Please read the information below to assist you in submitting the on-line application and the supplemental forms.
|
|
|
- Claire Erin Robbins
- 9 years ago
- Views:
Transcription
1 DMC Corporate Medical Affairs/CVO 4707 St. Antoine, Ste. E510/Hutzel Building Mail Code 522 Detroit, Michigan Phone Fax Dear Applicant: Thank you for your interest in joining The Detroit Medical Center (DMC). We are pleased to offer you a more efficient and convenient way to complete and submit your application for membership and privileges. DMC now utilizes the CAQH Universal Provider Datasource online application. Please read the information below to assist you in submitting the on-line application and the supplemental forms. Once you have submitted all necessary documentation, the DMC Central Verification Office (CVO) will periodically contact you and provide an update on the processing of your application. If we are experiencing difficulty in obtaining any of the required verifications and references, we will ask your assistance in facilitating. Upon completion of the credentialing verification process, your application and supporting documentation will be forwarded to the appropriate Department to which you are applying for consideration and recommendation. Final action with respect to your application is the responsibility of the governing body of the DMC. You will be notified upon that final action. If you have any questions, please contact us at We look forward to receiving your completed application. Sincerely, Mary l. Merity, CPCS Mary L. Merity, CPCS Corporate Director DMC Corporate Medical Affairs

2 IMPORTANT CREDENTIALING INFORMATION Thank you for requesting an application for membership and privileges at the Detroit Medical Center (DMC). The DMC is committed to the highest quality of care and patient safety. In support of this goal, please review the following important information. I. BOARD CERTIFICATION REQUIREMENTS Effective July 1st, 2009, all applicants to the DMC Medical Staff must be board certified, or in the active certification process with board certification attained within five (5) years of completion of formal training. Board certification must be in the specific practice area in which clinical privileges are requested and by a recognized certifying board, i.e. American Board of Medical Specialties, American Osteopathic Association, American Dental Association or the American Board of Podiatric Surgery. Please note that the board certification requirements by individual clinical departments may be more stringent. If so, the department s requirements supersede the DMC minimum board certification requirement. Board certification must be maintained in those specialty boards that are time-limited. II. MEDICAL STAFF CATEGORY DETERMINED BY LEVEL OF ACTIVITY To maintain quality patient care and safety, the DMC must be able to review and evaluate a physician s clinical and professional performance. This requires active utilization of the DMC hospitals/ambulatory centers and meeting the activity requirements defined by the clinical department. If you are only planning to refer patients and/or anticipate minimum DMC patient volume, you may wish to request Affiliate status, Membership only (with no clinical privileges). This affiliation will allow you to electronically track your referred patients and participate in other WSU/DMC opportunities without having to meet certain medical staff requirements. IF YOU HAVE ANY QUESTIONS OR WISH ADDITIONAL INFORMATION, PLEASE CONTACT DMC CENTRAL VERIFICATION OFFICE AT

3 Central Verification Office (CVO) INSTRUCTIONS Completing the DMC Credentialing Application Process 1. ACCESS: DMC utilizes the CAQH provider credentialing application that is accessed via the Internet. If you are a registered user, click on This will take you to the CAQH website to complete/update the provider application. Click on Universal Provider DataSource. Then click on CAQH Provider Credentialing Application and follow the instructions. Once the application is complete, please ensure the Detroit Medical Center has been added as an authorized healthcare organization. If you are not registered with CAQH, please contact the DMC Central Verification Office to facilitate this process. 2. COMPLETE: Complete the following DMC hospital-specific documents: DMC Supplemental Application DMC Authorization for Release of Information/Liability form DMC Appointment and Membership Desired form DMC MPRO Medicare Statement DMC CME Attestation form DMC Delineation of Privileges form. Please review form carefully and note any extra documentation that may be required for your particular specialty, i.e., surgical summary, evidence of additional training, 2 year surgical case summary for pediatric surgical privileges, etc. DMC Health Access Center (if applicable) DMC Auto Fax Enrollment form (if applicable) 3. SUBMIT: Submit the following to the DMC Central Verification Office: DMC supplemental application and documents listed in #2 above. Copy of government-issued photo identification (driver s license). 1.5 x1.5 color photo. You may provide either a passport photo or a clear photo with a head shot. You may also e- mail a digital photo to [email protected]. $ DMC application fee. (For membership only, application fee is $200.) Make check payable to The Detroit Medical Center. Proof of U.S. citizenship (VISA, Green Card), if applicable. Proof of current and past professional liability insurance. For current insurance, documentation must state that this coverage extends to your practice within the DMC facilities. DMC policy mandates a minimum of $100,000/$300,000 coverage. Board certification certificates. Internship, residency program(s), and fellowship program(s) certificates of completion. Written explanation of any gaps in education/training and work history greater than 30 days. ACLS/BLS certificates, as required. Evidence of compliance with mandatory Tuberculosis Evaluation (within the last 12 months).

4 DMC SUPPLEMENTAL APPLICATION A. PERSONAL INFORMATION Applicant Full Name: Marital Status: Ethnicity (optional): Applicant Personal Spouse s Name: Citizenship: If not a US citizen, do you have authorization to work in the US? Yes No In addition to the three (3) professional peer references provided on your CAQH application, please provide two (2) additional references, preferably within your clinical specialty. These references may not be your residency director, fellowship director, current clinical department chairperson, current partners or associates in your practice. Name: Specialty: Address: Phone: City, State, Zip: Fax: address: Name: Specialty: Address: Phone: City, State, Zip: Fax: address: B. OFFICE PRACTICE INFORMATION 1. Type of practice Corporation Partnership Solo Hospital Based Hospital Employed Institution Rural/Federal Qualified Health Clinic 2. Do all offices have: Internet access Electronic medical record keeping system Capability for electronic billing billing code: 3. Do you have any investment or other financial interest in any health care delivery organization (i.e., home health care, laboratory, managed care organization, etc.)? Yes No If yes, please describe: 4. List financial partners:

5 C. DISCLOSURE INFORMATION Please provide a detailed explanation on a separate sheet for any YES responses to the questions below. Have any of the following been or are currently in the process of being denied, revoked, not renewed, suspended, limited, restricted, reviewed, placed on probation, or placed under other disciplinary action, either voluntarily or involuntarily? YES NO Employment by any hospital or institution? Professional society membership? At any time, have you ever been: YES NO Convicted of any criminal offense in any jurisdiction Convicted of a misdemeanor relating to a health profession, or received probation without a verdict, disposition in lieu of a trial, or an accelerated rehabilitation disposition of felony charges in any state, territory or country? Have you ever, at any time, or are you currently: YES NO Under audit by a Health Care Agency (i.e., Medicare, Medicaid, MDCH, or any insurance) Under indictment for any crime? The subject of an investigation by any private, federal or state health insurance program or state, territory or country licensing board? The subject of any adverse action reports to a state or federal agency? Sanctioned by a government program or agency for any reason? Have you ever, at any time, either voluntarily or involuntarily: YES NO Withdrawn your application for medical staff membership at any facility? Withdrawn your request for any clinical privileges at any facility? D. ATTESTATION STATEMENT I attest that the information provided in this supplemental application is true and complete to the best of my knowledge. Signature: Date:

6 DMC AUTHORIZATION FOR RELEASE OF INFORMATION/LIABILITY Full Name (PLEASE PRINT) Date For purposes of this authorization, hospital(s), means The Detroit Medical Center ( DMC ), each Detroit Medical Center hospital(s), DMC CARE (DMC owned and/or affiliated managed care plans), any entity for which DMC performs delegated credentialing or recredentialing services DMC Professional Liability Program ( DMC PLP ), DMC Physicians Group to which I am applying for medical staff(s) privileges and/or membership and includes members of its board of trustees, its medical staff(s), its administration and any other employee or agent of the hospital(s) having responsibility for collecting information, evaluating my competence and qualifications; or acting upon this application; Information includes all records, documents, medical records, and otherwise privileged or confidential information; Competence and qualifications including clinical ability, professional ethics, character, physical and mental health, emotional stability, ability to work with others, and moral and other qualifications for medical staff appointment(s), reappointment(s) and clinical privileges; and third-parties include without limitation (i) other hospitals and their trustees, directors, employees or agents, medical staffs and associations, (ii) licensing boards, (iii) other organizations and persons concerned with provider or physician performance or the quality and efficiency of patient care, (iv) malpractice carriers and other providers of professional liability coverage, and (v) the National Practitioner Data Bank. AUTHORIZATION By applying for appointment or reappointment to the medical staff(s) of the hospital(s): A I authorize the hospital(s) to consult with all third parties with whom or which I have been associated concerning my competence and qualification, or with any third parties who may have information bearing thereon (including malpractice carriers and defense counsel), and to receive and utilize any information received in response thereto, and to inspect any and all information which may be material to my qualifications and competence and I hereby release all third parties who provide information to hospital(s), from any and all liability for the transmittal in good faith and without malice of any information bearing on my qualifications and competence; in connection with any such request for but not limited to appointment and reappointment of medical staff(s) privileges and/or membership; B If the hospital(s) seek to gather information relating to my competence and qualifications from current or prior professional liability claims in which I am or was represented by counsel, I hereby waive any attorney-client privilege, whether such privilege is granted by the statues or case law of the State of Michigan or any other jurisdiction, and I hereby release any attorney or other person from any and all liability in connection with the release of such information to the hospital(s). C I authorize and release the hospital(s) from all liability for forwarding to any other hospital(s) or entity to which I may apply for privileges any information concerning me, my competence and qualifications, as hospital(s) has at the time of my application for appointment or hereafter acquires in accordance with the medical staff(s) bylaws; D I authorize and release the hospital(s) from all liability for forwarding to any affiliate of the hospital(s) copies of my application for appointment and/or membership including all attachments, and if appointed to the medical staff(s) of hospital(s), any and all information regarding any proceedings or action taken by hospital(s) regarding appointment, reappointment, and/or clinical privileges (including the granting, extension, reduction, suspension or termination thereof), utilization review of quality assurance information and any other information including without limitation information received from the National Practitioner Data Bank concerning my competence and qualifications which hospital(s) has at the time of my application for medical staff appointment(s) or hereafter acquires; E I release from all liability the hospital(s) and all third parties from any statements made or any action taken in good faith and without malice in connection with this application or any other applications made simultaneously herewith, and in connection with any proceedings for reappointment, and/or clinical privileges (including the granting, extension, reduction, suspension or termination thereof), or in connection with a transfer to any other department or section of the medical staff(s), or in connection with any other form of review of my qualifications and competence or of my professional practices in the hospital(s) conducted in accordance with the medical staff(s) bylaws; UNDERSTANDING & COMMITMENT F I express my willingness to appear for interviews with all individuals and before all committees of the medical staff(s) which may be requested of me by hospital(s) in regard to my application. G I acknowledge that I have received, or been given access to, the bylaws of the medical staff(s) and articles of incorporation and bylaws of the hospital(s) to which I have applied. H I agree to abide by the bylaws of the medical staff(s), and for clinical privileges, and by such rules and regulations as the medical staff(s) or any department thereof may from time to time enact, as the same may be amended from time to time. If I am granted appointment or clinical privileges at the hospital(s), I agree to conform to the then current articles of incorporation and bylaws of the hospital(s), their policies, including the DMC Code of Conduct. Further I agree to complete compliance and sexual harassment prevention training required during the term of my appointment. Whether or not I am granted appointment or clinical privileges at the hospital(s), I agree to be bound by the Medical Staff and hospital(s) rules and policies in all matters relating to the consideration of my application for appointment and reappointment; I If I am granted staff appointment(s) and clinical privileges, I agree to abide by all ethical requirements of the bylaws of the medical staff(s), including, without limitation, the requirement to provide for continuous care and supervision of my patients. I pledge to maintain the highest ethical standards and to abide by the codes and principles of ethics of my state and national professional societies and associations.
