Radiotherapy for Non-Small Cell Lung Cancer. Standard Treatment Options Radiotherapy Planning
|
|
|
- Cordelia Small
- 8 years ago
- Views:
Transcription
1 Radiotherapy for Non-Small Cell Lung Cancer I II Standard Treatment Options Radiotherapy Planning

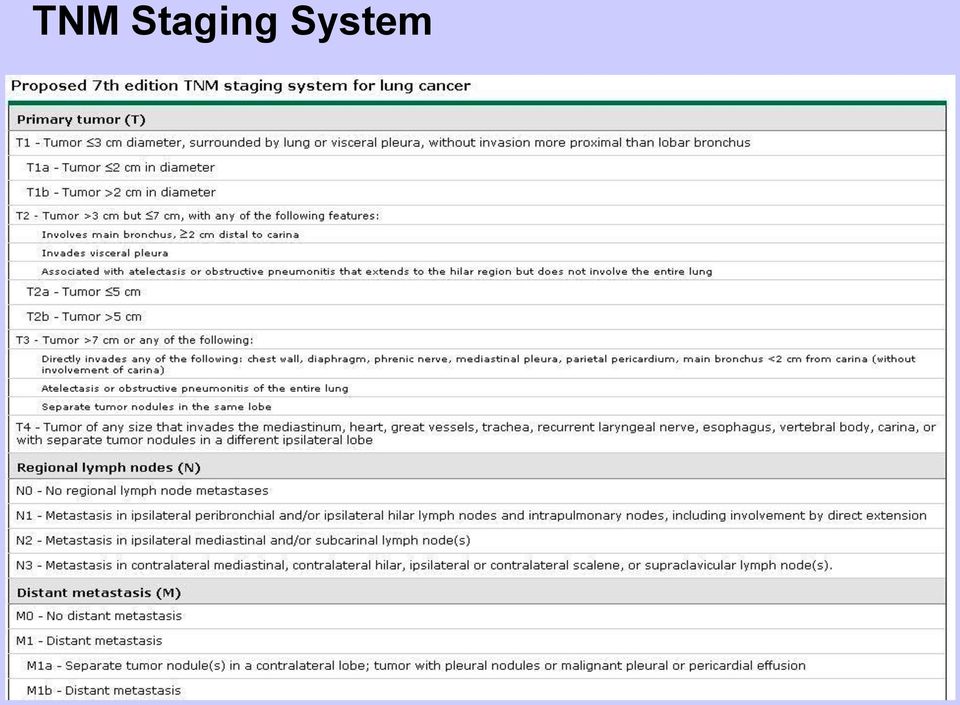
2 TNM Staging System
3 Disease Staging - Management is based on disease stage - Stage I-II: early stage - Stage IIIA: locally advanced (surgery feasible) - Stage IIIB: locally advanced (surgery not feasible) - Stage IV: metastatic disease
 - Stage IV:")
4 Types of Staging -Symptoms and physical findings -Laboratory tests -x-ray, CT, PET - Mediastinal LN sampling mediastinoscopy thoracoscopy endoscopic ultrasound transbronchial needle aspiration - Cytologic examination of pleural effusions

5 Staging Algorithm

6 Lymph Node Map Nomenclature (American College of Surgeons)

7 Management of Stage I + II NSCLC -Surgery alone is the standard treatment choice! -Lobectomy: optimal procedure -Wedge resection: 3x LR / 30% more mortality (Ginsberg 1995) but newer series show no worse outcome with limited surgery (Lee 2003, El Sherif 2006) -Wedge resection for small tumors (<3cm) and elderly patients -No randomized trials, but excellent results (randomized trial Surgery Radiotherapy underway) -Adjuvant Cisplatin-based ChT for stage II for stage IB data is conflicting -No adjuvant radiotherapy after radical surgery (i.e. R0)
 -Adjuvant Cisplatin-based ChT for stage II for stage IB data is")
8 Stage I: Outcome after Surgery

9 Stage I - III: Outcome after Surgery

10 Definitive Radiotherapy for Stage I + II NSCLC -Alternative for comorbid patients who are not fit for surgery -For patients who refuse surgery Gy to primary (+/- 50Gy to part of mediastinum, if feasible) Review of 26 nonrandomized trials (Powell 2001) Cancer-specific Survival OS (RT) OS (surgery) 2y 54 93% 22 72% 67% 3y 22 56% 17 55% 5y 13 39% 0 42% 47% Non-cancer deaths following RT: 11 43% (reflecting the poor health status of pts. treated in these studies) -Clinical stage I only in 57% pathologic stage I (Lopez 2005)

11 Radical RT Stage I II: Selected Studies Autor Jahr / Journal Stadium Dosis (Gy) Resultat Dosoretz 1992 / IJROBP T1-3 N % (2-JÜ) / 10% (5-JÜ) Jeremic 1997 / IJROBP T1-2 N0 69,6 (hyperfrakt.) 30% (5-JÜ) Jeremic 1999 / Lung Cancer T1-2 N1 69,6 (hyperfrakt.) 25% (5-JÜ) Cheung 2002 / IJROBP T1-2 N (akzell.) 46% (2-JÜ) Rosenzweig 2005 / Cancer T1-3 N0-2 <= 81 40% (OS) 52% (2y loc.control rate) -Results 20-30% worse compared to surgery -Stage IA: 5y OS 60% (almost comparable to surgery)
 46% (2-JÜ) Rosenzweig 2005 / Cancer T1-3 N0-2 <= 81 40% (OS) 52% (2y loc.")
12 Stereotactic Body Radiation Therapy (SBRT) -Ultra precise treatment planning (fixation, IGRT) -High doses (e.g. 4x12Gy), but optimal dose /fx not known -Dose response relationship: BED >100Gy vs. <100Gy Results (Lagerwaard 2008): 1y- / 2y OS: 81 / 64% 1y- / 2y DFS: 83 / 68% (88 / 81% for stage IA) Median OS: 34 months Local failure rate: 7% Regional failure: 9% Distant failure: 11% Severe late toxicities: <3% -Results superior to conventional 3D-CRT -For stage IA results near surgery

13 SBRT Example -T2 N0 -CR after radical radiation -COPD with emphysema

14 Other Techniques improving Outcome Hyperfractionation (Jeremic 1997, 1999) Stage I Stage II Median survival 33mts. 27mts. 5y-OS 30% 25% Protons (Bush 2004) 3y local control 74% Disease-specific survival Pneumonitis, esophageal or late cardiac toxicity 72% 0%

15 Adjuvant Radiotherapy for Stage I + II NSCLC -No postoperative RT after R0-Resection -54Gy after R1-Resection to the bronchial stump Gy after R2-Resection Randomized trials: -Local recurrence: reduced -Survival: unchanged, worse or improved! (likely relate to different radiation techniques) PORT-Metaanalysis (1998): -decreased OS after postoperative RT (55 vs. 48%)
 PORT-Metaanalysis (1998): -decreased OS")
16 Adjuvant Radiotherapy for Stage I + II NSCLC PORT-Study has been criticized: -Bias: 1/3 pts. from French Trial with high fractions + doses (60Gy/2.5Gy) -Partly used old techniques (e.g. Cobalt) -More recent randomized trial: (Trodella 2002) Modern 3D-CRT Safe fractions (1.8Gy) and small doses (50.4Gy) Target: bronchial stump and homolateral hilum LR 2% vs. 23% OS 67% vs. 58% Long-term toxicity acceptable
 -More recent randomized trial: (Trodella 2002) Modern 3D-CRT Safe fractions (1.")
17 Summary: Management of Stage I+II NSCLC -Pathologic stage I+II represents a minority of cases (staging!) -In contrast to advanced stages curable with aggressive therapy and have good prognosis -Surgery is the standard treatment of choice (Lobectomy) -Adjuvant ChT (Cisplatin) for stage II and selected IB -Definitive RT as an alternative for medical inoperable patients and for those who refuse surgery -No adjuvant RT after R0-Resection -Adjuvant RT after R1-/ R2-Resection -Further trials are needed to establish the role of RT in a postoperative setting and its optimal dose/fractionation/technique in a radical setting

18 Management of Stage III NSCLC -Locoregionally advanced stages IIIA IIIB surgery feasible surgery not feasible -Usually combined therapy approach -Optimal regime uncertain -Trend toward trimodality therapy -Initial nonoperative treatment generally recommended -No single regime for all patients (clinical heterogeneity) -Management individually to be discussed (tumor board)
 -Management individually to be discussed")
19 Radiotherapy for Stage III NSCLC Definitive radiotherapy alone -for patients who are not fit for combined treatment -isolated thoracic recurrence after surgery -palliative for patients with poor performance status or stage IV Early randomized trial: RT vs. Placebo (Roswit 1968) modest but significant survival benefit (18 vs. 14% at 1 year) RT alone: MS 10mts. 5y-OS 5% Factors associated with improved prognosis: (Basaki 2006, RTOG ) -small primary tumor -small total tumor volume
 RT alone: MS 10mts.")
20 Radiotherapy for Stage III NSCLC Definitive radiotherapy alone Should it be given immediately or deferred? Randomized trial: immediate RT vs. RT reserved for symptoms (Falk 2002) -median survival -rate of symptom control ns similar Palliative symptomatic care is a valuable option for patients with locoregionally advanced NSCLC who are not candidates for combined modality treatment.

21 Radiotherapy for Stage III NSCLC Dose and local control RTOG phase III trial: (Perez 1986) 40Gy 50Gy 60Gy (2Gy/fx) Local Control 52% 62% 73% Survival similar -60Gy / 30 fractions: standard today -phase II data show better local control with higher doses -limiting factor: normal tissue tolerance Improved therapeutic index -altered fractionation schedules -Amifostine -IMRT, IGRT, Tomotherapy, Protons..
22 Radiotherapy for Stage III NSCLC Altered Fractionation Schedules CHART (Saunders 1997,1999): 2y-survival 29% vs. 20% Severe dysphagia 19% vs. 3% ECOG 2597 (Belani 2005): No statistical significance reached Central Cancer Treatment Group (Schild 2002): No statistical significance in terms of TTP, OS, Toxicities
23 Management of Stage IIIA NSCLC -High risk for both local and distal failure after resection -Role of postoperative RT controversial -Survival benefit of RT not confirmed in randomized trials Lung Cancer Study Group, 1986: LR 3% vs. 41% OS n.s. PORT Study, 1998: decreased OS 48% vs. 55% (stages I-III) (subgroup analysis: no clear evidence for stage III) Studies on toxicities (Lally 2006, 2007): Limited LN-involvement: decreased OS after RT (31 vs. 41%) N2-disease: improved OS after postop. RT (27 vs. 20%) Death from cardiac toxicities: increased for pts. treated in early studies ( ) not increased for those treated after 1989
24 Management of Stage IIIA NSCLC -Postoperative ChT: modest but significant better OS (4-5%) -Promising results from preoperative ChT
25 Management of Stage IIIA NSCLC -Better survival after adjuvant ChT -Promising results of phase II data with induction ChT New Protocols: -Role of preoperative RT-ChT (SAKK) -Role of postoperative RT (EORTC)
26 Summary: Management of Stage IIIA NSCLC -Pre- or postoperative ChT -No established role of pre- or postoperative RT RT in Clinical Trials (e.g. SAKK 16/00: RT/ChT OP vs. ChT OP) -No postoperative RT recommended routinely Postoperative RT recommended: N2 (multilevel) R1/R2 -Preoperative RT for Pancoast Tumor (45-50Gy) -Radical RT (+/- ChT) for medically inoperable patients (60Gy) (concomitant better than sequential, see stage IIIB)
27 Management of Stage IIIB NSCLC -Long Term OS < 5%! (Hagen 1997) -Most patients die from metastasis -Median survival prolonged 8-10 months with RT-ChT for younger patients with good performance status (Sause 1997) -Other patients: good palliation by RT -Combined ChT-RT better survival than RT alone (Pignon 1994) -Concomitant ChT-RT better than sequential, but more toxicities (Furuse 1999, RTOG 9410) -Role of surgery uncertain (SAKK 16/01: preoperative ChT-RT)
28 Management of Stage IIIB NSCLC Definitive Chemoradiotherapy Objective: treat locoregional and micrometastasic disease -initially sequential therapy to avoid overlapping toxicities -initial trials established benefit of combined approach -subsequent studies compared sequential vs. concurrent chemoradiotherapy
29 Management of Stage IIIB NSCLC Sequential Chemoradiotherapy
30 Management of Stage IIIB NSCLC Concurrent Chemoradiotherapy Objective: early treatment of micrometastases radio-sensitization (better local control) -randomized trials established this approach as the preferred treatment -toxicity is increased but manageable
31 Management of Stage IIIB NSCLC Concurrent Chemoradiotherapy
32 Management of Stage IIIB NSCLC Superiority of Concurrent Chemoradiotherapy over Sequential Two large multicenter trials 1. Furuse, JCO 1999 Randomized -conc. ChT (CMV) + 56Gy (split course RT) -same regime sequential Concurrent Sequential Response Rate 84% 86% Median Survival 17mts. 13mts. 2y-survival 35% 17% 5y-survival 16% 9%
33 Management of Stage IIIB NSCLC Superiority of Concurrent Chemoradiotherapy over Sequential Two large multicenter trials 2. RTOG 9410 Randomized -conc. ChT (CV) + 60Gy -same regime sequential Concurrent Sequential Median Survival 17mts. 14.6mts. 4y-survival 21% 127% Toxicity Increased, but nut increased treatment related death
34 Management of Stage IIIB NSCLC Concurrent low dose Chemoradiotherapy Objective: improved locoregional control minimize toxicity -only one randomized trial demonstrate benefit over RT alone (Schaake-Koning, 1992) -several other studies failed to demonstrate survival benefit -no trials comparing low dose vs. standard dose ChT -option for elderly patients
35 Management of Stage IIIB NSCLC Recommendations: -Concomitant ChT-RT as first choice -Concomitant daily low-dose Cisplatin + RT 60Gy elderly patients (Schake-Koning, 1992) -Sequential ChT-RT: Cisplatin + 60Gy (Dillman, 1990) for large tumors -RT only (30 x 2Gy x 3Gy) poor performance status, palliation -Surgery only within study protocol or selected patients (e.g. T4 N0-1 after induction therapy)
36 Summary: Management of Stage IIIB NSCLC -Heterogeneous group, therapy to be discussed at tumor board -Radical multimodality treatment vs. good palliation -Combined Radio-Chemotherapy is standard treatment -Concomitant better than sequential (survival benefit) but more toxicities -Sequential Chemo- Radiotherapy or RT alone for unfit patients -Induction Chemotherapy for extensive tumor-volume which can not be encompassed in reasonable RT portals -Role of Surgery uncertain, only selected patients -Optimal regime not clear, therapy within clinical trials as possible: Induction-therapy OP Accelerated RT schemes New drugs + concomitant RT..
37 Management of RT Toxicity - Pneumonitis Pneumonitis: 4-6 wks. after RT (Fibrosis after mts.) Symptoms: fever, cough, illness Risk factors: -Lung function (FEV1) -Treated volume: -Dmean: <10Gy - very small risk 20Gy - 15% risk 30Gy - 50% risk Treatment: V20=25% (8% pneumonitis) V20=37% (39% pneumonitis) V10, V5,. V30-40 (fibrosis) Antibiotics (e.g. Roxithromycin) for 10d Steroids (e.g. Prednisone) beginning with high dose for 6wks. (reducing doses)
38 Management of RT Toxicity - Pneumonitis Radiographic finding: diffuse interstitial infiltrate Radiation portal (left) with subsequent radiation pneumonitis Sequential transverse images through lung showing radiation pneumonitis in right lung
39 Management of RT Toxicity - Fibrosis Rosen, I. I. et al. Radiology 2001;221:
40 RT-Planning Definition of Target Volumes ICRU Gross Tumour Volume Clinical Target Volume Planning Target Volume = critical step = weakest link in radiotherapy chain
41 RT-Planning Defining the GTV CT: standard imaging modality Complementary information by MRI and PET scanning Limiting factors of CT imaging for lung cancer: -planning-ct without intravenous contrast so as not to disturb the electron density information interpretation always in conjunction with diagnostic CT -not routinely possible to distinguish T3 T4 (MRI some advantages) -MRI used for imaging apical primary tumours (Pancoast) -Sensitivity / specificity only 60 / 77% for LN knowledge of normal anatomy (LN levels, hilar anatomy)! knowledge of patterns of lymphatic drainage
42 RT-Planning Defining the GTV Knowledge of anatomy LN levels (American College of Surgeons)
43 RT-Planning Defining the GTV Knowledge of anatomy LN levels - Cross Sectional Anatomy Murray JG, Eur J Radiol, 1993,17:61-68.
44
45 RT-Planning - Defining the GTV Cross Sectional Anatomy - Suggested Paper
46 RT-Planning Defining the GTV Knowledge of lymphatic drainage according to localisation of PT (Hata 1990)
47 RT-Planning Defining the GTV Integrating PET Value of PET for PT: Atelectasis reduction of irradiated volume Value of PET for LN staging: Sensitivity 79% Specificity 91% Negative predictive value 95% Positive predictive value 80% (hot spots still require verification) Value of PET for Metastases: metastases detected in10-15% of surgical candidates
48 RT-Planning Defining the GTV Impact of PET on RT planning PTV increased in 64% (detected nodes) decreased in 36% (exclusion of atelectasis) (Erdi 2002) Average reduction of PTV by 29% Average reduction of V20 by 27% (Vanuytsel 2000) Interobserver variability reduced: mean ratio of GTV without PET: 2.31 mean ratio of GTV with PET: 1.56 (Caldwell 2001)
49 RT-Planning Defining the GTV Impact of PET: Atelectasis
50 RT-Planning Defining the GTV Impact of PET: PTV
51 RT-Planning Defining the GTV Impact of PET: PTV
52 RT-Planning Defining the GTV Impact of PET: PTV RT Plan
53 RT-Planning Defining the GTV Limiting factors of PET -Resolution 4-8mm (depending on scanner and institution) -Registration errors (esp. with software based fusion) -Threshold value (SUV) individually to be determined Summary: PET is a promising complementary tool in RT planning of NSCLC. Its value for staging has been established and preliminary reports suggest that it may lead to more consistent definition of GTV in RT planning. However, it is still not clear, whether this will translate into better survival.
54 RT-Planning Defining the CTV 1. Margin around primary tumour (microscopic spread) Histopathologic quantification of subclinical cancer around the grossly visible primary (Giraud 2000): Microscopic extension Adeno Squamos mean value 2.69mm 1.48mm 5mm margin covers: 80% 91% margin to cover 95% 8mm 6mm This data could also be used for IMRT planning: -define constraint for GTV (dose escalation to primary) -define constraint for subclinical disease (less dose) -increase therapeutic index
55 RT-Planning Defining the CTV 2. Subclinical lymph nodes (ENI) -high risk of nodal spread in lung cancer -but value of ENI is not proven Reasons against ENI: -less than 20% locally controlled 1y after RT with conventional dose (Arriagada 1991) -need for more intense treatment to gross tumour -large volumes prevent dose escalation (normal tissue tolerance) -small primary tumor and small total tumor volume predictive (Basaki 2006, RTOG ) -modern chemotherapy regimens may lead to better control of microscopic disease
56 RT-Planning Defining the CTV 2. Subclinical lymph nodes (ENI)
57 RT-Planning Defining the CTV 2. Subclinical lymph nodes (ENI) From large... Old Standard (Perez 1997)
58 RT-Planning Defining the CTV 2. Subclinical lymph nodes (ENI)... to small! New Trend (IMRT 2007)
59 RT-Planning Defining the PTV ICRU recommendations CTV... + Internal Margin (Internal Target Volume) variations in position, size and shape of CTV (internal reference system attached to the patient) + Set-up Margin variations in relation patient - beam (external reference system attached to machine)
60 RT-Planning Defining the PTV Reducing set-up uncertainty: -Tattoos (instead of skin markers) -Custom immobilisation devices
61 RT-Planning Defining the PTV Reducing set-up uncertainty: -Daily EPID: -matching DRR - EPI -distinguish between systematic (needs correction) and random error (no correction needed)
62 RT-Planning Defining the PTV Reducing respiration induced errors: -Breath - hold -Voluntary (Deep Inspiration Breath Hold) -Forced (Active Breathing Control) -CT scanning -Slow scanning -Respiration correlated CT -Gating
63 RT-Planning Defining the PTV Reducing respiration induced errors: Size of movement dependent on: - tumour location in the lung - fixation to adjacent structures - lung capacity and oxygenation - patient fixation and anxiety Average movement in normal breathing: - Upper lobe 0-0.5cm - Lower lobe cm - Middle lobe cm - Hilum cm Steppenwoolde 2004
64 RT-Planning Defining the PTV Reducing respiration induced errors: Gated CT normally reduces the margin PTV - CTV (compared to using published data):
65 RT-Planning Defining the PTV Drawing PTV in gated planning CT: -Define GTV/CTV for inspiration and expiration phase -Give a margin of 0.5-1cm in all directions (setup uncertainty) Closing Words: DON T use dose escalation and highly conformal techniques such as IMRT for lung cancer until tumour motion can be taken into account! In the meantime... -Outline GTV as best as possible -Construct CTV based on the literature -Construct PTV based on measured tumour motion and known setup uncertainty.
Table of Contents. Data Supplement 1: Summary of ASTRO Guideline Statements. Data Supplement 2: Definition of Terms
 Definitive and Adjuvant Radiotherapy in Locally Advanced Non-Small-Cell Lung Cancer: American Society of Clinical Oncology Clinical Practice Guideline Endorsement of the American Society for Radiation
Definitive and Adjuvant Radiotherapy in Locally Advanced Non-Small-Cell Lung Cancer: American Society of Clinical Oncology Clinical Practice Guideline Endorsement of the American Society for Radiation
Lung Cancer Treatment Guidelines
 Updated June 2014 Derived and updated by consensus of members of the Providence Thoracic Oncology Program with the aid of evidence-based National Comprehensive Cancer Network (NCCN) national guidelines,
Updated June 2014 Derived and updated by consensus of members of the Providence Thoracic Oncology Program with the aid of evidence-based National Comprehensive Cancer Network (NCCN) national guidelines,
Radiation Therapy in the Treatment of
 Lung Cancer Radiation Therapy in the Treatment of Lung Cancer JMAJ 46(12): 537 541, 2003 Kazushige HAYAKAWA Professor and Chairman, Department of Radiology, Kitasato University School of Medicine Abstract:
Lung Cancer Radiation Therapy in the Treatment of Lung Cancer JMAJ 46(12): 537 541, 2003 Kazushige HAYAKAWA Professor and Chairman, Department of Radiology, Kitasato University School of Medicine Abstract:
Treatment Algorithms for the Management of Lung Cancer in NSW Guide for Clinicians
 Treatment Algorithms for the Management of Lung Cancer in NSW Guide for Clinicians Background The Cancer Institute New South Wales Oncology Group Lung (NSWOG Lung) identified the need for the development
Treatment Algorithms for the Management of Lung Cancer in NSW Guide for Clinicians Background The Cancer Institute New South Wales Oncology Group Lung (NSWOG Lung) identified the need for the development
GUIDELINES FOR THE MANAGEMENT OF LUNG CANCER
 GUIDELINES FOR THE MANAGEMENT OF LUNG CANCER BY Ali Shamseddine, MD (Coordinator); as04@aub.edu.lb Fady Geara, MD Bassem Shabb, MD Ghassan Jamaleddine, MD CLINICAL PRACTICE GUIDELINES FOR THE TREATMENT
GUIDELINES FOR THE MANAGEMENT OF LUNG CANCER BY Ali Shamseddine, MD (Coordinator); as04@aub.edu.lb Fady Geara, MD Bassem Shabb, MD Ghassan Jamaleddine, MD CLINICAL PRACTICE GUIDELINES FOR THE TREATMENT
Particle Therapy for Lung Cancer. Bradford Hoppe MD, MPH Assistant Professor University of Florida bhoppe@floridaproton.org
 Particle Therapy for Lung Cancer Bradford Hoppe MD, MPH Assistant Professor University of Florida bhoppe@floridaproton.org Content Rationale for Particle Therapy in Lung Cancer Proof of Principle Treatment
Particle Therapy for Lung Cancer Bradford Hoppe MD, MPH Assistant Professor University of Florida bhoppe@floridaproton.org Content Rationale for Particle Therapy in Lung Cancer Proof of Principle Treatment
Radiotherapy in locally advanced & metastatic NSC lung cancer
 Radiotherapy in locally advanced & metastatic NSC lung cancer Dr Raj Hegde. MD. FRANZCR Consultant Radiation Oncologist. William Buckland Radiotherapy Centre. Latrobe Regional Hospital. Locally advanced
Radiotherapy in locally advanced & metastatic NSC lung cancer Dr Raj Hegde. MD. FRANZCR Consultant Radiation Oncologist. William Buckland Radiotherapy Centre. Latrobe Regional Hospital. Locally advanced
SMALL CELL LUNG CANCER
 Protocol for Planning and Treatment The process to be followed in the management of: SMALL CELL LUNG CANCER Patient information given at each stage following agreed information pathway 1. DIAGNOSIS New
Protocol for Planning and Treatment The process to be followed in the management of: SMALL CELL LUNG CANCER Patient information given at each stage following agreed information pathway 1. DIAGNOSIS New
CANCER PULMON: ESTADIOS INICIALES POSTMUNDIAL PULMON DENVER 2015. 8-10-2015.Manuel Cobo Dols S. Oncología Médica HU Málaga Regional y VV
 CANCER PULMON: ESTADIOS INICIALES POSTMUNDIAL PULMON DENVER 2015 8-10-2015.Manuel Cobo Dols S. Oncología Médica HU Málaga Regional y VV Meta-analisis LACE: adyuvancia vs no adyuvancia Pignon JP, et al.
CANCER PULMON: ESTADIOS INICIALES POSTMUNDIAL PULMON DENVER 2015 8-10-2015.Manuel Cobo Dols S. Oncología Médica HU Málaga Regional y VV Meta-analisis LACE: adyuvancia vs no adyuvancia Pignon JP, et al.
Radiotherapy in Lung
 Radiotherapy in Lung CancerAnatomy Oblique fissure in both lungs. Horizontal fissure in Right lung. Trachea bifurcates at the level of T5. Lymph nodes are divided into stations. Intrapulmonary, bronchopulmonary
Radiotherapy in Lung CancerAnatomy Oblique fissure in both lungs. Horizontal fissure in Right lung. Trachea bifurcates at the level of T5. Lymph nodes are divided into stations. Intrapulmonary, bronchopulmonary
REPORT ASCO 1998 LOS ANGELES : LUNG CANCER Johan F. Vansteenkiste, MD, PhD, Univ. Hospital and Leuven Lung Cancer Group
 REPORT ASCO 1998 LOS ANGELES : LUNG CANCER Johan F. Vansteenkiste, MD, PhD, Univ. Hospital and Leuven Lung Cancer Group Educational session Treatment of stage III non-small cell lung cancer (NSCLC) in
REPORT ASCO 1998 LOS ANGELES : LUNG CANCER Johan F. Vansteenkiste, MD, PhD, Univ. Hospital and Leuven Lung Cancer Group Educational session Treatment of stage III non-small cell lung cancer (NSCLC) in
Alternatives to Surgical Resection for Early Stage Lung Cancer
 Alternatives to Surgical Resection for Early Stage Lung Cancer Neil A. Christie MD University of Pittsburgh Medical Center Department of Thoracic Surgery Allied Health Personnel Symposium AATS 2014 Conflicts
Alternatives to Surgical Resection for Early Stage Lung Cancer Neil A. Christie MD University of Pittsburgh Medical Center Department of Thoracic Surgery Allied Health Personnel Symposium AATS 2014 Conflicts
A Practical Guide to Advances in Staging and Treatment of NSCLC
 A Practical Guide to Advances in Staging and Treatment of NSCLC Robert J. Korst, M.D. Director, Thoracic Surgery Medical Director, The Blumenthal Cancer Center The Valley Hospital Objectives Revised staging
A Practical Guide to Advances in Staging and Treatment of NSCLC Robert J. Korst, M.D. Director, Thoracic Surgery Medical Director, The Blumenthal Cancer Center The Valley Hospital Objectives Revised staging
Management of Non-Small Cell Lung Cancer Guide for General Practitioners
 Management of n-small Cell Lung Cancer Guide for General Practitioners Clinical Stage I Cancer only in one lobe of lung and
Management of n-small Cell Lung Cancer Guide for General Practitioners Clinical Stage I Cancer only in one lobe of lung and
B. Dingle MD, FRCPC, Brian Yaremko MD,FRCPC, R. Ash, MD, FRCPC, P. Truong, MD, FRCPC
 Lung Cancer B. Dingle MD, FRCPC, Brian Yaremko MD,FRCPC, R. Ash, MD, FRCPC, P. Truong, MD, FRCPC EPIDEMIOLOGY The estimated incidence of lung cancer in Canada for 2007 is 23,300 with 12,400 occurring in
Lung Cancer B. Dingle MD, FRCPC, Brian Yaremko MD,FRCPC, R. Ash, MD, FRCPC, P. Truong, MD, FRCPC EPIDEMIOLOGY The estimated incidence of lung cancer in Canada for 2007 is 23,300 with 12,400 occurring in
Moving forward, where are we with Clinical Trials?
 Moving forward, where are we with Clinical Trials? Dennis A. Wigle Division of Thoracic Surgery Mayo Clinic AATS/STS General Thoracic Surgery Symposium Sunday, April 27 th 2014 2012 MFMER slide-1 Where
Moving forward, where are we with Clinical Trials? Dennis A. Wigle Division of Thoracic Surgery Mayo Clinic AATS/STS General Thoracic Surgery Symposium Sunday, April 27 th 2014 2012 MFMER slide-1 Where
Stage IIIB disease includes patients with T4 tumors,
 Guidelines on Treatment of Stage IIIB Non-small Cell Lung Cancer* James R. Jett, MD, FCCP; Walter J. Scott, MD, FCCP; M. Patricia Rivera MD, FCCP; and William T. Sause, MD, FACR Stage IIIB includes patients
Guidelines on Treatment of Stage IIIB Non-small Cell Lung Cancer* James R. Jett, MD, FCCP; Walter J. Scott, MD, FCCP; M. Patricia Rivera MD, FCCP; and William T. Sause, MD, FACR Stage IIIB includes patients
SAKK Lung Cancer Group. Current activities and future projects
 SAKK Lung Cancer Group Current activities and future projects SAKK Lung Cancer Group Open group of physicians interested in lung cancer Mostly Medical Oncologists, but also Thoracic Surgeons Radiation
SAKK Lung Cancer Group Current activities and future projects SAKK Lung Cancer Group Open group of physicians interested in lung cancer Mostly Medical Oncologists, but also Thoracic Surgeons Radiation
Jedi Wisdom for Lung Cancer Radiotherapy: May the Force Be With You
 Jedi Wisdom for Lung Cancer Radiotherapy: May the Force Be With You SHAUN LOEWEN MD PhD FRCPC Assistant Professor, University of Manitoba Radiation Oncologist, CancerCare Manitoba Disclosure Relationship
Jedi Wisdom for Lung Cancer Radiotherapy: May the Force Be With You SHAUN LOEWEN MD PhD FRCPC Assistant Professor, University of Manitoba Radiation Oncologist, CancerCare Manitoba Disclosure Relationship
Small Cell Lung Cancer
 Small Cell Lung Cancer Types of Lung Cancer Non-small cell carcinoma (NSCC) (87%) Adenocarcinoma (38%) Squamous cell (20%) Large cell (5%) Small cell carcinoma (13%) Small cell lung cancer is virtually
Small Cell Lung Cancer Types of Lung Cancer Non-small cell carcinoma (NSCC) (87%) Adenocarcinoma (38%) Squamous cell (20%) Large cell (5%) Small cell carcinoma (13%) Small cell lung cancer is virtually
Lung cancer forms in tissues of the lung, usually in the cells lining air passages.
 Scan for mobile link. Lung Cancer Lung cancer usually forms in the tissue cells lining the air passages within the lungs. The two main types are small-cell lung cancer (usually found in cigarette smokers)
Scan for mobile link. Lung Cancer Lung cancer usually forms in the tissue cells lining the air passages within the lungs. The two main types are small-cell lung cancer (usually found in cigarette smokers)
Corso Integrato di Clinica Medica ONCOLOGIA MEDICA AA 2010-2011 LUNG CANCER. VIII. THERAPY. V. SMALL CELL LUNG CANCER Prof.
 Corso Integrato di Clinica Medica ONCOLOGIA MEDICA AA 2010-2011 LUNG CANCER. VIII. THERAPY. V. SMALL CELL LUNG CANCER Prof. Alberto Riccardi SMALL CELL LUNG CARCINOMA Summary of treatment approach * limited
Corso Integrato di Clinica Medica ONCOLOGIA MEDICA AA 2010-2011 LUNG CANCER. VIII. THERAPY. V. SMALL CELL LUNG CANCER Prof. Alberto Riccardi SMALL CELL LUNG CARCINOMA Summary of treatment approach * limited
Adjuvant Therapy Non Small Cell Lung Cancer. Sunil Nagpal MD Director, Thoracic Oncology Jan 30, 2015
 Adjuvant Therapy Non Small Cell Lung Cancer Sunil Nagpal MD Director, Thoracic Oncology Jan 30, 2015 No Disclosures Number of studies Studies Per Month 12 10 8 6 4 2 0 1 2 3 4 5 6 7 8 9 10 11 12 1 2 3
Adjuvant Therapy Non Small Cell Lung Cancer Sunil Nagpal MD Director, Thoracic Oncology Jan 30, 2015 No Disclosures Number of studies Studies Per Month 12 10 8 6 4 2 0 1 2 3 4 5 6 7 8 9 10 11 12 1 2 3
Management of stage III A-B of NSCLC. Hamed ALHusaini Medical Oncologist
 Management of stage III A-B of NSCLC Hamed ALHusaini Medical Oncologist Global incidence, CA cancer J Clin 2011;61:69-90 Stage III NSCLC Includes heterogeneous group of patients with differences in the
Management of stage III A-B of NSCLC Hamed ALHusaini Medical Oncologist Global incidence, CA cancer J Clin 2011;61:69-90 Stage III NSCLC Includes heterogeneous group of patients with differences in the
Helical TomoTherapy for Lung Cancer Radiotherapy: Good Science Pays Clinical Dividends Peter Hoban, Ph.D., TomoTherapy Inc.
 CLINICAL FEATURE Helical TomoTherapy for Lung Cancer Radiotherapy: Good Science Pays Clinical Dividends Peter Hoban, Ph.D., TomoTherapy Inc. The Challenge Lung cancer kills more people each year in the
CLINICAL FEATURE Helical TomoTherapy for Lung Cancer Radiotherapy: Good Science Pays Clinical Dividends Peter Hoban, Ph.D., TomoTherapy Inc. The Challenge Lung cancer kills more people each year in the
Epidemiology, Staging and Treatment of Lung Cancer. Mark A. Socinski, MD
 Epidemiology, Staging and Treatment of Lung Cancer Mark A. Socinski, MD Associate Professor of Medicine Multidisciplinary Thoracic Oncology Program Lineberger Comprehensive Cancer Center University of
Epidemiology, Staging and Treatment of Lung Cancer Mark A. Socinski, MD Associate Professor of Medicine Multidisciplinary Thoracic Oncology Program Lineberger Comprehensive Cancer Center University of
Accelerated hemithoracic radiation followed by extrapleural pneumonectomy for malignant pleural mesothelioma
 Accelerated hemithoracic radiation followed by extrapleural pneumonectomy for malignant pleural mesothelioma Marc de Perrot, Ronald Feld, Natasha B Leighl, Andrew Hope, Thomas K Waddell, Shaf Keshavjee,
Accelerated hemithoracic radiation followed by extrapleural pneumonectomy for malignant pleural mesothelioma Marc de Perrot, Ronald Feld, Natasha B Leighl, Andrew Hope, Thomas K Waddell, Shaf Keshavjee,
Stomach (Gastric) Cancer. Prof. M K Mahajan ACDT & RC Bathinda
 Cancer. Prof. M K Mahajan ACDT & RC Bathinda") Stomach (Gastric) Cancer Prof. M K Mahajan ACDT & RC Bathinda Gastric Cancer Role of Radiation Layers of the Stomach Mucosa Submucosa Muscularis Serosa Stomach and Regional Lymph Nodes Stomach and Regional
Stomach (Gastric) Cancer Prof. M K Mahajan ACDT & RC Bathinda Gastric Cancer Role of Radiation Layers of the Stomach Mucosa Submucosa Muscularis Serosa Stomach and Regional Lymph Nodes Stomach and Regional
Radiation therapy involves using many terms you may have never heard before. Below is a list of words you could hear during your treatment.
 Dictionary Radiation therapy involves using many terms you may have never heard before. Below is a list of words you could hear during your treatment. Applicator A device used to hold a radioactive source
Dictionary Radiation therapy involves using many terms you may have never heard before. Below is a list of words you could hear during your treatment. Applicator A device used to hold a radioactive source
PET/CT in Lung Cancer
 PET/CT in Lung Cancer Rodolfo Núñez Miller, M.D. Nuclear Medicine and Diagnostic Imaging Section Division of Human Health International Atomic Energy Agency Vienna, Austria GLOBOCAN 2012 #1 #3 FDG-PET/CT
PET/CT in Lung Cancer Rodolfo Núñez Miller, M.D. Nuclear Medicine and Diagnostic Imaging Section Division of Human Health International Atomic Energy Agency Vienna, Austria GLOBOCAN 2012 #1 #3 FDG-PET/CT
How To Treat A Cancer With A Radical
 Management of mesothelioma Jan.vanmeerbeeck@ugent.be Amsterdam, March 6, 2010 1 management Palliation Symptomatic care Pain Breathlessness Radiotherapy Chemotherapy Surgery Radical (intention to cure)
Management of mesothelioma Jan.vanmeerbeeck@ugent.be Amsterdam, March 6, 2010 1 management Palliation Symptomatic care Pain Breathlessness Radiotherapy Chemotherapy Surgery Radical (intention to cure)
Clinical Trials and Radiation Treatment. Gerard Morton Odette Cancer Centre Sunnybrook Research Institute University of Toronto
 Clinical Trials and Radiation Treatment Gerard Morton Odette Cancer Centre Sunnybrook Research Institute University of Toronto What I will cover.. A little about radiation treatment The clinical trials
Clinical Trials and Radiation Treatment Gerard Morton Odette Cancer Centre Sunnybrook Research Institute University of Toronto What I will cover.. A little about radiation treatment The clinical trials
Non-Small Cell Lung Cancer Treatment Comparison to NCCN Guidelines
 Non-Small Cell Lung Cancer Treatment Comparison to NCCN Guidelines April 2008 (presented at 6/12/08 cancer committee meeting) By Shelly Smits, RHIT, CCS, CTR Conclusions by Dr. Ian Thompson, MD Dr. James
Non-Small Cell Lung Cancer Treatment Comparison to NCCN Guidelines April 2008 (presented at 6/12/08 cancer committee meeting) By Shelly Smits, RHIT, CCS, CTR Conclusions by Dr. Ian Thompson, MD Dr. James
Prostate Cancer Treatment: What s Best for You?
 Prostate Cancer Treatment: What s Best for You? Prostate Cancer: Radiation Therapy Approaches I. Choices There is really a variety of options in prostate cancer management overall and in radiation therapy.
Prostate Cancer Treatment: What s Best for You? Prostate Cancer: Radiation Therapy Approaches I. Choices There is really a variety of options in prostate cancer management overall and in radiation therapy.
Objectives. Mylene T. Truong, MD. Malignant Pleural Mesothelioma Background
 Imaging of Pleural Tumors Mylene T. Truong, MD Imaging of Pleural Tumours Mylene T. Truong, M. D. University of Texas M.D. Anderson Cancer Center, Houston, TX Objectives To review tumors involving the
Imaging of Pleural Tumors Mylene T. Truong, MD Imaging of Pleural Tumours Mylene T. Truong, M. D. University of Texas M.D. Anderson Cancer Center, Houston, TX Objectives To review tumors involving the
Disease/Illness GUIDE TO ASBESTOS LUNG CANCER. What Is Asbestos Lung Cancer? www.simpsonmillar.co.uk Telephone 0844 858 3200
 GUIDE TO ASBESTOS LUNG CANCER What Is Asbestos Lung Cancer? Like tobacco smoking, exposure to asbestos can result in the development of lung cancer. Similarly, the risk of developing asbestos induced lung
GUIDE TO ASBESTOS LUNG CANCER What Is Asbestos Lung Cancer? Like tobacco smoking, exposure to asbestos can result in the development of lung cancer. Similarly, the risk of developing asbestos induced lung
Survey on the treatment of non-small cell lung cancer (NSCLC) in England and Wales
 in England and Wales") Eur Respir J 1997; 10: 1552 1558 DOI: 10.1183/09031936.97.10071552 Printed in UK - all rights reserved Copyright ERS Journals Ltd 1997 European Respiratory Journal ISSN 0903-1936 Survey on the treatment
Eur Respir J 1997; 10: 1552 1558 DOI: 10.1183/09031936.97.10071552 Printed in UK - all rights reserved Copyright ERS Journals Ltd 1997 European Respiratory Journal ISSN 0903-1936 Survey on the treatment
Treatment of Stage III Non-small Cell Lung Cancer
 CHEST Supplement DIAGNOSIS AND MANAGEMENT OF LUNG CANCER, 3RD ED: ACCP GUIDELINES Treatment of Stage III Non-small Cell Lung Cancer Diagnosis and Management of Lung Cancer, 3rd ed: American College of
CHEST Supplement DIAGNOSIS AND MANAGEMENT OF LUNG CANCER, 3RD ED: ACCP GUIDELINES Treatment of Stage III Non-small Cell Lung Cancer Diagnosis and Management of Lung Cancer, 3rd ed: American College of
Stage I, II Non Small Cell Lung Cancer
 Stage I, II Non Small Cell Lung Cancer Best Results T1 (less 3 cm) N0 80% 5 year survival No Role Adjuvant Chemotherapy Radiation Therapy Reduces Local Recurrence No Improvement in Survival 1 Staging Mediastinal
Stage I, II Non Small Cell Lung Cancer Best Results T1 (less 3 cm) N0 80% 5 year survival No Role Adjuvant Chemotherapy Radiation Therapy Reduces Local Recurrence No Improvement in Survival 1 Staging Mediastinal
Principles of Radiation Therapy A Bapsi Chakravarthy, MD Associate e P rofessor Professor Radiation Oncology
 Principles of Radiation Therapy A Bapsi Chakravarthy, MD Associate Professor Radiation Oncology Disclosure Information I have no financial relationships to disclose relevant to the conten of this presentation.
Principles of Radiation Therapy A Bapsi Chakravarthy, MD Associate Professor Radiation Oncology Disclosure Information I have no financial relationships to disclose relevant to the conten of this presentation.
Surgery. Wedge resection only part of the lung, not. not a lobe, is removed. Cancer Council NSW
 The treatment you receive will depend on your lung cancer type, for example, whether you have a non-small cell lung cancer Adenocarcinoma or Squamous cell carcinoma, and if this is a sub-type with a mutation.
The treatment you receive will depend on your lung cancer type, for example, whether you have a non-small cell lung cancer Adenocarcinoma or Squamous cell carcinoma, and if this is a sub-type with a mutation.
Mesothelioma. 1. Introduction. 1.1 General Information and Aetiology
 Mesothelioma 1. Introduction 1.1 General Information and Aetiology Mesotheliomas are tumours that arise from the mesothelial cells of the pleura, peritoneum, pericardium or tunica vaginalis [1]. Most are
Mesothelioma 1. Introduction 1.1 General Information and Aetiology Mesotheliomas are tumours that arise from the mesothelial cells of the pleura, peritoneum, pericardium or tunica vaginalis [1]. Most are
General Information About Non-Small Cell Lung Cancer
 General Information About Non-Small Cell Lung Cancer Non-small cell lung cancer is a disease in which malignant (cancer) cells form in the tissues of the lung. The lungs are a pair of cone-shaped breathing
General Information About Non-Small Cell Lung Cancer Non-small cell lung cancer is a disease in which malignant (cancer) cells form in the tissues of the lung. The lungs are a pair of cone-shaped breathing
Adiuwantowe i neoadiuwantowe leczenie chorych na zaawansowanego raka żołądka
 Adiuwantowe i neoadiuwantowe leczenie chorych na zaawansowanego raka żołądka Neoadiuvant and adiuvant therapy for advanced gastric cancer Franco Roviello, IT Neoadjuvant and adjuvant therapy for advanced
Adiuwantowe i neoadiuwantowe leczenie chorych na zaawansowanego raka żołądka Neoadiuvant and adiuvant therapy for advanced gastric cancer Franco Roviello, IT Neoadjuvant and adjuvant therapy for advanced
3.0 With final Comments for presentation at Sub Group Meeting 24. 24.11.10
 Guideline for the Treatment of Lung Cancer Version History 2.0 Endorsed by the Governance Committee as treatment of lung cancer 27.07.09 with radiotherapy and chemotherapy. 2.1 Re-written to include the
Guideline for the Treatment of Lung Cancer Version History 2.0 Endorsed by the Governance Committee as treatment of lung cancer 27.07.09 with radiotherapy and chemotherapy. 2.1 Re-written to include the
Innovative RT SBRT. The variables with REQ in superscript are required.
 The variables with REQ in superscript are required. The variables with a are single-select variables; only one answer can be selected. The variables with a are multi-select variables; multiple answers
The variables with REQ in superscript are required. The variables with a are single-select variables; only one answer can be selected. The variables with a are multi-select variables; multiple answers
Current Status and Perspectives of Radiation Therapy for Breast Cancer
 Breast Cancer Current Status and Perspectives of Radiation Therapy for Breast Cancer JMAJ 45(10): 434 439, 2002 Masahiro HIRAOKA, Masaki KOKUBO, Chikako YAMAMOTO and Michihide MITSUMORI Department of Therapeutic
Breast Cancer Current Status and Perspectives of Radiation Therapy for Breast Cancer JMAJ 45(10): 434 439, 2002 Masahiro HIRAOKA, Masaki KOKUBO, Chikako YAMAMOTO and Michihide MITSUMORI Department of Therapeutic
Radioterapia panencefalica. Umberto Ricardi
 Radioterapia panencefalica Umberto Ricardi Background Systemic disease to the brain is unfortunately a quite common event Radiotherapy, especially with the great technical development during the past decades,
Radioterapia panencefalica Umberto Ricardi Background Systemic disease to the brain is unfortunately a quite common event Radiotherapy, especially with the great technical development during the past decades,
Corso Integrato di Clinica Medica ONCOLOGIA MEDICA AA 2010-2011 LUNG CANCER. IV. THERAPY. I. NON SMALL CELL LUNG CANCER Prof.
 Corso Integrato di Clinica Medica ONCOLOGIA MEDICA AA 2010-2011 LUNG CANCER. IV. THERAPY. I. NON SMALL CELL LUNG CANCER Prof. Alberto Riccardi TREATMENT OF LUNG CARCINOMA * overall treatment approach to
Corso Integrato di Clinica Medica ONCOLOGIA MEDICA AA 2010-2011 LUNG CANCER. IV. THERAPY. I. NON SMALL CELL LUNG CANCER Prof. Alberto Riccardi TREATMENT OF LUNG CARCINOMA * overall treatment approach to
Non-Small Cell Lung Cancer Therapies
 Non-Small Cell Lung Cancer Therapies Guest Expert: Roy, MD, PhD Assistant Professor of Therapeutic Radiology Scott, MD Assistant Professor of Medical Oncology www.wnpr.org www.yalecancercenter.org Welcome
Non-Small Cell Lung Cancer Therapies Guest Expert: Roy, MD, PhD Assistant Professor of Therapeutic Radiology Scott, MD Assistant Professor of Medical Oncology www.wnpr.org www.yalecancercenter.org Welcome
National Clinical Trials Network Groups Update Fall 2014
 National Clinical Trials Network Groups Update Fall 2014 Walter J Curran, Jr, MD An NRG Oncology Group Chair Executive Director Winship Cancer Institute of Emory University Atlanta, GA NCTN Groups Update
National Clinical Trials Network Groups Update Fall 2014 Walter J Curran, Jr, MD An NRG Oncology Group Chair Executive Director Winship Cancer Institute of Emory University Atlanta, GA NCTN Groups Update
Approccio multidisciplinare nei tumori del retto
 Approccio multidisciplinare nei tumori del retto F. Muñoz Radiation Oncology Department University of Torino, Italy RECENT CHANGES IN RECTAL CANCER DIAGNOSIS AND THERAPY Optimal staging by EUS and MRI
Approccio multidisciplinare nei tumori del retto F. Muñoz Radiation Oncology Department University of Torino, Italy RECENT CHANGES IN RECTAL CANCER DIAGNOSIS AND THERAPY Optimal staging by EUS and MRI
Concurrent Chemotherapy and Radiotherapy for Head and Neck Cancer
 Concurrent Chemotherapy and Radiotherapy for Head and Neck Cancer Ryan J. Burri; Nancy Y. Lee Published: 03/23/2009 Abstract and Introduction Abstract Head and neck cancer is best managed in a multidisciplinary
Concurrent Chemotherapy and Radiotherapy for Head and Neck Cancer Ryan J. Burri; Nancy Y. Lee Published: 03/23/2009 Abstract and Introduction Abstract Head and neck cancer is best managed in a multidisciplinary
Brain Tumor Treatment
 Scan for mobile link. Brain Tumor Treatment Brain Tumors Overview A brain tumor is a group of abnormal cells that grows in or around the brain. Tumors can directly destroy healthy brain cells. They can
Scan for mobile link. Brain Tumor Treatment Brain Tumors Overview A brain tumor is a group of abnormal cells that grows in or around the brain. Tumors can directly destroy healthy brain cells. They can
Management of Stage III, N2 NSCLC: A Virtual Thoracic Oncology Tumor Board
 Management of Stage III, N2 NSCLC: A Virtual Thoracic Oncology Tumor Board Abstract Introduction Management of stage III non small-cell lung cancer (NSCLC) is complex and requires careful work-up, staging,
Management of Stage III, N2 NSCLC: A Virtual Thoracic Oncology Tumor Board Abstract Introduction Management of stage III non small-cell lung cancer (NSCLC) is complex and requires careful work-up, staging,
a commitment in their practice to the roles and responsibilities of clinical oncologists X
 CLINICAL ONCOLOGY BLUEPRINT OF ASSESSMENT SYSTEM Good Medical Practice areas of curriculum - ST5 (Intermediate) Standards GMP criterion Workplace based assessment By the end of the third year of training
CLINICAL ONCOLOGY BLUEPRINT OF ASSESSMENT SYSTEM Good Medical Practice areas of curriculum - ST5 (Intermediate) Standards GMP criterion Workplace based assessment By the end of the third year of training
Radiotherapy in Lung Cancer. Dr. Vassilis Kouloulias. Radiotherapy in lung cancer. Dr. V. Kouloulias
 Radiotherapy in Lung Cancer Dr. Vassilis Kouloulias Assistant Professor of Radiation Oncologist, 2 nd Dpt. Radiology, University of Athens, Greece. Key Words Small cell lung cancer (SCLC), Non-small cell
Radiotherapy in Lung Cancer Dr. Vassilis Kouloulias Assistant Professor of Radiation Oncologist, 2 nd Dpt. Radiology, University of Athens, Greece. Key Words Small cell lung cancer (SCLC), Non-small cell
Lung Cancer Treatment
 Scan for mobile link. Lung Cancer Treatment Lung cancer overview More than one in four of all diagnosed cancers involve the lung, and lung cancer remains the most common cancer-related cause of death among
Scan for mobile link. Lung Cancer Treatment Lung cancer overview More than one in four of all diagnosed cancers involve the lung, and lung cancer remains the most common cancer-related cause of death among
Lung Cancer: Diagnosis, Staging and Treatment
 PATIENT EDUCATION patienteducation.osumc.edu Lung Cancer: Diagnosis, Staging and Treatment Cancer begins in our cells. Cells are the building blocks of our tissues. Tissues make up the organs of the body.
PATIENT EDUCATION patienteducation.osumc.edu Lung Cancer: Diagnosis, Staging and Treatment Cancer begins in our cells. Cells are the building blocks of our tissues. Tissues make up the organs of the body.
FOLLOW UP OF TREATED NON-SMALL CELL LUNG CANCER PATIENTS
 FOLLOW UP OF TREATED NON-SMALL CELL LUNG CANCER PATIENTS THE ART AND THE SCIENCE GIOVANNI BATTISTA MORGAGNI 1682-1771 ITALIAN ANATOMIST FATHER OF PATHOLOGIC ANATOMY 1 ST DESCRIPTION OF LUNG CANCER IN 1761
FOLLOW UP OF TREATED NON-SMALL CELL LUNG CANCER PATIENTS THE ART AND THE SCIENCE GIOVANNI BATTISTA MORGAGNI 1682-1771 ITALIAN ANATOMIST FATHER OF PATHOLOGIC ANATOMY 1 ST DESCRIPTION OF LUNG CANCER IN 1761
Lung Cancer. This reference summary will help you better understand lung cancer and the treatment options that are available.
