Evaluation and Treatment of Sacral Somatic Dysfunction
|
|
|
- Katherine Merritt
- 7 years ago
- Views:
Transcription
1 Evaluation and Treatment of Sacral Somatic Dysfunction Diagnosis and Treatment of Sacral Somatic Dysfunction, with Indirect,Direct and HVLA Techniques (Counterstrain and Muscle Energy) F. P Wedel, D.O. Associate Adjunct Professor in Osteopathic Principles and Practice A.T. Still University School of Osteopathic Medicine in Arizona

2 Learning Objectives Review the following diagnostic and treatment techniques related to sacral somatic dysfunction: Lumbosacral spring test Sacral palpation Respiratory motion test Seated flexion test Sacral somatic dysfunctions see table Clinical presentations applicable to sacral diagnosis and treatment Techniques for sacral somatic dysfunction

3 Sacral Techniques Covered: 1. Supine, indirect, respiratory cooperation, for bilateral flexion - 2. Supine, direct, muscle energy, for bilateral flexion - 3. Prone, direct, respiratory cooperation, for bilateral extension - Supine, indirect, respiratory cooperation, for bilateral extension- Prone, direct, LVMA, for sacral rotation on same axis (anterior torsions)- 4. Prone, direct, muscle energy, for sacral rotation on same axis (anterior torsions)-prone, direct, LVMA, for unilateral flexion (shear) - Prone, direct, LVMA, for unilateral extension (shear) 5. HVLA for Anterior and Posterior sacral torsions
- 4.")
4 Sacral Clinical Presentations Presentations commonly associated with sacral somatic dysfunction and/or benefiting from correction of that dysfunction: Low back pain traumatic history Status Post Labor History of difficult labor Constipation Menstrual cramps / dysfunction Prostate dysfunction

5 BACKGROUND SACRAL STRUCTURE,LIGAMENTS AND MUSCLES

6 THE SACRUM Means sacred because of its density it is the last bone to decay and because it protects the reproductive system

7

8 Forces on the sacrum Angle of the sacroiliac joint wedges the sacrum in an anterior direction Prevents posterior movement Dorsal (posterior) sacroiliac ligaments much stronger than anterior sacroiliac ligaments Purpose: counteract significant pelvic forces pushing apex posteriorly.

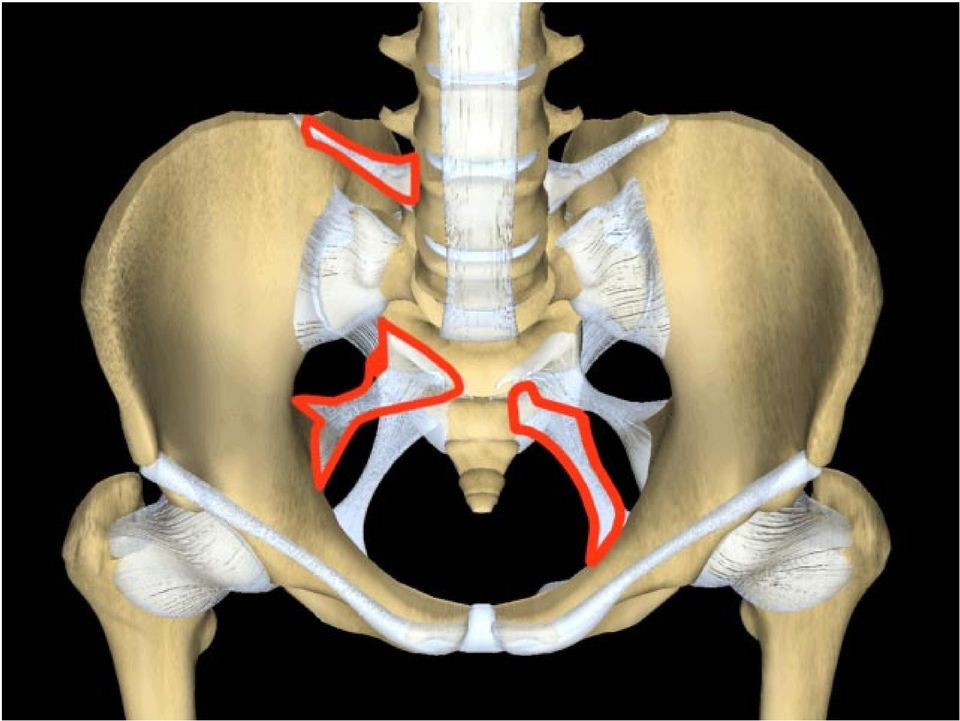
9 Major Pelvic Ligaments Iliolumbar from ilia to 5 th lumbar vertebrae Sacrospinous Sacrum to spine of the ischium Sacrotuberous Sacrum to ischial tuberosity Sacroiliac Ligament Covers much of the sacroiliac joint, ant & post

10 Iliolumbar ligaments Stabilizes the 5th (4th) Lumbar vertebrae to the ilia
 Lumbar")
11 Wedging of the sacrum creates an anterior force

12 Iliolumbar lig Sacrospinous
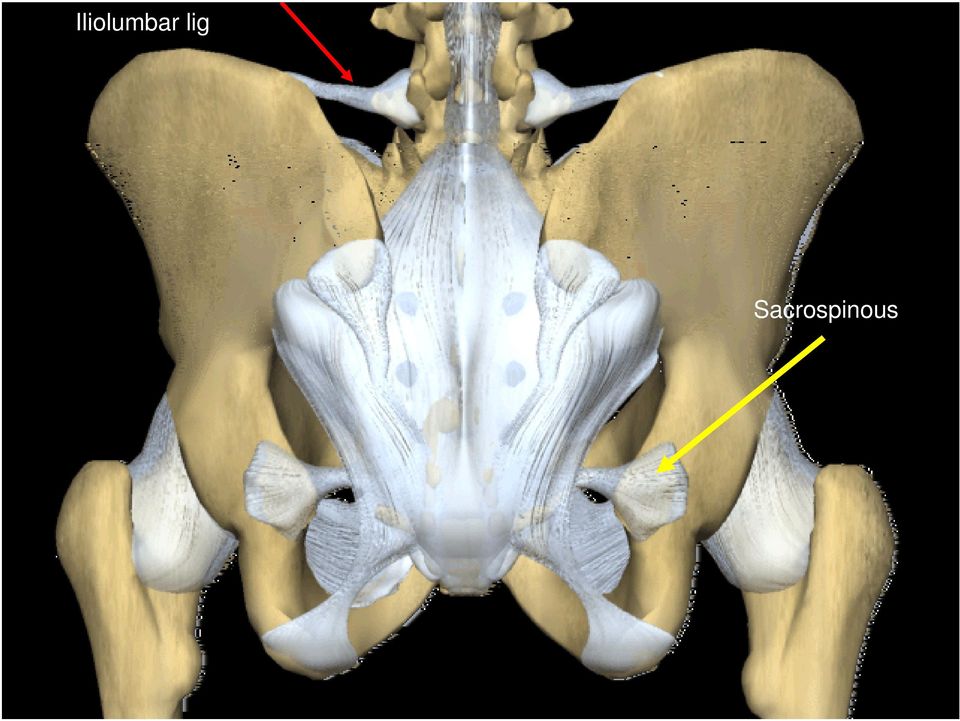
13 Sacrotuberous Ligament Runs from lower sacral tubercles to ischial tuberosity Gluteus maximus attachment Tendon of the biceps femoris attachment Connects with fascia of the pelvis from sacrum to ischial tuberosity stabilizes anterior motion

14 Sacrospinous ligament Sacrotuberous ligament

15
16 Both Sacrospinous & Sacrotuberous stabilize to prevent posterior - superior rotation of the sacral apex around a transverse axis

17 Sacroiliac Ligament Sacroiliac actually three ligaments Anterior or ventral sacroiliac from 3rd sacral segment to lateral preauricular sulcus interosseous sacroiliac massive bond between the upper parts of the joint dorsal sacroiliac Partly covers the interosseous, from lateral sacral crest to PSIS and internal iliac crest.

