CHEST Antithrombotic Therapy and Prevention of Thrombosis, 9 th ed Sarah Meyer, PharmD November 9, 2012
|
|
|
- Bernard Booker
- 8 years ago
- Views:
Transcription
1 CHEST Antithrombotic Therapy and Prevention of Thrombosis, 9 th ed Sarah Meyer, PharmD November 9, CHEST has made a few changes 1 a. For patients sufficiently healthy to be treated as outpatients, we suggest initiating vitamin K antagonist (VKA) therapy with warfarin 10 mg daily for the first 2 days followed by dosing based on international normalized ratio (INR) measurements, rather than starting with the estimated maintenance dose. b. For patients taking VKA therapy with consistently stable INRs, we suggest an INR testing frequency of up to 12 weeks rather than every 4 weeks. 2. Abbreviations a. ACCP: American College of Chest Physicians b. CAD: Coronary artery disease c. HF: Heart failure d. INR: International normalized ratio e. TTR: Time in therapeutic range f. VKA: Vitamin K antagonists g. VTE: Venous thromboembolism 3. Objectives a. List the new recommendations b. Identify key research used to formulate recommendations c. Describe the safety concerns associated with the recommendations d. Describe the benefits of the recommendations e. Apply the guidelines to an appropriate population 4. Background 2 a. Anticoagulation use in 2007 in the USA (outpatient, civilian use) i. Anticoagulant use: 24.5 million people ii. Coumadin use: 21.5 million people 5. ACCP 3 a. Guidelines released in February 2012 b. Update from 2008 c. Articles written by a methodologist, typically a practicing physician d. Even more emphasis on patients values and preference e. Recommendations for the diagnosis of DVT 1

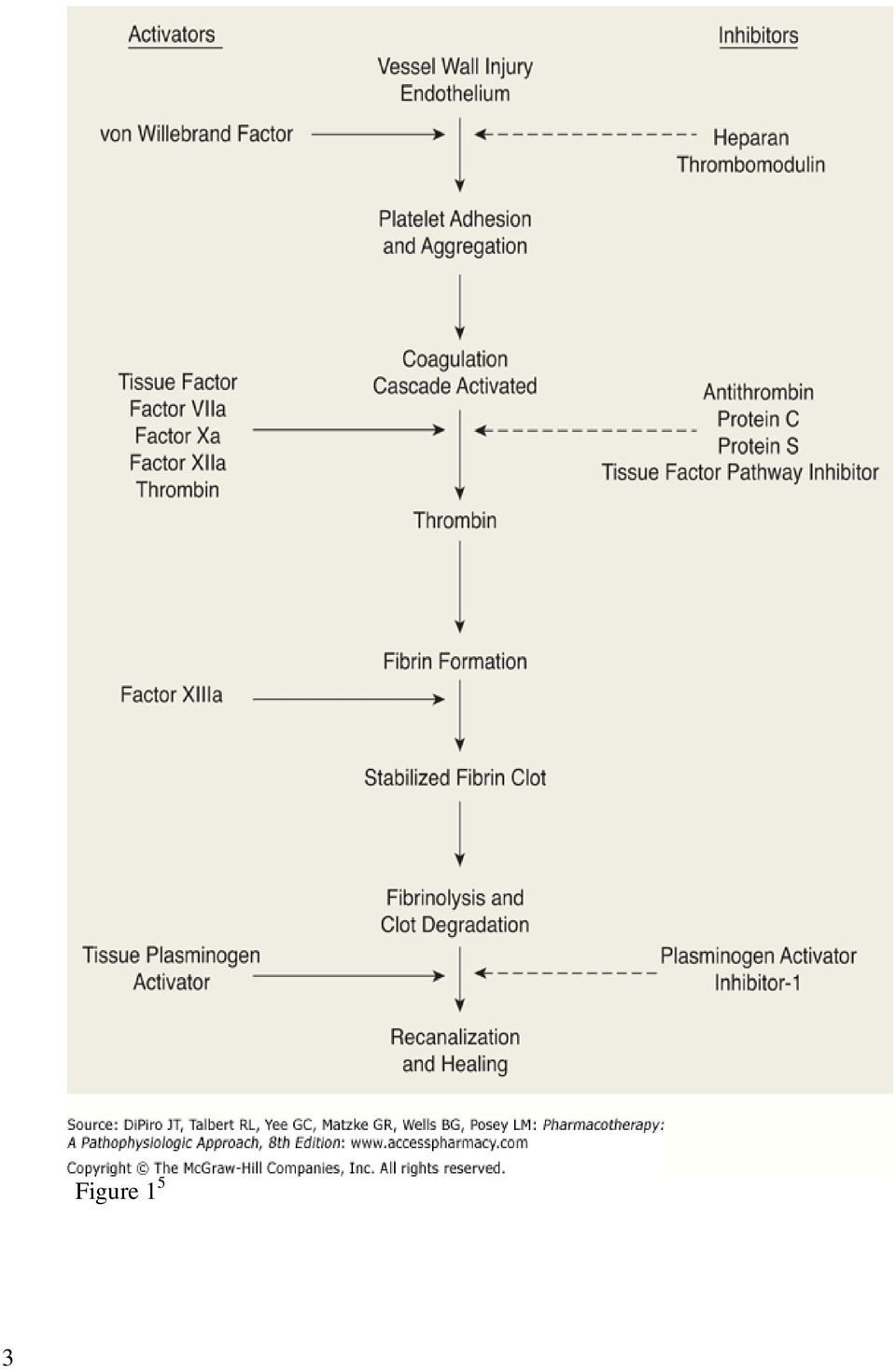
2 6. Recommendations from ACCP 8 th edition 4 a. In patients beginning VKA therapy, we recommend the initiation of oral anticoagulation, with doses between 5 and 10 mg for the first 1 to 2 days for most individuals and subsequent dosing based on INR response. b. For patients who are receiving a stable dose of oral anticoagulants, we suggest monitoring at an interval of no longer than every 4 weeks. Initiating Therapy 1. Mechanism of action of warfarin 5 a. Blocks the regeneration of vitamin K epoxide b. Inhibits synthesis of vitamin K-dependent clotting factors c. Vitamin K-dependent clotting factors: II, VII, IX, X, and anticoagulant proteins C and S 2. How warfarin exerts its effects 6 a. Prothrombin time affected by factors II, VII, and X b. Anticoagulant effect due to depletion of factor VII i. Factor VII half-life = 6 hours c. Antithrombotic effect of warfarin due to reduction of factor II i. Factor II half-life = 60 hours d. Procoagulant effect due to depletion of protein C i. Protein C half-life = 6 hours 2

3 3 Figure 1 5
4 Table 1 6 Comparison of 5-mg and 10-mg Loading Doses in Initiation of Warfarin Therapy Harrison L, RN; Johnston M, ART; Massicotte MP, MD; et al. Ann Intern Med. 1997;126: Background Objective Outcome Measures Patients are often initiated on warfarin using a 10 mg loading dose as opposed to starting with an average maintenance dose of 5 mg. Due to the mechanism by which warfarin creates an anticoagulant and antithrombotic effect, patients may reach a therapeutic INR without having antithrombotic protection. To compare the effect of 5- and 10-mg loading doses of warfarin on laboratory markers of warfarin s anticoagulant effect. Time to achieve an INR of Proportion of INRs greater than 3.0 Time for reduction in levels of factors II, X, VII, IX, and protein C Methods Randomized control trial Patients with no contraindications to warfarin and needing anticoagulation in a tertiary teaching hospital in Ontario, Canada Followed for a maximum 108 hours, receiving 5 dose of warfarin Blood samples taken before warfarin, 12 hours after the first dose, and every 24 hours for 5 days 25 patients received a 10-mg loading dose for two days 24 patients received a 5-mg loading dose for two days A nomogram was used to adjust all warfarin doses starting on study day two 48 patients received concomitant heparin Data Analysis 95% confidence intervals used No additional information reported Results Rate of decline in factors II and X did not differ significantly Levels of factor VII and protein C decreased significantly more rapidly in the 10 mg group at 36 and 60 hours At 36 hours, 11 of 25 (44%, [CI, 34-54%]) in the 10 mg group and 2 of 24 (8%, [CI 3-14%]) in the 5 mg group had INR s greater than 2.0 (p=0.005) At 60 hours, 9 of 25 (36%, [CI 17-54%]) of the 10 mg group and none of the patients in the 5 mg group had INRs greater than 3.0 (p=0.002) At 60 hours, 10 patients in the 5 mg group and 9 patients in the 10 mg group had INRs of Vitamin K was given to 4 of the 10 mg group patients and 1 of the 5 mg group patients, no patient bled. Limitations Used surrogate markers for safety and efficacy Very limited information on data analysis provided Conclusion A 5-mg loading dose of warfarin results in less excess anticoagulation compared to a 10-mg loading dose, and avoids a possibly hypercoagulable state seen when protein C is substantially reduced before factors II and X. 4

5 Table 2 8 A Randomized Trial Comparing 5-mg and 10-mg Warfarin Loading Doses Crowther MA, MD; Ginsberg JB, MD; Kearon C, MD; et al. Arch Intern Med. 1999;159: Background In the past, warfarin therapy has been initiated using a loading dose to expedite the time needed to reach a therapeutic INR. This group found in a previous study that initiating therapy with 5 mg was just as effective as giving a loading dose of 10 Objective Outcome Measures mg in achieving time to a therapeutic INR. To confirm that initiating warfarin therapy with a 5 mg loading dose is as effective as initiating with a 10 mg loading dose. Proportion of patients whose INR never exceeded 3.0 Proportion of patients who had INR values between on two consecutive daily tests on days 3 and 4 or 4 and 5 of the study Methods Randomized trial Patients with no contraindications to warfarin and geographically accessible, seen in a hospital in Ontario, Canada Patients had daily INR tests drawn until they were either therapeutic for two consecutive days, received phytonadione, or 108 hours had passed 32 patients received a 5 mg loading dose for two days 21 patients received a 10 mg loading dose for two days Subsequent doses were given based on a nomogram Patients received concomitant anticoagulation therapy Data Proportions, 95% confidence intervals, relative risks used Analysis Fisher exact test or χ 2 test for comparison of proportions Results Proportion of patients within range was higher at all points during observation with the 5 mg group than the 10 mg group Primary endpoint achieved by 5 of the 21 patients (24%) in the 10 mg group and 21 of the 32 patients (66%) in the 5 mg group (RR, 2.22; 95% CI, [p<0.003]) Limitations INR of used as a surrogate marker for safety and efficacy Conclusion Initiating patients on 5 mg of warfarin as opposed to 10 mg does not increase the time to a therapeutic INR of 2.0 to 3.0 on day 3, 4, or 5 of therapy. 5

6 Table 3 9 Comparison of 10-mg and 5-mg Warfarin Initiation Nomograms Together with Low- Molecular-Weight Heparin for Outpatient Treatment of Acute Venous Thromboembolism Kovacs MJ, MD, FRCPC; Rodger M, MD, FRCPC, MSc; Anderson DR, MD, FRCPC, MSc, et al. Ann Intern Med. 2003;138: Background Nomograms should be used to initiate warfarin in order to safely achieve a therapeutic INR. This group had previously created a 10-mg nomogram, but it required daily INR tests. Revision of the nomogram to reduce INR tests has proved successful. Objective To compare the effectiveness and feasibility of a warfarin nomogram using a 10- mg loading dose with a nomogram using a 5-mg loading dose for the management of outpatients with acute VTE. Outcome Time in days to an INR >1.9 Measures Proportion of patients with INRs of on day 5 Incidence of recurrent VTE within 90 days of diagnosis Incidence of major bleeding within 28 days of diagnosis Number of INRs > 5.0 Number of INR tests in the first 28 days 90 day survival Methods Randomized, double-blind, controlled trial Patients with a diagnosis of acute VTE INRs tests drawn on days 3, 4, and 5. Daily INR tests were drawn if the patient was not therapeutic by day patients received a 10 mg loading dose for two days 97 patients received a 5 mg loading dose for two days Subsequent doses were given based on the respective nomogram Patients were followed for 90 days Data Intention to treat Analysis Mean TTR comparison using the unpaired Student t-test Proportions compared using the unadjusted chi-squared test Two-sided significance tests A P value less than 0.05 considered significant Results Mean time to INR > 1.9 (days): 4.2 ± 1.1 for the 10 mg group, and 5.6 ± 1.4 for the 5 mg group, p < Patients with INR of by day 5: 86 (83% [95% CI 74-89]) in the 10 mg group, and 45(46% [95% CI ]) in the 5 mg group, p < Mean INR tests in the first 28 days: 8.1 ± 2.4 in the 10 mg group, and 5.6 ± 1.4 in the 5 mg group, p = 0.04 No other results statistically significant Limitations Underpowered for clinical endpoints, so no safe conclusions can be drawn from the lack of statistical difference Participating patients not at high risk of bleeding Conclusion The 10-mg nomogram is superior to the 5-mg nomogram because it allows more outpatients to achieve a therapeutic INR in a shorter amount of time. 6

