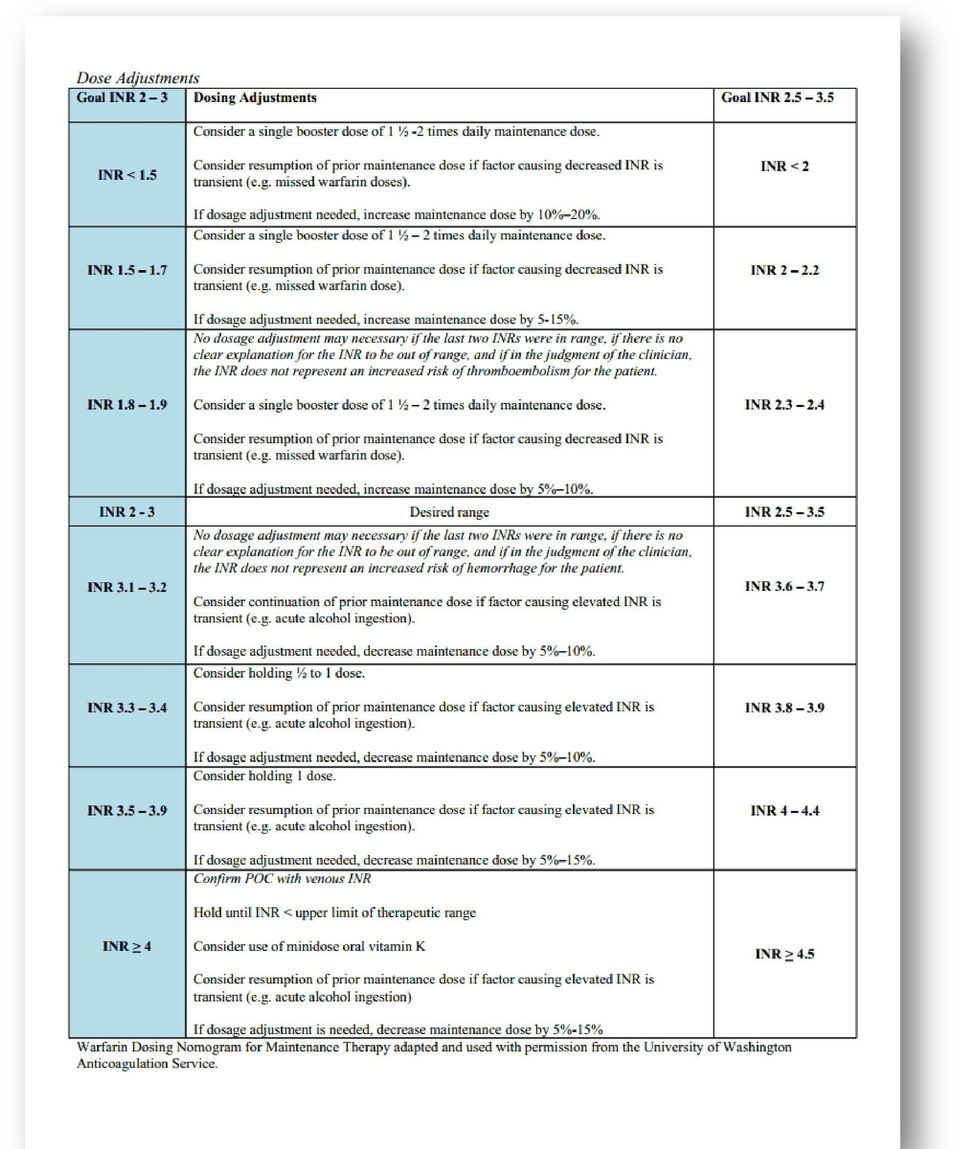
How To Increase Warfarin
|
|
|
- Theresa O’Brien’
- 5 years ago
- Views:
Transcription
1 Anticoagulants for venous thromboembolic disease- Optimizing the old, ushering in the new. Daniel A. Forman, DO RPS Hematology Oncology cell

2 RHS Anticoagulation Clinic Opening in November Doctors office building. 3 rd floor. Patient will need to be referred by a physician with basic information (EPIC). Pharmacy consult on first visit. Twice year visit. You are still in charge! (holding, discontinuation, etc.) Point of care testing available.

3 Goals Discuss ways to improve the safety and more convenient administration of warfarin. Review efficacy and pharmacologic issues associated with the newer oral anticoagulants.

4 Warfarin Basics VII, XI, X, II Protein C & S Inhibits Vitamin K Oxide Reductase ( recycles Vit. K) Lack vitamin K prohibits carboxylation of clotting factors (Inactive clotting factors produced) Genetic factors can predict warfarin sensitivity or resistance VKORC1 genotypes CYP2C9 polymorphism
 Genetic factors can predict warfarin")
5 Warfarin Basics Protein C Anticoagulant 8 hours Protein S Anticoagulant 30 hours Factor VII Procoagulant 7 hours Factor IX Procoagulant 24 hours Factor X Procoagulant 36 hours Factor II Procoagulant 50 hours All factors need to be suppressed for anticoagulant effect (takes two days after INR therapeutic)!

6 Avoid loading doses. INR reflective of rapid decline in factor VII. Confounds the patient s real dose.

7 Warfarin Dosing African-American mg/d European - mean ~ 5 mg/d Asian - lower ~ mg/d Obese 14%/S.D. Age 13%/decade Drugs (100 s interactions) Ex. Amiodarone 24% ~ mg/d Asian - lower ~ mg/d
 Ex.")
8 You are treating a 55 y.o. black male presenting with an acute L. lower extremity DVT with IV Heparin, and warfarin that was started on his first hospital day. His dose of warfarin is 5 mg daily. His day 3 INR was 1.0. What is the next best action? A. Stop IV Heparin, start LMWH at therapeutic dosing. Continue warfarin 5 mg daily. B. Change to LMWH as above; but increase warfarin 10 mg daily. C. Continue IV Heparin. Continue warfarin 5 mg daily. D. Continue IV Heparin. Increase warfarin 10 mg daily.

9 Newly diagnosed VTE disease case: If the INR = 1.0 on Day 3 then double starting dose. LMWH is better than UFH for VTE Disease! No lab testing, Less risk HIT, more clot regression, lower recurrence, lower bleeding, less deaths One study reported 60% patient on UFH failed to achieve adequate aptt response in 24 hours. ACCP 2B recommendation. Arch Intern Med 1988; 148:1321 Chest 2012; 141: e495s

10 Patient is a 50 y.o. male with a mechanic AVR and atrial fibrillation with a difficult to control INR. The patient s time in the therapeutic range is less than 40 %. His INR today is 5.0, last week it was 1.5. His dose was changed last week from 5 mg daily to 5 mg alternating with 7.5 mg. The patient has seen a dietician and said that he does not eat any vitamin k containing foods. Which of the following is the most reasonable advice? A. Stop warfarin and start dabigatran (Pradaxa) 150 mg bid. B. Continue warfarin at the current dose and recheck the INR in 4 weeks. C. Stop warfarin and start aspirin therapy. D. Start low dose daily vitamin K.
 150 mg bid. B. Continue warfarin at the current dose and recheck the INR in 4 weeks. C. Stop warfarin and start aspirin therapy.")
11 Low dose vitamin k for erratic patients Multiple studies have suggested that daily low dose vitamin k improves INR control Mcg day Increasing dietary intake of vitamin K may suffice Not recommended for routine use. Chest 2012;141:e44S-e88S

12 Patient is a 70 year old man on warfarin for recurrent DVT. The first DVT was 15 years ago after surgery, and the second one was idiopathic and occurred 3 years ago. The patient s INR has been at goal on 5 mg daily. You received a call that his most recent INR is 1.5. The patient is feeling fine, just got back from a cruise, and reports no health changes. What is the next best action? A. Start enoxaparin 1mg/kg SQ Q12 hours and increase dose of warfarin to 7.5mg. B. Increase dose of warfarin to 6mg daily. C. Continue same dose warfarin and repeat INR in two weeks. D. Send the patient to the ER for a stat INR.

13 INR out of range?? Stable patients with single outlier INR will often fall back into therapeutic range at time of recheck with NO adjustment (60% time) Guidelines support rechecking 1-2 weeks at same dose (2C) One Observational study suggests only adjusting warfarin dose if INR is less than 1.7 or greater than 3.3. Schuman et al Throm Res 2010; 125:393 Rose et al J Throm Haemost 2009; 7:94 Chest 2012; 141S: e44

14
15 Next patient is a 42 year old female with multiple dvt s, a second trimester miscarriage, and laboratory confirmed Anti-phospholipid Antibody Syndrome (APAS). She has to leave work early for INR testing and it is causing conflict with her employer. Her INR s have been therapeutic for 6 months on 3 mg alternating with 4mg warfarin every other day. Which of the following is the best approach for this patient? A. Change to dabigatran 150mg po bid. B. Change to aspirin 81mg daily. C. Change to enoxaparin 1.5 mg/kg/day. D. Check the INR every 3 months.