 having responsibility for collecting information, evaluating my competence and qualifications; or acting upon this application; Information includes all")
7 I further agree to abide by the professional practice act of the State of Michigan under which I am licensed. I pledge to maintain the standards of, and meet the requirements of, the Michigan Department of Public Health and the Joint Commission on Accreditation of Healthcare Organizations, so that hospital(s) may receive full licensure and accreditation at all times. I agree that I will not participate in any form of fee splitting. In complying with this principle, I understand that I am not to collect fees for others referring patients to me, nor permit other physicians or surgeons to collect fees from me; J I agree that the decision of the board of trustees on this or any other application or proceeding concerning my appointment(s) or privileges shall be final and binding; K I agree to keep the hospital(s) informed of the status, and any changes in status, of professional liability coverage and professional liability claims that may from time to time be brought against me. I also agree to keep the hospital(s) informed of any adverse actions taken or proposed to be taken against me by peer review organizations, the state licensing board, and other hospital(s) or health care entities with which I am also affiliated; L I agree that, in connection with the health history requested in this application an in any situation in which my physical or mental health is at issue, I will waive, in favor of the hospital(s), its agents and employees, and all members of its board of trustees, administration and medical staff(s), any medical or physician-patient privilege relating to such physical or mental condition, whether such privilege is granted by the statues or case law of the State of Michigan or any other jurisdiction, or is granted by the provisions of federal regulations relating to alcohol and drug abuse. I do agree to release, and I do hereby release any physician, hospital(s) or other person or entity providing such information, from any and all liability for the release of any information which, except for such waiver, would be privileges and confidential; I further agree to facilitate the release of such information by providing appropriate release and authorization forms; I understand that, in the event that any physician or hospital(s) continues to refuse to provide such information, the hospital(s) shall give no further consideration to my application for a staff appointment(s) or membership, and privileges, if previously granted, shall be terminated; M I further specifically acknowledge that the provisions of the medical staff(s) relating to confidentiality and release from liability are express conditions of my application for, and acceptance of, medical staff appointment(s) and the continuation of such appointment(s) and to my exercise of clinical privileges; N I understand and agree that I, as an applicant for a medical staff appointment(s), have the burden of producing adequate information for proper evaluation of my competence and qualifications, and for resolving any doubts about such competence and qualifications; O I understand that I am obligated to disclose in the above application all information which would be material to my being granted a medical staff appointment(s) of this hospital(s), and further understand that any misstatement(s) in, or omission(s) from, this application will constitute cause for denial of appointment, reappointment, or cause for summary dismissal from the medical staff(s); P I understand that under the Health Care Quality Improvement Act of 1986, as amended, the hospital(s) are required to query the National Practitioner Data Bank and to include the response from that agency in the materials to be reviewed by persons involved in the credentialing process. I also understand that the hospital(s) are required by law to advise the National Practitioner Data Bank of any adverse action which it takes with regard to a physician or dentist s application for staff privileges (i.e. active, courtesy), application for increase of privileges, if the hospital(s) decisions are based upon a physician or dentist s level of competency or upon any act of improper professional conduct. I understand that the hospital(s) have elected to comply with the voluntary or permissive reporting of any action taken by the hospital(s) with regard to applications of licensed health care practitioners other than physicians and dentists. For purposes of Health Care Quality Improvement Act an adverse action includes, but is not necessarily limited to a decision to deny privileges, or to grant privileges at a lower level than applied for, where the decision is based upon an evaluation or competence or an act of improper professional conduct. I further understand that the hospital(s) may query and/or report to any other data bank or agency which may be required by Federal or State law, and include responses from such queries in the materials to be reviewed by persons involved in the credentialing process. Q In the event I am applying to participate in DMC owned and/or affiliated managed care plans, I understand that references in this Authorization for Release of Information form to medical staff appointment(s) or reappointment(s) to the medical staff(s) shall be deemed to mean designation as a participating member of DMC owned and/or affiliated managed care plans. I understand, unless otherwise indicated, any DMC employed and/or faculty physician will be considered as applying for membership in DMC owned and affiliated managed care plans. I also understand that references to medical staff(s) bylaws shall be deemed to mean the DMC owned and/or affiliated managed care plan participation and/or appointment standards, whether in the form of medical staff(s) bylaws, rules, regulations or otherwise; and R I understand that the term Detroit Medical Center Hospitals shall mean and include Children s Hospital of Michigan, Detroit Receiving Hospital and University Health Center, Harper Hospital, Huron Valley Sinai Hospital, Hutzel Hospital, Rehabilitation Institute of Michigan, and Sinai-Grace Hospital, any successors and assignees of the foregoing, and any other designee of The Detroit Medical Center for credentialing for the purposes of managed care plans. I hereby represent that all information submitted by me in this application is true and complete to the best of my knowledge and belief. Signature of Applicant Date JCC (revised)

8 APPOINTMENT AND MEMBERSHIP DESIRED MEDICAL STAFF CATEGORY Please check one: ACTIVE AFFILIATE AFFILIATE/Membership Only No Clinical Privileges HOSPITAL MEMBERSHIP AND/OR PRIVILEGES Please check all hospitals where you intend to practice (this does not restrict privileges and you may add hospitals at any time upon notification to DMC Corporate Medical Affairs. You must also indicate which hospital will be your primary hospital. HOSPITALS Children s Hospital of Michigan Detroit Receiving Hospital Harper University Hospital Huron Valley Sinai Hospital Hutzel Women s Hospital Rehabilitation Institute of Michigan Sinai Grace Hospital DMC Surgical Hospital Berry Surgery Center PRACTICE LOCATIONS (Check all hospitals you wish to practice at) PRIMARY HOSPITAL (Select only one) MANAGED CARE PARTICIPATION Practitioners approved for DMC staff privileges will also receive DMC Managed Care privileges as part of the credentialing process. DMC Managed Care privileges will allow you to be enrolled in DMC Affiliated Managed Care Health Plans. Upon approval of DMC Managed Care privileges, practitioners will receive a Health Plan Enrollment packet. The packet will be sent to the mailing address indicated on your application, unless we are notified otherwise. Are you currently enrolled in any Health Plans? Yes No Are you affiliated with a Hospital Organization or Physician Organization Group? Yes No If so, please list This is a confidential professional/peer review and quality improvement document of the DMC. It is protected from disclosure pursuant to one or more of the provisions of MCL , MCL , MCL , MCL , MCL , and MCL a and other state and federal laws. Unauthorized disclosure or duplication is absolutely prohibited

