GUIDELINE 11.9 MANAGING ACUTE DYSRHYTHMIAS. (To be read in conjunction with Guideline 11.7 Post-Resuscitation Therapy in Adult Advanced Life Support)
|
|
|
- Joleen Black
- 8 years ago
- Views:
Transcription
1 AUSTRALIAN RESUSCITATION COUNCIL GUIDELINE 11.9 MANAGING ACUTE DYSRHYTHMIAS (To be read in conjunction with Guideline 11.7 Post-Resuscitation Therapy in Adult Advanced Life Support) The term cardiac arrhythmia refers to an abnormality of the heart rhythm. The normal heart rate is usually between 60 and 100 beats per minute. The heart may beat excessively fast (tachycardia or tachyarrhythmia), excessively slow (bradycardia or bradyarrhythmia), and may be in a regular or an irregular pattern (commonly atrial fibrillation). Both fast and slow abnormalities of the heart rhythm may lead to cardiac arrest. Most (about 80%) cardiac arrests are related to excessively fast rhythms that originate in the lower chambers of the heart (ventricular tachycardia and fibrillation). Complete cessation of all heart electrical activity (asystole) may be seen following a prolonged period of tachycardia or as a result of bradycardia. Fast rhythms of the heart may respond to synchronized electrical therapy (cardioversion) to reset the normal activity of the heart. They may also respond to drug therapy. Unsynchronised electrical therapy (defibrillation) is the mainstay of treatment of fast rhythms of the heart when the patient is in cardiac arrest. Slow rhythms of the heart may be treated with drugs to increase the heart rate such as atropine (anti-cholinergic) or adrenergic agents. Alternately, an electrical impulse may be applied to the heart either internally (internal pacemaker) by cardiac pacing wires or externally (external pacemaker) by pads. All anti-arrhythmic treatments (physical maneuvers, drugs, cardioversion, pacing) have the potential to make the rhythm worse rather than better, causing clinical deterioration. Furthermore most anti-arrhythmic drugs cause myocardial depression, which may worsen heart failure or hypotension. It is important to recognise patients who are stable and have no adverse signs from an arrhythmia. If there is no immediate urgency for treatment, and especially if there is any uncertainty about the best choice of treatment, seek expert help (eg. cardiology). Guideline 11.9 Page 1 of 11
, excessively slow (bradycardia or bradyarrhythmia), and may be in a regular or an irregular pattern (commonly atrial fibrillation).")
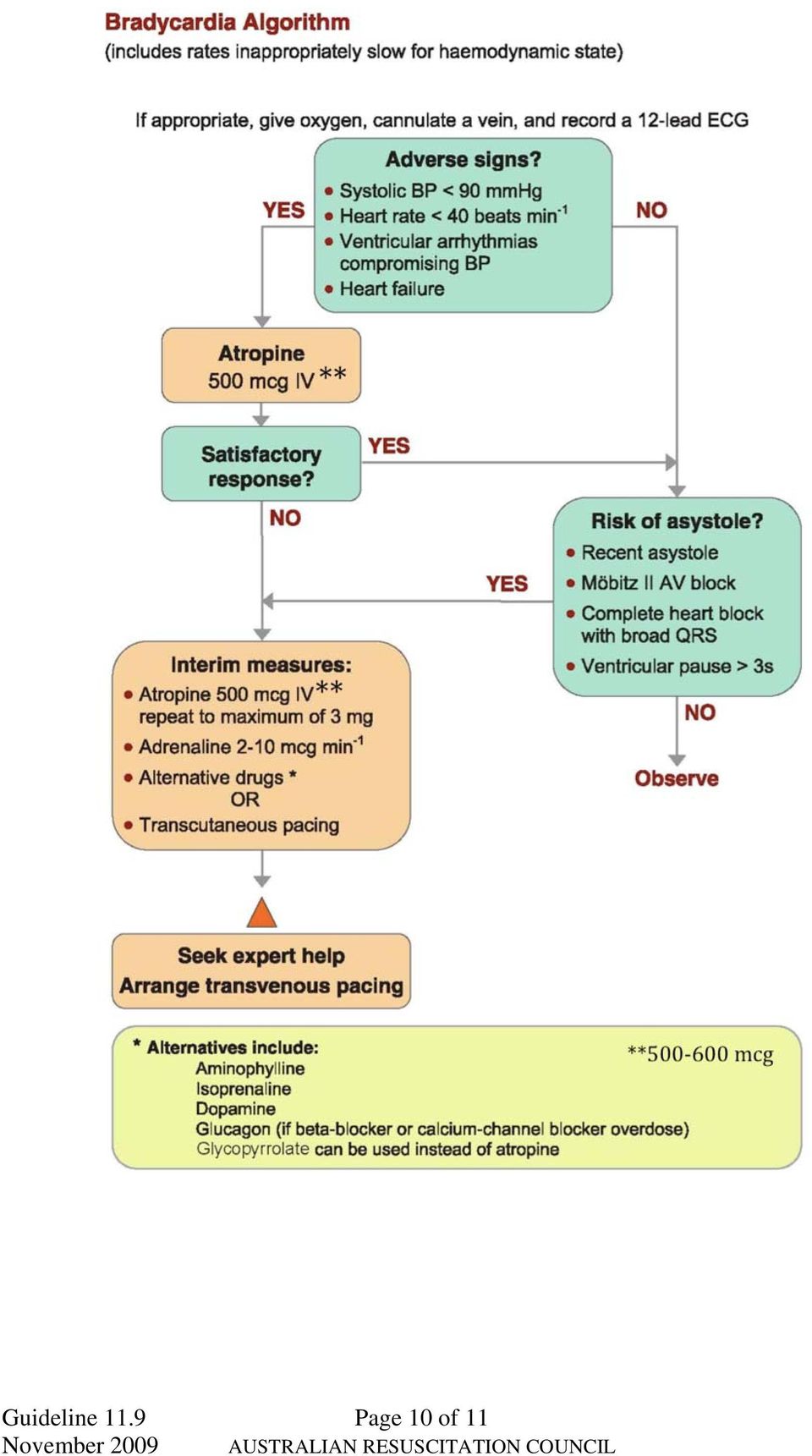
2 Whilst assessing the patient: give oxygen and obtain IV access if not already done (particularly if adverse signs are present); and record a 12-lead ECG if not already done (without delaying treatment). BRADYARRHYTHMIA The conventional definition of bradyarrhythmia is a heart rate < 60/min; however, for some people or some situations heart rates of < 60/min are not harmful and may be entirely physiological. Patients with a slow heart beat who do not experience symptoms usually do not require emergency therapy. The common symptoms of bradycardia include syncope (fainting), shortness of breath, dizziness or chest pain. The following adverse signs suggest a need for immediate treatment (see bradycardia algorithm): systolic BP < 90 mmhg; heart rate < 40/min; ventricular arrhythmia; heart failure. A pulseless patient with a bradyarrhythmia requires cardiac arrest management according to the cardiac arrest algorithm (see ARC Guideline 11.2). Drug therapy Atropine is the initial treatment and is administered intravenously in doses of mcg (repeated as necessary every 3-5 min up to a total dose of 3 mg). ( Level of evidence III-2) If this fails low dose adrenaline is the second line agent (as a bolus or as an infusion). Adrenaline is usually administered at a rate of 2-10 mcg/min to maintain a satisfactory heart rate (stable heart rate with a mean arterial pressure of 70 mm Hg). Other drugs that can be given for the treatment of bradycardia include isoprenaline (2-5 mcg/minute), dopamine (2-5mcg/kg/minute, theophylline (Level III-2) and glycopyrrolate. In the presence of therapy with beta blockers much higher doses may be required to overcome the effects of these agents. Consider giving intravenous glucagon [1] or insulin/glucose/potassium therapy [2] if a beta-blocker or calcium channel blocker is the cause of the bradycardia (Level of evidence IV). Do not give atropine to patients with cardiac transplant as the heart is denervated and will not respond to vagal blockade, and there is some risk of inducing paradoxical atrioventricular block. [1] Pacing Patients who fail to respond to pharmacotherapy, or who are at high risk of asystole, may require electrical pacing (via either an internal or external route). The potential risk of asystole is indicated by the presence of any of the following: recent asystole; Mobitz II atrioventricular (AV) block; complete AV block (3rd degree heart block) (especially with broad QRS or initial heart rate < 40/min); ventricular standstill of > 3 sec. Many defibrillators now have the capacity to provide external pacing via the defibrillation paddles or adhesive pads. External pacing stimulates skeletal muscle as well as cardiac muscle and may produce discomfort to the patient. Guideline 11.9 Page 2 of 11

3 The pacing is usually set to demand (as required) at beats per minute starting low (eg. 30 ma) and increasing until electrical capture with established output occurs. In some settings (such as pre-hospital) where there is a concern that electrical artifact may inhibit pacing in the demand mode, it is reasonable to use a fixed (asynchronous) mode. Class of Recommendation A Reference [1, 3] TACHYARRHYTHMIA A tachyarrythmia may arise from the upper chambers of the heart (atria) or the lower chambers of the heart (ventricular). In the setting of cardiac arrest most arrhythmias will be ventricular in origin. Patients who do not experience symptoms associated with a tachycardia / tachyarrhythmia do not usually require emergency therapy specifically directed at the heart rhythm. Most sudden cardiac arrests (approximately 80%) occur as a result of abnormally fast and often disorganised electrical activity arising from the ventricle. These arrhythmias are called ventricular tachycardia (VT) when the rhythm is organised and ventricular fibrillation (VF) when the ECG appears to exhibit disorganised electrical activity (due to multiple complex reentry electrical circuits). The common symptoms of tachycardia include syncope (fainting), shortness of breath, dizziness, chest pain or palpitations. The following adverse features suggest a need for immediate treatment (see tachycardia algorithm): systolic BP < 90 mmhg; heart rate > 150/min; chest pain; heart failure; or drowsiness or confusion A pulseless patient with a tachyarrhythmia requires cardiac arrest management according to the cardiac arrest algorithm (see ARC Guideline 11.2). In the peri-arrest setting, if the patient is unstable and deteriorating with adverse features caused by the tachyarrythmia, attempt immediate synchronised cardioversion, with sedation as required. If cardioversion is unsuccessful give amiodarone 300 mg intravenously over min, then repeat attempted cardioversion. Follow the initial dose with an amiodarone infusion 900 mg over 24 h. If there are no adverse features during a tachyarrhythmia, determine whether the arrhythmia has narrow (i.e., normal duration) QRS complexes or whether they are broad (0.12 sec or longer). This distinguishes broad-complex tachycardia from narrow-complex tachycardia. Broad-complex tachycardia Although broad-complex tachycardia can be a supraventricular tachycardia with aberrant conduction (i.e., bundle branch block), in the peri-arrest setting assume that broad-complex tachycardias are ventricular in origin. Treating a supraventricular tachycardia (SVT) as if it were ventricular tachycardia (VT) is less likely to lead to deterioration than treating VT as SVT. Guideline 11.9 Page 3 of 11
![Class of Recommendation A Reference [1, 3] TACHYARRHYTHMIA A tachyarrythmia may arise from the upper chambers of the heart (atria) or the lower chambers of the heart (ventricular).](/docs-images/43/12633981/images/page_3.jpg "In the setting of cardiac arrest most arrhythmias will be ventricular in origin.")
