),1$/5(3257'HFHPEHU±0DUFK. Joan G.M. Deckers François G. Schellevis
|
|
|
- Drusilla Morrison
- 8 years ago
- Views:
Transcription
1 +($/7+,1)250$7,21)52035,0$5<&$5( ),1$/5(3257'HFHPEHU±0DUFK Joan G.M. Deckers François G. Schellevis
2 Project title: Project number: Contract number: Programme: Institute: Project coordinator: Project leader: Health information from primary care 2001/IND/2096 SI (2001CVG3-508) Health Monitoring Directorate General SanCo European Commission Netherlands Institute for Health Services Research (NIVEL) PO Box BN UTRECHT the Netherlands Tel Fax Joan G.M. Deckers François G. Schellevis ISBN nivel@nivel.nl 2004 NIVEL, Postbus 1568, 3500 BN UTRECHT 7KLVUHSRUWZDVSURGXFHGE\DFRQWUDFWRUIRU+HDOWK &RQVXPHU3URWHFWLRQ'LUHFWRUDWH *HQHUDODQGUHSUHVHQWVWKHYLHZVRIWKHDXWKRU7KHVHYLHZVKDYHQRWEHHQDGRSWHGRULQ DQ\ZD\DSSURYHGE\WKH&RPPLVVLRQDQGGRQRWQHFHVVDULO\UHSUHVHQWWKHYLHZRIWKH &RPPLVVLRQRUWKH'LUHFWRUDWH*HQHUDOIRU+HDOWKDQG&RQVXPHU3URWHFWLRQ7KH (XURSHDQ&RPPLVVLRQGRHVQRWJXDUDQWHHWKHDFFXUDF\RIWKHGDWDLQFOXGHGLQWKLVVWXG\ QRUGRHVLWDFFHSWUHVSRQVLELOLW\IRUDQ\XVHPDGHWKHUHRI

3 Contents ([HFXWLYH6XPPDU\ $EEUHYLDWLRQV,QWURGXFWLRQ 1.1 Background Project aims Participants and meetings Overview of the report 11 'HVFULSWLRQRISULPDU\FDUHUHJLVWUDWLRQQHWZRUNV 2.1 Summary Background Purpose Methods Findings Future of primary care networks Conclusion 19 3ULPDU\FDUH±VLWXDWLRQLQVHYHQ(XURSHDQFRXQWULHV 3.1 Summary Background Purpose Methods Findings New developments Conclusion 26 'HYHORSPHQWRIKHDOWKLQGLFDWRUSURILOHV 4.1 Summary Background Purpose Methods Results Conclusion 31,QWHUQDWLRQDOFRPSDULVRQRIGLVHDVHV 5.1 Summary Introduction Methods and general results Asthma Low back pain Chickenpox 38!"$#%&('*) +,+- 3

4 5.7 Depression Diabetes mellitus Gastroenteritis Herper zoster Stroke Conclusion 49 &RQFOXVLRQVDQGUHFRPPHQGDWLRQV 6.1 Introduction Primary care networks Primary care in seven European countries Health indicator profiles International comparison of diseases Future developments Final conclusion 54 $FNQRZOHGJPHQWV 5HIHUHQFHV $SSHQGLFHV 4!"$#%&('*) +,+-

5 ([HFXWLYH6XPPDU\ This is the final report of the project Health Information from Primary Care which was carried out between December 1, 2001 and March 31, 2004 as part of the Health Monitoring sub-programme of the Public Health Programme of the European Commission (Directorate-General Health and Consumer Protection). 2EMHFWLYH The objective of the project was (1) to establish the appropriateness of information from routine primary care as a source for epidemiological data on European Community Health Indicators and (2) to develop and test the feasibility of Health Indicator Profiles for establishing the validity and comparability of the information from Member States. A secondary aim was to extend the project activities to EU Member States which cannot deliver these epidemiological data so far. $FWLYLWLHV The project activities included the following: (1) collect epidemiological information for eight selected diseases in eight primary care based networks; (2) perform site visits with standardised questionnaires and checklist to the participating primary care networks to collect methodological and circumstantial information about the provided epidemiological data; (3) develop Health Indicator Profiles for the selected diseases to clarify the appropriateness of primary care as source of epidemiological information and (4) to provide information on the validity and international comparability of information from primary care; (5) contact representatives from non-participating countries in order to study the possibilities of collecting and/or delivering data from primary care, (6) formulate recommendations on data collection and data analysis by primary care networks and the suitability of primary care as information source. 5HVXOWV The results of the project can be summarised as follows: œ Eight primary care networks in Belgium, England & Wales, France (two networks), Germany, the Netherlands, Portugal and Spain delivered epidemiological information. In general, the networks comprise a stable group of general practitioners and monitor a representative sample of the general population (either at regional or national level). All networks apply procedures to ensure the quality of the collected data; œ Epidemiological information was obtained for acute diarrhoea/gastroenteritis, asthma, low back pain, chickenpox, depression, diabetes mellitus, herpes zoster and stroke/tia. For these conditions information was available from at least three countries in the period ; œ Specific health indicator profiles (HIPs) have been developed for each disease. These profiles contain information on epidemiological, clinical and contextual information per country;!"$#%&('*) +,+- 5
 to develop and test the feasibility of Health Indicator Profiles for establishing the validity and comparability of the information from Member States.")
6 !"$#%&('*) +,+œ œ Health indicator profiles were applied to the information obtained for the selected diseases. The least variation in clinical and contextual information was observed for chickenpox, diabetes mellitus, herpes zoster and stroke. The incidence rates for these diseases were to a large extent comparable or differences could be explained. The clinical and contextual information for asthma, low back pain, depression and gastroenteritis showed more variation in the incidence rates. When comparing primary care based morbidity data from different countries, differences with regard to the primary care context have to be taken into account. Although in most countries primary care is the entry point to the health care system, the number of directly accessible health care professionals providing diagnostic services, including the general practitioner, is variable between countries; A follow-up project concerning the provision of data from electronic medical records in primary care not only has participants from Spain, England & Wales, France and the Netherlands but also from Denmark, Italy and Malta. &RQFOXVLRQVDQGUHFRPPHQGDWLRQV œ Primary care networks can fill the information gap between population-based health information and hospital-based data; œ Minimum criteria that need to be fulfilled in order to establish a reliable primary care network include continuous surveillance of public health issues. Age and gender specificity is required for most conditions and the epidemiological denominator needs to established in a reliable way. The frequency of reporting depends on the disease but has to be at least annually and should be more frequent in case of infectious diseases. Lastly quality measures need to be in place; œ Structural funding is an essential prerequisite to establish and maintain a network; œ In those countries where the general practitioner does not function as a gatekeeper we recommend the inclusion of directly accessible specialists like paediatricians and gynaecologists in a primary care network; œ Health indicator profiles have been developed as a generic model to facilitate and validate international comparisons. Although developed for primary care, its use can be extended beyond that; œ Primary care networks can be used as an information source for chickenpox, diabetes mellitus, herpes zoster and stroke. More validation and harmonisation of findings for low back pain, chickenpox, depression and gastroenteritis has to be performed before primary care can be used as a valuable information source for these conditions. We expect the influences of different health care systems and cultural background to be smallest for somatic diseases affecting adults; œ Primary care networks can have a role in public health monitoring and therefore strongly advise the implementation of a primary care network in each country. 6

7 $EEUHYLDWLRQV $EEUHYLDWLRQ 'HVFULSWLRQ A&E Accidents and emergency BE Belgium COPD Chronic obstructive pulmonary disease CVA Cerebrovascular accident DE Germany DM Diabetes mellitus E&W England & Wales EC European commission ECHI European community health indicators EISS European influenza surveillance scheme ES Spain ES-CyL Spain (region Castilla & Léon) ES-MA Spain (region Madrid) ES-PV Spain (region Basque Country) ES-VA Spain (region Valencia) EUPHIN/HIEMS European union public health information network / health indicators exchange and monitoring system FR-I France Inserm FR-OR France Open Rome fte Full-time equivalent GP General practitioner HES Health examination survey HIP Health indicator profile HIS Health interview survey ICD International classification of disease ICPC International classification of primary care IOM Institute of medicine LBP Low back pain NIVEL Netherlands institute for health services research NL the Netherlands NL-NS2 the Netherlands (2 nd Dutch National Survey of General Practice) OMG Observatoire de la médecine générale PT Portugal SESAM Sächsischen epidemiologischen Studie in der Allegemeinmedizin SFMG la Société Française de médecine générale STD Sexually transmitted disease TIA Transient ischemic attack WHO World health organization WONCA World organization of family doctors!"$#%&('*) +,+- 7

8 8!"$#%&('*) +,+-

9 ,QWURGXFWLRQ %DFNJURXQG The Health Information from Primary Care project was funded by the European Commission, DG Sanco as part of the Community Action Programme on Health Monitoring (adopted ). The objective of the programme ZDVµWRFRQWULEXWHWR WKHHVWDEOLVKPHQWRID&RPPXQLW\KHDOWKPRQLWRULQJV\VWHPZKLFKPDNHVLWSRVVLEOHWR DPHDVXUHKHDOWKVWDWXVWUHQGVDQGGHWHUPLQDQWVWKURXJKRXWWKH&RPPXQLW\E IDFLOLWDWHWKHSODQQLQJPRQLWRULQJDQGHYDOXDWLRQRI&RPPXQLW\SURJUDPPHVDQG DFWLRQVDQGFSURYLGH0HPEHU6WDWHVZLWKDSSURSULDWHKHDOWKLQIRUPDWLRQWRPDNH FRPSDULVRQVDQGWRVXSSRUWWKHLUQDWLRQDOKHDOWKSROLFLHVE\HQFRXUDJLQJFRRSHUDWLRQ EHWZHHQ0HPEHU6WDWHVDQGLIQHFHVVDU\E\VXSSRUWLQJWKHLUDFWLRQWKURXJKSURPRWLQJ FRRUGLQDWLRQRIWKHLUSROLFLHVDQGSURJUDPPHVLQWKLVILHOGDQGHQFRXUDJLQJFRRSHUDWLRQ ZLWKQRQPHPEHUFRXQWULHVDQGWKHFRPSHWHQWLQWHUQDWLRQDORUJDQL]DWLRQV 1 A previous project ( Health Monitoring in Sentinel Practice Networks ) performed by our institute has made an inventory of primary care networks that collect primary care based data related to health status (i.e. morbidity) on a continuous basis. 2 Furthermore in this project a pilot study has been performed on the international comparability of disease data collected by primary care networks. In the scope of another project within the framework of the Health Monitoring Programme a set of European Community Health Indicators (ECHI) has been developed to prepare a Community health data exchange system. 3 This proposed list of health indicators includes diseases responsible for a large share of the burden of ill health and diseases related to certain risk factors or issues of prevention and health care. The need for comparable epidemiological data is identified as an important development area. The results and recommendations from these two projects were the basis for this project. A pan-european surveillance system using primary care networks already exists for influenza. 4 The European Influenza Surveillance Scheme (EISS) began in 1995 with the participation of seven countries: Belgium, France, Germany, the Netherlands, Portugal, Spain and the United Kingdom. The clinical surveillance of influenza is based on reports from GPs in primary care networks. There are many reasons why influenza surveillance networks in Europe have got together to share information. Influenza is a communicable disease that spreads rapidly and efficiently; this means that it is very beneficial for countries to be informed about influenza activity in neighbouring countries (clinical incidences and types/subtypes/strains). Other benefits of working together are that surveillance systems can learn from each other and improve their surveillance activities. Collaboration also helps the creation and development of disease surveillance networks across the whole of Europe.!"$#%&('*) +,+- 9

