Evaluation & Management. Guidelines. Presented by: Kristi A. Gutierrez CCS-P, CPC, CEMC
|
|
|
- Darren Fleming
- 10 years ago
- Views:
Transcription
1 Evaluation & Management Documentation and Coding Guidelines Presented by: Kristi A. Gutierrez CCS-P, CPC, CEMC

2 Objectives Participants will gain a working knowledge of Medicare s 1995 Evaluation & Management Documentation Guidelines. Participants will be able to apply the knowledge in everyday ysituations while seeing gpatients in order to utilize the correct level of Evaluation & Management Service and document that service to meet Medicare s Guidelines.

3 Agenda Medicare s 95 Documentation Guidelines (DG) for Providers New and Established Patient Visits Consultations Hospital Services C di E l i & M S i B d Coding an Evaluation & Management Service Based on Time

4 Overview Medicare s 1995 guidelines were developed to assist providers in choosing a level of service. Per Medicare s DG the visit is made up of three (3) key components: History; Physical Exam; and Mdi Medical Decision ii Mki Making.

5 What does Medicare need documented to bill a level of service? History Chief Complaint (CC) History of Present Illness (HPI) Review of Systems (ROS) Past, family and/or social history (PFSH) Examination Medical Decision Making (MDM)
 Review of Systems (ROS) Past, family and/or social")
6 Medical Decision Making (MDM) Medical Decision Making refers to the complexity of establishing a diagnosis and/or selecting a management option as measured by:

7 MDM Cont d Number of possible diagnoses and/or number of management options that must be considered; The amount and/or complexity of medical records, diagnostic tests, and/or other information that must be obtained, reviewed and analyzed; and The risk of significant complications, morbidity and/or mortality, as well as co-morbities, associated with the patients presenting problem(s), the diagnostic procedure(s) and/or the possible management options.
, the diagnostic procedure(s) and/or the possible management")
8 Number of Management Options/Diagnoses Self limited/minor (max 2 problems) or Est prob stable/improved = 1 point Established Problem worsening = 2 points New problem; no additional work up planned (max 1 prob) = 3 points New problem; additional work up pp planned (max 1 prob) = 4 points
 = 3 points New problem; additional work up pp planned (max 1")
9

10 Scoring the Number of Diagnoses or Management Options 1 point = Minimal 2 points 3 points 4 points or more = Limited = Multiple = Extensive

11 Amount or complexity of data reviewed Review and/or order of clinical lab tests =1 point (max) Review and/or order radiology tests =1 point (max) Review and/or order series tests t =1 point (max) Discussion of test results w/performing physician =1 point Decision to obtain old records and/or obtain history from someone other than the patient Review and summarization of old records and/or obtaining history from someone other than the patient and/or discussion i of case with another health care provider Independent visualization of image, tracing or specimen itself (not simply reviewing report) =1 point =2 points =2 points
 =1 point")
12
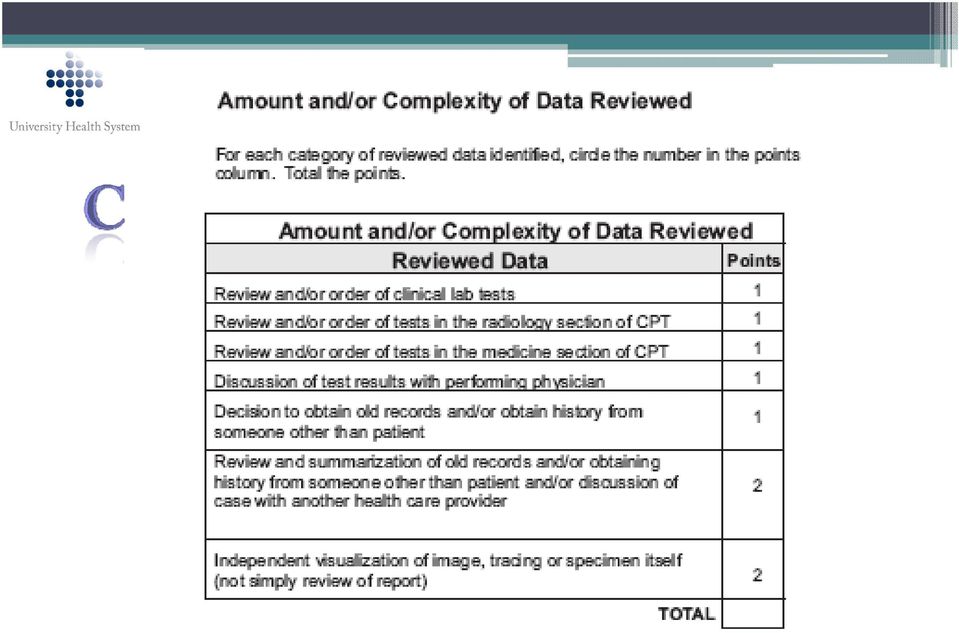
13 Scoring the Amount or Complexity of Data Reviewed 1 point = Minimal 2 points 3 points 4 points or more = Limited = Moderate = Extensive

14 Table of Risk Presenting Problem(s) Diagnostic Proc.Ordered Management Option(s) Selected One self limited or minor problem e.g. cold, insect bite, tinea corporis. 2 or more self-limited or minor problems 1 stable chronic illness Acute uncomp illness or inj 1 or more chronic illnesses w/ mild exacerbation 2 or more stable chronic illnesses 1 or more chronic illnesses w/ severe exacerbation Acute or chronic illness w/ threat to life/limb Lab tests req. venipuncture, chest X-rays rays, EKG-EEG EEG, UA, Ultrasound, e.g. echo, KOH prep. Physiologic tests not under stress Non-cardiovascular imaging Superficial needle biopsies Physiologic tests under stress Diagnostic endoscopies Deep needle biopsies Cardiovascular imaging Cardiac EP studies Diagnostic endo w/risks Discography Rest Gargles Elastic bandages Superficial dressings Level of Risk G l Minimal OTC drugs Minor surg no risks PT/OT IV fluids no additives Minor surg w/ risks Elective major surg Rx drug manage IV fluid w/ additives Elec. major surg w/ risks Emerg major surg Parenteral controlled Rx Low Moderate High **** This is an abbreviated Table of Risk. Use Medicare guidelines for full Table of Risk

15

16 Scoring the Table of Risk The highest level of risk from any column is the level to choose.

17 Scoring the Overall MDM Number Diagnoses or Management Options Amount or Complexity of Data Reviewed Risk MDM Level Minimal Minimal Minimal Straightforward Limited Limited Low Low Multiple Moderate Moderate Moderate Extensive Extensive High High Circle the score for each area of the MDM. Two (2) out of three (3) must meet or exceed the level chosen.

18

19 History The history portion of the chart is made up of four (4) components Chief Complaint (CC) History of Present Illness (HPI) Review of Systems (ROS) Past, Family and/or Social History (PFSH) The HPI, ROS and PFSH must all meet or exceed the scoring for the overall level chosen for the History portion of the chart.

20 Chief Complaint (CC) Every patient visit needs to list a CC. The CC is a concise statement describing the symptom, problem, condition, diagnosis, provider recommended return or other factor that is the reason for the encounter.