16 Give your patient a break! PRINT Study- Randomized Controlled Trial, Concluded: Stable patients can have INR s performed every 12 weeks. Less dose change (2% vs. 18%) no increased bleeding. Accepted by CHEST guidelines (2B). Not for Everyone (CHF, New Disease Development, etc). Schulman et al Ann Intern Med 2011; 155:653-9
 no increased bleeding. Accepted by CHEST guidelines (2B).")
17 What is the best way to determine a patient s warfarin dose if he was previously on this medication? A. Genetic testing for VKOR1 polymorphisms. B. Genetic testing for Cytochrome P450 CYP2C9 polymorphisms. C. Dose based upon age, weight, and sex. D. Find out his/her previous dose.

18 You receive a call from the lab with an INR of 8.6. You call the 70 y.o. patient with PAF and HTN, and he has no bleeding symptoms. He just started ciprofloxin last week for sinusitis given to him by a provider at an urgent care clinic. What is the risk of major bleeding in this patient over the next month? A. 1% B. 5% C. 10% D. 20%

19 Supratherapeutic INR s Risk of major bleeding is low (1%) when single INR 5-9. Spurious INR suspected if doesn t make sense. Bleeding risk scoring systems for warfarin are not better than clinicians judgment. Donzé J et al. Am J Med 2012; 125:1095 Ageno et al. Chest 2012; 141S: e44

20 Reversing warfarin without bleeding Wait it out: INR will fall from 6-10 to < 4 in 2.4 days. Vitamin K1 (phytonadione) given orally takes about 1.4 days to bring INR 6-10 to <4. Follow CHEST Guidelines Ageno et al Chest 2012; 141S: e44