18 Ventral/Anterior Sacroiliac

19 Sacroiliac Ligament

20 interosseous Posterior sacroiliac

21
22 Pelvic muscle attachments from above. Posterior Muscular Attachments Attach to Sacrum Erector Spinae Iliocostalis Longissimus Erector Spinae Multifidus Attach to Innominates Obliques (internal, external, transverse) Quadratus Lumborum
23 Posterior Muscles
24 Iliocostalis
25 Longissimus
26 Erector Spinae (sacrospinalis)
27
28 Terminal Attachment of S 1 the Spinal Dura S 2 S 3 S 4 S 5
29 Multiple axes of motion: Transverse (3) Superior S1 Middle S2 Inferior S3 Vertical (sagittal) A/P Oblique (2) Left Right Sacral Axes
30 SACRAL ANATOMICAL AXIS Transverse axis Superior: the cranial&primary respiratory mechanism creates motion around this axis Middle: sacral base anterior and posterior (FB/BB) occur around this axis Inferior: the innominates rotate around this axis
31
32 SACRAL PHYSIOLOGIC AXIS Oblique: both left and right oblique axes are named for the superior pole Sagittal: includes both mid-sagittal and an infinite number of parasagittal axes Horizontal: functional axis of sacral flexion/extension occur around this axis (analogous to the middle transverse axis above)
33 (footnote on functional anatomy) Why are the Oblique Axes so significant? They are the Axes of Walking.
34 The walking cycle as it applies to our discussion 1. From a standing (neutral) position, when you take a step forward, your weight is shifted onto one lower extremity. 2. This induces spinal column SB to the weight bearing side, and pins the upper pole of the sacrum on the side of the SB. 3. As the free lower extremity swings forward, it carries the free pole of the sacrum anterior, creating rotation of the sacrum about the Oblique Axis, towards the weight bearing extremity. Ex.: R L on LOA R R on ROA Bottom Line: You form Oblique Axes with every step you take!
35 TESTS
36 To make a Sacral Diagnosis you will need to know the following: Static (Pure) Landmarks Sacral base - Ant/ Post ILA -Ant/Post ASIS & PSIS -Sup./Inf. Pubes -Sup./Inf & Ant./Post Mixed Landmarks Sacral Sulcus - Deep/Shallow STL - Tight/ Loose/ Equal Motion Testing Spring test L5 Sacrum
37
38 Record Positive Right, Positive Left, or Negative Test
39 Most of those pieces we have discussed, except... There is one that we have not talked much about yet. The Spring Test. It s purpose: To be an indicator of whether you are dealing with a sacral Oblique Axis that is a: Forward Torsion (Neutral) or Backward Torsion (Non-Neutral). Vs.
40 Spring Test 1. Find sacral base 2. Place heel of hand over Lumbosacral junction 3. Spring in an Anterior motion 4. Results: a. Positive test = If there is NO springing allowed = Non-neutral condition (AKA Backward torsion) b. Negative test = If there is springing allowed = Neutral condition.
41 Prone Landmarks
42 Judge whether the tip of the thumb is more anterior on one side than the tip of the thumb on the other side. Can also bring index fingers over onto sacral base and take measurement on the lateralized side. Record which base is anterior. Sacral Base
43 Palpable groove just medial to PSIS. Space between sacral spines and lateral sacral crest. Place thumbs in inferior border of PSIS. Move ½-1 up and medial to PSIS. Push thumb tips on sacral base. Pads of thumbs are on ilium and tips on sacral base. Measure the depth of each sacral sulcus relative to opposite sulcus? Record even, deep, or shallow, comparing one side to the other. Both sides may be shallow or deep as well. Sacral Sulcus Depth
44 Inferior Lateral Angle 1. Place flat of hand over sacrum near its caudal end and identify the coccyx. 2. Thumbs approximately 1 apart. Place thumbs in gluteal area about 1 caudal and on each side of coccyx. 3. Push thumbs cephalad until pads rest on inferior margin of ILA. Take a reading on the lateralized side: Inferior or superior? Possibly even? 4. Move thumbs approximately 1 cephalad from the inferior margin of the ILAs and place the pads of the thumbs over the posterior surface of the ILAs near the apex of the sacrum. 5. Use moderate equal pressure & judge if one side is more anterior or posterior than the other one or are they equal? Record on the lateralized side.
45 1. Place thumbs on the inferior margin of ILA. 2. Move thumbs inferiorly and laterally from the ILA bilaterally, palpating for the sacrotuberous ligament. 3. Ligament will be found between the ILA and the ischial tuberosity on each side. 4. Press thumbs anteriorly, superiorly, and degrees laterally to check the tension on the sacrotuberous ligaments. 5. Are they equal in tension or is one tighter or looser than the other? Note which side is looser and which is tighter, relative to the other side. Sacrotuberous Ligament
46 L5 Locate L5 transverse processes, bilaterally Place thumbs over L5 transverse processes, bilaterally Note relative positions of L5 transverse processes bilaterally Which is anterior? Which is posterior? What is the preference of motion at L5 for Rotation? Record the Rotation of L5, Right, Left, or No Rotation
47 Motion Tests for Sacral Diagnosis
48 Lumbosacral Spring Test Patient Prone Physician at Side of Table Place Heel of Hand over Lumbosacral Junction (L5-S1) Keep arms straight, and lean with body Spring Several Times Negative Test is a Mobility to Springing (motion is felt at joint) extension restriction Positive Test is Restriction to Anterior Springing (absent or restricted springing) flexion restriction
49
50 Hip Flop
51 ASIS Compression Test Have the patient lie supine. The patient is then asked to raise his/her bottom up off the table and then set it back down again. Doctor Stands with head and shoulders centered over the patient. Contact the ASIS Stabilize one ASIS while applying pressure at a 45 degree angle to the other ASIS Positive test - restricted movement of the Sacroiliac joint -> rock like motion Negative test - a sense of give or resilience => bounce or spring like motion
52 ASIS compression test figure Approx. 45 degree angle Stabilization Aim toward SI Joint Positive - Resistance to compression (or a lack of spring)
53 DIAGNOSIS AND TREATMENT
54 Yes Sacral Dysfunction Assessment Are ILA s Symmetric Superior/Inferior? No Physiologic: Oblique Axis: Sacral Torsions Non - physiologic: Upslipped Innominate Unilateral Sacral Shear (Unilateral Sacral Flexion) Is the Sacral Base Symmetric Anterior /Posterior? No Yes Sacral Base Posterior Sacral Base Anterior Sacral Margin Posterior Neutral Sacrum
55
56 Sacral Base Anterior-synonyms (several terms describing the same motion) Sagittal Plane-Middle Transverse Axis Bilateral Sacral Flexion Kimberly manual 2006, p. 193 ( A-E) (different than the sacral flexion & extension in the Magoun-type cranial field model) Nutation From the Latin nutare - to nod Nutated Sacrum Anterior Nutation
57 Sacral Base Anterior: Base bilat. anterior on the middle transverse axis Name: Sacral Base Anterior, Or bilat. Sacral Flexion, Or Nutation Landmarks: Sacral Base: Bilat. Anterior Sacral Sulcus: Bilat. Deep ILA: Bilat. Posterior STL: Bilat. Tight Motion: Sacral Base: Bilat. + ILA: Bilat. A + A+ Deep Deep P - P-
58 Sacral Base Anterior (Bilateral Sacral Flexion) Inferolateral angles level Sulci deep bilaterally Sacral base anterior bilaterally Sacrotuberous ligaments tight bilaterally Base anterior springing present Apex anterior springing restricted Look for discontinuity at the lumbo-sacral junction
59
60 Supine, indirect, respiratory cooperation, for bilateral flexion C
61
62
63 Sacral Base Posterior-synonyms Sagittal Plane-Middle Transverse Axis Bilateral Sacral Extension Kimberly manual 2006, p. 197 ( A-C) (different than sacral flexion & extension in the Magoun-type cranial field model) Counter Nutation Posterior Nutation
64 Sacral Base Posterior: Base bilat. posterior on the middle transverse axis Name: Sacral Base Posterior, Bilat. sacral extension,or Counternutation Landmarks: Sacral Base: Bilat. Posterior Sacral Sulcus: Bilat. Shallow ILA: Bilat. Anterior STL: Bilat. Loose Motion: Sacral Base: Bilat. ILA: Bilat. + P - P- Shallow A + A+ Shallow
65 Sacral Base Posterior (Bilateral Sacral Extension) Inferolateral angles level Sulci shallow bilaterally Sacral base posterior bilaterally Sacrotuberous ligaments relaxed bilaterally Apex anterior springing present Base anterior springing restricted
66
67
68
69 SACRAL MECHANICS Physiologic diagnoses of the sacrum occur in neutral and non-neutral mechanics:
70 Neutral Mechanics a.k.a. or or Left rotation on a Left Oblique Axis Forward Torsion Sacral Nutation (all three are equivalent terms!!) In neutral mechanics, the sacrum rotates in the same direction as the oblique axis (left rotation on a left oblique axis)
71 Non-neutral Mechanics a.k.a. or or Right rotation on a Left Oblique Axis Backward Torsion Sacral Counter-Nutation (all three are equivalent terms!!) In non-neutral mechanics, the sacrum rotates in the opposite direction of the oblique axis (right rotation on a left oblique axis)
72 Lumbosacral motion Lumbar spine and sacrum rotate in OPPOSITE directions Neutral (type I) mechanics: Example: L on LOA, the right sacral base moves anteriorly while L5 is S L R R In non-neutral (type 2) mechanics, the sacral base rotates backwards Example: R on LOA, the right sacral base moves posteriorly while L5 is R L S L
