Substance Use Guideline 4B PERINATAL OPIOID EXPOSURE, CARE OF THE NEWBORN
|
|
|
- Ursula Lambert
- 9 years ago
- Views:
Transcription
1 British Columbia Reproductive Care Program Substance Use Guideline 4B PERINATAL OPIOID EXPOSURE, CARE OF THE NEWBORN INTRODUCTION During the antenatal period, the opportunity exists for the primary care giver and other involved team members to establish a relationship of trust with the woman. With the birth of the infant, consistency of approach with the mother / newborn pair is mandatory. A case manager should be identified, and team roles and tasks should be clearly defined and articulated. INITIAL ASSESSMENT (AT TIME OF BIRTH) 1) Review Prenatal History. 2) Complete physical exam See Newborn Record. Specific attention should be given to tone and neurological state. 3) Assess intoxication and withdrawal signs and symptoms. 4) Consider other causes of abnormal / unstable CNS status, which includes: sepsis / meningitis hypoglycemia hypocalcemia CNS haemorrhage 5) Initiate laboratory and radiologic investigations as clinically indicated. 6) Assess HIV, HCV, HBV status. Consider retesting mother if serology obtained early in pregnancy and high risk behaviors present during pregnancy (only if unobtainable from mother, or if mother is positive & followup of newborn s serostatus is required). 7) Options for drug screening include urine, meconium, or hair analysis. Hair analysis and meconium are useful drug screens to detect longitudinal exposure in pregnancy, but are not usually readily available. Urine drug screens can detect recent exposure just prior to delivery and are readily available in most centres in the province. It is important to note on the urine drug screen that methadone appears as methadone and not as an opiate. Heroin and codeine both are seen as opiates and breakdown to codeine and morphine. Drug screening may be indicated in some cases where the clinical picture of substance use is unclear. Informed consent from the mother is required. However, if the pediatrician/family physician deems that a neonatal drug screen is necessary for management, it can be obtained without maternal consent. November,1999 Page 1 of 8
 Complete physical exam See Newborn Record. Specific attention should be given to tone and neurological state. 3) Assess intoxication and withdrawal signs and symptoms.")
2 MANAGEMENT OF OPIOID WITHDRAWAL Not all infants exposed to opioids have withdrawal. If withdrawal is present the onset depends on the half life and the amount of substance used during pregnancy and when the last maternal dose was taken. In addition, the state of the neonatal liver plays a role in withdrawal onset. For example, infants usually begin heroin withdrawal within 1-3 days, whereas methadone withdrawal can take over a week to manifest. Thus when opioid use has occurred, the infant needs to be observed for 7-9 days prior to discharge (Wagner et al., 1998). If withdrawal is observed, then the neonate needs to stay in hospital for management. I ACUTE PHASE OF WITHDRAWAL A. Initial Assessment 1) Review maternal health status during pregnancy. 2) Consider the need for treatment of the newborn. 3) Use of a standardized withdrawal scoring sheet such as the Neonatal Withdrawal Observation Sheet (See Appendix A) can be useful both initially and for daily observation of response to treatment. 4) Consider where the newborn will be cared for e.g. Special Care Nursery, Neonatal Care Nursery, or Rooming in with the mother? (Usually a Level II nursery is appropriate) As much as is possible, maintain maternal-infant bond. B. Nonpharmacological Management 1) Begin with a quiet, darkened environment and then increase stimulation as tolerated. Typically, this would not begin until there has been a period of appropriate behavior e.g. good feeding and weight gain. Titrate intervention to newborn s signs and symptoms. 2) Breastfeeding should be encouraged unless contraindicated. For breastfeeding information please see Substance Use Guideline 4A: Perinatal Opioid Use, Care of the Mother, page 10. 3) Consider use of higher cal (24 cal/oz) formula if poor weight gain is demonstrated. C. Pharmacological Management Opiates are the drug of choice to manage neonatal withdrawal (American Academy of Pediatrics, 1998; Theis et al., 1997). Morphine solution is readily available and easily titrated. Clinical management recommendations using morphine solution are indicated below. Despite their mothers being on opioids during pregnancy, some newborns do not require morphine at all. Thus they should only be given morphine if their symptoms indicate. The decision to start morphine should be based on a constellation of physical signs and general behaviors, and should be considered based on clinical judgment. Treatment of Neonatal Withdrawal should be considered, having ruled out other medical November,1999 Page 2 of 8

3 conditions, when there is a constellation of the following signs and symptoms unresponsive to environmental control: 1) Convulsions. 2) Inconsolability / crying continuously for 3 hours. 3) Persistent tremors / jitteriness when undisturbed. 4) Continuous central nervous system irritability including hyperactive Moro reflex, tremors / jitteriness, increased muscle tone and unprovoked muscle jerks. 5) Persistent vomiting or projectile vomiting over a 12 hour period. 6) Explosive diarrhea for 2-3 consecutive episodes. The neonatal withdrawal sheet should be used to assess overall withdrawal symptoms. While sneezing and jitteriness are signs of early withdrawal, they rarely need morphine. However, in combination with clinical signs such as tachycardia, tachypnea, water loss in stools, fever, or weight loss > 10%, morphine may be required. It is important that a differential diagnosis for the signs and symptoms be considered (See page 1). Calculating Morphine Dose Concentration of Oral Morphine Solution is 1 mg/ml. Some institutions dilute this to 0.4 mg/ml, which may result in confusion. The recommendation is to use the standard 1 mg/ml. solution, and use 1:10 dilution if dilution is required (see tapering doses). All doses should be written as mg of morphine to prevent confusion when different dilutions are used. For morphine doses, see Table I on page 4. November,1999 Page 3 of 8
 Persistent vomiting or projectile vomiting over a 12 hour period. 6) Explosive diarrhea for 2-3 consecutive episodes.")
