Less is more in: Emergency Oxygen Therapy
|
|
|
- Derrick Cox
- 7 years ago
- Views:
Transcription

1 Less is more in: Emergency Oxygen Therapy Dr Ronan O Driscoll Consultant Respiratory Physician Salford Royal University Hospital Salford M6 8 HD ronan.o.driscoll@srft.nhs.uk

2 Oxygen is the most commonly used drug in emergency medicine 34% of emergency ambulance patients receive oxygen Oxygen is used in about 2 million ambulance journeys in the UK each year
3 Oxygen in Hospital 15-17% of UK hospital patients were receiving oxygen during BTS audits About 18,000 people every day More than 2 million per year
4 Oxygen saves lives But too much oxygen may cause death Essential in severely ill patients with low blood oxygen levels High concentration oxygen probably causes >1,000 avoidable COPD deaths per year in the UK >100,000 COPD admissions per annum in UK with 7.5% mortality: Mortality 9% on high concentration O2 but 4% with controlled O2 Hyperoxaemia is linked to increased risk of death in strokes, ICU patients and survivors of cardiac arrest
5 Chaos reigned until 2008 Most patients were given too much oxygen And there was disagreement about how much oxygen to give Oxygen was rarely prescribed 68% of UK hospital patients who were using oxygen in 2008 had no prescription and most prescriptions were incomplete Doctors and nurses had very little knowledge about safe use of oxygen and many false beliefs
6 UK Emergency Oxygen Guideline published 2008 The Solution Endorsed or supported by 21 other Societies and Colleges
7 R O'Driscoll AAGBI WSM 2012
8 Key Principles of the Guideline Oxygen is a treatment for Hypoxemia (Giving oxygen does not relieve breathlessness or increase the oxygen supply to vital organs if the patient s oxygen level is normal to start with) Aim for a normal or near-normal oxygen saturation level for most patients (94-98%) Aim at a lower level for (88-92%) for those at risk from higher doses of oxygen Doctors prescribe a target range Nurses adjust equipment and flow rates to achieve the desired target range

9 What is normal and what is dangerous?
10 Normal Range for Oxygen saturation Normal range for healthy young adults is approximately 96-98% Slight fall with advancing age SpO2 ~0.5% lower above age 70
11 Effects of sudden hypoxia (e.g Removal of oxygen mask at altitude or in a pressure chamber) Impaired mental function; Onset at mean SaO 2 64% No evidence of mental impairment above SaO 2 of 84% Loss of consciousness: Onset at mean saturation of 56% Organ damage: Brain tissue is the most sensitive Death: Risk depends on extent and speed of onset and duration of hypoxia (no experimental studies in man) Test Pilots in decompression chambers do not experience breathlessness when the oxygen tension is lowered
12 Defining safe lower and upper limits of oxygen saturation
13 What is the minimum arterial oxygen level recommended in acute illness Target oxygen Saturation Critical care consensus guidelines Minimum 90% Surviving sepsis campaign Aim at 88-95% But these patients have intensive levels of nursing & monitoring BTS guideline recommends a minimum of 94% for most patients combines what is near normal and what is safe


14 Pulmonary Oxygen Toxicity Lorrain-Smith Effect
15
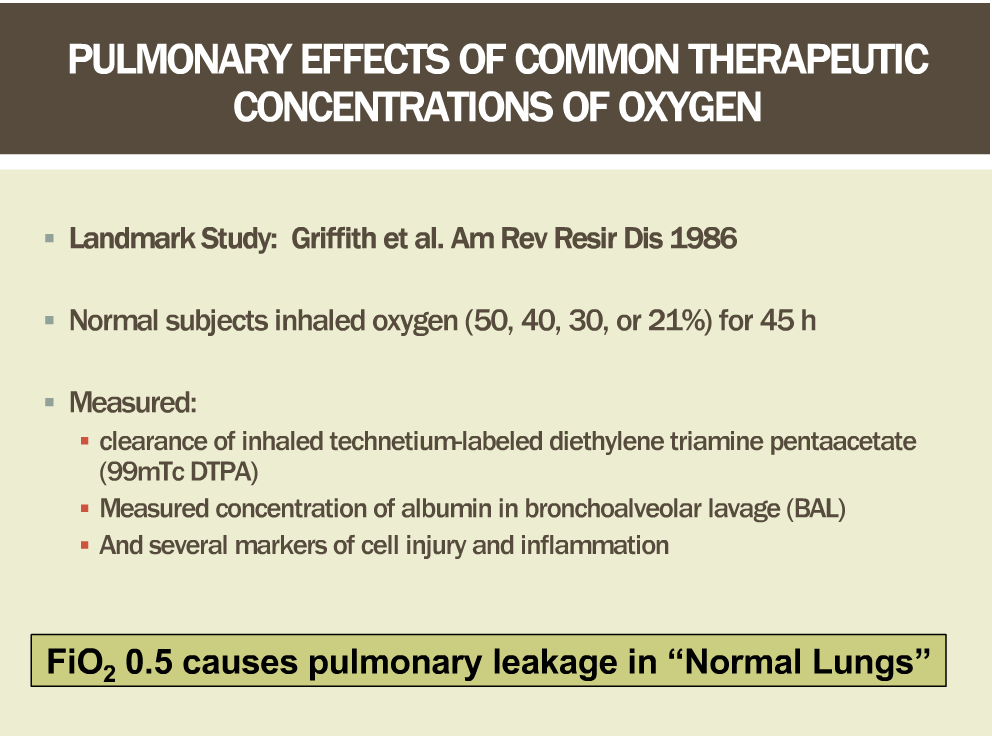
16 Exposure to high concentrations of oxygen may be harmful Absorption Atelectasis even at FIO % 1 Intrapulmonary shunting and post-operative hypoxaemia (on return to room air) 1 Risk to COPD patients 2 Coronary vasoconstriction 3 Increased Systemic Vascular Resistance 3 Reduced Cardiac Index after coronary bypass surgery 4 Possible reperfusion injury post Myocardial Infarction 5 Oxygen therapy increased mortality in non-hypoxic patients with mild-moderate stroke 6 Hyperoxaemia was associated with increased mortality in survivors of cardiac arrest 7 Hyperoxaemia was associated with increased mortality in the first 24 hours on ICU 8 BTS guideline recommends an upper limit of 98% for most patients. Combination of what is normal and safe
17 What is a safe lower Oxygen level in acute COPD? OxyHaemoglobin Dissociation Curve In acute COPD po 2 above 6.7 kpa or 50 mm Hg will prevent death SaO 2 above about 85% (Keep SpO 2 88% to allow for oximeter error and ensure SaO2 >85% ) SaO 2 mmhg PaO 2 Murphy R, Driscoll P, O Driscoll R Emerg Med J 2001; 18:333-9 BTS guideline recommends a minimum saturation of 88% for most COPD patients
18 What is a safe upper limit of oxygen target range in acute COPD? 47% of 982 patients with exacerbation of COPD were hypercapnic on arrival in hospital 20% had Respiratory Acidosis (ph < 7.35) 5% had ph < 7.25 (and were likely to need ICU care) Most hypercapnic patients with po 2 > 10 kpa were acidotic (equivalent to oxygen saturation of above ~ 92%) i.e. They had been given too much oxygen Plant et al Thorax 2000; 55:550 RECOMMENDED UPPER LIMITS Keep PaO2 below 10 kpa and keep SpO 2 92% in acute COPD
19 Recent clinical evidence Mortality in acute COPD was 9% when high concentration oxygen was given compared with 4% mortality with controlled oxygen (target range 88-92%) 1 Mortality in acute COPD was 11% when >35% oxygen was given but 7% when lower doses of oxygen were used 2 Need for ventilatory support; 22% v 9% 2 1. Austin MA, et al. BMJ Oct 18;341:c5462. doi: /bmj.c Roberts CM et al. Thorax 2011: 66: 43
20 Recommended target saturations The target ranges are a consensus agreement by the guidelines group and the endorsing colleges and societies Rationale for the target saturations is combination of what is normal and what is safe Most patients 94-98% Risk of hypercapnic respiratory failure 88 92%* *Or patient specific saturation on Alert Card
21 Oxygen saturation on air and survival for 37,593 acute medical admissions Smith GB et al. Resuscitation 2012 ;83:1201-5
22 Oxygen saturation on air and survival for 37,593 acute medical admissions Smith GB et al. Resuscitation 2012 ;83: Our findings suggest that the BTS should consider changing its target saturation for actively treated patients not at risk of hypercapnic respiratory failure to 96-98% Thus giving Oxygen to an extra 20% of all medical patients
23 Would normalising the respiratory rate with morphine and normalising the heart rate with beta blockers and increasing blood oxygen content by 2% be expected to save lives? BUT. There was an average 2% fall in mean and median saturation above age 65 (and age is a strong predictor of death) Hypoxaemia is a marker of disease severity just like tachycardia and tachypnoea