73 Lumbosacral Mechanics Example L rotation on LOA Lumbar spine neutral: S L R R (note in all torsions, L5 will rotate opposite of sacrum) Requires normal lordosis Occurs when (R) sacral base rotates anterior ( forward ) and does not rotate back (feels springy ) left ILA posterior, & inferior S L R R A L on LOA P
74
75 L5 Sacrum Relationship
76 There are 2 types of Sacral Oblique Axis Dysfunctions. Neutral & NonNeutral Let s start with Neutral Dysfunctions. Left Midline Right
77
78 Neutral - Left Oblique Axis Findings Name: L on LOA, R L on LOA, L Forward Torsion Landmarks Static: Sacral Base: L posterior Sacral Sulcus: L shallow ILA: L Post/ Inf. STL: L Tight Motion Testing: Spring: - (neg) L5: S L R R L5: S L R R Sacral Base L - R + ILA: L +/- R +/- P +/- A + Left Midline Right
79 Neutral - Right Oblique Axis Findings: A+ Name: R on ROA, R R on ROA, R Forward Torsion Landmarks Static: Sacral Base: R posterior Sacral Sulcus: R shallow ILA: R Post/Inf. STL: R tight Motion Testing: Spring: - (neg) L5: S R R L Sacral Base: L + R - ILA: L +/- R +/- P +/- Left Right Midline Right Forward Torsion R R on ROA
80 Palpatory Experience We can induce these Neutral diagnoses using the mechanics of the sacrum and spine SB L --> L on LOA A+ P +/-
81
82
83
84 HVLA FOR ANTERIOR SACRUM Anterior Sacrum Leg Pull HVLA (SDOFM ) Associated with forward sacral torsions, eg. L on L 1. Patient supine, physician stands at foot of table 2. Grasp patient s right ankle just Above malleoli with both hands. 3. Instruct patient to relax all muscles in low back and leg 4. Internally rotate leg to accumulate forces at Right Sacroiliac Joint (Gaps the SI joint) 5. Keep leg and thigh at level of table 6. Apply quick pull on leg, carrying right innominate anteriorly to meet sacrum (correcting the somatic dysfunction) 7. Recheck Contraindicated in knee instability Posterior Sacrum Leg Pull HVLA (SDOFM ) Eg. Right Posterior Sacrum = Sacrum rotated Right on the Left Oblique Axis. 1. Patient supine, physician stands at foot of table 2. Grasp patient s right ankle just Above malleoli with both hands. 3. Instruct patient to relax all muscles in low back and leg 4. Internally rotate leg to accumulate forces at Right Sacroiliac Joint (Gaps the SI joint) 5. Keep the knee extended and flex hip until tension is felt on hamstrings 6. Apply final corrective force (quick pull on leg), carrying right innominate posteriorly to meet sacrum. 7. Recheck Contraindicated in knee instability
85
86 Next, there are the Non-Neutral Sacral Dysfunctions Left Right Midline
87 Non-Neutral: Left Oblique Axis Findings L5: R L S L Name: R on LOA, R R on LOA, L Backward Torsion Landmarks Static: Sacral Base: L Anterior Sacral Sulcus: L Deep ILA: L Ant/ Sup STL: L Loose Motion Testing: Spring: + (positive) L5: R L S L Sacral Base L - R +/- ILA: L + R +/- P+/- A + Left Right Midline
88 Non-Neutral: Right Oblique Axis Findings Name: L on ROA, R L on ROA, Landmarks: Sacral Base: R backward Torsion Sacral Sulcus: ILA: STL: R Anterior R Deep R loose Motion Testing: Spring: + L5: R R S R Sacral Base: L +/- R - ILA: L +/- R + R Ant./Sup. P+/- Left A + Midline Right Right Backward Torsion R L on ROA
89 Palpatory Experience We can induce these Non-Neutral diagnoses using the mechanics of the sacrum and spine... SB L -> R on LOA P+/- A +
90
91
92 HVLA FOR POSTERIOR SACRUM Anterior Sacrum Leg Pull HVLA (SDOFM ) Associated with forward sacral torsions, eg. L on L 1. Patient supine, physician stands at foot of table 2. Grasp patient s right ankle just Above malleoli with both hands. 3. Instruct patient to relax all muscles in low back and leg 4. Internally rotate leg to accumulate forces at Right Sacroiliac Joint (Gaps the SI joint) 5. Keep leg and thigh at level of table 6. Apply quick pull on leg, carrying right innominate anteriorly to meet sacrum (correcting the somatic dysfunction) 7. Recheck Contraindicated in knee instability Posterior Sacrum Leg Pull HVLA (SDOFM ) Eg. Right Posterior Sacrum = Sacrum rotated Right on the Left Oblique Axis. 1. Patient supine, physician stands at foot of table 2. Grasp patient s right ankle just Above malleoli with both hands. 3. Instruct patient to relax all muscles in low back and leg 4. Internally rotate leg to accumulate forces at Right Sacroiliac Joint (Gaps the SI joint) 5. Keep the knee extended and flex hip until tension is felt on hamstrings 6. Apply final corrective force (quick pull on leg), carrying right innominate posteriorly to meet sacrum. 7. Recheck Contraindicated in knee instability
93 COUNTERSTRAIN FOR SACRAL TORSION (not the same as counterstrain for the sacrum) Paper published by Ramirez in 1990s describing the following: Both anterior and sacral torsions were treated by: 1)noting the side of the tender sacral foramena (will be the same as the axis side of the torsion) 2)sitting on opposite side of the tender points and abducting prone patient s leg 30 degrees off table and flexing hip 30 degrees 3) pushing anteriorly on ipsilateral PSIS with operator s forearm for 90 seconds
94
95 SACRAL DIAGNOSIS Diagnosis Seated Flexion Test Sacral Base/Sulci ILA levelness L5 Rot Spring Test LS Flexion Asymmtry Left on left Right Anterior right Posterior left Right Negative Decreased Left on Right Left Anterior right Posterior left Right Positive Increased Right on right Left Anterior left Posterior Right Left Negative Decreased Right on Left Right Anterior Left Posterior Right Left Positive Increased Left Unilat Flex Left Anterior Left Posterior Left - Negative Decreased Left Unilat Ext Left Anterior Right Posterior Right - Positive Increased Right Unilat Right Anterior Right Posterior right - Negative Decreased Flex Right Unilat Ext Right Anterior Right Posterior left - Positive Increased Ant Margin - R Right Anterior Right Anterior Right Left Negative Decreased Ant Margin L Left Anterior Left Anterior Left Right Negative Decreased Post Margin Right Shallow R Posterior Right Right Positive Increased R Post Margin L Left Shallow L Posterior Left Left Positive Increased Bilateral Flexion N/A Deep Bilateral Shallow Bilateral - Negative N/A Bilateral Extnsn N/A Shallow Bilateral Deep Bilateral - Positive N/A
96
97
98 Produced when the sacrum shifts forward within the sacroiliac joint. Two Types: Unilateral Sacral Flexion Unilateral Sacral Extension Sx: Chronic low back pain.
99
100
101
102 Naming the Shear The shear is named for the side of the inferior ILA.. The sulcus is deep on same side- (which distinguishes this from a torsion) The seated flexion positive side will tell you how to interpret whether it is a unilateral flexion or extension, i.e.,sulcus deep and ILA on R with R seated flexion + = R unilateral Flexion; L unilateral extension if seated is + L with the same findings of: deep sulcus R and ILA post/inf R
103
104
105
106
107
108
109 THANK YOU
110
111
112 Sacral Somatic Dysfunction (AKA Sacroiliac Dysfunction) Physiologic: Dysfunction that occurs around a Physiologic Axis 1. Vertical 2. Transverse 3. Oblique: Neutral and Non-Neutral Non - physiologic: Dysfunction that does not occur around an axis. Usually caused by trauma. 1. Upslipped Innominate 2. Unilateral Sacral Shear (Unilateral Sacral Flexion)
113 Piriformis Movement
114
115 The only Vertical Axis Diagnosis is Name: Sacral Margin Posterior For Left Sacral Margin Posterior: Landmarks: Sacral Base: L Posterior Sacral Sulcus: L Shallow ILA: L Posterior STL: L Tight Motion: Sacral Base: L ILA: L P Shallow P -
116 Sacral Margin Posterior cont... For right sacral margin posterior: Landmarks: Sacral Base: R posterior Sacral Sulcus: R shallow ILA: R posterior STL: R tight Motion: Sacral Base: R - ILA: R - P Shallow P Right Sacral Margin Posterior
117 Sacral Margin Posterior: (ILA s are level superiorly/inferiorly) On the posterior side: Entire sacral margin is posterior Base is posterior ILA is posterior Sulcus is shallow Sacrotuberous ligament is tight Anterior springing at the superior and inferior poles is restricted
118 Sacral Margin Posterior can occur on either side of a Vertical axis, but it is always named for the posterior side! P Shallow P Shallow P P Left Sacral Margin Posterior Right Sacral Margin Posterior
119
120
Anatomy and Pathomechanics of the Sacrum and Pelvis. Charles R. Thompson Head Athletic Trainer Princeton University
 Anatomy and Pathomechanics of the Sacrum and Pelvis Charles R. Thompson Head Athletic Trainer Princeton University Simplify Everything There are actually only three bones: Two innominates, one sacrum.
Anatomy and Pathomechanics of the Sacrum and Pelvis Charles R. Thompson Head Athletic Trainer Princeton University Simplify Everything There are actually only three bones: Two innominates, one sacrum.
Treatment of Sacroiliac Joint Dysfunction. Movement of sacrum on ilium
 Treatment of Sacroiliac Joint Dysfunction Movement of sacrum on ilium Sacroiliac Joint Axes Superior Middle Inferior Right Oblique Left Oblique Sacroiliac Joint Movement Nutation: : Anterior nutation or
Treatment of Sacroiliac Joint Dysfunction Movement of sacrum on ilium Sacroiliac Joint Axes Superior Middle Inferior Right Oblique Left Oblique Sacroiliac Joint Movement Nutation: : Anterior nutation or
