ISLET TRANSPLANT APPLICATION FORM
|
|
|
- Candace Butler
- 8 years ago
- Views:
Transcription
1 5/2014 Page 1 of 17 ISLET TRANSPLANT APPLICATION FORM INSTRUCTIONS: This application and the information you provide will be used to determine if you are able to participate in an islet transplant trial at the. We will maintain your information in a secure location and it will be accessed only by our research staff. This information will not be reused or disclosed to any other person or entity, except as required by law. The information you will provide will be stored in our files for a period not to exceed ten (10) years. If you give us permission, even if you are not eligible, we would like to keep your information in our files. CONSENT TO BE CONTACTED FOR CLINICAL TRIALS AT THE DIABETES RESEARCH INSTITUTE: I, (Print Name) agree to be contacted by the Clinical Islet Transplantation Program (CITP) team regarding future clinical trials for which I may be eligible. I also agree and consent that my name and contact information may be provided by the CITP to other departments at the for the purpose of clinical trial information and/or eligibility screening. Signature: Date: Phone # Please complete the entire application form and mail it to us at: Clinical Islet Transplant Program PO Box (R134) Miami, FL You may fax a copy of the completed form to , but we ask that you also mail the original form to us. Be sure to keep copies for your records.
 years.")
2 5/2014 Page 2 of 17 ISLET TRANSPLANT CANDIDATE INFORMATION FORM Please read all questions carefully and complete ALL the pages. Print clearly and do not leave any blanks. Write N/A for any questions that do not apply. Ap p l i c a n t s Personal Information (please print clearly). 1. Name (Last, MI, First) 2.Date of Birth(MM/DD/YY) 3. Age: 4. Gender: Male 5. Street Address 6. Occupation: Female 7. City 8. State/Prov 9.Zip/Postal Code 10. Address 11. Home Telephone 12. Work Telephone 13. Cell Phone Number 14. Fax Number 15.Emergency Contact 16. Telephone 17. Relationship 18. How did you hear about us? Complete this section (about yourself) if you are entering the information for the applicant 19. Name (Last, First) 20. Address, City, State, ZIP 21.Telephone 22. Address 23. Relationship Social Information 24. Marital Status: Never married Married Separated Divorced Widowed 25. Ethnic/Race Background: American Indian or Alaskan Native Asian Black or African American Hispanic or Latino Native Hawaiian or other Pacific Islander White or Caucasian 26. Current weight: lbs. Your height: ft. in. 27. Are you a current smoker? Yes No If yes, enter number of cigarettes per day and for how long you have been smoking years 28. Do you have a history of smoking? Yes No If yes, how many cigarettes per day did you smoke? What year did you stop smoking? How many years did you smoke? 29. Do you consume alcoholic beverages? Yes No If yes, enter the average number of alcoholic beverages you drink per week Type of beverage 30. Are you of childbearing age? Yes No If yes, are you currently: pregnant breast feeding List any method of birth control you currently use:
 if you are entering the information for the applicant 19. Name (Last, First) 20.")
3 5/2014 Page 3 of 17 Diabetes Information: 31. Diabetes: Type 1 Type2 32. Date Diagnosed: Month/year 33. Age at Diagnosis: 34. Diabetes Duration: years History of Diabetes Complications of the eyes, kidneys, nerves, cardiovascular & DKA 35. Do you have or have you ever had diabetic eye disease (retinopathy)? YES NO If you answer no to the previous question, go to question #36. If you answered yes to the previous question, please answer the following questions: 35.a. Which eye is/was affected? Left Right Both 35.b. What kind of retinopathy do you have? Active proliferative Stable proliferative Non-proliferative 35.c. Have you ever had eye surgery (laser therapy or vitrectomy)? YES NO If yes, which eye? Date of procedure: 36. Do you have diabetic kidney disease (nephropathy)? YES NO If you answer no to the previous question, go to question #37. If you answered yes to the previous question, please answer the following questions: 36.a What kidney condition do you have? Elevated creatinine Microalbuminuria Moderate to severe proteinuria Kidney failure 36.b. Are you on dialysis? YES NO 36.c. Have you had a kidney transplant? YES NO If Yes, date: Hospital/Surgeon:_ 37. Do you have diabetic nerve damage (neuropathy)? YES NO 37.a. If you answered yes to the previous question, please check all that apply: Numbness in hands/feet Sensory loss dizziness on standing rapid heartbeat at rest Nausea/Vomiting Diarrhea Bloating Problems with sexual function Other: 38. Do you have diabetic damage of the blood vessels (cardiovascular disease)? YES NO 38.a. If you answered yes to the previous question, please check all (treated and untreated) that apply: High blood pressure High cholesterol High triglycerides Low HDL High LDL Heart (heart attack/angina) Stroke/TIA Leg pain when walking (PVD/claudication) Bypass surgery Amputation (specify site): Other:
?")
4 5/2014 Page 4 of Do you have unstable diabetes that has failed to respond to intensive insulin therapy as judged by an Endocrinologist or Diabetologist? YES NO 40.. Have you ever had diabetic Ketoacidosis (DKA) or high blood sugar with ketones requiring hospitalization? YES NO 40.a. If you answered yes to DKA, how many times in the past year? History of Diabetes Complications, Hypoglycemia 41. Do you suffer from frequent low blood sugars that result in loss of YES NO consciousness? 42. Do you have hypoglycemia unawareness? YES NO (inability to sense when your blood sugar is low) Hypoglycemia score (recall) 43. Have you ever needed help from someone else to recognize a low blood YES NO sugar? 43.a. If you answered, yes to the previous question, how many times has this occurred in the last 12 months? 44. Have you ever needed help from someone else to treat a low blood YES NO sugar? 44.a. If you answered, yes to the previous question, how many times has this occurred in the last 12 months? 45. Have you ever needed glucagon injections to treat a low blood sugar? YES NO 45.a. If you have answered, yes to the previous question, how many times has this occurred in the past 12 months? 46. Have you ever been taken to an Emergency Room or had an YES NO ambulance called for you in order to treat a low blood sugar? 46.a. If you have answered, yes to the previous question, how many times has this occurred in the past 12 month?
 Hypoglycemia score (recall) 43. Have you ever needed help from someone else to recognize a low blood YES NO sugar? 43.a. If you answered, yes to the previous question, how many times has this occurred in the last 12 months?")
5 5/2014 Page 5 of 17 Clarke Hypoglycemia Survey: 47. Check category that best describes you (check one only) I always have symptoms when my blood sugar is low. I sometimes have symptoms when my blood sugar is low. I no longer have symptoms when my blood sugar is low. 48. Have you lost some of the symptoms that used to occur when your blood sugar was low? Yes No 49. In the past 6 months, how often have you had hypoglycemia episodes (low blood sugar) where you felt confused, disoriented, or lethargic and were unable to treat yourself (required assistance from another person)? Never Once or twice Every other month Once a month More than once a month 50. In the past 12 months, how often have you had hypoglycemia episodes (low blood sugar) where you were unconscious or had a seizure and needed glucagon injection or intravenous glucose? Circle one or more 51. How often, in the last month, have you had readings less than 70 mg/dl (3.9 mmol/l) WITH symptoms? Never 1-3 times 1 time/week 2-3 times/week 4-5 times/week Almost daily 52. How often, in the last month, have you had readings less than 70 mg/dl (3.9 mmol/l) WITHOUT symptoms? Never 1-3 times 1 time/week 2-3 times/week 4-5 times/week Almost daily 53. How low does your blood sugar go before you feel symptoms? Above 70 mg/dl mg/dl mg/dl mg/dl less than 40mg/dL 54. To what extent can you tell by your symptoms that your blood sugar is low? Never Rarely Sometimes Often Always
 where you felt confused, disoriented, or lethargic and were unable to treat yourself (required assistance from")
6 5/2014 Page 6 of 17 Diabetes Management: 55. Are you under the care of an endocrinologist or diabetes specialist? YES NO If yes, how many times have you visited him/her in the past year? If no, who helps you look after your diabetes? 56. What is your last HbA1C result? Date: 57. How many times a day do you test your blood sugars? 58. How do you administer your insulin? Insulin injection Insulin Pump 59. If you use insulin injections, please answer the following questions: 67.a. How many injections do you administer per day? 67.b. What is the average total insulin that you take per day? 60. If you use an insulin pump, please answer the following questions: a. What is the average total BASAL INSULIN that you require per day? b. What is the average total BOLUS insulin that you use per day? 61. Please Circle all the insulin preparations that you are currently using? Rapid acting: Short acting Humalog/Lispro Regular NPH Intermediate acting: Novolog/Aspart Humulin R Humulin N Apidra/Glulisine Long acting: Lantus/ Glargine Levemir/ Detemir Mixed insulin: 50/50 70/30 Other: (write in if not listed) Novolin R Novolin N 75/25 Non-Insulin Exubera/ inhaled insulin Symlin/ Pramlintide

7 5/2014 Page 7 of 17 In the tables below, list any significant illnesses other than diabetes and/or major surgeries you have had. (Attach additional page, if necessary). 62. Medical History Please list any relevant medical problems not listed in the previous sections of the form. Date Current Date Treatment (medication/surgery Major Illness Onset Status ** Resolved etc) **Choose from the following options: Active, Stable, Stable/treated, Intermittent, or Resolved 63. Surgical History (Please print clearly) Surgery Date Outcome Complications Additional Medical/ Surgical Background 64. Do you have a history of liver disease? YES NO 65. Have you had any type of cancer including skin cancer? YES NO 66. If yes to the previous question, please explain: 67. Have you ever had a transplant other than k dney? YES NO 68. If yes to the previous question, what organ(s)?