10 3URMHFWDLPV The project seeks primarily to contribute to the European Union Public Health Information Network / Health Indicators Exchange and Monitoring System (EUPHIN/HIEMS). The project aim is to study the feasibility of providing epidemiological information on health indicators. Data will be derived from routine primary care delivery for diseases that are exclusively or predominantly managed in primary care. Health Indicator Profiles (HIP) will be developed that help to clarify the appropriateness of primary care as source of epidemiological information. A second aim of these profiles will be to provide information on the validity and international comparability of information from primary care. This will allow adequate interpretation of the information and enable valid comparisons between countries. Moreover an attempt will be made to extend the project activities to EU member states which so far have not been able to deliver these epidemiological data. 3DUWLFLSDQWVDQGPHHWLQJV The project was carried out at the Netherlands Institute for Health Services Research (NIVEL) by Joan Deckers (researcher) and François Schellevis (project leader). The European primary care networks had the following representatives taking part in the project: œ Aad Bartelds (Continue Morbiditeits Registratie Peilstations, NIVEL, Utrecht, the Netherlands) œ Nathalie Bossuyt (Belgisch network van Huisartsenpeilpraktijken, Scientific Institute for Public Health, Brussels, Belgium) œ Jean-Marie Cohen (Open Rome, Paris, France) œ Isabel Falcao (Médicos-Sentinela, Instituto Nacional da Saude, Lisbon, Portugal) œ Antoine Flahault (Réseau Sentinelles, Inserm, Paris, France) œ Douglas Fleming (Weekly Returns Service, Birmingham Research Unit of Royal College of General Practitioners, Birmingham, United Kingdom) œ Anja Frenzen (Sächsischen epidemiologischen Studie in der Allgemeinmedizin (SESAM) III, Leipzig University, Leipzig, Germany) œ Jean-Luc Gallais (Observatoire de la Médecine Générale (OMG) de la Société Française de Médecine Générale (SFMG), Issy les Moulineaux, France) œ Hagen Sandholzer (SESAM III, Leipzig University, Leipzig, Germany) œ Viviane van Casteren (Belgisch network van Huisartsenpeilpraktijken, Scientific Institute for Public Health, Brussels, Belgium) œ Tomas Vega Alonso (Red de Médicos Centinelas de Castilla y León, Dirección General de Salud Pública y Consumo, Valladolid, Spain) on behalf of the regional Spanish primary care networks. A total of five meetings was organised in which the progress of the project was discussed. These meetings took place on February 2002 (Utrecht, NL), June !"$#%&('*) +,+-
 will be developed that help to clarify the appropriateness of primary care as source of epidemiological information.")
11 (Paris, FR), March 2003 (Utrecht, NL), 30 September-1 October 2003 (Valladolid, ES) and February 2003 (Brussels, BE). The meeting minutes can be found in appendix A. 2YHUYLHZRIWKHUHSRUW One of the aims of the European Public Health Programme is to collect information on health status in the individual Member States and to make this information on a European level available to the individual Member States. To achieve this, a set of European Community Health Indicators has been established. In general, an indicator needs to be valid (i.e. measure what one thinks it measures), be sensitive to changes over time and be comparable between countries and regions. Disease-specific morbidity at the population level is one of the areas of interest. This report studies the feasibility of routinely collected data from primary care as an information source for these health indicators. When using morbidity data as indicator for (differences in) health status between countries, it is important that the actual data are valid and comparable. Differences in operation and recording by the networks, and differences in health systems affect the validity and comparability of morbidity data from primary care. We therefore start with a description of the structure and operation of various primary care based registration networks in Europe (Chapter 2), to explore whether methodological issues can account for observed differences. We continue with a discussion of the primary care situation in the participating countries in chapter 3, to see to what extent variation in health systems may affect the results. We then present health indicator profiles, a tool for international comparison of health data (Chapter 4). The profiles represent a structured approach for international comparisons. These profiles are applied in chapter 5 in which primary care data for eight diseases from various networks are compared. Finally, we give recommendations and conclusions for the use of primary care data in European perspective in chapter 6.!"$#%&('*) +,+- 11

12 12!"$#%&('*) +,+-

13 'HVFULSWLRQRISULPDU\FDUHUHJLVWUDWLRQQHWZRUNV 6XPPDU\ In many European countries, primary care practice networks are in place and play a major role in public health surveillance. These networks are organised and function in varying ways. Information from them is one of the potential sources for a European health information and monitoring system which is envisaged in the European Public Health Programme. However, a detailed description of each data source is a prerequisite to ensure the validity and quality of the data and the validity of comparisons. In a previous project, an inventory was made of functioning primary care networks collecting morbidity data on a continuous basis, according to the definition: µ$qhwzrunrisudfwlfhvrufrppxqlw\edvhgsulpdu\fduh SK\VLFLDQVZKRPRQLWRURQHRUPRUHVSHFLILFLOOQHVVSUREOHPVRQDUHJXODUDQGFRQWLQXLQJEDVLV. Site visits were made to those networks cooperating in the current project which delivered epidemiological information. A standardised questionnaire was used to investigate aspects of function and recording quality. Eight primary care networks in Belgium, England & Wales, France (two networks), Germany, the Netherlands, Portugal and Spain delivered basic epidemiological information (case definition, numerator/denominator stratified for gender and age groups) on diseases mainly managed in primary care. Most of these networks are funded by their respective Ministries of Health, some others by governmental research funds. In general, the networks comprise a stable group of general practitioners (GPs) and monitor a representative sample of the general population (either at regional or national level). Some networks monitor all diagnoses presented and others a limited selection of diseases. Many of the networks use disease-specific questionnaires to provide enhanced data on selected diseases for specific purposes. The frequency of reporting by the central organisation of the networks varies from daily to annually. Primary care surveillance networks are an important tool for public health surveillance in Europe (particularly for, but not restricted to infectious diseases). Organisations running a primary care network can learn from networks in other countries and where necessary improve their own functioning. When all networks fulfil identical minimal criteria these networks can provide comparable estimates of morbidity attributed to certain diseases and this will ultimately lead to improved surveillance nationally and internationally. %DFNJURXQG The health of the population is a major concern for every national government. International comparisons help us to understand the reason for apparent national differences. Reliable and continuing information on health (and health related problems) and on the prevalence and incidence of disease are paramount. This information need is the basis for national surveillance-systems. Several sources of data are available: for example mortality statistics, hospital discharge registers, disease-specific registers, notification registers, prescription databases. However, no data source is totally comprehensive and all data sources provide information, limited to the purpose for which!"$#%&('*) +,+- 13

14 each was established. Many conditions do not lead to hospital admission or death but have a great impact on the health and wellbeing of the population and on national economies Data from primary care and health interview and health examination surveys (HIS/HES) are needed to inform on these. Primary care is often the entry-point into the health care system and the majority of health problems are managed exclusively in primary care. Therefore primary care based registration networks delivering reliable data in a consistent manner are potentially an important source of public health information. Moreover, primary care is the first and nearest source of medical information to the general population. In comparison to information obtained in HIS, data from primary care have the added advantage of professional assessment being described by the doctor rather than the patient. From an epidemiological point of view, although sometimes problematic, the epidemiological denominator can be defined more easily than in secondary health care facilities. In countries where universal patient registration with a primary care practice is usual, characteristics of the denominator population are readily available. Primary care networks are composed of a sample of general practitioners who report the occurrence of (a group of selected) diseases to a central office. These networks were often originally established to enable practitioners to engage in research and comprised willing and motivated volunteers. Nowadays the systems commonly provide data on infectious diseases, particularly vaccine preventable infections. Participating practices are called sentinel practices, with the implication of acting as a guardian or warning information system for the whole population in respect of the morbidity encountered. A distinction between surveillance and monitoring has to be made. Surveillance is actively observing incidence of diseases either in the short term (early warning) or long term (time trends). Monitoring is more passively surveying the health of a population. In general surveillance is focused on communicable diseases whereas monitoring is mainly concerned with chronic conditions. 3XUSRVH In the previous project an inventory of primary care registration networks was performed using the following definition: µ$qhwzrunrisudfwlfhvrufrppxqlw\edvhgsulpdu\fduh SK\VLFLDQVZKRPRQLWRURQHRUPRUHVSHFLILFLOOQHVVSUREOHPVRQDUHJXODUDQG FRQWLQXLQJEDVLV 2 In order to receive more background information on the networks and to facilitate international comparison of the information provided by the networks, site visits have been performed. These visits are also important for establishing the quality of these networks and hence the validity of the information provided. Site visits were conducted to provide a consistent description of each network and to clarify details of their functioning. A standardised questionnaire was used. We hoped to define minimal structural and recording conditions for a successful network. By providing feedback information to the participating networks we hoped to stimulate improvements in the networks; we can all learn from the experience of others. In 14!"$#%&('*) +,+-