9 Name: Address: City, State, Zip Code: In accord with 42 Code of Federal Regulations (CFR) we are providing the following: NOTICE TO PHYSICIANS Medicare payment to hospitals is based in part on each patient s principal and secondary diagnoses and the major procedures performed on the patient, as attested to by the patient s attending physician by virtue of his or her signature in the medical record. Anyone who misrepresents, falsifies, or conceals essential information required for payment of Federal funds, may be subject to fine, imprisonment, or civil penalty under applicable Federal laws. (42 CRF ) Your acknowledgment of receipt of this notice must be kept on file at the Detroit Medical Center for its hospitals: Children s Hospital of Michigan, Detroit Receiving Hospital, Harper University Hospital, Huron Valley-Sinai Hospital, Hutzel Women s Hospital, Rehabilitation Institute of Michigan, and Sinai-Grace Hospital. PLEASE SIGN THIS LETTER AND RETURN IT WITH YOUR APPLICATION PACKET. If you have any questions, please contact DMC Medical Affairs at (313) RECEIVED: Signature Date This is a confidential professional/peer review and quality improvement document of the DMC. It is protected from disclosure pursuant to one or more of the provisions of MCL , MCL , MCL , MCL , MCL , and MCL a and other state and federal laws. Unauthorized disclosure or duplication is absolutely prohibited

10 CONTINUING MEDICAL EDUCATION ATTESTATION In applying for appointment/reappointment to the medical staff (s) of the Detroit Medical Center, I attest and affirm that: 1. I am in full compliance with the State of Michigan requirements for Continuing Medical Education (CME) hours; 2. I meet the DMC Medical Staff requirements for Compliance Education as provided by the DMC; 3. I further attest that the majority of my attendance at CME programs were directly related to my areas of practice; and 4. I agree to provide proof of attendance and program content upon request. I understand and agree that I, as an applicant for a medical staff appointment(s) or reappointment, have the burden of producing adequate information for the proper evaluation of my competence and qualifications, and for resolving any doubts about such competence and qualifications. I understand that any misstatement(s) in, or omission(s) from, this CME Attestation will constitute just cause for denial of appointment, reappointment, or become cause for discipline, up to and including summary dismissal from the medical staff(s) and represent that all information submitted by me in this application is true and complete to the best of my knowledge and belief. Print Name Signature Date This is a confidential professional/peer review and quality improvement document of the DMC. It is protected from disclosure pursuant to one or more of the provisions of MCL , MCL , MCL , MCL , MCL , and MCL a and other state and federal laws. Unauthorized disclosure or duplication is absolutely prohibited

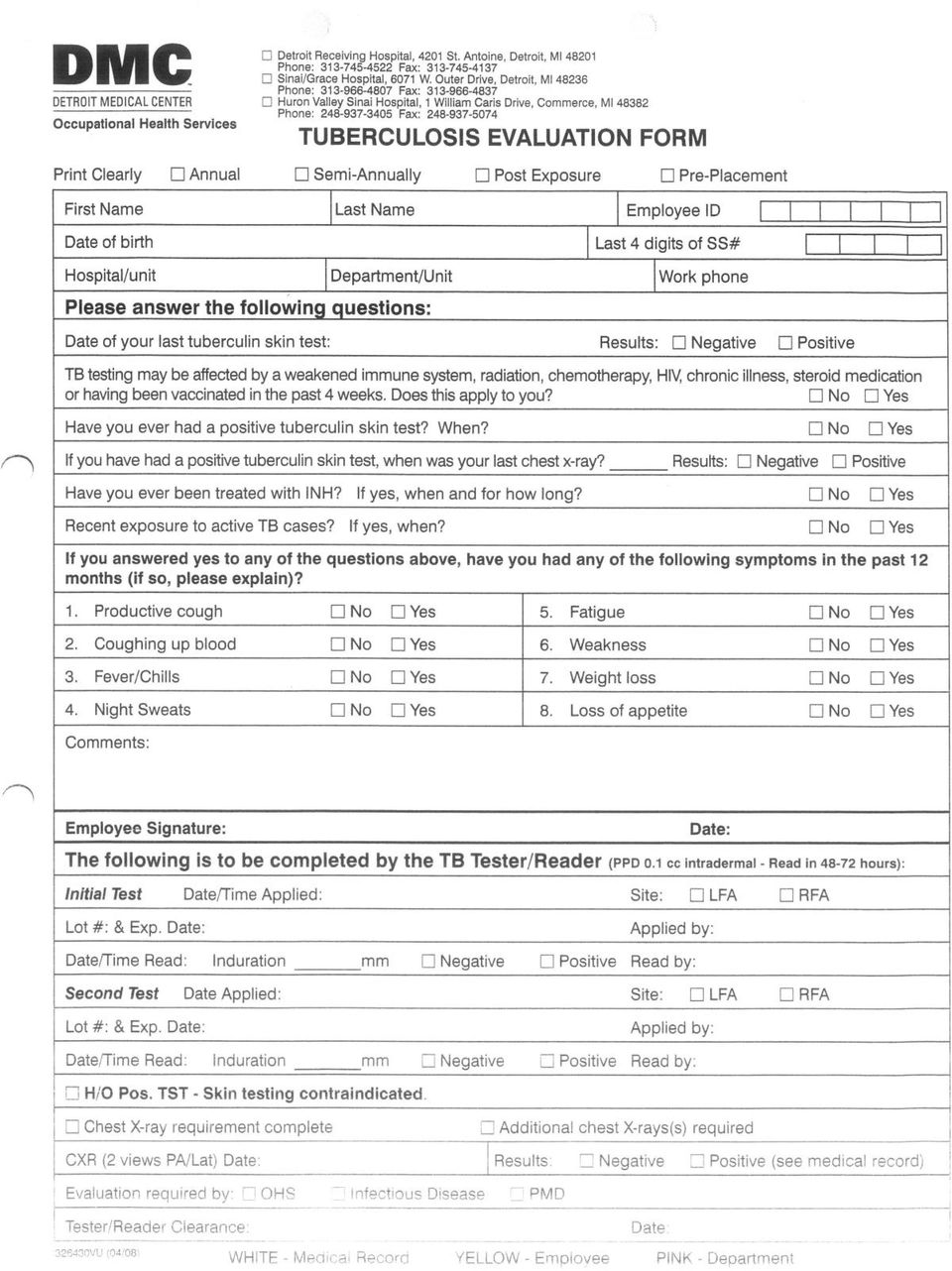
11 TB COMPLIANCE The Occupational Health and Safety Administration (OSHA) and the DMC (policy 1 CLN 013) require annual tuberculosis (TB) evaluation for all healthcare professionals. Evidence of this annual evaluation must be submitted with your initial application packet and annually thereafter. Results of your TB evaluation must be current, within the last twelve (12) months. It must be documented when read, in millimeters of induration. Free TB (Mantoux) test may be performed at any DMC hospital Occupational Health Services (OHS) department. If you are PPD positive, documentation of a recent chest x-ray is required. Chest x- ray (PA and lateral view) may be performed at any DMC facility where diagnostic radiology services are available, and may be covered by your insurance. Recent conversion to positive PPD and/or positive PPD refusing isoniazid prophylaxis treatment will need chest x-ray s for two (2) consecutive years. Following two consecutive clear x-rays and annual evaluation is sufficient. Form for completion of this evaluation is available via OHS or DMC Medical Affairs. DMC Occupational Health Services sites are available to assist you with the required testing or evaluation. OHS Central Region, University Health Center 4K OHS Sinai-Grace Hospital, 6071 W. Outer Drive, One South/Express Care OHS Huron Valley-Sinai Hospital, 1 st Floor Please call for hours of operation or if you have any other questions related to your TB evaluation. THANK YOU! This is a confidential professional/peer review and quality improvement document of the DMC. It is protected from disclosure pursuant to one or more of the provisions of MCL , MCL , MCL , MCL , MCL , and MCL a and other state and federal laws. Unauthorized disclosure or duplication is absolutely prohibited

12
13

14

Surgical Center of Greensboro/Orthopaedic Surgical Center Div of Surgical Care Affiliates
 Allied Health Staff Application Instructions We are pleased to provide you with our Allied Health Staff application packet. Please do not write see attached or see resume or CV on the application. All
Allied Health Staff Application Instructions We are pleased to provide you with our Allied Health Staff application packet. Please do not write see attached or see resume or CV on the application. All
APPLICATION FOR ALLIED PROFESSIONAL STAFF
 Office of Medical Affairs 736 Irving Ave Syracuse NY 13210 Phone: 315-470-7646 APPLICATION FOR ALLIED PROFESSIONAL STAFF Circle appropriate category CRNA Medical Physicist Research Assistant CST/Dntal
Office of Medical Affairs 736 Irving Ave Syracuse NY 13210 Phone: 315-470-7646 APPLICATION FOR ALLIED PROFESSIONAL STAFF Circle appropriate category CRNA Medical Physicist Research Assistant CST/Dntal
New Jersey Physician Recredentialing Application (Please type or print)
") New Jersey Physician Recredentialing Application (Please type or print) All sections must be completed fully or clearly marked as not applicable. No area should be left blank. SECTION 1 Personal Information
New Jersey Physician Recredentialing Application (Please type or print) All sections must be completed fully or clearly marked as not applicable. No area should be left blank. SECTION 1 Personal Information
MOONLIGHTING INSTRUCTIONS:
 MOONLIGHTING INSTRUCTIONS: Please Complete and Send the Forms on the Following 6 Pages to the Medical Staff Office at Box URMFG 278911. 1) URMC Moonlighting (extra work shift) Request Form, p. 1 of 6 2)
MOONLIGHTING INSTRUCTIONS: Please Complete and Send the Forms on the Following 6 Pages to the Medical Staff Office at Box URMFG 278911. 1) URMC Moonlighting (extra work shift) Request Form, p. 1 of 6 2)
LOCUM TENENS APPLICATION Page 1 of 4
 Page 1 of 4 This form is only valid for Locum Tenens providing coverage for up to 60 days. SECTION I PROVIDER INFORMATION This section to be completed by the PacificSource participating practitioner. Please
Page 1 of 4 This form is only valid for Locum Tenens providing coverage for up to 60 days. SECTION I PROVIDER INFORMATION This section to be completed by the PacificSource participating practitioner. Please
CREDENTIALING PROCEDURES MANUAL
 CREDENTIALING PROCEDURES MANUAL Page PART I Appointment Procedures 1 PART II Reappointment Procedures 5 PART III Delineation of Clinical Privileges Procedures 7 PART IV Leave of Absence, Reinstatement,
CREDENTIALING PROCEDURES MANUAL Page PART I Appointment Procedures 1 PART II Reappointment Procedures 5 PART III Delineation of Clinical Privileges Procedures 7 PART IV Leave of Absence, Reinstatement,
North Carolina Department of Insurance. Uniform Application. To Participate as a Health Care Practitioner
 orth Carolina Department of Insurance Uniform Application To Participate as a Health Care Practitioner ote: Please send completed applications directly to the organizations with which you seek to contract.