4 TABLE I MORPHINE DOSE Starting Dose: Morphine Solution 0.03 mg/kg/dose given orally every 3 hours. Round dose to the nearest 0.01 ml of morphine solution. Prn Dose: 50% of initial morphine dose may be administered between maintenance doses for breakthrough symptoms of withdrawal. Round dose to the nearest 0.01 ml morphine. Calculating Ongoing Daily Dose: Add total morphine received the day before (regular dose + prn doses). Divide into 8 equal doses and give every 3 hours as the new regular dose. Calculate the new prn dose as 50% of new regular dose. Note: Morphine dose must be reviewed daily and recalculated based on daily weights and ongoing symptoms. Note: The smallest volume that can be accurately measured in a 1 ml syringe is 0.05 ml. The volume delivered includes the dead space at the end of the syringe i.e. do not flush the syringe to get the full dose. If tubing is used, flush the drug through the tubing to ensure that the full dose is administered. Use a new syringe to flush the tubing, otherwise the morphine intended to stay in the dead space of the syringe is being administered. The medical management of an infant with symptoms of withdrawal from prenatal drug exposure should be guided by the infant s vital signs and symptoms. As a result, dosages and weaning schedules should be individually titrated to the desired clinical effect e.g. behavior, weight gain, successful feedings, etc. Although other drugs such as phenobarbital and diazepam are used in some centers, opioids are considered the drugs of choice. Paregoric contains alcohol and camphor so instead we recommend morphine as the drug of choice when treating neonatal opioid withdrawal. D. Other Broader Social / Medical Issues Encourage mothers and partners to be actively involved with the care of their infants as appropriate. When appropriate, have parents stay at the hospital to provide all aspects of care, with the exception of medication and nursing duties. Alternate units for mother not needing care but needing to be near her infant are ideal and should be utilized if available. This is key since bonding can be difficult for a variety of reasons. Vaccinations: If mother is Hepatitis B positive, the infant should receive Hepatitis B vaccine (e.g. Energix B) and Hepatitis B Immuno Globulin (HBIG) as per protocol. If mother is Hepatitis B negative, then the newborn should be considered high risk and should be initiated on a Hepatitis B vaccination series. November,1999 Page 4 of 8

5 II STABILIZATION AND RESOLUTION PHASE Once the newborn is stable on morphine solution with minimum and/or declining symptoms of withdrawal for 3-5 days and the infant is gaining gms per day, then tapering of morphine can begin. TABLE II TAPERING OF MORPHINE Taper the stable morphine dose by 10% q2days. Round dose to the nearest 0.01 ml morphine oral solution. A prn dose may be considered for significant breakthrough symptoms that do not settle with interventions such as swaddling, holding, rocking, etc. If withdrawal symptoms occur give PRN doses (50% of last dose, no more frequently than q3h). Include prn doses in new effective dose. Once each dose reaches 0.05 mg, dilute morphine to 1:10 to make a solution of 0.1 mg/ml. Continue tapering until a dose of 0.02 mg every 3 hours is reached, then discontinue. Note: Do not increase dose interval as a strategy to taper morphine. Similarly, to manage symptoms between regular doses, use a prn that is ½ of the regular dose, rather than decreasing the dose interval. III BEFORE DISCHARGE, CONTINUE TO ASSESS 1) Infant growth and development: a weight gain of grams/day (may be lower if mother is breastfeeding) is the ideal or target. 2) Feeding the baby should be receiving high caloric formula for 3-5 days prior to discharge if the mother is not breastfeeding. 3) Assess handling and state regulation (sleeping, cry, behavior). 4) Assess environmental adaptation return to normal light conditions 3-5 days prior to discharge. 5) Assess for other medical concerns. November,1999 Page 5 of 8
. Include prn doses in new effective dose. Once each dose reaches 0.")
6 REFERENCES American Academy of Pediatrics committee on Drugs. (1998). Neonatal drug withdrawal. Pediatrics (101). NO.6, Theis, J., Selby, P., Ikizler, Y. & Koren, G. (1997). Current management of the neonatal abstinence syndrome: A critical analysis of the evidence. Biol Neonate ( 71) Wagner, C., Katikaneni, L., Cox, J., & Ryan, R. (1998). The impact of prenatal drug exposure on the neonate. Obstetrical and Gynecological Clinics of North America (25). No.1, November,1999 Page 6 of 8
. The impact of prenatal drug exposure on the neonate.")
7 November,1999 Page 7 of 8
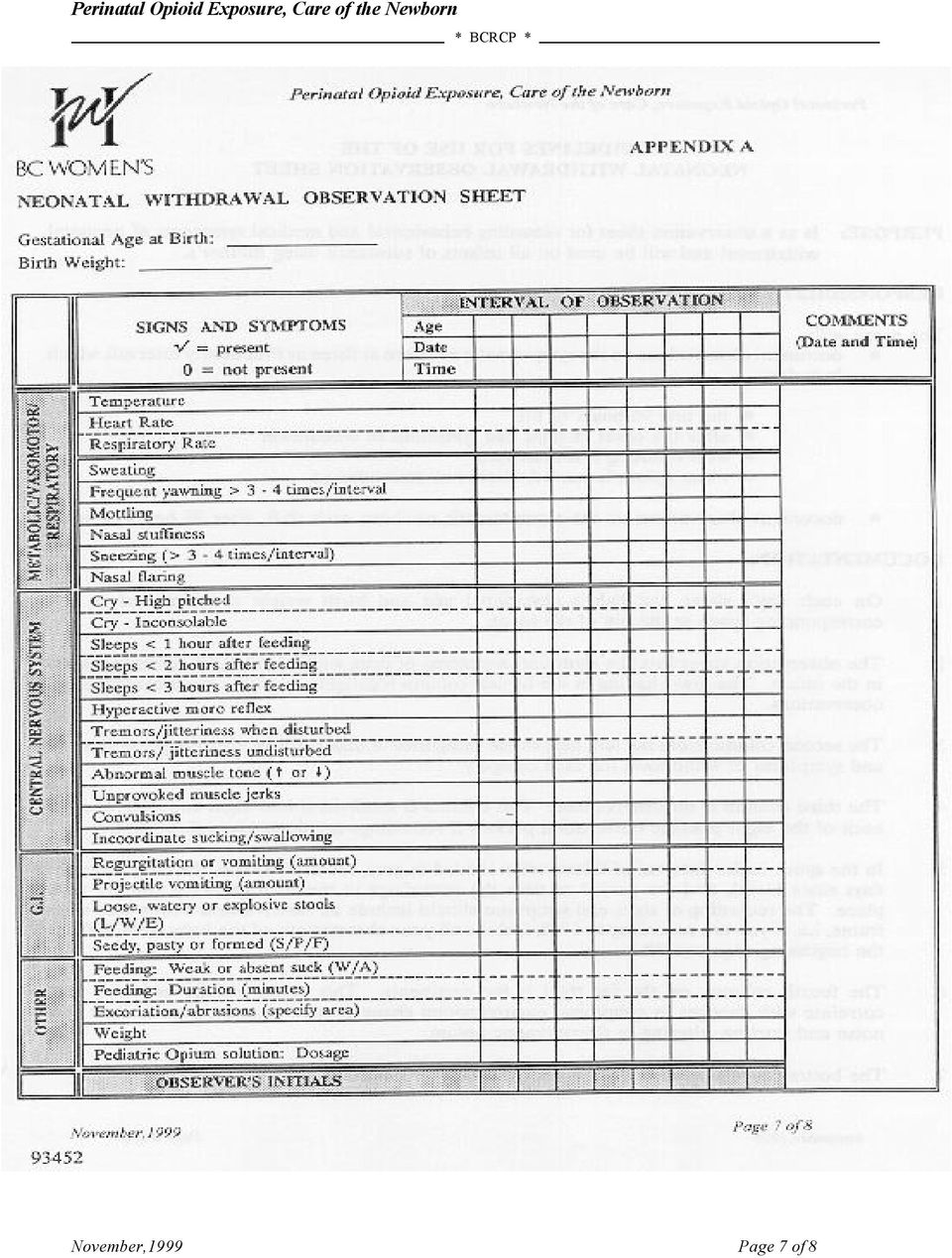
8 PURPOSE: RESPONSIBILITIES: GUIDELINES FOR USE OF THE NEONATAL WITHDRAWAL OBSERVATION SHEET Is as a observation sheet for recording behavioural and medical symptoms of neonatal withdrawal and will be used on all infants of substance using mother s. The nurse will: document observations on the symptomatic newborn at three or four hourly intervals which includes: The first 96 hours of life After the onset of signs and symptoms of withdrawal With vomiting and diarrhoea When opium is started, altered or discontinued document observations on the asymptomatic newborn each shift, after 96 hours of age. DOCUMENTATION: 1. On each day s sheet, the baby s gestational age and birth weight are recorded in the corresponding space at the top of the sheet. 2. The observation sheet lists the signs and symptoms of drug withdrawal most commonly seen in the infant. The grey shading in the far left column highlights the three main categories of observations. 3. The second column from the left, next to the categories of observations, lists the possible signs and symptoms of withdrawal for each category. 4. The third column is for observations. This column is subdivided into eight columns, one for each of the eight possible observation periods if recordings are done every three hours. 5. In the space under Interval of Observation shaded in grey, record the date, the baby s age (in days since birth), and the period of time the recordings in the corresponding column take place. The recording of signs and symptoms should include all observations within that time frame, i.e. if you are recording at 1100, include all your observations of the baby from 0700 at the beginning of your shift. 6. The fourth column, on the far right is for comments. This could include activities that correlate with changes in symptoms, environmental changes, such as alterations in light and noise and starting, altering or discontinuing opium. 7. The bottom row, shaded in grey, is for the Observer s Initials. November,1999 Page 8 of 8

