|
|
|
- Edwin Short
- 10 years ago
- Views:
Transcription
1 Renewal Page 1 of 3 9/4/2012 Renewal Name MARK A BLUMENFELD MD Credential Fee Details Renewal Application Fee $ $ Address Maintenance Demographic Information 2. Please provide your Date of Birth. 02/06/1945 Workforce Survey Introduction Dear Licensee: Thank you for renewing your license online. It IS NOT necessary that you mail your hardcopy renewal application to the Department after you have renewed online. The purpose of the next several questions is to allow the Department of Public Health to collect valuable workforce data that is currently unavailable but critical in identifying and addressing healthcare workforce shortage issues. Thank you for assisting the Department in this important initiative. Current Workforce Status 3. What is your current work status in Medicine? Part-time (less than 30 hours per week) Workforce Survey 4. In the next 12 months, do you plan to (please mark all that apply): Significantly reduce patient care hours? 5. If you are NOT working in your licensed profession, please indicate your plans for returning to work in your licensed field. I plan to return to work in my licensed profession within the next year 6. Please provide the number of hours per week that you provide DIRECT PATIENT CARE in your primary professional position. If you do not provide hours in this category, please indicate Please provide the number of hours per week that you work as an ADMINISTRATOR/MANAGER in your primary professional position. If you do not provide hours in this category, please indicate Please provide the number of hours per week that you work as an EDUCATOR/FACULTY in your primary professional position. If you do not provide hours in this category, please indicate Please provide the number of hours per week that you work as a RESEARCHER in your primary professional position. If you do not provide hours in this category, please indicate 0. 0

2 Renewal Page 2 of 3 9/4/ If your primary profesional position is in a category other than those above, please provide that category in the box below and indicate the number of hours per week. If you do not provide hours in this category, please indicate Please indicate the setting of your primary professional employment. Enter comments if "Other" is selected. Outpatient Clinic 12. Gender Male 13. Race: Choose all that apply: 14. Ethnicity: Please choose one: Not Hispanic or Latino Practice Location If you are providing direct patient care, please identify the location of the primary site where you spend the most time providing direct patient care. 15. Address Market Street 16. Address City Hartford 18. State CT 19. Zip Code Primary Source of Payment What percent of your patients have the following source of Payment? 20. Medicare less than 10% 21. Medicaid 51-75% 22. Self-Pay less than 10% 23. Private Insurance 11-25% 24. Other None Attestation 25. Have you been convicted of a felony since your last application? No

3 Renewal Page 3 of 3 9/4/ Have you had any disciplinary action taken against you or any such actions pending by another State's licensing/certification authority since your last application? No By completing this renewal online, I verify that all the information I have provided is accurate and that I satisfy the renewal requirements that apply to my license. Important Note Please note that you will receive your new licensing documents (2 wallet-sized cards and 1 suitable for posting) during the third week of next month. DO NOT submit the hardcopy renewal application with an additional fee. To continue processing your renewal, please click "Next" below. On the review screen, click "Add to Invoice." On the top right of the invoice screen, you will be given the option to "Pay Invoice" or "Print Invoice." When you are ready to pay the renewal fee, choose "Pay Invoice" to process your credit card payment. Thank you for processing your renewal online. Review
 during the third week of next month.")
4 Renewal Page 1 of 3 9/4/2012 Renewal Name MARK A BLUMENFELD MD Credential Fee Details Renewal Application Fee $ $ Address Maintenance Demographic Information 2. Please provide your Date of Birth. 02/06/1945 Workforce Survey Introduction Dear Licensee: Thank you for renewing your license online. It IS NOT necessary that you mail your hardcopy renewal application to the Department after you have renewed online. The purpose of the next several questions is to allow the Department of Public Health to collect valuable workforce data that is currently unavailable but critical in identifying and addressing healthcare workforce shortage issues. Thank you for assisting the Department in this important initiative. Current Workforce Status in Medicine 3. What is your current work status in Medicine? Inactive in the profession Workforce Survey 4. In the next 12 months, do you plan to (please mark all that apply): 5. If you are NOT working in your licensed profession, please indicate your plans for returning to work in your licensed field. 6. Please provide the number of hours per week that you provide DIRECT PATIENT CARE in your primary professional position. If you do not provide hours in this category, please indicate Please provide the number of hours per week that you work as an ADMINISTRATOR/MANAGER in your primary professional position. If you do not provide hours in this category, please indicate Please provide the number of hours per week that you work as an EDUCATOR/FACULTY in your primary professional position. If you do not provide hours in this category, please indicate Please provide the number of hours per week that you work as a RESEARCHER in your primary professional position. If you do not provide hours in this category, please indicate If your primary profesional position is in a category other than those above, please provide that category in the box below and indicate the number of hours per week. If you do not provide hours in this category, please indicate 0.

5 Renewal Page 2 of 3 9/4/ Please indicate the setting of your primary professional employment. Enter comments if "Other" is selected. 12. Gender 13. Race: Choose all that apply: 14. Ethnicity: Please choose one: Practice Location If you are providing direct patient care, please identify the location of the primary site where you spend the most time providing direct patient care. 15. Address Address City 18. State 19. Zip Code Primary Source of Payment What percent of your patients have the following source of Payment? 20. Medicare None 21. Medicaid None 22. Self-Pay None 23. Private Insurance None 24. Other None Attestation 25. Have you been convicted of a felony since your last application? No 26. Have you had any disciplinary action taken against you or any such actions pending by another State's licensing/certification authority since your last application? No By completing this renewal online, I verify that all the information I have provided is accurate and that I satisfy the renewal requirements that apply to my license. Important Note Please note that you will receive your new licensing documents (2 wallet-sized cards and 1 suitable for posting) during the third week of next month. DO NOT submit the hardcopy renewal application with an additional fee.

6 Renewal Page 3 of 3 9/4/2012 To continue processing your renewal, please click "Next" below. On the review screen, click "Add to Invoice." On the top right of the invoice screen, you will be given the option to "Pay Invoice" or "Print Invoice." When you are ready to pay the renewal fee, choose "Pay Invoice" to process your credit card payment. Thank you for processing your renewal online. Review

7

8

9
10 Credential Profile Page 1 of 3 9/4/2012 Credential Profile This profile contains information that may be used as a starting point in evaluating a health care provider. This profile should not, however, be the sole basis for selecting a health care provider. Please direct questions and comments about this profile to: Connecticut Department of Public Health, Physician Profiles, 410 Capitol Ave., M.S. 12 APP, P.O. Box , Hartford, CT , [email protected]. Name MARK A BLUMENFELD MD Credential Current Practice Locations 1. Are you currently practicing medicine in Connecticut? Yes 2. Are you actively involved in Patient Care? Yes 3. Enter your practice locations Practice Name Summit Medical Center Address 1 Address Market St. Address 3 City State Zip Code Hartford Connecticut Primary Practice Yes Languages Spoken at this Location Connecticut Staff Privileges 4. Indicate the Connecticut Hospitals or Nursing Homes for which you have Staff privileges. Facility Name City State SAINT FRANCIS HOSPITAL AND MEDICAL CENTER MT SINAI HOSP Medical School 5. Medical School Universidad Autonomao De Guadalajara 6. Enter the Year of Graduation from Medical School 1974 Post Graduate Training 7. List your postgraduate training: Site Name City State Country Start Date End Date Level Type Saint Francis Hospital and Medical Center Hartford Connecticut UNITED STATES 07/01/ /30/1978 Resident Dalhousie Medical School Halifax CANADA 07/01/ /30/1975 Intern Specialty Area/American Board Certification This physician has reported the Certification information below. For more information regarding Board Certification please contact: The American Board of Medical Specialties at or The American Osteopathic Association at 8. Please indicate practice specialties, subspecialties and the date you were certified by ABMS or ABOMS. Specialty Subspecialty Certifying Board Certification Date Medical Education Responsibilities 9. Are you a member of the faculty of a Connecticut medical school?

