PHARMACEUTICAL OPIOID PROBLEMS AND CHANGING TREATMENT NEEDS: An Australian perspective
|
|
|
- Christopher Sutton
- 8 years ago
- Views:
Transcription
1 PHARMACEUTICAL OPIOID PROBLEMS AND CHANGING TREATMENT NEEDS: An Australian perspective Suzanne Nielsen BPharm PhD Public Lecture: Waterford Institute of Technology September 7 th 2015

2 Overview Pharmaceutical opioid use and definitions Characteristics of people who use pharmaceutical opioids (PO) The evidence base for treatment of pharmaceutical opioid dependence Treatment models Other at risk populations 2

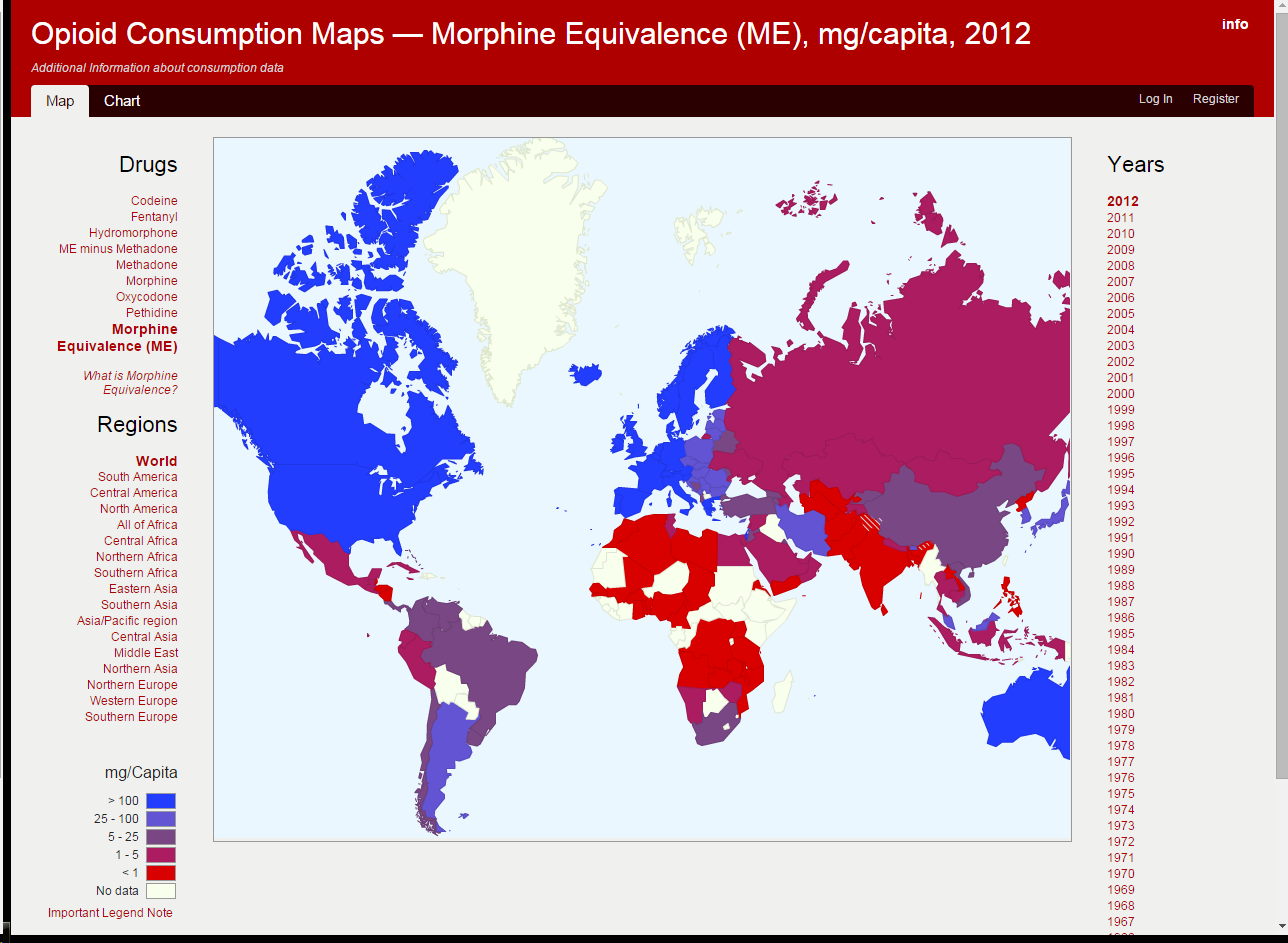
3 Pharmaceutical Opioids Use of opioids for pain has increased dramatically over the past years in many high income countries Opioids are an important and effective group of medications, especially for acute pain (which many countries have poor access to) Large increases in opioids don t equate to problematic use HOWEVER there are strong correlations between increasing use and harms Fischer B, Jones W, Rehm J. High correlations between levels of consumption and mortality related to strong prescription opioid analgesics in British Columbia and Ontario, Pharmacoepidemiol Drug Saf Rintoul AC, Dobbin MDH, Drummer OH, Ozanne-Smith J. Increasing deaths involving oxycodone, Victoria, Australia, Injury Prevention

4 4


5 5
6 PBS-subsidised opioid dispensings in Australia, Blanch et al (2014). An overview of the patterns of prescription opioid use, costs and related harms in Australia. BJ Clinical Pharmacology. 6

7 National opioid utilisation Packs sold Number % of total packs sold Strong Prescribed Opioids 10,096, Fentanyl 859,518 2 Oxycodone 5,812, Hydromorphone 224, Methadone 541, Morphine 775, Buprenorphine 1,881, Other Prescribed Opioids 16,762, Tapentadol 5,074 0 Tramadol 4,002, Dextropropoxyphene 464, Codeine (Prescribed) 12,290, Total prescribed opioids 26,858, Over-the-counter opioids 15,490, Total opioids 42,348, Degenhardt et al Under review 7
 12,290,027 29 Total prescribed opioids 26,858,419 63.")


8 Opioid utilisation by geographical area Degenhardt et al Under review 8

9 Hospitalisations from opioids in Australia Blanch et al (2014). An overview of the patterns of prescription opioid use, costs and related harms in Australia. BJ Clinical Pharmacology. 9

10 Non-medical Pharmaceutical use in Australia Most drugs (alcohol, tobacco, heroin, ecstasy) decreasing Pharmaceuticals one of the few categories that increased from o 8% ever used non-medically o 5% in the past 12 months Majority of opioid mortality and poisonings are now from pharmaceutical opioids Who develops problems with pharmaceutical opioids and what do we know about treatment? 10

11 Who develops problems with pharmaceutical opioids? 11

12 Defining non-medical or problematic opioid use 12

13 Definitions Addiction / Dependence Physiological adaptation addiction Withdrawal/tolerance addiction 13

14 How is Substance Use Disorder defined Substance taken in larger amounts or over a longer period than was intended. Persistent desire or unsuccessful efforts to cut down or control the substance use A great deal of time spent obtaining, using/recovering from substance use Craving Recurrent substance use resulting in a failure to fulfill responsibilities Given up or reducing social, occupational, or recreational activities because of substance use Recurrent hazardous substance use / use despite harm Loss of control over use of opioids DSM-5 Substances Use Disorder Definitions 14

15 People who use pharmaceutical opioids are a heterogeneous population Nonmedical Users Pain Patients Passik SD, Kirsh KL. The interface between pain and drug abuse and the evolution of strategies to optimize pain management while minimizing drug abuse. Experimental and Clinical Psychopharmacology. 2008; 16(5):

16 Developing dependence to pain medications "The headache would go temporarily and would return again..i started off taking them four hourly... It sort of got into a vicious cycle where I could take six Panadeine Forte and then two hours later take four Panadeine.. It was only when I swapped Dr s and I went for a Panadeine Forte prescription and she said but I only gave you one three weeks ago and I said but they re all gone that she actually picked up that I was addicted to them." (Female, 54 yrs) 16

 most (66%) initiated PO use")
17 Developing dependence to pain medications Cohort of treatment entrants (n = 108) most (66%) initiated PO use for pain 17
 initiated PO use")
18 Why do people keep taking them? "by that stage, when I was having that many when I started to feel really sick, trying to get them down, I got back down to 36 in one go and even that was pretty difficult because you d retch trying to get them down but you just knew you needed to get them in there to make you feel OK again. (Female, 42yrs) 18

19 The Four A s of Pain Treatment Outcomes Analgesia (pain relief) Activities of Daily Living (psychosocial functioning) Adverse effects (side effects) Aberrant drug taking (addiction-related outcomes) Is the patient receiving benefits without being harmed by their medication?(c Stannard, UK) Passik & Weinreb, 1998

20 Dependence with OTC codeine Increased dose (above daily maximum dose) Taking for reasons other than pain Difficulty going without codeine Codeine no longer effective Codeine no longer helps with pain Need higher doses/ exceeding maximum dose 20

