PROCEDURES FOR COMPLETION OF WORK COMP CLAIMS PAPERWORK
|
|
|
- Rosalind Gray
- 8 years ago
- Views:
Transcription
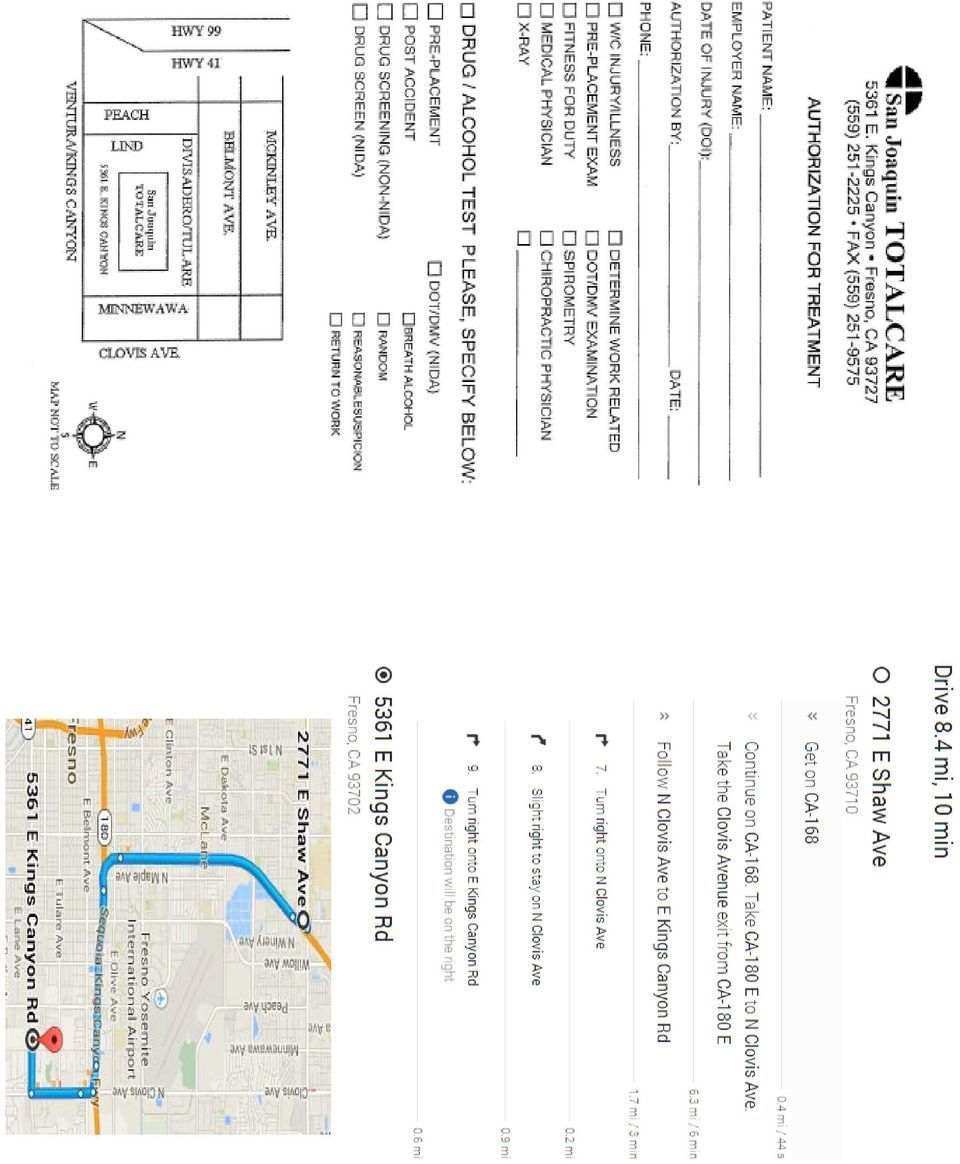
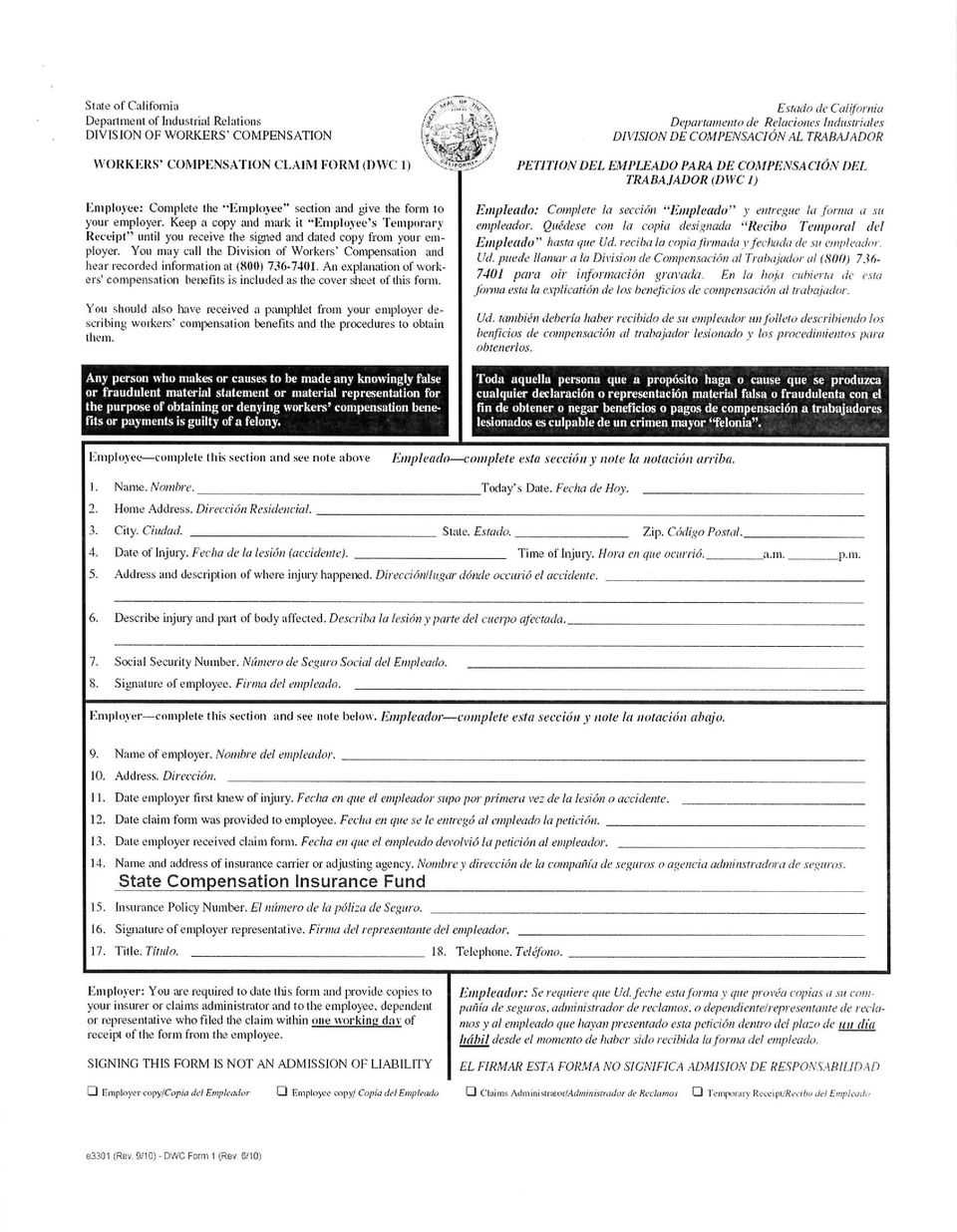
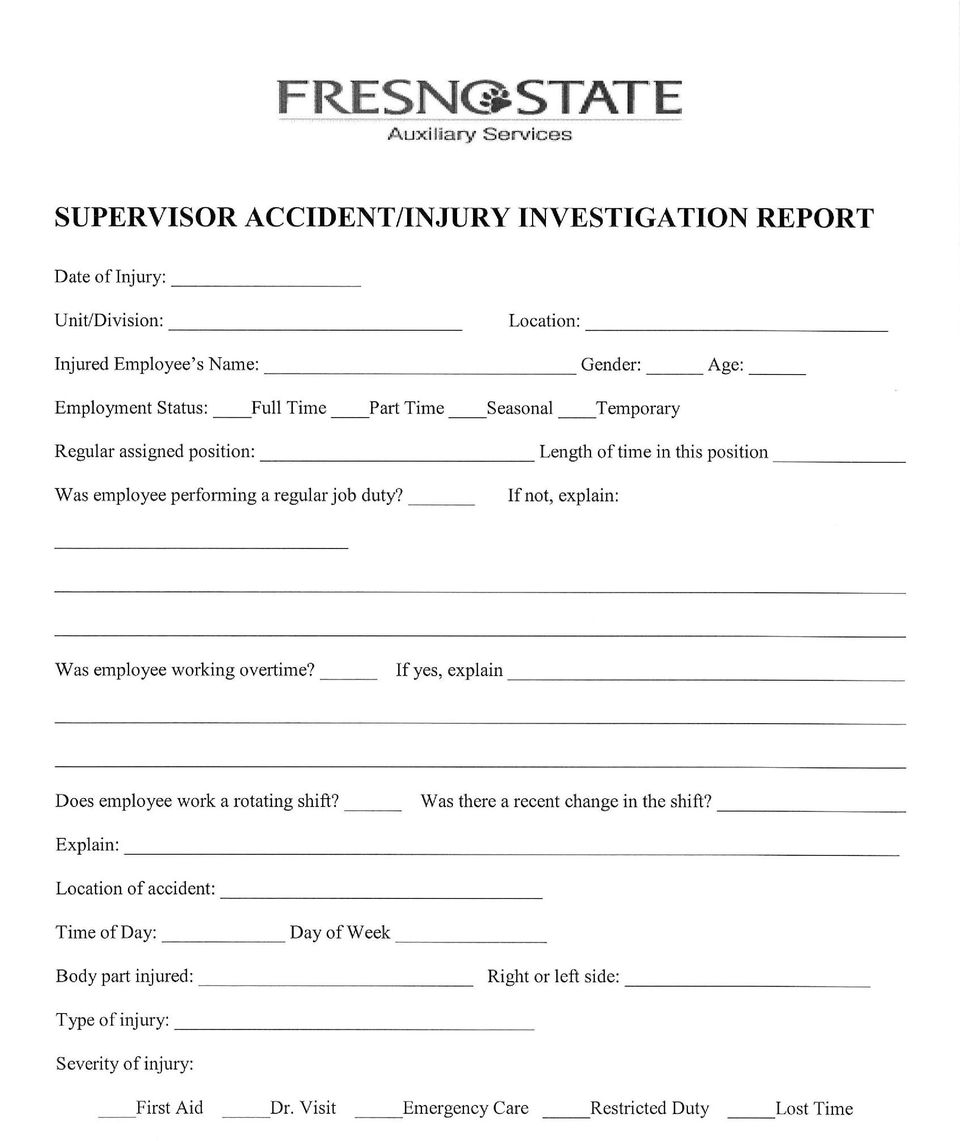
1 PROCEDURES FOR COMPLETION OF WORK COMP CLAIMS PAPERWORK Please complete the attached packet in the following manner. Forms must be completed within 24 hours of reporting the injury/illness to supervisor. Notify Human Resources at (559) if paperwork cannot be completed in a timely manner. Waiving Medical Treatment If the employee refuses medical treatment, the Workers Comp Refusal of Treatment and The Supervisor Accident/Injury Investigation Report forms must be completed. Return these forms to Human Resources. Seeking Medical Treatment The Policy on Absences is given to the employee for work-related injury/illness. The Authorization for Treatment form is used for referral to San Joaquin Total Care, our work comp doctors in Fresno. You can also use the form for referral to Clovis Community Hospital Emergency Room, or St. Agnes Hospital Emergency Room. You may complete and indicate the employer is California State University, Fresno (Foundation, Association, Ag Fdn, or Programs for Children). Give this form to the employee if referring to doctor. Form 5020 must be completed by the supervisor. Please be sure to pay special attention to the section describing the injury or illness. Return this form to Human Resources. Form DWC 1 must be completed by the Employee and Supervisor (employer). Employee must complete the top section, and supervisor completes the bottom section. Please give a copy to the employee. Return the original copy to Human Resources. The New Claim Injury Form must be signed by the Employee. Return this form to Human Resources. The Supervisor Accident/Injury Investigation Report must be completed by the supervisor. Please be as specific as possible, indicating names of witnesses and causes of injury/illness. Return this form to Human Resources. The Worker s Compensation Claim Declaration in Compliance with Labor Code Section 4906(g) must be signed by the Employee. Return this form to Human Resources. Our work comp carrier is: State Compensation Insurance Fund P. O. Box 4000 Fresno, CA Phone: (559) Fax: (559) Please call Human Resources at if you have questions regarding these forms. Revised: 07/2012

2 Work Related Injury Contact Sheet Type of Injury Who to Contact Contact Information All Injuries: Auxiliary Human Resources Amanda Chamberlain (559) For an injury that requires immediate medical attention: For medical treatment: San Joaquin Total Care (559) E. Kings Canyon Fresno, CA Weekend and After hours medical treatment: St. Agnes Medical Center (559) E. Spruce Ave. Fresno, Ca Auxiliary Employees consist of the following corporations: California State University, Fresno Association, Inc. California State University, Fresno Foundation Agricultural Foundation of California State University, Fresno Fresno State Programs for Children, Inc. Associated Students, Inc.

3 The Agricultural Foundation of California State University, Fresno policy with regard to absences for work-related injury/illness is as follows: Employee will be paid for the full shift on the date of injury. Benefited employees will be charged sick leave for doctor visits, physical therapy appointments, lab work and tests for work-related injury/illness, etc. These absences should be designated with a C on attendance reports. Non-benefited employees should attempt to schedule doctor visits, physical therapy appointments, etc., outside of normally scheduled work hours. If employee has been released to modified or regular work and is unable to perform work duties, Human Resources should be notified immediately. Auxiliary Human Resources Office: Telephone

