Bruce Nash, MD, MBA Senior VP / Chief Medical Officer Capital District Physicians Health Plan, Inc. March 9, 2009
|
|
|
- Nancy Clarke
- 8 years ago
- Views:
Transcription
1 Bruce Nash, MD, MBA Senior VP / Chief Medical Officer Capital District Physicians Health Plan, Inc. March 9, 2009 page 1.1 page 1.1

2 CDPHP Pilot Payment Reform Practice Reform page 1.2 page 1.2

3 Resources TransforMed Payment Reform DxCG/Verisk: Arlene Ash, PhD ; Randy Ellis PhD (Boston University) Ingenix: Dogu Celebi, MD, MPH Bridges to Excellence: Francois de Brantes, MBA Evaluation Allan Goroll, MD (Massachusetts General Hospital) David Bates, MD (Brigham & Women s Hospital) page 1.3 page 1.3
 David Bates, MD (Brigham & Women s")
4 Payment Reform page 1.4 page 1.4

5 Payment Reform Comprehensive payment for comprehensive care Align financial incentives Create an opportunity to significantly increase primary care physician income (35 50%) Goroll AH, Berenson RA, Schoenbaum SC, Gardner LB. Fundamental reform of payment for adult primary care: comprehensive payment for comprehensive care. J Gen Intern Med 2007; 22: page 1.5 page 1.5

6 Payment Reform CDPHP Pilot 27% Bonus Payment 3% FFS - RBRVS 70% Risk-Adjusted Comprehensive Payment * Targeted at improving base reimbursement approximately $35,000 to page 1.6 reflect increased costs of implementing and operating a medical home. page 1.6

7 Pilot Practice Opportunity Per physician with average panel size/risk $35K base payment increase to cover Medical Home expenses $50K bonus potential Performance will be reported at the individual physician level and the practice All payments will be made at the practice level page 1.7 page 1.7

8 Risk Adjusted Comprehensive Base Payment page 1.8 page 1.8

9 Primary Care Activity Level Model DxCG/Verisk developed a risk-adjustment model (PCAL) for the CDPHP Medical Home project. A risk-adjusted base capitation payment linked to the expected level of activity needed to provide optimal primary care for a physician's patient panel. page 1.9 page 1.9

10 Risk Adjusted Comprehensive Base Payment Two components of the formula PCAL = Primary Care Activity Level CF = Conversion Factor PMPM = PCAL x CF page 1.10 page 1.10

11 CDPHP Panel Attribution We will be using the Ingenix imputation logic for CDPHP patient attribution. Patients who have not been seen within the past 24 months will not be included. We will not be using HMO assignment. page 1.11 page 1.11

12 Bonus Payment Model page 1.12 page 1.12

13 Bonus Model Components Satisfaction / Access Effectiveness (Quality) Efficiency (Cost) page 1.13 page 1.13
 page 1.")
14 Challenge of Bonus Measure Design To identify those metrics upon which to base a bonus payment which are strongly correlated to lesser costs and the maintenance or improvement of quality page 1.14 page 1.14

15 Bonus Program $50K potential per physician with average patient panel. A minimum performance of satisfaction/access is a threshold requirement for any bonus eligibility. Effectiveness (BTE) will determine available bonus. Risk adjusted efficiency measurement (Ingenix) will determine distribution. Measurement and payment will be at the practice level, however, data for individual physician performance will also be reported. page 1.15 page 1.15
 will determine distribution.")
16 Effectiveness To ensure that the quality of health care delivery is at least maintained or preferably enhanced under this payment model. Measures of: Population Health Acute Disease Management Chronic Disease Management Bridges to Excellence tool set page 1.16 page 1.16

17 Clinical areas of measurement Population health Hypertension Diabetes CHF CAD Asthma COPD Back Pain IVD/Stroke Some measures are cross-cutting: BP LDL Use of diuretics Smoking cessation page 1.17 page 1.17

18 Example page 1.18 page 1.18
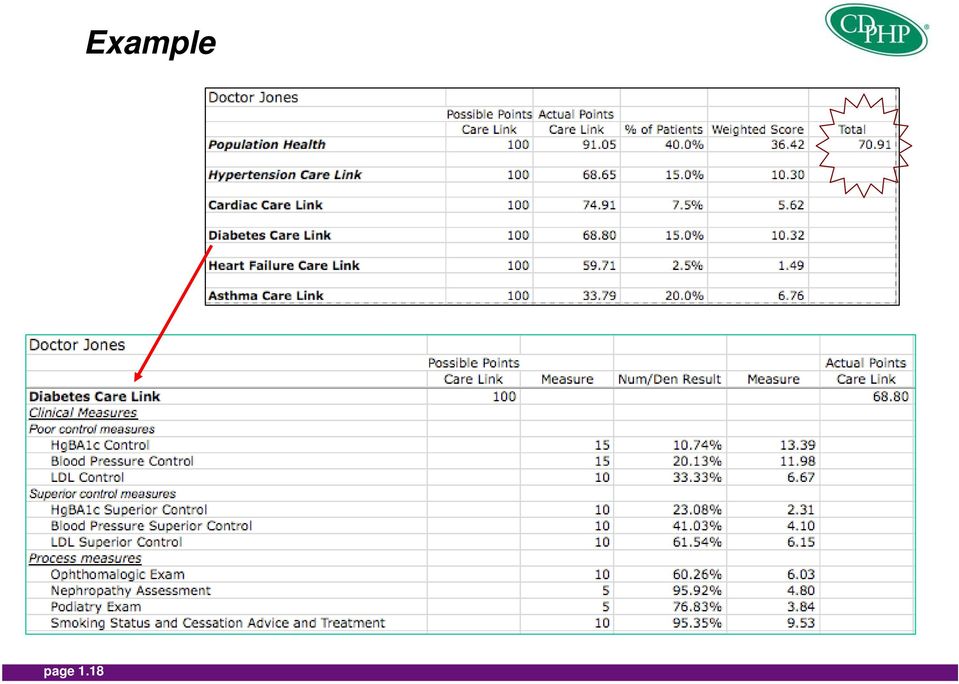
19 Available Bonus On an Effectiveness scale of 100, a physician needs to score a minimum of 50 in order to qualify for a bonus. Assuming average size physician panel, every point over 50 will qualify for a bonus of $1,250 per point. Physician with a score >=90 will receive the maximum bonus amount. Example: For a physician with effectiveness score of 71: (Effectiveness score 50) x $1,250 = Available Bonus Amount (71-50) x $1,250 = $26,250 page 1.19 page 1.19

20 Efficiency To ensure that bonus payments are associated with aggregate cost savings to allow for a sustainable payment model Claims based measurement Ingenix tools page 1.20 page 1.20

