Acute Hospitals in London: Sustainable and Financially Effective
|
|
|
- Junior Allison
- 8 years ago
- Views:
Transcription
1 Acute Hospitals in London: Sustainable and Financially Effective February
2 Acute Hospitals in London: Sustainable and Financially Effective Introduction 1. Health services in London have been improving. However, many challenges remain as the NHS in London seeks to create a clinically sustainable and financially effective provider landscape. These issues are raised with Ministers, other politicians and NHS leaders frequently, but in isolation. They present themselves in news coverage of clinical failures, finance and performance challenges, reports from the Care Quality Commission, the Tripartite Formal Agreement (TFA) 1 process, reviews undertaken by the Independent Reconfiguration Panel and service reconfiguration debates. This report brings a strategic perspective to the issues. 2. The report presents the output from a significant piece of strategic analysis that was undertaken between May 2011 and September 2011 by NHS London and covers the 18 acute NHS Trusts 2 in London yet to achieve Foundation Trust (FT) status. The analysis was designed to test the financial viability and clinical sustainability of each of the 18 Trusts. 3. The work concludes that the 18 Trusts have a productivity opportunity of between 1.168bn and 1.272bn 3, which could potentially be captured over the four years to 2014/15. Even if this unprecedented level of savings were achieved there would still be an aggregate deficit of 170m in 2014/15, with 13 of the 18 Trusts still in underlying deficit amounting to 233m. There are a number of factors that make this an optimistic assessment, including the Trusts being able to respond to decreases in activity and Trusts being able to keep their costs within the inflation that is captured within tariff. In modelling just one of the factors in the optimistic assessment, a 1 percent cost inflation sensitivity test 4 increases the financial gap to 329m, with all but two of the Trusts in underlying deficit amounting to 358m. Both these financial scenarios would compound the quality and safety challenges already apparent in some Trusts. 4. The report outlines these conclusions and proposes next steps, including a series of interventions to begin making a step change in acute providers capability to capture productivity opportunities as well as a number of different approaches for addressing the outstanding financial gap. 1 All NHS trusts yet to achieve Foundation Trust (FT) status must sign a Tripartite Formal Agreement (TFA) with the Department of Health and their Strategic Health Authority. Once agreed, the TFA sets out a journey for each NHS trust to enable it to pass strict tests on quality of care and on finances and is a public record of the commitments each trust has made to achieve FT status by a particular date. 2 The 18 organisations covered by the analysis were non-specialist acute NHS Trusts. Two specialist acute Trusts Great Ormond Street Hospital NHS Trust and the Royal National Orthopaedic Hospital NHS Trust were excluded from the analysis. 3 Potential productivity gains are based on benchmarking against peer groups bn based on achieving upper quartile productivity, 1.272bn on top 3 productivity (see technical annex). 4 Historically, Trusts have failed to constrain cost increases to NHS inflation assumptions 2
3 5. The work that has been undertaken was based on an analysis of 2010/11 financial results in combination with 2011/12 Operating Plans and the pressures evident within them. It is aligned to the work carried out by the Department of Health to look at the medium-term challenges faced by NHS Trusts with significant PFIs. It also builds on the TFA process and the necessary actions to ensure NHS Trusts reach FT status. Background 6. The case and opportunity for improving Londoners health and London s health services has been well understood for some years. Much of the case is universal to the NHS, but some is unique to London. London s NHS faces pressure from: increasing demand for healthcare; a growing, diverse, mobile and ageing population; changing patterns of disease and health; changing public expectations; and innovations in medical technology. All of this, alongside the slowing down in funding growth for the NHS, poses a significant challenge to London s healthcare system. 7. The NHS in London has made significant progress on improving the quality of some services such as cardiac, stroke, trauma and vascular. System-wide there is now a focus on improving cancer care, primary care and screening, with the newly-constituted London Health Improvement Board, chaired by the Mayor, agreeing priority actions for London. Locally, organisations are working with local government to progress integrated care initiatives, particularly focussed at patients with long-term conditions and the frail elderly. However, concerns relating to the safety and quality of many services remain. This is compounded by the financial challenges, which are a historic feature of the London health economy and are exacerbated by the need to contain funding growth over the next few years whilst continuing to improve services in line with quality standards, which adds a further financial pressure on Trusts, particularly the smaller ones. 8. In the summer of 2010, commissioners began to undertake a revised QIPP planning process for 2011/ /15. PCT clusters produced a series of commissioning intentions that would enable them to maintain financial balance over this period. Their plans were less ambitious than the Healthcare for London vision in terms of commissioning levers (eg. delivering more care in lower cost community settings, proactive management of patients with long-term conditions, improving productivity in primary care). Nonetheless, they resulted in 692m of pressure on the 18 Trusts covered in this analysis, in addition to 309m of net tariff deflation 5. This more than offset the underlying activity growth projected, resulting in an overall reduction in projected income for the 18 Trusts of 210m over the four-year period. Trusts were also under pressure to improve quality and safety, some elements of which would result in additional cost. 5 The overall reduction in the amount paid to a hospital Trust for a procedure to take account of expected efficiencies, more than offsetting cost inflation. 3
4 9. The multiple pressures on Trusts prevented most from creating credible Long Term Financial Plans and made agreeing TFAs difficult, with 14 of the 18 TFAs relating to Trusts covered in this analysis still to be signed off by the Department of Health at the time the analysis was undertaken. Therefore, NHS London decided to undertake a work programme with acute NHS Trusts between May 2011 and September 2011 Sustainable and Financially Effective (SaFE) to understand the individual positions of the Trusts in more depth, which would help in agreeing TFAs for each of the 18 Trusts. The ultimate aim of the work programme was to develop an approach to securing the highest quality acute care services in London, delivered by financially viable providers capable of becoming FTs. 10. SaFE provides a simulation based on a robust analysis of financial data and an initial analysis of quality and safety issues facing the NHS in London. It is consistent across London and determines whether the 18 acute Trusts can achieve FT status by 2014, taking into account current cost and income trajectories, quality / safety requirements and potential productivity improvements. Context 11. London has a relatively high number of acute NHS Trusts that have still not achieved FT status, compared with other Strategic Health Authority regions. The average catchment population of London s acute hospitals is lower than many other regions in the country (eg. around 265,000 per hospital in London compared to around 370,000 per hospital in East Midlands) and London has a wide variation between very big and relatively small hospital sites. Consequently, activity rates in some sites are low (except in the case of A&E attendances and maternity services for most sites in London) and this causes Trusts to experience clinical sustainability challenges, particularly because of medical staffing. These low activity rates, combined in some cases with relatively low productivity, mean some Trusts face major financial challenges in meeting their high fixed costs in the context of tightening economic conditions. 12. Some of London s acute Trusts currently treat some patients in a secondary care setting whose outcomes would be better if they were treated in community settings. This pattern of service provision shifts the financial burden to commissioners and means that London spends around 59 percent of its funding on acute care, slightly higher than the average elsewhere in the country. 13. London s commissioners aim to improve patients care and achieve financial sustainability by shifting the provision of care for many conditions, particularly those that are long-term, from the acute sector to primary, community and other settings, such as patients own homes. This approach - whilst securing the funding for investment in both primary and community care that is necessary to ensure that these sectors are equipped to deal with increased levels of activity and, at the same time, putting commissioners financial affairs on a sustainable footing - reduces or reverses the pattern of activity / income growth on which providers are reliant, at a time when they will also need to deal with the challenge of real terms reduction in tariff. 4
5 Analysis 14. Significant potential risks were identified to realising the ambition that all Trusts achieve FT status by Therefore, a deep financial analysis of the 18 acute Trusts was scoped, to confirm each organisation s likely long-term position and the potential for productivity improvement. This analysis was intended to enable a simulation of a range of potential responses to the risks to achieving clinically sustainable and financially effective services. 15. The approach taken in estimating a Trust s financial position for each year through to 2014/15 is set out in the technical annex to this report (see Annex A). But, in summary, the approach: took 2010/11 as the baseline starting point; took account of expected demand trends and cost pressures through to 2014/15; benchmarked productivity opportunities against a peer groups of trusts across the country; showed the resulting net surplus or deficit position on acute services at the end of each period; and added the contribution earned from community services, where these had been merged with an acute Trust, assuming a 3 percent surplus to include the inherent savings opportunity in managing these services in an integrated way. The approach was anchored in a detailed reconciliation to the Trust s 2011/12 plan and to the PCT Clusters commissioning intentions. Quality and Safety 16. In forecasting the position of the Trusts, it was felt critical to include the costs of meeting appropriate minimum standards of emergency and maternity care. These costs are necessary to ensure reliable provision of care. Clinical advice suggests meeting minimum standards of care will reduce mortality and morbidity. Further details are set out in Annex B. Conclusions 17. A maximum of 6 out of 18 Trusts are in a viable long-term financial position in their present form in 2014/15, even after the full percent productivity opportunity is realised. 18. The categorisation of the 18 Trusts is set out in the table below: 5