11 Credential Profile Page 2 of 3 9/4/ Select the state medical schools at which you are a member of the faculty. University of Connecticut School of Medicine 11. Do you have current responsibility for graduate medical education? Yes Publications, Professional Services, Activities, and Awards 12. Publications, Professional Services, Activities, and Awards Publisher/Issuer Title/Award Name Date Medical Malpractice Information 13. Indicate your malpractice insurance carrier: 14. Indicate the Medical Malpractice Payments you have made within the past ten years. Some studies have shown that there is no significant correlation between malpractice history and a physician s competence. At the same time, consumers should have access to malpractice information. This profile contains information about the malpractice payment history of the physician. Payment amounts have been placed into three statistical categories: below average, average and above average. To make the best health care decisions, you should view this information in perspective. You could miss an opportunity for high quality care by selecting a doctor based solely on malpractice history. When considering malpractice data, please keep in mind: Malpractice histories tend to vary by specialty. Some specialties are more likely than others to be the subject of litigation. This report compares physicians only to the members of their specialty, not all physicians, in order to make an individual physician s history more meaningful. This malpractice information reflects data for the last 10 years of the physician s practice. For physicians practicing less than 10 years, the data covers their total years of practice. You should take into account how long the doctor has been in practice when considering malpractice averages. The incident causing the malpractice claim may have happened years before payment is finally made. Sometimes it takes a long time for a malpractice lawsuit to move through the legal system. Some physicians work primarily with high-risk patients. These physicians may have malpractice histories that are higher than average because they specialize in cases or patients who are at very high risk of problems. Settlement of a claim may occur for a variety of reasons that do not necessarily reflect negatively on the professional competence or conduct of the physician. A payment in settlement of a medical malpractice action or claim should not be construed as creating a presumption that medical malpractice has occurred. For example, an insurer may choose to settle a case even if the physician opposes such settlement. You may wish to discuss the information provided in this report, and malpractice generally, with your physician. Payments made by or on behalf of this healthcare provider: Resolved Date Payment Category Specialty 06/05/2003 Average Obstetrics and Gynecology Connecticut Hospital Discipline This section contains categories disciplinary actions taken by hospitals during the past ten years which are specifically required by law to be released in the physician's profile. 16. Hospital Discipline Hospital Name City State Country Discipline Date Disciplinary Action Other State License 18. Indicate States outside of CT where licenses are held.

12 Credential Profile Page 3 of 3 9/4/2012 State New York Disciplinary Action No Connecticut Licensure Disciplinary Actions 19. The following lists any past disciplinary actions taken against this licensee. If there is no data present, there have been no disciplinary action taken. Date of Action Action License Status 09/19/2000 Consent Order ACTIVE 05/21/1996 Consent Order ACTIVE Felony Convictions 20. Felony Convictions within the previous ten years. Conviction Date Conviction Profile Attestation I hereby certify that to the best of my knowledge, the information contained in this profile is true and accurate and understand that providing false information may be grounds for sanction, which may include suspension revocation of my license to practice medicine in Connecticut. 21. Enter the date. 01/22/2011 Review

