Benzodiazepine case based discussion. Charlie Reznikoff ACP Pain precourse November 1 st 2012
|
|
|
- Bartholomew Payne
- 8 years ago
- Views:
Transcription
1 Benzodiazepine case based discussion Charlie Reznikoff ACP Pain precourse November 1 st 2012

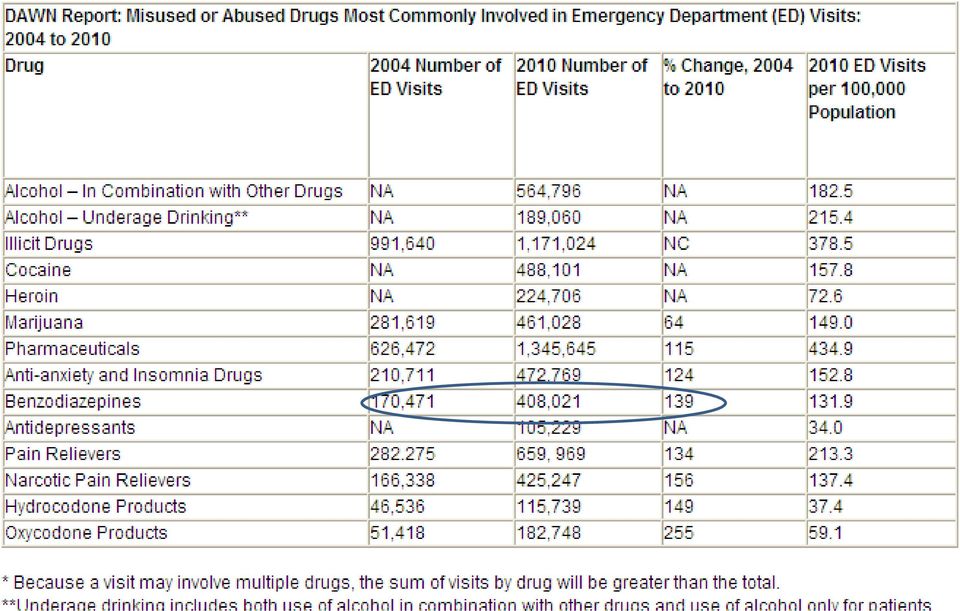
2 Medicaid recipients

3

4
5 Most commonly prescribed benzo, also the benzo favored by addicts?

6 Alprazolam

7 Alprazolam s suitable replacement?

8 Alprazolam s suitable replacements Clonazepam if in withdrawal due to structural homology and cross tolerance Lorazepam for the psychiatric indications for the time of onset and duration

9 Case 1

10 55 year-old woman with depression and insomnia presents for an insurance evaluation after a minor car crash. Her motor vehicle crash was a minor fender bender one week ago. She did not fall asleep at the wheel. She didn t see that the car had stopped in front of her. She says she had minor whiplash. She is pain free and has no neurologic symptoms

11 She has a had an episode of depression for nine weeks, characterized by poor concentration, decreased appetite, low energy, tearfulness, and difficulty getting to sleep. She is not suicidal. Two weeks ago another provider started fluoxetine 20 mg and clonazepam 1 mg at bedtime. Her sleep has improved but her other symptoms are unchanged. She has hypertension treated with HCTZ but no other medical issues or medications. Vitals and physical exam are unremarkable other than a decreased mood and psychomotor retardation.

12 55 year-old woman recently started on clonazepam and fluoxetine with a minor car accident, still appearing depressed. You should 1. Add methylphenidate for neurovegetative symptoms 2. Change clonazepam to temazepam 3. Do nothing at this point, follow up in 2 weeks for fluoxetine effect 4. Ask her to surrender her car keys, and arrange a ride home from clinic

13 55 year-old woman recently started on clonazepam and fluoxetine with a minor car accident, still appearing depressed. You should 1. Add methylphenidate for neurovegetative symptoms 2. Change clonazepam to temazepam 3. Do nothing at this point, follow up in 2 weeks for fluoxetine effect 4. Ask her to surrender her car keys, and arrange a ride home from clinic

14 Commonly used benzos and why Clonazepam for GAD/adjustment disorder Longer action, less euphoria Lorazepam for panic/specific phobia More rapid onset, shorter half life, less euphoria Diazepam for detoxification Self tapering, rapid onset, long half life Midazolam for anesthesia Very short half life, easy to titrate IV Temazepam for sleep Half life appropriate for 8 hour sleep, less euphoria

15

16 Benzos and driving Strong evidence that any benzo use is associated with motor vehicle crashes Impairment related to long half life of benzos Coingestion of alcohol very high risk Of the antidepressants, tricyclics are the most problematic (in elderly) Dassanayake T. Michie P. Carter G. Jones A. Drug Safety. 34(2):125-56, 2011 Feb 1.
 Dassanayake T. Michie P. Carter G. Jones A. Drug Safety.")
17

18 Bottom line Case 1 Long acting benzodiazepines for sleep are associated with MVCs the next day Be aware of the different times of onset, half life, and indications for benzos Intoxicated patients should be asked to surrender their car keys Patients on controlled substances should be educated about driving laws

19 Case 2

20 A 57 year-old man with alcohol-related cirrhosis is admitted to the hospital for alcohol detoxification. He has had two previous episodes of delirium tremens and at least one alcohol-related seizures. He is 12 hours from his last drink. He feels shaky but otherwise reports no symptoms. He would like detox and admission to an addiction treatment program