 Lung Cancer Introduction Lung cancer is the number one cancer killer of men and women. Over 165,000 people die of lung cancer every year in the United States. Most cases of lung cancer are related to cigarette
Lung Cancer Introduction Lung cancer is the number one cancer killer of men and women. Over 165,000 people die of lung cancer every year in the United States. Most cases of lung cancer are related to cigarette
Malignant Mesothelioma State of the Art
 Malignant Mesothelioma State of the Art Paul Baas The Netherlands Cancer Institute August 12, 2011, Carlsbad, CA Summary Diagnosis; epithelial type subdivided Pleiomorphic vs other Staging: IASLC-IMIG
Malignant Mesothelioma State of the Art Paul Baas The Netherlands Cancer Institute August 12, 2011, Carlsbad, CA Summary Diagnosis; epithelial type subdivided Pleiomorphic vs other Staging: IASLC-IMIG
7. Prostate cancer in PSA relapse
 7. Prostate cancer in PSA relapse A patient with prostate cancer in PSA relapse is one who, having received a primary treatment with intent to cure, has a raised PSA (prostate-specific antigen) level defined
7. Prostate cancer in PSA relapse A patient with prostate cancer in PSA relapse is one who, having received a primary treatment with intent to cure, has a raised PSA (prostate-specific antigen) level defined
Mesothelioma. Malignant Pleural Mesothelioma
 Mesothelioma William G. Richards, PhD Brigham and Women s Hospital Malignant Pleural Mesothelioma 2,000-3,000 cases per year (USA) Increasing incidence Asbestos (50-80%, decreasing) 30-40 year latency
Mesothelioma William G. Richards, PhD Brigham and Women s Hospital Malignant Pleural Mesothelioma 2,000-3,000 cases per year (USA) Increasing incidence Asbestos (50-80%, decreasing) 30-40 year latency
بسم هللا الرحمن الرحيم
 بسم هللا الرحمن الرحيم Updates in Mesothelioma By Samieh Amer, MD Professor of Cardiothoracic Surgery Faculty of Medicine, Cairo University History Wagner and his colleagues (1960) 33 cases of mesothelioma
بسم هللا الرحمن الرحيم Updates in Mesothelioma By Samieh Amer, MD Professor of Cardiothoracic Surgery Faculty of Medicine, Cairo University History Wagner and his colleagues (1960) 33 cases of mesothelioma
POLICY A. INDICATIONS
 Alimta (pemetrexed) Line(s) of Business: HMO; PPO; QUEST Integration Akamai Advantage Original Effective Date: 09/01/2007 Current Effective Date: 10/01/2015 POLICY A. INDICATIONS The indications below
Alimta (pemetrexed) Line(s) of Business: HMO; PPO; QUEST Integration Akamai Advantage Original Effective Date: 09/01/2007 Current Effective Date: 10/01/2015 POLICY A. INDICATIONS The indications below
The Need for Accurate Lung Cancer Staging
 The Need for Accurate Lung Cancer Staging Peter Baik, DO Thoracic Surgery Cancer Treatment Centers of America Oklahoma Osteopathic Association 115th Annual Convention Financial Disclosures: None 2 Objectives
The Need for Accurate Lung Cancer Staging Peter Baik, DO Thoracic Surgery Cancer Treatment Centers of America Oklahoma Osteopathic Association 115th Annual Convention Financial Disclosures: None 2 Objectives
Rotation Specific Goals & Objectives: University Health Network-Princess Margaret Hospital/ Sunnybrook Breast/Melanoma
 Rotation Specific Goals & Objectives: University Health Network-Princess Margaret Hospital/ Sunnybrook Breast/Melanoma Medical Expert: Breast Rotation Specific Competencies/Objectives 1.0 Medical History
Rotation Specific Goals & Objectives: University Health Network-Princess Margaret Hospital/ Sunnybrook Breast/Melanoma Medical Expert: Breast Rotation Specific Competencies/Objectives 1.0 Medical History
Guidelines on the radical management of patients with lung cancer A Quick Reference Guide
 ISSN 2040-2023 October 2010 Guidelines on the radical management of patients with lung cancer A Quick Reference Guide British Thoracic Society GUIDELINES ON THE RADICAL MANAGEMENT OF PATIENTS WITH LUNG
ISSN 2040-2023 October 2010 Guidelines on the radical management of patients with lung cancer A Quick Reference Guide British Thoracic Society GUIDELINES ON THE RADICAL MANAGEMENT OF PATIENTS WITH LUNG
Radiotherapy in Plasmacytoma and Myeloma. David Cutter Multiple Myeloma NSSG Annual Meeting 14 th September 2015
 Radiotherapy in Plasmacytoma and Myeloma David Cutter Multiple Myeloma NSSG Annual Meeting 14 th September 2015 Contents Indications for radiotherapy: Palliation in Multiple Myeloma Solitary Bone Plasmacytoma
Radiotherapy in Plasmacytoma and Myeloma David Cutter Multiple Myeloma NSSG Annual Meeting 14 th September 2015 Contents Indications for radiotherapy: Palliation in Multiple Myeloma Solitary Bone Plasmacytoma
INTRODUCTION. liver neoplasms, adrenal gland neoplasms, non small-cell lung cancer, radionuclide imaging, bisphosphonates,
 VOLUME 22 NUMBER 2 JANUARY 15 2004 JOURNAL OF CLINICAL ONCOLOGY A S C O S P E C I A L A R T I C L E American Society of Clinical Oncology Treatment of Unresectable Non Small-Cell Lung Cancer Guideline:
VOLUME 22 NUMBER 2 JANUARY 15 2004 JOURNAL OF CLINICAL ONCOLOGY A S C O S P E C I A L A R T I C L E American Society of Clinical Oncology Treatment of Unresectable Non Small-Cell Lung Cancer Guideline:
Malignant Mesothelioma: an Update
 Malignant Mesothelioma: an Update Nico van Zandwijk Asbestos Diseases Research Institute Bernie Banton Centre University of Sydney Australia Physicians Week RACP 19-5-2009 Health Risks of Asbestos Fibers
Malignant Mesothelioma: an Update Nico van Zandwijk Asbestos Diseases Research Institute Bernie Banton Centre University of Sydney Australia Physicians Week RACP 19-5-2009 Health Risks of Asbestos Fibers
2.2.5 Target Volumes in Small Cell Lung Cancer
 Target Volumes in Small Cell Lung Cancer 111 2.2.5 Target Volumes in Small Cell Lung Cancer Yolanda I. Garces and James A. Bonner CONTENTS 2.2.5.1 Introduction 111 2.2.5.2 Tumor Volume Definitions 111
Target Volumes in Small Cell Lung Cancer 111 2.2.5 Target Volumes in Small Cell Lung Cancer Yolanda I. Garces and James A. Bonner CONTENTS 2.2.5.1 Introduction 111 2.2.5.2 Tumor Volume Definitions 111
Case Number: RT2009-124(M) Potential Audiences: Intent Doctor, Oncology Special Nurse, Resident Doctor
 Potential Audiences: Intent Doctor, Oncology Special Nurse, Resident Doctor") Renal Cell Carcinoma of the Left Kidney Post Radical Surgery with pt4 Classification with Multiple Lung and Single Brain Metastases: the Role and Treatment Consideration of Radiotherapy Case Number: RT2009-124(M)
Renal Cell Carcinoma of the Left Kidney Post Radical Surgery with pt4 Classification with Multiple Lung and Single Brain Metastases: the Role and Treatment Consideration of Radiotherapy Case Number: RT2009-124(M)
How To Know When To Stage Lung Cancer
 WHITE PAPER - SBRT for Non Small Cell Lung Cancer I. Introduction This white paper will focus on non-small cell lung carcinoma with sections one though six comprising a general review of lung cancer from
WHITE PAPER - SBRT for Non Small Cell Lung Cancer I. Introduction This white paper will focus on non-small cell lung carcinoma with sections one though six comprising a general review of lung cancer from
Implementation Date: April 2015 Clinical Operations
 National Imaging Associates, Inc. Clinical guideline PROSTATE CANCER Original Date: March 2011 Page 1 of 5 Radiation Oncology Last Review Date: March 2015 Guideline Number: NIA_CG_124 Last Revised Date:
National Imaging Associates, Inc. Clinical guideline PROSTATE CANCER Original Date: March 2011 Page 1 of 5 Radiation Oncology Last Review Date: March 2015 Guideline Number: NIA_CG_124 Last Revised Date:
Diagnosis and multimodality management of stage III non-small cell lung cancer Review Article
 Cancer Therapy Vol 6, page 81 Cancer Therapy Vol 6, 81-94, 2008 Diagnosis and multimodality management of stage III non-small cell lung cancer Review Article Kevin Sullivan, Zujun Li, John Rescigno, Michael
Cancer Therapy Vol 6, page 81 Cancer Therapy Vol 6, 81-94, 2008 Diagnosis and multimodality management of stage III non-small cell lung cancer Review Article Kevin Sullivan, Zujun Li, John Rescigno, Michael
Primary -Benign - Malignant Secondary
 TUMOURS OF THE LUNG Primary -Benign - Malignant Secondary The incidence of lung cancer has been increasing almost logarithmically and is now reaching epidemic levels. The overall cure rate is very low
TUMOURS OF THE LUNG Primary -Benign - Malignant Secondary The incidence of lung cancer has been increasing almost logarithmically and is now reaching epidemic levels. The overall cure rate is very low
Detection and staging of recurrent prostate cancer is still one of the important clinical problems in prostate cancer. A rise in PSA or biochemical
 Summary. 111 Detection and staging of recurrent prostate cancer is still one of the important clinical problems in prostate cancer. A rise in PSA or biochemical recurrence (BCR) is the first sign of recurrent
Summary. 111 Detection and staging of recurrent prostate cancer is still one of the important clinical problems in prostate cancer. A rise in PSA or biochemical recurrence (BCR) is the first sign of recurrent
Tricia Cox on 7/18/2012 at Oncology Center. Sarah Randolf. Female
 SAMPLE This Survivorship Care Plan will facilitate cancer care following active treatment. It may include important contact information, a treatment summary, recommendations for follow-up care testing,
SAMPLE This Survivorship Care Plan will facilitate cancer care following active treatment. It may include important contact information, a treatment summary, recommendations for follow-up care testing,