NEONATAL ABSTINENCE SYNDROME AND SCORING SYSTEM
 VIDANT MEDICAL CENTER PATIENT CARE _ SUBJECT: Abstinence Scoring NUMBER: A-1 PAGE: 1 OF: 5 _ NEONATAL ABSTINENCE SYNDROME AND SCORING SYSTEM POLICY: A thorough evaluation of the infant is required in order
VIDANT MEDICAL CENTER PATIENT CARE _ SUBJECT: Abstinence Scoring NUMBER: A-1 PAGE: 1 OF: 5 _ NEONATAL ABSTINENCE SYNDROME AND SCORING SYSTEM POLICY: A thorough evaluation of the infant is required in order
NEONATAL ABSTINENCE SYNDROME. Osama Naga, M.D. PGY2
 NEONATAL ABSTINENCE SYNDROME Osama Naga, M.D. PGY2 Objective: Describe the common causes of NAS Clinical Presentation Diagnosis Identify the different scoring system for pharmacologic therapy Minimize
NEONATAL ABSTINENCE SYNDROME Osama Naga, M.D. PGY2 Objective: Describe the common causes of NAS Clinical Presentation Diagnosis Identify the different scoring system for pharmacologic therapy Minimize
Treatment Guidelines for Neonatal Narcotic Abstinence Syndrome with Diluted Oral Morphine and Clonidine
 Treatment Guidelines for Neonatal Narcotic Abstinence Syndrome with Diluted Oral Morphine and Clonidine Background Morphine sulfate has been recommended by the AAP as the first-line agent for the pharmacologic
Treatment Guidelines for Neonatal Narcotic Abstinence Syndrome with Diluted Oral Morphine and Clonidine Background Morphine sulfate has been recommended by the AAP as the first-line agent for the pharmacologic
CHILDREN S SERVICES. Neonatal Abstinence Syndrome
 CHILDREN S SERVICES Neonatal Abstinence Syndrome Background Neonatal Abstinence Syndrome (NAS) is a combination of behavioural and physiological signs and symptoms that occur in newborns going through
CHILDREN S SERVICES Neonatal Abstinence Syndrome Background Neonatal Abstinence Syndrome (NAS) is a combination of behavioural and physiological signs and symptoms that occur in newborns going through
Management of Neonatal Abstinence Syndrome and Iatrogenic Drug Withdrawal
 Management of Neonatal Abstinence Syndrome and Iatrogenic Drug Withdrawal Kirsten H. Ohler, Pharm.D., BCPS Clinical Assistant Professor Neonatal / Pediatric Clinical Pharmacist University of Illinois at
Management of Neonatal Abstinence Syndrome and Iatrogenic Drug Withdrawal Kirsten H. Ohler, Pharm.D., BCPS Clinical Assistant Professor Neonatal / Pediatric Clinical Pharmacist University of Illinois at
Identifying Neonatal Abstinence Syndrome (NAS) and Treatment Guidelines University of Iowa Children s Hospital -2/11/13
 and Treatment Guidelines University of Iowa Children s Hospital -2/11/13") Identifying Neonatal Abstinence Syndrome (NAS) and Treatment Guidelines University of Iowa Children s Hospital -// What is Neonatal Abstinence Syndrome? Neonatal withdrawal after intrauterine exposure
Identifying Neonatal Abstinence Syndrome (NAS) and Treatment Guidelines University of Iowa Children s Hospital -// What is Neonatal Abstinence Syndrome? Neonatal withdrawal after intrauterine exposure
SOUTH CENTRAL NEONATAL NETWORK GUIDELINE. South Central (North) Guideline for Neonatal Drug Withdrawal
 Guideline for Neonatal Drug Withdrawal") SOUTH CENTRAL NEONATAL NETWORK GUIDELINE South Central (North) Guideline for Neonatal Drug Withdrawal Approved by & South Central Neonatal Steering Group for South Central North. date Date of Implementation
SOUTH CENTRAL NEONATAL NETWORK GUIDELINE South Central (North) Guideline for Neonatal Drug Withdrawal Approved by & South Central Neonatal Steering Group for South Central North. date Date of Implementation
Current Trends In Identifying And Treating Newborns With Withdrawal Syndromes 6/24/2010
 Current Trends In Identifying And Treating Newborns With Withdrawal Syndromes 6/24/2010 Substance Exposed Newborns Alcohol Tobacco Caffeine Amphetamines Cocaine Barbituates Selective Serotonin Re-uptake
Current Trends In Identifying And Treating Newborns With Withdrawal Syndromes 6/24/2010 Substance Exposed Newborns Alcohol Tobacco Caffeine Amphetamines Cocaine Barbituates Selective Serotonin Re-uptake
Wales Neonatal Network Guideline
 Guideline on the Management of Neonatal Abstinence Syndrome Introduction Neonatal Abstinence Syndrome (NAS) is a constellation of symptoms and signs occurring in a baby as a result of withdrawal from physically
Guideline on the Management of Neonatal Abstinence Syndrome Introduction Neonatal Abstinence Syndrome (NAS) is a constellation of symptoms and signs occurring in a baby as a result of withdrawal from physically
Management of Pregnancy. Opioid Addiction Treatment
 Management of Pregnancy Opioid Addiction Treatment Perinatal Opioid Addiction Pharmacotherapy and co-ordination of care are essential elements in the comprehensive care of pregnant patients with opioid
Management of Pregnancy Opioid Addiction Treatment Perinatal Opioid Addiction Pharmacotherapy and co-ordination of care are essential elements in the comprehensive care of pregnant patients with opioid
NEONATAL ABSTINENCE SYNDROME (NAS)- THE CARE YOUR BABY MAY NEED
- THE CARE YOUR BABY MAY NEED") NEONATAL ABSTINENCE SYNDROME (NAS)- THE CARE YOUR BABY MAY NEED Information Leaflet Your Health. Our Priority. Page 2 of 8 Welcome to Stepping Hill Hospital Women's Unit The aims of this leaflet are to:
NEONATAL ABSTINENCE SYNDROME (NAS)- THE CARE YOUR BABY MAY NEED Information Leaflet Your Health. Our Priority. Page 2 of 8 Welcome to Stepping Hill Hospital Women's Unit The aims of this leaflet are to:
Established in 1974 Non-Profit Federal Block Grant recipient Accept Medicaid, Private Insurance, and Self-Pay.