orth Carolina Department of Insurance Uniform Application To Participate as a Health Care Practitioner ote: Please send completed applications directly to the organizations with which you seek to contract.
Doctors Hospital Allied Health Professional Application for Appointment
 Doctors Hospital Allied Health Professional Application for Appointment Applying for the following job (please check): Allied Health Delineation of Privileges Allied Health Scope of Practice Category 1
Doctors Hospital Allied Health Professional Application for Appointment Applying for the following job (please check): Allied Health Delineation of Privileges Allied Health Scope of Practice Category 1
6325 Hospital Parkway Johns Creek, Georgia 30097 Phone 678-474-7000 emoryjohnscreek.com Dear Provider,
 Dear Provider, Thank you for your recent inquiry in credentialing at Emory Johns Creek Hospital. Through our affiliation with Emory Healthcare, we are pleased to announce that our application process is
Dear Provider, Thank you for your recent inquiry in credentialing at Emory Johns Creek Hospital. Through our affiliation with Emory Healthcare, we are pleased to announce that our application process is
Terrebonne General Medical Center 8166 Main Street Houma, Louisiana 70360 Human Resources (985) 873-4628 Phone 985-873-4481 Fax
 873-4628 Phone 985-873-4481 Fax") Terrebonne General Medical Center 8166 Main Street Houma, Louisiana 70360 Human Resources (985) 873-4628 Phone 985-873-4481 Fax APPLICATION FOR APPOINTMENT TO THE NON-CLINICAL ALLIED HEALTH STAFF Instructions
Terrebonne General Medical Center 8166 Main Street Houma, Louisiana 70360 Human Resources (985) 873-4628 Phone 985-873-4481 Fax APPLICATION FOR APPOINTMENT TO THE NON-CLINICAL ALLIED HEALTH STAFF Instructions
REHAB PROVIDER NETWORK Professional Staff Credentialing Form
 REHAB PROVIDER NETWORK Professional Staff Credentialing Form ***** THERAPIST LICENSE MUST BE ATTACHED TO THIS FORM ***** The information requested on this form is required to certify your status as a licensed
REHAB PROVIDER NETWORK Professional Staff Credentialing Form ***** THERAPIST LICENSE MUST BE ATTACHED TO THIS FORM ***** The information requested on this form is required to certify your status as a licensed
HENDRICK MEDICAL CENTER INITIAL APPOINTMENT ADDENDUM
 Attachment H HENDRICK MEDICAL CENTER INITIAL APPOINTMENT ADDENDUM TO THE TEXAS DEPARTMENT OF INSURANCE (TDI) STANDARDIZED CREDENTIALING APPLICATION SECTION ONE - PERSONAL INFORMATION Last Name: First Name:
Attachment H HENDRICK MEDICAL CENTER INITIAL APPOINTMENT ADDENDUM TO THE TEXAS DEPARTMENT OF INSURANCE (TDI) STANDARDIZED CREDENTIALING APPLICATION SECTION ONE - PERSONAL INFORMATION Last Name: First Name:
All Physicians must attend orientation. Your office will be contacted to schedule a time convenient for you.
 Dear Doctor: Thank you for your interest in applying for Medical Staff Membership and or Clinical Privileges at Northwest Texas Healthcare System/Northwest Texas Surgery Center and or Alliance Regional
Dear Doctor: Thank you for your interest in applying for Medical Staff Membership and or Clinical Privileges at Northwest Texas Healthcare System/Northwest Texas Surgery Center and or Alliance Regional
Resident Credentialing Policy Wayne State University
 Resident Credentialing Policy Wayne State University REQUIREMENTS FOR INITIAL RESIDENT APPOINTMENT Residency Office Responsibilities: 1. Resident Initial Appointment Recommendation Letter: Initial applications
Resident Credentialing Policy Wayne State University REQUIREMENTS FOR INITIAL RESIDENT APPOINTMENT Residency Office Responsibilities: 1. Resident Initial Appointment Recommendation Letter: Initial applications
MEDICAL STAFF POLICY & PROCEDURE
 240 Maple Street PO Box 470 Woodruff, WI 54568 (715) 356-8000 MEDICAL STAFF POLICY & PROCEDURE NUMBER: MS.4 EFFECTIVE/APPROVAL DATE: TITLE: CREDENTIALING POLICY REVISION DATE: 4/97; 1/98; 7/98; 2/99; 12/00;
240 Maple Street PO Box 470 Woodruff, WI 54568 (715) 356-8000 MEDICAL STAFF POLICY & PROCEDURE NUMBER: MS.4 EFFECTIVE/APPROVAL DATE: TITLE: CREDENTIALING POLICY REVISION DATE: 4/97; 1/98; 7/98; 2/99; 12/00;
Los Angeles County Department of Mental Health Credentialing Application for Prescribing Practitioners Delivering Services to DCFS Children
 Los Angeles County Department of Mental Health Credentialing Application for Prescribing Practitioners Delivering Services to DCFS Children This application is exclusively for prescribing practitioners
Los Angeles County Department of Mental Health Credentialing Application for Prescribing Practitioners Delivering Services to DCFS Children This application is exclusively for prescribing practitioners
Medical Staff Services. Dear Applicant,
 Dear Applicant, Thank you for your interest in seeking appointment to the Medical or Allied Health Professional (AHP) Staff of MedStar Montgomery Medical Center. All initial appointments to the Medical
Dear Applicant, Thank you for your interest in seeking appointment to the Medical or Allied Health Professional (AHP) Staff of MedStar Montgomery Medical Center. All initial appointments to the Medical
Rehab Net of Arkansas. Provider Application
 Rehab Net of Arkansas Provider Application Discipline P.T. O.T. S.L.P. (1) Business Name Physical Address FACILITY DATA Phone Fax (2) Billing Address Phone Fax (3) Mailing Address (4) Owner/Contact Person
Rehab Net of Arkansas Provider Application Discipline P.T. O.T. S.L.P. (1) Business Name Physical Address FACILITY DATA Phone Fax (2) Billing Address Phone Fax (3) Mailing Address (4) Owner/Contact Person
ONE CALL MEDICAL INC. NEURODIAGNOSTIC PHYSICIAN APPLICATION
 ONE CALL MEDICAL INC. NEURODIAGNOSTIC PHYSICIAN APPLICATION Provider has the right to review information submitted to support credentialing, correct erroneous information, to be informed of application
ONE CALL MEDICAL INC. NEURODIAGNOSTIC PHYSICIAN APPLICATION Provider has the right to review information submitted to support credentialing, correct erroneous information, to be informed of application
Dental Initial Credentialing Application
 Dental Initial Credentialing Application Practitioner and Practice Information Name(last) (First) (Middle) Degree Social Security Number Personal NPI Date of Birth Gender Practice Name Practice Taxpayer
Dental Initial Credentialing Application Practitioner and Practice Information Name(last) (First) (Middle) Degree Social Security Number Personal NPI Date of Birth Gender Practice Name Practice Taxpayer
LIBERTY DENTAL PLAN Provider Credentialing Application
 (Complete one application per Provider) (* Required Fields) Credentialing Information: Owner: Associate: *PROVIDER NAME: DDS DMD Other (specify) *DATE OF BIRTH: / / Gender: Male Female Owning Dentist Name:
(Complete one application per Provider) (* Required Fields) Credentialing Information: Owner: Associate: *PROVIDER NAME: DDS DMD Other (specify) *DATE OF BIRTH: / / Gender: Male Female Owning Dentist Name:
To Apply for BlueCross BlueShield of South Carolina and BlueChoice HealthPlan
 To Apply for BlueCross BlueShield of South Carolina and BlueChoice HealthPlan 1. Complete the SC Uniform Managed Care Provider Credentialing Application. 2. Enclose copies of the following items: A. State
To Apply for BlueCross BlueShield of South Carolina and BlueChoice HealthPlan 1. Complete the SC Uniform Managed Care Provider Credentialing Application. 2. Enclose copies of the following items: A. State
Please Note: Please send all documentation related to the credentialing portion of this documentation to:
 Please ote: The application process is split into different actions. Please send all documentation related to the contracting portion of this documentation to: Fax to: (916)350-8860 Or email to: [email protected]
Please ote: The application process is split into different actions. Please send all documentation related to the contracting portion of this documentation to: Fax to: (916)350-8860 Or email to: [email protected]
EFFECTIVE DATE: 10/04. SUBJECT: Primary Care Nurse Practitioners SECTION: CREDENTIALING POLICY NUMBER: CR-31
 SUBJECT: Primary Care Nurse Practitioners SECTION: CREDENTIALING POLICY NUMBER: CR-31 EFFECTIVE DATE: 10/04 Applies to all products administered by the plan except when changed by contract Policy Statement:
SUBJECT: Primary Care Nurse Practitioners SECTION: CREDENTIALING POLICY NUMBER: CR-31 EFFECTIVE DATE: 10/04 Applies to all products administered by the plan except when changed by contract Policy Statement:
PERSONAL DATA NOTE: SHADED PORTIONS N/A TO ALLIED HEALTH PROFESSIONALS. 1. Name. 2. Other Name(s) Previously Used Effective
 Previously Used Effective") For Credentialing Staff Use Only Specialty Date Application Received Attach a recent 2 x 2 passport size photograph for the master file and each facility marked on this application Date Application Signature
For Credentialing Staff Use Only Specialty Date Application Received Attach a recent 2 x 2 passport size photograph for the master file and each facility marked on this application Date Application Signature
To be appointed to Ohio Valley General Hospital's Medical Staff, the following items must be sent in the enclosed return envelope:
 MEDICAL STAFF APPOINTMENT CHECKLIST **Please complete entire application. Statements such as see attached are not acceptable and will be returned for completion. In order to process your application in
MEDICAL STAFF APPOINTMENT CHECKLIST **Please complete entire application. Statements such as see attached are not acceptable and will be returned for completion. In order to process your application in
GEORGIA UNIFORM HEALTHCARE PRACTITIONER CREDENTIALING APPLICATION FORM
 GEORGIA UNIFORM HEALTHCARE PRACTITIONER CREDENTIALING APPLICATION FORM Please contact the Hospital, Health Plan or other Healthcare Organization, hereinafter "Healthcare Entity(ies)", to which you are
GEORGIA UNIFORM HEALTHCARE PRACTITIONER CREDENTIALING APPLICATION FORM Please contact the Hospital, Health Plan or other Healthcare Organization, hereinafter "Healthcare Entity(ies)", to which you are
CRNA APPLICATION/CHECKLIST INSTRUCTIONS:
 MAXIM is an equal opportunity Employer and does not discriminate against otherwise qualified applicants on the basis of race, color, creed, religion, ancestry, age, sex, marital status, national origin,
MAXIM is an equal opportunity Employer and does not discriminate against otherwise qualified applicants on the basis of race, color, creed, religion, ancestry, age, sex, marital status, national origin,
CHECK THE CIRCUMSTANCE UNDER WHICH YOU ARE SEEKING A TEMPORARY LICENSE: REQUIRED DOCUMENTS
 Regular Mailing Address P.O. BOX 2649 HARRISBURG, PA 17105-2649 717-783-1400/717-787-2381 Email: [email protected] Courier Delivery Address 2601 NORTH THIRD STREET HARRISBURG, PA 17110 APPLICATION FOR
Regular Mailing Address P.O. BOX 2649 HARRISBURG, PA 17105-2649 717-783-1400/717-787-2381 Email: [email protected] Courier Delivery Address 2601 NORTH THIRD STREET HARRISBURG, PA 17110 APPLICATION FOR
ARKANSAS BOARD OF PODIATRIC MEDICINE
 ARKANSAS BOARD OF PODIATRIC MEDICINE APPLICATION FOR LICENSE TO PRACTICE PODIATRIC MEDICINE 1. Name: Social Security Number: (As to appear on License) 2. Address: 3. Address you wish License to be mailed:
ARKANSAS BOARD OF PODIATRIC MEDICINE APPLICATION FOR LICENSE TO PRACTICE PODIATRIC MEDICINE 1. Name: Social Security Number: (As to appear on License) 2. Address: 3. Address you wish License to be mailed:
MARYLAND HOSPITAL CREDENTIALING APPLICATION
 Error! STATE OF MARYLAND DHMH MARYLAND HOSPITAL CREDENTIALING APPLICATION Please type or print. Incomplete or illegible applications will not be processed. I. PERSONAL INFORMATION Name (Last, First, Middle)
Error! STATE OF MARYLAND DHMH MARYLAND HOSPITAL CREDENTIALING APPLICATION Please type or print. Incomplete or illegible applications will not be processed. I. PERSONAL INFORMATION Name (Last, First, Middle)
North Carolina Delta Dental s Recredentialing Application
 Delta Dental of North Carolina North Carolina Delta Dental s Recredentialing Application INCOMPLETE APPLICATIONS WILL BE RETURNED, WHICH WILL DELAY THE RECREDENTIALING PROCESS 1. The attached Recredentialing
Delta Dental of North Carolina North Carolina Delta Dental s Recredentialing Application INCOMPLETE APPLICATIONS WILL BE RETURNED, WHICH WILL DELAY THE RECREDENTIALING PROCESS 1. The attached Recredentialing
State of Tennessee Department of Health BOARD OF VETERINARY MEDICAL EXAMINERS
 State of Tennessee Department of Health BOARD OF VETERINARY MEDICAL EXAMINERS 665 Mainstream Drive Nashville TN 37243 (Toll Free Instate) 1-800-778-4123 Ext. 5325090 615-532-5090 tn.gov/health Procedures
State of Tennessee Department of Health BOARD OF VETERINARY MEDICAL EXAMINERS 665 Mainstream Drive Nashville TN 37243 (Toll Free Instate) 1-800-778-4123 Ext. 5325090 615-532-5090 tn.gov/health Procedures
DUE DATE: Please note: There will be a $175 late fee assessed for any packets that are received incomplete or not returned prior to this date.
 Dear Medical/Adjunct Staff Member: It is time for your biannual reappointment to the Medical Staff/Adjunct Staff of The University Hospital. Attached, you will find your application and delineation of
Dear Medical/Adjunct Staff Member: It is time for your biannual reappointment to the Medical Staff/Adjunct Staff of The University Hospital. Attached, you will find your application and delineation of
FLORIDA DEPARTMENT OF HEALTH BOARD OF DENTISTRY
 DENTAL RADIOGRAPHY CERTIFICATION APPLICATION Chapter 466.004 and 466.017(5), Florida Statutes Rule 64B5-9.011, Florida Administrative Code SPECIAL TES AND INSTRUCTIONS: 1. A N-REFUNDABLE fee of $35.00
DENTAL RADIOGRAPHY CERTIFICATION APPLICATION Chapter 466.004 and 466.017(5), Florida Statutes Rule 64B5-9.011, Florida Administrative Code SPECIAL TES AND INSTRUCTIONS: 1. A N-REFUNDABLE fee of $35.00
Initial Credentialing Application: Certified Registered Nurse Anesthetist (CRNA)
") Updated 1/1/2013 Specialty Surgery Center Initial Credentialing Application: Certified Registered Nurse Anesthetist (CRNA) Dear Anesthesia Provider, Thank you for your interest in providing services at
Updated 1/1/2013 Specialty Surgery Center Initial Credentialing Application: Certified Registered Nurse Anesthetist (CRNA) Dear Anesthesia Provider, Thank you for your interest in providing services at
NURSE PRACTITIONER/PHYSICIANS ASSISTANT APPLICATION GENERAL INFORMATION. Last Name First Middle. Place of Birth Social Security #
 Page 1 NURSE PRACTITIONER/PHYSICIANS ASSISTANT APPLICATION GENERAL INFORMATION Last Name First Middle Place of Birth Social Security # Home Address City State Zip Office Address City State Zip DOB Emergency
Page 1 NURSE PRACTITIONER/PHYSICIANS ASSISTANT APPLICATION GENERAL INFORMATION Last Name First Middle Place of Birth Social Security # Home Address City State Zip Office Address City State Zip DOB Emergency
REVISED 07-15 STATE BOARD OF SOCIAL WORKERS, MARRIAGE AND FAMILY THERAPISTS AND PROFESSIONAL COUNSELORS P.O. BOX 2649 HARRISBURG, PA 17105-2649
 STATE BOARD OF SOCIAL WORKERS, MARRIAGE AND FAMILY THERAPISTS AND PROFESSIONAL COUNSELORS P.O. BOX 2649 HARRISBURG, PA 17105-2649 Email [email protected] www.dos.pa.gov/social APPLICATION FOR A LICENSE
STATE BOARD OF SOCIAL WORKERS, MARRIAGE AND FAMILY THERAPISTS AND PROFESSIONAL COUNSELORS P.O. BOX 2649 HARRISBURG, PA 17105-2649 Email [email protected] www.dos.pa.gov/social APPLICATION FOR A LICENSE
MICHIGAN ASSOCIATION OF HEALTH PLANS Standard Practitioner Application
 MICHIGAN ASSOCIATION OF HEALTH PLANS Standard Practitioner Application This document was developed by the Michigan Association of Health Plans (MAHP) to serve as a standard, single application for practitioner
MICHIGAN ASSOCIATION OF HEALTH PLANS Standard Practitioner Application This document was developed by the Michigan Association of Health Plans (MAHP) to serve as a standard, single application for practitioner
REQUIREMENTS FOR LICENSURE:
 Email: [email protected] INITIAL APPLICATION FOR A NURSE-MIDWIFE LICENSE 1. This license class does not include prescriptive authority. If you wish to hold a certificate for prescriptive authority, you
Email: [email protected] INITIAL APPLICATION FOR A NURSE-MIDWIFE LICENSE 1. This license class does not include prescriptive authority. If you wish to hold a certificate for prescriptive authority, you
CREDENTIALING POLICY FOR ALLIED HEALTH PROFESSIONALS
 CREDENTIALING POLICY FOR ALLIED HEALTH PROFESSIONALS TABLE OF CONTENTS Article Page 1 DEFINITIONS.. 1 2 SCOPE AND OVERVIEW OF POLICY 2.1 Scope of Policy 3 2.2 Classification of Allied Health Professionals..