13

14

15

16

17
18
19

20

21
22
23
24
25
26
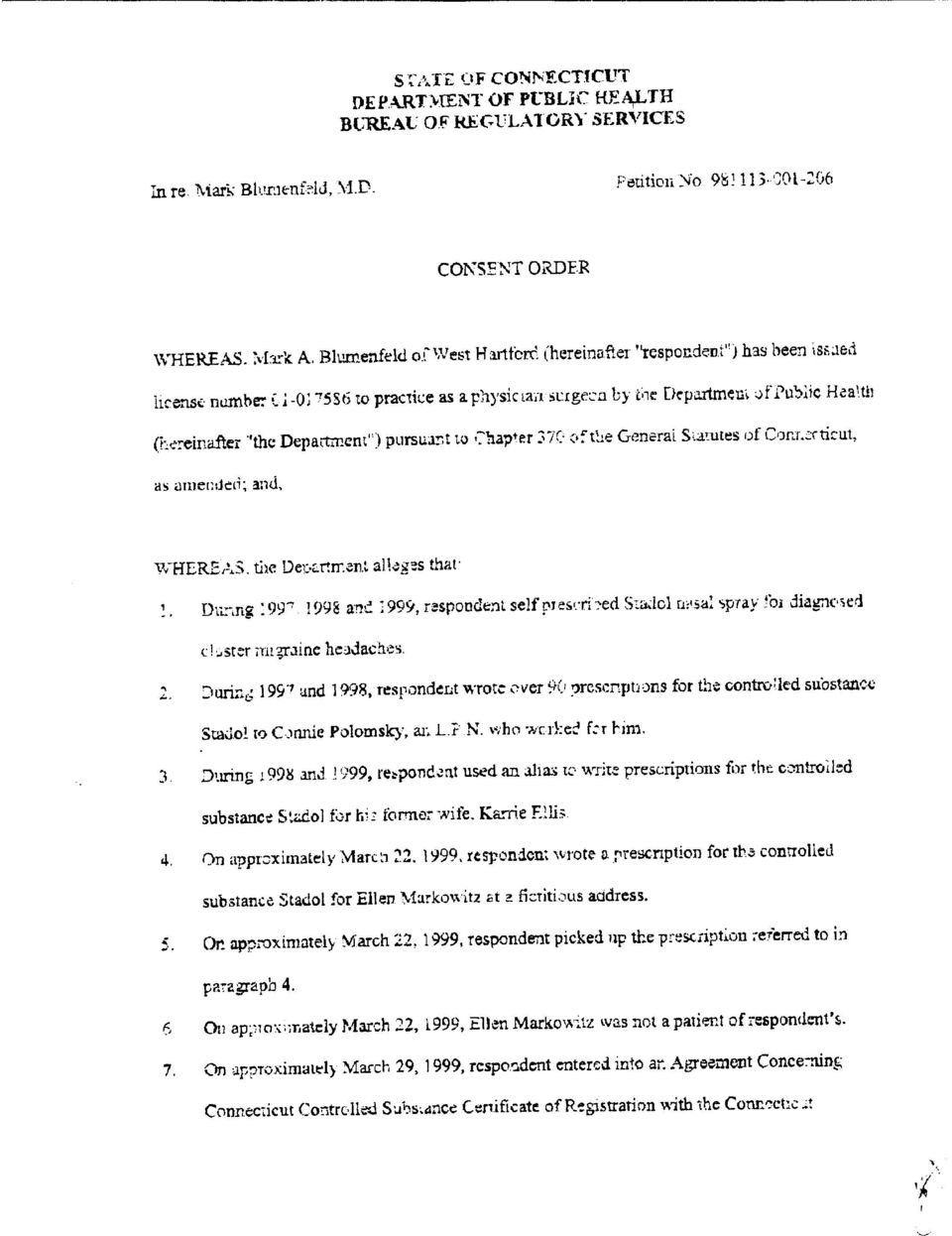
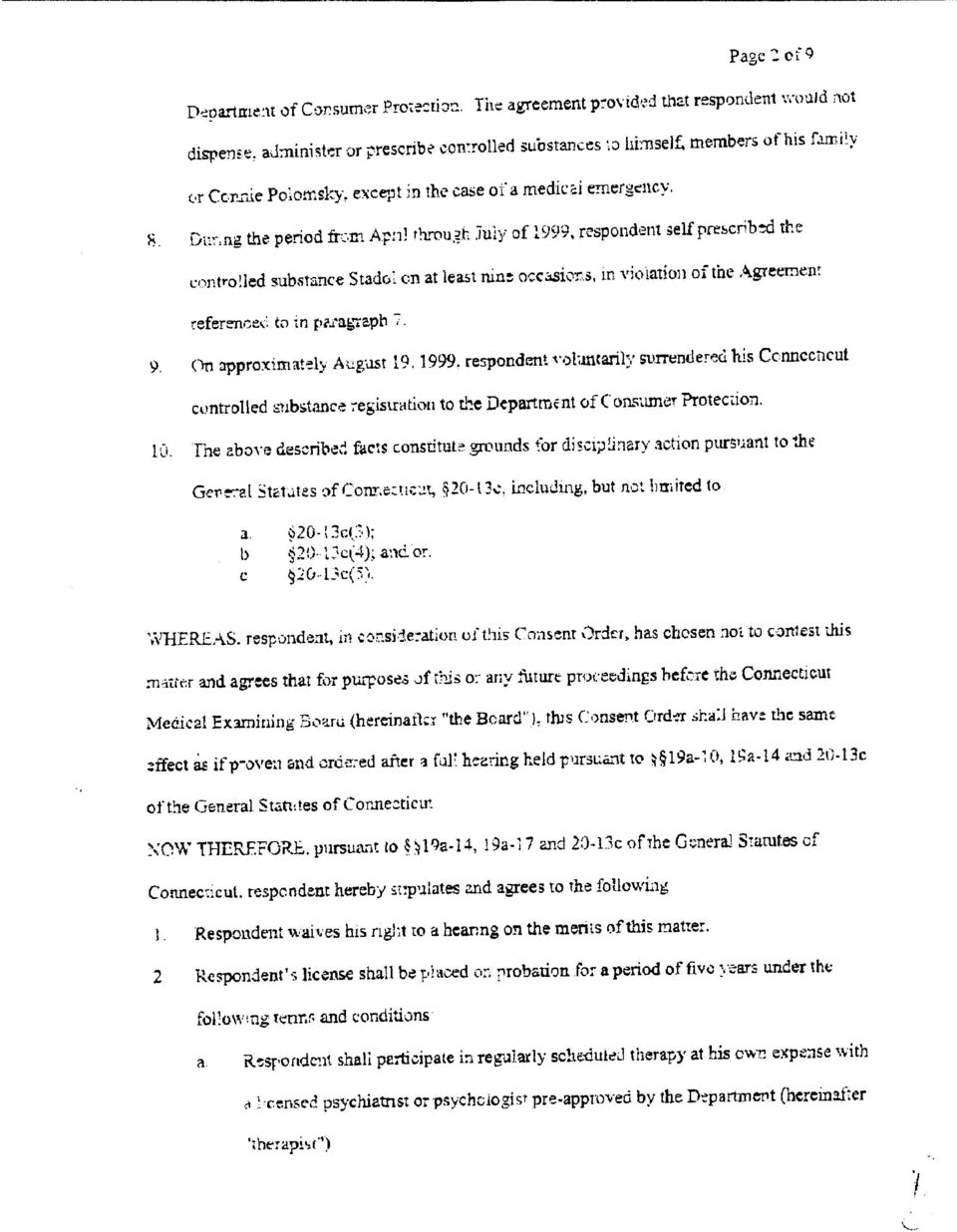
27 STATE OF CONNECTICUT DEPARTMENT OF PUBLIC HEALTH September 4, 2012 TO WHOM IT MAY CONCERN: LICENSURE VERIFICATION Please be advised that Connecticut General Statutes, certain matters involving the investigation and rehabilitation of Physician/Surgeon remain confidential. Therefore, in response to your inquiry regarding the status of the Physician/Surgeon identified below, at this time we are providing only publically disclosable information. In order for this office to confirm or deny whether there is any confidential information relevant to your inquiry, a release form from such Physician/Surgeon must be provided. IF YOU WISH TO ESTABLISH WHETHER CONFIDENTIAL INFORMATION EXISTS CONCERNING THIS Physician/Surgeon, PLEASE HAVE HIM/HER SIGN THE REVERSE SIDE OF THIS FORM, WHICH CONSTITUTES A RELEASE FOR SUCH INFORMATION, AND RETURN IT TO THIS OFFICE. PLEASE NOTE THAT ONLY THIS DEPARTMENT S RELEASE FORM WILL BE ACCEPTED. This is to certify that the records of the Connecticut Department of Public Health indicate that: MARK A BLUMENFELD MD Was issued Connecticut: Physician/Surgeon License Date of Issuance: 03/15/1976 License Number: Expiration Date: 02/28/2013 Status of License: ACTIVE, PRIOR DISCIPLINE Past or Pending Disciplinary History: Yes Sincerely, Stephen B. Carragher Health Program Supervisor Office of Practitioner Licensing and Investigation Printed by: Jan Cordero Phone: (860) Telephone Device for the Deaf (860) Capitol Avenue - MS # 12 APP P.O. Box Hartford, CT An Equal Opportunity Employer
LIBERTY DENTAL PLAN Provider Credentialing Application
 (Complete one application per Provider) (* Required Fields) Credentialing Information: Owner: Associate: *PROVIDER NAME: DDS DMD Other (specify) *DATE OF BIRTH: / / Gender: Male Female Owning Dentist Name:
(Complete one application per Provider) (* Required Fields) Credentialing Information: Owner: Associate: *PROVIDER NAME: DDS DMD Other (specify) *DATE OF BIRTH: / / Gender: Male Female Owning Dentist Name:
CLINICAL SOCIAL WORKER LICENSURE APPLICATION
 P.O. Box 110806, Juneau, Alaska 99811-0806 Telephone: (907) 465-2551 E-mail: [email protected] Website: www.commerce.alaska.gov/occ CLINICAL SOCIAL WORKER LICENSURE APPLICATION READ THESE INSTRUCTIONS
P.O. Box 110806, Juneau, Alaska 99811-0806 Telephone: (907) 465-2551 E-mail: [email protected] Website: www.commerce.alaska.gov/occ CLINICAL SOCIAL WORKER LICENSURE APPLICATION READ THESE INSTRUCTIONS
Practitioner Profile General Information License Number:
 Practitioner Profile General Information Primary Practice Address: (456.039 (1) (a) 3., F.S.) Medicaid: (456.039 (1) (b) (5) d., F.S.) Select Medicaid Statement: This practitioner does participate in the
Practitioner Profile General Information Primary Practice Address: (456.039 (1) (a) 3., F.S.) Medicaid: (456.039 (1) (b) (5) d., F.S.) Select Medicaid Statement: This practitioner does participate in the
PART II. LICENSURE BY CREDENTIALS
 State of Alaska P.O. Box 110806, Juneau, Alaska 99811-0806 Telephone: (907) 465-2551 E-mail: [email protected] Website: www.commerce.alaska.gov/occ BACCALAUREATE SOCIAL WORKER LICENSURE APPLICATION READ
State of Alaska P.O. Box 110806, Juneau, Alaska 99811-0806 Telephone: (907) 465-2551 E-mail: [email protected] Website: www.commerce.alaska.gov/occ BACCALAUREATE SOCIAL WORKER LICENSURE APPLICATION READ
PRACTITIONER CREDENTIALING APPLICATION Advanced Practice Nurse Prescriber, Certified Nurse Midwife, Physician Assistant
 PRACTITIONER CREDENTIALING APPLICATION Advanced Practice Nurse Prescriber, Certified Nurse Midwife, Physician Assistant Prior to submitting this application it is required that you contact the Provider
PRACTITIONER CREDENTIALING APPLICATION Advanced Practice Nurse Prescriber, Certified Nurse Midwife, Physician Assistant Prior to submitting this application it is required that you contact the Provider
EFFECTIVE DATE: 10/04. SUBJECT: Primary Care Nurse Practitioners SECTION: CREDENTIALING POLICY NUMBER: CR-31
 SUBJECT: Primary Care Nurse Practitioners SECTION: CREDENTIALING POLICY NUMBER: CR-31 EFFECTIVE DATE: 10/04 Applies to all products administered by the plan except when changed by contract Policy Statement:
SUBJECT: Primary Care Nurse Practitioners SECTION: CREDENTIALING POLICY NUMBER: CR-31 EFFECTIVE DATE: 10/04 Applies to all products administered by the plan except when changed by contract Policy Statement:
Los Angeles County Department of Mental Health Credentialing Application for Prescribing Practitioners Delivering Services to DCFS Children
 Los Angeles County Department of Mental Health Credentialing Application for Prescribing Practitioners Delivering Services to DCFS Children This application is exclusively for prescribing practitioners
Los Angeles County Department of Mental Health Credentialing Application for Prescribing Practitioners Delivering Services to DCFS Children This application is exclusively for prescribing practitioners
Please Note: Please send all documentation related to the credentialing portion of this documentation to:
 Please ote: The application process is split into different actions. Please send all documentation related to the contracting portion of this documentation to: Fax to: (916)350-8860 Or email to: [email protected]
Please ote: The application process is split into different actions. Please send all documentation related to the contracting portion of this documentation to: Fax to: (916)350-8860 Or email to: [email protected]
Initial Credentialing Application: Certified Registered Nurse Anesthetist (CRNA)
") Updated 1/1/2013 Specialty Surgery Center Initial Credentialing Application: Certified Registered Nurse Anesthetist (CRNA) Dear Anesthesia Provider, Thank you for your interest in providing services at
Updated 1/1/2013 Specialty Surgery Center Initial Credentialing Application: Certified Registered Nurse Anesthetist (CRNA) Dear Anesthesia Provider, Thank you for your interest in providing services at
State of Utah Department of Commerce Division of Occupational and Professional Licensing
 State of Utah Department of Commerce Division of Occupational and Professional Licensing Official Use Only Number: Date Approved/Denied: Approved/Denied By: Psychologist APPLICANT INFORMATION Full Legal
State of Utah Department of Commerce Division of Occupational and Professional Licensing Official Use Only Number: Date Approved/Denied: Approved/Denied By: Psychologist APPLICANT INFORMATION Full Legal
A. Clearly print or type information in each block. Complete each section entirely, indicate NOT APPLICABLE (N/A) where necessary.
 where necessary.") Provider Application For use by Physicians and Independent Health Care Professionals BCBSF Provider Number: HCFA UPIN #: NPI #: PURPOSE: This Provider Application will be used for assigning a provider
Provider Application For use by Physicians and Independent Health Care Professionals BCBSF Provider Number: HCFA UPIN #: NPI #: PURPOSE: This Provider Application will be used for assigning a provider
ANCILLARY PROVIDER APPLICATION FOR PARTICIPATION PHYSICIANS HEALTH PLAN PO Box 30377, Lansing, MI 48909-7877 517.364.8312
 ANCILLARY PROVIDER APPLICATION FOR PARTICIPATION PHYSICIANS HEALTH PLAN PO Box 30377, Lansing, MI 48909-7877 517.364.8312 INSTRUCTIONS: Please provide answers to all questions. If the answer is none, or
