Respiratory failure and Oxygen Therapy
|
|
|
- Harold Charles
- 7 years ago
- Views:
Transcription
1 Respiratory failure and Oxygen Therapy

2

3
4 A patient with Hb 15 G % will carry 3X more O2 in his blood than someone with Hb 5G % Give Controlled O2 treatment in acute pulmonary oedema to avoid CO2 retention Exacerbation of COPD is a classical example of type 1 respiratory failure % FIO2 should be given in COPD exacerbation Oxygen is routinely recommended for AMI patient Oxygen is routinely recommended for acute stroke patient

5

6 O2 dissociation curve

7 Essential pressure concepts Partial pressure = % (total pressure) x Room Air = 21% P(atmos) =760 mm Hg Partial pressure O2 in room air =760 (21/100)= mm Hg x

8 More pressure concepts In airways water vapour Pressure =47 mm Hg Dry gas pressure = =713 mm Hg inspired i air =713 21% PO2 x PI(O2) =149 mm Hg
")
9 Finally! Alveolar Gas Equation PAO2 = PIO2 -(PACO2)/(0.8) = =100
/(0.")
10 O2 dissociation curve

11 Haemoglobin and O2 Carriage Dissolved O2 =0.3ml in 100ml blood 1G Hb = 1.4ml O2 15G Hb = 20ml O2 (un 100 ml blood) i.e Hb O2 carriage X 70-fold

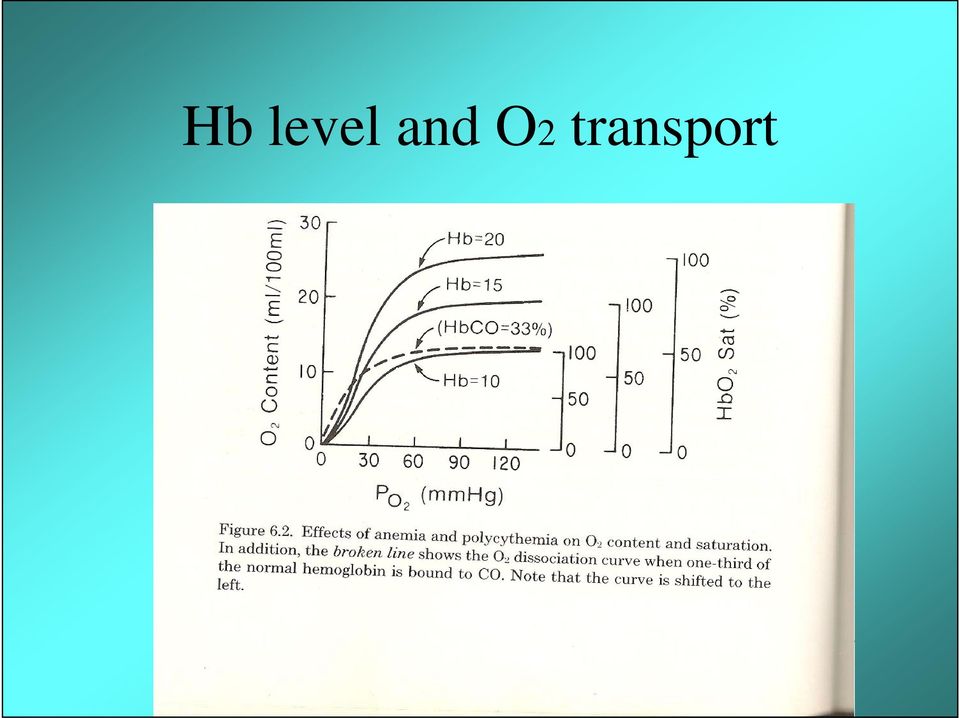
12 Importance of anaemia 15 G Hb = 20ml O2 10 G Hb = 13.3ml 3ml O2 5G Hb = 6.6ml O2

13 Hb level and O2 transport
14 Respiratory Failure 1 Hypoxaemia (PaO2 < 60 mmhg or SaO2 < 90% with N or PaCO2 TYPE Hypercapnia (PaCO2 > 46 mm Hg) II Usually with hypoxaemia
 II Usually with")
15 Type I Parenchymal disease Hypoxic environments

16 Type II COPD Obesity hypoventilation syndrome Neuromuscular disease Kyphoscoliosis

17 Hypoxaemia assessment - pitfalls Detection of cyanosis -fraught with error ie hypoxaemia often missed specially if anaemic oximetry much better Tachypnoea, tachycardia a often present but not always so

18 Hypoxaemia assessment- pitfalls Confusion, restlessness maybe more prominent especially in the elderly respiratory rate is the single best predictor of severe e illness- but beware e the calm patient hypoventilating from opiates!

19 Assessment of hypoxaemia Hx and examination Previously healthy or features of COPD Other illnesses predisposing to CO2 retention Clinical picture will usually point towards correct diagnosis In dire emergencies resuscitate first then go In dire emergencies resuscitate first then go through above steps

20 Pulse Oximetry Principle : differential absorption of Infrared light by HbO2 and deoxy Hb Accurate at SPO2> 88% ( cf ABGs) THE FIFTH VITAL SIGN
 THE FIFTH")
21
22
23
24 Pulse Oximetry-Disadvantages Inaccurate when poor perfusion, shock Does not measure Hb, ph, PaCO2 Normal reading with COHb and methb
25 Pulse Oximetry-Disadvantages Dark skinned subjects ( overestimates SpO2) Sickle cell crisis (underestimates) Nail varnish, false nails Thick fingers
26 Pulse Oximetry Does not mean Arterial blood gases should not be done
27 Arterial blood gases: indications All critically ill patient Unexpected hypoxaemia Worsening hypoxaemia Any patient at risk of type II respiratory failure who worsens Breathless patient who could be metabolic Unable to obtain reliable pulse oximetry
28 How to give O2 Set a target 94-98% SpO2 in those without hypercapnic risk ik 88-92% when risk of CO2 retention exists
29 O2 administration Administering O2 via most appropriate device 24-28% if risk of CO2 retention Monitor( pulse oximetry) )O2 saturation Do ABG after 1hr if risk of retention Careful clinical observation
30 Essentials of O2 treatment Aim at PaO2 and Sa O2 Acute therapy High FIO2 eg Pneumonia, pulmonary oedema Controlled FIO2 (when risk of CO2 retention and coma Chronic O2 treatment - home Chronic O2 treatment home O2 (COPD, CF, ILD, BPD
31 Remember O2 delivery to tissues is what matters SO SaO2 is important But so are [Hb] and Cardiac output
32 COPD dx. - pointers Age > 50 yrs > 10 pack yr smoking Chronic cough, Sputum Pre existing exertional dyspnoea Previous exacerbations
33 O2 - dangers CO2 retention (hypercapnia) Respiratory Acidosis (ph decreased) Occurs in pathology associated with hypoventilation Commonest: COPD Also Morbid Obesity Neuromuscular disease Kyphoscoliosis
34 Mechanism of CO2 retention Classically loss of hypoxic drive Current favourite V/Q mismatch (loss of hypoxic vasoconstriction) ti
35 CO2 retention: ti Symptom and Headache Tremor (flap) Confusion signs COMA (PaCO2 > 90mmHg) Flushed Bounding pulse
36 Rebound Hypoxaemia Room Air Excess Air O2 Stopped PaO2 6.5 (49) 32(240) 3.4 (255) PaCO2 7.5 (56) 10(75) 10(75) PAO (87) 8.5 (64)
37 O2 - Dangers Paraquat poisoning Bleomycin lung injury
38 Oxygen- Potentially dangerous Post MI (normoxaemic) Post Stroke Paediatric resuscitation
39 Hyperoxaemia - beneficial CO poisoning Pneumothorax 2hr Post-op bowel surgery? Diabetic foot ulcers? Cluster headaches
40 Oxygen cylinders Size C (170 L) G (3400) J(6800) Black cylinder with white shoulder Check label l Check state of filling
41
42
43 Oxygen Concentration Air intake Filter out non- O2 gases 95-99% 99% pure O2 out Up to 6 Lpm
44 High FIO2 High reservoir mask 60-90% O L/min Major trauma ER when no CO2 retention likely
45
46 Simple face mask O2 concentration 40 60% Never er use O2 flow < 5l/min * inappropriate for COPD
47
48
49 Venturi principle Gas flowing out from small orifice will lead to a flli fall in pressure
50 Venturi principle
51 Venturi masks
52 Fixed O2 conc provided minimum O2 flow rate
53 Venturi masks Most suitable for controlled O2 in COPD Also if RR > 30 Lpm with very high h inspiratory flow rate
54 Nasal Cannulae Low to medium O2 concentration 1 4 Lpm = 24% - 40 % O2 Breathing pattern dependent d thus, monitor oximetry
55 Nasal cannulae vs Simple face mask Comparable efficacy to deliver 02 around 40% NC mm appropriate for low concentration O2 cf. simple mask NC better than venturi to achieve longer NC better than venturi to achieve longer periods > 90% saturation
56 Nasal cannulae v face mask Advantages Comfort Adjustable flow gives wide oxygen dose range Patient preference No claustrophobic sensation Not taken off to eat or speak Less affected by movement of the face Less inspiratory resistance than simple face masks No risk of rebreathing of fcarbon dioxide id cheaper