7 Table 4 6,7,8,9,10,11 Trials Study Design Primary Monkman K, et al. Thromb Res 2009;124(3): Wells PS, et al. Blood Coagu Fibrinolysis 2009; 20(6): Kovacs MJ, et al. Ann Intern Med 2003;138(9): Crowther MA, et al. Arch Intern Med 1999;159(1):46-48 Harrison L, et al. Ann Intern Med 1997;126(2): Quiroz R, et al. Am J Cardiol 2006;98(4): Retrospective chart reviews and randomized control trial Approximately 1,050 charts reviewed 210 patients included in trial Randomized control trials Approximately 100 patients total Primarily inpatients Open label, randomized trial 50 patients included 322 patients excluded Endpoints 90 day cumulative incidence of recurrent VTE Effectiveness and safety of using a 10-mg nomogram in real life practice Time in days to a therapeutic INR (>1.9) Comparing the abilities of a 5- and 10-mg nomogram to reach a stable INR in 5 days The effects of 5- and 10-mg loading doses on surrogate laboratory markers for safety and efficacy Number of days required to achieve 2 consecutive INRs > 1.9 Results 8/414 recurrent VTEs within 90 days in patients using 10 mg nomogram 36/640 with INRs > 5.0 Mean time to INR >1.9: 4.2 ± 1.1 days (10 mg group) vs. 5.6 ± 1.4 days (5 mg group) Proportion of patients with INRs of 2-3 was higher at all times in 5 mg group Levels of factor VII and protein C, but not factor II, declined significantly faster in the 10 mg group No statistical difference in median time to 2 consecutive INRs between the two groups Conclusion The 10 mg nomogram is safe and effective. The 10 mg nomogram achieves a therapeutic INR faster than a 5 mg nomogram. The 5 mg nomogram does not delay attainment of a therapeutic INR and possibly avoids excess anticoagulation No significant difference between either a 5- or 10-mg initiation nomogram 7

8 3. Benefits of New Changes a. Patients reach therapeutic INR faster b. Less LMWH injections i. Less pain ii. Less money c. Potentially fewer INR tests required 4. Safety Concerns a. Warfarin sensitive patients b. Elevated INRs c. Major Bleeding 5. Application of Guidelines a. Outpatient setting b. Low risk of bleeding c. Few comorbidities d. Able to have INR tested e. Under good management Testing Frequency 1. Heart of the Problem 12 a. Frequency of testing is tied to therapeutic control b. Therapeutic control correlates to clinical outcomes and adverse effects c. Is frequency of testing tied to clinical outcomes and adverse effects? 2. D. A. Fitzmaurice 13 a. There really is no evidence for either of these approaches and both management strategies have essentially evolved from routine practise. 3. Definition of Stable 1 a. Three months of consistent results with no dose changes b. Does not apply to self-testing c. Testing frequency increased when dose changes required 8

9 Table 5 14 Twelve-month outcomes and predictors of very stable INR control in prevalent warfarin users. Witt DM, Delate T, Clark NP, et al. J Thromb Haemost 2010;8(4): Background The recommended INR testing interval of four weeks may possibly be extended safely in a select group of stable patients. Objective To identify patients with stable INRs and compare the occurrences of thromboembolism, bleeding, and death between stable patients and a group of comparator patients. Outcome Characteristics of patients with very stable INR control Measures Rate of thromboembolic events Rate of bleeding events Rate of death Methods Retrospective longitudinal, cohort study Patients were on warfarin for > 90 days, over 18, and continuing warfarin for at least 12 months Stable defined as all INR values within range for a continuous 12 month period Comparator patients did not have a continuous 12 month period with INR values within range Must have an INR test at least every 8 weeks 533 patients classified as stable; 2555 patients in the comparator group Data Analysis α level set at 0.05 Chi-squared test used for categorical variables; independent samples t- test or Wilcoxon rank sum test used for continuous variables Results Stable patients were older (72.9 vs. 67.9, p <0.001), have an INR target < 3.0 (93.6% vs. 79.7%, p <0.001), were receiving warfarin for atrial fibrillation (51.0% vs. 41.4%, p <0.001), were less likely to have heart failure (5.1% vs. 10.6%, p < 0.001), and were more likely to have a lower mean chronic disease score (6.2 vs. 6.7, p < 0.001) The number of anticoagulation related deaths did not differ (0 in the stable group vs. 2 in the comparator group, p = 0.518) Rate of anticoagulation related thrombosis: 1 in the stable group vs. 34 in the comparator group (p=0.022) Rate of anticoagulation related bleeding: 11 in the stable group vs. 104 in the comparator group (p=0.026) Limitations Not all variables affecting INR control could be collected Possible that some clinical events were missed Not able to draw definitive cause and effect relationships between study variables and outcomes Conclusion A subgroup of patients with consistently stable INRs can be identified, and these patients tend to have fewer adverse outcomes related to anticoagulation. 9

10 Table 6 15 A comparison between six- and four-week intervals in surveillance of oral anticoagulant treatment. Pengo V, MD, Barbero F, MD, Biasiolo A, DSc, et al. Am J Clin Pathol 2003;120(6): Background Warfarin testing is recommended at least once a month, although some organizations are suggesting that interval can be extended. Testing frequency is largely determined by stability, which can be affected by a patient s INR target. Less testing can possibly improve a patient s quality of life and reduce costs. Objective To compare the biological risk in patients with prosthetic heart valves randomized to maximum testing intervals of 6 weeks vs. maximum testing intervals of 4 weeks Outcome Measures Biologic risk of maintaining INR values that expose patients to risk of hemorrhagic or thromboembolic events Rate of INR values > 5 or < 1.5 Methods Randomized control trial Patients must have a prosthetic heart valve for > 6 months, followed by a clinic for > 6 months, and have an INR target of 3 59 patients assigned to maximum 6 week intervals, 65 patients assigned to maximum 4 week intervals Testing intervals were shortened when INR values were out of range or when a dose change was needed Data Analysis Used a 1-tailed test, with a significant P being less than 0.05 Results No statistical difference between the 2 groups in INRs > 5.0 (29 in 6 week group vs. 20 in 4 week group, p = 0.06) or INRs < 1.5 (28 in 6 week group vs. 46 in 4 week group, p = 0.26) Vitamin k administration was greater in the 6 week group (14 times) vs. the 4 week group (4 times), p = 0.01 Mean time between INR tests was 24.9 ± 18.1 days in the 6 week group vs ± 9.5 days in the 4 week group, p < Limitations Surrogate markers used as the primary endpoints Underpowered to show a difference in clinical outcomes Conclusion In stable patients with prosthetic heart valves, it may be possible to extend the testing interval to 6 weeks, reducing costs and improving quality of life. 10