21 Vital signs are normal. The patient is anxious but has clear mentation. He has slight jaundice and stigmata of cirrhosis. Extremities wasted and a slightly protuberant abdomen. AST 170; ALT 100; Creatinine 0.5; Bili 2.3; INR 1.3; Blood alcohol level is 0.03%. Platelets are 89, and sodium is 135, other labs are normal. Abdominal ultrasound is consistent with cirrhosis and minimal ascites.
22 57 year-old man with stable alcoholic cirrhosis and a history of DTs and seizures presents for Alcohol detoxification. You should use: 1. Alcohol withdrawal protocol (symptom driven) using diazepam 2. Alcohol withdrawal protocol (symptom driven) using lorazepam 3. Scheduled diazepam 4. Scheduled lorazepam
23 57 year-old man with stable alcoholic cirrhosis and a history of DTs and seizures presents for Alcohol detoxification. You should use: 1. Alcohol withdrawal protocol (symptom driven) using diazepam 2. Alcohol withdrawal protocol (symptom driven) using lorazepam 3. Scheduled diazepam 4. Scheduled lorazepam
24 Alcohol Withdrawal (mayo clinic proceedings, 1995)
25 Delirium Tremens Risk factors for DTs: Previous DTs History predicts future Age >30 Concurrent illness Sustained drinking Poor nutrition
26 Alcohol WD Seizures Occur early after alcohol cessation Often the first sign of W/D 3 % of alcohol dependent patients Generalized convulsions Brief often isolated episodes Suppressed easily with benzodiazepines
27
28 The Biochemical Basis of Neuropharmacology Cooper, Bloom & Roth
29 Bottom line case 2 Choose lorazepam for elderly, cirrhosis, or renal insufficiency no active metabolites Unlike diazepam, lorazepam is not self tapering, and requires a scheduled taper Symptom driven alcohol protocols are appropriate for mild to moderate withdrawal If high risk for DTs or seizure, schedule benzodiazepines for withdrawal
30 Case 3
31 A 45 year-old woman with generalized anxiety disorder is on clonazepam 1 mg TID and Sertraline 150 mg daily. She presents to you wishing to taper off clonazepam because of side effects. She feels dopey and reports forgetting things. Also she dislikes being on a potentially addictive controlled substance
32 She has been on this dose of clonazepam for 10 months uninterrupted, and prior to that she was not on another sedative. She has no history of addiction including no alcohol use. She does not have a seizure disorder. Other than her psychiatric illness she has no medical issues and is on no other medications. She is clearly anxious about withdrawal otherwise her exam is totally normal
33 45 year-old woman wishing to taper off clonazepam after eight months. Your plan for her is: 1. Discontinue clonazepam at any time. She is not at risk of withdrawal 2. Discontinue Clonazepam and add amitriptyline 50 mg QHS to treat symptoms clonazepam withdrawal 3. Taper clonazepam slowly over 30 days with no additional medication change 4. Switch clonazepam to phenobarbitol and taper slowly over 30 days
34 45 year-old woman wishing to taper off clonazepam after eight months. Your plan for her is: 1. Discontinue clonazepam at any time. She is not at risk of withdrawal 2. Discontinue Clonazepam and add amitriptyline 50 mg QHS to treat symptoms clonazepam withdrawal 3. Taper clonazepam slowly over 30 days with no additional medication change 4. Switch clonazepam to phenobarbitol and taper slowly over 30 days
35 Benzo Cessation Syndromes Recurrence Rebound Withdrawal
36 Recurrence You were anxious before you started benzos, you ll be anxious when you stop
37 Recurrence Recurrence of the underlying disorder Usually insomnia or anxiety Universal after cessation of benzos Educate and reassure the patient Find appropriate alternative to benzos
38 Rebound recurrence with a vengeance Whatever anxiety (or insomnia) you had before you started benzos is amplified for 1-2 weeks after stopping
39 Rebound Heightening of underlying condition the benzo was suppressing Classically insomnia, panic, and anxiety Self limited, <2 weeks No autonomic discharge, seizure, or delirium Reassure, educate and find alternatives Benzo taper optional for comfort only
40 (True) Withdrawal Delirium, psychosis, autonomic arousal, seizure, death
41 (True) Withdrawal Akin to alcohol withdrawal Autonomic discharge Seizures Psychosis Delirium Mortality on the order of DTs Variable severity and time course
42 Risk assessment for withdrawal Benzo exposure sufficient for physiologic dependence is highly variable! 6 months daily use moderate dose 3 months daily use 3X normal dose Any duration in an alcohol/barbiturate dependent patient Lowinson Substance abuse
43 Benzo users are notoriously poor historians, and unreliable pill takers
44 Likelihood of withdrawal Short acting meds No metabolites High dose Concomitant alcohol use cessation Concomitant medical illness
45 Timing of Withdrawal Timing of onset of withdrawal is characteristic to the half life of the benzo used Midaz (<24 hours) Loraz (48 hours) Diaz (up to seven days)
46 Principles of Tapering Find symptom suppressing dose Replace short acting with long acting chlordiazepox phenobarb diazepam clonazepam Taper with 10% steps daily (fastest!) to weekly Halt or reverse taper if recurrence of symptoms
47 Tapers Uncomplicated outpatient Complicated outpatient Complicated inpatient
48 Uncomplicated Outpatient Taper Non-addicted patient No aberrant behavior No previous serious withdrawal Physiologic dependence Leave medication the same and taper over 30 days
49 Complicated Outpatient Taper Failed uncomplicated taper Addiction history or aberrant behavior No previous serious withdrawal Physiologic dependence Change to long acting and taper over 30 days
50 Inpatient Taper Multiple failed tapers Serious addictive behavior Serious withdrawal history Change to long acting, day taper inpatient facility or highly structured outpatient, possible commitment
51 Find The Suppressing Dose In serious withdrawal, the commonest reason for a failed taper is insufficient dose Never begin to taper before the symptom suppressing dose is found Titrate benzos until the patient is calm and autonomic storm resolved
52
53 Using Alcohol Protocols Safe for moderate withdrawal Not helpful for severe withdrawal Physician should schedule large doses Use longer acting sedatives if possible
54 Case 3 bottom line Understand benzo rebound phenomenon Be able to assess the risk of true withdrawal Construct an appropriate taper based on your patient s demographics Find the symptom suppressing dose and taper slowly
55 Case 4
56 A 76 year-old woman with COPD and osteoporosis requests a medication for sleep. She is unable to sleep, due to the recent loss of her spouse who died one week ago unexpectedly. She is tearful and she blames herself as she describes to you finding her husband s deceased body. She is not suicidal. She has slept less than 2 hours nightly since this event.
57 She has on average two COPD exacerbations per year. She takes an inhaled short-acting beta agonist, long-acting anticholinergic, and an inhaled glucocorticoid. She is not on home oxygen. She takes phosphodiesterase inhibitors for osteoporosis. She is formerly tobacco dependent and alcohol dependent with 2 years abstinence from both. She is willing to see a grief counselor, but would also like a sleeping aid.
58 76 year-old woman with copd, osteoporosis and acute insomnia. The most important contraindication to using a benzodiazepine is: 1. Benzodiazepines interfere with talk therapy due to their amnestic effect 2. Benzodiazepines cause respiratory suppression increasing the severity of COPD exacerbations 3. Benzodiazepines at night in older patients are associated with falls and hip fractures 4. Benzodiazepines in recovering alcoholics are associated with alcohol relapse 5. Benzodiazepines are not indicated for acute insomnia
59 76 year-old woman with copd. osteoporosis and acute insomnia. The most important contraindication to using a benzodiazepine is: 1. Benzodiazepines interfere with talk therapy due to their amnestic effect 2. Benzodiazepines cause respiratory suppression increasing the severity of COPD exacerbations 3. Benzodiazepines at night in older patients are associated with falls and hip fractures 4. Benzodiazepines in recovering alcoholics are associated with alcohol relapse 5. Benzodiazepines are not indicated for acute insomnia