4
5

6

7

8
9 EMPLOYEE NAME (Nombré): DATE OF INJURY (Fecha en que se Lastimó): NEW CLAIM INJURY FORM DESCRIBE HOW THE INJURY OR ILLNESS OCCURRED (Cómo pasó la lesíon o enfermedad): PLEASE MARK THE BODY PART INJURED (Por favor marque la parte del cuerpo lesionada): = No pain (Ningún dolor) 10= Greatest pain (Dolor más fuerte) Please circle the number between 0 and 10 that best describes your pain. (Por favor circule el número entre el 0 y 10 que mejor describe su dolor). DISCLAIMER Any person who makes or causes to be made any false or fraudulent material statement, or material representation for the purpose of obtaining or denying workers compensation benefits or payment s is guilty of a felony. (Cualquier persona que haga o cause que se produzca cualquier declaración falsa o fraudulenta, o representación material con el propósito de obtener o negar beneficios de compensación al trabajador o el pago, es culpable de un delito grave.) SIGNATURE OF EMPLOYEE (FIRMA DEL EMPLEADO) DATE (FECHA)

10
11

12

13 (Association, Foundation, Agricultural Foundation, Associated Students, Programs for Children) Worker s Compensation Claim Declaration in Compliance With Labor Code Section 4906(g) Policy # It is declared by the undersigned, under penalty of perjury under the laws of the State of California, that I/we have not violated Labor Code Section (prohibited physician referrals) and that I/we have not offered, delivered, received, or accepted any unlawful rebate, refund, commission, preference, patronage dividend, discount, or other consideration, whether in the form of money or otherwise, as compensation or inducement for any referred examination or evaluation. Employee Signature Employer Signature Insurer Signature Attorney Signature Date Date Date Date

14 WORKERS COMP REFUSAL OF TREATMENT DATE: EMPLOYEE: TYPE OF INJURY: As of the above noted date, I am notifying California State University, Fresno Auxiliary Corporations of an injury that occurred on. This injury was; was not initially reported by me to my supervisor on. At this time I have been requested by a representative of California State University, Fresno Auxiliary Corporations to be medically evaluated by San Joaquin TOTALCARE. However, I decline to be medically evaluated for the above noted condition. I understand that by signing this document any future claims regarding this injury will require a medical evaluation by the Auxiliary health care provider listed below. I also understand that should I decide to seek medical treatment for this injury, I must immediately notify my supervisor and go the below listed provider: PROVIDER: San Joaquin TOTALCARE ADDRESS: 5361 E. Kings Canyon Fresno, CA PHONE: (559) I, have; have not, sought medical treatment for this injury from: TREATING PHYSICIAN S NAME/ADDRESS (including City and State) STATEMENT: I have read and agree that the above information is factual and true. Employee Signature Date Supervisor Signature Date

CLIENT INFORMATION SHEET CITY: STATE: ZIP: DOB: SEX: E-MAIL ADDRESS: EMPLOYER: PHONE ADDRESS: FELONY CONVICTIONS?
