PATIENT /GUARDIAN SIGNATURE
|
|
|
- Regina Brown
- 8 years ago
- Views:
Transcription
1 PATIENT INFORMATION ADDRESS: First Name: Last Name: Middle Initial: Date: / / Address: City: State: Zip: Birth date: / / Age: Male Female S.S. #: - - Home Phone: ( ) - Alternative Phone (Cell, Pager): ( ) - Spouse: Chose Clinic Because/ Referred to Clinic By Dr.: Insurance Plan Family Friend Former Patient Close to Work/Home Website Yellow Pages Street Sign Other: WORK INFORMATION Employer: Work Phone ( ) - Ext. Occupation: Employment Status Full Time Part Time Retired Not Employed CARE PROVIDER INFORMATION Referring Dr: Referring Dr. Phone: ( ) - Regular Dr./PCP Regular Dr./PCP Phone: ( ) - INSURANCE INFORMATION ( PLEASE GIVE YOUR INSURANCE CARD TO THE RECEPTIONIST ) Primary Insurance Name: Subscriber s Name (If different): Birth date : / / ID. #: Group/Policy # Patient s Relationship to Subscriber: Self Spouse Child Other: Name of Secondary Insurance: Subscriber s Name: Birth date : / / ID. #: Group/Policy # Patient s Relationship to Subscriber: Self Spouse Child Other: AUTO OR WORK INJURY CLAIM ( PLEASE PROVIDE YOUR INSURANCE INFORMATION FOR BACKUP ) Insurance Name: Auto : Labor & Industries: Adjuster/Claim Manager: Phone: Ext.: Address: City State: Zip: Claim #: Accident Date: / / Cause: ATTORNEY INFORMATION Name: Law Firm: Phone: ( ) - Address City State: Zip: IN CASE OF EMERGENCY Name of Local Friend or Relative (Not Living at Same Address): Relationship to Patient: Home Phone: ( ) - Work Phone: ( ) - I authorize my insurance benefits be paid directly to Universal Physical Therapy, PC. I understand that I am financially responsible for any balance. I also authorize to release any information required to process my claims. PATIENT /GUARDIAN SIGNATURE DATE
 - INSURANCE INFORMATION ( PLEASE GIVE YOUR INSURANCE CARD TO THE RECEPTIONIST ) Primary Insurance Name: Subscriber s Name (If different): Birth date : / / ID.")
2 PAST MEDICAL HISTORY FORM Patient Name BLOOD PRESSURE YES NO JOINT CONDITIONS YES NO Hypertension Upper Extremity Low Blood Pressure Dislocation Normal Blood Pressure Lower Extremity Dislocation HEART DISEASE YES NO OTHER CONDITIONS YES NO Heart Attack Muscular Dystrophy Atherosclerotic Disease Rheumatoid Arthritis Myocardial Infarction Multiple Sclerosis Rheumatic Heart Disease Epilepsy Heart Murmur Gout Fibromyalgia MUSCLE CONDITION YES NO Diabetes Carpal Tunnel R/L Hearing Loss Tennis Elbow R/L Poor Eyesight Back/Neck Problems Fainting Limited Limb Movement Polio Other: LUNGS YES NO Asthma Emphysema Shortness of Breath EXERCISE WORK ACTIVITY STRESS LEVEL HABITS None Sitting Low Smoking Packs a Day 1-2 x Week Standing Medium Alcohol Drinks a Week 3-4 x Week Light Labor High Coffee/Soda Cups a Week 5+ x Week Heavy Labor What types of exercise do you perform? : What things cause stress in your life? : Are you taking any seizure medication? YES NO If yes list name: Are you taking any medications that might affect your lungs, heart, consciousness or general well-being while participating in therapy? YES NO If yes list name: List all medications you a currently taking: List all surgeries in the past two years (Including dates): Are you pregnant? YES NO What week?: Have you had any injuries related to work? YES NO If yes list body part and date.: Have you had any Auto Accidents YES NO If yes list body part and date.: Have you had Physical Therapy or Massage Therapy before? YES NO Where: Signature of Patient, Parent, Guardian, Personal Representative Date

3
4 NOTICE OF PATIENT INFORMATION PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED OR DISCLOSED HOW YOU CAN GET ACCESS TO INFORMATION. PLEASE REVIEW IT CAREFULLY. UNIVERSAL PHYSICAL THERAPY, PC S LEGAL DUTY UNIVERSAL PHYSICAL THERAPY, PC is required by law to protect the privacy of your personal health information, provide this notice about our information practices and follow the information practices that are described herein. USES AND DISCLOSURES OF HEALTH INFORMATION UNIVERSAL PHYSICAL THERAPY, PC uses your personal health information primarily for treatment; obtaining payment for treatment; conducting internal administrative activities and evaluating the quality of care that we provide. For example, we may use your personal health information to contact you to provide appointment reminders, or information about treatment alternatives or other health related benefits that could be of interest to you. UNIVERSAL PHYSICAL THERAPY, PC may also use or disclose your personal health information without prior authorization for emergencies, research studies, auditing purposes, and public heath/statistical purposes. We also provide information when required by law. In any other situation, our policy is to obtain your written authorization before disclosing your personal health information. If you provide us with a written authorization to release your information for any reason, you may later revoke that authorization to stop future disclosures at any time. UNIVERSAL PHYSICAL THERAPY, PC may change its policy at any time. When changes are made, a new Notice of Information Practices will be posted in the waiting room and patient exam areas and will be provided to you on your next visit. You may also request an updated copy of our Notice of Information Practices at any time. PATIENT S INDIVIDUAL RIGHTS You have the right to review or obtain a copy of your personal health information at any time. You have the right to request that we correct any inaccurate or incomplete information in your records. You also have the right to request a list of instances where we have disclosed your personal health information for reasons other than treatment, payment or other related administrative purposes. You may also request in writing that we not use or disclose your personal health information for treatment, payment and administrative purposes except when specifically authorized by you, when required by law or in emergency circumstances. UNIVERSAL PHYSICAL THERAPY, PC will consider all such requests on a case-by-case basis, but the practice is not legally required to accept them. CONCERNS AND COMPLAINTS If you are concerned that we may have violated your privacy rights or if you disagree with any decisions we have made regarding access or disclosure of your personal health information, please contact our Privacy Officer at the address listed below. You may also send a written complaint to the US Department of Health and Human Services. For further information on our health information practices or if you have a complaint, please contact the following person: UNIVERSAL PHYSICAL THERAPY, PC Attn: Privacy Officer 3250 WESTCHESTER AVE BRONX, NY 10461

5 PATIENT INFORMATION CONSENT FORM I have read and fully understand UNIVERSAL PHYSICAL THERAPY, PC s Notice of Information Practices. I understand that UNIVERSAL PHYSICAL THERAPY, PC may use or disclose my personal health information for the purposes of carrying out treatment, obtaining payment, evaluating the quality of services provided and any administrative operations related to treatment or payment. I understand that I have the right to restrict how my personal health information is used and disclosed for treatment, payment and administrative operations if I notify the practice. I also understand that UNIVERSAL PHYSICAL THERAPY, PC will consider requests for restriction on a case-by-case basis, but does not have to agree to requests for restrictions. I hereby consent to the use and disclosure of my personal health information for purposes as noted in UNIVERSAL PHYSICAL THERAPY, PC s Notice of Information practices. I understand that I retain the right to revoke this consent by notifying the practice in writing at any time. Patient Name Signature Date I also authorize UNIVERSAL PHYSICAL THERAPY, PC to use my protected health information for targeted marketing, fund raising, and/or solicitation of participation in research studies. I understand I have the right to copy or inspect any information used for these purposes. I also understand this authorization does not affect my consent to use my protected health information for treatment, billing, or operations related to treatment and billing. Patient Name Signature Date