60 Benzos and hip fractures All benzos (and Z-drugs) associated with increased risk of falls and hip fractures Rate ratios of hip fracture were > 2.2 Polypharmacy and alcohol magnify the risk Finkle WD. Der JS. Greenland S. Adams JL. Ridgeway G. Blaschke T. Wang Z. Dell RM. VanRiper KB. Journal of the American Geriatrics Society. 59(10): , 2011 Oct.
61 Benzos and alcoholism Benzo use is not consistently associated with relapse to alcohol consumption Those with an addiction or first degree relative with an addiction prefer benzos to placebo, and escalate doses over time Those without an addiction prefer placebo to benzos, and self moderate use over time Benzos are rarely the primary addictive substance Woods, katz, winger Jama dec 16 vol 260 no p3476
62 Case 5
63 A 50 year-old man presents to the emergency room with alcohol on his breath and a variety of pills in his possession. Your nurse identifies two of the pills as alprazolam and oxymorphone. He has a respiratory rate of 4 breaths per minute and an oxygen saturation of 84%. His heart rate is 50 and his systolic blood pressure is 95 mm hg. He is responsive to noxious stimulus only. His pupils are small but not pinpoint. He appears cyanotic. You have no medical records on this man.
64 This is a 50 year-old man with an apparent overdose of alcohol, benzos, and opioids. Your next step is: 1. Give IV naloxone 2. Give IV flumazenil 3. Give both Flumazenil and Naloxone IV 4. Intubate
65 This is a 50 year-old man with an apparent overdose of alcohol, benzos, and opioids. Your next step is: 1. Give IV naloxone 2. Give IV flumazenil 3. Give both Flumazenil and Naloxone IV 4. Intubate
66 When to use flumazenil?
67 Limited use of flumazenil Reversal of brief procedural sedation Not in patients dependent on benzos, barbs or alcohol Not a diagnostic test! May precipitate seizures
68 Thank You!
1. According to recent US national estimates, which of the following substances is associated
 1 Chapter 36. Substance-Related, Self-Assessment Questions 1. According to recent US national estimates, which of the following substances is associated with the highest incidence of new drug initiates
1 Chapter 36. Substance-Related, Self-Assessment Questions 1. According to recent US national estimates, which of the following substances is associated with the highest incidence of new drug initiates
MOH CLINICAL PRACTICE GUIDELINES 2/2008 Prescribing of Benzodiazepines
 MOH CLINICL PRCTICE GUIELINES 2/2008 Prescribing of Benzodiazepines College of Family Physicians, Singapore cademy of Medicine, Singapore Executive summary of recommendations etails of recommendations
MOH CLINICL PRCTICE GUIELINES 2/2008 Prescribing of Benzodiazepines College of Family Physicians, Singapore cademy of Medicine, Singapore Executive summary of recommendations etails of recommendations
New York State Office of Alcoholism & Substance Abuse Services Addiction Services for Prevention, Treatment, Recovery
 New York State Office of Alcoholism & Substance Abuse Services Addiction Services for Prevention, Treatment, Recovery USING THE 48 HOUR OBSERVATION BED USING THE 48 HOUR OBSERVATION BED Detoxification
New York State Office of Alcoholism & Substance Abuse Services Addiction Services for Prevention, Treatment, Recovery USING THE 48 HOUR OBSERVATION BED USING THE 48 HOUR OBSERVATION BED Detoxification
INTOXICATED PATIENTS AND DETOXIFICATION
 VAMC Detoxification Decision Tree Updated May 2006 INTOXICATED PATIENTS AND DETOXIFICATION Patients often present for evaluation of substance use and possible detoxification. There are certain decisions
VAMC Detoxification Decision Tree Updated May 2006 INTOXICATED PATIENTS AND DETOXIFICATION Patients often present for evaluation of substance use and possible detoxification. There are certain decisions
The CCB Science 2 Service Distance Learning Program
 S2S 2055 DETOXIFICATION Module 1 Post-Test 1. A common use of a biochemical marker is. a. to support or refute other information that leads to proper diagnosis b. for forensic purposes c. in detecting
S2S 2055 DETOXIFICATION Module 1 Post-Test 1. A common use of a biochemical marker is. a. to support or refute other information that leads to proper diagnosis b. for forensic purposes c. in detecting
BENZODIAZEPINE CONSIDERATIONS IN WORKERS COMPENSATION: IMPLICATIONS FOR WORK DISABILITY AND CLAIM COSTS By: Michael Erdil MD, FACOEM
 3 rd Quarter 2015 BENZODIAZEPINE CONSIDERATIONS IN WORKERS COMPENSATION: IMPLICATIONS FOR WORK DISABILITY AND CLAIM COSTS By: Michael Erdil MD, FACOEM Introduction Benzodiazepines, sometimes called "benzos",
3 rd Quarter 2015 BENZODIAZEPINE CONSIDERATIONS IN WORKERS COMPENSATION: IMPLICATIONS FOR WORK DISABILITY AND CLAIM COSTS By: Michael Erdil MD, FACOEM Introduction Benzodiazepines, sometimes called "benzos",
ADVANCED BEHAVIORAL HEALTH, INC. Clinical Level of Care Guidelines - 2015
 The Clinical Level of Care Guidelines contained on the following pages have been developed as a guide to assist care managers, physicians and providers in making medical necessity decisions about the least
The Clinical Level of Care Guidelines contained on the following pages have been developed as a guide to assist care managers, physicians and providers in making medical necessity decisions about the least
Medical Malpractice Treatment Alprazolam benzodiazepine - A Case Study
 Improving Outcomes in Patients Who are Prescribed Alprazolam with Concurrent Use of Opioids Pik-Sai Yung, M.D. Staff Psychiatrist Center for Counseling at Walton Background and Rationale Alprazolam is
Improving Outcomes in Patients Who are Prescribed Alprazolam with Concurrent Use of Opioids Pik-Sai Yung, M.D. Staff Psychiatrist Center for Counseling at Walton Background and Rationale Alprazolam is
MEDICATION ABUSE IN OLDER ADULTS
 MEDICATION ABUSE IN OLDER ADULTS Clifford Milo Singer, MD Adjunct Professor, University of Maine, Orono ME Chief, Division of Geriatric Mental Health and Neuropsychiatry The Acadia Hospital and Eastern
MEDICATION ABUSE IN OLDER ADULTS Clifford Milo Singer, MD Adjunct Professor, University of Maine, Orono ME Chief, Division of Geriatric Mental Health and Neuropsychiatry The Acadia Hospital and Eastern
Care Manager Resources: Common Questions & Answers about Treatments for Depression
 Care Manager Resources: Common Questions & Answers about Treatments for Depression Questions about Medications 1. How do antidepressants work? Antidepressants help restore the correct balance of certain
Care Manager Resources: Common Questions & Answers about Treatments for Depression Questions about Medications 1. How do antidepressants work? Antidepressants help restore the correct balance of certain
GUIDELINES FOR COMMUNITY ALCOHOL DETOXIFICATION IN SHARED CARE
 GUIDELINES FOR COMMUNITY ALCOHOL DETOXIFICATION IN SHARED CARE Dr Millicent Chikoore MBBS MRCPsych Dr O Lagundoye MBBS MRCPsych Community based alcohol detoxification is a safe and effective option for
GUIDELINES FOR COMMUNITY ALCOHOL DETOXIFICATION IN SHARED CARE Dr Millicent Chikoore MBBS MRCPsych Dr O Lagundoye MBBS MRCPsych Community based alcohol detoxification is a safe and effective option for
Outpatient Treatment of Alcohol Withdrawal. Daniel Duhigg, DO, MBA
 Outpatient Treatment of Alcohol Withdrawal Daniel Duhigg, DO, MBA DSM V criteria for Alcohol Withdrawal A. Cessation or reduction of heavy/prolonged alcohol use B. 2 or more of the following in hours to
Outpatient Treatment of Alcohol Withdrawal Daniel Duhigg, DO, MBA DSM V criteria for Alcohol Withdrawal A. Cessation or reduction of heavy/prolonged alcohol use B. 2 or more of the following in hours to
Alcohol Withdrawal Syndrome & CIWA Assessment
 Alcohol Withdrawal Syndrome & CIWA Assessment Alcohol Withdrawal Syndrome is a set of symptoms that can occur when an individual reduces or stops alcoholic consumption after long periods of use. Prolonged
Alcohol Withdrawal Syndrome & CIWA Assessment Alcohol Withdrawal Syndrome is a set of symptoms that can occur when an individual reduces or stops alcoholic consumption after long periods of use. Prolonged
COUNTY OF LOS ANGELES - DEPARTMENT OF MENTAL HEALTH OFFICE OF THE MEDICAL DIRECTOR. 3.4 PARAMETERS FOR THE USE OF ANXIOLYTIC MEDICATIONS October 2014
 COUNTY OF LOS ANGELES - DEPARTMENT OF MENTAL HEALTH OFFICE OF THE MEDICAL DIRECTOR 3.4 PARAMETERS FOR THE USE OF ANXIOLYTIC MEDICATIONS October 2014 I. GENERAL CONSIDERATIONS A. Definition: Anxiolytic
COUNTY OF LOS ANGELES - DEPARTMENT OF MENTAL HEALTH OFFICE OF THE MEDICAL DIRECTOR 3.4 PARAMETERS FOR THE USE OF ANXIOLYTIC MEDICATIONS October 2014 I. GENERAL CONSIDERATIONS A. Definition: Anxiolytic