21 Efficiency will be measured along three dimensions A. Utilization Based B. Population Based C. Episode Based page 1.21 page 1.21
22 A. Utilization-Based 1. Hospitalization rates (inpatient admissions per 1000 patients) Hospitalization rates will be calculated only for Ambulatory Care Sensitive Conditions. page 1.22 page 1.22
23 A. Utilization-Based (continued) page 1.23 Ambulatory Care Sensitive Conditions Epileptic convulsions Severe ear, nose, and throat infections Chronic obstructive pulmonary disease Bacterial pneumonia Asthma Congestive heart failure Hypertension Angina Cellulitis Diabetes "A" Hypoglycemia Gastroenteritis Kidney/urinary infection Dehydration - volume depletion Iron deficiency anemia Pelvic inflammatory disease page 1.23
24 A. Utilization-Based (continued) 2. Emergency Room Rates (ER visit rate per 1000 members) Exclusions: ER visits with an eventual admission Trauma Random events Acute High intensity/severe (cancer, etc.) page 1.24 page 1.24
25 B. Population-Based Population-based efficiency will be measured in three categories ($PMPM costs by type of service.) 1. Specialty care and outpatient Includes all specialties Includes all non - radiology, non - lab outpatient costs Excludes inpatient, surgical centers, and ER costs 2. Radiology All professional and facility radiology costs Excludes inpatient radiology costs 3. Pharmacy Pharmacy costs associated with pharmacy benefit page 1.25 page 1.25
26 C. Episode-Based All medical costs associated with a given medical condition, adjusted for differences in case-mix Selection criteria: Clinical significance High prevalence High incidence Economic significance Sensitive/amenable to primary care, i.e., actionable Demonstrated variations in cost/utilization of care page 1.26 page 1.26
27 C. Episode-Based (continued) Episodes for selected medical conditions (cost per episode) Diabetes, asthma, CAD, CHF, sinusitis, GERD, hypertension, and low back pain The same three types of services as population-based measures: 1. Specialty care and outpatient 2. Pharmacy 3. Radiology page 1.27 page 1.27
28 Summary of Efficiency Metrics A. Utilization-based Inpatient hospital admissions (selected) Emergency room encounters (selected) B. Population-based Specialty care and outpatient Pharmacy Radiology C. Episode-based Specialty care and outpatient Pharmacy Radiology page 1.28 page 1.28
29 Efficiency Example Ingenix Index A. Utilization Index Inpatient hospital admissions (selected) 1.50 Emergency room encounters (selected) 0.90 B. Population-Based Specialty care and other outpatient hospital 1.20 Pharmacy 0.90 Radiology 1.35 C. Episode-Based Specialty care and other outpatient hospital 1.35 Pharmacy 0.85 Radiology 0.95 page 1.29 page 1.29
30 Efficiency Example Weightings A. Utilization Weight Index Inpatient hospital admissions (selected) 5% 1.50 Emergency room encounters (selected) 5% 0.90 B. Population-Based Specialty care and other outpatient hospital 35% 1.20 Pharmacy 15% 0.90 Radiology 10% 1.35 C. Episode-Based Specialty care and other outpatient hospital 15% 1.35 Pharmacy 10% 0.85 Radiology 5% 0.95 page 1.30 page 1.30
31 Efficiency Example Composite Population-Based Weight Index Composite Specialty care and other outpatient hospital 35% Pharmacy 15% Radiology 10% Episode-Based Specialty care and other outpatient hospital 15% Pharmacy 10% Radiology 5% Utilization Inpatient hospital admissions (selected) 5% Emergency room encounters (selected) 5% Composite Total page 1.31 page 1.31
32 Ranking Each physician s Composite Efficiency Score will be ranked relative to the peer group Ranking determines the payout of the available bonus page 1.32 page 1.32
33 Bonus Distribution Efficiency Each practice s Composite Efficiency Score will be ranked relative to their peer group of primary care physicians in the Capital District If a practice is below the 60 th percentile (Efficiency Threshold), the practice will not be eligible for any bonus. If a practice ranked between 60 th and 90 th percentile, each additional percentile point is worth 2.5% of the available bonus. If a practice is above 90th, the practice will receive 100% of the available bonus. page 1.33 page 1.33
34 Bonus Distribution Summary (for average panel size) Create the Bonus Opportunity Effectiveness Score 0 50 = No opportunity = $1,250 per point above 50 > 90 = $50,000 opportunity Distribute the Bonus Opportunity Efficiency Ranking 0 60 th = No distribution 61 st to 90 th = 2.5% per percentile above 60 th > 90 th = $50,000 page 1.34 page 1.34
35 Illustration of Bonus Program Scenarios Practice Average Effectiveness Score Available Bonus amount per MD Average Efficiency ranking Bonus Per physician Total Practice Bonus A (10 MDs) B (5 MDs) 92 $50, th $0 $0 45 $0 92 nd $0 $0 C (4 MDs) 94 $50, th (85-60) x 2.5% = 62.5% of $50,000 or $31,250 $125,000 page 1.35 page 1.35
36 Pilot Hypothesis Is the aggregate savings associated with better health outcomes and lower utilization sufficient to fund the enhanced compensation to a primary care physician as well as provide a surplus to the plan? page 1.36 page 1.36
37 Cumulative Member Spend Cumulative Spend By Members $900M $600k $800M $700M 95% of Spend 52.4% of Members Total: $848M Spend 355k Members $500k Cumulative CDPHP Spend $600M $500M $400M $300M 50% of Spend 4.5% of Members 80% of Spend 21.3% of Members $400k $300k $200k Spend Per Member $200M $100M $0M 30% of Spend 1.2% of Members 0k 50k 100k 150k 200k 250k 300k 350k 400k CDPHP Members $100k $0k Note: Data does page not 1.37 include LabCorp or pharma spend Sources: 2006 CDPHP Medical Claims, ChapterHouse Analysis page 1.37
38 While Only Accounting for 6% of Total Spend, $4.5M Was Spent on Doctor X s Patients Total Payments Made - $4.5M $900k $800k $700k $600k Dr Fees Evaluation and Management Radiology Other Services Other Room and Board Surgical Laboratory Ambsurg $500k $400k $300k $200k $100k $0k Stroke Cancer Coronary Heart Disease Diabetes Hypertension Low Back Pain COPD Mental Illness Congestive Heart Failure Asthma Other Healthy Members Notes: 1. Does not page include 1.38 LabCorp or pharma spend 2. Shows total spend for any member who visited doctor during 2006 Sources: page CDPHP claims data; ChapterHouse Analysis
39 Pilot Economics In our payment model, < 2% of total health care expense for a primary care physician s practice would need to be saved to support an increased payment opportunity of $85,000 per physician. page 1.39 page 1.39
40 page 1.40 page 1.40
41 Questions?
The Future of Population-Based Reimbursement
 Thomas Jefferson University Jefferson Digital Commons Jefferson College of Population Health Forum Jefferson College of Population Health 11-12-2014 The Future of Population-Based Reimbursement David Chin,
Thomas Jefferson University Jefferson Digital Commons Jefferson College of Population Health Forum Jefferson College of Population Health 11-12-2014 The Future of Population-Based Reimbursement David Chin,
Value-Based Programs. Blue Plans Improving Healthcare Quality and Affordability through Innovative Partnerships with Clinicians
 Value-Based Programs Blue Plans Improving Healthcare Quality and Affordability through Innovative Partnerships with Clinicians Issue: U.S. healthcare spending exceeds $2.8 trillion annually. 1 With studies
Value-Based Programs Blue Plans Improving Healthcare Quality and Affordability through Innovative Partnerships with Clinicians Issue: U.S. healthcare spending exceeds $2.8 trillion annually. 1 With studies
Accountable Care Organization
 Accountable Care Organization April 13, 2011 The Indianapolis Association of Health Underwriters Drivers of Payment Reform Increased attention to regional variation in costs and quality Payment for care
Accountable Care Organization April 13, 2011 The Indianapolis Association of Health Underwriters Drivers of Payment Reform Increased attention to regional variation in costs and quality Payment for care