6 OFFICE PAYMENT POLICY - UNIVERSAL PHYSICAL THERAPY, PC It is the policy of UNIVERSAL PHYSICAL THERAPY, PC, Inc, to collect any moneys due for all applicable deductible, coinsurance, co-pay's and/or self payments on the date services are rendered as indicated as due and payable by the patient's insurance company (if applicable). A receipt will be given for the collection of moneys received in the facility. It is also the policy of UNIVERSAL PHYSICAL THERAPY, PC, Inc. to assure that all fiscal obligations are satisfactory for the patient and that every effort is made to assure the patient receives the scheduled care without regard to fiscal obligations. Our physical therapy charges are based on the procedures and modalities used and the length of your treatment. Treatments are usually 30, 45 or 60 minutes long. If you are covered by health insurance with physical therapy benefits, we will be happy to bill your insurance. Please provide your insurance information to the office manager and we will verify your coverage as a courtesy. Although we are contracted with most insurance carriers, our services may not be covered by your particular insurance plan. Being referred to our clinic by a physician does not necessarily guarantee that your insurance will cover our services. Please remember that you are 100% responsible for all charges incurred: your physician s referral and our verification of your insurance benefits are not a guarantee of payment. Therefore, we highly recommend you also contact your insurance carrier and check into your coverage for physical therapy. Do not assume that you will not owe anything if you have more than one insurance policy. If you need special arrangements to be made, please discuss this with the office manger before starting your treatments. Please initial your payment method and sign below that you have read, understand, and agree with all of the information on this page: 1. PRIVATE HEALTH INSURANCE (PPO): Some insurance plans require authorization or a referral from your primary physician. Most insurance plans have a patient responsibility of a deductible (amount paid by the patient before the insurance policy begins payment for services) and either a copay (a set dollar amount per visit) or coinsurance (a percent of the allowed charges). Deductibles and copays are due at the time of service. We will bill you for coinsurance or other payment due after we have been paid by your insurance or notified of their denial for payment. 2. HMO Insurance: Authorization from your insurance must be obtained prior to treatment. Any copay or coinsurance is due at the time of treatment. If your HMO plan also has a Point of Service option you are using, please be sure you understand the difference in your Point of Service coverage verses your HMO coverage. 3. MEDICARE: UNIVERSAL PHYSICAL THERAPY, PC. is a certified Medicare provider. Medicare has an annual deductible of $ for PT and Speech and a service cap of $1740. Medi-Gap insurance may cover the patient portion due until your Medicare benefits are exhausted. Some insurance plans that are secondary to Medicare cover the patient portion due and services after Medicare benefits are exhausted, but not always. Please verify all of your insurance benefits and be sure you understand your insurance coverage. 4. NO INSURANCE: If you do not have insurance and we do not have administrative costs for your services, you may be eligible for an administrative discount. Please notify the office staff that you do not have insurance so that a payment plan can be discussed. 5. OTHER: Please list the other type of payment: 6. WORKER S COMPENSATION CLAIMS: Authorization from your insurance adjuster is required before you can begin treatment. Please provide the office manager with the name and phone number of your adjuster, the date of your injury and your claim number, and any other pertinent information. 7. THIRD PARTY PAYERS AND AUTO LIENS: We will bill your insurance, however, third party payments will be sent to you for our services, not to us. You are responsible for payment of all service provided. Please be sure to contact this office when your case is settled to ensure your account has been paid. ATTENTION AUTO ACCIDENT VICTIMS AND WORKER S COMPENSATION INJURY PATIENTS: Please sign a release of information authorizing us to discuss your treatment with your attorney. If you retain an attorney during or after your course of treatment, please inform the office manager of this change. If you plan for your attorney to settle your account with us, you must sign a LIEN agreement. A statement of account will be sent to you or your attorney on a monthly basis until the account is paid. I have reviewed this office policies statement and discussed it with the clinical office manager. All my questions have been answered to my satisfaction and I understand all the information that has been explained to me. Signature: Date:

EZ REHAB SOLUTIONS: Patient Intake Information
 EZ REHAB SOLUTIONS: Patient Intake Information PATIENT INFORMATION EMAIL ADDRESS: First Name: Last Name: Middle Initial: : / / Address: City: State: Zip: Birth date: / / Age: Male Female S.S. #: - - Home
EZ REHAB SOLUTIONS: Patient Intake Information PATIENT INFORMATION EMAIL ADDRESS: First Name: Last Name: Middle Initial: : / / Address: City: State: Zip: Birth date: / / Age: Male Female S.S. #: - - Home
MONTESANO PHYSICAL THERAPY, INC. Patient Intake Information
 MONTESANO PHYSICAL THERAPY, INC. Patient Intake Information PATIENT INFORMATION EMAIL ADDRESS: First Name: Last Name: Middle Initial: : / / Address: City: State: Zip: Birth date: / / Age: Male Female S.S.
MONTESANO PHYSICAL THERAPY, INC. Patient Intake Information PATIENT INFORMATION EMAIL ADDRESS: First Name: Last Name: Middle Initial: : / / Address: City: State: Zip: Birth date: / / Age: Male Female S.S.
THINK PHYSICAL THERAPY PATIENT INFORMATION Please present your insurance card(s) for copying. Patient Name: Sex: Date of Birth: Age:
 for copying. Patient Name: Sex: Date of Birth: Age:") THINK PHYSICAL THERAPY PATIENT INFORMATION Please present your insurance card(s) for copying. Patient Name: Sex: Date of Birth: Age: Social Security Number: Employment Status: Marital Status: Emp Unemp
THINK PHYSICAL THERAPY PATIENT INFORMATION Please present your insurance card(s) for copying. Patient Name: Sex: Date of Birth: Age: Social Security Number: Employment Status: Marital Status: Emp Unemp
Employment Status Full Time Part Time Retired Not Employed Work Address: City: State: Zip:
 PATIENT INFORMATION First Name: Last Name: Middle Initial: Date: / / Address: City: State: Zip: Email: DOB: Male Female S.S. #: - - Home Phone: ( ) Mobile Phone: ( ) Work Phone: ( ) Employer: Occupation:
PATIENT INFORMATION First Name: Last Name: Middle Initial: Date: / / Address: City: State: Zip: Email: DOB: Male Female S.S. #: - - Home Phone: ( ) Mobile Phone: ( ) Work Phone: ( ) Employer: Occupation:
1455 West Fair, Marquette, MI 49855 Phone - 906.226.0574 // Fax - 1.888.347.1135 // info@mqtrehab.com
 To our valued patients, In order to speed up the registration process and begin your treatment as soon as possible, please complete the forms listed below and bring the proper documentation to your first
To our valued patients, In order to speed up the registration process and begin your treatment as soon as possible, please complete the forms listed below and bring the proper documentation to your first
REHAB XCEL, LLC. NEW PATIENT INFORMATION
 REHAB XCEL, LLC. NEW PATIENT INFORMATION DATE: NAME: LAST: FIRST: MID: MAIL ADDRESS: HOME PHONE: CELL PHONE: WORK PHONE: DATE OF BIRTH: SS# SEX: M OR F EMERGENCY CONTACT: PHONE: MARITAL STATUS: M OR S
REHAB XCEL, LLC. NEW PATIENT INFORMATION DATE: NAME: LAST: FIRST: MID: MAIL ADDRESS: HOME PHONE: CELL PHONE: WORK PHONE: DATE OF BIRTH: SS# SEX: M OR F EMERGENCY CONTACT: PHONE: MARITAL STATUS: M OR S
PATIENT /GUARDIAN SIGNATURE
 PATIENT INFORMATION EMAIL ADDRESS: First Name: Last Name: Middle Initial: Date: / / Address: City: State: Zip: Birth date: / / Age: Male Female S.S. #: - - Home Phone: ( ) - Alternative Phone (Cell, Pager):
PATIENT INFORMATION EMAIL ADDRESS: First Name: Last Name: Middle Initial: Date: / / Address: City: State: Zip: Birth date: / / Age: Male Female S.S. #: - - Home Phone: ( ) - Alternative Phone (Cell, Pager):
Orthopedic Initial Questionnaire
 Orthopedic Initial Questionnaire Name: Date: Height: Weight: In order to allow the therapist to have a better understanding of the nature of your injury and evaluate your condition fully, please complete
Orthopedic Initial Questionnaire Name: Date: Height: Weight: In order to allow the therapist to have a better understanding of the nature of your injury and evaluate your condition fully, please complete
Orthopedic Initial Questionnaire. Date: Weight:
 Orthopedic Initial Questionnaire Name: Height: Date: Weight: In order to allow the therapist to have a better understanding of the nature of your injury and evaluate your condition fully, please complete
Orthopedic Initial Questionnaire Name: Height: Date: Weight: In order to allow the therapist to have a better understanding of the nature of your injury and evaluate your condition fully, please complete
Medical History Questionnaire
 Medical History Questionnaire Name: Date: Allergies (including latex): List all medications that you are currently taking, either prescription or non- prescription. Please specify dosage and length of
Medical History Questionnaire Name: Date: Allergies (including latex): List all medications that you are currently taking, either prescription or non- prescription. Please specify dosage and length of
Body Region: Surgery Type: Date:,, Body Region: Surgery Type: Date:,, Body Region: Surgery Type: Date:,, Body Region: Surgery Type: Date:,,
 Medical History Existing or Relevant Previous Conditions Allergies Yes No Dizzy Spells Yes No MRSA Yes No Anemia Yes No Emphysema/Bronchitis Yes No Multiple Sclerosis Yes No Anxiety Yes No Fibromyalgia
Medical History Existing or Relevant Previous Conditions Allergies Yes No Dizzy Spells Yes No MRSA Yes No Anemia Yes No Emphysema/Bronchitis Yes No Multiple Sclerosis Yes No Anxiety Yes No Fibromyalgia
DATE OF BIRTH SOCIAL SECURITY (Last 4 digits): SEX: Male Female
: SEX: Male Female") PATIENT DATA SHEET PATIENT INFORMATION Please complete this form in its entirety prior to your first visit. Also, please bring your insurance information and/or cards to our office at your first visit.
PATIENT DATA SHEET PATIENT INFORMATION Please complete this form in its entirety prior to your first visit. Also, please bring your insurance information and/or cards to our office at your first visit.