57 Nasal cannulae v face mask Disadvantages May cause nasal irritation or soreness Will not work if nose is severely congested or blocked
58 Humidification i Not required for low flow O2 Possibly required for high flow O2 >24 hrs Needed for tracheotomy mask May be of value to assist clearance of secretions
59 Humidification devices Bubble humidification No benefit re:comfort Infection risk
60 Large volume nebulisation based humidifier Used in patients with viscid sputum
61 Nebulisation Asthma: Use O2 COPD: Use compressed air or electrical nebuliser
Oxygen - update April 2009 OXG
 PRESENTATION Oxygen (O 2 ) is a gas provided in compressed form in a cylinder. It is also available in liquid form, in a system adapted for ambulance use. It is fed via a regulator and flow meter to the
PRESENTATION Oxygen (O 2 ) is a gas provided in compressed form in a cylinder. It is also available in liquid form, in a system adapted for ambulance use. It is fed via a regulator and flow meter to the
Oxygen Therapy. Oxygen therapy quick guide V3 July 2012.
 PRESENTATION Oxygen (O 2 ) is a gas provided in a compressed form in a cylinder. It is also available in a liquid form. It is fed via a regulator and flow meter to the patient by means of plastic tubing
PRESENTATION Oxygen (O 2 ) is a gas provided in a compressed form in a cylinder. It is also available in a liquid form. It is fed via a regulator and flow meter to the patient by means of plastic tubing
Oxygenation. Chapter 21. Anatomy and Physiology of Breathing. Anatomy and Physiology of Breathing*
 Oxygenation Chapter 21 Anatomy and Physiology of Breathing Inspiration ~ breathing in Expiration ~ breathing out Ventilation ~ Movement of air in & out of the lungs Respiration ~ exchange of O2 & carbon
Oxygenation Chapter 21 Anatomy and Physiology of Breathing Inspiration ~ breathing in Expiration ~ breathing out Ventilation ~ Movement of air in & out of the lungs Respiration ~ exchange of O2 & carbon
Lothian Guideline for Domiciliary Oxygen Therapy Service for COPD
 Lothian Guideline for Domiciliary Oxygen Therapy Service for COPD This document describes the standard for clinical assessment, prescription, optimal management and follow-up of patients receiving domiciliary
Lothian Guideline for Domiciliary Oxygen Therapy Service for COPD This document describes the standard for clinical assessment, prescription, optimal management and follow-up of patients receiving domiciliary
Oxygenation and Oxygen Therapy Michael Billow, D.O.
 Oxygenation and Oxygen Therapy Michael Billow, D.O. The delivery of oxygen to all body tissues is the essence of critical care. Patients in respiratory distress/failure come easily to mind as the ones
Oxygenation and Oxygen Therapy Michael Billow, D.O. The delivery of oxygen to all body tissues is the essence of critical care. Patients in respiratory distress/failure come easily to mind as the ones
Understanding Hypoventilation and Its Treatment by Susan Agrawal
 www.complexchild.com Understanding Hypoventilation and Its Treatment by Susan Agrawal Most of us have a general understanding of what the term hyperventilation means, since hyperventilation, also called
www.complexchild.com Understanding Hypoventilation and Its Treatment by Susan Agrawal Most of us have a general understanding of what the term hyperventilation means, since hyperventilation, also called
GUIDELINES FOR ACUTE OXYGEN THERAPY FOR WESTERN AUSTRALIAN HOSPITALS
 GUIDELINES FOR ACUTE OXYGEN THERAPY FOR WESTERN AUSTRALIAN HOSPITALS Key Points 1. No patient should be denied oxygen therapy in an emergency. Patients in cardiac and/or respiratory arrest should be managed
GUIDELINES FOR ACUTE OXYGEN THERAPY FOR WESTERN AUSTRALIAN HOSPITALS Key Points 1. No patient should be denied oxygen therapy in an emergency. Patients in cardiac and/or respiratory arrest should be managed
Common Ventilator Management Issues
 Common Ventilator Management Issues William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center You have just admitted a 28 year-old
Common Ventilator Management Issues William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center You have just admitted a 28 year-old
Ventilation Perfusion Relationships
 Ventilation Perfusion Relationships VENTILATION PERFUSION RATIO Ideally, each alveolus in the lungs would receive the same amount of ventilation and pulmonary capillary blood flow (perfusion). In reality,
Ventilation Perfusion Relationships VENTILATION PERFUSION RATIO Ideally, each alveolus in the lungs would receive the same amount of ventilation and pulmonary capillary blood flow (perfusion). In reality,
Prescribing and Administration of Emergency Oxygen in Adults Policy
 This is an official Northern Trust policy and should not be edited in any way Prescribing and Administration of Emergency Oxygen in Adults Policy Reference Number: NHSCT/12/542 Target audience: Medical,
This is an official Northern Trust policy and should not be edited in any way Prescribing and Administration of Emergency Oxygen in Adults Policy Reference Number: NHSCT/12/542 Target audience: Medical,
GUIDELINES FOR THE MANAGEMENT OF OXYGEN THERAPY
 SOUTH DURHAM HEALTH CARE NHS TRUST GUIDELINES FOR THE MANAGEMENT OF OXYGEN THERAPY AIM To supplement oxygen intake using the appropriate equipment in order to correct hypoxia and relieve breathlessness.
SOUTH DURHAM HEALTH CARE NHS TRUST GUIDELINES FOR THE MANAGEMENT OF OXYGEN THERAPY AIM To supplement oxygen intake using the appropriate equipment in order to correct hypoxia and relieve breathlessness.
Policy for the Prescription and Administration of Oxygen to Adults in Inpatient Facilities
 Policy for the Prescription and Administration of Oxygen to Adults in Inpatient Facilities August 2013 Page 1 of 32 Policy Title Policy for the Prescription and Administration of Oxygen to Adults in Inpatient
Policy for the Prescription and Administration of Oxygen to Adults in Inpatient Facilities August 2013 Page 1 of 32 Policy Title Policy for the Prescription and Administration of Oxygen to Adults in Inpatient
Homeostasis. The body must maintain a delicate balance of acids and bases.