 Established in 1974 Non-Profit Federal Block Grant recipient Accept Medicaid, Private Insurance, and Self-Pay. Patients are not denied treatment if they do not have the ability to pay for services Schedule
Established in 1974 Non-Profit Federal Block Grant recipient Accept Medicaid, Private Insurance, and Self-Pay. Patients are not denied treatment if they do not have the ability to pay for services Schedule
V11.2 NPIC/QAS. Special Quarterly Report: Linked Analysis Neonatal Abstinence Syndrome
 V11.2 NPIC/QAS Special Quarterly Report: Linked Analysis Neonatal Abstinence Syndrome I. Background The use of drugs and alcohol during pregnancy has been shown in several studies to affect the health
V11.2 NPIC/QAS Special Quarterly Report: Linked Analysis Neonatal Abstinence Syndrome I. Background The use of drugs and alcohol during pregnancy has been shown in several studies to affect the health
Neonatal Abstinence Syndrome: Indian Health Service (IHS) Best Practices Guidelines
 Best Practices Guidelines") Neonatal Abstinence Syndrome: Indian Health Service (IHS) Best Practices Guidelines 1. Neonatal Drug Withdrawal Intrauterine exposure to certain drugs and medications can cause clinical symptoms in the
Neonatal Abstinence Syndrome: Indian Health Service (IHS) Best Practices Guidelines 1. Neonatal Drug Withdrawal Intrauterine exposure to certain drugs and medications can cause clinical symptoms in the
Neonatal Abstinence Syndrome
 Neonatal Abstinence Syndrome D COGHLAN, *M MILNER, T CLARKE, I LAMBERT, C MCDERMOT, M MCNALLY, M BECKETT. T MATTHEWS Department of Paediatrics and *Obstetrics. Rotunda Hospital. Parnell Square. Dublin
Neonatal Abstinence Syndrome D COGHLAN, *M MILNER, T CLARKE, I LAMBERT, C MCDERMOT, M MCNALLY, M BECKETT. T MATTHEWS Department of Paediatrics and *Obstetrics. Rotunda Hospital. Parnell Square. Dublin
Methadone and Pregnancy
 Methadone and Pregnancy Methadone 101/Hospitalist Workshop Launette Rieb, MD, MSc, CCFP, CCSAM, FCFP Clinical Associate Professor, Dept. Family Practice, UBC American Board of Addiction Medicine Certified
Methadone and Pregnancy Methadone 101/Hospitalist Workshop Launette Rieb, MD, MSc, CCFP, CCSAM, FCFP Clinical Associate Professor, Dept. Family Practice, UBC American Board of Addiction Medicine Certified
Neonatal Abstinence Syndrome (NAS)
") Women and Newborn Health Service King Edward Memorial Hospital Neonatal Abstinence Syndrome (NAS) W O M E N A N D N E W B O R N drug and alcohol service (wandas) Delivering a Healthy WA Neonatal Abstinence
Women and Newborn Health Service King Edward Memorial Hospital Neonatal Abstinence Syndrome (NAS) W O M E N A N D N E W B O R N drug and alcohol service (wandas) Delivering a Healthy WA Neonatal Abstinence
Neonatal Abstinence Syndrome. A Guide for Families
 Neonatal Abstinence Syndrome A Guide for Families Contents What is Neonatal Abstinence Syndrome (NAS)?...................... 4 When will my baby show signs of NAS?..................................................
Neonatal Abstinence Syndrome A Guide for Families Contents What is Neonatal Abstinence Syndrome (NAS)?...................... 4 When will my baby show signs of NAS?..................................................
Algorithm for Initiating Antidepressant Therapy in Depression
 Algorithm for Initiating Antidepressant Therapy in Depression Refer for psychotherapy if patient preference or add cognitive behavioural office skills to antidepressant medication Moderate to Severe depression
Algorithm for Initiating Antidepressant Therapy in Depression Refer for psychotherapy if patient preference or add cognitive behavioural office skills to antidepressant medication Moderate to Severe depression
Introduction to Neonatal Abstinence Syndrome
 Introduction to Neonatal Abstinence Syndrome Cara Christ, MD Director, Arizona Department of Health Services Learning Objectives 1.Define Neonatal Abstinence Syndrome 2.Describe Neonatal Abstinence Syndrome
Introduction to Neonatal Abstinence Syndrome Cara Christ, MD Director, Arizona Department of Health Services Learning Objectives 1.Define Neonatal Abstinence Syndrome 2.Describe Neonatal Abstinence Syndrome
NHS FORTH VALLEY Management of Neonatal Abstinence Syndrome
 NHS FORTH VALLEY Management of Neonatal Abstinence Syndrome Date of First Issue 25/10/2011 Approved 25/11/2011 Current Issue Date 30/11/2011 Review Date 30/11/2013 Version 1.00 EQIA Yes 06/12/2011 Author
NHS FORTH VALLEY Management of Neonatal Abstinence Syndrome Date of First Issue 25/10/2011 Approved 25/11/2011 Current Issue Date 30/11/2011 Review Date 30/11/2013 Version 1.00 EQIA Yes 06/12/2011 Author
BABIES BORN TO ADDICTED MOTHERS
 BABIES BORN TO ADDICTED MOTHERS PATRICA M. MESSERLE LICENSED CLINICAL PSYCHOLOGIST, M.A., ABSNP LICENSED SCHOOL PSYCHOLOGIST DIPLOMATE OF THE AMERICAN BOARD OF SCHOOL- NEUROPSYCHOLOGY 1 Signs and Symptoms
BABIES BORN TO ADDICTED MOTHERS PATRICA M. MESSERLE LICENSED CLINICAL PSYCHOLOGIST, M.A., ABSNP LICENSED SCHOOL PSYCHOLOGIST DIPLOMATE OF THE AMERICAN BOARD OF SCHOOL- NEUROPSYCHOLOGY 1 Signs and Symptoms
Challenges of Foster Parents who Care for Infants with Neonatal Abstinence Syndrome
 Challenges of Foster Parents who Care for Infants with Neonatal Abstinence Syndrome All Health Care Providers are required by law to make a referral to the Department of Children s Services (DCS) Child
Challenges of Foster Parents who Care for Infants with Neonatal Abstinence Syndrome All Health Care Providers are required by law to make a referral to the Department of Children s Services (DCS) Child
NNEPQIN Guideline for the Management of Labor, Delivery and the Newborn in the Opioid Dependent Pregnancy. March 2014
 The following guidelines are intended only as a general educational resource for hospitals and clinicians, and are not intended to reflect or establish a standard of care or to replace individual clinician
The following guidelines are intended only as a general educational resource for hospitals and clinicians, and are not intended to reflect or establish a standard of care or to replace individual clinician
Evaluation of a Morphine Weaning Protocol in Pediatric Intensive Care Patients
 Evaluation of a Morphine Weaning Protocol in Pediatric Intensive Care Patients Jennifer Kuhns, Pharm.D. Pharmacy Practice Resident Children s Hospital of Michigan **The speaker has no actual or potential
Evaluation of a Morphine Weaning Protocol in Pediatric Intensive Care Patients Jennifer Kuhns, Pharm.D. Pharmacy Practice Resident Children s Hospital of Michigan **The speaker has no actual or potential
Ethical Issues Related to Long-Term Consequences of Neonatal Abstinence Syndrome (NAS) Christopher Church, Ph.D.