21 Pharmaceutical opioid use amongst different populations 22
22 Use of Pharmaceutical Opioids by PWID (IDRS) (Annual AUS survey, people who regularly inject) Injecting use of morphine increased between 2001 and 2007 (from 40% to 50%), declined to 35% in Increase in oxycodone injecting use among IDRS participants, from 17% in 2005 to 31% in % reported injecting fentanyl (past six months in 2013) Heroin still main drug injected Oxycodone use weekly or less on average Summary: PO use usually opportunistic and occasional.. harm reduction, and existing treatments the focus IDRS 2013 Stafford and Burns 23
23 Mortality from pharmaceutical opioids Oxycodone (n = 465, ) o Most deaths involved prescribed oxycodone (55%), noninjectors (54%) and chronic pain (52%) Fentanyl (n = 136, ) o Minority (1/3) prescribed, most (55%) injecting, and 38% have chronic pain Codeine (n = 1200, ) (In press) o o o High rates of comorbid mental health (53%), substance use (36%) and chronic pain (35%), history of injection (16%) 49% accidental, 35% intentional Source mostly (60%) not reported, 60% of coded cases are prescription codeine 24 National Coronial Information System; Roxburgh, et al (MJA 2011); Roxburgh et al (2013), Roxburgh et al (2015, in press)
24 Treatment demand in increasing USA increase from < 1.0% (1998) to 10 % (2011) of all treatment demand o Heroin treatment stable (14% -16%) for the past 15 years In 2011, 5% of all patients entering drug treatment programmes in Europe reported prescription opioids as their primary drug Increasing mortality in the UK European Monitoring Centre for Drugs and Drug Addiction.(2011) Annual report. Lisbon: Giraudon et al. Prescription opioid abuse in the UK. Br J Clin Pharmacol 2013;76: Treatment Episode Data Set : Admissions (TEDS) Substance Abuse and Mental Health Services Administration; 2014 (USA) 25
 European drug report, 2015, EMCDDA")
25 Treatment for opioids other than heroin (2015) European drug report, 2015, EMCDDA 26
26 Australian PO Treatment samples Explore existing sources: National Minimum Dataset AOD Treatment Opioid pharmacotherapy data (NOPSAD) Develop new studies: Retrospective case review Cohort studies 27
27 National Minimum Data on Drug Treatment Closed treatment episodes from the Alcohol and Other Drug Treatment Services National Minimum Data Set (AODTS-NMDS) for to odata on publicly funded alcohol and other drug treatment services omost pharmacotherapy services and private services are outside the scope of AODTS- NMDS a non-ost sample Nielsen et al (2015) Changes in non-opioid substitution treatment episodes for pharmaceutical opioids and heroin from 2002 to 2011 Drug and Alcohol Dependence 28
28 Number of closed tretment episodes Changing treatment demand in Australia In PO represent one in five treatment episodes All Heroin Heroin principal DOC All PO PO Principal DOC Year Nielsen et al (2015) Changes in non-opioid substitution treatment episodes for pharmaceutical opioids and heroin from 2002 to 2011 Drug and Alcohol Dependence 29
29 N0. closed treatment episodes Results: Changes in individual PO over time Increases in codeine, oxycodone and fentanyl episodes Morphine Codeine Oxycodone Fentanyl 0 Year Nielsen et al (2015) Changes in non-opioid substitution treatment episodes for pharmaceutical opioids and heroin from 2002 to 2011 Drug and Alcohol Dependence 30
30 Episode Characteristics by Opioid Type Heroin (n = 68517) Strong Opioids Codeine (n=11458) (n = 4424) Median Age (IQR)# 30.0 (12.0) 35 (15.0) 36.0 (14.0) Gender (%Male) Regional or remote location Method of use of Principal DOC Injects Swallow Reports 'never injected' Other Drugs of Concern Benzodiazepine Alcohol Cannabis and related drugs Meth/Amphetamines p<.01 Compared to heroin p <.01Codeine compared to strong opioids Nielsen et al (2015) Changes in non-opioid substitution treatment episodes for pharmaceutical opioids and heroin from 2002 to 2011 Drug and Alcohol Dependence 31
31 Male Results: Changes in gender over time Codeine Oxycodone Heroin Morphine 100.0% 90.0% 80.0% 70.0% 60.0% 50.0% 40.0% 30.0% 20.0% 10.0% 0.0% Increasing proportion of males for codeine and oxycodone, changing significantly faster for codeine Year Nielsen et al (2015) Changes in non-opioid substitution treatment episodes for pharmaceutical opioids and heroin from 2002 to 2011 Drug and Alcohol Dependence 32
")
32 National Opioid Pharmacotherapy Statistics Annual Data (NOPSAD) 33
33 Pharmaceutical opioids: treatment populations International research has identified that there are important differences between people who use pharmaceutical opioids and heroin o Greater pain, more mental health comorbidity o Shorter opioid use histories, less treatment experience o More likely to be white, employed Brands et al 2004; Moore et al 2007; Fischer et al
34 Consistent patterns across multiple studies Gender Employment Mental health Physical Health Drug use history Codeine web survey (n = 800) Most female Mainly employed Poor Poor physical functioning, Chronic pain Around 60% ever used any illicit drugs (not different to non-dependent) Retrospective case series (n = 147) Codeine female/ strong PO male Higher amongst codeine High levels of comorbidity Most report pain as reason for initiation Varied by opioid type, multiple opioids and injection history for strong PO Nielsen et al 2011 Journal of Opioid Management Nielsen et al 2014 Drug and Alcohol Review Nielsen et al 2015 In preparation POUT cohort POUT Cohort study (n = 108) Overall 52% female More females 29% overall (higher for codeine) Most report depression, anxiety, trauma, highly medicated 85% report problematic pain in past year (41% current chronic pain) 58% ever injected, 17% used heroin in the past year Greater levels of employment Significant mental health problems Significant physical health problems Significant minority have never injected/used heroin 35
35 Comparing codeine (n = 53) users to other pharmaceutical opioid users (n = 82) in treatment in NSW Nielsen S, et al. (2014) Comparing treatment-seeking codeine users and strong opioid users: Findings from a novel case series. Drug and Alcohol Review
36 Summary Increasing PO treatment presentations In comparison to heroin treatment o Non-injectors o More chronic pain o Over-represented at rural/regional treatment service Important differences between pharmaceutical opioids Some characteristics that might support good treatment outcomes (e.g. higher levels of employment) Some characteristics might complicate treatment (e.g. pain) 37
37 Treatment for pharmaceutical opioid dependence 38
38 Opioid agonist treatments Much of the focus of the rest of the talk Not all patients are ready or suitable for opioid agonist treatments (e.g. methadone, buprenorphine) These treatments have the strongest evidence To enter pharmacotherapy treatment met criteria for opioid dependence (most severe end of the spectrum) i.e. not all problematic use 39
39 Is treatment for PO dependence different? Q: Can we just use the same old treatments? A: it depends There are a number of important characteristics that might inform treatment needs Level of tolerance/opioid dependence Other comorbidities (mental and physical health especially pain) History of injection? History of heroin use? Treatment access (e.g. supervised dosing, employment, families) What treatments do people want? (reluctance to enter `drug treatment) 40
40 Detoxification versus maintenance Why detoxification for PO? Shorter use histories, greater social support, employment, lower levels of neuroadaptation (i.e. lower doses of opioids) Unwilling to enter long term treatment (stigma/employment) Australian treatment research: Codeine users are more likely to receive detox that strong opioid users (Nielsen et al 2014 Drug and Alcohol Review) PO more likely to have shorter/less intensive treatment (e.g. assessment only) compared to heroin users (Nielsen et al 2015 Drug and Alcohol Dependence) 41
41 Long or short-term treatment? 42
42 Short term buprenorphine treatment POATS study: 653 treatment-seeking people dependent on prescription opioids 2 and 12 weeks of buprenorphine Two weeks of buprenorphine 93% relapsed Twelve weeks of buprenorphine 91% relapsed Short-term treatment is rarely enough Weiss R, et al. (2011) A Two-Phase Randomized Controlled Trial of Adjunctive Counseling during Brief and Extended Buprenorphine-Naloxone Treatment for Prescription Opioid Dependence. Arch Gen Psychiatry. 43
43 Randomised trials comparing detox to maintenance Buprenorphine (1,2 and 4 week) taper then naltrexone (n = 70) Buprenorphine taper (+ NTX) vs maintenance treatment (n = 113) Better retention and less substance use with maintenance/longer buprenorphine treatment Sigmon et al 2013, Fiellin et al