REHAB RESOURCES, INC. CONSENT FOR TREATMENT ASSIGNMENT OF BENEFITS BILLING AUTHORZATION ADULT (18 years and over)
") CONSENT FOR TREATMENT ASSIGNMENT OF BENEFITS BILLING AUTHORZATION ADULT (18 years and over) Rehab Resources, Inc. is a certified agency that provides outpatient therapy services. Occupational, Physical,
CONSENT FOR TREATMENT ASSIGNMENT OF BENEFITS BILLING AUTHORZATION ADULT (18 years and over) Rehab Resources, Inc. is a certified agency that provides outpatient therapy services. Occupational, Physical,
HI *Home Phone: Alternate Phone: Driver License No.: Email Address: INSURANCE COVERAGE & SUBSCRIBER INFORMATION (person that has the insurance policy)
") HAWAII PHYSICAL THERAPY INC. -- PATIENT REGISTRATION FORM Please fill out this form to register as a patient of Hawaii Physical Therapy Inc. All fields with an asterisk (*) are REQUIRED. We cannot register
HAWAII PHYSICAL THERAPY INC. -- PATIENT REGISTRATION FORM Please fill out this form to register as a patient of Hawaii Physical Therapy Inc. All fields with an asterisk (*) are REQUIRED. We cannot register
Medicare Patient Information. Patient Name: SS#: - - Date of Birth: / / Sex: Female Male. City: State: Zip Code:
 Medicare Patient Information Patient Name: SS#: - - Date of Birth: / / Sex: Female Male Address: Street: City: State: Zip Code: Home Phone: ( ) - Work/Mobile Phone: ( ) - Please print your name as it Appears
Medicare Patient Information Patient Name: SS#: - - Date of Birth: / / Sex: Female Male Address: Street: City: State: Zip Code: Home Phone: ( ) - Work/Mobile Phone: ( ) - Please print your name as it Appears
Grey Physical Therapy and Sports Medicine Center
 Grey Physical Therapy and Sports Medicine Center 101 Phoenix Ave, 2D Body Made Better by Grey A Tradition of Caring Since 1984 Enfield, CT 06082 Ph (860) 741-2541 F (860) 745-5264 Patient Information First
Grey Physical Therapy and Sports Medicine Center 101 Phoenix Ave, 2D Body Made Better by Grey A Tradition of Caring Since 1984 Enfield, CT 06082 Ph (860) 741-2541 F (860) 745-5264 Patient Information First
PATIENT REGISTRATION
 PATIENT REGISTRATION NAME: HOME ADDRESS: CITY, STATE, & ZIP CODE: HOME PHONE: CELL: WORK: SOCIAL SECURITY NUMBER: SEX: MALE/FEMALE DATE OF BIRTH: AGE: EMERGENCY CONTACT: RELATIONSHIP: EMERGENCY CONTACT
PATIENT REGISTRATION NAME: HOME ADDRESS: CITY, STATE, & ZIP CODE: HOME PHONE: CELL: WORK: SOCIAL SECURITY NUMBER: SEX: MALE/FEMALE DATE OF BIRTH: AGE: EMERGENCY CONTACT: RELATIONSHIP: EMERGENCY CONTACT
Worker s Compensation Intake Form
 Worker s Compensation Intake Form Patient Information: Name Home Phone Address Work Phone Social Security No. Date of Birth Sex Male Female Height Weight lbs Occupation Marital Status Employer No of Children
Worker s Compensation Intake Form Patient Information: Name Home Phone Address Work Phone Social Security No. Date of Birth Sex Male Female Height Weight lbs Occupation Marital Status Employer No of Children
Jaworski Physical Therapy, Inc. Private Health Insurance. Worker s Compensation (complete the following)
") Jaworski Physical Therapy, Inc. Patient Name: Date: Private Health Insurance Name of Private Health Insurance: ID#: Group#: Cardholder Name: Cardholder Date of Birth: Relationship to Patient: Phone: Address
Jaworski Physical Therapy, Inc. Patient Name: Date: Private Health Insurance Name of Private Health Insurance: ID#: Group#: Cardholder Name: Cardholder Date of Birth: Relationship to Patient: Phone: Address
920 NE 112 th Avenue, Suite 103, Vancouver, WA 98648 Phone: 360-567-2002 Fax: 360-567-2005 www.timberlinept.com
 920 NE 112 th Avenue, Suite 103, Vancouver, WA 98648 Phone: 360-567-2002 Fax: 360-567-2005 www.timberlinept.com Thank you for selecting Timberline to be a part of your rehabilitation. Below we have condensed
920 NE 112 th Avenue, Suite 103, Vancouver, WA 98648 Phone: 360-567-2002 Fax: 360-567-2005 www.timberlinept.com Thank you for selecting Timberline to be a part of your rehabilitation. Below we have condensed
Joint Effort Rehab, LLC New Patient Forms
 Patient Information DEMOGRAPHICS Joint Effort Rehab, LLC First Name: MI: Last Name: Sex: M F Home Phone: Work Phone: Cell Phone: SSN: of Birth: Email: Referring Physician: Employer Name: Primary Insurance
Patient Information DEMOGRAPHICS Joint Effort Rehab, LLC First Name: MI: Last Name: Sex: M F Home Phone: Work Phone: Cell Phone: SSN: of Birth: Email: Referring Physician: Employer Name: Primary Insurance
LAST NAME FIRST MI AGE ADDRESS APT CITY STATE ZIP OCCUPATION EMPLOYER/SCHOOL WORK PH
 PLEASE PRINT PATIENT INFORMATION TODAY S DATE: LAST NAME FIRST MI AGE ADDRESS APT CITY STATE ZIP E-MAIL HOME CELL OCCUPATION EMPLOYER/SCHOOL WORK SOCIAL SECURITY NO SEX: M / F DATE OF BIRTH MARITAL STATUS:
PLEASE PRINT PATIENT INFORMATION TODAY S DATE: LAST NAME FIRST MI AGE ADDRESS APT CITY STATE ZIP E-MAIL HOME CELL OCCUPATION EMPLOYER/SCHOOL WORK SOCIAL SECURITY NO SEX: M / F DATE OF BIRTH MARITAL STATUS:
PATIENT INSURANCE AUTHORIZATION WORKSHEET
 PATIENT INSURANCE AUTHORIZATION WORKSHEET We accept all insurances that have in-network and out-of-network benefits. If you do not have insurance benefits for physical therapy, please call us at 858-457-3545
PATIENT INSURANCE AUTHORIZATION WORKSHEET We accept all insurances that have in-network and out-of-network benefits. If you do not have insurance benefits for physical therapy, please call us at 858-457-3545
Welcome to Tri-State Rehab Services
 Welcome to Tri-State Rehab Services Ashland Ironton Jackson Louisa New Boston Westmoreland Thank you for choosing our facility. To help us meet all your physical therapy needs, please fill out forms completely
Welcome to Tri-State Rehab Services Ashland Ironton Jackson Louisa New Boston Westmoreland Thank you for choosing our facility. To help us meet all your physical therapy needs, please fill out forms completely
Physical Therapy Services Medical History Form
 Physical Therapy Services Medical History Form Last Name First Name DOB Age Diagnosis: Physician: Check Yes or No. If yes, please explain in the space provided. Yes No Are you pregnant? Yes No Currently
Physical Therapy Services Medical History Form Last Name First Name DOB Age Diagnosis: Physician: Check Yes or No. If yes, please explain in the space provided. Yes No Are you pregnant? Yes No Currently
PACIFIC PHYSICAL THERAPY & SPORTS REHABILITATION HERMOSA BEACH
 PACIFIC PHYSICAL THERAPY & SPORTS REHABILITATION HERMOSA BEACH PATIENT INFORMATION Patient Name: Address: Telephone: E-mail address: Birthdate: SS#: Employer: Occupation: Home Cell Work Gender: Male Female
PACIFIC PHYSICAL THERAPY & SPORTS REHABILITATION HERMOSA BEACH PATIENT INFORMATION Patient Name: Address: Telephone: E-mail address: Birthdate: SS#: Employer: Occupation: Home Cell Work Gender: Male Female
PATIENT INFORMATION. Patient: S.S.# Address: D.O.B. Home Phone: Bus Phone: Male Female. Emergency contact: Relation to Patient: PH#
 Massage 258 West 91 st Street, Suite 1-B Physical THERAPY EXPERTS, PLLC WELCOME 212-875-8345 T PLEASE FILL IN FORM COMPLETELY TO AVOID INSURANCE PAYMENT DELAY! PATIENT INFORMATION Patient: S.S.# Address:
Massage 258 West 91 st Street, Suite 1-B Physical THERAPY EXPERTS, PLLC WELCOME 212-875-8345 T PLEASE FILL IN FORM COMPLETELY TO AVOID INSURANCE PAYMENT DELAY! PATIENT INFORMATION Patient: S.S.# Address:
Name Last) (First) ( (M.I.) Birth Date Social Security Age Sex: Home Address. City State Zip. Complaint/ Area to be treated Email Address
 (First) ( (M.I.) Birth Date Social Security Age Sex: Home Address. City State Zip. Complaint/ Area to be treated Email Address") PLEASE PRINT CLEARLY : NEW PATIENT FORM Name Last) (First) ( (M.I.) Birth Social Security Age Sex: M / F Home Address City State Zip Complaint/ Area to be treated Email Address Home Phone ( ) Drivers Lic
PLEASE PRINT CLEARLY : NEW PATIENT FORM Name Last) (First) ( (M.I.) Birth Social Security Age Sex: M / F Home Address City State Zip Complaint/ Area to be treated Email Address Home Phone ( ) Drivers Lic
MVA New Patient Paperwork
 Please Complete Entire Form MVA New Patient Paperwork Patient Name: M F Today s Date / / Address: Employer: _ City, State, Zip: Address: Home Phone: ( ) City, State, Zip: Cell Phone: ( ) Work Phone: (
Please Complete Entire Form MVA New Patient Paperwork Patient Name: M F Today s Date / / Address: Employer: _ City, State, Zip: Address: Home Phone: ( ) City, State, Zip: Cell Phone: ( ) Work Phone: (
Patient Information: In Case of Emergency: Physician: Insurance:
 For office use only: Start of Care: ICD-9 Codes: Patient Information: Name: Address: City: State: IL Zip: Patient of Birth: Policy Holders of Birth: of Injury or Onset of Symptoms: Home Phone: Work Phone:
For office use only: Start of Care: ICD-9 Codes: Patient Information: Name: Address: City: State: IL Zip: Patient of Birth: Policy Holders of Birth: of Injury or Onset of Symptoms: Home Phone: Work Phone:
Please fill out the new patient paperwork and bring it with you, along with a photo ID and health insurance or Medicare card.