4 Regular broad-complex tachycardia In the absence of adverse features, give amiodarone 300 mg intravenously over min, followed by an infusion of 900 mg over 24 h. Continue to monitor and assess the patient, seek expert help, and be prepared to use electrical cardioversion if adverse signs develop, or if the arrhythmia persists for several hours. Irregular broad complex tachycardia This is most likely to be atrial fibrillation (AF) with bundle branch block, but careful examination of a 12-lead ECG (if necessary by an expert) may enable confident identification of the rhythm. Other possible causes are AF with ventricular pre-excitation (in patients with Wolff-Parkinson-White (WPW) Syndrome), and polymorphic VT (e.g., torsades de pointes ). Seek expert help with the assessment and treatment of irregular broad-complex tachyarrhythmia. If pre-excited AF (or atrial flutter) is suspected, avoid adenosine, digoxin, verapamil and diltiazem. These drugs block the AV node and cause a relative increase in pre-excitation. Electrical cardioversion is usually the safest treatment option. Torsades de pointes is a specific type of ventricular tachyarrhythmia that occurs in the setting of acquired or congenital prolongation of the QT interval on the ECG (repolarisation phase). Torsades may be self limiting or sustained leading to cardiac arrest. Torsades leading to cardiac arrest is managed according to the cardiac arrest algorithm (see ARC Guideline 11.2). Treat torsades de pointes VT immediately by stopping all drugs known to prolong the QT interval and correct electrolyte abnormalities (especially hypokalaemia) and other causes (eg. ischaemia). Give a bolus of 5mmol of magnesium intravenously over 10 min, which may be repeated once and followed by an infusion of 20mmol over four hours. Acute pacing is recommended for patients presenting with torsades de pointes due to heart block and symptomatic bradycardia. Obtain expert help as other treatment (e.g. including overdrive pacing or isoprenaline) may be indicated to prevent relapse once the arrhythmia has been corrected. If adverse signs develop, arrange immediate synchronised cardioversion. Amiodarone should be avoided as this can make the situation worse. Summary Recommendations Sustained Monomorphic Ventricular Tachycardia Summary Recommendations Class A Wide-QRS tachycardia should be presumed to be VT if the diagnosis is unclear. (Level of Evidence: C) Direct current cardioversion with appropriate sedation is recommended at any point in the treatment cascade in patients with suspected sustained monomorphic VT with hemodynamic compromise. (Level of Evidence: IV) Class B Intravenous amiodarone is reasonable in patients with sustained monomorphic VT that is haemodynamically unstable, refractory to conversion with countershock, or recurrent despite other agents. (Level of Evidence: IV) Guideline 11.9 Page 4 of 11
 Syndrome), and polymorphic VT (e.g.")
5 Transvenous catheter pacing termination can be useful to treat patients with sustained monomorphic VT that is refractory to cardioversion or is frequently recurrent despite anti-arrhythmic medication. (Level of Evidence: IV) Intravenous lignocaine is reasonable for the initial treatment of patients with stable sustained monomorphic VT specifically associated with acute myocardial ischemia or infarction. (Level of Evidence: IV) Calcium channel blockers such as verapamil and diltiazem should not be used in patients to terminate wide-qrs-complex tachycardia of unknown origin, especially in patients with a history of myocardial dysfunction. (Level of Evidence: IV) Torsades de Pointes Summary Recommendations Class A Withdrawal of any offending drugs and correction of electrolyte abnormalities are recommended in patients presenting with torsades de pointes. (Level of Evidence:III- 2) Acute pacing is recommended for patients presenting with torsades de pointes due to heart block and symptomatic bradycardia. (Level of Evidence: III-2) Class B Management with intravenous magnesium sulfate is reasonable for patients who present with Long QT Syndrome (LQTS) and episodes of torsades de pointes. Magnesium is not likely to be effective in patients with a normal QT interval. (Level of Evidence: Acute pacing is reasonable for patients who present with recurrent pause-dependent torsades de pointes. (Level of Evidence: II) Beta blockade combined with pacing is reasonable acute therapy for patients who present with torsades de pointes and sinus bradycardia. (Level of Evidence:IV)) Isoprenaline is reasonable as temporary treatment in acute patients who present with recurrent pause dependent torsades de pointes who do not have congenital LQTS. (Level of Evidence:II) Reference [4] Narrow-complex tachycardia Narrow-complex tachycardias can be subdivided into regular and irregular types. Regular narrow-complex tachycardia Regular narrow-complex tachycardia include: sinus tachycardia; AV nodal re-entry tachycardia AVNRT (the commonest type of SVT); AV re-entry tachycardia - AVRT (caused by WPW Syndrome); and atrial flutter with regular AV conduction (usually 2:1). If the patient is unstable with adverse signs caused by the arrhythmia (other than sinus tachycardia), attempt synchronised electrical cardioversion, with sedation as required. Guideline 11.9 Page 5 of 11
 Calcium channel blockers such as verapamil and diltiazem should not be used in patients to terminate wide-qrs-complex tachycardia of unknown origin, especially in patients")
6 It is reasonable to give adenosine to an unstable patient with a regular narrow-complex tachycardia, while preparations are made for synchronized cardioversion. However, do not delay electrical cardioversion if the adenosine fails to restore sinus rhythm. In the absence of adverse features, start with vagal manoeuvres ( eg. the Valsalva manoeuvre [5]) If the arrhythmia persists and is not atrial flutter, use adenosine. Give 6 mg as a rapid intravenous bolus followed a minimum 20 ml flush. If the ventricular rate slows transiently, but the arrhythmia then persists, look for atrial activity such as atrial flutter or other atrial tachycardia and treat accordingly. If there is no response to adenosine 6 mg give a 12 mg bolus (which may be repeated). If adenosine is contra-indicated or fails to terminate a regular narrow-complex tachycardia without demonstrating that it is atrial flutter, give a calcium channel blocker (e.g. verapamil mg IV over 2 min; or diltiazem mg over 2 min). Level of Evidence (Verapamil IV, Diltiazem and beta blockers IV) Class of Recommendation Class A Reference: [6] Irregular narrow-complex tachycardia Irregular narrow-complex tachycardia is most commonly atrial fibrillation (AF) or sometimes atrial flutter with variable AV conduction (variable block). Atrial fibrillation is the most common of all arrhythmias arising from the upper chambers of the heart. The arrhythmia is caused by multiple re-entry circuits within the upper chamber usually triggered by ectopic (abnormal) foci located in tissue within the pulmonary veins that empty into the atria. The arrhythmia may arise in an otherwise normal heart or in the setting of major structural abnormalities (especially of the heart valves) or systemic disease states. This arrhythmia occurs with increasing frequency in older patient groups where it is often associated with underlying disease process. The hallmark of this rhythm disturbance is that it produces an irregularly irregular heart rhythm. Atrial flutter is a related but distinct arrhythmia caused by re-entry within the atria. It may be managed similarly to atrial fibrillation in the emergency setting. If the patient is unstable with adverse signs caused by the arrhythmia, attempt synchronised electrical cardioversion, with sedation as required. If there are no adverse features, treatment options include: rate control by drug therapy; rhythm control using drugs to encourage chemical cardioversion; rhythm control by electrical cardioversion; and treatment to prevent complications (e.g., anticoagulation). The longer a patient remains in AF the greater the likelihood of atrial clot developing. In general, patients who have been in AF for more than 48 hours should not be treated by cardioversion (electrical or chemical) until they have been fully anticoagulated or unless absence of atrial clot has been shown by trans-oesophageal echocardiography. Obtain expert help to determine the most appropriate treatment for the individual patient. Guideline 11.9 Page 6 of 11
![the Valsalva manoeuvre [5]) If the arrhythmia persists and is not atrial flutter, use adenosine. Give 6 mg as a rapid intravenous bolus followed a minimum 20 ml flush.](/docs-images/43/12633981/images/page_6.jpg "If the ventricular rate slows transiently, but the arrhythmia then persists, look for atrial activity such as atrial flutter or other atrial tachycardia and treat accordingly.")