24 Why is oxygen used?
25 Aims of emergency oxygen therapy To correct / prevent potentially harmful hypoxaemia To alleviate breathlessness (only if hypoxaemic) Oxygen has no effect on breathlessness if the oxygen saturation is normal
26 Five common beliefs (But wrong in most circumstances) Routine administration of supplemental oxygen is useful, harmless and clinically indicated Giving oxygen is the most effective way to increase oxygen delivery to the tissues Oxygen relieves breathlessness at normal oxygen saturations High concentration oxygen is safe in all emergency situations apart from COPD Many patients are at risk from hypoxaemia and only a few near terminal COPD patients are at risk from hyperoxaemia
27 Prophylactic oxygen Less or More? Little increase in oxygen-carrying capacity (e.g. 3% rise in blood oxygen content at SpO 2 97%) Renders pulse oximetry worthless as a measure of ventilation May prevent early diagnosis & specific treatment of hypoventilation
28 Perioperative Oximetry Data from 23,000 patients in Cochrane Review Hypoxaemia was 1.5 to 3 times less common amongst patients monitored with oximetry if the results were made available to the clinicians More oxygen was given to these patients compared with patients where the oximetry reading was concealed from the clinicians No difference observed in complications or mortality i.e. Correcting modest hypoxaemia may confer no benefit to patients although clinicians who saw oximeter results believed that they had prevented harm to several patients
29 Five common beliefs (But wrong in most circumstances) Routine administration of supplemental oxygen is useful, harmless and clinically indicated Giving oxygen is the most effective way to increase oxygen delivery to the tissues Oxygen relieves breathlessness at normal oxygen saturations High concentration oxygen is safe in all emergency situations apart from COPD Many patients are at risk from hypoxaemia and only a few near terminal COPD patients are at risk from hyperoxaemia
30 Oxygen therapy is only one element in the resuscitation of a critically ill patient The oxygen carrying power of blood may be increased by Safeguarding the airway Enhancing circulating volume Correcting severe anaemia Enhancing cardiac output Avoiding/Reversing Respiratory Depressants Increasing Fraction of Inspired Oxygen (FIO 2 ) Establish the reason for Hypoxaemia and treat the underlying cause (e.g Bronchospasm, LVF etc) Patient may need, CPAP or NIV or Invasive ventilation
31 Five common beliefs (But wrong in most circumstances) Routine administration of supplemental oxygen is useful, harmless and clinically indicated Giving oxygen is the most effective way to increase oxygen delivery to the tissues Oxygen relieves breathlessness at normal oxygen saturations High concentration oxygen is safe in all emergency situations apart from COPD Many patients are at risk from hypoxaemia and only a few near terminal COPD patients are at risk from hyperoxaemia
32 Does oxygen relieve breathlessness in COPD and in Palliative Care? Short Burst Oxygen Therapy administered after exercise does not relieve breathlessness in non-hypoxaemic patients with COPD 1 Nasal oxygen did not relieve breathlessness in palliative care patients with PaO2 > 7.3 kpa 2
33 Five common beliefs (But wrong in most circumstances) Routine administration of supplemental oxygen is useful, harmless and clinically indicated Giving oxygen is the most effective way to increase oxygen delivery to the tissues Oxygen relieves breathlessness at normal oxygen saturations High concentration oxygen is safe in all emergency situations apart from COPD Many patients are at risk from hypoxaemia and only a few near terminal COPD patients are at risk from hyperoxaemia
34 Patients at risk of hypercapnia/acidosis due to high concentration oxygen (even with PaO 2 in the normal range) Chronic hypoxic lung diseases COPD Severe Chronic Asthma Bronchiectasis / Cystic Fibrosis Chest wall disease Kyphoscoliosis Thoracoplasty Neuromuscular disease Obesity hypoventilation
 2 Hyperoxaemia was associated with increased")
35 Patients at potential risk from hyperoxaemia COPD patients and other groups shown in the previous slide are at risk if oxygen saturation is elevated beyond 92% are at increased risk if SpO 2 is raised above 98% Myocardial Infarction 1 Increased mortality in non-hypoxic patients with mildmoderate stroke randomised to oxygen (controlled trial) 2 Hyperoxaemia was associated with increased mortality in survivors of cardiac arrest 3 Hyperoxaemia was associated with increased mortality in the first 24 hours on ICU 4
36 Hospital Mortality Hyperoxia 63% Normoxia 45% Hypoxia 57%
37

38
39 Mortality for each quintile Mortality according to calculated oxygen saturation level Adapted from dejonge et al Critical Care 2008; Overall mortality 31% <93% % % % >98.8% Estimated oxygen saturation based on conversion from PaO2 Adapted from table 2 in de-jonge et al Critical Care 2008, 12:R156 Multivariate regression analysis of in-hospital mortality based on arterial oxygen tension in first 24 hours on ICU Overall hospital mortality for 36,307 consecutive ICU patients was 31%
40 Five common beliefs (But wrong in most circumstances) Routine administration of supplemental oxygen is useful, harmless and clinically indicated Giving oxygen is the most effective way to increase oxygen delivery to the tissues Oxygen relieves breathlessness at normal oxygen saturations High concentration oxygen is safe in all emergency situations apart from COPD Many patients are at risk from hypoxaemia and only a few near terminal COPD patients are at risk from hyperoxaemia
41 Audit of 7956 blood gas samples at one hospital over one year 10% of samples outside A&E had Type 1 respiratory failure with PO2 <8 kpa and normal or low PCO2 (30% of A&E samples showed Type 1 Failure) 22% had Type 2 respiratory failure (including 7% with respiratory acidosis) 24% of patients who had blood gases sampled had risk factors for Type 2 Respiratory Failure and 73% of these samples had saturation >92% 26% of samples had saturation >98%
42 Oxygen prescription Model for oxygen section in hospital prescription charts DRUG OXYGEN (Refer To Trust Oxygen Policy) Circle target oxygen saturation 88-92% 94-98% Other STOP DATE Starting device/flow rate PRN / Continuous Tick if saturation not indicated PHARM (Saturation is indicated in almost all cases except for palliative terminal care) SIGNATURE / PRINT NAME DATE ddmmyy
43 What device and flow rate should you use in each situation?
44 Standard Oxygen Therapy 1960s-2008 Acute Patients Stable Patients
45 Oxygen therapy 2008 onwards Critical illness Selected COPD patients Most patients
46 Prescribe to target BTS Recommendations Critical Illness Requiring High Levels of Oxygen Supplementation Serious Illness Requiring Moderate Levels of Oxygen if the Patient is Hypoxaemic COPD and Other Conditions Requiring Controlled or low-dose Oxygen Therapy Conditions for which patients should be monitored closely but oxygen therapy is not required unless the patient is hypoxaemic
47 Some patients need high-dose oxygen to normalise saturation (Usually for short periods of time) Severe Pneumonia Severe LVF Major Trauma Sepsis and Shock Major atelectasis Pulmonary Embolism Exacerbation Lung Fibrosis etc
48 Titrating Oxygen up and down. This table below shows APPROXIMATE conversion values. Venturi 24% (blue) 2-4l/min OR Nasal specs 1L Venturi 28% (white) 4-6 l/min OR Nasal specs 2L Venturi 35% (yellow) 8-10l/min OR Nasal spec 4L Venturi 40% (red)10-12l/min OR Simple face mask 5-6L/min Venturi 60% (green) 15l/min OR Simple face mask 7-10L/min Reservoir mask at 15L oxygen flow seek medical advice I f reservoir mask required seek senior medical Input immediately
49 Monitoring patients Oxygen saturation and delivery system should be recorded on the monitoring chart Delivery devices and/or flow rates should be adjusted to keep oxygen saturation in target range
50 Implementation and Dissemination Incorporation of Emergency Oxygen Guidelines in other Guidelines JRCALC (Joint Royal Colleges Ambulance Liaison Committee) Oxygen Guideline April 2009 BTS Pneumonia Guideline 2009 NICE Guideline for Chest Pain of Recent Onset March 2010 Resuscitation Council (UK) Guideline 2010 European Resuscitation Guideline 2010 BTS-SIGN Asthma Guideline 2011
51 Summary Oxygen is like every other drug Use no more than is necessary If it is used properly for the right indications, it is beneficial and safe Giving oxygen to those who do not need it or giving too much or too little oxygen may cause harm Compared with present practice, it is likely that a reduction in oxygen use will deliver safer care, especially for patients at risk of hypercapnia. Further information at
52 Who was the first person to realise that moderate oxygen may be safer than pure oxygen? Less is More
Oxygen - update April 2009 OXG
 PRESENTATION Oxygen (O 2 ) is a gas provided in compressed form in a cylinder. It is also available in liquid form, in a system adapted for ambulance use. It is fed via a regulator and flow meter to the
PRESENTATION Oxygen (O 2 ) is a gas provided in compressed form in a cylinder. It is also available in liquid form, in a system adapted for ambulance use. It is fed via a regulator and flow meter to the
Oxygen Therapy. Oxygen therapy quick guide V3 July 2012.