 CLIENT INFORMATION SHEET DATE: NAME: REFERRED BY: ADDRESS: CITY: STATE: ZIP: PHONE: (H) (EMERG) (CELL) DOB: SEX: E-MAIL ADDRESS: SS#: SPOUSE EMPLOYER: PHONE ADDRESS: OCCUPATION: WEEKLY EARNINGS: FELONY
CLIENT INFORMATION SHEET DATE: NAME: REFERRED BY: ADDRESS: CITY: STATE: ZIP: PHONE: (H) (EMERG) (CELL) DOB: SEX: E-MAIL ADDRESS: SS#: SPOUSE EMPLOYER: PHONE ADDRESS: OCCUPATION: WEEKLY EARNINGS: FELONY
NSU Employee Manual. Workers Compensation System Guide
 Workers Compensation System Guide 1 NSU Employee Manual For more information regarding prevention of risk visit our website at http://www.nova.edu/cwis/fop/risk/ Table of Contents Florida Guidelines -
Workers Compensation System Guide 1 NSU Employee Manual For more information regarding prevention of risk visit our website at http://www.nova.edu/cwis/fop/risk/ Table of Contents Florida Guidelines -
AIG Primary Medical Provider Network Implementation Notice. Aviso de Implementación de la Red Primaria de Proveedores Médicos de AIG
 AIG Primary Medical Provider Network Implementation Notice Unless you pre-designate a physician or medical group, a new work injury arising on or after 10/8/10_ will be treated by providers in the AIG
AIG Primary Medical Provider Network Implementation Notice Unless you pre-designate a physician or medical group, a new work injury arising on or after 10/8/10_ will be treated by providers in the AIG
Group Claim Fraud Statements
 Group Claim Fraud Statements A Mutual of Omaha Company The following fraud language is attached to, and made part of this claim form. Please read and do not remove these pages from this claim form. **
Group Claim Fraud Statements A Mutual of Omaha Company The following fraud language is attached to, and made part of this claim form. Please read and do not remove these pages from this claim form. **
For Employees: Employees: What What to to do do when when an an accident occurs 08/19/14/dmv
 For Employees: What to do when an accident occurs 08/19/14/dmv When there is a work-related accident or illness, procedures must be taken to ensure the employees needs are met with respect to treatment
For Employees: What to do when an accident occurs 08/19/14/dmv When there is a work-related accident or illness, procedures must be taken to ensure the employees needs are met with respect to treatment
Acalanes Union HSD Board Policy Work-Related Injuries
 Board Policy BP 4157.1 District employees shall be insured for on-the-job specific or cumulative injuries in accordance with law. In order to reduce costs and facilitate employee recovery, the Governing
Board Policy BP 4157.1 District employees shall be insured for on-the-job specific or cumulative injuries in accordance with law. In order to reduce costs and facilitate employee recovery, the Governing
STATE FUND LOCATIONS CUSTOMER SERVICE CENTER. BAKERSFIELD Policy (661) 664-4000 Claims (661) 664-4000
 664-4000 Claims (661) 664-4000") California State Employees Assn. STATE FUND LOCATIONS BAKERSFIELD Policy (661) 664-4000 Claims (661) 664-4000 EUREKA Policy (707) 443-9721 Claims (707) 443-9721 FRESNO Policy (559) 433-2600 Claims (559)
California State Employees Assn. STATE FUND LOCATIONS BAKERSFIELD Policy (661) 664-4000 Claims (661) 664-4000 EUREKA Policy (707) 443-9721 Claims (707) 443-9721 FRESNO Policy (559) 433-2600 Claims (559)
Worker s Compensation. What to do when an employee is injured at work.
 Worker s Compensation What to do when an employee is injured at work. OCM BOCES is subject to New York State Worker s Compensation Law If an injury requires treatment by a medical provider, The BOCES must
Worker s Compensation What to do when an employee is injured at work. OCM BOCES is subject to New York State Worker s Compensation Law If an injury requires treatment by a medical provider, The BOCES must
Employee Injury/Illness Reporting and Managed Return to Work. April 15, 2011 HR 23. Human Resources Responsible Key Business
 Managed Return to Work Date Effective April 15, 2011 City Manager Revision Date Effective Code Number HR 23 Human Resources Responsible Key Business Objective: The City of Charlotte seeks to ensure the
Managed Return to Work Date Effective April 15, 2011 City Manager Revision Date Effective Code Number HR 23 Human Resources Responsible Key Business Objective: The City of Charlotte seeks to ensure the
Your Workers Compensation Benefits
 Your Workers Compensation Benefits CALIFORNIA This form should be given to all newly hired employees in the State of California. Its content applies to industrial injuries on or after January 1, 2013.
Your Workers Compensation Benefits CALIFORNIA This form should be given to all newly hired employees in the State of California. Its content applies to industrial injuries on or after January 1, 2013.
Work Injury Reporting Hotline 877 682-7778
 FACTS ABOUT WORKERS COMPENSATION The content of this pamphlet has been approved by the Administrative Director of the Division of Workers Compensation. The information in this pamphlet is available in
FACTS ABOUT WORKERS COMPENSATION The content of this pamphlet has been approved by the Administrative Director of the Division of Workers Compensation. The information in this pamphlet is available in
EMPLOYEE INJURY REPORTING PROCEDURE
 Updated 8/1/2014 TDY MEDICAL STAFFING, Inc. EMPLOYEE INJURY REPORTING PROCEDURE STEP 1: IS INJURY LIFE THREATENING/EMERGENCY? Call 911/go to ER if yes. STEP 2: CALL CLAIM INTO TDY 215-736-5147 STEP 3:
Updated 8/1/2014 TDY MEDICAL STAFFING, Inc. EMPLOYEE INJURY REPORTING PROCEDURE STEP 1: IS INJURY LIFE THREATENING/EMERGENCY? Call 911/go to ER if yes. STEP 2: CALL CLAIM INTO TDY 215-736-5147 STEP 3:
Workers Compensation Packet and Instructions Effective March 6, 2014 PINK PACKET
 Main Office: Phone (607)778-2402 Fax: (607)778-2918 Workers Compensation Packet and Instructions Effective March 6, 2014 PINK PACKET 1. Instructions to be read by employee (claimant) and supervisor and
Main Office: Phone (607)778-2402 Fax: (607)778-2918 Workers Compensation Packet and Instructions Effective March 6, 2014 PINK PACKET 1. Instructions to be read by employee (claimant) and supervisor and
The following State forms have been included in your claims kit packet:
 RE: Workers Compensation Claims Kit Dear Policyholder: Welcome to Tower Group Companies Workers Compensation Insurance Program. Although we hope that your company never experiences an injury to an employee,
RE: Workers Compensation Claims Kit Dear Policyholder: Welcome to Tower Group Companies Workers Compensation Insurance Program. Although we hope that your company never experiences an injury to an employee,
WORKER S COMPENSATION TREATMENT AUTHORIZATION FORM
 FLORIDA TECH EMPLOYEE ACCIDENT/ INJURY REPORT Contact Financial Affairs @ 674-7297 OR 8885 IMMEDIATELY regarding an Employee's Injury. Employee AND Supervisor must complete this report. EMPLOYEE INFORMATION
FLORIDA TECH EMPLOYEE ACCIDENT/ INJURY REPORT Contact Financial Affairs @ 674-7297 OR 8885 IMMEDIATELY regarding an Employee's Injury. Employee AND Supervisor must complete this report. EMPLOYEE INFORMATION
THE INJURED WORKER. The first step is to report the injury or illness to your employer.