Alcohol Withdrawal. Introduction. Blood Alcohol Concentration. DSM-IV Criteria/Alcohol Abuse. Pharmacologic Effects of Alcohol
 Pharmacologic Effects of Alcohol Alcohol Withdrawal Kristi Theobald, Pharm.D., BCPS Therapeutics III Fall 2003 Inhibits glutamate receptor function (NMDA receptor) Inhibits excitatory neurotransmission
Pharmacologic Effects of Alcohol Alcohol Withdrawal Kristi Theobald, Pharm.D., BCPS Therapeutics III Fall 2003 Inhibits glutamate receptor function (NMDA receptor) Inhibits excitatory neurotransmission
Assessment and Management of Opioid, Benzodiazepine, and Sedative-Hypnotic Withdrawal
 Assessment and Management of Opioid, Benzodiazepine, and Sedative-Hypnotic Withdrawal Roger Cicala, M. D. Assistant Medical Director Tennessee Physician s Wellness Program Step 1 Don t 1 It is legal in
Assessment and Management of Opioid, Benzodiazepine, and Sedative-Hypnotic Withdrawal Roger Cicala, M. D. Assistant Medical Director Tennessee Physician s Wellness Program Step 1 Don t 1 It is legal in
Substance Use Learning Event Nov 3, 2015 Bill Bullock MD, CCFP
 Substance Use Learning Event Nov 3, 2015 Bill Bullock MD, CCFP Medical assessment of patient with Alcohol Use Disorder Identification patients suitable for home detox Process for referral to inpatient
Substance Use Learning Event Nov 3, 2015 Bill Bullock MD, CCFP Medical assessment of patient with Alcohol Use Disorder Identification patients suitable for home detox Process for referral to inpatient
Alcohol Withdrawal Recognition and Treatment
 Alcohol Withdrawal Recognition and Treatment Thomas Meyer BS EMS, MICP SREMSC Page 1 Purpose As EMTs a mantle of responsibility is placed upon you to ensure the safety and well-being of those in your charge
Alcohol Withdrawal Recognition and Treatment Thomas Meyer BS EMS, MICP SREMSC Page 1 Purpose As EMTs a mantle of responsibility is placed upon you to ensure the safety and well-being of those in your charge
Care Management Council submission date: August 2013. Contact Information
 Clinical Practice Approval Form Clinical Practice Title: Acute use of Buprenorphine for the Treatment of Opioid Dependence and Detoxification Type of Review: New Clinical Practice Revisions of Existing
Clinical Practice Approval Form Clinical Practice Title: Acute use of Buprenorphine for the Treatment of Opioid Dependence and Detoxification Type of Review: New Clinical Practice Revisions of Existing
Depression is a common biological brain disorder and occurs in 7-12% of all individuals over
 Depression is a common biological brain disorder and occurs in 7-12% of all individuals over the age of 65. Specific groups have a much higher rate of depression including the seriously medically ill (20-40%),
Depression is a common biological brain disorder and occurs in 7-12% of all individuals over the age of 65. Specific groups have a much higher rate of depression including the seriously medically ill (20-40%),
SUBSTANCE ABUSE SCREENING
 OVERVIEW Substance abuse in the elderly is a common problem that is frequently under- diagnosed by primary care doctors and families. Alcohol abuse is present in 10% to 15% of elderly individuals who seek
OVERVIEW Substance abuse in the elderly is a common problem that is frequently under- diagnosed by primary care doctors and families. Alcohol abuse is present in 10% to 15% of elderly individuals who seek
SPECIFICATION FOR THE LOCAL COMMISSIONED SERVICE FOR THE MANAGEMENT ALCOHOL MISUSE
 SPECIFICATION FOR THE LOCAL COMMISSIONED SERVICE FOR THE MANAGEMENT OF ALCOHOL MISUSE Date: March 2015 1 1. Introduction Alcohol misuse is a major public health problem in Camden with high rates of hospital
SPECIFICATION FOR THE LOCAL COMMISSIONED SERVICE FOR THE MANAGEMENT OF ALCOHOL MISUSE Date: March 2015 1 1. Introduction Alcohol misuse is a major public health problem in Camden with high rates of hospital
1. Which of the following SSRIs requires up to a 5-week washout period because of the
 1 Chapter 38. Major Depressive Disorders, Self-Assessment Questions 1. Which of the following SSRIs requires up to a 5-week washout period because of the long half-life of its potent active metabolite?
1 Chapter 38. Major Depressive Disorders, Self-Assessment Questions 1. Which of the following SSRIs requires up to a 5-week washout period because of the long half-life of its potent active metabolite?
A Growing Problem. Substance Abuse In The Eldery 1
 A Growing Problem Substance Abuse In The Eldery 1 A substantial and growing percentage of older adults misuse alcohol, prescription drugs, or other substances. The number of older adults in need of substance
A Growing Problem Substance Abuse In The Eldery 1 A substantial and growing percentage of older adults misuse alcohol, prescription drugs, or other substances. The number of older adults in need of substance
Co-morbid physical disorders e.g. HIV, hepatitis C, diabetes, hypertension. Medical students will gain knowledge in
 1.0 Introduction Medications are used in the treatment of drug, alcohol and nicotine dependence to manage withdrawal during detoxification, stabilisation and substitution as well as for relapse prevention,
1.0 Introduction Medications are used in the treatment of drug, alcohol and nicotine dependence to manage withdrawal during detoxification, stabilisation and substitution as well as for relapse prevention,
HIV Case Conference: Use of Common Benzodiazepines
 F/C AETC Faculty Psych Thursday, May 15, 2014 12:30 1:30pm (EDT) Didactic Presenter Patrick Marsh, MD University of South Florida Facilitator Debbie Cestaro Seifer, MS, RN University of South Florida HIV
F/C AETC Faculty Psych Thursday, May 15, 2014 12:30 1:30pm (EDT) Didactic Presenter Patrick Marsh, MD University of South Florida Facilitator Debbie Cestaro Seifer, MS, RN University of South Florida HIV
Alcohol Withdrawal Syndromes
 Alcohol Withdrawal Syndromes Should You Treat This Patient s Alcohol Withdrawal With Benzodiazepines?! Meta-analysis of RCTs of benzodiazepines for the treatment of alcohol withdrawal! 11 RCTs identified,
Alcohol Withdrawal Syndromes Should You Treat This Patient s Alcohol Withdrawal With Benzodiazepines?! Meta-analysis of RCTs of benzodiazepines for the treatment of alcohol withdrawal! 11 RCTs identified,
Triage, Assessment & Treatment
 Triage, Assessment & Treatment Launette Rieb, MSc, MD, CCFP, FCFP, dip ABAM Clinical Associate Professor, Dept. Family Practice, UBC Physician Director, St. Paul's Hospital Goldcorp Addiction Medicine
Triage, Assessment & Treatment Launette Rieb, MSc, MD, CCFP, FCFP, dip ABAM Clinical Associate Professor, Dept. Family Practice, UBC Physician Director, St. Paul's Hospital Goldcorp Addiction Medicine
Alcohol Abuse and Addiction Management Protocol
 Alcohol Abuse and Addiction Management Protocol All Team Members: Patient Self-Management Education and Support Alcohol is the most commonly abused drug in the United States. About 18 million people in
Alcohol Abuse and Addiction Management Protocol All Team Members: Patient Self-Management Education and Support Alcohol is the most commonly abused drug in the United States. About 18 million people in
Triage, Assessment & Treatment Methadone 101/Hospitalist Workshop
 Triage, Assessment & Treatment Methadone 101/Hospitalist Workshop Launette Rieb, MSc, MD, CCFP, FCFP Clinical Associate Professor, Dept. Family Practice UBC American Board of Addiction Medicine Certified
Triage, Assessment & Treatment Methadone 101/Hospitalist Workshop Launette Rieb, MSc, MD, CCFP, FCFP Clinical Associate Professor, Dept. Family Practice UBC American Board of Addiction Medicine Certified
Benzodiazepine Detoxification and Reduction of Long term Use
 Benzodiazepine Detoxification and Reduction of Long term Use Malcolm Lader 1 Model of general drug misuse and dependence. Tactical interventional options Social dimension Increasing breaking of social
Benzodiazepine Detoxification and Reduction of Long term Use Malcolm Lader 1 Model of general drug misuse and dependence. Tactical interventional options Social dimension Increasing breaking of social
Benzodiazepines: A Model for Central Nervous System (CNS) Depressants
 Depressants") Benzodiazepines: A Model for Central Nervous System (CNS) Depressants Objectives Summarize the basic mechanism by which benzodiazepines work in the brain. Describe two strategies for reducing and/or eliminating
Benzodiazepines: A Model for Central Nervous System (CNS) Depressants Objectives Summarize the basic mechanism by which benzodiazepines work in the brain. Describe two strategies for reducing and/or eliminating