 PRESENTATION Oxygen (O 2 ) is a gas provided in a compressed form in a cylinder. It is also available in a liquid form. It is fed via a regulator and flow meter to the patient by means of plastic tubing
PRESENTATION Oxygen (O 2 ) is a gas provided in a compressed form in a cylinder. It is also available in a liquid form. It is fed via a regulator and flow meter to the patient by means of plastic tubing
Respiratory failure and Oxygen Therapy
 Respiratory failure and Oxygen Therapy A patient with Hb 15 G % will carry 3X more O2 in his blood than someone with Hb 5G % Give Controlled O2 treatment in acute pulmonary oedema to avoid CO2 retention
Respiratory failure and Oxygen Therapy A patient with Hb 15 G % will carry 3X more O2 in his blood than someone with Hb 5G % Give Controlled O2 treatment in acute pulmonary oedema to avoid CO2 retention
Lothian Guideline for Domiciliary Oxygen Therapy Service for COPD
 Lothian Guideline for Domiciliary Oxygen Therapy Service for COPD This document describes the standard for clinical assessment, prescription, optimal management and follow-up of patients receiving domiciliary
Lothian Guideline for Domiciliary Oxygen Therapy Service for COPD This document describes the standard for clinical assessment, prescription, optimal management and follow-up of patients receiving domiciliary
Oxygenation and Oxygen Therapy Michael Billow, D.O.
 Oxygenation and Oxygen Therapy Michael Billow, D.O. The delivery of oxygen to all body tissues is the essence of critical care. Patients in respiratory distress/failure come easily to mind as the ones
Oxygenation and Oxygen Therapy Michael Billow, D.O. The delivery of oxygen to all body tissues is the essence of critical care. Patients in respiratory distress/failure come easily to mind as the ones
Policy for the Prescription and Administration of Oxygen to Adults in Inpatient Facilities
 Policy for the Prescription and Administration of Oxygen to Adults in Inpatient Facilities August 2013 Page 1 of 32 Policy Title Policy for the Prescription and Administration of Oxygen to Adults in Inpatient
Policy for the Prescription and Administration of Oxygen to Adults in Inpatient Facilities August 2013 Page 1 of 32 Policy Title Policy for the Prescription and Administration of Oxygen to Adults in Inpatient
ANZCOR Guideline 11.6.1 Targeted Oxygen Therapy in Adult Advanced Life Support
 ANZCOR Guideline 11.6.1 Targeted Oxygen Therapy in Adult Advanced Life Support Summary This guideline provides advice on the administration of oxygen in the peri-arrest period. Who does this guideline
ANZCOR Guideline 11.6.1 Targeted Oxygen Therapy in Adult Advanced Life Support Summary This guideline provides advice on the administration of oxygen in the peri-arrest period. Who does this guideline
GUIDELINES FOR ACUTE OXYGEN THERAPY FOR WESTERN AUSTRALIAN HOSPITALS
 GUIDELINES FOR ACUTE OXYGEN THERAPY FOR WESTERN AUSTRALIAN HOSPITALS Key Points 1. No patient should be denied oxygen therapy in an emergency. Patients in cardiac and/or respiratory arrest should be managed
GUIDELINES FOR ACUTE OXYGEN THERAPY FOR WESTERN AUSTRALIAN HOSPITALS Key Points 1. No patient should be denied oxygen therapy in an emergency. Patients in cardiac and/or respiratory arrest should be managed
Pulmonary Diseases. Lung Disease: Pathophysiology, Medical and Exercise Programming. Overview of Pathophysiology
 Lung Disease: Pathophysiology, Medical and Exercise Programming Overview of Pathophysiology Ventilatory Impairments Increased airway resistance Reduced compliance Increased work of breathing Ventilatory
Lung Disease: Pathophysiology, Medical and Exercise Programming Overview of Pathophysiology Ventilatory Impairments Increased airway resistance Reduced compliance Increased work of breathing Ventilatory
NICE Pathways bring together all NICE guidance, quality standards and other NICE information on a specific topic.
 bring together all NICE guidance, quality standards and other NICE information on a specific topic. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published.
bring together all NICE guidance, quality standards and other NICE information on a specific topic. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published.
Prescribing and Administration of Emergency Oxygen in Adults Policy
 This is an official Northern Trust policy and should not be edited in any way Prescribing and Administration of Emergency Oxygen in Adults Policy Reference Number: NHSCT/12/542 Target audience: Medical,
This is an official Northern Trust policy and should not be edited in any way Prescribing and Administration of Emergency Oxygen in Adults Policy Reference Number: NHSCT/12/542 Target audience: Medical,
CLINICAL COMPONENT FOR THE HOME OXYGEN SERVICE IN ENGLAND AND WALES
 CLINICAL COMPONENT FOR THE HOME OXYGEN SERVICE IN ENGLAND AND WALES This document has been prepared by members of the British Thoracic Society (BTS) Working Group on Home Oxygen Services, which is a Sub-Committee
CLINICAL COMPONENT FOR THE HOME OXYGEN SERVICE IN ENGLAND AND WALES This document has been prepared by members of the British Thoracic Society (BTS) Working Group on Home Oxygen Services, which is a Sub-Committee
Understanding Hypoventilation and Its Treatment by Susan Agrawal
 www.complexchild.com Understanding Hypoventilation and Its Treatment by Susan Agrawal Most of us have a general understanding of what the term hyperventilation means, since hyperventilation, also called
www.complexchild.com Understanding Hypoventilation and Its Treatment by Susan Agrawal Most of us have a general understanding of what the term hyperventilation means, since hyperventilation, also called
Applicant Information Sheet for MASS 45 Adult Oxygen: Initial Application and 4 Month Review
 , Queensland Health Applicant Information Sheet for Applicants should retain this section for their records Eligibility Administrative eligibility is dependent upon the applicant being a permanent Queensland
, Queensland Health Applicant Information Sheet for Applicants should retain this section for their records Eligibility Administrative eligibility is dependent upon the applicant being a permanent Queensland
Common Ventilator Management Issues
 Common Ventilator Management Issues William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center You have just admitted a 28 year-old
Common Ventilator Management Issues William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center You have just admitted a 28 year-old
MECHINICAL VENTILATION S. Kache, MD
 MECHINICAL VENTILATION S. Kache, MD Spontaneous respiration vs. Mechanical ventilation Natural spontaneous ventilation occurs when the respiratory muscles, diaphragm and intercostal muscles pull on the
MECHINICAL VENTILATION S. Kache, MD Spontaneous respiration vs. Mechanical ventilation Natural spontaneous ventilation occurs when the respiratory muscles, diaphragm and intercostal muscles pull on the
The Sepsis Puzzle: Identification, Monitoring and Early Goal Directed Therapy
 The Sepsis Puzzle: Identification, Monitoring and Early Goal Directed Therapy Cindy Goodrich RN, MS, CCRN Content Description Sepsis is caused by widespread tissue injury and systemic inflammation resulting
The Sepsis Puzzle: Identification, Monitoring and Early Goal Directed Therapy Cindy Goodrich RN, MS, CCRN Content Description Sepsis is caused by widespread tissue injury and systemic inflammation resulting
Cardio-Pulmonary Resuscitation (CPR): A Decision Aid For. KGH Patients And Their Families
: A Decision Aid For. KGH Patients And Their Families") Cardio-Pulmonary Resuscitation (CPR): A Decision Aid For KGH Patients And Their Families The goal of this pamphlet is to provide information about cardiopulmonary resuscitation (CPR) so you can be adequately
Cardio-Pulmonary Resuscitation (CPR): A Decision Aid For KGH Patients And Their Families The goal of this pamphlet is to provide information about cardiopulmonary resuscitation (CPR) so you can be adequately
Peninsula Community Health. Policy for the Prescription, Administration. monitoring of Oxygen and Emergency Oxygen in Adults
 Peninsula Community Health Policy for the Prescription, Administration and monitoring of Oxygen and Emergency Oxygen in Adults Title: Policy for the Prescription, Administration and monitoring of Emergency
Peninsula Community Health Policy for the Prescription, Administration and monitoring of Oxygen and Emergency Oxygen in Adults Title: Policy for the Prescription, Administration and monitoring of Emergency
GUIDELINES FOR THE MANAGEMENT OF OXYGEN THERAPY
 SOUTH DURHAM HEALTH CARE NHS TRUST GUIDELINES FOR THE MANAGEMENT OF OXYGEN THERAPY AIM To supplement oxygen intake using the appropriate equipment in order to correct hypoxia and relieve breathlessness.