 Surgery Date Outcome Complications Additional Medical/ Surgical Background 64. Do you have a history of liver disease? YES NO 65.")
8 5/2014 Page 8 of 17 In the table below, list any medications you are currently taking (attach additional page, if necessary). 69. Current Medications (please print clearly) Drug Name Trade Name Date Started Dose Units mg, etc. Route Frequency Indication/ Reason Prescribed by 70. List known allergies to medications: 71. Referral Information (please print clearly) How did you find out about this program? Doctor Newspaper Friend DRIwebsite Other patient Magazine Other If you were referred to us by a doctor, complete the information below. 72. Referring Physician (please print clearly) Name (Last, MI, First include MD, PhD etc.) Family practitioner Internist Endocrinologist/Diabetologist Address City State/Province Zip/Postal Code Address (if known) Work Telephone (if outside the US, include country code) Fax Number

9 5/2014 Page 9 of Primary Care Physician Information (please print clearly) If Referring Physician check here Name (Last, MI, First include MD, ARNP, PhD etc.) Family practitioner Internist Address City State/Province Zip/Postal Code Address (if known) Work Telephone (if outside the US, include country code) Fax Number 74. Endocrinologist/Diabetologist Information (please print clearly) If Referring Physician check here Name (Last, MI, First include MD, PhD etc.) Family practitioner Internist Endocrinologist/Diabetologist Address City State/Province Zip/Postal Code Address (if known) Work Telephone (if outside the US, include country code) Fax Number I,, understand that by completing this form and returning it to the, I am granting the permission to use the information contained in this form for research purposes in islet transplantation. Your records and results will be kept confidential to the extent permitted by law and according to current HIPAA guidelines. The Food and Drug Administration (FDA) and the Department of Health and Human Services (DHHS) may request to review and retain copies of these research records. SIGNATURE: DATE: Note: If available, please include results from your last 24-hour urine collection and eye exam done within the last 6 months.
 Family practitioner Internist Endocrinologist/Diabetologist Address City State/Province Zip/Postal Code E-Mail Address (if known) Work Telephone (if outside the US, include country code) Fax Number")
10 5/2014 Page 10 of 17 During the next 28 days of monitoring, complete one section of the diary below for each hypoglycemic event that meets the following criteria: a. Any fingerstick glucose reading equal to or less than 54mg/dl (3.0mmol/L) b. Any symptoms of hypoglycemia even without a fingerstick reading Answer all questions in the box and do not leave any blanks. Write N/A if not applicable. If you do not have any episodes of hypoglycemia during the 28 days check this box. Date: Time: Blood sugar Value: OR Low 1. Symptoms felt or what did you notice? (Please circle all the symptoms you had) Sweating Problems with Vision Seizure OR None Shaking Change in behaviour Other Heart palpitations Confusion 2. The reaction was recognized by (Please circle one): Yourself Routine test on your meter Someone else 3. Treatment for the reaction needed (Please circle all that apply): Juice/Food Help from someone else Injection of glucagon Hospital/Ambulance Date: Time: Blood sugar Value: OR Low 1. Symptoms felt or what did you notice? (Please circle all the symptoms you had) Sweating Problems with Vision Seizure OR None Shaking Change in behaviour Other Heart palpitations Confusion 2. The reaction was recognized by (Please circle one): Yourself Routine test on your meter Someone else 3. Treatment for the reaction needed (Please circle all that apply): Juice/Food Help from someone else Injection of glucagon Hospital/Ambulance Date: Time: Blood sugar Value: OR Low 1. Symptoms felt or what did you notice? (Please circle all the symptoms you had) Sweating Problems with Vision Seizure OR None Shaking Change in behaviour Other Heart palpitations Confusion 2. The reaction was recognized by (Please circle one): Yourself Routine test on your meter Someone else 3. Treatment for the reaction needed (Please circle all that apply):

11 5/2014 Page 11 of 17 During the next 28 days of monitoring, complete one section of the diary below for each hypoglycemic event that meets the following criteria: c. Any fingerstick glucose reading equal to or less than 54mg/dl (3.0mmol/L) d. Any symptoms of hypoglycemia even without a fingerstick reading Answer all questions in the box and do not leave any blanks. Write N/A if not applicable. If you do not have any episodes of hypoglycemia during the 28 days check this box. Date: Time: Blood sugar Value: OR Low 1. Symptoms felt or what did you notice? (Please circle all the symptoms you had) Sweating Problems with Vision Seizure OR None Shaking Change in behaviour Other Heart palpitations Confusion 2. The reaction was recognized by (Please circle one): Yourself Routine test on your meter Someone else 3. Treatment for the reaction needed (Please circle all that apply): Juice/Food Help from someone else Injection of glucagon Hospital/Ambulance Date: Time: Blood sugar Value: OR Low 1. Symptoms felt or what did you notice? (Please circle all the symptoms you had) Sweating Problems with Vision Seizure OR None Shaking Change in behaviour Other Heart palpitations Confusion 2. The reaction was recognized by (Please circle one): Yourself Routine test on your meter Someone else 3. Treatment for the reaction needed (Please circle all that apply): Juice/Food Help from someone else Injection of glucagon Hospital/Ambulance Date: Time: Blood sugar Value: OR Low 1. Symptoms felt or what did you notice? (Please circle all the symptoms you had) Sweating Problems with Vision Seizure OR None Shaking Change in behaviour Other Heart palpitations Confusion 2. The reaction was recognized by (Please circle one): Yourself Routine test on your meter Someone else 3. Treatment for the reaction needed (Please circle all that apply): Juice/Food Help from someone else Injection of glucagon Hospital/Ambulance

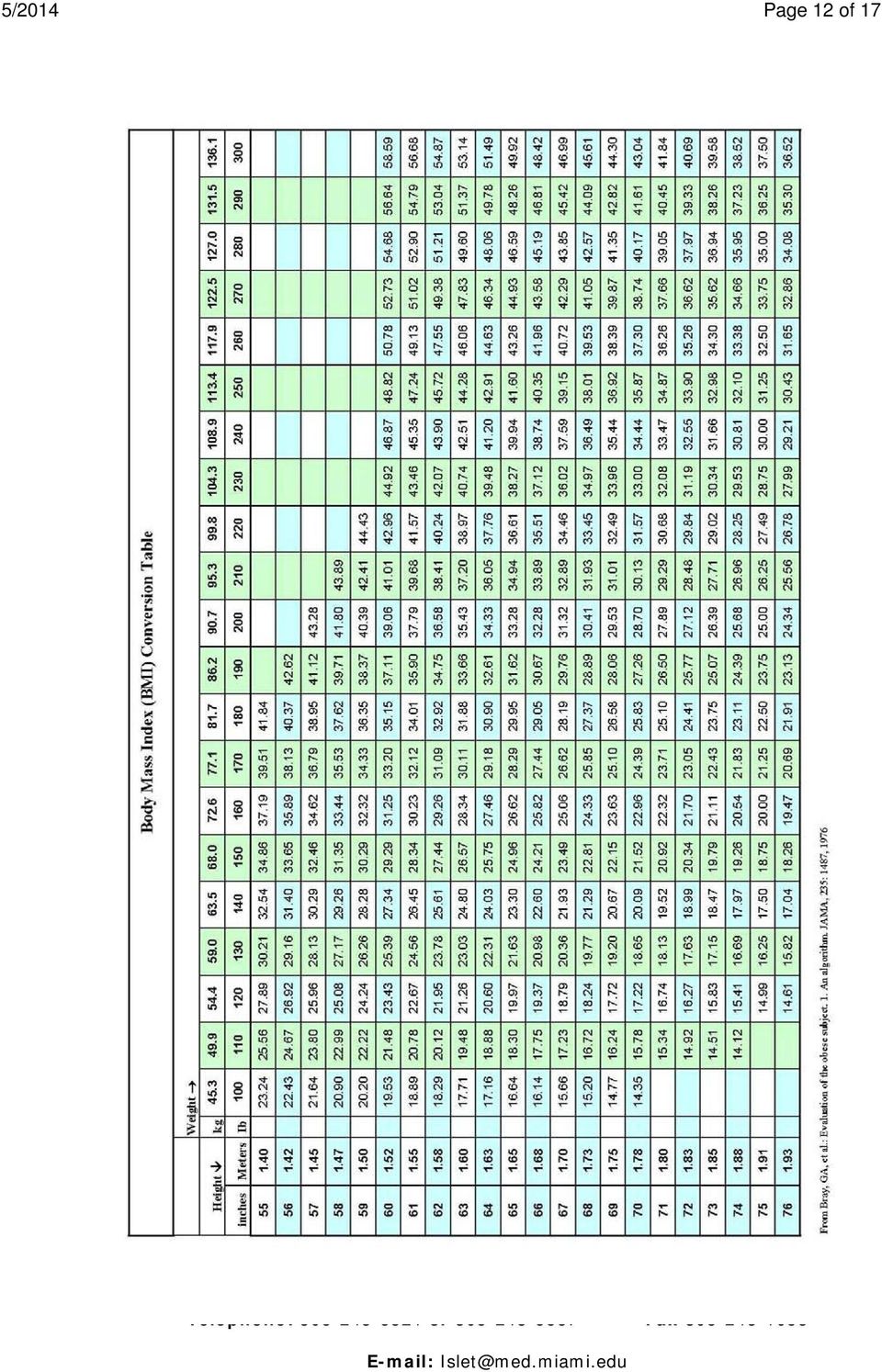
12 5/2014 Page 12 of 17
13 5/2014 Page 13 of 17

14 5/2014 Page 14 of 17

15 5/2014 Page 15 of 17 PROOF OF MEDICAL INSURANCE(S) Please be aware, that in order for you to be enrolled in the Clinical Islet Transplant Program, we must have proof of your medical insurance coverage for the past six months on file. Please complete the form below with your medical insurance information and attach a photocopy (back and front) of your current active insurance card (primary and secondary). Return this form and the photocopy of your card(s) with the Islet Transplantation Patient Evaluation Form to the address listed below: Clinical Islet Transplant program PO Box (R134) Miami, Fl Primary Insurance Name of Primary Insurance: Policy Number: Policy Holder Member(s) covered: Insurance phone number: Other/Secondary Insurance Name of Secondary Insurance: Policy Number: Policy Holder: Member(s) covered: Insurance phone number:
 with the Islet Transplantation Patient Evaluation Form to the address listed below: Clinical Islet Transplant program PO Box 016960 (R134) Miami, Fl")
16 5/2014 Page 16 of 17 PROOF OF MEDICAL CARE BY YOUR PRIMARY PHYSICIAN Of GREATER THAN 6 MONTHS Date: / / Name of Patient: Name of Primary Care Physician: Address: Tel: This letter is to confirm that I have been providing care to this patient for more than 6 months and continues to be under my medical care. I support this patient s application for islet transplant clinical trials. Sincerely, Signature of Primary Care Physician _/ / Date signed

17 5/2014 Page 17 of 17 PROOF OF MEDICAL CARE BY YOUR DIABETES CARE SPECIALIST (ENDOCRINOLOGIST OR DIABETOLOGIST) GREATER THAN 6 MONTHS Date: / / Name of Patient: Name of Diabetes Care Specialist: Address: Tel: This letter is to confirm that I have been providing care to this patient for more than 6 months. This patient has the following diabetes related problems: hypoglycemia unawareness severe hypoglycemia labile diabetes diabetes complications retinopathy nephropathy neuropathy gastroparesis cardiovascular disease If yes, please specify none of the above I support this patient s application for islet transplant clinical trials Sincerely, Signature of Diabetes Care Specialist _/ / Date signed