Prescribing and Tapering Benzodiazepines
 E-Resource October, 2014 Prescribing and Tapering Benzodiazepines The use of benzodiazepines has grown over time and evidence has shown that long term use of these drugs has very little benefit with many
E-Resource October, 2014 Prescribing and Tapering Benzodiazepines The use of benzodiazepines has grown over time and evidence has shown that long term use of these drugs has very little benefit with many
COMMUNITY BUPRENORPHINE PRESCRIBING IN OPIATE DEPENDENCE
 COMMUNITY BUPRENORPHINE PRESCRIBING IN OPIATE DEPENDENCE INTRODUCTION High dose sublingual buprenorphine (Subutex) tablets are available in the following strengths 0.4 mg, 2 mg, and 8 mg. Suboxone tablets,
COMMUNITY BUPRENORPHINE PRESCRIBING IN OPIATE DEPENDENCE INTRODUCTION High dose sublingual buprenorphine (Subutex) tablets are available in the following strengths 0.4 mg, 2 mg, and 8 mg. Suboxone tablets,
UNDERSTANDING ADDICTION to BENZOS
 Alan Stevens, MSW, LSW, ACSW UNDERSTANDING ADDICTION to BENZOS UNDERSTANDING ADDICTION TO BENZOS Alan Stevens, MSW, LSW, ACSW Copyright 2013 Behavioral Health of the Palm Beaches Publisher: Mary Pomerantz
Alan Stevens, MSW, LSW, ACSW UNDERSTANDING ADDICTION to BENZOS UNDERSTANDING ADDICTION TO BENZOS Alan Stevens, MSW, LSW, ACSW Copyright 2013 Behavioral Health of the Palm Beaches Publisher: Mary Pomerantz
Adjunctive psychosocial intervention. Conditions requiring dose reduction. Immediate, peak plasma concentration is reached within 1 hour.
 Shared Care Guideline for Prescription and monitoring of Naltrexone Hydrochloride in alcohol dependence Author(s)/Originator(s): (please state author name and department) Dr Daly - Consultant Psychiatrist,
Shared Care Guideline for Prescription and monitoring of Naltrexone Hydrochloride in alcohol dependence Author(s)/Originator(s): (please state author name and department) Dr Daly - Consultant Psychiatrist,
Medical marijuana for pain and anxiety: A primer for methadone physicians. Meldon Kahan MD CPSO Methadone Prescribers Conference November 6, 2015
 Medical marijuana for pain and anxiety: A primer for methadone physicians Meldon Kahan MD CPSO Methadone Prescribers Conference November 6, 2015 Conflict of interest statement No conflict of interest to
Medical marijuana for pain and anxiety: A primer for methadone physicians Meldon Kahan MD CPSO Methadone Prescribers Conference November 6, 2015 Conflict of interest statement No conflict of interest to
Prescription Drug Addiction
 Prescription Drug Addiction Dr Gilbert Whitton FAChAM Clinical Director Drug & Alcohol Loddon Mallee Murray Medicare Local Deniliquin 14 th May 2014 Prescription Drug Addiction Overview History Benzodiazepines
Prescription Drug Addiction Dr Gilbert Whitton FAChAM Clinical Director Drug & Alcohol Loddon Mallee Murray Medicare Local Deniliquin 14 th May 2014 Prescription Drug Addiction Overview History Benzodiazepines
THE BASICS. Community Based Medically Assisted Alcohol Withdrawal. World Health Organisation 2011. The Issues 5/18/2011. RCGP Conference May 2011
 RCGP Conference May 2011 Community Based Medically Assisted Alcohol Withdrawal THE BASICS An option for consideration World Health Organisation 2011 Alcohol is the world s third largest risk factor for
RCGP Conference May 2011 Community Based Medically Assisted Alcohol Withdrawal THE BASICS An option for consideration World Health Organisation 2011 Alcohol is the world s third largest risk factor for
Elizabeth A. Crocco, MD Assistant Clinical Professor Chief, Division of Geriatric Psychiatry Department of Psychiatry and Behavioral Sciences Miller
 Elizabeth A. Crocco, MD Assistant Clinical Professor Chief, Division of Geriatric Psychiatry Department of Psychiatry and Behavioral Sciences Miller School of Medicine/University of Miami Question 1 You
Elizabeth A. Crocco, MD Assistant Clinical Professor Chief, Division of Geriatric Psychiatry Department of Psychiatry and Behavioral Sciences Miller School of Medicine/University of Miami Question 1 You
Michael Brennan, MA, LMHC Providence St. Peter Hospital Crisis Services
 Michael Brennan, MA, LMHC Providence St. Peter Hospital Crisis Services Welcome to the E.R.: Emergency: noun Webster 1. a sudden, urgent, usually unexpected occurrence or occasion requiring immediate action.
Michael Brennan, MA, LMHC Providence St. Peter Hospital Crisis Services Welcome to the E.R.: Emergency: noun Webster 1. a sudden, urgent, usually unexpected occurrence or occasion requiring immediate action.
Alcohol and nicotine are widely abused substances and are often used together One study showed that 15% of patients visiting a primary care practice
 Dr IM Joubert Alcohol and nicotine are widely abused substances and are often used together One study showed that 15% of patients visiting a primary care practice for any reason had either an at-risk pattern
Dr IM Joubert Alcohol and nicotine are widely abused substances and are often used together One study showed that 15% of patients visiting a primary care practice for any reason had either an at-risk pattern
Benzodiazepine & Z drugs withdrawal protocol
 Benzodiazepine & Z drugs withdrawal protocol Rationale The NSF for Older People has highlighted the issues of dependence, sedation and fall in the elderly when taking these types of medications. It has
Benzodiazepine & Z drugs withdrawal protocol Rationale The NSF for Older People has highlighted the issues of dependence, sedation and fall in the elderly when taking these types of medications. It has
Depression in Older Persons
 Depression in Older Persons How common is depression in later life? Depression affects more than 6.5 million of the 35 million Americans aged 65 or older. Most people in this stage of life with depression
Depression in Older Persons How common is depression in later life? Depression affects more than 6.5 million of the 35 million Americans aged 65 or older. Most people in this stage of life with depression
Prescription Drugs: Abuse and Addiction
 EAP Drug Free Workplace Newsletter March 2014 Prescription Drugs: Abuse and Addiction What are some of the commonly abused prescription drugs? Although many prescription drugs can be abused or misused,
EAP Drug Free Workplace Newsletter March 2014 Prescription Drugs: Abuse and Addiction What are some of the commonly abused prescription drugs? Although many prescription drugs can be abused or misused,
SUBSTANCE USE DISORDER SOCIAL DETOXIFICATION SERVICES [ASAM LEVEL III.2-D]
![SUBSTANCE USE DISORDER SOCIAL DETOXIFICATION SERVICES [ASAM LEVEL III.2-D]](/thumbs/27/9667060.jpg "SUBSTANCE USE DISORDER SOCIAL DETOXIFICATION SERVICES [ASAM LEVEL III.2-D]") SUBSTANCE USE DISORDER SOCIAL DETOXIFICATION SERVICES [ASAM LEVEL III.2-D] I. Definitions: Detoxification is the process of interrupting the momentum of compulsive drug and/or alcohol use in an individual
SUBSTANCE USE DISORDER SOCIAL DETOXIFICATION SERVICES [ASAM LEVEL III.2-D] I. Definitions: Detoxification is the process of interrupting the momentum of compulsive drug and/or alcohol use in an individual
DEPRESSION CARE PROCESS STEP EXPECTATIONS RATIONALE
 1 DEPRESSION CARE PROCESS STEP EXPECTATIONS RATIONALE ASSESSMENT/PROBLEM RECOGNITION 1. Did the staff and physician seek and document risk factors for depression and any history of depression? 2. Did staff
1 DEPRESSION CARE PROCESS STEP EXPECTATIONS RATIONALE ASSESSMENT/PROBLEM RECOGNITION 1. Did the staff and physician seek and document risk factors for depression and any history of depression? 2. Did staff
PHSW Procedural Sedation Post-Test Answer Key. For the following questions, circle the letter of the correct answer(s) or the word true or false.
 or the word true or false.") PHSW Procedural Sedation Post-Test Answer Key 1 1. Define Procedural (Conscious) Sedation: A medically controlled state of depressed consciousness where the patient retains the ability to continuously
PHSW Procedural Sedation Post-Test Answer Key 1 1. Define Procedural (Conscious) Sedation: A medically controlled state of depressed consciousness where the patient retains the ability to continuously
Management of benzodiazepine misuse
 York Service Management of benzodiazepine misuse Version 2 JT July 2013 page 1 background Note: not all those who use benzodiazepines are dependent, and not all those who are dependent will benefit from