7 In the acute care setting the simplest approach to managing this condition is to control the rate of ventricular response. This can be achieved with agents such as oral or intravenous beta blockers (metoprolol 5mg IV) (contraindications would include a history of bronchospasm or evidence of decompensated heart failure) or digoxin (250 mcg to 500mcg IV or PO). In cases of paroxysmal (intermittent) atrial fibrillation many patients revert to a normal heart rhythm spontaneously. Pharmacological Rate Control During Atrial Fibrillation RECOMMENDATIONS Class A Measurement of the heart rate at rest and control of the rate using pharmacological agents (either a beta blocker or nondihydropyridine calcium channel antagonist (verapamil, diltiazem) in most cases) are recommended for patients with persistent or permanent AF.(Level of Evidence: II) In the absence of pre-excitation, intravenous administration of beta blockers or nondihydropyridine calcium channel antagonists (verapamil, diltiazem) is recommended to slow the ventricular response to AF in the acute setting, exercising caution in patients with hypotension or HF. (Level of Evidence: II Intravenous administration of digoxin or amiodarone is recommended to control the heart rate in patients with AF and HF who do not have an accessory pathway. (Level of Evidence: II) In patients who experience symptoms related to AF during activity, the adequacy of heart rate control should be assessed during exercise, adjusting pharmacological treatment as necessary to keep the rate in the physiological range. (Level of Evidence: IV) Digoxin is effective following oral administration to control the heart rate at rest in patients with AF and is indicated for patients with HF, LV dysfunction, or for sedentary individuals. (Level of Evidence:IV) Class B A combination of digoxin and either a beta blocker or nondihydropyridine calcium channel antagonist is reasonable to control the heart rate both at rest and during exercise in patients with AF. The choice of medication should be individualized and the dose modulated to avoid bradycardia. (Level of Evidence:II) Amiodarone can be useful to control the heart rate in patients with AF when other measures are unsuccessful or contraindicated. (Level of Evidence: II) Class C When the ventricular rate cannot be adequately controlled both at rest and during exercise in patients with AF using a beta blocker, nondihydropyridine calcium channel antagonist or digoxin, alone or in combination, oral amiodarone may be administered to control the heart rate. (Level of Evidence: III-2) Guideline 11.9 Page 7 of 11

8 Amiodarone may be considered for hemodynamically stable patients with AF involving conduction over an accessory pathway. (Level of Evidence: III-2) Class C Digoxin should not be used as the sole agent to control the rate of ventricular response in patients with paroxysmal AF. (Level of Evidence: II) Intravenous administration of digoxin or nondihydropyridine calcium channel antagonists to patients with AF and a preexcitation syndrome may paradoxically accelerate the ventricular response and is not recommended. (Level of Evidence: IV) Reference: [7] REFERENCES International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Part 4: Advanced Life Support. Resuscitation Nov-Dec; 67(2-3): Shepherd G. Treatment of poisoning caused by beta-adrenergic and calcium-channel blockers. Am J Health Syst Pharm. 2006;63(19): Advanced Life Support 5 th Edition (Australian Edition). Melbourne. Australian Resuscitation Council Zipes DP, et al; American College of Cardiology/American Heart Association Task Force; European Society of Cardiology Committee for Practice Guidelines; European Heart Rhythm Association; Heart Rhythm Society. ACC/AHA/ESC 2006 Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: a report of the American College of Cardiology/American Heart Association Task Force and the European Society of Cardiology Committee for Practice Guidelines (writing committee to develop Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death): developed in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. Circulation Sep 5;114(10):e Wong LF, Taylor DM, Bailey M. Vagal Response Varies With Valsalva Maneuver Technique: A Repeated-Measures Clinical Trial in Healthy Subjects. Ann Emerg Med. 2004;43: Blomström-Lundqvist C, et al; European Society of Cardiology Committee, NASPE- Heart Rhythm Society. ACC/AHA/ESC guidelines for the management of patients with supraventricular arrhythmias--executive summary. A report of the American College of Cardiology/American heart association task force on practice guidelines and the European Society of Cardiology Committee for practice guidelines (writing committee to develop guidelines for the management of patients with supraventricular arrhythmias) developed in collaboration with NASPE-Heart Rhythm Society. J Am Coll Cardiol Oct 15;42(8): Guideline 11.9 Page 8 of 11
 Reference: [7] REFERENCES 1.")
9 7. Fuster V, et al; American College of Cardiology/American Heart Association Task Force on Practice Guidelines; European Society of Cardiology Committee for Practice Guidelines; European Heart Rhythm Association; Heart Rhythm Society. ACC/AHA/ESC 2006 Guidelines for the Management of Patients with Atrial Fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Revise the 2001 Guidelines for the Management of Patients With Atrial Fibrillation): developed in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. Circulation Aug 15;114(7):e Erratum in: Circulation Aug 7;116(6):e138. FURTHER READING ARC Guideline 7 Cardiopulmonary Resuscitation ARC Guideline 11.2 Protocols for Adult Advanced Life Support ARC Guideline 11.8 Post-resuscitation therapy in Adult Advanced Life Support Guideline 11.9 Page 9 of 11
: developed in")
10 Guideline 11.9 Page 10 of 11
11 Guideline 11.9 November 2009 Page 11 of 11 AUSTRALIAN RESUSCITATION COUNCIL

8 Peri-arrest arrhythmias
 8 Peri-arrest arrhythmias Introduction Cardiac arrhythmias are relatively common in the peri-arrest period. They are common in the setting of acute myocardial infarction and may precipitate ventricular
8 Peri-arrest arrhythmias Introduction Cardiac arrhythmias are relatively common in the peri-arrest period. They are common in the setting of acute myocardial infarction and may precipitate ventricular
Recurrent AF: Choosing the Right Medication.
 In the name of God Shiraz E-Medical Journal Vol. 11, No. 3, July 2010 http://semj.sums.ac.ir/vol11/jul2010/89015.htm Recurrent AF: Choosing the Right Medication. Basamad Z. * Assistant Professor, Department
In the name of God Shiraz E-Medical Journal Vol. 11, No. 3, July 2010 http://semj.sums.ac.ir/vol11/jul2010/89015.htm Recurrent AF: Choosing the Right Medication. Basamad Z. * Assistant Professor, Department
ACLS PHARMACOLOGY 2011 Guidelines
 ACLS PHARMACOLOGY 2011 Guidelines ADENOSINE Narrow complex tachycardias or wide complex tachycardias that may be supraventricular in nature. It is effective in treating 90% of the reentry arrhythmias.
ACLS PHARMACOLOGY 2011 Guidelines ADENOSINE Narrow complex tachycardias or wide complex tachycardias that may be supraventricular in nature. It is effective in treating 90% of the reentry arrhythmias.
ACLS PRE-TEST ANNOTATED ANSWER KEY
 ACLS PRE-TEST ANNOTATED ANSWER KEY June, 2011 Question 1: Question 2: There is no pulse with this rhythm. Question 3: Question 4: Question 5: Question 6: Question 7: Question 8: Question 9: Question 10:
ACLS PRE-TEST ANNOTATED ANSWER KEY June, 2011 Question 1: Question 2: There is no pulse with this rhythm. Question 3: Question 4: Question 5: Question 6: Question 7: Question 8: Question 9: Question 10:
Atrial & Junctional Dysrhythmias
 Atrial & Junctional Dysrhythmias Atrial & Junctional Dysrhythmias Atrial Premature Atrial Complex Wandering Atrial Pacemaker Atrial Tachycardia (ectopic) Multifocal Atrial Tachycardia Atrial Flutter Atrial
Atrial & Junctional Dysrhythmias Atrial & Junctional Dysrhythmias Atrial Premature Atrial Complex Wandering Atrial Pacemaker Atrial Tachycardia (ectopic) Multifocal Atrial Tachycardia Atrial Flutter Atrial
Tachyarrhythmias (fast heart rhythms)
") Patient information factsheet Tachyarrhythmias (fast heart rhythms) The normal electrical system of the heart The heart has its own electrical conduction system. The conduction system sends signals throughout
Patient information factsheet Tachyarrhythmias (fast heart rhythms) The normal electrical system of the heart The heart has its own electrical conduction system. The conduction system sends signals throughout
Present : PGY 王 淳 峻 Supervisor: F1 王 德 皓 991109
 Present : PGY 王 淳 峻 Supervisor: F1 王 德 皓 991109 Interventions to prevent cardiac arrest + Airway management + Ventilation support + Treatment of bradyarrhythmias & Tachyarrhythmias Treat cardiac arrest
Present : PGY 王 淳 峻 Supervisor: F1 王 德 皓 991109 Interventions to prevent cardiac arrest + Airway management + Ventilation support + Treatment of bradyarrhythmias & Tachyarrhythmias Treat cardiac arrest
If you do not wish to print the entire pre-test you may print Page 2 only to write your answers, score your test, and turn in to your instructor.