ANCILLARY PROVIDER APPLICATION FOR PARTICIPATION PHYSICIANS HEALTH PLAN PO Box 30377, Lansing, MI 48909-7877 517.364.8312 INSTRUCTIONS: Please provide answers to all questions. If the answer is none, or
PHYSICIAN APPLICATION FOR EMPLOYMENT
 PLEASE COMPLETE The Following. DATE Name Last First Middle Maiden Address City State Zip Date of Birth Place of Birth Social Security Number US Citizen Home Phone Email Address Specialty/Sub-specialty
PLEASE COMPLETE The Following. DATE Name Last First Middle Maiden Address City State Zip Date of Birth Place of Birth Social Security Number US Citizen Home Phone Email Address Specialty/Sub-specialty
North Carolina Department of Insurance. Uniform Application. To Participate as a Health Care Practitioner
 orth Carolina Department of Insurance Uniform Application To Participate as a Health Care Practitioner ote: Please send completed applications directly to the organizations with which you seek to contract.
orth Carolina Department of Insurance Uniform Application To Participate as a Health Care Practitioner ote: Please send completed applications directly to the organizations with which you seek to contract.
North Carolina Delta Dental s Recredentialing Application
 Delta Dental of North Carolina North Carolina Delta Dental s Recredentialing Application INCOMPLETE APPLICATIONS WILL BE RETURNED, WHICH WILL DELAY THE RECREDENTIALING PROCESS 1. The attached Recredentialing
Delta Dental of North Carolina North Carolina Delta Dental s Recredentialing Application INCOMPLETE APPLICATIONS WILL BE RETURNED, WHICH WILL DELAY THE RECREDENTIALING PROCESS 1. The attached Recredentialing
PLEASE ALLOW AT LEAST 60 DAYS FOR PROCESSING INSTRUCTIONS FOR APPLICANTS WHO HOLD NCCPA CERTIFICATION
 Regular Mailing Address P.O. BOX 2649 HARRISBURG, PA 17105-2649 Email: [email protected] Courier Delivery Address 2601 NORTH THIRD STREET HARRISBURG, PA 17110 717-783-1400/717-787-2381 APPLICATION FOR
Regular Mailing Address P.O. BOX 2649 HARRISBURG, PA 17105-2649 Email: [email protected] Courier Delivery Address 2601 NORTH THIRD STREET HARRISBURG, PA 17110 717-783-1400/717-787-2381 APPLICATION FOR
State of Utah Department of Commerce Division of Occupational and Professional Licensing
 State of Utah Department of Commerce Official Use Only Number: Date Approved/Denied: Approved/Denied By: Certified Nurse Midwife APPLICANT INFORMATION Full Legal Name: First Middle Last All Previous Legal
State of Utah Department of Commerce Official Use Only Number: Date Approved/Denied: Approved/Denied By: Certified Nurse Midwife APPLICANT INFORMATION Full Legal Name: First Middle Last All Previous Legal
New Jersey Physician Recredentialing Application (Please type or print)
") New Jersey Physician Recredentialing Application (Please type or print) All sections must be completed fully or clearly marked as not applicable. No area should be left blank. SECTION 1 Personal Information
New Jersey Physician Recredentialing Application (Please type or print) All sections must be completed fully or clearly marked as not applicable. No area should be left blank. SECTION 1 Personal Information
Rehab Net of Arkansas. Provider Application
 Rehab Net of Arkansas Provider Application Discipline P.T. O.T. S.L.P. (1) Business Name Physical Address FACILITY DATA Phone Fax (2) Billing Address Phone Fax (3) Mailing Address (4) Owner/Contact Person
Rehab Net of Arkansas Provider Application Discipline P.T. O.T. S.L.P. (1) Business Name Physical Address FACILITY DATA Phone Fax (2) Billing Address Phone Fax (3) Mailing Address (4) Owner/Contact Person
State of Utah Department of Commerce Division of Occupational and Professional Licensing
 State of Utah Department of Commerce Division of Occupational and Professional Licensing Official Use Only Number: Date Approved/Denied: Approved/Denied By: Retired Volunteer Health Care Practitioner APPLICANT
State of Utah Department of Commerce Division of Occupational and Professional Licensing Official Use Only Number: Date Approved/Denied: Approved/Denied By: Retired Volunteer Health Care Practitioner APPLICANT
2015 PSYCHOLOGIST BIENNIAL RENEWAL
 New Mexico Regulation and Licensing Department BOARDS AND COMMISSIONS DIVISION Board of Psychologist Examiners PO Box 25101 2550 Cerrillos Road Santa Fe, New Mexico 87504 (505) 476-4622 Fax (505) 476-4545
New Mexico Regulation and Licensing Department BOARDS AND COMMISSIONS DIVISION Board of Psychologist Examiners PO Box 25101 2550 Cerrillos Road Santa Fe, New Mexico 87504 (505) 476-4622 Fax (505) 476-4545
BOARD OF MEDICINE APPLICATION MATERIALS FOR INITIAL REGISTRATION & RENEWAL OF INTERN/RESIDENT/FELLOW & HOUSE PHYSICIAN PURSUANT TO 458.345, F.S.
 BOARD OF MEDICINE APPLICATION MATERIALS FOR INITIAL REGISTRATION & RENEWAL OF INTERN/RESIDENT/FELLOW & HOUSE PHYSICIAN PURSUANT TO 458.345, F.S. DEPARTMENT OF HEALTH 1 TABLE OF CONTENTS SECTION I: Application
BOARD OF MEDICINE APPLICATION MATERIALS FOR INITIAL REGISTRATION & RENEWAL OF INTERN/RESIDENT/FELLOW & HOUSE PHYSICIAN PURSUANT TO 458.345, F.S. DEPARTMENT OF HEALTH 1 TABLE OF CONTENTS SECTION I: Application
CHECK THE CIRCUMSTANCE UNDER WHICH YOU ARE SEEKING A TEMPORARY LICENSE: REQUIRED DOCUMENTS
 Regular Mailing Address P.O. BOX 2649 HARRISBURG, PA 17105-2649 717-783-1400/717-787-2381 Email: [email protected] Courier Delivery Address 2601 NORTH THIRD STREET HARRISBURG, PA 17110 APPLICATION FOR
Regular Mailing Address P.O. BOX 2649 HARRISBURG, PA 17105-2649 717-783-1400/717-787-2381 Email: [email protected] Courier Delivery Address 2601 NORTH THIRD STREET HARRISBURG, PA 17110 APPLICATION FOR
ONE CALL MEDICAL INC. NEURODIAGNOSTIC PHYSICIAN APPLICATION
 ONE CALL MEDICAL INC. NEURODIAGNOSTIC PHYSICIAN APPLICATION Provider has the right to review information submitted to support credentialing, correct erroneous information, to be informed of application
ONE CALL MEDICAL INC. NEURODIAGNOSTIC PHYSICIAN APPLICATION Provider has the right to review information submitted to support credentialing, correct erroneous information, to be informed of application
State of Utah Department of Commerce Division of Occupational and Professional Licensing
 State of Utah Department of Commerce Division of Occupational and Professional Licensing Official Use Only Number: Date Approved/Denied: Approved/Denied By: Clinical Mental Health Counselor APPLICANT INFORMATION
State of Utah Department of Commerce Division of Occupational and Professional Licensing Official Use Only Number: Date Approved/Denied: Approved/Denied By: Clinical Mental Health Counselor APPLICANT INFORMATION
APPLICATION FOR ALLIED PROFESSIONAL STAFF
 Office of Medical Affairs 736 Irving Ave Syracuse NY 13210 Phone: 315-470-7646 APPLICATION FOR ALLIED PROFESSIONAL STAFF Circle appropriate category CRNA Medical Physicist Research Assistant CST/Dntal
Office of Medical Affairs 736 Irving Ave Syracuse NY 13210 Phone: 315-470-7646 APPLICATION FOR ALLIED PROFESSIONAL STAFF Circle appropriate category CRNA Medical Physicist Research Assistant CST/Dntal
NURSE PRACTITIONER/PHYSICIANS ASSISTANT APPLICATION GENERAL INFORMATION. Last Name First Middle. Place of Birth Social Security #
 Page 1 NURSE PRACTITIONER/PHYSICIANS ASSISTANT APPLICATION GENERAL INFORMATION Last Name First Middle Place of Birth Social Security # Home Address City State Zip Office Address City State Zip DOB Emergency