21 Rapid Correction of warfarin in an unstable patient or ICH Vitamin K1 10 mg iv FFP 15ml/kg (4-8 units) Prothrombin Complex Concentrates 3 Factor (II, IX, X) & 4 Factor (II, VII, IX, X) Effective, but thrombogenic Recommended over FFP by ACCP guidelines. rfactor VIIa- Not FDA approved for reversal Lawrence and Shander Blood 2011; 1182
22 Your patient is a 50 y.o. male who presented 6 months ago with syncope due to an idiopathic PE. He is afraid of dying and does not want to stop warfarin, but he is an international traveler and is concerned about work related travel due to his INR testing. His INR s have not been stable. He takes no other medications. What is the best option for this patient? A. Stop warfarin and recommend aspirin. B. Check INR every 3 months. C. Change to LMWH. D. Change to Rivaroxaban 20 mg daily.
23 Idiopathic Clot Risk of recurrence 10% per year ( 50% long term) New paradigm and recommendations are to continue indefinite therapy for idiopathic proximal DVT and PE (ACCP 2B) Big Picture: First 3 months: Vigilant therapeutic anticoagulation After 3 months treatment is prophylactic
24 Ideal anticoagulant Safe and effective Rapid acting Available p.o. and parenteral Rapid elimination Free of drug interactions Predictable effect and wide therapeutic window No need for monitoring Minimal toxicity and side effects Reversible with an antidote
25 Warfarin VS. Newer Rxs Features Warfarin Newer Agents Onset Slow (days) Rapid Dosing Variable Fixed Half life Long Short Food effects Yes No Drug Interactions Many Few Monitoring Yes No Antidote Yes No (but short ½ life) Cost Low High
26 Newer Anticoagulants FDA Approval Drug Dabigatran (Pradaxa) Prophylaxis (ortho) A. Fib ACUTE DVT Prolonged treatment DVT/PE x Rivaroxaban (Xarelto) x x x x Apixaban (Eliquis) X x Edoxaban
27
28 Drug CYP 3A4 P-gp Dabigatran (Pradaxa) Rivaroxaban (Xarelto) Apixaban (Eliquis) Yes Yes Yes Yes
29 Dabigatran (Pradaxa) Direct thrombin inhibitor Renal excretion Not for use with mechanical heart valves (increase CVA and bleeding) NEJM 2013; 369:1206 Slight increase for CAD (0.2%) Circulation 2012; 125:669 Dyspepsia
30 Rivaroxaban (Xarelto) Once daily with food (BID for acute VTE x 3wk) Avoid with medications that affect both the P-gp and Cytochrome P450 3A4. Cyp3A4 inhibitors: (HIV protease inhibitors, ketoconazole, voriconazole) CYP3A4 inducers: (Rifampin, carbamazepine, or phenytoin) No need for overlapping parenteral Tx (ex. LMWH)
31 Patient is a 57 y.o. male school teacher recently diagnosed with AIDS while admitted for an acute PE. Which of the following is correct? A. HIV/AIDS is not a risk factor for VTE disease. B. Intravenous unfractionated heparin is preferred in HIV patients with acute VTE disease. C. Rivaroxaban is contraindicated in patient on protease inhibitor therapy due to CYP3A inhibition.
32 Rivaroxaban (Xarelto) vs. Warfarin for acute PE Symptomatic PE +/- DVT Excluded: Cr clearance < 30, Liver disease, SBP <110 or >180, drugs that affect CYP 3A4 Average age 57 10% treated outpatient 12% ICU Conclusion: Rivaroxaban is non-inferior with similar bleeding risk (less major bleeding) N Engl J Med 2012; 366:
33 Apixaban (Eliquis) Twice daily Less bleeding? AMPLIFY Major bleeding or clinically relevant for acute DVT/PE 4.3% vs. 9.7% (warfarin) AMPLIFY EXT for continued therapy after 6-12 months no higher bleeding then placebo. Risk of DVT 12 mo. 1.7% 2.5mg, 1.7% 5mg, and 8% placebo Risk of Death 12mo 3.8%, 4.2%, 11.6% N Engl J Med 2013; 368:699-70
34 Edoxaban Once daily (60mg) 30mg/d. Cr.Cl or weight less than 60kg. Approx. 10% < 60 kg Approx. 10% > 75 y.o. More effective than warfarin in patients with high risk PE. (RV enlargement, elevated BNP). N Engl J Med 2013; 369:
35 Bleeding Patients Supportive measures Last dose? Renal or hepatic dysfunction? Other anticoagulants? If PT normal, unlikely any effect of rivaroxaban. If PTT is normal, unlikely any effect of dabigatran. Oral Anticoagulants: The old and the new. 2012; American Society of Hematology Webinar King et al Chest 2013; 143;:1362
36 Control of bleeding Modality Dabigatran Rivaroxaban Apixaban Charcoal X X X Hemodialysis X Prothrombin Complex Concentrates X X avii??? King et al Chest 2013; 143: 1362 Gonsalves et al Mayo Clin Proc. 2013; 88: 495
37 Future is here: 59 y.o. female with breast cancer. Oct 24 th, 2013 Hi Dr. Dan, I bet you thought I died or something. Just got back from the Italy trip on Monday night - had a wonderful time. Didn't think that I was going to be able to go. About a month ago, I had such bad chest pain that I thought I was having a heart attack - turned out to be a blood clot on my lung. Was in the hospital for a week until they got my INR levels correct. Now I am on Warfarin. Oct 25 th, 2013 Dr. Dan, Just had a chemo. treatment today and they checked my pro-time levels must have been all that wine I drank in Italy. Dr. Latif told me not to take my warfarin tonight and also tomorrow night, but I am to resume on Sunday, but only 5 mg. not the 7.5 mg s- present Future One week in the hospital Numerous tests Exposure to sick patients Discharged on therapeutic warfarin Outpatient labs, risk of over and under dosing. Missed work, bills, etc. Start rivoroxaban BID for three weeks then daily. Discharge from the ED or hospital the next day.
38 Newer Oral Anticoagulants:
39 Mayo Clinic Proceedings: Wilson I. Gonsalves, MD, et al. Volume 88, Issue 5, Pages , May 2013 The New Oral Anticoagulants in Clinical Practice /PIIS X/fulltext Good Review on the newer anticoagulants Pragmatic advice about how long to hold these agents prior to surgery, changing to warfarin while on these agents, etc.
40 Summary Try to avoid unnecessary adjustments when managing warfarin. Stable patients on warfarin need less frequent testing. The newer agents appear to be well tolerated with similar, or less bleeding risk. Be careful with potential serious drug interactions, and watch organ function with the newer agents.
41 Questions?
Hypercoagulable States
 Hypercoagulable States Daniel A. Forman, DO [email protected] 610 509 5067 April 26, 2014 Risk Factors for Venous Thromboembolism (VTE) Hereditary thrombophilias How long to treat Newer agents
Hypercoagulable States Daniel A. Forman, DO [email protected] 610 509 5067 April 26, 2014 Risk Factors for Venous Thromboembolism (VTE) Hereditary thrombophilias How long to treat Newer agents
Venous Thromboembolism: Long Term Anticoagulation. Dan Johnson, Pharm.D.
 Venous Thromboembolism: Long Term Anticoagulation Dan Johnson, Pharm.D. Disclosures No financial relationships with products discussed Off-label use of drug therapy always discussed Objectives Review clinical
Venous Thromboembolism: Long Term Anticoagulation Dan Johnson, Pharm.D. Disclosures No financial relationships with products discussed Off-label use of drug therapy always discussed Objectives Review clinical
DVT/PE Management with Rivaroxaban (Xarelto)
") DVT/PE Management with Rivaroxaban (Xarelto) Rivaroxaban is FDA approved for the acute treatment of DVT and PE and reduction in risk of recurrence of DVT and PE. FDA approved indications: Non valvular
DVT/PE Management with Rivaroxaban (Xarelto) Rivaroxaban is FDA approved for the acute treatment of DVT and PE and reduction in risk of recurrence of DVT and PE. FDA approved indications: Non valvular
New Anticoagulants: When and Why Should I Use Them? Disclosures
 Winship Cancer Institute of Emory University New Anticoagulants: When and Why Should I Use Them? Christine L. Kempton, MD, MSc Associate Professor of Pediatrics and Hematology and Medical Oncology Hemophilia
Winship Cancer Institute of Emory University New Anticoagulants: When and Why Should I Use Them? Christine L. Kempton, MD, MSc Associate Professor of Pediatrics and Hematology and Medical Oncology Hemophilia
Traditional anticoagulants
 TEGH Family Practice Clinic Day April 4, 03 Use of Anticoagulants in 03: What s New (and What Isn t) Bill Geerts, MD, FRCPC Director, Thromboembolism Program, Sunnybrook HSC Professor of Medicine, University
TEGH Family Practice Clinic Day April 4, 03 Use of Anticoagulants in 03: What s New (and What Isn t) Bill Geerts, MD, FRCPC Director, Thromboembolism Program, Sunnybrook HSC Professor of Medicine, University
Objectives. New and Emerging Anticoagulants. Objectives (continued) 2/18/2014. Development of New Anticoagulants
 2/18/2014. Development of New Anticoagulants") Objectives New and Emerging Anticoagulants Adraine Lyles, PharmD, BCPS Clinical Pharmacy Specialist VCU Medical Center Describe the pharmacology of the novel oral anticoagulants Discuss the clinical evidence
Objectives New and Emerging Anticoagulants Adraine Lyles, PharmD, BCPS Clinical Pharmacy Specialist VCU Medical Center Describe the pharmacology of the novel oral anticoagulants Discuss the clinical evidence