6 Category 1 Financially viable if productivity opportunities equal to their top quartile peer are achieved Category 2 Financially viable if productivity opportunities equal to the average of the top 3 peers are achieved Category 3 Financially viable if given a longer period to achieve the highest level of productivity opportunities Category 4 Not financially viable with productivity opportunities alone Royal Free Hampstead St George s Croydon Health Services Kingston Lewisham Barnet and Chase Farm 6 some additional capital expenditure modelled in, in view of significant estate deficiencies. Imperial College Healthcare has a significant productivity opportunity; however, it is beyond the 20 percent 7 threshold assumed achievable in 4 years. In theory, Imperial could achieve a 1 percent net surplus in 2016/17, but would have a cumulative deficit of at least 85m by this point. Barts and The London has a significant productivity opportunity beyond the 20 percent threshold. In theory, it could achieve a 1 percent net surplus by 2017/18, but would have a cumulative deficit of at least 23m by this point. Achieving this improvement will be challenging while the Trust relocates to its new buildings. Whittington Health is able to achieve a 1 percent net surplus by 2017/18 including a 3 percent surplus on its integrated community services. It will remain in cumulative breakeven in the intervening period. Ealing is only in Category 3 because of the integration of community services, which are assumed to be able to achieve a 3 percent net surplus. With this assumption, Ealing can achieve a 1 percent net surplus by 2015/16. It will remain in cumulative breakeven in the intervening period. West Middlesex large PFI 8 North Middlesex large PFI Barking, Havering and Redbridge Hospitals large PFI South London Healthcare large PFI Newham large PFI Whipps Cross some additional capital expenditure modelled in, in view of significant estate deficiencies North West London Hospitals may require additional capital expenditure (not modelled) Epsom and St Helier impact of hospital redevelopment comes in period beyond this analysis 6 Barnet and Chase Farm Trust is forecast to be in surplus in 2014/15. However, at site level Chase Farm is forecast to be losing 4.5m due to the additional costs of meeting new service standards and the cost of funding the estate redevelopment. 7 NHS experience and international case studies suggest there is no evidence of health organisations achieving more than a 20% productivity gain over 4 years see technical annex. 8 West Middlesex, North Middlesex, Barking, Havering and Redbridge Hospitals, South London Healthcare and Newham all have unitary charges above 10m. 6
7 19. Whilst only three of the Trusts covered by the analysis failed to achieve break even in 2010/11, further analysis 9 of their underlying positions indicates that, as in previous years, this was in many cases only possible with the benefit of significant non-recurrent income support and cost reductions. Stripped of these items, there were 11 underlying deficits within a net aggregate deficit of 108m. The individual financial positions are outlined in Annex A. 20. The Operating Plans for 2011/12, presented on a similar basis, show a 165m deficit, albeit with a slightly reduced number of individual deficit organisations. This deterioration, despite an unprecedented level of expected delivery from cost improvement programmes (6 percent in year), reflects front-loaded demand management plans by commissioners and significant cost pressures, partly driven by quality challenges, in excess of tariff funding. 21. Despite some improvement in the intervening years, driven by the sustained levels of productivity improvement modelled, the net deficit position of the 18 Trusts is projected to reach 170m in 2014/15, with only five organisations in surplus and only two achieving a surplus of at least 1 percent, compatible with achieving FT status. This includes a recurrent investment of 70m in relation to quality and safety as outlined in paragraph 16 above. 22. This analysis assumes cost inflation in line with national tariff assumptions for future years; this is modelled here at 2.5 percent, but the level of (funded) inflation has a negligible impact on the provider analysis. However, in practice acute Trusts across the country have generally been unable to contain cost inflation at the level assumed in tariff. We have, therefore, run a sensitivity analysis with an additional 1 percent cost inflation, similar to that experienced in both 2010/11 and 2011/12 (plans). In this scenario 16 Trusts are in deficit. Only Royal Free Hampstead and St George s remain viable. The net deficit is 329m. The individual financial positions are outlined in Annex A. Response 23. There have been many attempts to resolve the challenges of the capital s health care system the Tomlinson Report (1992), Turnberg Report (1998), reviews by the King s Fund (1992 and 1997) and, most recently, Healthcare for London (2007). It is clear that effective political, clinical and managerial leadership committed to working together will be required, if there is to be any chance of succeeding where others have failed. The success of the changes to London s stroke services shows how coordinated action, led by clinicians, can deliver significant improvement. 24. The analysis that has been undertaken paints a compelling picture of a serious problem. Doing nothing is not an option. 9 Analysis consisted of a desktop review by NHS London using centrally collected data. 7
8 Realising the productivity opportunity 25. The analysis undertaken by NHS London suggests that the 18 Trusts can theoretically realise productivity savings of 1.168bn by 2014/15. This would represent a dramatic and unprecedented improvement, greater than 5 percent per annum on a sustained basis. It requires challenging actions to be taken, and, if these productivity opportunities are not realised, the scale of the gap at the end of 2014/15 increases accordingly. When compared to an improving peer group the savings opportunities are: 421m (28.9%) in nursing from, for example, optimising skill mix, reducing agency use, increasing share of patient-facing time, and aligning staffing levels with clinical need; 184m (15.0%) in medical from, for example, higher utilisation and reducing downtime in theatres and outpatient services; 187m (32.0%) in scientific, technical and therapeutic staff from, for example, increasing utilisation through better scheduling and balancing staff skill mix in line with requirements; 177m ( 25.0%) in non-clinical staff from, for example, reducing nonvalue-added tasks (eg. redundant reporting) and better use of technology; 155m (13.9%) in clinical supplies from, for example, negotiating lower unit prices, standardising demand and using lower-cost options; and 45m (32.6%) from reducing other variable costs like laundry and catering. 26. To achieve this unprecedented scale of change in London, a number of building blocks are required: system leadership political, clinical and managerial to create a compelling narrative that explains why change is needed; strong Board-level and clinical leadership to drive productivity internally; timely and accurate information that provides insight into performance and productivity relative to peers; well-defined tools and the skills and capabilities to use them; and the incentives in place to drive high performance at the system, organisation, team and individual level. 27. While a detailed understanding about the challenge faced by each Trust is required, NHS London s initial assessment suggests that few have approached delivering significant productivity gains with sufficient leadership focus. This can be seen across a number of dimensions: at present there is no consistent shared understanding of the urgent need to take radical action on productivity, and the change narrative across London remains rooted in the quality story of Healthcare for London and High Quality Care For All, which needs to be expanded to give sufficient weight to financial imperatives and value for money; there are systemic weaknesses in Board capabilities in some Trusts; there is, in many organisations, a lack of actionable information linking operational levers to financial outcomes at the service line level; 8
9 tools exist to support productivity improvements, but these have not been systematically applied or used in a way that releases resources; while crude organisational incentives exist via the tariff deflator, there are no effective incentives at the team or individual level; and the failure regime is not sufficiently linked to productivity and has not yet been approved for use. 28. Given this starting point, the Trusts need to make unprecedented changes, and the system needs to support this. Any notion that maintaining the status quo is acceptable needs to be dispelled; clinical processes need transforming; and to ensure sustainability, new ways of working must be embedded. This means that leaders will need to develop the capacity to identify improvement opportunities constantly, wherever they lie; they need to do so with real urgency and intent; and do so at the same time as providing evidence and assurance that the impact on the quality and safety of care and services is not compromised. It will also require a commitment at system level so everyone is clear about the kinds of change that are both possible and expected and which will be supported by clinicians, staff, the public and their representatives. 29. The most significant productivity gain can be made in nursing. There is no clear evidence that investment in simply increasing the number of nurses as the mechanism to increase the quality of nursing care is a guarantee of good patient care and many of the best health organisations in the world combine high productivity and excellent quality. This suggests that other factors, such as ways of working, may be more important than resourcing levels per se and, whilst some individual clinical areas will undoubtedly require more resource (including increasing the numbers working in those areas), efficiency improvements will enable others to deliver improved quality with fewer staff. 30. To transform clinical processes, standards will need to be agreed - and Trusts will need to apply them consistently. Clinicians able to lead the implementation of new standards will need to be identified, in the same way that they lead the quality debate. To ensure these changes become embedded, Trusts need sharper information, incentives and robust processes. All of this will ensure that change initiatives move from being ways of making existing business models work harder to radical new ways of delivering high quality service. 31. To embed these changes, four potential cross-cutting actions have been identified: a) Development of a compelling narrative, explaining the need for unprecedented focus and change in both quality and operational efficiency. b) Investment in leadership development and capability building for Boards and clinical leaders, sufficient to equip them to drive change. c) Integration of productivity opportunity realisation with performance regimes to provide graduated interventions in the event of Trusts not delivering. This should link the support of deficits and financing of historic debt to changes in operating models and productivity. 9