Page 1 NURSE PRACTITIONER/PHYSICIANS ASSISTANT APPLICATION GENERAL INFORMATION Last Name First Middle Place of Birth Social Security # Home Address City State Zip Office Address City State Zip DOB Emergency
EFFECTIVE NEBRASKA HEALTH AND HUMAN SERVICES 172 NAC 100 7/21/04 REGULATION AND LICENSURE PROFESSIONAL AND OCCUPATIONAL LICENSURE TABLE OF CONTENTS
 TITLE 172 CHAPTER 100 PROFESSIONAL AND OCCUPATIONAL LICENSURE ADVANCED PRACTICE REGISTERED NURSE TABLE OF CONTENTS SUBJECT CODE SECTION PAGE Administrative Penalty 010 23 Continuing Competency 004 8 Definitions
TITLE 172 CHAPTER 100 PROFESSIONAL AND OCCUPATIONAL LICENSURE ADVANCED PRACTICE REGISTERED NURSE TABLE OF CONTENTS SUBJECT CODE SECTION PAGE Administrative Penalty 010 23 Continuing Competency 004 8 Definitions
STATE OF CONNECTICUT DEPARTMENT OF PUBLIC HEALTH ASBESTOS Worker and Supervisor Application
 STATE OF CONNECTICUT ASBESTOS Worker and Supervisor Application General Policies and Procedures IMPORTANT: THE DEPARTMENT WILL NOT REVIEW HAND-DELIVERED APPLICATIONS AT THE TIME OF RECEIPT. PROFESSIONAL
STATE OF CONNECTICUT ASBESTOS Worker and Supervisor Application General Policies and Procedures IMPORTANT: THE DEPARTMENT WILL NOT REVIEW HAND-DELIVERED APPLICATIONS AT THE TIME OF RECEIPT. PROFESSIONAL
REQUIREMENTS FOR LICENSURE:
 Email: [email protected] INITIAL APPLICATION FOR A NURSE-MIDWIFE LICENSE 1. This license class does not include prescriptive authority. If you wish to hold a certificate for prescriptive authority, you
Email: [email protected] INITIAL APPLICATION FOR A NURSE-MIDWIFE LICENSE 1. This license class does not include prescriptive authority. If you wish to hold a certificate for prescriptive authority, you
Dental Initial Credentialing Application
 Dental Initial Credentialing Application Practitioner and Practice Information Name(last) (First) (Middle) Degree Social Security Number Personal NPI Date of Birth Gender Practice Name Practice Taxpayer
Dental Initial Credentialing Application Practitioner and Practice Information Name(last) (First) (Middle) Degree Social Security Number Personal NPI Date of Birth Gender Practice Name Practice Taxpayer
State of Utah Department of Commerce Division of Occupational and Professional Licensing
 State of Utah Department of Commerce Official Use Only Number: Date Approved/Denied: Approved/Denied By: Temporary Physical Therapist Temporary Physical Therapist Assistant APPLICANT INFORMATION Full Legal
State of Utah Department of Commerce Official Use Only Number: Date Approved/Denied: Approved/Denied By: Temporary Physical Therapist Temporary Physical Therapist Assistant APPLICANT INFORMATION Full Legal
WELCOME! C. Wayne Ray, MD President, Medical Staff. Page 1 of 6
 Medical Staff Services 12401 Washington Blvd. Whittier, CA 90602-1006 T: 562.698.0811 Ext. 13632 F: 562.789.4365 E: [email protected] WELCOME! Thank you for your interest in PIH Health Hospital - Whittier.
Medical Staff Services 12401 Washington Blvd. Whittier, CA 90602-1006 T: 562.698.0811 Ext. 13632 F: 562.789.4365 E: [email protected] WELCOME! Thank you for your interest in PIH Health Hospital - Whittier.
LOCUM TENENS APPLICATION Page 1 of 4
 Page 1 of 4 This form is only valid for Locum Tenens providing coverage for up to 60 days. SECTION I PROVIDER INFORMATION This section to be completed by the PacificSource participating practitioner. Please
Page 1 of 4 This form is only valid for Locum Tenens providing coverage for up to 60 days. SECTION I PROVIDER INFORMATION This section to be completed by the PacificSource participating practitioner. Please
CREDENTIALING PROFILE
 CREDENTIALING PROFILE Please type or print all of the information requested on this Profile. Incomplete profiles cannot be accepted and will be returned for completion. Faxed and photocopies of this form
CREDENTIALING PROFILE Please type or print all of the information requested on this Profile. Incomplete profiles cannot be accepted and will be returned for completion. Faxed and photocopies of this form
REHAB PROVIDER NETWORK Professional Staff Credentialing Form
 REHAB PROVIDER NETWORK Professional Staff Credentialing Form ***** THERAPIST LICENSE MUST BE ATTACHED TO THIS FORM ***** The information requested on this form is required to certify your status as a licensed
REHAB PROVIDER NETWORK Professional Staff Credentialing Form ***** THERAPIST LICENSE MUST BE ATTACHED TO THIS FORM ***** The information requested on this form is required to certify your status as a licensed
6325 Hospital Parkway Johns Creek, Georgia 30097 Phone 678-474-7000 emoryjohnscreek.com Dear Provider,
 Dear Provider, Thank you for your recent inquiry in credentialing at Emory Johns Creek Hospital. Through our affiliation with Emory Healthcare, we are pleased to announce that our application process is
Dear Provider, Thank you for your recent inquiry in credentialing at Emory Johns Creek Hospital. Through our affiliation with Emory Healthcare, we are pleased to announce that our application process is
INFORMATION FOR COMPLETING APPLICATION FOR A LOCUM TENENS LICENSE TO PRACTICE PHYSICAL THERAPY
 Mail To: P.O. Box 8935 Ship To: 1400 E. Washington Avenue Madison, WI 53708-8935 Madison, WI 53703 FAX #: (608) 261-7083 E-Mail: [email protected] Phone #: (608) 266-2112 Website: http:dsps.wi.gov PHYSICAL
Mail To: P.O. Box 8935 Ship To: 1400 E. Washington Avenue Madison, WI 53708-8935 Madison, WI 53703 FAX #: (608) 261-7083 E-Mail: [email protected] Phone #: (608) 266-2112 Website: http:dsps.wi.gov PHYSICAL
INSTRUCTIONS FOR APPLICANTS WHO HOLD NBRC CERTIFICATION
 Email: [email protected] [email protected] Medicine 717-783-1400/717-787-2381 Osteopathic 717-783-4858 APPLICATION FOR LICENSURE AS A RESPIRATORY THERAPIST This application can be used for licensure
Email: [email protected] [email protected] Medicine 717-783-1400/717-787-2381 Osteopathic 717-783-4858 APPLICATION FOR LICENSURE AS A RESPIRATORY THERAPIST This application can be used for licensure
REQUIREMENTS FOR CERTIFICATION:
 Email: [email protected] INITIAL APPLICATION FOR NURSE-MIDWIFE PRESCRIPTIVE AUTHORITY * A separate prescriptive authority collaborative agreement must be submitted for each physician, physician group
Email: [email protected] INITIAL APPLICATION FOR NURSE-MIDWIFE PRESCRIPTIVE AUTHORITY * A separate prescriptive authority collaborative agreement must be submitted for each physician, physician group
DEPARTMENT OF HEALTH. APPLICATION FOR LIMITED LICENSURE and Instructions
 DEPARTMENT OF HEALTH BOARD OF CLINICAL SOCIAL WORK, MARRIAGE AND FAMILY THERAPY AND MENTAL HEALTH COUNSELING APPLICATION FOR LIMITED LICENSURE and Instructions APPLICATION FOR LIMITED LICENSURE INSTRUCTIONS
DEPARTMENT OF HEALTH BOARD OF CLINICAL SOCIAL WORK, MARRIAGE AND FAMILY THERAPY AND MENTAL HEALTH COUNSELING APPLICATION FOR LIMITED LICENSURE and Instructions APPLICATION FOR LIMITED LICENSURE INSTRUCTIONS
Last Name First Middle
 P.O. Box 327 Seattle, WA 98111-0327 DENTAL PROVIDER CREDENTIALING APPLICATION This application is not a contract. The information provided in this application is used to determine whether a practitioner
P.O. Box 327 Seattle, WA 98111-0327 DENTAL PROVIDER CREDENTIALING APPLICATION This application is not a contract. The information provided in this application is used to determine whether a practitioner
Department of Health