15 particular procedures for quality control developed in one network can be applied elsewhere. The concept of a minimum standard could be seen as a pre-requisite for using the data to describe trends and to make national comparisons. 0HWKRGV Site visits were performed in eight primary care networks. The site visits consisted of a visit to one participating GP and to the central organisation. Both completed a standardised questionnaire before the visit and another standardised questionnaire was used at the actual visit (see Appendix B). The pre-visit questionnaire for the central organisation consisted of the following topics: 1 background information on network and its organisation, 2 operational organisation, 3 data collection, 4 use of data 5 a brief description of the health care system. The actual site visit included the following topics: 1 data transmission and data entry, 2 data storage, 3 data analysis, 4 questions based upon pre-visit questionnaire 5 additional comments. The pre-visit practice questionnaire concerned practice information on recording procedures, data summary/analysis, data transmission, support from network organisation and additional comments. During the site visit to the sentinel GP basic information on the practice, on the sentinel activities of the practice, operational information and personal comments were observed and collected. )LQGLQJV %DFNJURXQGLQIRUPDWLRQRQQHWZRUNDQGRUJDQLVDWLRQ A summarising overview of all findings can be found in appendix B (Table B1). The original site visit reports are also in Appendix B. All networks, except the German one in Saxony, have existed for more than ten years. The year of establishment varied from 1964 to Despite this variation, the aims of the networks were similar, all providing information on morbidity encountered in primary care. Funding generally came from government and university budgets, though the two French networks also received money from the private sector. Diseases were recorded in a continuous manner (this was a prerequisite to join the project). The number of diseases surveyed varied from a selection (usually between 5 and 10) to comprehensive recording of all GP contacts. All organisations had scientific and administrative personnel and most also technical. The number of personnel involved in managing the network varied from 0.9 in the Netherlands to 6.8!"$#%&('*) +,+- 15
.")
16 full-time equivalents (fte) in France (SFMG). In Belgium, the Netherlands and England & Wales participating GPs receive financial compensation, in the other countries there was no compensation except for the conduct of special studies (France Inserm) or when given as technical support (Castilla & Léon, Portugal). The population monitored varied from 0.5% to 5% of the national or regional population. Most networks were representative for age, gender and geographical distribution but in some, representativeness was assumed without supporting evidence. The representativeness of the population is a critical issue. Representativeness for age and sex can be assumed in most countries, however information on other health-determining factors like socio-economic status or ethnic origin are not readily available. Where networks report on GP-interventions there is also a need to consider the representativeness of the GPs. However studies of representativeness require resources and funding that are not routinely available in sentinel networks. 2SHUDWLRQDOLQIRUPDWLRQ The median number of participating GPs in the national networks was 170 (range ). In France Inserm there were 1300 registered participants of which on average 150 participate in weekly surveillance. In most cases the minimum number of participants was determined by the number needed to guarantee national coverage. In the Spanish region of Castilla & Léon a maximum number of participants was defined based upon adequate operational control and cost-effectiveness. Some networks organise training courses on recording, use of software or research methodology. In others this is limited to an annual (written) instruction for recording. Where relevant comparisons could be made, (for example by age, gender, size of practice) participating GPs were often not representative of the national GP population. Participating GPs are willing to spend extra time for public health surveillance which is not always financially compensated, which inevitably leads to selective bias in the recruitment of well motivated practices. Though motivation may bias attitudes, it is unlikely to influence recording behaviour. The requirements for GPs to join networks were mostly based upon the maintenance of representative coverage. In France (Open Rome/SFMG) and England & Wales another requirement was compatibility of software packages with the central system. The turnover of the networks was limited to 5%. Compliance of GPs was defined differently in each network. In most networks a minimum participation rate exists, if participants report less than this defined number of days or weeks, their data were not included in the analysis. Overall the majority of the GPs reported on a regular basis. Feedback to participants consisted of newsletters, annual reports and meetings. In some countries GPs received each year an overview consisting of their individual results in relation to the results from the whole network. In Spain and France internet was also used as a means of discussion and information. Communication between participants within the networks was unusual. 'DWDFROOHFWLRQDQGDQDO\VLV Data collection was performed either by standardised paper forms (Belgium, Germany, Spain, the Netherlands and Portugal) or electronically. For electronic data collection 16!"$#%&('*) +,+-

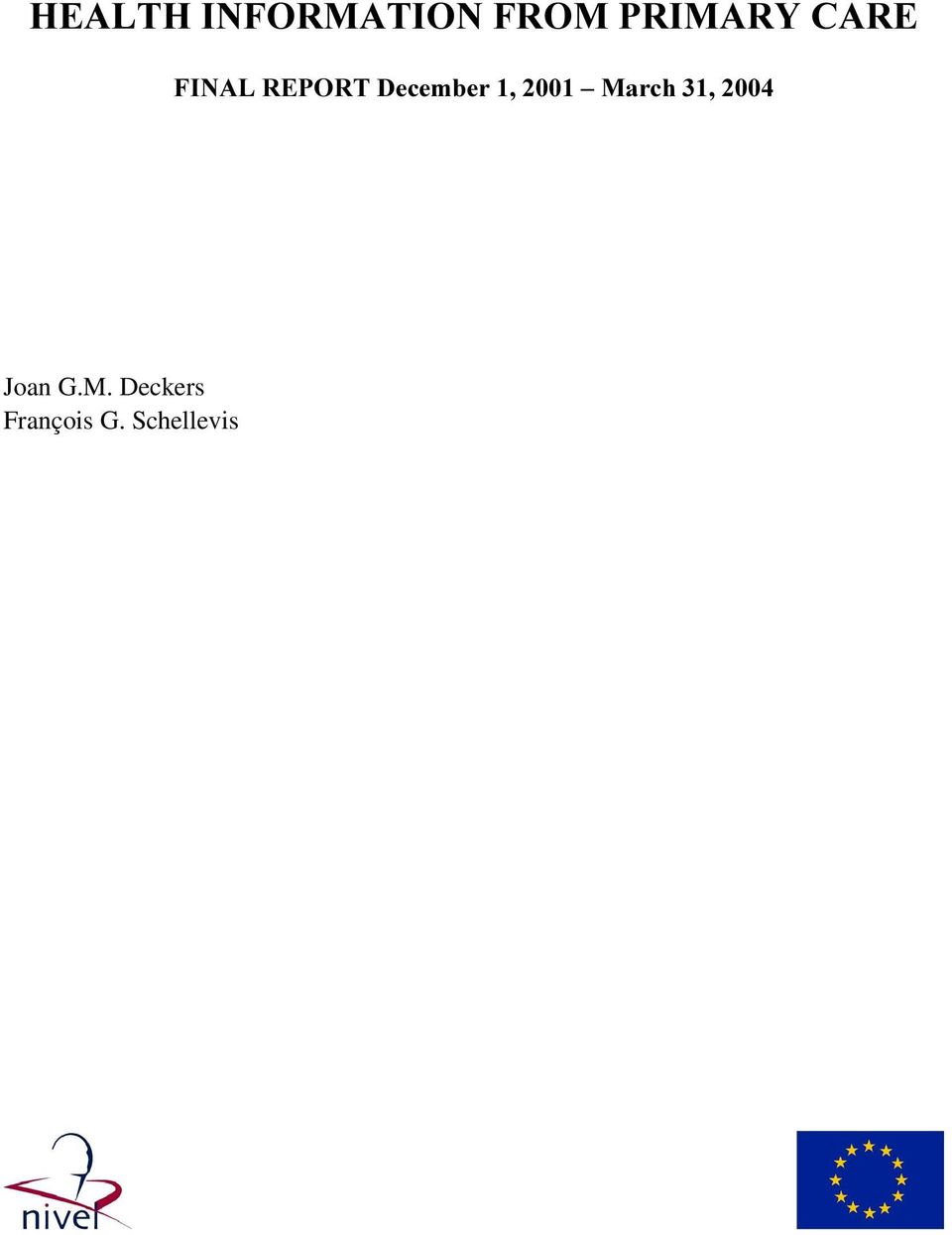
17 standardised extractions from electronic medical records (France Open Rome/SFMG, England & Wales) or standardised forms on internet (France Inserm) were used. In most countries there were several software packages for electronic medical records, presenting organisational problems for automated recording. Networks need specific extraction software for each of the existing electronic medical record packages. Updating the extraction programmes requires staff and financial resources. This is an important issue for countries considering the transition from a paper system to a electronic system. The minimum data set in all countries consisted of GP and/or patient ID, diagnosis, age and gender of patient. In some countries the number of patient contacts, number of days recorded, week number or date were also collected to calculate or estimate the denominator. A case definition to classify the diagnosis was used when possible, but this varied with the topic. Data from paper forms were entered by administrative staff at the respective institutes. In Germany the textual information on the diagnosis or reason for encounter was recoded in international classification of disease (ICD)-10 resp. international classification of primary care (ICPC) by three independent GPs. For electronic data collection transfer occurred automatically on a daily to monthly basis. Information was stored in various types of databases which either contained all information in one file or in separate files per disease and/or year. Where possible, missing data were followed up and when not corrected excluded from the analysis. The frequency of reporting by the GPs to the central database is generally weekly, except for France (Open Rome/SFMG) and Germany where it was monthly or quarterly and England & Wales where it was twice weekly. There were a number of quality control measures in place in the various networks, an overview of possible measures is shown in Figure 2.1. Paper forms were visually inspected, consistency checks were incorporated in the data-entry programmes and double data entry was applied. Preliminary analyses were performed to compare data to expected figures or national averages. Furthermore data samples were used for interobserver reliability testing. Potential external validation sources are for instance mortality statistics, disease registers or prescription data.!"$#%&('*) +,+- 17