21 Scoring the CC Per Medicare s DG there is no scoring of the CC although the guidelines do state that the CC needs to be present.
22 History of Present Illness (HPI) The HPI is a chronological description of the development of the patient s present illness from the first sign and/or symptom or from the previous encounter to the present.
23 HPI Cont d Per Medicare DG the HPI includes: Location Quality Severity Duration Timing Context Modifying factors Associated signs and symptoms.
24 Scoring the HPI Count the number of elements the provider documented for the HPI. One (1) to three (3) elements constitutes a Brief HPI Four (4) or more elements constitutes an Extended HPI
25
26 Review of Systems (ROS) A ROS is an inventory of the body systems obtained through a series of questions seeking to identify signs and/or symptoms which the patient may be experiencing or has experienced. The ROS may be obtained dby ancillary staff or by a form the patient fills out (this may also be obtained by Medical Students.) It must be evidenced that it was reviewed by the provider and any information supplementing or confirming i the ROS must be documented. d
27 ROS Cont d Per Medicare DG the following systems are recognized: Constitutional Eyes Ears, nose, mouth, throat Cardiovascular Respiratory Gastrointestinal Genitourinary Musculoskeletal Integumentary Neurological Psychiatric Endocrine Hematologic/Lymphatic ti Allergic/Immunologic
28 ROS Cont d If a template is used to document the ROS, each box must be individually marked and all positive systems must be commented on. When documenting the patient record, the statement all other systems reviewed and negative is considered a complete ROS after commenting on the systems with positive responses. The statement non contributory is not sufficient i documentation of a ROS.
29 Scoring the ROS Count the number of elements documented in the ROS. One (1) element is a Problem Pertinent ROS Two (2) to nine (9) elements is an Extended ROS Ten (10) or more elements is a Complete ROS
30
31 Past, Family, Social History (PFSH) The PFSH consists of a review of three areas: Past history (the patient s past experiences with illnesses, surgeries, injuries, etc) Family history (the patient s review of significant family medical events) Social history (an age appropriate review of past and current activities) i i
32 PFSH Cont d The PFSH may be obtained by ancillary staff or through a form the patient fills out (this too may be obtained by a Medical Student.) It must be evidenced that it was reviewed by the provider and any information supplementing or confirming the PFSH must be documented.
33 Scoring the PFSH Count the number of elements documented for the PFSH One (1) element from any of the three (3) areas constitutes a Pertinent PFSH One (1) element from two (2) of the three (3) areas constitutes t a Complete PFSH for: established patients, ED, subsequent nursing facility care, domiciliary care (est. pt),or home care (est. pt) One (1) element from all of the three (3) areas constitutes a Complete PFSH for: new patients, hospital observation services, hospital inpatient services initial care, consults, comprehensive nursing facility evals, domiciliary care (new pt) or home care (new pt)
34
35 Scoring the Overall History HPI ROS PFSH Overall History Brief N/A N/A Problem Focused Brief Problem Pertinent N/A Expanded Problem Focused Extended Extended Pertinent Detailed Extended Complete Complete Comprehensive Circle the score in each column. All three (3) must meet or exceed the level of service chosen.
36
37 Exam Medicare s DG recognize the following body areas and organ systems: Head, including the face Neck Chest, including the breasts & axillae Abdomen Genitalia, groin, buttocks Back, including spine Each extremity Constitutional (e.g. vitals, appearance) Eyes Ears, nose, mouth and throat Cardiovascular Respiratory Gastrointestinal
38 Exam Cont d Genitourinary Musculoskeletal Skin Neurologic Psychiatric Hematologic/lymphatic/immunologic
39 Exam Cont d Specific abnormal and relevant negative findings of the affected area should be documented. A notation of abnormal without elaboration is not sufficient. A brief statement or notation noting negative or normal is sufficient for unaffected/asymptomatic areas.
40 Scoring the Exam Count the number of elements documented as examined by the provider: Problem Focused Examination - limited exam of affected body area or organ system (1) Expanded Problem Focused Examination - limited exam of affected body area or organ system and other symptomatic related organ systems (2-7) Detailed - extended exam of affected body areas or organ systems and other symptomatic or related organ systems (2-7) Comprehensive -a general multi-system t exam or complete exam of a single organ system (8 or more)
41
42 Scoring the Overall Chart New patients 3 out of 3 areas must meet or exceed the level of service chosen Etblihd Established patients t 2 out of 3 areas must meet or exceed the level of service chosen Consultations 3 out of 3 areas must meet or exceed the level of service chosen Initial Observation Services 3 out of 3 areas must meet or exceed the level of service chosen Initial Hospital Services 3 out of 3 areas must meet or exceed the level of service chosen
43
44 New Patient Office Visits New Patient A new patient is a patient who has not had a face to face encounter in the last three years: By the same provider By a provider of the same specialty in the same group
45 New Patients History Exam MDM CPT Problem Focused Problem Focused Straightforward Expanded Expanded Problem Focused Problem Focused Straightforward Detailed Detailed Low Comprehensive Comprehensive Moderate Comprehensive Comprehensive High ** All three must meet or exceed the level of service you have chosen
46
47 Established Patients History Exam MDM CPT NA NA NA Problem Focused Problem Focused Straightforward Expanded Problem Focused Expanded Problem Focused Low Detailed Detailed Moderate Comprehensive Comprehensive High ** Two out of the three elements must meet or exceed the level of service you have chosen
48 Consultations A consultation is distinguished from a visit because it is done at the request of a referring provider and the consultant prepares a report of his/her findings that is provided to the referring provider for his or her use in treatment of the patient.
49 The three R s of a Consultation Request - Documentation of the Request for consultation from the referring provider Reason - The Reason for the consult which must be medically reasonable and necessary Report - The written Report by the consultant which was provided back to the referring physician
50
51 Outpatient Consultations History Exam MDM CPT Problem Focused Problem Focused Straightforward Expanded Problem Expanded Problem Straightforward Focused Focused Detailed Detailed Low Comprehensive Comprehensive Moderate Comprehensive Comprehensive High **Three out of the three must meet or exceed the level of service you have chosen
52 Inpatient Consultations History Exam MDM CPT Problem Focused Problem Focused Straightforward hf Expanded Problem Focused Expanded Problem Focused Straightforward Detailed Detailed Low Comprehensive Comprehensive Moderate Comprehensive Comprehensive High **Three out of the three must meet or exceed the level of service you have chosen
53
54 Initial Hospital Observation Services History Exam MDM CPT Detailed/ Comprehensive Detailed/ Comprehensive Straightforward/ Low Comprehensive Comprehensive Moderate Comprehensive Comprehensive High **Three out of the three must meet or exceed the level of service you have chosen