 This is a SAMPLE of the pretest you can access with your AHA PALS Course Manual at Heart.org/Eccstudent using your personal code that comes with your PALS Course Manual The American Heart Association strongly
This is a SAMPLE of the pretest you can access with your AHA PALS Course Manual at Heart.org/Eccstudent using your personal code that comes with your PALS Course Manual The American Heart Association strongly
American Heart Association ACLS Pre-Course Self Assessment Dec., 2006. ECG Analysis. Name the following rhythms from the list below:
 American Heart Association ACLS Pre-Course Self Assessment Dec., 2006 ECG Analysis This pre-test is exactly the same as the pretest on the ACLS Provider manual CD. This paper version can be completed in
American Heart Association ACLS Pre-Course Self Assessment Dec., 2006 ECG Analysis This pre-test is exactly the same as the pretest on the ACLS Provider manual CD. This paper version can be completed in
Crash Cart Drugs Drugs used in CPR. Dr. Layla Borham Professor of Clinical Pharmacology Umm Al Qura University
 Crash Cart Drugs Drugs used in CPR Dr. Layla Borham Professor of Clinical Pharmacology Umm Al Qura University Introduction A list of the drugs kept in the crash carts. This list has been approved by the
Crash Cart Drugs Drugs used in CPR Dr. Layla Borham Professor of Clinical Pharmacology Umm Al Qura University Introduction A list of the drugs kept in the crash carts. This list has been approved by the
Cardiac Arrest VF/Pulseless VT Learning Station Checklist
 Cardiac Arrest VF/Pulseless VT Learning Station Checklist VF/VT 00 American Heart Association Adult Cardiac Arrest Shout for Help/Activate Emergency Response Epinephrine every - min Amiodarone Start CPR
Cardiac Arrest VF/Pulseless VT Learning Station Checklist VF/VT 00 American Heart Association Adult Cardiac Arrest Shout for Help/Activate Emergency Response Epinephrine every - min Amiodarone Start CPR
ACLS Cardiac Arrest Algorithm Neumar, R. W. et al. Circulation 2010;122:S729-S767
 ACLS Cardiac Arrest Algorithm Neumar, R. W. et al. Circulation 2010;122:S729-S767 Copyright 2010 American Heart Association ACLS Cardiac Arrest Circular Algorithm Neumar, R. W. et al. Circulation 2010;122:S729-S767
ACLS Cardiac Arrest Algorithm Neumar, R. W. et al. Circulation 2010;122:S729-S767 Copyright 2010 American Heart Association ACLS Cardiac Arrest Circular Algorithm Neumar, R. W. et al. Circulation 2010;122:S729-S767
Current Management of Atrial Fibrillation DISCLOSURES. Heart Beat Anatomy. I have no financial conflicts to disclose
 Current Management of Atrial Fibrillation Mary Macklin, MSN, APRN Concord Hospital Cardiac Associates DISCLOSURES I have no financial conflicts to disclose Book Women: Fit at Fifty. A Guide to Living Long.
Current Management of Atrial Fibrillation Mary Macklin, MSN, APRN Concord Hospital Cardiac Associates DISCLOSURES I have no financial conflicts to disclose Book Women: Fit at Fifty. A Guide to Living Long.
PRO-CPR. 2015 Guidelines: PALS Algorithm Overview. (Non-AHA supplementary precourse material)
") PRO-CPR 2015 Guidelines: PALS Algorithm Overview (Non-AHA supplementary precourse material) Please reference Circulation (from our website), the ECC Handbook, or the 2015 ACLS Course Manual for correct
PRO-CPR 2015 Guidelines: PALS Algorithm Overview (Non-AHA supplementary precourse material) Please reference Circulation (from our website), the ECC Handbook, or the 2015 ACLS Course Manual for correct
PRACTICAL APPROACH TO SVT. Graham C. Wong MD MPH Division of Cardiology Vancouver General Hospital University of British Columbia
 PRACTICAL APPROACH TO SVT Graham C. Wong MD MPH Division of Cardiology Vancouver General Hospital University of British Columbia CONDUCTION SYSTEM OF THE HEART SA node His bundle Left bundle AV node Right
PRACTICAL APPROACH TO SVT Graham C. Wong MD MPH Division of Cardiology Vancouver General Hospital University of British Columbia CONDUCTION SYSTEM OF THE HEART SA node His bundle Left bundle AV node Right
Official Online ACLS Exam
 \ Official Online ACLS Exam Please fill out this form before you take the exam. Name : Email : Phone : 1. Hypovolemia initially produces which arrhythmia? A. PEA B. Sinus tachycardia C. Symptomatic bradyarrhythmia
\ Official Online ACLS Exam Please fill out this form before you take the exam. Name : Email : Phone : 1. Hypovolemia initially produces which arrhythmia? A. PEA B. Sinus tachycardia C. Symptomatic bradyarrhythmia
Guideline for the management of arrhythmias
 Guideline for the management of arrhythmias The following guideline is approved only for use at University College London Hospitals NHS Foundation Trust. It is provided as supporting information for the
Guideline for the management of arrhythmias The following guideline is approved only for use at University College London Hospitals NHS Foundation Trust. It is provided as supporting information for the
ACLS Provider Manual Comparison Sheet Based on 2010 AHA Guidelines for CPR and ECC. BLS Changes
 ACLS Provider Manual Comparison Sheet Based on 2010 AHA Guidelines for CPR and ECC CPR Chest compressions, Airway, Breathing (C-A-B) BLS Changes New Old Rationale New science indicates the following order:
ACLS Provider Manual Comparison Sheet Based on 2010 AHA Guidelines for CPR and ECC CPR Chest compressions, Airway, Breathing (C-A-B) BLS Changes New Old Rationale New science indicates the following order:
ANNE ARUNDEL MEDICAL CENTER CRITICAL CARE MEDICATION MANUAL DEPARTMENT OF NURSING AND PHARMACY. Guidelines for Use of Intravenous Isoproterenol
 ANNE ARUNDEL MEDICAL CENTER CRITICAL CARE MEDICATION MANUAL DEPARTMENT OF NURSING AND PHARMACY Guidelines for Use of Intravenous Isoproterenol Major Indications Status Asthmaticus As a last resort for
ANNE ARUNDEL MEDICAL CENTER CRITICAL CARE MEDICATION MANUAL DEPARTMENT OF NURSING AND PHARMACY Guidelines for Use of Intravenous Isoproterenol Major Indications Status Asthmaticus As a last resort for
HTEC 91. Topic for Today: Atrial Rhythms. NSR with PAC. Nonconducted PAC. Nonconducted PAC. Premature Atrial Contractions (PACs)
") HTEC 91 Medical Office Diagnostic Tests Week 4 Topic for Today: Atrial Rhythms PACs: Premature Atrial Contractions PAT: Paroxysmal Atrial Tachycardia AF: Atrial Fibrillation Atrial Flutter Premature Atrial
HTEC 91 Medical Office Diagnostic Tests Week 4 Topic for Today: Atrial Rhythms PACs: Premature Atrial Contractions PAT: Paroxysmal Atrial Tachycardia AF: Atrial Fibrillation Atrial Flutter Premature Atrial
An Introduction to Tachyarrhythmias R. A. Seyon MN, NP, CCN(C) & Dr. R. G. Williams
 & Dr. R. G. Williams") Arrhythmias 1 An Introduction to Tachyarrhythmias R. A. Seyon MN, NP, CCN(C) & Dr. R. G. Williams Things to keep in mind when analyzing arrhythmias: Electrical activity recorded in 12 and 15 leads Examine
Arrhythmias 1 An Introduction to Tachyarrhythmias R. A. Seyon MN, NP, CCN(C) & Dr. R. G. Williams Things to keep in mind when analyzing arrhythmias: Electrical activity recorded in 12 and 15 leads Examine
Catheter Ablation. A Guided Approach for Treating Atrial Arrhythmias
 Catheter Ablation A Guided Approach for Treating Atrial Arrhythmias A P A T I E N T H A N D B O O K This brochure will provide an overview of atrial arrhythmias (heart rhythm problems affecting the upper
Catheter Ablation A Guided Approach for Treating Atrial Arrhythmias A P A T I E N T H A N D B O O K This brochure will provide an overview of atrial arrhythmias (heart rhythm problems affecting the upper
Treating AF: The Newest Recommendations. CardioCase presentation. Ethel s Case. Wayne Warnica, MD, FACC, FACP, FRCPC
 Treating AF: The Newest Recommendations Wayne Warnica, MD, FACC, FACP, FRCPC CardioCase presentation Ethel s Case Ethel, 73, presents with rapid heart beating and mild chest discomfort. In the ED, ECG
Treating AF: The Newest Recommendations Wayne Warnica, MD, FACC, FACP, FRCPC CardioCase presentation Ethel s Case Ethel, 73, presents with rapid heart beating and mild chest discomfort. In the ED, ECG
JAPI VOL. 52 NOVEMBER 2004 www.japi.org 883
 Review Article Wide Complex Tachycardia : Recognition and Management in the Emergency Room IB Ray Abstract Cardiac arrhythmias often present as urgent medical conditions requiring immediate care. Patient
Review Article Wide Complex Tachycardia : Recognition and Management in the Emergency Room IB Ray Abstract Cardiac arrhythmias often present as urgent medical conditions requiring immediate care. Patient
School of Health Sciences
 School of Health Sciences Cardiology Teaching Package A Beginners Guide to Normal Heart Function, Sinus Rhythm & Common Cardiac Arrhythmias Welcome This document extends subjects covered in the Cardiology
School of Health Sciences Cardiology Teaching Package A Beginners Guide to Normal Heart Function, Sinus Rhythm & Common Cardiac Arrhythmias Welcome This document extends subjects covered in the Cardiology
ATRIAL FIBRILLATION (RATE VS RHYTHM CONTROL)
") ATRIAL FIBRILLATION (RATE VS RHYTHM CONTROL) By Prof. Dr. Helmy A. Bakr Mansoura Universirty 2014 AF Classification: Mechanisms of AF : Selected Risk Factors and Biomarkers for AF: WHY AF? 1. Atrial fibrillation
ATRIAL FIBRILLATION (RATE VS RHYTHM CONTROL) By Prof. Dr. Helmy A. Bakr Mansoura Universirty 2014 AF Classification: Mechanisms of AF : Selected Risk Factors and Biomarkers for AF: WHY AF? 1. Atrial fibrillation
COVERAGE GUIDANCE: ABLATION FOR ATRIAL FIBRILLATION
 COVERAGE GUIDANCE: ABLATION FOR ATRIAL FIBRILLATION Question: How should the EGBS Coverage Guidance regarding ablation for atrial fibrillation be applied to the Prioritized List? Question source: Evidence
COVERAGE GUIDANCE: ABLATION FOR ATRIAL FIBRILLATION Question: How should the EGBS Coverage Guidance regarding ablation for atrial fibrillation be applied to the Prioritized List? Question source: Evidence
Atrial Fibrillation: Drugs, Ablation, or Benign Neglect. Robert Kennedy, MD October 10, 2015
 Atrial Fibrillation: Drugs, Ablation, or Benign Neglect Robert Kennedy, MD October 10, 2015 Definitions 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation: Executive Summary.