CREDENTIALING POLICY FOR ALLIED HEALTH PROFESSIONALS TABLE OF CONTENTS Article Page 1 DEFINITIONS.. 1 2 SCOPE AND OVERVIEW OF POLICY 2.1 Scope of Policy 3 2.2 Classification of Allied Health Professionals..
Applicants will be notified within 15 working days of receipt of a completed application as to the status of the application.
 2/09, 03/11, 11/11, 01/13, 01/15 Page 1 of 10 MONTANA BOARD OF RADIOLOGIC TECHLOGISTS 301 SOUTH PARK, 4TH FLOOR PO BOX 200513 HELENA, MONTANA 59620-0513 (406) 841-2202 FAX: (406) 841-2305 email: [email protected]
2/09, 03/11, 11/11, 01/13, 01/15 Page 1 of 10 MONTANA BOARD OF RADIOLOGIC TECHLOGISTS 301 SOUTH PARK, 4TH FLOOR PO BOX 200513 HELENA, MONTANA 59620-0513 (406) 841-2202 FAX: (406) 841-2305 email: [email protected]
Practice Name: Brief overview of your intended scope of practice at Anna Jaques Hospital:
 Medical Staff Application for Initial Appointment Supplemental Page Introduction (to be presented to the Credential Committee): Practice Name: Brief overview of your intended scope of practice at Anna
Medical Staff Application for Initial Appointment Supplemental Page Introduction (to be presented to the Credential Committee): Practice Name: Brief overview of your intended scope of practice at Anna
FLORIDA DEPARTMENT OF HEALTH BOARD OF DENTISTRY NON-PROFIT CORPORATION PERMIT APPLICATION
 FLORIDA DEPARTMENT OF HEALTH BOARD OF DENTISTRY N-PROFIT CORPORATION PERMIT APPLICATION Applications will be accepted only if completed by an officer of the non-profit organization. Any questions not applicable
FLORIDA DEPARTMENT OF HEALTH BOARD OF DENTISTRY N-PROFIT CORPORATION PERMIT APPLICATION Applications will be accepted only if completed by an officer of the non-profit organization. Any questions not applicable
FLORIDA DEPARTMENT OF HEALTH BOARD OF DENTISTRY
 FLORIDA DEPARTMENT OF HEALTH BOARD OF DENTISTRY APPLICATION FOR TEACHING PERMIT Chapter 466.002, Florida Statutes Rule 64B5-7.005, Florida Administrative Code Applications will be accepted only if completed
FLORIDA DEPARTMENT OF HEALTH BOARD OF DENTISTRY APPLICATION FOR TEACHING PERMIT Chapter 466.002, Florida Statutes Rule 64B5-7.005, Florida Administrative Code Applications will be accepted only if completed
FLORIDA DEPARTMENT OF HEALTH BOARD OF DENTISTRY APPLICATION FOR LIMITED LICENSURE DENTIST/DENTAL HYGIENIST
 Statute and Rule References: -Section 456.015, Florida Statutes -Rule 64B5-7.007, Florida Administrative Code APPLICATION FOR LIMITED LICENSURE DENTIST/DENTAL HYGIENIST General Requirements and Information
Statute and Rule References: -Section 456.015, Florida Statutes -Rule 64B5-7.007, Florida Administrative Code APPLICATION FOR LIMITED LICENSURE DENTIST/DENTAL HYGIENIST General Requirements and Information
Application for Medical Staff Appointment and Clinical Privileges. Part I. Credential Review
 Application for Medical Staff Appointment and Clinical Privileges Part I. Credential Review I am applying for clinical privileges at the location(s) checked below: 6209 16 th Avenue, Brooklyn, NY 11214
Application for Medical Staff Appointment and Clinical Privileges Part I. Credential Review I am applying for clinical privileges at the location(s) checked below: 6209 16 th Avenue, Brooklyn, NY 11214
ANCILLARY PROVIDER APPLICATION FOR PARTICIPATION PHYSICIANS HEALTH PLAN PO Box 30377, Lansing, MI 48909-7877 517.364.8312
 ANCILLARY PROVIDER APPLICATION FOR PARTICIPATION PHYSICIANS HEALTH PLAN PO Box 30377, Lansing, MI 48909-7877 517.364.8312 INSTRUCTIONS: Please provide answers to all questions. If the answer is none, or
ANCILLARY PROVIDER APPLICATION FOR PARTICIPATION PHYSICIANS HEALTH PLAN PO Box 30377, Lansing, MI 48909-7877 517.364.8312 INSTRUCTIONS: Please provide answers to all questions. If the answer is none, or
HOUSTON LAWYER REFERRAL SERVICE, INC. RULES OF MEMBERSHIP
 HOUSTON LAWYER REFERRAL SERVICE, INC. RULES OF MEMBERSHIP The Houston Lawyer Referral Service, Inc. (HLRS) is a non-profit corporation sponsored by the Houston Bar Association, Houston Young Lawyers Association,
HOUSTON LAWYER REFERRAL SERVICE, INC. RULES OF MEMBERSHIP The Houston Lawyer Referral Service, Inc. (HLRS) is a non-profit corporation sponsored by the Houston Bar Association, Houston Young Lawyers Association,
Credentials Policy Manual. Reviewed & Approved by MEC 8/13/2012 Reviewed & Approved by Board of Commissioners 9/11/12
 Credentials Policy Manual Reviewed & Approved by MEC 8/13/2012 Reviewed & Approved by Board of Commissioners 9/11/12 Credentialing Policy Manual Table of Contents I. Application for Appointment to Staff...1
Credentials Policy Manual Reviewed & Approved by MEC 8/13/2012 Reviewed & Approved by Board of Commissioners 9/11/12 Credentialing Policy Manual Table of Contents I. Application for Appointment to Staff...1
TEMPLE UNIVERSITY HOSPITAL
 u TEMPLE UNIVERSITY HOSPITAL INSTRUCTIONS FOR APPLYING FOR EMERGENCY TEMPORARY PRIVILEGES FOR NON-APPLICANTS (these privileges are for care of patients during and emergency disaster) ************************************************************************
u TEMPLE UNIVERSITY HOSPITAL INSTRUCTIONS FOR APPLYING FOR EMERGENCY TEMPORARY PRIVILEGES FOR NON-APPLICANTS (these privileges are for care of patients during and emergency disaster) ************************************************************************
Washington Practitioner Application
 Washington Practitioner Application To use the Washington Practitioner Application (WPA), follow these instructions: Keep an unsigned and undated copy of the application on file for future requests. When
Washington Practitioner Application To use the Washington Practitioner Application (WPA), follow these instructions: Keep an unsigned and undated copy of the application on file for future requests. When
Revised July 2014 MEDICAL STAFF BYLAWS OF MINISTRY OUR LADY OF VICTORY HOSPITAL, INC.
