Neglect. Senior Social Worker. Child Protection Unit, PMH
|
|
|
- Whitney Lambert
- 8 years ago
- Views:
Transcription
1 Neglect Jo Smith Alice Johnson Senior Social Worker Paediatrician Child Protection Unit, PMH

2 Neglect a definition Definition: neglect is when a child is not provided with adequate food or shelter, effective medical, therapeutic or remedial care, and/or nurturance or supervision to a severe and/or persistent extent DCP Policy on neglect 2007

3 Definition - difficulties No universal definition Looking for absence of care Difficulties child protection agencies courts research Common agreement lack of one or more aspects of care resulting in harm or risk of harm

4 The neglect of neglect Neglect is common and serious Consequences as serious/more serious than other forms of abuse Child neglect has been an overlooked area in child protection Focus on research has been on inflicted injury and CSA

5 Forms of Neglect Abandonment: parents or guardians are dead, incapacitated, unable to be found, or are unwilling to care for the child Physical neglect: basic physical needs are not met as the child is not provided with necessary food, shelter, and clothing Medical neglect: the child is not provided with medical care Supervisory neglect: the guardians of the child are unable or unwilling to exercise adequate supervision and control of the child

6 Forms of neglect Psychological neglect: the child is likely to suffer psychological harm detrimental to the child's wellbeing Developmental neglect: the child or young person's safety, wellbeing, or development is threatened due to the caregiver not taking into account the child's developmental capabilities Failure to provide guidance : permitting criminal behaviour. Educational neglect: the school-aged child is not regularly attending school ((NSW Children and Young Persons (Care and Protection) Act, 1998, s.71.2).

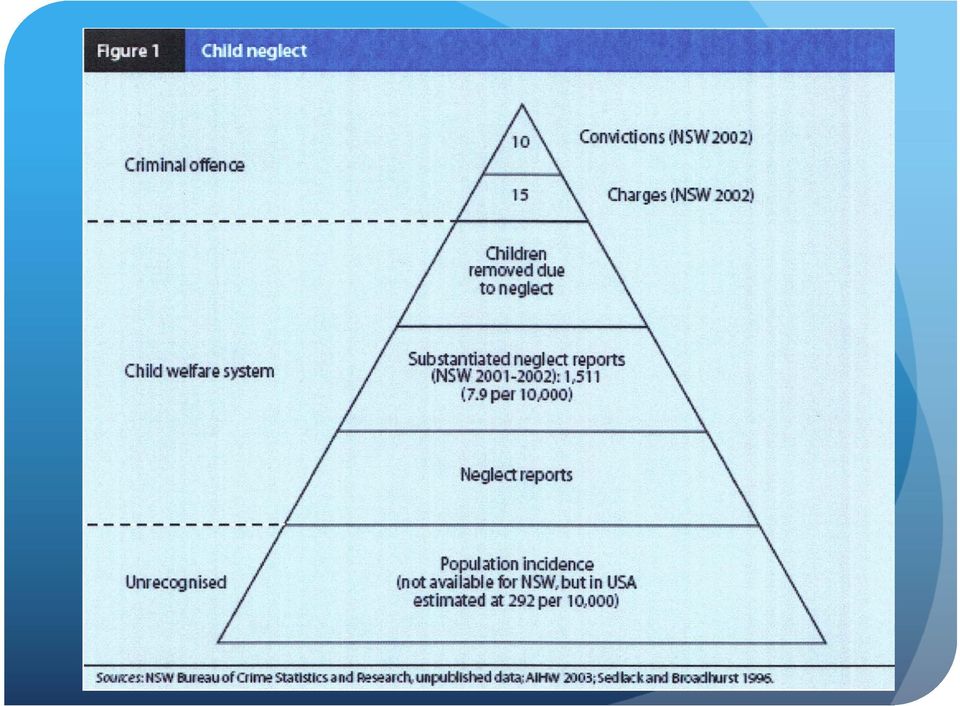
7 Neglect in WA Data from AIHW Commonest reason for substantiation by DCP (41% of all cases of abuse ) Commonest reason for Child Protection Orders