 Christopher Church, Ph.D.") Ethical Issues Related to Long-Term Consequences of Neonatal Abstinence Syndrome (NAS) Christopher Church, Ph.D. Content and Objectives Content: Describe common ethical issues related to caring for babies
Ethical Issues Related to Long-Term Consequences of Neonatal Abstinence Syndrome (NAS) Christopher Church, Ph.D. Content and Objectives Content: Describe common ethical issues related to caring for babies
Substance Abuse During Pregnancy: Moms on Meds. Jennifer Anderson Maddron, M.D LeConte Womens Healthcare Associates
 Substance Abuse During Pregnancy: Moms on Meds Jennifer Anderson Maddron, M.D LeConte Womens Healthcare Associates 2010 National Survey on Drug Use and Health An estimated 4.4% of pregnant women reported
Substance Abuse During Pregnancy: Moms on Meds Jennifer Anderson Maddron, M.D LeConte Womens Healthcare Associates 2010 National Survey on Drug Use and Health An estimated 4.4% of pregnant women reported
4/18/14. Background. Evaluation of a Morphine Weaning Protocol in Pediatric Intensive Care Patients. Background. Signs and Symptoms of Withdrawal
 Background 1 Evaluation of a Morphine Weaning Protocol in Pediatric Intensive Care Patients Alyssa Cavanaugh, PharmD PGY1 Pharmacy Resident Children s Hospital of Michigan **The speaker has no actual or
Background 1 Evaluation of a Morphine Weaning Protocol in Pediatric Intensive Care Patients Alyssa Cavanaugh, PharmD PGY1 Pharmacy Resident Children s Hospital of Michigan **The speaker has no actual or
Management of Neonatal Opioid Withdrawal
 Management of Neonatal Opioid Withdrawal Neonatal Abstinence Syndrome Overview... 1 Opioid Addiction... 1 Opioids and Pregnancy... 1 GUIDELINES FOR MANAGEMENT OF OPIOID-EXPOSED NEWBORNS... 3 Site of Care
Management of Neonatal Opioid Withdrawal Neonatal Abstinence Syndrome Overview... 1 Opioid Addiction... 1 Opioids and Pregnancy... 1 GUIDELINES FOR MANAGEMENT OF OPIOID-EXPOSED NEWBORNS... 3 Site of Care
New York State Office of Alcoholism & Substance Abuse Services Addiction Services for Prevention, Treatment, Recovery
 New York State Office of Alcoholism & Substance Abuse Services Addiction Services for Prevention, Treatment, Recovery USING THE 48 HOUR OBSERVATION BED USING THE 48 HOUR OBSERVATION BED Detoxification
New York State Office of Alcoholism & Substance Abuse Services Addiction Services for Prevention, Treatment, Recovery USING THE 48 HOUR OBSERVATION BED USING THE 48 HOUR OBSERVATION BED Detoxification
Welcome. How Do I Ask Questions? Agenda. Thank you for joining us today. The webinar will begin in a few moments.
 Welcome How Do I Ask Questions? Thank you for joining us today. The webinar will begin in a few moments. If you are experiencing technical problems with the GoToWebinar program, contact the GoToWebinar
Welcome How Do I Ask Questions? Thank you for joining us today. The webinar will begin in a few moments. If you are experiencing technical problems with the GoToWebinar program, contact the GoToWebinar
A guide for parents of babies at risk of Neonatal Abstinence Syndrome Planning care for you and your baby
 A guide for parents of babies at risk of Neonatal Abstinence Syndrome Planning care for you and your baby Reading this booklet can help you: learn how certain drugs can affect your baby during pregnancy
A guide for parents of babies at risk of Neonatal Abstinence Syndrome Planning care for you and your baby Reading this booklet can help you: learn how certain drugs can affect your baby during pregnancy
WITHDRAWAL OF ANALGESIA AND SEDATION
 WITHDRAWAL OF ANALGESIA AND SEDATION Patients receiving analgesia and/or sedation for longer than 5-7 days may suffer withdrawal if these drugs are suddenly stopped. To prevent this happening drug doses
WITHDRAWAL OF ANALGESIA AND SEDATION Patients receiving analgesia and/or sedation for longer than 5-7 days may suffer withdrawal if these drugs are suddenly stopped. To prevent this happening drug doses
Naloxone Hydrochloride Injection PRODUCT INFORMATION
 Naloxone Hydrochloride Injection PRODUCT INFORMATION DESCRIPTION Naloxone hydrochloride is 17-allyl-4,5α-epoxy-3,14-dihydroxymorphinan-6-one hydrochloride; C 19 H 21 NO 4.HCl. It is an off-white powder
Naloxone Hydrochloride Injection PRODUCT INFORMATION DESCRIPTION Naloxone hydrochloride is 17-allyl-4,5α-epoxy-3,14-dihydroxymorphinan-6-one hydrochloride; C 19 H 21 NO 4.HCl. It is an off-white powder
10/19/15. Stephen Loyd, M.D., F.A.C.P Healthy Kingsport Meadowview Convention Center Kingsport, Tennessee October 17, 2015
 Stephen Loyd, M.D., F.A.C.P Healthy Kingsport Meadowview Convention Center Kingsport, Tennessee October 17, 2015 Receives no commercial support, in any form, from pharmaceutical companies or anyone else
Stephen Loyd, M.D., F.A.C.P Healthy Kingsport Meadowview Convention Center Kingsport, Tennessee October 17, 2015 Receives no commercial support, in any form, from pharmaceutical companies or anyone else
Massachusetts Department of Public Health Guidelines for Community Standard for Maternal/Newborn Screening For Alcohol/Substance Use
 The Commonwealth of Massachusetts Executive Office of Health and Human Services Department of Public Health 250 Washington Street, Boston, MA 02108-4619 DEVAL L. PATRICK GOVERNOR TIMOTHY P. MURRAY LIEUTENANT
The Commonwealth of Massachusetts Executive Office of Health and Human Services Department of Public Health 250 Washington Street, Boston, MA 02108-4619 DEVAL L. PATRICK GOVERNOR TIMOTHY P. MURRAY LIEUTENANT
Prevention and Treatment of Opioid and Benzodiazepine Withdrawal
 1.0 Introduction The purpose of this guideline is to ensure that patients who are at risk of developing withdrawal symptoms can be weaned off opioids and benzodiazepines in a timely fashion. It is appropriate
1.0 Introduction The purpose of this guideline is to ensure that patients who are at risk of developing withdrawal symptoms can be weaned off opioids and benzodiazepines in a timely fashion. It is appropriate
DRUG AND ALCOHOL DETOXIFICATION: A GUIDE TO OUR SERVICES
 01736 850006 www.bosencefarm.co.uk DRUG AND ALCOHOL DETOXIFICATION: A GUIDE TO OUR SERVICES An environment for change Boswyns provides medically-led drug and alcohol assessment, detoxification and stabilisation.
01736 850006 www.bosencefarm.co.uk DRUG AND ALCOHOL DETOXIFICATION: A GUIDE TO OUR SERVICES An environment for change Boswyns provides medically-led drug and alcohol assessment, detoxification and stabilisation.