18 Figure 2.1 Possible quality measures in primary care registration networks *3 75$16)(5 &225',1$7,21&(175( - Coding: - Security: - Inconsistencies: - Reliability - Passwords - Age - Inter-observer testing - Double entries - Sex - Case definition - Privacy (patients) - Total number (tolerance matrix) - Pilot study (for recording) - Confirmation of receipt - Data entry (limited codes) - Practice visits - Double data entry - Training - Corrections - Feedback: - Publications - Results - External validation - Bulletin - Meeting questionnaire - Diagnosis verification (by lab) - Completeness of diagnosis - Privacy aspects (patients) - Representativeness However, the basic and determining quality of primary care networks is the quality of the diagnosis made by the GPs. If influencing the diagnosis is at all possible it is certainly very expensive. The costs of investigating the diagnostic validity of common self-limiting illnesses are often not justifiable. Therefore, control measures to check for correct use of diagnoses are not applied. In contrast, many efforts are made to validate the information on the level of the entire network, e.g. by comparing this with other information sources. In general, the absolute number of patients is expressed as relative frequency of disease per 10,000 or 100,000 persons. In some cases standardisation for age and sex to the national population is also performed. As explained before, GPs who do not record on a regular basis (defined as < 50% in most cases) are excluded from the analyses. As a routine, the incidence or prevalence per 10,000 or 100,000 persons by age and gender is determined by scientific and technical staff. Those networks that record a selection of diseases often collect additional information about specific diseases on an ad hoc basis; for example description of symptoms, follow-up, referral to other health care professionals and prescribing information. This information was analysed on a case by case basis. Annual analyses are performed routinely in all networks. Some analyse more regularly, in England & Wales twice weekly, in France (Inserm) weekly, and in the Spanish region of Castilla & Léon quarterly. The only exception concerns the surveillance of influenza-like-illness which during winter is analysed on a weekly basis everywhere. Problems encountered in the process of data collection, transfer and analysis included incompleteness of data, technical problems with software packages and dataretrieval, discontinuation of recording by GPs because of a high workload, limited staff resources leading to delays in analysis and publications. 18!"$#%&('*) +,+-
 - Completeness of diagnosis")
19 )XWXUHRISULPDU\FDUHQHWZRUNV An important issue to consider is the future of primary care networks in general and in the context of the future European Health Information System. How will the current networks be functioning in 5 to 10 years time? The views of the individual networks can be found in Appendix A (meeting minutes for the 3rd meeting, March 2003). Currently all networks monitor and report on morbidity in the general practice population. It is thought that in the future paper forms will no longer be used. Most networks will switch to automated recording and are likely to expand to comprehensive recording of all morbidity, although some networks expressed a preference only to analyse selected diseases. Monitoring selected diseases has the advantage of the possibility of collecting additional information on diagnosis and management. On the other hand, comprehensive recording allows an overview of all GP contacts and provides added context especially with regard to prescribing information and referral behaviour. However specific details about individual problems are less readily available. A clear-cut answer to the question which is the best system cannot be given, though the precise purpose of the network will often determine the answer. Switching to automated data collection also means that the frequency of reporting can be increased to weekly or even daily. Cooperation with laboratories and other health care professionals and research institutes, is an issue foreseen by most participants. All these changes are largely determined by funding arrangements. For most networks funding is secure for 2-3 years, even though most of the networks have existed for more than ten years. However it is necessary to implement changes (comprehensive recording and automated data collection) to maintain primary care networks as an important source of health information to support health policy and public health surveillance. To guarantee adequate monitoring and development of the systems continuous financial support is required. Excessive funding however might exert an influence on the recording of diagnoses. It would seem undesirable for funding to come from a source with a vested interest in specific aspects of the data, e.g. prescribing. The participants in Belgium, the Netherlands and England & Wales are currently financially compensated at a low level which does not cover the recording costs. In the Spanish region of Castilla & Léon and in Portugal compensation is given in the form of technical support. Financial compensation for the GPs gives the network organisers greater scope to dismiss poor recorders and generally to control the quality of recording. &RQFOXVLRQ Primary care surveillance networks are an important tool for public health surveillance in Europe. Although some networks are limited to the surveillance of infectious diseases, primary care networks are a useful source of information on health-related problems in general and not only morbidity. At first sight there seems to be wide variation in the operation of these networks. From the programme of site visits we consider the differences limited. The networks are either part of the respective national health service authorities or funded by them. Although they differ in size, most networks cover a!"$#%&('*) +,+- 19

20 representative sample of the population. Participating GPs are interested in public health and very few discontinue recording. All networks produce an annual report containing their findings and report more frequently as appropriate to the public health issue concerned. In our opinion, organisations running a primary care network can learn from networks in other countries and where necessary improve their own. Minimal criteria and operational standards need to be defined for inclusion of data from networks in a national and European information system. These include: œ FRQWLQXRXVVXUYHLOODQFH of a representative sample (around 1%) of the population œ representativeness of the SRSXODWLRQE\DJHDQGVH[ œ the use of VWDQGDUGDJHJURXSV with break points at years. Additional breakpoints at 25 and 75 years are highly recommended. œ a registered patient list is preferred for determination of the GHQRPLQDWRU, although methods can be developed to make good estimates. œ ability to GHOLYHULQIRUPDWLRQ on a WLPHO\ basis. For surveillance of infectious diseases and diseases with a high seasonal influence reporting by the network is preferred to be on a weekly basis. For other conditions annual feedback suffices. œ TXDOLW\FRQWURO measures, although time-consuming and therefore costly, must be in place to ensure reliable and valid data. One option that needs further study is the development of methods to verify the completeness and representativeness of the data exploiting inconsistencies within the data. For the future the move towards comprehensive recording and automated data collection is desirable. However to implement these changes and to guarantee adequate monitoring continuous financial support is essential. 20!"$#%&('*) +,+-