Table 1 Performance Measures. Quality Monitoring P4P Yr1 Yr2 Yr3. Specification Source. # Category Performance Measure
 Table 1 Performance Measures # Category Performance Measure 1 Behavioral Health Risk Assessment and Follow-up 1) Behavioral Screening/ Assessment within 60 days of enrollment New Enrollees who completed
Table 1 Performance Measures # Category Performance Measure 1 Behavioral Health Risk Assessment and Follow-up 1) Behavioral Screening/ Assessment within 60 days of enrollment New Enrollees who completed
Medicare Shared Savings Program Quality Measure Benchmarks for the 2014 Reporting Year
 Medicare Shared Savings Program Quality Measure Benchmarks for the 2014 Reporting Year Release Notes/Summary of Changes (February 2015): Issued correction of 2014 benchmarks for ACO-9 and ACO-10 quality
Medicare Shared Savings Program Quality Measure Benchmarks for the 2014 Reporting Year Release Notes/Summary of Changes (February 2015): Issued correction of 2014 benchmarks for ACO-9 and ACO-10 quality
Supplemental Technical Information
 An Introductory Analysis of Potentially Preventable Health Care Events in Minnesota Overview Supplemental Technical Information This document provides additional technical information on the 3M Health
An Introductory Analysis of Potentially Preventable Health Care Events in Minnesota Overview Supplemental Technical Information This document provides additional technical information on the 3M Health
Pay for Performance: Its Influence on the Use of IT in Physician Organizations
 Pay for Performance: Its Influence on the Use of IT in Physician Organizations Thomas R. Williams, M.B.A., M.P.H.,* Kristiana Raube, Ph.D., Cheryl L. Damberg, Ph.D., and Russell E. Mardon, Ph.D.** T he
Pay for Performance: Its Influence on the Use of IT in Physician Organizations Thomas R. Williams, M.B.A., M.P.H.,* Kristiana Raube, Ph.D., Cheryl L. Damberg, Ph.D., and Russell E. Mardon, Ph.D.** T he
Texas Medicaid Managed Care and Children s Health Insurance Program
 Texas Medicaid Managed Care and Children s Health Insurance Program External Quality Review Organization Summary of Activities and Trends in Healthcare Quality Contract Year 2013 Measurement Period: September
Texas Medicaid Managed Care and Children s Health Insurance Program External Quality Review Organization Summary of Activities and Trends in Healthcare Quality Contract Year 2013 Measurement Period: September
Employee Population Health Management:
 Employee Population Health Management: a stepping stone for accountable care Richard Boehler, MD, MBA, FACPE President and Chief Executive Officer St. Joseph Hospital, Nashua N.H. Learning to Manage Populations
Employee Population Health Management: a stepping stone for accountable care Richard Boehler, MD, MBA, FACPE President and Chief Executive Officer St. Joseph Hospital, Nashua N.H. Learning to Manage Populations
Navigating CMS Incentive Programs for Eligible Professionals Why It Matters and What You Need to Know. Dr. Paul Mulhausen, CMO
 Navigating CMS Incentive Programs for Eligible Professionals Why It Matters and What You Need to Know Dr. Paul Mulhausen, CMO Objectives Better understand CMS Incentive Programs and payment adjustments
Navigating CMS Incentive Programs for Eligible Professionals Why It Matters and What You Need to Know Dr. Paul Mulhausen, CMO Objectives Better understand CMS Incentive Programs and payment adjustments
Arkansas Health Care Payment Improvement Initiative
 Arkansas Health Care Payment Improvement Initiative Joseph W. Thompson, MD, MPH Arkansas Surgeon General Director, Arkansas Center for Health Improvement Arkansas System Transformation Strategy Workforce
Arkansas Health Care Payment Improvement Initiative Joseph W. Thompson, MD, MPH Arkansas Surgeon General Director, Arkansas Center for Health Improvement Arkansas System Transformation Strategy Workforce
ACO Program: Quality Reporting Requirements. Jennifer Faerberg Mary Wheatley April 28, 2011
 ACO Program: Quality Reporting Requirements Jennifer Faerberg Mary Wheatley April 28, 2011 Agenda for Today s Call Overview Quality Reporting Requirements Benchmarks/Thresholds Scoring Model Scoring Methodology
ACO Program: Quality Reporting Requirements Jennifer Faerberg Mary Wheatley April 28, 2011 Agenda for Today s Call Overview Quality Reporting Requirements Benchmarks/Thresholds Scoring Model Scoring Methodology
Early Results of a Marketwide ACO Initiative: The Alternative Quality Contract (AQC)
") Early Results of a Marketwide ACO Initiative: The Alternative Quality Contract (AQC) Dana Gelb Safran, Sc.D. Senior Vice President Performance Measurement and Improvement 13 July 2011 Twin Goals of Improving
Early Results of a Marketwide ACO Initiative: The Alternative Quality Contract (AQC) Dana Gelb Safran, Sc.D. Senior Vice President Performance Measurement and Improvement 13 July 2011 Twin Goals of Improving
HEDIS/CAHPS 101. August 13, 2012 Minnesota Measurement and Reporting Workgroup
 HEDIS/CAHPS 101 Minnesota Measurement and Reporting Workgroup Objectives Provide introduction to NCQA Identify HEDIS/CAHPS basics Discuss various components related to HEDIS/CAHPS usage, including State
HEDIS/CAHPS 101 Minnesota Measurement and Reporting Workgroup Objectives Provide introduction to NCQA Identify HEDIS/CAHPS basics Discuss various components related to HEDIS/CAHPS usage, including State
Impact Intelligence. Flexibility. Security. Ease of use. White Paper
 Impact Intelligence Health care organizations continue to seek ways to improve the value they deliver to their customers and pinpoint opportunities to enhance performance. Accurately identifying trends
Impact Intelligence Health care organizations continue to seek ways to improve the value they deliver to their customers and pinpoint opportunities to enhance performance. Accurately identifying trends
Patient Centered Medical Home
 Patient Centered Medical Home 2013 2014 Program Overview Florida Blue is a trade name of Blue Cross and Blue Shield of Florida Inc., an Independent Licensee of the Blue Cross and Blue Shield Association.
Patient Centered Medical Home 2013 2014 Program Overview Florida Blue is a trade name of Blue Cross and Blue Shield of Florida Inc., an Independent Licensee of the Blue Cross and Blue Shield Association.
Brief Research Report: Fountain House and Use of Healthcare Resources
 ! Brief Research Report: Fountain House and Use of Healthcare Resources Zachary Grinspan, MD MS Department of Healthcare Policy and Research Weill Cornell Medical College, New York, NY June 1, 2015 Fountain
! Brief Research Report: Fountain House and Use of Healthcare Resources Zachary Grinspan, MD MS Department of Healthcare Policy and Research Weill Cornell Medical College, New York, NY June 1, 2015 Fountain
PIONEER ACO A REVIEW OF THE GRAND EXPERIMENT. Norris Vivatrat, MD Associate Medical Director Monarch HealthCare
 PIONEER ACO A REVIEW OF THE GRAND EXPERIMENT Norris Vivatrat, MD Associate Medical Director Monarch HealthCare 2 Agenda Pioneer ACO basics, performance and challenges Monarch HealthCare Post-acute network
PIONEER ACO A REVIEW OF THE GRAND EXPERIMENT Norris Vivatrat, MD Associate Medical Director Monarch HealthCare 2 Agenda Pioneer ACO basics, performance and challenges Monarch HealthCare Post-acute network
PIONEER ACO A REVIEW OF THE GRAND EXPERIMENT
 PIONEER ACO A REVIEW OF THE GRAND EXPERIMENT Norris Vivatrat, MD Associate Medical Director Monarch HealthCare 2 Agenda Pioneer ACO basics, performance and challenges Monarch HealthCare Post-acute network
PIONEER ACO A REVIEW OF THE GRAND EXPERIMENT Norris Vivatrat, MD Associate Medical Director Monarch HealthCare 2 Agenda Pioneer ACO basics, performance and challenges Monarch HealthCare Post-acute network