 THE INJURED WORKER Who is entitled to workers compensation benefits? If you have an injury or illness caused by your job you may be entitle to workers compensation benefits, which are provided for you
THE INJURED WORKER Who is entitled to workers compensation benefits? If you have an injury or illness caused by your job you may be entitle to workers compensation benefits, which are provided for you
New Hire Submission and Return Receipt PLEASE SUBMIT FORMS TO: SERVICE@ADVANCEDPEO.COM OR FAX 1-866-611-9598
 1933 E EDGEWOOD DR SUITE 102 LAKELAND, FL 33803 1-877-518-2881 WWW.ADVANCEDPEO.COM New Hire Submission and Return Receipt PLEASE SUBMIT FORMS TO: SERVICE@ADVANCEDPEO.COM OR FAX 1-866-611-9598 Notice to
1933 E EDGEWOOD DR SUITE 102 LAKELAND, FL 33803 1-877-518-2881 WWW.ADVANCEDPEO.COM New Hire Submission and Return Receipt PLEASE SUBMIT FORMS TO: SERVICE@ADVANCEDPEO.COM OR FAX 1-866-611-9598 Notice to
The Worker s Compensation Process
 Workers Compensation Basics The Worker s Compensation Process Kenda Weigang MARCH 2015 What should be posted Workers Compensation ACT Notice to Employees Authorized Treating Physician (ATP) Notification
Workers Compensation Basics The Worker s Compensation Process Kenda Weigang MARCH 2015 What should be posted Workers Compensation ACT Notice to Employees Authorized Treating Physician (ATP) Notification
Modified Duty/Return to Work (RTW) Program
 Program") Modified Duty/Return to Work (RTW) Program Client Name: Effective Date: PROGRAM OUTLINE 1. Accident Reporting and Return to Work Process 2. Modified Duty/Return to Work (RTW) Program 3. Employee Responsibility
Modified Duty/Return to Work (RTW) Program Client Name: Effective Date: PROGRAM OUTLINE 1. Accident Reporting and Return to Work Process 2. Modified Duty/Return to Work (RTW) Program 3. Employee Responsibility
Monterey County Behavioral Health Policy and Procedure
 Monterey County Behavioral Health Policy and Procedure 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 Policy Number 144 Policy Title Disclosure of Unlicensed Status for License
Monterey County Behavioral Health Policy and Procedure 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 Policy Number 144 Policy Title Disclosure of Unlicensed Status for License
Middle Name: Suffix: Social Security No.: City: State: Zip Code: City: State: Zip Code: City: State: Zip Code:
 Please print clearly. Form may be returned for unanswered questions. 1. CLAIMANT Last Name: Middle Name: Suffix: Social Security No.: Patient No.: Birthdate: Gender: Male Female Height: Weight: Spouse/Domestic
Please print clearly. Form may be returned for unanswered questions. 1. CLAIMANT Last Name: Middle Name: Suffix: Social Security No.: Patient No.: Birthdate: Gender: Male Female Height: Weight: Spouse/Domestic
How To Get A Workers Compensation Check In The United States
 New Hire Notice -- Injuries Caused By Work What does workers compensation cover? You may be entitled to workers' compensation benefits if you are injured or become ill because of your job. Workers' compensation
New Hire Notice -- Injuries Caused By Work What does workers compensation cover? You may be entitled to workers' compensation benefits if you are injured or become ill because of your job. Workers' compensation
A Transitional Work Program benefits employees in several ways:
 Workmen s Compensation Policy Number: 7390 Effective Date: All employees of Snake River School District 52 are covered by Workmen's Compensation insurance for bodily injury, disease, or death caused by
Workmen s Compensation Policy Number: 7390 Effective Date: All employees of Snake River School District 52 are covered by Workmen's Compensation insurance for bodily injury, disease, or death caused by
Important Information about Medical Care if you have a Work-Related Injury or Illness
 Important Information about Medical Care if you have a Work-Related Injury or Illness Initial Written Employee Notification Re: Medical Provider Network (Title 8, California Code of Regulations, section
Important Information about Medical Care if you have a Work-Related Injury or Illness Initial Written Employee Notification Re: Medical Provider Network (Title 8, California Code of Regulations, section
WORKERS COMPENSATION HANDBOOK
 WORKERS COMPENSATION HANDBOOK WHAT IS WORKERS COMPENSATION? If you get hurt on the job, your employer is required by law to pay for workers compensation benefits. You could get hurt by: One event at work.
WORKERS COMPENSATION HANDBOOK WHAT IS WORKERS COMPENSATION? If you get hurt on the job, your employer is required by law to pay for workers compensation benefits. You could get hurt by: One event at work.
Workers Compensation Policy and Procedure
 EL PASO COUNTY DEPARTMENT OF HUMAN RESOURCES Workers Compensation Policy and Procedure Revised Date: March 21, 2016 I. Purpose The County of El Paso provides workers compensation benefits for incidental
EL PASO COUNTY DEPARTMENT OF HUMAN RESOURCES Workers Compensation Policy and Procedure Revised Date: March 21, 2016 I. Purpose The County of El Paso provides workers compensation benefits for incidental
ASU SUPERVISOR S ACCIDENT/ILLNESS INVESTIGATION FORM
 ASU SUPERVISOR S ACCIDENT/ILLNESS INVESTIGATION FORM Return to: ASU Office of Human Resources, Workers Comp Office, PO Box 32010, Human Resources Building, 330 University Hall Drive, Boone, NC 28608 This
ASU SUPERVISOR S ACCIDENT/ILLNESS INVESTIGATION FORM Return to: ASU Office of Human Resources, Workers Comp Office, PO Box 32010, Human Resources Building, 330 University Hall Drive, Boone, NC 28608 This
The following state forms have been included in your claims kit packet:
 RE: Workers Compensation Claims Kit Dear Policyholder: Welcome to Tower Group Companies Workers Compensation Insurance Program. Although we hope that your company never has to experience an injury to an
RE: Workers Compensation Claims Kit Dear Policyholder: Welcome to Tower Group Companies Workers Compensation Insurance Program. Although we hope that your company never has to experience an injury to an
workers compensation?
 This pamphlet may be given to all newly hired employees in the State of California. Employers and claims administrators may use the content of this document and put their logos and additional information
This pamphlet may be given to all newly hired employees in the State of California. Employers and claims administrators may use the content of this document and put their logos and additional information
Benedictine College Financial Aid
 2015 2016 Institutional Verification Document V4 Dependent Your 2015 2016 Free Application for Federal Student Aid (FAFSA) was selected for review in a process called verification. The law says that before
2015 2016 Institutional Verification Document V4 Dependent Your 2015 2016 Free Application for Federal Student Aid (FAFSA) was selected for review in a process called verification. The law says that before
Make Your Return-to-Work Process Fit Your Company
 1 Make Your Return-to-Work Process Fit Your Company At Texas Mutual Insurance Company, we work hard to help employers maintain a safe work place, but we know that no business is immune to on-the-job injuries.
1 Make Your Return-to-Work Process Fit Your Company At Texas Mutual Insurance Company, we work hard to help employers maintain a safe work place, but we know that no business is immune to on-the-job injuries.
Information for the New Claimant WORKER S COMPENSATION
 Information for the New Claimant WORKER S COMPENSATION Published by: Worker s Compensation and Human Resources University of Wisconsin Milwaukee P.O.BOX 413 Milwaukee, WI 53144-0413 Daim ntawv no muaj
Information for the New Claimant WORKER S COMPENSATION Published by: Worker s Compensation and Human Resources University of Wisconsin Milwaukee P.O.BOX 413 Milwaukee, WI 53144-0413 Daim ntawv no muaj
WORKERS COMPENSATION PROGRAM MARINE CORPS COMMUNITY SERVICES CAMP LEJEUNE-NEW RIVER, NC
 WORKERS COMPENSATION PROGRAM MARINE CORPS COMMUNITY SERVICES CAMP LEJEUNE-NEW RIVER, NC APPLICABILITY: Provisions of the Longshore & Harbor Workers Compensation Act (LHWCA) apply to benefits for disability
WORKERS COMPENSATION PROGRAM MARINE CORPS COMMUNITY SERVICES CAMP LEJEUNE-NEW RIVER, NC APPLICABILITY: Provisions of the Longshore & Harbor Workers Compensation Act (LHWCA) apply to benefits for disability
The Long Term Disability Benefits application includes claim forms and an Authorization.