MEASURING INEQUALITY BY HEALTH AND DISEASE CATEGORIES (USING DATA FROM ADMINISTRATIVE SOURCES)
") SECTION 3 MEASURING INEQUALITY BY HEALTH AND DISEASE CATEGORIES (USING DATA FROM ADMINISTRATIVE SOURCES) This section looks at how death and illness are recorded and measured by administrative data sources.
SECTION 3 MEASURING INEQUALITY BY HEALTH AND DISEASE CATEGORIES (USING DATA FROM ADMINISTRATIVE SOURCES) This section looks at how death and illness are recorded and measured by administrative data sources.
Ministry of Social Development: Changes to the case management of sickness and invalids beneficiaries
 Ministry of Social Development: Changes to the case management of sickness and invalids beneficiaries This is the report of a performance audit we carried out under section 16 of the Public Audit Act 2001
Ministry of Social Development: Changes to the case management of sickness and invalids beneficiaries This is the report of a performance audit we carried out under section 16 of the Public Audit Act 2001
Measuring quality along care pathways
 Measuring quality along care pathways Sarah Jonas, Clinical Fellow, The King s Fund Veena Raleigh, Senior Fellow, The King s Fund Catherine Foot, Senior Fellow, The King s Fund James Mountford, Director
Measuring quality along care pathways Sarah Jonas, Clinical Fellow, The King s Fund Veena Raleigh, Senior Fellow, The King s Fund Catherine Foot, Senior Fellow, The King s Fund James Mountford, Director
Electronic Health Records Research in a Health Sector with Multiple Provider Types
 Electronic Health Records Research in a Health Sector with Multiple Provider Types Samantha Crossfield Susan Clamp Presented by Samantha Crossfield AMBCS, MSc info@researchone.org Outline Section Setting
Electronic Health Records Research in a Health Sector with Multiple Provider Types Samantha Crossfield Susan Clamp Presented by Samantha Crossfield AMBCS, MSc info@researchone.org Outline Section Setting
Chapter 4. Planning a cancer registry
 Chapter 4. Planning a cancer registry 0. M. Jensenl and S. Whelan2 Danish Cancer Registry, Danish Cancer Society, Rosenvaengets Hoveduej 35, PO Box 839, Copenhagen 21nternational Agency for Research on
Chapter 4. Planning a cancer registry 0. M. Jensenl and S. Whelan2 Danish Cancer Registry, Danish Cancer Society, Rosenvaengets Hoveduej 35, PO Box 839, Copenhagen 21nternational Agency for Research on
Seasonal influenza vaccination in Europe: vaccination policy and vaccination coverage. Summary of VENICE surveys
 Seasonal influenza vaccination in Europe: vaccination policy and vaccination coverage. Summary of VENICE surveys D.O Flanagan S.Cotter, J.Mereckiene On behalf of VENICE Project ECDC and WHO EURO Annual
Seasonal influenza vaccination in Europe: vaccination policy and vaccination coverage. Summary of VENICE surveys D.O Flanagan S.Cotter, J.Mereckiene On behalf of VENICE Project ECDC and WHO EURO Annual
Health Information: Priorities in the Work Plan 2006. DG SANCO Unit C-2 Health Information Luxembourg
 Health Information: Priorities in the Work Plan 2006 DG SANCO Unit C-2 Health Information Luxembourg Our objectives (I) The purpose of the European Union Health Information System is to provide quality,
Health Information: Priorities in the Work Plan 2006 DG SANCO Unit C-2 Health Information Luxembourg Our objectives (I) The purpose of the European Union Health Information System is to provide quality,
Can a tulip become a rose?
 Can a tulip become a rose? The Dutch route of guided self-regulation towards a community based integrated health care system. Niek Klazinga, Diana Delnoij, Isik Kulu-Glasgow Department of Social Medicine
Can a tulip become a rose? The Dutch route of guided self-regulation towards a community based integrated health care system. Niek Klazinga, Diana Delnoij, Isik Kulu-Glasgow Department of Social Medicine
THE EUROPEAN DEFINITION OF GENERAL PRACTICE / FAMILY MEDICINE
 Network organisation within WONCA Region Europe - ESGP/FM European Academy of Teachers in General Practice (Network within WONCA Europe) THE EUROPEAN DEFINITION OF GENERAL PRACTICE / FAMILY MEDICINE SHORT
Network organisation within WONCA Region Europe - ESGP/FM European Academy of Teachers in General Practice (Network within WONCA Europe) THE EUROPEAN DEFINITION OF GENERAL PRACTICE / FAMILY MEDICINE SHORT
How To Manage A Hospital Emergency
 ENHANCED SERVICE SPECIFICATION RISK PROFILING AND CARE MANAGEMENT SCHEME Introduction 1. This enhanced service has been designed by the NHS Commissioning Board (NHS CB) to reward GP practices 1 for the
ENHANCED SERVICE SPECIFICATION RISK PROFILING AND CARE MANAGEMENT SCHEME Introduction 1. This enhanced service has been designed by the NHS Commissioning Board (NHS CB) to reward GP practices 1 for the
Information Governance. A Clinician s Guide to Record Standards Part 1: Why standardise the structure and content of medical records?
 Information Governance A Clinician s Guide to Record Standards Part 1: Why standardise the structure and content of medical records? Contents Page 3 A guide for clinicians Pages 4 and 5 Why have standards
Information Governance A Clinician s Guide to Record Standards Part 1: Why standardise the structure and content of medical records? Contents Page 3 A guide for clinicians Pages 4 and 5 Why have standards
EUROPEAN CITIZENS DIGITAL HEALTH LITERACY
 Flash Eurobarometer EUROPEAN CITIZENS DIGITAL HEALTH LITERACY REPORT Fieldwork: September 2014 Publication: November 2014 This survey has been requested by the European Commission, Directorate-General
Flash Eurobarometer EUROPEAN CITIZENS DIGITAL HEALTH LITERACY REPORT Fieldwork: September 2014 Publication: November 2014 This survey has been requested by the European Commission, Directorate-General
Submission by the Irish Pharmacy Union to the Department of Health on the Scope for Private Health Insurance to incorporate Additional Primary Care
 Submission by the Irish Pharmacy Union to the Department of Health on the Scope for Private Health Insurance to incorporate Additional Primary Care Services January 2015 1 IPU Submission to the Department
Submission by the Irish Pharmacy Union to the Department of Health on the Scope for Private Health Insurance to incorporate Additional Primary Care Services January 2015 1 IPU Submission to the Department
Intermediate care and reablement
 Factsheet 76 May 2015 About this factsheet This factsheet explains intermediate care, a term that includes reablement. It consists of a range of integrated services that can be offered on a short term
Factsheet 76 May 2015 About this factsheet This factsheet explains intermediate care, a term that includes reablement. It consists of a range of integrated services that can be offered on a short term
Overview of the national laws on electronic health records in the EU Member States National Report for Lithuania
 Overview of the national laws on electronic health records in the EU Member States and their interaction with the provision of cross-border ehealth services Contract 2013 63 02 Overview of the national
Overview of the national laws on electronic health records in the EU Member States and their interaction with the provision of cross-border ehealth services Contract 2013 63 02 Overview of the national
ADULT HEALTH AND WELLBEING LONG-TERM NEUROLOGICAL CONDITIONS
 ADULT HEALTH AND WELLBEING LONG-TERM NEUROLOGICAL CONDITIONS i. Summary The National Service Framework for long-term neurological conditions categorises neurological conditions as: Sudden-onset conditions
ADULT HEALTH AND WELLBEING LONG-TERM NEUROLOGICAL CONDITIONS i. Summary The National Service Framework for long-term neurological conditions categorises neurological conditions as: Sudden-onset conditions
Description of the OECD Health Care Quality Indicators as well as indicator-specific information
 Appendix 1. Description of the OECD Health Care Quality Indicators as well as indicator-specific information The numbers after the indicator name refer to the report(s) by OECD and/or THL where the data
Appendix 1. Description of the OECD Health Care Quality Indicators as well as indicator-specific information The numbers after the indicator name refer to the report(s) by OECD and/or THL where the data
Electronic Health Record Systems and Secondary Data Use
 Electronic Health Record Systems and Secondary Data Use HCQI Expert Group Meeting 10 May 2012 Jillian Oderkirk OECD/HD Background and Needs The 2010 Health Ministerial Communiqué noted that health care
Electronic Health Record Systems and Secondary Data Use HCQI Expert Group Meeting 10 May 2012 Jillian Oderkirk OECD/HD Background and Needs The 2010 Health Ministerial Communiqué noted that health care
ECDC SURVEILLANCE REPORT
 ECDC SURVEILLANCE REPORT Pandemic (H1N1) 2009 Weekly report: Individual case reports EU/EEA countries 31 July 2009 Summary The pandemic A(H1N1) 2009 is still spreading despite the fact that the regular
ECDC SURVEILLANCE REPORT Pandemic (H1N1) 2009 Weekly report: Individual case reports EU/EEA countries 31 July 2009 Summary The pandemic A(H1N1) 2009 is still spreading despite the fact that the regular
Harness Care Cooperative Ltd Quality primary care services provided through local cooperation Company registration: 06584450
 Harness Care Cooperative Ltd Quality primary care services provided through local cooperation Company registration: 06584450 Job Description Job title: Nurse Practitioner /Lead Nurse ACCOUNTIBILITY The
Harness Care Cooperative Ltd Quality primary care services provided through local cooperation Company registration: 06584450 Job Description Job title: Nurse Practitioner /Lead Nurse ACCOUNTIBILITY The
Age differences in graduate employment across Europe
 November 2008 The Flexible Professional in the Knowledge Society new demands on higher education in Europe (Report 5) Age differences in graduate employment across Europe Report to HEFCE by Centre for
November 2008 The Flexible Professional in the Knowledge Society new demands on higher education in Europe (Report 5) Age differences in graduate employment across Europe Report to HEFCE by Centre for
THE ORGANISATION AND FINANCING OF HEALTH CARE SYSTEM IN LATVIA
 THE ORGANISATION AND FINANCING OF HEALTH CARE SYSTEM IN LATVIA Eriks Mikitis Ministry of Health of the Republic of Latvia Department of Health Care Director General facts, financial resources Ministry
THE ORGANISATION AND FINANCING OF HEALTH CARE SYSTEM IN LATVIA Eriks Mikitis Ministry of Health of the Republic of Latvia Department of Health Care Director General facts, financial resources Ministry
Draft guidelines and measures to improve ICT procurement. Survey results
 Draft guidelines and measures to improve ICT procurement Survey results Europe Economics Chancery House 53-64 Chancery Lane London WC2A 1QU Tel: (+44) (0) 20 7831 4717 Fax: (+44) (0) 20 7831 4515 www.europe-economics.com
Draft guidelines and measures to improve ICT procurement Survey results Europe Economics Chancery House 53-64 Chancery Lane London WC2A 1QU Tel: (+44) (0) 20 7831 4717 Fax: (+44) (0) 20 7831 4515 www.europe-economics.com
User language preferences online. Analytical report
 Flash Eurobarometer 313 The Gallup Organization Flash Eurobarometer European Commission User language preferences online Analytical report Fieldwork: January 2011 Publication: May 2011 This survey was
Flash Eurobarometer 313 The Gallup Organization Flash Eurobarometer European Commission User language preferences online Analytical report Fieldwork: January 2011 Publication: May 2011 This survey was
EU DIRECTIVE ON GOOD CLINICAL PRACTICE IN CLINICAL TRIALS DH & MHRA BRIEFING NOTE
 EU DIRECTIVE ON GOOD CLINICAL PRACTICE IN CLINICAL TRIALS DH & MHRA BRIEFING NOTE Purpose 1. The Clinical Trials Directive 2001/20/EC heralds certain additional responsibilities for the Medicines and Healthcare