10 d) Trusts providing sufficiently detailed operational data to allow assessment of progress against the productivity requirement. 32. In addition, the work undertaken in this programme identified a number of initiatives that could be taken forward to support Trusts to make the necessary improvements. Examples of these included: supporting one or more organisations to become a model hospital ; creating targeted incentives for nurses to work in deprived areas and/or failing Trusts; establishing staffing banks including nurses, across a network of Trusts; consolidating or outsourcing clinical support such as pathology; and increasing the leverage and scope of the London Procurement Programme. 33. It would also be important to look at merging some Trusts to save money on back office functions, thereby reducing bureaucracy. But mergers and drives to improve productivity alone will not be sufficient to ensure hospitals across London can balance their books and continue to provide excellent care. Trusts are currently trying to sustain services over too many sites. Therefore, a planned process of capacity reduction, leading to higher utilisation in the remaining sites, could resolve some of the financial issues and clinical quality challenges. However, currently any intervention made by the system takes far too long to implement, either because of insufficient commitment and collaboration in taking action or because of weak leadership. Given that delay is costly, how to streamline processes needs to be worked through. Conclusion and Next Steps 34. The SaFE analysis shows that London s acute providers are not sustainable in their present form. Substantial progress can be made if Trusts are able to meet world-class improvements in productivity levels. In itself, this would be a challenging enough problem, as organisations have so far not been able to make progress at the required pace and scale. However, the most important point to emerge from the analysis is that most organisations cannot achieve financial and clinical sustainability in their present form, even if they do meet these productivity benchmarks. 35. A series of meetings was held in September 2011 between NHS London and the Boards of each of the 18 acute NHS Trusts with the aim of securing a deep understanding of the SaFE analysis and the challenges it presents. The Trusts responses to the challenges are reflected in updated TFAs, which have since been published. 36. While each Trust has its own unique challenges, a number of cross-cutting themes are being addressed, including: Productivity Working with the Department of Health, a programme of initiatives to support, monitor and drive the delivery of the 1.2bn improvement in Trust productivity is being finalised. This includes a productivity support programme for Trusts, based on productivity diagnostic linked to a network of accredited tools (with the Department of Health and the NHS Institute for Innovation and 10
11 Improvement), intensive exploration with top peer organisations of how to realise the productivity potential, and developing more detailed information for Trusts to identify the right productivity opportunities. Last month Heather Lawrence, chief executive of Chelsea and Westminster Hospital NHS Foundation Trust, joined NHS London to lead the work programme. Given the centrality of clinical productivity to the programme, Trish Morris-Thompson, NHS London s Chief Nurse, and Dr Andy Mitchell, NHS London s Medical Director, are establishing dedicated transformational programmes within this overall initiative, led by top clinicians from across London and drawing on external expertise. Board capability NHS London plans to invest in leadership development and capability building for Trust Boards and clinical leaders, to equip them to drive change. The Department of Health s Board Governance Assurance Framework (BGAF), launched last month, is mandatory for all NHS Trusts as part of the FT assurance process. It has begun to be rolled out across London, with those Trusts that are due to submit their FT application to the Department in April 2012 being the first to undergo this process. Where relevant, other Trusts are being encouraged to adopt BGAF as soon as possible. Quality and Safety - Improving the quality and safety of acute emergency and maternity services (in response to the issues highlighted in Annex B) has been identified by the NHS in London as one of the key priorities to deliver by 31 March The programme should address the current variation that currently exists in service arrangements and patient outcomes for these services between hospitals and within hospitals, and between weekdays and weekends. It builds on the case for change in adult emergency services - which demonstrated the marked variation in acute medicine and emergency general surgery services and outcomes for patients across London and commissioning standards that have subsequently been agreed. A review of paediatric emergency services is under way to develop clinical standards to ensure children also access high quality and safe care. The development of minimum clinical standards will now be expanded to include all acute emergency and maternity services. Mergers and service change - The NHS in London is looking at merging some Trusts to save money on back office functions, reducing bureaucracy and saving public money. For example, the proposed merger of Barts and The London NHS Trust, Newham University Hospital NHS Trust and Whipps Cross University Hospital NHS Trust would alone save 32m while improving care at the same time. At the same time, the NHS in London is also taking forward hospital improvements that have already been agreed for the Chase Farm site in Enfield, the Queen Mary s Sidcup site in Bexley and the King George site in Ilford. Finally, Clinical Commissioning Groups and hospital clinicians, supported by the relevant PCT Clusters, are also reviewing hospital services in north west and south west London and expect to be asking the public for their views on options for improving those services through formal consultations later this year. 11
12 Annex A Sustainable and Financially Effective (SaFE) Methodology Introduction The objective of this work is to simulate the financial performance of the 18 acute non-foundation Trusts (non-fts) in London and to assess their resilience in meeting the requirements to become Foundation Trusts (FTs) by SaFE estimates Trusts financial position in 2014/15 in 5 steps: 1 Establish 10/11 baseline 2 Estimate income changes 11/12-14/15 3 Estimate cost changes 11/12-14/15 4 Develop yearby-year forecast 5 Evaluate financial outlook Trust s underlying position in 10/11 Based on: net activity change; tariff deflation; nonclinical income changes As a result of changes in activity, cost inflation and necessary investments in quality, offset by productivity improvements Based on modelled cost and income changes Against 1% surplus target 1 Establish 2010/11 Baseline SaFE uses Trusts 2010/11 final accounts to establish their underlying position in 2010/11. The underlying position is calculated net of non-recurrent income (such as transitional funding) and costs (such as redundancy costs and additional temporary costs of double-running new services). 2 Estimate Income Changes by 2014/15 Income is forecast until 2014/15 based on four factors: Net clinical activity growth based on commissioners intentions. According to commissioning plans, projected clinical activity changes are driven by three sub-components: o Underlying demand growth (as projected by commissioners) leading to activity increases for providers. Acute activity across London is expected to grow year on year, driven by increases in population, the ageing of population and additional demand caused by increasing numbers of people with chronic conditions, innovations in medical technology and changing public expectations. 12
13 o Reductions in activity driven by commissioners demand management QIPP plans, net of any reinvestment in services provided by Trusts in the community; and o Agreed changes to specialist acute care (eg. stroke care). Commissioners have estimated these factors by PCT (as a proxy for emerging clinical commissioner groups) by year and converted these into impacts on individual providers. Additional analysis has been undertaken to estimate demand management from commissioners outside London. The overall effect of these three sub-components is a small net increase in acute activity over the four years of the analysis (approximately 0.5% per annum), but this impact varies significantly by Trust. Price reduction of 1.5% per year across both PbR and non-pbr clinical income, reflecting likely deflation of national tariff prices in line with PbR policy. Forecast of non-clinical income (R&D, education and training) based on NHS London existing analysis. The first year forecasts for 2011/12 were calibrated with Trusts own Operating Plans submitted to NHS London (for income and cost elements). 3 Estimate Cost Changes by 2014/15 Forecasted cost changes were based on: Net impact of activity changes: Cost scaling assumptions have been calculated for individual Trusts based on their internal cost structure and assumptions on how these scale with activity. This analysis leads to cost scaling of assumptions of between 70 and 80% for increases in activity and between 55 and 65% for reductions in activity. In other words, all other things being equal, Trusts make a 20 to 30% marginal profit on activity increases and a 35 to 45% marginal loss on activity reductions. These margins reflect the high proportion of acute Trusts costs that are fixed or semi-variable. Additional PFI costs: These are based on DH schedules for existing PFI schemes and new hospital building in London (eg. Barts and the Royal London). Additional costs to meet new service standards: These costs were estimated based on the required number of additional consultants to cover the rotas, given the new service standards. Capital expenditure: Cost forecasts include the impact on Income & Expenditure of the agreed capital expenditure programmes, and potential programmes to bring estates to required minimum standards where initial 13
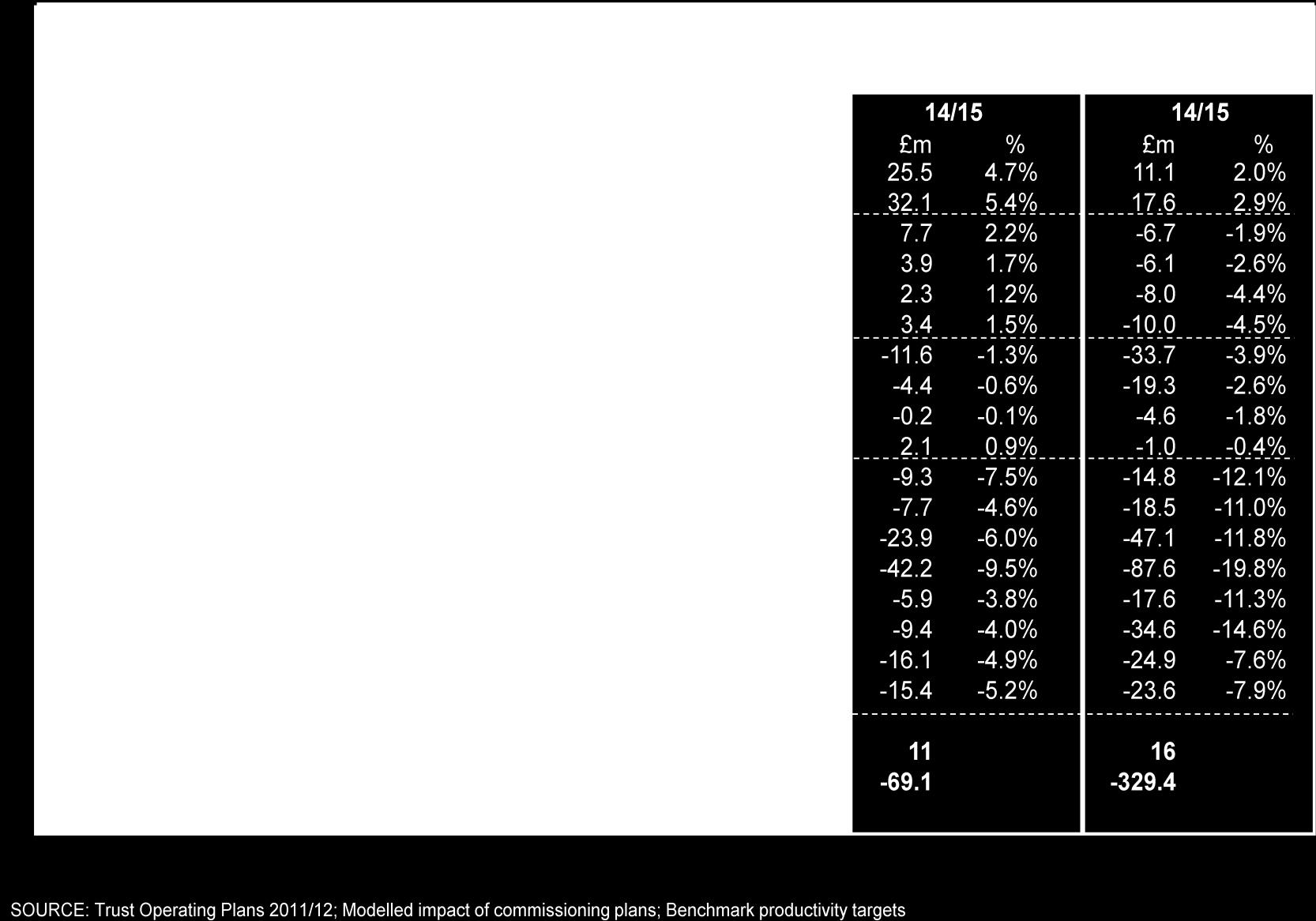
14 plans have been developed (this is particularly important for sites with significant additional capital expenditure requirements, such as Whipps Cross and Chase Farm). Cost inflation: Costs are inflated using NHS cost inflation rates, assumed to be in line with current tariff assumptions at 2.5% (see below for sensitivity). Productivity: For each Trust the projected costs are reduced by the estimated productivity improvement opportunities (ie. reduction in unit costs driven by a more efficient utilisation of resources). Productivity improvement (sixth bullet above) is one of the most significant cost drivers for the Trusts, and thus the estimation of productivity improvement opportunities is a critical part of the analysis. Delivering significant improvements in productivity is central to ensuring a cost effective provider landscape in London. SaFE estimates potential productivity improvements through a comprehensive and rigorous national benchmarking exercise. Each Trust was benchmarked against its peers. Peer groups were identified by statistical analysis of factors correlated to productivity. The factors used in the analysis are: teaching / non-teaching; multi site / single site; size of Trust (based on turnover). Other factors considered were urban vs non-urban, deprivation, foreign language rates in the local community and nurse turnover; however, the data available did not enable us to establish a statistically robust correlation between these other factors and Trusts productivity. Five national peer groups, comprising both non-fts and FTs, relevant to the 18 London acute non-fts were used for this analysis. Trusts in the bottom quartile for Hospital Standardised Mortality Rate (HSMR) were excluded due to potential issues with quality 10. The resulting comparator Trusts are summarised in the table below, comprising: a) Teaching, multi-site, large (turnover > 300 million): 25 Trusts b) Non-teaching, single site, small (turnover < 200 million): 33 Trusts c) Non-teaching, single site, medium (turnover 200 million to 400 million): 17 Trusts d) Non-teaching, multi-site, medium (turnover 200 million to 400 million): 29 Trusts e) Non-teaching, multi-site, large (turnover > 400 million) were in practice benchmarked against all non-teaching hospitals due to small sample size, and individual sites being comparable to smaller Trusts 10 For the peer groups to be relevant to the productivity programme going forward, the position of Trusts in relation to their quality and safety outcomes, including HSMR, will need to be reviewed on an ongoing basis to ensure that they should either be included or excluded in the peer group. 14