 Disability Benefits Claim Packet Instructions Your Disability Benefit Claim This packet contains the forms necessary to apply for Long Term Disability benefits. Every space on these forms should be filled
Disability Benefits Claim Packet Instructions Your Disability Benefit Claim This packet contains the forms necessary to apply for Long Term Disability benefits. Every space on these forms should be filled
Information for the New Claimant WORKER S COMPENSATION
 Information for the New Claimant WORKER S COMPENSATION Published by: Employee Compensation and Benefits Services University of Wisconsin Madison 21 N Park Street, Suite 5101 Madison, WI 53715 Daim ntawv
Information for the New Claimant WORKER S COMPENSATION Published by: Employee Compensation and Benefits Services University of Wisconsin Madison 21 N Park Street, Suite 5101 Madison, WI 53715 Daim ntawv
IMPORTANT INFORMATION ABOUT MEDICAL CARE IF YOU HAVE A WORK- RELATED INJURY OR ILLNESS EMPLOYEE NOTIFICATION RE: THE SENTRY MEDICAL PROVIDER NETWORK
 IMPORTANT INFORMATION ABOUT MEDICAL CARE IF YOU HAVE A WORK- RELATED INJURY OR ILLNESS EMPLOYEE NOTIFICATION RE: THE SENTRY MEDICAL PROVIDER NETWORK (Title 8, California Code of Regulations, section 9767.12)
IMPORTANT INFORMATION ABOUT MEDICAL CARE IF YOU HAVE A WORK- RELATED INJURY OR ILLNESS EMPLOYEE NOTIFICATION RE: THE SENTRY MEDICAL PROVIDER NETWORK (Title 8, California Code of Regulations, section 9767.12)
Workers Compensation Fraud
 Workers Compensation Fraud Martin Gonzalez Chief Investigator CA Department of Insurance Fraud Division 5999 E. Slauson Ave. Commerce, CA 90040 (323) 278-5000 1 State of California Department of Insurance
Workers Compensation Fraud Martin Gonzalez Chief Investigator CA Department of Insurance Fraud Division 5999 E. Slauson Ave. Commerce, CA 90040 (323) 278-5000 1 State of California Department of Insurance
WORKERS COMPENSATION PROCEDURES FOR NAF SUPERVISORS EMERGENCY KIT
 WORKERS COMPENSATION PROCEDURES FOR NAF SUPERVISORS EMERGENCY KIT 1 TABLE OF CONTENTS GENERAL INFORMATION 3 SUPERVISOR RESPONSIBILITIES 3 EMPLOYEE RESPONSIBILITIES & BENEFITS 4 REDUCTION OF COSTS 4 "IN
WORKERS COMPENSATION PROCEDURES FOR NAF SUPERVISORS EMERGENCY KIT 1 TABLE OF CONTENTS GENERAL INFORMATION 3 SUPERVISOR RESPONSIBILITIES 3 EMPLOYEE RESPONSIBILITIES & BENEFITS 4 REDUCTION OF COSTS 4 "IN
THE EMPLOYEE S ROLE: When an Employee is Injured on the Job. Human Resources Management Workers Compensation Program
 THE EMPLOYEE S ROLE: When an Employee is Injured on the Job Human Resources Management Workers Compensation Program August 16, 2010 This guidebook gives an overview of the California workers compensation
THE EMPLOYEE S ROLE: When an Employee is Injured on the Job Human Resources Management Workers Compensation Program August 16, 2010 This guidebook gives an overview of the California workers compensation
What s New With CSU Workers Compensation & Workers Compensation Basics. Kenda Weigang November 2015
 What s New With CSU Workers Compensation & Workers Compensation Basics Kenda Weigang November 2015 Updated Website & WC Process Risk Management has a new website http://rmi.prep.colostate.edu/ Workers
What s New With CSU Workers Compensation & Workers Compensation Basics Kenda Weigang November 2015 Updated Website & WC Process Risk Management has a new website http://rmi.prep.colostate.edu/ Workers
PATIENT INFORMATION PATIENT NAME: BIRTHDATE: / / AGE: SOCIAL SECURITY # MARITAL STATUS: ( ) S ( ) M ( ) W ( ) D HOME TELEPHONE # CELLULAR # RELIGION:
 S ( ) M ( ) W ( ) D HOME TELEPHONE # CELLULAR # RELIGION:") NEW PATIENT INFORMATION PRIMARY CARE DOCTOR: PCP # FAX # PATIENT NAME: BIRTHDATE: / / AGE: SOCIAL SECURITY # MARITAL STATUS: ( ) S ( ) M ( ) W ( ) D HOME TELEPHONE # _ CELLULAR # RELIGION: STREET ADDRESS:
NEW PATIENT INFORMATION PRIMARY CARE DOCTOR: PCP # FAX # PATIENT NAME: BIRTHDATE: / / AGE: SOCIAL SECURITY # MARITAL STATUS: ( ) S ( ) M ( ) W ( ) D HOME TELEPHONE # _ CELLULAR # RELIGION: STREET ADDRESS:
DISABILITY CLAIM FORM
 ACE American Insurance Company PROOF OF LOSS Mail to: ACE American Insurance Company Name of Group: UNIVERSITY OF CALIFORNIA P.O. Box 15417 Wilmington, DE 19850 800-336-0627 or 302-476-6194 Policy Number:
ACE American Insurance Company PROOF OF LOSS Mail to: ACE American Insurance Company Name of Group: UNIVERSITY OF CALIFORNIA P.O. Box 15417 Wilmington, DE 19850 800-336-0627 or 302-476-6194 Policy Number:
www.shawnsteel.com Shawn Steel ServicesI 10/28/2013 The first thing we do is kill all the lawyers (Shakespeare s Henry VI)
") www.shawnsteel.com 1(800)-626-0003 Palos Verdes Newport Beach Visit our website! Shawn Steel ServicesI www.shawnsteel.com New Personal Injury Cases - We review any serious case in California - We travel
www.shawnsteel.com 1(800)-626-0003 Palos Verdes Newport Beach Visit our website! Shawn Steel ServicesI www.shawnsteel.com New Personal Injury Cases - We review any serious case in California - We travel
Employer: Employee: Date of Loss: File Number: State Case Num:
 , Claim Department Office Employer: Employee: Date of Loss: File Number: State Case Num: For compensable Workers' Compensation claims, your employer provides medical care through its Workers Compensation
, Claim Department Office Employer: Employee: Date of Loss: File Number: State Case Num: For compensable Workers' Compensation claims, your employer provides medical care through its Workers Compensation
ACCIDENT / INJURY REPORTING PROCEDURES FOR GEORGIA STATE UNIVERSITY
 ACCIDENT / INJURY REPORTING PROCEDURES FOR GEORGIA STATE UNIVERSITY FOR ANY LIFE THREATENING EMERGENCY ** SEEK TREATMENT IMMEDIATELY THEN FOLLOW THE PROCEDURES THAT FOLLOW **LIFE THREATENING EMERGENCIES
ACCIDENT / INJURY REPORTING PROCEDURES FOR GEORGIA STATE UNIVERSITY FOR ANY LIFE THREATENING EMERGENCY ** SEEK TREATMENT IMMEDIATELY THEN FOLLOW THE PROCEDURES THAT FOLLOW **LIFE THREATENING EMERGENCIES
FACTS ABOUT WORKERS COMPENSATION
 FACTS ABOUT WORKERS COMPENSATION What Is It Since 1913, California Workers' Compensation law has guaranteed prompt, automatic benefits to workers who become injured or ill because of their jobs. It is
FACTS ABOUT WORKERS COMPENSATION What Is It Since 1913, California Workers' Compensation law has guaranteed prompt, automatic benefits to workers who become injured or ill because of their jobs. It is
I M M I G R A N T WORKERS HEALTH & SAFETY
 I M M I G R A N T WORKERS HEALTH & SAFETY 1-HOUR HAZARD IDENTIFICATION TRAINING GOAL: This training is designed for a one-hour session with immigrant workers from a variety of industries and from multiple
I M M I G R A N T WORKERS HEALTH & SAFETY 1-HOUR HAZARD IDENTIFICATION TRAINING GOAL: This training is designed for a one-hour session with immigrant workers from a variety of industries and from multiple
THREE RIVERS COMMUNITY COLLEGE PERSONNEL REGULATION
 Last Revision: 03/30/10 Page 1 of 7 Workers Compensation The purpose of this regulation is to ensure that employees of Three Rivers Community College injured within the course and scope of their employment
Last Revision: 03/30/10 Page 1 of 7 Workers Compensation The purpose of this regulation is to ensure that employees of Three Rivers Community College injured within the course and scope of their employment
Who It Covers All UCLA employees and registered volunteers are covered for Workers' Compensation.