44 Which pharmacotherapy? Little evidence to compare pharmacotherapy o Four open label studies, two recruited buprenorphine injectors (previously opium/herion use) Neumann (2014) recruited PO with pain (n = 54) o o o o Used low doses of OST (esp methadone) Improved pain (no diff b/w MTD and BPN) Less opioid use with MTD No difference in retention, other drug use between groups Saxon (2013) n = 1269 (170 PO only) RCT comparing methadone with buprenorphine-naloxone o For PO there was NO difference in drug use OR retention between the groups (in contrast to heroin users) Saxon et al. (2013) Buprenorphine/Naloxone and methadone effects on laboratory indices of liver health: A randomized trial. Drug and Alcohol Dependence. Neumann et al (2013) A preliminary study comparing methadone and buprenorphine in patients with chronic pain and coexistent opioid addiction. Journal of addictive diseases 45
45 Buprenorphine for pharmaceutical opioid dependence Rationale for buprenorphine similar to other opioid dependent populations o Less overdose risk o Fewer supervision requirements compared with methadone (higher employment among PO) o Less stigma o May also have benefits in pain 46
46 Buprenorphine treatment for PO dependence Induction for PO dependent people: 1) Rates of precipitated withdrawal were same or lower than with heroin users 2) Doses required are comparable 3) Few differences between PO Caution: specific protocol for methadone induction Nielsen S, et al. (2014) The relationship between primary prescription opioid and buprenorphine-naloxone induction outcomes in a prescription opioid dependent sample. The American Journal on Addictions. Nielsen S, et al (2012) Comparing buprenorphine induction experience with heroin and prescription opioid users. JSAT 47
47 Predictors of treatment outcomes: Heroin use Treatment outcomes for pharmaceutical opioid dependence compares favourably to those for heroin use Better retention Less substance use PO may have better outcomes with psychosocial adjunct treatments (e.g. CBT, contingency management) Any heroin use predicts poorer outcomes (more opioid use, poorer retention) Nielsen S et al (2015). Buprenorphine Pharmacotherapy and Behavioral Treatment: Comparison of Outcomes among Prescription Opioid Users, Heroin Users and Combination users. JSAT. Nielsen S, et al (2013) A comparison of buprenorphine taper outcomes between prescription opioid and heroin users. Journal of Addiction Medicine. Weiss R, et al. (2011) A Two-Phase Randomized Controlled Trial of Adjunctive Counseling during Brief and Extended Buprenorphine- Naloxone Treatment for Prescription Opioid Dependence. Arch Gen Psychiatry. 48
48 Predictors of treatment outcomes: Pain Mixed findings: Weiss et al 2011 (POATS) no difference in outcome by pain status at baseline Potter et al examined effect of pain on taper outcomes; Those with moderate to severe pain did better DURING treatment Those with pain had more self-reported use at follow-up (no difference in UDS) **Note that most of these studies were specifically excluding patients with significant pain that needed opioids for management 49
49 Buprenorphine for opioid dependence in pain patients Open label with patients transferring from full opioid agonists (e.g. oxycodone) to buprenorphine (retrospective reports) lower quality evidence Daitch D, et al. Pain Medicine.2012, 2014 Malinoff et al. American Journal of Therapeutics o Pain report less pain after transfer to buprenorphine o mean doses of 8 28 mg per day(dose frequency not reported) o patients on high opioid doses (> 200 mg OME a day) show comparable or greater improvements in pain and quality of life after transfer Evidence is low quality but promising 50
50 Buprenorphine for codeine dependence Isn t codeine a weak opioid? People presenting with codeine dependence less likely to receive maintenance treatment Where maintenance offered doses required are comparable to other patients o Median buprenorphine dose was mg (range 4-32 mg) Buprenorphine doses received markedly higher than estimated codeine doses based on standard dose conversion tables. Nielsen S, et al. (2015, in press) Treating codeine dependence with buprenorphine. Drug and Alcohol Review. Nielsen S, et al. (2014) Comparing treatment-seeking codeine users and strong opioid users: Findings from a novel case series. Drug and Alcohol Review. 51
51 Buprenorphine doses for codeine dependence Estimated BPN dose using conversion tables for pain treatment Actual BPN dose day 7 Codeine Dose (20-32 tabs) (70-100tabs)
52 In summary: treatment for PO dependence We have treatments that work They work in similar ways The treatment system, rather than the treatments, may need tailoring o Higher levels of employment o More females o Pain o Non-injectors Specific PO Clinics 53
53 The importance of treatment setting The only thing that concerns me sometimes is that I have to line up with the methadone people, or the other heroin users at the clinic" (Male, 42 yrs) 54
54 Tailoring services for PO dependence Detailed assessment including pain history Separate physical location Transfer quickly to community pharmacy OTP Clinic PO Clinic 55
55 Are we treating the at-risk patients? Existing research focus treating opioid dependence HOWEVER: Most at-risk patients are nowhere near AOD treatment services Pain and Opioids IN Treatment (POINT) cohort study 1500 patients with chronic pain prescribed opioids o 40% prescribed >90mg oral morphine equivalents daily, 15% >200mg OME daily o One third use benzodiazepines (most daily) o Median of 3-4 sedative medications (up to 32 medication in total) o High levels of depression/anxiety o 1 in 5 PO SUD, most (68%) report problems/concerns with opioids 56
56 Often we may be missing the point it's a difficult balancing act to make sure the drug is accessible to those who need it, without making it too easy to get for those who might misuse it (Kos Sclavos Pharmacy Guild) False dichotomy of good and bad patients Usually the patient with a pain condition develops dependence Earlier detection and intervention where problems are developing OR opioids not working Opioid dependence is a health problem health response 60
57 Future work Helping pharmacists to talk to people about pain, and the role of opioids Universal precautions Evidence based medicine Public education about the role of opioids (and the role of other treatments) especially in chronic pain Is the patient receiving benefits without being harmed by their medication? 61
58 Acknowledgements CODEMISUSED SN supported by NHMRC research fellowships (# ). The National Drug and Alcohol Research Centre at UNSW is supported by funding from the Australian Government under the Substance Misuse Prevention and Service Improvements Grant Fund. Numerous collaborators and co-authors and students 62
Non medical use of prescription medicines existing WHO advice
 Non medical use of prescription medicines existing WHO advice Nicolas Clark Management of Substance Abuse Team WHO, Geneva Vienna, June 2010 clarkn@who.int Medical and Pharmaceutical role Recommendations
Non medical use of prescription medicines existing WHO advice Nicolas Clark Management of Substance Abuse Team WHO, Geneva Vienna, June 2010 clarkn@who.int Medical and Pharmaceutical role Recommendations
Death in the Suburbs: How Prescription Painkillers and Heroin Have Changed Treatment and Recovery
 Death in the Suburbs: How Prescription Painkillers and Heroin Have Changed Treatment and Recovery Marvin D. Seppala, MD Chief Medical Officer Hazelden Betty Ford Foundation This product is supported by
Death in the Suburbs: How Prescription Painkillers and Heroin Have Changed Treatment and Recovery Marvin D. Seppala, MD Chief Medical Officer Hazelden Betty Ford Foundation This product is supported by
Jennifer Sharpe Potter, PhD, MPH Associate Professor Division of Alcohol and Drug Addiction Department of Psychiatry
 Buprenorphine/Naloxone and Methadone Maintenance Treatment Outcomes for Opioid Analgesic, Heroin, and Combined Users: Findings From Starting Treatment With Agonist Replacement Therapies (START) Jennifer
Buprenorphine/Naloxone and Methadone Maintenance Treatment Outcomes for Opioid Analgesic, Heroin, and Combined Users: Findings From Starting Treatment With Agonist Replacement Therapies (START) Jennifer
Treatment of Prescription Opioid Dependence
 Treatment of Prescription Opioid Dependence Roger D. Weiss, MD Chief, Division of Alcohol and Drug Abuse McLean Hospital, Belmont, MA Professor of Psychiatry, Harvard Medical School, Boston, MA Prescription
Treatment of Prescription Opioid Dependence Roger D. Weiss, MD Chief, Division of Alcohol and Drug Abuse McLean Hospital, Belmont, MA Professor of Psychiatry, Harvard Medical School, Boston, MA Prescription
Treatment of opioid use disorders
 Treatment of opioid use disorders Gerardo Gonzalez, MD Associate Professor of Psychiatry Director, Division of Addiction Psychiatry Disclosures I have no financial conflicts to disclose I will review evidence
Treatment of opioid use disorders Gerardo Gonzalez, MD Associate Professor of Psychiatry Director, Division of Addiction Psychiatry Disclosures I have no financial conflicts to disclose I will review evidence
Treatment of Opioid Dependence: A Randomized Controlled Trial. Karen L. Sees, DO, Kevin L. Delucchi, PhD, Carmen Masson, PhD, Amy
 Category: Heroin Title: Methadone Maintenance vs 180-Day psychosocially Enriched Detoxification for Treatment of Opioid Dependence: A Randomized Controlled Trial Authors: Karen L. Sees, DO, Kevin L. Delucchi,