THE BENJAMIN INSTITUTE PRESENTS. Excerpt from Listen To Your Pain. Assessment & Treatment of. Low Back Pain. Ben E. Benjamin, Ph.D.
 THE BENJAMIN INSTITUTE PRESENTS Excerpt from Listen To Your Pain Assessment & Treatment of Low Back Pain A B E N J A M I N I N S T I T U T E E B O O K Ben E. Benjamin, Ph.D. 2 THERAPIST/CLIENT MANUAL The
THE BENJAMIN INSTITUTE PRESENTS Excerpt from Listen To Your Pain Assessment & Treatment of Low Back Pain A B E N J A M I N I N S T I T U T E E B O O K Ben E. Benjamin, Ph.D. 2 THERAPIST/CLIENT MANUAL The
MET: Posterior (backward) Rotation of the Innominate Bone.
 Rotation of the Innominate Bone.") MET: Posterior (backward) Rotation of the Innominate Bone. Purpose: To reduce an anterior rotation of the innominate bone at the SI joint. To increase posterior (backward) rotation of the SI joint. Precautions:
MET: Posterior (backward) Rotation of the Innominate Bone. Purpose: To reduce an anterior rotation of the innominate bone at the SI joint. To increase posterior (backward) rotation of the SI joint. Precautions:
Breakout 2 - OMT for the Lumbar Spine and Sacrum Gretta A. Gross, DO
 Breakout 2 - OMT for the Lumbar Spine and Sacrum Gretta A. Gross, DO Osteopathic Diagnosis and Treatment of the Lumbar Spine and Sacrum Gretta A. Gross, DO, MMedEd, FACOFP DOME/PD Houston Healthcare Family
Breakout 2 - OMT for the Lumbar Spine and Sacrum Gretta A. Gross, DO Osteopathic Diagnosis and Treatment of the Lumbar Spine and Sacrum Gretta A. Gross, DO, MMedEd, FACOFP DOME/PD Houston Healthcare Family
NETWORK FITNESS FACTS THE HIP
 NETWORK FITNESS FACTS THE HIP The Hip Joint ANATOMY OF THE HIP The hip bones are divided into 5 areas, which are: Image: www.health.com/health/static/hw/media/medical/hw/ hwkb17_042.jpg The hip joint is
NETWORK FITNESS FACTS THE HIP The Hip Joint ANATOMY OF THE HIP The hip bones are divided into 5 areas, which are: Image: www.health.com/health/static/hw/media/medical/hw/ hwkb17_042.jpg The hip joint is
Ilio-Sacral Diagnosis and Treatment, Part Two
 Ilio-Sacral Diagnosis and Treatment, Part Two by Marc Heller, DC Let's continue exploring the ilio-sacral (IS) joint. I'll start with flares, which are rotations in the transverse plane. Next, I'll cover
Ilio-Sacral Diagnosis and Treatment, Part Two by Marc Heller, DC Let's continue exploring the ilio-sacral (IS) joint. I'll start with flares, which are rotations in the transverse plane. Next, I'll cover
CHAPTER V SACROILIAC JOINT & PELVIS
 CHAPTER V SACROILIAC JOINT & PELVIS Chapter V: Sacroiliac Joint & Pelvis Note to Reader 151 Chapter Organization 152 Part I: Clinical Implications of Anatomy & Physiology 153 Anatomical Structures & Landmarks
CHAPTER V SACROILIAC JOINT & PELVIS Chapter V: Sacroiliac Joint & Pelvis Note to Reader 151 Chapter Organization 152 Part I: Clinical Implications of Anatomy & Physiology 153 Anatomical Structures & Landmarks
Chapter 9 The Hip Joint and Pelvic Girdle
 Copyright The McGraw-Hill Companies, Inc. Reprinted by permission. The Hip Joint and Pelvic Girdle Chapter 9 The Hip Joint and Pelvic Girdle Structural Kinesiology R.T. Floyd, Ed.D, ATC, CSCS Hip joint
Copyright The McGraw-Hill Companies, Inc. Reprinted by permission. The Hip Joint and Pelvic Girdle Chapter 9 The Hip Joint and Pelvic Girdle Structural Kinesiology R.T. Floyd, Ed.D, ATC, CSCS Hip joint
SPINE. Postural Malalignments 4/9/2015. Cervical Spine Evaluation. Thoracic Spine Evaluation. Observations. Assess position of head and neck
 SPINE Observations Body type Postural alignments and asymmetries should be observed from all views Assess height differences between anatomical landmarks Figure 25-9 Figure 25-10 Figure 25-11 & 12 Postural
SPINE Observations Body type Postural alignments and asymmetries should be observed from all views Assess height differences between anatomical landmarks Figure 25-9 Figure 25-10 Figure 25-11 & 12 Postural
CHAPTER 3: BACK & ABDOMINAL STRETCHES. Standing Quad Stretch Athletic Edge - www.athleticedge.biz - (650) 815-6552
 815-6552") CHAPTER : BACK & ABDOMINAL STRETCHES Standing Quad Stretch ) Stand and grasp right ankle with same hand, use a wall or chair to Lower maintain Back balance with left hand. Maintain an upright Stretches
CHAPTER : BACK & ABDOMINAL STRETCHES Standing Quad Stretch ) Stand and grasp right ankle with same hand, use a wall or chair to Lower maintain Back balance with left hand. Maintain an upright Stretches
International Standards for the Classification of Spinal Cord Injury Motor Exam Guide
 C5 Elbow Flexors Biceps Brachii, Brachialis Patient Position: The shoulder is in neutral rotation, neutral flexion/extension, and adducted. The elbow is fully extended, with the forearm in full supination.
C5 Elbow Flexors Biceps Brachii, Brachialis Patient Position: The shoulder is in neutral rotation, neutral flexion/extension, and adducted. The elbow is fully extended, with the forearm in full supination.
Stabilizing the Pelvis With Exercise
 Stabilizing the Pelvis With Exercise (Relatively) Simple Rehab Strategies I thought I was finished with this rehab series. After months of intensive rehab study, I had reached the burnout stage: Rehab
Stabilizing the Pelvis With Exercise (Relatively) Simple Rehab Strategies I thought I was finished with this rehab series. After months of intensive rehab study, I had reached the burnout stage: Rehab
Stretching the Major Muscle Groups of the Lower Limb
 2 Stretching the Major Muscle Groups of the Lower Limb In this chapter, we present appropriate stretching exercises for the major muscle groups of the lower limb. All four methods (3S, yoga, slow/static,
2 Stretching the Major Muscle Groups of the Lower Limb In this chapter, we present appropriate stretching exercises for the major muscle groups of the lower limb. All four methods (3S, yoga, slow/static,
Flexibility Assessment and Improvement Compiled and Adapted by Josh Thompson
 Flexibility Assessment and Improvement Compiled and Adapted by Josh Thompson Muscles must have a full and normal range of motion in order for joints and skeletal structure to function properly. Flexibility
Flexibility Assessment and Improvement Compiled and Adapted by Josh Thompson Muscles must have a full and normal range of motion in order for joints and skeletal structure to function properly. Flexibility
Structure and Function of the Hip
 Structure and Function of the Hip Objectives Identify the bones and bony landmarks of the hip and pelvis Identify and describe the supporting structures of the hip joint Describe the kinematics of the
Structure and Function of the Hip Objectives Identify the bones and bony landmarks of the hip and pelvis Identify and describe the supporting structures of the hip joint Describe the kinematics of the
The One-Leg Standing Test and the Active Straight Leg Raise Test: A Clinical Interpretation of Two Tests of Load Transfer through the Pelvic Girdle
 Diane Lee BSR, FCAMT, CGIMS Published in the Orthopaedic Division Review 2005 I read with interest and some concern the discussion in the last issue of the Orthopaedic Division Review on evidence based
Diane Lee BSR, FCAMT, CGIMS Published in the Orthopaedic Division Review 2005 I read with interest and some concern the discussion in the last issue of the Orthopaedic Division Review on evidence based
Massage and Movement
 Massage and Movement Incorporating Movement into Massage Part One: Theory and Technique in Prone With Lee Stang, LMT NCBTMB #450217-06 1850 West Street Southington, CT 06489 860.747.6388 www.bridgestohealthseminars.com
Massage and Movement Incorporating Movement into Massage Part One: Theory and Technique in Prone With Lee Stang, LMT NCBTMB #450217-06 1850 West Street Southington, CT 06489 860.747.6388 www.bridgestohealthseminars.com
Manual Therapy for the Upper and Lower Quadrant: What Do I Need to Know? Objectives
 Manual Therapy for the Upper and Lower Quadrant: What Do I Need to Know? Objectives 1. Describe the current best evidence for manual therapy in the management of a variety of disorders. 2. Recognize subgroups
Manual Therapy for the Upper and Lower Quadrant: What Do I Need to Know? Objectives 1. Describe the current best evidence for manual therapy in the management of a variety of disorders. 2. Recognize subgroups
The Pilates Studio of Los Angeles / PilatesCertificationOnline.com
 Anatomy Review Part I Anatomical Terminology and Review Questions (through pg. 80) Define the following: 1. Sagittal Plane 2. Frontal or Coronal Plane 3. Horizontal Plane 4. Superior 5. Inferior 6. Anterior
Anatomy Review Part I Anatomical Terminology and Review Questions (through pg. 80) Define the following: 1. Sagittal Plane 2. Frontal or Coronal Plane 3. Horizontal Plane 4. Superior 5. Inferior 6. Anterior
Range of Motion. A guide for you after spinal cord injury. Spinal Cord Injury Rehabilitation Program
 Range of Motion A guide for you after spinal cord injury Spinal Cord Injury Rehabilitation Program This booklet has been written by the health care providers who provide care to people who have a spinal
Range of Motion A guide for you after spinal cord injury Spinal Cord Injury Rehabilitation Program This booklet has been written by the health care providers who provide care to people who have a spinal