11 Table 7 16 Warfarin dose assessment every 4 weeks versus every 12 weeks in patients with stable international normalized ratios Schulman S, MD, PhD, Parpla S, MSc, Stewart C, MA, et al. Ann Intern Med 2011;155(10): Background Objective Outcome Measures Clinical guidelines differ in their recommendations of testing intervals for patients on oral anticoagulants. This group previously reported that one third of their patients have stable INRs, for which less INR tests could decrease the burden of anticoagulation therapy for these patients. To ascertain whether INR testing every 12 weeks is as safe as testing every 4 weeks TTR percentage Extreme INRs Changes in maintenance dose Major bleeding events Thromboembolic events Deaths Methods Randomized control trial Patients followed for 12 months as outpatients Patients had INR targets of either 2-3 or , had been managed by the clinic for > 6 months, and had unchanged doses for the previous 6 months 72 patients were randomized to 4 weeks and 70 patients were randomized to 12 week testing intervals Patients assigned to the 12 week interval had INR results reported to physicians every 4 weeks; however, one out of three was a true INR level, and the other 2 out of 3 were sham values. Data Analysis Based on an informal sampling of experts, the noninferiority margin was set at 7.5 percentage points A 1-sided α level of 2.5% and a power of 90% was used Linear interpolation to calculate TTR 1-sided 2-sample t tests, linear modeling, and chi-square tests used where appropriate Results Mean TTR percentage was 74.1% in the 4 week group and 71.6% in the 12 week group, shown to be noninferior (p= 0.02) 70 patients in the 4 week group had 1 dose change vs. 46 in the 12 week group (p= 0.004) No statistical difference in other secondary outcomes Major bleeding: 1 in the 4 week group vs. 2 in the 12 week group Thromboembolic event: 1 in the 4 week group vs. 0 in the 12 week group Death: 5 in the 4 week group vs. 2 in the 12 week group Limitations Not a true evaluation of testing and monitoring every 12 weeks, as all patients were tested every 4 weeks Used a surrogate primary outcome, not based on clinical outcomes Conclusion For stable patients, 12 week testing intervals are noninferior to 4 week testing intervals in terms of TTR and safety. 11

12 Table 8 14,15,16,17,18,19,20,21,22 Fihn SD, et al. J Gen Intern Med 1994;9(3): Pengo V, et al. Am J Clin Pathol 2003;120(6): Schulman S, et al. Ann Intern Med 2011;155(10): Trial Study Design Primary Endpoints Results Conclusion Randomized Testing intervals control trials can be safely Compared extended to as various testing much as 12 week intervals from intervals weeks Pengo V, et al studied heart valve patients with a higher goal INR Rose AJ, et al. Chest 2011;140(2): Shalev V. et al. Thromb Res 2007;120(2): Witt DM, et al. J Thromb Haemost 2010;8(4): Witt DM, et al. Blood 2009;114(5): Rose AJ, et al. J Thromb Haemost 2008;6(10): Lidstone V, et al. Clin Lab Haematol 2000;22(5): Retrospective review Databases from Veterans Affairs and Israel First 6 months of INR values excluded Retrospective, longitudinal cohort studies Stable classified by TTR or a period of consistently in-range INRs Prospective, observational study Outpatient setting Retrospective study Computer program increased the interval up to 14 weeks based on stability Length of follow up interval recommended, actual follow up interval, and quality of control Rate of INR values < 1.5 and > 5.0 Safety of 12 week vs. 4 week testing measured as TTR Find the maximum follow-up interval based on TTR Find the optimal interval between tests Identify patients with stable INR control Study patterns of care in anticoagulation Evaluate the use of longer testing intervals and whether this led to less anticoagulation control Follow up was 4.4 weeks ± 1.8 days when optimizing interval based on risk factors vs. 4.1 ± 1.8 days in control group No statistical difference between rate of INR values <1.5 and > 5.0 when comparing 6 vs. 4 week intervals Mean TTR of 74.1% in the 4 week group vs. 71.6% in the 12 week group showed noninferiority At the patient level, each additional day of follow up resulted in a 0.35% higher TTR. At the site level, each additional day of follow up resulted in a 0.51% drop in TTR As the interval between tests increased, the TTR decreased Patients more likely to be stable were: older, have an INR target <3.0, receiving warfarin for atrial fibrillation, less likely to have heart valve replacement or be treated with estrogen therapy, and have a lower mean chronic disease score Patients with excellent TTR scores were less likely to be female; those with poor TTR scores were more likely to have HF or CAD Percentage of INR within range at 6 weeks: 70% (95% CI 68-71%), and 14 weeks: 76% (95% CI 75-81%) Shorter testing intervals are associated with better INR control A group of patients with stable INR control can be identified. These patients may benefit from tailored treatment and may be able to extend their testing interval further Patients with the best TTR had the longest time between INR tests Patients with longer testing intervals were more likely to be within range than patients with shorter intervals
:744-749 Witt DM, et al. Blood 2009;114(5):952-956 Rose AJ, et al. J Thromb Haemost 2008;6(10):1647-1645 Lidstone V, et al.")
13 4. Benefits of Longer Intervals a. Patient preference b. Less costs c. Fewer dose changes 5. Safety Concerns a. Deviations in INR going undetected b. Adverse events c. Compliance 6. Application of Guideline a. Very stable patients ( 3 months) b. Reliable patients c. No foreseeable changes in diet or medications d. Not testing at home 13
 b. Reliable patients c.")
14 References: 1. Holbrook A, Schulman S, Witt DM, et al. Evidence-based management of anticoagulation therapy. Chest 2012;141(2)(Suppl):e152S-184S. 2. Schappert SM, Rechtsteiner EA. Ambulatory medical care utilization estimates for National Center for Health Statistics. Vital Health Stat 13(169) Guyatt GH, Akl EA, Crowther M, et al. CHEST 2012;141(2_suppl):48S-52S. 4. Ansell J, Hirsh J, Hylek E, et al. American College of Chest Physicians. Pharmacology and management of vitamin K antagonists: American College of Chest Physicians evidence-based clinical practice guidelines (8 th edition). Chest 2008;133(suppl 6):160S- 198S. 5. Witt DM, Nutescu EA, Haines ST. Venous thromboembolism. In: Dipiro JT, Talber RL, Yee GC, editors. Pharmacotherapy a pathophysiologic approach. 8 th ed. McGraw-Hill Companies, Inc.;2008. p Harrison L, Johnston M, Massicotte MP, et al. Comparison of 5-mg and 10-mg loading doses in initiation of warfarin therapy. Ann Intern Med 1997;126(2): Crowther MA, Ginsberg JB, Kearon C, et al. A randomized trial comparing 5-mg and 10- mg warfarin loading does. Arch Intern Med 1999;159(1): Kovacs, MJ, Rodger M, Anderson DR, et al. Comparison of 10-mg and 5-mg warfarin initiation nomograms together with low-molecular-weight heparin for outpatient treatment of acute venous thromboembolism. A randomized, double-blind, controlled trial. Ann Intern Med 2003;138(9): Monkman K, Lazo-Langner A, Kovacs MJ. A 10 mg warfarin initiation nomogram is safe and effective in outpatients starting oral anticoagulant therapy for venous thromboembolism. Thromb Res 2009;124(3): Wells PS, Le Gala G, Tierney S, et al. Practical application of the 10-mg warfarin initiation nomogram. Blood Coagul Fibrinolysis 2009;20: Quiroz R, Gerhard-Herman M, Kosowsky JM, et al. Comparison of a single end point to determine optimal initial warfarin dosing (5 mg versus 10 mg) for venous thromboembolism. Am J Cardiol 2006;98(4): White HD, Gruber M, Feyzi J, et al. Comparison of outcomes among patients randomized to warfarin therapy according to anticoagulant control: results from SPORTIF III and V. Arch Intern Med. 2007;167: Fitzmaurice DA. Oral anticoagulation should be managed in the community with treatment aimed at standard therapeutic targets and increased recall intervals. J Thromb Haemost 2008;6(10): Witt DM, Delate T, Clark NP, et al. Warped Consortium. Twelve-month outcomes and predictors of very stable INR control in prevalent warfarin users. J Thromb Haemost 2010;8(4): Pengo V, Barbero F, Biasiolo A, et al. A comparison between six- and four-week intervals in surveillance of oral anticoagulant treatment. Am J Clin Pathol 2003;120(6): Schulman S, Parpia S, Stewart C, et al. Warfarin dose assessment every 4 weeks versus every 12 weeks in patients with stable international normalized ratios: a randomized trial. Ann Intern Med 2011;155(10):
. Chest 2008;133(suppl 6):160S- 198S. 5.")