New Oral Anticoagulants. How safe are they outside the trials?
 New Oral Anticoagulants How safe are they outside the trials? Objectives The need for anticoagulant therapy Indications for anticoagulation Traditional anticoagulant therapies Properties of new oral anticoagulants
New Oral Anticoagulants How safe are they outside the trials? Objectives The need for anticoagulant therapy Indications for anticoagulation Traditional anticoagulant therapies Properties of new oral anticoagulants
Management for Deep Vein Thrombosis and New Agents
 Management for Deep Vein Thrombosis and New Agents Mark Malesker, Pharm.D., FCCP, FCCP, FASHP, BCPS Professor of Pharmacy Practice and Medicine Creighton University 5 th Annual Creighton Cardiovascular
Management for Deep Vein Thrombosis and New Agents Mark Malesker, Pharm.D., FCCP, FCCP, FASHP, BCPS Professor of Pharmacy Practice and Medicine Creighton University 5 th Annual Creighton Cardiovascular
Anticoagulation at the end of life. Rhona Maclean [email protected]
 Anticoagulation at the end of life Rhona Maclean [email protected] Content Anticoagulant Therapies Indications for anticoagulation Venous thromboembolism (VTE) Atrial Fibrillation Mechnical Heart
Anticoagulation at the end of life Rhona Maclean [email protected] Content Anticoagulant Therapies Indications for anticoagulation Venous thromboembolism (VTE) Atrial Fibrillation Mechnical Heart
TSOAC Initiation Checklist
 Task Establish appropriate dose based on anticoagulant selected, indication and patient factors such as renal function. Evaluate for medication interactions that may necessitate TSOAC dose adjustment.
Task Establish appropriate dose based on anticoagulant selected, indication and patient factors such as renal function. Evaluate for medication interactions that may necessitate TSOAC dose adjustment.
Analyzing Clinical Trial Findings of the Efficacy and Safety Profiles of Novel Anticoagulants for Stroke Prevention in Atrial Fibrillation
 Analyzing Clinical Trial Findings of the Efficacy and Safety Profiles of Novel Anticoagulants for Stroke Prevention in Atrial Fibrillation Drew Baldwin, MD Virginia Mason Seattle, Washington NCVH May 29,
Analyzing Clinical Trial Findings of the Efficacy and Safety Profiles of Novel Anticoagulants for Stroke Prevention in Atrial Fibrillation Drew Baldwin, MD Virginia Mason Seattle, Washington NCVH May 29,
3/25/14. To Clot or Not What s New In Anticoagulation? Clotting Cascade. Anticoagulant drug targets. Anita Ralstin, MS CNS CNP. Heparin.
 To Clot or Not What s New In Anticoagulation? Anita Ralstin, MS CNS CNP 1 Clotting Cascade 2 Anticoagulant drug targets Heparin XI VIII IX V X VII LMWH II Warfarin Fibrin clot 1 Who Needs Anticoagulation
To Clot or Not What s New In Anticoagulation? Anita Ralstin, MS CNS CNP 1 Clotting Cascade 2 Anticoagulant drug targets Heparin XI VIII IX V X VII LMWH II Warfarin Fibrin clot 1 Who Needs Anticoagulation
The speakers have attested that their presentation will be free of all commercial bias toward a specific company and its products.
 Update on New Anticoagulants (Apixaban, Dabigatran and Rivaroxaban) Patient Safety Daniel B. DiCola, MD and Paul Ament,, Pharm.D Excela Heath, Latrobe, PA Disclosures: Paul Ament discloses that he receives
Update on New Anticoagulants (Apixaban, Dabigatran and Rivaroxaban) Patient Safety Daniel B. DiCola, MD and Paul Ament,, Pharm.D Excela Heath, Latrobe, PA Disclosures: Paul Ament discloses that he receives
New Oral Anticoagulants
 New Oral Anticoagulants Tracy Minichiello, MD Associate Professor of Medicine Chief, San FranciscoVA Anticoagulation and Thrombosis Service Ansell, J. Hematology Copyright 2010 American Society of Hematology.
New Oral Anticoagulants Tracy Minichiello, MD Associate Professor of Medicine Chief, San FranciscoVA Anticoagulation and Thrombosis Service Ansell, J. Hematology Copyright 2010 American Society of Hematology.
FDA Approved Oral Anticoagulants
 FDA Approved Oral Anticoagulants Generic (Trade Name) Warfarin (Coumadin, Jantoven ) 1 FDA approved indication Prophylaxis and treatment of venous thromboembolism (VTE) Prophylaxis and treatment of thromboembolic
FDA Approved Oral Anticoagulants Generic (Trade Name) Warfarin (Coumadin, Jantoven ) 1 FDA approved indication Prophylaxis and treatment of venous thromboembolism (VTE) Prophylaxis and treatment of thromboembolic
New Anticoagulants: What to Use What to Avoid
 New Anticoagulants: What to Use What to Avoid Bruce Davidson, MD, MPH Clinical Professor of Medicine Pulmonary and Critical Care Medicine Division University of Washington School of Medicine Seattle USA
New Anticoagulants: What to Use What to Avoid Bruce Davidson, MD, MPH Clinical Professor of Medicine Pulmonary and Critical Care Medicine Division University of Washington School of Medicine Seattle USA
The Role of the Newer Anticoagulants
 The Role of the Newer Anticoagulants WARFARIN = Coumadin DAGIBATRAN = Pradaxa RIVAROXABAN = Xarelto APIXABAN = Eliquis INDICATION DABIGATRAN (Pradaxa) RIVAROXABAN (Xarelto) APIXABAN (Eliquis) Stroke prevention
The Role of the Newer Anticoagulants WARFARIN = Coumadin DAGIBATRAN = Pradaxa RIVAROXABAN = Xarelto APIXABAN = Eliquis INDICATION DABIGATRAN (Pradaxa) RIVAROXABAN (Xarelto) APIXABAN (Eliquis) Stroke prevention
Time of Offset of Action The Trial
 New Antithrombotic Agents DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant Amgen Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University What I am Talking About
New Antithrombotic Agents DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant Amgen Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University What I am Talking About
5/21/2012. Perioperative Use Issues. On admission: During hospitalization:
 Dabigatran and Rivaroxaban: Challenges in the Perioperative Setting Claudia Swenson, Pharm.D., CDE, BC-ADM, FASHP Central Washington Hospital Wenatchee, WA [email protected] Dabigatran and Rivaroxaban:
Dabigatran and Rivaroxaban: Challenges in the Perioperative Setting Claudia Swenson, Pharm.D., CDE, BC-ADM, FASHP Central Washington Hospital Wenatchee, WA [email protected] Dabigatran and Rivaroxaban:
Speaker Disclosure. Outline. Pharmacist Objectives. Patient Case. Outline 9/4/2014
 Speaker Disclosure Matthew K. Pitlick, Pharm.D., BCPS St. Louis College of Pharmacy/VA St. Louis HCS [email protected] Matthew K. Pitlick, Pharm.D., BCPS declares no conflicts of interest, real or apparent,
Speaker Disclosure Matthew K. Pitlick, Pharm.D., BCPS St. Louis College of Pharmacy/VA St. Louis HCS [email protected] Matthew K. Pitlick, Pharm.D., BCPS declares no conflicts of interest, real or apparent,
Thrombosis and Hemostasis
 Thrombosis and Hemostasis Wendy Lim, MD, MSc, FRCPC Associate Professor, Department of Medicine McMaster University, Hamilton, ON Overview To review the important developments in venous thromboembolism
Thrombosis and Hemostasis Wendy Lim, MD, MSc, FRCPC Associate Professor, Department of Medicine McMaster University, Hamilton, ON Overview To review the important developments in venous thromboembolism
Devang M. Desai, MD, FACC, FSCAI Chief of Interventional Cardiology Director of Cardiac Catheterization Lab St. Mary s Hospital and Regional Medical
 Devang M. Desai, MD, FACC, FSCAI Chief of Interventional Cardiology Director of Cardiac Catheterization Lab St. Mary s Hospital and Regional Medical Center A.Fib affects 2.2 million Americans. The lifetime
Devang M. Desai, MD, FACC, FSCAI Chief of Interventional Cardiology Director of Cardiac Catheterization Lab St. Mary s Hospital and Regional Medical Center A.Fib affects 2.2 million Americans. The lifetime
Pulmonary Embolism Treatment Update
 UC SF Pulmonary Embolism Treatment Update Jeffrey Tabas, MD Professor UCSF School of Medicine Emergency Department San Francisco General Hospital sf g h Disclosure No Financial Relationships to Disclose
UC SF Pulmonary Embolism Treatment Update Jeffrey Tabas, MD Professor UCSF School of Medicine Emergency Department San Francisco General Hospital sf g h Disclosure No Financial Relationships to Disclose
Disclosure. New Agents for Treatment of DVT. Prevalence of DVT VTE. Normal Hemostasis 7/17/2015. Mark Oliver, MD, RVT, RPVI,FSVU
 New Agents for Treatment of DVT Disclosure PI Adopt and Amplify trials Mark Oliver, MD, RVT, RPVI,FSVU BMS and Pfizer Speaker VTE Venous Thromboembolism Recognized DVT s New : 170,000 Recurrent : 90,000
New Agents for Treatment of DVT Disclosure PI Adopt and Amplify trials Mark Oliver, MD, RVT, RPVI,FSVU BMS and Pfizer Speaker VTE Venous Thromboembolism Recognized DVT s New : 170,000 Recurrent : 90,000
Xabans Good for What Ails Ya? Brian Tiffany, MD, PhD, FACEP Dept of Emergency Medicine Chandler Regional Medical Center Mercy Gilbert Medical Center