Atrial Fibrillation: Drugs, Ablation, or Benign Neglect Robert Kennedy, MD October 10, 2015 Definitions 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation: Executive Summary.
E C C. American Heart Association. Advanced Cardiovascular Life Support. Written Precourse Self-Assessment. May 2011. 2011 American Heart Association
 E C C American Heart Association Advanced Cardiovascular Life Support Written Precourse Self-Assessment May 2011 2011 American Heart Association 2011 ACLS Written Precourse Self-Assessment 1. Ten minutes
E C C American Heart Association Advanced Cardiovascular Life Support Written Precourse Self-Assessment May 2011 2011 American Heart Association 2011 ACLS Written Precourse Self-Assessment 1. Ten minutes
TOP 5. The term cardiac arrhythmia encompasses all cardiac. Arrhythmias in Dogs & Cats. Sinus Arrhythmia. TOP 5 Arrhythmias Seen in Dogs & Cats
 Top 5 ardiology Peer reviewed TOP 5 rrhythmias in Dogs & ats shley Jones, DVM mara Estrada, DVM, DVIM (ardiology) University of Florida The term cardiac arrhythmia encompasses all cardiac rhythms other
Top 5 ardiology Peer reviewed TOP 5 rrhythmias in Dogs & ats shley Jones, DVM mara Estrada, DVM, DVIM (ardiology) University of Florida The term cardiac arrhythmia encompasses all cardiac rhythms other
Cardioversion for. Atrial Fibrillation. Your Heart s Electrical System Cardioversion Living with Atrial Fibrillation
 Cardioversion for Atrial Fibrillation Your Heart s Electrical System Cardioversion Living with Atrial Fibrillation When You Have Atrial Fibrillation You ve been told you have a heart condition called atrial
Cardioversion for Atrial Fibrillation Your Heart s Electrical System Cardioversion Living with Atrial Fibrillation When You Have Atrial Fibrillation You ve been told you have a heart condition called atrial
Wide-Complex Tachycardias in the ED: Myths and Pitfalls
 Wide-Complex Tachycardias in the ED: Myths and Pitfalls, FACEP, FAAEM Professor and Vice Chair Director, Emergency Cardiology Fellowship Department of Emergency Medicine University of Maryland School of
Wide-Complex Tachycardias in the ED: Myths and Pitfalls, FACEP, FAAEM Professor and Vice Chair Director, Emergency Cardiology Fellowship Department of Emergency Medicine University of Maryland School of
Atrial Fibrillation Peter Santucci, MD Revised May, 2008
 Atrial Fibrillation Peter Santucci, MD Revised May, 2008 Atrial fibrillation (AF) is an irregular, disorganized rhythm characterized by a lack of organized mechanical atrial activity. The atrial rate is
Atrial Fibrillation Peter Santucci, MD Revised May, 2008 Atrial fibrillation (AF) is an irregular, disorganized rhythm characterized by a lack of organized mechanical atrial activity. The atrial rate is
Quiz 4 Arrhythmias summary statistics and question answers
 1 Quiz 4 Arrhythmias summary statistics and question answers The correct answers to questions are indicated by *. All students were awarded 2 points for question #2 due to no appropriate responses for
1 Quiz 4 Arrhythmias summary statistics and question answers The correct answers to questions are indicated by *. All students were awarded 2 points for question #2 due to no appropriate responses for
RUSSELLS HALL HOSPITAL EMERGENCY DEPARTMENT
 RUSSELLS HALL HOSPITAL EMERGENCY DEPARTMENT CLINICAL GUIDELINE ATRIAL FIBRILLATION March 2011 For quick links to AF algorithms: UNSTABLE PATIENT STABLE PATIENT - 1 - Introduction Atrial fibrillation is
RUSSELLS HALL HOSPITAL EMERGENCY DEPARTMENT CLINICAL GUIDELINE ATRIAL FIBRILLATION March 2011 For quick links to AF algorithms: UNSTABLE PATIENT STABLE PATIENT - 1 - Introduction Atrial fibrillation is
Atrial Fibrillation An update on diagnosis and management
 Dr Arvind Vasudeva Consultant Cardiologist Atrial Fibrillation An update on diagnosis and management Atrial fibrillation (AF) remains the commonest disturbance of cardiac rhythm seen in clinical practice.
Dr Arvind Vasudeva Consultant Cardiologist Atrial Fibrillation An update on diagnosis and management Atrial fibrillation (AF) remains the commonest disturbance of cardiac rhythm seen in clinical practice.
IU Health ACLS Study Guide
 IU Health ACLS Study Guide Preparing for your upcoming ACLS Class REVISED SEPTEMBER 2011 ON APRIL 1, 2011 WE BEGAN TEACHING THE 2010 AHA GUIDELINES. WE HIGHLY RECOMMEND REVIEWING THE NEW ALGORYHMS FOUND
IU Health ACLS Study Guide Preparing for your upcoming ACLS Class REVISED SEPTEMBER 2011 ON APRIL 1, 2011 WE BEGAN TEACHING THE 2010 AHA GUIDELINES. WE HIGHLY RECOMMEND REVIEWING THE NEW ALGORYHMS FOUND
Presenter Disclosure Information
 2:15 3 pm Managing Arrhythmias in Primary Care Presenter Disclosure Information The following relationships exist related to this presentation: Raul Mitrani, MD, FACC, FHRS: Speakers Bureau for Medtronic.
2:15 3 pm Managing Arrhythmias in Primary Care Presenter Disclosure Information The following relationships exist related to this presentation: Raul Mitrani, MD, FACC, FHRS: Speakers Bureau for Medtronic.
Treatments to Restore Normal Rhythm
 Treatments to Restore Normal Rhythm In many instances when AF causes significant symptoms or is negatively impacting a patient's health, the major goal of treatment is to restore normal rhythm and prevent
Treatments to Restore Normal Rhythm In many instances when AF causes significant symptoms or is negatively impacting a patient's health, the major goal of treatment is to restore normal rhythm and prevent
Medical management of CHF: A New Class of Medication. Al Timothy, M.D. Cardiovascular Institute of the South
 Medical management of CHF: A New Class of Medication Al Timothy, M.D. Cardiovascular Institute of the South Disclosures Speakers Bureau for Amgen Background Chronic systolic congestive heart failure remains
Medical management of CHF: A New Class of Medication Al Timothy, M.D. Cardiovascular Institute of the South Disclosures Speakers Bureau for Amgen Background Chronic systolic congestive heart failure remains
Diagnosis Code Crosswalk : ICD-9-CM to ICD-10-CM Cardiac Rhythm and Heart Failure Diagnoses
 Diagnosis Code Crosswalk : to 402.01 Hypertensive heart disease, malignant, with heart failure 402.11 Hypertensive heart disease, benign, with heart failure 402.91 Hypertensive heart disease, unspecified,
Diagnosis Code Crosswalk : to 402.01 Hypertensive heart disease, malignant, with heart failure 402.11 Hypertensive heart disease, benign, with heart failure 402.91 Hypertensive heart disease, unspecified,
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT of Atrial Fibrillation (AF)
 MANAGEMENT of Atrial Fibrillation (AF)") DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT of Atrial Fibrillation (AF) Key priorities Identification and diagnosis Treatment for persistent AF Treatment for permanent AF Antithrombotic
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT of Atrial Fibrillation (AF) Key priorities Identification and diagnosis Treatment for persistent AF Treatment for permanent AF Antithrombotic
Atrial fibrillation. Quick reference guide. Issue date: June 2006. The management of atrial fibrillation
 Quick reference guide Issue date: June 2006 Atrial fibrillation The management of atrial fibrillation Developed by the National Collaborating Centre for Chronic Conditions Contents Contents Patient-centred
Quick reference guide Issue date: June 2006 Atrial fibrillation The management of atrial fibrillation Developed by the National Collaborating Centre for Chronic Conditions Contents Contents Patient-centred
Evaluation and Initial Treatment of Supraventricular Tachycardia
 T h e n e w e ngl a nd j o u r na l o f m e dic i n e clinical practice Evaluation and Initial Treatment of Supraventricular Tachycardia Mark S. Link, M.D. This Journal feature begins with a case vignette
T h e n e w e ngl a nd j o u r na l o f m e dic i n e clinical practice Evaluation and Initial Treatment of Supraventricular Tachycardia Mark S. Link, M.D. This Journal feature begins with a case vignette
Protocol for the management of atrial fibrillation in primary care
 Protocol for the management of atrial fibrillation in primary care Protocol for the management of atrial fibrillation in primary care Contents Page no Definition 2 Classification of AF 2 3 Identification
Protocol for the management of atrial fibrillation in primary care Protocol for the management of atrial fibrillation in primary care Contents Page no Definition 2 Classification of AF 2 3 Identification
Equine Cardiovascular Disease
 Equine Cardiovascular Disease 3 rd most common cause of poor performance in athletic horses (after musculoskeletal and respiratory) Cardiac abnormalities are rare Clinical Signs: Poor performance/exercise
Equine Cardiovascular Disease 3 rd most common cause of poor performance in athletic horses (after musculoskeletal and respiratory) Cardiac abnormalities are rare Clinical Signs: Poor performance/exercise
Introduction to Electrophysiology. Wm. W. Barrington, MD, FACC University of Pittsburgh Medical Center
 Introduction to Electrophysiology Wm. W. Barrington, MD, FACC University of Pittsburgh Medical Center Objectives Indications for EP Study How do we do the study Normal recordings Abnormal Recordings Limitations
Introduction to Electrophysiology Wm. W. Barrington, MD, FACC University of Pittsburgh Medical Center Objectives Indications for EP Study How do we do the study Normal recordings Abnormal Recordings Limitations
Team Leader. Ensures high-quality CPR at all times Assigns team member roles Ensures that team members perform well. Bradycardia Management
 ACLS Megacode Case 1: Sinus Bradycardia (Bradycardia VF/Pulseless VT Asystole Out-of-Hospital Scenario You are a paramedic and arrive on the scene to find a 57-year-old woman complaining of indigestion.