York Service Management of benzodiazepine misuse Version 2 JT July 2013 page 1 background Note: not all those who use benzodiazepines are dependent, and not all those who are dependent will benefit from
Residential Sub-Acute Detoxification Guidelines
 I. Background Information A. Definition of Detoxification Residential Sub-Acute Detoxification Guidelines SAMSA s TIP #45, Detoxification and Substance Abuse Treatment: Treatment Improvement Protocols
I. Background Information A. Definition of Detoxification Residential Sub-Acute Detoxification Guidelines SAMSA s TIP #45, Detoxification and Substance Abuse Treatment: Treatment Improvement Protocols
How To Treat Alcohol Withdrawal In The Elderly
 ALCOHOL ABUSE AND WITHDRAWAL SYNDROME IN THE ELDERLY Colin Muscat Family Medicine Case 90 year old Female Lives with son on vacation Admitted for FTT Consult -? GARP Develops increasing confusion during
ALCOHOL ABUSE AND WITHDRAWAL SYNDROME IN THE ELDERLY Colin Muscat Family Medicine Case 90 year old Female Lives with son on vacation Admitted for FTT Consult -? GARP Develops increasing confusion during
Teen Misuse and Abuse of Alcohol and Prescription Drugs. Information for Parents
 Teen Misuse and Abuse of Alcohol and Prescription Drugs Information for Parents Terminology Misuse: Using a drug in a way in which it was not intended Example: Using a higher dose of medication than was
Teen Misuse and Abuse of Alcohol and Prescription Drugs Information for Parents Terminology Misuse: Using a drug in a way in which it was not intended Example: Using a higher dose of medication than was
75-09.1-08-02. Program criteria. A social detoxi cation program must provide:
 CHAPTER 75-09.1-08 SOCIAL DETOXIFICATION ASAM LEVEL III.2-D Section 75-09.1-08-01 De nitions 75-09.1-08-02 Program Criteria 75-09.1-08-03 Provider Criteria 75-09.1-08-04 Admission and Continued Stay Criteria
CHAPTER 75-09.1-08 SOCIAL DETOXIFICATION ASAM LEVEL III.2-D Section 75-09.1-08-01 De nitions 75-09.1-08-02 Program Criteria 75-09.1-08-03 Provider Criteria 75-09.1-08-04 Admission and Continued Stay Criteria
Opioid Treatment Services, Office-Based Opioid Treatment
 Optum 1 By United Behavioral Health U.S. Behavioral Health Plan, California Doing Business as OptumHealth Behavioral Solutions of California ( OHBS-CA ) 2015 Level of Care Guidelines Opioid Treatment Services,
Optum 1 By United Behavioral Health U.S. Behavioral Health Plan, California Doing Business as OptumHealth Behavioral Solutions of California ( OHBS-CA ) 2015 Level of Care Guidelines Opioid Treatment Services,
ALCOHOL DETOXIFICATION (IN-PATIENTS) PRESCRIBING GUIDELINE
 PRESCRIBING GUIDELINE") ALCOHOL DETOXIFICATION (IN-PATIENTS) PRESCRIBING GUIDELINE Authors Sponsor Responsible committee Ratified by Consultant Psychiatrist; Pharmacist Team Manager Medical Director Medicines Management Group
ALCOHOL DETOXIFICATION (IN-PATIENTS) PRESCRIBING GUIDELINE Authors Sponsor Responsible committee Ratified by Consultant Psychiatrist; Pharmacist Team Manager Medical Director Medicines Management Group
CHAPTER 5 MENTAL, BEHAVIOR AND NEURODEVELOPMENT DISORDERS (F01-F99) March 2014. 2014 MVP Health Care, Inc.
 March 2014. 2014 MVP Health Care, Inc.") CHAPTER 5 MENTAL, BEHAVIOR AND NEURODEVELOPMENT DISORDERS (F01-F99) March 2014 2014 MVP Health Care, Inc. CHAPTER 5 CHAPTER SPECIFIC CATEGORY CODE BLOCKS F01-F09 Mental disorders due to known physiological
CHAPTER 5 MENTAL, BEHAVIOR AND NEURODEVELOPMENT DISORDERS (F01-F99) March 2014 2014 MVP Health Care, Inc. CHAPTER 5 CHAPTER SPECIFIC CATEGORY CODE BLOCKS F01-F09 Mental disorders due to known physiological
Alcohol Dependence and Motivational Interviewing
 Alcohol Dependence and Motivational Interviewing Assessment of Alcohol Misuse Checklist Establish rapport patients are often resistant Longitudinal history of alcohol use Assess additional drug use Establish
Alcohol Dependence and Motivational Interviewing Assessment of Alcohol Misuse Checklist Establish rapport patients are often resistant Longitudinal history of alcohol use Assess additional drug use Establish
How To Know If You Should Be Treated
 Comprehensive ehavioral Care, Inc. delivery system that does not include sufficient alternatives to a particular LOC and a particular patient. Therefore, CompCare considers at least the following factors
Comprehensive ehavioral Care, Inc. delivery system that does not include sufficient alternatives to a particular LOC and a particular patient. Therefore, CompCare considers at least the following factors
SEDATIVE - HYPNOTICS. Gregory L. Kirk, MD Rocky Mountain Psychiatry Consultants, LLC 2036 E 17th Avenue Denver, CO 80220. Tuesday, June 19, 12
 SEDATIVE - HYPNOTICS Gregory L. Kirk, MD Rocky Mountain Psychiatry Consultants, LLC 2036 E 17th Avenue Denver, CO 80220 DRUG CLASSES OVERVIEW Benzodiazepines will be the main focus of the discussion. Benzodiazepines
SEDATIVE - HYPNOTICS Gregory L. Kirk, MD Rocky Mountain Psychiatry Consultants, LLC 2036 E 17th Avenue Denver, CO 80220 DRUG CLASSES OVERVIEW Benzodiazepines will be the main focus of the discussion. Benzodiazepines
Appendix to Tennessee Department of Health: Tennessee Clinical Practice Guidelines for Outpatient Management of Chronic Non- Malignant Pain
 Appendix to Tennessee Department of Health: Tennessee Clinical Practice Guidelines for Outpatient Management of Chronic Non- Malignant Pain Division of Workers Compensation 04.01.2015 Background Opioids
Appendix to Tennessee Department of Health: Tennessee Clinical Practice Guidelines for Outpatient Management of Chronic Non- Malignant Pain Division of Workers Compensation 04.01.2015 Background Opioids
Philip Moore DO, Toxicology Fellow, PinnacleHealth Toxicology Center Joanne Konick-McMahan RN MSRN, Staff RN, PinnacleHealth
 Philip Moore DO, Toxicology Fellow, PinnacleHealth Toxicology Center Joanne Konick-McMahan RN MSRN, Staff RN, PinnacleHealth I. II. Background A. AWS can occur in anyone who consumes alcohol B. Risk correlates
Philip Moore DO, Toxicology Fellow, PinnacleHealth Toxicology Center Joanne Konick-McMahan RN MSRN, Staff RN, PinnacleHealth I. II. Background A. AWS can occur in anyone who consumes alcohol B. Risk correlates
Treatment and Interventions for Opioid Addictions: Challenges From the Medical Director s Perspective
 Treatment and Interventions for Opioid Addictions: Challenges From the Medical Director s Perspective Dale K. Adair, MD Medical Director/Chief Psychiatric Officer OMHSAS 1 Treatment and Interventions for
Treatment and Interventions for Opioid Addictions: Challenges From the Medical Director s Perspective Dale K. Adair, MD Medical Director/Chief Psychiatric Officer OMHSAS 1 Treatment and Interventions for
KAP Keys. For Physicians. Based on TIP 40 Clinical Guidelines for the Use of Buprenorphine in the Treatment. of Opioid Addiction
 Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction Knowledge Application Program KAP Keys For Physicians Based on TIP 40 Clinical Guidelines for the Use of Buprenorphine
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction Knowledge Application Program KAP Keys For Physicians Based on TIP 40 Clinical Guidelines for the Use of Buprenorphine
EMS Branch / Office of the Medical Director. Active Seziures (d) Yes Yes Yes Yes. Yes Yes No No. Agitation (f) No Yes Yes No.
 Yes Yes Yes Yes. Yes Yes No No. Agitation (f) No Yes Yes No.") M07 Medications 2015-07-15 All ages EMS Branch / Office of the Medical Director Benzodiazepines Primary Intermediate Advanced Critical INDICATIONS Diazepam (c) Lorazepam (c) Midazolam (c) Intranasal Midazolam
M07 Medications 2015-07-15 All ages EMS Branch / Office of the Medical Director Benzodiazepines Primary Intermediate Advanced Critical INDICATIONS Diazepam (c) Lorazepam (c) Midazolam (c) Intranasal Midazolam
What Is Medically. Supervised Detoxification? Chapter 13
 Chapter 13 What Is Medically Supervised Detoxification? T I have been a heroin addict for three years and am desperately trying to stop. As the withdrawal symptoms are very severe, the muscle cramps, shakes,
Chapter 13 What Is Medically Supervised Detoxification? T I have been a heroin addict for three years and am desperately trying to stop. As the withdrawal symptoms are very severe, the muscle cramps, shakes,
Prescription Drug Abuse
 Prescription Drug Abuse Introduction Most people take medicines only for the reasons their health care providers prescribe them. But millions of people around the world have used prescription drugs for