 Xabans Good for What Ails Ya? Brian Tiffany, MD, PhD, FACEP Dept of Emergency Medicine Chandler Regional Medical Center Mercy Gilbert Medical Center DISCLOSURES No relevant financial disclosures I will
Xabans Good for What Ails Ya? Brian Tiffany, MD, PhD, FACEP Dept of Emergency Medicine Chandler Regional Medical Center Mercy Gilbert Medical Center DISCLOSURES No relevant financial disclosures I will
New Anticoagulants for the Treatment of Thromboembolism With a little subplot on superficial thrombophlebitis. Mark Crowther
 New Anticoagulants for the Treatment of Thromboembolism With a little subplot on superficial thrombophlebitis Mark Crowther 1 Disclosures Advisory Boards in last 24 months Pfizer, Alexion, Bayer, CSL Behring,
New Anticoagulants for the Treatment of Thromboembolism With a little subplot on superficial thrombophlebitis Mark Crowther 1 Disclosures Advisory Boards in last 24 months Pfizer, Alexion, Bayer, CSL Behring,
Failure or significant adverse effects to all of the alternatives: Eliquis and Xarelto
 This policy has been developed through review of medical literature, consideration of medical necessity, generally accepted medical practice standards, and approved by the IEHP Pharmacy and Therapeutics
This policy has been developed through review of medical literature, consideration of medical necessity, generally accepted medical practice standards, and approved by the IEHP Pharmacy and Therapeutics
48 th Annual Meeting. Non-VKA Oral Anticoagulants: Prevention & Treatment of Bleeding. Terminology. Disclosure. Public Health Impact.
 48 th Annual Meeting Terminology Non-VKA Oral Anticoagulants: Prevention & Treatment of Bleeding Stacy A. Voils, PharmD, MS, BCPS Navigating the Oceans of Opportunity Target-specific oral anticoagulants
48 th Annual Meeting Terminology Non-VKA Oral Anticoagulants: Prevention & Treatment of Bleeding Stacy A. Voils, PharmD, MS, BCPS Navigating the Oceans of Opportunity Target-specific oral anticoagulants
Novel Anticoagulation Agents DISCLOSURES. Objectives ATRIAL FIBRILLATION TRIALS. NOAC Comparison 6/12/2015
 Novel Anticoagulation Agents DISCLOSURES James W. Haynes, MD Department of Family Medicine Univ of TN Health Science Center (Chattanooga) Objectives Understand mechanism of action behind the NOAC agents
Novel Anticoagulation Agents DISCLOSURES James W. Haynes, MD Department of Family Medicine Univ of TN Health Science Center (Chattanooga) Objectives Understand mechanism of action behind the NOAC agents
Dabigatran (Pradaxa) Guidelines
 Guidelines") Dabigatran (Pradaxa) Guidelines Dabigatran is a new anticoagulant for reducing the risk of stroke in patients with atrial fibrillation. Dabigatran is a direct thrombin inhibitor, similar to warfarin, without
Dabigatran (Pradaxa) Guidelines Dabigatran is a new anticoagulant for reducing the risk of stroke in patients with atrial fibrillation. Dabigatran is a direct thrombin inhibitor, similar to warfarin, without
Anticoagulation Essentials! Parenteral and Oral!
 Anticoagulation Essentials! Parenteral and Oral! Anti-Xa and Anti-IIa! Parenteral Anticoagulants! Heparin family (indirect anti-xa and anti-iia):! UFH! LMWH (enoxaparin, fondaparinux)! Direct thrombin
Anticoagulation Essentials! Parenteral and Oral! Anti-Xa and Anti-IIa! Parenteral Anticoagulants! Heparin family (indirect anti-xa and anti-iia):! UFH! LMWH (enoxaparin, fondaparinux)! Direct thrombin
How To Compare The New Oral Anticoagulants
 Disclosures The New Oral Anticoagulants: Are they better than Warfarin? Alan P. Agins, Ph.D. does not have any actual or potential conflicts of interest in relation to this CE activity. Alan Agins, Ph.D.
Disclosures The New Oral Anticoagulants: Are they better than Warfarin? Alan P. Agins, Ph.D. does not have any actual or potential conflicts of interest in relation to this CE activity. Alan Agins, Ph.D.
New Anticoagulation Options for Stroke Prevention in Atrial Fibrillation. Joy Wahawisan, Pharm.D., BCPS April 25, 2012
 New Anticoagulation Options for Stroke Prevention in Atrial Fibrillation Joy Wahawisan, Pharm.D., BCPS April 25, 2012 Stroke in Atrial Fibrillation % Stroke 1991;22:983. Age Range (years) CHADS 2 Risk
New Anticoagulation Options for Stroke Prevention in Atrial Fibrillation Joy Wahawisan, Pharm.D., BCPS April 25, 2012 Stroke in Atrial Fibrillation % Stroke 1991;22:983. Age Range (years) CHADS 2 Risk
NEWER ANTICOAGULANTS: FOCUS ON STROKE PREVENTION IN ATRIAL FIBRILLATION AND DEEP VEIN THROMBOSIS/PULMONARY EMBOLISM
 NEWER ANTICOAGULANTS: FOCUS ON STROKE PREVENTION IN ATRIAL FIBRILLATION AND DEEP VEIN THROMBOSIS/PULMONARY EMBOLISM Carol Lee, Pharm.D., Jessica C. Song, M.A., Pharm.D. INTRODUCTION For many years, warfarin
NEWER ANTICOAGULANTS: FOCUS ON STROKE PREVENTION IN ATRIAL FIBRILLATION AND DEEP VEIN THROMBOSIS/PULMONARY EMBOLISM Carol Lee, Pharm.D., Jessica C. Song, M.A., Pharm.D. INTRODUCTION For many years, warfarin
1/7/2012. Objectives. Epidemiology of Atrial Fibrillation(AF) Stroke in AF. Stroke Risk Stratification in AF
 Stroke in AF. Stroke Risk Stratification in AF") Objectives Atrial Fibrillation and Prevention of Thrombotic Complications: Therapeutic Update Andrea C. Flores Pharm.D Pharmacy Resident at the Miami VA Healthcare System Review the epidemiology, pathophysiology
Objectives Atrial Fibrillation and Prevention of Thrombotic Complications: Therapeutic Update Andrea C. Flores Pharm.D Pharmacy Resident at the Miami VA Healthcare System Review the epidemiology, pathophysiology
Anticoagulation and Reversal
 Anticoagulation and Reversal John Howard, PharmD, BCPS Clinical Pharmacist Internal Medicine Affiliate Associate Clinical Professor South Carolina College of Pharmacy Disclosures I have no Financial, Industry,
Anticoagulation and Reversal John Howard, PharmD, BCPS Clinical Pharmacist Internal Medicine Affiliate Associate Clinical Professor South Carolina College of Pharmacy Disclosures I have no Financial, Industry,
Comparison between New Oral Anticoagulants and Warfarin
 Comparison between New Oral Anticoagulants and Warfarin Warfarin was the mainstay of oral anticoagulant therapy until the recent discovery of more precise targets for therapy. In recent years, several
Comparison between New Oral Anticoagulants and Warfarin Warfarin was the mainstay of oral anticoagulant therapy until the recent discovery of more precise targets for therapy. In recent years, several
The author has no disclosures
 Mary Bradbury, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Surgery September 18, 2012 [email protected] This presentation will discuss unlabeled and investigational use of products The author
Mary Bradbury, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Surgery September 18, 2012 [email protected] This presentation will discuss unlabeled and investigational use of products The author
Stop the Bleeding: Management of Drug-induced Coagulopathy. Stacy A. Voils, PharmD, BCPS Critical Care Specialist, Neurosurgery
 Stop the Bleeding: Management of Drug-induced Coagulopathy Stacy A. Voils, PharmD, BCPS Critical Care Specialist, Neurosurgery Objectives Discuss contemporary management of warfarin reversal in patients
Stop the Bleeding: Management of Drug-induced Coagulopathy Stacy A. Voils, PharmD, BCPS Critical Care Specialist, Neurosurgery Objectives Discuss contemporary management of warfarin reversal in patients
COMPARISON OF NEW ORAL ANTICOAGULANTS AND FREQUENTLY- ASKED QUESTIONS FROM PATIENTS. TARGET AUDIENCE: All Canadian health care professionals.
 COMPARISON OF NEW ORAL ANTICOAGULANTS AND FREQUENTLY- ASKED QUESTIONS FROM PATIENTS AND PHYSICIANS TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVES: To provide a comparison of the new
COMPARISON OF NEW ORAL ANTICOAGULANTS AND FREQUENTLY- ASKED QUESTIONS FROM PATIENTS AND PHYSICIANS TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVES: To provide a comparison of the new
Anticoagulation Dosing at UCDMC Indication Agent Standard Dose Comments and Dose Adjustments VTE Prophylaxis All Services UFH 5,000 units SC q 8 h
 Indication Agent Standard Dose Comments and Dose Adjustments VTE Prophylaxis All Services UFH 5,000 units SC q 8 h See EMR adult VTE prophylaxis CI order set Enoxaparin See service specific dosing Assess
Indication Agent Standard Dose Comments and Dose Adjustments VTE Prophylaxis All Services UFH 5,000 units SC q 8 h See EMR adult VTE prophylaxis CI order set Enoxaparin See service specific dosing Assess
Guideline for the Prescribing of Novel Oral Anticoagulants (NOACs): Dabigatran (Pradaxa ), Rivaroxaban (Xarelto ), Apixaban (Eliquis )