Mar. 31, 2011 (202) 690-6145. Improving Quality of Care for Medicare Patients: Accountable Care Organizations
 690-6145. Improving Quality of Care for Medicare Patients: Accountable Care Organizations") DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 Office of Media Affairs MEDICARE FACT SHEET FOR IMMEDIATE RELEASE
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 Office of Media Affairs MEDICARE FACT SHEET FOR IMMEDIATE RELEASE
2013 ACO Quality Measures
 ACO 1-7 Patient Satisfaction Survey Consumer Assessment of HealthCare Providers Survey (CAHPS) 1. Getting Timely Care, Appointments, Information 2. How well Your Providers Communicate 3. Patient Rating
ACO 1-7 Patient Satisfaction Survey Consumer Assessment of HealthCare Providers Survey (CAHPS) 1. Getting Timely Care, Appointments, Information 2. How well Your Providers Communicate 3. Patient Rating
Description of the OECD Health Care Quality Indicators as well as indicator-specific information
 Appendix 1. Description of the OECD Health Care Quality Indicators as well as indicator-specific information The numbers after the indicator name refer to the report(s) by OECD and/or THL where the data
Appendix 1. Description of the OECD Health Care Quality Indicators as well as indicator-specific information The numbers after the indicator name refer to the report(s) by OECD and/or THL where the data
Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION
 Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION At the end of this session, you will be able to: Identify ways RT skills can be utilized for
Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION At the end of this session, you will be able to: Identify ways RT skills can be utilized for
See page 331 of HEDIS 2013 Tech Specs Vol 2. HEDIS specs apply to plans. RARE applies to hospitals. Plan All-Cause Readmissions (PCR) *++
 *++") Hospitalizations Inpatient Utilization General Hospital/Acute Care (IPU) * This measure summarizes utilization of acute inpatient care and services in the following categories: Total inpatient. Medicine.
Hospitalizations Inpatient Utilization General Hospital/Acute Care (IPU) * This measure summarizes utilization of acute inpatient care and services in the following categories: Total inpatient. Medicine.
Medicare Shared Savings Program Quality Measure Benchmarks for the 2015 Reporting Year
 Medicare Shared Savings Program Quality Measure Benchmarks for the 2015 Reporting Year Release Notes/Summary of Changes (February 2015): Issued correction of 2015 benchmarks for ACO-9 and ACO-10 quality
Medicare Shared Savings Program Quality Measure Benchmarks for the 2015 Reporting Year Release Notes/Summary of Changes (February 2015): Issued correction of 2015 benchmarks for ACO-9 and ACO-10 quality
Care Coordination. The Embedded Care Manager. Presented by Thomas Decker, MD Mary Finnegan, BSN, M.Ed
 Care Coordination The Embedded Care Manager Presented by Thomas Decker, MD Mary Finnegan, BSN, M.Ed Goals of Care Management The goals of care Management are consistent with the Triple Aim: Improve population
Care Coordination The Embedded Care Manager Presented by Thomas Decker, MD Mary Finnegan, BSN, M.Ed Goals of Care Management The goals of care Management are consistent with the Triple Aim: Improve population
New York Presbyterian Innovations in Health Care Reform at Academic Medical Centers
 New York Presbyterian Innovations in Health Care Reform at Academic Medical Centers October 28, 2011 Timothy G Ferris, MD, MPH Mass General Physicians Organization, Medical Director Associate Professor,
New York Presbyterian Innovations in Health Care Reform at Academic Medical Centers October 28, 2011 Timothy G Ferris, MD, MPH Mass General Physicians Organization, Medical Director Associate Professor,
2013 MEDICARE FEE-FOR-SERVICE QUALITY AND RESOURCE USE REPORT
 2013 MEDICARE FEE-FOR-SERVICE QUALITY AND RESOURCE USE REPORT Sample Medical Practice Last Four Digits of Your Taxpayer Identification Number (TIN): 1530 ABOUT THIS REPORT FROM MEDICARE WHAT This Quality
2013 MEDICARE FEE-FOR-SERVICE QUALITY AND RESOURCE USE REPORT Sample Medical Practice Last Four Digits of Your Taxpayer Identification Number (TIN): 1530 ABOUT THIS REPORT FROM MEDICARE WHAT This Quality
MaineCare Value Based Purchasing Initiative
 MaineCare Value Based Purchasing Initiative The Accountable Communities Strategy Jim Leonard, Deputy Director, MaineCare Peter Kraut, Acting Accountable Communities Program Manager Why Value-Based Purchasing
MaineCare Value Based Purchasing Initiative The Accountable Communities Strategy Jim Leonard, Deputy Director, MaineCare Peter Kraut, Acting Accountable Communities Program Manager Why Value-Based Purchasing
Improving Quality of Care for Medicare Patients: Accountable Care Organizations
 DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Improving Quality of Care for Medicare Patients: FACT SHEET Overview http://www.cms.gov/sharedsavingsprogram On October
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Improving Quality of Care for Medicare Patients: FACT SHEET Overview http://www.cms.gov/sharedsavingsprogram On October
Achieving Quality and Value in Chronic Care Management
 The Burden of Chronic Disease One of the greatest burdens on the US healthcare system is the rapidly growing rate of chronic disease. These statistics illustrate the scope of the problem: Nearly half of
The Burden of Chronic Disease One of the greatest burdens on the US healthcare system is the rapidly growing rate of chronic disease. These statistics illustrate the scope of the problem: Nearly half of
HEDIS 2012 Results
 Capital District Physicians Health Plan, Inc. Nonprofit Health Plan Albany, New York Capital District Physicians Health Plan, Inc. (CDPHP ) is featured as a high performer in cardiovascular care, identified
Capital District Physicians Health Plan, Inc. Nonprofit Health Plan Albany, New York Capital District Physicians Health Plan, Inc. (CDPHP ) is featured as a high performer in cardiovascular care, identified
Accountable Care Organizations: Notice of Proposed Rulemaking
 Accountable Care Organizations: Notice of Proposed Rulemaking Presentation by: Pam Silberman, JD, DrPH North Carolina Institute of Medicine April 15, 2011 1 Accountable Care Organizations (ACOs) An ACO
Accountable Care Organizations: Notice of Proposed Rulemaking Presentation by: Pam Silberman, JD, DrPH North Carolina Institute of Medicine April 15, 2011 1 Accountable Care Organizations (ACOs) An ACO
RESEARCH BRIEF SICKER AND COSTLIER: HEALTHCARE UTILIZATION OF U.S. HOSPITAL EMPLOYEES
 RESEARCH BRIEF SICKER AND COSTLIER: HEALTHCARE UTILIZATION OF HOSPITAL EMPLOYEES AUGUST 2011 EXECUTIVE SUMMARY hospital workers are less healthy, consume more medical services, and accrue higher healthcare
RESEARCH BRIEF SICKER AND COSTLIER: HEALTHCARE UTILIZATION OF HOSPITAL EMPLOYEES AUGUST 2011 EXECUTIVE SUMMARY hospital workers are less healthy, consume more medical services, and accrue higher healthcare
Atrius Health ACO Initiative. Agenda
 Atrius Health ACO Initiative November 9, 2012 Mark Yurkofsky MD Mark_yurkofsky@vmed.org 11/13/2012 1 Agenda Why the interest in the Pioneer ACO? What actually is Pioneer ACO anyway? What is Atrius Health?
Atrius Health ACO Initiative November 9, 2012 Mark Yurkofsky MD Mark_yurkofsky@vmed.org 11/13/2012 1 Agenda Why the interest in the Pioneer ACO? What actually is Pioneer ACO anyway? What is Atrius Health?
Continuity of Care Guide for Ambulatory Medical Practices
 Continuity of Care Guide for Ambulatory Medical Practices www.himss.org t ra n sf o r m i ng he a lth c a re th rou g h IT TM Table of Contents Introduction 3 Roles and Responsibilities 4 List of work/responsibilities