8
9 Neglect often co-exists with other forms of abuse physical abuse sexual abuse emotional or psychological abuse neglect Fabricated and induced illness

10 Drug Use and Neglect Parental drug use is a major risk factor for neglect Both chronic and episodic neglect Chronic: drug use compromises ability to perform basic functions like regular feeding, stimulation, hygiene Episodic: lack of supervision, ingestion of substances by child

11 Other risk factors for neglect Poverty Social deprivation Neighbourhood/community poverty Lack of education Family of origin abuse Intergenerational neglect Indigenous communities

12 Consequences of Neglect Short Term: death, serious injury/disability, impaired development, educational impact, attachment and self esteem issues. Long Term: psychological problems, relationship difficulties, criminal behaviour, financial problems, inter-generational neglect

13 Fatal neglect Deaths directly due to inadequate care 0.6% deaths in childhood due to maltreatment (WHO 2006) 30-40% deaths due to maltreatment are due to neglect (Berkowitz 2001) USA children died from abuse (35% due to neglect) 55 law enforcement officers were killed in the line of duty (Petit 1999)
 55 law enforcement officers were killed in")
14 Who is responsible? Parents/care-givers Neglect often seen as a failure of the caregiver (often the Mother) However several layers of responsibility exist Community Structural context: poverty, deprivation, social isolation, inadequate schooling/health care Seen in Indigenous communities

15 Case Example Wade Michael Scale age 11months Was found drowned in bath tub that hadn t been emptied from previous evening Prescription medication (diazepam) found in his system and parents stated no knowledge of how this could be Coroner found he had been immersed for minutes Parental history of illicit and prescribed drug use and physical violence DCP were involved and had recently returned child

16 Neglect reasons for CPU consultation Risk of neglect Medical neglect Supervision neglect FTT Other parents with mental illness/ substance abuse delay in presentation with acute illness, failure to attend OPD with chronic illness recurrent and/or serious accidents/ingestions non-organic failure to thrive children taken into care, children with other forms of abuse

17 CPU approach to neglect Joint medical and social work assessment Interviews with parents Observation of parents interaction with child Reviews of medical notes of child and siblings Gather information from Child Health Nurse/GP/other family members Information from DCP

18 CPU approach to neglect Examination General appearance/cleanliness/clo thing Wt/ht/OFC (? FTT) Skin (? Severe nappy rash/scabies/sores) Teeth (?hygiene?decay) Emotional state (?withdrawn? interaction with carer)
 Teeth (?hygiene?")
19 CPU approach to neglect Investigations Nutritional deficiencies Other forms of abuse Hb,iron studies,vit D skeletal survey, STI screening Consultation/referral DCP Police if concerns about criminal element

20 Difficulty in diagnosis When is parenting not good enough? Inflicted injury/csa definite event happened or not happened Neglect omission of care grey area subjective difficult to assess