 Homeostasis The body must maintain a delicate balance of acids and bases. Metabolic and respiratory processes must work together to keep hydrogen ion (H+) levels normal and stable. ph of Blood The ph of
Homeostasis The body must maintain a delicate balance of acids and bases. Metabolic and respiratory processes must work together to keep hydrogen ion (H+) levels normal and stable. ph of Blood The ph of
AT HOME DR. D. K. PILLAI MUG @ UOM
 NON - INVASIVE VENTILATION AT HOME DR. D. K. PILLAI 07.09.2011 MUG @ UOM In the beginning came. OSA (HS) 1. CPAP for OSAHS (Obstructive Sleep Apnoea Hypopnoea Syndrome) 2 NIPPV 2. NIPPV (Non
NON - INVASIVE VENTILATION AT HOME DR. D. K. PILLAI 07.09.2011 MUG @ UOM In the beginning came. OSA (HS) 1. CPAP for OSAHS (Obstructive Sleep Apnoea Hypopnoea Syndrome) 2 NIPPV 2. NIPPV (Non
OXYGEN THERAPY. DR :Gehan Ali. Lecturer of chest Ds Menoufia university
 OXYGEN THERAPY DR :Gehan Ali Lecturer of chest Ds Menoufia university O 2 Therapy : Indications Documented hypoxemia as evidenced by PaO 2 < 60 mmhg or SaO 2 < 90% on room air PaO 2 or SaO 2 below desirable
OXYGEN THERAPY DR :Gehan Ali Lecturer of chest Ds Menoufia university O 2 Therapy : Indications Documented hypoxemia as evidenced by PaO 2 < 60 mmhg or SaO 2 < 90% on room air PaO 2 or SaO 2 below desirable
Adult Home Oxygen Therapy. Purpose To provide guidance on the requirements for and procedures relating to domiciliary oxygen therapy.
 Contents Purpose... 1 Scope/Audience... 1 Categories for Home Oxygen Therapy... 2 Assessment for Home Oxygen Therapy... 3 Investigations... 3 Requests for home oxygen... 3 Provision of Home Oxygen... 4
Contents Purpose... 1 Scope/Audience... 1 Categories for Home Oxygen Therapy... 2 Assessment for Home Oxygen Therapy... 3 Investigations... 3 Requests for home oxygen... 3 Provision of Home Oxygen... 4
PULMONARY PHYSIOLOGY
 I. Lung volumes PULMONARY PHYSIOLOGY American College of Surgeons SCC Review Course Christopher P. Michetti, MD, FACS and Forrest O. Moore, MD, FACS A. Tidal volume (TV) is the volume of air entering and
I. Lung volumes PULMONARY PHYSIOLOGY American College of Surgeons SCC Review Course Christopher P. Michetti, MD, FACS and Forrest O. Moore, MD, FACS A. Tidal volume (TV) is the volume of air entering and
NICE Pathways bring together all NICE guidance, quality standards and other NICE information on a specific topic.
 bring together all NICE guidance, quality standards and other NICE information on a specific topic. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published.
bring together all NICE guidance, quality standards and other NICE information on a specific topic. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published.
Hypoxia and Oxygenation Hypoxia is a serious threat to patients and escorts alike when
 Chapter 4 2 71 Hypoxia and Oxygenation Hypoxia is a serious threat to patients and escorts alike when they fly. Air medical escorts need to understand what causes hypoxia, why some people are more likely
Chapter 4 2 71 Hypoxia and Oxygenation Hypoxia is a serious threat to patients and escorts alike when they fly. Air medical escorts need to understand what causes hypoxia, why some people are more likely
Guideline for the prescription and administration of oxygen in children. Royal Hospital for Sick Children, Glasgow
 Guideline for the prescription and administration of oxygen in children. Royal Hospital for Sick Children, Glasgow Author: Dr Louise Thomson, Paediatric Respiratory Consultant Lynda Peacock, Complex Respiratory
Guideline for the prescription and administration of oxygen in children. Royal Hospital for Sick Children, Glasgow Author: Dr Louise Thomson, Paediatric Respiratory Consultant Lynda Peacock, Complex Respiratory
Eileen Whitehead 2010 East Lancashire HC NHS Trust
 Eileen Whitehead 2010 East Lancashire HC NHS Trust 1 Introduction: Arterial blood gas analysis is an essential part of diagnosing and managing a patient s oxygenation status and acid-base balance However,
Eileen Whitehead 2010 East Lancashire HC NHS Trust 1 Introduction: Arterial blood gas analysis is an essential part of diagnosing and managing a patient s oxygenation status and acid-base balance However,
POLICIES & PROCEDURES. ID Number: 1115
 POLICIES & PROCEDURES Title: OXYGEN ADMINISTRATION ID Number: 1115 Authorization [X] SHR Nursing Practice Committee Source: Nursing, Respiratory Therapy, Physiotherapy Date Revised: March 2015 Date of
POLICIES & PROCEDURES Title: OXYGEN ADMINISTRATION ID Number: 1115 Authorization [X] SHR Nursing Practice Committee Source: Nursing, Respiratory Therapy, Physiotherapy Date Revised: March 2015 Date of
Arterial Blood Gas Case Questions and Answers
 Arterial Blood Gas Case Questions and Answers In the space that follows you will find a series of cases that include arterial blood gases. Each case is then followed by an explanation of the acid-base
Arterial Blood Gas Case Questions and Answers In the space that follows you will find a series of cases that include arterial blood gases. Each case is then followed by an explanation of the acid-base
Rules on Oxygen Therapy:
 Rules on Oxygen Therapy: Physiology: 1. PO 2, SaO 2, CaO 2 are all related but different. 2. PaO2 is a sensitive and non-specific indicator of the lungs ability to exchange gases with the atmosphere. 3.
Rules on Oxygen Therapy: Physiology: 1. PO 2, SaO 2, CaO 2 are all related but different. 2. PaO2 is a sensitive and non-specific indicator of the lungs ability to exchange gases with the atmosphere. 3.
Peninsula Community Health. Policy for the Prescription, Administration. monitoring of Oxygen and Emergency Oxygen in Adults
 Peninsula Community Health Policy for the Prescription, Administration and monitoring of Oxygen and Emergency Oxygen in Adults Title: Policy for the Prescription, Administration and monitoring of Emergency
Peninsula Community Health Policy for the Prescription, Administration and monitoring of Oxygen and Emergency Oxygen in Adults Title: Policy for the Prescription, Administration and monitoring of Emergency
Acute heart failure may be de novo or it may be a decompensation of chronic heart failure.