15 15
16 In addition a quality floor was assumed to avoid unsustainable nursing cost reductions. The modelling assumes no Trust reduces nursing costs below that corresponding to 8 nurse hours per inpatient bed day. This limited the nursing productivity gain opportunity for four Trusts: Barking, Havering and Redbridge Hospitals; Epsom & St Helier; Barnet & Chase Farm; and (marginally) Croydon Health Services. Two levels of potential savings were modelled for each London Trust: Opportunity based on peer at upper quartile threshold Opportunity based on average of top 3 peers An additional 2% p.a. improvement above benchmark opportunity is modelled to reflect the continuing improvement of peers over the four-year period of the modelling. An upper limit of a 20% reduction on the total starting cost base over four years has been assumed, based on an assessment of the maximum sustained cost improvement achieved both within and outside the NHS/UK. This translates to a reduction of 5.4% of the total starting cost base per year, or around 6.6% on the variable and semi-variable costs. 4 Develop Year-by-Year Financial Forecasts Modelling all the above gives a year-by-year financial position for each Trust, which is used to analyse each Trust s in-year net surplus / deficit and the accumulated net surplus / deficit over time. The core analysis considered only the acute services provided by the Trusts concerned to ensure consistency with the commissioning intentions on the income side. However, some of the Trusts in the analysis have been or are being merged with local community services providers previously managed by PCTs. In these cases we have additionally modelled the impact of the community services, assuming a 3% surplus to allow for integration synergies. The analysis forecasts a deterioration in the acute position from a net underlying deficit in 2010/11 of - 109m to - 182m in 2014/15. When offset against 12m additional community services contribution, this results in a net underlying deficit of the 18 Trusts in aggregate of 170m in 2014/15 (all figures in current prices). 16

17 17
18 A number of potential downsides to Trusts financial projections have not been included in the above modelling: Cost scaling was undertaken as described above. However, some Trusts Operating Plans and/or in-year performance imply higher scaling (less margin) for increases and limited / no scaling with decreases. If these alternative cost scaling assumptions were modelled for the future years, then the projected financial position of Trusts would be significantly worse. A 2.5% cost inflation assumption was made. This is aligned with the net 1.5% tariff deflation, and alternative assumptions regarding levels of inflation would not have a material impact on the financial outcomes for Trusts as long as they were reflected in the construction of tariff. However, recent experience, including 2011/12 Operating Plans, suggests that many Trusts are experiencing a significantly higher cost inflation than the tariff assumes. A sensitivity analysis was conducted to assess the impact of 1% inflation above the level included in tariff and indicated an additional cost pressure rising to 160m, which would take the 2014/15 deficit to - 330m. No allowance is made in income projections of any additional price pressures from new tariff rules or the risk of commissioners imposing income caps in the event of unaffordable activity growth. 5 Evaluate Financial Outlook Each Trust s financial outlook was evaluated against a benchmark of 1% surplus, which is viewed as a prerequisite for the more complex set of metrics applied by Monitor for potential FTs. Trusts were placed into 4 categories depending on the evaluation: 1. Trusts that can achieve 1% net surplus by 2014/15 by delivering top quartile productivity opportunity. As described above, this is the level of productivity that the top quartile peer achieves now plus a further 2% annual improvement by the peer, capped at a total improvement of 20% over the period 2. Trusts that can achieve 1% net surplus by 2014/15 by delivering top 3 peers productivity, including the additional 2% p.a. and capped at 20% 3. Trusts, whose achievement of a 1% surplus is constrained by the 20% cap, but who would ultimately reach the target surplus level in the period beyond 14/ Trusts that cannot achieve 1% surplus even over an extended period. The outcome is the categorisation of the 18 acute London NHS Trusts into these 4 categories. The following table sets out the results by Trust: 18
19 19
20 Annex B Quality and Safety Emergency care 1. Numerous reports highlight issues relating to the provision of emergency care services and a consistent message from them is that early involvement of senior medical personnel in assessment and subsequent management of many acutely ill patients improves outcomes. Therefore, in March 2011, NHS London commissioned a clinician-led review of acute emergency services across London. 2. A self-reported Trust survey shows significant variation between clinical staffing provided on weekdays compared to weekends. Findings include: Consultant cover in acute medicine and emergency general surgery at the weekends, when compared to cover during the week, is halved; Only three sites in London reported that consultants always review both acute medical and emergency surgery patients within the recommended 12 hours; and 50% of sites reported that consultants are not always freed from other clinical duties when on-call, therefore reducing their focus on emergency patients even when on-site. 3. Admission to hospitals at weekends is associated with a significantly increased risk of death 14. When applied to London, the risk is in excess of 10%, meaning that there will be more than 500 deaths across the capital per year that need not have occurred. 4. The reasons for this are not entirely clear, but are likely to be multi-factorial. There may be an association with the severity of illness of these patients, in that they might be intrinsically more sick. This is an area of continuing research. However, we know that our systems and processes for dealing with ill patients in London s hospitals at weekends are variable. The relationship between improved outcomes and the availability of experienced, senior medical staff with the ability to make appropriate decisions has been highlighted in many reports. There is further evidence emerging from the Royal College of Physicians that draws this correlation more clearly. 5. In services where there is more consistency and uniformity of provision, such as with stroke and cardiac services, which function throughout 24-hour periods, one would expect to see this relative risk reduce. This is the case with 11 National Confidential Enquiry into Patient Outcome and Death. (2007) - Emergency admissions: A step in the right direction, NCEPOD 12 Royal College of Surgeons (2011) Emergency Surgery: standards for unscheduled surgical care Guidance for providers, commissioners and service planners, The Royal College of Surgeons of England 13 Royal College of Physicians. (2007) Acute Medical Care: The right person, in the right setting first time. Report of the acute medicine task force. Royal College of Physicians 14 Aylin et al. (2010). Weekend mortality for emergency admissions. A large, multicentre study. Quality and Safety in Healthcare. 19:
21 myocardial infarction; we also hope to demonstrate this with regard to stroke and trauma. 6. It can be postulated that across the health system in London the most fragile and ill patients are admitted to hospital at a time when senior decision-making capacity and the required support systems are least available. The acute emergency services review demonstrates huge variability. For the most part, smaller hospitals have the least comprehensive cover. For London, this represents a significant and urgent clinical problem in relation to quality and safety that must be explored further and addressed as a priority. 7. Therefore as part of the review, clinical expert panels, informed by a patients panel, have developed a set of commissioning standards to address the clinical case for change, namely the variation in adult emergency care service provision across London and the marked variation in working patterns that takes place overnight and during the weekend, compared to those during normal working hours. Significantly, the standards are minimum standards of care and not standards that hospitals may aspire to achieve over time. They represent the minimum quality of care that patients admitted as an emergency should expect to receive in every hospital in London that accepts patients on an emergency basis. 8. The financial implications for the 18 acute Trusts to meet these recommended minimum standards for on-call 24/7 rotas, together with appropriate 24/7 consultant cover for A&E departments and anaesthetics, are included in the analysis for sites where this is necessary. Maternity care 9. There has been a 30 percent increase in the number of births in London in 10 years. 55 percent of women who use London s maternity services are born outside the UK. London has the most complex case mix in terms of pre-existing medical conditions, previous obstetric outcome and complex social factors. London's maternity services do not perform uniformly well, with unacceptable inequalities in outcomes. Royal College guidance emphasises the importance of midwives, one-to-one care during labour and increased presence of consultant obstetricians on labour wards. The 2007 Healthcare Commission national review of maternity services highlighted London s services as performing very poorly when compared nationally. One of the main issues was women feeling they are being left alone in labour. 10. London s Trusts have struggled to improve their performance. Due to concerns about the rate of maternal deaths in the capital 19.3 deaths per 100,000 maternity episodes in 2009 and the first half of 2010 a review commissioned into 34 deaths showed 26 had avoidable factors, some of which may have contributed to the outcome. 11. Addressing these concerns requires Trusts to ensure they have appropriate staffing levels of both midwives and consultant obstetricians. The analysis 21
22 includes the cost requirements of meeting the consultant presence requirements for each of the sites where they do not currently do so. 22
North Middlesex University Hospital NHS Trust. Annual Audit Letter 2005/06. Report to the Directors of the Board
 North Middlesex University Hospital NHS Trust Annual Audit Letter 2005/06 Report to the Directors of the Board 1 Introduction The Purpose of this Letter 1.1 The purpose of this Annual Audit Letter (letter)
North Middlesex University Hospital NHS Trust Annual Audit Letter 2005/06 Report to the Directors of the Board 1 Introduction The Purpose of this Letter 1.1 The purpose of this Annual Audit Letter (letter)
HARINGEY CLINICAL COMMISSIONING GROUP MAY 2013 GOVERNING BODY 2013/14 FINANCIAL PLAN
 HARINGEY CLINICAL COMMISSIONING GROUP MAY 2013 GOVERNING BODY 2013/14 FINANCIAL PLAN 1. Introduction The purpose of this paper is to provide an update to the Governing Body of the CCGs 2013/14 financial
HARINGEY CLINICAL COMMISSIONING GROUP MAY 2013 GOVERNING BODY 2013/14 FINANCIAL PLAN 1. Introduction The purpose of this paper is to provide an update to the Governing Body of the CCGs 2013/14 financial
THE QUALITY OF MATERNITY SERVICES IN LONDON: A SUMMARY OF THE HEALTHCARE COMMISSION SURVEYS KEY MESSAGES FOR LONDON:
 THE QUALITY OF MATERNITY SERVICES IN LONDON: A SUMMARY OF THE HEALTHCARE COMMISSION SURVEYS KEY MESSAGES FOR LONDON: London is different: the mobility and diversity of London s pregnant mothers together
