Semmelweis University Department of Traumatology Dr. Gál Tamás
|
|
|
- Randolf Flowers
- 8 years ago
- Views:
Transcription
1 Semmelweis University Department of Traumatology Dr. Gál Tamás

2 Anatomy

3 Ankle injuries DIRECT INDIRECT Vertical Compression (Tibia plafond Pilon) AO 43-A,B,C Suppination (adduction + inversion) AO 44-A Pronation (abduction + eversion) AO 44-B,C
 AO 44-A Pronation (abduction +")
4 Ankle injuries DIRECT Vertical Compression (Tibia plafond Pilon) AO 43-A,B,C
 AO")
5 Pilon fractures
6 C: Total articular surface injury AO classification according to the fracture of the tibia 43 A: Extraarticular B: Partial articular surface injury

7 Tibia pilon fracture treatment 1. Non-operative treatment: Non-dislocated fracture apply cast If operation is contraindicated traction + cast No weight bearing for 8-10 weeks

8 Tibia pilon fracture treatment 2. Surgical treatment in one session: 1.Reconstruction of the fibula 2.Reconstruction of the tibia articular surface 3.Autologous bone grafting 4.Anteromedial plate fixation

9 Tibia pilon fracture treatment 3. Two step surgical treatment First session 1. Temporary fixation with External Fixation (bridging) 2. Plate synthesis of fibula + Tibia External Fixation 3. Tibia plafond reconstruction + External fixation 4. Shortening (in case of major soft tissue damage or bone defect) Second session 7-10 days later autologous bone graft + definitive surgical stabilization

10 Tibia pilon fracture treatment 4. Timing of operation depends on soft tissue damage Open fracture, major soft tissue damage primary operation within 6-8 hours Uncomplicated fracture, no major soft tissue damage primary, one-step surgery In all other cases postponed definitive reconstruction in multiple sessions or calcaneal traction Consultant operation

11 Pilon AO 43 C2 (no fracture of the fibula)

12 Screw fixation articular surface reconstruction no weight bearing for weeks

13 Pilon C3 Plate synthesis of fibula on lateral side length External fixation for support on the medial

14 Significant soft tissue injury High risk of soft tissue loss and infection Posttraumatic arthritis May require late arthrodesis

15 Ankle injuries INDIRECT Supination (adduction + inversion) AO 44-A Pronation (abduction + eversion) AO 44-B,C

16 Supination injuries Weber A Fracture Distorsion/strain Talofibular ligament rupture/sprain Talocrural sub/luxation Chopart joint distorsion Avulsion fracture of navicular bone V. metatarsus base fracture

17 Ligament injuries Anterior
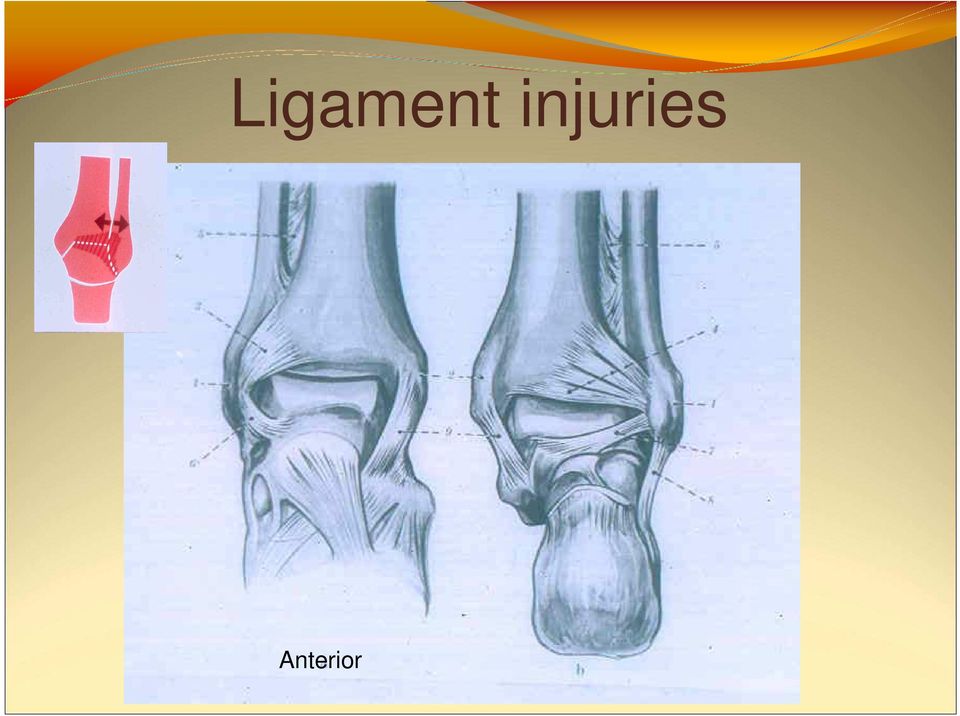
18 Distorsions-sprains Physical examination Radiography Diagnosis: Arthrography Stress radiographs 1. Adduction 2. Anterior drawer Talus tilt Less than 10 = distorsion/strain = partial sprain or rupture (usually anterior talofibular lig.) More than 15 = total rupture