 Dear Patient, Thank you for choosing San Antonio Center for Physical Therapy for your rehabilitation needs. We want your time with us to be a positive experience, one that leads you down a road of successful
Dear Patient, Thank you for choosing San Antonio Center for Physical Therapy for your rehabilitation needs. We want your time with us to be a positive experience, one that leads you down a road of successful
Atlantis Physical Therapy Associates
 Atlantis Physical Therapy Associates Date Called/Walk-In: Appointment Date: Time: PT/OT: Diagnosis/ICD9/Body Parts: Frequency & Duration: X Referring Doctor: Dr. Phone#: Fax: NPI: Addresss: Ins Type: (Circle
Atlantis Physical Therapy Associates Date Called/Walk-In: Appointment Date: Time: PT/OT: Diagnosis/ICD9/Body Parts: Frequency & Duration: X Referring Doctor: Dr. Phone#: Fax: NPI: Addresss: Ins Type: (Circle
HAND & ORTHOPEDIC PHYSICAL THERAPY ASSOCIATES, A NJ P.C.
 Consent for Care and Treatment I, the undersigned, do hereby agree and give my consent for HAND & ORTHOPEDIC PHYSICAL THERAPY ASSOCIATES, A NJ P.C., to provide Care and Treatment to considered necessary
Consent for Care and Treatment I, the undersigned, do hereby agree and give my consent for HAND & ORTHOPEDIC PHYSICAL THERAPY ASSOCIATES, A NJ P.C., to provide Care and Treatment to considered necessary
Welcome to North Texas Orthopaedic & Spine 955 Garden Park Dr. Ste. 200 Allen Texas 75013. Today s Date: How did you hear of our practice?
 Welcome to North Texas Orthopaedic & Spine 955 Garden Park Dr. Ste. 200 Allen Texas 75013 Name: First Middle Last Today s Date: How did you hear of our practice? Home Address: City: State: Zip: Home Phone:
Welcome to North Texas Orthopaedic & Spine 955 Garden Park Dr. Ste. 200 Allen Texas 75013 Name: First Middle Last Today s Date: How did you hear of our practice? Home Address: City: State: Zip: Home Phone:
MILLENNIUM PHYSICAL THERAPY & SPORTS MEDICINE
 A) PATIENT INTAKE/TREATMENT FORM 1) Patient Name: 2) Social Security #: 3) Home Phone number: ( ), Cell: ( ), Work: ( ) 4) Address: City, State, Zip Code 5) Gender: M F 6) Date of Birth (DOB): / / 7) Marital
A) PATIENT INTAKE/TREATMENT FORM 1) Patient Name: 2) Social Security #: 3) Home Phone number: ( ), Cell: ( ), Work: ( ) 4) Address: City, State, Zip Code 5) Gender: M F 6) Date of Birth (DOB): / / 7) Marital
11120 New Hampshire Ave., Suite 411 Silver Spring MD 20904 Office (301)754-0505 Fax (301)754-0509
754-0505 Fax (301)754-0509") PATIENT REGISTRATION FORM (PLEASE PRINT) PATIENT S LAST FIRST MIDDLE DATE OF BIRTH / / AGE: SEX: M F SOCIAL SECURITY # STREET ADDRESS APT # CITY STATE ZIP HOME CELL EMAIL MARITAL STATUS: SINGLE / MARRIED
PATIENT REGISTRATION FORM (PLEASE PRINT) PATIENT S LAST FIRST MIDDLE DATE OF BIRTH / / AGE: SEX: M F SOCIAL SECURITY # STREET ADDRESS APT # CITY STATE ZIP HOME CELL EMAIL MARITAL STATUS: SINGLE / MARRIED
X Guarantor/Parent/Guardian Signature
 Patient Name: Last First Address City State Zip Phone# (C) (H) (W) Date of Birth Social Security# (REQUIRED FOR BILLING) If Patient is a Minor, a Parent s Name & Social Security# are Required Emergency
Patient Name: Last First Address City State Zip Phone# (C) (H) (W) Date of Birth Social Security# (REQUIRED FOR BILLING) If Patient is a Minor, a Parent s Name & Social Security# are Required Emergency
RIDGE PHYSICAL THERAPY & WELLNESS CENTER. Intake Form
 Intake Form : Personal Information please print clearly Name: last first middle initial Home Address: Home Telephone: ( ) Cell Phone: E-Mail Address: Social Security #: of Birth: Age: Sex: M F Marital
Intake Form : Personal Information please print clearly Name: last first middle initial Home Address: Home Telephone: ( ) Cell Phone: E-Mail Address: Social Security #: of Birth: Age: Sex: M F Marital
Next Level Physical Therapy PC Patient Information
 Next Level Physical Therapy PC Patient Information First Name M.I. Last Name Date of Birth SS# (if minor, leave blank) Student? F/T P/T NO Street Address Billing Address (if different) City State Zip Home
Next Level Physical Therapy PC Patient Information First Name M.I. Last Name Date of Birth SS# (if minor, leave blank) Student? F/T P/T NO Street Address Billing Address (if different) City State Zip Home
ST. LAWRENCE REHABILITATION CENTER OUTPATIENT POLICIES AND REGISTRATION INFORMATION
 Outpatient Services 2381 Lawrenceville Road 609-896-9500 voice Patient Name: Account #: ST. LAWRENCE REHABILITATION CENTER OUTPATIENT POLICIES AND REGISTRATION INFORMATION Your first day of outpatient
Outpatient Services 2381 Lawrenceville Road 609-896-9500 voice Patient Name: Account #: ST. LAWRENCE REHABILITATION CENTER OUTPATIENT POLICIES AND REGISTRATION INFORMATION Your first day of outpatient
PACIFIC PHYSICAL THERAPY 14650 Aviation Blvd., Suite 200 Manhattan Beach, CA 90250. Referring Doctor: PLEASE PRINT CLEARLY Email Address:
 PACIFIC PHYSICAL THERAPY 14650 Aviation Blvd., Suite 200 Manhattan Beach, CA 90250 Date: Referring Doctor: PLEASE PRINT CLEARLY First Name: Last Name: Height: Address: City, St., Zip:_ Email Address: _
PACIFIC PHYSICAL THERAPY 14650 Aviation Blvd., Suite 200 Manhattan Beach, CA 90250 Date: Referring Doctor: PLEASE PRINT CLEARLY First Name: Last Name: Height: Address: City, St., Zip:_ Email Address: _
Referring Physician: Type (Circle): Insurance Fitness Work/Comp Personal Injury Auto D/A:
: Insurance Fitness Work/Comp Personal Injury Auto D/A:") Patient Information Referred By: Referring Physician: Patient Name: Appointment Date: Time: Last First Middle Int. Date of Birth: SS#: Street Address: City/State/Zip: Phone Numbers: Home: Work: Cell: Email:
Patient Information Referred By: Referring Physician: Patient Name: Appointment Date: Time: Last First Middle Int. Date of Birth: SS#: Street Address: City/State/Zip: Phone Numbers: Home: Work: Cell: Email:
WELCOME TO AMOSKEAG CHIROPRACTIC, INC. SPINAL CORRECTIVE CARE FOR THE ENTIRE FAMILY ADULT. Full Name: What would you prefer to be called?