 Management of Acute Left Ventricular Failure Acute left ventricular failure presents as pulmonary oedema due to increased pressure in the pulmonary capillaries. It is important to realise though that left
Management of Acute Left Ventricular Failure Acute left ventricular failure presents as pulmonary oedema due to increased pressure in the pulmonary capillaries. It is important to realise though that left
From AARC Protocol Committee; Subcommittee Adult Critical Care Version 1.0a (Sept., 2003), Subcommittee Chair, Susan P. Pilbeam
, Subcommittee Chair, Susan P. Pilbeam") AARC - ADULT MECHANICAL VENTILATOR PROTOCOLS 1. Guidelines for Using Ventilator Protocols 2. Definition of Modes and Suggestions for Use of Modes 3. Adult Respiratory Ventilator Protocol - Guidelines for
AARC - ADULT MECHANICAL VENTILATOR PROTOCOLS 1. Guidelines for Using Ventilator Protocols 2. Definition of Modes and Suggestions for Use of Modes 3. Adult Respiratory Ventilator Protocol - Guidelines for
Pathophysiology of hypercapnic and hypoxic respiratory failure and V/Q relationships. Dr.Alok Nath Department of Pulmonary Medicine PGIMER Chandigarh
 Pathophysiology of hypercapnic and hypoxic respiratory failure and V/Q relationships Dr.Alok Nath Department of Pulmonary Medicine PGIMER Chandigarh Jan 2006 Respiratory Failure inadequate blood oxygenation
Pathophysiology of hypercapnic and hypoxic respiratory failure and V/Q relationships Dr.Alok Nath Department of Pulmonary Medicine PGIMER Chandigarh Jan 2006 Respiratory Failure inadequate blood oxygenation
Pulmonary Diseases. Lung Disease: Pathophysiology, Medical and Exercise Programming. Overview of Pathophysiology
 Lung Disease: Pathophysiology, Medical and Exercise Programming Overview of Pathophysiology Ventilatory Impairments Increased airway resistance Reduced compliance Increased work of breathing Ventilatory
Lung Disease: Pathophysiology, Medical and Exercise Programming Overview of Pathophysiology Ventilatory Impairments Increased airway resistance Reduced compliance Increased work of breathing Ventilatory
EMERGENCY MEDICINE. Oxygen Therapy. CP Singh*, Nachhattar Singh**, Jagraj Singh***, Gurmeet Kaur Brar****, Gagandeep Singh****
 EMERGENCY MEDICINE Oxygen Therapy CP Singh*, Nachhattar Singh**, Jagraj Singh***, Gurmeet Kaur Brar****, Gagandeep Singh**** Abstract The primary goal of oxygen therapy is to correct alveolar and/or tissue
EMERGENCY MEDICINE Oxygen Therapy CP Singh*, Nachhattar Singh**, Jagraj Singh***, Gurmeet Kaur Brar****, Gagandeep Singh**** Abstract The primary goal of oxygen therapy is to correct alveolar and/or tissue
CLINICAL USE OF PULSE OXIMETRY
 CLINICAL USE OF PULSE OXIMETRY POCKET REFERENCE 2010 INTERNATIONAL Helping the World Breathe Free TM GLOBAL PRIMARY CARE AND PATIENT EDUCATION THE PURPOSE OF THIS GUIDE Chronic respiratory diseases such
CLINICAL USE OF PULSE OXIMETRY POCKET REFERENCE 2010 INTERNATIONAL Helping the World Breathe Free TM GLOBAL PRIMARY CARE AND PATIENT EDUCATION THE PURPOSE OF THIS GUIDE Chronic respiratory diseases such
Prescription and Administration of Emergency Oxygen in Adults in Hospital. Charlie Turner, Senior Nurse Patient Safety
 Policy: Prescription and Administration of Emergency Oxygen in Adults in Hospital Executive or Associate Director lead Policy author/ lead Feedback on implementation to Karen Tomlinson, Executive/Chief
Policy: Prescription and Administration of Emergency Oxygen in Adults in Hospital Executive or Associate Director lead Policy author/ lead Feedback on implementation to Karen Tomlinson, Executive/Chief
MECHINICAL VENTILATION S. Kache, MD
 MECHINICAL VENTILATION S. Kache, MD Spontaneous respiration vs. Mechanical ventilation Natural spontaneous ventilation occurs when the respiratory muscles, diaphragm and intercostal muscles pull on the
MECHINICAL VENTILATION S. Kache, MD Spontaneous respiration vs. Mechanical ventilation Natural spontaneous ventilation occurs when the respiratory muscles, diaphragm and intercostal muscles pull on the
6 Easy Steps to ABG Analysis
 6 Easy Steps to ABG Analysis E-Booklet David W. Woodruff, MSN, RN- BC, CNS, CMSRN, CEN 571 Ledge Road, Macedonia, OH 44056 Telephone (800) 990-2629 Fax (800) 990-2585 1997-2012 Ed4Nurses, Inc. All rights
6 Easy Steps to ABG Analysis E-Booklet David W. Woodruff, MSN, RN- BC, CNS, CMSRN, CEN 571 Ledge Road, Macedonia, OH 44056 Telephone (800) 990-2629 Fax (800) 990-2585 1997-2012 Ed4Nurses, Inc. All rights
Chapter 26. Assisting With Oxygen Needs. Elsevier items and derived items 2014, 2010 by Mosby, an imprint of Elsevier Inc. All rights reserved.
 Chapter 26 Assisting With Oxygen Needs Oxygen (O 2 ) is a gas. Oxygen It has no taste, odor, or color. It is a basic need required for life. Death occurs within minutes if breathing stops. Brain damage
Chapter 26 Assisting With Oxygen Needs Oxygen (O 2 ) is a gas. Oxygen It has no taste, odor, or color. It is a basic need required for life. Death occurs within minutes if breathing stops. Brain damage
Introduction to Cardiopulmonary Exercise Testing
 Introduction to Cardiopulmonary Exercise Testing 2 nd Edition Andrew M. Luks, MD Robb Glenny, MD H. Thomas Robertson, MD Division of Pulmonary and Critical Care Medicine University of Washington Section
Introduction to Cardiopulmonary Exercise Testing 2 nd Edition Andrew M. Luks, MD Robb Glenny, MD H. Thomas Robertson, MD Division of Pulmonary and Critical Care Medicine University of Washington Section
James F. Kravec, M.D., F.A.C.P
 James F. Kravec, M.D., F.A.C.P Chairman, Department of Internal Medicine, St. Elizabeth Health Center Chair, General Internal Medicine, Northeast Ohio Medical University Associate Medical Director, Hospice
James F. Kravec, M.D., F.A.C.P Chairman, Department of Internal Medicine, St. Elizabeth Health Center Chair, General Internal Medicine, Northeast Ohio Medical University Associate Medical Director, Hospice
Emergency Scenario. Chest Pain
 Emergency Scenario Chest Pain This emergency scenario reviews chest pain in a primary care patient, and is set up for roleplay and case review with your staff. 1) The person facilitating scenarios can
Emergency Scenario Chest Pain This emergency scenario reviews chest pain in a primary care patient, and is set up for roleplay and case review with your staff. 1) The person facilitating scenarios can
Determinants of Blood Oxygen Content Instructor s Guide
 Determinants of Blood Oxygen Content Instructor s Guide Time to Complete This activity will take approximately 75 minutes, but can be shortened depending on how much time the instructor takes to review
Determinants of Blood Oxygen Content Instructor s Guide Time to Complete This activity will take approximately 75 minutes, but can be shortened depending on how much time the instructor takes to review
RES Non-Invasive Positive Pressure Ventilation Guideline Page 1 of 9
 Page 1 of 9 Scope: Respiratory Care Department, Physicians, Advanced Nurse Practitioners (APRN), Physician Assistants (PA) Population: Patients receiving rescue or non-rescue non-invasive positive pressure
Page 1 of 9 Scope: Respiratory Care Department, Physicians, Advanced Nurse Practitioners (APRN), Physician Assistants (PA) Population: Patients receiving rescue or non-rescue non-invasive positive pressure