21 When is a child in need of protection? the child has suffered, or is likely to suffer, harm as a result of any one or more of the following (i) physical abuse;(ii) sexual abuse;(iii) emotional abuse; (iv) psychological abuse; (v) neglect, and the child s parents have not protected, or are unlikely or unable to protect, the child from harm, or further harm, of that kind; CCSA 2004
22 Best interests of the child Best interests of the child: Need to protect the child from harm Capacity of the child s parents to protect them from harm Capacity of the child s parents or carers to provide for the child s needs CCSA 2004
23 Medical neglect
24 Medical neglect Includes 1)Failure to seek medical attention for obvious signs of serious illness 2)Failure to follow physician s instructions once medical advice has been sought Either of these can lead to serious disability or death
25 Case example medical neglect Jordan is a 13 year old boy with IDDM (diagnosed 2 years previously). His control has been poor and his last HbA1c was 12%. His school attendance is very poor. He lives with his mother (who has bipolar disorder) and his 3 siblings. He has not attended the diabetes clinic for 1 year.
26 What factors are necessary for a diagnosis of medical neglect? a) child is harmed or is at risk of harm because of lack of health care b) recommended health care offers significant net benefit to child c) benefit of treatment outweighs its morbidity so that reasonable caregivers would choose treatment over nontreatment d) access to healthcare is available e) caregiver understands the medical advice Jenny Pediatrics 2007
27 Why do families fail to seek/maintain medical care? Families Parent is intellectually impaired/mentally ill/substance affected Poverty Family chaos Lack of awareness of signs/symptoms of illness Lack of trust in health care Carers beliefs Child/adolescent s rejection Physician Lack of communication
28 Assessment and management of medical neglect 1) Chronology of PMH chart 2) Multidisciplinary meeting (may be PMH staff only initially) 3) Meet with parents (+ child/adolescent if appropriate) to ensure good understanding of what is required 4) Consider written contract outlining child s needs 5) Provide assistance to meet needs 6) Referral to DCP
29 Religious objections to medical care We focus on the child s needs NOT the caregiver s religious beliefs Religious objections are not granted different status to other types of objections Whilst we show sensitivity and flexibility towards religious beliefs, the best interests of the child overrides this
30 Medical neglect - summary Medical neglect can cause harm or death Paediatrician s responsibility is to the child If parents are not meeting the child s medical needs and the child is at risk of/has suffered harm this constitutes medical neglect
31 Failure to thrive and neglect
32 Definitions of FTT Weight for age decreasing across 2 centile lines (from a previously stable pattern) Weight < 3 rd centile or < 0.4 th centile Weight for length <80%
33 How common is FTT? FTT in infants born in inner cities in the UK 5% (Skuse 1988) PMH referrals FTT/poor growth 6-7% referral to DPAM
34 Nutritional atrophy 1905
35 Aetiology of FTT
36 How common is FTT as a manifestation of neglect? MINORITY of children with non-organic FTT are suffering from child neglect (Black and Dubowitz 2006) 5-10% children with non-organic FTT substantiated for neglect (Skuse 1995 and Wright 2000)
37 Deaths due to starvation
38 Assessment for FTT Moderate/severe FTT detailed history/examination plot growth accurately tests for causes of FTT tests for effects of FTT hospital admission monitoring for re-feeding syndrome
39 FTT - When to refer to CPU? Parents unable to provide adequate nutrition due to: intellectual impairment mental illness drug/alcohol addiction
40 FTT - When to refer to CPU? Parents unwilling to provide adequate nutrition Intentional with-holding of food Parents resistant to recommended interventions Strong beliefs in health/nutrition regimens that jeopardise a child s well-being Concerns about other forms of abuse
41 Case example - neglect 9 year old twin boys and 18/12 brother Not visible in community/not attending school Father admitted to Graylands 18/12 FTT /no imms/iron def anaemia/vit D def 9 year old twins vit D def/poor motor skills Nutritional/educational and developmental neglect
42 FTT - summary In cases of FTT a minority are a result of child neglect Child with FTT - refer to CPU if: parents unable to provide nutrition to child parents unwilling to provide nutrition to child other signs of abuse
43 Obesity is this ever neglect?
44 Is childhood obesity ever child neglect?
45 Case example morbid obesity 5 year old girl referred to PMH with morbid obesity 69kg morbidly obese Obstructive sleep apnoea (BIPAP) Insulin resistance Psychological problems CLASP programme
46 Obesity Viner BMJ 2010 Consider referral to child protection services when: Consistent failure to engage in support/treatment in a child with morbid obesity Parents actively promoting weight gain (Especially when child has secondary complications of obesity eg OSA, diabetes) Other abuse concerns (as well as obesity)
47 Neglect Common and serious Difficult to define Strong association with poverty and with substance abuse Neglected in terms of research
48 Thank you Any questions?
49