EU DIRECTIVE ON GOOD CLINICAL PRACTICE IN CLINICAL TRIALS DH & MHRA BRIEFING NOTE Purpose 1. The Clinical Trials Directive 2001/20/EC heralds certain additional responsibilities for the Medicines and Healthcare
To provide standardized Supervised Exercise Programs across the province.
 TITLE ALBERTA HEALTHY LIVING PROGRAM SUPERVISED EXERCISE PROGRAM DOCUMENT # HCS-67-01 APPROVAL LEVEL Executive Director Primary Health Care SPONSOR Senior Consultant Central Zone, Primary Health Care CATEGORY
TITLE ALBERTA HEALTHY LIVING PROGRAM SUPERVISED EXERCISE PROGRAM DOCUMENT # HCS-67-01 APPROVAL LEVEL Executive Director Primary Health Care SPONSOR Senior Consultant Central Zone, Primary Health Care CATEGORY
National Clinical Programmes
 National Clinical Programmes Section 3 Background information on the National Clinical Programmes Mission, Vision and Objectives July 2011 V0. 6_ 4 th July, 2011 1 National Clinical Programmes: Mission
National Clinical Programmes Section 3 Background information on the National Clinical Programmes Mission, Vision and Objectives July 2011 V0. 6_ 4 th July, 2011 1 National Clinical Programmes: Mission
National Minimum Standards for Immunisation Training
 National Minimum Standards for Immunisation Training Contributors The following formed the advisory group which, hosted by the Health Protection Agency, produced these Minimum Standards for Immunisation
National Minimum Standards for Immunisation Training Contributors The following formed the advisory group which, hosted by the Health Protection Agency, produced these Minimum Standards for Immunisation
(Resolutions, recommendations and opinions) RECOMMENDATIONS COUNCIL
 RECOMMENDATIONS COUNCIL") 3.7.2009 Official Journal of the European Union C 151/1 I (Resolutions, recommendations and opinions) RECOMMENDATIONS COUNCIL COUNCIL RECOMMENDATION of 9 June 2009 on patient safety, including the prevention
3.7.2009 Official Journal of the European Union C 151/1 I (Resolutions, recommendations and opinions) RECOMMENDATIONS COUNCIL COUNCIL RECOMMENDATION of 9 June 2009 on patient safety, including the prevention
OECD Study of Electronic Health Record Systems
 OECD Study of Electronic Health Record Systems Ministry of Health of the Czech Republic E health Expert Group Meeting 19 June 2012 Jillian Oderkirk OECD/HD Background and Needs The 2010 Health Ministerial
OECD Study of Electronic Health Record Systems Ministry of Health of the Czech Republic E health Expert Group Meeting 19 June 2012 Jillian Oderkirk OECD/HD Background and Needs The 2010 Health Ministerial
An international approach to the implementation of SNOMED CT and ICPC-2 in Family/General Practice
 An international approach to the implementation of SNOMED CT and ICPC-2 in Family/General Practice Nick Booth 1,2, Graeme Miller 1,2,3, Julie O Halloran 1,2,3, John Bennett 4 1 IHTSDO IFP/GP RefSet and
An international approach to the implementation of SNOMED CT and ICPC-2 in Family/General Practice Nick Booth 1,2, Graeme Miller 1,2,3, Julie O Halloran 1,2,3, John Bennett 4 1 IHTSDO IFP/GP RefSet and
Original Research Paper
 Original Research Paper Sore throat diagnosis and management in a general practice after-hours service Marjan Kljakovic is a senior lecturer, department of general practice, Wellington School of Medicine
Original Research Paper Sore throat diagnosis and management in a general practice after-hours service Marjan Kljakovic is a senior lecturer, department of general practice, Wellington School of Medicine
Guideline: Medical supervision of Diabetes Registered Nurse Prescribing 2014
 Guideline: Medical supervision of Diabetes Registered Nurse Prescribing 2014 The Nursing Council of New Zealand has adapted this Guideline which was developed by the New Zealand Society for the Study of
Guideline: Medical supervision of Diabetes Registered Nurse Prescribing 2014 The Nursing Council of New Zealand has adapted this Guideline which was developed by the New Zealand Society for the Study of
Wandsworth Respiratory Clinical Reference Group Annual Progress Report 2014/15
 Wandsworth Respiratory Clinical Reference Group Annual Progress Report 2014/15 April 2015 Dr Kieron Earney & Kate Symons Acknowledgements Dr Sarah Deedat Public Health Lead for Long Term Conditions 1 1.
Wandsworth Respiratory Clinical Reference Group Annual Progress Report 2014/15 April 2015 Dr Kieron Earney & Kate Symons Acknowledgements Dr Sarah Deedat Public Health Lead for Long Term Conditions 1 1.
Commissioning fact sheet for clinical commissioning groups
 Commissioning fact sheet for clinical groups July 2012 This fact sheet sets out the services to be commissioned by clinical groups (CCGs) from April 2013. It also sets out the complementary services to
Commissioning fact sheet for clinical groups July 2012 This fact sheet sets out the services to be commissioned by clinical groups (CCGs) from April 2013. It also sets out the complementary services to
To precertify inpatient admissions or transitional care services, call 1-866-688-3400 and select option #1.
 Security Health Plan provides coverage of various mental health/aoda (alcohol and other drug abuse) benefits to individual and employer group members. These benefits are managed by Security Health Plan.
Security Health Plan provides coverage of various mental health/aoda (alcohol and other drug abuse) benefits to individual and employer group members. These benefits are managed by Security Health Plan.
The Open University s repository of research publications and other research outputs. Age differences in graduate employment across Europe
 Open Research Online The Open University s repository of research publications and other research outputs Age differences in graduate employment across Europe Other How to cite: Little, Brenda and Tang,
Open Research Online The Open University s repository of research publications and other research outputs Age differences in graduate employment across Europe Other How to cite: Little, Brenda and Tang,
Policy and Procedure Manual
 Policy and Procedure Manual Resident Assessment (RA) Table of Contents RA-01 RA-02 RA-03 RA-04 RA-05 RA-06 RA-07 RA-08 RA-09 RA-10 RA-11 RA-12 RA-13 Admission. History, Physicals and Routine Health Care
Policy and Procedure Manual Resident Assessment (RA) Table of Contents RA-01 RA-02 RA-03 RA-04 RA-05 RA-06 RA-07 RA-08 RA-09 RA-10 RA-11 RA-12 RA-13 Admission. History, Physicals and Routine Health Care
Executive Summary and Recommendations: National Audit of Learning Disabilities Feasibility Study
 Executive Summary and Recommendations: National Audit of Learning Disabilities Feasibility Study Contents page Executive Summary 1 Rationale and potential impact of a future audit 2 Recommendations Standards
Executive Summary and Recommendations: National Audit of Learning Disabilities Feasibility Study Contents page Executive Summary 1 Rationale and potential impact of a future audit 2 Recommendations Standards
The practice of medicine comprises prevention, diagnosis and treatment of disease.
 English for Medical Students aktualizované texty o systému zdravotnictví ve Velké Británii MUDr Sylva Dolenská Lesson 16 Hospital Care The practice of medicine comprises prevention, diagnosis and treatment
English for Medical Students aktualizované texty o systému zdravotnictví ve Velké Británii MUDr Sylva Dolenská Lesson 16 Hospital Care The practice of medicine comprises prevention, diagnosis and treatment
GP SERVICES COMMITTEE Conferencing and Telephone Management INCENTIVES. Revised 2015. Society of General Practitioners
 GP SERVICES COMMITTEE Conferencing and Telephone Management INCENTIVES Revised 2015 Society of General Practitioners Conference & Telephone Fees (G14077, G14015, G14016, G14017, G14018, G14019, G14021,
GP SERVICES COMMITTEE Conferencing and Telephone Management INCENTIVES Revised 2015 Society of General Practitioners Conference & Telephone Fees (G14077, G14015, G14016, G14017, G14018, G14019, G14021,
Improving Emergency Care in England
 Improving Emergency Care in England REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1075 Session 2003-2004: 13 October 2004 LONDON: The Stationery Office 11.25 Ordered by the House of Commons to be printed
Improving Emergency Care in England REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1075 Session 2003-2004: 13 October 2004 LONDON: The Stationery Office 11.25 Ordered by the House of Commons to be printed
SURVEY ON THE TRAINING OF GENERAL CARE NURSES IN THE EUROPEAN UNION. The current minimum training requirements for general care nurses
 SURVEY ON THE TRAINING OF GENERAL CARE NURSES IN THE EUROPEAN UNION This survey serves as a background document for the discussion of the Commission's legislative proposal to modernize the minimum requirements
SURVEY ON THE TRAINING OF GENERAL CARE NURSES IN THE EUROPEAN UNION This survey serves as a background document for the discussion of the Commission's legislative proposal to modernize the minimum requirements
Nurse Practitioner Frequently Asked Questions
 HEALTH SERVICES Nurse Practitioner Frequently Asked Questions The Frequently Asked Questions (FAQs) have been designed to increase awareness and understanding of the Nurse Practitioner role within the
HEALTH SERVICES Nurse Practitioner Frequently Asked Questions The Frequently Asked Questions (FAQs) have been designed to increase awareness and understanding of the Nurse Practitioner role within the
ANALYSIS OF THE STAKEHOLDER CONSULTATION ON
 ANALYSIS OF THE STAKEHOLDER CONSULTATION ON Science and Technology, the key to Europe s future: guidelines for future European policy to support research COM(353)2004 DG Research, European Commission,
ANALYSIS OF THE STAKEHOLDER CONSULTATION ON Science and Technology, the key to Europe s future: guidelines for future European policy to support research COM(353)2004 DG Research, European Commission,
Diabetes mellitus care in Malta
 Diabetes mellitus care in Malta The role of the family doctor Jean K Soler Diabetes mellitus care in Malta The role of the family doctor Aims and objectives of care Aims of diabetes care Avoiding complications
Diabetes mellitus care in Malta The role of the family doctor Jean K Soler Diabetes mellitus care in Malta The role of the family doctor Aims and objectives of care Aims of diabetes care Avoiding complications
Family Law. Analytical Report
 Flash Eurobarometer European Commission Family Law Analytical Report Fieldwork: June 2006 Report: October 2006 Flash Eurobarometer 188 The Gallup Organization This survey was requested by Directorate-General
Flash Eurobarometer European Commission Family Law Analytical Report Fieldwork: June 2006 Report: October 2006 Flash Eurobarometer 188 The Gallup Organization This survey was requested by Directorate-General
Structures and organization of services for medical rehabilitation in Germany* Wilfried Mau. Halle (Saale), Germany
, Germany") Structures and organization of services for medical rehabilitation in Germany* Wilfried Mau Halle (Saale), Germany Address for Correspondence: Professor Wilfried Mau, MD Director of the Institute for Rehabilitation
Structures and organization of services for medical rehabilitation in Germany* Wilfried Mau Halle (Saale), Germany Address for Correspondence: Professor Wilfried Mau, MD Director of the Institute for Rehabilitation
Case-management by the GP of domestic violence
 Case-management by the GP of domestic violence an example of results from a sentinel network of general practitioners Nathalie Bossuyt Sentinel network of general practitioners Outline Introduction Research
Case-management by the GP of domestic violence an example of results from a sentinel network of general practitioners Nathalie Bossuyt Sentinel network of general practitioners Outline Introduction Research
CIRCULAR 13 OF 2014: MANAGED CARE ACCREDITATION - FINAL MANAGED HEALTH CARE SERVICES DOCUMENT
 CIRCULAR Reference: Classification and naming conventions of Managed Health Care Services Contact person: Hannelie Cornelius Accreditation Manager: Administrators & MCOs Tel: (012) 431 0406 Fax: (012)