Opioid/Opiate Dependent Pregnant Women
 Opioid/Opiate Dependent Pregnant Women The epidemic, safety, stigma, and how to help. Presented by Lisa Ramirez MA,LCDC & Kerby Stewart MD The prescription painkiller epidemic is killing more women than
Opioid/Opiate Dependent Pregnant Women The epidemic, safety, stigma, and how to help. Presented by Lisa Ramirez MA,LCDC & Kerby Stewart MD The prescription painkiller epidemic is killing more women than
COMMUNITY BUPRENORPHINE PRESCRIBING IN OPIATE DEPENDENCE
 COMMUNITY BUPRENORPHINE PRESCRIBING IN OPIATE DEPENDENCE INTRODUCTION High dose sublingual buprenorphine (Subutex) tablets are available in the following strengths 0.4 mg, 2 mg, and 8 mg. Suboxone tablets,
COMMUNITY BUPRENORPHINE PRESCRIBING IN OPIATE DEPENDENCE INTRODUCTION High dose sublingual buprenorphine (Subutex) tablets are available in the following strengths 0.4 mg, 2 mg, and 8 mg. Suboxone tablets,
Medication Assisted Treatment
 Medication Assisted Treatment Tanya Hiser, MS, LPC State Opioid Treatment Authority Bureau Of Prevention, Treatment, & Recovery State of Wisconsin Elizabeth Collier, MSW, CSAC, ICS, LCSW TANF Best Practice
Medication Assisted Treatment Tanya Hiser, MS, LPC State Opioid Treatment Authority Bureau Of Prevention, Treatment, & Recovery State of Wisconsin Elizabeth Collier, MSW, CSAC, ICS, LCSW TANF Best Practice
Assessment and Management of Opioid, Benzodiazepine, and Sedative-Hypnotic Withdrawal
 Assessment and Management of Opioid, Benzodiazepine, and Sedative-Hypnotic Withdrawal Roger Cicala, M. D. Assistant Medical Director Tennessee Physician s Wellness Program Step 1 Don t 1 It is legal in
Assessment and Management of Opioid, Benzodiazepine, and Sedative-Hypnotic Withdrawal Roger Cicala, M. D. Assistant Medical Director Tennessee Physician s Wellness Program Step 1 Don t 1 It is legal in
NHS FORTH VALLEY Guidelines for Hepatitis B Vaccination in High Risk Groups
 NHS FORTH VALLEY Guidelines for Hepatitis B Vaccination in High Risk Groups Approved 01/04/2012 Version 1.0 Date of First Issue 01/04/2012 Review Date 01/02/2014 Date of Issue 01/04/2012 EQIA Yes Author
NHS FORTH VALLEY Guidelines for Hepatitis B Vaccination in High Risk Groups Approved 01/04/2012 Version 1.0 Date of First Issue 01/04/2012 Review Date 01/02/2014 Date of Issue 01/04/2012 EQIA Yes Author
From the street to the NICU. Richard Christensen, PA, CAS
 From the street to the NICU Richard Christensen, PA, CAS Treatment works Truths Disconnect with pregnant women seeking treatment Disconnect between community and science Medication is not a stand-alone
From the street to the NICU Richard Christensen, PA, CAS Treatment works Truths Disconnect with pregnant women seeking treatment Disconnect between community and science Medication is not a stand-alone
3/31/2015. Objectives. Alcohol. Long term effects. Substance abuse increases the risk of: Substance Abuse in Pregnancy
 Objectives Substance Abuse in Pregnancy Basics of screening and counseling Minako Watabe, MD Obstetrics and Gynecology Ventura County Medical Center 1) Discuss the risks of alcohol, tobacco, and drug use
Objectives Substance Abuse in Pregnancy Basics of screening and counseling Minako Watabe, MD Obstetrics and Gynecology Ventura County Medical Center 1) Discuss the risks of alcohol, tobacco, and drug use
Substitution Therapy for Opioid Dependence The Role of Suboxone. Mandy Manak, MD, ABAM, CCSAM Methadone 101-Hospitalist Workshop, October 3, 2015
 Substitution Therapy for Opioid Dependence The Role of Suboxone Mandy Manak, MD, ABAM, CCSAM Methadone 101-Hospitalist Workshop, October 3, 2015 Objectives Recognize the options available in treating opioid
Substitution Therapy for Opioid Dependence The Role of Suboxone Mandy Manak, MD, ABAM, CCSAM Methadone 101-Hospitalist Workshop, October 3, 2015 Objectives Recognize the options available in treating opioid
Heroin. How Is Heroin Abused? How Does Heroin Affect the Brain? What Other Adverse Effects Does Heroin Have on Health?
 Heroin Heroin is an opiate drug that is synthesized from morphine, a naturally occurring substance extracted from the seed pod of the Asian opium poppy plant. Heroin usually appears as a white or brown
Heroin Heroin is an opiate drug that is synthesized from morphine, a naturally occurring substance extracted from the seed pod of the Asian opium poppy plant. Heroin usually appears as a white or brown
Alcohol and drugs Be proactive
 Alcohol and drugs Be proactive PREGNANCY: a critical time to take care of yourself and your future baby Pregnant women must often change certain daily habits and are bombarded with recommendations from
Alcohol and drugs Be proactive PREGNANCY: a critical time to take care of yourself and your future baby Pregnant women must often change certain daily habits and are bombarded with recommendations from
Magee-Womens Hospital
 Magee-Womens Hospital Magee Pregnancy Recovery Program: History Pregnancy Recovery Center A Medical Home Model Approach to Strengthen Families Bawn Maguire, MSN, RN Programmatic Nurse Specialist Stephanie
Magee-Womens Hospital Magee Pregnancy Recovery Program: History Pregnancy Recovery Center A Medical Home Model Approach to Strengthen Families Bawn Maguire, MSN, RN Programmatic Nurse Specialist Stephanie
MEDICATION GUIDE. What is Morphine Sulfate Oral Solution?
 MEDICATION GUIDE Morphine Sulfate (mor-pheen) (CII) Oral Solution IMPORTANT: Keep Morphine Sulfate Oral Solution in a safe place away from children. Accidental use by a child is a medical emergency and
MEDICATION GUIDE Morphine Sulfate (mor-pheen) (CII) Oral Solution IMPORTANT: Keep Morphine Sulfate Oral Solution in a safe place away from children. Accidental use by a child is a medical emergency and
March of Dimes. FAQ on Drug Use and Pregnancy. November 2006. <http://www.marchofdimes.com/14332_1169.asp>. [accessed February 2010]
![March of Dimes. FAQ on Drug Use and Pregnancy. November 2006. <http://www.marchofdimes.com/14332_1169.asp>. [accessed February 2010]](/thumbs/27/11703693.jpg "March of Dimes. FAQ on Drug Use and Pregnancy. November 2006. <http://www.marchofdimes.com/14332_1169.asp>. [accessed February 2010]") March of Dimes. FAQ on Drug Use and Pregnancy. November 2006. . [accessed February 2010] After delivery, babies who were exposed to amphetamines before birth
March of Dimes. FAQ on Drug Use and Pregnancy. November 2006. . [accessed February 2010] After delivery, babies who were exposed to amphetamines before birth
Naltrexone Shared Care Guideline for the treatment of alcohol dependence and opioid dependance
 Naltrexone Shared Care Guideline for the treatment of alcohol dependence and opioid dependance Introduction Indication/Licensing information: Naltrexone is licensed for use as an additional therapy, within
Naltrexone Shared Care Guideline for the treatment of alcohol dependence and opioid dependance Introduction Indication/Licensing information: Naltrexone is licensed for use as an additional therapy, within
Opiate treatment for opiate withdrawal in newborn infants (Review)
") (Review) Osborn DA, Jeffery HE, Cole MJ This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library 2010, Issue 10 http://www.thecochranelibrary.com
(Review) Osborn DA, Jeffery HE, Cole MJ This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library 2010, Issue 10 http://www.thecochranelibrary.com
Neonatal Abstinence Syndrome Anthony E. Burgos and Bryan L. Burke, Jr. DOI: 10.1542/neo.10-5-e222