Continuity of Care Guide for Ambulatory Medical Practices www.himss.org t ra n sf o r m i ng he a lth c a re th rou g h IT TM Table of Contents Introduction 3 Roles and Responsibilities 4 List of work/responsibilities
Risk Adjustment: Implications for Community Health Centers
 Risk Adjustment: Implications for Community Health Centers Todd Gilmer, PhD Division of Health Policy Department of Family and Preventive Medicine University of California, San Diego Overview Program and
Risk Adjustment: Implications for Community Health Centers Todd Gilmer, PhD Division of Health Policy Department of Family and Preventive Medicine University of California, San Diego Overview Program and
US Medicare Accountable Care Organizations (ACOs)
") James H Thrall MD Chairman Emeritus, Department of Radiology Massachusetts General Hospital Distinguished Juan M Taveras Professor of Radiology Harvard Medical School US Medicare Accountable Care Organizations
James H Thrall MD Chairman Emeritus, Department of Radiology Massachusetts General Hospital Distinguished Juan M Taveras Professor of Radiology Harvard Medical School US Medicare Accountable Care Organizations
ALBERTA S HEALTH SYSTEM PERFORMANCE MEASURES
 ALBERTA S HEALTH SYSTEM PERFORMANCE MEASURES 1.0 Quality of Health Services: Access to Surgery Priorities for Action Acute Care Access to Surgery Reduce the wait time for surgical procedures. 1.1 Wait
ALBERTA S HEALTH SYSTEM PERFORMANCE MEASURES 1.0 Quality of Health Services: Access to Surgery Priorities for Action Acute Care Access to Surgery Reduce the wait time for surgical procedures. 1.1 Wait
A partnership that offers an exclusive insurance product! The Chambers of Commerce in Hamilton County and ADVANTAGE Health Solutions, Inc.
 The Chambers of Commerce in Hamilton County and ADVANTAGE Health Solutions, Inc. SM A partnership that offers an exclusive insurance product! CHAMBER OF COMMERCE The Chambers of Commerce in Hamilton County
The Chambers of Commerce in Hamilton County and ADVANTAGE Health Solutions, Inc. SM A partnership that offers an exclusive insurance product! CHAMBER OF COMMERCE The Chambers of Commerce in Hamilton County
OUR ACO QUALITY RESULTS 2012 AND 2013
 OUR ACO QUALITY RESULTS 2012 AND 2013 2012-2013 Patient and Caregiver Experience Source 2012 2013 ACO - 1 CAHPS: Getting Timely Care, Appointments and Information Survey 81.98 84.47 ACO - 2 CAHPS: How
OUR ACO QUALITY RESULTS 2012 AND 2013 2012-2013 Patient and Caregiver Experience Source 2012 2013 ACO - 1 CAHPS: Getting Timely Care, Appointments and Information Survey 81.98 84.47 ACO - 2 CAHPS: How
Ambulatory Care Sensitive Emergency Department Visits Chronic Disease Conditions New Hampshire, 2001-2005. Background:
 Ambulatory Care Sensitive Emergency Department Visits Chronic Disease Conditions New Hampshire, 21-25 Background: Hospital Emergency Departments (ED) provide a spectrum of medical care, some of which for
Ambulatory Care Sensitive Emergency Department Visits Chronic Disease Conditions New Hampshire, 21-25 Background: Hospital Emergency Departments (ED) provide a spectrum of medical care, some of which for
Physician and other health professional services
 O n l i n e A p p e n d i x e s 4 Physician and other health professional services 4-A O n l i n e A p p e n d i x Access to physician and other health professional services 4 a1 Access to physician care
O n l i n e A p p e n d i x e s 4 Physician and other health professional services 4-A O n l i n e A p p e n d i x Access to physician and other health professional services 4 a1 Access to physician care
Report on comparing quality among Medicare Advantage plans and between Medicare Advantage and fee-for-service Medicare
 O N L I N E A P P E N D I X E S 6 Report on comparing quality among Medicare Advantage plans and between Medicare Advantage and fee-for-service Medicare 6-A O N L I N E A P P E N D I X Current quality
O N L I N E A P P E N D I X E S 6 Report on comparing quality among Medicare Advantage plans and between Medicare Advantage and fee-for-service Medicare 6-A O N L I N E A P P E N D I X Current quality
HOW TO UNDERSTAND YOUR QUALITY AND RESOURCE USE REPORT
 HOW TO UNDERSTAND YOUR QUALITY AND RESOURCE USE REPORT CONTENTS A BACKGROUND AND PURPOSE OF THE MID-YEAR QUALITY AND RESOURCE USE REPORTS... 1 B EXHIBITS INCLUDED IN THE MID-YEAR QUALITY AND RESOURCE USE
HOW TO UNDERSTAND YOUR QUALITY AND RESOURCE USE REPORT CONTENTS A BACKGROUND AND PURPOSE OF THE MID-YEAR QUALITY AND RESOURCE USE REPORTS... 1 B EXHIBITS INCLUDED IN THE MID-YEAR QUALITY AND RESOURCE USE
Accountable Care Fundamentals for Medical Practice Executives
 Accountable Care Fundamentals for Medical Practice Executives Nathan Anspach, FACMPE Senior Vice President and Chief Executive Officer John C. Lincoln Accountable Care Organization and John C. Lincoln
Accountable Care Fundamentals for Medical Practice Executives Nathan Anspach, FACMPE Senior Vice President and Chief Executive Officer John C. Lincoln Accountable Care Organization and John C. Lincoln
Quality Oversight in the Health Care Marketplace, Spring 2010 Tufts Health Care Institute
 Quality Oversight in the Health Care Marketplace, Spring 2010 Tufts Health Care Institute Session 16: C.1. Performance Reports National Reports Some reports present information on a category of providers
Quality Oversight in the Health Care Marketplace, Spring 2010 Tufts Health Care Institute Session 16: C.1. Performance Reports National Reports Some reports present information on a category of providers
kaiser medicaid commission on and the uninsured May 2009 Community Care of North Carolina: Putting Health Reform Ideas into Practice in Medicaid
 P O L I C Y B R I E F kaiser commission on medicaid SUMMARY and the uninsured Community Care of North Carolina: Putting Health Reform Ideas into Practice in Medicaid May 2009 Why is Community Care of North
P O L I C Y B R I E F kaiser commission on medicaid SUMMARY and the uninsured Community Care of North Carolina: Putting Health Reform Ideas into Practice in Medicaid May 2009 Why is Community Care of North
Building a Post Acute Network: Care Management and ACOs
 Building a Post Acute Network: Care Management and ACOs A high level summary of proposed rules for ACOs and the shared savings program most relevant to post acute providers. Prepared By: Kathleen M. Griffin,
Building a Post Acute Network: Care Management and ACOs A high level summary of proposed rules for ACOs and the shared savings program most relevant to post acute providers. Prepared By: Kathleen M. Griffin,
Appendix VI. Patient-Centered Medical Homes (Initiative Memorandum) APRIL 2013
 APRIL 2013") Appendix VI. Patient-Centered Medical Homes (Initiative Memorandum) APRIL 2013 http://berkeleyhealthcareforum.berkeley.edu 1 Appendix VI. Patient-Centered Medical Homes (Initiative Memorandum) See Appendix
Appendix VI. Patient-Centered Medical Homes (Initiative Memorandum) APRIL 2013 http://berkeleyhealthcareforum.berkeley.edu 1 Appendix VI. Patient-Centered Medical Homes (Initiative Memorandum) See Appendix
Coventry Health Care of Florida, Inc. Coventry Health Plan of Florida, Inc. Summit Health Plan of Florida
 Coventry Health Care of Florida, Inc. Coventry Health Plan of Florida, Inc. Summit Health Plan of Florida Medicare Quality Management Program Overview Quality Improvement (QI) Overview At Coventry, we
Coventry Health Care of Florida, Inc. Coventry Health Plan of Florida, Inc. Summit Health Plan of Florida Medicare Quality Management Program Overview Quality Improvement (QI) Overview At Coventry, we
Coventry Health Care of Florida, Inc. Coventry Health Plan of Florida, Inc. Coventry Health and Life Insurance Company Commercial Lines of Business
 Coventry Health Care of Florida, Inc. Coventry Health Plan of Florida, Inc. Coventry Health and Life Insurance Company Commercial Lines of Business Quality Management Program 2012 Overview Quality Improvement