: Dabigatran (Pradaxa ), Rivaroxaban (Xarelto ), Apixaban (Eliquis )") Guideline for the Prescribing of Novel Oral Anticoagulants (NOACs): Dabigatran (Pradaxa ), Rivaroxaban (Xarelto ), Apixaban (Eliquis ) The contents of this CPG are to be used as a guide. Healthcare professionals
Guideline for the Prescribing of Novel Oral Anticoagulants (NOACs): Dabigatran (Pradaxa ), Rivaroxaban (Xarelto ), Apixaban (Eliquis ) The contents of this CPG are to be used as a guide. Healthcare professionals
Anticoagulation Initiation,Monitoring and Titration. Ng Heng Joo Department of Haematology Singapore General Hospital
 Anticoagulation Initiation,Monitoring and Titration Ng Heng Joo Department of Haematology Singapore General Hospital The 3 I s on the Anticoagulated Patient Indication? Intensity? Indefinite? Indications
Anticoagulation Initiation,Monitoring and Titration Ng Heng Joo Department of Haematology Singapore General Hospital The 3 I s on the Anticoagulated Patient Indication? Intensity? Indefinite? Indications
3/3/2015. Patrick Cobb, MD, FACP March 2015
 Patrick Cobb, MD, FACP March 2015 I, Patrick Cobb, MD, DO NOT have a financial interest/arrangement or affiliation with one or more organizations that could be perceived as a real or apparent conflict
Patrick Cobb, MD, FACP March 2015 I, Patrick Cobb, MD, DO NOT have a financial interest/arrangement or affiliation with one or more organizations that could be perceived as a real or apparent conflict
How To Treat Aneuricaagulation
 Speaker Introduction Jessica Wilhoite, PharmD, BCACP Doctor of Pharmacy: Purdue University Postgraduate Residency Training: PGY1 Pharmacy Practice St. Vincent Hospital PGY2 Ambulatory Care St. Vincent
Speaker Introduction Jessica Wilhoite, PharmD, BCACP Doctor of Pharmacy: Purdue University Postgraduate Residency Training: PGY1 Pharmacy Practice St. Vincent Hospital PGY2 Ambulatory Care St. Vincent
Reversal of Antiplatelet and Anticoagulant Therapy: What You Need To Know. Ronald Walsh, MD Chief Medical Officer Community Blood Services
 Reversal of Antiplatelet and Anticoagulant Therapy: What You Need To Know Ronald Walsh, MD Chief Medical Officer Community Blood Services HEMOSTATIC PROCESS Initiation and formation of the platelet plug
Reversal of Antiplatelet and Anticoagulant Therapy: What You Need To Know Ronald Walsh, MD Chief Medical Officer Community Blood Services HEMOSTATIC PROCESS Initiation and formation of the platelet plug
Comparative Anticoagulation
 Comparative Anticoagulation Laurajo Ryan, PharmD, MSc, BCPS, CDE Clinical Associate Professor The University of Texas at Austin College of Pharmacy The University of Texas Health Science Center Pharmacotherapy
Comparative Anticoagulation Laurajo Ryan, PharmD, MSc, BCPS, CDE Clinical Associate Professor The University of Texas at Austin College of Pharmacy The University of Texas Health Science Center Pharmacotherapy
UHS CLINICAL CARE COLLABORATION: Outpatient & Inpatient
 Guidelines for Anticoagulation Initiation and Management Y2014 UHS CLINICAL CARE COLLABORATION: Outpatient & Inpatient Topic Page Number MEDICATION FLOW AND PATIENT FLOW... 2 AND 3 PARENTERAL ANTICOAGULANTS...
Guidelines for Anticoagulation Initiation and Management Y2014 UHS CLINICAL CARE COLLABORATION: Outpatient & Inpatient Topic Page Number MEDICATION FLOW AND PATIENT FLOW... 2 AND 3 PARENTERAL ANTICOAGULANTS...
New Oral Anticoagulants (NOACs)
") New Oral Anticoagulants (NOACs) Dabigatran (Pradaxa) Rivaroxaban (Xarelto) Apixaban (Eliquis) Edoxaban (Savaysa) Janice Lawson, MD Tallahassee Memorial Hospital Cancer and Hematology Specialists Disclosure
New Oral Anticoagulants (NOACs) Dabigatran (Pradaxa) Rivaroxaban (Xarelto) Apixaban (Eliquis) Edoxaban (Savaysa) Janice Lawson, MD Tallahassee Memorial Hospital Cancer and Hematology Specialists Disclosure
Program Objectives. Why Use Anticoagulants? 6/5/2014
 Larry Reis RPh CGP FASCP Prepared June 2014 for NADONA REIS RXCARE CONSULTING [email protected] 1 Program Objectives Discuss complications of current anticoagulant Rx Identify risks of using anticoagulants
Larry Reis RPh CGP FASCP Prepared June 2014 for NADONA REIS RXCARE CONSULTING [email protected] 1 Program Objectives Discuss complications of current anticoagulant Rx Identify risks of using anticoagulants
Update on Antiplatelets and anticoagulants. Outlines. Antiplatelets and Anticoagulants 1/23/2013. Timir Paul, MD, PhD
 Update on Antiplatelets and anticoagulants Timir Paul, MD, PhD Antiplatelets Indications Doses Long term use (beyond 12 months) ASA and combination use of NSAIDS ASA resistance Plavix resistance Plavix
Update on Antiplatelets and anticoagulants Timir Paul, MD, PhD Antiplatelets Indications Doses Long term use (beyond 12 months) ASA and combination use of NSAIDS ASA resistance Plavix resistance Plavix
4/9/2015. Risk Stratify Our Patients. Stroke Risk in AF: CHADS2 Scoring system JAMA 2001; 285: 2864-71
 Anticoagulation in the 21 st Century Adam Karpman, D.O. Saint Francis Medical Center/Oklahoma State University Medical Center Disclosures: None Atrial Fibrillation Most common arrhythmia in clinical practice.
Anticoagulation in the 21 st Century Adam Karpman, D.O. Saint Francis Medical Center/Oklahoma State University Medical Center Disclosures: None Atrial Fibrillation Most common arrhythmia in clinical practice.
STARTING, SWITCHING OR STOPPING NEW ORAL ANTICOAGULANTS: A Practical Approach
 STARTING, SWITCHING OR STOPPING NEW ORAL ANTICOAGULANTS: A Practical Approach Jeffrey I Weitz, MD, FRCP(C), FACP Professor of Medicine and Biochemistry McMaster University Canada Research Chair in Thrombosis
STARTING, SWITCHING OR STOPPING NEW ORAL ANTICOAGULANTS: A Practical Approach Jeffrey I Weitz, MD, FRCP(C), FACP Professor of Medicine and Biochemistry McMaster University Canada Research Chair in Thrombosis
Reversing the New Anticoagulants
 Reversing the New Anticoagulants Disclosure Susan C. Lambe, MD Assistant Clinical Professor Department of Emergency Medicine University of California, San Francisco Roadmap for today 1 Roadmap for today
Reversing the New Anticoagulants Disclosure Susan C. Lambe, MD Assistant Clinical Professor Department of Emergency Medicine University of California, San Francisco Roadmap for today 1 Roadmap for today
2.5mg SC daily. INR target 2-3 30 mg SC q 12 hr or 40mg daily. 10 mg PO q day (CrCl 30 ml/min). Avoid if < 30 ml/min. 2.
. Avoid if < 30 ml/min. 2.") Anticoagulation dosing at UCDMC (SC=subcutaneously; CI=continuous infusion) Indication Agent Dose Comments Prophylaxis Any or No bleeding risk factors see adult heparin (VTE prophylaxis) IV infusion order
Anticoagulation dosing at UCDMC (SC=subcutaneously; CI=continuous infusion) Indication Agent Dose Comments Prophylaxis Any or No bleeding risk factors see adult heparin (VTE prophylaxis) IV infusion order
New Oral Anticoagulants for VTE, A-fib, and ACS
 New Oral Anticoagulants for VTE, A-fib, and ACS KCUMB Fall CME 2014 September 18, 2014 Schoen W. Kruse, Ph.D. Assistant Dean Associate Professor of Pharmacology KCUMB An 82 y/o male presents to the ED
New Oral Anticoagulants for VTE, A-fib, and ACS KCUMB Fall CME 2014 September 18, 2014 Schoen W. Kruse, Ph.D. Assistant Dean Associate Professor of Pharmacology KCUMB An 82 y/o male presents to the ED
Prescriber Guide. 20mg. 15mg. Simply Protecting More Patients. Simply Protecting More Patients
 Prescriber Guide 20mg Simply Protecting More Patients 15mg Simply Protecting More Patients 1 Dear Doctor, This prescriber guide was produced by Bayer Israel in cooperation with the Ministry of Health as
Prescriber Guide 20mg Simply Protecting More Patients 15mg Simply Protecting More Patients 1 Dear Doctor, This prescriber guide was produced by Bayer Israel in cooperation with the Ministry of Health as
Making Sense of the Newer Anticoagulants
 Making Sense of the Newer Anticoagulants Brian Tiffany, MD, PhD, FACEP Dept of Emergency Medicine Chandler Regional Medical Center Mercy Gilbert Medical Center I M FROM ARIZONA! DISCLOSURES No relevant
Making Sense of the Newer Anticoagulants Brian Tiffany, MD, PhD, FACEP Dept of Emergency Medicine Chandler Regional Medical Center Mercy Gilbert Medical Center I M FROM ARIZONA! DISCLOSURES No relevant
Non- Valvular Atrial Fibrillation and Stroke Prevention: Which OAC Do I Choose. Warfarin vs the NOACs
 Non- Valvular Atrial Fibrillation and Stroke Prevention: Which OAC Do I Choose Warfarin vs the NOACs Dr. Lori McIntosh D.O. Board Certified Neurologist Objectives Be able to list the current options of
Non- Valvular Atrial Fibrillation and Stroke Prevention: Which OAC Do I Choose Warfarin vs the NOACs Dr. Lori McIntosh D.O. Board Certified Neurologist Objectives Be able to list the current options of
Three new/novel oral anticoagulants (NOAC) have been licensed in Ireland since 2008:
 have been licensed in Ireland since 2008:") Key Points to consider when prescribing NOACs Introduction Three new/novel oral anticoagulants (NOAC) have been licensed in Ireland since 2008: Dabigatran Etexilate (Pradaxa ) 75mg, 110mg, 150mg. Rivaroxaban
Key Points to consider when prescribing NOACs Introduction Three new/novel oral anticoagulants (NOAC) have been licensed in Ireland since 2008: Dabigatran Etexilate (Pradaxa ) 75mg, 110mg, 150mg. Rivaroxaban
DOACs. What s in a name? or TSOACs. Blood Clot. Darra Cover, Pharm D. Clot Formation DOACs work here. Direct Oral AntiCoagulant
 DOACs NOACs or TSOACs Generic Name DOACs Brand Name Mechanism of Action Direct Xa Inhibitor Direct Thrombin Inhibitor Dabigatran Pradaxa X Rivaroxaban Xarelto X Darra Cover, Pharm D Apixaban Eliquis X
DOACs NOACs or TSOACs Generic Name DOACs Brand Name Mechanism of Action Direct Xa Inhibitor Direct Thrombin Inhibitor Dabigatran Pradaxa X Rivaroxaban Xarelto X Darra Cover, Pharm D Apixaban Eliquis X
Post-ISTH review: Thrombosis-I New Oral Anticoagulants 臺 大 醫 院 內 科 部 血 液 科 周 聖 傑 醫 師
 Post-ISTH review: Thrombosis-I New Oral Anticoagulants 臺 大 醫 院 內 科 部 血 液 科 周 聖 傑 醫 師 The antithrombotic efficacy is limited but the risk of bleeding is indefinite Fuster V et al. Circulation 2011;123:e269-e367
Post-ISTH review: Thrombosis-I New Oral Anticoagulants 臺 大 醫 院 內 科 部 血 液 科 周 聖 傑 醫 師 The antithrombotic efficacy is limited but the risk of bleeding is indefinite Fuster V et al. Circulation 2011;123:e269-e367
2/17/2015 ANTICOAGULATION UPDATE OBJECTIVES BRIEF REVIEW: CLASSES OF ORAL ANTICOAGULANTS
 ANTICOAGULATION UPDATE C AR R I E P AL M E R, D N P, RN, AN P - BC OBJECTIVES At the end of the presentation, the NP will be able to: Identify new indications for target-specific oral anticoagulants (TSOACs),
ANTICOAGULATION UPDATE C AR R I E P AL M E R, D N P, RN, AN P - BC OBJECTIVES At the end of the presentation, the NP will be able to: Identify new indications for target-specific oral anticoagulants (TSOACs),
Outpatient Treatment of Deep Vein Thrombosis with Low Molecular Weight Heparin (LMWH) Clinical Practice Guideline August 2013
 Clinical Practice Guideline August 2013") Outpatient Treatment of Deep Vein Thrombosis with Low Molecular Weight Heparin (LMWH) Clinical Practice Guideline August 2013 General Principles: There is compelling data in the medical literature to support
Outpatient Treatment of Deep Vein Thrombosis with Low Molecular Weight Heparin (LMWH) Clinical Practice Guideline August 2013 General Principles: There is compelling data in the medical literature to support
MEDICAL ASSISTANCE HANDBOOK PRIOR AUTHORIZATION OF PHARMACEUTICAL SERVICES. A. Prescriptions That Require Prior Authorization
 MEDICAL ASSISTANCE HBOOK I. Requirements for Prior Authorization of Anticoagulants A. Prescriptions That Require Prior Authorization Prescriptions for Anticoagulants which meet any of the following conditions
MEDICAL ASSISTANCE HBOOK I. Requirements for Prior Authorization of Anticoagulants A. Prescriptions That Require Prior Authorization Prescriptions for Anticoagulants which meet any of the following conditions
Direct Oral Anticoagulants (DOACs) Who Gets What?
 Who Gets What?") Direct Oral Anticoagulants (DOACs) Who Gets What? Kathryn Hassell, MD Professor of Medicine, Division of Hematology University of Colorado Denver Disclosures No financial or commercial conflicts of interest
Direct Oral Anticoagulants (DOACs) Who Gets What? Kathryn Hassell, MD Professor of Medicine, Division of Hematology University of Colorado Denver Disclosures No financial or commercial conflicts of interest
Laboratory Testing in Patients on Novel Oral Anticoagulants (NOACs)
") Laboratory Testing in Patients on Novel Oral Anticoagulants (NOACs) Dr. Art Szkotak [email protected] University of Alberta Hospital Edmonton, AB NOACs Direct Thrombin Inhibitors (DTI):
Laboratory Testing in Patients on Novel Oral Anticoagulants (NOACs) Dr. Art Szkotak [email protected] University of Alberta Hospital Edmonton, AB NOACs Direct Thrombin Inhibitors (DTI):
Xarelto (Rivaroxaban)
") Xarelto (Rivaroxaban) Hightly selective, reversible, direct oral FXa inhibitor Maxium concentratiion after 2 to 4 hrs High bioavailability(66%),increase with food ( suggest with food) 1/3 from renal excretion,
Xarelto (Rivaroxaban) Hightly selective, reversible, direct oral FXa inhibitor Maxium concentratiion after 2 to 4 hrs High bioavailability(66%),increase with food ( suggest with food) 1/3 from renal excretion,
MEDICAL ASSISTANCE BULLETIN
 ISSUE DATE June 22, 2015 SUBJECT EFFECTIVE DATE MEDICAL ASSISTANCE BULLETIN NUMBER *See below BY Prior Authorization of Anticoagulants Pharmacy Service Leesa M. Allen, Deputy Secretary Office of Medical
ISSUE DATE June 22, 2015 SUBJECT EFFECTIVE DATE MEDICAL ASSISTANCE BULLETIN NUMBER *See below BY Prior Authorization of Anticoagulants Pharmacy Service Leesa M. Allen, Deputy Secretary Office of Medical
Novel oral anticoagulant (NOAC) for stroke prevention in atrial fibrillation Special situations
 for stroke prevention in atrial fibrillation Special situations") Novel oral anticoagulant (NOAC) for stroke prevention in atrial fibrillation Special situations Dardo E. Ferrara MD Cardiac Electrophysiology North Cascade Cardiology PeaceHealth Medical Group Which anticoagulant
Novel oral anticoagulant (NOAC) for stroke prevention in atrial fibrillation Special situations Dardo E. Ferrara MD Cardiac Electrophysiology North Cascade Cardiology PeaceHealth Medical Group Which anticoagulant
Thrombosis management: A time for change practical management with NOACs Dr Wala Elizabeth Medical Director, Bayer Healthcare
 Thrombosis management: A time for change practical management with NOACs Dr Wala Elizabeth Medical Director, Bayer Healthcare Kenya Association of Physicians Conference 10 th May 2013 New anticoagulants:
Thrombosis management: A time for change practical management with NOACs Dr Wala Elizabeth Medical Director, Bayer Healthcare Kenya Association of Physicians Conference 10 th May 2013 New anticoagulants:
Advanced Issues in Peri-Operative VTE Prevention
 Advanced Issues in Peri-Operative VTE Prevention Michael-Anthony (M-A) Williams, M.D. Consultant Physician Centura Medical Consultants September 27th, 2012 Main Topics 1. The perils of the early mover-
Advanced Issues in Peri-Operative VTE Prevention Michael-Anthony (M-A) Williams, M.D. Consultant Physician Centura Medical Consultants September 27th, 2012 Main Topics 1. The perils of the early mover-
Disclosure/Conflict of Interest
 NEW ORAL ANTICOAGULANTS: WHAT EVERY PHARMACIST SHOULD KNOW LORI B. HORNSBY, PHARMD, BCPS ASSOCIATE CLINICAL PROFESSOR AUHSOP CLINICAL PHARMACIST MIDTOWN MEDICAL CENTER OUTPATIENT CLINIC COLUMBUS, GEORGIA
NEW ORAL ANTICOAGULANTS: WHAT EVERY PHARMACIST SHOULD KNOW LORI B. HORNSBY, PHARMD, BCPS ASSOCIATE CLINICAL PROFESSOR AUHSOP CLINICAL PHARMACIST MIDTOWN MEDICAL CENTER OUTPATIENT CLINIC COLUMBUS, GEORGIA
The Brave New (Anticoagulant) World
 World") The Brave New (Anticoagulant) World Diane M. Birnbaumer, M.D., FACEP Emeritus Professor of Medicine University of California, Los Angeles Senior Clinical Educator Department of Emergency Medicine Harbor-UCLA
The Brave New (Anticoagulant) World Diane M. Birnbaumer, M.D., FACEP Emeritus Professor of Medicine University of California, Los Angeles Senior Clinical Educator Department of Emergency Medicine Harbor-UCLA
New Treatments for Stroke Prevention in Atrial Fibrillation. John C. Andrefsky, MD, FAHA NEOMED Internal Medicine Review course May 5 th, 2013
 New Treatments for Stroke Prevention in Atrial Fibrillation John C. Andrefsky, MD, FAHA NEOMED Internal Medicine Review course May 5 th, 2013 Classification Paroxysmal atrial fibrillation (AF) Last < 7
New Treatments for Stroke Prevention in Atrial Fibrillation John C. Andrefsky, MD, FAHA NEOMED Internal Medicine Review course May 5 th, 2013 Classification Paroxysmal atrial fibrillation (AF) Last < 7
Oral Anticoagulants: What s New?
 Oral Anticoagulants: What s New? Sallie Young, Pharm.D., BCPS (AQ-Cardiology) Clinical Pharmacy Specialist, Cardiology Penn State Hershey Medical Center [email protected] August 2012 Oral Anticoagulant
Oral Anticoagulants: What s New? Sallie Young, Pharm.D., BCPS (AQ-Cardiology) Clinical Pharmacy Specialist, Cardiology Penn State Hershey Medical Center [email protected] August 2012 Oral Anticoagulant
Use of Novel Oral Anticoagulants (NOACs) and the new DAWN modules at Scripps
 and the new DAWN modules at Scripps") Use of Novel Oral Anticoagulants (NOACs) and the new DAWN modules at Scripps Cheryl Ea, Pharm D. Anticoagulation Services Scripps Clinic and Scripps Green Hospital La Jolla, California Pharmacist Management
Use of Novel Oral Anticoagulants (NOACs) and the new DAWN modules at Scripps Cheryl Ea, Pharm D. Anticoagulation Services Scripps Clinic and Scripps Green Hospital La Jolla, California Pharmacist Management