 Neonatal Abstinence Syndrome Anthony E. Burgos and Bryan L. Burke, Jr NeoReviews 2009;10;e222-e229 DOI: 10.1542/neo.10-5-e222 The online version of this article, along with updated information and services,
Neonatal Abstinence Syndrome Anthony E. Burgos and Bryan L. Burke, Jr NeoReviews 2009;10;e222-e229 DOI: 10.1542/neo.10-5-e222 The online version of this article, along with updated information and services,
Collaborative Care for Pregnant Women with Substance Use Disorders
 Collaborative Care for Pregnant Women with Substance Use Disorders Alane O Connor DNP Maine Dartmouth Family Medicine Residency MaineGeneral Medical Center Dartmouth Medical School Vanderbilt University
Collaborative Care for Pregnant Women with Substance Use Disorders Alane O Connor DNP Maine Dartmouth Family Medicine Residency MaineGeneral Medical Center Dartmouth Medical School Vanderbilt University
Could you care for a baby withdrawing from drugs and/or alcohol? Family Futures Practice Paper Series
 Could you care for a baby withdrawing from drugs and/or alcohol? Family Futures Practice Paper Series To promote the attachment that is vital for their healthy development a drug or alcohol addicted baby
Could you care for a baby withdrawing from drugs and/or alcohol? Family Futures Practice Paper Series To promote the attachment that is vital for their healthy development a drug or alcohol addicted baby
Neonatal Drug Withdrawal. John Wareham, MD Department of Neonatology, St. Vincent Women s Hospital
 Neonatal Drug Withdrawal John Wareham, MD Department of Neonatology, St. Vincent Women s Hospital Neonatal Drug Withdrawal What are we going to cover? Overview of the problem in neonates Opioid exposure/dependence
Neonatal Drug Withdrawal John Wareham, MD Department of Neonatology, St. Vincent Women s Hospital Neonatal Drug Withdrawal What are we going to cover? Overview of the problem in neonates Opioid exposure/dependence
for Management Guidelines Infants with Neonatal Abstinence Syndrome BACKGROUND DIFFERENTIAL DIAGNOSIS
 Management Guidelines for Infants with Neonatal Abstinence Syndrome BACKGROUND Neonatal drug withdrawal can occur when newborn infants are exposed to medications or addictive substances in-utero, or can
Management Guidelines for Infants with Neonatal Abstinence Syndrome BACKGROUND Neonatal drug withdrawal can occur when newborn infants are exposed to medications or addictive substances in-utero, or can
The Federation of State Medical Boards 2013 Model Guidelines for Opioid Addiction Treatment in the Medical Office
 The Federation of State Medical Boards 2013 Model Guidelines for Opioid Addiction Treatment in the Medical Office Adopted April 2013 for Consideration by State Medical Boards 2002 FSMB Model Guidelines
The Federation of State Medical Boards 2013 Model Guidelines for Opioid Addiction Treatment in the Medical Office Adopted April 2013 for Consideration by State Medical Boards 2002 FSMB Model Guidelines
A Guide for Hospitals and Health Care Providers Perinatal Substance Use: Promoting Healthy Outcomes
 A Guide for Hospitals and Health Care Providers Perinatal Substance Use: Promoting Healthy Outcomes Virginia Legal Requirements and Health Care Practice Implications Perinatal Care To promote healthy maternal
A Guide for Hospitals and Health Care Providers Perinatal Substance Use: Promoting Healthy Outcomes Virginia Legal Requirements and Health Care Practice Implications Perinatal Care To promote healthy maternal
Perinatal Substance Use: Promoting Healthy Outcomes
 A Guide for Hospitals and Health Care Providers Perinatal Substance Use: Promoting Healthy Outcomes Virginia Legal Requirements and Health Care Practice Implications Perinatal Care To promote healthy maternal
A Guide for Hospitals and Health Care Providers Perinatal Substance Use: Promoting Healthy Outcomes Virginia Legal Requirements and Health Care Practice Implications Perinatal Care To promote healthy maternal
Review of Pharmacological Pain Management
 Review of Pharmacological Pain Management CHAMP Activities are possible with generous support from The Atlantic Philanthropies and The John A. Hartford Foundation The WHO Pain Ladder The World Health Organization
Review of Pharmacological Pain Management CHAMP Activities are possible with generous support from The Atlantic Philanthropies and The John A. Hartford Foundation The WHO Pain Ladder The World Health Organization
GUIDELINE FOR ADMINISTRATION OF FENTANYL FOR PAIN RELIEF IN LABOUR
 GUIDELINE FOR ADMINISTRATION OF FENTANYL FOR PAIN RELIEF IN LABOUR INTRODUCTION Intravenous (IV) Fentanyl is a good option for pain management during labour and should be administered in a safe and competent
GUIDELINE FOR ADMINISTRATION OF FENTANYL FOR PAIN RELIEF IN LABOUR INTRODUCTION Intravenous (IV) Fentanyl is a good option for pain management during labour and should be administered in a safe and competent
Heroin. How Is Heroin Abused? How Does Heroin Affect the Brain? What Other Adverse Effects Does Heroin Have on Health?
 Heroin Heroin is an opiate drug that is synthesized from morphine, a naturally occurring substance extracted from the seed pod of the Asian opium poppy plant. Heroin usually appears as a white or brown
Heroin Heroin is an opiate drug that is synthesized from morphine, a naturally occurring substance extracted from the seed pod of the Asian opium poppy plant. Heroin usually appears as a white or brown
UNIT VIII NARCOTIC ANALGESIA
 UNIT VIII NARCOTIC ANALGESIA Objective Review the definitions of Analgesic, Narcotic and Antagonistic. List characteristics of Opioid analgesics in terms of mechanism of action, indications for use and
UNIT VIII NARCOTIC ANALGESIA Objective Review the definitions of Analgesic, Narcotic and Antagonistic. List characteristics of Opioid analgesics in terms of mechanism of action, indications for use and
SUPPORT OF BREASTFEEDING FAMILIES IN NICU THE WOMEN S HOSPITAL AT JACKSON MEMORIAL
 SUPPORT OF BREASTFEEDING FAMILIES IN NICU THE WOMEN S HOSPITAL AT JACKSON MEMORIAL OBJECTIVES To verbalize the benefits of breast milk for preterm and critical ill infants To recognize how to assist mother
SUPPORT OF BREASTFEEDING FAMILIES IN NICU THE WOMEN S HOSPITAL AT JACKSON MEMORIAL OBJECTIVES To verbalize the benefits of breast milk for preterm and critical ill infants To recognize how to assist mother
Heroin. How is Heroin Abused? What Other Adverse Effects Does Heroin Have on Health? How Does Heroin Affect the Brain?
 Heroin Heroin is a synthetic opiate drug that is highly addictive. It is made from morphine, a naturally occurring substance extracted from the seed pod of the Asian opium poppy plant. Heroin usually appears
Heroin Heroin is a synthetic opiate drug that is highly addictive. It is made from morphine, a naturally occurring substance extracted from the seed pod of the Asian opium poppy plant. Heroin usually appears
Presentation to Senate Health and Human Services Committee: Prescription Drug Abuse in Texas
 Presentation to Senate Health and Human Services Committee: Prescription Drug Abuse in Texas David Lakey, MD Commissioner, Department of State Health Services Lauren Lacefield Lewis Assistant Commissioner,
Presentation to Senate Health and Human Services Committee: Prescription Drug Abuse in Texas David Lakey, MD Commissioner, Department of State Health Services Lauren Lacefield Lewis Assistant Commissioner,
Remove this cover sheet before redistributing and replace it with your own. Please ensure that DPHHS is included on your HAN distribution list.