Borgess Diabetes Center PATIENT REGISTRATION/DEMOGRAPHICS
 Borgess Diabetes Center PATIENT REGISTRATION/DEMOGRAPHICS Please complete the following form by filling in the blanks or by circling the answer provided. Last Name: First Name M.I. Address: City, State,
Borgess Diabetes Center PATIENT REGISTRATION/DEMOGRAPHICS Please complete the following form by filling in the blanks or by circling the answer provided. Last Name: First Name M.I. Address: City, State,
Diabetes Fundamentals
 Diabetes Fundamentals Prevalence of Diabetes in the U.S. Undiagnosed 10.7% of all people 20+ 23.1% of all people 60+ (12.2 million) Slide provided by Roche Diagnostics Sources: ADA, WHO statistics Prevalence
Diabetes Fundamentals Prevalence of Diabetes in the U.S. Undiagnosed 10.7% of all people 20+ 23.1% of all people 60+ (12.2 million) Slide provided by Roche Diagnostics Sources: ADA, WHO statistics Prevalence
ISLET CELL TRANSPLANT PROGRAM INTAKE QUESTIONNAIRE DEMOGRAPHIC INFORMATION INSURANCE INFORMATION PHYSICIAN INFORMATION
 ISLET CELL TRANSPLANT PROGRAM INTAKE QUESTIONNAIRE Last Name First Name Middle Initial Date of Birth Social Security Number DEMOGRAPHIC INFORMATION Address City State Zip E-mail address Home Phone Work
ISLET CELL TRANSPLANT PROGRAM INTAKE QUESTIONNAIRE Last Name First Name Middle Initial Date of Birth Social Security Number DEMOGRAPHIC INFORMATION Address City State Zip E-mail address Home Phone Work
Insulin is a hormone produced by the pancreas to control blood sugar. Diabetes can be caused by too little insulin, resistance to insulin, or both.
 Diabetes Definition Diabetes is a chronic (lifelong) disease marked by high levels of sugar in the blood. Causes Insulin is a hormone produced by the pancreas to control blood sugar. Diabetes can be caused
Diabetes Definition Diabetes is a chronic (lifelong) disease marked by high levels of sugar in the blood. Causes Insulin is a hormone produced by the pancreas to control blood sugar. Diabetes can be caused
PATIENT INFORMATION - Please complete and/or verify all information and make changes as necessary.
 PATIENT INFORMATION - Please complete and/or verify all information and make changes as necessary. Today s : Are you here for an injury that is work-related? YES NO N/A Patient Name (First-Middle-Last)
PATIENT INFORMATION - Please complete and/or verify all information and make changes as necessary. Today s : Are you here for an injury that is work-related? YES NO N/A Patient Name (First-Middle-Last)
Statistics of Type 2 Diabetes
 Statistics of Type 2 Diabetes Of the 17 million Americans with diabetes, 90 percent to 95 percent have type 2 diabetes. Of these, half are unaware they have the disease. People with type 2 diabetes often
Statistics of Type 2 Diabetes Of the 17 million Americans with diabetes, 90 percent to 95 percent have type 2 diabetes. Of these, half are unaware they have the disease. People with type 2 diabetes often
PATIENT INFORMATION PATIENT ETHNICITY / RACE SPOUSE INFORMATION EMERGENCY CONTACT
 Conway Orthopaedic & Sports Medicine Clinic, PA 550 Club Lane Conway AR, 72034 501.329.1510 Account #: : Patient's Name: Patient's Street Address: Apt #: of Birth: Patient's Mailing Address/PO Box: Sex:
Conway Orthopaedic & Sports Medicine Clinic, PA 550 Club Lane Conway AR, 72034 501.329.1510 Account #: : Patient's Name: Patient's Street Address: Apt #: of Birth: Patient's Mailing Address/PO Box: Sex:
Diabetes Self Management Training Insulin Pump Follow Up
 701 East Marshall Street, West Chester, PA 19380 www.chestercountyhospital.org 610.431.5000 Diabetes Self Management Training Insulin Pump Follow Up Patient Name: Visit Date: Time: To prepare for your
701 East Marshall Street, West Chester, PA 19380 www.chestercountyhospital.org 610.431.5000 Diabetes Self Management Training Insulin Pump Follow Up Patient Name: Visit Date: Time: To prepare for your
Personal Injury Questionnaire
 Personal Injury Questionnaire Patient Information Date Date of Birth Health Insurance Do you have a Flex Spending (FSA) or Health Savings (HSA) Account? Y N Patient Name First M Last What do you prefer
Personal Injury Questionnaire Patient Information Date Date of Birth Health Insurance Do you have a Flex Spending (FSA) or Health Savings (HSA) Account? Y N Patient Name First M Last What do you prefer
Electronic Health Records Intake Form
 Dr. Sam Yoder, D.C. 101 Winston Way Ste B Campbellsville, KY 42718 Electronic Health Records Intake Form In compliance with requirements for the government EHR incentive program First Name: Address: Last
Dr. Sam Yoder, D.C. 101 Winston Way Ste B Campbellsville, KY 42718 Electronic Health Records Intake Form In compliance with requirements for the government EHR incentive program First Name: Address: Last
Causes, incidence, and risk factors
 Causes, incidence, and risk factors Insulin is a hormone produced by the pancreas to control blood sugar. Diabetes can be caused by too little insulin, resistance to insulin, or both. To understand diabetes,
Causes, incidence, and risk factors Insulin is a hormone produced by the pancreas to control blood sugar. Diabetes can be caused by too little insulin, resistance to insulin, or both. To understand diabetes,
Diabetes Self-Management Questionnaire
 Diabetes Self-Management Questionnaire Name: Date: Date of Birth: / / Gender: F M Address: Street City State Zip Phone: Home ( ) Work: ( ) Mobile: ( ) Ethnic Background: White/Caucasian Black/A-A Hispanic
Diabetes Self-Management Questionnaire Name: Date: Date of Birth: / / Gender: F M Address: Street City State Zip Phone: Home ( ) Work: ( ) Mobile: ( ) Ethnic Background: White/Caucasian Black/A-A Hispanic
Diabetes Mellitus Type 2
 Diabetes Mellitus Type 2 What is it? Diabetes is a common health problem in the U.S. and the world. In diabetes, the body does not use the food it digests well. It is hard for the body to use carbohydrates
Diabetes Mellitus Type 2 What is it? Diabetes is a common health problem in the U.S. and the world. In diabetes, the body does not use the food it digests well. It is hard for the body to use carbohydrates
PATIENT REGISTRATION
 Orthopedic & Sports Therapy Center PATIENT REGISTRATION NAME DATE OF BIRTH SSN# FIRST MI LAST PHONE INFO: HOME BEST WAY TO CONFIRM APPOINTMENTS WORK CALL TEXT EMAIL MOBILE (TEXT) MOBILE CARRIER EMAIL ADDRESS
Orthopedic & Sports Therapy Center PATIENT REGISTRATION NAME DATE OF BIRTH SSN# FIRST MI LAST PHONE INFO: HOME BEST WAY TO CONFIRM APPOINTMENTS WORK CALL TEXT EMAIL MOBILE (TEXT) MOBILE CARRIER EMAIL ADDRESS
Anchor Bay School District Diabetic Medical Care Plan. Student Name Date Grade Teacher
 Rev: 4/2009 Anchor Bay School District Diabetic Medical Care Plan Place Child s Picture Here Student Name Date Grade Teacher Emergency Contact information (Please list in order to be called) #1 Parent
Rev: 4/2009 Anchor Bay School District Diabetic Medical Care Plan Place Child s Picture Here Student Name Date Grade Teacher Emergency Contact information (Please list in order to be called) #1 Parent
(928) 854-4307 MEDICAL HISTORY. Weight: _ Shoe size: _
 854-4307 MEDICAL HISTORY. Weight: _ Shoe size: _") 2302 N. Stockton Hill Rd Ste. G 1731 Mesquite Ave Ste 4 1200 Mohave Rd MEDICAL HISTORY Weight: Shoe size: ~~~~~~~~~~~~~~~~~~~~~~~~~~PLEASECIRCLE: RIGHT or LE~ Is your problem due to an accident? YES or
2302 N. Stockton Hill Rd Ste. G 1731 Mesquite Ave Ste 4 1200 Mohave Rd MEDICAL HISTORY Weight: Shoe size: ~~~~~~~~~~~~~~~~~~~~~~~~~~PLEASECIRCLE: RIGHT or LE~ Is your problem due to an accident? YES or
New England Pain Management Consultants At New England Baptist Hospital
 New England Pain Management Consultants At New England Baptist Hospital Pain Management Center Health Assessment Dear New Pain Management Patient, Welcome to the New England Pain Management Consultants
New England Pain Management Consultants At New England Baptist Hospital Pain Management Center Health Assessment Dear New Pain Management Patient, Welcome to the New England Pain Management Consultants
Diabetes Brief. Pre diabetes occurs when glucose levels are elevated in the blood, but are not as high as someone who has diabetes.