Novel Oral Anticoagulants (NOACs) Prescriber Update 2013
 Prescriber Update 2013") Novel Oral Anticoagulants (NOACs) Prescriber Update 2013 Indications/Contraindications Indications Orthopedic VTE Prophylaxis VTE Treatment Stroke Prevention for non-valvular AF Contraindications 150 mg
Novel Oral Anticoagulants (NOACs) Prescriber Update 2013 Indications/Contraindications Indications Orthopedic VTE Prophylaxis VTE Treatment Stroke Prevention for non-valvular AF Contraindications 150 mg
Breadth of indications matters One drug for multiple indications
 Breadth of indications matters One drug for multiple indications Sylvia Haas, MD, PhD Formerly of the Technical University of Munich Munich, Germany Disclosures: Sylvia Haas 1 Novel oral anticoagulants:
Breadth of indications matters One drug for multiple indications Sylvia Haas, MD, PhD Formerly of the Technical University of Munich Munich, Germany Disclosures: Sylvia Haas 1 Novel oral anticoagulants:
Venous Thromboembolic Treatment Guidelines
 Venous Thromboembolic Treatment Guidelines About the NYU Venous Thromboembolic Center (VTEC) The center s mission is to deliver advanced screening, detection, care, and management services for patients
Venous Thromboembolic Treatment Guidelines About the NYU Venous Thromboembolic Center (VTEC) The center s mission is to deliver advanced screening, detection, care, and management services for patients
Disclosures. Objective (NRHS) Self Assessment #2
 Self Assessment #2") Development and Implementation of a Protocol for Reversing the Effects of Anticoagulants for Use in a Community Hospital Samantha Sepulveda, Pharm.D. PGY1 Pharmacy Resident Norman Regional Health System
Development and Implementation of a Protocol for Reversing the Effects of Anticoagulants for Use in a Community Hospital Samantha Sepulveda, Pharm.D. PGY1 Pharmacy Resident Norman Regional Health System
The New Oral Anticoagulants: When and When Not to Use Them Philip C. Comp, M.D., Ph.D. Professor of Medicine, University of Oklahoma Health Sciences
 The New Oral Anticoagulants: When and When Not to Use Them Philip C. Comp, M.D., Ph.D. Professor of Medicine, University of Oklahoma Health Sciences Center September 25, 2015 Question: With which of the
The New Oral Anticoagulants: When and When Not to Use Them Philip C. Comp, M.D., Ph.D. Professor of Medicine, University of Oklahoma Health Sciences Center September 25, 2015 Question: With which of the
To provide an evidenced-based approach to treatment of patients presenting with deep vein thrombosis.
 DEEP VEIN THROMBOSIS: TREATMENT TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To provide an evidenced-based approach to treatment of patients presenting with deep vein thrombosis.
DEEP VEIN THROMBOSIS: TREATMENT TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To provide an evidenced-based approach to treatment of patients presenting with deep vein thrombosis.
To Bridge or Not to Bridge. Periop Anticoagulation Management. Don Weinshenker, MD Ambulatory Care Denver VAMC
 To Bridge or Not to Bridge Periop Anticoagulation Management Don Weinshenker, MD Ambulatory Care Denver VAMC Financial Disclosure Information Nothing to report Periop AC Management Chronically anti-coagulated
To Bridge or Not to Bridge Periop Anticoagulation Management Don Weinshenker, MD Ambulatory Care Denver VAMC Financial Disclosure Information Nothing to report Periop AC Management Chronically anti-coagulated
MEDICAL ASSISTANCE HANDBOOK PRIOR AUTHORIZATION OF PHARMACEUTICAL SERVICES. A. Prescriptions That Require Prior Authorization
 MEDICAL ASSISTANCE HBOOK PRI AUTHIZATION OF PHARMACEUTICAL SERVICES I. Requirements for Prior Authorization of Anticoagulants A. Prescriptions That Require Prior Authorization Prescriptions for Anticoagulants
MEDICAL ASSISTANCE HBOOK PRI AUTHIZATION OF PHARMACEUTICAL SERVICES I. Requirements for Prior Authorization of Anticoagulants A. Prescriptions That Require Prior Authorization Prescriptions for Anticoagulants
New anticoagulants: Monitoring or not Monitoring? Not Monitoring
 The 2 nd World Congress on CONTROVERSIES IN HEMATOLOGY (COHEM) Barcelona, Spain September 6 8, 2012 New anticoagulants: Monitoring or not Monitoring? Not Monitoring Anna Falanga, MD Immunohematology and
The 2 nd World Congress on CONTROVERSIES IN HEMATOLOGY (COHEM) Barcelona, Spain September 6 8, 2012 New anticoagulants: Monitoring or not Monitoring? Not Monitoring Anna Falanga, MD Immunohematology and
Committee Approval Date: September 12, 2014 Next Review Date: September 2015
 Medication Policy Manual Policy No: dru361 Topic: Pradaxa, dabigatran Date of Origin: September 12, 2014 Committee Approval Date: September 12, 2014 Next Review Date: September 2015 Effective Date: November
Medication Policy Manual Policy No: dru361 Topic: Pradaxa, dabigatran Date of Origin: September 12, 2014 Committee Approval Date: September 12, 2014 Next Review Date: September 2015 Effective Date: November
Dr Gordon Royle Haematologist, Middlemore Hospital
 The New Oral Anticoagulants (NOACs) Dr Gordon Royle Haematologist, Middlemore Hospital Disclaimers Boehringer-Ingelheim Bayer Sanofi Douglas Pharmaceuticals Preventing disasters: lessons learned A cautionary
The New Oral Anticoagulants (NOACs) Dr Gordon Royle Haematologist, Middlemore Hospital Disclaimers Boehringer-Ingelheim Bayer Sanofi Douglas Pharmaceuticals Preventing disasters: lessons learned A cautionary
How to Manage Warfarin Management
 How to Manage Warfarin Management Katie McClendon, PharmD, BCPS University of Mississippi School of Pharmacy AS MANDATED BY ACCME SPEAKERS ARE ASKED TO DISCLOSE ANY REAL OR APPARENT CONFLICT RELATED TO
How to Manage Warfarin Management Katie McClendon, PharmD, BCPS University of Mississippi School of Pharmacy AS MANDATED BY ACCME SPEAKERS ARE ASKED TO DISCLOSE ANY REAL OR APPARENT CONFLICT RELATED TO
Critical Bleeding Reversal Protocol
 Critical Bleeding Reversal Protocol Coagulopathy, either drug related or multifactorial, is a major contributing factor to bleeding related mortality in a variety of clinical settings. Standard therapy
Critical Bleeding Reversal Protocol Coagulopathy, either drug related or multifactorial, is a major contributing factor to bleeding related mortality in a variety of clinical settings. Standard therapy
New Oral Anticoagulant Drugs What monitoring if any is required?
 New Oral Anticoagulant Drugs What monitoring if any is required? Michelle Williamson Supervising Scientist High Throughput Haematology Pathology Queensland PAH Laboratory Overview Background What new oral
New Oral Anticoagulant Drugs What monitoring if any is required? Michelle Williamson Supervising Scientist High Throughput Haematology Pathology Queensland PAH Laboratory Overview Background What new oral
New Oral Anticoagulants Increase Risk for Gastrointestinal Bleeding - A Systematic Review and Meta-Analysis
 New Oral Anticoagulants Increase Risk for Gastrointestinal Bleeding - A Systematic Review and Meta-Analysis Holster IL, Valkhoff VE, Kuipers EJ, Tjwa ET Departments of Gastroenterology and Hepatology,
New Oral Anticoagulants Increase Risk for Gastrointestinal Bleeding - A Systematic Review and Meta-Analysis Holster IL, Valkhoff VE, Kuipers EJ, Tjwa ET Departments of Gastroenterology and Hepatology,
Anticoagulant therapy
 Anticoagulation: The risks Anticoagulant therapy 1990 2002: 600 incidents reported 120 resulted in death of patient 92 deaths related to warfarin usage 28 reports related to heparin usage Incidents in
Anticoagulation: The risks Anticoagulant therapy 1990 2002: 600 incidents reported 120 resulted in death of patient 92 deaths related to warfarin usage 28 reports related to heparin usage Incidents in
Conserva)ve Treatment of PE/ DVT
ve Treatment of PE/ DVT") Conserva)ve Treatment of PE/ DVT Amir Kaki, MD FACC FSCAI Asst Prof of Medicine Wayne St SOM Medical Director Cardiac Catheteriza)on Lab Heart Hospital DMC Detroit, MI Incidence Acute pulmonary embolism
Conserva)ve Treatment of PE/ DVT Amir Kaki, MD FACC FSCAI Asst Prof of Medicine Wayne St SOM Medical Director Cardiac Catheteriza)on Lab Heart Hospital DMC Detroit, MI Incidence Acute pulmonary embolism
Rivaroxaban for the treatment of deep vein thrombosis and prevention of recurrent deep vein thrombosis and pulmonary embolism
 Implementation of NICE TA 261 Rivaroxaban for the treatment of deep vein thrombosis and prevention of recurrent deep vein thrombosis and pulmonary embolism Contents 1. Executive summary 2. Introduction
Implementation of NICE TA 261 Rivaroxaban for the treatment of deep vein thrombosis and prevention of recurrent deep vein thrombosis and pulmonary embolism Contents 1. Executive summary 2. Introduction