 Today s Date: / / WELCOME TO AMOSKEAG CHIROPRACTIC, INC. SPINAL CORRECTIVE CARE FOR THE ENTIRE FAMILY ADULT Full Name: What would you prefer to be called? Street Address (If P. O. Box, provide street address
Today s Date: / / WELCOME TO AMOSKEAG CHIROPRACTIC, INC. SPINAL CORRECTIVE CARE FOR THE ENTIRE FAMILY ADULT Full Name: What would you prefer to be called? Street Address (If P. O. Box, provide street address
Nephrology Associates New Patient Registration Forms
 Registration Information Authorization form: Last First Middle Address: City: State: Zip: DOB: / / - - Home # ( ) - - Cell # ( ) - - Email Address: Alternate Contact Information Phone Number Relationship
Registration Information Authorization form: Last First Middle Address: City: State: Zip: DOB: / / - - Home # ( ) - - Cell # ( ) - - Email Address: Alternate Contact Information Phone Number Relationship
PRO SPORTS THERAPY, INC. (P.S.T.)
") Dear Patient, Thank you for choosing Pro Sports Therapy. Enclosed is the paperwork that you will need to complete and bring with you for your physical therapy evaluation. Please arrive at least 15 minutes
Dear Patient, Thank you for choosing Pro Sports Therapy. Enclosed is the paperwork that you will need to complete and bring with you for your physical therapy evaluation. Please arrive at least 15 minutes
Patient Case Information (Please Fill Out Forms Completely) (IF PATIENT IS UNDER 18 YEARS OF AGE LEGAL GUARDIAN MUST SIGN ALL PAPERWORK)
 (IF PATIENT IS UNDER 18 YEARS OF AGE LEGAL GUARDIAN MUST SIGN ALL PAPERWORK)") Patient Name: Patient Case Information (Please Fill Out Forms Completely) (IF PATIENT IS UNDER 18 YEARS OF AGE LEGAL GUARDIAN MUST SIGN ALL PAPERWORK) (Last), (First) (Middle Initial) Address: City: State:
Patient Name: Patient Case Information (Please Fill Out Forms Completely) (IF PATIENT IS UNDER 18 YEARS OF AGE LEGAL GUARDIAN MUST SIGN ALL PAPERWORK) (Last), (First) (Middle Initial) Address: City: State:
EXCEL PHYSICAL THERAPY, INC.
 EXCEL PHYSICAL THERAPY, INC. Medical History Form Name: Date of Birth: Date: Are you employed? YES NO Right Handed Left Handed If NO, last day worked? Do you smoke? YES NO #of packs/day Occupation: Height:
EXCEL PHYSICAL THERAPY, INC. Medical History Form Name: Date of Birth: Date: Are you employed? YES NO Right Handed Left Handed If NO, last day worked? Do you smoke? YES NO #of packs/day Occupation: Height:
If you miss 3 consecutive appointments we may have to notify your physician and will require a new referral in order to continue your treatment.
 Welcome to POST Physical Therapy Brookline. We strive to provide our patients with excellent service and quality care. Our commitment to your well-being and health care is something that we at POST Physical
Welcome to POST Physical Therapy Brookline. We strive to provide our patients with excellent service and quality care. Our commitment to your well-being and health care is something that we at POST Physical
PATIENT INFORMATION - Please complete and/or verify all information and make changes as necessary.
 PATIENT INFORMATION - Please complete and/or verify all information and make changes as necessary. Today s : Are you here for an injury that is work-related? YES NO N/A Patient Name (First-Middle-Last)
PATIENT INFORMATION - Please complete and/or verify all information and make changes as necessary. Today s : Are you here for an injury that is work-related? YES NO N/A Patient Name (First-Middle-Last)
Hand & Orthopedic Physical Therapy Associates, P.C.
 Patient Name: Hand & Orthopedic Physical Therapy Associates, P.C. Date of Birth: ADVANCE BENEFICIARY NOTICE OF NONCOVERAGE (ABN) NOTE: If Medicare doesn t pay for items listed below, you may have to pay.
Patient Name: Hand & Orthopedic Physical Therapy Associates, P.C. Date of Birth: ADVANCE BENEFICIARY NOTICE OF NONCOVERAGE (ABN) NOTE: If Medicare doesn t pay for items listed below, you may have to pay.
RETINA CONSULTANTS OF HOUSTON. Date of Birth: Age: Sex: M F Martial Status: S M W D. Name of Spouse: Emergency Contact Name: Number:
 RETINA CONSULTANTS OF HOUSTON 6560 FANNIN, SUITE 750, HOUSTON TX 77030 PATIENT INFORMATION Patient's Legal Name: Date of Today's Visit: Social Security # Date of Birth: Age: Sex: M F Martial Status: S
RETINA CONSULTANTS OF HOUSTON 6560 FANNIN, SUITE 750, HOUSTON TX 77030 PATIENT INFORMATION Patient's Legal Name: Date of Today's Visit: Social Security # Date of Birth: Age: Sex: M F Martial Status: S
AON Physical Therapy & Wellness
 AON Physical Therapy & Wellness PATIENT REGISTRATION Patients First and Last Name Intake Taken By- Appointment Date / Therapist Date- Date of Birth: Is the patient Under 18? If so, who is the guarantor?
AON Physical Therapy & Wellness PATIENT REGISTRATION Patients First and Last Name Intake Taken By- Appointment Date / Therapist Date- Date of Birth: Is the patient Under 18? If so, who is the guarantor?
IN CASE OF EMERGENCY
 THE INFORMATION REQUESTED ON THIS FORM IS USED TO FILE MEDICAL CLAIMS AND FOR OTHER IMPORTANT MEDICAL DOCUMENTATION. PLEASE PRINT LEGIBLY SO THAT WE MAY ACCURATELY REFLECT YOUR PERSONAL INFORMATION IN
THE INFORMATION REQUESTED ON THIS FORM IS USED TO FILE MEDICAL CLAIMS AND FOR OTHER IMPORTANT MEDICAL DOCUMENTATION. PLEASE PRINT LEGIBLY SO THAT WE MAY ACCURATELY REFLECT YOUR PERSONAL INFORMATION IN
Made to Move Physical Therapy, Inc. 615 N Nash St., Ste # 306 El Segundo, CA 90245 310.535.0008
 Name Last First MI Date Current/Permanent address City State Zip Phone H W Cell Email Address: Marital Status Single Married Other Date of Birth: Age: Gender Male Female Spouses DOB: Employer Occupation
Name Last First MI Date Current/Permanent address City State Zip Phone H W Cell Email Address: Marital Status Single Married Other Date of Birth: Age: Gender Male Female Spouses DOB: Employer Occupation
PATIENT REGISTRATION Must complete entirely. Reason for today's visit: New Patient: Y N Existing Patient: Y N. Date of Birth: Age:
 Anthony N. Dardano, D.O., P.A., F.A.C.S. AESTHETIC AND RECONSTRUCTIVE PLASTIC SURGERY Diplomate of the American Board of Plastic Surgery Diplomate of the American Board of Surgery 951 N.W. 13 th Street,
Anthony N. Dardano, D.O., P.A., F.A.C.S. AESTHETIC AND RECONSTRUCTIVE PLASTIC SURGERY Diplomate of the American Board of Plastic Surgery Diplomate of the American Board of Surgery 951 N.W. 13 th Street,
CAMARILLO AQUATICS AND REHABILITATION SERVICES
 CAMARILLO AQUATICS AND REHABILITATION SERVICES Last Name First M.I. Address Apt.# City State Zip Code Phone # SS# Date of Birth Sex M F Driver s License # Marital Status: S M D W Spouse s Name How did
CAMARILLO AQUATICS AND REHABILITATION SERVICES Last Name First M.I. Address Apt.# City State Zip Code Phone # SS# Date of Birth Sex M F Driver s License # Marital Status: S M D W Spouse s Name How did
Dear Patient: Photo ID Insurance card(s) Prescription/referral for physical therapy Any Claim documentation (auto/w/c)
 Prescription/referral for physical therapy Any Claim documentation (auto/w/c)") 7500 Hanover Pkwy Ste. 103 Greenbelt, MD 20770 Phone: 301.446.1644 Fax: 301.446.1647 6510 Kenilworth Ave. Ste. 1100 Riverdale MD 20737 Phone: 240.770.8750 Fax: 240.770.8156 Dear Patient: Attached is your
7500 Hanover Pkwy Ste. 103 Greenbelt, MD 20770 Phone: 301.446.1644 Fax: 301.446.1647 6510 Kenilworth Ave. Ste. 1100 Riverdale MD 20737 Phone: 240.770.8750 Fax: 240.770.8156 Dear Patient: Attached is your
MVA/ PI Registration Form. Is this accident work related? YES or No If yes, stop here and notify front desk for different forms.