 Diabetes Brief What is Diabetes? Diabetes mellitus is a disease of abnormal carbohydrate metabolism in which the level of blood glucose, or blood sugar, is above normal. The disease occurs when the body
Diabetes Brief What is Diabetes? Diabetes mellitus is a disease of abnormal carbohydrate metabolism in which the level of blood glucose, or blood sugar, is above normal. The disease occurs when the body
CIGI Direct Insurance Services, Inc. QUICK QUOTE CORONARY ANGIOPLASTY/CORONARY BYPASS
 QUICK QUOTE CORONARY ANGIOPLASTY/CORONARY BYPASS Amount of Insurance $ Type of Insurance 1. Has patient had: Date of last symptom, list date (or dates if more than one ) Angina pectoris (heart pain)? r
QUICK QUOTE CORONARY ANGIOPLASTY/CORONARY BYPASS Amount of Insurance $ Type of Insurance 1. Has patient had: Date of last symptom, list date (or dates if more than one ) Angina pectoris (heart pain)? r
DIABETIC EDUCATION MODULE ONE GENERAL OVERVIEW OF TREATMENT AND SAFETY
 DIABETIC EDUCATION MODULE ONE GENERAL OVERVIEW OF TREATMENT AND SAFETY First Edition September 17, 1997 Kevin King R.N., B.S., C.C.R.N. Gregg Kunder R.N., B.S.N., C.C.T.C. 77-120 CHS UCLA Medical Center
DIABETIC EDUCATION MODULE ONE GENERAL OVERVIEW OF TREATMENT AND SAFETY First Edition September 17, 1997 Kevin King R.N., B.S., C.C.R.N. Gregg Kunder R.N., B.S.N., C.C.T.C. 77-120 CHS UCLA Medical Center
DCCT and EDIC: The Diabetes Control and Complications Trial and Follow-up Study
 DCCT and EDIC: The Diabetes Control and Complications Trial and Follow-up Study National Diabetes Information Clearinghouse U.S. Department of Health and Human Services NATIONAL INSTITUTES OF HEALTH What
DCCT and EDIC: The Diabetes Control and Complications Trial and Follow-up Study National Diabetes Information Clearinghouse U.S. Department of Health and Human Services NATIONAL INSTITUTES OF HEALTH What
A new insulin order form should be completed for subsequent changes to type of insulin and/or frequency of administration
 of nurse A new insulin order form should be completed for subsequent changes to type of insulin and/or frequency of administration 1. Check times for point of care meter blood glucose testing. Pre-Breakfast
of nurse A new insulin order form should be completed for subsequent changes to type of insulin and/or frequency of administration 1. Check times for point of care meter blood glucose testing. Pre-Breakfast
ARIZONA INTRASTATE DIABETES WAIVER PROGRAM
 40-1505 R10/14 azdot.gov Dear Applicant: Mail Drop 818Z Medical Review Program PO Box 2100 Phoenix AZ 85001-2100 ARIZONA INTRASTATE DIABETES WAIVER PROGRAM Thank you for your interest in the Arizona Intrastate
40-1505 R10/14 azdot.gov Dear Applicant: Mail Drop 818Z Medical Review Program PO Box 2100 Phoenix AZ 85001-2100 ARIZONA INTRASTATE DIABETES WAIVER PROGRAM Thank you for your interest in the Arizona Intrastate
Orthopaedic Institute of Ohio Demographic Information Date:
 Orthopaedic Institute of Ohio Demographic Information Date: Patient Name Home Phone Cell Phone Employer Phone Mailing Address (include PO Box and Apt. #) Family Doctor Name and Phone Number City, State,
Orthopaedic Institute of Ohio Demographic Information Date: Patient Name Home Phone Cell Phone Employer Phone Mailing Address (include PO Box and Apt. #) Family Doctor Name and Phone Number City, State,
Your appointment is scheduled for at with Dr. Your arrival time is.
 Dear : We appreciate your selection of our office for your complete eye care. Your appointment is scheduled for at with Dr. Your arrival time is. First visits usually take approximately one and a half
Dear : We appreciate your selection of our office for your complete eye care. Your appointment is scheduled for at with Dr. Your arrival time is. First visits usually take approximately one and a half
PATIENT INFORMATION INTAKE F O R M BESSMER CHIROPRACTIC P. C.
 PATIENT INFORMATION INTAKE F O R M BESSMER CHIROPRACTIC P. C. Date today: _ PERSONAL INFORMATION Full Name: SS#: Address: City: State: Home Phone: Cell Phone: W o r k Phone: Email: Birthdate: Age: Sex:
PATIENT INFORMATION INTAKE F O R M BESSMER CHIROPRACTIC P. C. Date today: _ PERSONAL INFORMATION Full Name: SS#: Address: City: State: Home Phone: Cell Phone: W o r k Phone: Email: Birthdate: Age: Sex:
Personal Injury Intake Form
 Personal Injury Intake Form Patient Information: Name Home Phone Address Work Phone Cell Phone Date of Birth Social Security # Sex Male Female Height Weight lbs Occupation Marital Status Employer No of
Personal Injury Intake Form Patient Information: Name Home Phone Address Work Phone Cell Phone Date of Birth Social Security # Sex Male Female Height Weight lbs Occupation Marital Status Employer No of
P.S. Please remember to bring your completed forms to your office visit!
 Dear Patient: Please print the following forms and complete them as accurately as possible and bring them with you to your office visit. If you have any questions about the forms you can call my office
Dear Patient: Please print the following forms and complete them as accurately as possible and bring them with you to your office visit. If you have any questions about the forms you can call my office
Welcome to Diabetes Education! Why Should I Take Control of My Diabetes?