55 Initial Hospital Services History Exam MDM CPT Detailed/ Detailed/ Straightforward/ Comprehensive Comprehensive Low Comprehensive Comprehensive Moderate Comprehensive Comprehensive High **Three out of the three must meet or exceed the level of service you have chosen
56
57 Subsequent Hospital Services History Exam MDM CPT Detailed/ Detailed/ Straightforward/ Comprehensive Comprehensive Low Comprehensive Comprehensive Moderate Comprehensive Comprehensive High **Two out of the three must meet or exceed the level of service you have chosen
58 Observation or Inpatient Care Services History Exam MDM CPT Detailed/ Comprehensive Detailed/ Comprehensive Straightforward/ Low Comprehensive Comprehensive Moderate Comprehensive Comprehensive High **Three out of the three must meet or exceed the level of service you have chosen These codes are for patients that are admitted and discharged on the same day.
59 Time Based Evaluation & Management Services Time may be the controlling factor when determining a level of service. In order to use time as the controlling factor, the provider must document the following: The total face-to-face time spent with the patient That over 50% of that time was spent in counseling or coordination of care for the patient The nature or content of the counseling and coordination of care
60 Time Based Evaluation & Management Services cont d Medicare expects that coding based on time is the exception to the rule not a regular occurrence. In order to determine what level of service was provided based on time, look at the average time spent for that level of service. For example, the average time spent (according to the CPT manual) for a is 25 minutes.
61 Now that I know how to document to support coding based on time. Where can I find the average time spent for each visit?
62
63 Thank You Please click here to take the quiz for this course.
1995 DOCUMENTATION GUIDELINES FOR EVALUATION AND MANAGEMENT SERVICES
 1995 DOCUMENTATION GUIDELINES FOR EVALUATION AND MANAGEMENT SERVICES I. INTRODUCTION WHAT IS DOCUMENTATION AND WHY IS IT IMPORTANT? Medical record documentation is required to record pertinent facts, findings,
1995 DOCUMENTATION GUIDELINES FOR EVALUATION AND MANAGEMENT SERVICES I. INTRODUCTION WHAT IS DOCUMENTATION AND WHY IS IT IMPORTANT? Medical record documentation is required to record pertinent facts, findings,
Empire BlueCross BlueShield Professional Reimbursement Policy
 Subject: Documentation and Reporting Guidelines for Evaluation and Management Services NY Policy: 0024 Effective: 12/01/2013-03/31/2014 Coverage is subject to the terms, conditions, and limitations of
Subject: Documentation and Reporting Guidelines for Evaluation and Management Services NY Policy: 0024 Effective: 12/01/2013-03/31/2014 Coverage is subject to the terms, conditions, and limitations of
E/M Documentation Auditors Worksheet
 E/M Documentation Auditors Worksheet Patient s ID/MR #: _ Y R Physician s Name and/or ID#: _ Resident yes no Staff Physician s Name and/or ID#(if resident is used): _ Date of Service Billed: Actual Date
E/M Documentation Auditors Worksheet Patient s ID/MR #: _ Y R Physician s Name and/or ID#: _ Resident yes no Staff Physician s Name and/or ID#(if resident is used): _ Date of Service Billed: Actual Date
2014 E&M Oncology Documentation & Coding Basics Working Smarter, Not Harder!
 2014 E&M Oncology Documentation & Coding Basics Working Smarter, Not Harder! West Virginia Oncology Society October 2, 2014 This presentation is offered as an educational tool. E&M Consulting Inc. does
2014 E&M Oncology Documentation & Coding Basics Working Smarter, Not Harder! West Virginia Oncology Society October 2, 2014 This presentation is offered as an educational tool. E&M Consulting Inc. does
Practical E/M Audit Form: Established Outpatient Visit (p.1)
") Patient: Name: Chart #: Date of visit: / / Reviewer: Date of review: / / Medical History Review Select the level corresponding to lowest of the components PFSH ROS HPI Level of History 5 2 elements 0 or
Patient: Name: Chart #: Date of visit: / / Reviewer: Date of review: / / Medical History Review Select the level corresponding to lowest of the components PFSH ROS HPI Level of History 5 2 elements 0 or
Step 2 Use the Medical Decision-Making Table
 Step 2 Use the Medical Decision-Making Table In Step 1, we determined the patient location and patient type. For most patient encounters, this determines the first 4 digits of the 5-digit CPT code. Three
Step 2 Use the Medical Decision-Making Table In Step 1, we determined the patient location and patient type. For most patient encounters, this determines the first 4 digits of the 5-digit CPT code. Three
E/M Learning Tips INTRODUCTION TO EVALUATION. Introduction to Evaluation and Management (E/M) Coding for the Child and Adolescent Psychiatrist
 Coding for the Child and Adolescent Psychiatrist") INTRODUCTION TO EVALUATION AND MANAGEMENT (E/M) CODING FOR THE CHILD AND ADOLESCENT PSYCHIATRIST Benjamin Shain, MD, PhD David Berland, MD Sherry Barron-Seabrook, MD Copyright 2012 by the American Academy
INTRODUCTION TO EVALUATION AND MANAGEMENT (E/M) CODING FOR THE CHILD AND ADOLESCENT PSYCHIATRIST Benjamin Shain, MD, PhD David Berland, MD Sherry Barron-Seabrook, MD Copyright 2012 by the American Academy
(For use with 1995 and 1997 CMS Documentation Guidelines for Evaluation & Management Coding )
") Appendix I: E/M Codebuilder (For use with 1995 and 1997 CMS Documentation Guidelines for Evaluation & Management Coding ) Introduction The evaluation and management (E/M) code reported to a third-party
Appendix I: E/M Codebuilder (For use with 1995 and 1997 CMS Documentation Guidelines for Evaluation & Management Coding ) Introduction The evaluation and management (E/M) code reported to a third-party
Medical Decision Making
 Disclaimer This presentation is intended only for use by Tulane University faculty, staff, and students. No copy or use of this presentation should occur without the permission of Tulane University. Tulane
Disclaimer This presentation is intended only for use by Tulane University faculty, staff, and students. No copy or use of this presentation should occur without the permission of Tulane University. Tulane
Current Procedural Terminology (CPT) Code Changes for 2013
 Code Changes for 2013") Current Procedural Terminology (CPT) Code Changes for 2013 For 2013 there have been major changes to the codes in the Psychiatry section of the AMA s Current Procedural Terminology, the codes that must
Current Procedural Terminology (CPT) Code Changes for 2013 For 2013 there have been major changes to the codes in the Psychiatry section of the AMA s Current Procedural Terminology, the codes that must
Patient Progress Note & Dictation Standard
 Objective: The patient progress note serves as a basis for planning patient care, documenting communication between the health care provider and any other health professional contributing to the patient's
Objective: The patient progress note serves as a basis for planning patient care, documenting communication between the health care provider and any other health professional contributing to the patient's
The file and the documentation should create a clean chronological record of the patient and their interactions with the provider.
 Documentation and Coding Guidelines for Athletic Trainers Table of Contents What is documentation and why is it important? Documentation and SOAP What do payers want and why? General guidelines of medical