Category: Heroin Title: Methadone Maintenance vs 180-Day psychosocially Enriched Detoxification for Treatment of Opioid Dependence: A Randomized Controlled Trial Authors: Karen L. Sees, DO, Kevin L. Delucchi,
Office-based Treatment of Opioid Dependence with Buprenorphine
 Office-based Treatment of Opioid Dependence with Buprenorphine David A. Fiellin, M.D Professor of Medicine, Investigative Medicine and Public Health Yale University School of Medicine Dr. Fiellin s Disclosures
Office-based Treatment of Opioid Dependence with Buprenorphine David A. Fiellin, M.D Professor of Medicine, Investigative Medicine and Public Health Yale University School of Medicine Dr. Fiellin s Disclosures
The Changing Face of Opioid Addiction:
 9th Annual Training and Educational Symposium September 6, 2012 The Changing Face of Opioid Addiction: A Review of the Research and Considerations for Care Mark Stanford, Ph.D. Santa Clara County Dept
9th Annual Training and Educational Symposium September 6, 2012 The Changing Face of Opioid Addiction: A Review of the Research and Considerations for Care Mark Stanford, Ph.D. Santa Clara County Dept
MEDICATION ASSISTED TREATMENT FOR OPIOID ADDICTION
 MEDICATION ASSISTED TREATMENT FOR OPIOID ADDICTION Sidarth Wakhlu,M.D. Addiction Team Leader North Texas VA Health Care System Addiction Psychiatry Fellowship Director Associate Professor Of Psychiatry
MEDICATION ASSISTED TREATMENT FOR OPIOID ADDICTION Sidarth Wakhlu,M.D. Addiction Team Leader North Texas VA Health Care System Addiction Psychiatry Fellowship Director Associate Professor Of Psychiatry
One example: Chapman and Huygens, 1988, British Journal of Addiction
 This is a fact in the treatment of alcohol and drug abuse: Patients who do well in treatment do well in any treatment and patients who do badly in treatment do badly in any treatment. One example: Chapman
This is a fact in the treatment of alcohol and drug abuse: Patients who do well in treatment do well in any treatment and patients who do badly in treatment do badly in any treatment. One example: Chapman
Considerations when Using Controlled Substances to Treat Chronic Pain
 Considerations when Using Controlled Substances to Treat Chronic Pain By Mary-Beth F. Plum, Pharm.D. Impact of Chronic Pain Acute pain is the body s response to environmental dangers, and it helps protect
Considerations when Using Controlled Substances to Treat Chronic Pain By Mary-Beth F. Plum, Pharm.D. Impact of Chronic Pain Acute pain is the body s response to environmental dangers, and it helps protect
Substitution Therapy for Opioid Dependence The Role of Suboxone. Mandy Manak, MD, ABAM, CCSAM Methadone 101-Hospitalist Workshop, October 3, 2015
 Substitution Therapy for Opioid Dependence The Role of Suboxone Mandy Manak, MD, ABAM, CCSAM Methadone 101-Hospitalist Workshop, October 3, 2015 Objectives Recognize the options available in treating opioid
Substitution Therapy for Opioid Dependence The Role of Suboxone Mandy Manak, MD, ABAM, CCSAM Methadone 101-Hospitalist Workshop, October 3, 2015 Objectives Recognize the options available in treating opioid
Minimum Insurance Benefits for Patients with Opioid Use Disorder The Opioid Use Disorder Epidemic: The Evidence for Opioid Treatment:
 Minimum Insurance Benefits for Patients with Opioid Use Disorder By David Kan, MD and Tauheed Zaman, MD Adopted by the California Society of Addiction Medicine Committee on Opioids and the California Society
Minimum Insurance Benefits for Patients with Opioid Use Disorder By David Kan, MD and Tauheed Zaman, MD Adopted by the California Society of Addiction Medicine Committee on Opioids and the California Society
EPIDEMIC 4.6 % OF INDIVIDUALS 18 25 USED PAIN RELIEVERS FOR NON-MEDICAL REASONS. 1.5 MILLION YOUNG ADULTS USED PAIN RELIEVERS IN THE PAST MONTH.
 Drug Court EPIDEMIC In the 10 years (1997 2007) the per capita retail purchases of Methadone, Hydrocodone and Oxycodone in the United States increased 13-fold, 4-fold and 9-fold, respectively. 4.6 % OF
Drug Court EPIDEMIC In the 10 years (1997 2007) the per capita retail purchases of Methadone, Hydrocodone and Oxycodone in the United States increased 13-fold, 4-fold and 9-fold, respectively. 4.6 % OF
How To Treat Anorexic Addiction With Medication Assisted Treatment
 Medication Assisted Treatment for Opioid Addiction Tanya Hiser, MS, LPC Premier Care of Wisconsin, LLC October 21, 2015 How Did We Get Here? Civil War veterans and women 19th Century physicians cautious
Medication Assisted Treatment for Opioid Addiction Tanya Hiser, MS, LPC Premier Care of Wisconsin, LLC October 21, 2015 How Did We Get Here? Civil War veterans and women 19th Century physicians cautious
Care Management Council submission date: August 2013. Contact Information
 Clinical Practice Approval Form Clinical Practice Title: Acute use of Buprenorphine for the Treatment of Opioid Dependence and Detoxification Type of Review: New Clinical Practice Revisions of Existing
Clinical Practice Approval Form Clinical Practice Title: Acute use of Buprenorphine for the Treatment of Opioid Dependence and Detoxification Type of Review: New Clinical Practice Revisions of Existing
EPIDEMIOLOGY OF OPIATE USE
 Opiate Dependence EPIDEMIOLOGY OF OPIATE USE Difficult to estimate true extent of opiate dependence Based on National Survey of Health and Mental Well Being: 1.2% sample used opiates in last 12 months
Opiate Dependence EPIDEMIOLOGY OF OPIATE USE Difficult to estimate true extent of opiate dependence Based on National Survey of Health and Mental Well Being: 1.2% sample used opiates in last 12 months
Opioids for Pain Treatment. Opioids for Chronic Pain and Addiction Treatment. Outline for Today. Opioids for pain treatment
 Opioids for Chronic Pain and Addiction Treatment Joseph Merrill M.D., M.P.H. University of Washington February 24, 2012 Outline for Today Opioids for pain treatment Trends Problems High dose prescribing
Opioids for Chronic Pain and Addiction Treatment Joseph Merrill M.D., M.P.H. University of Washington February 24, 2012 Outline for Today Opioids for pain treatment Trends Problems High dose prescribing
Medical Malpractice Treatment Alprazolam benzodiazepine - A Case Study
 Improving Outcomes in Patients Who are Prescribed Alprazolam with Concurrent Use of Opioids Pik-Sai Yung, M.D. Staff Psychiatrist Center for Counseling at Walton Background and Rationale Alprazolam is
Improving Outcomes in Patients Who are Prescribed Alprazolam with Concurrent Use of Opioids Pik-Sai Yung, M.D. Staff Psychiatrist Center for Counseling at Walton Background and Rationale Alprazolam is
Medical marijuana for pain and anxiety: A primer for methadone physicians. Meldon Kahan MD CPSO Methadone Prescribers Conference November 6, 2015
 Medical marijuana for pain and anxiety: A primer for methadone physicians Meldon Kahan MD CPSO Methadone Prescribers Conference November 6, 2015 Conflict of interest statement No conflict of interest to
Medical marijuana for pain and anxiety: A primer for methadone physicians Meldon Kahan MD CPSO Methadone Prescribers Conference November 6, 2015 Conflict of interest statement No conflict of interest to
Opioid Agonist Therapy: The Duration Dilemma Edwin A. Salsitz, MD, FASAM Mount Sinai Beth Israel, New York, NY March 10, 2015
 Q: I have read 40 mg of methadone stops withdrawal, so why don t we start at 30mg and maybe later in the day add 10mg? A: Federal Regulations stipulate that 30mg is the maximum first dose in an Opioid
Q: I have read 40 mg of methadone stops withdrawal, so why don t we start at 30mg and maybe later in the day add 10mg? A: Federal Regulations stipulate that 30mg is the maximum first dose in an Opioid
DMRI Drug Misuse Research Initiative
 DMRI Drug Misuse Research Initiative Executive Summary Dexamphetamine Substitution as a Treatment of Amphetamine Dependence: a Two-Centre Randomised Controlled Trial Final Report submitted to the Department
DMRI Drug Misuse Research Initiative Executive Summary Dexamphetamine Substitution as a Treatment of Amphetamine Dependence: a Two-Centre Randomised Controlled Trial Final Report submitted to the Department
Support to Primary Care from Derbyshire Substance Misuse Service for prescribed / OTC drug dependence
 Support to Primary Care from Derbyshire Substance Misuse Service for prescribed / OTC drug dependence SUMMARY 1) Derbyshire Substance misuse service provides Psycho-social treatment interventions for ALL
Support to Primary Care from Derbyshire Substance Misuse Service for prescribed / OTC drug dependence SUMMARY 1) Derbyshire Substance misuse service provides Psycho-social treatment interventions for ALL
OVERVIEW OF MEDICATION ASSISTED TREATMENT
 Sarah Akerman MD Assistant Professor of Psychiatry Director of Addiction Services Geisel School of Medicine/Dartmouth-Hitchcock Medical Center OVERVIEW OF MEDICATION ASSISTED TREATMENT Conflicts of Interest
Sarah Akerman MD Assistant Professor of Psychiatry Director of Addiction Services Geisel School of Medicine/Dartmouth-Hitchcock Medical Center OVERVIEW OF MEDICATION ASSISTED TREATMENT Conflicts of Interest
2015 OPSC Annual Convention. syllabus. February 4-8, 2015 Hyatt Regency Mission Bay San Diego, California