THE QUALITY OF MATERNITY SERVICES IN LONDON: A SUMMARY OF THE HEALTHCARE COMMISSION SURVEYS KEY MESSAGES FOR LONDON: London is different: the mobility and diversity of London s pregnant mothers together
TRUST BOARD PUBLIC SEPTEMBER 2014 Agenda Item Number: 163/14 Enclosure Number: (4) 2015/16 Business Planning Board Discussion Paper
 2015/16 Business Planning Board Discussion Paper") TRUST BOARD PUBLIC SEPTEMBER 2014 Agenda Item Number: 163/14 Enclosure Number: (4) Subject: Prepared by: Sponsored & Presented by: Purpose of paper Key points for Trust Board members Options and decisions
TRUST BOARD PUBLIC SEPTEMBER 2014 Agenda Item Number: 163/14 Enclosure Number: (4) Subject: Prepared by: Sponsored & Presented by: Purpose of paper Key points for Trust Board members Options and decisions
Financial Strategy 5 year strategy 2015/16 2019/20
 Item 4.3 Paper 15 Financial Strategy 5 year strategy 2015/16 2019/20 NHS Guildford and Waverley Clinical Commissioning Group Medium Term Financial Strategy / Finance and Performance Committee May 2015
Item 4.3 Paper 15 Financial Strategy 5 year strategy 2015/16 2019/20 NHS Guildford and Waverley Clinical Commissioning Group Medium Term Financial Strategy / Finance and Performance Committee May 2015
1. Introduction. 2. Context
 Shaping a Healthier Future for North West London consultation response by Richmond upon Thames Health, Housing and Adult Services Overview and Scrutiny Committee. 1. Introduction Shaping a Healthier Future
Shaping a Healthier Future for North West London consultation response by Richmond upon Thames Health, Housing and Adult Services Overview and Scrutiny Committee. 1. Introduction Shaping a Healthier Future
Draft financial impact assessment of draft new standards for paediatric cardiac and adult congenital heart disease services
 ANNEX C Draft financial impact assessment of draft new standards for paediatric cardiac and adult congenital heart disease services Executive Summary 1. The aim of the new Congenital Heart Disease review
ANNEX C Draft financial impact assessment of draft new standards for paediatric cardiac and adult congenital heart disease services Executive Summary 1. The aim of the new Congenital Heart Disease review
Proposed 5 year clinical and financial plan
 Proposed 5 year clinical and financial plan Introduction The Trust s financial problems stem from the major investment into the estate, to replace inadequate and inappropriate Victorian workhouse buildings
Proposed 5 year clinical and financial plan Introduction The Trust s financial problems stem from the major investment into the estate, to replace inadequate and inappropriate Victorian workhouse buildings
Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014
 TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Walsall Healthcare NHS Trust NHS West Midlands Department of Health Introduction
TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Walsall Healthcare NHS Trust NHS West Midlands Department of Health Introduction
Financial performance
 Financial performance In our first NHS Financial Temperature Check briefing 2 we noted the number of organisations that were overspending or reporting a deficit has increased since the 2012/13 financial
Financial performance In our first NHS Financial Temperature Check briefing 2 we noted the number of organisations that were overspending or reporting a deficit has increased since the 2012/13 financial
Progress on the System Sustainability Programme. Submitted to: NHS West Norfolk CCG Governing Body, 31 July 2014
 Agenda Item: 9.1 Subject: Presented by: Progress on the System Sustainability Programme Dr Sue Crossman, Chief Officer Submitted to: NHS West Norfolk CCG Governing Body, 31 July 2014 Purpose of Paper:
Agenda Item: 9.1 Subject: Presented by: Progress on the System Sustainability Programme Dr Sue Crossman, Chief Officer Submitted to: NHS West Norfolk CCG Governing Body, 31 July 2014 Purpose of Paper:
Anaesthetics, Pain Relief & Critical Care Services Follow-Up Study REGIONAL REPORT. Performance Review Unit
 Anaesthetics, Pain Relief & Critical Care Services Follow-Up Study REGIONAL REPORT Performance Review Unit CONTENTS page I INTRODUCTION... 2 II PRE-OPERATIVEASSESSMENT... 4 III ANAESTHETIC STAFFING AND
Anaesthetics, Pain Relief & Critical Care Services Follow-Up Study REGIONAL REPORT Performance Review Unit CONTENTS page I INTRODUCTION... 2 II PRE-OPERATIVEASSESSMENT... 4 III ANAESTHETIC STAFFING AND
Submitted to: NHS West Norfolk CCG Governing Body, 29 January 2015
 Agenda Item: 11.2 Subject: Draft Financial Plan 2015/16 Presented by: John Ingham, Chief Financial Officer Submitted to: NHS West Norfolk CCG Governing Body, 29 January 2015 Purpose of Paper: For information
Agenda Item: 11.2 Subject: Draft Financial Plan 2015/16 Presented by: John Ingham, Chief Financial Officer Submitted to: NHS West Norfolk CCG Governing Body, 29 January 2015 Purpose of Paper: For information
EXECUTIVE SUMMARY FRONT SHEET
 EXECUTIVE SUMMARY FRONT SHEET Agenda Item: Meeting: Quality and Safety Forum Date: 09.07.2015 Title: Monthly Board Report- Publication of Nursing and Midwifery Staffing Levels June 2015 Exception Report
EXECUTIVE SUMMARY FRONT SHEET Agenda Item: Meeting: Quality and Safety Forum Date: 09.07.2015 Title: Monthly Board Report- Publication of Nursing and Midwifery Staffing Levels June 2015 Exception Report
RCN London Safe Staffing Report 2014
 RCN London Safe Staffing Report 2014 RCN Legal Disclaimer This publication contains information, advice and guidance to help members of the RCN. It is intended for use within the UK but readers are advised
RCN London Safe Staffing Report 2014 RCN Legal Disclaimer This publication contains information, advice and guidance to help members of the RCN. It is intended for use within the UK but readers are advised
London Health Libraries Induction 12 th May 2011. The NHS in London
 Induction 12 th May 2011 The NHS in London Alan Fricker Knowledge & Library Service Manager Newham University Hospital NHS Trust Outline NHS structure Trust functions Regulators Clinical governance Policy
Induction 12 th May 2011 The NHS in London Alan Fricker Knowledge & Library Service Manager Newham University Hospital NHS Trust Outline NHS structure Trust functions Regulators Clinical governance Policy
EXPLANATORY MEMORANDUM TO THE SOUTH LONDON HEALTHCARE NATIONAL HEALTH SERVICE TRUST (APPOINTMENT OF TRUST SPECIAL ADMINISTRATOR) ORDER 2012
 ORDER 2012") EXPLANATORY MEMORANDUM TO THE SOUTH LONDON HEALTHCARE NATIONAL HEALTH SERVICE TRUST (APPOINTMENT OF TRUST SPECIAL ADMINISTRATOR) ORDER 2012 2012 No. 1806 AND THE SOUTH LONDON HEALTHCARE NATIONAL HEALTH
EXPLANATORY MEMORANDUM TO THE SOUTH LONDON HEALTHCARE NATIONAL HEALTH SERVICE TRUST (APPOINTMENT OF TRUST SPECIAL ADMINISTRATOR) ORDER 2012 2012 No. 1806 AND THE SOUTH LONDON HEALTHCARE NATIONAL HEALTH
Delivering in a challenging environment
 Trust Development Authority Delivering in a challenging environment Refreshed plans for 2015/16 Planning Guidance for NHS Trust Boards December 2014 Delivering in a challenging environment: refreshed plans
Trust Development Authority Delivering in a challenging environment Refreshed plans for 2015/16 Planning Guidance for NHS Trust Boards December 2014 Delivering in a challenging environment: refreshed plans
South West London 5 Year Strategic Plan South West London Collaborative Commissioning
 South West London 5 Year Strategic Plan South West London 5 Year Strategic Plan 20 th June 2014 South West London 5 Year Strategic Plan Table of Contents Chapter 1: Introduction... 1 Chapter 2: Vision...
South West London 5 Year Strategic Plan South West London 5 Year Strategic Plan 20 th June 2014 South West London 5 Year Strategic Plan Table of Contents Chapter 1: Introduction... 1 Chapter 2: Vision...
2013-18 Business Plan. Executive Summary UK Shared Business Services Ltd
 2013-18 Business Plan Executive Summary UK Shared Business Services Ltd Published June 2013 Contents I Introduction 3 II Executive Summary 6 Introduction: Geared for Growth in the Service of our Customers
2013-18 Business Plan Executive Summary UK Shared Business Services Ltd Published June 2013 Contents I Introduction 3 II Executive Summary 6 Introduction: Geared for Growth in the Service of our Customers
NORTHUMBERLAND, TYNE AND WEAR NHS FOUNDATION TRUST BOARD OF DIRECTORS MEETING
 NORTHUMBERLAND, TYNE AND WEAR NHS FOUNDATION TRUST Meeting Date: 25 March 2015 BOARD OF DIRECTORS MEETING Title and Author of Paper: 2015/16 Budget & Financial Plans 15/16 & 16/17 James Duncan, Deputy
NORTHUMBERLAND, TYNE AND WEAR NHS FOUNDATION TRUST Meeting Date: 25 March 2015 BOARD OF DIRECTORS MEETING Title and Author of Paper: 2015/16 Budget & Financial Plans 15/16 & 16/17 James Duncan, Deputy
A Health and Wellbeing Strategy for Bexley Listening to you, working for you
 A Health and Wellbeing Strategy for Bexley Listening to you, working for you www.bexley.gov.uk Introduction FOREWORD Health and wellbeing is everybody s business, and our joint aim is to improve the health
A Health and Wellbeing Strategy for Bexley Listening to you, working for you www.bexley.gov.uk Introduction FOREWORD Health and wellbeing is everybody s business, and our joint aim is to improve the health
WP6: Costing and pricing of acute hospital services in England. Centre for Health Economics, York, UK
 WP6: Costing and pricing of acute hospital services in England Centre for Health Economics, York, UK Contents Structure of NHS The flow of funds Types of contract Hospital contracts before 2004 Tariff
WP6: Costing and pricing of acute hospital services in England Centre for Health Economics, York, UK Contents Structure of NHS The flow of funds Types of contract Hospital contracts before 2004 Tariff
Strategic Plan Document for 2013-14. Central Manchester University Hospitals NHS Foundation Trust
 Strategic Plan Document for 2013-14 Central Manchester University Hospitals NHS Foundation Trust 1 Contents Page 1. Executive Summary 3 2. Strategic Context and Direction 4 2.1 Strategic Position 2.2 Commissioner
Strategic Plan Document for 2013-14 Central Manchester University Hospitals NHS Foundation Trust 1 Contents Page 1. Executive Summary 3 2. Strategic Context and Direction 4 2.1 Strategic Position 2.2 Commissioner
A&E Recovery & Improvement Plan
 Engagement and Patient Experience Committee (A Sub-Committee of NHS Southwark CCG Governing Body) ENCLOSURE B A&E Recovery & Improvement Plan DATE OF MEETING: September 2013 CCG DIRECTOR RESPONSIBLE: Tamsin
Engagement and Patient Experience Committee (A Sub-Committee of NHS Southwark CCG Governing Body) ENCLOSURE B A&E Recovery & Improvement Plan DATE OF MEETING: September 2013 CCG DIRECTOR RESPONSIBLE: Tamsin
COUNCIL OF GOVERNORS 23 rd June 2014
 Paper 7.2 COUNCIL OF GOVERNORS 23 rd June 2014 TITLE EXECUTIVE SUMMARY The Council is asked to: Submitted by: Complaints procedure Driven by the national context of changes in expectation, scrutiny and
Paper 7.2 COUNCIL OF GOVERNORS 23 rd June 2014 TITLE EXECUTIVE SUMMARY The Council is asked to: Submitted by: Complaints procedure Driven by the national context of changes in expectation, scrutiny and
Measuring quality along care pathways
 Measuring quality along care pathways Sarah Jonas, Clinical Fellow, The King s Fund Veena Raleigh, Senior Fellow, The King s Fund Catherine Foot, Senior Fellow, The King s Fund James Mountford, Director
Measuring quality along care pathways Sarah Jonas, Clinical Fellow, The King s Fund Veena Raleigh, Senior Fellow, The King s Fund Catherine Foot, Senior Fellow, The King s Fund James Mountford, Director
Financial Plan 2013/14-2014/15
 Financial Plan 2013/14-2014/15 Final May 2013 1.0 Synopsis and Recommendations This Plan provides detail of NHS North Staffordshire Clinical Commissioning Group financial planning intentions for 2013/14.
Financial Plan 2013/14-2014/15 Final May 2013 1.0 Synopsis and Recommendations This Plan provides detail of NHS North Staffordshire Clinical Commissioning Group financial planning intentions for 2013/14.