 Welcome to Diabetes Education! Why Should I Take Control of My Diabetes? NEEDS and BENEFITS of SELF-MANAGEMENT You make choices about your life and health Controlling diabetes needs every day decisions
Welcome to Diabetes Education! Why Should I Take Control of My Diabetes? NEEDS and BENEFITS of SELF-MANAGEMENT You make choices about your life and health Controlling diabetes needs every day decisions
Type 2 diabetes Definition
 Type 2 diabetes Definition Type 2 diabetes is a lifelong (chronic) disease in which there are high levels of sugar (glucose) in the blood. Type 2 diabetes is the most common form of diabetes. Causes Diabetes
Type 2 diabetes Definition Type 2 diabetes is a lifelong (chronic) disease in which there are high levels of sugar (glucose) in the blood. Type 2 diabetes is the most common form of diabetes. Causes Diabetes
Male New Patient Package
 Male New Patient Package The contents of this package are your first step to restore your vitality. Please take time to read this carefully and answer all the questions as completely as possible. Thank
Male New Patient Package The contents of this package are your first step to restore your vitality. Please take time to read this carefully and answer all the questions as completely as possible. Thank
Appendix 1. CAHPS Health Plan Survey 5.0H Adult Questionnaire (Commercial)
") Appendix 1 CAHPS Health Plan Survey 5.0H Adult Questionnaire (Commercial) 1-2 Appendix 1 CAHPS 5.0H Adult Questionnaire (Commercial) 1-3 CAHPS 5.0H Adult Questionnaire (Commercial) SURVEY INSTRUCTIONS
Appendix 1 CAHPS Health Plan Survey 5.0H Adult Questionnaire (Commercial) 1-2 Appendix 1 CAHPS 5.0H Adult Questionnaire (Commercial) 1-3 CAHPS 5.0H Adult Questionnaire (Commercial) SURVEY INSTRUCTIONS
1MFBTF GJMM PVU GPSNT BOE GBY 'PSNT XJMM CF TJHOFE BU ZPVS BQQPJOUNFOU
 CELL PHONE: PATIENT HISTORY FORM - CONFIDENTIAL DATE: PATIENT: (LAST NAME) (FIRST NAME) (Ml) (NICKNAME) DOB: Primary Physician/ Family Doctor: Phone: Past Medical History (Click all that apply) High blood
CELL PHONE: PATIENT HISTORY FORM - CONFIDENTIAL DATE: PATIENT: (LAST NAME) (FIRST NAME) (Ml) (NICKNAME) DOB: Primary Physician/ Family Doctor: Phone: Past Medical History (Click all that apply) High blood
Physician address. Physician phone
 PATIENT QUESTIONNAIRE Name (first, middle initial, last) Address City, State, Zip Social security number Michigan SportsMedicine and Orthopedic Center www.michigansportsmedicine.com Your family physician
PATIENT QUESTIONNAIRE Name (first, middle initial, last) Address City, State, Zip Social security number Michigan SportsMedicine and Orthopedic Center www.michigansportsmedicine.com Your family physician
Diabetes and Heart Disease
 Diabetes and Heart Disease Diabetes and Heart Disease According to the American Heart Association, diabetes is one of the six major risk factors of cardiovascular disease. Affecting more than 7% of the
Diabetes and Heart Disease Diabetes and Heart Disease According to the American Heart Association, diabetes is one of the six major risk factors of cardiovascular disease. Affecting more than 7% of the
TALLAHASSEE EYE CENTER
 TALLAHASSEE EYE CENTER PATIENT INFORMATION Date: Name: Gender: M / F First MI Last Date of Birth: / / Address: City: State: ZIP: Phone Numbers: Home: Cellular: Work: E-Mail: SS#: - - What is the best way
TALLAHASSEE EYE CENTER PATIENT INFORMATION Date: Name: Gender: M / F First MI Last Date of Birth: / / Address: City: State: ZIP: Phone Numbers: Home: Cellular: Work: E-Mail: SS#: - - What is the best way
OFFICE OF CATHOLIC SCHOOLS DIOCESE OF ARLINGTON DIABETES MEDICAL MANAGEMENT PLAN Page 1 of 5 TO BE COMPLETED BY PARENT OR GUARDIAN
 PART I OFFICE OF CATHOLIC SCHOOLS DIOCESE OF ARLINGTON DIABETES MEDICAL MANAGEMENT PLAN Page 1 of 5 TO BE COMPLETED BY PARENT OR GUARDIAN Student School Date of Birth Date of Diagnosis Grade/ Teacher Physical
PART I OFFICE OF CATHOLIC SCHOOLS DIOCESE OF ARLINGTON DIABETES MEDICAL MANAGEMENT PLAN Page 1 of 5 TO BE COMPLETED BY PARENT OR GUARDIAN Student School Date of Birth Date of Diagnosis Grade/ Teacher Physical
THE EYE INSTITUTE. Dear Patient:
 THE EYE INSTITUTE Eye Associates of Wayne P.A. 968 Hamburg Turnpike Wayne, NJ 07470 p. 973-696-0300 f. 973-696-0464 Eye Institute North, LLC 5677 Berkshire Valley Rd. Oak Ridge, NJ 07438 p. 973-208-0600
THE EYE INSTITUTE Eye Associates of Wayne P.A. 968 Hamburg Turnpike Wayne, NJ 07470 p. 973-696-0300 f. 973-696-0464 Eye Institute North, LLC 5677 Berkshire Valley Rd. Oak Ridge, NJ 07438 p. 973-208-0600
NEUROSURGERY SERVICES AT APD LOCATED AT UPPER VALLEY MEDICAL GROUP 106 Hanover Street, Lebanon, NH 03766 Phone: 603.448.0447 Fax: 603.448.
 DATE NEUROSURGERY SERVICES AT APD LOCATED AT UPPER VALLEY MEDICAL GROUP 106 Hanover Street, Lebanon, NH 03766 Phone: 603.448.0447 Fax: 603.448.0019 Joseph M. Phillips, M.D., Ph.D. Board Certified in Pain
DATE NEUROSURGERY SERVICES AT APD LOCATED AT UPPER VALLEY MEDICAL GROUP 106 Hanover Street, Lebanon, NH 03766 Phone: 603.448.0447 Fax: 603.448.0019 Joseph M. Phillips, M.D., Ph.D. Board Certified in Pain
ALBANY PLASTIC SURGEONS, PLLC 4 Executive Park Drive Albany NY 12203 (518) 438-1434 PATIENT INFORMATION FORM
 438-1434 PATIENT INFORMATION FORM") ALBANY PLASTIC SURGEONS, PLLC 4 Executive Park Drive Albany NY 12203 (518) 438-1434 PATIENT INFORMATION FORM Today s Date: PERSONAL INFORMATION First Name: Last Name: MI: Address: City: State/Province:
ALBANY PLASTIC SURGEONS, PLLC 4 Executive Park Drive Albany NY 12203 (518) 438-1434 PATIENT INFORMATION FORM Today s Date: PERSONAL INFORMATION First Name: Last Name: MI: Address: City: State/Province:
MVA/ PI Registration Form. Is this accident work related? YES or No If yes, stop here and notify front desk for different forms.
 MVA/ PI Registration Form Is this accident work related? YES or No If yes, stop here and notify front desk for different forms. Date: Patient # Patient Name: DOB; Gender: M or F SSN Address: City/State:
MVA/ PI Registration Form Is this accident work related? YES or No If yes, stop here and notify front desk for different forms. Date: Patient # Patient Name: DOB; Gender: M or F SSN Address: City/State:
Potomac Valley Chiropractic Personal Injury
 Potomac Valley Chiropractic Personal Injury Spiro Theodore, D.C. 12105 Darnestown Road, L8 Gaithersburg MD 20878 Please Complete all applicable fields Date: -------------------------------------------------------DEMOGRAPHICS--------------------------------------------------------------
Potomac Valley Chiropractic Personal Injury Spiro Theodore, D.C. 12105 Darnestown Road, L8 Gaithersburg MD 20878 Please Complete all applicable fields Date: -------------------------------------------------------DEMOGRAPHICS--------------------------------------------------------------
Welcome to North Texas Orthopaedic & Spine 955 Garden Park Dr. Ste. 200 Allen Texas 75013. Today s Date: How did you hear of our practice?
 Welcome to North Texas Orthopaedic & Spine 955 Garden Park Dr. Ste. 200 Allen Texas 75013 Name: First Middle Last Today s Date: How did you hear of our practice? Home Address: City: State: Zip: Home Phone:
Welcome to North Texas Orthopaedic & Spine 955 Garden Park Dr. Ste. 200 Allen Texas 75013 Name: First Middle Last Today s Date: How did you hear of our practice? Home Address: City: State: Zip: Home Phone:
Type 2 Diabetes Type 2 Diabetes
 Pennington Nutrition Series Healthier lives through education in nutrition and preventive medicine Pub No. 33 Type 2 is the most common form of diabetes. In this form, the body does not produce enough
Pennington Nutrition Series Healthier lives through education in nutrition and preventive medicine Pub No. 33 Type 2 is the most common form of diabetes. In this form, the body does not produce enough
NOTICE ABOUT REFRACTION
 NOTICE ABOUT REFRACTION We have you scheduled for a complete eye exam today. A complete eye exam involves two components: 1. Refraction this portion of the examination determines the best lens correction
NOTICE ABOUT REFRACTION We have you scheduled for a complete eye exam today. A complete eye exam involves two components: 1. Refraction this portion of the examination determines the best lens correction
Registration Forms (Please leave NO blanks, if something does not apply write N/A and if unknown write unknown)
") Registration Forms (Please leave NO blanks, if something does not apply write N/A and if unknown write unknown) Patient Name: Date of Birth Mailing Address: City: State Zip: Apt/Ste/Unit/Bldg Primary Number:
Registration Forms (Please leave NO blanks, if something does not apply write N/A and if unknown write unknown) Patient Name: Date of Birth Mailing Address: City: State Zip: Apt/Ste/Unit/Bldg Primary Number:
VEIN CLINIC OF NORTH CAROLINA 3318 HEALY DR. WINSTON SALEM, NC 27103 PH. 336-768-3530 FAX- 768-1329. Scott W. Baker, MD. Patient Instructions
 18 HEALY DR. WINSTON SALEM, NC 710 PH. 6-768-50 FAX- 768-19 Scott W. Baker, MD Patient Instructions 1. Bring a list of all regular medications and dosages.. Bring your insurance card and all necessary
18 HEALY DR. WINSTON SALEM, NC 710 PH. 6-768-50 FAX- 768-19 Scott W. Baker, MD Patient Instructions 1. Bring a list of all regular medications and dosages.. Bring your insurance card and all necessary
460 Main St, East. Unit M3 Hamilton, ON L8N 1K4 T: 905 524 3709 F: 905 524 4866 info@physiotherapyclinic.ca
 Page 1 of 6 Date Patient Information (Please complete all fields below) Last Name First Name Intl. Street Address Home Tel. City/Town Province Postal Code Work Tel. Date of Birth (mm/dd/yyyy) Gender M
Page 1 of 6 Date Patient Information (Please complete all fields below) Last Name First Name Intl. Street Address Home Tel. City/Town Province Postal Code Work Tel. Date of Birth (mm/dd/yyyy) Gender M
Understanding Diabetes
 Patient Education Understanding Diabetes This handout describes diabetes, the complications related to the disease, and how you can prevent these complications. Blood Sugar Control Diabetes is a disease
Patient Education Understanding Diabetes This handout describes diabetes, the complications related to the disease, and how you can prevent these complications. Blood Sugar Control Diabetes is a disease
Types of insulin and How to Use Them
 Diabetes and Insulin Pumps Amy S. Pullen Pharm.D ISHP Spring Meeting April 2012 Objectives Describe the different types of insulin used in diabetes Identify the types of insulin that are compatible with
Diabetes and Insulin Pumps Amy S. Pullen Pharm.D ISHP Spring Meeting April 2012 Objectives Describe the different types of insulin used in diabetes Identify the types of insulin that are compatible with
Managing Diabetes in the Athletic Population
 Managing Diabetes in the Athletic Population Michael Prybicien, LA, ATC, CSCS, CES, PES Athletic Trainer, Passaic High School Overlook Medical Center & Adjunct Faculty, William Paterson University Dedicated
Managing Diabetes in the Athletic Population Michael Prybicien, LA, ATC, CSCS, CES, PES Athletic Trainer, Passaic High School Overlook Medical Center & Adjunct Faculty, William Paterson University Dedicated
HUMULIN R REGULAR INSULIN HUMAN INJECTION, USP (rdna ORIGIN) 100 UNITS PER ML (U-100)
 100 UNITS PER ML (U-100)") 1 PATIENT INFORMATION HUMULIN R REGULAR INSULIN HUMAN INJECTION, USP (rdna ORIGIN) 100 UNITS PER ML (U-100) WARNINGS Do not share your syringes with other people, even if the needle has been changed. You
1 PATIENT INFORMATION HUMULIN R REGULAR INSULIN HUMAN INJECTION, USP (rdna ORIGIN) 100 UNITS PER ML (U-100) WARNINGS Do not share your syringes with other people, even if the needle has been changed. You
Patient Registration Form
 Patient Registration Form MRN #: Patient Name: Provider: Sort ID: DOB: Date: Address Home Phone Cell Phone Work Social Security Number Date of Birth Male Female E-mail Address Is your visit today due to
Patient Registration Form MRN #: Patient Name: Provider: Sort ID: DOB: Date: Address Home Phone Cell Phone Work Social Security Number Date of Birth Male Female E-mail Address Is your visit today due to
This information explains the advice about type 2 diabetes in adults that is set out in NICE guideline NG28.