 Department of Health Board of Clinical Social Work, Marriage and Family Therapy and Mental Health Counseling MARRIAGE AND FAMILY THERAPY DUAL LICENSURE APPLICATION Qualifications for Marriage and Family
Department of Health Board of Clinical Social Work, Marriage and Family Therapy and Mental Health Counseling MARRIAGE AND FAMILY THERAPY DUAL LICENSURE APPLICATION Qualifications for Marriage and Family
Application for Licensing as an Occupational Therapist or Occupational Therapy Assistant
 Health Occupations Program Attn: Kim Ruberg P.O. Box 64882 St. Paul, MN 55164-0882 (651) 201-3725 TDD: (651) 201-5797 For office use only Application for Licensing as an Occupational Therapist or Occupational
Health Occupations Program Attn: Kim Ruberg P.O. Box 64882 St. Paul, MN 55164-0882 (651) 201-3725 TDD: (651) 201-5797 For office use only Application for Licensing as an Occupational Therapist or Occupational
APPLICANTS MUST COMPLETE THE FOLLOWING:
 Regular Mailing Address P.O. BOX 2649 HARRISBURG, PA 17105-2649 717-783-1400/717-787-2381 Email: [email protected] Courier Delivery Address 2601 NORTH THIRD STREET HARRISBURG, PA 17110 APPLICATION FOR
Regular Mailing Address P.O. BOX 2649 HARRISBURG, PA 17105-2649 717-783-1400/717-787-2381 Email: [email protected] Courier Delivery Address 2601 NORTH THIRD STREET HARRISBURG, PA 17110 APPLICATION FOR
Instructions For Clinical Nurse Specialist (CNS) Applicants
 Applicants") RETAIN FOR REFERENCE Instructions For Clinical Nurse Specialist (CNS) Applicants GENERAL INFORMATION: An applicant for Clinical Nurse Specialist certification must hold a current, unrestricted license
RETAIN FOR REFERENCE Instructions For Clinical Nurse Specialist (CNS) Applicants GENERAL INFORMATION: An applicant for Clinical Nurse Specialist certification must hold a current, unrestricted license
Independent Contractor Information CRNA
 Dear Provider: Thank you for your interest in Locum Leaders, your premier locum tenens agency. Locum Leaders provides A++ rated occurrence malpractice insurance through Med Pro. Please complete this entire
Dear Provider: Thank you for your interest in Locum Leaders, your premier locum tenens agency. Locum Leaders provides A++ rated occurrence malpractice insurance through Med Pro. Please complete this entire
STATE OF FLORIDA BOARD OF ACUPUNCTURE APPLICATION FOR LICENSURE WITH INSTRUCTIONS
 STATE OF FLORIDA BOARD OF ACUPUNCTURE APPLICATION FOR LICENSURE WITH INSTRUCTIONS Board of Acupuncture 4052 Bald Cypress Way, Bin # C-06 Tallahassee, FL 32399-3256 (850) 488-0595 September 2012 Edition
STATE OF FLORIDA BOARD OF ACUPUNCTURE APPLICATION FOR LICENSURE WITH INSTRUCTIONS Board of Acupuncture 4052 Bald Cypress Way, Bin # C-06 Tallahassee, FL 32399-3256 (850) 488-0595 September 2012 Edition
APPLICATION PACKET PSYCHOLOGIST LICENSE BY CREDENTIALS
 Department of Commerce, Community, and Economic Development Division of Corporations, Business and Professional Licensing Juneau, Alaska 99811-0806 Telephone: (907) 465-5470 E-mail: [email protected]
Department of Commerce, Community, and Economic Development Division of Corporations, Business and Professional Licensing Juneau, Alaska 99811-0806 Telephone: (907) 465-5470 E-mail: [email protected]
Allied Healthcare Professional (AHP) Professional Liability Application
 Professional Liability Application") Allied Healthcare Professional (AHP) Professional Liability Application Coverys RRG, Inc. Agency Name NOTICE: This policy is issued by your risk retention group. Your risk retention group may not be subject
Allied Healthcare Professional (AHP) Professional Liability Application Coverys RRG, Inc. Agency Name NOTICE: This policy is issued by your risk retention group. Your risk retention group may not be subject
Why is doctor credentialing important to Aetna members? What does the Aetna doctor credentialing process involve?
 Medical Credentialing What is doctor credentialing? Why is doctor credentialing important to Aetna members? What does the Aetna doctor credentialing process involve? What are the results of Aetna's commitment
Medical Credentialing What is doctor credentialing? Why is doctor credentialing important to Aetna members? What does the Aetna doctor credentialing process involve? What are the results of Aetna's commitment
Harrisburg, PA 17105-2649 Harrisburg, PA 17110
 Regular Mailing Address Courier Delivery Address 2601 North Third Street Harrisburg, PA 17105-2649 Harrisburg, PA 17110 Medical Board 717-787-2381 [email protected] Osteopathic Board 717-783-4858
Regular Mailing Address Courier Delivery Address 2601 North Third Street Harrisburg, PA 17105-2649 Harrisburg, PA 17110 Medical Board 717-787-2381 [email protected] Osteopathic Board 717-783-4858
MARYLAND BOARD OF PROFESSIONAL COUNSELORS AND THERAPISTS 4201 PATTERSON AVENUE 316 BALTIMORE, MARYLAND 21215 410-764-4732 www.dhmh.state.md.
 MARYLAND BOARD OF PROFESSIONAL COUNSELORS AND THERAPISTS 4201 PATTERSON AVENUE 316 BALTIMORE, MARYLAND 21215 410-764-4732 www.dhmh.state.md.us/bopc/ INSTRUCTIONS ALCOHOL AND OTHER DRUG COUNSELING OUT OF
MARYLAND BOARD OF PROFESSIONAL COUNSELORS AND THERAPISTS 4201 PATTERSON AVENUE 316 BALTIMORE, MARYLAND 21215 410-764-4732 www.dhmh.state.md.us/bopc/ INSTRUCTIONS ALCOHOL AND OTHER DRUG COUNSELING OUT OF
To Apply for BlueCross BlueShield of South Carolina and BlueChoice HealthPlan
 To Apply for BlueCross BlueShield of South Carolina and BlueChoice HealthPlan 1. Complete the SC Uniform Managed Care Provider Credentialing Application. 2. Enclose copies of the following items: A. State
To Apply for BlueCross BlueShield of South Carolina and BlueChoice HealthPlan 1. Complete the SC Uniform Managed Care Provider Credentialing Application. 2. Enclose copies of the following items: A. State
Surgical Center of Greensboro/Orthopaedic Surgical Center Div of Surgical Care Affiliates
 Allied Health Staff Application Instructions We are pleased to provide you with our Allied Health Staff application packet. Please do not write see attached or see resume or CV on the application. All
Allied Health Staff Application Instructions We are pleased to provide you with our Allied Health Staff application packet. Please do not write see attached or see resume or CV on the application. All
NEIGHBORHOOD HEALTH PLAN OFRHODE ISLAND CREDENTIALING PRACTITIONER APPLICATION
 NEIGHBORHOOD HEALTH PLAN OFRHODE ISLAND CREDENTIALING PRACTITIONER APPLICATION Neighborhood accepts the Council for Affordable Quality Healthcare (CAQH) application in lieu of Neighborhood s standard credentialing
NEIGHBORHOOD HEALTH PLAN OFRHODE ISLAND CREDENTIALING PRACTITIONER APPLICATION Neighborhood accepts the Council for Affordable Quality Healthcare (CAQH) application in lieu of Neighborhood s standard credentialing
MARYLAND HOSPITAL CREDENTIALING APPLICATION
 Error! STATE OF MARYLAND DHMH MARYLAND HOSPITAL CREDENTIALING APPLICATION Please type or print. Incomplete or illegible applications will not be processed. I. PERSONAL INFORMATION Name (Last, First, Middle)
Error! STATE OF MARYLAND DHMH MARYLAND HOSPITAL CREDENTIALING APPLICATION Please type or print. Incomplete or illegible applications will not be processed. I. PERSONAL INFORMATION Name (Last, First, Middle)
APPLICATION FOR A TEACHER S LICENSE - DENTISTRY OR DENTAL HYGIENE
 Maryland State Board of Dental Examiners Spring Grove Hospital Center Benjamin Rush Building 55 Wade Avenue Catonsville, Maryland 21228 (410) 402-8510 APPLICATION FOR A TEACHER S LICENSE - DENTISTRY OR