Summary Strategic Plan 2014-2019
 Summary Strategic Plan 2014-2019 NTWFT Summary Strategic Plan 2014-2019 1 Contents Page No. Introduction 3 The Trust 3 Market Assessment 3 The Key Factors Influencing this Strategy 4 The impact of a do
Summary Strategic Plan 2014-2019 NTWFT Summary Strategic Plan 2014-2019 1 Contents Page No. Introduction 3 The Trust 3 Market Assessment 3 The Key Factors Influencing this Strategy 4 The impact of a do
Coventry and Warwickshire Repatriation Programme
 NHS Arden Commissioning Support Unit Coventry and Warwickshire Repatriation Programme Large-scale service redesign and innovation to benefit patients Arden Commissioning Support Unit worked with Coventry
NHS Arden Commissioning Support Unit Coventry and Warwickshire Repatriation Programme Large-scale service redesign and innovation to benefit patients Arden Commissioning Support Unit worked with Coventry
Board of Directors Meeting
 Board of Directors Meeting 23 rd July 2014 (BDA/14/26) part Performance Report Monitor Key Indicators Status: A Paper for Information History: Amanda Pritchard Chief Operating Officer Page 1 of 10 Performance
Board of Directors Meeting 23 rd July 2014 (BDA/14/26) part Performance Report Monitor Key Indicators Status: A Paper for Information History: Amanda Pritchard Chief Operating Officer Page 1 of 10 Performance
Agenda Item No: 6.1 Enclosure: 3
 Date of Meeting: 14/02/2012 Intended Outcome: For noting Agenda Item No: 6.1 Enclosure: 3 For information Title of Report: Acquisition of North Cumbria University Hospitals NHS Trust Aims: To provide the
Date of Meeting: 14/02/2012 Intended Outcome: For noting Agenda Item No: 6.1 Enclosure: 3 For information Title of Report: Acquisition of North Cumbria University Hospitals NHS Trust Aims: To provide the
Whole Site Master Planning Excercise
 Whole Site Master Planning Excercise 2008 2018 Consultant Briefing Paper Delivering the best in care www.uhb.nhs.uk/wholesitemasterplanning Queen Elizabeth Medical Centre Multistorey Car Park Birmingham
Whole Site Master Planning Excercise 2008 2018 Consultant Briefing Paper Delivering the best in care www.uhb.nhs.uk/wholesitemasterplanning Queen Elizabeth Medical Centre Multistorey Car Park Birmingham
A Route Map to the 2020 Vision for Health and Social Care
 A Route Map to the 2020 Vision for Health and Social Care 02 A Route Map to the 2020 Vision for Health and Social Care Introduction This paper sets out a new and accelerated focus on a number of priority
A Route Map to the 2020 Vision for Health and Social Care 02 A Route Map to the 2020 Vision for Health and Social Care Introduction This paper sets out a new and accelerated focus on a number of priority
FINANCIAL PLAN 2014/15 2018/19
 Appendix 11a Financial Plan 2014/15 2018/19 NHS LOTHIAN Board Meeting 2 April 2014 Director of Finance FINANCIAL PLAN 2014/15 2018/19 1 Purpose of the Report 1.1 The purpose of this report is to seek approval
Appendix 11a Financial Plan 2014/15 2018/19 NHS LOTHIAN Board Meeting 2 April 2014 Director of Finance FINANCIAL PLAN 2014/15 2018/19 1 Purpose of the Report 1.1 The purpose of this report is to seek approval
Rehabilitation Network Strategy 2014 2017. Final Version 30 th June 2014
 Rehabilitation Network Strategy 2014 2017 Final Version 30 th June 2014 Contents Foreword 3 Introduction Our Strategy 4 Overview of the Cheshire and Merseyside Rehabilitation Network 6 Analysis of our
Rehabilitation Network Strategy 2014 2017 Final Version 30 th June 2014 Contents Foreword 3 Introduction Our Strategy 4 Overview of the Cheshire and Merseyside Rehabilitation Network 6 Analysis of our
High Quality Care for All Measuring for Quality Improvement: the approach
 High Quality Care for All Measuring for Quality Improvement: the approach Our vision 1. Improving quality has always been a central motivation for all who work in the NHS. High Quality Care for All, the
High Quality Care for All Measuring for Quality Improvement: the approach Our vision 1. Improving quality has always been a central motivation for all who work in the NHS. High Quality Care for All, the
Cancer Patient Experience Survey: Insight Report and League Table 2012 13
 Cancer Patient Experience Survey: Insight Report and League Table 2012 13 September 2013 Macmillan Cancer Support, registered charity in England and Wales (261017), Scotland (SC039907) and the Isle of
Cancer Patient Experience Survey: Insight Report and League Table 2012 13 September 2013 Macmillan Cancer Support, registered charity in England and Wales (261017), Scotland (SC039907) and the Isle of
National Clinical Programmes
 National Clinical Programmes Section 3 Background information on the National Clinical Programmes Mission, Vision and Objectives July 2011 V0. 6_ 4 th July, 2011 1 National Clinical Programmes: Mission
National Clinical Programmes Section 3 Background information on the National Clinical Programmes Mission, Vision and Objectives July 2011 V0. 6_ 4 th July, 2011 1 National Clinical Programmes: Mission
NHS Services, Seven Days a Week Forum. Costing seven day services
 NHS Services, Seven Days a Week Forum Costing seven day services The financial implications of seven day services for acute emergency and urgent services and supporting diagnostics Gateway reference: 00889
NHS Services, Seven Days a Week Forum Costing seven day services The financial implications of seven day services for acute emergency and urgent services and supporting diagnostics Gateway reference: 00889
Quality and Safety Programme Fractured neck of femur services
 Quality and Safety Programme Fractured neck of femur services London quality standards February 2013 1 Introduction The case for change for fractured neck of femur services in London demonstrates that
Quality and Safety Programme Fractured neck of femur services London quality standards February 2013 1 Introduction The case for change for fractured neck of femur services in London demonstrates that
Caring for Vulnerable Babies: The reorganisation of neonatal services in England
 Caring for Vulnerable Babies: The reorganisation of neonatal services in England LONDON: The Stationery Office 13.90 Ordered by the House of Commons to be printed on 17 December 2007 REPORT BY THE COMPTROLLER
Caring for Vulnerable Babies: The reorganisation of neonatal services in England LONDON: The Stationery Office 13.90 Ordered by the House of Commons to be printed on 17 December 2007 REPORT BY THE COMPTROLLER
Section 6. Strategic & Service Planning
 Section 6 Strategic & Service Planning 6 Strategic & Service Planning 6.1 Strategic Planning Responsibilities Section 6 Strategic & Service Planning 6.1.1 Role of Local Health Districts and Specialty
Section 6 Strategic & Service Planning 6 Strategic & Service Planning 6.1 Strategic Planning Responsibilities Section 6 Strategic & Service Planning 6.1.1 Role of Local Health Districts and Specialty
TRUST BOARD. Date of Meeting: 05/04/2011 Enclosure: 5
 TRUST BOARD Date of Meeting: 05/04/2011 Enclosure: 5 Title of Report: Merger and Acquisition Update Agenda Item No: 7.1 Aims: This report informs and updates the Board on the development of the process
TRUST BOARD Date of Meeting: 05/04/2011 Enclosure: 5 Title of Report: Merger and Acquisition Update Agenda Item No: 7.1 Aims: This report informs and updates the Board on the development of the process
THE AUTUMN STATEMENT: NHS FUNDING
 THE AUTUMN STATEMENT: NHS FUNDING Summary The NHS faces huge pressures as a result of an ongoing funding squeeze, rising demand for services and the need to safeguard quality of care following the Francis
THE AUTUMN STATEMENT: NHS FUNDING Summary The NHS faces huge pressures as a result of an ongoing funding squeeze, rising demand for services and the need to safeguard quality of care following the Francis
North West Surrey CCG - Head of Ambulance Contracts. Job Description
 North West Surrey CCG - Head of Ambulance Contracts Job Description Job Title: Band: Responsible to: Responsible for: Accountable to: Head of Ambulance Contracts Band 8c Associate Director of Contracts
North West Surrey CCG - Head of Ambulance Contracts Job Description Job Title: Band: Responsible to: Responsible for: Accountable to: Head of Ambulance Contracts Band 8c Associate Director of Contracts
Trust Board Meeting: Wednesday 14 May 2014 TB2014.53. Nursing and Midwifery - Safe staffing levels report for the month of March 2014
 Trust Board Meeting: Wednesday 14 May 2014 Title Nursing and Midwifery - Safe staffing levels report for the month of March 2014 Status For information History Trust Board Seminar 21 st October 2013 Trust
Trust Board Meeting: Wednesday 14 May 2014 Title Nursing and Midwifery - Safe staffing levels report for the month of March 2014 Status For information History Trust Board Seminar 21 st October 2013 Trust
Engagement for commissioning success. {Smart Guides} to ENGAGEMENT. For better commissioning
 Engagement for commissioning success {Smart Guides} to ENGAGEMENT For better commissioning Engagement for commissioning success Part of the Smart Guides to Engagement series, this guide looks at the benefits
Engagement for commissioning success {Smart Guides} to ENGAGEMENT For better commissioning Engagement for commissioning success Part of the Smart Guides to Engagement series, this guide looks at the benefits
BOROUGH BRIEFING THE LONDON BRIEFING
 BRIEFING BOROUGHS London s 32 boroughs, together with the City of London, provide their residents with the majority of services including schools, social care, public health, highways, environmental health
BRIEFING BOROUGHS London s 32 boroughs, together with the City of London, provide their residents with the majority of services including schools, social care, public health, highways, environmental health
5-Year Financial Plan Update September 2013. Croydon CCG. Longer, healthier lives for all the people in Croydon
 5-Year Financial Plan Update September 2013 Croydon CCG Financial Strategy Background (1) This 5-Year Plan builds on the full financial strategy document incorporated in the 3-Year Financial Improvement
5-Year Financial Plan Update September 2013 Croydon CCG Financial Strategy Background (1) This 5-Year Plan builds on the full financial strategy document incorporated in the 3-Year Financial Improvement
Appendix 1 Business Case to Support the Relocation of Mental Health Inpatient Services in Manchester (Clinical Foreword and Executive Summary)
") Appendix 1 Business Case to Support the Relocation of Mental Health Inpatient Services in Manchester (Clinical Foreword and Executive Summary) Together we are better Foreword by the Director of Nursing
Appendix 1 Business Case to Support the Relocation of Mental Health Inpatient Services in Manchester (Clinical Foreword and Executive Summary) Together we are better Foreword by the Director of Nursing
DIRECTOR OF ESTATES AND FACILITIES ROLE PROFILE. Draft and subject to refinement
 DIRCTOR OF STATS AND FACILITIS ROL PROFIL Draft and subject to refinement 21 September 2015 1 INTRODUCTION Barts Health was established in 2012 following a merger of three former organisations and is the
DIRCTOR OF STATS AND FACILITIS ROL PROFIL Draft and subject to refinement 21 September 2015 1 INTRODUCTION Barts Health was established in 2012 following a merger of three former organisations and is the
Northumberland, Tyne and Wear NHS Foundation Trust. Council of Governors Meeting. Paper for Debate, Decision or Information: For information
 Agenda item 7) Northumberland, Tyne and Wear NHS Foundation Trust Council of Governors Meeting Meeting Date: Thursday 12 November 2015 Title and Author of Paper: Chief Executive s Report John Lawlor, Chief
Agenda item 7) Northumberland, Tyne and Wear NHS Foundation Trust Council of Governors Meeting Meeting Date: Thursday 12 November 2015 Title and Author of Paper: Chief Executive s Report John Lawlor, Chief
REMOVING THE POLICY BARRIERS TO INTEGRATED CARE
 REMOVING THE POLICY BARRIERS TO INTEGRATED CARE THINKING THROUGH AN INTEGRATED CARE SYSTEM IN THE NHS: THE TRAFFORD EXPERIENCE Dr Martin Connor, Programme Director, Trafford ICO and Dr George Kissen, Medical
REMOVING THE POLICY BARRIERS TO INTEGRATED CARE THINKING THROUGH AN INTEGRATED CARE SYSTEM IN THE NHS: THE TRAFFORD EXPERIENCE Dr Martin Connor, Programme Director, Trafford ICO and Dr George Kissen, Medical
Integrated Care Organisation
 Integrated Care Organisation Business Case Part 1 Committed to Local Healthcare 1 A) Executive Summary This Business Case sets out an exciting vision of new ways of providing health care by a new type
Integrated Care Organisation Business Case Part 1 Committed to Local Healthcare 1 A) Executive Summary This Business Case sets out an exciting vision of new ways of providing health care by a new type
Our five-year strategy 2015-19
 Draft summary for comment Draft summary for comment Draft summary for comment Draft summary for comment Draft summary for comment Draft summary Our five-year strategy 2015-19 Introduction Foreword from
Draft summary for comment Draft summary for comment Draft summary for comment Draft summary for comment Draft summary for comment Draft summary Our five-year strategy 2015-19 Introduction Foreword from
Supporting information pack
 Supporting information pack The new commissioning system As part of the modernisation of the NHS, a number of changes to how health services are managed came into effect from April 2013. Primary Care Trusts
Supporting information pack The new commissioning system As part of the modernisation of the NHS, a number of changes to how health services are managed came into effect from April 2013. Primary Care Trusts
Acute care toolkit 2
 Acute care toolkit 2 High-quality acute care October 2011 Consultant physicians are at the forefront of delivering care to patients presenting to hospital with medical emergencies. Delivering this care
Acute care toolkit 2 High-quality acute care October 2011 Consultant physicians are at the forefront of delivering care to patients presenting to hospital with medical emergencies. Delivering this care
Data Management, Audit and Outcomes of the NHS
 Data Management, Audit and Outcomes Providing Accurate Outcomes and Activity Data The Trust has in place robust mechanisms for capturing and reporting on all oesophago-gastric cancer surgery activity and
Data Management, Audit and Outcomes Providing Accurate Outcomes and Activity Data The Trust has in place robust mechanisms for capturing and reporting on all oesophago-gastric cancer surgery activity and
Civica Health & Social Care
 Civica Health & Social Care Focus on > SLAM for Healthcare Providers Improved communications with commissioners, leading to clarity and better relationships Civica Focus on> The solution SLAM is the ideal
Civica Health & Social Care Focus on > SLAM for Healthcare Providers Improved communications with commissioners, leading to clarity and better relationships Civica Focus on> The solution SLAM is the ideal
The practice of medicine comprises prevention, diagnosis and treatment of disease.