Pointing you in the right direction
 Pointing you in the right direction Dr Bronwyn Avard Ms Heather McKay Ms Nicole Slater Dr Kathryn Daveson Dr Paul Lamberth Dr Tony Lafferty Ms Susan Chen Mr John Darvill Dr Imogen Mitchell COMPASS 2008
Pointing you in the right direction Dr Bronwyn Avard Ms Heather McKay Ms Nicole Slater Dr Kathryn Daveson Dr Paul Lamberth Dr Tony Lafferty Ms Susan Chen Mr John Darvill Dr Imogen Mitchell COMPASS 2008
How To Treat A Patient With A Lung Condition
 NHS FORTH VALLEY BIPAP Guideline Date of First Issue 27 / 10 / 2010 Approved 27 / 10 / 2010 Current Issue Date 27 / 10 / 2010 Review Date 27 / 10 / 2012 Version Version 1.00 EQIA Yes 27 / 10 / 2010 Author
NHS FORTH VALLEY BIPAP Guideline Date of First Issue 27 / 10 / 2010 Approved 27 / 10 / 2010 Current Issue Date 27 / 10 / 2010 Review Date 27 / 10 / 2012 Version Version 1.00 EQIA Yes 27 / 10 / 2010 Author
OXYGEN AND ASSISTED VENTILATION FOR COPD
 OXYGEN AND ASSISTED VENTILATION FOR COPD INTERNATIONAL COPD COALITION PHYSICIANS POCKET GUIDE 2011 Aim of this Guide COPD is the fourth leading cause of death in the world, and its prevalence and health
OXYGEN AND ASSISTED VENTILATION FOR COPD INTERNATIONAL COPD COALITION PHYSICIANS POCKET GUIDE 2011 Aim of this Guide COPD is the fourth leading cause of death in the world, and its prevalence and health
Lothian Diabetes Handbook MANAGEMENT OF DIABETIC KETOACIDOSIS
 MANAGEMENT OF DIABETIC KETOACIDOSIS 90 MANAGEMENT OF DIABETIC KETOACIDOSIS Diagnosis elevated plasma and/or urinary ketones metabolic acidosis (raised H + /low serum bicarbonate) Remember that hyperglycaemia,
MANAGEMENT OF DIABETIC KETOACIDOSIS 90 MANAGEMENT OF DIABETIC KETOACIDOSIS Diagnosis elevated plasma and/or urinary ketones metabolic acidosis (raised H + /low serum bicarbonate) Remember that hyperglycaemia,
Importance of Protocols in the Decision to Use Noninvasive Ventilation
 Importance of Protocols in the Decision to Use Noninvasive Ventilation Janice L. Zimmerman, M.D. Weill Cornell Medical College The Methodist Hospital Houston, Texas Objectives Review application of protocols
Importance of Protocols in the Decision to Use Noninvasive Ventilation Janice L. Zimmerman, M.D. Weill Cornell Medical College The Methodist Hospital Houston, Texas Objectives Review application of protocols
Tests. Pulmonary Functions
 Pulmonary Functions Tests Static lung functions volumes Dynamic lung functions volume and velocity Dynamic Tests Velocity dependent on Airway resistance Resistance of lung tissue to change in shape Dynamic
Pulmonary Functions Tests Static lung functions volumes Dynamic lung functions volume and velocity Dynamic Tests Velocity dependent on Airway resistance Resistance of lung tissue to change in shape Dynamic
Medical Section. Email : acmedical@aircanada.ca. Fax : 1 888 334-7717 (toll-free) or 514 828-0027
 or 514 828-0027") Departure Date: Medical Section Hours of Operation MON-FRI 06:00-20:00 EST SAT-SUN 06:00-18 :00 EST Email : acmedical@aircanada.ca Fax : 1 888 334-7717 (toll-free) or 514 828-0027 Telephone : 1 800 667-4732
Departure Date: Medical Section Hours of Operation MON-FRI 06:00-20:00 EST SAT-SUN 06:00-18 :00 EST Email : acmedical@aircanada.ca Fax : 1 888 334-7717 (toll-free) or 514 828-0027 Telephone : 1 800 667-4732
Vtial sign #1: PULSE. Vital Signs: Assessment and Interpretation. Factors that influence pulse rate: Importance of Vital Signs
 Vital Signs: Assessment and Interpretation Elma I. LeDoux, MD, FACP, FACC Associate Professor of Medicine Vtial sign #1: PULSE Reflects heart rate (resting 60-90/min) Should be strong and regular Use 2
Vital Signs: Assessment and Interpretation Elma I. LeDoux, MD, FACP, FACC Associate Professor of Medicine Vtial sign #1: PULSE Reflects heart rate (resting 60-90/min) Should be strong and regular Use 2
How To Treat A Heart Attack
 13 Resuscitation and preparation for anaesthesia and surgery Key Points 13.1 MANAGEMENT OF EMERGENCIES AND CARDIOPULMONARY RESUSCITATION ESSENTIAL HEALTH TECHNOLOGIES The emergency measures that are familiar
13 Resuscitation and preparation for anaesthesia and surgery Key Points 13.1 MANAGEMENT OF EMERGENCIES AND CARDIOPULMONARY RESUSCITATION ESSENTIAL HEALTH TECHNOLOGIES The emergency measures that are familiar
Original Article COPD and Hospital Stay Pak Armed Forces Med J 2014; 64 (1): 46-50. Ahmed Raza, Mahmood Iqbal Malik*, Yousaf Jamal**
: 46-50. Ahmed Raza, Mahmood Iqbal Malik*, Yousaf Jamal**") Original Article COPD and Hospital Stay Pak Armed Forces Med J 2014; 64 (1): 46-50 COMPARISON OF NIPPV WITH STANDARD TREATMENT IN PATIENTS WITH ACUTE EXACERBATIONS OF COPD IN TERMS OF IMPROVEMENT IN ABGS
Original Article COPD and Hospital Stay Pak Armed Forces Med J 2014; 64 (1): 46-50 COMPARISON OF NIPPV WITH STANDARD TREATMENT IN PATIENTS WITH ACUTE EXACERBATIONS OF COPD IN TERMS OF IMPROVEMENT IN ABGS
Hyperbaric Oxygen Therapy WWW.RN.ORG
 Hyperbaric Oxygen Therapy WWW.RN.ORG Reviewed September, 2015, Expires September, 2017 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2015 RN.ORG, S.A.,
Hyperbaric Oxygen Therapy WWW.RN.ORG Reviewed September, 2015, Expires September, 2017 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2015 RN.ORG, S.A.,
3100B Clinical Training Program. 3100B HFOV VIASYS Healthcare
 3100B Clinical Training Program 3100B HFOV VIASYS Healthcare HFOV at Alveolar Level Nieman,, G, SUNY 1999 Who DO We Treat? Only Pathology studied to date has been ARDS Questions about management of adults
3100B Clinical Training Program 3100B HFOV VIASYS Healthcare HFOV at Alveolar Level Nieman,, G, SUNY 1999 Who DO We Treat? Only Pathology studied to date has been ARDS Questions about management of adults
TRANSPORT OF BLOOD GASES From The Lungs To The Tissues & Back
 TRANSPORT OF BLOOD GASES From The Lungs To The Tissues & Back Dr. Sally Osborne Department of Cellular & Physiological Sciences University of British Columbia Room 3602, D.H Copp Building 604 822-3421
TRANSPORT OF BLOOD GASES From The Lungs To The Tissues & Back Dr. Sally Osborne Department of Cellular & Physiological Sciences University of British Columbia Room 3602, D.H Copp Building 604 822-3421
Acid-Base Balance and the Anion Gap
 Acid-Base Balance and the Anion Gap 1. The body strives for electrical neutrality. a. Cations = Anions b. One of the cations is very special, H +, and its concentration is monitored and regulated very
Acid-Base Balance and the Anion Gap 1. The body strives for electrical neutrality. a. Cations = Anions b. One of the cations is very special, H +, and its concentration is monitored and regulated very
IMPAIRED BLOOD-GAS EXCHANGE. Intraoperative blood gas analysis
 IMPAIRED BLOOD-GAS EXCHANGE Intraoperative blood gas analysis When do you perform BGA Intraoperatively? Informe actual NEVER Routine:Thoracic Thoracic, Cardiac,Neurosurgery Emergency situation Drop in
IMPAIRED BLOOD-GAS EXCHANGE Intraoperative blood gas analysis When do you perform BGA Intraoperatively? Informe actual NEVER Routine:Thoracic Thoracic, Cardiac,Neurosurgery Emergency situation Drop in
The patient s response to therapy within the first hour in the Emergency Room is one of the most reliable ways to predict need for hospitalization.