ACLS Megacode Case 1: Sinus Bradycardia (Bradycardia VF/Pulseless VT Asystole Out-of-Hospital Scenario You are a paramedic and arrive on the scene to find a 57-year-old woman complaining of indigestion.
Electrophysiology Heart Study - EPS -
 Electrophysiology Heart Study - EPS - What is an EPS? EPS is short for ElectroPhysiology heart Study. This procedure looks at the electrical system of your heart. An EPS will show if you have a heart rhythm
Electrophysiology Heart Study - EPS - What is an EPS? EPS is short for ElectroPhysiology heart Study. This procedure looks at the electrical system of your heart. An EPS will show if you have a heart rhythm
Novartis Gilenya FDO Program Clinical Protocol and Highlights from Prescribing Information (PI)
") Novartis Gilenya FDO Program Clinical Protocol and Highlights from Prescribing Information (PI) Highlights from Prescribing Information - the link to the full text PI is as follows: http://www.pharma.us.novartis.com/product/pi/pdf/gilenya.pdf
Novartis Gilenya FDO Program Clinical Protocol and Highlights from Prescribing Information (PI) Highlights from Prescribing Information - the link to the full text PI is as follows: http://www.pharma.us.novartis.com/product/pi/pdf/gilenya.pdf
MEDICATIONS USED IN ADULT CODE BLUE EMERGENCIES. Source: ACLS Provider Manual. American Heart Association. 2001, 2002. Updated 2003.
 MEDICATIONS USED IN ADULT CODE BLUE EMERGENCIES Source: ACLS Provider Manual. American Heart Association. 2001, 2002. Updated 2003. 1 ET Administration Atropine o First drug for symptomatic sinus bradycardia
MEDICATIONS USED IN ADULT CODE BLUE EMERGENCIES Source: ACLS Provider Manual. American Heart Association. 2001, 2002. Updated 2003. 1 ET Administration Atropine o First drug for symptomatic sinus bradycardia
Management of ATRIAL FIBRILLATION. in general practice. 22 BPJ Issue 39
 Management of ATRIAL FIBRILLATION in general practice 22 BPJ Issue 39 What is atrial fibrillation? Atrial fibrillation (AF) is the most common cardiac arrhythmia encountered in primary care. It is often
Management of ATRIAL FIBRILLATION in general practice 22 BPJ Issue 39 What is atrial fibrillation? Atrial fibrillation (AF) is the most common cardiac arrhythmia encountered in primary care. It is often
Ngaire has Palpitations
 Ngaire has Palpitations David Heaven Cardiac Electrophysiologist/Heart Rhythm Specialist Middlemore, Auckland City and Mercy Hospitals Auckland Heart Group MCQ Ms A is 45, and a healthy marathon runner.
Ngaire has Palpitations David Heaven Cardiac Electrophysiologist/Heart Rhythm Specialist Middlemore, Auckland City and Mercy Hospitals Auckland Heart Group MCQ Ms A is 45, and a healthy marathon runner.
TABLE 1 Clinical Classification of AF. New onset AF (first detected) Paroxysmal (<7 days, mostly < 24 hours)
 Paroxysmal (<7 days, mostly < 24 hours)") Clinical Practice Guidelines for the Management of Patients With Atrial Fibrillation Deborah Ritchie RN, MN, Robert S Sheldon MD, PhD Cardiovascular Research Group, University of Calgary, Alberta Partly
Clinical Practice Guidelines for the Management of Patients With Atrial Fibrillation Deborah Ritchie RN, MN, Robert S Sheldon MD, PhD Cardiovascular Research Group, University of Calgary, Alberta Partly
Atrial Fibrillation Management Across the Spectrum of Illness
 Disclosures Atrial Fibrillation Management Across the Spectrum of Illness NONE Barbara Birriel, MSN, ACNP-BC, FCCM The Pennsylvania State University Objectives AF Discuss the pathophysiology, diagnosis,
Disclosures Atrial Fibrillation Management Across the Spectrum of Illness NONE Barbara Birriel, MSN, ACNP-BC, FCCM The Pennsylvania State University Objectives AF Discuss the pathophysiology, diagnosis,
Atrial fibrillation (AF) care pathways. for the primary care physicians
 care pathways. for the primary care physicians") Atrial fibrillation (AF) care pathways for the primary care physicians by University of Minnesota Physicians Heart, October, 2011 Evaluation by the primary care physician: 1. Comprehensive history and
Atrial fibrillation (AF) care pathways for the primary care physicians by University of Minnesota Physicians Heart, October, 2011 Evaluation by the primary care physician: 1. Comprehensive history and
22 Arrhythmias. C. Scharf and F. Duru. Siegenthaler, Differential Diagnosis in Internal Medicine (ISBN9783131421418), 2007 Georg Thieme Verlag
, 2007 Georg Thieme Verlag") 22 22 Arrhythmias C. Scharf and F. Duru 22 712 Arrhythmias 22.1 Differential Diagnosis of Arrhythmias 714 Medical History 714 Clinical Examination 714 Electrocardiogram (ECG) 715 Additional Tools for the
22 22 Arrhythmias C. Scharf and F. Duru 22 712 Arrhythmias 22.1 Differential Diagnosis of Arrhythmias 714 Medical History 714 Clinical Examination 714 Electrocardiogram (ECG) 715 Additional Tools for the
Electrophysiology Daymar College. Lisa H. Young, RN, BSN, MAE 2011
 Electrophysiology Daymar College Lisa H. Young, RN, BSN, MAE 2011 Electrical Conduction Pathway Chemical Basis for Impulse Formation Cardiac Action Potential Phases http://www.youtube.com/watch?v=oqpffilde0e
Electrophysiology Daymar College Lisa H. Young, RN, BSN, MAE 2011 Electrical Conduction Pathway Chemical Basis for Impulse Formation Cardiac Action Potential Phases http://www.youtube.com/watch?v=oqpffilde0e
INFORMATION FOR PATIENTS AND FAMILIES A Patient s Guide to Living with Atrial Fibrillation
 INFORMATION FOR PATIENTS AND FAMILIES A Patient s Guide to Living with Atrial Fibrillation 30 Bond Street, Toronto, ON M5B 1W8 Canada 416.864.6060 stmichaelshospital.com Form No. XXXXX Dev. XX/XXXX GOALS
INFORMATION FOR PATIENTS AND FAMILIES A Patient s Guide to Living with Atrial Fibrillation 30 Bond Street, Toronto, ON M5B 1W8 Canada 416.864.6060 stmichaelshospital.com Form No. XXXXX Dev. XX/XXXX GOALS
By the end of this continuing education module the clinician will be able to:
 EKG Interpretation WWW.RN.ORG Reviewed March, 2015, Expires April, 2017 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2015 RN.ORG, S.A., RN.ORG, LLC Developed
EKG Interpretation WWW.RN.ORG Reviewed March, 2015, Expires April, 2017 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2015 RN.ORG, S.A., RN.ORG, LLC Developed
Introduction 2/9/2015
 Thomas Haffey, D.O. FACC, FACOI, FNLA, CSOM February, 2015 Atrial Tachycardias Diagram summarizing types of atrial tachycardias often encountered in patients with a history of AF, including those seen
Thomas Haffey, D.O. FACC, FACOI, FNLA, CSOM February, 2015 Atrial Tachycardias Diagram summarizing types of atrial tachycardias often encountered in patients with a history of AF, including those seen
Potential Causes of Sudden Cardiac Arrest in Children
 Potential Causes of Sudden Cardiac Arrest in Children Project S.A.V.E. When sudden death occurs in children, adolescents and younger adults, heart abnormalities are likely causes. These conditions are
Potential Causes of Sudden Cardiac Arrest in Children Project S.A.V.E. When sudden death occurs in children, adolescents and younger adults, heart abnormalities are likely causes. These conditions are
Atrial Fibrillation and Cardiac Device Therapy RAKESH LATCHAMSETTY, MD DIVISION OF ELECTROPHYSIOLOGY UNIVERSITY OF MICHIGAN HOSPITAL ANN ARBOR, MI
 Atrial Fibrillation and Cardiac Device Therapy RAKESH LATCHAMSETTY, MD DIVISION OF ELECTROPHYSIOLOGY UNIVERSITY OF MICHIGAN HOSPITAL ANN ARBOR, MI Outline Atrial Fibrillation What is it? What are the associated
Atrial Fibrillation and Cardiac Device Therapy RAKESH LATCHAMSETTY, MD DIVISION OF ELECTROPHYSIOLOGY UNIVERSITY OF MICHIGAN HOSPITAL ANN ARBOR, MI Outline Atrial Fibrillation What is it? What are the associated
ACLS Study Guide BLS Overview CAB
 ACLS Study Guide The ACLS Provider exam is 50-mutiple choice questions. Passing score is 84%. Student may miss 8 questions. For students taking ACLS for the first time or renewing students with a current
ACLS Study Guide The ACLS Provider exam is 50-mutiple choice questions. Passing score is 84%. Student may miss 8 questions. For students taking ACLS for the first time or renewing students with a current
Episode 20 Atrial fibrillation Prepared by Dr. Lucas Chartier
 Episode 20 Atrial fibrillation Prepared by Dr. Lucas Chartier Most common dysrhythmia seen in ED, and incidence increasing with ageing population Presentation Common presentations: younger patients often