 English for Medical Students aktualizované texty o systému zdravotnictví ve Velké Británii MUDr Sylva Dolenská Lesson 16 Hospital Care The practice of medicine comprises prevention, diagnosis and treatment
English for Medical Students aktualizované texty o systému zdravotnictví ve Velké Británii MUDr Sylva Dolenská Lesson 16 Hospital Care The practice of medicine comprises prevention, diagnosis and treatment
Delivering the Forward View: NHS planning guidance 2016/17 2020/21
 Delivering the Forward View: NHS planning guidance 2016/17 2020/21 Planning Guidance 2016/17 Published December 2015 Spending Review National Priorities 2 separate but connected plans CCG Operational plan
Delivering the Forward View: NHS planning guidance 2016/17 2020/21 Planning Guidance 2016/17 Published December 2015 Spending Review National Priorities 2 separate but connected plans CCG Operational plan
Brighton and Sussex University Hospital NHS Trust
 Brighton and Sussex University Hospital NHS Trust Year Ending 31 March 2013 Annual Audit Letter July 2013 Ernst & Young LLP Executive summary Ernst & Young LLP 1 More London Place London SE1 2AF Tel: +44
Brighton and Sussex University Hospital NHS Trust Year Ending 31 March 2013 Annual Audit Letter July 2013 Ernst & Young LLP Executive summary Ernst & Young LLP 1 More London Place London SE1 2AF Tel: +44
Improving data quality in the NHS Executive summary
 Improving data quality in the NHS Executive summary Health 2010 The Audit Commission is an independent watchdog, driving economy, efficiency and effectiveness in local public services to deliver better
Improving data quality in the NHS Executive summary Health 2010 The Audit Commission is an independent watchdog, driving economy, efficiency and effectiveness in local public services to deliver better
Governing Body. Date of Meeting: 29 May 2014 Paper No: 14/39. Title of Presentation: Update to the CCG Financial Plan 2014-15 to 2018-19
 Oxfordshire Clinical Commissioning Group Oxfordshire Clinical Commissioning Group Governing Body Date of Meeting: 29 May 2014 Paper No: 14/39 Title of Presentation: Update to the CCG Financial Plan 2014-15
Oxfordshire Clinical Commissioning Group Oxfordshire Clinical Commissioning Group Governing Body Date of Meeting: 29 May 2014 Paper No: 14/39 Title of Presentation: Update to the CCG Financial Plan 2014-15
Health Policy & Scrutiny Urgency Sub-Committee MINUTES OF PROCEEDINGS
 CITY OF WESTMINSTER MINUTES Health Policy & Scrutiny Urgency Sub-Committee MINUTES OF PROCEEDINGS Minutes of a meeting of the Health Policy & Scrutiny Urgency Sub-Committee Committee held on Thursday 7th
CITY OF WESTMINSTER MINUTES Health Policy & Scrutiny Urgency Sub-Committee MINUTES OF PROCEEDINGS Minutes of a meeting of the Health Policy & Scrutiny Urgency Sub-Committee Committee held on Thursday 7th
South Eastern Health and Social Care Trust
 South Eastern Health and Social Care Trust JOB DESCRIPTION TITLE OF POST: Consultant General Surgeon LOCATION: This post is part of the South Eastern Trust and will be based at the Ulster Hospital. However,
South Eastern Health and Social Care Trust JOB DESCRIPTION TITLE OF POST: Consultant General Surgeon LOCATION: This post is part of the South Eastern Trust and will be based at the Ulster Hospital. However,
The Financial Plan 2013/14 was re balanced in July to reflect agreed contract values, expected QIPP savings and known over performance.
 Number: 5 NHS VALE OF YORK CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING Meeting Date: 3 October 2013 Report Sponsor: Kevin Howells Interim Chief Finance Officer Report Author: Andrew Wilson Interim
Number: 5 NHS VALE OF YORK CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING Meeting Date: 3 October 2013 Report Sponsor: Kevin Howells Interim Chief Finance Officer Report Author: Andrew Wilson Interim
D04/ODN/a NHS STANDARD CONTRACT FOR NEUROMUSCULAR OPERATIONAL DELIVERY NETWORKS SCHEDULE 2- THE SERVICES A. SERVICE SPECIFICATIONS
 D04/ODN/a NHS STANDARD CONTRACT FOR NEUROMUSCULAR OPERATIONAL DELIVERY NETWORKS SCHEDULE 2- THE SERVICES A. SERVICE SPECIFICATIONS Service Specification No. Service Commissioner Lead Provider Lead Period
D04/ODN/a NHS STANDARD CONTRACT FOR NEUROMUSCULAR OPERATIONAL DELIVERY NETWORKS SCHEDULE 2- THE SERVICES A. SERVICE SPECIFICATIONS Service Specification No. Service Commissioner Lead Provider Lead Period
Effective Approaches in Urgent and Emergency Care. Priorities within Acute Hospitals
 Effective Approaches in Urgent and Emergency Care Paper 1 Priorities within Acute Hospitals When people are taken to hospital as an emergency, they want prompt, safe and effective treatment that alleviates
Effective Approaches in Urgent and Emergency Care Paper 1 Priorities within Acute Hospitals When people are taken to hospital as an emergency, they want prompt, safe and effective treatment that alleviates
Person-centred, coordinated care. London s progress and learning
 Person-centred, coordinated care London s progress and learning London is developing integrated care systems that serve whole populations Outer North West London 4 Clinical Commissioning Groups 4 local
Person-centred, coordinated care London s progress and learning London is developing integrated care systems that serve whole populations Outer North West London 4 Clinical Commissioning Groups 4 local
TRUST BOARD 24 OCTOBER 2012. OCH Phase 4 Chemotherapy Project The Macmillan Cancer Treatment and Support Centre Outline Business Case
 Our vision: To be amongst the best TRUST BOARD 24 OCTOBER 2012 def Agenda Item: 8 OCH Phase 4 Chemotherapy Project The Macmillan Cancer Treatment and Support Centre Outline Business Case PURPOSE PREVIOUSLY
Our vision: To be amongst the best TRUST BOARD 24 OCTOBER 2012 def Agenda Item: 8 OCH Phase 4 Chemotherapy Project The Macmillan Cancer Treatment and Support Centre Outline Business Case PURPOSE PREVIOUSLY
Cancer Patient Experience Survey: Insight Report and League Table 2014
 Cancer Patient Experience Survey: Insight Report and League Table 2014 October 2014 Macmillan Cancer Support, registered charity in England and Wales (261017), Scotland (SC039907) and the Isle of Man (604).
Cancer Patient Experience Survey: Insight Report and League Table 2014 October 2014 Macmillan Cancer Support, registered charity in England and Wales (261017), Scotland (SC039907) and the Isle of Man (604).
Improving access to insulin pump therapy: The role of the Insulin Pump Network
 Article Improving access to insulin pump therapy: The role of the Insulin Pump Network Peter Hammond Citation: Hammond, P (2013) Improving access to insulin pump therapy: The role of the Insulin Pump Network.
Article Improving access to insulin pump therapy: The role of the Insulin Pump Network Peter Hammond Citation: Hammond, P (2013) Improving access to insulin pump therapy: The role of the Insulin Pump Network.