15 Fihn SD, McDonnel MB, Vermes D, et al; National Consortium of Anticoagulation Clinics. A computerized intervention to improve timing of outpatient follow-up: a multicenter randomized trial in patients treated with warfarin. J Gen Intern Med 1994;9(3): Rose AJ, Ozonoff A, Berlowitz DR, et al. Reexamining the recommended follow-up interal after obtaining an in-range international normalized ratio value: results from the Veterans Affairs study to improve anticoagulation. Chest 2011;140(2): Shalev V, Rogowski O, Shimron O, et al. The interval between prothrombin time tests and the quality of oral anticoagulants treatment in patients with chronic atrial fibrillation. Thromb Res 2007;120(2): Witt DM, Delate T, Clark NP, et al; Warfarin Associated Research Projects and other EnDeavors (WARPED) Consortium. Outcomes and predictors of very stable INR control during chronic anticoagulation therapy. Blood 2009;114(5): Rose AJ, Ozonoff A, Henault LE, et al. Warfarin for atrial fibrillation in communitybased practise. J Thromb Haemost 2008;6(10): Lidstone V, Janes S, Stross P. INR: Intervals of measurement can safely extend to 14 weeks. Clin Lab Haematol 2000;22(5):

Anticoagulation Initiation,Monitoring and Titration. Ng Heng Joo Department of Haematology Singapore General Hospital
 Anticoagulation Initiation,Monitoring and Titration Ng Heng Joo Department of Haematology Singapore General Hospital The 3 I s on the Anticoagulated Patient Indication? Intensity? Indefinite? Indications
Anticoagulation Initiation,Monitoring and Titration Ng Heng Joo Department of Haematology Singapore General Hospital The 3 I s on the Anticoagulated Patient Indication? Intensity? Indefinite? Indications
Failure or significant adverse effects to all of the alternatives: Eliquis and Xarelto
 This policy has been developed through review of medical literature, consideration of medical necessity, generally accepted medical practice standards, and approved by the IEHP Pharmacy and Therapeutics
This policy has been developed through review of medical literature, consideration of medical necessity, generally accepted medical practice standards, and approved by the IEHP Pharmacy and Therapeutics
PROTOCOL TITLE: Ambulatory Initiation and Management of Warfarin for Adults
 PROTOCOL NUMBER: 7 PROTOCOL TITLE: Ambulatory Initiation and Management of Warfarin for Adults THIS PROTOCOL APPLIES TO: UW Health Clinics: all adult outpatients with an active order for warfarin TARGET
PROTOCOL NUMBER: 7 PROTOCOL TITLE: Ambulatory Initiation and Management of Warfarin for Adults THIS PROTOCOL APPLIES TO: UW Health Clinics: all adult outpatients with an active order for warfarin TARGET
To Bridge or Not to Bridge. Periop Anticoagulation Management. Don Weinshenker, MD Ambulatory Care Denver VAMC
 To Bridge or Not to Bridge Periop Anticoagulation Management Don Weinshenker, MD Ambulatory Care Denver VAMC Financial Disclosure Information Nothing to report Periop AC Management Chronically anti-coagulated
To Bridge or Not to Bridge Periop Anticoagulation Management Don Weinshenker, MD Ambulatory Care Denver VAMC Financial Disclosure Information Nothing to report Periop AC Management Chronically anti-coagulated
DVT/PE Management with Rivaroxaban (Xarelto)
") DVT/PE Management with Rivaroxaban (Xarelto) Rivaroxaban is FDA approved for the acute treatment of DVT and PE and reduction in risk of recurrence of DVT and PE. FDA approved indications: Non valvular
DVT/PE Management with Rivaroxaban (Xarelto) Rivaroxaban is FDA approved for the acute treatment of DVT and PE and reduction in risk of recurrence of DVT and PE. FDA approved indications: Non valvular
Anticoagulation at the end of life. Rhona Maclean Rhona.maclean@sth.nhs.uk
 Anticoagulation at the end of life Rhona Maclean Rhona.maclean@sth.nhs.uk Content Anticoagulant Therapies Indications for anticoagulation Venous thromboembolism (VTE) Atrial Fibrillation Mechnical Heart
Anticoagulation at the end of life Rhona Maclean Rhona.maclean@sth.nhs.uk Content Anticoagulant Therapies Indications for anticoagulation Venous thromboembolism (VTE) Atrial Fibrillation Mechnical Heart
Disclosures. Objective (NRHS) Self Assessment #2
 Self Assessment #2") Development and Implementation of a Protocol for Reversing the Effects of Anticoagulants for Use in a Community Hospital Samantha Sepulveda, Pharm.D. PGY1 Pharmacy Resident Norman Regional Health System
Development and Implementation of a Protocol for Reversing the Effects of Anticoagulants for Use in a Community Hospital Samantha Sepulveda, Pharm.D. PGY1 Pharmacy Resident Norman Regional Health System
THE INTERNET STROKE CENTER PRESENTATIONS AND DISCUSSIONS ON STROKE MANAGEMENT
 THE INTERNET STROKE CENTER PRESENTATIONS AND DISCUSSIONS ON STROKE MANAGEMENT Stroke Prevention in Atrial Fibrillation Gregory Albers, M.D. Director Stanford Stroke Center Professor of Neurology and Neurological
THE INTERNET STROKE CENTER PRESENTATIONS AND DISCUSSIONS ON STROKE MANAGEMENT Stroke Prevention in Atrial Fibrillation Gregory Albers, M.D. Director Stanford Stroke Center Professor of Neurology and Neurological
Summary and general discussion
 Chapter 7 Summary and general discussion Summary and general discussion In this thesis, treatment of vitamin K antagonist-associated bleed with prothrombin complex concentrate was addressed. In this we
Chapter 7 Summary and general discussion Summary and general discussion In this thesis, treatment of vitamin K antagonist-associated bleed with prothrombin complex concentrate was addressed. In this we
How To Treat Aneuricaagulation
 Speaker Introduction Jessica Wilhoite, PharmD, BCACP Doctor of Pharmacy: Purdue University Postgraduate Residency Training: PGY1 Pharmacy Practice St. Vincent Hospital PGY2 Ambulatory Care St. Vincent
Speaker Introduction Jessica Wilhoite, PharmD, BCACP Doctor of Pharmacy: Purdue University Postgraduate Residency Training: PGY1 Pharmacy Practice St. Vincent Hospital PGY2 Ambulatory Care St. Vincent
STROKE PREVENTION IN ATRIAL FIBRILLATION. TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: ABBREVIATIONS: BACKGROUND:
 STROKE PREVENTION IN ATRIAL FIBRILLATION TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To guide clinicians in the selection of antithrombotic therapy for the secondary prevention
STROKE PREVENTION IN ATRIAL FIBRILLATION TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To guide clinicians in the selection of antithrombotic therapy for the secondary prevention
Disclosure. New Agents for Treatment of DVT. Prevalence of DVT VTE. Normal Hemostasis 7/17/2015. Mark Oliver, MD, RVT, RPVI,FSVU
 New Agents for Treatment of DVT Disclosure PI Adopt and Amplify trials Mark Oliver, MD, RVT, RPVI,FSVU BMS and Pfizer Speaker VTE Venous Thromboembolism Recognized DVT s New : 170,000 Recurrent : 90,000
New Agents for Treatment of DVT Disclosure PI Adopt and Amplify trials Mark Oliver, MD, RVT, RPVI,FSVU BMS and Pfizer Speaker VTE Venous Thromboembolism Recognized DVT s New : 170,000 Recurrent : 90,000
Use of Novel Oral Anticoagulants (NOACs) and the new DAWN modules at Scripps
 and the new DAWN modules at Scripps") Use of Novel Oral Anticoagulants (NOACs) and the new DAWN modules at Scripps Cheryl Ea, Pharm D. Anticoagulation Services Scripps Clinic and Scripps Green Hospital La Jolla, California Pharmacist Management
Use of Novel Oral Anticoagulants (NOACs) and the new DAWN modules at Scripps Cheryl Ea, Pharm D. Anticoagulation Services Scripps Clinic and Scripps Green Hospital La Jolla, California Pharmacist Management
4/9/2015. Risk Stratify Our Patients. Stroke Risk in AF: CHADS2 Scoring system JAMA 2001; 285: 2864-71
 Anticoagulation in the 21 st Century Adam Karpman, D.O. Saint Francis Medical Center/Oklahoma State University Medical Center Disclosures: None Atrial Fibrillation Most common arrhythmia in clinical practice.
Anticoagulation in the 21 st Century Adam Karpman, D.O. Saint Francis Medical Center/Oklahoma State University Medical Center Disclosures: None Atrial Fibrillation Most common arrhythmia in clinical practice.
The author has no disclosures
 Mary Bradbury, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Surgery September 18, 2012 Mary.bradbury@inova.org This presentation will discuss unlabeled and investigational use of products The author
Mary Bradbury, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Surgery September 18, 2012 Mary.bradbury@inova.org This presentation will discuss unlabeled and investigational use of products The author
Thrombosis and Hemostasis
 Thrombosis and Hemostasis Wendy Lim, MD, MSc, FRCPC Associate Professor, Department of Medicine McMaster University, Hamilton, ON Overview To review the important developments in venous thromboembolism
Thrombosis and Hemostasis Wendy Lim, MD, MSc, FRCPC Associate Professor, Department of Medicine McMaster University, Hamilton, ON Overview To review the important developments in venous thromboembolism
Order and/or Delegated Procedure :
 MEDICAL DIRECTIVE Guelph Family Health Team Responsible Person: Cathy Brown Approval Date: December 2007 Re-approval date: Approved by: INR CLINIC Medical Directive Number: GFHTMD 020 Review or Revision
MEDICAL DIRECTIVE Guelph Family Health Team Responsible Person: Cathy Brown Approval Date: December 2007 Re-approval date: Approved by: INR CLINIC Medical Directive Number: GFHTMD 020 Review or Revision
Gruppo di lavoro: Malattie Tromboemboliche
 Gruppo di lavoro: Malattie Tromboemboliche 2381 Soluble Recombinant Thrombomodulin Ameliorates Hematological Malignancy-Induced Disseminated Intravascular Coagulation More Promptly Than Conventional Anticoagulant
Gruppo di lavoro: Malattie Tromboemboliche 2381 Soluble Recombinant Thrombomodulin Ameliorates Hematological Malignancy-Induced Disseminated Intravascular Coagulation More Promptly Than Conventional Anticoagulant
New Anticoagulation Options for Stroke Prevention in Atrial Fibrillation. Joy Wahawisan, Pharm.D., BCPS April 25, 2012
 New Anticoagulation Options for Stroke Prevention in Atrial Fibrillation Joy Wahawisan, Pharm.D., BCPS April 25, 2012 Stroke in Atrial Fibrillation % Stroke 1991;22:983. Age Range (years) CHADS 2 Risk
New Anticoagulation Options for Stroke Prevention in Atrial Fibrillation Joy Wahawisan, Pharm.D., BCPS April 25, 2012 Stroke in Atrial Fibrillation % Stroke 1991;22:983. Age Range (years) CHADS 2 Risk
UHS CLINICAL CARE COLLABORATION: Outpatient & Inpatient
 Guidelines for Anticoagulation Initiation and Management Y2014 UHS CLINICAL CARE COLLABORATION: Outpatient & Inpatient Topic Page Number MEDICATION FLOW AND PATIENT FLOW... 2 AND 3 PARENTERAL ANTICOAGULANTS...
Guidelines for Anticoagulation Initiation and Management Y2014 UHS CLINICAL CARE COLLABORATION: Outpatient & Inpatient Topic Page Number MEDICATION FLOW AND PATIENT FLOW... 2 AND 3 PARENTERAL ANTICOAGULANTS...