SOUTH DURHAM HEALTH CARE NHS TRUST GUIDELINES FOR THE MANAGEMENT OF OXYGEN THERAPY AIM To supplement oxygen intake using the appropriate equipment in order to correct hypoxia and relieve breathlessness.
Management of exacerbations in chronic obstructive pulmonary disease in Primary Care
 Management of exacerbations in chronic obstructive pulmonary disease in Primary Care Acute exacerbations of chronic obstructive pulmonary disease (COPD) are associated with significant morbidity and mortality.
Management of exacerbations in chronic obstructive pulmonary disease in Primary Care Acute exacerbations of chronic obstructive pulmonary disease (COPD) are associated with significant morbidity and mortality.
Pathophysiology of hypercapnic and hypoxic respiratory failure and V/Q relationships. Dr.Alok Nath Department of Pulmonary Medicine PGIMER Chandigarh
 Pathophysiology of hypercapnic and hypoxic respiratory failure and V/Q relationships Dr.Alok Nath Department of Pulmonary Medicine PGIMER Chandigarh Jan 2006 Respiratory Failure inadequate blood oxygenation
Pathophysiology of hypercapnic and hypoxic respiratory failure and V/Q relationships Dr.Alok Nath Department of Pulmonary Medicine PGIMER Chandigarh Jan 2006 Respiratory Failure inadequate blood oxygenation
Guideline for the prescription and administration of oxygen in children. Royal Hospital for Sick Children, Glasgow
 Guideline for the prescription and administration of oxygen in children. Royal Hospital for Sick Children, Glasgow Author: Dr Louise Thomson, Paediatric Respiratory Consultant Lynda Peacock, Complex Respiratory
Guideline for the prescription and administration of oxygen in children. Royal Hospital for Sick Children, Glasgow Author: Dr Louise Thomson, Paediatric Respiratory Consultant Lynda Peacock, Complex Respiratory
Critical Care Billing and Coding. Date: February 2015 Presented by: Part B Provider Outreach & Education (POE)
") Critical Care Billing and Coding Date: February 2015 Presented by: Part B Provider Outreach & Education (POE) Workshop Protocol Cannot register with WebEx using mobile device Must use desktop or laptop
Critical Care Billing and Coding Date: February 2015 Presented by: Part B Provider Outreach & Education (POE) Workshop Protocol Cannot register with WebEx using mobile device Must use desktop or laptop
Medical Section. Email : acmedical@aircanada.ca. Fax : 1 888 334-7717 (toll-free) or 514 828-0027
 or 514 828-0027") Departure Date: Medical Section Hours of Operation MON-FRI 06:00-20:00 EST SAT-SUN 06:00-18 :00 EST Email : acmedical@aircanada.ca Fax : 1 888 334-7717 (toll-free) or 514 828-0027 Telephone : 1 800 667-4732
Departure Date: Medical Section Hours of Operation MON-FRI 06:00-20:00 EST SAT-SUN 06:00-18 :00 EST Email : acmedical@aircanada.ca Fax : 1 888 334-7717 (toll-free) or 514 828-0027 Telephone : 1 800 667-4732
The Initial and 24 h (After the Patient Rehabilitation) Deficit of Arterial Blood Gases as Predictors of Patients Outcome
 Deficit of Arterial Blood Gases as Predictors of Patients Outcome") Biomedical & Pharmacology Journal Vol. 6(2), 259-264 (2013) The Initial and 24 h (After the Patient Rehabilitation) Deficit of Arterial Blood Gases as Predictors of Patients Outcome Vadod Norouzi 1, Ali
Biomedical & Pharmacology Journal Vol. 6(2), 259-264 (2013) The Initial and 24 h (After the Patient Rehabilitation) Deficit of Arterial Blood Gases as Predictors of Patients Outcome Vadod Norouzi 1, Ali
Acute heart failure may be de novo or it may be a decompensation of chronic heart failure.
 Management of Acute Left Ventricular Failure Acute left ventricular failure presents as pulmonary oedema due to increased pressure in the pulmonary capillaries. It is important to realise though that left
Management of Acute Left Ventricular Failure Acute left ventricular failure presents as pulmonary oedema due to increased pressure in the pulmonary capillaries. It is important to realise though that left
Heart Attack: What You Need to Know
 A WorkLife4You Guide Heart Attack: What You Need to Know What is a Heart Attack? The heart works 24 hours a day, pumping oxygen and nutrient-rich blood to the body. Blood is supplied to the heart through
A WorkLife4You Guide Heart Attack: What You Need to Know What is a Heart Attack? The heart works 24 hours a day, pumping oxygen and nutrient-rich blood to the body. Blood is supplied to the heart through
Overview. Geriatric Overview. Chapter 26. Geriatrics 9/11/2012
 Chapter 26 Geriatrics Slide 1 Overview Trauma Common Medical Emergencies Special Considerations in the Elderly Medication Considerations Abuse and Neglect Expanding the Role of EMS Slide 2 Geriatric Overview
Chapter 26 Geriatrics Slide 1 Overview Trauma Common Medical Emergencies Special Considerations in the Elderly Medication Considerations Abuse and Neglect Expanding the Role of EMS Slide 2 Geriatric Overview
Early Warning Scores (EWS) Clinical Sessions 2011 By Bhavin Doshi
 Clinical Sessions 2011 By Bhavin Doshi") Early Warning Scores (EWS) Clinical Sessions 2011 By Bhavin Doshi What is EWS? After qualifying, junior doctors are expected to distinguish between the moderately sick patients who can be managed in the
Early Warning Scores (EWS) Clinical Sessions 2011 By Bhavin Doshi What is EWS? After qualifying, junior doctors are expected to distinguish between the moderately sick patients who can be managed in the
Arterial Blood Gas Case Questions and Answers
 Arterial Blood Gas Case Questions and Answers In the space that follows you will find a series of cases that include arterial blood gases. Each case is then followed by an explanation of the acid-base
Arterial Blood Gas Case Questions and Answers In the space that follows you will find a series of cases that include arterial blood gases. Each case is then followed by an explanation of the acid-base
Chapter 26. Assisting With Oxygen Needs. Elsevier items and derived items 2014, 2010 by Mosby, an imprint of Elsevier Inc. All rights reserved.
 Chapter 26 Assisting With Oxygen Needs Oxygen (O 2 ) is a gas. Oxygen It has no taste, odor, or color. It is a basic need required for life. Death occurs within minutes if breathing stops. Brain damage
Chapter 26 Assisting With Oxygen Needs Oxygen (O 2 ) is a gas. Oxygen It has no taste, odor, or color. It is a basic need required for life. Death occurs within minutes if breathing stops. Brain damage
More detailed background information and references can be found at the end of this guideline
 Neonatal Intensive Care Unit Clinical Guideline Oxygen Over the past few years there have been significant changes, based on high quality research, in our understanding of how to give the right amount
Neonatal Intensive Care Unit Clinical Guideline Oxygen Over the past few years there have been significant changes, based on high quality research, in our understanding of how to give the right amount
Documenting & Coding. Chronic Obstructive Pulmonary Disease (COPD) Presented by: David S. Brigner, MLA, CPC
 Presented by: David S. Brigner, MLA, CPC") Documenting & Coding Chronic Obstructive Pulmonary Disease (COPD) Presented by: David S. Brigner, MLA, CPC Sr. Provider Training & Development Consultant Professional Profile David Brigner currently performs
Documenting & Coding Chronic Obstructive Pulmonary Disease (COPD) Presented by: David S. Brigner, MLA, CPC Sr. Provider Training & Development Consultant Professional Profile David Brigner currently performs
Adult Home Oxygen Therapy. Purpose To provide guidance on the requirements for and procedures relating to domiciliary oxygen therapy.