 Emergency Room Asthma Management Algorithm The Emergency Room Asthma Management Algorithm is to be used for any patient seen in the Emergency Room with the diagnosis of asthma. (The initial history should
Emergency Room Asthma Management Algorithm The Emergency Room Asthma Management Algorithm is to be used for any patient seen in the Emergency Room with the diagnosis of asthma. (The initial history should
Applicant Information Sheet for MASS 45 Adult Oxygen: Initial Application and 4 Month Review
 , Queensland Health Applicant Information Sheet for Applicants should retain this section for their records Eligibility Administrative eligibility is dependent upon the applicant being a permanent Queensland
, Queensland Health Applicant Information Sheet for Applicants should retain this section for their records Eligibility Administrative eligibility is dependent upon the applicant being a permanent Queensland
CLINICAL COMPONENT FOR THE HOME OXYGEN SERVICE IN ENGLAND AND WALES
 CLINICAL COMPONENT FOR THE HOME OXYGEN SERVICE IN ENGLAND AND WALES This document has been prepared by members of the British Thoracic Society (BTS) Working Group on Home Oxygen Services, which is a Sub-Committee
CLINICAL COMPONENT FOR THE HOME OXYGEN SERVICE IN ENGLAND AND WALES This document has been prepared by members of the British Thoracic Society (BTS) Working Group on Home Oxygen Services, which is a Sub-Committee
Acute Care Day Respiratory. SCENARIO The Patient with Acute Asthma
 Acute Care Day Respiratory SCENARIO The Patient with Acute Asthma Notes for the instructor not volunteered to students 30 minutes have been allocated to the running of the scenario with an additional 10
Acute Care Day Respiratory SCENARIO The Patient with Acute Asthma Notes for the instructor not volunteered to students 30 minutes have been allocated to the running of the scenario with an additional 10
Your Lungs and COPD. Patient Education Pulmonary Rehabilitation. A guide to how your lungs work and how COPD affects your lungs
 Patient Education Your Lungs and COPD A guide to how your lungs work and how COPD affects your lungs Your lungs are organs that process every breath you take. They provide oxygen (O 2 ) to the blood and
Patient Education Your Lungs and COPD A guide to how your lungs work and how COPD affects your lungs Your lungs are organs that process every breath you take. They provide oxygen (O 2 ) to the blood and
How To Get On A Jet Plane
 Nature of disability Hospital Details TEL : +91 22 6711 6618 / 09 l FAX : +91 22 26156290 +91 11 49637953 +91 44 22568009 +91 33 25111359 Information Sheet for Guest Requiring Medical Clearance (to be
Nature of disability Hospital Details TEL : +91 22 6711 6618 / 09 l FAX : +91 22 26156290 +91 11 49637953 +91 44 22568009 +91 33 25111359 Information Sheet for Guest Requiring Medical Clearance (to be
Gas Exchange. Graphics are used with permission of: Pearson Education Inc., publishing as Benjamin Cummings (http://www.aw-bc.com)
") Gas Exchange Graphics are used with permission of: Pearson Education Inc., publishing as Benjamin Cummings (http://www.aw-bc.com) Page 1. Introduction Oxygen and carbon dioxide diffuse between the alveoli
Gas Exchange Graphics are used with permission of: Pearson Education Inc., publishing as Benjamin Cummings (http://www.aw-bc.com) Page 1. Introduction Oxygen and carbon dioxide diffuse between the alveoli
The Sepsis Puzzle: Identification, Monitoring and Early Goal Directed Therapy
 The Sepsis Puzzle: Identification, Monitoring and Early Goal Directed Therapy Cindy Goodrich RN, MS, CCRN Content Description Sepsis is caused by widespread tissue injury and systemic inflammation resulting
The Sepsis Puzzle: Identification, Monitoring and Early Goal Directed Therapy Cindy Goodrich RN, MS, CCRN Content Description Sepsis is caused by widespread tissue injury and systemic inflammation resulting
Pneumonia. Pneumonia is an infection that makes the tiny air sacs in your lungs inflamed (swollen and sore). They then fill with liquid.
. They then fill with liquid.") Pneumonia Pneumonia is an infection that makes the tiny air sacs in your lungs inflamed (swollen and sore). They then fill with liquid. People with mild (not so bad) pneumonia can usually be treated at
Pneumonia Pneumonia is an infection that makes the tiny air sacs in your lungs inflamed (swollen and sore). They then fill with liquid. People with mild (not so bad) pneumonia can usually be treated at
Interpretation of the Arterial Blood Gas Self-Learning Packet
 Interpretation of the Arterial Blood Gas Self-Learning Packet * See SWIFT for list of qualifying boards for continuing education hours. Table of Contents Purpose... 3 Objectives... 3 Instructions... 4
Interpretation of the Arterial Blood Gas Self-Learning Packet * See SWIFT for list of qualifying boards for continuing education hours. Table of Contents Purpose... 3 Objectives... 3 Instructions... 4
5/30/2014 OBJECTIVES THE ROLE OF A RESPIRATORY THERAPIST IN THE DELIVERY ROOM. Disclosure
 THE ROLE OF A RESPIRATORY THERAPIST IN THE DELIVERY ROOM Ona Fofah, MD FAAP Assistant Professor of Pediatrics Director, Division of Neonatology Department of Pediatrics Rutgers- NJMS, Newark OBJECTIVES
THE ROLE OF A RESPIRATORY THERAPIST IN THE DELIVERY ROOM Ona Fofah, MD FAAP Assistant Professor of Pediatrics Director, Division of Neonatology Department of Pediatrics Rutgers- NJMS, Newark OBJECTIVES
Key Facts about Influenza (Flu) & Flu Vaccine
 & Flu Vaccine") Key Facts about Influenza (Flu) & Flu Vaccine mouths or noses of people who are nearby. Less often, a person might also get flu by touching a surface or object that has flu virus on it and then touching
Key Facts about Influenza (Flu) & Flu Vaccine mouths or noses of people who are nearby. Less often, a person might also get flu by touching a surface or object that has flu virus on it and then touching
ACID- BASE and ELECTROLYTE BALANCE. MGHS School of EMT-Paramedic Program 2011
 ACID- BASE and ELECTROLYTE BALANCE MGHS School of EMT-Paramedic Program 2011 ACID- BASE BALANCE Ions balance themselves like a see-saw. Solutions turn into acids when concentration of hydrogen ions rises
ACID- BASE and ELECTROLYTE BALANCE MGHS School of EMT-Paramedic Program 2011 ACID- BASE BALANCE Ions balance themselves like a see-saw. Solutions turn into acids when concentration of hydrogen ions rises
What, roughly, is the dividing line between the upper and lower respiratory tract? The larynx. What s the difference between the conducting zone and
 What, roughly, is the dividing line between the upper and lower respiratory tract? The larynx. What s the difference between the conducting zone and the respiratory zone? Conducting zone is passageways
What, roughly, is the dividing line between the upper and lower respiratory tract? The larynx. What s the difference between the conducting zone and the respiratory zone? Conducting zone is passageways
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) S. Agarwal, MD, S. Kache MD
 S. Agarwal, MD, S. Kache MD") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) S. Agarwal, MD, S. Kache MD Definition ARDS is a clinical syndrome of lung injury with hypoxic respiratory failure caused by intense pulmonary inflammation that
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) S. Agarwal, MD, S. Kache MD Definition ARDS is a clinical syndrome of lung injury with hypoxic respiratory failure caused by intense pulmonary inflammation that
Using home NIV for the management of hypercapnic COPD
 Home NIV Program for COPD Using home NIV for the management of hypercapnic COPD This program offers COPD treatment guidelines to physicians to help appropriately target and qualify patients for noninvasive
Home NIV Program for COPD Using home NIV for the management of hypercapnic COPD This program offers COPD treatment guidelines to physicians to help appropriately target and qualify patients for noninvasive
Home Oxygen Therapy Policy and Administration Manual. April 2014. Assistive Devices Program Ministry of Health and Long-Term Care
 Home Oxygen Therapy Policy and Administration Manual April 2014 Assistive Devices Program Ministry of Health and Long-Term Care Table of Amendments This page will list all substantive changes to policies
Home Oxygen Therapy Policy and Administration Manual April 2014 Assistive Devices Program Ministry of Health and Long-Term Care Table of Amendments This page will list all substantive changes to policies
Safe Zone: CV PIP < 26; HFOV: MAP < 16; HFJV: MAP < 16 Dopamine infusion up to 20 mcg/kg/min Epinephrine infusion up to 0.1 mcg /kg/min.