Maryland State Board of Dental Examiners Spring Grove Hospital Center Benjamin Rush Building 55 Wade Avenue Catonsville, Maryland 21228 (410) 402-8510 APPLICATION FOR A TEACHER S LICENSE - DENTISTRY OR
THE SOCIAL WORK LICENSURE (LCSW) LAW
 LAW") THE SOCIAL WORK LICENSURE (LCSW) LAW REQUIREMENTS FOR THE LICENSE: To be eligible to sit for the licensing exam the applicant must have attained a MSW from a social work program that is accredited by the
THE SOCIAL WORK LICENSURE (LCSW) LAW REQUIREMENTS FOR THE LICENSE: To be eligible to sit for the licensing exam the applicant must have attained a MSW from a social work program that is accredited by the
Application for Registration or Renewal of Athlete Agent
 11 F0091 OFFICE OF THE MISSISSIPPI SECRETARY OF STATE Post Office Box 136, Jackson, MS 39205-0136 (601)359-9055 Application for Registration or Renewal of Athlete Agent A Certificate of Registration or
11 F0091 OFFICE OF THE MISSISSIPPI SECRETARY OF STATE Post Office Box 136, Jackson, MS 39205-0136 (601)359-9055 Application for Registration or Renewal of Athlete Agent A Certificate of Registration or
State of Oregon - Board of Licensed Social Workers 3218 Pringle Rd. SE, Ste. 240, Salem, OR 97302 (503) 378-5735 [email protected].
 378-5735 Oregon.BLSW@state.or.") State of Oregon - Board of Licensed Social Workers 3218 Pringle Rd. SE, Ste. 240, Salem, OR 97302 (503) 378-5735 [email protected] LCSW License Renewal Application License Number: Renewal Date (end
State of Oregon - Board of Licensed Social Workers 3218 Pringle Rd. SE, Ste. 240, Salem, OR 97302 (503) 378-5735 [email protected] LCSW License Renewal Application License Number: Renewal Date (end
STATE OF CONNECTICUT DEPARTMENT OF PUBLIC HEALTH ASBESTOS Contractor License Application
 STATE OF CONNECTICUT DEPARTMENT OF PUBLIC HEALTH ASBESTOS Contractor License Application General Policies and Procedures IMPORTANT: THE DEPARTMENT WILL NOT REVIEW HAND-DELIVERED APPLICATIONS AT THE TIME
STATE OF CONNECTICUT DEPARTMENT OF PUBLIC HEALTH ASBESTOS Contractor License Application General Policies and Procedures IMPORTANT: THE DEPARTMENT WILL NOT REVIEW HAND-DELIVERED APPLICATIONS AT THE TIME
INSTRUCTIONS FOR APPLICANTS WHO HOLD NBRC CERTIFICATION
 Email: [email protected] [email protected] Medicine 717-783-1400/717-787-2381 Osteopathic 717-783-4858 APPLICATION FOR LICENSURE AS A RESPIRATORY THERAPIST This application can be used for licensure
Email: [email protected] [email protected] Medicine 717-783-1400/717-787-2381 Osteopathic 717-783-4858 APPLICATION FOR LICENSURE AS A RESPIRATORY THERAPIST This application can be used for licensure
ARKANSAS BOARD OF PODIATRIC MEDICINE
 ARKANSAS BOARD OF PODIATRIC MEDICINE APPLICATION FOR LICENSE TO PRACTICE PODIATRIC MEDICINE 1. Name: Social Security Number: (As to appear on License) 2. Address: 3. Address you wish License to be mailed:
ARKANSAS BOARD OF PODIATRIC MEDICINE APPLICATION FOR LICENSE TO PRACTICE PODIATRIC MEDICINE 1. Name: Social Security Number: (As to appear on License) 2. Address: 3. Address you wish License to be mailed:
Dear Applicant: Sincerely, Kelli Dalrymple, Coordinator Medical and Specialized Health. Licensure Unit
 Please Reply To: Licensure Unit P.O. Box 94986, Lincoln, NE 68509-4986 Phone (402) 471-2118 FAX (402) 471-3577 Dear Applicant: Thank you for your interest in becoming licensed to practice your profession
Please Reply To: Licensure Unit P.O. Box 94986, Lincoln, NE 68509-4986 Phone (402) 471-2118 FAX (402) 471-3577 Dear Applicant: Thank you for your interest in becoming licensed to practice your profession
Physical Therapist Physical Therapist Assistant by Endorsement
 State of Maine BOARD OF EXAMINERS IN PHYSICAL THERAPY Application information to assist in completing your application. This information is not designed to include all information on laws and rules and
State of Maine BOARD OF EXAMINERS IN PHYSICAL THERAPY Application information to assist in completing your application. This information is not designed to include all information on laws and rules and
Mississippi Medicaid Enrollment Application (Ordering/Referring/Prescribing Provider)
") This application is for the sole purpose of ordering/referring/prescribing items and services for MS Medicaid beneficiaries. This type of enrollment does not allow MS Medicaid to reimburse the applicant/provider
This application is for the sole purpose of ordering/referring/prescribing items and services for MS Medicaid beneficiaries. This type of enrollment does not allow MS Medicaid to reimburse the applicant/provider
State of Utah Department of Commerce Division of Occupational and Professional Licensing
 State of Utah Department of Commerce Official Use Only Number: Date Approved/Denied: Approved/Denied By: Veterinarian APPLICANT INFORMATION Full Legal Name: First Middle Last All Previous Legal Names:
State of Utah Department of Commerce Official Use Only Number: Date Approved/Denied: Approved/Denied By: Veterinarian APPLICANT INFORMATION Full Legal Name: First Middle Last All Previous Legal Names:
Provider Credentialing Application
 1515 North Saint Joseph Avenue PO Box 8000 Marshfield, WI 54449-8000 1.800.472.2363 or 715.221.9555 TTY: 1.877.727.2232 or 715.221.9898 Provider Credentialing Application Security Health Plan s Expectations
1515 North Saint Joseph Avenue PO Box 8000 Marshfield, WI 54449-8000 1.800.472.2363 or 715.221.9555 TTY: 1.877.727.2232 or 715.221.9898 Provider Credentialing Application Security Health Plan s Expectations
Credentialing CREDENTIALING
 CREDENTIALING Based on standards set forth by the National Committee for Quality Assurance (NCQA) all Providers listed in literature for Molina Healthcare will be credentialed. All designated practitioners,
CREDENTIALING Based on standards set forth by the National Committee for Quality Assurance (NCQA) all Providers listed in literature for Molina Healthcare will be credentialed. All designated practitioners,
ALL APPLICANTS MUST COMPLETE THE FOLLOWING:
 APPLICATION FOR ATHLETIC TRAINER LICENSE (This application may also be used for a temporary license) 1. An applicant for licensure shall meet one of the following requirements: a. Be a graduate of an approved
APPLICATION FOR ATHLETIC TRAINER LICENSE (This application may also be used for a temporary license) 1. An applicant for licensure shall meet one of the following requirements: a. Be a graduate of an approved
30 Day Limited Permits for Professional Engineers and Land Surveyors
 THE STATE EDUCATION DEPARTMENT / THE UNIVERSITY OF THE STATE OF NEW YORK / ALBANY, NY 12234 Office of the Professions, State Board for Engineering and Land Surveying PHONE: 518-474-3817 ext. 140 FAX: 518-473-6282
THE STATE EDUCATION DEPARTMENT / THE UNIVERSITY OF THE STATE OF NEW YORK / ALBANY, NY 12234 Office of the Professions, State Board for Engineering and Land Surveying PHONE: 518-474-3817 ext. 140 FAX: 518-473-6282
MARYLAND BOARD OF PROFESSIONAL COUNSELORS AND THERAPISTS 4201 PATTERSON AVENUE 316 BALTIMORE, MARYLAND 21215 410-764-4732 www.dhmh.maryland.
 MARYLAND BOARD OF PROFESSIONAL COUNSELORS AND THERAPISTS 4201 PATTERSON AVENUE 316 BALTIMORE, MARYLAND 21215 410-764-4732 www.dhmh.maryland.gov/bopc/ INSTRUCTIONS ALCOHOL AND OTHER DRUG COUNSELING OUT
MARYLAND BOARD OF PROFESSIONAL COUNSELORS AND THERAPISTS 4201 PATTERSON AVENUE 316 BALTIMORE, MARYLAND 21215 410-764-4732 www.dhmh.maryland.gov/bopc/ INSTRUCTIONS ALCOHOL AND OTHER DRUG COUNSELING OUT