 2015 OPSC Annual Convention syllabus February 4-8, 2015 Hyatt Regency Mission Bay San Diego, California FRIDAY, FEBRUARY 6, 2015: 9:30am - 10:30am Opioid Addiction and Buprenorphine Use * Presented by
2015 OPSC Annual Convention syllabus February 4-8, 2015 Hyatt Regency Mission Bay San Diego, California FRIDAY, FEBRUARY 6, 2015: 9:30am - 10:30am Opioid Addiction and Buprenorphine Use * Presented by
Considerations in Medication Assisted Treatment of Opiate Dependence. Stephen A. Wyatt, D.O. Dept. of Psychiatry Middlesex Hospital Middletown, CT
 Considerations in Medication Assisted Treatment of Opiate Dependence Stephen A. Wyatt, D.O. Dept. of Psychiatry Middlesex Hospital Middletown, CT Disclosures Speaker Panels- None Grant recipient - SAMHSA
Considerations in Medication Assisted Treatment of Opiate Dependence Stephen A. Wyatt, D.O. Dept. of Psychiatry Middlesex Hospital Middletown, CT Disclosures Speaker Panels- None Grant recipient - SAMHSA
Pain, Addiction & Methadone
 Pain, Addiction & Methadone A CHALLENGING INTERFACE METHADONE AND SUBOXONE OPIOID SUBSTITUTION CONFERENCE Objectives 2 Explore the interface between concurrent pain and addiction. Appreciate the challenges
Pain, Addiction & Methadone A CHALLENGING INTERFACE METHADONE AND SUBOXONE OPIOID SUBSTITUTION CONFERENCE Objectives 2 Explore the interface between concurrent pain and addiction. Appreciate the challenges
Opioid Treatment Services, Office-Based Opioid Treatment
 Optum 1 By United Behavioral Health U.S. Behavioral Health Plan, California Doing Business as OptumHealth Behavioral Solutions of California ( OHBS-CA ) 2015 Level of Care Guidelines Opioid Treatment Services,
Optum 1 By United Behavioral Health U.S. Behavioral Health Plan, California Doing Business as OptumHealth Behavioral Solutions of California ( OHBS-CA ) 2015 Level of Care Guidelines Opioid Treatment Services,
Opioid Addiction and Methadone: Myths and Misconceptions. Nicole Nakatsu WRHA Practice Development Pharmacist
 Opioid Addiction and Methadone: Myths and Misconceptions Nicole Nakatsu WRHA Practice Development Pharmacist Learning Objectives By the end of this presentation you should be able to: Understand how opioids
Opioid Addiction and Methadone: Myths and Misconceptions Nicole Nakatsu WRHA Practice Development Pharmacist Learning Objectives By the end of this presentation you should be able to: Understand how opioids
+ + + + + ECSTASY. Trends in Drug Use and Related Harms in Australia, 2001 to 2013. National Drug and Alcohol Research Centre
 ALCOHOL PHARMACEUTICAL OPIOIDS HEROIN 21-212 COCAINE DRUG TRENDS CANNABIS + + + + + + ECSTASY Trends in Drug Use and Related Harms in Australia, 21 to 213 Medicine APC POP- UP STAND National Drug and Alcohol
ALCOHOL PHARMACEUTICAL OPIOIDS HEROIN 21-212 COCAINE DRUG TRENDS CANNABIS + + + + + + ECSTASY Trends in Drug Use and Related Harms in Australia, 21 to 213 Medicine APC POP- UP STAND National Drug and Alcohol
Buprenorphine: what is it & why use it?
 Buprenorphine: what is it & why use it? Dr Nicholas Lintzeris, MBBS, PhD, FAChAM Locum Consultant, Oaks Resource Centre, SLAM National Addiction Centre, Institute of Psychiatry Overview of presentation
Buprenorphine: what is it & why use it? Dr Nicholas Lintzeris, MBBS, PhD, FAChAM Locum Consultant, Oaks Resource Centre, SLAM National Addiction Centre, Institute of Psychiatry Overview of presentation
Buprenorphine/Naloxone Maintenance Treatment for Opioid Dependence
 Buprenorphine/Naloxone Maintenance Treatment for Opioid Dependence Information for Family Members Family members of patients who have been prescribed buprenorphine/naloxone for treatment of opioid addiction
Buprenorphine/Naloxone Maintenance Treatment for Opioid Dependence Information for Family Members Family members of patients who have been prescribed buprenorphine/naloxone for treatment of opioid addiction
Guidelines for Cancer Pain Management in Substance Misusers Dr Jane Neerkin, Dr Chi-Chi Cheung and Dr Caroline Stirling
 Guidelines for Cancer Pain Management in Substance Misusers Dr Jane Neerkin, Dr Chi-Chi Cheung and Dr Caroline Stirling Patients with a substance misuse history are at increased risk of receiving inadequate
Guidelines for Cancer Pain Management in Substance Misusers Dr Jane Neerkin, Dr Chi-Chi Cheung and Dr Caroline Stirling Patients with a substance misuse history are at increased risk of receiving inadequate
Testimony Engrossed House Bill 1101 Department of Human Services Senate Human Services Committee Senator Judy Lee, Chairman February 19, 2013
 Testimony Engrossed House Bill 1101 Department of Human Services Senate Human Services Committee Senator Judy Lee, Chairman February 19, 2013 Chairman Lee, members of the Senate Human Services Committee,
Testimony Engrossed House Bill 1101 Department of Human Services Senate Human Services Committee Senator Judy Lee, Chairman February 19, 2013 Chairman Lee, members of the Senate Human Services Committee,
The Federation of State Medical Boards 2013 Model Guidelines for Opioid Addiction Treatment in the Medical Office
 The Federation of State Medical Boards 2013 Model Guidelines for Opioid Addiction Treatment in the Medical Office Adopted April 2013 for Consideration by State Medical Boards 2002 FSMB Model Guidelines
The Federation of State Medical Boards 2013 Model Guidelines for Opioid Addiction Treatment in the Medical Office Adopted April 2013 for Consideration by State Medical Boards 2002 FSMB Model Guidelines
A Review of the Impacts of Opiate Use in Ontario: Summary Report
 A Review of the Impacts of Opiate Use in Ontario: Summary Report A Provincial Summary Report of the Impacts of the Discontinuation of Oxycontin in Ontario: January to August 2013 December 2013 This report
A Review of the Impacts of Opiate Use in Ontario: Summary Report A Provincial Summary Report of the Impacts of the Discontinuation of Oxycontin in Ontario: January to August 2013 December 2013 This report
Jane Maxwell, UT Addiction Research Institute, 512 232-0610. Prescription Pain Medications and Heroin: A Changing Picture
 Prescription Pain Medications and : A Changing Picture Jane Maxwell, Ph.D. Center for Social Work Research The University of Texas at Austin Disclosure to Participants Commercial Support: This educational
Prescription Pain Medications and : A Changing Picture Jane Maxwell, Ph.D. Center for Social Work Research The University of Texas at Austin Disclosure to Participants Commercial Support: This educational
Harnessing National Data Sets to Measure Safety of Opioid Treatment: National Survey on Drug Use and Health (NSDUH) and VA Data
 and VA Data") Harnessing National Data Sets to Measure Safety of Opioid Treatment: National Survey on Drug Use and Health (NSDUH) and VA Data William C. Becker, MD Assistant Professor, General Internal Medicine VA Connecticut
Harnessing National Data Sets to Measure Safety of Opioid Treatment: National Survey on Drug Use and Health (NSDUH) and VA Data William C. Becker, MD Assistant Professor, General Internal Medicine VA Connecticut
Opioid overdose can occur when a patient misunderstands the directions
 Facts About Opioid Overdose How Does an Overdose Occur? Opioid overdose can occur when a patient misunderstands the directions for use, accidentally takes an extra dose, or deliberately misuses a prescription
Facts About Opioid Overdose How Does an Overdose Occur? Opioid overdose can occur when a patient misunderstands the directions for use, accidentally takes an extra dose, or deliberately misuses a prescription
Update on Buprenorphine: Induction and Ongoing Care
 Update on Buprenorphine: Induction and Ongoing Care Elizabeth F. Howell, M.D., DFAPA, FASAM Department of Psychiatry, University of Utah School of Medicine North Carolina Addiction Medicine Conference
Update on Buprenorphine: Induction and Ongoing Care Elizabeth F. Howell, M.D., DFAPA, FASAM Department of Psychiatry, University of Utah School of Medicine North Carolina Addiction Medicine Conference
MANAGEMENT OF CHRONIC NON MALIGNANT PAIN
 MANAGEMENT OF CHRONIC NON MALIGNANT PAIN Introduction The Manitoba Prescribing Practices Program (MPPP) recognizes the important role served by physicians in relieving pain and suffering and acknowledges
MANAGEMENT OF CHRONIC NON MALIGNANT PAIN Introduction The Manitoba Prescribing Practices Program (MPPP) recognizes the important role served by physicians in relieving pain and suffering and acknowledges
Neurobiology and Treatment of Opioid Dependence. Nebraska MAT Training September 29, 2011
 Neurobiology and Treatment of Opioid Dependence Nebraska MAT Training September 29, 2011 Top 5 primary illegal drugs for persons age 18 29 entering treatment, % 30 25 20 15 10 Heroin or Prescription Opioids
Neurobiology and Treatment of Opioid Dependence Nebraska MAT Training September 29, 2011 Top 5 primary illegal drugs for persons age 18 29 entering treatment, % 30 25 20 15 10 Heroin or Prescription Opioids
Drug-related hospital stays in Australia 1993 2009
 in Australia 1993 29 Prepared by Funded by Amanda Roxburgh and Lucy Burns, National Drug and Alcohol Research Centre the Australian Government Department of Health and Ageing Recommended Roxburgh, A.,