Prescription Drug Abuse Introduction Most people take medicines only for the reasons their health care providers prescribe them. But millions of people around the world have used prescription drugs for
Management of dependence and withdrawal
 Section 9 Management of dependence and withdrawal SECTION CONTENTS 20. Physical dependence type 1 238 21. Physical dependence type 2 245 22. Physical dependence type 3 254 References 262 20 Physical dependence
Section 9 Management of dependence and withdrawal SECTION CONTENTS 20. Physical dependence type 1 238 21. Physical dependence type 2 245 22. Physical dependence type 3 254 References 262 20 Physical dependence
opiates alcohol 27 opiates and alcohol 30 April 2016 drug addiction signs 42 Ranked #1 123 Drug Rehab Centers in New Jersey 100 Top 10 380
 opiates alcohol 27 opiates and alcohol 30 April 2016 drug addiction signs 42 ed #1 123 Drug Rehab Centers in New Jersey 100 Top 10 380 effects of alcohol in the brain 100 Top 30 698 heroin addiction 100
opiates alcohol 27 opiates and alcohol 30 April 2016 drug addiction signs 42 ed #1 123 Drug Rehab Centers in New Jersey 100 Top 10 380 effects of alcohol in the brain 100 Top 30 698 heroin addiction 100
Performance Measurement for the Medicare and Medicaid Eligible (MME) Population in Connecticut Survey Analysis
 Population in Connecticut Survey Analysis") Performance Measurement for the Medicare and Medicaid Eligible (MME) Population in Connecticut Survey Analysis Methodology: 8 respondents The measures are incorporated into one of four sections: Highly
Performance Measurement for the Medicare and Medicaid Eligible (MME) Population in Connecticut Survey Analysis Methodology: 8 respondents The measures are incorporated into one of four sections: Highly
Case. History of psoriatic arthritis, htn, essential tremor Meds: propranolol, etodolac, etanercept No history of prior psychiatric disease.
 Case 48 year old man admitted complaining of hallucinations. Mild hallucinations for a year. Worsened tremor for 3 weeks and then markedly worse hallucinations last 2 days History of psoriatic arthritis,
Case 48 year old man admitted complaining of hallucinations. Mild hallucinations for a year. Worsened tremor for 3 weeks and then markedly worse hallucinations last 2 days History of psoriatic arthritis,
Algorithm for Initiating Antidepressant Therapy in Depression
 Algorithm for Initiating Antidepressant Therapy in Depression Refer for psychotherapy if patient preference or add cognitive behavioural office skills to antidepressant medication Moderate to Severe depression
Algorithm for Initiating Antidepressant Therapy in Depression Refer for psychotherapy if patient preference or add cognitive behavioural office skills to antidepressant medication Moderate to Severe depression
Review of Pharmacological Pain Management
 Review of Pharmacological Pain Management CHAMP Activities are possible with generous support from The Atlantic Philanthropies and The John A. Hartford Foundation The WHO Pain Ladder The World Health Organization
Review of Pharmacological Pain Management CHAMP Activities are possible with generous support from The Atlantic Philanthropies and The John A. Hartford Foundation The WHO Pain Ladder The World Health Organization
Psychotherapeutic Medications: What Every Counselor Should Know
 Psychotherapeutic Medications: What Every Counselor Should Know Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Antipsychotics/Neuroleptics Antipsychotics,
Psychotherapeutic Medications: What Every Counselor Should Know Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Antipsychotics/Neuroleptics Antipsychotics,
Symptom Based Alcohol Withdrawal Treatment
 Symptom Based Alcohol Withdrawal Treatment -Small Rural Hospital- Presenter CDR Dwight Humpherys, DO dwight.humpherys@ihs.gov Idaho State University Baccalaureate Nursing Program Lake Erie College of Osteopathic
Symptom Based Alcohol Withdrawal Treatment -Small Rural Hospital- Presenter CDR Dwight Humpherys, DO dwight.humpherys@ihs.gov Idaho State University Baccalaureate Nursing Program Lake Erie College of Osteopathic
Hospital Management of Opioid Dependence. Dependence. Disclosure. Pharmacologic Management. Methadone Utilization. Hospital Management of Opioid
 Disclosure Hospital Management of Opioid Dependence Attended Buprenorphine advisory board meeting (Schering Canada) May 2007, but personal honorarium/compensation was declined Dr. Alex Chan alexchchan@hotmail.com
Disclosure Hospital Management of Opioid Dependence Attended Buprenorphine advisory board meeting (Schering Canada) May 2007, but personal honorarium/compensation was declined Dr. Alex Chan alexchchan@hotmail.com
Treatment for Anxiety Disorders in Primary Care
 Treatment for Anxiety Disorders in Primary Care Dr Terence Leong Associate Consultant Dept of Psychological Medicine Research Clinical Care Education 1 1.1 Topic goes here Project number 14.12.08 Copyright
Treatment for Anxiety Disorders in Primary Care Dr Terence Leong Associate Consultant Dept of Psychological Medicine Research Clinical Care Education 1 1.1 Topic goes here Project number 14.12.08 Copyright
309.28 F43.22 Adjustment disorder with mixed anxiety and depressed mood Adjustment disorder with disturbance of conduct
 Description ICD-9-CM Code ICD-10-CM Code Adjustment reaction with adjustment disorder with depressed mood 309.0 F43.21 Adjustment disorder with depressed mood Adjustment disorder with anxiety 309.24 F43.22
Description ICD-9-CM Code ICD-10-CM Code Adjustment reaction with adjustment disorder with depressed mood 309.0 F43.21 Adjustment disorder with depressed mood Adjustment disorder with anxiety 309.24 F43.22
ALCOHOL AND OTHER DRUG WITHDRAWAL: PRACTICE GUIDELINES
 ALCOHOL AND OTHER DRUG WITHDRAWAL: PRACTICE GUIDELINES 2009 Pauline Kenny Amy Swan Lynda Berends Linda Jenner Barbara Hunter Janette Mugavin CHAPTER 12: BENZODIAZEPINE WITHDRAWAL 12 BENZODIAZEPINES These
ALCOHOL AND OTHER DRUG WITHDRAWAL: PRACTICE GUIDELINES 2009 Pauline Kenny Amy Swan Lynda Berends Linda Jenner Barbara Hunter Janette Mugavin CHAPTER 12: BENZODIAZEPINE WITHDRAWAL 12 BENZODIAZEPINES These
MOH CLINICAL PRACTICE GUIDELINES 6/2011 DEPRESSION
 MOH CLINICAL PRACTICE GUIDELINES 6/2011 DEPRESSION Executive summary of recommendations Details of recommendations can be found in the main text at the pages indicated. Clinical evaluation D The basic
MOH CLINICAL PRACTICE GUIDELINES 6/2011 DEPRESSION Executive summary of recommendations Details of recommendations can be found in the main text at the pages indicated. Clinical evaluation D The basic
Does This Hospital Serve Cocktails? Alcohol Withdrawal: A Nursing Perspective. Written and presented by: Susan Laffan, RN, CCHP-RN, CCHP-A
 Does This Hospital Serve Cocktails? Alcohol Withdrawal: A Nursing Perspective Written and presented by: Susan Laffan, RN, CCHP-RN, CCHP-A Disclaimer: This speaker has no financial disclaimers to report.
Does This Hospital Serve Cocktails? Alcohol Withdrawal: A Nursing Perspective Written and presented by: Susan Laffan, RN, CCHP-RN, CCHP-A Disclaimer: This speaker has no financial disclaimers to report.
Recognition and Treatment of Depression in Parkinson s Disease
 Recognition and Treatment of Depression in Parkinson s Disease Web Ross VA Pacific Islands Health Care System What is depression? Depression is a serious medical condition that affects a person s feelings,
Recognition and Treatment of Depression in Parkinson s Disease Web Ross VA Pacific Islands Health Care System What is depression? Depression is a serious medical condition that affects a person s feelings,
Alcohol use disorders: sample chlordiazepoxide dosing regimens for use in managing alcohol withdrawal
 Alcohol use disorders: sample chlordiazepoxide dosing regimens for use in managing alcohol withdrawal February 2010 NICE clinical guidelines 100 and 115 1 These sample chlordiazepoxide dosing regimens
Alcohol use disorders: sample chlordiazepoxide dosing regimens for use in managing alcohol withdrawal February 2010 NICE clinical guidelines 100 and 115 1 These sample chlordiazepoxide dosing regimens
GP Drug & Alcohol Supplement No.7 May 1997
 GP Drug & Alcohol Supplement No.7 May 1997 This is the seventh of the monthly Drug and Alcohol Supplements prepared for Central Coast GPs. Detoxification from Alcohol Dr Tony Gill Introduction The management
GP Drug & Alcohol Supplement No.7 May 1997 This is the seventh of the monthly Drug and Alcohol Supplements prepared for Central Coast GPs. Detoxification from Alcohol Dr Tony Gill Introduction The management