 MVA/ PI Registration Form Is this accident work related? YES or No If yes, stop here and notify front desk for different forms. Date: Patient # Patient Name: DOB; Gender: M or F SSN Address: City/State:
MVA/ PI Registration Form Is this accident work related? YES or No If yes, stop here and notify front desk for different forms. Date: Patient # Patient Name: DOB; Gender: M or F SSN Address: City/State:
Advantage Physical Therapy Patient Registration
 Appointment Date/Time: Therapist: Advantage Physical Therapy Patient Registration ****Please note ALL patients are required to have a prescription for Physical Therapy from a referring Physician prior
Appointment Date/Time: Therapist: Advantage Physical Therapy Patient Registration ****Please note ALL patients are required to have a prescription for Physical Therapy from a referring Physician prior
CONSENT FOR MEDICAL TREATMENT
 CONSENT FOR MEDICAL TREATMENT Patient Name DOB Date I, the patient or authorized representative, consent to any examination, evaluation and treatment regarding any illness, injury or other health concern
CONSENT FOR MEDICAL TREATMENT Patient Name DOB Date I, the patient or authorized representative, consent to any examination, evaluation and treatment regarding any illness, injury or other health concern
Welcome to Avida PT. The purpose of this letter is to provide you with some helpful information to prepare you for your visits to our facility.
 AVIDAPT 1391 Dublin Rd, Columbus, OH 43215 614-487-9715 avidapt.com Welcome to Avida PT. The purpose of this letter is to provide you with some helpful information to prepare you for your visits to our
AVIDAPT 1391 Dublin Rd, Columbus, OH 43215 614-487-9715 avidapt.com Welcome to Avida PT. The purpose of this letter is to provide you with some helpful information to prepare you for your visits to our
THANK YOU FOR CHOOSING QPT FOR YOUR PHYSICAL THERAPY NEEDS!
 THANK YOU FOR CHOOSING QPT FOR YOUR PHYSICAL THERAPY NEEDS! Please complete and sign all of the enclosed forms. Bring these forms, your physician s referral if required and any other documents required
THANK YOU FOR CHOOSING QPT FOR YOUR PHYSICAL THERAPY NEEDS! Please complete and sign all of the enclosed forms. Bring these forms, your physician s referral if required and any other documents required
P.S. Please remember to bring your completed forms to your office visit!
 Dear Patient: Please print the following forms and complete them as accurately as possible and bring them with you to your office visit. If you have any questions about the forms you can call my office
Dear Patient: Please print the following forms and complete them as accurately as possible and bring them with you to your office visit. If you have any questions about the forms you can call my office
Patient Registration Please Print Patient Name Last First Middle
 Patient Registration Please Print Patient Name Last First Middle Address City Zip Home Phone Work Ext Cell Birthdate - - Social Security # - - Gender Marital Status Employer Referred by_emergency Contact
Patient Registration Please Print Patient Name Last First Middle Address City Zip Home Phone Work Ext Cell Birthdate - - Social Security # - - Gender Marital Status Employer Referred by_emergency Contact
PATIENT INFORMATION EMERGENCY CONTACT LAST FIRST RELATIONSHIP REFERRAL SOURCE DOCTOR / REFERRING CLINICIAN: FAMILY MEMBER/FRIEND: INSURANCE:
 PATIENT INFORMATION LAST FIRST MI GENDER M F BIRTHDATE MO./ DAY/ YEAR SS# - - ADDRESS CITY ST ZIP PHONE (CELL) PHONE (HOME) EMAIL MARITAL STATUS EMPLOYER ADDRESS OCCUPATION WORK PHONE EXT WHO IS YOUR PRIMARY
PATIENT INFORMATION LAST FIRST MI GENDER M F BIRTHDATE MO./ DAY/ YEAR SS# - - ADDRESS CITY ST ZIP PHONE (CELL) PHONE (HOME) EMAIL MARITAL STATUS EMPLOYER ADDRESS OCCUPATION WORK PHONE EXT WHO IS YOUR PRIMARY
Welcome to Back Country Physical Therapy, Intake Form
 Welcome to Back Country Physical Therapy, Intake Form Patient Information: Name: Social Security #: Sex (Circle): M / F Address: City: State: Zip: Home Phone: Birth date: Age: Marital Status (Circle):
Welcome to Back Country Physical Therapy, Intake Form Patient Information: Name: Social Security #: Sex (Circle): M / F Address: City: State: Zip: Home Phone: Birth date: Age: Marital Status (Circle):
Patient Information. Date: Date of Birth: / / Name: Social Security: _- - Address: Street City State Zip
 Personal Insurance Intake Form Patient Information Date of Birth: / / Social Security: _- - Address: Street City State Zip Email Address: Home Phone: Sex: M or F Work Phone:. Cell Phone: Height: Weight:
Personal Insurance Intake Form Patient Information Date of Birth: / / Social Security: _- - Address: Street City State Zip Email Address: Home Phone: Sex: M or F Work Phone:. Cell Phone: Height: Weight:
Physical Occupational and Speech Therapy Patient Information Sheet
 Physical Occupational and Speech Therapy Patient Information Sheet FIRST NAME: MI: LAST NAME: ADDRESS: HOME PHONE: WORK PHONE: MALE FEMALE CELLPHONE: DOB: SS# EMERGENCY CONTACT: PHONE: RELATIONSHIP: PRIMARY
Physical Occupational and Speech Therapy Patient Information Sheet FIRST NAME: MI: LAST NAME: ADDRESS: HOME PHONE: WORK PHONE: MALE FEMALE CELLPHONE: DOB: SS# EMERGENCY CONTACT: PHONE: RELATIONSHIP: PRIMARY
Dymond Speech & Rehab., P.A. Patient Registration Information
 Dymond Speech & Rehab., P.A. Patient Registration Information Client s Name: First Middle Last Street Address: Mailing Address: City : State: Zip code: Sex: Marital Status: Home Phone: ( ) - Cell: ( )
Dymond Speech & Rehab., P.A. Patient Registration Information Client s Name: First Middle Last Street Address: Mailing Address: City : State: Zip code: Sex: Marital Status: Home Phone: ( ) - Cell: ( )
INTEGRATED PHYSICAL THERAPY a whole- istic approach to physical therapy
 Patient s Name: D.O.B.: Age: Address: City: State: _ Zip Code: Home Phone #: Cell #: _ Business #:_ Social Security Number: E- mail Address: Referring Physician? _ How do you hear about us: Dr. Referral
Patient s Name: D.O.B.: Age: Address: City: State: _ Zip Code: Home Phone #: Cell #: _ Business #:_ Social Security Number: E- mail Address: Referring Physician? _ How do you hear about us: Dr. Referral
4765 Carmel Mountain Rd. Ste 202, San Diego, CA 92130 Phone (848) 847-0055 Fax (858) 847-9944
 847-0055 Fax (858) 847-9944") 4765 Carmel Mountain Rd. Ste 202, San Diego, CA 92130 Phone (848) 847-0055 Fax (858) 847-9944 Dear Patient, Your insurance may pay your total bill for services rendered by Pilates People Torrey Hills.
4765 Carmel Mountain Rd. Ste 202, San Diego, CA 92130 Phone (848) 847-0055 Fax (858) 847-9944 Dear Patient, Your insurance may pay your total bill for services rendered by Pilates People Torrey Hills.
Wayne Physical Medicine & Rehabilitation Associates 401 Hamburg Turnpike, Suite 105 Wayne, NJ 07470
 PLEASE FILL OUT THIS SHEET COMPLETELY AND CORRECTLY. PLEASE PROVIDE ALL INSURANCE CARDS TO THE RECEPTIONIST TO COPY. Name Social Security # Address City, State & Zip Code Home Phone No. ( ) Cell Phone
PLEASE FILL OUT THIS SHEET COMPLETELY AND CORRECTLY. PLEASE PROVIDE ALL INSURANCE CARDS TO THE RECEPTIONIST TO COPY. Name Social Security # Address City, State & Zip Code Home Phone No. ( ) Cell Phone
IMS Allergy & Immunology New Patient Registration Sheet. Personal Information
 Personal Information Today s : Patient First Name: Initial: Last Name: DOB: Age: Social Security #: E-mail: Address: City: State: Zip: Home Phone: Work Phone: Cell Phone: Gender: M F Language: ENGLISH
Personal Information Today s : Patient First Name: Initial: Last Name: DOB: Age: Social Security #: E-mail: Address: City: State: Zip: Home Phone: Work Phone: Cell Phone: Gender: M F Language: ENGLISH
2015 Annual Patient Paperwork Update for Existing Patients
 2015 Annual Patient Paperwork Update for Existing Patients DATE: ͺͺͺͺ ŚĞĐŬ WƌĞĨĞƌƌĞĚ ůŝŷŝđ &ƚ tăljŷğ 'ƌğğŷǁžžě
2015 Annual Patient Paperwork Update for Existing Patients DATE: ͺͺͺͺ ŚĞĐŬ WƌĞĨĞƌƌĞĚ ůŝŷŝđ &ƚ tăljŷğ 'ƌğğŷǁžžě
ANA PAIN MANAGEMENT, P.C.