Documentation and Coding Guidelines for Athletic Trainers Table of Contents What is documentation and why is it important? Documentation and SOAP What do payers want and why? General guidelines of medical
E&M Coding- It s All About The Documentation
 E&M Coding- It s All About The Documentation Presented for Anthem Blue Cross and Blue Shield By: Penny Osmon, BA, CPC Coding & Reimbursement Educator WI Medical Society Wisconsin Medical Society, Copyright
E&M Coding- It s All About The Documentation Presented for Anthem Blue Cross and Blue Shield By: Penny Osmon, BA, CPC Coding & Reimbursement Educator WI Medical Society Wisconsin Medical Society, Copyright
Documentation Guidelines for Physicians Interventional Pain Services
 Documentation Guidelines for Physicians Interventional Pain Services Pamela Gibson, CPC Assistant Director, VMG Coding Anesthesia and Surgical Divisions 343.8791 1 General Principles of Medical Record
Documentation Guidelines for Physicians Interventional Pain Services Pamela Gibson, CPC Assistant Director, VMG Coding Anesthesia and Surgical Divisions 343.8791 1 General Principles of Medical Record
A GUIDE TO EVALUATION & MANAGEMENT CODING AND DOCUMENTATION
 A GUIDE TO EVALUATION & MANAGEMENT CODING AND DOCUMENTATION Produced by ConnectiCare, Inc. in conjunction with its affiliate Group Health Incorporated TABLE OF CONTENTS Summary and Overview...Page 3 Part
A GUIDE TO EVALUATION & MANAGEMENT CODING AND DOCUMENTATION Produced by ConnectiCare, Inc. in conjunction with its affiliate Group Health Incorporated TABLE OF CONTENTS Summary and Overview...Page 3 Part
Let's Play a Game: Emergency Medical Documentation Coding for Emergency PHYSICIANS (not coders) Georgia College of Emergency Physicians June 5, 2012
 Georgia College of Emergency Physicians June 5, 2012") Let's Play a Game: Emergency Medical Documentation Coding for Emergency PHYSICIANS (not coders) Georgia College of Emergency Physicians June 5, 2012 Definitions: CPT: Current Procedural Terminology; every
Let's Play a Game: Emergency Medical Documentation Coding for Emergency PHYSICIANS (not coders) Georgia College of Emergency Physicians June 5, 2012 Definitions: CPT: Current Procedural Terminology; every
Forms designed to collect this information will help staff collect all pertinent information.
 1 CPT AUDIT TOOL INSTRUCTIONS The Nursing Consultants from the Public Health Nursing and Professional Development Unit based on multiple Evaluation & Management audits across the state have developed these
1 CPT AUDIT TOOL INSTRUCTIONS The Nursing Consultants from the Public Health Nursing and Professional Development Unit based on multiple Evaluation & Management audits across the state have developed these
Coding for the Internist: The Basics
 Coding for the Internist: The Basics Evaluation and management is the most important part of the practice for an internist and coding for these visits can have an important effect for the bottom line of
Coding for the Internist: The Basics Evaluation and management is the most important part of the practice for an internist and coding for these visits can have an important effect for the bottom line of
Evaluation and Management Services Guide
 DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services R Evaluation and Management Services Guide November 2014 / ICN: 006764 PREFACE This guide is offered as a reference tool
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services R Evaluation and Management Services Guide November 2014 / ICN: 006764 PREFACE This guide is offered as a reference tool
CPT Coding Compliance Program
 CPT Coding Compliance Program In December of 2008, in support of the Office of the Inspector General s initiative for Current Procedural Terminology ( CPT ) coding compliance, Empire Blue Cross Blue Shield
CPT Coding Compliance Program In December of 2008, in support of the Office of the Inspector General s initiative for Current Procedural Terminology ( CPT ) coding compliance, Empire Blue Cross Blue Shield
Maximizing Third Party Reimbursement Through Enhanced Medical Documentation and Coding. Installment One of the Webinar Series
 Maximizing Third Party Reimbursement Through Enhanced Medical Documentation and Coding Installment One of the Webinar Series Provides education and capacity building services to a variety of individuals
Maximizing Third Party Reimbursement Through Enhanced Medical Documentation and Coding Installment One of the Webinar Series Provides education and capacity building services to a variety of individuals
Evaluation and Management Services Guide
 DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services R Evaluation and Management Services Guide December 2010 / ICN: 006764 PREFACE This guide is offered as a reference tool
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services R Evaluation and Management Services Guide December 2010 / ICN: 006764 PREFACE This guide is offered as a reference tool
Strategies for Coding, Billing and Getting Paid Appropriately
 Strategies for Coding, Billing and Getting Paid Appropriately CONTENTS A Guide for Family Physicians Introduction 2 1 Tools of the Trade 5 2 The Reimbursement Team 7 3 Documentation of Services 13 4 Coding
Strategies for Coding, Billing and Getting Paid Appropriately CONTENTS A Guide for Family Physicians Introduction 2 1 Tools of the Trade 5 2 The Reimbursement Team 7 3 Documentation of Services 13 4 Coding
Coding Flow Charts. What is Medical Coding? 9/17/2012. Diagnosis Codes ICD-9-CM. Volume 1 & 2* Speakers
 Speakers Welcome to Coding Basics - Essentials You Must Know to Thrive Brought to you by ACC s Cardiovascular Administrator Work Group Presented by the ACC in conjunction with the MedAxiom Business Office
Speakers Welcome to Coding Basics - Essentials You Must Know to Thrive Brought to you by ACC s Cardiovascular Administrator Work Group Presented by the ACC in conjunction with the MedAxiom Business Office
NHIC, Corp. Evaluation & Management (E/M) Coding Requirements
 Coding Requirements") Evaluation & Management (E/M) Coding Requirements Medical Review offers this article and the attached worksheet to assist you in understanding the documentation and policy requirements associated with
Evaluation & Management (E/M) Coding Requirements Medical Review offers this article and the attached worksheet to assist you in understanding the documentation and policy requirements associated with
Compliance Department Overview of Non-Physician Practitioner Guidelines 11/2010
 Compliance Department Overview of Non-Physician Practitioner Guidelines 11/2010 The Role of the Compliance Department The Compliance Department assists physicians and other practitioners with complying
Compliance Department Overview of Non-Physician Practitioner Guidelines 11/2010 The Role of the Compliance Department The Compliance Department assists physicians and other practitioners with complying
NEW YORK STATE MEDICAID PROGRAM PHYSICIAN PROCEDURE CODES. SECTION 2 MEDICINE, DRUGS and DRUG ADMINISTRATION
 NEW YORK STATE MEDICAID PROGRAM PHYSICIAN PROCEDURE CODES SECTION 2 MEDICINE, DRUGS and DRUG ADMINISTRATION Table of Contents GENERAL RULES AND INFORMATION... 3 MMIS MODIFIERS... 15 EVALUATION AND MANAGEMENT
NEW YORK STATE MEDICAID PROGRAM PHYSICIAN PROCEDURE CODES SECTION 2 MEDICINE, DRUGS and DRUG ADMINISTRATION Table of Contents GENERAL RULES AND INFORMATION... 3 MMIS MODIFIERS... 15 EVALUATION AND MANAGEMENT
PROFESSIONAL BILLING COMPLIANCE TRAINING PROGRAM MODULE 2 EVALUATION AND MANAGEMENT (E/M) SERVICES