 Contents Purpose... 1 Scope/Audience... 1 Categories for Home Oxygen Therapy... 2 Assessment for Home Oxygen Therapy... 3 Investigations... 3 Requests for home oxygen... 3 Provision of Home Oxygen... 4
Contents Purpose... 1 Scope/Audience... 1 Categories for Home Oxygen Therapy... 2 Assessment for Home Oxygen Therapy... 3 Investigations... 3 Requests for home oxygen... 3 Provision of Home Oxygen... 4
Importance of Protocols in the Decision to Use Noninvasive Ventilation
 Importance of Protocols in the Decision to Use Noninvasive Ventilation Janice L. Zimmerman, M.D. Weill Cornell Medical College The Methodist Hospital Houston, Texas Objectives Review application of protocols
Importance of Protocols in the Decision to Use Noninvasive Ventilation Janice L. Zimmerman, M.D. Weill Cornell Medical College The Methodist Hospital Houston, Texas Objectives Review application of protocols
James F. Kravec, M.D., F.A.C.P
 James F. Kravec, M.D., F.A.C.P Chairman, Department of Internal Medicine, St. Elizabeth Health Center Chair, General Internal Medicine, Northeast Ohio Medical University Associate Medical Director, Hospice
James F. Kravec, M.D., F.A.C.P Chairman, Department of Internal Medicine, St. Elizabeth Health Center Chair, General Internal Medicine, Northeast Ohio Medical University Associate Medical Director, Hospice
Oxygenation. Chapter 21. Anatomy and Physiology of Breathing. Anatomy and Physiology of Breathing*
 Oxygenation Chapter 21 Anatomy and Physiology of Breathing Inspiration ~ breathing in Expiration ~ breathing out Ventilation ~ Movement of air in & out of the lungs Respiration ~ exchange of O2 & carbon
Oxygenation Chapter 21 Anatomy and Physiology of Breathing Inspiration ~ breathing in Expiration ~ breathing out Ventilation ~ Movement of air in & out of the lungs Respiration ~ exchange of O2 & carbon
EMERGENCY MEDICINE. Oxygen Therapy. CP Singh*, Nachhattar Singh**, Jagraj Singh***, Gurmeet Kaur Brar****, Gagandeep Singh****
 EMERGENCY MEDICINE Oxygen Therapy CP Singh*, Nachhattar Singh**, Jagraj Singh***, Gurmeet Kaur Brar****, Gagandeep Singh**** Abstract The primary goal of oxygen therapy is to correct alveolar and/or tissue
EMERGENCY MEDICINE Oxygen Therapy CP Singh*, Nachhattar Singh**, Jagraj Singh***, Gurmeet Kaur Brar****, Gagandeep Singh**** Abstract The primary goal of oxygen therapy is to correct alveolar and/or tissue
Recommendations: Other Supportive Therapy of Severe Sepsis*
 Recommendations: Other Supportive Therapy of Severe Sepsis* K. Blood Product Administration 1. Once tissue hypoperfusion has resolved and in the absence of extenuating circumstances, such as myocardial
Recommendations: Other Supportive Therapy of Severe Sepsis* K. Blood Product Administration 1. Once tissue hypoperfusion has resolved and in the absence of extenuating circumstances, such as myocardial
Prescription and Administration of Emergency Oxygen in Adults in Hospital. Charlie Turner, Senior Nurse Patient Safety
 Policy: Prescription and Administration of Emergency Oxygen in Adults in Hospital Executive or Associate Director lead Policy author/ lead Feedback on implementation to Karen Tomlinson, Executive/Chief
Policy: Prescription and Administration of Emergency Oxygen in Adults in Hospital Executive or Associate Director lead Policy author/ lead Feedback on implementation to Karen Tomlinson, Executive/Chief
Ventilation Perfusion Relationships
 Ventilation Perfusion Relationships VENTILATION PERFUSION RATIO Ideally, each alveolus in the lungs would receive the same amount of ventilation and pulmonary capillary blood flow (perfusion). In reality,
Ventilation Perfusion Relationships VENTILATION PERFUSION RATIO Ideally, each alveolus in the lungs would receive the same amount of ventilation and pulmonary capillary blood flow (perfusion). In reality,
How To Get On A Jet Plane
 Nature of disability Hospital Details TEL : +91 22 6711 6618 / 09 l FAX : +91 22 26156290 +91 11 49637953 +91 44 22568009 +91 33 25111359 Information Sheet for Guest Requiring Medical Clearance (to be
Nature of disability Hospital Details TEL : +91 22 6711 6618 / 09 l FAX : +91 22 26156290 +91 11 49637953 +91 44 22568009 +91 33 25111359 Information Sheet for Guest Requiring Medical Clearance (to be
AT HOME DR. D. K. PILLAI MUG @ UOM
 NON - INVASIVE VENTILATION AT HOME DR. D. K. PILLAI 07.09.2011 MUG @ UOM In the beginning came. OSA (HS) 1. CPAP for OSAHS (Obstructive Sleep Apnoea Hypopnoea Syndrome) 2 NIPPV 2. NIPPV (Non
NON - INVASIVE VENTILATION AT HOME DR. D. K. PILLAI 07.09.2011 MUG @ UOM In the beginning came. OSA (HS) 1. CPAP for OSAHS (Obstructive Sleep Apnoea Hypopnoea Syndrome) 2 NIPPV 2. NIPPV (Non
Telemedicine Resuscitation & Arrest Trials (TreAT)
") Telemedicine Resuscitation & Arrest Trials (TreAT) Telemedicine within the ED for treating Severe Sepsis: A Hub and Spoke Telemedicine pilot SUMR Intern: Karole Collier Mentor: Dr. Brendan Carr & Dr. Anish
Telemedicine Resuscitation & Arrest Trials (TreAT) Telemedicine within the ED for treating Severe Sepsis: A Hub and Spoke Telemedicine pilot SUMR Intern: Karole Collier Mentor: Dr. Brendan Carr & Dr. Anish
RGN JOY LAUDE WATFORD GENERAL HOSPITAL, ENGLAND
 RGN JOY LAUDE WATFORD GENERAL HOSPITAL, ENGLAND Monitor patient on the ward to detect trends in vital signs and to manage accordingly To recognise deteriorating trends and request relevant medical/out
RGN JOY LAUDE WATFORD GENERAL HOSPITAL, ENGLAND Monitor patient on the ward to detect trends in vital signs and to manage accordingly To recognise deteriorating trends and request relevant medical/out
NHS FORTH VALLEY Neonatal Oxygen Saturation Guideline
 NHS FORTH VALLEY Neonatal Oxygen Saturation Guideline Date of First Issue 11/07/2011 Approved 30/09/2011 Current Issue Date 07/09/2011 Review Date July 2013 Version 1 EQIA Yes 22/10/2011 Author / Contact
NHS FORTH VALLEY Neonatal Oxygen Saturation Guideline Date of First Issue 11/07/2011 Approved 30/09/2011 Current Issue Date 07/09/2011 Review Date July 2013 Version 1 EQIA Yes 22/10/2011 Author / Contact
From AARC Protocol Committee; Subcommittee Adult Critical Care Version 1.0a (Sept., 2003), Subcommittee Chair, Susan P. Pilbeam
, Subcommittee Chair, Susan P. Pilbeam") AARC - ADULT MECHANICAL VENTILATOR PROTOCOLS 1. Guidelines for Using Ventilator Protocols 2. Definition of Modes and Suggestions for Use of Modes 3. Adult Respiratory Ventilator Protocol - Guidelines for
AARC - ADULT MECHANICAL VENTILATOR PROTOCOLS 1. Guidelines for Using Ventilator Protocols 2. Definition of Modes and Suggestions for Use of Modes 3. Adult Respiratory Ventilator Protocol - Guidelines for
Medicare C/D Medical Coverage Policy
 Medicare C/D Medical Coverage Policy Oxygen and Oxygen Supplements Origination: April 10, 1992 Review Date: July 15, 2015 Next Review: July, 2017 DESCRIPTION OF PROCEDURE OR SERVICE USP Oxygen is a gaseous
Medicare C/D Medical Coverage Policy Oxygen and Oxygen Supplements Origination: April 10, 1992 Review Date: July 15, 2015 Next Review: July, 2017 DESCRIPTION OF PROCEDURE OR SERVICE USP Oxygen is a gaseous
The patient s response to therapy within the first hour in the Emergency Room is one of the most reliable ways to predict need for hospitalization.