Episode 20 Atrial fibrillation Prepared by Dr. Lucas Chartier Most common dysrhythmia seen in ED, and incidence increasing with ageing population Presentation Common presentations: younger patients often
BASIC CARDIAC ARRHYTHMIAS Revised 10/2001
 BASIC CARDIAC ARRHYTHMIAS Revised 10/2001 A Basic Arrhythmia course is a recommended prerequisite for ACLS. A test will be given that will require you to recognize cardiac arrest rhythms and the most common
BASIC CARDIAC ARRHYTHMIAS Revised 10/2001 A Basic Arrhythmia course is a recommended prerequisite for ACLS. A test will be given that will require you to recognize cardiac arrest rhythms and the most common
ACUTE ATRIAL FIBRILLATION TREATMENT IN THE SURGICAL PATIENT
 DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
Patient Information Sheet Electrophysiological study
 Patient Information Sheet Electrophysiological study Your doctor has recommended performing an electrophysiological study (also called EPS). EPS is a diagnostic procedure designed to test and evaluate
Patient Information Sheet Electrophysiological study Your doctor has recommended performing an electrophysiological study (also called EPS). EPS is a diagnostic procedure designed to test and evaluate
Cardiac Arrhythmias. Introduction. Sinus Rhythms. Premature Beats. Secondary article. John A Kastor, University of Maryland, Baltimore, Maryland, USA
 John A Kastor, University of Maryland, Baltimore, Maryland, USA Cardiac arrhythmias are disturbances in the rhythm of the heart manifested by irregularity or by abnormally fast rates ( tachycardias ) or
John A Kastor, University of Maryland, Baltimore, Maryland, USA Cardiac arrhythmias are disturbances in the rhythm of the heart manifested by irregularity or by abnormally fast rates ( tachycardias ) or
cme: The Emergency Management of Cardiac Arrhythmia
 cme: The Emergency Management of Cardiac Arrhythmia Thorsten Lewalter, Lars Lickfett, Jörg O. Schwab, Alexander Yang, Berndt Lüderitz SUMMARY Introduction: The treatment of acute arrhythmias requires quick
cme: The Emergency Management of Cardiac Arrhythmia Thorsten Lewalter, Lars Lickfett, Jörg O. Schwab, Alexander Yang, Berndt Lüderitz SUMMARY Introduction: The treatment of acute arrhythmias requires quick
Tachyarrhythmias in the ICU
 Tachyarrhythmias in the ICU ACNP/PA Critical Care Boot Camp Vanderbilt University Medical Center September 21, 2015 Ariel Kappa RN, MSN, ACNP-BC Acute Arrhythmias are the gremlins of the ICU because they
Tachyarrhythmias in the ICU ACNP/PA Critical Care Boot Camp Vanderbilt University Medical Center September 21, 2015 Ariel Kappa RN, MSN, ACNP-BC Acute Arrhythmias are the gremlins of the ICU because they
These guidelines have been withdrawn
 These guidelines have been withdrawn MOH clinical practice guidelines are considered withdrawn five years after publication unless otherwise specified in individual guidelines. Users should keep in mind
These guidelines have been withdrawn MOH clinical practice guidelines are considered withdrawn five years after publication unless otherwise specified in individual guidelines. Users should keep in mind
The Emerging Atrial Fibrillation Epidemic: Treat It, Leave It or Burn It?
 The Emerging Atrial Fibrillation Epidemic: Treat It, Leave It or Burn It? Indiana Chapter-ACC 17 th Annual Meeting Indianapolis, Indiana October 19, 2013 Deepak Bhakta MD FACC FACP FAHA FHRS CCDS Associate
The Emerging Atrial Fibrillation Epidemic: Treat It, Leave It or Burn It? Indiana Chapter-ACC 17 th Annual Meeting Indianapolis, Indiana October 19, 2013 Deepak Bhakta MD FACC FACP FAHA FHRS CCDS Associate
INTRODUCTORY GUIDE TO IDENTIFYING ECG IRREGULARITIES
 INTRODUCTORY GUIDE TO IDENTIFYING ECG IRREGULARITIES NOTICE: This is an introductory guide for a user to understand basic ECG tracings and parameters. The guide will allow user to identify some of the
INTRODUCTORY GUIDE TO IDENTIFYING ECG IRREGULARITIES NOTICE: This is an introductory guide for a user to understand basic ECG tracings and parameters. The guide will allow user to identify some of the
NEW ONSET ATRIAL FIBRILLATION IN THE SURGICAL PATIENT
 DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
Atrial Fibrillation 2014 How to Treat How to Anticoagulate. Allan Anderson, MD, FACC, FAHA Division of Cardiology
 Atrial Fibrillation 2014 How to Treat How to Anticoagulate Allan Anderson, MD, FACC, FAHA Division of Cardiology Projection for Prevalence of Atrial Fibrillation: 5.6 Million by 2050 Projected number of
Atrial Fibrillation 2014 How to Treat How to Anticoagulate Allan Anderson, MD, FACC, FAHA Division of Cardiology Projection for Prevalence of Atrial Fibrillation: 5.6 Million by 2050 Projected number of
Addendum to the Guideline on antiarrhythmics on atrial fibrillation and atrial flutter
 22 July 2010 EMA/CHMP/EWP/213056/2010 Addendum to the Guideline on antiarrhythmics on atrial fibrillation and atrial flutter Draft Agreed by Efficacy Working Party July 2008 Adoption by CHMP for release
22 July 2010 EMA/CHMP/EWP/213056/2010 Addendum to the Guideline on antiarrhythmics on atrial fibrillation and atrial flutter Draft Agreed by Efficacy Working Party July 2008 Adoption by CHMP for release
Adult Drug Reference. Dopamine Drip Chart. Pediatric Drug Reference. Pediatric Drug Dosage Charts DRUG REFERENCES
 Adult Drug Reference Dopamine Drip Chart Pediatric Drug Reference Pediatric Drug Dosage Charts DRUG REFERENCES ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments ADENOSINE Paroxysmal
Adult Drug Reference Dopamine Drip Chart Pediatric Drug Reference Pediatric Drug Dosage Charts DRUG REFERENCES ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments ADENOSINE Paroxysmal
Atrial Fibrillation Centre
 About this guide We have prepared this guide to help you to: learn about atrial fibrillation manage atrial fibrillation and reduce the risk of stroke find out about medicines and other treatment options
About this guide We have prepared this guide to help you to: learn about atrial fibrillation manage atrial fibrillation and reduce the risk of stroke find out about medicines and other treatment options
table of contents drug reference
 table of contents drug reference ADULT DRUG REFERENCE...155 161 PEDIATRIC DRUG REFERENCE...162 164 PEDIATRIC WEIGHT-BASED DOSING CHARTS...165 180 Adenosine...165 Amiodarone...166 Atropine...167 Defibrillation...168
table of contents drug reference ADULT DRUG REFERENCE...155 161 PEDIATRIC DRUG REFERENCE...162 164 PEDIATRIC WEIGHT-BASED DOSING CHARTS...165 180 Adenosine...165 Amiodarone...166 Atropine...167 Defibrillation...168
Adding IV Amiodarone to the EMS Algorithm for Cardiac Arrest Due to VF/Pulseless VT
 Adding IV Amiodarone to the EMS Algorithm for Cardiac Arrest Due to VF/Pulseless VT Introduction Before the year 2000, the traditional antiarrhythmic agents (lidocaine, bretylium, magnesium sulfate, procainamide,
Adding IV Amiodarone to the EMS Algorithm for Cardiac Arrest Due to VF/Pulseless VT Introduction Before the year 2000, the traditional antiarrhythmic agents (lidocaine, bretylium, magnesium sulfate, procainamide,
Unrestricted grant Boehringer Ingelheim
 ED Management of Recent Onset tat Atrial Fibrillation and Flutter (RAFF) Canadian Cardiovascular Society Guidelines 2010 CAEP St John s 2011 Ian Stiell MD MSc FRCPC Professor and Chair, Dept of Emergency
ED Management of Recent Onset tat Atrial Fibrillation and Flutter (RAFF) Canadian Cardiovascular Society Guidelines 2010 CAEP St John s 2011 Ian Stiell MD MSc FRCPC Professor and Chair, Dept of Emergency
Managing the Patient with Atrial Fibrillation
 Pocket Guide Managing the Patient with Atrial Fibrillation Updated April 2012 Editor Stephen R. Shorofsky, MD, Ph.D. Assistant Editors Anastasios Saliaris, MD Shawn Robinson, MD www.hrsonline.org DEFINITION
Pocket Guide Managing the Patient with Atrial Fibrillation Updated April 2012 Editor Stephen R. Shorofsky, MD, Ph.D. Assistant Editors Anastasios Saliaris, MD Shawn Robinson, MD www.hrsonline.org DEFINITION
ACCIDENT AND EMERGENCY DEPARTMENT/CARDIOLOGY
 Care Pathway Triage category ATRIAL FIBRILLATION PATHWAY ACCIDENT AND EMERGENCY DEPARTMENT/CARDIOLOGY AF/ FLUTTER IS PRIMARY REASON FOR PRESENTATION YES NO ONSET SYMPTOMS OF AF./../ TIME DURATION OF AF
Care Pathway Triage category ATRIAL FIBRILLATION PATHWAY ACCIDENT AND EMERGENCY DEPARTMENT/CARDIOLOGY AF/ FLUTTER IS PRIMARY REASON FOR PRESENTATION YES NO ONSET SYMPTOMS OF AF./../ TIME DURATION OF AF
What Are Arrhythmias?