Financial Risk Share and Transitional Investment Fund North Central London Clinical Commissioning Groups 2013/14-2017/18
 Financial Risk Share and Transitional Investment Fund North Central London Clinical Commissioning Groups 2013/14-2017/18 1. Background The North Central London Clinical Commissioning Groups (Barnet, Camden,
Financial Risk Share and Transitional Investment Fund North Central London Clinical Commissioning Groups 2013/14-2017/18 1. Background The North Central London Clinical Commissioning Groups (Barnet, Camden,
The anatomy of health spending 2011/12
 A review of NHS expenditure and labour productivity The anatomy of health spending 2011/12 Research report Nick M. Jones and Anita Charlesworth March 2013 About this work programme Understanding how NHS
A review of NHS expenditure and labour productivity The anatomy of health spending 2011/12 Research report Nick M. Jones and Anita Charlesworth March 2013 About this work programme Understanding how NHS
briefing Papering over the cracks: the impact of social care funding on the NHS NHS reform and transition Key points September 2012 Issue 248
 NHS reform and transition briefing September 2012 Issue 248 Papering over the cracks: the impact of social care funding on the NHS Key points Demand for health and social care will continue to rise, particularly
NHS reform and transition briefing September 2012 Issue 248 Papering over the cracks: the impact of social care funding on the NHS Key points Demand for health and social care will continue to rise, particularly
Time to Act Urgent Care and A&E: the patient perspective
 Time to Act Urgent Care and A&E: the patient perspective May 2015 Executive Summary The NHS aims to put patients at the centre of everything that it does. Indeed, the NHS Constitution provides rights to
Time to Act Urgent Care and A&E: the patient perspective May 2015 Executive Summary The NHS aims to put patients at the centre of everything that it does. Indeed, the NHS Constitution provides rights to
Integrated Performance Report
 Integrated Performance Report M03 June 2015 Presented by: Angela Stevenson (Deputy Chief Operating Officer) Des Holden (Medical Director) Fiona Alsop (Chief Nurse) Paul Simpson (Chief Financial Officer)
Integrated Performance Report M03 June 2015 Presented by: Angela Stevenson (Deputy Chief Operating Officer) Des Holden (Medical Director) Fiona Alsop (Chief Nurse) Paul Simpson (Chief Financial Officer)
The Way Forward: Strategic clinical networks
 The Way Forward: Strategic clinical networks The Way Forward Strategic clinical networks First published: 26 July 2012 Prepared by NHS Commissioning Board, a special health authority Contents Foreword...
The Way Forward: Strategic clinical networks The Way Forward Strategic clinical networks First published: 26 July 2012 Prepared by NHS Commissioning Board, a special health authority Contents Foreword...
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY COUNCIL OF GOVERNORS 2 ND DECEMBER 2014
 SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST C EXECUTIVE SUMMARY COUNCIL OF GOVERNORS 2 ND DECEMBER 2014 Subject: Supporting Director: Author: Status 1 NHS England Five Year Forward View A Summary
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST C EXECUTIVE SUMMARY COUNCIL OF GOVERNORS 2 ND DECEMBER 2014 Subject: Supporting Director: Author: Status 1 NHS England Five Year Forward View A Summary
Performance Detailed Report. May 2008. Review of Performance Management. Norwich City Council. Audit 2007/08
 Performance Detailed Report May 2008 Review of Performance Management Audit 2007/08 External audit is an essential element in the process of accountability for public money and makes an important contribution
Performance Detailed Report May 2008 Review of Performance Management Audit 2007/08 External audit is an essential element in the process of accountability for public money and makes an important contribution
Agenda Item: 4.1.2. REPORT TO THE TRUST BOARD MEETING IN PUBLIC August 2013. Integrated Performance Report. Title
 REPORT TO THE TRUST BOARD MEETING IN PUBLIC August 2013 Title Lead Director Author(s) Purpose Previously considered by Executive Summary Integrated Performance Report Agenda Item: 4.1.2 Paul Scott - Director
REPORT TO THE TRUST BOARD MEETING IN PUBLIC August 2013 Title Lead Director Author(s) Purpose Previously considered by Executive Summary Integrated Performance Report Agenda Item: 4.1.2 Paul Scott - Director
Directors of Public Health in Local Government
 Directors of Public Health in Local Government i) Roles, responsibilities and context 1 DH INFORMATION READER BOX Policy Clinical Estates HR / Workforce Commissioner Development IM & T Management Provider
Directors of Public Health in Local Government i) Roles, responsibilities and context 1 DH INFORMATION READER BOX Policy Clinical Estates HR / Workforce Commissioner Development IM & T Management Provider
SUBJECT: Procurement Strategy for Substance Misuse Residential Detox and Rehabilitation Services
 Housing and Adult Social Services 7 Newington Barrow Way, London, N7 7EP Report of: Executive Member for Health and Well-Being Meeting of: Date Ward(s) Executive 16 July 2015 All Delete as appropriate
Housing and Adult Social Services 7 Newington Barrow Way, London, N7 7EP Report of: Executive Member for Health and Well-Being Meeting of: Date Ward(s) Executive 16 July 2015 All Delete as appropriate
The Newcastle upon Tyne Hospitals NHS Foundation Trust. National Early Warning Score (NEWS) Policy
 Policy") The Newcastle upon Tyne Hospitals NHS Foundation Trust National Early Warning Score (NEWS) Policy Version.: 1.0 Effective From: 3 December 2014 Expiry Date: 3 December 2016 Date Ratified: 1 September 2014
The Newcastle upon Tyne Hospitals NHS Foundation Trust National Early Warning Score (NEWS) Policy Version.: 1.0 Effective From: 3 December 2014 Expiry Date: 3 December 2016 Date Ratified: 1 September 2014
A Review of the NHSLA Incident Reporting and Management and Learning from Experience Standards. Assessment Outcomes. April 2003 - March 2004
 A Review of the NHSLA Incident Reporting and Management and Learning from Experience Standards Assessment Outcomes April 2003 - March 2004 September 2004 1 Background The NHS Litigation Authority (NHSLA)
A Review of the NHSLA Incident Reporting and Management and Learning from Experience Standards Assessment Outcomes April 2003 - March 2004 September 2004 1 Background The NHS Litigation Authority (NHSLA)
Unbundling recovery: Recovery, rehabilitation and reablement national audit report
 NHS Improving Quality Unbundling recovery: Recovery, rehabilitation and reablement national audit report Implementing capitated budgets within long term conditions for people with complex needs LTC Year
NHS Improving Quality Unbundling recovery: Recovery, rehabilitation and reablement national audit report Implementing capitated budgets within long term conditions for people with complex needs LTC Year
Together for Health Delivering End of Life Care A Delivery Plan up to 2016 for NHS Wales and its Partners
 Together for Health Delivering End of Life Care A Delivery Plan up to 2016 for NHS Wales and its Partners The highest standard of care for everyone at the end of life Digital ISBN 978 0 7504 8708 5 Crown
Together for Health Delivering End of Life Care A Delivery Plan up to 2016 for NHS Wales and its Partners The highest standard of care for everyone at the end of life Digital ISBN 978 0 7504 8708 5 Crown
CENTRAL MANCHESTER UNIVERSITY HOSPITALS NHS FOUNDATION TRUST
 CENTRAL MANCHESTER UNIVERSITY HOSPITALS NHS FOUNDATION TRUST Agenda Item 9.1 Report of: Executive Director of Human & Corporate Resources Margot Johnson Paper prepared by: Head of Operational HR - Gill
CENTRAL MANCHESTER UNIVERSITY HOSPITALS NHS FOUNDATION TRUST Agenda Item 9.1 Report of: Executive Director of Human & Corporate Resources Margot Johnson Paper prepared by: Head of Operational HR - Gill
Meets all objectives. In line with Council policy.
 ITEM NO: 5 Report to: HEALTH AND WELLBEING BOARD Date: 1 October 2015 Executive Member / Reporting Officer: Subject: Report Summary: Recommendations: Councillor Brenda Warrington Executive Member (Adult
ITEM NO: 5 Report to: HEALTH AND WELLBEING BOARD Date: 1 October 2015 Executive Member / Reporting Officer: Subject: Report Summary: Recommendations: Councillor Brenda Warrington Executive Member (Adult
London Sexual Health Transformation project
 London Sexual Health Transformation project Update October 2015 Background Councils took on the responsibility for commissioning many sexual health services in April 2013, as part of changes under the
London Sexual Health Transformation project Update October 2015 Background Councils took on the responsibility for commissioning many sexual health services in April 2013, as part of changes under the
How is the health and social care system performing? Quarterly monitoring report
 How is the health and social care system performing? Quarterly monitoring report January 214 January 214 The King s Fund published its first Quarterly monitoring report in April 211 as part of its work
How is the health and social care system performing? Quarterly monitoring report January 214 January 214 The King s Fund published its first Quarterly monitoring report in April 211 as part of its work
East Midlands Ambulance Service
 Appendix 1 East Midlands Ambulance Service New Service Delivery Model Summary Document Trust Executive Board 05 April 2012 Contents Introduction... 3 1. The Strategic Context... 4 2. Overview... 7 3. Objectives...
Appendix 1 East Midlands Ambulance Service New Service Delivery Model Summary Document Trust Executive Board 05 April 2012 Contents Introduction... 3 1. The Strategic Context... 4 2. Overview... 7 3. Objectives...
Stroke rehabilitation
 Costing report Stroke rehabilitation Published: June 2013 http://guidance.nice.org.uk/cg162 This costing report accompanies the clinical guideline: Stroke rehabilitation (available online at http://guidance.nice.org.uk/cg162).
Costing report Stroke rehabilitation Published: June 2013 http://guidance.nice.org.uk/cg162 This costing report accompanies the clinical guideline: Stroke rehabilitation (available online at http://guidance.nice.org.uk/cg162).
In good health. Public health teams in local authorities Year 2. February 2015
 In good health Public health teams in local authorities Year 2 February 2015 Foreword The public health workforce is at the heart of both improving and protecting the public s health and as such the views
In good health Public health teams in local authorities Year 2 February 2015 Foreword The public health workforce is at the heart of both improving and protecting the public s health and as such the views
Sandwell and West Birmingham Hospitals NHS Trust Midland Metropolitan Hospital Project. Outline Business Case. Appendix 10a Soft FM Services Review
 Sandwell and West Birmingham Hospitals NHS Trust Midland Metropolitan Hospital Project Outline Business Case Appendix 10a Soft FM Services Review SANDWELL AND WEST BIRMINGHAM HOSPITALS NHS TRUST PFI PROJECT
Sandwell and West Birmingham Hospitals NHS Trust Midland Metropolitan Hospital Project Outline Business Case Appendix 10a Soft FM Services Review SANDWELL AND WEST BIRMINGHAM HOSPITALS NHS TRUST PFI PROJECT
Background... 1. What is it?... 2. Why is it important?... 2. What is essential for your plan?... 3. What is recommended for your plan?...
 Contents Background... 1 What is it?... 2 Why is it important?... 2 What is essential for your plan?... 3 What is recommended for your plan?... 3 Sensitivity Analysis... 13 Financial Risk... 15 How do
Contents Background... 1 What is it?... 2 Why is it important?... 2 What is essential for your plan?... 3 What is recommended for your plan?... 3 Sensitivity Analysis... 13 Financial Risk... 15 How do
Emergency admissions to hospital: managing the demand
 Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 Our vision is to help the nation spend wisely.
Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 Our vision is to help the nation spend wisely.