 SERVICES") PROFESSIONAL BILLING COMPLIANCE TRAINING PROGRAM MODULE 2 EVALUATION AND MANAGEMENT (E/M) SERVICES Evaluation and Management (E/M) Documentation E/M Documentation Background: Physician payment for inpatient
PROFESSIONAL BILLING COMPLIANCE TRAINING PROGRAM MODULE 2 EVALUATION AND MANAGEMENT (E/M) SERVICES Evaluation and Management (E/M) Documentation E/M Documentation Background: Physician payment for inpatient
POLICY-DOCUMENTATION GUIDELINES
 POLICY-DOCUMENTATION GUIDELINES Introduction What is documentation & why is it important? Medical record documentation is required to record pertinent facts, findings, and observations about an individual's
POLICY-DOCUMENTATION GUIDELINES Introduction What is documentation & why is it important? Medical record documentation is required to record pertinent facts, findings, and observations about an individual's
Compliant Documentation in the EHR. Introduction
 Compliant Documentation in the EHR Lynn Myers MD, CPC, CHC 1 Introduction The perspective of a physician and a coder Going over to the dark side of medicine Death by a thousand cuts? Why it helps coders
Compliant Documentation in the EHR Lynn Myers MD, CPC, CHC 1 Introduction The perspective of a physician and a coder Going over to the dark side of medicine Death by a thousand cuts? Why it helps coders
2 nd Floor CS&E Building A current UMHS identification badge is required to obtain medical records
 Location Hours 2 nd Floor CS&E Building A current UMHS identification badge is required to obtain medical records The Health Information Services Department is open to the public Monday through Friday,
Location Hours 2 nd Floor CS&E Building A current UMHS identification badge is required to obtain medical records The Health Information Services Department is open to the public Monday through Friday,
NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES
 NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES Table of Contents GENERAL INFORMATION... 3 SERVICES PROVIDED IN ARTICLE 28 FACILITIES... 4 MMIS MODIFIERS... 4 MEDICINE SECTION... 7 GENERAL INFORMATION
NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES Table of Contents GENERAL INFORMATION... 3 SERVICES PROVIDED IN ARTICLE 28 FACILITIES... 4 MMIS MODIFIERS... 4 MEDICINE SECTION... 7 GENERAL INFORMATION
Selection of Evaluation and Management Service Codes 1995 E&M Guidelines. Laura Sullivan, CPC Coordinator Corporate Compliance Auditing & Education
 Selection of Evaluation and Management Service Codes 1995 E&M Guidelines Laura Sullivan, CPC Coordinator Corporate Compliance Auditing & Education 1 Legal Stuff The information provided here is personal
Selection of Evaluation and Management Service Codes 1995 E&M Guidelines Laura Sullivan, CPC Coordinator Corporate Compliance Auditing & Education 1 Legal Stuff The information provided here is personal
E/M and Psychotherapy Coding Algorithm
 Inpatient PHP Outpatient E/M and Psychotherapy Coding Algorithm CPT five-digit codes, descriptions, and other data only are copyright 2012 by the American Medical Association (AMA). All Rights Reserved.
Inpatient PHP Outpatient E/M and Psychotherapy Coding Algorithm CPT five-digit codes, descriptions, and other data only are copyright 2012 by the American Medical Association (AMA). All Rights Reserved.
DOCUMENTATION OF MEDICAL NOTES (Based on 1995 Guidelines)
") DOCUMENTATION OF MEDICAL NOTES (Based on 1995 Guidelines) General Principles Medical records are legal documents. All notes must be legible and complete. The auditor will decide if they are legible. All
DOCUMENTATION OF MEDICAL NOTES (Based on 1995 Guidelines) General Principles Medical records are legal documents. All notes must be legible and complete. The auditor will decide if they are legible. All
Codes and Documentation for Evaluation and Management Services
 4 Codes and Documentation for Evaluation and Management Services The evaluation and management (E/M) codes were introduced in the 1992 update to the fourth edition of Physicians Current Procedural Terminology
4 Codes and Documentation for Evaluation and Management Services The evaluation and management (E/M) codes were introduced in the 1992 update to the fourth edition of Physicians Current Procedural Terminology
Workbook STD Clinic Billing Coding Evaluation & Management Visits
 Workbook STD Clinic Billing Coding Evaluation & Management Visits Developed by the University of Rochester Center for Health & Behavioral Training Capacity Building Assistance (CBA) Adapted from 1997 CMS
Workbook STD Clinic Billing Coding Evaluation & Management Visits Developed by the University of Rochester Center for Health & Behavioral Training Capacity Building Assistance (CBA) Adapted from 1997 CMS
NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES
 NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES Table of Contents GENERAL INFORMATION... 3 STATE DEPARTMENT OF HEALTH CONDITIONS FOR PAYMENT... 6 PRACTITIONER SERVICES PROVIDED IN HOSPITALS...
NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES Table of Contents GENERAL INFORMATION... 3 STATE DEPARTMENT OF HEALTH CONDITIONS FOR PAYMENT... 6 PRACTITIONER SERVICES PROVIDED IN HOSPITALS...
E/M LEVEL WORKSHEET. Category. Subcategory (if applicable) (new/established, etc.)
 (new/established, etc.)") E/M LEVEL WORKSHEET STEP 1 : IDENTIFY THE CATEGORY AND SUBCATEGORY OF SERVICE Carefully read the documentation. Using the Table of Contents, identify the appropriate category/subcategory. Category Subcategory
E/M LEVEL WORKSHEET STEP 1 : IDENTIFY THE CATEGORY AND SUBCATEGORY OF SERVICE Carefully read the documentation. Using the Table of Contents, identify the appropriate category/subcategory. Category Subcategory
Medical Compliance with Billing and Coding 2013: Will your Records Survive an Audit from a Third Party Payer or the OIG?
 Medical Compliance with Billing and Coding 2013: Will your Records Survive an Audit from a Third Party Payer or the OIG? Michael J. McGovern, OD, FAAO; Richard Soden, OD, FAAO American Academy of Optometry
Medical Compliance with Billing and Coding 2013: Will your Records Survive an Audit from a Third Party Payer or the OIG? Michael J. McGovern, OD, FAAO; Richard Soden, OD, FAAO American Academy of Optometry
TRANSITIONAL CARE MANAGEMENT CHECKLIST
 _ Name of TCM Qualified Healthcare Professional (QHP) Provider: Discharge Date: TCM End Date (29 days after day of discharge): TCM services are for an established patient whose medical and/or psychosocial
_ Name of TCM Qualified Healthcare Professional (QHP) Provider: Discharge Date: TCM End Date (29 days after day of discharge): TCM services are for an established patient whose medical and/or psychosocial
Emory Standards For Documenting, Coding, & Billing Professional Services TABLE OF CONTENTS
 TABLE OF CONTENTS 1. Medical Record Documentation 2 2. Evaluation and Management Documentation Guidelines for Billing 3 Key Component: History 4 Key Component: Examination 6 Key Component: Medical Decision
TABLE OF CONTENTS 1. Medical Record Documentation 2 2. Evaluation and Management Documentation Guidelines for Billing 3 Key Component: History 4 Key Component: Examination 6 Key Component: Medical Decision
Best Practices in Billing and Coding. Janet Bull, MD, FAAHPM, HMDC Four Seasons
 Best Practices in Billing and Coding Janet Bull, MD, FAAHPM, HMDC Four Seasons Disclosure o Salix Pharm Scientific Advisory Board o Grant Funding CMS Innovations, HRSA, AHRQ Disclaimer o o o The information