 FACTS ABOUT WORKERS COMPENSATION What Is It Since 1913, California Workers' Compensation law has guaranteed prompt, automatic benefits to workers who become injured or ill because of their jobs. It is
FACTS ABOUT WORKERS COMPENSATION What Is It Since 1913, California Workers' Compensation law has guaranteed prompt, automatic benefits to workers who become injured or ill because of their jobs. It is
If you get hurt on the job, your employer is required by law to pay for workers compensation benefits. You could get hurt by:
 UNIVERSITY CORPORATION, SAN FRANCISCO STATE TIME OF HIRE PAMPHLET WHAT IS WORKERS COMPENSATION? If you get hurt on the job, your employer is required by law to pay for workers compensation benefits. You
UNIVERSITY CORPORATION, SAN FRANCISCO STATE TIME OF HIRE PAMPHLET WHAT IS WORKERS COMPENSATION? If you get hurt on the job, your employer is required by law to pay for workers compensation benefits. You
How To Get A Workers Compensation Check In California
 If Your Employer is Illegally Uninsured How to Apply for Workers Compensation Benefits Prepared by the Institute for Research on Labor and Employment, University of California, Berkeley For the Commission
If Your Employer is Illegally Uninsured How to Apply for Workers Compensation Benefits Prepared by the Institute for Research on Labor and Employment, University of California, Berkeley For the Commission
FLORIDA ATLANTIC UNIVERSITY WORKERS COMPENSATION RETURN TO WORK PROGRAM
 FLORIDA ATLANTIC UNIVERSITY WORKERS COMPENSATION RETURN TO WORK PROGRAM APPLICABILITY/ACCOUNTABILITY: In compliance with statutory requirement, this program provides general guidelines for employees who
FLORIDA ATLANTIC UNIVERSITY WORKERS COMPENSATION RETURN TO WORK PROGRAM APPLICABILITY/ACCOUNTABILITY: In compliance with statutory requirement, this program provides general guidelines for employees who
FACTS FOR INJURED WORKERS
 FACTS FOR INJURED WORKERS Hurt On the Job? That can be a terrible experience. But fortunately, the California workers compensation system takes away a lot of the worry about job injuries and illnesses.
FACTS FOR INJURED WORKERS Hurt On the Job? That can be a terrible experience. But fortunately, the California workers compensation system takes away a lot of the worry about job injuries and illnesses.
PREDESIGNATION OF PERSONAL PHYSICIANS AND REPORTING DUTIES OF THE PRIMARY TREATING PHYSICIAN REGULATIONS
 PREDESIGNATION OF PERSONAL PHYSICIANS AND REPORTING DUTIES OF THE PRIMARY TREATING PHYSICIAN REGULATIONS Title 8, California Code of Regulations Chapter 4.5. Division of Workers Compensation Subchapter
PREDESIGNATION OF PERSONAL PHYSICIANS AND REPORTING DUTIES OF THE PRIMARY TREATING PHYSICIAN REGULATIONS Title 8, California Code of Regulations Chapter 4.5. Division of Workers Compensation Subchapter
TEXAS DEPARTMENT OF CRIMINAL JUSTICE Supervisor s Report Packet for Workers Compensation CONTENTS
 Supervisor s Report Packet for Workers Compensation CONTENTS PERS 299-1, Supervisor s Guidelines for Workers Compensation PERS 299-2, Witness Statement PERS 299-3, Supplemental Worksheet PERS 299 (09/15)
Supervisor s Report Packet for Workers Compensation CONTENTS PERS 299-1, Supervisor s Guidelines for Workers Compensation PERS 299-2, Witness Statement PERS 299-3, Supplemental Worksheet PERS 299 (09/15)
WORKER'S COMPENSATION PEMBERTON TOWNSHIP SCHOOLS FIRST REPORT EMPLOYEE INJURY/TREATMENT FORM
 WORKER'S COMPENSATION PEMBERTON TOWNSHIP SCHOOLS FIRST REPORT EMPLOYEE INJURY/TREATMENT FORM Per District Policy 8440, all work related injuries must be reported to the Nurse or Jim Flanagan (609) 893-8141
WORKER'S COMPENSATION PEMBERTON TOWNSHIP SCHOOLS FIRST REPORT EMPLOYEE INJURY/TREATMENT FORM Per District Policy 8440, all work related injuries must be reported to the Nurse or Jim Flanagan (609) 893-8141
California AIG Primary Medical Provider Network. Employee Notification
 California AIG Primary Medical Provider Network Employee Notification 2013 American International Group, Inc. All rights reserved. 95816 SP 0897A (Rev 10/13) Contents What is an MPN?... 2 How do I find
California AIG Primary Medical Provider Network Employee Notification 2013 American International Group, Inc. All rights reserved. 95816 SP 0897A (Rev 10/13) Contents What is an MPN?... 2 How do I find
Workers' Compensation: A Timekeeper's Handbook
 Workers' Compensation: A Timekeeper's Handbook c o n t e n t s Introduction Procedures For All Claims Procedures for Accepted Claims 80% Extended Sick Leave Procedures for Pending Claims Procedures for
Workers' Compensation: A Timekeeper's Handbook c o n t e n t s Introduction Procedures For All Claims Procedures for Accepted Claims 80% Extended Sick Leave Procedures for Pending Claims Procedures for
Employee s Report of Incident and the Supervisor's Investigation
 HOW TO REPORT A WORKERS COMPENSATION INJURY 1. The employee must complete the Employee s Report of Incident and submit it to his/her supervisor within 2 hours of the incident. 2. The supervisor must complete
HOW TO REPORT A WORKERS COMPENSATION INJURY 1. The employee must complete the Employee s Report of Incident and submit it to his/her supervisor within 2 hours of the incident. 2. The supervisor must complete
Important Information about Medical Care if you have a Work-Related Injury or Illness
 Important Information about Medical Care if you have a Work-Related Injury or Illness Initial Written Employee Notification Re: Medical Provider Network (Title 8, California Code of Regulations, section
Important Information about Medical Care if you have a Work-Related Injury or Illness Initial Written Employee Notification Re: Medical Provider Network (Title 8, California Code of Regulations, section
Thank you. Should you have any questions, please call us at (800) 541-3522.