 Emergency Room Asthma Management Algorithm The Emergency Room Asthma Management Algorithm is to be used for any patient seen in the Emergency Room with the diagnosis of asthma. (The initial history should
Emergency Room Asthma Management Algorithm The Emergency Room Asthma Management Algorithm is to be used for any patient seen in the Emergency Room with the diagnosis of asthma. (The initial history should
Perioperative Management of Patients with Obstructive Sleep Apnea. Kalpesh Ganatra,MD Diplomate, American Board of Sleep Medicine
 Perioperative Management of Patients with Obstructive Sleep Apnea Kalpesh Ganatra,MD Diplomate, American Board of Sleep Medicine Disclosures. This activity is supported by an education grant from Trivalley
Perioperative Management of Patients with Obstructive Sleep Apnea Kalpesh Ganatra,MD Diplomate, American Board of Sleep Medicine Disclosures. This activity is supported by an education grant from Trivalley
Original Article COPD and Hospital Stay Pak Armed Forces Med J 2014; 64 (1): 46-50. Ahmed Raza, Mahmood Iqbal Malik*, Yousaf Jamal**
: 46-50. Ahmed Raza, Mahmood Iqbal Malik*, Yousaf Jamal**") Original Article COPD and Hospital Stay Pak Armed Forces Med J 2014; 64 (1): 46-50 COMPARISON OF NIPPV WITH STANDARD TREATMENT IN PATIENTS WITH ACUTE EXACERBATIONS OF COPD IN TERMS OF IMPROVEMENT IN ABGS
Original Article COPD and Hospital Stay Pak Armed Forces Med J 2014; 64 (1): 46-50 COMPARISON OF NIPPV WITH STANDARD TREATMENT IN PATIENTS WITH ACUTE EXACERBATIONS OF COPD IN TERMS OF IMPROVEMENT IN ABGS
THE AIRWAY IN AEROMEDICAL EVACUATION. PBLD (Problem Based Learning Discussion)
") THE AIRWAY IN AEROMEDICAL EVACUATION PBLD (Problem Based Learning Discussion) D. John Doyle MD PhD 2012 Edition Image Credit: http://www.arabianaerospace.aero/media/images/stories/medevac%20services.jpg
THE AIRWAY IN AEROMEDICAL EVACUATION PBLD (Problem Based Learning Discussion) D. John Doyle MD PhD 2012 Edition Image Credit: http://www.arabianaerospace.aero/media/images/stories/medevac%20services.jpg
Vtial sign #1: PULSE. Vital Signs: Assessment and Interpretation. Factors that influence pulse rate: Importance of Vital Signs
 Vital Signs: Assessment and Interpretation Elma I. LeDoux, MD, FACP, FACC Associate Professor of Medicine Vtial sign #1: PULSE Reflects heart rate (resting 60-90/min) Should be strong and regular Use 2
Vital Signs: Assessment and Interpretation Elma I. LeDoux, MD, FACP, FACC Associate Professor of Medicine Vtial sign #1: PULSE Reflects heart rate (resting 60-90/min) Should be strong and regular Use 2
DRG 475 Respiratory System Diagnosis with Ventilator Support. ICD-9-CM Coding Guidelines
 DRG 475 Respiratory System Diagnosis with Ventilator Support ICD-9-CM Coding G The below listed g are not inclusive. The coder should refer to the applicable Coding Clinic g for additional information.
DRG 475 Respiratory System Diagnosis with Ventilator Support ICD-9-CM Coding G The below listed g are not inclusive. The coder should refer to the applicable Coding Clinic g for additional information.
Homeostasis. The body must maintain a delicate balance of acids and bases.
 Homeostasis The body must maintain a delicate balance of acids and bases. Metabolic and respiratory processes must work together to keep hydrogen ion (H+) levels normal and stable. ph of Blood The ph of
Homeostasis The body must maintain a delicate balance of acids and bases. Metabolic and respiratory processes must work together to keep hydrogen ion (H+) levels normal and stable. ph of Blood The ph of
Respiratory Care. A Life and Breath Career for You!
 Respiratory Care A Life and Breath Career for You! Respiratory Care Makes a Difference At 9:32 am, Lori Moreno brought a newborn baby struggling to breathe back to life What have you accomplished today?
Respiratory Care A Life and Breath Career for You! Respiratory Care Makes a Difference At 9:32 am, Lori Moreno brought a newborn baby struggling to breathe back to life What have you accomplished today?
A National Early Warning Score for the NHS
 A National Early Warning Score for the NHS Professor Gary B Smith FRCA FRCP Centre of Postgraduate Medical Research & Education, School of Health and Social Care, Bournemouth University - from local data
A National Early Warning Score for the NHS Professor Gary B Smith FRCA FRCP Centre of Postgraduate Medical Research & Education, School of Health and Social Care, Bournemouth University - from local data
Pediatric Airway Management
 Pediatric Airway Management Dec 2003 Dr. Shapiro I., PICU Adult Chain of Survival EMS CPR ALS Early Defibrillation Pediatric Chain of Survival Prevention CPR EMS ALS Out-of-Hospital Cardiac Arrest SIDS
Pediatric Airway Management Dec 2003 Dr. Shapiro I., PICU Adult Chain of Survival EMS CPR ALS Early Defibrillation Pediatric Chain of Survival Prevention CPR EMS ALS Out-of-Hospital Cardiac Arrest SIDS
Irish Association for Emergency Medicine (IAEM) submission to the National COPD Strategy
 submission to the National COPD Strategy") 31 st Irish Association for Emergency Medicine (IAEM) submission to the National COPD Strategy 1 Introduction Chronic obstructive pulmonary disease (COPD) is an important disease for patients, the health
31 st Irish Association for Emergency Medicine (IAEM) submission to the National COPD Strategy 1 Introduction Chronic obstructive pulmonary disease (COPD) is an important disease for patients, the health
OXYGEN AND ASSISTED VENTILATION FOR COPD
 OXYGEN AND ASSISTED VENTILATION FOR COPD INTERNATIONAL COPD COALITION PHYSICIANS POCKET GUIDE 2011 Aim of this Guide COPD is the fourth leading cause of death in the world, and its prevalence and health
OXYGEN AND ASSISTED VENTILATION FOR COPD INTERNATIONAL COPD COALITION PHYSICIANS POCKET GUIDE 2011 Aim of this Guide COPD is the fourth leading cause of death in the world, and its prevalence and health
IMPAIRED BLOOD-GAS EXCHANGE. Intraoperative blood gas analysis
 IMPAIRED BLOOD-GAS EXCHANGE Intraoperative blood gas analysis When do you perform BGA Intraoperatively? Informe actual NEVER Routine:Thoracic Thoracic, Cardiac,Neurosurgery Emergency situation Drop in
IMPAIRED BLOOD-GAS EXCHANGE Intraoperative blood gas analysis When do you perform BGA Intraoperatively? Informe actual NEVER Routine:Thoracic Thoracic, Cardiac,Neurosurgery Emergency situation Drop in
Surgery in Individuals Age 65+ Possible Risks. Possible Benefits. Potential Causes of POCD 11/24/2014. What is POCD?
 Surgery in Individuals Age 65+ Postoperative Cognitive Dysfunction in Older Adults Ryan W. Schroeder, Psy.D., LP, ABPP-CN Neuropsychologist & Assistant Professor University of Kansas School of Medicine
Surgery in Individuals Age 65+ Postoperative Cognitive Dysfunction in Older Adults Ryan W. Schroeder, Psy.D., LP, ABPP-CN Neuropsychologist & Assistant Professor University of Kansas School of Medicine
NURSING SERVICES DEPARTMENT
 NURSING SERVICES DEPARTMENT TITLE: Mechanical Ventilation PATIENT CARE PLAN DIAGNOSIS: DISCHARGE CRITERIA: 1 The patient will: Maintain adequate mechanics of PERTINENT INFORMATION:. ventilation as demonstrated
NURSING SERVICES DEPARTMENT TITLE: Mechanical Ventilation PATIENT CARE PLAN DIAGNOSIS: DISCHARGE CRITERIA: 1 The patient will: Maintain adequate mechanics of PERTINENT INFORMATION:. ventilation as demonstrated
240- PROBLEM SET INSERTION OF SWAN-GANZ SYSTEMIC VASCULAR RESISTANCE. Blood pressure = f(cardiac output and peripheral resistance)
") 240- PROBLEM SET INSERTION OF SWAN-GANZ 50 kg Pig Rt Jugular 0 cm Rt Atrium 10 cm Rt ventricle 15 cm Wedge 20-25 cm SYSTEMIC VASCULAR RESISTANCE Blood pressure = f(cardiac output and peripheral resistance)
240- PROBLEM SET INSERTION OF SWAN-GANZ 50 kg Pig Rt Jugular 0 cm Rt Atrium 10 cm Rt ventricle 15 cm Wedge 20-25 cm SYSTEMIC VASCULAR RESISTANCE Blood pressure = f(cardiac output and peripheral resistance)
First Responder (FR) and Emergency Medical Responder (EMR) Progress Log
 and Emergency Medical Responder (EMR) Progress Log") First Responder (FR) and Emergency Medical Responder (EMR) Progress Log Note: Those competencies that are for EMR only are denoted by boldface type. For further details on the National Occupational Competencies
First Responder (FR) and Emergency Medical Responder (EMR) Progress Log Note: Those competencies that are for EMR only are denoted by boldface type. For further details on the National Occupational Competencies
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) S. Agarwal, MD, S. Kache MD
 S. Agarwal, MD, S. Kache MD") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) S. Agarwal, MD, S. Kache MD Definition ARDS is a clinical syndrome of lung injury with hypoxic respiratory failure caused by intense pulmonary inflammation that
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) S. Agarwal, MD, S. Kache MD Definition ARDS is a clinical syndrome of lung injury with hypoxic respiratory failure caused by intense pulmonary inflammation that
Using home NIV for the management of hypercapnic COPD
 Home NIV Program for COPD Using home NIV for the management of hypercapnic COPD This program offers COPD treatment guidelines to physicians to help appropriately target and qualify patients for noninvasive
Home NIV Program for COPD Using home NIV for the management of hypercapnic COPD This program offers COPD treatment guidelines to physicians to help appropriately target and qualify patients for noninvasive
Why and how to have end-of-life discussions with your patients:
 Why and how to have end-of-life discussions with your patients: A guide with a suggested script and some basic questions to use The medical literature consistently shows that physicians can enhance end-of-life
Why and how to have end-of-life discussions with your patients: A guide with a suggested script and some basic questions to use The medical literature consistently shows that physicians can enhance end-of-life
CH CONSCIOUS SEDATION
 Summary: CH CONSCIOUS SEDATION It is the policy of Carondelet Health that moderate conscious sedation of patients will be undertaken with appropriate evaluation and monitoring. Effective Date: 9/4/04 Revision
Summary: CH CONSCIOUS SEDATION It is the policy of Carondelet Health that moderate conscious sedation of patients will be undertaken with appropriate evaluation and monitoring. Effective Date: 9/4/04 Revision
Hypoxia and Oxygenation Hypoxia is a serious threat to patients and escorts alike when
 Chapter 4 2 71 Hypoxia and Oxygenation Hypoxia is a serious threat to patients and escorts alike when they fly. Air medical escorts need to understand what causes hypoxia, why some people are more likely
Chapter 4 2 71 Hypoxia and Oxygenation Hypoxia is a serious threat to patients and escorts alike when they fly. Air medical escorts need to understand what causes hypoxia, why some people are more likely
Update on Small Animal Cardiopulmonary Resuscitation (CPR)- is anything new?