CIRCULAR Reference: Classification and naming conventions of Managed Health Care Services Contact person: Hannelie Cornelius Accreditation Manager: Administrators & MCOs Tel: (012) 431 0406 Fax: (012)
» Edito. Challenges of Tele-underwriting. June 2009 Newsletter. Definition. www.scor.com
 June 2009 Newsletter Challenges of Tele-underwriting» Edito Tele-underwriting, a concept launched initially in the United States, is now getting momentum in various markets in Europe and in the rest of
June 2009 Newsletter Challenges of Tele-underwriting» Edito Tele-underwriting, a concept launched initially in the United States, is now getting momentum in various markets in Europe and in the rest of
Australian Federation of AIDS Organisations (AFAO) Primary Health Care Reform
 Primary Health Care Reform") Australian Federation of AIDS Organisations (AFAO) Primary Health Care Reform 27 February 2009 1 Introduction The Australian Federation of AIDS Organisations (AFAO) is the peak body for Australia s community
Australian Federation of AIDS Organisations (AFAO) Primary Health Care Reform 27 February 2009 1 Introduction The Australian Federation of AIDS Organisations (AFAO) is the peak body for Australia s community
THE CHALLENGES OF FUNDING HEALTHCARE FOR AN AGEING POPULATION A COMPARISON OF ACTUARIAL METHODS AND BENEFIT DESIGNS
 THE CHALLENGES OF FUNDING HEALTHCARE FOR AN AGEING POPULATION A COMPARISON OF ACTUARIAL METHODS AND BENEFIT DESIGNS 19 th November 2013 Stephen Bishop Challenges of Old Age Healthcare Provisions 1. Clinical
THE CHALLENGES OF FUNDING HEALTHCARE FOR AN AGEING POPULATION A COMPARISON OF ACTUARIAL METHODS AND BENEFIT DESIGNS 19 th November 2013 Stephen Bishop Challenges of Old Age Healthcare Provisions 1. Clinical
Towards this end, a number of steps will be taken over the upcoming years. This results in the following multi-annual planning.
 Multi-annual agenda on antibiotic resistance in healthcare Parties have agreed on a 'Multi-annual agenda on antibiotic resistance in healthcare ' containing transparent agreements to prevent the effects
Multi-annual agenda on antibiotic resistance in healthcare Parties have agreed on a 'Multi-annual agenda on antibiotic resistance in healthcare ' containing transparent agreements to prevent the effects
Physician and other health professional services
 O n l i n e A p p e n d i x e s 4 Physician and other health professional services 4-A O n l i n e A p p e n d i x Access to physician and other health professional services 4 a1 Access to physician care
O n l i n e A p p e n d i x e s 4 Physician and other health professional services 4-A O n l i n e A p p e n d i x Access to physician and other health professional services 4 a1 Access to physician care
Diabetes care in the Netherlands Providers perspective
 in the Netherlands Providers perspective Care-standards Euro Consumer Diabetes Index 2008 1. Denmark (837 points out of 1000) 2. UK (836 points). 3. France (814) 4. The Netherlands (813) 5. Belgium (803)
in the Netherlands Providers perspective Care-standards Euro Consumer Diabetes Index 2008 1. Denmark (837 points out of 1000) 2. UK (836 points). 3. France (814) 4. The Netherlands (813) 5. Belgium (803)
BIRMINGHAM CITY UNIVERSITY ACADEMIES TRUST SICK PAY AND ABSENCE MANAGEMENT SCHEME
 BIRMINGHAM CITY UNIVERSITY ACADEMIES TRUST SICK PAY AND ABSENCE MANAGEMENT SCHEME 1. Introduction 1.1. BCUAT wants to ensure that employees who are absent from work due to ill-health or injury receive
BIRMINGHAM CITY UNIVERSITY ACADEMIES TRUST SICK PAY AND ABSENCE MANAGEMENT SCHEME 1. Introduction 1.1. BCUAT wants to ensure that employees who are absent from work due to ill-health or injury receive
Mapping quality assurance approaches in Europe
 Mapping quality assurance approaches in Europe Reinhard Busse (with Helena Legido-Quigley & Martin McKee) Professor of Health Care Management, Technische Universität Berlin European Observatory on Health
Mapping quality assurance approaches in Europe Reinhard Busse (with Helena Legido-Quigley & Martin McKee) Professor of Health Care Management, Technische Universität Berlin European Observatory on Health
INNOBAROMETER 2015 - THE INNOVATION TRENDS AT EU ENTERPRISES
 Eurobarometer INNOBAROMETER 2015 - THE INNOVATION TRENDS AT EU ENTERPRISES REPORT Fieldwork: February 2015 Publication: September 2015 This survey has been requested by the European Commission, Directorate-General
Eurobarometer INNOBAROMETER 2015 - THE INNOVATION TRENDS AT EU ENTERPRISES REPORT Fieldwork: February 2015 Publication: September 2015 This survey has been requested by the European Commission, Directorate-General
Good Practice Guidelines for Appraisal
 Good Practice Guidelines for Appraisal Dr Laurence Mynors Wallis Dr David Fearnley February 2010 1 Contents Page Introduction 3 Link between appraisal and revalidation 4 Preparation for the appraisal meeting
Good Practice Guidelines for Appraisal Dr Laurence Mynors Wallis Dr David Fearnley February 2010 1 Contents Page Introduction 3 Link between appraisal and revalidation 4 Preparation for the appraisal meeting
How To Use An Electronic Health Record
 STRENGTHENING HEALTH INFORMATION INFRASTRUCTURE FOR QUALITY MEASUREMENT 5 th Conference on Quality Assurance in Health Care of the Federal Joint Committee, Berlin 14 October 2013 Jillian.Oderkirk@oecd.org
STRENGTHENING HEALTH INFORMATION INFRASTRUCTURE FOR QUALITY MEASUREMENT 5 th Conference on Quality Assurance in Health Care of the Federal Joint Committee, Berlin 14 October 2013 Jillian.Oderkirk@oecd.org
Chapter 13. The hospital-based cancer registry
 Chapter 13. The hospital-based cancer registry J.L. Young California Tumor Registry, 1812 14th Street, Suite 200, Sacramento, CA 95814, USA Introduction The purposes of a hospital-based cancer registry
Chapter 13. The hospital-based cancer registry J.L. Young California Tumor Registry, 1812 14th Street, Suite 200, Sacramento, CA 95814, USA Introduction The purposes of a hospital-based cancer registry
Responsibilities of Public Health Departments to Control Tuberculosis
 Responsibilities of Public Health Departments to Control Tuberculosis Purpose: Tuberculosis (TB) is an airborne infectious disease that endangers communities. This document articulates the activities that
Responsibilities of Public Health Departments to Control Tuberculosis Purpose: Tuberculosis (TB) is an airborne infectious disease that endangers communities. This document articulates the activities that
Henriëtte van der Horst VUmc Head of Department of General Practice and Elderly Care Medicine
 MUS and psychiatry in primary care Henriëtte van der Horst VUmc Head of Department of General Practice and Elderly Care Medicine Double Dutch: two topics Major changes in the mental health care organisation
MUS and psychiatry in primary care Henriëtte van der Horst VUmc Head of Department of General Practice and Elderly Care Medicine Double Dutch: two topics Major changes in the mental health care organisation
EUROPEAN UNION OF GENERAL PRACTITIONERS/FAMILY PHYSICIANS UNION EUROPEENNE DES MEDECINS OMNIPRATICIENS/MEDECINS DE FAMILLE
 EUROPEAN UNION OF GENERAL PRACTITIONERS/FAMILY PHYSICIANS UNION EUROPEENNE DES MEDECINS OMNIPRATICIENS/MEDECINS DE FAMILLE PRESIDENT: Dr. Ferenc Hajnal (Hungary) Dr. Eirik Bø Larsen (Norway) Dr. Francisco
EUROPEAN UNION OF GENERAL PRACTITIONERS/FAMILY PHYSICIANS UNION EUROPEENNE DES MEDECINS OMNIPRATICIENS/MEDECINS DE FAMILLE PRESIDENT: Dr. Ferenc Hajnal (Hungary) Dr. Eirik Bø Larsen (Norway) Dr. Francisco
HEALTH PROFESSIONALS IN EUROPE: NEW ROLES, NEW SKILLS
 HEALTH PROFESSIONALS IN EUROPE: NEW ROLES, NEW SKILLS "HEALTH PROFESSIONALS IN EUROPE: NEW ROLES, NEW SKILLS" HOPE EXCHANGE PROGRAMME 2009 HOPE, the European Hospital and Healthcare Federation, is a non-profit
HEALTH PROFESSIONALS IN EUROPE: NEW ROLES, NEW SKILLS "HEALTH PROFESSIONALS IN EUROPE: NEW ROLES, NEW SKILLS" HOPE EXCHANGE PROGRAMME 2009 HOPE, the European Hospital and Healthcare Federation, is a non-profit
Connection with other policy areas and (How does it fit/support wider early years work and partnerships)
") Illness such as gastroenteritis and upper respiratory tract infections, along with injuries caused by accidents in the home, are the leading causes of attendances at Accident & Emergency and hospitalisation
Illness such as gastroenteritis and upper respiratory tract infections, along with injuries caused by accidents in the home, are the leading causes of attendances at Accident & Emergency and hospitalisation
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Advocate Medical Group Case Study Organization Profile Advocate Medical Group is part of Advocate Health Care, a large, integrated, not-for-profit
Best Practices Managing Patients with Multiple Chronic Conditions Advocate Medical Group Case Study Organization Profile Advocate Medical Group is part of Advocate Health Care, a large, integrated, not-for-profit
NHS outcomes framework and CCG outcomes indicators: Data availability table
 NHS outcomes framework and CCG outcomes indicators: Data availability table December 2012 NHS OF objectives Preventing people from dying prematurely DOMAIN 1: preventing people from dying prematurely Potential
NHS outcomes framework and CCG outcomes indicators: Data availability table December 2012 NHS OF objectives Preventing people from dying prematurely DOMAIN 1: preventing people from dying prematurely Potential
Guidelines for Animal Disease Control
 Guidelines for Animal Disease Control 1. Introduction and objectives The guidelines are intended to help countries identify priorities, objectives and the desired goal of disease control programmes. Disease
Guidelines for Animal Disease Control 1. Introduction and objectives The guidelines are intended to help countries identify priorities, objectives and the desired goal of disease control programmes. Disease
Consultation: Two proposals for registered nurse prescribing
 Consultation: Two proposals for registered nurse prescribing Submission Form Please read and refer to the consultation document Two proposals for registered nurse prescribing available on the Nursing Council
Consultation: Two proposals for registered nurse prescribing Submission Form Please read and refer to the consultation document Two proposals for registered nurse prescribing available on the Nursing Council
EUCERD RECOMMENDATIONS QUALITY CRITERIA FOR CENTRES OF EXPERTISE FOR RARE DISEASES IN MEMBER STATES
 EUCERD RECOMMENDATIONS QUALITY CRITERIA FOR CENTRES OF EXPERTISE FOR RARE DISEASES IN MEMBER STATES 24 OCTOBER 2011 INTRODUCTION 1. THE EUROPEAN CONTEXT Centres of expertise (CE) and European Reference
EUCERD RECOMMENDATIONS QUALITY CRITERIA FOR CENTRES OF EXPERTISE FOR RARE DISEASES IN MEMBER STATES 24 OCTOBER 2011 INTRODUCTION 1. THE EUROPEAN CONTEXT Centres of expertise (CE) and European Reference
The Scottish Ambulance Service Improving Care, Reducing Costs. Working together for better patient care
 The Scottish Ambulance Service Improving Care, Reducing Costs Working together for better patient care Key points The Scottish Ambulance Service is seeing more people, faster, and offering better quality
The Scottish Ambulance Service Improving Care, Reducing Costs Working together for better patient care Key points The Scottish Ambulance Service is seeing more people, faster, and offering better quality
Rehabilitation. Care
 Rehabilitation Care Bruyère Continuing Care is the champion of well-being for aging Canadians and those requiring Continuing Care, helping them to become and remain as healthy and independent as possible
Rehabilitation Care Bruyère Continuing Care is the champion of well-being for aging Canadians and those requiring Continuing Care, helping them to become and remain as healthy and independent as possible
Standards of proficiency. Occupational therapists