 Congenital Diaphragmatic Hernia: Management Guidelines 5-2006 Issued By: Division of Neonatology Reviewed: Effective Date: Categories: Chronicity Document Congenital Diaphragmatic Hernia: Management Guidelines
Congenital Diaphragmatic Hernia: Management Guidelines 5-2006 Issued By: Division of Neonatology Reviewed: Effective Date: Categories: Chronicity Document Congenital Diaphragmatic Hernia: Management Guidelines
MODULE. POSITIVE AIRWAY PRESSURE (PAP) Titrations
 Titrations") MODULE POSITIVE AIRWAY PRESSURE (PAP) Titrations POSITIVE AIRWAY PRESSURE (PAP) TITRATIONS OBJECTIVES At the end of this module the student must be able to: Identify the standards of practice for administering
MODULE POSITIVE AIRWAY PRESSURE (PAP) Titrations POSITIVE AIRWAY PRESSURE (PAP) TITRATIONS OBJECTIVES At the end of this module the student must be able to: Identify the standards of practice for administering
Pharmacology for the EMT
 Pharmacology for the EMT Presented by Wade Scoles RRT, NREMT Pharmacodynamics Everybody reacts to drugs differently Factors altering drug responses Age Body mass Sex Pathologic state Genetic factors Psychological
Pharmacology for the EMT Presented by Wade Scoles RRT, NREMT Pharmacodynamics Everybody reacts to drugs differently Factors altering drug responses Age Body mass Sex Pathologic state Genetic factors Psychological
Management of exacerbations in chronic obstructive pulmonary disease in Primary Care
 Management of exacerbations in chronic obstructive pulmonary disease in Primary Care Acute exacerbations of chronic obstructive pulmonary disease (COPD) are associated with significant morbidity and mortality.
Management of exacerbations in chronic obstructive pulmonary disease in Primary Care Acute exacerbations of chronic obstructive pulmonary disease (COPD) are associated with significant morbidity and mortality.
Guideline for the use of Non-Invasive Ventilation (NIV) TCP 180
 TCP 180") Guideline for the use of Non-Invasive Ventilation (NIV) CROSS REFERENCE Progress/date of approval This Strategy/ Policy should be read in conjunction with: Mental Capacity Act Policy -TCP 199 June 2009
Guideline for the use of Non-Invasive Ventilation (NIV) CROSS REFERENCE Progress/date of approval This Strategy/ Policy should be read in conjunction with: Mental Capacity Act Policy -TCP 199 June 2009
CLINICAL SKILLS: THE 'DR ABCDE' ASSESSMENT
 CLINICAL SKILLS: THE 'DR ABCDE' ASSESSMENT The 'DR ABCDE' approach to assessing an acutely unwell patient should be at the front of every junior doctor's mind whenever they get bleeped or asked to see
CLINICAL SKILLS: THE 'DR ABCDE' ASSESSMENT The 'DR ABCDE' approach to assessing an acutely unwell patient should be at the front of every junior doctor's mind whenever they get bleeped or asked to see
240- PROBLEM SET INSERTION OF SWAN-GANZ SYSTEMIC VASCULAR RESISTANCE. Blood pressure = f(cardiac output and peripheral resistance)
") 240- PROBLEM SET INSERTION OF SWAN-GANZ 50 kg Pig Rt Jugular 0 cm Rt Atrium 10 cm Rt ventricle 15 cm Wedge 20-25 cm SYSTEMIC VASCULAR RESISTANCE Blood pressure = f(cardiac output and peripheral resistance)
240- PROBLEM SET INSERTION OF SWAN-GANZ 50 kg Pig Rt Jugular 0 cm Rt Atrium 10 cm Rt ventricle 15 cm Wedge 20-25 cm SYSTEMIC VASCULAR RESISTANCE Blood pressure = f(cardiac output and peripheral resistance)
Update on Small Animal Cardiopulmonary Resuscitation (CPR)- is anything new?
- is anything new?") Update on Small Animal Cardiopulmonary Resuscitation (CPR)- is anything new? DVM, DACVA Objective: Update on the new Small animal guidelines for CPR and a discussion of the 2012 Reassessment Campaign on
Update on Small Animal Cardiopulmonary Resuscitation (CPR)- is anything new? DVM, DACVA Objective: Update on the new Small animal guidelines for CPR and a discussion of the 2012 Reassessment Campaign on
Gas Exchange Graphics are used with permission of: adam.com (http://www.adam.com/) Benjamin Cummings Publishing Co (http://www.awl.
 Benjamin Cummings Publishing Co (http://www.awl.") Gas Exchange Graphics are used with permission of: adam.com (http://www.adam.com/) Benjamin Cummings Publishing Co (http://www.awl.com/bc) Page 1. Introduction Oxygen and carbon dioxide diffuse between
Gas Exchange Graphics are used with permission of: adam.com (http://www.adam.com/) Benjamin Cummings Publishing Co (http://www.awl.com/bc) Page 1. Introduction Oxygen and carbon dioxide diffuse between
Chronic obstructive pulmonary disease (COPD)
") Chronic obstructive pulmonary disease (COPD) Chronic obstructive pulmonary disease (COPD) is the name for a group of lung diseases including chronic bronchitis, emphysema and chronic obstructive airways
Chronic obstructive pulmonary disease (COPD) Chronic obstructive pulmonary disease (COPD) is the name for a group of lung diseases including chronic bronchitis, emphysema and chronic obstructive airways
Non-invasive ventilation in acute respiratory failure
 192 BTS GUIDELINE Non-invasive ventilation in acute respiratory failure British Thoracic Society Standards of Care Committee... Thorax 2002;57:192 211 Members of BTS Standards of Care Committee: S Baudouin,
192 BTS GUIDELINE Non-invasive ventilation in acute respiratory failure British Thoracic Society Standards of Care Committee... Thorax 2002;57:192 211 Members of BTS Standards of Care Committee: S Baudouin,
Lesson 7: Respiratory and Skeletal Systems and Tuberculosis
 Glossary 1. asthma: when the airways of the lungs narrow, making breathing difficult 2. bacteria: tiny living creatures that can only be seen with a microscope; some bacteria help the human body, and other
Glossary 1. asthma: when the airways of the lungs narrow, making breathing difficult 2. bacteria: tiny living creatures that can only be seen with a microscope; some bacteria help the human body, and other
On the Go with Oxygen
 On the Go with Oxygen Oxygen is in the air we breathe and is necessary to live. When we breathe in, oxygen enters the lungs and it goes into the blood. When the lungs cannot transfer enough oxygen into
On the Go with Oxygen Oxygen is in the air we breathe and is necessary to live. When we breathe in, oxygen enters the lungs and it goes into the blood. When the lungs cannot transfer enough oxygen into
ANZCOR Guideline 11.6.1 Targeted Oxygen Therapy in Adult Advanced Life Support
 ANZCOR Guideline 11.6.1 Targeted Oxygen Therapy in Adult Advanced Life Support Summary This guideline provides advice on the administration of oxygen in the peri-arrest period. Who does this guideline
ANZCOR Guideline 11.6.1 Targeted Oxygen Therapy in Adult Advanced Life Support Summary This guideline provides advice on the administration of oxygen in the peri-arrest period. Who does this guideline