 MEDICAL STAFF BYLAWS OF MINISTRY OUR LADY OF VICTORY HOSPITAL, INC. DEFINITIONS 1. MEDICAL STAFF means all Doctors of Medicine, Doctors of Osteopathy, Doctors of Dentistry and Doctors of Podiatry, who
MEDICAL STAFF BYLAWS OF MINISTRY OUR LADY OF VICTORY HOSPITAL, INC. DEFINITIONS 1. MEDICAL STAFF means all Doctors of Medicine, Doctors of Osteopathy, Doctors of Dentistry and Doctors of Podiatry, who
CREDENTIALING POLICY AND PROCEDURES MANUAL OF THE MEDICAL STAFF OF ADVENTIST HINSDALE HOSPITAL AND ADVENTIST LA GRANGE MEMORIAL HOSPITAL
 CREDENTIALING POLICY AND PROCEDURES MANUAL OF THE MEDICAL STAFF OF ADVENTIST HINSDALE HOSPITAL AND ADVENTIST LA GRANGE MEMORIAL HOSPITAL Approval: Medical Executive Committees: Hinsdale Hospital July 28,
CREDENTIALING POLICY AND PROCEDURES MANUAL OF THE MEDICAL STAFF OF ADVENTIST HINSDALE HOSPITAL AND ADVENTIST LA GRANGE MEMORIAL HOSPITAL Approval: Medical Executive Committees: Hinsdale Hospital July 28,
VANTAGE HEALTH PLAN FACILITY CREDENTIALING APPLICATION
 VANTAGE HEALTH PLAN FACILITY CREDENTIALING APPLICATION GENERAL INFORMATION Primary Practice Facility Location The type of application being submitted: Initial Credentialing Re-Credentialing Hospital (Acute,
VANTAGE HEALTH PLAN FACILITY CREDENTIALING APPLICATION GENERAL INFORMATION Primary Practice Facility Location The type of application being submitted: Initial Credentialing Re-Credentialing Hospital (Acute,
PRACTITIONER CREDENTIALING APPLICATION Advanced Practice Nurse Prescriber, Certified Nurse Midwife, Physician Assistant
 PRACTITIONER CREDENTIALING APPLICATION Advanced Practice Nurse Prescriber, Certified Nurse Midwife, Physician Assistant Prior to submitting this application it is required that you contact the Provider
PRACTITIONER CREDENTIALING APPLICATION Advanced Practice Nurse Prescriber, Certified Nurse Midwife, Physician Assistant Prior to submitting this application it is required that you contact the Provider
POLICY REGARDING ADVANCED PRACTICE NURSES, PHYSICIAN ASSISTANTS AND OTHER CREDENTIALED HEALTH CARE PROVIDERS
 MEDICAL-DENTAL STAFF BYLAWS, POLICIES, AND RULES AND REGULATIONS OF CHRISTIANA CARE HEALTH SERVICES, INC POLICY REGARDING ADVANCED PRACTICE NURSES, PHYSICIAN ASSISTANTS AND OTHER CREDENTIALED HEALTH CARE
MEDICAL-DENTAL STAFF BYLAWS, POLICIES, AND RULES AND REGULATIONS OF CHRISTIANA CARE HEALTH SERVICES, INC POLICY REGARDING ADVANCED PRACTICE NURSES, PHYSICIAN ASSISTANTS AND OTHER CREDENTIALED HEALTH CARE
The University of Utah Health Plans offers the following plans and networks. Please specify the networks you are interested in participating with:
 Provider Networks Provider Applicant Process University of Utah Health Plans (UUHP) contracts with physicians and other health care professionals and facilities to offer provider networks essential to
Provider Networks Provider Applicant Process University of Utah Health Plans (UUHP) contracts with physicians and other health care professionals and facilities to offer provider networks essential to
Allied Health Professional Liability Insurance Application Form
 Allied Health Professional Liability Insurance Application Form With your fully completed, signed and dated application, you must submit the following information: 1. Current insurance policy declarations
Allied Health Professional Liability Insurance Application Form With your fully completed, signed and dated application, you must submit the following information: 1. Current insurance policy declarations
HOSPITAL-ANCILLARY-CLINIC PROVIDER CREDENTIALING APPLICATION
 HOSPITAL-ANCILLARY-CLINIC PROVIDER CREDENTIALING APPLICATION INSTRUCTIONS: In order to be considered complete: 1. All information must be legible. Please print or type all information 2. Application must
HOSPITAL-ANCILLARY-CLINIC PROVIDER CREDENTIALING APPLICATION INSTRUCTIONS: In order to be considered complete: 1. All information must be legible. Please print or type all information 2. Application must
Allied Healthcare Professional (AHP) Professional Liability Application
 Professional Liability Application") Allied Healthcare Professional (AHP) Professional Liability Application Coverys RRG, Inc. Agency Name NOTICE: This policy is issued by your risk retention group. Your risk retention group may not be subject
Allied Healthcare Professional (AHP) Professional Liability Application Coverys RRG, Inc. Agency Name NOTICE: This policy is issued by your risk retention group. Your risk retention group may not be subject
NC General Statutes - Chapter 93B 1
 Chapter 93B. Occupational Licensing Boards. 93B-1. Definitions. As used in this Chapter: "License" means any license (other than a privilege license), certificate, or other evidence of qualification which
Chapter 93B. Occupational Licensing Boards. 93B-1. Definitions. As used in this Chapter: "License" means any license (other than a privilege license), certificate, or other evidence of qualification which
APPLICATION FOR A LICENSE BY EXAMINATION TO PRACTICE MARRIAGE AND FAMILY THERAPY
 QUALIFICATIONS STATE BOARD OF SOCIAL WORKERS, MARRIAGE AND FAMILY THERAPISTS AND PROFESSIONAL COUNSELORS P.O. BOX 2649 HARRISBURG, PA 17105-2649 Email [email protected] Website www.dos.pa.gov/social
QUALIFICATIONS STATE BOARD OF SOCIAL WORKERS, MARRIAGE AND FAMILY THERAPISTS AND PROFESSIONAL COUNSELORS P.O. BOX 2649 HARRISBURG, PA 17105-2649 Email [email protected] Website www.dos.pa.gov/social
ALL APPLICANTS MUST COMPLETE THE FOLLOWING:
 APPLICATION FOR ATHLETIC TRAINER LICENSE (This application may also be used for a temporary license) 1. An applicant for licensure shall meet one of the following requirements: a. Be a graduate of an approved
APPLICATION FOR ATHLETIC TRAINER LICENSE (This application may also be used for a temporary license) 1. An applicant for licensure shall meet one of the following requirements: a. Be a graduate of an approved
EMPLOYMENT/CREDENTIALING APPLICATION
 Beacon Specialized Living Services, Inc. EMPLOYMENT/CREDENTIALING APPLICATION We do not discriminate on the basis of race, color, religion, national origin, sex, age or disability. It is our intention
Beacon Specialized Living Services, Inc. EMPLOYMENT/CREDENTIALING APPLICATION We do not discriminate on the basis of race, color, religion, national origin, sex, age or disability. It is our intention
2. Be of good moral character. Have 2 recommendations completed on page 3.
 STATE BOARD OF SOCIAL WORKERS, MARRIAGE AND FAMILY THERAPISTS AND PROFESSIONAL COUNSELORS P.O. BOX 2649 HARRISBURG, PA 17105-2649 717-783-1389 FAX 717-787-7769 Email [email protected] Website www.dos.pa.gov/social
STATE BOARD OF SOCIAL WORKERS, MARRIAGE AND FAMILY THERAPISTS AND PROFESSIONAL COUNSELORS P.O. BOX 2649 HARRISBURG, PA 17105-2649 717-783-1389 FAX 717-787-7769 Email [email protected] Website www.dos.pa.gov/social
Dear Applicant: Sincerely, Kelli Dalrymple, Coordinator Medical and Specialized Health. Licensure Unit
 Please Reply To: Licensure Unit P.O. Box 94986, Lincoln, NE 68509-4986 Phone (402) 471-2118 FAX (402) 471-3577 Dear Applicant: Thank you for your interest in becoming licensed to practice your profession
Please Reply To: Licensure Unit P.O. Box 94986, Lincoln, NE 68509-4986 Phone (402) 471-2118 FAX (402) 471-3577 Dear Applicant: Thank you for your interest in becoming licensed to practice your profession
REQUIREMENTS FOR CERTIFICATION:
 Email: [email protected] INITIAL APPLICATION FOR NURSE-MIDWIFE PRESCRIPTIVE AUTHORITY * A separate prescriptive authority collaborative agreement must be submitted for each physician, physician group
Email: [email protected] INITIAL APPLICATION FOR NURSE-MIDWIFE PRESCRIPTIVE AUTHORITY * A separate prescriptive authority collaborative agreement must be submitted for each physician, physician group
Clinical Observership Program
 Clinical Observership Program PROGRAM APPLICATION (Please type or print) Please place a checkmark (X) indicating the primary campus you prefer to spend your clinical observership experience: Weill Cornell
Clinical Observership Program PROGRAM APPLICATION (Please type or print) Please place a checkmark (X) indicating the primary campus you prefer to spend your clinical observership experience: Weill Cornell
APPLICANTS MUST COMPLETE THE FOLLOWING:
 Regular Mailing Address P.O. BOX 2649 HARRISBURG, PA 17105-2649 717-783-1400/717-787-2381 Email: [email protected] Courier Delivery Address 2601 NORTH THIRD STREET HARRISBURG, PA 17110 APPLICATION FOR
Regular Mailing Address P.O. BOX 2649 HARRISBURG, PA 17105-2649 717-783-1400/717-787-2381 Email: [email protected] Courier Delivery Address 2601 NORTH THIRD STREET HARRISBURG, PA 17110 APPLICATION FOR
CREDENTIALING POLICY OF UNIVERSITY OF UTAH HOSPITAL AND CLINICS
 CREDENTIALING POLICY OF UNIVERSITY OF UTAH HOSPITAL AND CLINICS Revised November, 2004 TABLE OF CONTENTS PAGE 1. DEFINITIONS...1 1.A DEFINITIONS...1 1.B TIME LIMITS...2 1.C DELEGATION OF FUNCTIONS...2
CREDENTIALING POLICY OF UNIVERSITY OF UTAH HOSPITAL AND CLINICS Revised November, 2004 TABLE OF CONTENTS PAGE 1. DEFINITIONS...1 1.A DEFINITIONS...1 1.B TIME LIMITS...2 1.C DELEGATION OF FUNCTIONS...2
PHYSICIAN APPLICATION FOR EMPLOYMENT
 PLEASE COMPLETE The Following. DATE Name Last First Middle Maiden Address City State Zip Date of Birth Place of Birth Social Security Number US Citizen Home Phone Email Address Specialty/Sub-specialty
PLEASE COMPLETE The Following. DATE Name Last First Middle Maiden Address City State Zip Date of Birth Place of Birth Social Security Number US Citizen Home Phone Email Address Specialty/Sub-specialty
TECHNICIAN-IN-TRAING IS NOT PERMITTED TO PRACTICE IN MONTANA IN ANY MANNER WITHOUT AN ACTIVE MONTANA REGISTRATION
 Page 1 of 8 MONTANA BOARD OF PHARMACY (301 S PARK, 4 TH FLOOR, HELENA, MT 59601 - Delivery) P. O. Box 200513 Helena, Montana 59620-0513 PHONE (406) 841-2300 FAX (406) 841-2344 E-MAIL: [email protected]
Page 1 of 8 MONTANA BOARD OF PHARMACY (301 S PARK, 4 TH FLOOR, HELENA, MT 59601 - Delivery) P. O. Box 200513 Helena, Montana 59620-0513 PHONE (406) 841-2300 FAX (406) 841-2344 E-MAIL: [email protected]
INITIAL CREDENTIALING APPLICATION
 Attn: Fax #: Phone #: INITIAL CREDENTIALING APPLICATION Dear Provider: To participate in our Sierra Health Services network, all practitioners must complete our credentialing process prior to contracting.