in Australia 1993 29 Prepared by Funded by Amanda Roxburgh and Lucy Burns, National Drug and Alcohol Research Centre the Australian Government Department of Health and Ageing Recommended Roxburgh, A.,
Policy for the issue of permits to prescribe Schedule 8 poisons
 Policy for the issue of permits to prescribe Schedule 8 poisons May 2011 Introduction The Victorian Drugs, Poisons and Controlled Substances (DPCS) legislation sets out certain circumstances when a medical
Policy for the issue of permits to prescribe Schedule 8 poisons May 2011 Introduction The Victorian Drugs, Poisons and Controlled Substances (DPCS) legislation sets out certain circumstances when a medical
Prescriber Behavior, Pain Treatment and Addiction Treatment
 Prescriber Behavior, Pain Treatment and Addiction Treatment Mary Fleming, M.S. Director, Office of Policy, Planning, and Innovation Substance Abuse and Mental Health Services Administration NGA Policy
Prescriber Behavior, Pain Treatment and Addiction Treatment Mary Fleming, M.S. Director, Office of Policy, Planning, and Innovation Substance Abuse and Mental Health Services Administration NGA Policy
Massachusetts Substance Abuse Policy and Practices. Senator Jennifer L. Flanagan Massachusetts Worcester and Middlesex District
 Massachusetts Substance Abuse Policy and Practices Senator Jennifer L. Flanagan Massachusetts Worcester and Middlesex District November 2014 Substance Abuse and Addiction National and State opioid abuse
Massachusetts Substance Abuse Policy and Practices Senator Jennifer L. Flanagan Massachusetts Worcester and Middlesex District November 2014 Substance Abuse and Addiction National and State opioid abuse
young adults were at increased risk of nonmedical opioid use, which increases the risk of future substance use disorders. 5
 TITLE: Suboxone Versus Methadone for the Detoxification of Patients Addicted to Prescription Opioids: A Review of Comparative Clinical Effectiveness, Safety, and Guidelines DATE: 13 February 2014 CONTEXT
TITLE: Suboxone Versus Methadone for the Detoxification of Patients Addicted to Prescription Opioids: A Review of Comparative Clinical Effectiveness, Safety, and Guidelines DATE: 13 February 2014 CONTEXT
Impact of Systematic Review on Health Services: The US Experience
 Impact of Systematic Review on Health Services: The US Experience Walter Ling MD Integrated Substance Abuse Programs (ISAP) UCLA The effectiveness of interventions for addictions: The Drug and Alcohol
Impact of Systematic Review on Health Services: The US Experience Walter Ling MD Integrated Substance Abuse Programs (ISAP) UCLA The effectiveness of interventions for addictions: The Drug and Alcohol
Opioid Prescribing for Chronic Pain: Guidelines for Marin County Clinicians
 Opioid Prescribing for Chronic Pain: Guidelines for Marin County Clinicians Although prescription pain medications are intended to improve the lives of people with pain, their increased use and misuse
Opioid Prescribing for Chronic Pain: Guidelines for Marin County Clinicians Although prescription pain medications are intended to improve the lives of people with pain, their increased use and misuse
Applicant Webinar for BJA s Drug Court Discretionary Grant Solicitation
 Applicant Webinar for BJA s Drug Court Discretionary Grant Solicitation Cynthia Caporizzo, Senior Criminal Justice Advisor, Office of National Drug Control Policy (ONDCP) - Review of the administration
Applicant Webinar for BJA s Drug Court Discretionary Grant Solicitation Cynthia Caporizzo, Senior Criminal Justice Advisor, Office of National Drug Control Policy (ONDCP) - Review of the administration
August 2011. A. Introduction
 Recommendations of the Expert Group on the Regulatory Framework for products containing buprenorphine / naloxone and buprenorphine-only for the treatment of opioid dependence August 2011 A. Introduction
Recommendations of the Expert Group on the Regulatory Framework for products containing buprenorphine / naloxone and buprenorphine-only for the treatment of opioid dependence August 2011 A. Introduction
Triage, Assessment & Treatment Methadone 101/Hospitalist Workshop
 Triage, Assessment & Treatment Methadone 101/Hospitalist Workshop Launette Rieb, MSc, MD, CCFP, FCFP Clinical Associate Professor, Dept. Family Practice UBC American Board of Addiction Medicine Certified
Triage, Assessment & Treatment Methadone 101/Hospitalist Workshop Launette Rieb, MSc, MD, CCFP, FCFP Clinical Associate Professor, Dept. Family Practice UBC American Board of Addiction Medicine Certified
Table of Contents. I. Introduction... 2. II. Summary... 3. A. Total Drug Intoxication Deaths... 5. B. Opioid-Related Deaths... 9
 Table of Contents I. Introduction... 2 II. Summary... 3 III. Charts A. Total Drug Intoxication Deaths... 5 B. Opioid-Related Deaths... 9 C. Heroin-Related Deaths... 11 D. Prescription Opioid-Related Deaths...
Table of Contents I. Introduction... 2 II. Summary... 3 III. Charts A. Total Drug Intoxication Deaths... 5 B. Opioid-Related Deaths... 9 C. Heroin-Related Deaths... 11 D. Prescription Opioid-Related Deaths...
OVERVIEW WHAT IS POLyDRUG USE? Different examples of polydrug use
 Petrol, paint and other Polydrug inhalants use 237 11 Polydrug use Overview What is polydrug use? Reasons for polydrug use What are the harms of polydrug use? How to assess a person who uses several drugs
Petrol, paint and other Polydrug inhalants use 237 11 Polydrug use Overview What is polydrug use? Reasons for polydrug use What are the harms of polydrug use? How to assess a person who uses several drugs
Opioid dependence is a chronic relapsing condition that
 PEER REVIEWED FEATURE Treatment of patients with opioid dependence NICHOLAS LINTZERIS BMedSci, MB BS, PhD, FAChAM The prevalence of opioid dependence is growing in Australia with the increased use of pharmaceutical
PEER REVIEWED FEATURE Treatment of patients with opioid dependence NICHOLAS LINTZERIS BMedSci, MB BS, PhD, FAChAM The prevalence of opioid dependence is growing in Australia with the increased use of pharmaceutical
UNM Pain Center: Addressing New Mexico s Public Health Crises of Pain, Addiction, and Unintentional Opioid Overdose Deaths
 UNM Pain Center: Addressing New Mexico s Public Health Crises of Pain, Addiction, and Unintentional Opioid Overdose Deaths Joanna G Katzman, M.D., M.S.P.H Director, UNM Pain Center Associate Professor,
UNM Pain Center: Addressing New Mexico s Public Health Crises of Pain, Addiction, and Unintentional Opioid Overdose Deaths Joanna G Katzman, M.D., M.S.P.H Director, UNM Pain Center Associate Professor,
Populations at risk for opioid overdose
 Populations at risk for opioid overdose Len Paulozzi, MD, MPH Division of Unintentional Injury Prevention National Center for Injury Prevention and Control Centers for Disease Control and Prevention April
Populations at risk for opioid overdose Len Paulozzi, MD, MPH Division of Unintentional Injury Prevention National Center for Injury Prevention and Control Centers for Disease Control and Prevention April
Opioid Addiction & Corrections
 Opioid Addiction & Corrections Medication Assisted Treatment in the Connecticut Department of Correction April 30, 2015--CJPAC Kathleen F. Maurer, MD, MPH, MBA Medical Director and Director of Health and
Opioid Addiction & Corrections Medication Assisted Treatment in the Connecticut Department of Correction April 30, 2015--CJPAC Kathleen F. Maurer, MD, MPH, MBA Medical Director and Director of Health and
H-SOAP STUDY. Hospital-based Services for Opioid- and Alcohol-addicted Patients
 H-SOAP STUDY Hospital-based Services for Opioid- and Alcohol-addicted Patients Meldon Kahan, Anita Srivastava, Kate Hardy, Sarah Clarke Canadian Society of Addiction Medicine 2014 October 17, 2014 1 Few
H-SOAP STUDY Hospital-based Services for Opioid- and Alcohol-addicted Patients Meldon Kahan, Anita Srivastava, Kate Hardy, Sarah Clarke Canadian Society of Addiction Medicine 2014 October 17, 2014 1 Few
Integrating Medication- Assisted Treatment (MAT) for Opioid Use Disorders into Behavioral and Physical Healthcare Settings
 for Opioid Use Disorders into Behavioral and Physical Healthcare Settings") Integrating Medication- Assisted Treatment (MAT) for Opioid Use Disorders into Behavioral and Physical Healthcare Settings All-Ohio Conference 3/27/2015 Christina M. Delos Reyes, MD Medical Consultant,
Integrating Medication- Assisted Treatment (MAT) for Opioid Use Disorders into Behavioral and Physical Healthcare Settings All-Ohio Conference 3/27/2015 Christina M. Delos Reyes, MD Medical Consultant,
How To Treat A Drug Addiction
 1 About drugs Drugs are substances that change a person s physical or mental state. The vast majority of drugs are used to treat medical conditions, both physical and mental. Some, however, are used outside
1 About drugs Drugs are substances that change a person s physical or mental state. The vast majority of drugs are used to treat medical conditions, both physical and mental. Some, however, are used outside
Information for Pharmacists
 Page 43 by 42 CFR part 2. A general authorization for the release of medical or other information is NOT sufficient for this purpose. Information for Pharmacists SUBOXONE (buprenorphine HCl/naloxone HCl
Page 43 by 42 CFR part 2. A general authorization for the release of medical or other information is NOT sufficient for this purpose. Information for Pharmacists SUBOXONE (buprenorphine HCl/naloxone HCl
DEVELOPING MANUFACTURING SUPPLYING. Naltrexone Implants. Manufactured by NalPharm Ltd WWW.NALPHARM.COM
 DEVELOPING MANUFACTURING SUPPLYING Naltrexone Implants Background to Nalpharm NalPharm is a specialist pharmaceutical company supplying proprietary branded medications and generic drugs in the area of
DEVELOPING MANUFACTURING SUPPLYING Naltrexone Implants Background to Nalpharm NalPharm is a specialist pharmaceutical company supplying proprietary branded medications and generic drugs in the area of
Beyond SBIRT: Integrating Addiction Medicine into Primary Care
 Beyond SBIRT: Integrating Addiction Medicine into Primary Care Community Clinic Association of Los Angeles County 14 th Annual Health Care Symposium March 6, 2015 Keith Heinzerling MD, Karen Lamp MD; Allison
Beyond SBIRT: Integrating Addiction Medicine into Primary Care Community Clinic Association of Los Angeles County 14 th Annual Health Care Symposium March 6, 2015 Keith Heinzerling MD, Karen Lamp MD; Allison
Judith Martin, MD Medical Director, Substance Abuse Services, San Francisco DPH
 Western Occupational & Environmental Medical Association CME Webinar April 17, 2013 Judith Martin, MD Medical Director, Substance Abuse Services, San Francisco DPH PLEASE STAND BY - WEBINAR WILL BEGIN
Western Occupational & Environmental Medical Association CME Webinar April 17, 2013 Judith Martin, MD Medical Director, Substance Abuse Services, San Francisco DPH PLEASE STAND BY - WEBINAR WILL BEGIN
A G U I D E F O R U S E R S N a l t r e x o n e U
 A GUIDE FOR USERS UNaltrexone abstinence not using a particular drug; being drug-free. opioid antagonist a drug which blocks the effects of opioid drugs. dependence the drug has become central to a person
A GUIDE FOR USERS UNaltrexone abstinence not using a particular drug; being drug-free. opioid antagonist a drug which blocks the effects of opioid drugs. dependence the drug has become central to a person
Resources for the Prevention and Treatment of Substance Use Disorders
 Resources for the Prevention and Treatment of Substance Use Disorders Table of Contents Age-standardized DALYs, alcohol and drug use disorders, per 100 000 Age-standardized death rates, alcohol and drug
Resources for the Prevention and Treatment of Substance Use Disorders Table of Contents Age-standardized DALYs, alcohol and drug use disorders, per 100 000 Age-standardized death rates, alcohol and drug
Tufts Health Care Institute Program on Opioid Risk Management Pharmacotherapy for Prescription Opioid Addiction: Implications for Pain Management
 Tufts Health Care Institute Program on Opioid Risk Management Pharmacotherapy for Prescription Opioid Addiction: Implications for Pain Management June 10 and 11, 2011 Executive Summary Introduction Opioid
Tufts Health Care Institute Program on Opioid Risk Management Pharmacotherapy for Prescription Opioid Addiction: Implications for Pain Management June 10 and 11, 2011 Executive Summary Introduction Opioid
Naltrexone Pellet Treatment for Opiate, Heroin, and Alcohol Addiction. Frequently Asked Questions
 Naltrexone Pellet Treatment for Opiate, Heroin, and Alcohol Addiction Frequently Asked Questions What is Naltrexone? Naltrexone is a prescription drug that effectively blocks the effects of heroin, alcohol,
Naltrexone Pellet Treatment for Opiate, Heroin, and Alcohol Addiction Frequently Asked Questions What is Naltrexone? Naltrexone is a prescription drug that effectively blocks the effects of heroin, alcohol,
TENNESSEE BOARD OF MEDICAL EXAMINERS POLICY STATEMENT OFFICE-BASED TREATMENT OF OPIOID ADDICTION
 TENNESSEE BOARD OF MEDICAL EXAMINERS POLICY STATEMENT OFFICE-BASED TREATMENT OF OPIOID ADDICTION The Tennessee Board of Medical Examiners has reviewed the Model Policy Guidelines for Opioid Addiction Treatment
TENNESSEE BOARD OF MEDICAL EXAMINERS POLICY STATEMENT OFFICE-BASED TREATMENT OF OPIOID ADDICTION The Tennessee Board of Medical Examiners has reviewed the Model Policy Guidelines for Opioid Addiction Treatment
Patients are still addicted Buprenorphine is simply a substitute for heroin or
 BUPRENORPHINE TREATMENT: A Training For Multidisciplinary Addiction Professionals Module VI: Myths About the Use of Medication in Recovery Patients are still addicted Buprenorphine is simply a substitute
BUPRENORPHINE TREATMENT: A Training For Multidisciplinary Addiction Professionals Module VI: Myths About the Use of Medication in Recovery Patients are still addicted Buprenorphine is simply a substitute
These changes are prominent in individuals with severe disorders, but also occur at the mild or moderate level.
 Substance-Related Disorders DSM-V Many people use words like alcoholism, drug dependence and addiction as general descriptive terms without a clear understanding of their meaning. What does it really mean
Substance-Related Disorders DSM-V Many people use words like alcoholism, drug dependence and addiction as general descriptive terms without a clear understanding of their meaning. What does it really mean
Pain and problem drug use
 Pain and problem drug use Information for patients Prepared by the British Pain Society in consultation with the Royal College of Psychiatrists, the Royal College of General Practitioners and the Advisory
Pain and problem drug use Information for patients Prepared by the British Pain Society in consultation with the Royal College of Psychiatrists, the Royal College of General Practitioners and the Advisory
Use of Buprenorphine in the Treatment of Opioid Addiction
 Use of Buprenorphine in the Treatment of Opioid Addiction Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Executive Summary Which of the following is an
Use of Buprenorphine in the Treatment of Opioid Addiction Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Executive Summary Which of the following is an
Powder speed, whiz, velocity - Usually snorted, ingested or injected
 Dr Christine Watson Powder speed, whiz, velocity - Usually snorted, ingested or injected -most common -Approximately 10% purity -Generally produced locally Sticky/oily/waxy form Base, paste, point, pure,
Dr Christine Watson Powder speed, whiz, velocity - Usually snorted, ingested or injected -most common -Approximately 10% purity -Generally produced locally Sticky/oily/waxy form Base, paste, point, pure,
Frequently asked questions
 Naltrexone Pellet Treatment for Opiate, Heroin, and Alcohol Addiction Frequently asked questions What is Naltrexone? Naltrexone is a prescription drug that completely blocks the effects of all opioid drugs
Naltrexone Pellet Treatment for Opiate, Heroin, and Alcohol Addiction Frequently asked questions What is Naltrexone? Naltrexone is a prescription drug that completely blocks the effects of all opioid drugs
Prescription Drug Addiction
 Prescription Drug Addiction Dr Gilbert Whitton FAChAM Clinical Director Drug & Alcohol Loddon Mallee Murray Medicare Local Deniliquin 14 th May 2014 Prescription Drug Addiction Overview History Benzodiazepines
Prescription Drug Addiction Dr Gilbert Whitton FAChAM Clinical Director Drug & Alcohol Loddon Mallee Murray Medicare Local Deniliquin 14 th May 2014 Prescription Drug Addiction Overview History Benzodiazepines
INFO Brief. Prescription Opioid Use: Pain Management and Drug Abuse In King County and Washington State
 ADAI-IB 23-3 INFO Brief Prescription Opioid Use: Pain Management and Drug Abuse In King County and Washington State O ctober 23 Caleb Banta-Green (Alcohol and Drug Abuse Institute, University of Washington),
ADAI-IB 23-3 INFO Brief Prescription Opioid Use: Pain Management and Drug Abuse In King County and Washington State O ctober 23 Caleb Banta-Green (Alcohol and Drug Abuse Institute, University of Washington),
Treatment and Interventions for Opioid Addictions: Challenges From the Medical Director s Perspective
 Treatment and Interventions for Opioid Addictions: Challenges From the Medical Director s Perspective Dale K. Adair, MD Medical Director/Chief Psychiatric Officer OMHSAS 1 Treatment and Interventions for
Treatment and Interventions for Opioid Addictions: Challenges From the Medical Director s Perspective Dale K. Adair, MD Medical Director/Chief Psychiatric Officer OMHSAS 1 Treatment and Interventions for
National Perspectives in Medication Assisted Treatment
 National Perspectives in Medication Assisted Treatment Addiction Medicine Asheville March 21,2014 Melinda Campopiano, MD Medical Officer Substance Abuse & Mental Health Services Administration Guten Appetit
National Perspectives in Medication Assisted Treatment Addiction Medicine Asheville March 21,2014 Melinda Campopiano, MD Medical Officer Substance Abuse & Mental Health Services Administration Guten Appetit
Abstral Prescriber and Pharmacist Guide
 Abstral Prescriber and Pharmacist Guide fentanyl citrate sublingual tablets Introduction The Abstral Prescriber and Pharmacist Guide is designed to support healthcare professionals in the diagnosis of
Abstral Prescriber and Pharmacist Guide fentanyl citrate sublingual tablets Introduction The Abstral Prescriber and Pharmacist Guide is designed to support healthcare professionals in the diagnosis of
In 2010, approximately 8 million Americans 18 years and older were dependent on alcohol.
 Vivitrol Pilot Study: SEMCA/Treatment Providers Collaborative Efforts with the treatment of Opioid Dependent Clients Hakeem Lumumba, PhD, CAADC SEMCA Scott Schadel, MSW, LMSW, CAADC HEGIRA PROGRAMS, INC.
Vivitrol Pilot Study: SEMCA/Treatment Providers Collaborative Efforts with the treatment of Opioid Dependent Clients Hakeem Lumumba, PhD, CAADC SEMCA Scott Schadel, MSW, LMSW, CAADC HEGIRA PROGRAMS, INC.
Financial Disclosures
 Opioid Agonist Therapy: To Maintain or Not To Maintain - A Case Discussion PCSS-MAT American Psychiatric Association Drs. Ed Salsitz, John Renner, Timothy Fong April 14, 2015 Financial Disclosures Edwin
Opioid Agonist Therapy: To Maintain or Not To Maintain - A Case Discussion PCSS-MAT American Psychiatric Association Drs. Ed Salsitz, John Renner, Timothy Fong April 14, 2015 Financial Disclosures Edwin
Drug use and harm in rural Australia: Establishing a Rural Drug Monitoring System
 Drug use and harm in rural Australia: Establishing a Rural Drug Monitoring System Dr Jennifer Johnston Research Fellow SCHOOL OF PUBLIC HEALTH Funding to attend NRHC 2015 from University Centre for Rural
Drug use and harm in rural Australia: Establishing a Rural Drug Monitoring System Dr Jennifer Johnston Research Fellow SCHOOL OF PUBLIC HEALTH Funding to attend NRHC 2015 from University Centre for Rural
Scientific Facts on. Psychoactive Drugs. Tobacco, Alcohol, and Illicit Substances
 page 1/5 Scientific Facts on Psychoactive Drugs Tobacco, Alcohol, and Illicit Substances Source document: WHO (2004) Summary & Details: GreenFacts Context - Psychoactive drugs such as tobacco, alcohol,
page 1/5 Scientific Facts on Psychoactive Drugs Tobacco, Alcohol, and Illicit Substances Source document: WHO (2004) Summary & Details: GreenFacts Context - Psychoactive drugs such as tobacco, alcohol,
Discontinuation: Involuntary Discharge
 Discontinuation: Involuntary Discharge TYPICALLY A PROCESS NOT AN EVENT Objectives 2 Review indications for discharge. Develop a therapeutic approach, in the context of the nature of Substance Use Disorders.
Discontinuation: Involuntary Discharge TYPICALLY A PROCESS NOT AN EVENT Objectives 2 Review indications for discharge. Develop a therapeutic approach, in the context of the nature of Substance Use Disorders.
Research Article Predictors of Dropout from Inpatient Opioid Detoxification with Buprenorphine: A Chart Review
 Addiction, Article ID 965267, 5 pages http://dx.doi.org/10.1155/2014/965267 Research Article Predictors of Dropout from Inpatient Opioid Detoxification with Buprenorphine: A Chart Review Anders Hakansson
Addiction, Article ID 965267, 5 pages http://dx.doi.org/10.1155/2014/965267 Research Article Predictors of Dropout from Inpatient Opioid Detoxification with Buprenorphine: A Chart Review Anders Hakansson
Opioid/Opiate Dependent Pregnant Women
 Opioid/Opiate Dependent Pregnant Women The epidemic, safety, stigma, and how to help. Presented by Lisa Ramirez MA,LCDC & Kerby Stewart MD The prescription painkiller epidemic is killing more women than
Opioid/Opiate Dependent Pregnant Women The epidemic, safety, stigma, and how to help. Presented by Lisa Ramirez MA,LCDC & Kerby Stewart MD The prescription painkiller epidemic is killing more women than
Opiate Abusers What can the GP do?
 Opiate Abusers What can the GP do? Office Based management of Opiate Addiction Dr Nigel Hawkins 1 Managing opiate abuse in General Practice The extent of Opiate Abuse in Australia What treatment options
Opiate Abusers What can the GP do? Office Based management of Opiate Addiction Dr Nigel Hawkins 1 Managing opiate abuse in General Practice The extent of Opiate Abuse in Australia What treatment options
Do we need special programs for aging drug users?
 High risk drug use and drug treatment in Europe 2014 EMCDDA event: Continuity and Change Lisbon, 24-26 September 2014 Do we need special programs for aging drug users? Andrej Kastelic EUROPAD General Secretary
High risk drug use and drug treatment in Europe 2014 EMCDDA event: Continuity and Change Lisbon, 24-26 September 2014 Do we need special programs for aging drug users? Andrej Kastelic EUROPAD General Secretary
Dependence and Addiction. Marek C. Chawarski, Ph.D. Yale University David Metzger, Ph.D. University of Pennsylvania
 Dependence and Addiction Marek C. Chawarski, Ph.D. Yale University David Metzger, Ph.D. University of Pennsylvania Overview Heroin and other opiates The disease of heroin addiction or dependence Effective
Dependence and Addiction Marek C. Chawarski, Ph.D. Yale University David Metzger, Ph.D. University of Pennsylvania Overview Heroin and other opiates The disease of heroin addiction or dependence Effective
Medication-Assisted Addiction Treatment
 Medication-Assisted Addiction Treatment Molly Carney, Ph.D., M.B.A. Executive Director Evergreen Treatment Services Seattle, WA What is MAT? MAT is the use of medications, in combination with counseling
Medication-Assisted Addiction Treatment Molly Carney, Ph.D., M.B.A. Executive Director Evergreen Treatment Services Seattle, WA What is MAT? MAT is the use of medications, in combination with counseling
Using Buprenorphine in an Opioid Treatment Program
 Using Buprenorphine in an Opioid Treatment Program Thomas E. Freese, PhD Director of Training, UCLA Integrated Substance Abuse Programs Director, Pacific Southwest Addiction Technology Transfer Center
Using Buprenorphine in an Opioid Treatment Program Thomas E. Freese, PhD Director of Training, UCLA Integrated Substance Abuse Programs Director, Pacific Southwest Addiction Technology Transfer Center
Buprenorphine/Naloxone Training Workshop for Medical Practitioners
 Buprenorphine/Naloxone Training Workshop for Medical Practitioners Program developed by Dr Nicholas Lintzeris MBBS, PhD, FAChAM (RACP) Turning Point Alcohol and Drug Centre, Melbourne, Australia Federation
Buprenorphine/Naloxone Training Workshop for Medical Practitioners Program developed by Dr Nicholas Lintzeris MBBS, PhD, FAChAM (RACP) Turning Point Alcohol and Drug Centre, Melbourne, Australia Federation
Prescription Medication Abuse: Skills for Prevention and Intervention
 Prescription Medication Abuse: Skills for Prevention and Intervention icare Partnership www.icarenc.org James Finch, MD North Carolina Society of Addiction Medicine NC Governor s Institute on Alcohol and
Prescription Medication Abuse: Skills for Prevention and Intervention icare Partnership www.icarenc.org James Finch, MD North Carolina Society of Addiction Medicine NC Governor s Institute on Alcohol and
MEDICAL ASSISTANCE BULLETIN
 ISSUE DATE SUBJECT EFFECTIVE DATE MEDICAL ASSISTANCE BULLETIN NUMBER *See below BY Prior Authorization of Opiate Dependence Treatments Pharmacy Service Leesa M. Allen, Deputy Secretary Office of Medical
ISSUE DATE SUBJECT EFFECTIVE DATE MEDICAL ASSISTANCE BULLETIN NUMBER *See below BY Prior Authorization of Opiate Dependence Treatments Pharmacy Service Leesa M. Allen, Deputy Secretary Office of Medical
MEDICATION ASSISTED TREATMENT FOR OPIOID ADDICTION
 MEDICATION ASSISTED TREATMENT FOR OPIOID ADDICTION Mark Fisher Program Administrator State Opioid Treatment Adminstrator Kentucky Division of Behavioral Health OBJECTIVES Learn about types of opioids and
MEDICATION ASSISTED TREATMENT FOR OPIOID ADDICTION Mark Fisher Program Administrator State Opioid Treatment Adminstrator Kentucky Division of Behavioral Health OBJECTIVES Learn about types of opioids and
Guidelines for the Use of Controlled Substances in the Treatment of Pain Adopted by the New Hampshire Medical Society, July 1998
 Guidelines for the Use of Controlled Substances in the Treatment of Pain Adopted by the New Hampshire Medical Society, July 1998 Section I: Preamble The New Hampshire Medical Society believes that principles
Guidelines for the Use of Controlled Substances in the Treatment of Pain Adopted by the New Hampshire Medical Society, July 1998 Section I: Preamble The New Hampshire Medical Society believes that principles
IN THE GENERAL ASSEMBLY STATE OF. Ensuring Access to Medication Assisted Treatment Act
 IN THE GENERAL ASSEMBLY STATE OF Ensuring Access to Medication Assisted Treatment Act 1 Be it enacted by the People of the State of Assembly:, represented in the General 1 1 1 1 Section 1. Title. This
IN THE GENERAL ASSEMBLY STATE OF Ensuring Access to Medication Assisted Treatment Act 1 Be it enacted by the People of the State of Assembly:, represented in the General 1 1 1 1 Section 1. Title. This
How To Get A Tirf
 Transmucosal Immediate Release Fentanyl (TIRF) Products Risk Evaluation and Mitigation Strategy (REMS) Education Program for Prescribers and Pharmacists Products Covered Under This Program Abstral (fentanyl)
Transmucosal Immediate Release Fentanyl (TIRF) Products Risk Evaluation and Mitigation Strategy (REMS) Education Program for Prescribers and Pharmacists Products Covered Under This Program Abstral (fentanyl)