Coventry Health Care of Florida, Inc. Coventry Health Plan of Florida, Inc. Coventry Health and Life Insurance Company Commercial Lines of Business Quality Management Program 2012 Overview Quality Improvement
Chapter Seven Value-based Purchasing
 Chapter Seven Value-based Purchasing Value-based purchasing (VBP) is a pay-for-performance program that affects a significant and growing percentage of Medicare reimbursement for medical providers. It
Chapter Seven Value-based Purchasing Value-based purchasing (VBP) is a pay-for-performance program that affects a significant and growing percentage of Medicare reimbursement for medical providers. It
Leveraging Big Data Improving Performance. University of Missouri Thomas J. Selva, M.D. - CMIO
 Leveraging Big Data Improving Performance University of Missouri Thomas J. Selva, M.D. - CMIO University Hospital and Clinics Ellis Fischel Cancer Center Women s and Children s Hospital Missouri Orthopaedic
Leveraging Big Data Improving Performance University of Missouri Thomas J. Selva, M.D. - CMIO University Hospital and Clinics Ellis Fischel Cancer Center Women s and Children s Hospital Missouri Orthopaedic
Employer-Sponsored Clinics & Telemedicine Onsite, Online, Anywhere!
 Employer-Sponsored Clinics & Telemedicine Onsite, Online, Anywhere! Presented By: Todd Wolf General Manager QuadMed Evolution Expected Benefits Scope of Services Delivery Models Feasibility Accountability
Employer-Sponsored Clinics & Telemedicine Onsite, Online, Anywhere! Presented By: Todd Wolf General Manager QuadMed Evolution Expected Benefits Scope of Services Delivery Models Feasibility Accountability
Accountable Care Organizations: Forging Stakeholder Partnerships for Health Care Performance and Efficiency
 Accountable Care Organizations: Forging Stakeholder Partnerships for Health Care Performance and Efficiency Julie Lewis Director of Health Policy Dartmouth Institute for Health Policy and Clinical Practice
Accountable Care Organizations: Forging Stakeholder Partnerships for Health Care Performance and Efficiency Julie Lewis Director of Health Policy Dartmouth Institute for Health Policy and Clinical Practice
Maximizing Limited Care Management Resources to Improve Clinical Quality and Ensure Safe Transitions
 Maximizing Limited Care Management Resources to Improve Clinical Quality and Ensure Safe Transitions Scott Flinn MD Deborah Schutz RN JD Fritz Steen RN Arch Health Partners A medical foundation formed
Maximizing Limited Care Management Resources to Improve Clinical Quality and Ensure Safe Transitions Scott Flinn MD Deborah Schutz RN JD Fritz Steen RN Arch Health Partners A medical foundation formed
Converting BIG Data into Value. Alan Krumholz MD, FAAP, DFACMQ
 Converting BIG Data into Value Alan Krumholz MD, FAAP, DFACMQ Disclosure Statement I have no financial COI issues to disclose Neither myself nor Mayo Clinic endorse any of the sponsors of this meeting
Converting BIG Data into Value Alan Krumholz MD, FAAP, DFACMQ Disclosure Statement I have no financial COI issues to disclose Neither myself nor Mayo Clinic endorse any of the sponsors of this meeting
Wasteful spending in the U.S. health care. Strategies for Changing Members Behavior to Reduce Unnecessary Health Care Costs
 Strategies for Changing Members Behavior to Reduce Unnecessary Health Care Costs by Christopher J. Mathews Wasteful spending in the U.S. health care system costs an estimated $750 billion to $1.2 trillion
Strategies for Changing Members Behavior to Reduce Unnecessary Health Care Costs by Christopher J. Mathews Wasteful spending in the U.S. health care system costs an estimated $750 billion to $1.2 trillion
Designing Care Management Programs to Improve Outcomes
 Designing Care Management Programs to Improve Outcomes Society of Actuaries June 13-15, 2007 Holly Michaels Fisher, Senior Consultant Reden & Anders SPH81Fisher Ingenix, Inc. 2 Traditional Components of
Designing Care Management Programs to Improve Outcomes Society of Actuaries June 13-15, 2007 Holly Michaels Fisher, Senior Consultant Reden & Anders SPH81Fisher Ingenix, Inc. 2 Traditional Components of
DELIVERING VALUE THROUGH TECHNOLOGY
 DELIVERING VALUE THROUGH TECHNOLOGY Mark Nelson, MD - EMR Physician Champion Krishna Ramachandran - Chief Information and Transformation Officer Karen Adamson - Director, Epic Clinical Applications DuPage
DELIVERING VALUE THROUGH TECHNOLOGY Mark Nelson, MD - EMR Physician Champion Krishna Ramachandran - Chief Information and Transformation Officer Karen Adamson - Director, Epic Clinical Applications DuPage
Accountable Care Organizations (ACOs): Potential to Foster Quality While Reducing Costs
: Potential to Foster Quality While Reducing Costs") Accountable Care Organizations (ACOs): Potential to Foster Quality While Reducing Costs Debra Ness Co-Chair, Consumer-Purchaser Disclosure Project President, National Partnership for Women & Families David
Accountable Care Organizations (ACOs): Potential to Foster Quality While Reducing Costs Debra Ness Co-Chair, Consumer-Purchaser Disclosure Project President, National Partnership for Women & Families David
Care and EHR Integration Connecting Physical and Behavioral Health in the EHR. Tarzana Treatment Centers Integrated Healthcare
 Care and EHR Integration Connecting Physical and Behavioral Health in the EHR Tarzana Treatment Centers Integrated Healthcare Outline of Presentation Why Integrate Care? Integrated Care at Tarzana Treatment
Care and EHR Integration Connecting Physical and Behavioral Health in the EHR Tarzana Treatment Centers Integrated Healthcare Outline of Presentation Why Integrate Care? Integrated Care at Tarzana Treatment
ESSENTIA HEALTH AS AN ACO (ACCOUNTABLE CARE ORGANIZATION)
") ESSENTIA HEALTH AS AN ACO (ACCOUNTABLE CARE ORGANIZATION) Hello and welcome. Thank you for taking part in this presentation entitled "Essentia Health as an ACO or Accountable Care Organization -- What
ESSENTIA HEALTH AS AN ACO (ACCOUNTABLE CARE ORGANIZATION) Hello and welcome. Thank you for taking part in this presentation entitled "Essentia Health as an ACO or Accountable Care Organization -- What
Little Ado (yet) About Much (money)
 About Much (money)") The Concentration of Health Care Spending: Little Ado (yet) About Much (money) Walter P Wodchis Peter Austin, Alice Newman, Ashley Corallo, David Henry Institute for Clinical Evaluative Sciences CAHSPR
The Concentration of Health Care Spending: Little Ado (yet) About Much (money) Walter P Wodchis Peter Austin, Alice Newman, Ashley Corallo, David Henry Institute for Clinical Evaluative Sciences CAHSPR
A VISION TO TRANSFORM U.S. HEALTH CARE. The programs to make it a reality.
 A VISION TO TRANSFORM U.S. HEALTH CARE. The programs to make it a reality. HCI 3 IMPROVING HEALTH CARE QUALITY AND VALUE with evidence-based incentive programs and a fair and powerful model for payment
A VISION TO TRANSFORM U.S. HEALTH CARE. The programs to make it a reality. HCI 3 IMPROVING HEALTH CARE QUALITY AND VALUE with evidence-based incentive programs and a fair and powerful model for payment
Johns Hopkins HealthCare LLC: Care Management and Care Coordination for Chronic Diseases
 Johns Hopkins HealthCare LLC: Care Management and Care Coordination for Chronic Diseases Epidemiology Over 145 million people ( nearly half the population) - suffer from asthma, depression and other chronic
Johns Hopkins HealthCare LLC: Care Management and Care Coordination for Chronic Diseases Epidemiology Over 145 million people ( nearly half the population) - suffer from asthma, depression and other chronic
Performance Measurement for the Medicare and Medicaid Eligible (MME) Population in Connecticut Survey Analysis
 Population in Connecticut Survey Analysis") Performance Measurement for the Medicare and Medicaid Eligible (MME) Population in Connecticut Survey Analysis Methodology: 8 respondents The measures are incorporated into one of four sections: Highly