Best Practices in Billing and Coding Janet Bull, MD, FAAHPM, HMDC Four Seasons Disclosure o Salix Pharm Scientific Advisory Board o Grant Funding CMS Innovations, HRSA, AHRQ Disclaimer o o o The information
2013 PSYCHIATRY CPT CODES
 2013 PSYCHIATRY CPT CODES Benjamin Shain, MD, PhD David Berland, MD Sherry Barron-Seabrook, MD Copyright 2012 by the American Academy of Child and Adolescent Psychiatry OVERVIEW 2 The Old Psychiatry Codes
2013 PSYCHIATRY CPT CODES Benjamin Shain, MD, PhD David Berland, MD Sherry Barron-Seabrook, MD Copyright 2012 by the American Academy of Child and Adolescent Psychiatry OVERVIEW 2 The Old Psychiatry Codes
Non-Physician Practitioner Services Coding & Reporting. Karla R. Peter, RHIT, CCS, CCS-P, CPC Avera Health September 6, 2013
 Non-Physician Practitioner Services Coding & Reporting Karla R. Peter, RHIT, CCS, CCS-P, CPC Avera Health September 6, 2013 Medical Necessity Overarching Criterion Medicare Claims Processing Manual, Chapter
Non-Physician Practitioner Services Coding & Reporting Karla R. Peter, RHIT, CCS, CCS-P, CPC Avera Health September 6, 2013 Medical Necessity Overarching Criterion Medicare Claims Processing Manual, Chapter
E/M Components EVALUATION AND MANAGEMENT (E/M) CODING FOR CHILD AND ADOLESCENT PSYCHIATRIC OUTPATIENTS OVERVIEW
 CODING FOR CHILD AND ADOLESCENT PSYCHIATRIC OUTPATIENTS OVERVIEW") EVALUATION AND MANAGEMENT (E/M) CODING FOR CHILD AND ADOLESCENT PSYCHIATRIC OUTPATIENTS Benjamin Shain, MD, PhD David Berland, MD Sherry Barron-Seabrook, MD Copyright 2012 by the American Academy of Child
EVALUATION AND MANAGEMENT (E/M) CODING FOR CHILD AND ADOLESCENT PSYCHIATRIC OUTPATIENTS Benjamin Shain, MD, PhD David Berland, MD Sherry Barron-Seabrook, MD Copyright 2012 by the American Academy of Child
Evaluation & Management Place of Service
 Evaluation & Management Place of Service Hoda Henein, CHBME, CP President & CEO, Active Management A Practice Management Consulting and Billing Company Fellow, Speaker, Billing & Coding Advisor American
Evaluation & Management Place of Service Hoda Henein, CHBME, CP President & CEO, Active Management A Practice Management Consulting and Billing Company Fellow, Speaker, Billing & Coding Advisor American
Stuart B Black MD, FAAN Chief of Neurology Co-Medical Director: Neuroscience Center Baylor University Medical Center at Dallas
 Billing and Coding in Neurology and Headache Stuart B Black MD, FAAN Chief of Neurology Co-Medical Director: Neuroscience Center Baylor University Medical Center at Dallas CPT Codes vs. ICD Codes Category
Billing and Coding in Neurology and Headache Stuart B Black MD, FAAN Chief of Neurology Co-Medical Director: Neuroscience Center Baylor University Medical Center at Dallas CPT Codes vs. ICD Codes Category
Physician Practice E/M Guidelines
 Physician Practice E/M Guidelines Audio Seminar/Webinar November 10, 2009 Practical Tools for Seminar Learning Copyright 2009 American Health Information Management Association. All rights reserved. Disclaimer
Physician Practice E/M Guidelines Audio Seminar/Webinar November 10, 2009 Practical Tools for Seminar Learning Copyright 2009 American Health Information Management Association. All rights reserved. Disclaimer
Optimizing Revenue with Correct Documentation and Coding
 Optimizing Revenue with Correct Documentation and Coding OAAPN Sally Streiber, BS, MBA, CPC, CEMC Christine Williams, MSN, CNP, FAANP October 22, 2015 Objectives- Agenda Review OAAPN Reimbursement Goals,
Optimizing Revenue with Correct Documentation and Coding OAAPN Sally Streiber, BS, MBA, CPC, CEMC Christine Williams, MSN, CNP, FAANP October 22, 2015 Objectives- Agenda Review OAAPN Reimbursement Goals,
Introduction to Coding. Todd W. Frieze, MD, FACP, FACE, ECNU,CEC Member, AACE Socioeconomic & Member Advocacy Committee
 Introduction to Coding Todd W. Frieze, MD, FACP, FACE, ECNU,CEC Member, AACE Socioeconomic & Member Advocacy Committee Disclaimer Please note that any AACE proprietary information or intellectual property
Introduction to Coding Todd W. Frieze, MD, FACP, FACE, ECNU,CEC Member, AACE Socioeconomic & Member Advocacy Committee Disclaimer Please note that any AACE proprietary information or intellectual property
E/M coding workshop. The risk of not getting it right. PAMELA PULLY CPC, CPMA BILLING/CLAIMS SUPERVISOR GENESEE HEALTH SYSTEM
 E/M coding workshop. The risk of not getting it right. PAMELA PULLY CPC, CPMA BILLING/CLAIMS SUPERVISOR GENESEE HEALTH SYSTEM Disclaimer This information is accurate as of December 1, 2014 and is designed
E/M coding workshop. The risk of not getting it right. PAMELA PULLY CPC, CPMA BILLING/CLAIMS SUPERVISOR GENESEE HEALTH SYSTEM Disclaimer This information is accurate as of December 1, 2014 and is designed
Improving the Quality of Care for Prevention and Treatment of Childhood Obesity
 HFS Billing and Coding Guidance for Pediatric Obesity Prevention & Management Improving the Quality of Care for Prevention and Treatment of Childhood Obesity LaTrece Freeman-Baker, CPC, CPC-I, CPCO, CPMA
HFS Billing and Coding Guidance for Pediatric Obesity Prevention & Management Improving the Quality of Care for Prevention and Treatment of Childhood Obesity LaTrece Freeman-Baker, CPC, CPC-I, CPCO, CPMA
Determine the Appropriate Level E/M Code Based on the Encounter
 Determine the Appropriate Level E/M Code Based on the Encounter Jeffrey D. Lehrman, DPM, FACFAS, FASPS, FAPWH APMA Coding Committee Expert Panelist, Codingline.com Fellow, American Academy of Podiatric
Determine the Appropriate Level E/M Code Based on the Encounter Jeffrey D. Lehrman, DPM, FACFAS, FASPS, FAPWH APMA Coding Committee Expert Panelist, Codingline.com Fellow, American Academy of Podiatric
Hot Topics in E & M Coding for the ID Practice
 Hot Topics in E & M Coding for the ID Practice IDSA Webinar February, 2010 Barb Pierce, CCS-P, ACS-EM Consulting, LLC [email protected] www.barbpiercecodingandconsulting.com Disclaimer This information
Hot Topics in E & M Coding for the ID Practice IDSA Webinar February, 2010 Barb Pierce, CCS-P, ACS-EM Consulting, LLC [email protected] www.barbpiercecodingandconsulting.com Disclaimer This information
Disclaimers/Confessions. Best Practices for Eye Care Staff Related to Medical Records. Disclaimers/Confessions, con. National Guidelines for Records
 Disclaimers/Confessions Best Practices for Eye Care Staff Related to Medical Records Presented by. Charles B. Brownlow, O.D., F.A.A.O. Medical Records Consultant PMI, LLC DrBrownlow@PMI EYES.com This presentation
Disclaimers/Confessions Best Practices for Eye Care Staff Related to Medical Records Presented by. Charles B. Brownlow, O.D., F.A.A.O. Medical Records Consultant PMI, LLC DrBrownlow@PMI EYES.com This presentation
CPT 99213. The Key to E/M Documentation (and Reimbursement)? Rick Horsman DPM Olympia, WA
? Rick Horsman DPM Olympia, WA") CPT 99213 The Key to E/M Documentation (and Reimbursement)? Rick Horsman DPM Olympia, WA CodinglinePRINT www.codingline.com/silver.htm www.apmacodingrc.com COGNITIVE VS. PROCEDURAL SERVICES Cognitive Services
CPT 99213 The Key to E/M Documentation (and Reimbursement)? Rick Horsman DPM Olympia, WA CodinglinePRINT www.codingline.com/silver.htm www.apmacodingrc.com COGNITIVE VS. PROCEDURAL SERVICES Cognitive Services
99213 or 99214 Visit?
 JUST HOW MUCH DOCUMENTATION IS REQUIRED 1 99213 or 99214 Visit? Presented by: Leslie C. Bembry CPC Coding and Compliance Manager Montgomery Hospital Health Systems Fornance Physician Services Inc. Norristown