Calculation of Contra-lateral Lung Doses in Thoracic IMRT: An Experimental Evaluation
 Calculation of Contra-lateral Lung Doses in Thoracic IMRT: An Experimental Evaluation Deborah Schofield, Laurence Court, Aaron Allen, Fred Hacker, Maria Czerminska Department of Radiation Oncology Dana
Calculation of Contra-lateral Lung Doses in Thoracic IMRT: An Experimental Evaluation Deborah Schofield, Laurence Court, Aaron Allen, Fred Hacker, Maria Czerminska Department of Radiation Oncology Dana
Non-Small Cell Lung Cancer
 Non-Small Cell Lung Cancer John delcharco, MD (Statistics based on CVMC data 2009-2013) Statistics Lung cancer is the leading cause of cancer deaths in the United States. The American Cancer Society estimates
Non-Small Cell Lung Cancer John delcharco, MD (Statistics based on CVMC data 2009-2013) Statistics Lung cancer is the leading cause of cancer deaths in the United States. The American Cancer Society estimates
Protein kinase C alpha expression and resistance to neo-adjuvant gemcitabine-containing chemotherapy in non-small cell lung cancer
 Protein kinase C alpha expression and resistance to neo-adjuvant gemcitabine-containing chemotherapy in non-small cell lung cancer Dan Vogl Lay Abstract Early stage non-small cell lung cancer can be cured
Protein kinase C alpha expression and resistance to neo-adjuvant gemcitabine-containing chemotherapy in non-small cell lung cancer Dan Vogl Lay Abstract Early stage non-small cell lung cancer can be cured
5. Non small Cell Lung Cancer
 5. Non small Cell Lung Cancer Introduction The cancer registry in Sweden shows a continuous increase of lung cancer cases from 867 in 1958 when the registry started to 2 846 in 2000. The Swedish cancer
5. Non small Cell Lung Cancer Introduction The cancer registry in Sweden shows a continuous increase of lung cancer cases from 867 in 1958 when the registry started to 2 846 in 2000. The Swedish cancer
Understanding Your Surgical Options for Lung Cancer
 Information Booklet for Patients Understanding Your Surgical Options for Lung Cancer Understanding Lung Cancer If you have just been diagnosed with lung cancer, this booklet will serve as an informational
Information Booklet for Patients Understanding Your Surgical Options for Lung Cancer Understanding Lung Cancer If you have just been diagnosed with lung cancer, this booklet will serve as an informational
Rectal Cancer. To Radiate or not to radiate? Q: Should rectal cancer RT/CRT decisions be based solely on stage? 11/09/2014
 Rectal Cancer To Radiate or not to radiate?? Dr. Corinne Doll Radiation Oncologist Tom Baker Cancer Centre Calgary, Alberta Q: Should rectal cancer RT/CRT decisions be based solely on stage? 1 Q: Can RT/CRT
Rectal Cancer To Radiate or not to radiate?? Dr. Corinne Doll Radiation Oncologist Tom Baker Cancer Centre Calgary, Alberta Q: Should rectal cancer RT/CRT decisions be based solely on stage? 1 Q: Can RT/CRT
Definitive Treatment of Poor-Risk Patients with Stage I Lung Cancer. A Single Institution Experience
 ORIGINAL ARTICLE Definitive Treatment of Poor-Risk Patients with Stage I Lung Cancer A Single Institution Experience Michael Hsie, MD,* Stefania Morbidini-Gaffney, MD,* Leslie J. Kohman, MD, Elisabeth
ORIGINAL ARTICLE Definitive Treatment of Poor-Risk Patients with Stage I Lung Cancer A Single Institution Experience Michael Hsie, MD,* Stefania Morbidini-Gaffney, MD,* Leslie J. Kohman, MD, Elisabeth
Avastin: Glossary of key terms
 Avastin: Glossary of key terms Adenocarcinoma Adenoma Adjuvant therapy Angiogenesis Anti-angiogenics Antibody Antigen Avastin (bevacizumab) Benign A form of carcinoma that originates in glandular tissue.
Avastin: Glossary of key terms Adenocarcinoma Adenoma Adjuvant therapy Angiogenesis Anti-angiogenics Antibody Antigen Avastin (bevacizumab) Benign A form of carcinoma that originates in glandular tissue.
Management of Postmenopausal Women with T1 ER+ Tumors: Options and Tradeoffs. Case Study. Surgery. Lumpectomy and Radiation
 Management of Postmenopausal Women with T1 ER+ Tumors: Options and Tradeoffs Michael Alvarado, MD Associate Professor of Surgery University of California San Francisco Case Study 59 yo woman with new palpable
Management of Postmenopausal Women with T1 ER+ Tumors: Options and Tradeoffs Michael Alvarado, MD Associate Professor of Surgery University of California San Francisco Case Study 59 yo woman with new palpable
New Trends & Current Research in the Treatment of Lung Cancer, Pt. II
 New Trends & Current esearch in the Treatment of Lung Cancer, Pt. II Howard (Jack) West, MD President & CEO, GACE Medical Director, Thoracic Oncology Program Swedish Cancer Institute Seattle, WA Cancer
New Trends & Current esearch in the Treatment of Lung Cancer, Pt. II Howard (Jack) West, MD President & CEO, GACE Medical Director, Thoracic Oncology Program Swedish Cancer Institute Seattle, WA Cancer
Small cell lung cancer
 Small cell lung cancer Small cell lung cancer is a disease in which malignant (cancer) cells form in the tissues of the lung. The lungs are a pair of cone-shaped breathing organs that are found within
Small cell lung cancer Small cell lung cancer is a disease in which malignant (cancer) cells form in the tissues of the lung. The lungs are a pair of cone-shaped breathing organs that are found within
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES LUNG SITE LUNG CANCER Lung Site Group Lung Cancer Authors: Dr. Meredith Giuliani, Dr. Andrea Bezjak 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES LUNG SITE LUNG CANCER Lung Site Group Lung Cancer Authors: Dr. Meredith Giuliani, Dr. Andrea Bezjak 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING
the standard of care 2009 5/1/2009 Mesothelioma: The standard of care take home messages PILC 2006 Jan.vanmeerbeeck@ugent.be Brussels, March 7, 2009
 Mesothelioma: The standard of care Jan.vanmeerbeeck@ugent.be Brussels, March 7, 2009 take home messages PILC 2006 All patients should receive adequate palliation of dyspnea and pain before starting chemotherapy
Mesothelioma: The standard of care Jan.vanmeerbeeck@ugent.be Brussels, March 7, 2009 take home messages PILC 2006 All patients should receive adequate palliation of dyspnea and pain before starting chemotherapy
2009 Cancer Committee
 2009 Cancer Committee Lung (non-small cell) Cancer Study Stage IIIA and IIIB John Clouse, M.D. Alicia Stark, RHIT Jeff Robinson Table of Cont ent s Table of Contents... 1 Lung (non-small cell) Cancer Facts.2
2009 Cancer Committee Lung (non-small cell) Cancer Study Stage IIIA and IIIB John Clouse, M.D. Alicia Stark, RHIT Jeff Robinson Table of Cont ent s Table of Contents... 1 Lung (non-small cell) Cancer Facts.2
The National Clinical Lung Cancer Audit (LUCADA)
") The National Clinical Lung Cancer Audit (LUCADA) DATA MANUAL Title: Version: 3.1.5 Date: September 2013 LUCADA Lung Cancer Audit VERSION HISTORY Version Date Issued Brief Summary of Change Owner s Name
The National Clinical Lung Cancer Audit (LUCADA) DATA MANUAL Title: Version: 3.1.5 Date: September 2013 LUCADA Lung Cancer Audit VERSION HISTORY Version Date Issued Brief Summary of Change Owner s Name
Carcinoma of the Cervix. Kathleen M. Schmeler, MD Associate Professor Department of Gynecologic Oncology
 Carcinoma of the Cervix Kathleen M. Schmeler, MD Associate Professor Department of Gynecologic Oncology Cervical Cancer Treatment Treatment Microinvasive (Stage IA1): Simple (extrafascial) hysterectomy/cone
Carcinoma of the Cervix Kathleen M. Schmeler, MD Associate Professor Department of Gynecologic Oncology Cervical Cancer Treatment Treatment Microinvasive (Stage IA1): Simple (extrafascial) hysterectomy/cone
Radiation Therapy and Esophageal Cancer
 Neoadjuvant chemoradiotherapy followed by surgical resection is the current standard of care for localized cancer of the esophagus. Samuel Bak. BK1509 Questionable. Oil on canvas, 18ʺ 24ʺ. Radiation Therapy
Neoadjuvant chemoradiotherapy followed by surgical resection is the current standard of care for localized cancer of the esophagus. Samuel Bak. BK1509 Questionable. Oil on canvas, 18ʺ 24ʺ. Radiation Therapy
Corporate Medical Policy Intensity-Modulated Radiation Therapy (IMRT) of the Prostate
 of the Prostate") Corporate Medical Policy Intensity-Modulated Radiation Therapy (IMRT) of the Prostate File Name: Origination: Last CAP Review: Next CAP Review: Last Review: intensity_modulated_radiation_therapy_imrt_of_the_prostate
Corporate Medical Policy Intensity-Modulated Radiation Therapy (IMRT) of the Prostate File Name: Origination: Last CAP Review: Next CAP Review: Last Review: intensity_modulated_radiation_therapy_imrt_of_the_prostate
The evolution of rectal cancer therapy. Objectives
 The evolution of rectal cancer therapy Hagen Kennecke MD MHA FRCPC Western Canada Consensus Conference September 5, 2014 Objectives Identify standard therapy: stage II/III rectal cancer Update recent adjuvant
The evolution of rectal cancer therapy Hagen Kennecke MD MHA FRCPC Western Canada Consensus Conference September 5, 2014 Objectives Identify standard therapy: stage II/III rectal cancer Update recent adjuvant
Altered Fractionation of Radical Radiation Therapy in the Management of Unresectable Non-Small Cell Lung Cancer
 Evidence-based Series #7-12 Version 2 A Quality Initiative of the Program in Evidence-based Care (PEBC), Cancer Care Ontario (CCO) Altered Fractionation of Radical Radiation Therapy in the Management of
Evidence-based Series #7-12 Version 2 A Quality Initiative of the Program in Evidence-based Care (PEBC), Cancer Care Ontario (CCO) Altered Fractionation of Radical Radiation Therapy in the Management of