Performance Measurement for the Medicare and Medicaid Eligible (MME) Population in Connecticut Survey Analysis Methodology: 8 respondents The measures are incorporated into one of four sections: Highly
2014 Summary of benefits plan comparison
 2014 Summary of benefits plan comparison The tables below summarize the 2014 Benefits for the Samaritan Choice Medical Plan options (Basic, Wellness and High-Deductible Plans). Pease refer to your plan
2014 Summary of benefits plan comparison The tables below summarize the 2014 Benefits for the Samaritan Choice Medical Plan options (Basic, Wellness and High-Deductible Plans). Pease refer to your plan
Value-Based Health Care Reimbursement Programs
 Value-Based Health Care Reimbursement Programs Table of Contents Introduction to Florida Blue Value-Based Health Care Programs... 1 General Questions and Answers Regarding... 6 Q1. Why create value-based
Value-Based Health Care Reimbursement Programs Table of Contents Introduction to Florida Blue Value-Based Health Care Programs... 1 General Questions and Answers Regarding... 6 Q1. Why create value-based
OBJECTIVES AGING POPULATION AGING POPULATION AGING IMPACT ON MEDICARE AGING POPULATION
 OBJECTIVES Kimberly S. Hodge, PhDc, MSN, RN, ACNS-BC, CCRN- K Director, ACO Care Management & Clinical Nurse Specialist Franciscan ACO, Inc. Central Indiana Region Indianapolis, IN By the end of this session
OBJECTIVES Kimberly S. Hodge, PhDc, MSN, RN, ACNS-BC, CCRN- K Director, ACO Care Management & Clinical Nurse Specialist Franciscan ACO, Inc. Central Indiana Region Indianapolis, IN By the end of this session
Focus on preventable admissions
 Trends in emergency admissions for ambulatory care sensitive conditions, 2001 to 2013 Ian Blunt October 2013 About this work programme This QualityWatch Focus On report examines trends in emergency admissions
Trends in emergency admissions for ambulatory care sensitive conditions, 2001 to 2013 Ian Blunt October 2013 About this work programme This QualityWatch Focus On report examines trends in emergency admissions
National Survey of Physician Organizations and the Management of Chronic Illness II (Medical Groups) NOT FOR EXTERNAL DISTRIBUTION OR USE IN ANY FORM
 NOT FOR EXTERNAL DISTRIBUTION OR USE IN ANY FORM") If you want to use all or part of this questionnaire, please contact Patty Ramsay (email: pramsay@berkeley.edu; phone: 510/643-8063; mail: Patty Ramsay, University of California, SPH/HPM, 50 University
If you want to use all or part of this questionnaire, please contact Patty Ramsay (email: pramsay@berkeley.edu; phone: 510/643-8063; mail: Patty Ramsay, University of California, SPH/HPM, 50 University
Electronic Health Record (EHR) Data Analysis Capabilities
 Data Analysis Capabilities") Electronic Health Record (EHR) Data Analysis Capabilities January 2014 Boston Strategic Partners, Inc. 4 Wellington St. Suite 3 Boston, MA 02118 www.bostonsp.com Boston Strategic Partners is uniquely positioned
Electronic Health Record (EHR) Data Analysis Capabilities January 2014 Boston Strategic Partners, Inc. 4 Wellington St. Suite 3 Boston, MA 02118 www.bostonsp.com Boston Strategic Partners is uniquely positioned
Ohio Health Homes Learning Community Meeting. Overview of Health Homes Measures
 Ohio Health Homes Learning Community Meeting Overview of Health Homes Measures Tuesday, March 5, 2013 Presenter: Amber Saldivar, MHSM Associate Director, Informatics Analysis Health Services Advisory Group,
Ohio Health Homes Learning Community Meeting Overview of Health Homes Measures Tuesday, March 5, 2013 Presenter: Amber Saldivar, MHSM Associate Director, Informatics Analysis Health Services Advisory Group,
Small Physician Groups Aim High
 Small Physician Groups Aim High Arch Health Partners A medical foundation in San Diego formed by Palomar Health and PIMG, a 20 year old multispecialty medical group formerly known as Centre for Health
Small Physician Groups Aim High Arch Health Partners A medical foundation in San Diego formed by Palomar Health and PIMG, a 20 year old multispecialty medical group formerly known as Centre for Health
It Takes Two to ACO A Unique Management Partnership
 AMGA 2014 Annual Conference, April 4, 2014 It Takes Two to ACO A Unique Management Partnership Scott Hayworth MD, President & CEO Mount Kisco Medical Group Alan Bernstein MD, Senior Medical Director Mount
AMGA 2014 Annual Conference, April 4, 2014 It Takes Two to ACO A Unique Management Partnership Scott Hayworth MD, President & CEO Mount Kisco Medical Group Alan Bernstein MD, Senior Medical Director Mount
Accountable Care Organizations: What Are They and Why Should I Care?
 Accountable Care Organizations: What Are They and Why Should I Care? Adrienne Green, MD Associate Chief Medical Officer, UCSF Medical Center Ami Parekh, MD, JD Med. Director, Health System Innovation,
Accountable Care Organizations: What Are They and Why Should I Care? Adrienne Green, MD Associate Chief Medical Officer, UCSF Medical Center Ami Parekh, MD, JD Med. Director, Health System Innovation,
Benefit Design and ACOs: How Will Private Employers and Health Plans Proceed?
 Benefit Design and ACOs: How Will Private Employers and Health Plans Proceed? Accountable Care Organizations: Implications for Consumers October 14, 2010 Washington, DC Sam Nussbaum, M.D. Executive Vice
Benefit Design and ACOs: How Will Private Employers and Health Plans Proceed? Accountable Care Organizations: Implications for Consumers October 14, 2010 Washington, DC Sam Nussbaum, M.D. Executive Vice
STATISTICAL BRIEF #151
 HEALTHCARE COST AND UTILIZATION PROJECT STATISTICAL BRIEF #151 Agency for Healthcare Research and Quality March 2013 Trends in Potentially Preventable Hospital Admissions among Adults and Children, 2005
HEALTHCARE COST AND UTILIZATION PROJECT STATISTICAL BRIEF #151 Agency for Healthcare Research and Quality March 2013 Trends in Potentially Preventable Hospital Admissions among Adults and Children, 2005
RISK SELECTION IN THE MASSACHUSETTS STATE EMPLOYEE HEALTH INSURANCE PROGRAM. Running Title: Risk Selection in Health Insurance. Wei Yu, Ph.D.
 RISK SELECTION IN THE MASSACHUSETTS STATE EMPLOYEE HEALTH INSURANCE PROGRAM Running Title: Risk Selection in Health Insurance Wei Yu, Ph.D. 1 Randall P. Ellis, Ph.D. 2 Arlene Ash, Ph.D. 3 1 Health Economics
RISK SELECTION IN THE MASSACHUSETTS STATE EMPLOYEE HEALTH INSURANCE PROGRAM Running Title: Risk Selection in Health Insurance Wei Yu, Ph.D. 1 Randall P. Ellis, Ph.D. 2 Arlene Ash, Ph.D. 3 1 Health Economics
CMS Proposals for Quality Reporting Programs under the 2015 Medicare Physician Fee Schedule Proposed Rule. July 24, 2014
 CMS Proposals for Quality Reporting Programs under the 2015 Medicare Physician Fee Schedule Proposed Rule July 24, 2014 Medicare Learning Network This MLN Connects National Provider Call (MLN Connects
CMS Proposals for Quality Reporting Programs under the 2015 Medicare Physician Fee Schedule Proposed Rule July 24, 2014 Medicare Learning Network This MLN Connects National Provider Call (MLN Connects
Performance Measurement in CMS Programs Kate Goodrich, MD MHS Director, Quality Measurement and Health Assessment Group, CMS
 Performance Measurement in CMS Programs Kate Goodrich, MD MHS Director, Quality Measurement and Health Assessment Group, CMS Mind the Gap: Improving Quality Measures in Accountable Care Systems October
Performance Measurement in CMS Programs Kate Goodrich, MD MHS Director, Quality Measurement and Health Assessment Group, CMS Mind the Gap: Improving Quality Measures in Accountable Care Systems October
Improving Quality of Care for Medicare Patients: Accountable Care Organizations
 DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Improving Quality of Medicare Patients: Overview The Centers for Medicare & Medicaid Services (), an agency within the Department