- is anything new?") Update on Small Animal Cardiopulmonary Resuscitation (CPR)- is anything new? DVM, DACVA Objective: Update on the new Small animal guidelines for CPR and a discussion of the 2012 Reassessment Campaign on
Update on Small Animal Cardiopulmonary Resuscitation (CPR)- is anything new? DVM, DACVA Objective: Update on the new Small animal guidelines for CPR and a discussion of the 2012 Reassessment Campaign on
Clinical Indications for Hyperbaric Oxygen Therapy in 2011 Part 1
 Clinical Indications for Hyperbaric Oxygen Therapy in 2011 Part 1 Med LtCol Peter GERMONPRE Centre for Hyperbaric Oxygen Therapy Military Hospital Brussels What is HBO therapy? Breathing oxygen under pressure
Clinical Indications for Hyperbaric Oxygen Therapy in 2011 Part 1 Med LtCol Peter GERMONPRE Centre for Hyperbaric Oxygen Therapy Military Hospital Brussels What is HBO therapy? Breathing oxygen under pressure
Community health care services Alternatives to acute admission & Facilitated discharge options. Directory
 Community health care services Alternatives to acute admission & Facilitated discharge options Directory Introduction The purpose of this directory is to provide primary and secondary health and social
Community health care services Alternatives to acute admission & Facilitated discharge options Directory Introduction The purpose of this directory is to provide primary and secondary health and social
OXYGEN THERAPY AND SATURATION MONITORING OF THE NEONATE - CLINICAL GUIDELINE
 OYGEN THERAPY AND SATURATION MONITORING OF THE NEONATE - CLINICAL GUIDELINE 1. Aim/Purpose of this Guideline 1.1 To provide guidance on the assessment and management of infants requiring oxygen therapy
OYGEN THERAPY AND SATURATION MONITORING OF THE NEONATE - CLINICAL GUIDELINE 1. Aim/Purpose of this Guideline 1.1 To provide guidance on the assessment and management of infants requiring oxygen therapy
Department of Surgery
 What is emphysema? 2004 Regents of the University of Michigan Emphysema is a chronic disease of the lungs characterized by thinning and overexpansion of the lung-like blisters (bullae) in the lung tissue.
What is emphysema? 2004 Regents of the University of Michigan Emphysema is a chronic disease of the lungs characterized by thinning and overexpansion of the lung-like blisters (bullae) in the lung tissue.
Catheter insertion of a new aortic valve to treat aortic stenosis
 Issue date March 2012 Understanding NICE guidance Information for people who use NHS services NICE interventional procedures guidance advises the NHS on when and how new procedures can be used in clinical
Issue date March 2012 Understanding NICE guidance Information for people who use NHS services NICE interventional procedures guidance advises the NHS on when and how new procedures can be used in clinical
Introduction to Cardiopulmonary Exercise Testing
 Introduction to Cardiopulmonary Exercise Testing 2 nd Edition Andrew M. Luks, MD Robb Glenny, MD H. Thomas Robertson, MD Division of Pulmonary and Critical Care Medicine University of Washington Section
Introduction to Cardiopulmonary Exercise Testing 2 nd Edition Andrew M. Luks, MD Robb Glenny, MD H. Thomas Robertson, MD Division of Pulmonary and Critical Care Medicine University of Washington Section
Marilyn Borkgren-Okonek, APN, CCNS, RN, MS Suburban Lung Associates, S.C. Elk Grove Village, IL
 Marilyn Borkgren-Okonek, APN, CCNS, RN, MS Suburban Lung Associates, S.C. Elk Grove Village, IL www.goldcopd.com GLOBAL INITIATIVE FOR CHRONIC OBSTRUCTIVE LUNG DISEASE GLOBAL STRATEGY FOR DIAGNOSIS, MANAGEMENT
Marilyn Borkgren-Okonek, APN, CCNS, RN, MS Suburban Lung Associates, S.C. Elk Grove Village, IL www.goldcopd.com GLOBAL INITIATIVE FOR CHRONIC OBSTRUCTIVE LUNG DISEASE GLOBAL STRATEGY FOR DIAGNOSIS, MANAGEMENT
Limited Pay Policy (L-222B) - Underwriting Guidelines
 - Underwriting Guidelines") Limited Pay Policy (L-222B) - Underwriting Guidelines 1 Addiction/Abuser Drug - Past or Present Presently Recovered - AA for last 2 years 2 Aids 3 Alcoholic Presently Recovered - AA for last 2 years 4
Limited Pay Policy (L-222B) - Underwriting Guidelines 1 Addiction/Abuser Drug - Past or Present Presently Recovered - AA for last 2 years 2 Aids 3 Alcoholic Presently Recovered - AA for last 2 years 4
CLINICAL USE OF PULSE OXIMETRY
 CLINICAL USE OF PULSE OXIMETRY POCKET REFERENCE 2010 INTERNATIONAL Helping the World Breathe Free TM GLOBAL PRIMARY CARE AND PATIENT EDUCATION THE PURPOSE OF THIS GUIDE Chronic respiratory diseases such
CLINICAL USE OF PULSE OXIMETRY POCKET REFERENCE 2010 INTERNATIONAL Helping the World Breathe Free TM GLOBAL PRIMARY CARE AND PATIENT EDUCATION THE PURPOSE OF THIS GUIDE Chronic respiratory diseases such
Abdominal Aortic Aneurysm (AAA) General Information. Patient information Leaflet
 General Information. Patient information Leaflet") Abdominal Aortic Aneurysm (AAA) General Information Patient information Leaflet 1 st July 2016 WHAT IS THE AORTA? The aorta is the largest artery (blood vessel) in the body. It carries blood from the heart
Abdominal Aortic Aneurysm (AAA) General Information Patient information Leaflet 1 st July 2016 WHAT IS THE AORTA? The aorta is the largest artery (blood vessel) in the body. It carries blood from the heart
Corporate Medical Policy
 File Name: anesthesia_services Origination: 8/2007 Last CAP Review: 1/2016 Next CAP Review: 1/2017 Last Review: 1/2016 Corporate Medical Policy Description of Procedure or Service There are three main
File Name: anesthesia_services Origination: 8/2007 Last CAP Review: 1/2016 Next CAP Review: 1/2017 Last Review: 1/2016 Corporate Medical Policy Description of Procedure or Service There are three main
Using a Reservoir Nasal Cannula in Acute Care
 Using a Reservoir Nasal Cannula in Acute Care Cheryl Plate Dumont, RN, MSN, CCRN Brian L. Tiep, MD Oxymizer and Oxym i z e r Pendant (CHAD Therapeutics Inc, Chatsworth, Calif) brand reservoir cannulas
Using a Reservoir Nasal Cannula in Acute Care Cheryl Plate Dumont, RN, MSN, CCRN Brian L. Tiep, MD Oxymizer and Oxym i z e r Pendant (CHAD Therapeutics Inc, Chatsworth, Calif) brand reservoir cannulas
Guideline for the use of Non-Invasive Ventilation (NIV) TCP 180
 TCP 180") Guideline for the use of Non-Invasive Ventilation (NIV) CROSS REFERENCE Progress/date of approval This Strategy/ Policy should be read in conjunction with: Mental Capacity Act Policy -TCP 199 June 2009
Guideline for the use of Non-Invasive Ventilation (NIV) CROSS REFERENCE Progress/date of approval This Strategy/ Policy should be read in conjunction with: Mental Capacity Act Policy -TCP 199 June 2009
Training Manual for The National Early Warning Score and associated Education Programme
 Training Manual for The National Early Warning Score and associated Education Programme The National Early Warning Score Project and associated Education Programme is a work stream of the Acute Medicine