None. Dual Antiplatelet Therapy Plus Systemic Anticoagulation: Bleeding Risk and Management. 76 year old male LINGO 1/5/2015
 Financial Disclosure Information Dual Antiplatelet Therapy Plus Systemic Anticoagulation: Bleeding Risk and Management Robert D. McBane, M.D. Division of Cardiology Mayo Clinic Rochester Dual Antiplatelet
Financial Disclosure Information Dual Antiplatelet Therapy Plus Systemic Anticoagulation: Bleeding Risk and Management Robert D. McBane, M.D. Division of Cardiology Mayo Clinic Rochester Dual Antiplatelet
NnEeWw DdEeVvEeLlOoPpMmEeNnTtSs IiıNn OoRrAaLl AaNnTtIiıCcOoAaGgUuLlAaTtIiıOoNn AaNnDd RrEeVvEeRrSsAaLl
 NnEeWw DdEeVvEeLlOoPpMmEeNnTtSs IiıNn OoRrAaLl AaNnTtIiıCcOoAaGgUuLlAaTtIiıOoNn AaNnDd RrEeVvEeRrSsAaLl Mikele Wissing, RN June 2014 Introduction until recently, was the unrivaled medication for treatment
NnEeWw DdEeVvEeLlOoPpMmEeNnTtSs IiıNn OoRrAaLl AaNnTtIiıCcOoAaGgUuLlAaTtIiıOoNn AaNnDd RrEeVvEeRrSsAaLl Mikele Wissing, RN June 2014 Introduction until recently, was the unrivaled medication for treatment
New Anticoagulants for the Treatment of Thromboembolism With a little subplot on superficial thrombophlebitis. Mark Crowther
 New Anticoagulants for the Treatment of Thromboembolism With a little subplot on superficial thrombophlebitis Mark Crowther 1 Disclosures Advisory Boards in last 24 months Pfizer, Alexion, Bayer, CSL Behring,
New Anticoagulants for the Treatment of Thromboembolism With a little subplot on superficial thrombophlebitis Mark Crowther 1 Disclosures Advisory Boards in last 24 months Pfizer, Alexion, Bayer, CSL Behring,
Long term anticoagulant therapy in patients with atrial fibrillation at high risk of stroke: a new scenario after RE-LY trial
 Long term anticoagulant therapy in patients with atrial fibrillation at high risk of stroke: a new scenario after RE-LY trial Camillo Autore Università di Roma Sapienza II Facoltà di Medicina e Chirurgia
Long term anticoagulant therapy in patients with atrial fibrillation at high risk of stroke: a new scenario after RE-LY trial Camillo Autore Università di Roma Sapienza II Facoltà di Medicina e Chirurgia
Dabigatran etexilate for the treatment and secondary prevention of deep vein thrombosis and/or pulmonary embolism ERRATUM
 Dabigatran etexilate for the treatment and secondary prevention of deep vein thrombosis and/or pulmonary embolism ERRATUM This report was commissioned by the NIHR HTA Programme as project number 12/78
Dabigatran etexilate for the treatment and secondary prevention of deep vein thrombosis and/or pulmonary embolism ERRATUM This report was commissioned by the NIHR HTA Programme as project number 12/78
Atrial Fibrillation, Chronic - Antithrombotic Treatment - OBSOLETE
 Atrial Fibrillation, Chronic - Antithrombotic Treatment - OBSOLETE Clinical practice guidelines serve as an educational reference, and do not supersede the clinical judgment of the treating physician with
Atrial Fibrillation, Chronic - Antithrombotic Treatment - OBSOLETE Clinical practice guidelines serve as an educational reference, and do not supersede the clinical judgment of the treating physician with
Anticoagulant therapy
 Anticoagulation: The risks Anticoagulant therapy 1990 2002: 600 incidents reported 120 resulted in death of patient 92 deaths related to warfarin usage 28 reports related to heparin usage Incidents in
Anticoagulation: The risks Anticoagulant therapy 1990 2002: 600 incidents reported 120 resulted in death of patient 92 deaths related to warfarin usage 28 reports related to heparin usage Incidents in
Paul G. Lee. 2 ND YEAR RESEARCH ELECTIVE RESIDENT S JOURNAL Volume III, 1998-1999. A. Objective
 A comparison of six months of anticoagulation with extended anticoagulation for a first episode of venous thromboembolism in patients with thrombophilia Paul G. Lee A. Objective a. To evaluate the risk
A comparison of six months of anticoagulation with extended anticoagulation for a first episode of venous thromboembolism in patients with thrombophilia Paul G. Lee A. Objective a. To evaluate the risk
Investor News. Phase III J-ROCKET AF Study of Bayer s Xarelto (rivaroxaban) Meets Primary Endpoint. Not intended for U.S.
 Meets Primary Endpoint. Not intended for U.S.") Investor News Not intended for U.S. and UK Media Bayer AG Investor Relations 51368 Leverkusen Germany www.investor.bayer.com Phase III J-ROCKET AF Study of Bayer s Xarelto (rivaroxaban) Meets Primary Endpoint
Investor News Not intended for U.S. and UK Media Bayer AG Investor Relations 51368 Leverkusen Germany www.investor.bayer.com Phase III J-ROCKET AF Study of Bayer s Xarelto (rivaroxaban) Meets Primary Endpoint
Devang M. Desai, MD, FACC, FSCAI Chief of Interventional Cardiology Director of Cardiac Catheterization Lab St. Mary s Hospital and Regional Medical
 Devang M. Desai, MD, FACC, FSCAI Chief of Interventional Cardiology Director of Cardiac Catheterization Lab St. Mary s Hospital and Regional Medical Center A.Fib affects 2.2 million Americans. The lifetime
Devang M. Desai, MD, FACC, FSCAI Chief of Interventional Cardiology Director of Cardiac Catheterization Lab St. Mary s Hospital and Regional Medical Center A.Fib affects 2.2 million Americans. The lifetime
How diagnostics can help alleviate healthcare cost burden. James Creeden, Chief Medical Officer Roche Professional Diagnostics
 How diagnostics can help alleviate healthcare cost burden James Creeden, Chief Medical Officer Roche Professional Diagnostics Environment Stakeholders and requirements Patients Accurate testing Improved
How diagnostics can help alleviate healthcare cost burden James Creeden, Chief Medical Officer Roche Professional Diagnostics Environment Stakeholders and requirements Patients Accurate testing Improved
Committee Approval Date: September 12, 2014 Next Review Date: September 2015
 Medication Policy Manual Policy No: dru361 Topic: Pradaxa, dabigatran Date of Origin: September 12, 2014 Committee Approval Date: September 12, 2014 Next Review Date: September 2015 Effective Date: November
Medication Policy Manual Policy No: dru361 Topic: Pradaxa, dabigatran Date of Origin: September 12, 2014 Committee Approval Date: September 12, 2014 Next Review Date: September 2015 Effective Date: November
Rivaroxaban A new oral anti-thrombotic Dr. Hisham Aboul-Enein Professor of Cardiology Benha University 12/1/2012
 Rivaroxaban A new oral anti-thrombotic Dr. Hisham Aboul-Enein Professor of Cardiology Benha University 12/1/2012 Agenda Ideal anticoagulant. Drawbacks of warfarin. Rivaroxaban in clinical trails. Present
Rivaroxaban A new oral anti-thrombotic Dr. Hisham Aboul-Enein Professor of Cardiology Benha University 12/1/2012 Agenda Ideal anticoagulant. Drawbacks of warfarin. Rivaroxaban in clinical trails. Present
Novel Anticoagulation Agents DISCLOSURES. Objectives ATRIAL FIBRILLATION TRIALS. NOAC Comparison 6/12/2015
 Novel Anticoagulation Agents DISCLOSURES James W. Haynes, MD Department of Family Medicine Univ of TN Health Science Center (Chattanooga) Objectives Understand mechanism of action behind the NOAC agents
Novel Anticoagulation Agents DISCLOSURES James W. Haynes, MD Department of Family Medicine Univ of TN Health Science Center (Chattanooga) Objectives Understand mechanism of action behind the NOAC agents
Bios 6648: Design & conduct of clinical research
 Bios 6648: Design & conduct of clinical research Section 1 - Specifying the study setting and objectives 1. Specifying the study setting and objectives 1.0 Background Where will we end up?: (a) The treatment
Bios 6648: Design & conduct of clinical research Section 1 - Specifying the study setting and objectives 1. Specifying the study setting and objectives 1.0 Background Where will we end up?: (a) The treatment
USE AND INTERPRETATION OF LABORATORY COAGULATION TESTS IN PATIENTS WHO ARE RECEIVING A NEW ORAL ANTICOAGULANT (DABIGATRAN, RIVAROXABAN, APIXABAN)
") USE AND INTERPRETATION OF LABORATORY COAGULATION TESTS IN PATIENTS WHO ARE RECEIVING A NEW ORAL ANTICOAGULANT (DABIGATRAN, RIVAROXABAN, APIXABAN) TARGET AUDIENCE: All Canadian health care professionals:
USE AND INTERPRETATION OF LABORATORY COAGULATION TESTS IN PATIENTS WHO ARE RECEIVING A NEW ORAL ANTICOAGULANT (DABIGATRAN, RIVAROXABAN, APIXABAN) TARGET AUDIENCE: All Canadian health care professionals:
New Oral Anticoagulants. How safe are they outside the trials?
 New Oral Anticoagulants How safe are they outside the trials? Objectives The need for anticoagulant therapy Indications for anticoagulation Traditional anticoagulant therapies Properties of new oral anticoagulants
New Oral Anticoagulants How safe are they outside the trials? Objectives The need for anticoagulant therapy Indications for anticoagulation Traditional anticoagulant therapies Properties of new oral anticoagulants
Assessment of Clinical Outcomes of a Pharmacist Managed Anticoagulation Clinic in a Malaysian Tertiary Hospital
 ISPOR 5 th Asia Pacific Conference 2012 Taipei International Convention Center in Taipei, Taiwan. Assessment of Clinical Outcomes of a Pharmacist Managed Anticoagulation Clinic in a Malaysian Tertiary
ISPOR 5 th Asia Pacific Conference 2012 Taipei International Convention Center in Taipei, Taiwan. Assessment of Clinical Outcomes of a Pharmacist Managed Anticoagulation Clinic in a Malaysian Tertiary
Stop the Bleeding: Management of Drug-induced Coagulopathy. Stacy A. Voils, PharmD, BCPS Critical Care Specialist, Neurosurgery
 Stop the Bleeding: Management of Drug-induced Coagulopathy Stacy A. Voils, PharmD, BCPS Critical Care Specialist, Neurosurgery Objectives Discuss contemporary management of warfarin reversal in patients
Stop the Bleeding: Management of Drug-induced Coagulopathy Stacy A. Voils, PharmD, BCPS Critical Care Specialist, Neurosurgery Objectives Discuss contemporary management of warfarin reversal in patients
New Treatments for Stroke Prevention in Atrial Fibrillation. John C. Andrefsky, MD, FAHA NEOMED Internal Medicine Review course May 5 th, 2013
 New Treatments for Stroke Prevention in Atrial Fibrillation John C. Andrefsky, MD, FAHA NEOMED Internal Medicine Review course May 5 th, 2013 Classification Paroxysmal atrial fibrillation (AF) Last < 7
New Treatments for Stroke Prevention in Atrial Fibrillation John C. Andrefsky, MD, FAHA NEOMED Internal Medicine Review course May 5 th, 2013 Classification Paroxysmal atrial fibrillation (AF) Last < 7
ABOUT XARELTO CLINICAL STUDIES
 ABOUT XARELTO CLINICAL STUDIES FAST FACTS Xarelto (rivaroxaban) is a novel, oral direct Factor Xa inhibitor. On September 30, 2008, the European Commission granted marketing approval for Xarelto for the
ABOUT XARELTO CLINICAL STUDIES FAST FACTS Xarelto (rivaroxaban) is a novel, oral direct Factor Xa inhibitor. On September 30, 2008, the European Commission granted marketing approval for Xarelto for the
The Effect of Daily Low-Dose Vitamin K Bottle Refraction
 Low-Dose Vitamin K to Augment Anticoagulation Control Alicia M. Reese, Pharm.D., Lisa E. Farnett, Pharm.D., Roger M. Lyons, M.D., Bhavin Patel, Pharm.D., Laura Morgan, Pharm.D., and Henry I. Bussey, Pharm.D.