Withdrawal Symptoms: How Long Do They Last?
 Withdrawal Symptoms: How Long Do They Last? Posted by First Step Medical Detox on November 24, 2015 When considering stopping drugs or alcohol, many addicts and alcoholics are concerned about the withdrawal
Withdrawal Symptoms: How Long Do They Last? Posted by First Step Medical Detox on November 24, 2015 When considering stopping drugs or alcohol, many addicts and alcoholics are concerned about the withdrawal
Transitioning Chronic Pain Patients Out of the Hospital. Rosemary Quirk, MD, DTMH ACP, November 7, 2014
 Transitioning Chronic Pain Patients Out of the Hospital Rosemary Quirk, MD, DTMH ACP, November 7, 2014 Patients rate baseline chronic pain between 4/10-8/10 on clinic surveys This fact should fundamentally
Transitioning Chronic Pain Patients Out of the Hospital Rosemary Quirk, MD, DTMH ACP, November 7, 2014 Patients rate baseline chronic pain between 4/10-8/10 on clinic surveys This fact should fundamentally
MEDICALLY SUPERVISED OPIATE WITHDRAWAL FOR THE DEPENDENT PATIENT. An Outpatient Model
 MEDICALLY SUPERVISED OPIATE WITHDRAWAL FOR THE DEPENDENT PATIENT An Outpatient Model OBJECTIVE TO PRESENT A PROTOCOL FOR THE EVALUATION AND TREATMENT OF PATIENTS WHO ARE CHEMICALLY DEPENDENT ON OR SEVERLY
MEDICALLY SUPERVISED OPIATE WITHDRAWAL FOR THE DEPENDENT PATIENT An Outpatient Model OBJECTIVE TO PRESENT A PROTOCOL FOR THE EVALUATION AND TREATMENT OF PATIENTS WHO ARE CHEMICALLY DEPENDENT ON OR SEVERLY
DEPRESSION Depression Assessment PHQ-9 Screening tool Depression treatment Treatment flow chart Medications Patient Resource
 E-Resource March, 2015 DEPRESSION Depression Assessment PHQ-9 Screening tool Depression treatment Treatment flow chart Medications Patient Resource Depression affects approximately 20% of the general population
E-Resource March, 2015 DEPRESSION Depression Assessment PHQ-9 Screening tool Depression treatment Treatment flow chart Medications Patient Resource Depression affects approximately 20% of the general population
Considerations in Medication Assisted Treatment of Opiate Dependence. Stephen A. Wyatt, D.O. Dept. of Psychiatry Middlesex Hospital Middletown, CT
 Considerations in Medication Assisted Treatment of Opiate Dependence Stephen A. Wyatt, D.O. Dept. of Psychiatry Middlesex Hospital Middletown, CT Disclosures Speaker Panels- None Grant recipient - SAMHSA
Considerations in Medication Assisted Treatment of Opiate Dependence Stephen A. Wyatt, D.O. Dept. of Psychiatry Middlesex Hospital Middletown, CT Disclosures Speaker Panels- None Grant recipient - SAMHSA
Comprehensive Behavioral Care, Inc. Level of Care Guidelines Substance Abuse Children/Adolescents
 Medical Necessity In considering the appropriateness of any level of care, the four basic elements of Medical Necessity should be met: 1. A diagnosis as defined by standard diagnosis nomenclatures (DSM
Medical Necessity In considering the appropriateness of any level of care, the four basic elements of Medical Necessity should be met: 1. A diagnosis as defined by standard diagnosis nomenclatures (DSM
How To Know If You Can Get Help For An Addiction
 2014 FLORIDA SUBSTANCE ABUSE LEVEL OF CARE CLINICAL CRITERIA SUBSTANCE ABUSE LEVEL OF CARE CLINICAL CRITERIA Overview Psychcare strives to provide quality care in the least restrictive environment. An
2014 FLORIDA SUBSTANCE ABUSE LEVEL OF CARE CLINICAL CRITERIA SUBSTANCE ABUSE LEVEL OF CARE CLINICAL CRITERIA Overview Psychcare strives to provide quality care in the least restrictive environment. An
Benzodiazepines. And Sleeping Pills. Psychological Medicine
 Benzodiazepines And Sleeping Pills Psychological Medicine Introduction Benzodiazepines are a type of medication prescribed by doctors for its therapeutic actions in various conditions such as stress and
Benzodiazepines And Sleeping Pills Psychological Medicine Introduction Benzodiazepines are a type of medication prescribed by doctors for its therapeutic actions in various conditions such as stress and
Understanding Addiction: The Intersection of Biology and Psychology
 Understanding Addiction: The Intersection of Biology and Psychology Robert Heimer, Ph.D. Yale University School of Public Health Center for Interdisciplinary Research on AIDS New Haven, CT, USA November
Understanding Addiction: The Intersection of Biology and Psychology Robert Heimer, Ph.D. Yale University School of Public Health Center for Interdisciplinary Research on AIDS New Haven, CT, USA November
Benzodiazepine Overdose and Withdrawal Are Essentially Never Fatal 2014-11-10 by Zak Fallows CC-BY license, please reuse
 Benzodiazepine Overdose and Withdrawal Are Essentially Never Fatal 2014-11-10 by Zak Fallows CC-BY license, please reuse Caveat: Benzodiazepines are very dangerous when mixed with other sedating drugs
Benzodiazepine Overdose and Withdrawal Are Essentially Never Fatal 2014-11-10 by Zak Fallows CC-BY license, please reuse Caveat: Benzodiazepines are very dangerous when mixed with other sedating drugs
Reintegration. Recovery. Medication-Assisted Treatment for Alcohol Dependence. Reintegration. Resilience
 Reintegration Recovery Medication-Assisted Treatment for Alcohol Dependence Reintegration Resilience 02 How do you free yourself from the stress and risks of alcohol dependence? Most people cannot do it
Reintegration Recovery Medication-Assisted Treatment for Alcohol Dependence Reintegration Resilience 02 How do you free yourself from the stress and risks of alcohol dependence? Most people cannot do it
Alcohol Overuse and Abuse
 Alcohol Overuse and Abuse ACLI Medical Section CME Meeting February 23, 2015 Daniel Z. Lieberman, MD Professor and Vice Chair Department of Psychiatry George Washington University Alcohol OVERVIEW Definitions
Alcohol Overuse and Abuse ACLI Medical Section CME Meeting February 23, 2015 Daniel Z. Lieberman, MD Professor and Vice Chair Department of Psychiatry George Washington University Alcohol OVERVIEW Definitions
Depression Flow Chart
 Depression Flow Chart SCREEN FOR DEPRESSION ANNUALLY Assess for depression annually with the PHQ-9. Maintain a high index of suspicion in high risk older adults. Consider suicide risk and contributing
Depression Flow Chart SCREEN FOR DEPRESSION ANNUALLY Assess for depression annually with the PHQ-9. Maintain a high index of suspicion in high risk older adults. Consider suicide risk and contributing
Treatment of Opioid Dependence with Buprenorphine/Naloxone (Suboxone )
") Treatment of Opioid Dependence with Buprenorphine/Naloxone (Suboxone ) Elinore F. McCance-Katz, M.D., Ph.D. Professor and Chair, Addiction Psychiatry Virginia Commonwealth University Neurobiology of Opiate
Treatment of Opioid Dependence with Buprenorphine/Naloxone (Suboxone ) Elinore F. McCance-Katz, M.D., Ph.D. Professor and Chair, Addiction Psychiatry Virginia Commonwealth University Neurobiology of Opiate
THE OFFICE OF SUBSTANCE ABUSE SERVICES REQUIREMENTS FOR THE PROVISION OF RESIDENTIAL DETOXIFICATION SERVICES BY PROVIDERS FUNDED WITH DBHDS RESOURCES
 THE OFFICE OF SUBSTANCE ABUSE SERVICES REQUIREMENTS FOR THE PROVISION OF RESIDENTIAL DETOXIFICATION SERVICES BY PROVIDERS FUNDED WITH DBHDS RESOURCES PURPOSE: The goal of this document is to describe the
THE OFFICE OF SUBSTANCE ABUSE SERVICES REQUIREMENTS FOR THE PROVISION OF RESIDENTIAL DETOXIFICATION SERVICES BY PROVIDERS FUNDED WITH DBHDS RESOURCES PURPOSE: The goal of this document is to describe the
Pain Medication Taper Regimen Time frame to taper off 30-60 days
 Pain Medication Taper Regimen Time frame to taper off 30-60 days Medication to taper Taper Regimen Comments Methadone Taper by no more than 25% Morphine Taper by no more than 25% Tramadol Taper by no more
Pain Medication Taper Regimen Time frame to taper off 30-60 days Medication to taper Taper Regimen Comments Methadone Taper by no more than 25% Morphine Taper by no more than 25% Tramadol Taper by no more
Benzodiazepines. Understanding psychiatric medications. Information for consumers, families and friends. Titles in the
 Titles in the Understanding psychiatric medications series include: Antidepressants Antipsychotics Benzodiazepines Mood Stabilizers Understanding psychiatric medications Benzodiazepines For more information
Titles in the Understanding psychiatric medications series include: Antidepressants Antipsychotics Benzodiazepines Mood Stabilizers Understanding psychiatric medications Benzodiazepines For more information