Training Manual for The National Early Warning Score and associated Education Programme The National Early Warning Score Project and associated Education Programme is a work stream of the Acute Medicine
RES Non-Invasive Positive Pressure Ventilation Guideline Page 1 of 9
 Page 1 of 9 Scope: Respiratory Care Department, Physicians, Advanced Nurse Practitioners (APRN), Physician Assistants (PA) Population: Patients receiving rescue or non-rescue non-invasive positive pressure
Page 1 of 9 Scope: Respiratory Care Department, Physicians, Advanced Nurse Practitioners (APRN), Physician Assistants (PA) Population: Patients receiving rescue or non-rescue non-invasive positive pressure
The largest clinical study of Bayer's Xarelto (rivaroxaban) Wednesday, 14 November 2012 07:38
 Wednesday, 14 November 2012 07:38") Bayer HealthCare has announced the initiation of the COMPASS study, the largest clinical study of its oral anticoagulant Xarelto (rivaroxaban) to date, investigating the prevention of major adverse cardiac
Bayer HealthCare has announced the initiation of the COMPASS study, the largest clinical study of its oral anticoagulant Xarelto (rivaroxaban) to date, investigating the prevention of major adverse cardiac
Omega-3 fatty acids improve the diagnosis-related clinical outcome. Critical Care Medicine April 2006;34(4):972-9
:972-9") Omega-3 fatty acids improve the diagnosis-related clinical outcome 1 Critical Care Medicine April 2006;34(4):972-9 Volume 34(4), April 2006, pp 972-979 Heller, Axel R. MD, PhD; Rössler, Susann; Litz, Rainer
Omega-3 fatty acids improve the diagnosis-related clinical outcome 1 Critical Care Medicine April 2006;34(4):972-9 Volume 34(4), April 2006, pp 972-979 Heller, Axel R. MD, PhD; Rössler, Susann; Litz, Rainer
Level 1 Tower C Global Business Park MG Road Gurgaon,122 002 India T+91 124 406 2500 F+91 124 406 8536 goindigo.in
 APPLICATION FOR CARRIAGE OF MEDICAL PASSENGERS Detailed Medical Certificate must accompany this completed form. Medical Passenger Completed Application to be forwarded to the Medical Department DEL for
APPLICATION FOR CARRIAGE OF MEDICAL PASSENGERS Detailed Medical Certificate must accompany this completed form. Medical Passenger Completed Application to be forwarded to the Medical Department DEL for
Team Leader. Ensures high-quality CPR at all times Assigns team member roles Ensures that team members perform well. Bradycardia Management
 ACLS Megacode Case 1: Sinus Bradycardia (Bradycardia VF/Pulseless VT Asystole Out-of-Hospital Scenario You are a paramedic and arrive on the scene to find a 57-year-old woman complaining of indigestion.
ACLS Megacode Case 1: Sinus Bradycardia (Bradycardia VF/Pulseless VT Asystole Out-of-Hospital Scenario You are a paramedic and arrive on the scene to find a 57-year-old woman complaining of indigestion.
Non-invasive ventilation in acute respiratory failure
 192 BTS GUIDELINE Non-invasive ventilation in acute respiratory failure British Thoracic Society Standards of Care Committee... Thorax 2002;57:192 211 Members of BTS Standards of Care Committee: S Baudouin,
192 BTS GUIDELINE Non-invasive ventilation in acute respiratory failure British Thoracic Society Standards of Care Committee... Thorax 2002;57:192 211 Members of BTS Standards of Care Committee: S Baudouin,
ETCO2 Monitoring: Riding the Wave! Disclosure 4/11/2013
 ETCO2 Monitoring: Riding the Wave! Debbie Fox, MBA, RRT-NPS, FAARC Director, Respiratory Care Wesley Medical Center Disclosure I have no financial conflicts to disclose. I have participated in focus groups
ETCO2 Monitoring: Riding the Wave! Debbie Fox, MBA, RRT-NPS, FAARC Director, Respiratory Care Wesley Medical Center Disclosure I have no financial conflicts to disclose. I have participated in focus groups
CENTER FOR DRUG EVALUATION AND RESEARCH
 CENTER FOR DRUG EVALUATION AND RESEARCH APPLICATION NUMBER: 205029Orig1s000 SUMMARY REVIEW Cross Discipline Team Leader Review 4. Nonclinical Pharmacology/Toxicology In their review of the original application,
CENTER FOR DRUG EVALUATION AND RESEARCH APPLICATION NUMBER: 205029Orig1s000 SUMMARY REVIEW Cross Discipline Team Leader Review 4. Nonclinical Pharmacology/Toxicology In their review of the original application,
Non-Invasive Positive Pressure Ventilation in Heart Failure Patients: For Who, Wy & When?
 REUNIÃO CONJUNTA DOS GRUPOS DE ESTUDO DE CUIDADOS INTENSIVOS CARDÍACOS E DE FISIOPATOLOGIA DO ESFORÇO E REABILITAÇÃO CARDÍACA O L H Ã O 2 7 e 2 8 d e J a n e i r o 2 0 1 2 Non-Invasive Positive Pressure
REUNIÃO CONJUNTA DOS GRUPOS DE ESTUDO DE CUIDADOS INTENSIVOS CARDÍACOS E DE FISIOPATOLOGIA DO ESFORÇO E REABILITAÇÃO CARDÍACA O L H Ã O 2 7 e 2 8 d e J a n e i r o 2 0 1 2 Non-Invasive Positive Pressure
Medical Direction and Practices Board WHITE PAPER
 Medical Direction and Practices Board WHITE PAPER Use of Pressors in Pre-Hospital Medicine: Proper Indication and State of the Science Regarding Proper Choice of Pressor BACKGROUND Shock is caused by a
Medical Direction and Practices Board WHITE PAPER Use of Pressors in Pre-Hospital Medicine: Proper Indication and State of the Science Regarding Proper Choice of Pressor BACKGROUND Shock is caused by a
ACLS PHARMACOLOGY 2011 Guidelines
 ACLS PHARMACOLOGY 2011 Guidelines ADENOSINE Narrow complex tachycardias or wide complex tachycardias that may be supraventricular in nature. It is effective in treating 90% of the reentry arrhythmias.
ACLS PHARMACOLOGY 2011 Guidelines ADENOSINE Narrow complex tachycardias or wide complex tachycardias that may be supraventricular in nature. It is effective in treating 90% of the reentry arrhythmias.
Hyperbaric Oxygen Therapy WWW.RN.ORG
 Hyperbaric Oxygen Therapy WWW.RN.ORG Reviewed September, 2015, Expires September, 2017 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2015 RN.ORG, S.A.,
Hyperbaric Oxygen Therapy WWW.RN.ORG Reviewed September, 2015, Expires September, 2017 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2015 RN.ORG, S.A.,
Ischemia and Infarction
 Harvard-MIT Division of Health Sciences and Technology HST.035: Principle and Practice of Human Pathology Dr. Badizadegan Ischemia and Infarction HST.035 Spring 2003 In the US: ~50% of deaths are due to
Harvard-MIT Division of Health Sciences and Technology HST.035: Principle and Practice of Human Pathology Dr. Badizadegan Ischemia and Infarction HST.035 Spring 2003 In the US: ~50% of deaths are due to
Domiciliary oxygen therapy services
 Domiciliary oxygen therapy services CLINICAL GUIDELINES AND ADVICE FOR PRESCRIBERS A report of the Royal College of Physicians Commissioned by the Department of Health Acknowledgements We are grateful
Domiciliary oxygen therapy services CLINICAL GUIDELINES AND ADVICE FOR PRESCRIBERS A report of the Royal College of Physicians Commissioned by the Department of Health Acknowledgements We are grateful