Chapter 17 Medical Policy
 RAD-1 LCD for Respiratory Assist Devices (L11482) Contractor Information Contractor Name Contractor Number 00635 Contractor Type LCD Information LCD Database ID Number L11482 AdminaStar Federal, Inc. DMERC
RAD-1 LCD for Respiratory Assist Devices (L11482) Contractor Information Contractor Name Contractor Number 00635 Contractor Type LCD Information LCD Database ID Number L11482 AdminaStar Federal, Inc. DMERC
Using a Reservoir Nasal Cannula in Acute Care
 Using a Reservoir Nasal Cannula in Acute Care Cheryl Plate Dumont, RN, MSN, CCRN Brian L. Tiep, MD Oxymizer and Oxym i z e r Pendant (CHAD Therapeutics Inc, Chatsworth, Calif) brand reservoir cannulas
Using a Reservoir Nasal Cannula in Acute Care Cheryl Plate Dumont, RN, MSN, CCRN Brian L. Tiep, MD Oxymizer and Oxym i z e r Pendant (CHAD Therapeutics Inc, Chatsworth, Calif) brand reservoir cannulas
Chronic Obstructive Pulmonary Disease Patient Guidebook
 Chronic Obstructive Pulmonary Disease Patient Guidebook The Respiratory System The respiratory system consists of the lungs and air passages. The lungs are the part of the body where gases are exchanged
Chronic Obstructive Pulmonary Disease Patient Guidebook The Respiratory System The respiratory system consists of the lungs and air passages. The lungs are the part of the body where gases are exchanged
Pharmacology of the Respiratory Tract: COPD and Steroids
 Pharmacology of the Respiratory Tract: COPD and Steroids Dr. Tillie-Louise Hackett Department of Anesthesiology, Pharmacology and Therapeutics University of British Columbia Associate Head, Centre of Heart
Pharmacology of the Respiratory Tract: COPD and Steroids Dr. Tillie-Louise Hackett Department of Anesthesiology, Pharmacology and Therapeutics University of British Columbia Associate Head, Centre of Heart
Assessment of a breathless patient
 Assessment of a breathless patient 48-53 Multiple-choice questions and submission instructions 54 Practice profile assessment guide 56 Practice profile 26 By reading this article and writing a practice
Assessment of a breathless patient 48-53 Multiple-choice questions and submission instructions 54 Practice profile assessment guide 56 Practice profile 26 By reading this article and writing a practice
Oxygen Dissociation Curve
 122 Visit http://www.anaesthesiamcq.com for details Chapter 4 Dissociation Curve Can you draw the oxygen dissociation curve of normal adult haemoglobin? How many points on the curve can you indicate with
122 Visit http://www.anaesthesiamcq.com for details Chapter 4 Dissociation Curve Can you draw the oxygen dissociation curve of normal adult haemoglobin? How many points on the curve can you indicate with
Pediatric Airway Management
 Pediatric Airway Management Dec 2003 Dr. Shapiro I., PICU Adult Chain of Survival EMS CPR ALS Early Defibrillation Pediatric Chain of Survival Prevention CPR EMS ALS Out-of-Hospital Cardiac Arrest SIDS
Pediatric Airway Management Dec 2003 Dr. Shapiro I., PICU Adult Chain of Survival EMS CPR ALS Early Defibrillation Pediatric Chain of Survival Prevention CPR EMS ALS Out-of-Hospital Cardiac Arrest SIDS
Sign up to receive ATOTW weekly - email worldanaesthesia@mac.com
 ANAESTHESIA IN PATIENTS WITH CHRONIC OBSTRUCTIVE PULMONARY DISEASE ANAESTHESIA TUTORIAL OF THE WEEK 106 28 TH JULY 2008 Dr. Mai Wakatsuki Dr Tom Havelock SELF-ASSESSMENT Please answer questions 1-3 true
ANAESTHESIA IN PATIENTS WITH CHRONIC OBSTRUCTIVE PULMONARY DISEASE ANAESTHESIA TUTORIAL OF THE WEEK 106 28 TH JULY 2008 Dr. Mai Wakatsuki Dr Tom Havelock SELF-ASSESSMENT Please answer questions 1-3 true
SMO: Anaphylaxis and Allergic Reactions
 REGION I EMERGENCY MEDICAL SERVICES STANDING MEDICAL ORDERS EMT Basic SMO: Anaphylaxis and Allergic Reactions Overview: Allergic reactions can vary in severity from a mild reaction consisting of hives
REGION I EMERGENCY MEDICAL SERVICES STANDING MEDICAL ORDERS EMT Basic SMO: Anaphylaxis and Allergic Reactions Overview: Allergic reactions can vary in severity from a mild reaction consisting of hives
BLOOD GAS VARIATIONS. Respiratory Values PCO2 35-45 mmhg Normal range. PCO2 ( > 45) ph ( < 7.35) Respiratory Acidosis
 ph ( < 7.35) Respiratory Acidosis") BLOOD GAS VARIATIONS 1 BLOOD ph Normal range 7.35 7.45 Think of 7.40 as your new 0 or neutral If the reading is below 7.4 it is acid. Below 7.35 it is acid out of range or Acidosis If the reading is above
BLOOD GAS VARIATIONS 1 BLOOD ph Normal range 7.35 7.45 Think of 7.40 as your new 0 or neutral If the reading is below 7.4 it is acid. Below 7.35 it is acid out of range or Acidosis If the reading is above
Respiratory failure. (Respiratory insuficiency) MUDr Radim Kukla KAR FN Motol
 MUDr Radim Kukla KAR FN Motol") Respiratory failure (Respiratory insuficiency) MUDr Radim Kukla KAR FN Motol Respiratory failure definition Failure of ability to secure the metabolic needs of organism i.e. proper oxygenation and excretion
Respiratory failure (Respiratory insuficiency) MUDr Radim Kukla KAR FN Motol Respiratory failure definition Failure of ability to secure the metabolic needs of organism i.e. proper oxygenation and excretion
Understanding Pulmonary Function Testing. PFTs, Blood Gases and Oximetry Skinny Little Reference Guide
 Understanding Pulmonary Function Testing PFTs, Blood Gases and Oximetry Skinny Little Reference Guide INTRODUCTION This brochure is intended to help you understand the meaning of Pulmonary Function Testing,
Understanding Pulmonary Function Testing PFTs, Blood Gases and Oximetry Skinny Little Reference Guide INTRODUCTION This brochure is intended to help you understand the meaning of Pulmonary Function Testing,
Dehydration & Overhydration. Waseem Jerjes
 Dehydration & Overhydration Waseem Jerjes Dehydration 3 Major Types Isotonic - Fluid has the same osmolarity as plasma Hypotonic -Fluid has fewer solutes than plasma Hypertonic-Fluid has more solutes than
Dehydration & Overhydration Waseem Jerjes Dehydration 3 Major Types Isotonic - Fluid has the same osmolarity as plasma Hypotonic -Fluid has fewer solutes than plasma Hypertonic-Fluid has more solutes than
J. A. HILDES NORTHERN MEDICAL UNIT DEPARTMENT OF COMMUNITY HEALTH SCIENCES AND DEPARTMENT OF PEDIATRICS AND CHILD HEALTH FACULTY OF MEDICINE
 J. A. HILDES NORTHERN MEDICAL UNIT DEPARTMENT OF COMMUNITY HEALTH SCIENCES AND DEPARTMENT OF PEDIATRICS AND CHILD HEALTH FACULTY OF MEDICINE Recommendations for Evidence-Based Care for Bronchiolitis 2005
J. A. HILDES NORTHERN MEDICAL UNIT DEPARTMENT OF COMMUNITY HEALTH SCIENCES AND DEPARTMENT OF PEDIATRICS AND CHILD HEALTH FACULTY OF MEDICINE Recommendations for Evidence-Based Care for Bronchiolitis 2005