JUST HOW MUCH DOCUMENTATION IS REQUIRED 1 99213 or 99214 Visit? Presented by: Leslie C. Bembry CPC Coding and Compliance Manager Montgomery Hospital Health Systems Fornance Physician Services Inc. Norristown
Evaluation and Management Services
 Evaluation and Management Services Sticking to the Basics to Avoid Unnecessary Audits October 30, 2014 Disclaimer The purpose of this publication is to accompany a lecture prepared and presented by GILL
Evaluation and Management Services Sticking to the Basics to Avoid Unnecessary Audits October 30, 2014 Disclaimer The purpose of this publication is to accompany a lecture prepared and presented by GILL
E/M Documentation: Deal or No Deal? Documentation Guidelines. Documentation Elements 3/25/2013
 E/M Documentation: Deal or No Deal? Presented by Maggie Mac, CPC, CEMC, CHC, CMM, ICCE and Dennis Mihale, MD Documentation Guidelines 1995 vs 1997 guidelines 95 for? 97 for? General Multi-System? Specialty
E/M Documentation: Deal or No Deal? Presented by Maggie Mac, CPC, CEMC, CHC, CMM, ICCE and Dennis Mihale, MD Documentation Guidelines 1995 vs 1997 guidelines 95 for? 97 for? General Multi-System? Specialty
LaTrece Freeman-Baker, CPC, CPC-I, CPCO, CPMA
 HFS Billing and Coding Guidance for Pediatric Obesity Prevention & Management Improving the Quality of Care for Prevention and Treatment of Childhood Obesity LaTrece Freeman-Baker, CPC, CPC-I, CPCO, CPMA
HFS Billing and Coding Guidance for Pediatric Obesity Prevention & Management Improving the Quality of Care for Prevention and Treatment of Childhood Obesity LaTrece Freeman-Baker, CPC, CPC-I, CPCO, CPMA
EVALUATION AND MANAGEMENT SERVICES Q&A: HOW DOES YOUR MAC INTERPRET THE GUIDELINES?
 EVALUATION AND MANAGEMENT SERVICES Q&A: HOW DOES YOUR MAC INTERPRET THE GUIDELINES? The following questions and answers were found on Medicare administrative contractors (MACs) web sites. Table cells were
EVALUATION AND MANAGEMENT SERVICES Q&A: HOW DOES YOUR MAC INTERPRET THE GUIDELINES? The following questions and answers were found on Medicare administrative contractors (MACs) web sites. Table cells were
CODING AND BILLING. Mark R. Wright, OD, FCOVD. [email protected]
 CODING AND BILLING Mark R. Wright, OD, FCOVD [email protected] 1. INTRODUCTION The purpose of this document is to help with coding common office visits. This document is not meant to be comprehensive
CODING AND BILLING Mark R. Wright, OD, FCOVD [email protected] 1. INTRODUCTION The purpose of this document is to help with coding common office visits. This document is not meant to be comprehensive
Audit Challenges with E/M Services. Webinar Subscription Access Expires December 31.
 Audit Challenges with E/M Services Questions Answers Webinar Subscription Access Expires December 31. How long can I access the on demand version? You will find that in the same instructions box you utilized
Audit Challenges with E/M Services Questions Answers Webinar Subscription Access Expires December 31. How long can I access the on demand version? You will find that in the same instructions box you utilized
Hospital Coding Making the Rounds
 Hospital Coding Making the Rounds Initial & Subsequent Care, Consults, Discharges, Observation and Critical Care Objectives Participants will be educated on the documentation requirements for Initial and
Hospital Coding Making the Rounds Initial & Subsequent Care, Consults, Discharges, Observation and Critical Care Objectives Participants will be educated on the documentation requirements for Initial and
Does Your EMR Lead You to the Right Code? Amy Dunatov, MPH, FACMPE, CCS-P, ICDCT-CM April 29, 2015
 Does Your EMR Lead You to the Right Code? Amy Dunatov, MPH, FACMPE, CCS-P, ICDCT-CM April 29, 2015 Disclosure Information National Urgent Care Convention April 2015 Amy C. Dunatov, MPH, FACMPE, CCS-P,
Does Your EMR Lead You to the Right Code? Amy Dunatov, MPH, FACMPE, CCS-P, ICDCT-CM April 29, 2015 Disclosure Information National Urgent Care Convention April 2015 Amy C. Dunatov, MPH, FACMPE, CCS-P,
BILLING AND CODING UPDATE 2013
 BILLING AND CODING UPDATE 2013 IDSA Webinar February, 2013 Barb Pierce, CCS-P, ACS-EM Barb Pierce Coding and Consulting, Inc. [email protected] www.barbpiercecodingandconsulting.com OVERVIEW CPT
BILLING AND CODING UPDATE 2013 IDSA Webinar February, 2013 Barb Pierce, CCS-P, ACS-EM Barb Pierce Coding and Consulting, Inc. [email protected] www.barbpiercecodingandconsulting.com OVERVIEW CPT
What is Coding. Basics of Coding and Billing for the Optometric Staff. Vision Plan vs. Health Insurance. Vision Plan vs.
 What is Coding Basics of Coding and Billing for the Optometric Staff A system of diagnosis and procedure codes to describe an encounter, procedure, diagnostic test, or supplies provided to a patient. Jonathan
What is Coding Basics of Coding and Billing for the Optometric Staff A system of diagnosis and procedure codes to describe an encounter, procedure, diagnostic test, or supplies provided to a patient. Jonathan
CPT Coding Changes for 2013
 CPT Coding Changes for 2013 Getting Prepared Presenter Ronald Burd, MD Psychiatrist, Stanford Health, Fargo, ND Chair, APA Committee on Codes, RBRVS and Reimbursements APA Representative, AMA s RBRVS Update
CPT Coding Changes for 2013 Getting Prepared Presenter Ronald Burd, MD Psychiatrist, Stanford Health, Fargo, ND Chair, APA Committee on Codes, RBRVS and Reimbursements APA Representative, AMA s RBRVS Update
HCIM ICD-10 Training Online Course Catalog August 2015
 HCIM ICD-10 Training Online Course Catalog August 2015 Course/Content Duration Quiz Duration CME Credits Assessments: Assessment: Provider - Baseline - E/M Emergency Department 45 5/1/2015 Assessment:
HCIM ICD-10 Training Online Course Catalog August 2015 Course/Content Duration Quiz Duration CME Credits Assessments: Assessment: Provider - Baseline - E/M Emergency Department 45 5/1/2015 Assessment:
Rational Physician Coding for Emergency Department E/M Services and Critical Care
 Rational Physician Coding for Emergency Department E/M Services and Critical Care Peter R. Jensen, MD, CPC www.emuniversity.com Rational Physician Coding for Emergency E/M Services Peter R. Jensen, MD,
Rational Physician Coding for Emergency Department E/M Services and Critical Care Peter R. Jensen, MD, CPC www.emuniversity.com Rational Physician Coding for Emergency E/M Services Peter R. Jensen, MD,
EMR Documentation The Risks and Rewards. Agenda
 EMR Documentation The Risks and Rewards Shellie Sulzberger, LPN, CPC Coding & Compliance Initiatives, Inc. Agenda Outline potential compliance issues related to documentation with an electronic medical
EMR Documentation The Risks and Rewards Shellie Sulzberger, LPN, CPC Coding & Compliance Initiatives, Inc. Agenda Outline potential compliance issues related to documentation with an electronic medical
AHS s Headache Coding Corner A user-friendly guide to CPT and ICD coding
 AHS s Headache Coding Corner A user-friendly guide to CPT and ICD coding Stuart Black, MD Part 3 - Medical Decision Making (MDM) coding in Headache As stated in the CPT codebook, the classification of
AHS s Headache Coding Corner A user-friendly guide to CPT and ICD coding Stuart Black, MD Part 3 - Medical Decision Making (MDM) coding in Headache As stated in the CPT codebook, the classification of
Understanding Optometric Visit Coding. Ronald J Purnell MBA COE OCS
 Understanding Optometric Visit Coding Ronald J Purnell MBA COE OCS Ron BA, MBA, COE, OCS Optometric, ophthalmic work history Experience in almost every area Front office, phones, check in/check out Back