 Information for the public Published: 2 December 2015 nice.org.uk About this information NICE guidelines provide advice on the care and support that should be offered to people who use health and care
Information for the public Published: 2 December 2015 nice.org.uk About this information NICE guidelines provide advice on the care and support that should be offered to people who use health and care
Patient Information. Date: Date of Birth: / / Name: Social Security: _- - Address: Street City State Zip
 Personal Insurance Intake Form Patient Information Date of Birth: / / Social Security: _- - Address: Street City State Zip Email Address: Home Phone: Sex: M or F Work Phone:. Cell Phone: Height: Weight:
Personal Insurance Intake Form Patient Information Date of Birth: / / Social Security: _- - Address: Street City State Zip Email Address: Home Phone: Sex: M or F Work Phone:. Cell Phone: Height: Weight:
Referrals It is your responsibility to bring your referral if required. Failure to do so may result in cancellation of your appointment.
 Welcome to Capital Endocrinology! We are happy to have you as a patient in our practice. Please take note of the following policies. Following these policies will help in making your visit as efficient
Welcome to Capital Endocrinology! We are happy to have you as a patient in our practice. Please take note of the following policies. Following these policies will help in making your visit as efficient
Lake Oswego Eye Clinic 530 First ST, Suite A Lake Oswego, OR 97068 Office: (503) 636-9608 Fax: (503) 636-9600
 636-9608 Fax: (503) 636-9600") PAYMENT AGREEMENT: We accept most insurance plans as a courtesy. We encourage you to familiarize yourself with your individual plan. Insurance coverage is an agreement between patient and insurance company
PAYMENT AGREEMENT: We accept most insurance plans as a courtesy. We encourage you to familiarize yourself with your individual plan. Insurance coverage is an agreement between patient and insurance company
TYPE 2 DIABETES IN THE AFRICAN AMERICAN COMMUNITY. Understanding the Complications That May Happen Without Proper Care
 TYPE 2 DIABETES IN THE AFRICAN AMERICAN COMMUNITY Understanding the Complications That May Happen Without Proper Care STAYING HEALTHY THE IMPORTANCE OF PROPER MANAGEMENT OF TYPE 2 DIABETES Diabetes is
TYPE 2 DIABETES IN THE AFRICAN AMERICAN COMMUNITY Understanding the Complications That May Happen Without Proper Care STAYING HEALTHY THE IMPORTANCE OF PROPER MANAGEMENT OF TYPE 2 DIABETES Diabetes is
JAMES PETROS, M.D., INC. PHONE: (408) 528-8833 FAX: (408) 528-8557
 528-8833 FAX: (408) 528-8557") FIGHTING PAIN. TOUCHING LIVES. JAMES PETROS, M.D., INC. PHONE: (408) 528-8833 FAX: (408) 528-8557 Personal Information Emergency Contact Today s Date: Name: Patient: Realtionship: Birth Date: Age: Sex:
FIGHTING PAIN. TOUCHING LIVES. JAMES PETROS, M.D., INC. PHONE: (408) 528-8833 FAX: (408) 528-8557 Personal Information Emergency Contact Today s Date: Name: Patient: Realtionship: Birth Date: Age: Sex:
Markham Stouffville Hospital
 Markham Stouffville Hospital Adult Diabetes Education Frequently Asked Questions What is diabetes? Diabetes is a disease in which blood glucose levels are above normal. Most of the food we eat is turned
Markham Stouffville Hospital Adult Diabetes Education Frequently Asked Questions What is diabetes? Diabetes is a disease in which blood glucose levels are above normal. Most of the food we eat is turned
Diabetes: When To Treat With Insulin and Treatment Goals
 Diabetes: When To Treat With Insulin and Treatment Goals Lanita. S. White, Pharm.D. Director, UAMS 12 th Street Health and Wellness Center Assistant Professor of Pharmacy Practice, UAMS College of Pharmacy
Diabetes: When To Treat With Insulin and Treatment Goals Lanita. S. White, Pharm.D. Director, UAMS 12 th Street Health and Wellness Center Assistant Professor of Pharmacy Practice, UAMS College of Pharmacy
New Patient Information
 New Patient Information LAST FIRST NAME NAME M.I. DATE OF SOC. MARITAL BIRTH SEC. SEX STATUS PRIMARY ADDRESS PHONE CELL CITY STATE ZIP PHONE WORK EMPLOYER PHONE REFERRING/ YOUR PRIMARY PHYSICIAN E-MAIL
New Patient Information LAST FIRST NAME NAME M.I. DATE OF SOC. MARITAL BIRTH SEC. SEX STATUS PRIMARY ADDRESS PHONE CELL CITY STATE ZIP PHONE WORK EMPLOYER PHONE REFERRING/ YOUR PRIMARY PHYSICIAN E-MAIL
Post-Transplant Diabetes: What Every Patient Needs to Know
 Post-Transplant Diabetes: What Every Patient Needs to Know International Transplant Nurses Society What is Diabetes? Diabetes is an illness that effects how your body makes and uses a hormone called insulin.
Post-Transplant Diabetes: What Every Patient Needs to Know International Transplant Nurses Society What is Diabetes? Diabetes is an illness that effects how your body makes and uses a hormone called insulin.
Diabetes, Type 2. RelayClinical Patient Education Sample Topic Diabetes, Type 2. What is type 2 diabetes? How does it occur?
 What is type 2 diabetes? Type 2 diabetes is a disorder that happens when your body does not make enough insulin or is unable to use its own insulin properly. The inability to use insulin is called insulin
What is type 2 diabetes? Type 2 diabetes is a disorder that happens when your body does not make enough insulin or is unable to use its own insulin properly. The inability to use insulin is called insulin
Diabetes. Emergency Checklists. From A Child in Your Care Has Diabetes. A Collection of Information. Copyright 2005 by Elisa Hendel, M.Ed.