The Essential Lower Back Exam
 STFM National Convention 2011 New Orleans The Essential Lower Back Exam Judith A. Furlong, M.D., Cathee McGonigle, D.O. & Rob Rutherford, MD Objectives Brief review of the anatomy of the back, (hip and
STFM National Convention 2011 New Orleans The Essential Lower Back Exam Judith A. Furlong, M.D., Cathee McGonigle, D.O. & Rob Rutherford, MD Objectives Brief review of the anatomy of the back, (hip and
Anterior Superior Iliac Spine. Anterior Inferior Iliac Spine. head neck greater trochanter intertrochanteric line lesser trochanter
 Ilium Bones The Skeleton Ischium Pubis Sacro-iliac Joint Iliac Crest Anterior Superior Superior Pubic Ramus Anterior Inferior Acetabulum Obturator Foramen Ischio-pubic ramus Ischial tuberosity Pubic Crest
Ilium Bones The Skeleton Ischium Pubis Sacro-iliac Joint Iliac Crest Anterior Superior Superior Pubic Ramus Anterior Inferior Acetabulum Obturator Foramen Ischio-pubic ramus Ischial tuberosity Pubic Crest
SECTION II General Osteopathic Techniques
 SECTION II General Osteopathic Techniques Chapter Four The Lower Extremities 40 Ligamentous Articular Strain The lower extremities are among the most important structures of the body and yet are often
SECTION II General Osteopathic Techniques Chapter Four The Lower Extremities 40 Ligamentous Articular Strain The lower extremities are among the most important structures of the body and yet are often
LOW BACK PAIN EXAMINATION
 LOW BACK PAIN EXAMINATION John Petty, M.D. Medical Director Department of Physical Medicine & Rehabilitation Kettering Medical Center February 8, 2014 PRE-TEST QUESTION What part of the low back physical
LOW BACK PAIN EXAMINATION John Petty, M.D. Medical Director Department of Physical Medicine & Rehabilitation Kettering Medical Center February 8, 2014 PRE-TEST QUESTION What part of the low back physical
No Equipment Agility/Core/Strength Program for Full Body No Equip Trainer: Rick Coe
 No Equipment Agility/Core/Strength Program for Full Body No Equip Trainer: Rick Coe Introduction Program designed to be performed in a circuit. Perform exercises in sequence without rest 2-3 times. Increase
No Equipment Agility/Core/Strength Program for Full Body No Equip Trainer: Rick Coe Introduction Program designed to be performed in a circuit. Perform exercises in sequence without rest 2-3 times. Increase
Lower Body Exercise One: Glute Bridge
 Lower Body Exercise One: Glute Bridge Lying on your back hands by your side, head on the floor. Position your feet shoulder width apart close to your glutes, feet facing forwards. Place a theraband/mini
Lower Body Exercise One: Glute Bridge Lying on your back hands by your side, head on the floor. Position your feet shoulder width apart close to your glutes, feet facing forwards. Place a theraband/mini
Spine Conditioning Program Purpose of Program
 Prepared for: Prepared by: OrthoInfo Purpose of Program After an injury or surgery, an exercise conditioning program will help you return to daily activities and enjoy a more active, healthy lifestyle.
Prepared for: Prepared by: OrthoInfo Purpose of Program After an injury or surgery, an exercise conditioning program will help you return to daily activities and enjoy a more active, healthy lifestyle.
Anatomy and Physiology 121: Muscles of the Human Body
 Epicranius Anatomy and Physiology 121: Muscles of the Human Body Covers upper cranium Raises eyebrows, surprise, headaches Parts Frontalis Occipitalis Epicranial aponeurosis Orbicularis oculi Ring (sphincter)
Epicranius Anatomy and Physiology 121: Muscles of the Human Body Covers upper cranium Raises eyebrows, surprise, headaches Parts Frontalis Occipitalis Epicranial aponeurosis Orbicularis oculi Ring (sphincter)
HELPFUL HINTS FOR A HEALTHY BACK
 HELPFUL HINTS FOR A HEALTHY BACK 1. Standing and Walking For correct posture, balance your head above your shoulders, eyes straight ahead, everything else falls into place. Try to point toes straight ahead
HELPFUL HINTS FOR A HEALTHY BACK 1. Standing and Walking For correct posture, balance your head above your shoulders, eyes straight ahead, everything else falls into place. Try to point toes straight ahead
Lumbar/Core Strength and Stability Exercises
 Athletic Medicine Lumbar/Core Strength and Stability Exercises Introduction Low back pain can be the result of many different things. Pain can be triggered by some combination of overuse, muscle strain,
Athletic Medicine Lumbar/Core Strength and Stability Exercises Introduction Low back pain can be the result of many different things. Pain can be triggered by some combination of overuse, muscle strain,
Injury Prevention for the Back and Neck
 Injury Prevention for the Back and Neck www.csmr.org We have created this brochure to provide you with information regarding: Common Causes of Back and Neck Injuries and Pain Tips for Avoiding Neck and
Injury Prevention for the Back and Neck www.csmr.org We have created this brochure to provide you with information regarding: Common Causes of Back and Neck Injuries and Pain Tips for Avoiding Neck and
Movement in the human body occurs at joint
 Biomechanics of The Spine Richard A. Banton, DPT, OCS, CMPT, ATC Movement in the human body occurs at joint surfaces; movement occurs with bones; movement of muscles moves the bones; coordinated movements
Biomechanics of The Spine Richard A. Banton, DPT, OCS, CMPT, ATC Movement in the human body occurs at joint surfaces; movement occurs with bones; movement of muscles moves the bones; coordinated movements
DSM Spine+Sport - Mobility
 To set yourself up for success, practice keeping a neutral spine throughout all of these movements. This will ensure the tissue mobilization is being applied to the correct area, and make the techniques
To set yourself up for success, practice keeping a neutral spine throughout all of these movements. This will ensure the tissue mobilization is being applied to the correct area, and make the techniques
Post Operative Hip Arthroscopy Rehabilitation Protocol Dr. David Hergan Labral Repair with or without FAI Component
 Post Operative Hip Arthroscopy Rehabilitation Protocol Dr. David Hergan Labral Repair with or without FAI Component Initial Joint Protection Guidelines- (P.O. Day 1-4 wks): Joint Protection Patient education
Post Operative Hip Arthroscopy Rehabilitation Protocol Dr. David Hergan Labral Repair with or without FAI Component Initial Joint Protection Guidelines- (P.O. Day 1-4 wks): Joint Protection Patient education
Stretching the Low Back THERAPIST ASSISTED AND CLIENT SELF-CARE STRETCHES FOR THE LUMBOSACRAL SPINE
 EXPERT CONTENT by Joseph E. Muscolino photos by Yanik Chauvin body mechanics THE ESSENCE OF MOST MANUAL THERAPIES, and certainly clinical orthopedic massage therapy, is to loosen taut soft tissues, thereby
EXPERT CONTENT by Joseph E. Muscolino photos by Yanik Chauvin body mechanics THE ESSENCE OF MOST MANUAL THERAPIES, and certainly clinical orthopedic massage therapy, is to loosen taut soft tissues, thereby
Chapter 9 The Hip Joint and Pelvic Girdle
 Chapter 9 The Hip Joint and Pelvic Girdle Manual of Structural Kinesiology R.T. Floyd, EdD, ATC, CSCS Hip relatively joint (acetabularfemoral) functions bony strong large stable due to The enhanced architecture
Chapter 9 The Hip Joint and Pelvic Girdle Manual of Structural Kinesiology R.T. Floyd, EdD, ATC, CSCS Hip relatively joint (acetabularfemoral) functions bony strong large stable due to The enhanced architecture
The Correlation between Hamstring Tightness and Low Back Pain in Seated Workers Ahmed Radwan PT, DPT, PhD Thomas A. Crist, PhD
 The Correlation between Hamstring Tightness and Low Back Pain in Seated Workers Ahmed Radwan PT, DPT, PhD Thomas A. Crist, PhD Ahmed Radwan, PT, DPT, Ph.D. Associate Professor Physical Therapy Program
The Correlation between Hamstring Tightness and Low Back Pain in Seated Workers Ahmed Radwan PT, DPT, PhD Thomas A. Crist, PhD Ahmed Radwan, PT, DPT, Ph.D. Associate Professor Physical Therapy Program
Muscle Movements, Types, and Names
 Muscle Movements, Types, and Names A. Gross Skeletal Muscle Activity 1. With a few exceptions, all muscles cross at least one joint 2. Typically, the bulk of the muscle lies proximal to the joint it crossed
Muscle Movements, Types, and Names A. Gross Skeletal Muscle Activity 1. With a few exceptions, all muscles cross at least one joint 2. Typically, the bulk of the muscle lies proximal to the joint it crossed
by Ellen Saltonstall and Dr. Loren Fishman
 10 Yoga Poses for Low Back Pain Prevention by Ellen Saltonstall and Dr. Loren Fishman Introduction This series of poses is designed to prevent future back pain and also to relieve back pain that you may
10 Yoga Poses for Low Back Pain Prevention by Ellen Saltonstall and Dr. Loren Fishman Introduction This series of poses is designed to prevent future back pain and also to relieve back pain that you may
Sacroiliac Joint Exercises For Stability And Pain Relief
 Sacroiliac Joint Exercises For Stability And Pain Relief By Sam Visnic NMT SamVisnic.com Endyourbackpainnow.com 2011 Sam Visnic All Rights Reserved. Warning! This information is NOT medical advice, and
Sacroiliac Joint Exercises For Stability And Pain Relief By Sam Visnic NMT SamVisnic.com Endyourbackpainnow.com 2011 Sam Visnic All Rights Reserved. Warning! This information is NOT medical advice, and