 541-3522.") Dear Policyholder: Please complete and sign the attached claim form. Additionally, the following items are needed in order to process your Trip Cancellation claim in the most efficient and expedient way
Dear Policyholder: Please complete and sign the attached claim form. Additionally, the following items are needed in order to process your Trip Cancellation claim in the most efficient and expedient way
NOTIFICATION OF INJURY
 NOTIFICATION OF INJURY This Notification of Injury Form is to be used for accident medical claims. **Note: The SAI claim form (Parts A & B) should be submitted to Loomis (address on next page) as soon
NOTIFICATION OF INJURY This Notification of Injury Form is to be used for accident medical claims. **Note: The SAI claim form (Parts A & B) should be submitted to Loomis (address on next page) as soon
City of Los Angeles Disability Insurance Claim Packet Instructions
 Claim Packet Instructions Your Disability Benefit Claim This packet contains the forms necessary to apply for disability benefits. It also addresses common questions about Disability claims. Please save
Claim Packet Instructions Your Disability Benefit Claim This packet contains the forms necessary to apply for disability benefits. It also addresses common questions about Disability claims. Please save
THE SUPERVISOR S ROLE:
 THE SUPERVISOR S ROLE: Workers Compensation Information for CSU, Los Angeles Supervisors Human Resources Management (HRM) Workers Compensation Program August 16, 2010 Table of Contents Introduction..3
THE SUPERVISOR S ROLE: Workers Compensation Information for CSU, Los Angeles Supervisors Human Resources Management (HRM) Workers Compensation Program August 16, 2010 Table of Contents Introduction..3
Time of hire pamphlet
 This pamphlet, or a similar one that has been approved by the Administrative Director, must be given to all newly hired employees in the State of California. Employers and claims administrators may use
This pamphlet, or a similar one that has been approved by the Administrative Director, must be given to all newly hired employees in the State of California. Employers and claims administrators may use
WORKERS COMPENSATION POLICY
 Revised: 08/03/06 THE CITY OF POMONA SAFETY POLICIES AND PROCEDURES WORKERS COMPENSATION POLICY City Manager: I. PURPOSE This Policy describes the procedures for the City of Pomona s self-insured workers
Revised: 08/03/06 THE CITY OF POMONA SAFETY POLICIES AND PROCEDURES WORKERS COMPENSATION POLICY City Manager: I. PURPOSE This Policy describes the procedures for the City of Pomona s self-insured workers
ADMINISTRATIVE PROCEDURE
 NO: 5170 PAGE: 1 OF 8 ADMINISTRATIVE PROCEDURE CATEGORY: SUBJECT: Support Services, Safety Program Mandatory Reports for Employee Injury or Illness on the Job A. PURPOSE AND SCOPE 1. To outline administrative
NO: 5170 PAGE: 1 OF 8 ADMINISTRATIVE PROCEDURE CATEGORY: SUBJECT: Support Services, Safety Program Mandatory Reports for Employee Injury or Illness on the Job A. PURPOSE AND SCOPE 1. To outline administrative
Disability Insurance Claim Packet Instructions. Your Disability Benefit Claim. How To Apply For Benefits
 Claim Packet Instructions Your Disability Benefit Claim This packet contains the forms necessary to apply for disability benefits. It also addresses common questions about Disability claims. Please save
Claim Packet Instructions Your Disability Benefit Claim This packet contains the forms necessary to apply for disability benefits. It also addresses common questions about Disability claims. Please save
Supervisor s Guide for Injury Reporting
 Supervisor s Guide for Injury Reporting Table of Contents Topics Page Emergency Injury Reporting 3-4 Non-Emergency Injury Reporting 5 Employee Seeks Treatment 6-8 Employee Injury/Illness File 9-10 Employee
Supervisor s Guide for Injury Reporting Table of Contents Topics Page Emergency Injury Reporting 3-4 Non-Emergency Injury Reporting 5 Employee Seeks Treatment 6-8 Employee Injury/Illness File 9-10 Employee
#6-604 Accident Reporting Policy Page 1 of 5
 Page 1 of 5 Approved By: Cabinet Effective Date: January 2, 2013 Category: Contact: Human Resources Assistant Vice President for Human Resources (585) 245-5516 I. PURPOSE This document outlines the policies
Page 1 of 5 Approved By: Cabinet Effective Date: January 2, 2013 Category: Contact: Human Resources Assistant Vice President for Human Resources (585) 245-5516 I. PURPOSE This document outlines the policies
Princeton University Work-Related Injury Management Frequently Asked Questions for Supervisors
 Princeton University Work-Related Injury Management Frequently Asked Questions for Supervisors Section 1: Short-Term Disability and Workers Compensation... 2 Section 2: Reporting Injuries and Seeking Medical
Princeton University Work-Related Injury Management Frequently Asked Questions for Supervisors Section 1: Short-Term Disability and Workers Compensation... 2 Section 2: Reporting Injuries and Seeking Medical
Accident insurance plain claim form
 The Lincoln National Life Insurance Company PO Box 82087, Lincoln, NE 68501-2087 toll free (800) 423-2765 Fax (877) 843-3950 www.lincolnfinancial.com Accident insurance plain claim form Policy Holder Information
The Lincoln National Life Insurance Company PO Box 82087, Lincoln, NE 68501-2087 toll free (800) 423-2765 Fax (877) 843-3950 www.lincolnfinancial.com Accident insurance plain claim form Policy Holder Information
Your Guide to Workers Compensation
 What isworkers compensation? Your Guide to Workers Compensation Workers compensation is insurance that the law requires your employer to have to cover on the jobinjuries.ifyou become injuredon the jobor
What isworkers compensation? Your Guide to Workers Compensation Workers compensation is insurance that the law requires your employer to have to cover on the jobinjuries.ifyou become injuredon the jobor
Important Information about Medical Care if you have a Work-Related Injury or Illness
 Important Information about Medical Care if you have a Work-Related Injury or Illness Complete Written Employee Notification Re: Medical Provider Network (Title 8, California Code of Regulations, section
Important Information about Medical Care if you have a Work-Related Injury or Illness Complete Written Employee Notification Re: Medical Provider Network (Title 8, California Code of Regulations, section
Thank you for this important information. Should you have any questions, please call us at (800) 541-3522.
 541-3522.") Dear Policyholder: Please complete and sign the attached claim form. Additionally, the following are items needed in order to process your Travel Delay claim in the most efficient and expedient way possible.
Dear Policyholder: Please complete and sign the attached claim form. Additionally, the following are items needed in order to process your Travel Delay claim in the most efficient and expedient way possible.
5.42.2 Designated Workers Compensation Facilities
 5.42 Workers Compensation Policy (adopted May 12, 2014) The College provides Workers Compensation benefits for all College employees pursuant to the mandates of the Missouri Workers Compensation Law. Employees
5.42 Workers Compensation Policy (adopted May 12, 2014) The College provides Workers Compensation benefits for all College employees pursuant to the mandates of the Missouri Workers Compensation Law. Employees
Notice of Privacy Practices
 Effective May 1, 2013 Notice of Privacy Practices This notice describes how medical information about you may be used and disclosed and how you can get access to this information. Please review it carefully.
Effective May 1, 2013 Notice of Privacy Practices This notice describes how medical information about you may be used and disclosed and how you can get access to this information. Please review it carefully.
PARKWAY MEDICAL GROUP Phone: 828-293-0333 Fax: 828-298-0050 NAME: D.O.B. M/F ADDRESS: PHONE: ( ) CITY: STATE: ZIP: SS#: - - COMPANY:
 CITY: STATE: ZIP: SS#: - - COMPANY:") PARKWAY MEDICAL GROUP Phone: 828-293-0333 Fax: 828-298-0050 NAME: D.O.B. M/F ADDRESS: PHONE: ( ) CITY: STATE: ZIP: SS#: - - COMPANY: Please check and sign the appropriate consent: COMPANY EVALUATION: (Physical,
PARKWAY MEDICAL GROUP Phone: 828-293-0333 Fax: 828-298-0050 NAME: D.O.B. M/F ADDRESS: PHONE: ( ) CITY: STATE: ZIP: SS#: - - COMPANY: Please check and sign the appropriate consent: COMPANY EVALUATION: (Physical,
State of Nevada Public Employees Benefits Program (PEBP) Short Term Disability Insurance Claim Packet Instructions
 Short Term Disability Insurance Claim Packet Instructions") Claim Packet Instructions Your Disability Benefit Claim This packet contains the forms necessary to apply for disability benefits. It also addresses common questions about Disability claims. Please save
Claim Packet Instructions Your Disability Benefit Claim This packet contains the forms necessary to apply for disability benefits. It also addresses common questions about Disability claims. Please save
WORKERS COMPENSATION CHECKLIST
 WORKERS COMPENSATION CHECKLIST This checklist is provided to assist the employee and supervisor in being certain that an injured employee gets proper medical care and timely pay, as well as assisting to
WORKERS COMPENSATION CHECKLIST This checklist is provided to assist the employee and supervisor in being certain that an injured employee gets proper medical care and timely pay, as well as assisting to
The following state forms have been included in your claims kit packet:
 RE: Workers Compensation Claims Kit Dear Policyholder: Welcome to Tower Group Companies Workers Compensation Insurance Program. Although we hope that your company never experiences an injury to an employee,
RE: Workers Compensation Claims Kit Dear Policyholder: Welcome to Tower Group Companies Workers Compensation Insurance Program. Although we hope that your company never experiences an injury to an employee,
Worker s and Physician s Report for Workers Compensation Claim Form 827
 Worker s and Physician s Report for Workers Compensation Claim Form 827 NOTES to physician or nurse practitioner Ask the worker to complete this form ONLY in the following circumstances: First report of
Worker s and Physician s Report for Workers Compensation Claim Form 827 NOTES to physician or nurse practitioner Ask the worker to complete this form ONLY in the following circumstances: First report of
1. Full Name (last, first, middle initial) 2. Social Security Number 3. Phone Number (include area code)
 2. Social Security Number 3. Phone Number (include area code)") GROUP SHORT-TERM DISABILITY STATEMENT OF EMPLOYEE (BENEFITS MAY BE DELAYED IF CLAIM FORM IS NOT FULLY COMPLETED) Please sign this page and the authorization on page two of this form to avoid delays in
GROUP SHORT-TERM DISABILITY STATEMENT OF EMPLOYEE (BENEFITS MAY BE DELAYED IF CLAIM FORM IS NOT FULLY COMPLETED) Please sign this page and the authorization on page two of this form to avoid delays in
CLAIMS REPORTING TO REPORT AN INJURY CALL 1-866-274-6033. 24 hours a day / 7 days a week
 CLAIMS REPORTING TO REPORT AN INJURY CALL 1-866-274-6033 24 hours a day / 7 days a week You will need the following information to report a claim. However, do not delay reporting if you are missing information.