Attn: Fax #: Phone #: INITIAL CREDENTIALING APPLICATION Dear Provider: To participate in our Sierra Health Services network, all practitioners must complete our credentialing process prior to contracting.
APPLICATION FOR A TEACHER S LICENSE - DENTISTRY OR DENTAL HYGIENE
 Maryland State Board of Dental Examiners Spring Grove Hospital Center Benjamin Rush Building 55 Wade Avenue Catonsville, Maryland 21228 (410) 402-8510 APPLICATION FOR A TEACHER S LICENSE - DENTISTRY OR
Maryland State Board of Dental Examiners Spring Grove Hospital Center Benjamin Rush Building 55 Wade Avenue Catonsville, Maryland 21228 (410) 402-8510 APPLICATION FOR A TEACHER S LICENSE - DENTISTRY OR
NEIGHBORHOOD HEALTH PLAN OFRHODE ISLAND CREDENTIALING PRACTITIONER APPLICATION
 NEIGHBORHOOD HEALTH PLAN OFRHODE ISLAND CREDENTIALING PRACTITIONER APPLICATION Neighborhood accepts the Council for Affordable Quality Healthcare (CAQH) application in lieu of Neighborhood s standard credentialing
NEIGHBORHOOD HEALTH PLAN OFRHODE ISLAND CREDENTIALING PRACTITIONER APPLICATION Neighborhood accepts the Council for Affordable Quality Healthcare (CAQH) application in lieu of Neighborhood s standard credentialing
DEPARTMENT OF HEALTH CARE FINANCE
 DEPARTMENT OF HEALTH CARE FINANCE Dear Provider: Enclosed is the District of Columbia Medicaid provider enrollment application solely used for providers, who request to be considered for the Adult Substance
DEPARTMENT OF HEALTH CARE FINANCE Dear Provider: Enclosed is the District of Columbia Medicaid provider enrollment application solely used for providers, who request to be considered for the Adult Substance
Blue Cross Blue Shield of Arizona Dental Provider Contracting Request and Information Form
 . Blue Cross Blue Shield of Arizona Dental Provider Contracting Request and Information Form Thank you for your interest in becoming a contracted dental provider. In order to be considered for a contract
. Blue Cross Blue Shield of Arizona Dental Provider Contracting Request and Information Form Thank you for your interest in becoming a contracted dental provider. In order to be considered for a contract
APPLICATION FOR A LICENSE TO PRACTICE SOCIAL WORK (THIS APPLICATION MUST BE SUBMITTED FOR PRE-APPROVAL TO TAKE THE ASWB MASTER S EXAMINATION)
") STATE BOARD OF SOCIAL WORKERS, MARRIAGE AND FAMILY THERAPISTS AND PROFESSIONAL COUNSELORS P O BOX 2649 HARRISBURG, PA 17105 717-783-1389 [email protected] Fax 717-787-7769 www.dos.pa.gov/social APPLICATION
STATE BOARD OF SOCIAL WORKERS, MARRIAGE AND FAMILY THERAPISTS AND PROFESSIONAL COUNSELORS P O BOX 2649 HARRISBURG, PA 17105 717-783-1389 [email protected] Fax 717-787-7769 www.dos.pa.gov/social APPLICATION
Cenpatico Facility/Agency Credentialing Application INSTRUCTIONS
 Cenpatico Facility/Agency Credentialing Application INSTRUCTIONS Please complete the application thoroughly in its entirety. The checklist below may not be exhaustive of all materials, but is provided
Cenpatico Facility/Agency Credentialing Application INSTRUCTIONS Please complete the application thoroughly in its entirety. The checklist below may not be exhaustive of all materials, but is provided
PENNSYLVANIA STATE BOARD OF DENTISTRY P.O. BOX 2649 HARRISBURG, PA 17105-2649
 PENNSYLVANIA STATE BOARD OF DENTISTRY APPLICATION FOR CERTIFICATION AS A PUBLIC HEALTH DENTAL HYGIENE PRACTITIONER Introduction: Instructions and Application Form Please read the following instructions
PENNSYLVANIA STATE BOARD OF DENTISTRY APPLICATION FOR CERTIFICATION AS A PUBLIC HEALTH DENTAL HYGIENE PRACTITIONER Introduction: Instructions and Application Form Please read the following instructions
Community Health Group Allied Health Professional Application
 Community Health Group Allied Health Professional Application Nurse Practitioner Certified Nurse Midwife LCSW Clinical Psychologist MFCC Other I. INSTRUCTIONS This form should be typed or legibly printed
Community Health Group Allied Health Professional Application Nurse Practitioner Certified Nurse Midwife LCSW Clinical Psychologist MFCC Other I. INSTRUCTIONS This form should be typed or legibly printed
APPLICATION FOR ADDICTION COUNSELOR TRAINEE RECOGNITION OR ADDICTION COUNSELOR TRAINEE RENEWAL
 Board of Addiction and Prevention Professionals (BAPP) 3101 West 41 st Street, Suite 205, Sioux Falls, SD 57105 Phone: 605-332-2645 Fax: 605-332-6778 Email: [email protected] Web: www.dss.sd.gov/bapp
Board of Addiction and Prevention Professionals (BAPP) 3101 West 41 st Street, Suite 205, Sioux Falls, SD 57105 Phone: 605-332-2645 Fax: 605-332-6778 Email: [email protected] Web: www.dss.sd.gov/bapp
The Ideal Credentialing Standards: Best Practice Criteria and Protocol for Hospitals
 The Ideal Credentialing Standards: Best Practice Criteria and Protocol for Hospitals Credentialing best practices include an evidence-based evaluation that verifies 13 specific criteria from primary sources.
The Ideal Credentialing Standards: Best Practice Criteria and Protocol for Hospitals Credentialing best practices include an evidence-based evaluation that verifies 13 specific criteria from primary sources.
Allied Health Professional Rules and Regulations
 Allied Health Professional Rules and Regulations I. Purpose To maintain an organized Allied Health Professional Staff committed to promoting effective delivery of patient services, and continuous review
Allied Health Professional Rules and Regulations I. Purpose To maintain an organized Allied Health Professional Staff committed to promoting effective delivery of patient services, and continuous review
WRAPAROUND MILWAUKEE Policy & Procedure
 WRAPAROUND MILWAUKEE Policy & Procedure Wraparound Wraparound-REACH FISS Project O-Yeah I. POLICY Date Issued: 11/15/07 Effective Date: 1/1/15 Reviewed: 10/20/14 By: WA Last Revision: 10/20/14 Subject:
WRAPAROUND MILWAUKEE Policy & Procedure Wraparound Wraparound-REACH FISS Project O-Yeah I. POLICY Date Issued: 11/15/07 Effective Date: 1/1/15 Reviewed: 10/20/14 By: WA Last Revision: 10/20/14 Subject: