation of Malpositioned
Full Crown Module Restoration / Tooth # Full Gold Crown (FGC) / mesially tilted 30 Extensions: Porcelain Fused to Metal (PFM) / lingually 21 All Ceramic / rotated 12 Learner Level 3 Preparation of Malpositioned
Clinical Education for Achieving Great Dentistry
 NEW COURSES! MORE DATES! Clinical Education for Achieving Great Dentistry Occlusion Full Mouth Rehab Aesthetics Implants Photography Treatment Planning Lee Ann Brady, John Nosti, FICOI, FAGD, FACE Jason
NEW COURSES! MORE DATES! Clinical Education for Achieving Great Dentistry Occlusion Full Mouth Rehab Aesthetics Implants Photography Treatment Planning Lee Ann Brady, John Nosti, FICOI, FAGD, FACE Jason
Dental Implants and Esthetics
 Dental Implants and Esthetics Charles J. Goodacre, DDS, MSD; Chad J. Anderson, MS, DMD Continuing Education Units: 1 hour Online Course: www.dentalcare.com/en-us/dental-education/continuing-education/ce203/ce203.aspx
Dental Implants and Esthetics Charles J. Goodacre, DDS, MSD; Chad J. Anderson, MS, DMD Continuing Education Units: 1 hour Online Course: www.dentalcare.com/en-us/dental-education/continuing-education/ce203/ce203.aspx
Frequently Asked Whip Mix Articulator Questions
 Frequently Asked Whip Mix Articulator Questions 1. Why should I use a Whip Mix Articulator? Simple! The Whip Mix Articulator System is extremely easy to use. It is not intimidating for dentists who may
Frequently Asked Whip Mix Articulator Questions 1. Why should I use a Whip Mix Articulator? Simple! The Whip Mix Articulator System is extremely easy to use. It is not intimidating for dentists who may
CHAPTER 12 SURVEY LINES. portion of the tooth is undercut to the path of placement of the denture. DEFINITIONS
 CHAPTER 12 portion of the tooth is undercut to the path of placement of the denture. SURVEY LINES DEFINITIONS A SURVEY LINE is a line produced on a cast by a surveyor or scribe marking the greatest prominence
CHAPTER 12 portion of the tooth is undercut to the path of placement of the denture. SURVEY LINES DEFINITIONS A SURVEY LINE is a line produced on a cast by a surveyor or scribe marking the greatest prominence
What is a dental implant?
 What is a dental implant? Today, the preferred method of tooth replacement is a dental implant. They replace missing tooth roots and form a stable foundation for replacement teeth that look, feel and function
What is a dental implant? Today, the preferred method of tooth replacement is a dental implant. They replace missing tooth roots and form a stable foundation for replacement teeth that look, feel and function
CLASSIFICATION OF REMOVABLE PARTIAL DENTURES
 Unless otherwise noted, the content of this course material is licensed under a Creative Commons Attribution - Non-Commercial - Share Alike 3.0 License. Copyright 2008, Dr. Jeff Shotwell. The following
Unless otherwise noted, the content of this course material is licensed under a Creative Commons Attribution - Non-Commercial - Share Alike 3.0 License. Copyright 2008, Dr. Jeff Shotwell. The following
Choosing the right type of abutment
 50 Producing custom implant abutments using CAD/CAM Choosing the right type of abutment S. KHALILOVA 1, F. KISTLER 2, S. ADLER 3, S. WEISS 3, S. KISTLER 2 AND J. NEUGEBAUER 2,4 Rapid developments in the
50 Producing custom implant abutments using CAD/CAM Choosing the right type of abutment S. KHALILOVA 1, F. KISTLER 2, S. ADLER 3, S. WEISS 3, S. KISTLER 2 AND J. NEUGEBAUER 2,4 Rapid developments in the