CLAIMS REPORTING TO REPORT AN INJURY CALL 1-866-274-6033 24 hours a day / 7 days a week You will need the following information to report a claim. However, do not delay reporting if you are missing information.
NIGHT & ON-CALL EMPLOYEES WORKERS COMPENSATION INFORMATION GUIDE
 The 10 Rules of Workplace Safety Risk & Benefits Management 1. Always be responsible for the safety of yourself and others. 2. Always remember all accidents are preventable 3. Always follow company rules,
The 10 Rules of Workplace Safety Risk & Benefits Management 1. Always be responsible for the safety of yourself and others. 2. Always remember all accidents are preventable 3. Always follow company rules,
A Practical Guide on How to Handle Employee Injury/Accident. Employer Manual. (HR Contacts and Supervisors only)
") A Practical Guide on How to Handle Employee Injury/Accident 1 Employer Manual (HR Contacts and Supervisors only) For more information regarding prevention of risk visit our website at http://www.nova.edu/cwis/fop/risk/
A Practical Guide on How to Handle Employee Injury/Accident 1 Employer Manual (HR Contacts and Supervisors only) For more information regarding prevention of risk visit our website at http://www.nova.edu/cwis/fop/risk/
Important Information about Medical Care if you have a Work-Related Injury or Illness
 Important Information about Medical Care if you have a Work-Related Injury or Illness Initial Employee Written Notification Regarding Your Medical Provider Network Complete Written Employee Notification
Important Information about Medical Care if you have a Work-Related Injury or Illness Initial Employee Written Notification Regarding Your Medical Provider Network Complete Written Employee Notification
GROUP SHORT-TERM DISABILITY STATEMENT OF EMPLOYEE
 GROUP SHORT-TERM DISABILITY STATEMENT OF EMPLOYEE 1. Full Name (last, first, middle initial) 2. Social Security Number 3. Phone Number (include area code) 4. Street Address & Mailing Address 5. City 6.
GROUP SHORT-TERM DISABILITY STATEMENT OF EMPLOYEE 1. Full Name (last, first, middle initial) 2. Social Security Number 3. Phone Number (include area code) 4. Street Address & Mailing Address 5. City 6.
CITY OF NEWPORT NEWS PERSONNEL ADMINISTRATIVE MANUAL Effective: 4/01/08
 This section establishes policies and procedures pertaining to work-related injuries and diseases. I. PROCEDURES A. Any employee who sustains or witnesses a work-related injury or any employee who is diagnosed
This section establishes policies and procedures pertaining to work-related injuries and diseases. I. PROCEDURES A. Any employee who sustains or witnesses a work-related injury or any employee who is diagnosed
Disability Insurance Claim Packet Instructions. Your Disability Benefit Claim. The Standard Benefit Administrators. How To Apply For Benefits
 Claim Packet Instructions Your Disability Benefit Claim This packet contains the forms necessary to apply for disability benefits. It also addresses common questions about Disability claims. Please save
Claim Packet Instructions Your Disability Benefit Claim This packet contains the forms necessary to apply for disability benefits. It also addresses common questions about Disability claims. Please save
For Employees: What to do when an illness/accident occurs
 For Employees: What to do when an illness/accident occurs Effective March 30, 2015 06 29 15/DJ/dmv When there is a work-related accident or illness, procedures must be taken to ensure that our employees
For Employees: What to do when an illness/accident occurs Effective March 30, 2015 06 29 15/DJ/dmv When there is a work-related accident or illness, procedures must be taken to ensure that our employees
Important Information about Medical Care if you have a Work-Related Injury or Illness
 Important Information about Medical Care if you have a Work-Related Injury or Illness Complete Written Employee Notification regarding Medical Provider Network (Title 8, California Code of Regulations,
Important Information about Medical Care if you have a Work-Related Injury or Illness Complete Written Employee Notification regarding Medical Provider Network (Title 8, California Code of Regulations,
ELGIN LOCAL SCHOOLS. WORKERS COMPENSATION MANUALS AND FORMS For Elgin Administration
 ELGIN LOCAL SCHOOLS WORKERS COMPENSATION MANUALS AND FORMS For Elgin Administration Revised May 2014 1 ELGIN LOCAL SCHOOLS BUREAU OF WORKER S COMPENSATION CLAIM INSTRUCTIONS The Following steps must be
ELGIN LOCAL SCHOOLS WORKERS COMPENSATION MANUALS AND FORMS For Elgin Administration Revised May 2014 1 ELGIN LOCAL SCHOOLS BUREAU OF WORKER S COMPENSATION CLAIM INSTRUCTIONS The Following steps must be
NAVIGATORS INSURANCE COMPANY Real Estate Professional Errors and Omissions Insurance EXPRESS APPLICATION NEW HAMPSHIRE
 Clear Form To Submit: Save then email to info@orep.org; Fax: 708-570-5786 NAVIGATORS INSURANCE COMPANY Real Estate Professional Errors and Omissions Insurance EXPRESS APPLICATION NEW HAMPSHIRE To be eligible
Clear Form To Submit: Save then email to info@orep.org; Fax: 708-570-5786 NAVIGATORS INSURANCE COMPANY Real Estate Professional Errors and Omissions Insurance EXPRESS APPLICATION NEW HAMPSHIRE To be eligible
POLICY BULLETIN #06-95-ELI
 \FAMILY INDEPENDENCE ADMINISTRATION Seth W. Diamond, Executive Deputy Commissioner James K. Whelan, Deputy Commissioner Policy, Procedures and Training Lisa C. Fitzpatrick, Assistant Deputy Commissioner
\FAMILY INDEPENDENCE ADMINISTRATION Seth W. Diamond, Executive Deputy Commissioner James K. Whelan, Deputy Commissioner Policy, Procedures and Training Lisa C. Fitzpatrick, Assistant Deputy Commissioner
On behalf of our company, we wish to express our sincere condolences on your loss.
 Administrative Office: Valley Forge Pennsylvania 19493 Phone: 1-866-227-0379 Dear Claimant, On behalf of our company, we wish to express our sincere condolences on your loss. We hope that we may assist
Administrative Office: Valley Forge Pennsylvania 19493 Phone: 1-866-227-0379 Dear Claimant, On behalf of our company, we wish to express our sincere condolences on your loss. We hope that we may assist
HOW TO FILE A DISABILITY CLAIM (For Benefits Provided Pursuant to an Employer Provided Benefit Plan)
") HOW TO FILE A DISABILITY CLAIM (For Benefits Provided Pursuant to an Employer Provided Benefit Plan) If you have Short Term Disability and/or Long Term Disability coverage by virtue of your employment,
HOW TO FILE A DISABILITY CLAIM (For Benefits Provided Pursuant to an Employer Provided Benefit Plan) If you have Short Term Disability and/or Long Term Disability coverage by virtue of your employment,
The following State forms have been included in your claims kit packet:
 RE: Workers Compensation Claims Kit Dear Policyholder: Welcome to Tower Group Companies Workers Compensation Insurance Program. Although we hope that your company never has to experience an injury to an
RE: Workers Compensation Claims Kit Dear Policyholder: Welcome to Tower Group Companies Workers Compensation Insurance Program. Although we hope that your company never has to experience an injury to an
CLAIM FORM. List all dates unemployment benefits are being or have been paid: From: To ; From: To
 Reply To: Please attach a copy of your policy/certificate and a copy of your retail installment contract. incomplete forms may cause a delay in the processing of your claim. Claims Department P.O. Box
Reply To: Please attach a copy of your policy/certificate and a copy of your retail installment contract. incomplete forms may cause a delay in the processing of your claim. Claims Department P.O. Box