Understanding Optometric Visit Coding Ronald J Purnell MBA COE OCS Ron BA, MBA, COE, OCS Optometric, ophthalmic work history Experience in almost every area Front office, phones, check in/check out Back
Importance of Auditing
 Medicare 201: Practitioner Importance of Auditing EY Fraud Investigation and Dispute Services Jennifer Shimek, Senior Manager Gretchen Segado, Manager Agenda Importance of Auditing National and Local Coding
Medicare 201: Practitioner Importance of Auditing EY Fraud Investigation and Dispute Services Jennifer Shimek, Senior Manager Gretchen Segado, Manager Agenda Importance of Auditing National and Local Coding
Evaluation & Management Coding Category Selection Individual Exercises
 Evaluation & Management Coding Category Selection Individual Exercises Note: Unless otherwise stated, each problem is intended to be independent of the preceding problems. Do not assume that any facts
Evaluation & Management Coding Category Selection Individual Exercises Note: Unless otherwise stated, each problem is intended to be independent of the preceding problems. Do not assume that any facts
Maximizing Third Party Reimbursement Through Enhanced Medical Documentation and Coding
 National Center for Health Care Capacity Building Maximizing Third Party Reimbursement Through Enhanced Medical Documentation and Coding March 2014 2 TABLE OF CONTENTS Acronyms Used 3 Current Procedural
National Center for Health Care Capacity Building Maximizing Third Party Reimbursement Through Enhanced Medical Documentation and Coding March 2014 2 TABLE OF CONTENTS Acronyms Used 3 Current Procedural
Coding and Documentation in Practice
 Coding and Documentation in Practice Great Exam Documentation By: Kathy Mills Chang Kathy Mills Chang is a Certified Medical Compliance Expert, Reimbursement Consultant, Medicare Specialist, and a Documentation
Coding and Documentation in Practice Great Exam Documentation By: Kathy Mills Chang Kathy Mills Chang is a Certified Medical Compliance Expert, Reimbursement Consultant, Medicare Specialist, and a Documentation
Coding and Documentation How to Avoid Common Coding Mistakes
 Coding and Documentation How to Avoid Common Coding Mistakes Linda Gates-Striby CCS-P, ACS-CA Linda Gates-Striby has worked in the medical field for over 30 years. She has specialized in cardiology for
Coding and Documentation How to Avoid Common Coding Mistakes Linda Gates-Striby CCS-P, ACS-CA Linda Gates-Striby has worked in the medical field for over 30 years. She has specialized in cardiology for
www.healthhiv.org Maximizing Third Party Reimbursement Through Enhanced Medical Documentation and Coding
 www.healthhiv.org Maximizing Third Party Reimbursement Through Enhanced Medical Documentation and Coding Desk Reference March 2014 2 TABLE OF CONTENTS Acronyms Used 3 Current Procedural Terminology Coding
www.healthhiv.org Maximizing Third Party Reimbursement Through Enhanced Medical Documentation and Coding Desk Reference March 2014 2 TABLE OF CONTENTS Acronyms Used 3 Current Procedural Terminology Coding
Pediatric and Binocular Vision Examination and Billing Protocols
 Pediatric and Binocular Vision Examination and Billing Protocols Recommended Eye Examination Frequency for the Pediatric Patient... 3 Routine Comprehensive Pediatric Eye Examination... 4 Billing for Pediatric
Pediatric and Binocular Vision Examination and Billing Protocols Recommended Eye Examination Frequency for the Pediatric Patient... 3 Routine Comprehensive Pediatric Eye Examination... 4 Billing for Pediatric
My Little Book of Inpatient Billing & Coding
 My Little Book of Inpatient Billing & Coding I Read this carefully before you proceed Medical necessity should always guide your level of coding Disclaimer Read and use at your own risk, I am a family
My Little Book of Inpatient Billing & Coding I Read this carefully before you proceed Medical necessity should always guide your level of coding Disclaimer Read and use at your own risk, I am a family
Introduction. Procedure
 Page 1 of 8 Training Guide Clinical Evaluation Criteria for Technical Services TRAINING GUIDE FOR USE OF CLINIC EVALUATION & MANAGEMENT (E&M) CRITERIA FOR TECHNICAL CHARGES Introduction The following guidelines
Page 1 of 8 Training Guide Clinical Evaluation Criteria for Technical Services TRAINING GUIDE FOR USE OF CLINIC EVALUATION & MANAGEMENT (E&M) CRITERIA FOR TECHNICAL CHARGES Introduction The following guidelines
JOB DESCRIPTION NURSE PRACTITIONER
 JOB DESCRIPTION NURSE PRACTITIONER Related documents: Nurse Practitioner Process Protocol Authorization for Individuals to Provide Services as Allied Health Personnel in the LPCH/SCH Administrative Manual
JOB DESCRIPTION NURSE PRACTITIONER Related documents: Nurse Practitioner Process Protocol Authorization for Individuals to Provide Services as Allied Health Personnel in the LPCH/SCH Administrative Manual
MEDICAL CENTER POLICY NO. 0094. A. SUBJECT: Documentation of Patient Care (Electronic Medical Record)
") Clinical Staff Executive Committee MEDICAL CENTER POLICY NO. 0094 A. SUBJECT: Documentation of Patient Care (Electronic Medical Record) B. EFFECTIVE DATE: April 1, 2012 (R) C. POLICY: The University of
Clinical Staff Executive Committee MEDICAL CENTER POLICY NO. 0094 A. SUBJECT: Documentation of Patient Care (Electronic Medical Record) B. EFFECTIVE DATE: April 1, 2012 (R) C. POLICY: The University of
KINDRED HEALTHCARE. Billing & Coding for SNF Physician Visits. KINDRED HEALTHCARE Continue the Care
 KINDRED HEALTHCARE Billing & Coding for SNF Physician Visits KINDRED HEALTHCARE Continue the Care 1 SNF CPT Codes Initial Care Services 99304 99305 99306 Subsequent Care Services 99307 99308 99309 99310
KINDRED HEALTHCARE Billing & Coding for SNF Physician Visits KINDRED HEALTHCARE Continue the Care 1 SNF CPT Codes Initial Care Services 99304 99305 99306 Subsequent Care Services 99307 99308 99309 99310
Medical Records Analysis
 Medical Records Analysis Karen A. Mulroy, Partner Evans & Dixon, L.L.C. The analysis of medical legal issues posed in any case can be complicated, requiring some close reading and detective work to both
Medical Records Analysis Karen A. Mulroy, Partner Evans & Dixon, L.L.C. The analysis of medical legal issues posed in any case can be complicated, requiring some close reading and detective work to both
Examination Content Blueprint
 Examination Content Blueprint Overview The material on NCCPA s certification and recertification exams can be organized in two dimensions: (1) organ systems and the diseases, disorders and medical assessments
Examination Content Blueprint Overview The material on NCCPA s certification and recertification exams can be organized in two dimensions: (1) organ systems and the diseases, disorders and medical assessments
How To Write A Code Of Conduct
 Disclosures Behavioral Health Coding, Contracting and Billing, Part 1 Presented by Mimi Reed, BHSA, CPC A, MCP, MTA, Consultant, SCHA MI Mimi Reed, BHSA, CPC A, MCP, MTA, Consultant, SCHA MI Amy Valimont,
Disclosures Behavioral Health Coding, Contracting and Billing, Part 1 Presented by Mimi Reed, BHSA, CPC A, MCP, MTA, Consultant, SCHA MI Mimi Reed, BHSA, CPC A, MCP, MTA, Consultant, SCHA MI Amy Valimont,
School Based Health Care Coding at Your Best
 School Based Health Care Coding at Your Best Presented by Carley Spangler, CPC Account Manager, OCHIN Billing Services October 2011 OCHIN 707 SW Washington Suite 1200 Portland, OR 97205 P 503-943-2500
School Based Health Care Coding at Your Best Presented by Carley Spangler, CPC Account Manager, OCHIN Billing Services October 2011 OCHIN 707 SW Washington Suite 1200 Portland, OR 97205 P 503-943-2500