 Diabetes Emergency Checklists From A Child in Your Care Has Diabetes. A Collection of Information. Copyright 2005 by Elisa Hendel, M.Ed. Hyperglycemia High Blood Sugar * Hyperglycemia occurs when the blood
Diabetes Emergency Checklists From A Child in Your Care Has Diabetes. A Collection of Information. Copyright 2005 by Elisa Hendel, M.Ed. Hyperglycemia High Blood Sugar * Hyperglycemia occurs when the blood
Blood Glucose Management
 Blood Glucose Management What Influences Blood Sugar Levels? There are three main things that influence your blood sugar: Nutrition Exercise Medication What Influences Blood Sugar Levels? NUTRITION 4 Meal
Blood Glucose Management What Influences Blood Sugar Levels? There are three main things that influence your blood sugar: Nutrition Exercise Medication What Influences Blood Sugar Levels? NUTRITION 4 Meal
Challenges in Glycemic Control in Adult and Geriatric Patients. Denyse Gallagher, APRN-BC, CDE Endocrinology Nurse Practitioner
 Challenges in Glycemic Control in Adult and Geriatric Patients Denyse Gallagher, APRN-BC, CDE Endocrinology Nurse Practitioner Provide an overview of diabetes prevalence; discuss challenges and barriers
Challenges in Glycemic Control in Adult and Geriatric Patients Denyse Gallagher, APRN-BC, CDE Endocrinology Nurse Practitioner Provide an overview of diabetes prevalence; discuss challenges and barriers
D I D Y O U K N O W? D I A B E T E S R E S O U R C E G U I D E. Blindness Heart Disease Strokes Kidney Failure Amputation
 D I D Y O U K N O W? D I A B E T E S R E S O U R C E G U I D E Diabetes is a serious disease that can lead to Blindness Heart Disease Strokes Kidney Failure Amputation Diabetes kills almost 210,000 people
D I D Y O U K N O W? D I A B E T E S R E S O U R C E G U I D E Diabetes is a serious disease that can lead to Blindness Heart Disease Strokes Kidney Failure Amputation Diabetes kills almost 210,000 people
PREMIER PAIN CARE PA Carlos J Garcia MD 2435 W. Oak Street # 103 Denton, TX 76201 Phone 940-323-9404 Fax 940-323-9422 PATIENT REGISTRATION
 PREMIER PAIN CARE PA Carlos J Garcia MD 2435 W. Oak Street # 103 Denton, TX 76201 Phone 940-323-9404 Fax 940-323-9422 PATIENT REGISTRATION Last Name First Name MI Mailing Address City Zip code Home Phone
PREMIER PAIN CARE PA Carlos J Garcia MD 2435 W. Oak Street # 103 Denton, TX 76201 Phone 940-323-9404 Fax 940-323-9422 PATIENT REGISTRATION Last Name First Name MI Mailing Address City Zip code Home Phone
School Year 20 / 20. Diabetes Health Care Plan for Southgate Schools
 School Year 20 / 20 Diabetes Health Care Plan for Southgate Schools Diabetes Medical Management Plan, Initialized Healthcare Plan and Physician Orders Part A: Contact Information must be completed by the
School Year 20 / 20 Diabetes Health Care Plan for Southgate Schools Diabetes Medical Management Plan, Initialized Healthcare Plan and Physician Orders Part A: Contact Information must be completed by the
Advanced Rehab Solutions 609 Morris Avenue Springfield, NJ 07081
 Advanced Rehab Solutions 609 Morris Avenue Springfield, NJ 07081 PLEASE COMPLETE ALL OF THE INFORMATION. REFERRED BY: LAST NAME MIDDLE FIRST STREET ADDRESS CITY STATE ZIP CODE HOME PHONE ( ) - WORK ( )
Advanced Rehab Solutions 609 Morris Avenue Springfield, NJ 07081 PLEASE COMPLETE ALL OF THE INFORMATION. REFERRED BY: LAST NAME MIDDLE FIRST STREET ADDRESS CITY STATE ZIP CODE HOME PHONE ( ) - WORK ( )
Health Information Form for Adults
 A. Identification B. Emergency Contacts Name (Last) (First) (Middle) Maiden Name In Case of Emergency, Notify: Primary Contact Name (Last) (First) (Middle) Primary Alternate Relationship Home Work Home
A. Identification B. Emergency Contacts Name (Last) (First) (Middle) Maiden Name In Case of Emergency, Notify: Primary Contact Name (Last) (First) (Middle) Primary Alternate Relationship Home Work Home
HORIZON PHYSICAL THERAPY 9154 ESTATE THOMAS ST. THOMAS V.I 00802 (340)776-7667 P (340)714-1891 F WELCOME
776-7667 P (340)714-1891 F WELCOME") HORIZON PHYSICAL THERAPY 9154 ESTATE THOMAS ST. THOMAS V.I 00802 (340)776-7667 P (340)714-1891 F WELCOME We are pleased you have chosen us for your physical therapy needs. Our office is committed to providing
HORIZON PHYSICAL THERAPY 9154 ESTATE THOMAS ST. THOMAS V.I 00802 (340)776-7667 P (340)714-1891 F WELCOME We are pleased you have chosen us for your physical therapy needs. Our office is committed to providing
Nutrition. Type 2 Diabetes: A Growing Challenge in the Healthcare Setting NAME OF STUDENT
 1 Nutrition Type 2 Diabetes: A Growing Challenge in the Healthcare Setting NAME OF STUDENT 2 Type 2 Diabetes: A Growing Challenge in the Healthcare Setting Introduction and background of type 2 diabetes:
1 Nutrition Type 2 Diabetes: A Growing Challenge in the Healthcare Setting NAME OF STUDENT 2 Type 2 Diabetes: A Growing Challenge in the Healthcare Setting Introduction and background of type 2 diabetes:
Welcome! Thank you for choosing our practice for your eye care needs! Please fill out our new patient registration paperwork.
 Welcome! Thank you for choosing our practice for your eye care needs! Please fill out our new patient registration paperwork. So we may eliminate any potential waiting time, please fax the completed forms
Welcome! Thank you for choosing our practice for your eye care needs! Please fill out our new patient registration paperwork. So we may eliminate any potential waiting time, please fax the completed forms
Where World-Class Expertise and Genuine Compassion Come Together. AT THE FOREFRONT OF TRANSPLANT CARE Kidney Combined Kidney-Pancreas Pancreas Islets
 Where World-Class Expertise and Genuine Compassion Come Together 0011000110100111100110111100000101010011000101100010111000010010000100010000100001011110101010101111000 000010111000101110011000110100111100110111100000101010011000101100010111000010010000100010000100
Where World-Class Expertise and Genuine Compassion Come Together 0011000110100111100110111100000101010011000101100010111000010010000100010000100001011110101010101111000 000010111000101110011000110100111100110111100000101010011000101100010111000010010000100010000100
Copayment Is Due At Time Of Visit. Self-pay (payment due at time of service)
") REGISTRATION FORM Please present your insurance card and photo ID at time of check-in. Settlement of patient financial responsibility is expected at time of service. Copayment Is Due At Time Of Visit.
REGISTRATION FORM Please present your insurance card and photo ID at time of check-in. Settlement of patient financial responsibility is expected at time of service. Copayment Is Due At Time Of Visit.
PATIENT REGISTRATION
 PATIENT REGISTRATION Patient s Last Name: Patient s First Name: MI: Address: City, State Zip code: Patient s Date of Birth: Patient s Social Security: Best Number to contact: Secondary Number: Marital
PATIENT REGISTRATION Patient s Last Name: Patient s First Name: MI: Address: City, State Zip code: Patient s Date of Birth: Patient s Social Security: Best Number to contact: Secondary Number: Marital
High Blood Sugar. Printable Materials
 Printable Materials Activity Card #1 Symptoms of High Blood Sugar or Pre-Diabetes Symptoms People often don t know they have high blood sugar or pre-diabetes. There are no symptoms and pre-diabetes can
Printable Materials Activity Card #1 Symptoms of High Blood Sugar or Pre-Diabetes Symptoms People often don t know they have high blood sugar or pre-diabetes. There are no symptoms and pre-diabetes can
St. Luke s MS Center New Patient Questionnaire. Name: Date: Birth date: Right or Left handed? Who is your Primary Doctor?
 St. Luke s MS Center New Patient Questionnaire Name: Date: Birth date: Right or Left handed? Who is your Primary Doctor? Who referred you to the MS Center? List any other doctors you see: Reason you have
St. Luke s MS Center New Patient Questionnaire Name: Date: Birth date: Right or Left handed? Who is your Primary Doctor? Who referred you to the MS Center? List any other doctors you see: Reason you have
City: State: Zip: City: State: Zip: Phone: Birth Date: Age: Marital Status: Single Married Divorced Widowed Cell Phone: City: State: Zip:
 Name: Mailing Address: First M.I. Last Today s Date: Physical Address: Phone: Birth Date: Age: Marital Status: Single Married Divorced Widowed Cell Phone: Employer: Occupation: Employer s Address: Work
Name: Mailing Address: First M.I. Last Today s Date: Physical Address: Phone: Birth Date: Age: Marital Status: Single Married Divorced Widowed Cell Phone: Employer: Occupation: Employer s Address: Work
REGISTRATION FORM. How would you like to receive health information? Electronic Paper In Person. Daytime Phone Preferred.
 Signature Preferred Pharmacy Referral Info Emergency Contact Guarantor Information Patient Information Name (Last, First, MI) REGISTRATION FORM Today's Date Street Address City State Zip Gender M F SSN
Signature Preferred Pharmacy Referral Info Emergency Contact Guarantor Information Patient Information Name (Last, First, MI) REGISTRATION FORM Today's Date Street Address City State Zip Gender M F SSN
Diabetes. Patient Education. What you need to know. Diabetes Facts. Improving Health Through Education. What is Diabetes?