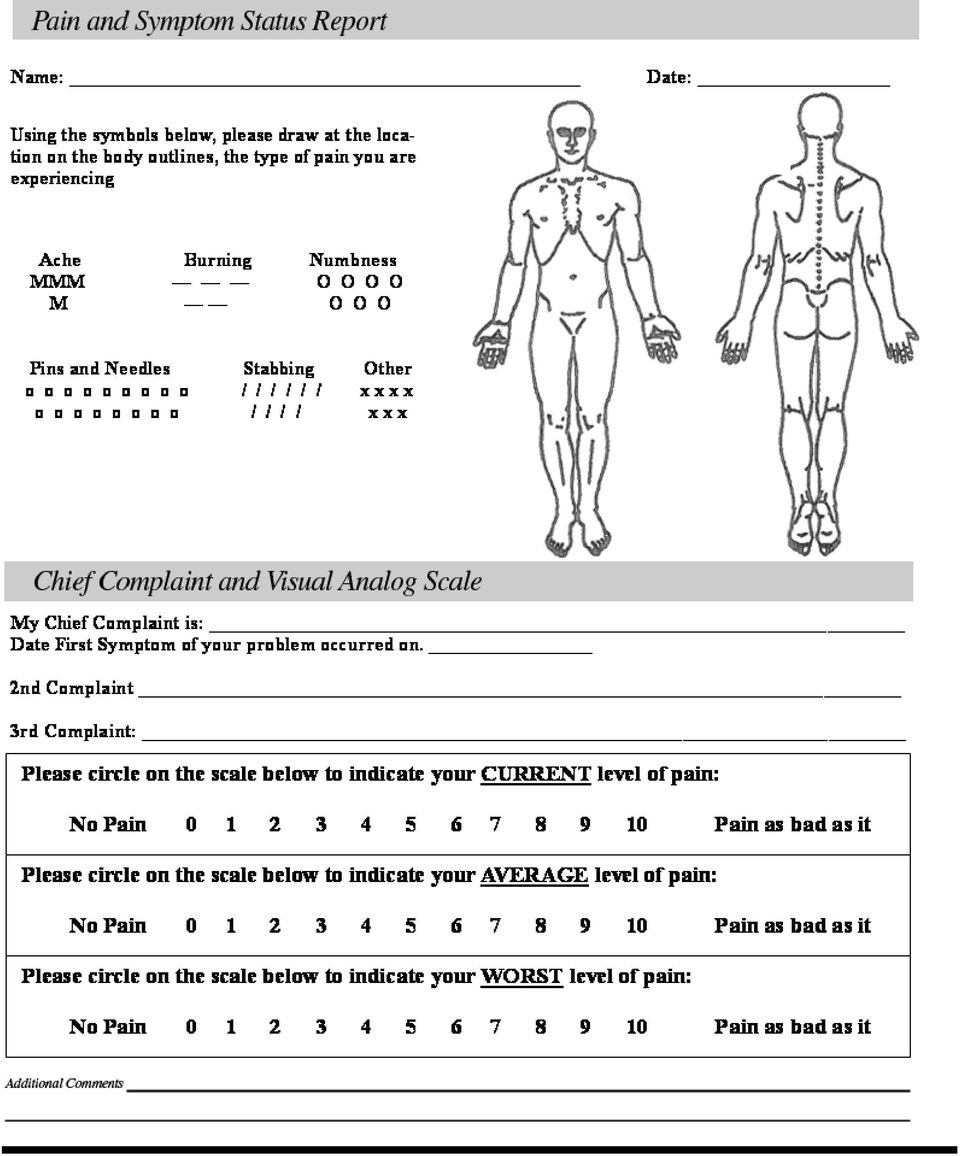
 Pain Assessment Patient s Name: Height: Weight: Where is the pain located? Mark with the appropriate letter: T= tingling N= numbness B= burning P= pain PLEASE COMPLETE PAIN LOCATION INFO BY HAND IN OFFICE
Pain Assessment Patient s Name: Height: Weight: Where is the pain located? Mark with the appropriate letter: T= tingling N= numbness B= burning P= pain PLEASE COMPLETE PAIN LOCATION INFO BY HAND IN OFFICE
Intake for Services. Birth date: Age: Gender: Name of Spouse: Years Married: Spouse's Age:
 Intake for Services Today's Date Last name: First name: Birth date: Age: Gender: Address: City/State/Zip Email: Home Phone: Cell phone: Marital Status: No. of Children & ages: If presently married: Name
Intake for Services Today's Date Last name: First name: Birth date: Age: Gender: Address: City/State/Zip Email: Home Phone: Cell phone: Marital Status: No. of Children & ages: If presently married: Name
Optimum Performance Physical Therapy, LLC
 Optimum Performance Physical Therapy, LLC Patient Information: Name: DOB: SS# Address: Phone: (H) (W) (C) Sex: Male Female Marital Status: M S D W Email: Employer Name/ Address: Referring Physician: (P)
Optimum Performance Physical Therapy, LLC Patient Information: Name: DOB: SS# Address: Phone: (H) (W) (C) Sex: Male Female Marital Status: M S D W Email: Employer Name/ Address: Referring Physician: (P)
BIRTHDATE - - AGE SEX EMERGENCY CONTACT PHONE( )
") PATIENT INFORMATION SOCIAL SECURITY # MARRIED SINGLE WIDOW DIVORCED NAME Last First MI HOME ADDRESS BILLING ADDRESS ACCT# DRIVER S LICENSE# BIRTHDATE - - AGE SEX CITY STATE ZIP CITY STATE ZIP PHONE HOME(
PATIENT INFORMATION SOCIAL SECURITY # MARRIED SINGLE WIDOW DIVORCED NAME Last First MI HOME ADDRESS BILLING ADDRESS ACCT# DRIVER S LICENSE# BIRTHDATE - - AGE SEX CITY STATE ZIP CITY STATE ZIP PHONE HOME(
Patient History Information
 Date: Body Technic Systems, Inc. 33790 Bainbridge Rd. Ste. 205 Solon, Ohio 44139 440-248-9255 phone 440-248-3608 fax Patient History Information Name: Date of birth: Address: City: State: Zip: Home phone:
Date: Body Technic Systems, Inc. 33790 Bainbridge Rd. Ste. 205 Solon, Ohio 44139 440-248-9255 phone 440-248-3608 fax Patient History Information Name: Date of birth: Address: City: State: Zip: Home phone:
HORIZON PHYSICAL THERAPY 9154 ESTATE THOMAS ST. THOMAS V.I 00802 (340)776-7667 P (340)714-1891 F WELCOME
776-7667 P (340)714-1891 F WELCOME") HORIZON PHYSICAL THERAPY 9154 ESTATE THOMAS ST. THOMAS V.I 00802 (340)776-7667 P (340)714-1891 F WELCOME We are pleased you have chosen us for your physical therapy needs. Our office is committed to providing
HORIZON PHYSICAL THERAPY 9154 ESTATE THOMAS ST. THOMAS V.I 00802 (340)776-7667 P (340)714-1891 F WELCOME We are pleased you have chosen us for your physical therapy needs. Our office is committed to providing
PATIENT INFORMATION: PATIENT CONTACT PHONE NUMBERS: PHYSICIAN INFORMATION: HEALTH INSURANCE INFORMATION:
 PATIENT INFORMATION: TODAY S DATE: HOW DID YOU HEAR ABOUT US?: LAST NAME: FIRST NAME: STREET CITY: STATE: ZIP: EMAIL MARTIAL STATUS: SINGLE MARRIED DIVORCED WIDOWED SEPARATED BIRTHDATE: AGE: SEX: MALE
PATIENT INFORMATION: TODAY S DATE: HOW DID YOU HEAR ABOUT US?: LAST NAME: FIRST NAME: STREET CITY: STATE: ZIP: EMAIL MARTIAL STATUS: SINGLE MARRIED DIVORCED WIDOWED SEPARATED BIRTHDATE: AGE: SEX: MALE
MVA Accident Questionnaire
 MVA Accident Questionnaire Name Date Date of Accident Time of Accident Road conditions at time of accident Were you the driver? Were you the passenger? Where were you seated in the vehicle? FRONT BACK
MVA Accident Questionnaire Name Date Date of Accident Time of Accident Road conditions at time of accident Were you the driver? Were you the passenger? Where were you seated in the vehicle? FRONT BACK
Welcome! We look forward to serving YOU. If we can do anything to make your time with us more enjoyable, please let us know.