Low-Dose Vitamin K to Augment Anticoagulation Control Alicia M. Reese, Pharm.D., Lisa E. Farnett, Pharm.D., Roger M. Lyons, M.D., Bhavin Patel, Pharm.D., Laura Morgan, Pharm.D., and Henry I. Bussey, Pharm.D.
Venous Thromboembolism: Long Term Anticoagulation. Dan Johnson, Pharm.D.
 Venous Thromboembolism: Long Term Anticoagulation Dan Johnson, Pharm.D. Disclosures No financial relationships with products discussed Off-label use of drug therapy always discussed Objectives Review clinical
Venous Thromboembolism: Long Term Anticoagulation Dan Johnson, Pharm.D. Disclosures No financial relationships with products discussed Off-label use of drug therapy always discussed Objectives Review clinical
The 50-year Quest to Replace Warfarin: Novel Anticoagulants Define a New Era. CCRN State of the Heart 2012 June 2, 2012
 The 50-year Quest to Replace Warfarin: Novel Anticoagulants Define a New Era CCRN State of the Heart 2012 June 2, 2012 Disclosures I have I have been involved in trials of new anticoagulants and have received
The 50-year Quest to Replace Warfarin: Novel Anticoagulants Define a New Era CCRN State of the Heart 2012 June 2, 2012 Disclosures I have I have been involved in trials of new anticoagulants and have received
2. Background This indication of rivaroxaban had not previously been considered by the PBAC.
 PUBLIC SUMMARY DOCUMENT Product: Rivaroxaban, tablets, 15mg and 20mg, Xarelto Sponsor: Bayer Australia Ltd Date of PBAC Consideration: March 2013 1. Purpose of Application The application requested the
PUBLIC SUMMARY DOCUMENT Product: Rivaroxaban, tablets, 15mg and 20mg, Xarelto Sponsor: Bayer Australia Ltd Date of PBAC Consideration: March 2013 1. Purpose of Application The application requested the
Reducing Adverse Drug Events With Anti Coagulation Clinics. McFarland Clinic. McFarland Protime Clinic 09/05/12
 Reducing Adverse Drug Events With Anti Coagulation Clinics Dr. Donald Skinner, MD McFarland Clinic 182 Physicians (149 Shareholders) 40 Mid Level Providers 13 Administrators/Executive Directors 1,200 Support
Reducing Adverse Drug Events With Anti Coagulation Clinics Dr. Donald Skinner, MD McFarland Clinic 182 Physicians (149 Shareholders) 40 Mid Level Providers 13 Administrators/Executive Directors 1,200 Support
Kirsten M. Roberts, 1 Tamara B. Knight, 2 Eimeira Padilla-Tolentino, 3 Manasa Murthy, 4 and Evan J. Peterson 5. 1. Introduction
 rombosis Volume 2015, Article ID 414523, 6 pages http://dx.doi.org/10.1155/2015/414523 Clinical Study Length of Stay Comparison between and Warfarin in the Treatment of Pulmonary Embolism: Results from
rombosis Volume 2015, Article ID 414523, 6 pages http://dx.doi.org/10.1155/2015/414523 Clinical Study Length of Stay Comparison between and Warfarin in the Treatment of Pulmonary Embolism: Results from
To Bridge or Not to Bridge
 To Bridge or Not to Bridge Delaney Ivy, Pharm.D. PGY- 2 Ambulatory Care Resident Blackstock Family Health Center University of Texas at Austin College of Pharmacy Pharmacotherapy Rounds October 7, 2011
To Bridge or Not to Bridge Delaney Ivy, Pharm.D. PGY- 2 Ambulatory Care Resident Blackstock Family Health Center University of Texas at Austin College of Pharmacy Pharmacotherapy Rounds October 7, 2011
Pulmonary Embolism Treatment Update
 UC SF Pulmonary Embolism Treatment Update Jeffrey Tabas, MD Professor UCSF School of Medicine Emergency Department San Francisco General Hospital sf g h Disclosure No Financial Relationships to Disclose
UC SF Pulmonary Embolism Treatment Update Jeffrey Tabas, MD Professor UCSF School of Medicine Emergency Department San Francisco General Hospital sf g h Disclosure No Financial Relationships to Disclose
Acute behandeling van longembolie. Peter Verhamme. Bloedings- en Vaatziekten UZ Leuven. Research support and/or honoraria:
 Acute behandeling van longembolie Peter Verhamme Bloedings- en Vaatziekten UZ Leuven Disclosures Research support and/or honoraria: Bayer, Boehringer-Ingelheim, Daiichi-Sankyo, Pfizer, BMS, Sanofi, Leo-pharma
Acute behandeling van longembolie Peter Verhamme Bloedings- en Vaatziekten UZ Leuven Disclosures Research support and/or honoraria: Bayer, Boehringer-Ingelheim, Daiichi-Sankyo, Pfizer, BMS, Sanofi, Leo-pharma
CDEC FINAL RECOMMENDATION
 CDEC FINAL RECOMMENDATION RIVAROXABAN (Xarelto Bayer Inc.) New Indication: Pulmonary Embolism Note: The Canadian Drug Expert Committee (CDEC) previously reviewed rivaroxaban for the treatment of deep vein
CDEC FINAL RECOMMENDATION RIVAROXABAN (Xarelto Bayer Inc.) New Indication: Pulmonary Embolism Note: The Canadian Drug Expert Committee (CDEC) previously reviewed rivaroxaban for the treatment of deep vein
AHA/ASA Scientific Statement Oral Antithrombotic Agents for the Prevention of Stroke in Atrial Fibrillation
 AHA/ASA Scientific Statement Oral Antithrombotic Agents for the Prevention of Stroke in Atrial Fibrillation A Statement for Healthcare Professionals from the American Heart Association/American Stroke
AHA/ASA Scientific Statement Oral Antithrombotic Agents for the Prevention of Stroke in Atrial Fibrillation A Statement for Healthcare Professionals from the American Heart Association/American Stroke
The importance of adherence and persistence: The advantages of once-daily dosing
 The importance of adherence and persistence: The advantages of once-daily dosing Craig I. Coleman, PharmD Professor, University of Connecticut School of Pharmacy Storrs, CT, USA Conflicts of interest Dr
The importance of adherence and persistence: The advantages of once-daily dosing Craig I. Coleman, PharmD Professor, University of Connecticut School of Pharmacy Storrs, CT, USA Conflicts of interest Dr
STROKE PREVENTION IN ATRIAL FIBRILLATION
 STROKE PREVENTION IN ATRIAL FIBRILLATION OBJECTIVE: To guide clinicians in the selection of antithrombotic therapy for the secondary prevention of ischemic stroke and arterial thromboembolism in patients
STROKE PREVENTION IN ATRIAL FIBRILLATION OBJECTIVE: To guide clinicians in the selection of antithrombotic therapy for the secondary prevention of ischemic stroke and arterial thromboembolism in patients
Prior Authorization Guideline
 Guideline Guideline Name Formulary Xarelto (rivaroxaban) UnitedHealthcare Community & State Approval Date 0/0/203 Revision Date 8//204 Technician Note: CPS Approval Date: /5/20; CPS Revision Date: 8/20/204
Guideline Guideline Name Formulary Xarelto (rivaroxaban) UnitedHealthcare Community & State Approval Date 0/0/203 Revision Date 8//204 Technician Note: CPS Approval Date: /5/20; CPS Revision Date: 8/20/204
Treating AF: The Newest Recommendations. CardioCase presentation. Ethel s Case. Wayne Warnica, MD, FACC, FACP, FRCPC
 Treating AF: The Newest Recommendations Wayne Warnica, MD, FACC, FACP, FRCPC CardioCase presentation Ethel s Case Ethel, 73, presents with rapid heart beating and mild chest discomfort. In the ED, ECG
Treating AF: The Newest Recommendations Wayne Warnica, MD, FACC, FACP, FRCPC CardioCase presentation Ethel s Case Ethel, 73, presents with rapid heart beating and mild chest discomfort. In the ED, ECG
CDEC RECORD OF ADVICE
 CDEC RECORD OF ADVICE RIVAROXABAN (Xarelto Bayer Inc.) Indication: Deep Vein Thrombosis Without Symptomatic Pulmonary Embolism This document summarizes the Canadian Drug Expert Committee (CDEC) response
CDEC RECORD OF ADVICE RIVAROXABAN (Xarelto Bayer Inc.) Indication: Deep Vein Thrombosis Without Symptomatic Pulmonary Embolism This document summarizes the Canadian Drug Expert Committee (CDEC) response
Anticoagulation before and after cardioversion; which and for how long
 Anticoagulation before and after cardioversion; which and for how long Sameh Samir, MD Cardiovascular medicine dept. Tanta faculty of medicine Atrial fibrillation goals of management Identify and treat
Anticoagulation before and after cardioversion; which and for how long Sameh Samir, MD Cardiovascular medicine dept. Tanta faculty of medicine Atrial fibrillation goals of management Identify and treat
Backgrounder. Current anticoagulant therapies
 Backgrounder Bayer AG Investor Relations 51368 Leverkusen Germany www.investor.bayer.com Current anticoagulant therapies Anticoagulant drugs have significantly reduced the risk of thromboembolic events
Backgrounder Bayer AG Investor Relations 51368 Leverkusen Germany www.investor.bayer.com Current anticoagulant therapies Anticoagulant drugs have significantly reduced the risk of thromboembolic events
Value-Based Purchasing
 Emerging Topics in Healthcare Reform Value-Based Purchasing Janssen Pharmaceuticals, Inc. Value-Based Purchasing The Patient Protection and Affordable Care Act (ACA) established the Hospital Value-Based
Emerging Topics in Healthcare Reform Value-Based Purchasing Janssen Pharmaceuticals, Inc. Value-Based Purchasing The Patient Protection and Affordable Care Act (ACA) established the Hospital Value-Based
RR 0.88 (95% CI: 0.77 1.00) P=0.051 (superiority) 3.75
 P=0.051 (superiority) 3.75") ALL-CAUSE MORTALITY RR 0.88 (95% CI: 0.77 1.00) P=0.051 (superiority) Rate per year (%) 5.0 4.0 3.0 2.0 1.0 0 3.64 D150 mg BID 3.75 D110 mg BID RR 0.91 (95% CI: 0.80 1.03) P=0.13 (superiority) 4.13 Warfarin
ALL-CAUSE MORTALITY RR 0.88 (95% CI: 0.77 1.00) P=0.051 (superiority) Rate per year (%) 5.0 4.0 3.0 2.0 1.0 0 3.64 D150 mg BID 3.75 D110 mg BID RR 0.91 (95% CI: 0.80 1.03) P=0.13 (superiority) 4.13 Warfarin
Objectives. Oral Anticoagulants. Assessment Question No. 1. FDA Approved Indications. Warfarin
 Assessment of Target Specific Oral Anticoagulant Prescribing Rationale and Adverse Event Pilot Comparison in Veterans Receiving Oral Anticoagulation Therapy Angela Mechelay, Pharm.D. PGY1 Pharmacy Resident
Assessment of Target Specific Oral Anticoagulant Prescribing Rationale and Adverse Event Pilot Comparison in Veterans Receiving Oral Anticoagulation Therapy Angela Mechelay, Pharm.D. PGY1 Pharmacy Resident
How To Manage An Anticoagulant
 PERI-OPERATIVE MANAGEMENT OF PATIENTS WHO ARE RECEIVING A NEW ORAL ANTICOAGULANT (DABIGATRAN, RIVAROXABAN, APIXABAN) TARGET AUDIENCE: All Canadian health care professionals, including primary care physicians,
PERI-OPERATIVE MANAGEMENT OF PATIENTS WHO ARE RECEIVING A NEW ORAL ANTICOAGULANT (DABIGATRAN, RIVAROXABAN, APIXABAN) TARGET AUDIENCE: All Canadian health care professionals, including primary care physicians,
Perioperative Bridging in Atrial Fibrillation: Is it necessary?