 Standards of proficiency Occupational therapists Contents Foreword 1 Introduction 3 Standards of proficiency 7 Foreword We are pleased to present the Health and Care Professions Council s standards of
Standards of proficiency Occupational therapists Contents Foreword 1 Introduction 3 Standards of proficiency 7 Foreword We are pleased to present the Health and Care Professions Council s standards of
Policy proposals to improve access to multiple sclerosis treatments in Europe
 Policy proposals to improve access to multiple sclerosis treatments in Europe Key findings and conclusions EMSP Conference Oslo, 17 May 2016 This research builds on a study conducted by CRA in 2014 There
Policy proposals to improve access to multiple sclerosis treatments in Europe Key findings and conclusions EMSP Conference Oslo, 17 May 2016 This research builds on a study conducted by CRA in 2014 There
School of Broad Based Training (BBT) Core Trainee Year 1 JOB DESCRIPTION
 Core Trainee Year 1 JOB DESCRIPTION") School of Broad Based Training (BBT) Core Trainee Year 1 JOB DESCRIPTION Human Resources Department Lead Employer Trust Waterfront 4 Goldcrest Way Newburn Riverside Newcastle upon Tyne Tyne and Wear NE15
School of Broad Based Training (BBT) Core Trainee Year 1 JOB DESCRIPTION Human Resources Department Lead Employer Trust Waterfront 4 Goldcrest Way Newburn Riverside Newcastle upon Tyne Tyne and Wear NE15
SALUS: Enabling the Secondary Use of EHRs for Post Market Safety Studies
 SALUS: Enabling the Secondary Use of EHRs for Post Market Safety Studies May 2015 A. Anil SINACI, Deputy Project Coordinator SALUS: Scalable, Standard based Interoperability Framework for Sustainable Proactive
SALUS: Enabling the Secondary Use of EHRs for Post Market Safety Studies May 2015 A. Anil SINACI, Deputy Project Coordinator SALUS: Scalable, Standard based Interoperability Framework for Sustainable Proactive
INVESTMENT AND FINANCIAL SERVICES ASSOCIATION LIMITED CLAIMS GUIDELINES
 INVESTMENT AND FINANCIAL SERVICES ASSOCIATION LIMITED CLAIMS GUIDELINES CLAIMS GUIDELINES FOR MENTAL HEALTH CONDITIONS IFSA Guidance Note No. 14 September 2003 TABLE OF CONTENTS Paragraph Page Introduction
INVESTMENT AND FINANCIAL SERVICES ASSOCIATION LIMITED CLAIMS GUIDELINES CLAIMS GUIDELINES FOR MENTAL HEALTH CONDITIONS IFSA Guidance Note No. 14 September 2003 TABLE OF CONTENTS Paragraph Page Introduction
REPORT FROM THE COMMISSION TO THE EUROPEAN PARLIAMENT AND THE COUNCIL
 EUROPEAN COMMISSION Brussels, 25.9.2014 COM(2014) 592 final REPORT FROM THE COMMISSION TO THE EUROPEAN PARLIAMENT AND THE COUNCIL on the implementation in the period from 4 December 2011 until 31 December
EUROPEAN COMMISSION Brussels, 25.9.2014 COM(2014) 592 final REPORT FROM THE COMMISSION TO THE EUROPEAN PARLIAMENT AND THE COUNCIL on the implementation in the period from 4 December 2011 until 31 December
Course Description. SEMESTER I Fundamental Concepts of Substance Abuse MODULE OBJECTIVES
 Course Description SEMESTER I Fundamental Concepts of Substance Abuse MODULE OBJECTIVES At the end of this course participants will be able to: Define and distinguish between substance use, abuse and dependence
Course Description SEMESTER I Fundamental Concepts of Substance Abuse MODULE OBJECTIVES At the end of this course participants will be able to: Define and distinguish between substance use, abuse and dependence
A Guide for the Utilization of HIRA National Patient Samples. Logyoung Kim, Jee-Ae Kim, Sanghyun Kim. Health Insurance Review and Assessment Service
 A Guide for the Utilization of HIRA National Patient Samples Logyoung Kim, Jee-Ae Kim, Sanghyun Kim (Health Insurance Review and Assessment Service) Jee-Ae Kim (Corresponding author) Senior Research Fellow
A Guide for the Utilization of HIRA National Patient Samples Logyoung Kim, Jee-Ae Kim, Sanghyun Kim (Health Insurance Review and Assessment Service) Jee-Ae Kim (Corresponding author) Senior Research Fellow
RETAIL FINANCIAL SERVICES
 Special Eurobarometer 373 RETAIL FINANCIAL SERVICES REPORT Fieldwork: September 211 Publication: April 212 This survey has been requested by the European Commission, Directorate-General Internal Market
Special Eurobarometer 373 RETAIL FINANCIAL SERVICES REPORT Fieldwork: September 211 Publication: April 212 This survey has been requested by the European Commission, Directorate-General Internal Market
Quality summary report:
 Quality summary report: PMS Practices CLCH Quality Report Jan Dec 2011 Service exact name Personal Medical Services Practices Address line 1 Address line 2 Town/city County Postcode No. beds Website London
Quality summary report: PMS Practices CLCH Quality Report Jan Dec 2011 Service exact name Personal Medical Services Practices Address line 1 Address line 2 Town/city County Postcode No. beds Website London
Manifesto for Acquired Brain Injury Rehabilitation
 Manifesto for Acquired Brain Injury Rehabilitation For further information please contact: Chloë Hayward UKABIF Executive Director PO Box 355 Plymouth PL3 4WD Tel: 01752 601318 Email: ukabif@btconnect.com
Manifesto for Acquired Brain Injury Rehabilitation For further information please contact: Chloë Hayward UKABIF Executive Director PO Box 355 Plymouth PL3 4WD Tel: 01752 601318 Email: ukabif@btconnect.com
Acceptability of Rapid HIV Diagnosis. Practitioners in Spain
 Acceptability of Rapid HIV Diagnosis Technology among Primary Health Care Practitioners in Spain Agustí C, Fernàndez L, Mascort J, Carrillo R, Aguado C, Montoliu A, Puigdangolas X, De la Poza M, Rifà B,
Acceptability of Rapid HIV Diagnosis Technology among Primary Health Care Practitioners in Spain Agustí C, Fernàndez L, Mascort J, Carrillo R, Aguado C, Montoliu A, Puigdangolas X, De la Poza M, Rifà B,
TRANSFoRm: TRANSFoRming health care research and its implementation
 TRANSFoRm: TRANSFoRming health care research and its implementation Frank Sullivan, on behalf of the TRANSFoRm Consortium. Health Informatics Centre Dundee TRANSFoRm is partially funded by the European
TRANSFoRm: TRANSFoRming health care research and its implementation Frank Sullivan, on behalf of the TRANSFoRm Consortium. Health Informatics Centre Dundee TRANSFoRm is partially funded by the European
Policy and Procedure Manual
 Policy and Procedure Manual Resident Assessment (RA) Table of Contents RA-01 RA-02 RA-03 RA-04 RA-05 RA-06 RA-07 RA-08 RA-09 RA-10 RA-11 RA-12 Physical Health Services Dental Services Initial Nursing Summary
Policy and Procedure Manual Resident Assessment (RA) Table of Contents RA-01 RA-02 RA-03 RA-04 RA-05 RA-06 RA-07 RA-08 RA-09 RA-10 RA-11 RA-12 Physical Health Services Dental Services Initial Nursing Summary
Guideline: responsibilities for direction and delegation of care to enrolled nurses
 Guideline: responsibilities for direction and delegation of care to enrolled nurses Te whakarite i ngā mahi tapuhi kia tiakina ai te haumaru ā-iwi Regulating nursing practice to protect public safety May
Guideline: responsibilities for direction and delegation of care to enrolled nurses Te whakarite i ngā mahi tapuhi kia tiakina ai te haumaru ā-iwi Regulating nursing practice to protect public safety May
Standards of Physical Therapy Practice
 Standards of Physical Therapy Practice The World Confederation for Physical Therapy (WCPT) aims to improve the quality of global healthcare by encouraging high standards of physical therapy education and
Standards of Physical Therapy Practice The World Confederation for Physical Therapy (WCPT) aims to improve the quality of global healthcare by encouraging high standards of physical therapy education and
a) Each facility shall have a medical record system that retrieves information regarding individual residents.
 Each facility shall have a medical record system that retrieves information regarding individual residents.") TITLE 77: PUBLIC HEALTH CHAPTER I: DEPARTMENT OF PUBLIC HEALTH SUBCHAPTER c: LONG-TERM CARE FACILITIES PART 300 SKILLED NURSING AND INTERMEDIATE CARE FACILITIES CODE SECTION 300.1810 RESIDENT RECORD REQUIREMENTS
TITLE 77: PUBLIC HEALTH CHAPTER I: DEPARTMENT OF PUBLIC HEALTH SUBCHAPTER c: LONG-TERM CARE FACILITIES PART 300 SKILLED NURSING AND INTERMEDIATE CARE FACILITIES CODE SECTION 300.1810 RESIDENT RECORD REQUIREMENTS
RETAIL FINANCIAL SERVICES
 Special Eurobarometer 373 RETAIL FINANCIAL SERVICES REPORT Fieldwork: September 211 Publication: March 212 This survey has been requested by Directorate-General Internal Market and Services and co-ordinated
Special Eurobarometer 373 RETAIL FINANCIAL SERVICES REPORT Fieldwork: September 211 Publication: March 212 This survey has been requested by Directorate-General Internal Market and Services and co-ordinated
Self Care in New Zealand
 Self Care in New Zealand A roadmap toward greater personal responsibility in managing health Prepared by the New Zealand Self Medication Industry Association. July 2009 What is Self Care? Self Care describes
Self Care in New Zealand A roadmap toward greater personal responsibility in managing health Prepared by the New Zealand Self Medication Industry Association. July 2009 What is Self Care? Self Care describes
Guide to Ensuring Data Quality in Clinical Audits
 Guide to Ensuring Data Quality in Clinical Audits Nancy Dixon and Mary Pearce Healthcare Quality Quest Clinical audit tool to promote quality for better health services Contents 1 Introduction 1 1.1 Who
Guide to Ensuring Data Quality in Clinical Audits Nancy Dixon and Mary Pearce Healthcare Quality Quest Clinical audit tool to promote quality for better health services Contents 1 Introduction 1 1.1 Who
LISTER MEDICAL CENTRE
 LISTER MEDICAL CENTRE TITLE OF POST: NURSE PRACTITIONER : GENERAL PRACTICE SALARY : TBC HOURS OF EMPLOYMENT : TBC APPOINTMENT : Permanent contract RESPONSIBLE TO: PARTNERS ACCOUNTABLE TO: PARTNERS JOB
LISTER MEDICAL CENTRE TITLE OF POST: NURSE PRACTITIONER : GENERAL PRACTICE SALARY : TBC HOURS OF EMPLOYMENT : TBC APPOINTMENT : Permanent contract RESPONSIBLE TO: PARTNERS ACCOUNTABLE TO: PARTNERS JOB
Telemedicine - a challenge rather than solution for payers and service providers in EU
 Telemedicine - a challenge rather than solution for payers and service providers in EU K. Dziadek, MAHTA G. Waligora Keywords: adherence, e-health, telemedicine, telemonitoring DOI: 10.7365 / JHPOR.2015.1.1
Telemedicine - a challenge rather than solution for payers and service providers in EU K. Dziadek, MAHTA G. Waligora Keywords: adherence, e-health, telemedicine, telemonitoring DOI: 10.7365 / JHPOR.2015.1.1
Leadership and management for all doctors
 Leadership and management for all doctors The duties of a doctor registered with the General Medical Council Patients must be able to trust doctors with their lives and health. To justify that trust you
Leadership and management for all doctors The duties of a doctor registered with the General Medical Council Patients must be able to trust doctors with their lives and health. To justify that trust you
HSE Transformation Programme. to enable people live healthier and more fulfilled lives. Easy Access-public confidence- staff pride
 HSE Transformation Programme. to enable people live healthier and more fulfilled lives Easy Access-public confidence- staff pride The Health Service Executive 4.1 Chronic Illness Framework July 2008 1
HSE Transformation Programme. to enable people live healthier and more fulfilled lives Easy Access-public confidence- staff pride The Health Service Executive 4.1 Chronic Illness Framework July 2008 1
Best Practices in Managing Patients With Chronic Obstructive Pulmonary Disease (COPD)
") Best Practices in Managing Patients With Chronic Obstructive Pulmonary Disease (COPD) DuPage Medical Group Case Study Organization Profile Established in 1999, DuPage Medical Group (DMG) is a multispecialty
Best Practices in Managing Patients With Chronic Obstructive Pulmonary Disease (COPD) DuPage Medical Group Case Study Organization Profile Established in 1999, DuPage Medical Group (DMG) is a multispecialty