 State of Montana Health Alert Network DPHHS HAN ADVISORY Cover Sheet DATE: May 15, 2012 SUBJECT: Pertussis INSTRUCTIONS: DISTRIBUTE to your local HAN contacts. This HAN is intended for general sharing
State of Montana Health Alert Network DPHHS HAN ADVISORY Cover Sheet DATE: May 15, 2012 SUBJECT: Pertussis INSTRUCTIONS: DISTRIBUTE to your local HAN contacts. This HAN is intended for general sharing
INTOXICATED PATIENTS AND DETOXIFICATION
 VAMC Detoxification Decision Tree Updated May 2006 INTOXICATED PATIENTS AND DETOXIFICATION Patients often present for evaluation of substance use and possible detoxification. There are certain decisions
VAMC Detoxification Decision Tree Updated May 2006 INTOXICATED PATIENTS AND DETOXIFICATION Patients often present for evaluation of substance use and possible detoxification. There are certain decisions
Abstral Prescriber and Pharmacist Guide
 Abstral Prescriber and Pharmacist Guide fentanyl citrate sublingual tablets Introduction The Abstral Prescriber and Pharmacist Guide is designed to support healthcare professionals in the diagnosis of
Abstral Prescriber and Pharmacist Guide fentanyl citrate sublingual tablets Introduction The Abstral Prescriber and Pharmacist Guide is designed to support healthcare professionals in the diagnosis of
KAP Keys. For Physicians. Based on TIP 40 Clinical Guidelines for the Use of Buprenorphine in the Treatment. of Opioid Addiction
 Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction Knowledge Application Program KAP Keys For Physicians Based on TIP 40 Clinical Guidelines for the Use of Buprenorphine
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction Knowledge Application Program KAP Keys For Physicians Based on TIP 40 Clinical Guidelines for the Use of Buprenorphine
Standard of Care: Neonatal Intensive Care Unit (NICU) Physical and Occupational Therapy Management of the high risk infant.
 Physical and Occupational Therapy Management of the high risk infant.") BRIGHAM & WOMEN S HOSPITAL Department of Rehabilitation Services Standard of Care: Neonatal Intensive Care Unit (NICU) Case Type / Diagnosis: The high-risk infant is defined as the baby with any event
BRIGHAM & WOMEN S HOSPITAL Department of Rehabilitation Services Standard of Care: Neonatal Intensive Care Unit (NICU) Case Type / Diagnosis: The high-risk infant is defined as the baby with any event
Identifying and Managing Substance Use During Pregnancy
 Identifying and Managing Substance Use During Pregnancy Joseph B. Landwehr, Jr., MD Director, Perinatal Center IU Health Ball Memorial Hospital OBJECTIVES Overview of illicit drug use in pregnant women
Identifying and Managing Substance Use During Pregnancy Joseph B. Landwehr, Jr., MD Director, Perinatal Center IU Health Ball Memorial Hospital OBJECTIVES Overview of illicit drug use in pregnant women
Opioid Treatment Services, Office-Based Opioid Treatment
 Optum 1 By United Behavioral Health U.S. Behavioral Health Plan, California Doing Business as OptumHealth Behavioral Solutions of California ( OHBS-CA ) 2015 Level of Care Guidelines Opioid Treatment Services,
Optum 1 By United Behavioral Health U.S. Behavioral Health Plan, California Doing Business as OptumHealth Behavioral Solutions of California ( OHBS-CA ) 2015 Level of Care Guidelines Opioid Treatment Services,
Adjunctive psychosocial intervention. Conditions requiring dose reduction. Immediate, peak plasma concentration is reached within 1 hour.
 Shared Care Guideline for Prescription and monitoring of Naltrexone Hydrochloride in alcohol dependence Author(s)/Originator(s): (please state author name and department) Dr Daly - Consultant Psychiatrist,
Shared Care Guideline for Prescription and monitoring of Naltrexone Hydrochloride in alcohol dependence Author(s)/Originator(s): (please state author name and department) Dr Daly - Consultant Psychiatrist,
Triage, Assessment & Treatment Methadone 101/Hospitalist Workshop
 Triage, Assessment & Treatment Methadone 101/Hospitalist Workshop Launette Rieb, MSc, MD, CCFP, FCFP Clinical Associate Professor, Dept. Family Practice UBC American Board of Addiction Medicine Certified
Triage, Assessment & Treatment Methadone 101/Hospitalist Workshop Launette Rieb, MSc, MD, CCFP, FCFP Clinical Associate Professor, Dept. Family Practice UBC American Board of Addiction Medicine Certified
PRENATAL DRUG USE AND NEWBORN HEALTH. Federal Efforts Need Better Planning and Coordination
 United States Government Accountability Office Report to Congressional Requesters February 2015 PRENATAL DRUG USE AND NEWBORN HEALTH Federal Efforts Need Better Planning and Coordination GAO-15-203 Highlights
United States Government Accountability Office Report to Congressional Requesters February 2015 PRENATAL DRUG USE AND NEWBORN HEALTH Federal Efforts Need Better Planning and Coordination GAO-15-203 Highlights
Discontinuation: Involuntary Discharge
 Discontinuation: Involuntary Discharge TYPICALLY A PROCESS NOT AN EVENT Objectives 2 Review indications for discharge. Develop a therapeutic approach, in the context of the nature of Substance Use Disorders.
Discontinuation: Involuntary Discharge TYPICALLY A PROCESS NOT AN EVENT Objectives 2 Review indications for discharge. Develop a therapeutic approach, in the context of the nature of Substance Use Disorders.
3/27/2013. Treating Women for Opioid Dependence during Pregnancy and the Postpartum Period: Objectives. Disclosures. Hendrée E.
 1 Treating Women for Opioid Dependence during Pregnancy and the Postpartum Period: The Importance of Science and Clinical Care Informing Each Other Hendrée E. Jones, PhD Director, Horizons Program Visiting
1 Treating Women for Opioid Dependence during Pregnancy and the Postpartum Period: The Importance of Science and Clinical Care Informing Each Other Hendrée E. Jones, PhD Director, Horizons Program Visiting
Obstetrical Emergencies
 Date: July 18, 2014 Page 1 of 5 Obstetrical Emergencies Purpose: To provide the process for the assessment and management of the patient with an obstetrical related emergency. Pre-Medical Control 1. Follow
Date: July 18, 2014 Page 1 of 5 Obstetrical Emergencies Purpose: To provide the process for the assessment and management of the patient with an obstetrical related emergency. Pre-Medical Control 1. Follow
SUBSTANCE USE DISORDER SOCIAL DETOXIFICATION SERVICES [ASAM LEVEL III.2-D]
![SUBSTANCE USE DISORDER SOCIAL DETOXIFICATION SERVICES [ASAM LEVEL III.2-D]](/thumbs/27/9667060.jpg "SUBSTANCE USE DISORDER SOCIAL DETOXIFICATION SERVICES [ASAM LEVEL III.2-D]") SUBSTANCE USE DISORDER SOCIAL DETOXIFICATION SERVICES [ASAM LEVEL III.2-D] I. Definitions: Detoxification is the process of interrupting the momentum of compulsive drug and/or alcohol use in an individual
SUBSTANCE USE DISORDER SOCIAL DETOXIFICATION SERVICES [ASAM LEVEL III.2-D] I. Definitions: Detoxification is the process of interrupting the momentum of compulsive drug and/or alcohol use in an individual