19 Stress radiography Painful Rarely needed for acute injury (no therapeutic consequence) Still used for to diagnose chronic instability

20

21
22 Treatment of ligament injuries Strain or sprain? Doesn t matter, treatment is the same for a distorsion and talofibular ligament rupture Can the patient bear weight? Yes Early rehabilitation NSAID + brace No Cast splint + thrombosis profilaxis (8-10 days) Rehabilitation time: 5-6 weeks
23 Distal joint distorsions/sprains Chopart, Lisfranc Physical exam Radiography (AP and lateral foot, not ankle) Small ligament sprains, sometimes with bone abruptions Treatment is the same, can the patient bear weight Could be painful for a long time (6-12 weeks)
24 Fifth metatarsal base avulsion fracture Insertion of the peroneus brevis tendon Tension band wiring
25 Ankle fractures Danis-Weber classification Supination Pronation Classification: level of fibula fracture in relation to the syndesmosis A: below B: at the level of the syndesmosis C: above (Lauge Hansen is another type of classification based on mechanism of fracture)
26 Weber A (AO 44-A1, A2, A3) supination ~5%
27 Level of syndesmosi s
28 Weber B (AO 44 B1, B2, ~85% Pronation mechanism, fibula is fractured AT the level of the syndesmosis B1: isolated lateral malleolus B2: lateral malleolar + avulsion medial malleolus or (rupture of deltoid ligament) B3: lateral and medial and Volkmann triangle (sometimes tuber Chaput) B3) Pronation
29 Weber B Rupture of the deltoid ligament Syndesmotic screw
30 Weber B Fibula fracture at level of syndesmosis Avulsion fracture of medial malleolus Lateral malleolus plate osteosynthesis Medial malleolus tension ban wiring
31 Weber B with Volkmann triangle fracture Avulsed posterior edge of tibia Anterior compression screw
32 Weber C fractures AO type 44 C Pronation mechanism Fractures are above the syndesmosis
33 Weber C Supramalleolar fracture, where the syndesmosis and the interosseus membrane are ruptured C 1: Lateral injury only C 2: Fibula + syndesmosis + medial malleolus/deltoid ligament C 3: Subcapital fibula (Maissoneuve), syndesmosis + interosseus membrane + medial malleolus + Volkmann triangle
34
35 Maissoneuve fracture Subcapital fracture of the fibula Tibia x-ray (below knee) The syndesmotic screw is removed after 6-8 weeks
36 Open fracture Grade III, Weber C Open fracture on the medial side Urgent operation, obtain bacterial culture, antibiotic profylaxis,tetanus toxoid, stable osteosynthesis
37 Soft tissue injury Soft tissue swelling, blister formation, skin necrosis Therefore ORIF is urgent even if the fracture is closed
38 Late complications ankle arthrodesis Weber B fracture ORIF posttraumatic arthritis
39 Calcaneus Talus Tarsal and metatarsal and the rest (Navicular, Cuboid, Cuneiform bones) injuries
40 Calcaneal fractures High energy, direct trauma. Usually caused by fall from height. Also called Lover's fracture and Don Juan fracture because a lover may jump from great heights while trying to escape from the lover's spouse Look for associated spine injuries Symptoms: Hematoma on sole of foot Soft tissue swelling X-rays Broden, Zadravecz (AP, lateral, axial directions) Calcaneus is a cancellous bone Depressed frx of articular surface Goal: reconstruction of articular surface and bone axis, no weight bearing
41 Böhler s angle
42
43 ORIF
44 Closed reduction Reduction with distracter
45 Closed reduction and screw fixation
46 Extra-articular Tongue-type fracture Achilles tendon
47 Talar fractures Avascular necrosis Titanium implants! MRI Classification: AVN Hawkins I. Nondisplaced 10% Hawkins II. Subtalar displacment30% Hawkins III. Ankle joint displacm. 90% Hawkins IV. Ankle + subtalar + 100% talonavic. displacm.
48
49 Titanium screws MRI follow up
50 Midfoot and metatarsal injuries Direct or Indirect trauma If direct associated soft tissue damage March fracture (stress fracture of metatarsals) soldiers, runners, organists, doctors Usually non-operative treatment Immobilization for 6 weeks Transverse and longitudinal arches!
51
52
53 Special considerations for foot injuries Foot skin quality is different than elsewhere The skin is potentially contaminated 26 small bones compose the structure and function of the foot Direct, high energy trauma is more common Foot compartment syndrome
54 Amputations only at determined levels
55 Levels of amputation 1. Toe amputation 2. Transmetatarsal? 3. Lisfranc, Chopart 4. Pirogov / Symes 5. BKA at the proximal-middle third of calf 6. AKA depends on circulation 7. Hip exarticulation
56 Pirogov
57 Thank you for your attention