PELVIS. 2007 Lippincott Williams & Wilkins S59 BONE: PELVIS (6) Location: Pelvic ring (61)
 Location: Pelvic ring (61)") PELVIS BONE: PELVIS (6) Location: Pelvic ring (61) Types: A. Lesion sparing (or with no displacement of) posterior arch (61-A) B. Incomplete disruption of posterior arch, partially stable (61-B) C. Complete
PELVIS BONE: PELVIS (6) Location: Pelvic ring (61) Types: A. Lesion sparing (or with no displacement of) posterior arch (61-A) B. Incomplete disruption of posterior arch, partially stable (61-B) C. Complete
Spinal Exercise Program/Core Stabilization Program Adapted from The Spine in Sports: Robert G. Watkins
 Spinal Exercise Program/Core Stabilization Program Adapted from The Spine in Sports: Robert G. Watkins Below is a description of a Core Stability Program, designed to improve the strength and coordination
Spinal Exercise Program/Core Stabilization Program Adapted from The Spine in Sports: Robert G. Watkins Below is a description of a Core Stability Program, designed to improve the strength and coordination
The Lumbosacral Dura and Sciatic Nerve Tension: Treatable Components of Discogenic Pain
 The Lumbosacral Dura and Sciatic Nerve Tension: Treatable Components of Discogenic Pain The first several articles in this miniseries addressed, among other things, some of the structures that can contribute
The Lumbosacral Dura and Sciatic Nerve Tension: Treatable Components of Discogenic Pain The first several articles in this miniseries addressed, among other things, some of the structures that can contribute
Screening Examination of the Lower Extremities BUY THIS BOOK! Lower Extremity Screening Exam
 Screening Examination of the Lower Extremities Melvyn Harrington, MD Department of Orthopaedic Surgery & Rehabilitation Loyola University Medical Center BUY THIS BOOK! Essentials of Musculoskeletal Care
Screening Examination of the Lower Extremities Melvyn Harrington, MD Department of Orthopaedic Surgery & Rehabilitation Loyola University Medical Center BUY THIS BOOK! Essentials of Musculoskeletal Care
Lumbar Back Pain in Young Athletes
 Lumbar Back Pain in Young Athletes MS CAQ in Sports Medicine Blair Orthopedics Altoona, PA OMED 2012 San Diego CA AOASM Tuesday October 9 th 1:00pm Lumbar Back Pain in Learning ObjecKves Epidemiology Anatomy
Lumbar Back Pain in Young Athletes MS CAQ in Sports Medicine Blair Orthopedics Altoona, PA OMED 2012 San Diego CA AOASM Tuesday October 9 th 1:00pm Lumbar Back Pain in Learning ObjecKves Epidemiology Anatomy
Human Anatomy & Physiology
 PowerPoint Lecture Slides prepared by Barbara Heard, Atlantic Cape Community College Ninth Edition Human Anatomy & Physiology C H A P T E R 7 The Skeleton: Part B Annie Leibovitz/Contact Press Images Vertebral
PowerPoint Lecture Slides prepared by Barbara Heard, Atlantic Cape Community College Ninth Edition Human Anatomy & Physiology C H A P T E R 7 The Skeleton: Part B Annie Leibovitz/Contact Press Images Vertebral
Ken Ross BSc ST, Nat Dip ST
 Ken Ross BSc ST, Nat Dip ST Trunk Most people will suffer from back pain at some point in their lives. Good spinal posture places minimal strain on the muscles which maintain the natural curve of the spine
Ken Ross BSc ST, Nat Dip ST Trunk Most people will suffer from back pain at some point in their lives. Good spinal posture places minimal strain on the muscles which maintain the natural curve of the spine
Hip and Trunk Exercise Program
 Hip and Trunk Exercise Program Hip and Pelvis Exercise Program Gluteus Medius and Minimus (Hip Abductors) Page 2 Lateral Hip Rotators Page 6 Tensor Fascia Lata (TFL) and Illiotibial Band (ITB) Page 7 Lower
Hip and Trunk Exercise Program Hip and Pelvis Exercise Program Gluteus Medius and Minimus (Hip Abductors) Page 2 Lateral Hip Rotators Page 6 Tensor Fascia Lata (TFL) and Illiotibial Band (ITB) Page 7 Lower
SAMPLE WORKOUT Full Body
 SAMPLE WORKOUT Full Body Perform each exercise: 30 secs each x 2 rounds or 2-3 sets of 8-12 reps Monday & Wednesday or Tuesday & Thursday Standing Squat Muscles: glutes (butt), quadriceps (thigh) Stand
SAMPLE WORKOUT Full Body Perform each exercise: 30 secs each x 2 rounds or 2-3 sets of 8-12 reps Monday & Wednesday or Tuesday & Thursday Standing Squat Muscles: glutes (butt), quadriceps (thigh) Stand
Coaching the Injury Prone Athlete. www.englandathletics.org www.englandathletics.org/east
 Coaching the Injury Prone Athlete Injury! The Causes? Frequently the consequence of poor physical preparation ( accidents excluded) Exceeding training loads the athlete can handle at that time Volume,
Coaching the Injury Prone Athlete Injury! The Causes? Frequently the consequence of poor physical preparation ( accidents excluded) Exceeding training loads the athlete can handle at that time Volume,
Range of Motion Exercises
 Range of Motion Exercises Range of motion (ROM) exercises are done to preserve flexibility and mobility of the joints on which they are performed. These exercises reduce stiffness and will prevent or at
Range of Motion Exercises Range of motion (ROM) exercises are done to preserve flexibility and mobility of the joints on which they are performed. These exercises reduce stiffness and will prevent or at
Self-mobilization methods
 Self-mobilization methods 5 Muscle energy techniques, as outlined in previous chapters, provide us with an excellent series of methods for relaxation and stretching of specific tight, shortened, contracted
Self-mobilization methods 5 Muscle energy techniques, as outlined in previous chapters, provide us with an excellent series of methods for relaxation and stretching of specific tight, shortened, contracted
Myofit Massage Therapy Stretches for Cycling
 Guidelines for Stretching Always assume the stretch start position and comfortably apply the stretch as directed. Think Yoga - gently and slowly, no ballistic actions or bouncing at joint end range. Once
Guidelines for Stretching Always assume the stretch start position and comfortably apply the stretch as directed. Think Yoga - gently and slowly, no ballistic actions or bouncing at joint end range. Once
American Osteopathic Academy of Sports Medicine James McCrossin MS ATC, CSCS Philadelphia Flyers April 23 rd, 2015
 American Osteopathic Academy of Sports Medicine James McCrossin MS ATC, CSCS Philadelphia Flyers April 23 rd, 2015 Coming together is a beginning; keeping together is progress; working together is success.
American Osteopathic Academy of Sports Medicine James McCrossin MS ATC, CSCS Philadelphia Flyers April 23 rd, 2015 Coming together is a beginning; keeping together is progress; working together is success.
CORRECTIVE CHIROPRACTIC EXERCISES
 CORRECTIVE CHIROPRACTIC EXERCISES J O W E T T & M O U L T O N C h i r o p r a c t o r s introduction This booklet, presented by Jowett and Moulton Chiropractors, is designed to provide you with a general
CORRECTIVE CHIROPRACTIC EXERCISES J O W E T T & M O U L T O N C h i r o p r a c t o r s introduction This booklet, presented by Jowett and Moulton Chiropractors, is designed to provide you with a general
Self-Myofascial Release Foam Roller Massage
 How it works. Self-Myofascial Release Foam Roller Massage Traditional stretching techniques simply cause increases in muscle length and can actually increase your chances of injury. Self-myofascial release
How it works. Self-Myofascial Release Foam Roller Massage Traditional stretching techniques simply cause increases in muscle length and can actually increase your chances of injury. Self-myofascial release
Don t. Hamstrings. Calf Muscles. both legs 2-3 times. stretch is felt in the back of the calf. Repeat with both legs 2-3 times.
 Remember to: Warm-up your muscles first before stretching (e.g. stretch after walking). Stretch until you feel mild discomfort, not pain. Never bounce or force a stretch. Hold the stretch for 10-30 seconds
Remember to: Warm-up your muscles first before stretching (e.g. stretch after walking). Stretch until you feel mild discomfort, not pain. Never bounce or force a stretch. Hold the stretch for 10-30 seconds
Muscles of the Spinal Column. Chapter 12
 Muscles of the Spinal Column Chapter 12 Cervical Muscles Splenius Splenius (capitis and cervicis) Origin: Cervicis spinous process of T3-T6 Capitis - lower half of ligmentum nuchea & spinous process of
Muscles of the Spinal Column Chapter 12 Cervical Muscles Splenius Splenius (capitis and cervicis) Origin: Cervicis spinous process of T3-T6 Capitis - lower half of ligmentum nuchea & spinous process of
Pelvic Drop Table Technique
 All materials contained in this PowerPoint Presentation are protected by copyright laws, and may not be reproduced, republished, distributed, transmitted electronically, displayed, broadcast or otherwise
All materials contained in this PowerPoint Presentation are protected by copyright laws, and may not be reproduced, republished, distributed, transmitted electronically, displayed, broadcast or otherwise
Strength Exercises for Improved Running Biomechanics
 2 CHAPTER Strength Exercises for Improved Running Biomechanics ssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssdd s Many gait abnormalities seen