NASI Per Diem Malpractice
 Dear Nurse Anesthetist, We appreciate your interest in NASI s Per Diem Malpractice Insurance. This service is for those providers who need a supplemental policy for working an assignment outside of their
Dear Nurse Anesthetist, We appreciate your interest in NASI s Per Diem Malpractice Insurance. This service is for those providers who need a supplemental policy for working an assignment outside of their
2. Be of good moral character. Have 2 recommendations completed on page 3.
 STATE BOARD OF SOCIAL WORKERS, MARRIAGE AND FAMILY THERAPISTS AND PROFESSIONAL COUNSELORS P.O. BOX 2649 HARRISBURG, PA 17105-2649 717-783-1389 FAX 717-787-7769 Email [email protected] Website www.dos.pa.gov/social
STATE BOARD OF SOCIAL WORKERS, MARRIAGE AND FAMILY THERAPISTS AND PROFESSIONAL COUNSELORS P.O. BOX 2649 HARRISBURG, PA 17105-2649 717-783-1389 FAX 717-787-7769 Email [email protected] Website www.dos.pa.gov/social
Community Health Group Allied Health Professional Application
 Community Health Group Allied Health Professional Application Nurse Practitioner Certified Nurse Midwife LCSW Clinical Psychologist MFCC Other I. INSTRUCTIONS This form should be typed or legibly printed
Community Health Group Allied Health Professional Application Nurse Practitioner Certified Nurse Midwife LCSW Clinical Psychologist MFCC Other I. INSTRUCTIONS This form should be typed or legibly printed
APPLICATION FOR A LICENSE BY EXAMINATION TO PRACTICE MARRIAGE AND FAMILY THERAPY
 QUALIFICATIONS STATE BOARD OF SOCIAL WORKERS, MARRIAGE AND FAMILY THERAPISTS AND PROFESSIONAL COUNSELORS P.O. BOX 2649 HARRISBURG, PA 17105-2649 Email [email protected] Website www.dos.pa.gov/social
QUALIFICATIONS STATE BOARD OF SOCIAL WORKERS, MARRIAGE AND FAMILY THERAPISTS AND PROFESSIONAL COUNSELORS P.O. BOX 2649 HARRISBURG, PA 17105-2649 Email [email protected] Website www.dos.pa.gov/social
STATE OF CONNECTICUT DEPARTMENT OF PUBLIC HEALTH LEAD Contractor License Application
 STATE OF CONNECTICUT DEPARTMENT OF PUBLIC HEALTH LEAD Contractor License Application General Policies and Procedures IMPORTANT: THE DEPARTMENT WILL NOT REVIEW HAND-DELIVERED APPLICATIONS AT THE TIME OF
STATE OF CONNECTICUT DEPARTMENT OF PUBLIC HEALTH LEAD Contractor License Application General Policies and Procedures IMPORTANT: THE DEPARTMENT WILL NOT REVIEW HAND-DELIVERED APPLICATIONS AT THE TIME OF
Nevada State Board of Osteopathic Medicine Application for Temporary Osteopathic Medical Physician Licensure
 Nevada State Board of Osteopathic Medicine Application for Temporary Osteopathic Medical Physician Licensure Dear Applicant: Thank you for considering obtaining a temporary Osteopathic Medicine License
Nevada State Board of Osteopathic Medicine Application for Temporary Osteopathic Medical Physician Licensure Dear Applicant: Thank you for considering obtaining a temporary Osteopathic Medicine License
This policy applies to: Stanford Hospital and Clinics Lucile Packard Children s Hospital. Date Written or Last Revision: Oct 2012
 Providers Page 1 of 13 I. PURPOSE To establish mechanisms for gathering relevant data that will serve as the basis for decisions regarding credentialing and privileging of licensed independent practitioners
Providers Page 1 of 13 I. PURPOSE To establish mechanisms for gathering relevant data that will serve as the basis for decisions regarding credentialing and privileging of licensed independent practitioners
American College of Legal Medicine Application for Membership
 I. Membership Categories I am applying for: American College of Legal Medicine Application for Membership o FELLOW ($100 member application fee*, $325 annual dues) A professional with either an MD, DO,
I. Membership Categories I am applying for: American College of Legal Medicine Application for Membership o FELLOW ($100 member application fee*, $325 annual dues) A professional with either an MD, DO,
Maryland Insurance Administration Individual Producer License Renewal / Reinstatement Checklist
 Maryland Insurance Administration Individual Producer License Renewal / Reinstatement Checklist Important Update: The attached application and supplement may be used to renew or reinstate an existing Maryland
Maryland Insurance Administration Individual Producer License Renewal / Reinstatement Checklist Important Update: The attached application and supplement may be used to renew or reinstate an existing Maryland
Wisconsin Department of Safety and Professional Services
 Mail To: P.O. Box 8935 1400 E. Washington Avenue Madison, WI 53708-8935 Madison, WI 53703 FAX #: (608) 261-7083 E-Mail: [email protected] Phone #: (608) 266-2112 Website: http://dsps.wi.gov BOARD OF NURSING
Mail To: P.O. Box 8935 1400 E. Washington Avenue Madison, WI 53708-8935 Madison, WI 53703 FAX #: (608) 261-7083 E-Mail: [email protected] Phone #: (608) 266-2112 Website: http://dsps.wi.gov BOARD OF NURSING
Individual Application for Massage Therapy Iowa Department of Public Health/Bureau of Professional Licensure Board Office Telephone (515) 281-6959
 281-6959") For Office Use License #: Date Issued: $120 Individual Application for Massage Therapy Iowa Department of Public Health/Bureau of Professional Licensure Board Office Telephone (515) 281-6959 Applicant
For Office Use License #: Date Issued: $120 Individual Application for Massage Therapy Iowa Department of Public Health/Bureau of Professional Licensure Board Office Telephone (515) 281-6959 Applicant
State of Maine BOARD OF COMPLEMENTARY HEALTH CARE PROVIDERS
 State of Maine BOARD OF COMPLEMENTARY HEALTH CARE PROVIDERS Application information to assist in completing your application. This information is not designed to include all information on laws and rules
State of Maine BOARD OF COMPLEMENTARY HEALTH CARE PROVIDERS Application information to assist in completing your application. This information is not designed to include all information on laws and rules
Board Respiratory Care
 Michigan Department of Licensing and Regulatory Affairs Bureau of Health Care Services Board of Respiratory Care PO Box 30670 Lansing MI 48909 (517) 335-0918 www.michigan.gov/healthlicense Page 1 of 14
Michigan Department of Licensing and Regulatory Affairs Bureau of Health Care Services Board of Respiratory Care PO Box 30670 Lansing MI 48909 (517) 335-0918 www.michigan.gov/healthlicense Page 1 of 14
Pharmacy Technician (this application applies only if you are an employee of a Maine pharmacy)
") MAINE BOARD OF PHARMACY Application information to assist in completing your application. This information is not designed to include all information on laws and rules and it is strongly recommended that
MAINE BOARD OF PHARMACY Application information to assist in completing your application. This information is not designed to include all information on laws and rules and it is strongly recommended that
Board of Speech-Language Pathology and Audiology
 Board of Speech-Language Pathology and Audiology Application for Speech-Language Pathology or Audiology Provisional Licensure With Instructions Attached Board of Speech-Language Pathology and Audiology
Board of Speech-Language Pathology and Audiology Application for Speech-Language Pathology or Audiology Provisional Licensure With Instructions Attached Board of Speech-Language Pathology and Audiology