 Welcome! We want to thank you for allowing us the opportunity to provide you with the highest level of quality rehabilitation services possible. We are committed to providing you with a comfortable, friendly
Welcome! We want to thank you for allowing us the opportunity to provide you with the highest level of quality rehabilitation services possible. We are committed to providing you with a comfortable, friendly
! 1220 Howell Street Ste. 110, Seattle, WA 98101 (206) 464-9002
 464-9002") ! 1220 Howell Street Ste. 110, Seattle, WA 98101 (206) 464-9002 PATIENT INFORMATION PATIENT NAME (Last, First, Middle Initial) DATE OF BIRTH AGE ADDRESS SOCIAL SECURITY NUMBER CITY, STATE, ZIP Male GENDER
! 1220 Howell Street Ste. 110, Seattle, WA 98101 (206) 464-9002 PATIENT INFORMATION PATIENT NAME (Last, First, Middle Initial) DATE OF BIRTH AGE ADDRESS SOCIAL SECURITY NUMBER CITY, STATE, ZIP Male GENDER
CENTENNIAL MEDICAL GROUP & CENTENNIAL SURGERY CENTER New Patient Paperwork
 New Patient Paperwork NAME OF PATIENT ( ) MALE ( ) FEMALE ADDRESS APT CITY STATE ZIP HOME PHONE # CELL PHONE # DATE OF BIRTH AGE SOCIAL SECURITY # MARITAL STATUS E-MAIL ADDERSS OCCUPATION EMPLOYER EMPLOYER
New Patient Paperwork NAME OF PATIENT ( ) MALE ( ) FEMALE ADDRESS APT CITY STATE ZIP HOME PHONE # CELL PHONE # DATE OF BIRTH AGE SOCIAL SECURITY # MARITAL STATUS E-MAIL ADDERSS OCCUPATION EMPLOYER EMPLOYER
RIDGEWOOD PHYSICAL THERAPY AND REHABILITATION CENTER PATIENT INFORMATION
 RIDGEWOOD PHYSICAL THERAPY AND REHABILITATION CENTER PATIENT INFORMATION Today s date: / / EMAIL: PATIENT INFORMATION Patient s last name: First: Middle: Mr. Mrs. Miss Ms. SS#: - - Birth date: Sex: [ ]
RIDGEWOOD PHYSICAL THERAPY AND REHABILITATION CENTER PATIENT INFORMATION Today s date: / / EMAIL: PATIENT INFORMATION Patient s last name: First: Middle: Mr. Mrs. Miss Ms. SS#: - - Birth date: Sex: [ ]
Keweenaw Holistic Family Medicine Patient Registration Form
 Keweenaw Holistic Family Medicine Patient Registration Form How did you first learn of our Clinic? Circle one: Attended Lecture Internet KHFM website Newspaper Sign in window Yellow Pages Physician Friend
Keweenaw Holistic Family Medicine Patient Registration Form How did you first learn of our Clinic? Circle one: Attended Lecture Internet KHFM website Newspaper Sign in window Yellow Pages Physician Friend
Lifetouch Orthopedic Physical Therapy. -- PLEASE PRINT -- Patient Information. Proper Name First Middle Last Name you use
 Lifetouch Orthopedic Physical Therapy How did you find out about Lincoln Orthopedic Physical Therapy? Past patient/friend or family Physician Yellow Pages Web Site Location/Street sign Attorney/Nurse Case
Lifetouch Orthopedic Physical Therapy How did you find out about Lincoln Orthopedic Physical Therapy? Past patient/friend or family Physician Yellow Pages Web Site Location/Street sign Attorney/Nurse Case
Personal Injury Intake Form
 Personal Injury Intake Form Patient Information: Name Home Phone Address Work Phone Cell Phone Date of Birth Social Security # Sex Male Female Height Weight lbs Occupation Marital Status Employer No of
Personal Injury Intake Form Patient Information: Name Home Phone Address Work Phone Cell Phone Date of Birth Social Security # Sex Male Female Height Weight lbs Occupation Marital Status Employer No of
Name: Birthdate: Age: Address: City, State, ZIP: Preferred Phone # (Home)(Cell)(Work): Marital Status: M S W D
(Cell)(Work): Marital Status: M S W D") Be Fit Physical Therapy & Pilates, LTD Patient Registration Form Date: Name: Birthdate: Age: Address: City, State, ZIP: Preferred Phone # (Home)(Cell)(Work): Marital Status: M S W D Secondary Phone# (Home)(Cell)(Work):
Be Fit Physical Therapy & Pilates, LTD Patient Registration Form Date: Name: Birthdate: Age: Address: City, State, ZIP: Preferred Phone # (Home)(Cell)(Work): Marital Status: M S W D Secondary Phone# (Home)(Cell)(Work):
J. Richard Lilly, M.D., A.B.F.P., & Associates, P.C.
 J. Richard Lilly, M.D., A.B.F.P., & Associates, P.C. PATIENT REGISTRATION - Please PRINT Clearly Patient Name First Middle Last Date of Birth Age Home Address Apt. No. City State Zip code Occupation Social
J. Richard Lilly, M.D., A.B.F.P., & Associates, P.C. PATIENT REGISTRATION - Please PRINT Clearly Patient Name First Middle Last Date of Birth Age Home Address Apt. No. City State Zip code Occupation Social
Retinal Consultants of San Antonio Diseases and Surgery of the Retina and Vitreous www.retinasanantonio. com
 Retinal Consultants of San Antonio Diseases and Surgery of the Retina and Vitreous www.retinasanantonio. com 1 Calvin E. Mein, MD 9480 Huebner Rd, Suite 310 (210) 615-1311 Moises A. Chica, MD San Antonio,
Retinal Consultants of San Antonio Diseases and Surgery of the Retina and Vitreous www.retinasanantonio. com 1 Calvin E. Mein, MD 9480 Huebner Rd, Suite 310 (210) 615-1311 Moises A. Chica, MD San Antonio,
Last Name First Name Middle Initial Address Apt # City State Zip Home Phone ( ) Mobile Phone ( ) Work Phone ( )
 Mobile Phone ( ) Work Phone ( )") Patient Registration A. P A T I E N T Please Print Legibly on Form Account # Address Apt # City State Zip DOB (mm/dd/yy) Gender Male Female SSN # Preferred Contact Method: Home Ph Mobile Ph Text E-mail
Patient Registration A. P A T I E N T Please Print Legibly on Form Account # Address Apt # City State Zip DOB (mm/dd/yy) Gender Male Female SSN # Preferred Contact Method: Home Ph Mobile Ph Text E-mail
PATIENT INFORMATION (Please Print Clearly)
") PATIENT INFORMATION (Please Print Clearly) Patient Name (Full): Address: City: State: Zip: Birthdate: EMAIL: Date of Injury: Date of Surgery Cell phone: Home Phone: Work Phone: Sex: M F Marital Status:
PATIENT INFORMATION (Please Print Clearly) Patient Name (Full): Address: City: State: Zip: Birthdate: EMAIL: Date of Injury: Date of Surgery Cell phone: Home Phone: Work Phone: Sex: M F Marital Status:
HSE Medical Associates Family Practice
 HSE Medical Associates Family Practice PLEASE CHECK WHICH PROVIDER YOU ARE HERE TO SEE M.D. P.A. David W. Hoefer, M.D. Paul E. Shepard, M.D. Alfredo T. Ermac, M.D. Sergio G. Perossa, Darcy Bevil, P.A.
HSE Medical Associates Family Practice PLEASE CHECK WHICH PROVIDER YOU ARE HERE TO SEE M.D. P.A. David W. Hoefer, M.D. Paul E. Shepard, M.D. Alfredo T. Ermac, M.D. Sergio G. Perossa, Darcy Bevil, P.A.
Dr. Ronnie Pollard, DPM 1563 Gilpin Street Denver, CO 80218 303-388-0976 www.elevationfoot.com
 1 Dr. Ronnie Pollard, DPM 1563 Gilpin Street Denver, CO 80218 303-388-0976 www.elevationfoot.com DEMOGRAPHICS & INSURANCE Patient Information Name: (First) (MI) (Last) SS#: DOB: Sex: Male Female Address:
1 Dr. Ronnie Pollard, DPM 1563 Gilpin Street Denver, CO 80218 303-388-0976 www.elevationfoot.com DEMOGRAPHICS & INSURANCE Patient Information Name: (First) (MI) (Last) SS#: DOB: Sex: Male Female Address:
Electronic Health Records Intake Form
 Dr. Sam Yoder, D.C. 101 Winston Way Ste B Campbellsville, KY 42718 Electronic Health Records Intake Form In compliance with requirements for the government EHR incentive program First Name: Address: Last
Dr. Sam Yoder, D.C. 101 Winston Way Ste B Campbellsville, KY 42718 Electronic Health Records Intake Form In compliance with requirements for the government EHR incentive program First Name: Address: Last
Dr. Brett Haderlie, D.C. Patient Information (Please Print)
") CONNECT CH I ROPRAC TIC Dr. Brett Haderlie, D.C. Patient Information (Please Print) Thank you for choosing our practice for your chiropractic needs. Name SS/HIC/Patient ID# Address City State Zip Birthdate
CONNECT CH I ROPRAC TIC Dr. Brett Haderlie, D.C. Patient Information (Please Print) Thank you for choosing our practice for your chiropractic needs. Name SS/HIC/Patient ID# Address City State Zip Birthdate
*WELCOME TO OUR OFFICE*
 *WELCOME TO OUR OFFICE* WE FIND THAT COMMUNICATION WITH OUR PATIENTS REGARDING OUR BUISNESS OFFICE POLICIES ASSISTS US IN PROVIDING YOU THE BEST SERVICE. THEREFORE WE HAVE PROVIDED A HIGHLIGHT OF SOME
*WELCOME TO OUR OFFICE* WE FIND THAT COMMUNICATION WITH OUR PATIENTS REGARDING OUR BUISNESS OFFICE POLICIES ASSISTS US IN PROVIDING YOU THE BEST SERVICE. THEREFORE WE HAVE PROVIDED A HIGHLIGHT OF SOME