 Diabetes What you need to know Diabetes Facts More than 3 million Canadians have diabetes (Canadian Diabetes Association, 2009). It is the 4th leading cause of death in the world (CDA, 2009). Patient Education
Diabetes What you need to know Diabetes Facts More than 3 million Canadians have diabetes (Canadian Diabetes Association, 2009). It is the 4th leading cause of death in the world (CDA, 2009). Patient Education
Medicare. Orientation Guide
 Medicare Orientation Guide Your Medicare Orientation Guide At MCS Classicare (HMO), we take care of you so you feel better every day. That s why we want to get you familiar and provide you with the tools
Medicare Orientation Guide Your Medicare Orientation Guide At MCS Classicare (HMO), we take care of you so you feel better every day. That s why we want to get you familiar and provide you with the tools
PATIENT INFORMATION INSURANCE INFORMATION
 PATIENT INFORMATION NAME DATE ADDRESS CITY ST ZIP PHONE(H) (C) (W) DATE OF BIRTH EMAIL AGE SEX: M F SS#(optional) EMPLOYER OCCUPATION ARE YOU CURRENTLY: MARRIED PARTNERED DIVORCED WIDOWED SINGLE SPOUSE/PARTNER
PATIENT INFORMATION NAME DATE ADDRESS CITY ST ZIP PHONE(H) (C) (W) DATE OF BIRTH EMAIL AGE SEX: M F SS#(optional) EMPLOYER OCCUPATION ARE YOU CURRENTLY: MARRIED PARTNERED DIVORCED WIDOWED SINGLE SPOUSE/PARTNER
How To Contact A Doctor From A Doctor'S Office
 Anthony S. Lombardi, MD, FACS Nilla Defazio, PA C Jessica Henderson, PA C PATIENT INFORMATION Date Patients Last Name First Name M.I. Suffix(i.e,Jr.,Sr.) Street Address City State Zip Code ( ) ( ) M S
Anthony S. Lombardi, MD, FACS Nilla Defazio, PA C Jessica Henderson, PA C PATIENT INFORMATION Date Patients Last Name First Name M.I. Suffix(i.e,Jr.,Sr.) Street Address City State Zip Code ( ) ( ) M S
LAWRENCE J. FINKEL, M.D., P.C. 360 CHURCH STREET WARRENTON, VA 20186 (540) 347-2020 PHONE (540) 341-7980 FAX www.finkelderm.net
 347-2020 PHONE (540) 341-7980 FAX www.finkelderm.net") 360 CHURCH STREET WARRENTON, VA 20186 (540) 347-2020 PHONE (540) 341-7980 FAX www.finkelderm.net Dear Patient: Welcome to our Practice. We have you scheduled for your first appointment at our office on
360 CHURCH STREET WARRENTON, VA 20186 (540) 347-2020 PHONE (540) 341-7980 FAX www.finkelderm.net Dear Patient: Welcome to our Practice. We have you scheduled for your first appointment at our office on
Health Information Form for Adults
 A. IDENTIFICATION B. EMERGENCY CONTACTS Name (Last) (First) (Middle) Maiden Name Primary Alternate In Case of Emergency, Notify: Primary Contact Name (Last) (First) (Middle) Relationship Home Work Home
A. IDENTIFICATION B. EMERGENCY CONTACTS Name (Last) (First) (Middle) Maiden Name Primary Alternate In Case of Emergency, Notify: Primary Contact Name (Last) (First) (Middle) Relationship Home Work Home
LOW T NATION TESTOSTERONE INTAKE FORM NAME: DATE: ADDRESS: CITY: STATE: ZIP: CELL #: HOME #: SOC SECURITY #: DATE OF BIRTH:
 LOW T NATION TESTOSTERONE INTAKE FORM NAME: DATE: ADDRESS: CITY: STATE: ZIP: CELL #: HOME #: SOC SECURITY #: DATE OF BIRTH: DRIVERS LICENSE NUMBER: STATE: EMAIL ADDRESS: MARITAL STATUS: ( ) SINGLE ( )
LOW T NATION TESTOSTERONE INTAKE FORM NAME: DATE: ADDRESS: CITY: STATE: ZIP: CELL #: HOME #: SOC SECURITY #: DATE OF BIRTH: DRIVERS LICENSE NUMBER: STATE: EMAIL ADDRESS: MARITAL STATUS: ( ) SINGLE ( )
Midha Medical Clinic REGISTRATION FORM
 Midha Medical Clinic REGISTRATION FORM Today s / / (PLEASE PRINT NEATLY) PATIENT INFORMATION Last Name: First Name: Middle Initial: IS THIS YOUR LEGAL NAME? YES NO IF NOT, WHAT IS YOUR LEGAL NAME DATE
Midha Medical Clinic REGISTRATION FORM Today s / / (PLEASE PRINT NEATLY) PATIENT INFORMATION Last Name: First Name: Middle Initial: IS THIS YOUR LEGAL NAME? YES NO IF NOT, WHAT IS YOUR LEGAL NAME DATE
X-Plain Diabetes - Introduction Reference Summary
 X-Plain Diabetes - Introduction Reference Summary Introduction Diabetes is a disease that affects millions of Americans every year. Your doctor may have informed you that you have diabetes. Although there
X-Plain Diabetes - Introduction Reference Summary Introduction Diabetes is a disease that affects millions of Americans every year. Your doctor may have informed you that you have diabetes. Although there
Voluntary Benefits Employee Enrollment and Change Form
 LifeMap Assurance Company TM P.O. Box 1271, MS E-3A Portland, OR 97207-1271 (503) 721-7161 (800) 794-5390 Voluntary Benefits Employee Enrollment and Change Form For residents of Oregon and Washington,
LifeMap Assurance Company TM P.O. Box 1271, MS E-3A Portland, OR 97207-1271 (503) 721-7161 (800) 794-5390 Voluntary Benefits Employee Enrollment and Change Form For residents of Oregon and Washington,
Diabetes Mellitus: Type 1
 Diabetes Mellitus: Type 1 What is type 1 diabetes mellitus? Type 1 diabetes is a disorder that happens when your body produces little or no insulin. The lack of insulin causes the level of sugar in your
Diabetes Mellitus: Type 1 What is type 1 diabetes mellitus? Type 1 diabetes is a disorder that happens when your body produces little or no insulin. The lack of insulin causes the level of sugar in your
Florida Eye Center Patient Registration Form (Please Print Clearly)
") Florida Eye Center Patient Registration Form (Please Print Clearly) Personal Information Legal Name: Last First MI Suffix Nickname: Social Security: - - Drivers License # Date of Birth: / / Mailing Address:
Florida Eye Center Patient Registration Form (Please Print Clearly) Personal Information Legal Name: Last First MI Suffix Nickname: Social Security: - - Drivers License # Date of Birth: / / Mailing Address:
Health Professional s. Guide to INSULIN PUMP THERAPY
 Health Professional s Guide to INSULIN PUMP THERAPY Table of Contents Introduction Presenting Insulin Pump Therapy to Your Patients When Your Patient Chooses the Pump Estimates for Starting Insulin Pump
Health Professional s Guide to INSULIN PUMP THERAPY Table of Contents Introduction Presenting Insulin Pump Therapy to Your Patients When Your Patient Chooses the Pump Estimates for Starting Insulin Pump
THE ROWANS SURGERY MEDICAL HISTORY QUESTIONNAIRE MALE & FEMALE 18+
 THE ROWANS SURGERY MEDICAL HISTORY QUESTIONNAIRE MALE & FEMALE 18+ Surname: First Name: Date of Birth: NHS Number: / / Mobile Telephone No: Male / Female If you wish to sign up for Vision On-Line services
THE ROWANS SURGERY MEDICAL HISTORY QUESTIONNAIRE MALE & FEMALE 18+ Surname: First Name: Date of Birth: NHS Number: / / Mobile Telephone No: Male / Female If you wish to sign up for Vision On-Line services
SLIDING SCALE INSULIN REGULAR PLAN
 PHYSICIAN S Weight Allergies DETAILS Patient Care POC Blood Sugar Check Per Sliding Scale Insulin Frequency AC & HS AC & HS 3 days TID BID q12h q6h q6h 24 hr q4h q2h Sliding Scale Insulin Regular Guidelines
PHYSICIAN S Weight Allergies DETAILS Patient Care POC Blood Sugar Check Per Sliding Scale Insulin Frequency AC & HS AC & HS 3 days TID BID q12h q6h q6h 24 hr q4h q2h Sliding Scale Insulin Regular Guidelines
Voluntary Benefits Employee Enrollment and Change Form
 Voluntary Benefits Employee Enrollment and Change Form LifeMap Assurance Company TM For residents of Oregon and Washington, the definition of a Spouse includes your legal husband or wife or your State
Voluntary Benefits Employee Enrollment and Change Form LifeMap Assurance Company TM For residents of Oregon and Washington, the definition of a Spouse includes your legal husband or wife or your State
PATIENT REGISTRATION AND HISTORY FORM ~ FAMILY EYE HEALTH ASSOCIATES
 PATIENT REGISTRATION AND HISTORY FORM ~ FAMILY EYE HEALTH ASSOCIATES PATIENT INFORMATION: Name (Last, First, MI) Date: Address: City State Zip Home Phone 2nd Phone Work Cell E-Mail Gender: M F Birthdate
PATIENT REGISTRATION AND HISTORY FORM ~ FAMILY EYE HEALTH ASSOCIATES PATIENT INFORMATION: Name (Last, First, MI) Date: Address: City State Zip Home Phone 2nd Phone Work Cell E-Mail Gender: M F Birthdate
Frederick County Department of Aging Meals on Wheels and Home Delivered Meal Service Application
 Frederick County Department of Aging Meals on Wheels and Home Delivered Meal Service Application Name Address Apt. # Apartment Complex or neighborhood City/State/Zip Primary Phone Date of Birth Secondary
Frederick County Department of Aging Meals on Wheels and Home Delivered Meal Service Application Name Address Apt. # Apartment Complex or neighborhood City/State/Zip Primary Phone Date of Birth Secondary