2 CHAPTER Strength Exercises for Improved Running Biomechanics ssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssdd s Many gait abnormalities seen
Sit stand desks and musculo skeletal health. Katharine Metters
 Sit stand desks and musculo skeletal health Katharine Metters Topics Sitting Standing Movement and activity Work and human change Sitting uses less energy Sitting provides support for the body to reduce
Sit stand desks and musculo skeletal health Katharine Metters Topics Sitting Standing Movement and activity Work and human change Sitting uses less energy Sitting provides support for the body to reduce
Chapter 5. The Shoulder Joint. The Shoulder Joint. Bones. Bones. Bones
 Copyright The McGraw-Hill Companies, Inc. Reprinted by permission. Chapter 5 The Shoulder Joint Structural Kinesiology R.T. Floyd, Ed.D, ATC, CSCS Structural Kinesiology The Shoulder Joint 5-1 The Shoulder
Copyright The McGraw-Hill Companies, Inc. Reprinted by permission. Chapter 5 The Shoulder Joint Structural Kinesiology R.T. Floyd, Ed.D, ATC, CSCS Structural Kinesiology The Shoulder Joint 5-1 The Shoulder
Sheet 1A. Treating short/tight muscles using MET. Pectorals. Upper trapezius. Levator scapula
 Sheet 1A Treating short/tight muscles using MET Pectorals Once daily lie at edge of bed holding a half-kilo can, arm out sideways. Raise arm and hold for 10 seconds, then allow arm to hang down, stretching
Sheet 1A Treating short/tight muscles using MET Pectorals Once daily lie at edge of bed holding a half-kilo can, arm out sideways. Raise arm and hold for 10 seconds, then allow arm to hang down, stretching
Stretching in the Office
 Stretching in the Office Legs: Quads, Hamstrings, IT band, Hip flexors, Gluts, Calves Quads: Standing @ desk maintaining upright posture, grab one leg @ a time by foot or ankle and bring it towards backside
Stretching in the Office Legs: Quads, Hamstrings, IT band, Hip flexors, Gluts, Calves Quads: Standing @ desk maintaining upright posture, grab one leg @ a time by foot or ankle and bring it towards backside
Patellofemoral Joint: Superior Glide of the Patella
 Patellofemoral Joint: Superior Glide of the Patella Purpose: To increase knee extension. Precautions: Do not compress the patella against the femoral condyles. Do not force the knee into hyperextension
Patellofemoral Joint: Superior Glide of the Patella Purpose: To increase knee extension. Precautions: Do not compress the patella against the femoral condyles. Do not force the knee into hyperextension
stretches and exercises
 stretches and exercises The enclosed sheets contain stretches and exercises which can be used to delay and minimise the development of contractures and deformities occurring in children with Duchenne muscular
stretches and exercises The enclosed sheets contain stretches and exercises which can be used to delay and minimise the development of contractures and deformities occurring in children with Duchenne muscular
McMaster Spikeyball Therapy Drills
 BODY BLOCKS In sequencing Breathing and Tempo Flexibility / Mobility and Proprioception (feel) Upper body segment Middle body segment Lower body segment Extension / Static Posture Office / Computer Travel
BODY BLOCKS In sequencing Breathing and Tempo Flexibility / Mobility and Proprioception (feel) Upper body segment Middle body segment Lower body segment Extension / Static Posture Office / Computer Travel
Integrated Low Back Examination
 Integrated Low Back Examination William Thomas, DO, VCOM PPC/OMM Internal Medicine, Pediatrics and Sports Medicine October 2015 Special thanks and appreciation to Mark Rogers, DO Objectives Utilize history
Integrated Low Back Examination William Thomas, DO, VCOM PPC/OMM Internal Medicine, Pediatrics and Sports Medicine October 2015 Special thanks and appreciation to Mark Rogers, DO Objectives Utilize history
Pelvic Drop Table Technique
 All materials contained in this PowerPoint Presentation are protected by copyright laws, and may not be reproduced, republished, distributed, transmitted electronically, displayed, broadcast or otherwise
All materials contained in this PowerPoint Presentation are protected by copyright laws, and may not be reproduced, republished, distributed, transmitted electronically, displayed, broadcast or otherwise
Exercise 1: Knee to Chest. Exercise 2: Pelvic Tilt. Exercise 3: Hip Rolling. Starting Position: Lie on your back on a table or firm surface.
 Exercise 1: Knee to Chest Starting Position: Lie on your back on a table or firm surface. Action: Clasp your hands behind the thigh and pull it towards your chest. Keep the opposite leg flat on the surface
Exercise 1: Knee to Chest Starting Position: Lie on your back on a table or firm surface. Action: Clasp your hands behind the thigh and pull it towards your chest. Keep the opposite leg flat on the surface
Sacroiliac Instability: An Overview
 Sacroiliac Instability: An Overview Marc Heller, DC, practices in Ashland, Ore. He can be contacted at MHeller@MarcHellerDC.com or www.marchellerdc.com. For more information, including a brief biography,
Sacroiliac Instability: An Overview Marc Heller, DC, practices in Ashland, Ore. He can be contacted at MHeller@MarcHellerDC.com or www.marchellerdc.com. For more information, including a brief biography,
Passive Range of Motion Exercises
 Exercise and ALS The physical or occupational therapist will make recommendations for exercise based upon each patient s specific needs and abilities. Strengthening exercises are not generally recommended
Exercise and ALS The physical or occupational therapist will make recommendations for exercise based upon each patient s specific needs and abilities. Strengthening exercises are not generally recommended
Biomechanical Analysis of the Deadlift (aka Spinal Mechanics for Lifters) Tony Leyland
 Tony Leyland") Biomechanical Analysis of the Deadlift (aka Spinal Mechanics for Lifters) Tony Leyland Mechanical terminology The three directions in which forces are applied to human tissues are compression, tension,
Biomechanical Analysis of the Deadlift (aka Spinal Mechanics for Lifters) Tony Leyland Mechanical terminology The three directions in which forces are applied to human tissues are compression, tension,
Low Back Pain Exercises Interactive Video Series Transcript July 2013
 Introduction Low Back Pain Exercises Interactive Video Series Transcript July 2013 ** Note: If an exercise causes an increase in your pain, stop the exercise.** [Music introduction; Dr. John Sheehan onscreen]
Introduction Low Back Pain Exercises Interactive Video Series Transcript July 2013 ** Note: If an exercise causes an increase in your pain, stop the exercise.** [Music introduction; Dr. John Sheehan onscreen]
PHYSICAL EXAMINATION
 The Evidence Based Clinical Examination of the Lumbar Spine, Pelvis, & Hip POSITION Standing PHYSICAL EXAMINATION Neurologic -Motor: Heel Walk (L4-5) Toe Raise (L5-S1) Squat or Step-up (L3-4) Observation/Palpation
The Evidence Based Clinical Examination of the Lumbar Spine, Pelvis, & Hip POSITION Standing PHYSICAL EXAMINATION Neurologic -Motor: Heel Walk (L4-5) Toe Raise (L5-S1) Squat or Step-up (L3-4) Observation/Palpation
Muscular System. Student Learning Objectives: Identify the major muscles of the body Identify the action of major muscles of the body
 Muscular System Student Learning Objectives: Identify the major muscles of the body Identify the action of major muscles of the body Structures to be identified: Muscle actions: Extension Flexion Abduction
Muscular System Student Learning Objectives: Identify the major muscles of the body Identify the action of major muscles of the body Structures to be identified: Muscle actions: Extension Flexion Abduction
A Capstone Project for PTY 768 Presented to the Faculty of the Physical Therapy Department Sage Graduate School
 The Use of Manual Physical Therapy in the Treatment of Sacroiliitis: A Case Report A Capstone Project for PTY 768 Presented to the Faculty of the Physical Therapy Department Sage Graduate School In Partial
The Use of Manual Physical Therapy in the Treatment of Sacroiliitis: A Case Report A Capstone Project for PTY 768 Presented to the Faculty of the Physical Therapy Department Sage Graduate School In Partial
What is the Hip? Femur pull-back prone stabilize pelvis and pull the femur up at the top
 Spinning the Hip Dr. George Russell 1133 Broadway, #1125 New York, NY 10010 george@georgerusselldc.com georgerusselldc.com Copyright George Russell 2014 What is the Hip? Front bone of the pelvis Anterior
Spinning the Hip Dr. George Russell 1133 Broadway, #1125 New York, NY 10010 george@georgerusselldc.com georgerusselldc.com Copyright George Russell 2014 What is the Hip? Front bone of the pelvis Anterior
Hip Conditioning Program. Purpose of Program
 Prepared for: Prepared by: OrthoInfo Purpose of Program After an injury or surgery, an exercise conditioning program will help you return to daily activities and enjoy a more active, healthy lifestyle.
Prepared for: Prepared by: OrthoInfo Purpose of Program After an injury or surgery, an exercise conditioning program will help you return to daily activities and enjoy a more active, healthy lifestyle.
Basic Stretch Programme 3. Exercise Circuit 4
 Basic Stretch Programme 3 Exercise Circuit 4 2 1 Calves Stand approximately 1 metre away from wall with legs straight and heels on floor. Step and lean forward and slowly push hips towards wall. Should
Basic Stretch Programme 3 Exercise Circuit 4 2 1 Calves Stand approximately 1 metre away from wall with legs straight and heels on floor. Step and lean forward and slowly push hips towards wall. Should
Low Back: Sacroiliac Dysfunction. Presented by Dr. Ben Benjamin
 Debilitating Orthopedic Injury Sampler #1 Low Back: Sacroiliac Dysfunction Presented by Dr. Ben Benjamin 1 Instructor: Ben Benjamin, Ph.D. 2 Instructor: Ben Benjamin, Ph.D. drben@benbenjamin.com 3 1 Thank
Debilitating Orthopedic Injury Sampler #1 Low Back: Sacroiliac Dysfunction Presented by Dr. Ben Benjamin 1 Instructor: Ben Benjamin, Ph.D. 2 Instructor: Ben Benjamin, Ph.D. drben@benbenjamin.com 3 1 Thank
Chapter 4 The Shoulder Girdle
 Chapter 4 The Shoulder Girdle Key Manubrium Clavicle Coracoidprocess Acromionprocess bony landmarks Glenoid fossa Bones Lateral Inferior Medial border angle McGraw-Hill Higher Education. All rights reserved.
Chapter 4 The Shoulder Girdle Key Manubrium Clavicle Coracoidprocess Acromionprocess bony landmarks Glenoid fossa Bones Lateral Inferior Medial border angle McGraw-Hill Higher Education. All rights reserved.
Integrated Manual Therapy & Orthopedic Massage For Low Back Pain, Hip Pain, and Sciatica
 Integrated Manual Therapy & Orthopedic Massage For Low Back Pain, Hip Pain, and Sciatica Assessment Protocols Treatment Protocols Treatment Protocols Corrective Exercises By Author & International Lecturer
Integrated Manual Therapy & Orthopedic Massage For Low Back Pain, Hip Pain, and Sciatica Assessment Protocols Treatment Protocols Treatment Protocols Corrective Exercises By Author & International Lecturer
General Guidelines. Neck Stretch: Side. Neck Stretch: Forward. Shoulder Rolls. Side Stretch
 Stretching Exercises General Guidelines Perform stretching exercises at least 2 3 days per week and preferably more Hold each stretch for 15 20 seconds Relax and breathe normally Stretching is most effective
Stretching Exercises General Guidelines Perform stretching exercises at least 2 3 days per week and preferably more Hold each stretch for 15 20 seconds Relax and breathe normally Stretching is most effective
Knee Conditioning Program. Purpose of Program
 Prepared for: Prepared by: OrthoInfo Purpose of Program After an injury or surgery, an exercise conditioning program will help you return to daily activities and enjoy a more active, healthy lifestyle.
Prepared for: Prepared by: OrthoInfo Purpose of Program After an injury or surgery, an exercise conditioning program will help you return to daily activities and enjoy a more active, healthy lifestyle.
Vertebral anatomy study guide. Human Structure Summer 2015. Prepared by Daniel Schmitt, Angel Zeininger, and Karyne Rabey.
 Vertebral anatomy study guide. Human Structure Summer 2015 Prepared by Daniel Schmitt, Angel Zeininger, and Karyne Rabey. 1. Plan of Action: In this guide you will learn to identify these structures: Cervical
Vertebral anatomy study guide. Human Structure Summer 2015 Prepared by Daniel Schmitt, Angel Zeininger, and Karyne Rabey. 1. Plan of Action: In this guide you will learn to identify these structures: Cervical
PHYSIOLOGY AND MAINTENANCE Vol. IV - Lumbar Muscle Function and Dysfunction in Low Back Pain - Markku Kankaanpää
 LUMBAR MUSCLE FUNCTION AND DYSFUNCTION IN LOW BACK PAIN Markku Department of Physical Medicine and Rehabilitation, Kuopio University Hospital, and Department of Physiology, University of Kuopio, Finland
LUMBAR MUSCLE FUNCTION AND DYSFUNCTION IN LOW BACK PAIN Markku Department of Physical Medicine and Rehabilitation, Kuopio University Hospital, and Department of Physiology, University of Kuopio, Finland
Addressing Pelvic Rotation
 1 of 5 4/20/2008 10:31 AM http://www.strengthcoach.com Addressing Pelvic Rotation Aaron Brooks of Perfect Postures When trying to address your athlete's or client's limitations due to pain or joint restriction,
1 of 5 4/20/2008 10:31 AM http://www.strengthcoach.com Addressing Pelvic Rotation Aaron Brooks of Perfect Postures When trying to address your athlete's or client's limitations due to pain or joint restriction,
Lower limb nerve blocks
 Lower limb nerve blocks Barry Nicholls is Consultant in Anaesthesia and Pain Management at Musgrove Hospital, Taunton, UK. He qualified from Liverpool University and trained in Newcastle, UK, and Seattle,
Lower limb nerve blocks Barry Nicholls is Consultant in Anaesthesia and Pain Management at Musgrove Hospital, Taunton, UK. He qualified from Liverpool University and trained in Newcastle, UK, and Seattle,
Sciatic Nerve A Case Report of the Treatment of Piriformis Syndrome (Muscle Related)
") Sciatic Nerve A Case Report of the Treatment of Piriformis Syndrome (Muscle Related) Elyse Silvia West August 5, 2007 Pacific Palisades Abstract Objective: The study assessed the benefits of Pilates training
Sciatic Nerve A Case Report of the Treatment of Piriformis Syndrome (Muscle Related) Elyse Silvia West August 5, 2007 Pacific Palisades Abstract Objective: The study assessed the benefits of Pilates training
Laboratory 1 Anatomical Planes and Regions
 Laboratory 1 Anatomical Planes and Regions Goals: Define the anatomical position, including the application of the terms right and left. List and correctly use the major directional terms used in anatomy.
Laboratory 1 Anatomical Planes and Regions Goals: Define the anatomical position, including the application of the terms right and left. List and correctly use the major directional terms used in anatomy.
Shoulders (free weights)
") Dumbbell Shoulder Raise Dumbbell Shoulder Raise 1) Lie back onto an incline bench (45 or less) with a DB in each hand. (You may rest each DB on the corresponding thigh.) 2) Start position: Bring the DB
Dumbbell Shoulder Raise Dumbbell Shoulder Raise 1) Lie back onto an incline bench (45 or less) with a DB in each hand. (You may rest each DB on the corresponding thigh.) 2) Start position: Bring the DB
Lectures of Human Anatomy
 Lectures of Human Anatomy Vertebral Column-I By DR. ABDEL-MONEM AWAD HEGAZY M.B. with honor 1983, Dipl."Gynecology and Obstetrics "1989, Master "Anatomy and Embryology" 1994, M.D. "Anatomy and Embryology"
Lectures of Human Anatomy Vertebral Column-I By DR. ABDEL-MONEM AWAD HEGAZY M.B. with honor 1983, Dipl."Gynecology and Obstetrics "1989, Master "Anatomy and Embryology" 1994, M.D. "Anatomy and Embryology"
Stability of the spine modelled as an arch
 Loughborough University Institutional Repository Stability of the spine modelled as an arch This item was submitted to Loughborough University's Institutional Repository by the/an author. Citation: XIAO,
Loughborough University Institutional Repository Stability of the spine modelled as an arch This item was submitted to Loughborough University's Institutional Repository by the/an author. Citation: XIAO,
COMMON OVERUSE INJURIES ATTRIBUTED TO CYCLING, AND WAYS TO MINIMIZE THESE INJURIES
 COMMON OVERUSE INJURIES ATTRIBUTED TO CYCLING, AND WAYS TO MINIMIZE THESE INJURIES Listed are a few of the most common overuse injuries associated with cycling long distances. 1. Cervical and upper back
COMMON OVERUSE INJURIES ATTRIBUTED TO CYCLING, AND WAYS TO MINIMIZE THESE INJURIES Listed are a few of the most common overuse injuries associated with cycling long distances. 1. Cervical and upper back
KNEE EXERCISE PROGRAM
 KNEE PROGRAM INTRODUCT ION Welcome to your knee exercise program. The exercises in the program are designed to improve your knee stability and strength of the muscles around your knee and hip. The strength
KNEE PROGRAM INTRODUCT ION Welcome to your knee exercise program. The exercises in the program are designed to improve your knee stability and strength of the muscles around your knee and hip. The strength
Exercises for Low Back Injury Prevention
 DIVISION OF AGRICULTURE RESEARCH & EXTENSION University of Arkansas System Family and Consumer Sciences Increasing Physical Activity as We Age Exercises for Low Back Injury Prevention FSFCS38 Lisa Washburn,
DIVISION OF AGRICULTURE RESEARCH & EXTENSION University of Arkansas System Family and Consumer Sciences Increasing Physical Activity as We Age Exercises for Low Back Injury Prevention FSFCS38 Lisa Washburn,
are you reaching your full potential...
 T h e r e s n o s u c h t h i n g a s b a d e x e r c i s e - j u s t e x e r c i s e d o n e b a d l y FIT for sport are you reaching your full potential... These tests are a series of exercises designed
T h e r e s n o s u c h t h i n g a s b a d e x e r c i s e - j u s t e x e r c i s e d o n e b a d l y FIT for sport are you reaching your full potential... These tests are a series of exercises designed
THE SHOULDER JOINT T H E G L E N O H U M E R A L ( G H ) J O I N T
 J O I N T") THE SHOULDER JOINT T H E G L E N O H U M E R A L ( G H ) J O I N T CLARIFICATION OF TERMS Shoulder girdle = scapula and clavicle Shoulder joint (glenohumeral joint) = scapula and humerus Lippert, p115
THE SHOULDER JOINT T H E G L E N O H U M E R A L ( G H ) J O I N T CLARIFICATION OF TERMS Shoulder girdle = scapula and clavicle Shoulder joint (glenohumeral joint) = scapula and humerus Lippert, p115