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Improving Quality of Medicare Patients: Overview The Centers for Medicare & Medicaid Services (), an agency within the Department
An Integrated, Holistic Approach to Care Management Blue Care Connection
 An Integrated, Holistic Approach to Care Management Blue Care Connection With health care costs continuing to rise, both employers and health plans need innovative solutions to help employees manage their
An Integrated, Holistic Approach to Care Management Blue Care Connection With health care costs continuing to rise, both employers and health plans need innovative solutions to help employees manage their
The role of t he Depart ment of Veterans Affairs (VA) as
 as") The VA Health Care System: An Unrecognized National Safety Net Veterans who use the VA health care system have a higher level of illness than the general population, and 60 percent have no private or Medigap
The VA Health Care System: An Unrecognized National Safety Net Veterans who use the VA health care system have a higher level of illness than the general population, and 60 percent have no private or Medigap
PRIMARY CARE MEASUREMENT INITIATIVE
 PRIMARY CARE MEASUREMENT INITIATIVE March 2014 Promoting and improving patient safety and health service quality across Alberta. TABLE OF CONTENTS EXECUTIVE SUMMARY... 3 INTRODUCTION... 4 Primary care...
PRIMARY CARE MEASUREMENT INITIATIVE March 2014 Promoting and improving patient safety and health service quality across Alberta. TABLE OF CONTENTS EXECUTIVE SUMMARY... 3 INTRODUCTION... 4 Primary care...
The Hypertherm Associate Wellness Center (HAWC)
") The The New England Chapter of the ESOP Association Spring 2015 Meeting Christopher DeClerk, Director of Total Rewards April 3, 2015 P L A S M A L A S E R W A T E R J E T A U T O M A T I O N S O F T W
The The New England Chapter of the ESOP Association Spring 2015 Meeting Christopher DeClerk, Director of Total Rewards April 3, 2015 P L A S M A L A S E R W A T E R J E T A U T O M A T I O N S O F T W
New Hampshire Accountable Care Project: Analytic Report User Guide
 New Hampshire Accountable Care Project: Analytic Report User Guide November 2015 Contents OVERVIEW... 2 Introduction... 2 User Guide Purpose... 2 USING THE ANALYTIC REPORT... 3 Report Access... 3 Report
New Hampshire Accountable Care Project: Analytic Report User Guide November 2015 Contents OVERVIEW... 2 Introduction... 2 User Guide Purpose... 2 USING THE ANALYTIC REPORT... 3 Report Access... 3 Report
The Evolution of UnitedHealth Premium
 The Evolution of UnitedHealth Premium Power to transform heath care delivery Why We Do What We Do? Achieving the The Triple Aim! The root of the problem in
The Evolution of UnitedHealth Premium Power to transform heath care delivery Why We Do What We Do? Achieving the The Triple Aim! The root of the problem in
Welcome The AAMC, UHC and FPSC Web Conference on 2014 PQRS Proposed Changes will begin shortly.
 Welcome The AAMC, UHC and FPSC Web Conference on 2014 PQRS Proposed Changes will begin shortly. Please do not place your phones on hold. If you need to leave the event, hang up and dial back into the conference.
Welcome The AAMC, UHC and FPSC Web Conference on 2014 PQRS Proposed Changes will begin shortly. Please do not place your phones on hold. If you need to leave the event, hang up and dial back into the conference.
Explanation of CMS Proposed Performance Measurement Framework for ACOs and Comparison with IHA P4P Measure Set April 2011
 Explanation of CMS Proposed Performance ment Framework for ACOs and Comparison with IHA P4P Set April 2011 This briefing outlines Section II E ( and Other Reporting Requirements) of the Shared Savings
Explanation of CMS Proposed Performance ment Framework for ACOs and Comparison with IHA P4P Set April 2011 This briefing outlines Section II E ( and Other Reporting Requirements) of the Shared Savings
How To Earn Shared Savings From An Insurance Program
 Commercial Business Medical Cost Target Measurement Period Handbook- For Enhanced Personal Health Care Measurement Period beginning: 01/01/16 CBMCT Version 010116 V1 Introduction: Welcome to your Commercial
Commercial Business Medical Cost Target Measurement Period Handbook- For Enhanced Personal Health Care Measurement Period beginning: 01/01/16 CBMCT Version 010116 V1 Introduction: Welcome to your Commercial
T h e M A RY L A ND HEALTH CARE COMMISSION
 T h e MARYLAND HEALTH CARE COMMISSION Discussion Topics Overview Learning Objectives Electronic Health Records Health Information Exchange Telehealth 2 Overview - Maryland Health Care Commission Advancing
T h e MARYLAND HEALTH CARE COMMISSION Discussion Topics Overview Learning Objectives Electronic Health Records Health Information Exchange Telehealth 2 Overview - Maryland Health Care Commission Advancing
Project Option 1.6.2 - C11 UT Health Nurse-line Medical Triage Call Center - Enhance Urgent Medical Advice
 Project Option 1.6.2 - C11 UT Health Nurse-line Medical Triage Call Center - Enhance Urgent Medical Advice Unique RHP Project Identification Number: 111810101.1.5 Performing Provider Name/TPI: UTHealth,
Project Option 1.6.2 - C11 UT Health Nurse-line Medical Triage Call Center - Enhance Urgent Medical Advice Unique RHP Project Identification Number: 111810101.1.5 Performing Provider Name/TPI: UTHealth,
CMS Innovation Center Improving Care for Complex Patients
 CMS Innovation Center Improving Care for Complex Patients ECRI Institute Dr. Patrick Conway, M.D., MSc CMS Chief Medical Officer and Deputy Administrator for Innovation and Quality Director, Center for
CMS Innovation Center Improving Care for Complex Patients ECRI Institute Dr. Patrick Conway, M.D., MSc CMS Chief Medical Officer and Deputy Administrator for Innovation and Quality Director, Center for
Kaiser Permanente: Integration, Innovation, and Information Systems in Health Care
 Kaiser Permanente: Integration, Innovation, and Information Systems in Health Care October 2012 Molly Porter, Director Kaiser Permanente International molly.porter@kp.org kp.org/international Copyright
Kaiser Permanente: Integration, Innovation, and Information Systems in Health Care October 2012 Molly Porter, Director Kaiser Permanente International molly.porter@kp.org kp.org/international Copyright
Integrated Care. C.E. Reed and Associates Presentation by Penny Black and Kathy Leitch, Partners October 20, 2011
 Integrated Care C.E. Reed and Associates Presentation by Penny Black and Kathy Leitch, Partners October 20, 2011 Why integrated care? Federal Perspectives on Dual Eligibles 9.2 million people (2008) eligible
Integrated Care C.E. Reed and Associates Presentation by Penny Black and Kathy Leitch, Partners October 20, 2011 Why integrated care? Federal Perspectives on Dual Eligibles 9.2 million people (2008) eligible
Disease Management Identifications and Stratification Health Risk Assessment Level 1: Level 2: Level 3: Stratification
 Disease Management UnitedHealthcare Disease Management (DM) programs are part of our innovative Care Management Program. Our Disease Management (DM) program is guided by the principles of the UnitedHealthcare
Disease Management UnitedHealthcare Disease Management (DM) programs are part of our innovative Care Management Program. Our Disease Management (DM) program is guided by the principles of the UnitedHealthcare
Chapter Three Accountable Care Organizations
 Chapter Three Accountable Care Organizations One of the most talked-about changes in health care delivery in recent decades is Accountable Care Organizations, or ACOs. Having gained the attention of both
Chapter Three Accountable Care Organizations One of the most talked-about changes in health care delivery in recent decades is Accountable Care Organizations, or ACOs. Having gained the attention of both