 Perioperative Bridging in Atrial Fibrillation: Is it necessary? Jason B. Thompson M.D., Ph.D. August 29, 2015 2015 NCVH Birmingham Hypothesis: When bridging, risk of bleeding < risk systemic embolism (SE).
Perioperative Bridging in Atrial Fibrillation: Is it necessary? Jason B. Thompson M.D., Ph.D. August 29, 2015 2015 NCVH Birmingham Hypothesis: When bridging, risk of bleeding < risk systemic embolism (SE).
New anticoagulants: Monitoring or not Monitoring? Not Monitoring
 The 2 nd World Congress on CONTROVERSIES IN HEMATOLOGY (COHEM) Barcelona, Spain September 6 8, 2012 New anticoagulants: Monitoring or not Monitoring? Not Monitoring Anna Falanga, MD Immunohematology and
The 2 nd World Congress on CONTROVERSIES IN HEMATOLOGY (COHEM) Barcelona, Spain September 6 8, 2012 New anticoagulants: Monitoring or not Monitoring? Not Monitoring Anna Falanga, MD Immunohematology and
Antiplatelet and Antithrombotics From clinical trials to guidelines
 Antiplatelet and Antithrombotics From clinical trials to guidelines Ashraf Reda, MD, FESC Prof and head of Cardiology Dep. Menofiya University Preisedent of EGYBAC Chairman of WGLVR One of the big stories
Antiplatelet and Antithrombotics From clinical trials to guidelines Ashraf Reda, MD, FESC Prof and head of Cardiology Dep. Menofiya University Preisedent of EGYBAC Chairman of WGLVR One of the big stories
New Anticoagulants and GI bleeding
 New Anticoagulants and GI bleeding DR DANNY MYERS MD FRCP(C) CLINICAL ASSISTANT PROFESSOR OF MEDICINE, UBC Conflicts of Interest None I am unbiased in the use of NOAC s vs Warfarin based on risk benefit
New Anticoagulants and GI bleeding DR DANNY MYERS MD FRCP(C) CLINICAL ASSISTANT PROFESSOR OF MEDICINE, UBC Conflicts of Interest None I am unbiased in the use of NOAC s vs Warfarin based on risk benefit
Point-of-care (POC) versus central laboratory instrumentation for monitoring oral anticoagulation
 versus central laboratory instrumentation for monitoring oral anticoagulation") Point-of-care (POC) versus central laboratory instrumentation for monitoring oral anticoagulation David M Dorfman a, Ellen M Goonan a, M Kay Boutilier a, Petr Jarolim a, Milenko Tanasijevic a and Samuel
Point-of-care (POC) versus central laboratory instrumentation for monitoring oral anticoagulation David M Dorfman a, Ellen M Goonan a, M Kay Boutilier a, Petr Jarolim a, Milenko Tanasijevic a and Samuel
Clinical Study Synopsis
 Clinical Study Synopsis This Clinical Study Synopsis is provided for patients and healthcare professionals to increase the transparency of Bayer's clinical research. This document is not intended to replace
Clinical Study Synopsis This Clinical Study Synopsis is provided for patients and healthcare professionals to increase the transparency of Bayer's clinical research. This document is not intended to replace
5/21/2012. Perioperative Use Issues. On admission: During hospitalization:
 Dabigatran and Rivaroxaban: Challenges in the Perioperative Setting Claudia Swenson, Pharm.D., CDE, BC-ADM, FASHP Central Washington Hospital Wenatchee, WA claudia.swenson@cwhs.com Dabigatran and Rivaroxaban:
Dabigatran and Rivaroxaban: Challenges in the Perioperative Setting Claudia Swenson, Pharm.D., CDE, BC-ADM, FASHP Central Washington Hospital Wenatchee, WA claudia.swenson@cwhs.com Dabigatran and Rivaroxaban:
Inpatient Anticoagulation Safety. To provide safe and effective anticoagulation therapy through a collaborative approach.
 Inpatient Anticoagulation Safety Purpose: Policy: To provide safe and effective anticoagulation therapy through a collaborative approach. Upon the written order of a physician, Heparin, Low Molecular Weight
Inpatient Anticoagulation Safety Purpose: Policy: To provide safe and effective anticoagulation therapy through a collaborative approach. Upon the written order of a physician, Heparin, Low Molecular Weight
Review of Non-VKA Oral AntiCoagulants (NOACs) and their use in Great Britain
 and their use in Great Britain") Review of Non-VKA Oral AntiCoagulants (NOACs) and their use in Great Britain Dr Alexander (Ander) Cohen Guy s and St Thomas Hospitals, King s College London, UK Pavia Spring Meeting 13 June 2014 Overview
Review of Non-VKA Oral AntiCoagulants (NOACs) and their use in Great Britain Dr Alexander (Ander) Cohen Guy s and St Thomas Hospitals, King s College London, UK Pavia Spring Meeting 13 June 2014 Overview
Adherence to NOACs. Disclosure. Patricia van den Bemt EAHP Hamburg 2015
 Adherence to NOACs Patricia van den Bemt EAHP Hamburg 2015 Disclosure Unrestricted research grants from Glaxo-SmithKline Boehringer Ingelheim Daiichi Sankyo Bayer Pfizer For research on medication safety
Adherence to NOACs Patricia van den Bemt EAHP Hamburg 2015 Disclosure Unrestricted research grants from Glaxo-SmithKline Boehringer Ingelheim Daiichi Sankyo Bayer Pfizer For research on medication safety
Are there sufficient indications for switching to new anticoagulant agents
 Are there sufficient indications for switching to new anticoagulant agents Meyer Michel Samama et Gregoris Gerotziafas Groupe Hémostase-Thrombose Hôtel-Dieu, Hôpital Tenon, Paris & Biomnis Ivry/seine,
Are there sufficient indications for switching to new anticoagulant agents Meyer Michel Samama et Gregoris Gerotziafas Groupe Hémostase-Thrombose Hôtel-Dieu, Hôpital Tenon, Paris & Biomnis Ivry/seine,
Out with the Old and in with the New? Target Specific Anticoagulants for Atrial Fibrillation
 Out with the Old and in with the New? Target Specific Anticoagulants for Atrial Fibrillation Goal Statement Pharmacists and technicians will gain knowledge in the use of target specific oral anticoagulants
Out with the Old and in with the New? Target Specific Anticoagulants for Atrial Fibrillation Goal Statement Pharmacists and technicians will gain knowledge in the use of target specific oral anticoagulants
New Oral Anticoagulants
 New Oral Anticoagulants Tracy Minichiello, MD Associate Professor of Medicine Chief, San FranciscoVA Anticoagulation and Thrombosis Service Ansell, J. Hematology Copyright 2010 American Society of Hematology.
New Oral Anticoagulants Tracy Minichiello, MD Associate Professor of Medicine Chief, San FranciscoVA Anticoagulation and Thrombosis Service Ansell, J. Hematology Copyright 2010 American Society of Hematology.
Thrombophilia. Steven R. Lentz, M.D. Ph.D. Carver College of Medicine The University of Iowa May 2003
 Thrombophilia Steven R. Lentz, M.D. Ph.D. Carver College of Medicine The University of Iowa May 2003 Thrombophilia Hereditary and acquired risk factors for thrombosis Venous thromboembolism Arterial thromboembolism
Thrombophilia Steven R. Lentz, M.D. Ph.D. Carver College of Medicine The University of Iowa May 2003 Thrombophilia Hereditary and acquired risk factors for thrombosis Venous thromboembolism Arterial thromboembolism
Clinical Study Synopsis
 Clinical Study Synopsis This Clinical Study Synopsis is provided for patients and healthcare professionals to increase the transparency of Bayer's clinical research. This document is not intended to replace
Clinical Study Synopsis This Clinical Study Synopsis is provided for patients and healthcare professionals to increase the transparency of Bayer's clinical research. This document is not intended to replace
New Anticoagulants: When and Why Should I Use Them? Disclosures
 Winship Cancer Institute of Emory University New Anticoagulants: When and Why Should I Use Them? Christine L. Kempton, MD, MSc Associate Professor of Pediatrics and Hematology and Medical Oncology Hemophilia
Winship Cancer Institute of Emory University New Anticoagulants: When and Why Should I Use Them? Christine L. Kempton, MD, MSc Associate Professor of Pediatrics and Hematology and Medical Oncology Hemophilia
Traditional anticoagulants
 TEGH Family Practice Clinic Day April 4, 03 Use of Anticoagulants in 03: What s New (and What Isn t) Bill Geerts, MD, FRCPC Director, Thromboembolism Program, Sunnybrook HSC Professor of Medicine, University
TEGH Family Practice Clinic Day April 4, 03 Use of Anticoagulants in 03: What s New (and What Isn t) Bill Geerts, MD, FRCPC Director, Thromboembolism Program, Sunnybrook HSC Professor of Medicine, University
Outpatient Treatment of Deep Vein Thrombosis with Low Molecular Weight Heparin (LMWH) Clinical Practice Guideline August 2013
 Clinical Practice Guideline August 2013") Outpatient Treatment of Deep Vein Thrombosis with Low Molecular Weight Heparin (LMWH) Clinical Practice Guideline August 2013 General Principles: There is compelling data in the medical literature to support
Outpatient Treatment of Deep Vein Thrombosis with Low Molecular Weight Heparin (LMWH) Clinical Practice Guideline August 2013 General Principles: There is compelling data in the medical literature to support
FOR THE PREVENTION OF ATRIAL FIBRILLATION RELATED STROKE
 www.bpac.org.nz keyword: warfarinaspirin FOR THE PREVENTION OF ATRIAL FIBRILLATION RELATED STROKE Key Concepts In atrial fibrillation (AF) warfarin is more effective than aspirin for stroke prevention.
www.bpac.org.nz keyword: warfarinaspirin FOR THE PREVENTION OF ATRIAL FIBRILLATION RELATED STROKE Key Concepts In atrial fibrillation (AF) warfarin is more effective than aspirin for stroke prevention.
3/3/2015. Patrick Cobb, MD, FACP March 2015
 Patrick Cobb, MD, FACP March 2015 I, Patrick Cobb, MD, DO NOT have a financial interest/arrangement or affiliation with one or more organizations that could be perceived as a real or apparent conflict
Patrick Cobb, MD, FACP March 2015 I, Patrick Cobb, MD, DO NOT have a financial interest/arrangement or affiliation with one or more organizations that could be perceived as a real or apparent conflict
1/12/2016. What s in a name? What s in a name? NO.Anti-Coagulation. DOACs in clinical practice. Practical aspects of using
 What s in a name? Practical aspects of using DOACs (Direct Oral Anticoagulants) James L. Sebastian, MD, MACP Professor of Medicine (GIM) Medical College of Wisconsin February 5, 2016 DOAC NOAC NOAC ODI
What s in a name? Practical aspects of using DOACs (Direct Oral Anticoagulants) James L. Sebastian, MD, MACP Professor of Medicine (GIM) Medical College of Wisconsin February 5, 2016 DOAC NOAC NOAC ODI
New Oral Anticoagulants Increase Risk for Gastrointestinal Bleeding - A Systematic Review and Meta-Analysis
 New Oral Anticoagulants Increase Risk for Gastrointestinal Bleeding - A Systematic Review and Meta-Analysis Holster IL, Valkhoff VE, Kuipers EJ, Tjwa ET Departments of Gastroenterology and Hepatology,
New Oral Anticoagulants Increase Risk for Gastrointestinal Bleeding - A Systematic Review and Meta-Analysis Holster IL, Valkhoff VE, Kuipers EJ, Tjwa ET Departments of Gastroenterology and Hepatology,
Hot Line Session at European Society of Cardiology (ESC) Congress 2014:
 Congress 2014:") Investor News Not intended for U.S. and UK Media Bayer AG Investor Relations 51368 Leverkusen Germany www.investor.bayer.com Hot Line Session at European Society of Cardiology (ESC) Congress 2014: Once-Daily
Investor News Not intended for U.S. and UK Media Bayer AG Investor Relations 51368 Leverkusen Germany www.investor.bayer.com Hot Line Session at European Society of Cardiology (ESC) Congress 2014: Once-Daily
2/17/2015 ANTICOAGULATION UPDATE OBJECTIVES BRIEF REVIEW: CLASSES OF ORAL ANTICOAGULANTS
 ANTICOAGULATION UPDATE C AR R I E P AL M E R, D N P, RN, AN P - BC OBJECTIVES At the end of the presentation, the NP will be able to: Identify new indications for target-specific oral anticoagulants (TSOACs),
ANTICOAGULATION UPDATE C AR R I E P AL M E R, D N P, RN, AN P - BC OBJECTIVES At the end of the presentation, the NP will be able to: Identify new indications for target-specific oral anticoagulants (TSOACs),
Supplementary Table 1: Risk of bias in included studies. Blinding of participants and personnel (performance bias)
") Random sequence generation (selection bias) Allocation concealment (selection bias) Blinding of participants and personnel (performance bias) Blinding of outcome assessment (detection bias) Incomplete
Random sequence generation (selection bias) Allocation concealment (selection bias) Blinding of participants and personnel (performance bias) Blinding of outcome assessment (detection bias) Incomplete
9/5/14. Objectives. Atrial Fibrillation (AF)
") Novel Anticoagulation for Prevention of Stroke in Patients with Atrial Fibrillation Objectives 1. Review current evidence on use of warfarin in individuals with atrial fibrillation 2. Compare the three
Novel Anticoagulation for Prevention of Stroke in Patients with Atrial Fibrillation Objectives 1. Review current evidence on use of warfarin in individuals with atrial fibrillation 2. Compare the three
Bayer Initiates Rivaroxaban Phase III Study to Support Dose Selection According to Individual Benefit-Risk Profile in Long- Term VTE Prevention
 Investor News Not intended for U.S. and UK Media Bayer AG Investor Relations 51368 Leverkusen Germany www.investor.bayer.com Long-term prevention of venous blood clots (VTE): Bayer Initiates Rivaroxaban
Investor News Not intended for U.S. and UK Media Bayer AG Investor Relations 51368 Leverkusen Germany www.investor.bayer.com Long-term prevention of venous blood clots (VTE): Bayer Initiates Rivaroxaban
Improving Anticoagulation Therapy Using Point-of-Care Testing and a Standardized Protocol. Ann Fam Med 2008;6(suppl 1):s28-s32. DOI: 10.1370/afm.739.
:s28-s32. DOI: 10.1370/afm.739.") Improving Anticoagulation Therapy Using Point-of-Care Testing and a Standardized Protocol Curtis A. Franke, MD 1 Lori M. Dickerson, PharmD 2 Peter J. Carek, MD, MS 2 1 Baylor Family Medicine at Uptown,
Improving Anticoagulation Therapy Using Point-of-Care Testing and a Standardized Protocol Curtis A. Franke, MD 1 Lori M. Dickerson, PharmD 2 Peter J. Carek, MD, MS 2 1 Baylor Family Medicine at Uptown,
Management for Deep Vein Thrombosis and New Agents
 Management for Deep Vein Thrombosis and New Agents Mark Malesker, Pharm.D., FCCP, FCCP, FASHP, BCPS Professor of Pharmacy Practice and Medicine Creighton University 5 th Annual Creighton Cardiovascular
Management for Deep Vein Thrombosis and New Agents Mark Malesker, Pharm.D., FCCP, FCCP, FASHP, BCPS Professor of Pharmacy Practice and Medicine Creighton University 5 th Annual Creighton Cardiovascular
Limitations of VKA Therapy
 Fibrillazione Atriale Non Valvolare Ischemia o Emorragia le Due Utopie Rivali nella Scelta dei NAO Gianluca Botto, MD, FESC, UO Elettrofisiologia, Dip Medicina Limitations of VKA Therapy Unpredictable
Fibrillazione Atriale Non Valvolare Ischemia o Emorragia le Due Utopie Rivali nella Scelta dei NAO Gianluca Botto, MD, FESC, UO Elettrofisiologia, Dip Medicina Limitations of VKA Therapy Unpredictable
} Most common arrhythmia. } Incidence increases with age. } Anticoagulants approved for AF
 Deniz Yavas, PharmD PGY-2 Ambulatory Care Pharmacy Resident Detroit Veterans Affairs Medical Center } Most common arrhythmia 0.4-1% of Americans (2.2 mil people) 1,2 } Incidence increases with age 6% (65
Deniz Yavas, PharmD PGY-2 Ambulatory Care Pharmacy Resident Detroit Veterans Affairs Medical Center } Most common arrhythmia 0.4-1% of Americans (2.2 mil people) 1,2 } Incidence increases with age 6% (65
Time of Offset of Action The Trial
 New Antithrombotic Agents DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant Amgen Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University What I am Talking About
New Antithrombotic Agents DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant Amgen Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University What I am Talking About
Kevin Saunders MD CCFP Rivergrove Medical Clinic Wellness Institute @ SOGH April 17 2013
 Kevin Saunders MD CCFP Rivergrove Medical Clinic Wellness Institute @ SOGH April 17 2013 Family physician with Rivergrove Medical Clinic Practice in the north end since 1985 Medical Director of the Wellness
Kevin Saunders MD CCFP Rivergrove Medical Clinic Wellness Institute @ SOGH April 17 2013 Family physician with Rivergrove Medical Clinic Practice in the north end since 1985 Medical Director of the Wellness
1/7/2012. Objectives. Epidemiology of Atrial Fibrillation(AF) Stroke in AF. Stroke Risk Stratification in AF
 Stroke in AF. Stroke Risk Stratification in AF") Objectives Atrial Fibrillation and Prevention of Thrombotic Complications: Therapeutic Update Andrea C. Flores Pharm.D Pharmacy Resident at the Miami VA Healthcare System Review the epidemiology, pathophysiology
Objectives Atrial Fibrillation and Prevention of Thrombotic Complications: Therapeutic Update Andrea C. Flores Pharm.D Pharmacy Resident at the Miami VA Healthcare System Review the epidemiology, pathophysiology
Speaker Disclosure. Outline. Pharmacist Objectives. Patient Case. Outline 9/4/2014
 Speaker Disclosure Matthew K. Pitlick, Pharm.D., BCPS St. Louis College of Pharmacy/VA St. Louis HCS mpitlick@stlcop.edu Matthew K. Pitlick, Pharm.D., BCPS declares no conflicts of interest, real or apparent,
Speaker Disclosure Matthew K. Pitlick, Pharm.D., BCPS St. Louis College of Pharmacy/VA St. Louis HCS mpitlick@stlcop.edu Matthew K. Pitlick, Pharm.D., BCPS declares no conflicts of interest, real or apparent,
New Oral Anticoagulants: Topic Brief
 New Oral Anticoagulants: Topic Brief June 9, 2015 High-Level Research Question In patients with nonvalvular atrial fibrillation (AF) or venous thromboembolic disease, or who have undergone surgery for
New Oral Anticoagulants: Topic Brief June 9, 2015 High-Level Research Question In patients with nonvalvular atrial fibrillation (AF) or venous thromboembolic disease, or who have undergone surgery for