 What Are Arrhythmias? Many people have questions about what the word arrhythmia means, and arrhythmias can be a difficult subject to understand. The text below should give you a better understanding of
What Are Arrhythmias? Many people have questions about what the word arrhythmia means, and arrhythmias can be a difficult subject to understand. The text below should give you a better understanding of
How To Understand What You Know
 Heart Disorders Glossary ABG (Arterial Blood Gas) Test: A test that measures how much oxygen and carbon dioxide are in the blood. Anemia: A condition in which there are low levels of red blood cells in
Heart Disorders Glossary ABG (Arterial Blood Gas) Test: A test that measures how much oxygen and carbon dioxide are in the blood. Anemia: A condition in which there are low levels of red blood cells in
Essential facts for med-surg nurses
 Emergency cardiac drugs: Essential facts for med-surg nurses Emergencies on a med-surg unit can be daunting. By Ira Gene Reynolds, MSNEd, RN, PCCN-CMC IN THE HOSPITAL SETTING, emergencies typically occur
Emergency cardiac drugs: Essential facts for med-surg nurses Emergencies on a med-surg unit can be daunting. By Ira Gene Reynolds, MSNEd, RN, PCCN-CMC IN THE HOSPITAL SETTING, emergencies typically occur
Atrial Fibrillation Based on ESC Guidelines. Moshe Swissa MD Kaplan Medical Center
 Atrial Fibrillation Based on ESC Guidelines Moshe Swissa MD Kaplan Medical Center Epidemiology AF affects 1 2% of the population, and this figure is likely to increase in the next 50 years. AF may long
Atrial Fibrillation Based on ESC Guidelines Moshe Swissa MD Kaplan Medical Center Epidemiology AF affects 1 2% of the population, and this figure is likely to increase in the next 50 years. AF may long
ACLS Rhythms for the ACLS Algorithms
 ACLS Rhythms for the ACLS Algorithms The Basics 1. Anatomy of the cardiac conduction system: relationship to the ECG cardiac cycle. A, Heart: anatomy of conduction system. B, P-QRS-T complex: lines to
ACLS Rhythms for the ACLS Algorithms The Basics 1. Anatomy of the cardiac conduction system: relationship to the ECG cardiac cycle. A, Heart: anatomy of conduction system. B, P-QRS-T complex: lines to
RATE VERSUS RHYTHM CONTROL OF ATRIAL FIBRILLATION: SPECIAL CONSIDERATION IN ELDERLY. Charles Jazra
 RATE VERSUS RHYTHM CONTROL OF ATRIAL FIBRILLATION: SPECIAL CONSIDERATION IN ELDERLY Charles Jazra NO CONFLICT OF INTEREST TO DECLARE Relationship Between Atrial Fibrillation and Age Prevalence, percent
RATE VERSUS RHYTHM CONTROL OF ATRIAL FIBRILLATION: SPECIAL CONSIDERATION IN ELDERLY Charles Jazra NO CONFLICT OF INTEREST TO DECLARE Relationship Between Atrial Fibrillation and Age Prevalence, percent
Atrial Fibrillation (AF) March, 2013
 March, 2013") Atrial Fibrillation (AF) March, 2013 This handout is meant to help with discussions about the condition, and it is not a complete discussion of AF. We hope it will complement your appointment with one
Atrial Fibrillation (AF) March, 2013 This handout is meant to help with discussions about the condition, and it is not a complete discussion of AF. We hope it will complement your appointment with one
Atrial Fibrillation Cardiac rate control or rhythm control could be the key to AF therapy
 Cardiac rate control or rhythm control could be the key to AF therapy Recent studies have proven that an option of pharmacologic and non-pharmacologic therapy is available to patients who suffer from AF.
Cardiac rate control or rhythm control could be the key to AF therapy Recent studies have proven that an option of pharmacologic and non-pharmacologic therapy is available to patients who suffer from AF.
ATRIAL FIBRILLATION AND ANAESTHESIA
 ATRIAL FIBRILLATION AND ANAESTHESIA Dr AD Theron, SHO in Anaesthesia, Royal Devon and Exeter Hospital, Exeter, UK. E-mail: drabrietheron@yahoo.co.uk Atrial fibrillation (AF) is one of the commonest arrhythmias.
ATRIAL FIBRILLATION AND ANAESTHESIA Dr AD Theron, SHO in Anaesthesia, Royal Devon and Exeter Hospital, Exeter, UK. E-mail: drabrietheron@yahoo.co.uk Atrial fibrillation (AF) is one of the commonest arrhythmias.
Atrial Fibrillation: The heart of the matter
 Atrial Fibrillation: The heart of the matter This booklet has been written especially for people with atrial fibrillation (AF), a heart condition often described as an irregular heartbeat (also known
Atrial Fibrillation: The heart of the matter This booklet has been written especially for people with atrial fibrillation (AF), a heart condition often described as an irregular heartbeat (also known
www.cprtrainingfast.com
 ADVANCED CARDIAC LIFE SUPPORT (ACLS) RECERTIFICATION EXAMINATION 1. Ten minutes after an 85 year old woman collapses, paramedics arrive and start CPR for the first time. The monitor shows fine (low amplitude)
ADVANCED CARDIAC LIFE SUPPORT (ACLS) RECERTIFICATION EXAMINATION 1. Ten minutes after an 85 year old woman collapses, paramedics arrive and start CPR for the first time. The monitor shows fine (low amplitude)
Efficacy and Safety of Pharmacological Options for Rate Control in Atrial Fibrillation
 AACN Advanced Critical Care Volume 23, Number 2, pp.120 125 2012, AACN ECG Challenges Earnest Alexander, PharmD, and Gregory M. Susla, PharmD Department Editors Efficacy and Safety of Pharmacological Options
AACN Advanced Critical Care Volume 23, Number 2, pp.120 125 2012, AACN ECG Challenges Earnest Alexander, PharmD, and Gregory M. Susla, PharmD Department Editors Efficacy and Safety of Pharmacological Options
ACLS RHYTHM TEST. 2. A 74-year-old woman with chest pain. Blood pressure 192/90 and rates her pain 9/10.
 ACLS RHYTHM TEST Name Date Choose the best answer for each of the following questions. Each of the following strips is 6 seconds in length. 1. Identify the following rhythm a. Sinus bradycardia with 2
ACLS RHYTHM TEST Name Date Choose the best answer for each of the following questions. Each of the following strips is 6 seconds in length. 1. Identify the following rhythm a. Sinus bradycardia with 2
How to control atrial fibrillation in 2013 The ideal patient for a rate control strategy
 How to control atrial fibrillation in 2013 The ideal patient for a rate control strategy L. Pison, MD Advances in Cardiac Arrhythmias and Great Innovations in Cardiology - Torino, September 28 th 2013
How to control atrial fibrillation in 2013 The ideal patient for a rate control strategy L. Pison, MD Advances in Cardiac Arrhythmias and Great Innovations in Cardiology - Torino, September 28 th 2013
Advanced Cardiovascular Life Support Case Scenarios
 Advanced Cardiovascular Life Support Case Scenarios ACLS Respiratory Arrest Case Out-of-Hospital Scenario You are a paramedic and respond to the scene of a possible cardiac arrest. A young man lies motionless
Advanced Cardiovascular Life Support Case Scenarios ACLS Respiratory Arrest Case Out-of-Hospital Scenario You are a paramedic and respond to the scene of a possible cardiac arrest. A young man lies motionless
E C C. American Heart Association. Advanced Cardiovascular Life Support. Written Exams. May 2011
 E C C American Heart Association Advanced Cardiovascular Life Support Written Exams Contents: Exam Memo Student Answer Sheet Version A Exam Version A Answer Key Version A Reference Sheet Version B Exam
E C C American Heart Association Advanced Cardiovascular Life Support Written Exams Contents: Exam Memo Student Answer Sheet Version A Exam Version A Answer Key Version A Reference Sheet Version B Exam